optimizing pain relief while reducing risk: finding your comfort zone colleen o’connell, md frcpc
TRANSCRIPT

Optimizing Pain Relief While Reducing Risk: Finding Your Comfort Zone
COLLEEN O’CONNELL, MD FRCPC
Faculty/Presenter Disclosure
• Faculty: Colleen O’Connell, MD FRCPC
• Relationships with commercial interests:– Grants/Research Support: industry-sponsored research by
Acorda, Allergan, Biogen, Cytokinetics, Eli-Lilly, Xenoport– Speakers Bureau/Honoraria: Allergan, Biogen, Boehringer,
Eli Lilly, Pfizer, Purdue Pharma, Valeant– Consulting Fees: Allergan, Biogen, Prairie Plant
Disclosure of Commercial Support
• This program has received financial support and in-kind support from Purdue Pharma in the forms of an educational grant and logistical support
• Potential for conflict(s) of interest:– The Speaker has received payment from Purdue Pharma– Purdue Pharma developed and distributes, and benefits from the sale of
products that will be discussed in this program:• Buprenorphine transdermal (BuTrans®)• Codeine monohydrate (Codeine Contin®)• Hydromorphone hydrochloride (DILAUDID®, HYDROMORPH CONTIN®)• Morphine sulfate (MS Contin®, MS•IR®)• Oxycodone Hydrochloride (Oxy•IR®, OxyNEO®)• Oxycodone Hydrochloride / Naloxone Hydrochloride (Targin®)• Tramadol hydrochloride (Zytram XL®)

Mitigating Potential Bias
Potential sources of bias identified in the preceding 2 slides have been mitigated as follows:• Information/recommendations provided in the following
program will be evidence- and/or guideline-based and opinions of the speaker will be identified as such.
• Material was developed and reviewed by a steering committee composed of independent third party experts responsible for vetting the program’s needs assessment and subsequent content development to ensure accuracy and fair balance.

Disclaimer
This presentation is for educational purposes only. It was developed by an independent team of subject-matter experts convened for this purpose.
The opinions expressed in this presentation are not necessarily those of the sponsor, and neither product descriptions nor opinions should be attributed to the sponsor.
The sponsor does not recommend any use of its products that is inconsistent with the product monographs of such products.

Question #1
What is your #1 barrier in dealing with CNCP patients1. Having enough time to do it properly2. Knowing what the proper outcomes are to measure3. Fear of the College4. Fear of creating Addiction 5. Fear of having opioids be diverted6. Fear of the patient overdosing on opioids
Issues in the Management of Chronic Non-cancer Pain
• Results from 2012 needs assessment of 403 primary care physicians:– Uncertainty with regard to assessment of chronic
non-cancer pain (CNCP)– Uncertainty with regard to effective treatment of
chronic pain– Potential for opioid addiction and misuse– Prior negative experiences effectively managing patients
with CNCP

Learning Objectives
After attending this program, participants should be able to:• Recognize the trajectory/continuum of
chronic non-cancer pain (CNCP)• Define an essential pain assessment
strategy• Break down barriers related to the use
of non-pharmacological, non-opioid, and opioid treatment options for CNCP
• Discuss “success” in the management of CNCP

Patient Case: Julie
• 43-year-old female• Executive secretary, mother
of 2• Breast cancer: treated with
mastectomy and chemotherapy
• Chemotherapy-induced peripheral neuropathy and myalgia x 4 years
Does Julie have chronic pain?

Definition of Chronic Non-cancer Pain
• An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage
• Pain without apparent biological value that has persisted beyond the normal tissue healing time (most commonly reported to be ≤3 months)
International Association for the Study of Pain. 2012.
Overlapping Aspects of Chronic Pain
Biological
SocialPsychological
PAIN

MIXED
Categorizing Chronic Non-cancer Pain
Superficial
Deep
Central
Peripheral
Other
NEUROPATHIC
NOCICEPTIVE(Inflammatory)
Visceral
Somatic
Ashby MA, et al. Pain. 1992;51:153-161.Nicholson B. Am J Managed Care. 2006;12:S256-S262.
Ballantyne JC. Oncologist. 2003;8:567-575.
Question #2
What would you want to accomplish in this pain assessment visit? 1. A measurement of pain severity 2. A differential diagnosis of her pain condition 3. A measurement of her addiction risk 4. A measurement of her functionality 5. All of the above

Pain Assessment: OPQRS
• Onset (and evolution)
• Pattern
• Quality
• Relieving / exacerbating factors
• SeverityAssessment tools:Brief Pain InventoryBody Pain DiagramLANSS / DN4
DN4, Douleur Neuropathique 4.LANSS, Leeds Assessment of Neuropathic Symptoms and Signs.
Pain Assessment: OPQRS
• Onset (and evolution)– Spontaneous or event-triggered?– Work / motor vehicle accident?– Illness / iatrogenic (post-surgical)?– Evolution of pain problem over time
Pain Assessment: OPQRS
• Pattern:– Number and location of different pains– Location (localized or radiating)– Timing (intermittent, constant, breakthrough)– Rapidly progressive or stable

Pain Assessment: OPQRS
• Quality:– Neuropathic pain:
• Burning, shooting, lancinating, tingling, pins and needles
– Nociceptive pain:• Somatic pain: aching, sharp, localized, increased by activity,
relieved by rest• Visceral pain: dull, crampy, diffuse
Pain Assessment: OPQRS
• Relieving / exacerbating factors– Movement / rest / specific positions– Physical measures (heat, cold, massage)– Anxiety / stress– Lack of sleep– Weather / seasonal
Pain Assessment: OPQRS
• Severity– Patient self-report is the best measure we have today to
assess pain severity– Descriptive, numeric and analog pain rating scales are
available– Most common measure is the “0 – 10” verbal rating
scale (VRS)
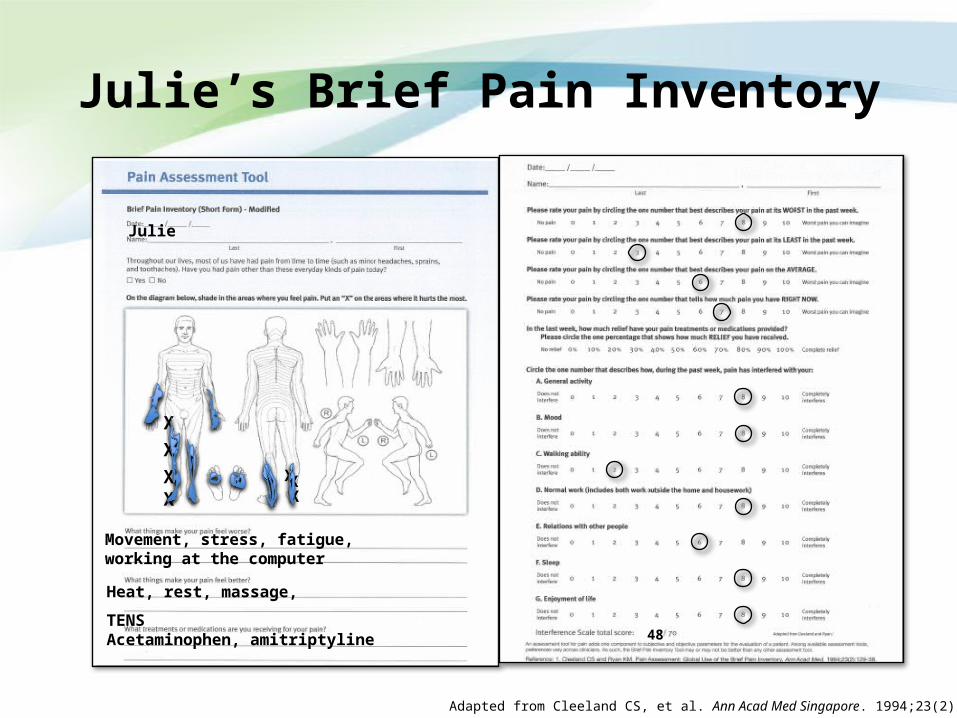
Julie’s Brief Pain Inventory
Julie
Movement, stress, fatigue, working at the computer
Heat, rest, massage, TENS
Acetaminophen, amitriptyline
Adapted from Cleeland CS, et al. Ann Acad Med Singapore. 1994;23(2):129-38.
XX
X
48
X
X
X X

Question #3
What type of pain is likely affecting Julie?1. Nociceptive 2. Neuropathic 3. Mixed

Julie’s Diagnosis
• Neuropathic pain• Possible nociceptive
elements• Sequelae of peripheral
neuropathy; potential impact of deconditioning
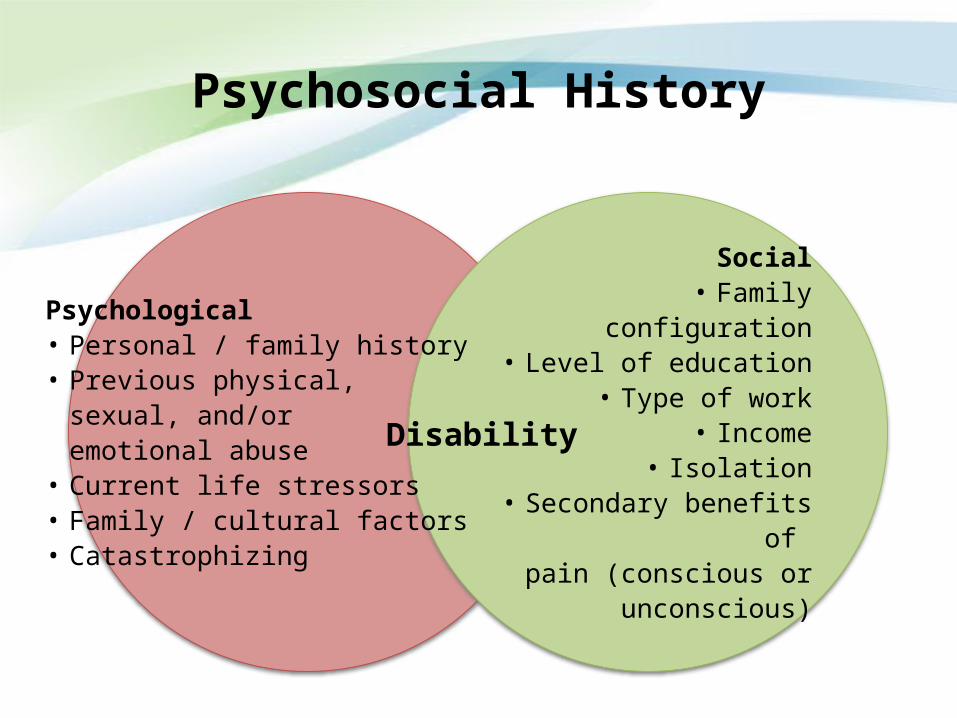
Psychosocial History
Psychological• Personal / family history • Previous physical,
sexual, and/or emotional abuse
• Current life stressors• Family / cultural factors• Catastrophizing
Social• Family configuration
• Level of education• Type of work
• Income• Isolation
• Secondary benefits of pain (conscious or
unconscious)
Disability
Physical Exam in Chronic Non-cancer Pain
• General exam – posture, muscular tone
• Spinal exam – mobility, palpation, look for trigger points
• Neurological exam – motor strength, reflexes, sensory exam (including presence of allodynia, hyperalgesia, hypo- or hyperesthesia)
• Inflammatory elements – pain, swelling, erythema

Question #4
Would you order imaging for Julie?
1. Yes, I always order imaging in all of my pain patients 2. No, I only order imaging if there are obvious signs of
serious pathology 3. Possible, I treat each case on an individual basis

Non-pharmacologic Treatment Options
Type of treatment Options
Lifestyle Cessation of tobacco products, weight loss, nutritional counselling
Physical Heat, cold, massage, exercise, manipulation, physical therapy, stretching and yoga, surgical therapies (nerve blocks, trigger point injections, spinal infusion, or stimulation), transcutaneous electric nerve stimulation, intramuscular stimulation, radiofrequency lesioning
Psychological/psychiatric Biofeedback, cognitive behaviour therapy, counselling, social worker support, hypnosis, relaxation
Occupational Occupational therapy, work conditioning programs
Complementary/alternative Acupuncture, herbal remedies, massage, mindfulness meditation, reflexology
Jackman RP, et al. Am Fam Physician. 2008;78(10):1155-62.

Pharmacologic Treatment Options: Non-opioid Analgesics
• Acetaminophen• NSAIDs – topical vs. systemic• Salicylates• Muscle relaxants• Tricyclic antidepressants (TCAs)• SNRIs• Gabapentenoids/anticonvulsants• Cannabinoids
?National Opioid Use Guideline Group (NOUGG), 2010.Moulin DE, et al. Pain Res Manage. 2007;12(1):13-21.
NSAID, non-steroidal anti-inflammatory drug.SNRI, serotonin noradrenaline reuptake inhibitors.
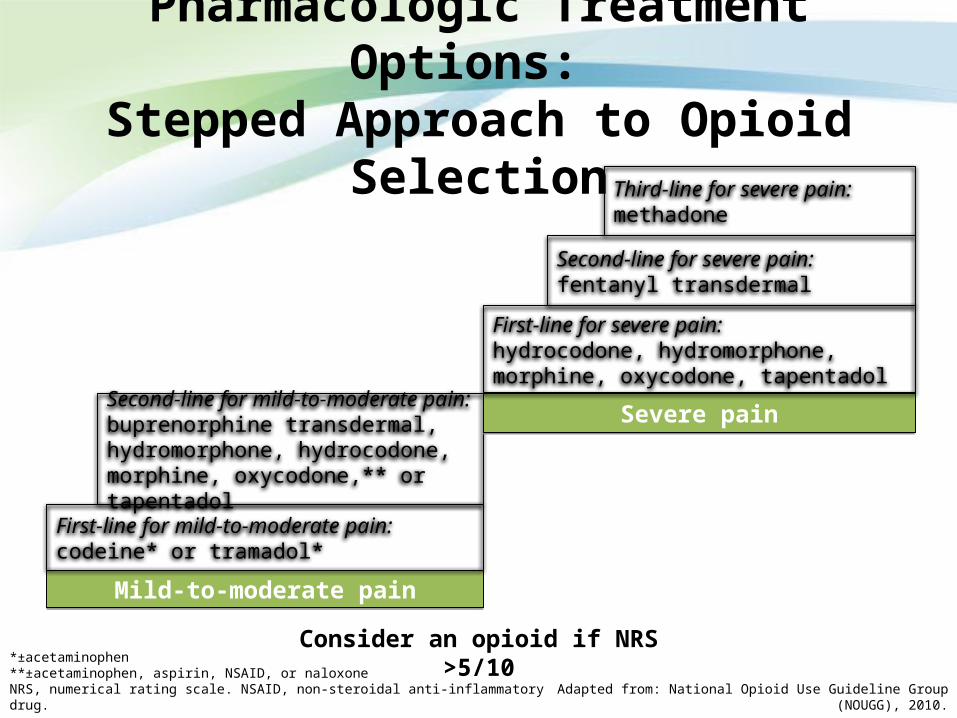
Pharmacologic Treatment Options: Stepped Approach to Opioid Selection
Mild-to-moderate painMild-to-moderate pain
First-line for mild-to-moderate pain:codeine* or tramadol*
Second-line for mild-to-moderate pain:buprenorphine transdermal, hydromorphone, hydrocodone, morphine, oxycodone,** or tapentadol
Severe painSevere pain
First-line for severe pain:hydrocodone, hydromorphone, morphine, oxycodone, tapentadol
Second-line for severe pain:fentanyl transdermal
Third-line for severe pain:methadone
Adapted from: National Opioid Use Guideline Group (NOUGG), 2010.
Consider an opioid if NRS >5/10*±acetaminophen**±acetaminophen, aspirin, NSAID, or naloxoneNRS, numerical rating scale. NSAID, non-steroidal anti-inflammatory drug.

Pharmacologic Treatment Options: Chronic Neuropathic Pain
Moulin DE, et al. Pain Res Manage. 2007;12(1):13-21.
TCA gabapentin or pregabalin
SNRI topical lidocaine*
tramadol or controlled-release opioid analgesic
fourth-line agents†
*5% gel or cream – useful for focal neuropathy such as postherpetic neuralgia.†Cannabinoids, methadone, lamotrigine, topiramate, valproic acid.‡Do not add SNRIs to TCAs.SNRI, serotonin noradrenaline reuptake inhibitors. TCA, tricyclic antidepressants.
Add additional agents sequentially
if partial butinadequate pain
relief‡
Question #5
What are my goals for this patient?1. Cure2. Complete pain relief3. Complete restoration of her function4. 75% relief in her pain by next visit5. Realistic improvement in her functionality
Patient’s Goals of Treatment
• Set SMART goals at each visit:– Specific– Measurable– Action-oriented / Achievable– Realistic / Relevant– Time-dependent goals
• Think of opioid prescribing as a test or trial
Walk through the park 2X / week
Take 2-hour car trip to visit mom
Try out a rehab yoga class

Cautions With The Use of Opioids
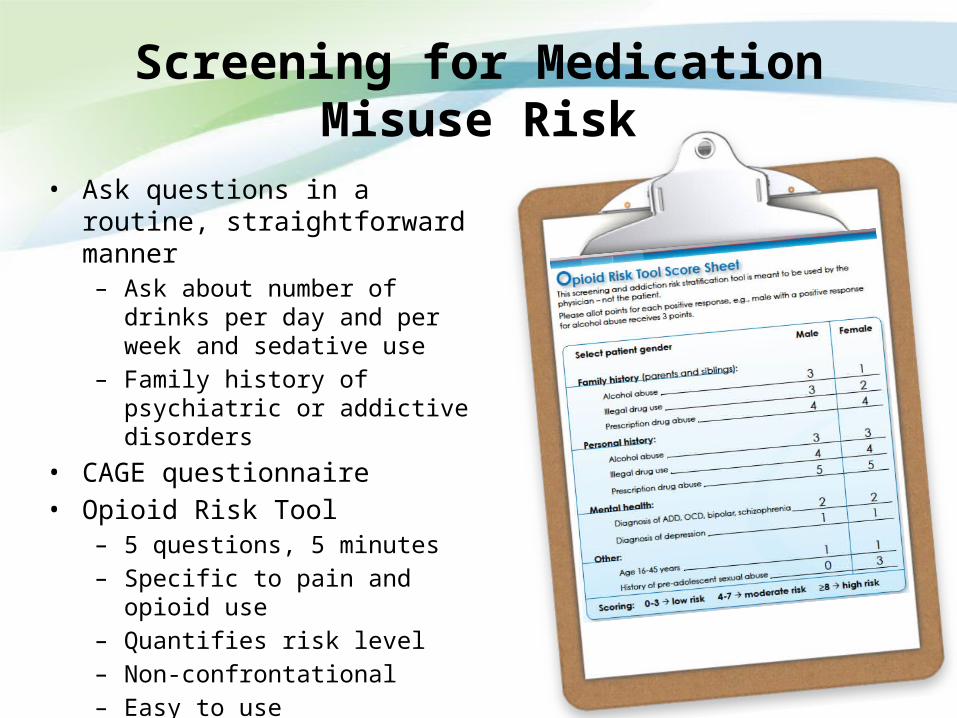
Screening for Medication Misuse Risk
• Ask questions in a routine, straightforward manner– Ask about number of drinks per day
and per week and sedative use– Family history of psychiatric or
addictive disorders• CAGE questionnaire• Opioid Risk Tool
– 5 questions, 5 minutes– Specific to pain and opioid use– Quantifies risk level– Non-confrontational– Easy to use

Opioid Risk Tool
Adapted from: Webster LR, et al. Pain Med. 2005;6:432-42.
X
XX
5

Incorporating Risk Level of Misuse/Addiction into Pain Management
Most patients
Fewest patients
Risk
leve
l
Group III – Preferably treat by addiction medicine• Methadone or Buprenorphine is 1st choice• Exhaust all other options before considering opioids • Daily dispensing weekly, less “abusable” meds
Group II – Trial of treatment by primary care physician with collaboration with Pain doctor(if available) • More assessment and focus on functional goals• Written Treatment Agreement, urine drug test 3-4 times per year, collateral
information. Be prepared for contingency plan• Follow-up monthly, dispense every 2 weeks, choose opioids carefully
Group I – Treatment by primary care physician• Utilize all treatment options, including opioids; focus on side effects• Written Treatment Agreement, urine drug test 1-2 times per year• Follow-up every 2-3 months, dispense meds every 4 weeks
Questions When Initiating Opioid Therapy
Initial choice of opioid?Dose?Route of administration?Frequency?Monitoring and follow up?
Safety? Adverse effects?

Initiating Opioid Therapy
Basic considerations:• Patient age• Patient opioid exposure and
experience• Patient fears (stigma)• Caregiver and physician
attitudes, preferences, and biases
• Compliance • Convenience • Cost/coverage
Pharmaco-clinical considerations:• Patient
sensitivities/allergies• Administration and
absorption limitations• Metabolism and clearance• Opioid profile
Fine PG. Journal of Pain. 2001.
Written Treatment Agreement
• Recommended in all guidelines
• Low-cost, low-tech strategy• Helps to demonstrate
informed consent• Effective boundary setting
tool• Must be readable,
reasonable, and have some flexibility
Fishman S, et al. J Pain Symptom Manage. 2002;24(3):335-44.Fishman S, et al. Clin J Pain. 2002;18(4 Suppl):S70-5.
Wallace LS, et al. J Pain. 2007;8(10):759-66.
TREATMENT AGREEMENTI,__________________, understand that compliance with the following guidelines is important in continuing pain treatment with Dr. __________.
I understand that I have the following responsibilities:I will take medications only at the dose and frequency prescribed.I will not increase or change medications without the approval of this doctor.I will not request opioids or any other pain medicine from physicians other than from this doctor.

FDA Issues Draft Guidance for Abuse-Deterrent Opioid Development
ABUSE-DETERRENT FORMULATIONS (ADFs) – Categorization
1. Physical/Chemical barriers– Physical barriers can prevent chewing, crushing, cutting, grating, or grinding– Chemical barriers can resist extraction of the opioid using common solvents
2. Agonist/Antagonist combinations – An opioid antagonist can be added to interfere with, reduce, or defeat the euphoria associated
with abuse 3. Aversion
– Substances can be combined to produce an unpleasant effect if the dosage form is manipulated prior to ingestion or a higher dosage than directed is used
4. Delivery System – Certain drug release designs or the method of drug delivery can offer resistance to abuse
5. Prodrug – Prodrug lacks opioid activity until transformed in the gastrointestinal tract
6. Combination – Two or more of the above methods can be combined to deter abuse
http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM334743.pdf January 2013
Novel Opioid Formulations with Potential to Reduce Abuse/Misuse
• CR morphine with a sequestered core of naltrexone– FDA approved August 2009– Voluntarily recalled from U.S. market March 2011, “leaking core” of naltrexone
• Oxycodone/Naloxone CR tablets– Health Canada NOC December 2009
• CR hydromorphone – tablet is non-deformable– Health Canada NOC November 2009; FDA approved March 2010
• CR oxycodone – reformulated (USA); CR oxycodone-resistant to crushing (Canada)– FDA approved April 2010; Health Canada NOC August 2011– FDA approved abuse-deterrent labelling April 20131
• New labelling indicates that the product has physical and chemical properties that are expected to make abuse by injection difficult and to reduce abuse via the intranasal route
• IR oxycodone – new formulation– FDA approved June 2011
• ER oxymorphone – reformulated– FDA approved December 2011– FDA denied petition that original formulation not withdrawn due to safety and efficacy
and allowed generics May 20132NOC, Notice of Compliance; CR, controlled release; ER, extended release; IR, immediate-release. 1http://www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm347857.htm; 2http://www.fda.gov/Drugs/DrugSafety/ucm351357.htm.

Titrating Opioids: Precautions
• Ideally start with immediate release opioid and switch to a long-acting preparation
• During titration, temporary drowsiness can occur• Patients should be advised not to drive or perform
potentially hazardous activities while titrating the opioid dose – until tolerance to drowsiness occurs
• Monitor for constipation– Consider prescribing a laxative at the start of treatment
• For individuals aged >70 years, start lower and go slower
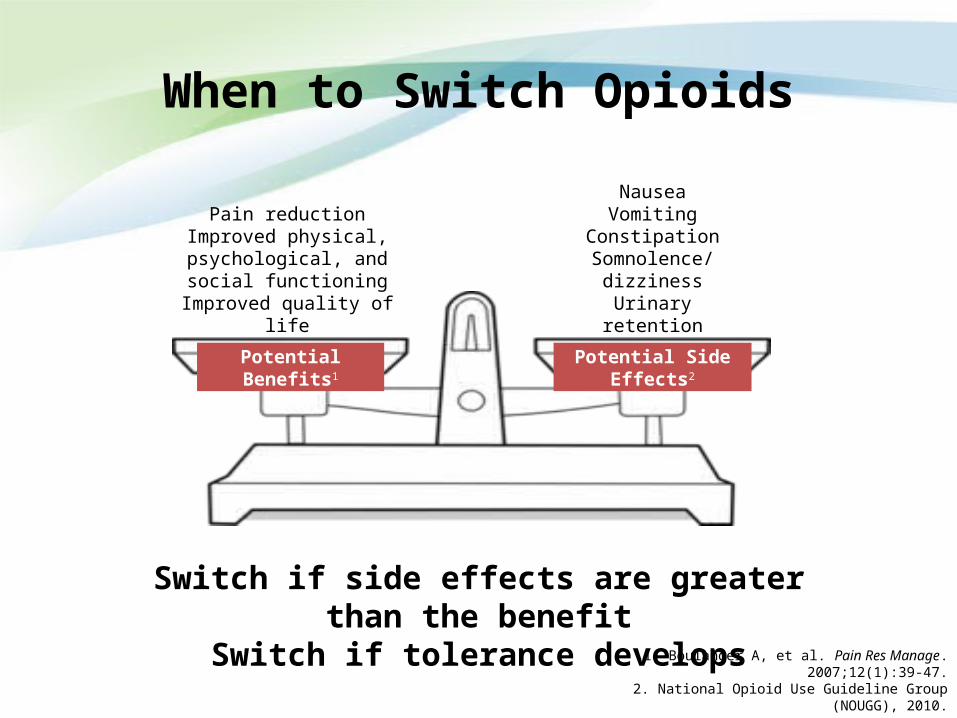
When to Switch Opioids
NauseaVomiting
ConstipationSomnolence/dizziness
Urinary retention
Pain reductionImproved physical,
psychological, and social functioning
Improved quality of life
Potential Benefits1 Potential Side Effects2
Switch if side effects are greater than the benefitSwitch if tolerance develops
1. Boulanger A, et al. Pain Res Manage. 2007;12(1):39-47.2. National Opioid Use Guideline Group (NOUGG), 2010.
How to Switch Opioids
Use opioid tables to calculate a total daily equianalgesic dose of the new opioid
1. Switch to 50-70% of the predicted dose of the new opioid and titrate to effect again– Decision to cut dose and by what percentage may depend on the
reason for switch
OR2. Start the new opioid and titrate while decreasing the dose of
the old opioid– Sustained-release morphine 15 mg ≅ controlled-release oxycodone
10 mg ≅ controlled-release hydromorphone 3 mg
Fine PG, et al. J Pain Symptom Manage. 2009;38(3):418-25.MacPherson ML. Demystifying Opioid Conversion Calculations. 2010.
Webster LR, et al. Pain Med. 2012;13(4):571-4.
When to Stop Opioid Therapy
• Resolution of underlying problem• No meaningful pain relief• Patient wants to discontinue• Does not achieve therapeutic goals even with effective pain relief
(e.g., improved physical or social functioning)• Persistent adverse effects despite careful titration and switching• Opioid hyperalgesia despite switching• Not cooperating with treatment plan (medication use or
activity/goals)• Persistent out-of-bounds behaviours consistent with
addiction/diversion– Unable to follow the treatment agreement
• Diagnosis of an addiction disorder and refuses referral for treatment
Ballantyne JC, et al. N Engl J Med. 2003;349(20):1943-53. Benyamin R, et al. Pain Physician. 2008;11(2 Suppl):S105-20. Chou R, et al. J Pain. 2009;10(2):131-46. Porreca F,
et al. Pain Med. 2009;10(4):654-62. Slatkin NE. Curr Med Res Opin. 2009;25(9):2133-50.

How To Stop Opioid Therapy
1. Discuss and document (with significant other?):– Withdrawal is not dangerous– Typical withdrawal symptoms and time course
2. Offer an alternative treatment plan3. Use caution with sedatives – withdrawal is more
risky
Patients who are diverting or addicted may refuse to comply and leave your practice

How to Stop Opioid Therapy (cont’d)
• It is not life threatening unless patient is “fragile”• Fast or slow
– 10% per day, daily pharmacy dispensing– 10% per week
• Use pharmacological aids– Clonidine, loperamide, NSAID, carbamazepine,
gabapentin, pregabalin
• Methadone (buprenorphine) taperEducating the patient is the most
effective treatment!
NSAID, non-steroidal anti-inflammatory drug.
Framing Treatment Success
• Make a plan with the patient to set goals for treatment success• Reframe success for you and the patient
– There may not be big improvements, but rather small and incremental ones (i.e., there is no “cure”)
• Reduction of pain by 30% or 2 points on scale of 0 to 10– Did the patient meet a functional goal or part of a goal?– Is the patient more positive than on previous visits?– Has there been even a small improvement in pain relief?– Has BPI scale gone down?– Has mobility improved?
• You must learn to accept situations that fail• Know when to refer to a specialist
Remember: You are treating the patient, not the pain
BPI, Brief Pain Inventory.

Essential Follow-up Documentation: The 6 As Checklist
• Analgesia (pain relief — BPI score)
• Activities (physical and psychosocial functioning — BPI interference score)
• Adverse effects (and your advice)
• Ambiguous drug-taking behaviours (and your advice)
• Accurate medication record
• Affect (use a validated scale)
Gourlay DL, et al. Pain Med. 2005;6:107-12.BPI, Brief Pain Inventory.

Making a Difference for People With Pain
• Active listening / empathy is often most important• Help patients find meaning in living a life with pain• Maintain a positive outlook / celebrate small gains• Advocate for improved pain management resources

Key Take-home Points
• Chronic pain is more than longstanding acute pain and requires a biopsychosocial approach to assessment and treatment
• Utilize a SMART goal-directed approach that focuses on functional improvement
• Search out and optimize non-pharmacological treatments in your community
• All pharmacotherapy should be prescribed using an individual risk-benefit approach
• Prescribe opioids with universal precautions according to the Canadian Opioid Guidelines
• Utilize validated clinical tools to demonstrate improved outcomes

Resources

Pain Assessment Tools
• Pain diagram• Brief Pain Inventory (BPI)• Visual Analogue Scale (VAS)• Quality of Life Scale for Pain• DN4 (Douleur Neuropathique en 4 Questions)

Opioid Risk Assessment Tools
• Opioid Risk Tool (ORT)• CAGE Questionnaire (adapted to include drugs)• Urine Drug Screening (UDS)• Screener and Opioid Assessment for Patients with Pain–
Revised (SOAPP-R)• Current Opioid Misuse Measure (COMM)• Aberrant Drug-Related Behaviours Indicative of Opioid
Misuse• Interview Guide for Alcohol Consumption • Interview Guide for Substance Use
Patient Management Tools
• The 6 As progress report• Opioid Manager (nationalpaincentre.mcmaster.ca)• Switching Opioids form (nationalpaincentre.mcmaster.ca)• Self-Management Toolkit (swselfmanagement.ca/smtoolkit/)
– The basics of helping patients better self-manage their health
• Strategies to Support Self-Management in Chronic Conditions: Collaboration with Clients (rnao.ca/bpg/guidelines/self-management)– Evidence-based practice guidelines published by the Registered
Nurses Association of Ontario

Resources for Patients
Organization
Chronic Pain Association of Canada chronicpaincanada.com
Canadian Pain Coalition canadianpaincoalition.ca
Canadian Institute for the Relief of Pain and Disability cirpd.org
Managing My Pain managingmypain.ca
Med School for You Chronic Pain Self-Management medschoolforyou.com
Arthritis Society arthritis.ca
Patients Like Me patientslikeme.com
Pain Toolkit paintoolkit.org

Provincial Resources for Patients
British Columbia
Pain BC painbc.ca
Chronic Disease Self-Management Programs selfmanagementbc.ca/chronicpainprogram
Alberta
Better Choices, Better Health albertahealthservices.ca/services.asp?pid=service&rid=1008382
People in Pain Network pipain.com
SaskatchewanLiveWell Chronic Disease Management www.saskatoonhealthregion.ca/your_health/p
s_cdm_livewell_with_chronic_conditions.htm
Manitoba
Get Better Together rha-central.mb.ca/service.php?id=65
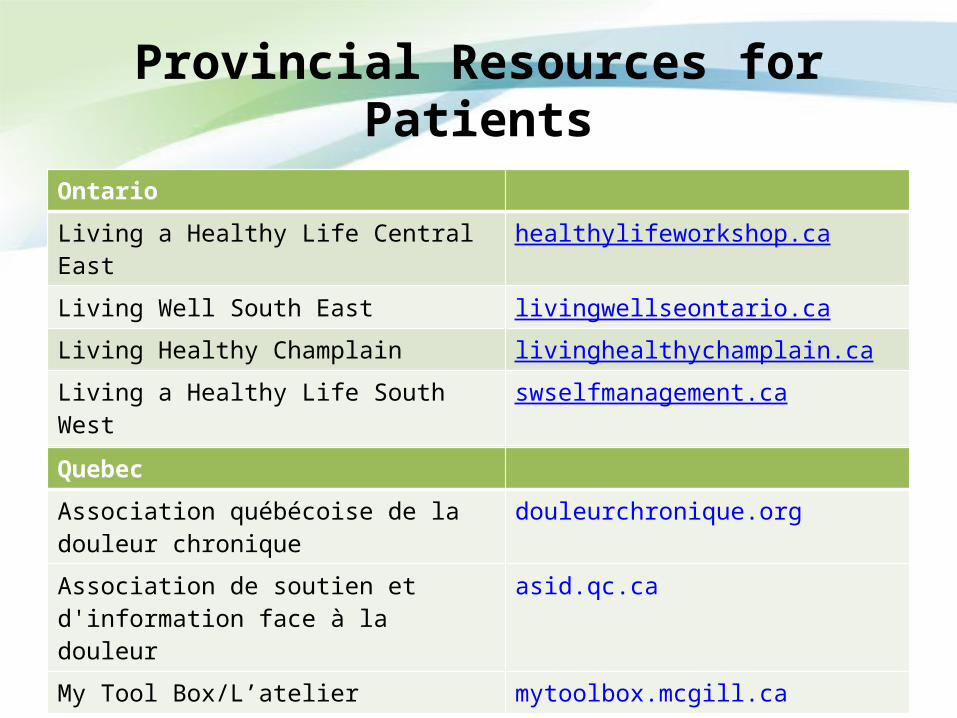
Provincial Resources for Patients
Ontario
Living a Healthy Life Central East healthylifeworkshop.ca
Living Well South East livingwellseontario.ca
Living Healthy Champlain livinghealthychamplain.ca
Living a Healthy Life South West swselfmanagement.ca
Take Control Take Charge takecontroltakecharge.ca
Healthy Change healthychange.ca
Quebec
Association québécoise de la douleur chronique
douleurchronique.org
Association de soutien et d'information face à la douleur
asid.qc.ca
My Tool Box/L’atelier mytoolbox.mcgill.ca
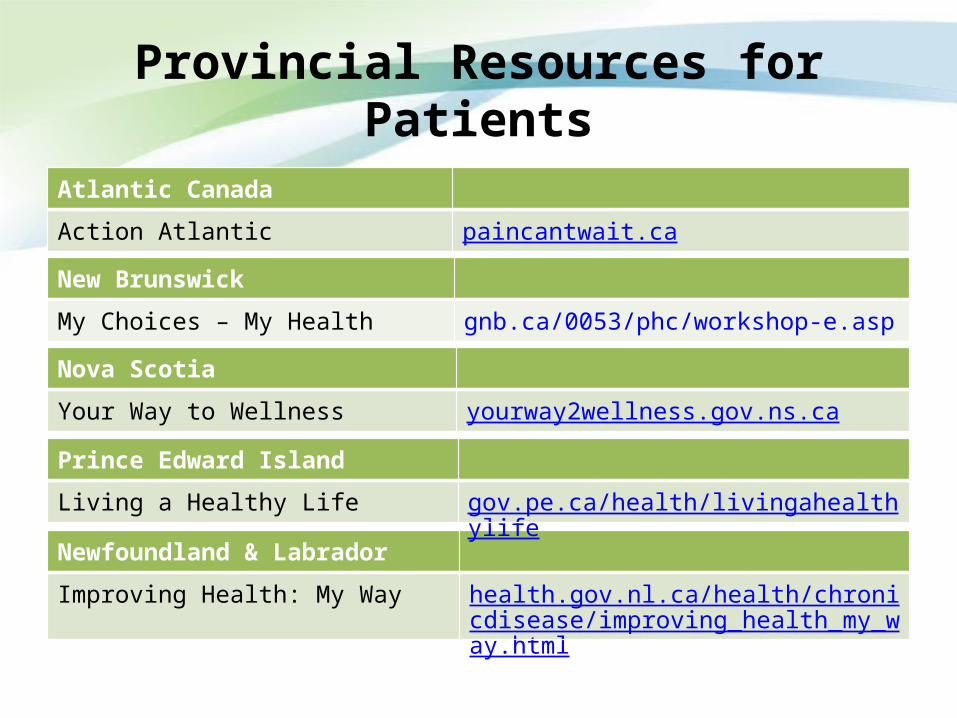
Provincial Resources for Patients
Atlantic Canada
Action Atlantic paincantwait.ca
New Brunswick
My Choices – My Health gnb.ca/0053/phc/workshop-e.asp
Nova Scotia
Your Way to Wellness yourway2wellness.gov.ns.ca
Newfoundland & Labrador
Improving Health: My Way health.gov.nl.ca/health/chronicdisease/improving_health_my_way.html
Prince Edward Island
Living a Healthy Life gov.pe.ca/health/livingahealthylife