optimizing infectious diseases outcomes in … · optimizing infectious diseases outcomes in...
TRANSCRIPT
Optimizing Infectious Diseases Outcomes in Antimicrobial Stewardship Programs
7/10/2013
1
OPTIMIZING INFECTIOUS DISEASES OUTCOMES IN ANTIMICROBIAL
STEWARDSHIP PROGRAMS(ACPE # 0072-9999-10-137-L04-P Knowledge-based)
Craig Martin, Pharm.D
UK HealthCare
University of Kentucky College of Pharmacy
DISCLOSURES
Dr. Martin has disclosed that he has received research grant funding from Pfizer.
OBJECTIVES
Discuss the importance of collaboration among healthcare professionals in the successful implementation of antimicrobial stewardship
List ways to optimize PK/PD relationships to optimize outcomes
Describe the development of evidence-based guidelines to implement clinical pathways
Optimizing Infectious Diseases Outcomes in Antimicrobial Stewardship Programs
7/10/2013
2
THE CRITICAL BALANCE
Importance of appropriate empiric therapy
Effect of broad-spectrum therapy on resistance
Infection Prevention and Antimicrobial Stewardship
Silver, L. L.. 2011. Clin. Microbiol. Rev. 24(1):71-109
THE DISCOVERY VOID
GUIDING ANTIMICROBIAL USE TENETS
For severe infections, start broad If you get it wrong, you’re in trouble
Get it in the patient quicklyDe-escalation of therapy is a necessity
The right drug is always the narrowest spectrum agent that produces a successful response and causes the fewest significant adverse effects and the least collateral damage
Treat for the most appropriate length of time, then stop Each of these can be addressed through collaborative
efforts
Optimizing Infectious Diseases Outcomes in Antimicrobial Stewardship Programs
7/10/2013
3
ANTIMICROBIAL STEWARDSHIP GUIDELINES: A SUMMARY
Multidisciplinary problem which cannot be solved unilaterally Core Members
ID Physician
ID trained Pharmacist
Additional members
Microbiologist
IT Specialist
IC Professional and/or Epidemiologist
Collaborative Antimicrobial Stewardship
Infection Control
Microbiology
ID Pharmacy and Medicine
Dellit, et al. CID 2007.
ANTIMICROBIAL STEWARDSHIP GUIDELINES
Core Strategies Prospective audit with intervention and feedback
Formulary restriction with preauthorization
Supplemental Strategies Education
Guidelines and clinical pathways
Antimicrobial cycling
Antimicrobial order forms
Combination therapy
Streamlining or de-escalation of therapy
Dose optimization
Parenteral to oral conversion
Dellit, et al. CID 2007.
UK HEALTHCARE ANTIMICROBIAL STEWARDSHIP: COLLABORATIVE EFFORTS
Pharmacist leads an Infection Control rounding team
Microbiology pages pharmacy and IC with MDR pathogen result
Microbiology obtains PNA FISH capability to decrease echinocandin use (and pages pharmacy with result)
Pharmacy reviews Microbiology antibiogram prior to publishing
Microbiology consults pharmacy for “selective” susceptibility reporting and panel purchasing
Pharmacy assists IC in handwashing surveillance
Antimicrobial subcommittee includes all 3 groups, in addition to others
Optimizing Infectious Diseases Outcomes in Antimicrobial Stewardship Programs
7/10/2013
4
CURRENT AND RECENT INITIATIVES
SCT/Leukemia Antifungal Guidelines Promote posaconazole for prophylaxis for some patients
Restrict combination therapy
Outline indications for all antifungals
Intraabdominal Infections Guidelines
Candidiasis Guidelines
MOVING FROM “RESTRICTION” TO “FACILITATION”
Martin CA, Armitstead JA, Mynatt RP, and Hoven AD AJHP2011; 68:109-10. Programs with a heavy-handed restriction approach may
inadvertently be doing a disservice to patients
We should be focusing more on getting the right drug to the patient rather than merely restricting drugs
The only dose of a drug proven to save lives is THE FIRST ONE
IMPROVING OUTCOMES THROUGH THOUGHTFUL DOSING AND ADMINISTRATION
Well known that maximizing the benefit of a drug requires maximizing the pharmacodynamic properties of the drug
HOWEVER, with low MIC isolates, it’s not as crucial
Previously, we always had other drugs we could use
With the lack of new drugs for MDR organisms, being strategic with dosing and administration is more important than ever
Optimizing Infectious Diseases Outcomes in Antimicrobial Stewardship Programs
7/10/2013
5
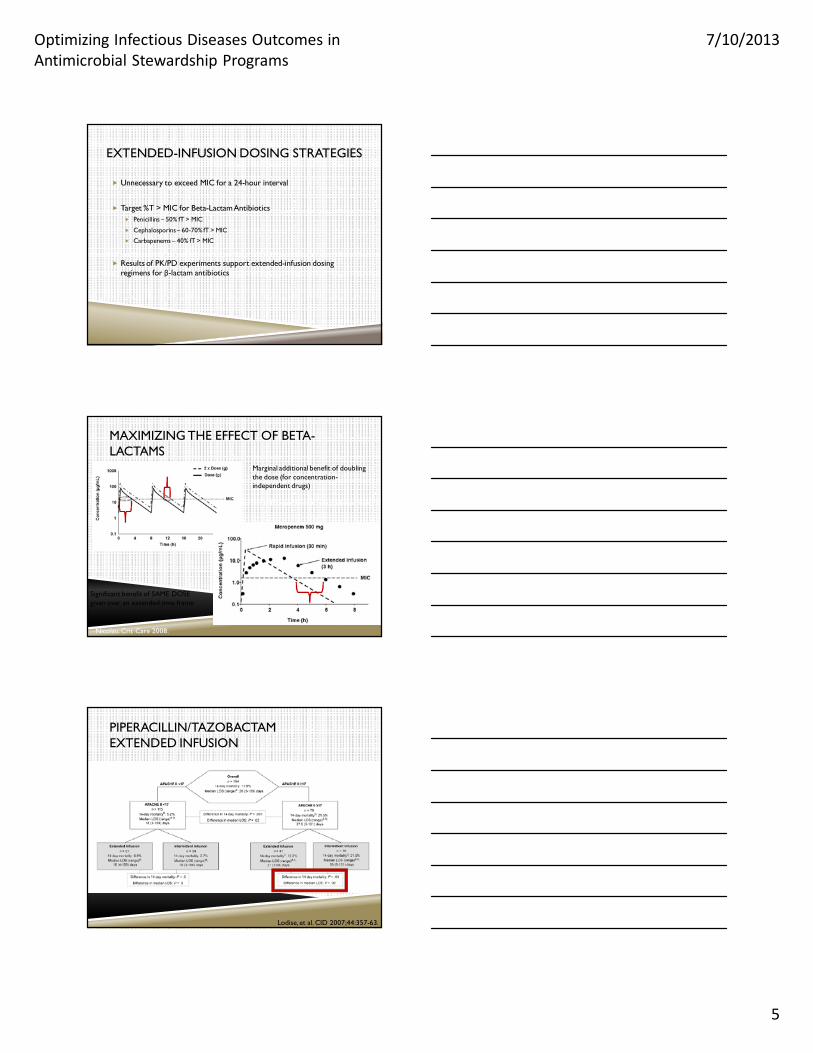
EXTENDED-INFUSION DOSING STRATEGIES
Unnecessary to exceed MIC for a 24-hour interval
Target %T > MIC for Beta-Lactam Antibiotics Penicillins – 50% fT > MIC
Cephalosporins – 60-70% fT > MIC
Carbapenems – 40% fT > MIC
Results of PK/PD experiments support extended-infusion dosing regimens for β-lactam antibiotics
MAXIMIZING THE EFFECT OF BETA-LACTAMS
Nicolau. Crit Care 2008.
Marginal additional benefit of doubling the dose (for concentration-independent drugs)
Significant benefit of SAME DOSE given over an extended time frame
PIPERACILLIN/TAZOBACTAMEXTENDED INFUSION
Lodise, et al. CID 2007;44:357-63.
Optimizing Infectious Diseases Outcomes in Antimicrobial Stewardship Programs
7/10/2013
6
DORIPENEM EXTENDED INFUSION
Doripenem vs. imipenem for VAP
Patients stratified Duration of mechanical ventilation (<5 vs>5 days)
APACHE (<15 vs>15)
Geography
Randomization Doripenem 500mg every 8h over 4 hours
Imipenem 500mg every 6 hours or 1000mg every 8 hours via 30 or 60min infusion
Chastre, et al. Crit Care Med 2008;36(4)
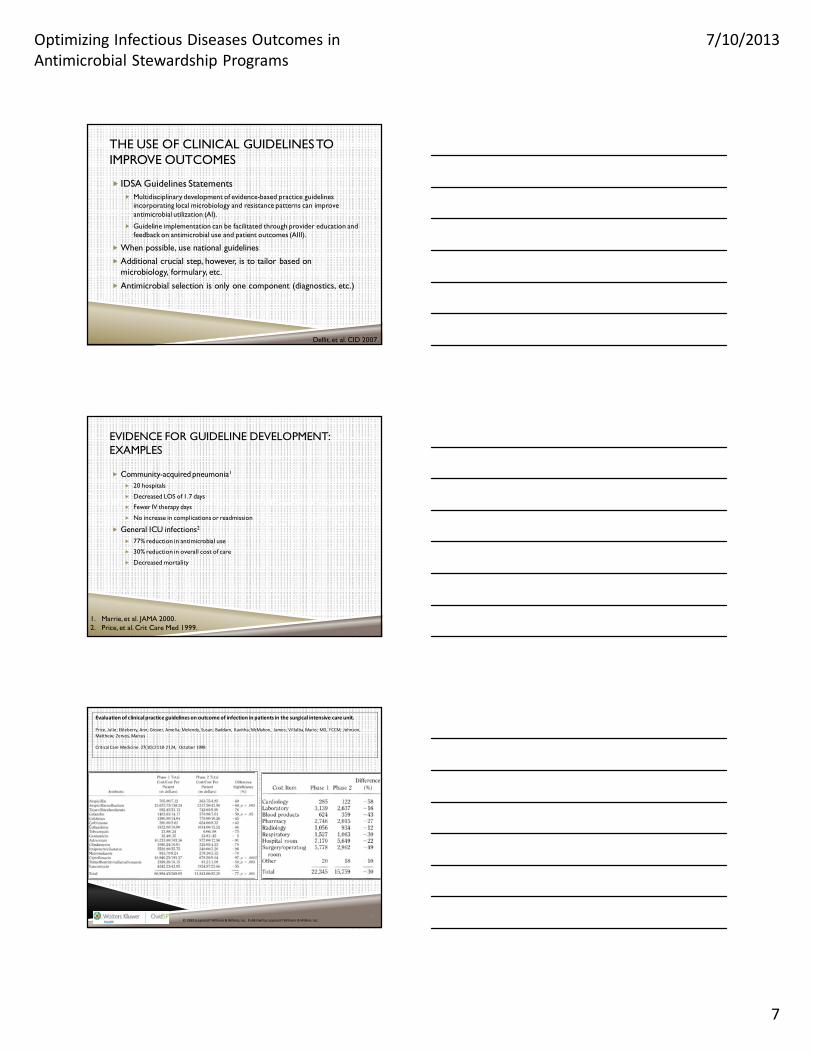
DORIPENEM EXTENDED INFUSION
Chastre, et al. Crit Care Med 2008;36(4)
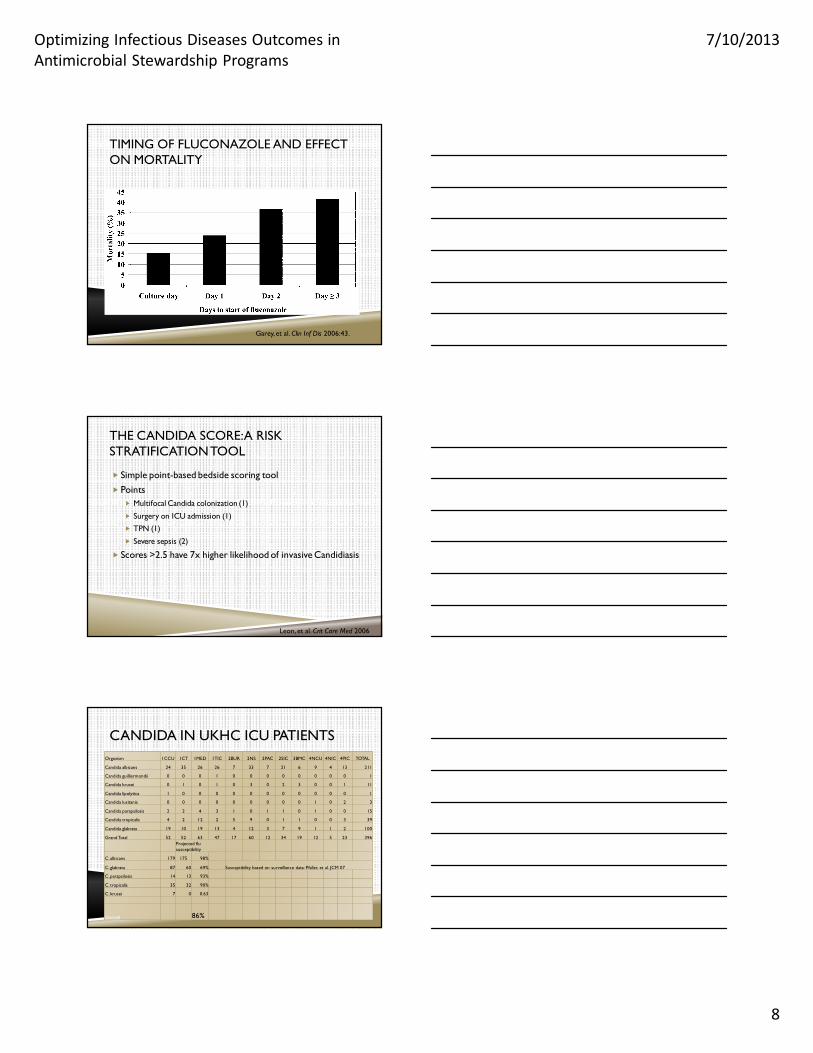
DORIPENEM EXTENDED INFUSION
Merchant, et al. Clinical Ther 2008.
Optimizing Infectious Diseases Outcomes in Antimicrobial Stewardship Programs
7/10/2013
7
THE USE OF CLINICAL GUIDELINES TO IMPROVE OUTCOMES
IDSA Guidelines Statements Multidisciplinary development of evidence-based practice guidelines
incorporating local microbiology and resistance patterns can improve antimicrobial utilization (AI).
Guideline implementation can be facilitated through provider education and feedback on antimicrobial use and patient outcomes (AIII).
When possible, use national guidelines
Additional crucial step, however, is to tailor based on microbiology, formulary, etc.
Antimicrobial selection is only one component (diagnostics, etc.)
Dellit, et al. CID 2007.
EVIDENCE FOR GUIDELINE DEVELOPMENT: EXAMPLES
Community-acquired pneumonia1
20 hospitals
Decreased LOS of 1.7 days
Fewer IV therapy days
No increase in complications or readmission
General ICU infections2
77% reduction in antimicrobial use
30% reduction in overall cost of care
Decreased mortality
1. Marrie, et al. JAMA 2000.2. Price, et al. Crit Care Med 1999.
© 1999 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc.2
Evaluation of clinical practice guidelines on outcome of infection in patients in the surgical intensive care unit.
Price, Julie; Ekleberry, Ann; Grover, Amelia; Melendy, Susan; Baddam, Kavitha; McMahon, James; Villalba, Mario; MD, FCCM; Johnson,
Matthew; Zervos, Marcus
Critical Care Medicine. 27(10):2118‐2124, October 1999.
Table 4 . Comparison of antibiotic treatment costs, Phase 1 vs . Phase 2
Optimizing Infectious Diseases Outcomes in Antimicrobial Stewardship Programs
7/10/2013
8
TIMING OF FLUCONAZOLE AND EFFECT ON MORTALITY
Garey, et al. Clin Inf Dis 2006:43.
THE CANDIDA SCORE: A RISK STRATIFICATION TOOL
Simple point-based bedside scoring tool
Points Multifocal Candida colonization (1)
Surgery on ICU admission (1)
TPN (1)
Severe sepsis (2)
Scores >2.5 have 7x higher likelihood of invasive Candidiasis
Leon, et al. Crit Care Med 2006
CANDIDA IN UKHC ICU PATIENTSOrganism 1CCU 1CT 1MED 1TIC 2BUR 2NS 2PAC 2SIC 3BMC 4NCU 4NIC 4PIC TOTAL
Candida albicans 24 35 26 26 7 33 7 21 6 9 4 13 211
Candida guilliermondii 0 0 0 1 0 0 0 0 0 0 0 0 1
Candida krusei 0 1 0 1 0 3 0 2 3 0 0 1 11
Candida lipolytica 1 0 0 0 0 0 0 0 0 0 0 0 1
Candida lusitania 0 0 0 0 0 0 0 0 0 1 0 2 3
Candida parapsilosis 2 2 4 3 1 0 1 1 0 1 0 0 15
Candida tropicalis 4 2 12 2 5 9 0 1 1 0 0 3 39
Candida glabrata 19 10 19 13 4 12 3 7 9 1 1 2 100
Grand Total 52 52 63 47 17 60 12 34 19 12 5 23 396Projected flu susceptibility
C. albicans 179 175 98%
C. glabrata 87 60 69% Susceptibility based on surveillance data: Pfaller, et al. JCM 07
C. parapsilosis 14 13 93%
C. tropicalis 35 32 90%
C. krusei 7 0 0.63
Overall 86%
Optimizing Infectious Diseases Outcomes in Antimicrobial Stewardship Programs
7/10/2013
9
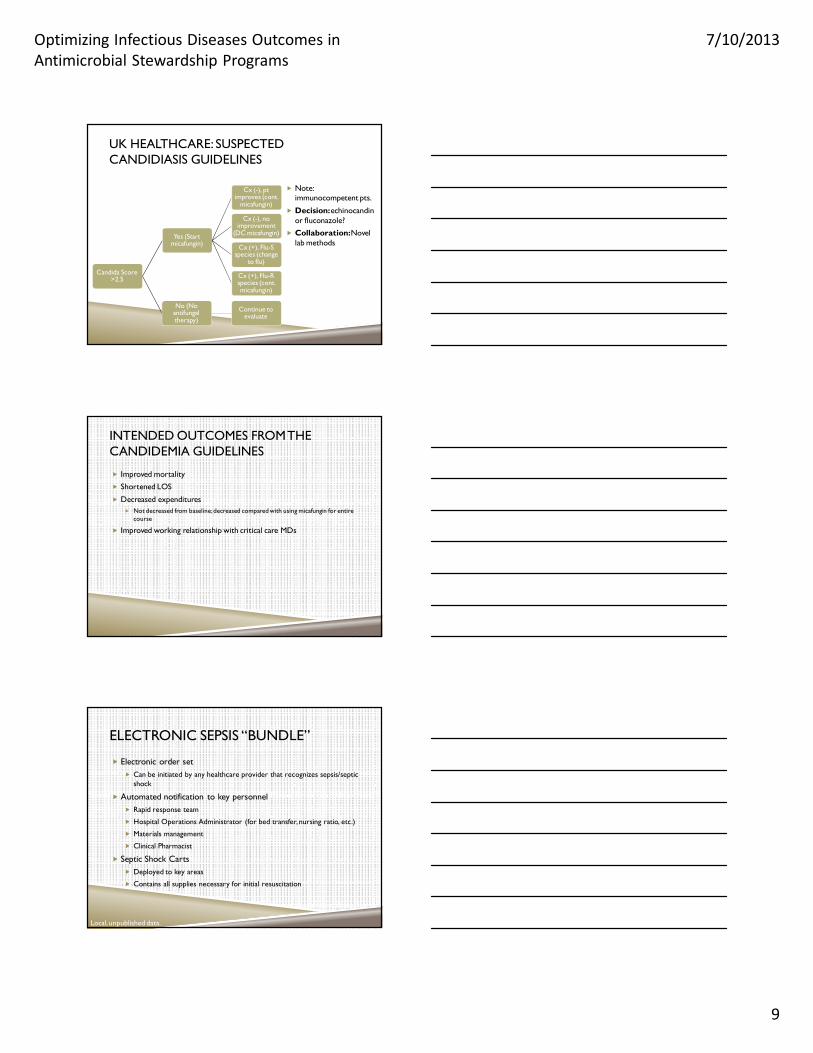
UK HEALTHCARE: SUSPECTED CANDIDIASIS GUIDELINES
Candida Score >2.5
Yes (Start micafungin)
Cx (-), pt improves (cont.
micafungin)
Cx (-), no improvement
(DC micafungin)
Cx (+), Flu-S species (change
to flu)
Cx (+), Flu-R species (cont. micafungin)
No (No antifungal therapy)
Continue to evaluate
Note: immunocompetent pts.
Decision: echinocandinor fluconazole?
Collaboration: Novel lab methods
INTENDED OUTCOMES FROM THE CANDIDEMIA GUIDELINES
Improved mortality
Shortened LOS
Decreased expenditures Not decreased from baseline; decreased compared with using micafungin for entire
course
Improved working relationship with critical care MDs
ELECTRONIC SEPSIS “BUNDLE”
Electronic order set Can be initiated by any healthcare provider that recognizes sepsis/septic
shock
Automated notification to key personnel Rapid response team
Hospital Operations Administrator (for bed transfer, nursing ratio, etc.)
Materials management
Clinical Pharmacist
Septic Shock Carts Deployed to key areas
Contains all supplies necessary for initial resuscitation
Local, unpublished data.
Optimizing Infectious Diseases Outcomes in Antimicrobial Stewardship Programs
7/10/2013
10
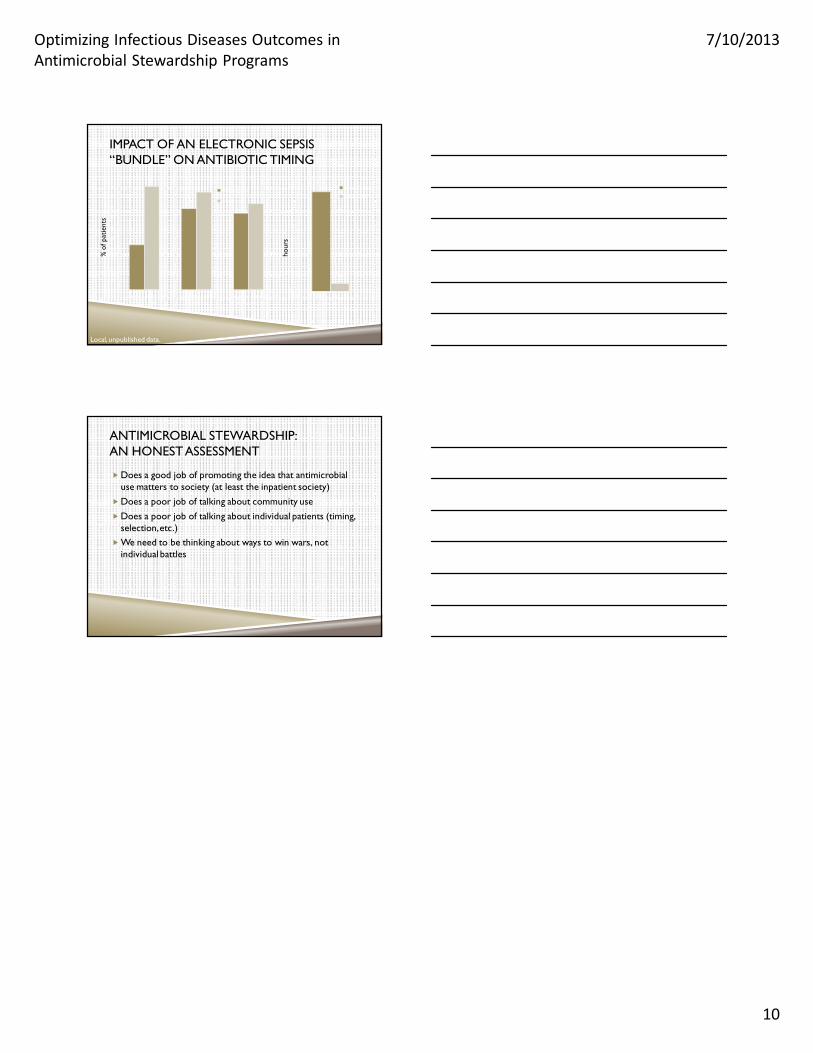
IMPACT OF AN ELECTRONIC SEPSIS “BUNDLE” ON ANTIBIOTIC TIMING
0
10
20
30
40
50
60
70
80
90
100
Antibiotics within 1 hour (3 hrs for ED)
Blood Cxs prior to antibiotics
Appropriate Antibiotics for positive cultures
Before (n=46)
After (n=18)
0
1
2
3
4
5
6
7
8
Time to 1st Dose Antibiotics (Hours)
Before (n=46)
After (n=18)
Local, unpublished data.
% o
f pat
ient
s
hour
s
ANTIMICROBIAL STEWARDSHIP: AN HONEST ASSESSMENT
Does a good job of promoting the idea that antimicrobial use matters to society (at least the inpatient society)
Does a poor job of talking about community use
Does a poor job of talking about individual patients (timing, selection, etc.)
We need to be thinking about ways to win wars, not individual battles