optimal approach to impacting medicine and patient...
TRANSCRIPT

Curriculum-Based Educational Initiatives:
OPTIMAL APPROACH TO IMPACTING MEDICINE AND PATIENT CARE
Grounded in science, fueled by innovation, driven to impact healthcare quality

Dear Colleague:
Measurement of curriculum-based educational initiatives has
demonstrated greater levels of impact than is often achieved
through single educational activities. Multi-component programs
deliver sustained exposure to education and have shown
statistically signifi cant change in knowledge, competence,
performance, and patient outcomes. Recognizing the potential
for curriculum-based initiatives to create such impact, many
commercial supporters of education have reallocated funding,
moving from single activities to larger-scale educational initiatives,
such as personalized learning, curriculum-based initiatives, and
PI CME. Medscape is proud to share examples of such initiatives,
which were accepted for presentation at scientifi c meetings and
educational conferences, underscoring the signifi cance of the
results produced by these larger-scale initiatives.
Regards,
The Medscape Education Team
TABLE OF CONTENTS
“ Assessment of Clinician Practices in Screening and Linkage to Care for Chronic Hepatitis B”
Melissa Osborn, MD1; Yelena Lyustikman, MS2; Wendy E. Cerenzia, MS3; Simi T. Hurst, PhD2
1MetroHealth Medical Center/Case Western in Cleveland, OH, USA; 2Medscape, LLC, New York, NY, USA; 3CE Outcomes, LLC, Birmingham, AL, USA
“ Current Clinical Practices in PAH: Challenges and Opportunities to Improve Care”
Nimish Mehta, PhD, MBA, CCMEP1; Tara Herrmann, PhD1; Chad Williamson, MS, MBA2; Steven D. Nathan, MD3
1Medscape, LLC, New York, NY, USA; 2CE Outcomes, LLC, Birmingham, AL, USA; 3Inova Fairfax Hospital, Falls Church, VA, USA
“ The Impact of a 12-Part Online CME Multimedia Curriculum Regarding Chronic Pain on Practice Patterns in Primary Care”
Anne Roc, PhD1; Stacey Ullman, MHS1; Perry G. Fine, MD2; Greg Salinas, PhD3; Sharon Hwang, MD3
1Medcape Education, New York, NY, USA; 2Department of Anesthesiology, University of Utah, Salt Lake City, UT, USA;3Research and Assessment Services, CE Outcomes, LLC, Birmingham, AL, USA
“ Personalized Learning: A Novel Educational Model to Bridge Clinical Practice Gaps in Chronic HBV Infection”
Nancy Reau, MD1; Susan L. Smith, MN, PhD2; Wendy Cerenzia, MS3; Simi T. Hurst, PhD2
1Center for Liver Diseases, University of Chicago Medical Center, Chicago, IL, USA; 2Medscape, LLC, New York, NY, USA; 3CE Outcomes, Birmingham, AL, USA
“ Elements to Consider in the Development, Implementation, and Evaluation of Performance Improvement CME”
Cyndi Grimes, CCMEP, and Jane Lowers
Medscape, LLC, New York, NY
T A B L E O F C O N T E N T S
p4
p8
p12
p16
p20
1
2
3
4
5
Copyright© 2013 by Medscape, LLC.
For more information, contact:Rejean Rochette,Group Vice [email protected]

AbstractBackground: Chronic hepatitis B virus (HBV) infection presents a significant clinical and public health burden, but remains largely underdiagnosed and undertreated in the United States. This study was designed to measure current clinician practices in HBV screening and linkage to care to inform a series of focused educational interventions to facilitate clinical performance improvement.
Methods: An Internet-based continuing medical education (CME)-certified self-assessment (SA) consisting of 25 case-based questions evaluating current knowledge, skills, attitudes, barriers, and clinical practices relating to HBV screening and linkage to care was administered to physicians, nurses/advanced practice nurses, and physician assistants free of charge. Data were collected between February 10, 2012 and March 31, 2012 and analyzed in aggregate to maintain the confidentiality of participants.
Results: A total of 681 clinicians completed the SA; 84% of completers were physicians (primary care providers, infectious disease specialists, pediatricians, and obstetricians/gynecologists). Of the physician completers, 43%, 38%, and 8% indicated some, moderate, or extreme confidence in recognizing HBV risk factors, respectively, but only 22% to 32% correctly identified individuals with HBV risk factors. Physicians also indicated confidence (some, 48%; moderate, 31%; extreme, 10%) in serological evaluation, but only 55% correctly interpreted serology data to diagnose chronic HBV infection. Gaps in preventing/understanding mother-to-child HBV transmission were identified: 85% of physicians recognized that all pregnant women should be screened for HBV, but only 19% recognized the high likelihood of the infant developing chronic HBV if infected during delivery. Further, only 48% recognized that mothers with chronic HBV infection may breastfeed their infants. Physicians reported that key barriers to screening and linkage to care included insufficient knowledge of HBV diagnostic tests and lack of education about risk factors.
Conclusion: Despite indicating confidence in their ability to recognize risk factors for HBV infection, the majority of physicians could not correctly identify patients to be screened for HBV infection nor properly interpret HBV serologic tests. Education focused on these and the other identified gaps can help improve clinical performance. Further outcomes analyses to evaluate the effectiveness of educational interventions are underway.
Introduction: Chronic HBV Infection in the United States
• As many as 80% of persons with chronic hepatitis B virus (HBV) infection may remain undiagnosed1-4
• Without treatment, chronic HBV infection can progress to end-stage liver disease and hepatocellular carcinoma, which is one of the nation’s fastest growing cancers and accounts for 80% of new cases of liver cancer5,6
• Preventing disease transmission and initiating treatment are both dependent on early diagnosis, but lack of awareness and poor screening practices for HBV are well cited6-9
• The Institute of Medicine (IOM) report and the US Department of Health and Human Services (DHHS) Action Plan for Viral Hepatitis recommend education of healthcare providers (HCPs) as a critical component of controlling this “silent epidemic”2,10
MethodsCurriculum Model for Education and Assessment• A multisource analysis* revealed practice
gaps and educational needs among primary care providers (PCPs), obstetricians/gynecologists (OB/GYNs), women’s health specialists, and other healthcare providers (HCPs) who are in a position to identify and link to care individuals at increased risk for chronic HBV infection (Figure 1)
• To address identified practice gaps, an Internet-based CME curriculum and assessment plan were developed using a step-wise process (Figure 2)
• CE Outcomes, LLC, collaborated with Medscape to assess the impact of the educational curriculum on HBV screening and linkage-to-care patterns of participating PCPs and OB/GYNs (physicians)
• The following CME activities were developed as part of the curriculum and were included in the assessment of educational impact. All activities are posted online at Medscape Education (www.medscape.org). — Combating the Silent Epidemic: A Clinical
Practice Assessment (Melissa Osborn, MD)— A Silent Epidemic: Why Chronic Hepatitis
B Matters (Robert P. Perrillo, MD; John W. Ward, MD)
— Best Practices in HBV Screening and Linkage to Care: The HIV/HBV-Coinfected Patient (Melissa Osborn, MD)
— Best Practices in HBV Screening and Linkage to Care: The Asian American Patient (Su Wang, MD, MPH)
— Hepatitis B Screening and Follow-up Care in a Pregnant Woman (Tram T. Tran, MD)
Data Collection and AnalysisA. Baseline Self-Assessment• The SA is available at www.medscape.org/
viewarticle/758033• Participant response data were gathered by
Medscape and provided electronically to CE Outcomes for analysis 30 days following online posting of the SA
• Baseline analysis was limited to practicing PCPs and OB/GYNs who completed at least 50% of the case vignette questions in the SA
• Data management, extraction, transformation, and statistical analyses were performed using IBM SPSS Statistics 20 — Responses were scored according to their
concordance with evidence-based answers — Overall mean scores and mean scores among
PCPs and OB/GYNs were calculated and served as the baseline group
— Baseline findings informed the development of CME activities
B. Post-education Assessment• CME activities posted online in a sequential
manner• Participant response data were gathered
by Medscape and provided electronically to CE Outcomes for analysis 30 days following online posting of the final CME activity included in the curriculum
• Post-education analysis was limited to practicing PCPs and OB/GYNs (physicians) who participated in the CME activities
• Data management, extraction, transformation, and statistical analyses were performed using IBM SPSS Statistics 20 — Presented findings reflect the aggregate
completed responses across all post-education activities
— Responses were scored according to their concordance with evidence-based answers
— Overall mean scores and mean scores among PCPs and OB/GYNs were calculated and served as the post-education assessment group
— Data from the post-education assessment group were compared with data from the baseline group to measure educational impact• Chi-square tests were conducted to detect
significant differences between the 2 groups
ResultsDemographics of SA Participants• 400 physicians were included in the final SA
participant sample (Table 1)
Educational Impact• In comparison with physicians who participated
in the baseline SA, physicians who participated in the CME activities included in this curriculum were better able to recognize the following: — Individuals at risk for HBV reactivation, such
as those beginning chemotherapy (P<.001, PCPs; P=.01, OB/GYNs)
— Risk factors for HBV infection, such as a history of intravenous drug use (P<.001, PCPs; P<.001, OB/GYNs)
— Individuals for whom screening is recommended, such as pregnant women (P<.001, PCPs; P=.001, OB/GYNs)
— The risk of perinatal transmission of HBV (P<.001, PCPs; P=.001, OB/GYNs) and the likelihood of a newborn developing chronic HBV infection without medical intervention (P<.001, PCPs; P<.001, OB/GYNs)
— Strategies to reduce perinatal transmission (P<.001, PCPs; P=.001, OB/GYNs)
— The relatively low risk of HBV transmission through breast milk and indications for breastfeeding for mothers with chronic HBV infection (P<.001, PCPs and OB/GYNs)
— Potential long-term complications associated with chronic HBV infection (P<.001, PCPs;P=.005, OB/GYNs)
• Physicians continued to struggle to recognize risk for HBV infection among persons originating from countries of endemicity, especially in areas of intermediate endemicity, where HBV prevalence ranges from 2% to 8% (Figure 3)
Attitudes and Perceptions• In comparison with physicians who
participated in the baseline SA, post-assessment analysis of physicians who participated in the CME activities included in this curriculum indicated significantly greater (P<.001, PCPs; P=.02, OB/GYNs) confidence in evaluating risk factors for HBV infection
• Importantly, although physicians expressed increased confidence (P<.001, PCPs; P=.10, OB/GYNs), analysis of post-activity questions indicated that 34% of PCPs and 50% of OB/GYNs did not correctly interpret HBV serology to characterize infection (Figure 4)
• Participation in the curriculum significantly increased physicians’ awareness and
understanding of important barriers to patient identification and care, including — Uncertainty about which
patient populations are at risk for HBV infection (P<.001, PCPs and OB/GYNs)
— Lack of knowledge about which screening tests are appropriate (P<.001, PCPs; P=.002, OB/GYNs)
— Patients’ perception that they do not need treatment because they do not have symptoms (P<.001, PCPs; P=.002, OB/GYNs)
— Language and cultural barriers that may impede effective communication (P<.001, PCPs and OB/GYNs)
Discussion and Conclusions
• Physicians who participated in the CME activities were 35% (effect size, 0.53) more likely to make evidence-based choices than those who participated in the baseline SA
• Physicians also indicated increased confidence across several categories; however, increased confidence did not always translate into evidence-based choices
• Although significant strides were made in improving physicians’ awareness, understanding, competence, and performance with respect to HBV screening and linkage to care, additional education is recommended in the following topic areas: — Geographic prevalence of HBV infection — Interpretation of HBV serology — Vaccination opportunities — Overcoming barriers to screening,
particularly among Asian AmericansAcknowledgementsThis CME curriculum focused on Screening and Linkage to Care for HBV Infection was funded through an independent educational grant from Gilead Sciences Medical Affairs. For more information contact Simi T. Hurst, PhD, Director Clinical Strategy, Infectious Disease, Medscape, LLC, [email protected].
* Interviews with experts, review of current literature and research findings, statistical and epidemiologic data, Medscape member surveys pre- and posttest results, and completed outcomes studies from previous or ongoing Medscape programs.
References1. Centers for Disease Control and Prevention. Recommendations for the
identification and public health management of persons with chronic hepatitis B virus infection. MMWR Recomm Rep. 2008;57(RR08):1-20.
2. Colvin HM, Mitchell AE, eds. Committee on the Prevention and Control of Viral Hepatitis Infections; Institute of Medicine. Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C. Washington, DC: National Academies Press; 2010.
3. Cohen C, Evans A, London WT, et al. Underestimation of chronic hepatitis B virus infection in the United States of America. J Viral Hepat. 2008;15:12-13.
4. Cohen C, Holmberg SD, McMahon BJ, et al. Is chronic hepatitis B being undertreated in the United States? J Viral Hepat. 2011;18(6):377-383.
5. American Cancer Society (ACS). ACS Cancer Facts and Figures 2010. www.cancer.org/research/cancerfactsfigures/cancerfactsfigures/cancer-facts-and-figures-2010. Accessed September 1, 2012.
6. Nguyen TT, McPhee SJ, Stewart S, et al. Factors associated with hepatitis B testing among Vietnamese Americans. J Gen Intern Med. 2010;25:694-700.
7. Chu D. Hepatitis B virus screening practices of Asian-American primary care physicians who treat Asian adults living in the United States. Program and abstracts of the 13th International Symposium on Viral Hepatitis and Liver Disease; Washington, DC: March 20-24, 2009.
8. Ferrante JM, Winston DG, Chen PH, de la Torre AN. Family physicians’ knowledge and screening of chronic hepatitis and liver cancer. Fam Med. 2008;40:345-351.
9. Kallman JB, Arsalla A, Park V, et al. Screening for hepatitis B, C and non-alcoholic fatty liver disease: a survey of community-based physicians. Aliment Pharmacol Ther. 2009;29:1019-1024.
10. US Department of Health and Human Services. Combating the silent epidemic of viral hepatitis: action plan for the prevention, care, and treatment of viral hepatitis. www.hhs.gov/ash/initiatives/hepatitis/actionplan_viralhepatitis2011.pdf. Accessed September 1, 2012.
Assessment of Clinician Practices in Screening and Linkage to Care for Chronic Hepatitis B
Figure 1. Identified practice gaps and educational needs
Table 1.
Number patients with HBV infection (acute or chronic) seen each week 0 42% 62% 1-10 46% 36% 11-20 8% 0% 21-30 2% 0% 31-40 1% 0% > 40 2% 2%
Practice location Northeast 36% 33% South 25% 33% Midwest 20% 23% West 17% 17%
Practice Setting Emergency department 20% 6% Hospital Group/Outpatient 27% 30% Private Practice 49% 64% Clinic 5% 64%
Primary Care OB/GYN (n=300) (n=100)
Melissa Osborn, MD1; Yelena Lyustikman, MS2; Wendy E. Cerenzia, MS3; Simi T. Hurst, PhD2
1MetroHealth Medical Center/Case Western in Cleveland, Ohio, USA; 2Medscape, LLC, New York, NY, USA; 3CE Outcomes LLC, Birmingham, AL, USA
always translate into evidence-based choices References
Figure 3. Inadequate recognition of countries where chronic HBV infection is endemic.
Figure 4. Discordance between expressed confidence and serological interpretation.
80%
60%
40%
20%
0%
8% 7%
Laborer born in Guatemala
Baseline PCP (n=296)
Baseline OB/GYN (n=93)
Post-education PCP (n=159) PCP P=.12OB/GYN P=.36Post-education OB/GYN (n=46)
College student born in Israel*
Indigenous native to Alaska Teacher born in Spain
4% 7%
32%25% 29%
22%28% 31%
37% 39%32% 37%
30% 33%
80%
60%
40%
20%
0%
10%2%
Not at all confident
Baseline PCP (n=300)
Baseline OB/GYN (n=100)
Post-education PCP (n=161) PCP P<.001OB/GYN P=.10Post-education OB/GYN (n=48)
Somewhat confident Moderately confident Extremely confident
16%6%
45%33%
46%40%
33%
48%
31%
50%
12% 17%7% 4%
80%
60%
40%
20%
0%
24% 21%
Early, acute infection
Baseline PCP (n=300)
Baseline OB/GYN (n=100)
Post-education PCP (n=160) PCP P=.21OB/GYN P=.65Post-education OB/GYN (n=46)
Immunity due toHBV vaccination
Chronic infection* Acute, resolving infection
31% 28%
7% 4%11% 11%
60%66%
46% 50%
10% 9% 12% 11%
Assessment Question: How confident are you in your ability to interpret serologic markers for HBV infection?
Assessment Question: How would you interpret these (data not shown) results?
Figure 2. Curriculum model for educational assessment
• Development of a CME-certified self-assessment (SA) consisting of 25 case-based questions evaluating current knowledge, skills, attitudes, barriers and clinical practices relating to HBV screening and linkage to care
• Online posting of SA on Medscape Education
• 30 days following online SA posting: Data collection and analysis to determine current clinical practice patterns among physicians in primary care and obstetrics/gynecology, (baseline)
• Development of CME activities that align with identified performance gaps and educational needs
• Each activity contains 3-5 post-activity questions aligned with the SA
• Activities integrate multimedia, interactive formats with instructional design principles
• Activities are posted online in a sequential manner
• 30 days following the online posting of last CME activity in the curriculum: Assessment of educational impact through comparison of participant responses to post-activity questions (post-assessment) with responses from the baseline SA
STAGE 1 STAGE 2 STAGE 3 STAGE 4
g g g
Observation:Estimates suggest >80% of persons with chronic
HBV infection may remain undiagnosed
Education Needs:Recognition of risk-
factors and screening of individuals who are at risk for HBV infection
Observation:Estimates suggest only
40% of persons diagnosed with chronic HBV infection
are linked to care
Education Needs:Linkage to care for persons
diagnosed with HBV infection, including timely and appropriate referral
Observation:The majority of clinicians
do not discuss HBV infection with patients
Education Needs:Communication strategies
to discuss risk for HBV infection and
follow-up care
Values represent the percentage of physicians in the sample who selected the indicated response option
Values represent the percentage of physicians in the sample who selected the indicated response option
Assessment Question: Which of the following patients would you not routinely screen for HBV infection?
1027
1
P O S T E R
Presented at ID Week in 2012; Poster contained data on baseline assessment and interim analysis.
“ Assessment of Clinician Practices in Screening and Linkage to Care for Chronic Hepatitis B”
4 5

1 “ Assessment of Clinician Practices in Screening and Linkage to Care for Chronic Hepatitis B”
F O R M A T
HBV Curriculum Based Initiative that included baseline assessment and curriculum-level outcomes. With the goal of improving patient care, Medscape identified performance gaps among primary care physicians (PCPs), OB/GYN and women’s health specialists, and other physicians who are in a position to screen at-risk patients for HBV infection. An educational grant was awarded to Medscape by Gilead Sciences Medical Affairs to develop continuing medical education (CME) using a curriculum model and to report metrics on the effect of the educational curriculum.
AbstractBackground: Chronic hepatitis B virus (HBV) infection presents a significant clinical and public health burden, but remains largely underdiagnosed and undertreated in the United States. This study was designed to measure current clinician practices in HBV screening and linkage to care to inform a series of focused educational interventions to facilitate clinical performance improvement.
Methods: An Internet-based continuing medical education (CME)-certified self-assessment (SA) consisting of 25 case-based questions evaluating current knowledge, skills, attitudes, barriers, and clinical practices relating to HBV screening and linkage to care was administered to physicians, nurses/advanced practice nurses, and physician assistants free of charge. Data were collected between February 10, 2012 and March 31, 2012 and analyzed in aggregate to maintain the confidentiality of participants.
Results: A total of 681 clinicians completed the SA; 84% of completers were physicians (primary care providers, infectious disease specialists, pediatricians, and obstetricians/gynecologists). Of the physician completers, 43%, 38%, and 8% indicated some, moderate, or extreme confidence in recognizing HBV risk factors, respectively, but only 22% to 32% correctly identified individuals with HBV risk factors. Physicians also indicated confidence (some, 48%; moderate, 31%; extreme, 10%) in serological evaluation, but only 55% correctly interpreted serology data to diagnose chronic HBV infection. Gaps in preventing/understanding mother-to-child HBV transmission were identified: 85% of physicians recognized that all pregnant women should be screened for HBV, but only 19% recognized the high likelihood of the infant developing chronic HBV if infected during delivery. Further, only 48% recognized that mothers with chronic HBV infection may breastfeed their infants. Physicians reported that key barriers to screening and linkage to care included insufficient knowledge of HBV diagnostic tests and lack of education about risk factors.
Conclusion: Despite indicating confidence in their ability to recognize risk factors for HBV infection, the majority of physicians could not correctly identify patients to be screened for HBV infection nor properly interpret HBV serologic tests. Education focused on these and the other identified gaps can help improve clinical performance. Further outcomes analyses to evaluate the effectiveness of educational interventions are underway.
Introduction: Chronic HBV Infection in the United States
• As many as 80% of persons with chronic hepatitis B virus (HBV) infection may remain undiagnosed1-4
• Without treatment, chronic HBV infection can progress to end-stage liver disease and hepatocellular carcinoma, which is one of the nation’s fastest growing cancers and accounts for 80% of new cases of liver cancer5,6
• Preventing disease transmission and initiating treatment are both dependent on early diagnosis, but lack of awareness and poor screening practices for HBV are well cited6-9
• The Institute of Medicine (IOM) report and the US Department of Health and Human Services (DHHS) Action Plan for Viral Hepatitis recommend education of healthcare providers (HCPs) as a critical component of controlling this “silent epidemic”2,10
MethodsCurriculum Model for Education and Assessment• A multisource analysis* revealed practice
gaps and educational needs among primary care providers (PCPs), obstetricians/gynecologists (OB/GYNs), women’s health specialists, and other healthcare providers (HCPs) who are in a position to identify and link to care individuals at increased risk for chronic HBV infection (Figure 1)
• To address identified practice gaps, an Internet-based CME curriculum and assessment plan were developed using a step-wise process (Figure 2)
• CE Outcomes, LLC, collaborated with Medscape to assess the impact of the educational curriculum on HBV screening and linkage-to-care patterns of participating PCPs and OB/GYNs (physicians)
• The following CME activities were developed as part of the curriculum and were included in the assessment of educational impact. All activities are posted online at Medscape Education (www.medscape.org). — Combating the Silent Epidemic: A Clinical
Practice Assessment (Melissa Osborn, MD)— A Silent Epidemic: Why Chronic Hepatitis
B Matters (Robert P. Perrillo, MD; John W. Ward, MD)
— Best Practices in HBV Screening and Linkage to Care: The HIV/HBV-Coinfected Patient (Melissa Osborn, MD)
— Best Practices in HBV Screening and Linkage to Care: The Asian American Patient (Su Wang, MD, MPH)
— Hepatitis B Screening and Follow-up Care in a Pregnant Woman (Tram T. Tran, MD)
Data Collection and AnalysisA. Baseline Self-Assessment• The SA is available at www.medscape.org/
viewarticle/758033• Participant response data were gathered by
Medscape and provided electronically to CE Outcomes for analysis 30 days following online posting of the SA
• Baseline analysis was limited to practicing PCPs and OB/GYNs who completed at least 50% of the case vignette questions in the SA
• Data management, extraction, transformation, and statistical analyses were performed using IBM SPSS Statistics 20 — Responses were scored according to their
concordance with evidence-based answers — Overall mean scores and mean scores among
PCPs and OB/GYNs were calculated and served as the baseline group
— Baseline findings informed the development of CME activities
B. Post-education Assessment• CME activities posted online in a sequential
manner• Participant response data were gathered
by Medscape and provided electronically to CE Outcomes for analysis 30 days following online posting of the final CME activity included in the curriculum
• Post-education analysis was limited to practicing PCPs and OB/GYNs (physicians) who participated in the CME activities
• Data management, extraction, transformation, and statistical analyses were performed using IBM SPSS Statistics 20 — Presented findings reflect the aggregate
completed responses across all post-education activities
— Responses were scored according to their concordance with evidence-based answers
— Overall mean scores and mean scores among PCPs and OB/GYNs were calculated and served as the post-education assessment group
— Data from the post-education assessment group were compared with data from the baseline group to measure educational impact• Chi-square tests were conducted to detect
significant differences between the 2 groups
ResultsDemographics of SA Participants• 400 physicians were included in the final SA
participant sample (Table 1)
Educational Impact• In comparison with physicians who participated
in the baseline SA, physicians who participated in the CME activities included in this curriculum were better able to recognize the following: — Individuals at risk for HBV reactivation, such
as those beginning chemotherapy (P<.001, PCPs; P=.01, OB/GYNs)
— Risk factors for HBV infection, such as a history of intravenous drug use (P<.001, PCPs; P<.001, OB/GYNs)
— Individuals for whom screening is recommended, such as pregnant women (P<.001, PCPs; P=.001, OB/GYNs)
— The risk of perinatal transmission of HBV (P<.001, PCPs; P=.001, OB/GYNs) and the likelihood of a newborn developing chronic HBV infection without medical intervention (P<.001, PCPs; P<.001, OB/GYNs)
— Strategies to reduce perinatal transmission (P<.001, PCPs; P=.001, OB/GYNs)
— The relatively low risk of HBV transmission through breast milk and indications for breastfeeding for mothers with chronic HBV infection (P<.001, PCPs and OB/GYNs)
— Potential long-term complications associated with chronic HBV infection (P<.001, PCPs;P=.005, OB/GYNs)
• Physicians continued to struggle to recognize risk for HBV infection among persons originating from countries of endemicity, especially in areas of intermediate endemicity, where HBV prevalence ranges from 2% to 8% (Figure 3)
Attitudes and Perceptions• In comparison with physicians who
participated in the baseline SA, post-assessment analysis of physicians who participated in the CME activities included in this curriculum indicated significantly greater (P<.001, PCPs; P=.02, OB/GYNs) confidence in evaluating risk factors for HBV infection
• Importantly, although physicians expressed increased confidence (P<.001, PCPs; P=.10, OB/GYNs), analysis of post-activity questions indicated that 34% of PCPs and 50% of OB/GYNs did not correctly interpret HBV serology to characterize infection (Figure 4)
• Participation in the curriculum significantly increased physicians’ awareness and
understanding of important barriers to patient identification and care, including — Uncertainty about which
patient populations are at risk for HBV infection (P<.001, PCPs and OB/GYNs)
— Lack of knowledge about which screening tests are appropriate (P<.001, PCPs; P=.002, OB/GYNs)
— Patients’ perception that they do not need treatment because they do not have symptoms (P<.001, PCPs; P=.002, OB/GYNs)
— Language and cultural barriers that may impede effective communication (P<.001, PCPs and OB/GYNs)
Discussion and Conclusions
• Physicians who participated in the CME activities were 35% (effect size, 0.53) more likely to make evidence-based choices than those who participated in the baseline SA
• Physicians also indicated increased confidence across several categories; however, increased confidence did not always translate into evidence-based choices
• Although significant strides were made in improving physicians’ awareness, understanding, competence, and performance with respect to HBV screening and linkage to care, additional education is recommended in the following topic areas: — Geographic prevalence of HBV infection — Interpretation of HBV serology — Vaccination opportunities — Overcoming barriers to screening,
particularly among Asian AmericansAcknowledgementsThis CME curriculum focused on Screening and Linkage to Care for HBV Infection was funded through an independent educational grant from Gilead Sciences Medical Affairs. For more information contact Simi T. Hurst, PhD, Director Clinical Strategy, Infectious Disease, Medscape, LLC, [email protected].
* Interviews with experts, review of current literature and research findings, statistical and epidemiologic data, Medscape member surveys pre- and posttest results, and completed outcomes studies from previous or ongoing Medscape programs.
References1. Centers for Disease Control and Prevention. Recommendations for the
identification and public health management of persons with chronic hepatitis B virus infection. MMWR Recomm Rep. 2008;57(RR08):1-20.
2. Colvin HM, Mitchell AE, eds. Committee on the Prevention and Control of Viral Hepatitis Infections; Institute of Medicine. Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C. Washington, DC: National Academies Press; 2010.
3. Cohen C, Evans A, London WT, et al. Underestimation of chronic hepatitis B virus infection in the United States of America. J Viral Hepat. 2008;15:12-13.
4. Cohen C, Holmberg SD, McMahon BJ, et al. Is chronic hepatitis B being undertreated in the United States? J Viral Hepat. 2011;18(6):377-383.
5. American Cancer Society (ACS). ACS Cancer Facts and Figures 2010. www.cancer.org/research/cancerfactsfigures/cancerfactsfigures/cancer-facts-and-figures-2010. Accessed September 1, 2012.
6. Nguyen TT, McPhee SJ, Stewart S, et al. Factors associated with hepatitis B testing among Vietnamese Americans. J Gen Intern Med. 2010;25:694-700.
7. Chu D. Hepatitis B virus screening practices of Asian-American primary care physicians who treat Asian adults living in the United States. Program and abstracts of the 13th International Symposium on Viral Hepatitis and Liver Disease; Washington, DC: March 20-24, 2009.
8. Ferrante JM, Winston DG, Chen PH, de la Torre AN. Family physicians’ knowledge and screening of chronic hepatitis and liver cancer. Fam Med. 2008;40:345-351.
9. Kallman JB, Arsalla A, Park V, et al. Screening for hepatitis B, C and non-alcoholic fatty liver disease: a survey of community-based physicians. Aliment Pharmacol Ther. 2009;29:1019-1024.
10. US Department of Health and Human Services. Combating the silent epidemic of viral hepatitis: action plan for the prevention, care, and treatment of viral hepatitis. www.hhs.gov/ash/initiatives/hepatitis/actionplan_viralhepatitis2011.pdf. Accessed September 1, 2012.
Assessment of Clinician Practices in Screening and Linkage to Care for Chronic Hepatitis B
Figure 1. Identified practice gaps and educational needs
Table 1.
Number patients with HBV infection (acute or chronic) seen each week 0 42% 62% 1-10 46% 36% 11-20 8% 0% 21-30 2% 0% 31-40 1% 0% > 40 2% 2%
Practice location Northeast 36% 33% South 25% 33% Midwest 20% 23% West 17% 17%
Practice Setting Emergency department 20% 6% Hospital Group/Outpatient 27% 30% Private Practice 49% 64% Clinic 5% 64%
Primary Care OB/GYN (n=300) (n=100)
Melissa Osborn, MD1; Yelena Lyustikman, MS2; Wendy E. Cerenzia, MS3; Simi T. Hurst, PhD2
1MetroHealth Medical Center/Case Western in Cleveland, Ohio, USA; 2Medscape, LLC, New York, NY, USA; 3CE Outcomes LLC, Birmingham, AL, USA
always translate into evidence-based choices References
Figure 3. Inadequate recognition of countries where chronic HBV infection is endemic.
Figure 4. Discordance between expressed confidence and serological interpretation.
80%
60%
40%
20%
0%
8% 7%
Laborer born in Guatemala
Baseline PCP (n=296)
Baseline OB/GYN (n=93)
Post-education PCP (n=159) PCP P=.12OB/GYN P=.36Post-education OB/GYN (n=46)
College student born in Israel*
Indigenous native to Alaska Teacher born in Spain
4% 7%
32%25% 29%
22%28% 31%
37% 39%32% 37%
30% 33%
80%
60%
40%
20%
0%
10%2%
Not at all confident
Baseline PCP (n=300)
Baseline OB/GYN (n=100)
Post-education PCP (n=161) PCP P<.001OB/GYN P=.10Post-education OB/GYN (n=48)
Somewhat confident Moderately confident Extremely confident
16%6%
45%33%
46%40%
33%
48%
31%
50%
12% 17%7% 4%
80%
60%
40%
20%
0%
24% 21%
Early, acute infection
Baseline PCP (n=300)
Baseline OB/GYN (n=100)
Post-education PCP (n=160) PCP P=.21OB/GYN P=.65Post-education OB/GYN (n=46)
Immunity due toHBV vaccination
Chronic infection* Acute, resolving infection
31% 28%
7% 4%11% 11%
60%66%
46% 50%
10% 9% 12% 11%
Assessment Question: How confident are you in your ability to interpret serologic markers for HBV infection?
Assessment Question: How would you interpret these (data not shown) results?
Figure 2. Curriculum model for educational assessment
• Development of a CME-certified self-assessment (SA) consisting of 25 case-based questions evaluating current knowledge, skills, attitudes, barriers and clinical practices relating to HBV screening and linkage to care
• Online posting of SA on Medscape Education
• 30 days following online SA posting: Data collection and analysis to determine current clinical practice patterns among physicians in primary care and obstetrics/gynecology, (baseline)
• Development of CME activities that align with identified performance gaps and educational needs
• Each activity contains 3-5 post-activity questions aligned with the SA
• Activities integrate multimedia, interactive formats with instructional design principles
• Activities are posted online in a sequential manner
• 30 days following the online posting of last CME activity in the curriculum: Assessment of educational impact through comparison of participant responses to post-activity questions (post-assessment) with responses from the baseline SA
STAGE 1 STAGE 2 STAGE 3 STAGE 4
g g g
Observation:Estimates suggest >80% of persons with chronic
HBV infection may remain undiagnosed
Education Needs:Recognition of risk-
factors and screening of individuals who are at risk for HBV infection
Observation:Estimates suggest only
40% of persons diagnosed with chronic HBV infection
are linked to care
Education Needs:Linkage to care for persons
diagnosed with HBV infection, including timely and appropriate referral
Observation:The majority of clinicians
do not discuss HBV infection with patients
Education Needs:Communication strategies
to discuss risk for HBV infection and
follow-up care
Values represent the percentage of physicians in the sample who selected the indicated response option
Values represent the percentage of physicians in the sample who selected the indicated response option
Assessment Question: Which of the following patients would you not routinely screen for HBV infection?
1027
G A PS
O V E R A L L I M P A C T S T A T E M E N T
P R I N C I P A L C U R R I C U L U M O U T C O M E S F I N D I N G S
P R I N C I P A L C U R R I C U L U M O U T C O M E S F I N D I N G S ( c o n t i n u e d )
E D U C A T I O N A L I M P A C T
• Frontline care providers do not routinely screen their patients for HBV infection. Estimates suggest that up to 80% of persons with chronic HBV infection remain undiagnosed.
• Frontline care providers lack strategies to eff ectively communicate with patients and discuss risks for HBV infection.
• Frontline care providers do not link patients with HBV infection into care. Fewer than 50% of persons diagnosed with chronic HBV infection are linked to care.
OB/GYNs and PCPs (n=1108) who participated in this educational curriculum were 37% (actual eff ect size of 0.58) more likely to make evidence-based choices than clinicians participating in the baseline clinical practice assessment conducted prior to the launch of
the educational curriculum. Evidence-based choices by the OB/GYNs and PCPs who completed the case-based post-education assessment demonstrate the impact of the education.
In comparing the curriculum post-education assessment responses (participants in the curriculum education) with the responses obtained in the baseline clinical practice assessment, the following fi ndings were observed:
Screening/Risk Factors
• Participants in the education were more confi dent in evaluating risk factors for HBV infection and were better able to recognize patients who did or did not need to be screened for HBV based on
patient characteristics, as compared with baseline respondents. In particular, educational participants recognized that all pregnant women should be screened for HBV.
Diagnosis and Interpretation of Serologic Markers
• Participants were more confi dent with respect to interpreting serologic markers for HBV infections and were slightly more likely to appropriately interpret HBV serology indicating chronic infection, as compared with baseline participants.
In comparison with physicians who participated in the baseline SA, physicians who participated in the CME activities included in this curriculum were better able to recognize the following:
• Individuals at risk for HBV reactivation, such as those beginning chemotherapy (P<.001, PCPs; P=.01, OB/GYNs).
• Risk factors for HBV infection, such as a history of intravenous drug use (P<.001, PCPs; P<.001, OB/GYNs).
• Individuals for whom screening is recommended, such as pregnant women (P<.001, PCPs; P=.001, OB/GYNs).
• The risk of perinatal transmission of HBV (P<.001, PCPs; P=.001, OB/GYNs) and the likelihood of a newborn developing chronic HBV infection without medical intervention (P<.001, PCPs; P<.001, OB/GYNs).
• Strategies to reduce perinatal transmission(P<.001, PCPs; P=.001, OB/GYNs).
• The relatively low risk of HBV transmission through breast milk and indications for breastfeeding for mothers with chronic HBV infection (P<.001, PCPs and OB/GYNs).
• Potential long-term complications associated with chronic HBV infection (P<.001, PCPs; P=.005, OB/GYNs).
• Physicians continued to struggle to recognize risk for HBV infection among persons originating from countries of endemicity, especially in areas of intermediate endemicity, where HBV prevalence ranges from 2% to 8%.
Perinatal HBV Transmission
• Compared with physicians who responded to the baseline survey, participants in the education had signifi cantly greater knowledge that mode of delivery does not have an impact on transmission of HBV.
• Education participants had a signifi cantly greater understanding, as compared with baseline respondents, of strategies to reduce perinatal transmission of HBV infection, including infant immunization, and that subsequent to immunization, breastfeeding was safe.
• Participants were signifi cantly more cognizant that if infected during delivery, an infant had a 90% risk of developing chronic HBV infection.
Follow-up/Complications
• Fewer physicians participating in the activity would refer a patient immediately upon diagnosis of HBV infection, compared with physicians in the baseline assessment, demonstrating a higher level of comfort in managing patients with HBV infection.
• Signifi cantly higher percentages of PCPs and OB/GYNs who participated in the activity recognized
that nonalcoholic steatosis is not a long-term complication of HBV infection and were aware that HBV infection can lead to glomerulonephritis. Primary care physicians and OB/GYNs who participated in the education indicated signifi cantly greater confi dence in HBV risk factor assessment, as compared with baseline respondents.
HBV/HIV Coinfection
• PCPs and OB/GYNs who participated in the education are more confi dent in being able to provide appropriate follow-up care to an HIV/HBV-coinfected patient, as compared with the physicians from the baseline assessment, and were signifi cantly more likely to recognize how coinfection with HIV aff ects the natural history of HBV infection and HBV vaccination response rates, compared with baseline respondents.
Cultural Competency
• Compared with baseline participants, more PCPs participating in the education recognized that family history of HBV infection should not be considered a barrier to HBV screening in Asian Americans.
EFFECTIVENESS OF COMPLETED OUTCOMES STUDY
6 7

PurposePulmonary arterial hypertension (PAH) -- a progressive and fatal disorder -- is underrecognized and inadequately treated based on current evidence-based guideline recommendations. Delays in diagnosis of more than 2 years and inadequate treatment have been identified from the REVEAL registry.1, 2 The objective of this study was to assess the current clinical practice of pulmonologists, cardiologists, and primary care physicians in PAH management to identify knowledge, competency, and practice gaps and barriers to improving the diagnosis and care of patients with this condition. An interim analysis of educational impact was also performed to determine improvement in clinical practice compared to baseline.
Methods• The needs assessment survey consisted of 25 items
based on current evidence-based consensus guidelines. • The assessment design included knowledge- and
case-based, multiple-choice questions made available online to Medscape membership of healthcare providers without monetary compensation or charge.
• Case vignettes and associated assessment question responses were used to analyze data on clinicians’ baseline knowledge, skills, attitudes, practice patterns, and perceived barriers related to the optimal management of patients with PAH.3-7
• The assessment instrument and the reporting metrics were organized by the assessment domains of diagnosis, pathophysiology, evidence-based treatment strategies, and monitoring.
• Confidentiality of survey respondents was maintained and responses were de-identified and aggregated prior to analysis. The assessment was posted online at http://www.medscape.org/viewarticle/758455. The survey launched on Medscape Education Pulmonary Medicine on February 17, 2012 and participant responses were collected until July 31, 2012.
• In addition to providing baseline data on clinical practice gaps, the data obtained from the baseline assessment were designed to serve as the control group for the practice outcomes assessment of the educational
curriculum. Questions from the clinical practice assessment are aligned to individual curriculum programs and posed to program participants following completion of each curriculum activity, to assess the curriculum outcomes.
ResultsIn total, 3071 physicians responded to the survey (1100 pulmonologists, 489 cardiologists, 1177 primary care providers [PCPs], and 305 other physicians). The results obtained demonstrate significant gaps in knowledge of PAH pathogenesis, and knowledge and skills surrounding diagnosis, risk
stratification, monitoring for disease activity, setting treatment goals, and interpreting the rationale for combination therapy in all clinical specialties.
Diagnosis• Nearly 20% of pulmonologists, 40% of cardiologists,
and 35% of PCPs did not recommend right heart catheterization to confirm a diagnosis of PAH (Figure 1).
• Most respondents lack confidence in diagnosing PAH, with the majority of pulmonologists (57%), cardiologists (63%), and PCPs (62%) being only somewhat confident.
• Lack of familiarity with PAH was cited most frequently by respondents as a barrier to appropriate diagnosis.
• A wide variation in recognition of the definition of pulmonary hypertension as mean pulmonary artery pressure (mPAP) ≥ 25 mm Hg was observed (Figure 2).
Pathophysiology• More than one-third of respondents (pulmonologists,
34%; cardiologists, 39%; PCPs, 52%) did not recognize the role of phosphodiesterase type 5 (PDE-5) inhibition in the pathophysiology of PAH.
Evidence-based Treatment Strategies• More than 68% of
pulmonologists, 74% of cardiologists, and 82% of PCPs reported that their practices do not use an algorithm for PAH management.
• Close to 20% of pulmonologists, 30% of cardiologists, and 50% of PCPs could not identify the correct risk level or therapy for the low-risk patient (Figure 3).
• Most respondents (pulmonologists, 61%; cardiologists, 59%; PCPs, 43%) are only somewhat confident in their ability to individualize PAH treatment based on functional classification, comorbid conditions, and risk assessment. Moreover, a substantial percentage of physicians are “not at all confident” (pulmonologists, 22%; cardiologists, 31%; PCPs, 54%).
• The majority of physicians (pulmonologists, 89%; cardiologists, 85%; PCPs, 78%) recognized that a patient with PAH who remains in WHO functional class 3 or 4 and whose mPAP remains elevated after initial therapy should receive dual or triple therapy.
Monitoring• When deciding to repeat right heart catheterization,
43% of pulmonologists, 39% of cardiologists, and 49% of PCPs would base their decision on parameters other than the magnitude of clinical deterioration (Figure 4).
• More than 16% of pulmonologists, 31% of cardiologists, and 56% of PCPs would not perform monthly liver function tests to monitor a patient taking bosentan.
• Almost 75% of pulmonologists, 80% of cardiologists, and 90% of PCPs are not at all confident or are somewhat confident in their ability to monitor patients with PAH for clinical deterioration and for treatment effects and toxicities.
Educational Impact An interim analysis of the assessment of a subset of physicians participating in 3 educational interventions showed significant improvement in the following areas:
• At least 75% of all respondents recognized that an elevated right atrial pressure and a cardiac index of 1.6 L/min/m2 would place a patient with PAH at greatest risk.
• Significantly more cardiologists (65% before participation in the activity and 88% after participation; P=.03) and pulmonologists (68% before and 87% after; P=.006) recognized the action of PDE-5 inhibitors in relation to PAH pathogenesis.
• When compared to baseline, 13% more pulmonologists (P=.04) and 16% more cardiologists (P=.12) correctly identified 25 mm Hg as the cut-off mPAP value to diagnose PAH.
• A total of 15% more pulmonologists were significantly more likely (P=.02) to recognize that the goal of combination therapy is to maximize efficacy, minimize toxicity, and allow for targeting of multiple pathologic pathways.
• Significantly more cardiologists would consider combination therapy for PAH in the appropriate clinical circumstance after participation in the educational activity compared with cardiologists in the baseline sample (76% before and 98% after; P=.002).
Conclusions and Clinical Implications
• This assessment of healthcare providers’ clinical practices identified gaps in PAH diagnosis and management among pulmonologists, cardiologists, and PCPs. — A significant proportion of physicians, regardless
of specialty, would fail to perform right heart catheterization to confirm a diagnosis of PAH, which may result in misdiagnosis or underdiagnosis of the condition. This may be due to a lack of physician familiarity with PAH and its diagnostic algorithm.
— Availability of a treatment algorithm can improve multiple aspects of care and management of patients with PAH. This is especially true in cases of rare diseases like PAH, where knowledge may be limited and physician confidence low. Thus, it is critical that more practices and medical institutions obtain and make available a PAH treatment decision tree for their clinicians.
— Knowledge of current PAH guideline recommendations on the management of PAH is suboptimal, particularly the monitoring and augmentation of therapy in patients with unstable disease.
— Future programs emphasizing the optimization of the timing of monitoring and appropriate augmentation of therapy in patients with PAH are needed to improve clinical outcomes.
• Significant improvement in the knowledge of pulmonologists and cardiologists observed in identifying risk parameters, PAH pathogenesis, diagnosis and combination therapy as a result of educational interventions is expected to result in improvement in clinical outcomes of patients with PAH.
AcknowledgementsThe clinical practice assessment was funded, in part, through an independent educational grant from Gilead Sciences Medical Affairs. Review and editorial help was provided by Karen Overstreet, EdD, RPh, FACEHP, CCMEP; Jennifer Brown, PhD; Christopher Clarke and Irina Kogan, all of Medscape Education.
References1. Brown LM, Chen H, Halpern S, et al. Delay in recognition of pulmonary arterial
hypertension: factors identified from the REVEAL Registry. Chest. 2011;140(1):19-26.2. Gillman J, BS, Farber HW, Miller DP, Meltzer LA, McGoon M. Pulmonary arterial hypertension
(PAH)-specific therapy at time of worsening to functional class IV in patients from The REVEAL Registry. Paper presented at: American Thoracic Society Meeting; May 18-23, 2012.
3. Badesch DB, Champion HC, Sanchez MA, et al. Diagnosis and assessment of pulmonary arterial hypertension. J Am Coll Cardiol. 2009; S61:555-566.
4. Tonelli AR, Alnuaimat H, Mubarak K. Pulmonary vasodilator testing and use of calcium channel blockers in pulmonary arterial hypertension. Respir Med. 2010; 104:481-496.
5. McLaughlin VV, Presberg KW, Doyle RL, et al; for the American Society of Chest Physicians. Prognosis of pulmonary arterial hypertension: ACCP evidence-based clinical practice guidelines. Chest. 2004;126(1 suppl):78S-92S.
6. McLaughlin V, Archer SL, Badesch DB, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension. J Am Coll Cardiol. 2009;53:1573-1619.
7. Barst RJ. Updated evidence-based treatment algorithm in pulmonary arterial hypertension. J Am Coll Cardiol. 2009; 54:(1):S78-S84.
Current Clinical Practices in PAH: Challenges and Opportunities to Improve Care Nimish Mehta, PhD, MBA, CCMEP1; Tara Herrmann, PhD1; Chad Williamson, MS, MBA2; Steven D Nathan, MD3
1Medscape, LLC, New York, NY, USA; 2CE Outcomes, LLC, Birmingham, AL, USA; 3Inova Fairfax Hospital, Falls Church, VA, USA
Availability of a treatment algorithm can improve
80%
60%
40%
20%
0%
11%16%
Every 3 months
Pulmonologists
Res
pons
es
CardiologistsPrimary Care Physicians Other Physicians
Every 6 months Only if there is an increase in the BNP level
Upon further clinical deterioration*
10%
24% 22% 21% 24% 24%
10% 13%6%
16%
58%51%
61%
37%
*Correct response
Figure 1. Right heart catheterization for diagnosis of PAH
80%
60%
40%
20%
0%6%
10%
Perform a cardiopulmonary exercise test
*Correct response
Pulmonologists
Res
pons
es
CardiologistsPrimary Care Physicians Other Physicians
Order a B-type natriureticpeptide (BNP) blood test
Perform a RHC* Perform a full cardiology workup
12% 13%5%
10%6%
13%
80%
66%61% 63%
10%16%
22%13%
80%
60%
40%
20%
0%
8%17%
20 mm Hg
Pulmonologists
Res
pons
es
CardiologistsPrimary Care Physicians Other Physicians
25 mm Hg* 30 mm Hg 45 mm Hg
13% 12%
77%
35%
58%50%
14%
66%
23%29%
2%
16%8% 9%
*Correct response
80%
60%
40%
20%
0%
13%
36%
The patient is high risk and should receive immediate
treatment with 2 prostanoid agents
Pulmonologists
Res
pons
es
CardiologistsPrimary Care Physicians Other Physicians
The patient is high risk andeither atrial septostomy orlung transplant should be
considered
The patient is low risk and should receive an initial
trial of an endothelin receptor antagonist (ERA)
or a PDE5 inhibitor.*
The patient is low risk andcould receive an initial trial
of an intravenous (IV)prostanoids.
20%
34%
3% 6% 3% 3%
80%
51%
72%63%
5% 9% 7%0%
*Correct response
A 42-year-old woman is referred to you for an evaluation of her PAH. She has an 8- to 9-month history of progressive dyspnea on exertion.• She ambulated 400 meters on 6-minute walk test (6MWT)• Echocardiogram showed an ejection fraction of 60%, an estimated right ventricular
systolic pressure of 48 mm Hg, normal right ventricular function, mild mitral regurgitation, and mild tricuspid regurgitation
Which of the following would be your next step in the diagnosis of this patient’s disease?
Figure 2. Recognition of appropriate mPAP value in the diagnosis of PAH
Pulmonary hypertension is generally defined as an mPAP value greater than or equal to:
Figure 3. Appropriate clinical decision in the setting of nonresponse to vasodilator challenge in PAH
If the patient is not a responder to a vasodilator challenge, which of the following would you do next?
Figure 4. Recognition of need for repeat right heart catheterization in PAH
When would you recommend a repeat RHC?
For more information contact Nimish Mehta, PhD, MBA, CCMEP, Director, Educational Strategy, Medscape, LLC, [email protected].
2
P O S T E R
Presented at CHEST in 2012; Poster contained data on baseline assessment and interim analysis.
“ Current Clinical Practices in PAH: Challenges and Opportunities to Improve Care”
8 9

2F O R M A T
PAH Curriculum with Baseline Assessment and Curriculum Level Outcomes. The PAH Curriculum, Living to Breathe, consisting of the baseline assessment and 4 educational activities, was posted online by Medscape on February 17, 2012. This educational grant was awarded to Medscape by Gilead Sciences Medical Affairs to develop continuing medical education (CME) using a curriculum model and to report metrics on the effect of the educational curriculum.
O V E R A L L I M P A C T S T A T E M E N T
G A P 1 : D I A G N O S I S ( B A S E L I N E A S S E S S M E N T )
G A P 2 : P A T H O P H Y S I O L O G Y ( B A S E L I N E A S S E S S M E N T )
G A P 4 : M O N I T O R I N G ( B A S E L I N E A S S E S S M E N T )
G A P 3 : E V I D E N C E - B A S E D T R E A T M E N T S T R A T E G I E S ( B A S E L I N E A S S E S S M E N T )
E D U C A T I O N A L I M P A C T
• Nearly 20% of pulmonologists, 40% of cardiologists, and 35% of PCPs did not recommend right heart catheterization to confi rm a diagnosis of PAH (Figure 1).
• Most respondents lacked confi dence in diagnosing PAH, with the majority of pulmonologists (57%), cardiologists (63%), and PCPs (62%) being only somewhat confi dent.
• Lack of familiarity with PAH was cited most frequently by respondents as a barrier to appropriate diagnosis.
• A wide variation in recognition of the defi nition of pulmonary hypertension as mean pulmonary artery pressure (mPAP) ≥ 25 mm Hg was observed (Figure 2).
• More than one-third of respondents (pulmonologists,34%; cardiologists, 39%; PCPs, 52%) did not recognize the role of phosphodiesterase type 5 (PDE-5) inhibition in the pathophysiology of PAH.
• When deciding to repeat right heart catheterization, 43% of pulmonologists, 39% of cardiologists, and 49% of PCPs would base their decision on parameters other than the magnitude of clinical deterioration.
• More than 16% of pulmonologists, 31% of cardiologists, and 56% of PCPs would not perform monthly liver function tests to monitor a patient taking bosentan.
• Almost 75% of pulmonologists, 80% of cardiologists, and 90% of PCPs are not at all confi dent or are somewhat confi dent in their ability to monitor patients with PAH for clinical deterioration and for treatment eff ects and toxicities.
• More than 68% of pulmonologists, 74% of cardiologists, and 82% of PCPs reported that their practices do not use an algorithm for PAH management.
• Close to 20% of pulmonologists, 30% of cardiologists, and 50% of PCPs could not identify the correct risk level or therapy for the low-risk patient (Figure 3).
• Most respondents (pulmonologists, 61%; cardiologists, 59%; PCPs, 43%) are only somewhat confi dent in their ability to individualize PAH treatment based on functional classifi cation, comorbid conditions, and risk assessment.
• A substantial percentage of physicians are “not at all confi dent” (pulmonologists, 22%; cardiologists, 31%; PCPs, 54%).
• The majority of physicians (pulmonologists, 89%; cardiologists, 85%; PCPs, 78%) recognized that a patient with PAH who remains in WHO functional class 3 or 4 and whose mPAP remains elevated after initial therapy should receive dual or triple therapy.
In total, 3071 physicians responded to the baseline assessment (1100 pulmonologists, 489 cardiologists, 1177 primary care providers [PCPs], and 305 other physicians). The results obtained demonstrate signifi cant gaps in knowledge of PAH pathogenesis and knowledge and skills surrounding diagnosis, risk
stratifi cation, monitoring for disease activity, setting treatment goals, and interpreting the rationale for combination therapy in all clinical specialties. After the educational intervention, physicians showed statistically signifi cant improvement.
An interim analysis of the assessment of a subset of physicians participating in 3 educational interventions showed signifi cant improvement in the following areas:
• At least 75% of all respondents recognized that an elevated right atrial pressure and a cardiac index of 1.6 L/min/m2 would place a patient with PAH at greatest risk.
• Signifi cantly more cardiologists (65% before participation in the activity and 88% after participation; P=.03) and pulmonologists (68% before and 87% after; P=.006) recognized the action of PDE-5 inhibitors in relation to PAH pathogenesis.
• When compared to baseline, 13% more pulmonologists (P=.04) and 16% more cardiologists (P=.12) correctly identifi ed 25 mm Hg as the cut-off mPAP value to diagnose PAH.
• A total of 15% of pulmonologists were signifi cantly more likely (P=.02) to recognize that the goal of combination therapy is to maximize effi cacy, minimize toxicity, and allow for targeting of multiplepathologic pathways.
• Signifi cantly more cardiologists would consider combination therapy for PAH in the appropriate clinical circumstance after participation in the educational activity compared with cardiologists in the baseline sample (76% before and 98% after; P=.002).
EFFECTIVENESS OF COMPLETED OUTCOMES STUDY
“ Current Clinical Practices in PAH: Challenges and Opportunities to Improve Care”
PurposePulmonary arterial hypertension (PAH) -- a progressive and fatal disorder -- is underrecognized and inadequately treated based on current evidence-based guideline recommendations. Delays in diagnosis of more than 2 years and inadequate treatment have been identified from the REVEAL registry.1, 2 The objective of this study was to assess the current clinical practice of pulmonologists, cardiologists, and primary care physicians in PAH management to identify knowledge, competency, and practice gaps and barriers to improving the diagnosis and care of patients with this condition. An interim analysis of educational impact was also performed to determine improvement in clinical practice compared to baseline.
Methods• The needs assessment survey consisted of 25 items
based on current evidence-based consensus guidelines. • The assessment design included knowledge- and
case-based, multiple-choice questions made available online to Medscape membership of healthcare providers without monetary compensation or charge.
• Case vignettes and associated assessment question responses were used to analyze data on clinicians’ baseline knowledge, skills, attitudes, practice patterns, and perceived barriers related to the optimal management of patients with PAH.3-7
• The assessment instrument and the reporting metrics were organized by the assessment domains of diagnosis, pathophysiology, evidence-based treatment strategies, and monitoring.
• Confidentiality of survey respondents was maintained and responses were de-identified and aggregated prior to analysis. The assessment was posted online at http://www.medscape.org/viewarticle/758455. The survey launched on Medscape Education Pulmonary Medicine on February 17, 2012 and participant responses were collected until July 31, 2012.
• In addition to providing baseline data on clinical practice gaps, the data obtained from the baseline assessment were designed to serve as the control group for the practice outcomes assessment of the educational
curriculum. Questions from the clinical practice assessment are aligned to individual curriculum programs and posed to program participants following completion of each curriculum activity, to assess the curriculum outcomes.
ResultsIn total, 3071 physicians responded to the survey (1100 pulmonologists, 489 cardiologists, 1177 primary care providers [PCPs], and 305 other physicians). The results obtained demonstrate significant gaps in knowledge of PAH pathogenesis, and knowledge and skills surrounding diagnosis, risk
stratification, monitoring for disease activity, setting treatment goals, and interpreting the rationale for combination therapy in all clinical specialties.
Diagnosis• Nearly 20% of pulmonologists, 40% of cardiologists,
and 35% of PCPs did not recommend right heart catheterization to confirm a diagnosis of PAH (Figure 1).
• Most respondents lack confidence in diagnosing PAH, with the majority of pulmonologists (57%), cardiologists (63%), and PCPs (62%) being only somewhat confident.
• Lack of familiarity with PAH was cited most frequently by respondents as a barrier to appropriate diagnosis.
• A wide variation in recognition of the definition of pulmonary hypertension as mean pulmonary artery pressure (mPAP) ≥ 25 mm Hg was observed (Figure 2).
Pathophysiology• More than one-third of respondents (pulmonologists,
34%; cardiologists, 39%; PCPs, 52%) did not recognize the role of phosphodiesterase type 5 (PDE-5) inhibition in the pathophysiology of PAH.
Evidence-based Treatment Strategies• More than 68% of
pulmonologists, 74% of cardiologists, and 82% of PCPs reported that their practices do not use an algorithm for PAH management.
• Close to 20% of pulmonologists, 30% of cardiologists, and 50% of PCPs could not identify the correct risk level or therapy for the low-risk patient (Figure 3).
• Most respondents (pulmonologists, 61%; cardiologists, 59%; PCPs, 43%) are only somewhat confident in their ability to individualize PAH treatment based on functional classification, comorbid conditions, and risk assessment. Moreover, a substantial percentage of physicians are “not at all confident” (pulmonologists, 22%; cardiologists, 31%; PCPs, 54%).
• The majority of physicians (pulmonologists, 89%; cardiologists, 85%; PCPs, 78%) recognized that a patient with PAH who remains in WHO functional class 3 or 4 and whose mPAP remains elevated after initial therapy should receive dual or triple therapy.
Monitoring• When deciding to repeat right heart catheterization,
43% of pulmonologists, 39% of cardiologists, and 49% of PCPs would base their decision on parameters other than the magnitude of clinical deterioration (Figure 4).
• More than 16% of pulmonologists, 31% of cardiologists, and 56% of PCPs would not perform monthly liver function tests to monitor a patient taking bosentan.
• Almost 75% of pulmonologists, 80% of cardiologists, and 90% of PCPs are not at all confident or are somewhat confident in their ability to monitor patients with PAH for clinical deterioration and for treatment effects and toxicities.
Educational Impact An interim analysis of the assessment of a subset of physicians participating in 3 educational interventions showed significant improvement in the following areas:
• At least 75% of all respondents recognized that an elevated right atrial pressure and a cardiac index of 1.6 L/min/m2 would place a patient with PAH at greatest risk.
• Significantly more cardiologists (65% before participation in the activity and 88% after participation; P=.03) and pulmonologists (68% before and 87% after; P=.006) recognized the action of PDE-5 inhibitors in relation to PAH pathogenesis.
• When compared to baseline, 13% more pulmonologists (P=.04) and 16% more cardiologists (P=.12) correctly identified 25 mm Hg as the cut-off mPAP value to diagnose PAH.
• A total of 15% more pulmonologists were significantly more likely (P=.02) to recognize that the goal of combination therapy is to maximize efficacy, minimize toxicity, and allow for targeting of multiple pathologic pathways.
• Significantly more cardiologists would consider combination therapy for PAH in the appropriate clinical circumstance after participation in the educational activity compared with cardiologists in the baseline sample (76% before and 98% after; P=.002).
Conclusions and Clinical Implications
• This assessment of healthcare providers’ clinical practices identified gaps in PAH diagnosis and management among pulmonologists, cardiologists, and PCPs. — A significant proportion of physicians, regardless
of specialty, would fail to perform right heart catheterization to confirm a diagnosis of PAH, which may result in misdiagnosis or underdiagnosis of the condition. This may be due to a lack of physician familiarity with PAH and its diagnostic algorithm.
— Availability of a treatment algorithm can improve multiple aspects of care and management of patients with PAH. This is especially true in cases of rare diseases like PAH, where knowledge may be limited and physician confidence low. Thus, it is critical that more practices and medical institutions obtain and make available a PAH treatment decision tree for their clinicians.
— Knowledge of current PAH guideline recommendations on the management of PAH is suboptimal, particularly the monitoring and augmentation of therapy in patients with unstable disease.
— Future programs emphasizing the optimization of the timing of monitoring and appropriate augmentation of therapy in patients with PAH are needed to improve clinical outcomes.
• Significant improvement in the knowledge of pulmonologists and cardiologists observed in identifying risk parameters, PAH pathogenesis, diagnosis and combination therapy as a result of educational interventions is expected to result in improvement in clinical outcomes of patients with PAH.
AcknowledgementsThe clinical practice assessment was funded, in part, through an independent educational grant from Gilead Sciences Medical Affairs. Review and editorial help was provided by Karen Overstreet, EdD, RPh, FACEHP, CCMEP; Jennifer Brown, PhD; Christopher Clarke and Irina Kogan, all of Medscape Education.
References1. Brown LM, Chen H, Halpern S, et al. Delay in recognition of pulmonary arterial
hypertension: factors identified from the REVEAL Registry. Chest. 2011;140(1):19-26.2. Gillman J, BS, Farber HW, Miller DP, Meltzer LA, McGoon M. Pulmonary arterial hypertension
(PAH)-specific therapy at time of worsening to functional class IV in patients from The REVEAL Registry. Paper presented at: American Thoracic Society Meeting; May 18-23, 2012.
3. Badesch DB, Champion HC, Sanchez MA, et al. Diagnosis and assessment of pulmonary arterial hypertension. J Am Coll Cardiol. 2009; S61:555-566.
4. Tonelli AR, Alnuaimat H, Mubarak K. Pulmonary vasodilator testing and use of calcium channel blockers in pulmonary arterial hypertension. Respir Med. 2010; 104:481-496.
5. McLaughlin VV, Presberg KW, Doyle RL, et al; for the American Society of Chest Physicians. Prognosis of pulmonary arterial hypertension: ACCP evidence-based clinical practice guidelines. Chest. 2004;126(1 suppl):78S-92S.
6. McLaughlin V, Archer SL, Badesch DB, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension. J Am Coll Cardiol. 2009;53:1573-1619.
7. Barst RJ. Updated evidence-based treatment algorithm in pulmonary arterial hypertension. J Am Coll Cardiol. 2009; 54:(1):S78-S84.
Current Clinical Practices in PAH: Challenges and Opportunities to Improve Care Nimish Mehta, PhD, MBA, CCMEP1; Tara Herrmann, PhD1; Chad Williamson, MS, MBA2; Steven D Nathan, MD3
1Medscape, LLC, New York, NY, USA; 2CE Outcomes, LLC, Birmingham, AL, USA; 3Inova Fairfax Hospital, Falls Church, VA, USA
Availability of a treatment algorithm can improve
80%
60%
40%
20%
0%
11%16%
Every 3 months
Pulmonologists
Res
pons
es
CardiologistsPrimary Care Physicians Other Physicians
Every 6 months Only if there is an increase in the BNP level
Upon further clinical deterioration*
10%
24% 22% 21% 24% 24%
10% 13%6%
16%
58%51%
61%
37%
*Correct response
Figure 1. Right heart catheterization for diagnosis of PAH
80%
60%
40%
20%
0%6%
10%
Perform a cardiopulmonary exercise test
*Correct response
Pulmonologists
Res
pons
es
CardiologistsPrimary Care Physicians Other Physicians
Order a B-type natriureticpeptide (BNP) blood test
Perform a RHC* Perform a full cardiology workup
12% 13%5%
10%6%
13%
80%
66%61% 63%
10%16%
22%13%
80%
60%
40%
20%
0%
8%17%
20 mm Hg
Pulmonologists
Res
pons
es
CardiologistsPrimary Care Physicians Other Physicians
25 mm Hg* 30 mm Hg 45 mm Hg
13% 12%
77%
35%
58%50%
14%
66%
23%29%
2%
16%8% 9%
*Correct response
80%
60%
40%
20%
0%
13%
36%
The patient is high risk and should receive immediate
treatment with 2 prostanoid agents
Pulmonologists
Res
pons
es
CardiologistsPrimary Care Physicians Other Physicians
The patient is high risk andeither atrial septostomy orlung transplant should be
considered
The patient is low risk and should receive an initial
trial of an endothelin receptor antagonist (ERA)
or a PDE5 inhibitor.*
The patient is low risk andcould receive an initial trial
of an intravenous (IV)prostanoids.
20%
34%
3% 6% 3% 3%
80%
51%
72%63%
5% 9% 7%0%
*Correct response
A 42-year-old woman is referred to you for an evaluation of her PAH. She has an 8- to 9-month history of progressive dyspnea on exertion.• She ambulated 400 meters on 6-minute walk test (6MWT)• Echocardiogram showed an ejection fraction of 60%, an estimated right ventricular
systolic pressure of 48 mm Hg, normal right ventricular function, mild mitral regurgitation, and mild tricuspid regurgitation
Which of the following would be your next step in the diagnosis of this patient’s disease?
Figure 2. Recognition of appropriate mPAP value in the diagnosis of PAH
Pulmonary hypertension is generally defined as an mPAP value greater than or equal to:
Figure 3. Appropriate clinical decision in the setting of nonresponse to vasodilator challenge in PAH
If the patient is not a responder to a vasodilator challenge, which of the following would you do next?
Figure 4. Recognition of need for repeat right heart catheterization in PAH
When would you recommend a repeat RHC?
For more information contact Nimish Mehta, PhD, MBA, CCMEP, Director, Educational Strategy, Medscape, LLC, [email protected].
10 11
background
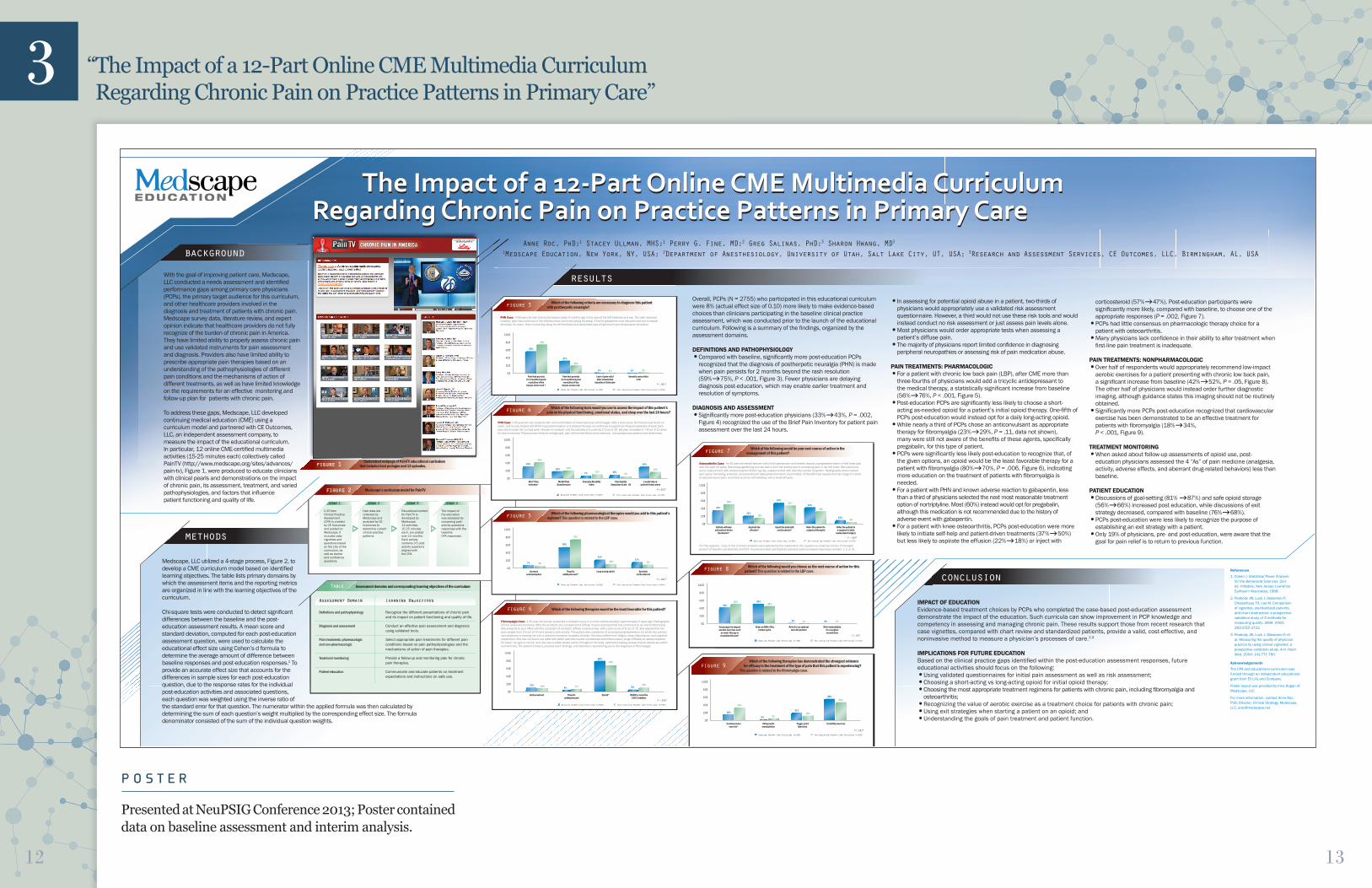
With the goal of improving patient care, Medscape, LLC conducted a needs assessment and identifi ed performance gaps among primary care physicians (PCPs), the primary target audience for this curriculum, and other healthcare providers involved in the diagnosis and treatment of patients with chronic pain. Medscape survey data, literature review, and expert opinion indicate that healthcare providers do not fully recognize of the burden of chronic pain in America. They have limited ability to properly assess chronic pain and use validated instruments for pain assessment and diagnosis. Providers also have limited ability to prescribe appropriate pain therapies based on an understanding of the pathophysiologies of different pain conditions and the mechanisms of action of different treatments, as well as have limited knowledge on the requirements for an effective monitoring and follow-up plan for patients with chronic pain.
To address these gaps, Medscape, LLC developed continuing medical education (CME) using a curriculum model and partnered with CE Outcomes, LLC, an independent assessment company, to measure the impact of the educational curriculum. In particular, 12 online CME-certifi ed multimedia activities (15-25 minutes each) collectively called PainTV (http://www.medscape.org/sites/advances/pain-tv), Figure 1, were produced to educate clinicians with clinical pearls and demonstrations on the impact of chronic pain, its assessment, treatment, and varied pathophysiologies, and factors that infl uence patient functioning and quality of life.
Anne Roc, PhD;1 Stacey Ullman, MHS;1 Perry G. Fine, MD;2 Greg Salinas, PhD;3 Sharon Hwang, MD3 1Medscape Education, New York, NY, USA; 2Department of Anesthesiology, University of Utah, Salt Lake City, UT, USA; 3Research and Assessment Services, CE Outcomes, LLC, Birmingham, AL, USA
The Impact of a 12-Part Online CME Multimedia Curriculum Regarding Chronic Pain on Practice Patterns in Primary Care
methods
Medscape, LLC utilized a 4-stage process, Figure 2, to develop a CME curriculum model based on identifi ed learning objectives. The table lists primary domains by which the assessment items and the reporting metrics are organized in line with the learning objectives of the curriculum.
Chi-square tests were conducted to detect signifi cant differences between the baseline and the post-education assessment results. A mean score and standard deviation, computed for each post-education assessment question, were used to calculate the educational effect size using Cohen’s d formula to determine the average amount of difference between baseline responses and post-education responses.1 To provide an accurate effect size that accounts for the differences in sample sizes for each post-education question, due to the response rates for the individual post-education activities and associated questions, each question was weighted using the inverse ratio of the standard error for that question. The numerator within the applied formula was then calculated by determining the sum of each question’s weight multiplied by the corresponding effect size. The formula denominator consisted of the sum of the individual question weights.
resultsOverall, PCPs (N = 2755) who participated in this educational curriculum were 8% (actual effect size of 0.10) more likely to make evidence-based choices than clinicians participating in the baseline clinical practice assessment, which was conducted prior to the launch of the educational curriculum. Following is a summary of the fi ndings, organized by the assessment domains.
DEFINITIONS AND PATHOPHYSIOLOGY• Compared with baseline, signifi cantly more post-education PCPs
recognized that the diagnosis of postherpetic neuralgia (PHN) is made when pain persists for 2 months beyond the rash resolution (59%75%, P < .001, Figure 3). Fewer physicians are delaying diagnosis post-education, which may enable earlier treatment and resolution of symptoms.
DIAGNOSIS AND ASSESSMENT • Signifi cantly more post-education physicians (33%43%, P = .002,
Figure 4) recognized the use of the Brief Pain Inventory for patient pain assessment over the last 24 hours.
• In assessing for potential opioid abuse in a patient, two-thirds of physicians would appropriately use a validated risk assessment questionnaire. However, a third would not use these risk tools and would instead conduct no risk assessment or just assess pain levels alone.
• Most physicians would order appropriate tests when assessing a patient’s diffuse pain.
• The majority of physicians report limited confi dence in diagnosing peripheral neuropathies or assessing risk of pain medication abuse.
PAIN TREATMENTS: PHARMACOLOGIC• For a patient with chronic low back pain (LBP), after CME more than
three-fourths of physicians would add a tricyclic antidepressant to the medical therapy, a statistically signifi cant increase from baseline (56%76%, P < .001, Figure 5).
• Post-education PCPs are signifi cantly less likely to choose a short-acting as-needed opioid for a patient’s initial opioid therapy. One-fi fth of PCPs post-education would instead opt for a daily long-acting opioid.
• While nearly a third of PCPs chose an anticonvulsant as appropriate therapy for fi bromyalgia (23%29%, P = .11, data not shown), many were still not aware of the benefi ts of these agents, specifi cally pregabalin, for this type of patient.
• PCPs were signifi cantly less likely post-education to recognize that, of the given options, an opioid would be the least favorable therapy for a patient with fi bromyalgia (80%70%, P = .006, Figure 6), indicating more education on the treatment of patients with fi bromyalgia is needed.
• For a patient with PHN and known adverse reaction to gabapentin, less than a third of physicians selected the next most reasonable treatment option of nortriptyline. Most (60%) instead would opt for pregabalin, although this medication is not recommended due to the history of adverse event with gabapentin.
• For a patient with knee osteoarthritis, PCPs post-education were more likely to initiate self-help and patient-driven treatments (37%50%) but less likely to aspirate the effusion (22%18%) or inject with
corticosteroid (57%47%). Post-education participants were signifi cantly more likely, compared with baseline, to choose one of the appropriate responses (P = .002, Figure 7).
• PCPs had little consensus on pharmacologic therapy choice for a patient with osteoarthritis.
• Many physicians lack confi dence in their ability to alter treatment when fi rst-line pain treatment is inadequate.
PAIN TREATMENTS: NONPHARMACOLOGIC• Over half of respondents would appropriately recommend low-impact
aerobic exercises for a patient presenting with chronic low back pain, a signifi cant increase from baseline (42%52%, P = .05, Figure 8). The other half of physicians would instead order further diagnostic imaging, although guidance states this imaging should not be routinely obtained.
• Signifi cantly more PCPs post-education recognized that cardiovascular exercise has been demonstrated to be an effective treatment for patients with fi bromyalgia (18%34%, P < .001, Figure 9).
TREATMENT MONITORING• When asked about follow-up assessments of opioid use, post-
education physicians assessed the 4 “As” of pain medicine (analgesia, activity, adverse effects, and aberrant drug-related behaviors) less than baseline.
PATIENT EDUCATION• Discussions of goal-setting (81% 87%) and safe opioid storage
(56%66%) increased post education, while discussions of exit strategy decreased, compared with baseline (76%68%).
• PCPs post-education were less likely to recognize the purpose of establishing an exit strategy with a patient.
• Only 19% of physicians, pre- and post-education, were aware that the goal for pain relief is to return to previous function.
conclusion
IMPACT OF EDUCATIONEvidence-based treatment choices by PCPs who completed the case-based post-education assessment demonstrate the impact of the education. Such curricula can show improvement in PCP knowledge and competency in assessing and managing chronic pain. These results support those from recent research that case vignettes, compared with chart review and standardized patients, provide a valid, cost-effective, and noninvasive method to measure a physician’s processes of care.2,3
IMPLICATIONS FOR FUTURE EDUCATIONBased on the clinical practice gaps identifi ed within the post-education assessment responses, future educational activities should focus on the following:• Using validated questionnaires for initial pain assessment as well as risk assessment;• Choosing a short-acting vs long-acting opioid for initial opioid therapy;• Choosing the most appropriate treatment regimens for patients with chronic pain, including fi bromyalgia and
osteoarthritis;• Recognizing the value of aerobic exercise as a treatment choice for patients with chronic pain;• Using exit strategies when starting a patient on an opioid; and• Understanding the goals of pain treatment and patient function.
References
1. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, New Jersey: Lawrence Earlbaum Associates; 1988.
2. Peabody JW, Luck J, Glassman P, Dresselhaus TR, Lee M. Comparison of vignettes, standardized patients, and chart abstraction: a prospective validation study of 3 methods for measuring quality. JAMA. 2000; 283:1715-1722.
3. Peabody JW, Luck J, Glassman P, et al. Measuring the quality of physician practice by using clinical vignettes: a prospective validation study. Ann Intern Med. 2004; 141:771-780.
Acknowledgements
The CPA and educational curriculum was funded through an independent educational grant from Eli Lilly and Company.
Poster layout was provided by Irina Kogan of Medscape, LLC.
For more information, contact Anne Roc, PhD, Director, Clinical Strategy, Medscape, LLC, [email protected].
figure 1 Customized webpage of PainTV educational curriculum that includes host prologue and 12 episodes.
The Impact of a 12-Part Online CME Multimedia Curriculum Regarding Chronic Pain on Practice Patterns in Primary Care
figure 2 Medscape’s curriculum model for PainTV
stage 1 stage 2 stage 3 stage 4
A 25 item Clinical Practice Assessment (CPA) is created by CE Outcomes and posted on Medscape. It includes case vignettes and questions based on the LOs of the curriculum, as well as barrier and confi dence questions.
User data are collected by Medscape and analyzed by CE Outcomes to determine current clinical practice patterns.
Educational content for PainTV is developed by Medscape: 12 activities, 15-25 minutes each, are posted over 12 months. Each activity contains 3-5 post-activity questions aligned with the CPA.
The impact of the education was assessed by comparing post-activity questions responses with the baseline CPA responses.
Table Assessment domains and corresponding learning objectives of the curriculum
Assessment Domain Learning Objectives
Defi nitions and pathophysiology Recognize the different presentations of chronic pain and its impact on patient functioning and quality of life.
Diagnosis and assessment Conduct an effective pain assessment and diagnosis using validated tools.
Pain treatments: pharmacologic Select appropriate pain treatments for different pain and non-pharmacologic conditions based on pain pathophysiologies and the mechanisms of action of pain therapies.
Treatment monitoring Provide a follow-up and monitoring plan for chronic pain therapies.
Patient education Communicate and educate patients on treatment expectations and instructions on safe use.
figure 3
Pain that persists for 2 months beyond
resolution of the herpes zoster rash *
Pain that persists for 6 months beyond
resolution of the herpes zoster rash
Lack of pain relief after intradermal
injection of lidocaine
Varicella zoster titler 1:16
Post-education Primary Care Physicians (n=349)Baseline Primary Care Physicians (n=290)
P<.001*
PHN Case: A 59-year-old man had acute herpes zoster 9 months ago in the area of his left forehead and eye. The rash resolved; however, pain has continued in the affected area and is disrupting his sleep. A trial of gabapentin was discontinued due to severe dizziness. On exam, there is scarring along his left forehead and associated loss of light touch and temperature sensation.
100%
80%
60%
40%
20%
0%
59%
37%
2%2%
75%
20%
4%1%
Which of the following criteria are necessary to diagnose this patient with postherpetic neuralgia?
figure 4
Brief Pain Inventory*
McGill Pain Questionnaire
I would rely on patient history alone
Oswestry Disability Index
Pain Anxiety Symptoms Scale - 20
Post-education Primary Care Physicians (n=750)Baseline Primary Care Physicians (n=290)
P =.002*
PHN Case: A 35-year-old man presents with a 6-month history of lower back pain which began after a work injury. No fracture was found on exam, and he was treated with 4000 mg acetaminophen and physical therapy. He continues to experience frequent episodes of lower back pain which cause him to miss work. His pain is constant, and he indicates it is currently 2-3 out of 10. His pain increases to 7-8 out of 10 when he tries to exercise. Physical exam fi nds an antalgic gait, pain with lumbar fl exion and extension, and paraspinous spasms and tenderness.
100%
80%
60%
40%
20%
0%
33%
20%
30%
10%7%
43%
22% 18%6%
11%
Which of the following tools would you use to assess the impact of this patient’s pain on his physical functioning, emotional status, and sleep over the last 24 hours?
figure 5
Increase acetaminophen
Tricyclic antidepressant*
Long-acting opioid Systemic corticosteroid
Post-education Primary Care Physicians (n=464)Baseline Primary Care Physicians (n=290)
P <.001*
100%
80%
60%
40%
20%
0%
7%
56%
17%21%
6%
76%
8%10%
Which of the following pharmacological therapies would you add to this patient’s regimen? This question is related to the LBP case.
figure 6
Anticonvulsant Tricyclic antidepressant
Opioid* NSAID or selective COX-2 inhibitor
Post-education Primary Care Physicians (n=320)Baseline Primary Care Physicians (n=290)
P=.006*
Fibromyalgia Case: A 45-year-old woman sustained a whiplash injury in a motor vehicle accident approximately 5 years ago. Radiographs did not reveal any fractures. After the accident, she complained of diffuse muscle soreness that has continued on an intermittent basis. She presents to your offi ce with the complaint of constant, diffuse muscle aches, with a pain score of 6 out of 10. She reports that her pain ranges from 3-9 out of 10 and worsens with activity. The patient also complains of accompanying depression, for which her primary care physician is treating her with a selective serotonin reuptake inhibitor. She also suffers from fatigue, sleep disturbance, and cognitive impairment. She has not found any relief with either over-the-counter nonsteroidal anti-infl ammatory drugs (NSAIDs) or acetaminophen. On exam, her gait is normal, and she has multiple tender points throughout her body. Laboratory testing reveals that all results are within normal limits. The patient’s history, physical exam fi ndings, and laboratory results bring you to the diagnosis of fi bromyalgia.
100%
80%
60%
40%
20%
0%
11%4% 5%
80%
10% 7% 12%
70%
Which of the following therapies would be the least favorable for this patient?
figure 7
Initiate self-help and patient-driven
treatments*
Aspirate the effusion*
Inject the joint with corticosteroid*
Refer the patient to a physical therapist
Refer the patient to a surgeon for joint
replacement surgery
Post-education Primary Care Physicians (n=245)Baseline Primary Care Physicians (n=290)P=.002*
Osteoarthritis Case: An 81-year-old retired teacher with mild hypertension and obesity reports a progressive history of left knee pain over the past 10 years. She enjoys gardening but has had to limit her activity due to increasing pain in her left knee. She has found some improvement with acetaminophen 4000 mg/day, supplemented with over-the-counter ibuprofen. Radiographs show marked joint space narrowing, sclerosis, and periarticular osteophyte formation. Examination of the left knee reveals that her range of motion is reduced due to pain, and there is some mild swelling, with a small effusion.
For this question, if any of the 3 correct answers were selected by the respondent, the question is coded as correct. Forty-eight percent of baseline participants and 61% of post-education participants selected evidence-based responses (answer 1, 2, or 3).
100%
80%
60%
40%
20%
0%
37%
22%
44%
12%
57%50%
18%
35%
6%
47%
Which of the following would be your next course of action in the management of this patient?
figure 8
Encourage low-impact aerobic exercises such
as water therapy or recumbent bicycle*
Order an MRI of the lumbar spine
Refer for an epidural steroid injection
Refer immediately for a surgical consultation
Post-education Primary Care Physicians (n=162)Baseline Primary Care Physicians (n=290)
P=.05*
100%
80%
60%
40%
20%
0%
42%54%
0%3%
52%46%
1%2%
Which of the following would you choose as the next course of action for this patient? This question is related to the LBP case.
figure 9
Cardiovascular exercise*
Chiropractic manipulation
Trigger point injections
Flexibility exercises
Post-education Primary Care Physicians (n=320)Baseline Primary Care Physicians (n=290)
P<.001*
100%
80%
60%
40%
20%
0%
18%
3%
58%
21%
34%
5%
45%
16%
Which of the following therapies has demonstrated the strongest evidence for effi cacy in the treatment of the type of pain that this patient is experiencing? This question is related to the fi bromyalgia case.
3
P O S T E R
Presented at NeuPSIG Conference 2013; Poster contained data on baseline assessment and interim analysis.
“ The Impact of a 12-Part Online CME Multimedia Curriculum Regarding Chronic Pain on Practice Patterns in Primary Care”
12 13

F O R M A T
PainTV Curriculum with Baseline Assessment and Curriculum Level Outcomes. The PainTV Curriculum, consisting of the baseline assessment and 12 educational activities, was posted online by Medscape on September 2011 and continued through 2012. The PainTV educational series was designed to address this significant public health problem by educating clinicians who treat patients with chronic pain through a series of short video commentaries that present clinical pearls and demonstrations on specific topics related to chronic pain management. Collectively, the series aimed to raise clinician awareness of the impact of chronic pain; its assessment, treatment, and varied pathophysiologies; and factors that can influence patient functioning and quality of life. This educational grant was awarded to Medscape by Lilly USA, LLC.
O V E R A L L I M P A C T S T A T E M E N T
G A P 1 : D E F I N I T I O N S A N D P A T H O P H Y S I O L O G Y
G A P 2 : D I A G N O S O S A N D A S S E S S M E N T
G A P 4 : P A I N T R E A T M E N T S — N O N P H A R M A C O L O G I C
G A P 5 : P A T I E N T E D U C A T I O N
G A P 3 : P A I N T R E A T M E N T S — P H A R M A C O L O G I C
E D U C A T I O N A L I M P A C T
• Compared with baseline, signifi cantly more post-education PCPs recognized that the diagnosis of postherpetic neuralgia (PHN) is made when pain persists for 2 months beyond the rash resolution
(59% at baseline vs 75% post-education, P< .001). Fewer physicians are delaying diagnosis post-education, which may enable earlier treatment and resolution of symptoms.
• Signifi cantly more post-education physicians (33% at baseline vs 43% post-education, P=.002) recognized the use of the Brief Pain Inventory for patient pain assessment over the last 24 hours.
• Over half of respondents would appropriately recommend low-impact aerobic exercises for a patient presenting with chronic low back pain, a signifi cant increase from baseline (42% at baseline vs 52% post-education, P=.05).
• The other half of physicians would instead order further diagnostic imaging, although guidance states this imaging should not be routinely obtained.
• Signifi cantly more PCPs post-education recognized that cardiovascular exercise has been demonstrated to be an eff ective treatment for patients with fi bromyalgia (18% at baseline vs 34% post-education,P<.001).
• Discussions of goal-setting (81% at baseline vs 87% post-education) and safe opioid storage (56% at baseline vs 66% post education) increased
post-education, while discussions of exit strategy decreased, compared with baseline (76% vs 68%).
• For a patient with chronic low back pain (LBP), after CME more than three-fourths of physicians would add a tricyclic antidepressant to the medical therapy, a statistically signifi cant increase from baseline (56% at baseline vs 76% post-education, P<.001).
• Post-education PCPs are signifi cantly less likely to choose a short acting as-needed opioid for a patient’s initial opioid therapy. One-fi fth of PCPs post-education would instead opt for a daily long-acting opioid.
• For a patient with knee osteoarthritis, PCPs post-education were more likely to initiate self-help and patient-driven treatments (37% at baseline vs 50% post-education) but less likely to aspirate the eff usion (22% at baseline vs 18% post-education) or inject with corticosteroid (57% at baseline vs 47% post-education). Post-education participants were signifi cantly more likely, compared with baseline, to choose one of the appropriate responses (P=.002).
Evidence-based treatment choices by PCPs who completed the case-based post-education assessment demonstrate the impact of the education. Such curricula can show improvement in PCP knowledge and competency in assessing and
managing chronic pain. These results support those from recent research that case vignettes, compared with chart review and standardized patients, provide a valid, cost-eff ective, and noninvasive method to measure a physician’s processes of care.
In comparing participants’ curriculum post-education assessment responses with the responses obtained in the baseline clinical practice assessment, primary care physicians are signifi cantly more likely post-education to:
• Recognize that the diagnosis of postherpetic neuralgia (PHN) is made when pain persists for 2 months beyond the rash resolution (75% post-education vs 59% at baseline, P<.001*);
• Utilize the Brief Pain Inventory to assess the impact of a patient’s pain on his physical functioning, emotional status, and sleep, over the last 24 hours (43% post education vs 33% at baseline, P=.02*);
• Properly adjust the pain medicine regimen of a patient with chronic low back pain (76% post-education vs 56% at baseline, P<.001*);
• Choose an appropriate course of action for a patient presenting with osteoarthritis of the knee (61% post education vs 48% at baseline, P=.002*);
• Recognize the value of cardiovascular exercise for a patient with fi bromyalgia (34% post education vs 18% at baseline, P<.001*); and
• Encourage low-impact aerobic exercises for a patient presenting with chronic low back pain (52% post education vs 42% at baseline, P=.05*).
EFFECTIVENESS OF COMPLETED OUTCOMES STUDY
3 “ The Impact of a 12-Part Online CME Multimedia Curriculum Regarding Chronic Pain on Practice Patterns in Primary Care”
background
With the goal of improving patient care, Medscape, LLC conducted a needs assessment and identifi ed performance gaps among primary care physicians (PCPs), the primary target audience for this curriculum, and other healthcare providers involved in the diagnosis and treatment of patients with chronic pain. Medscape survey data, literature review, and expert opinion indicate that healthcare providers do not fully recognize of the burden of chronic pain in America. They have limited ability to properly assess chronic pain and use validated instruments for pain assessment and diagnosis. Providers also have limited ability to prescribe appropriate pain therapies based on an understanding of the pathophysiologies of different pain conditions and the mechanisms of action of different treatments, as well as have limited knowledge on the requirements for an effective monitoring and follow-up plan for patients with chronic pain.
To address these gaps, Medscape, LLC developed continuing medical education (CME) using a curriculum model and partnered with CE Outcomes, LLC, an independent assessment company, to measure the impact of the educational curriculum. In particular, 12 online CME-certifi ed multimedia activities (15-25 minutes each) collectively called PainTV (http://www.medscape.org/sites/advances/pain-tv), Figure 1, were produced to educate clinicians with clinical pearls and demonstrations on the impact of chronic pain, its assessment, treatment, and varied pathophysiologies, and factors that infl uence patient functioning and quality of life.
Anne Roc, PhD;1 Stacey Ullman, MHS;1 Perry G. Fine, MD;2 Greg Salinas, PhD;3 Sharon Hwang, MD3 1Medscape Education, New York, NY, USA; 2Department of Anesthesiology, University of Utah, Salt Lake City, UT, USA; 3Research and Assessment Services, CE Outcomes, LLC, Birmingham, AL, USA
The Impact of a 12-Part Online CME Multimedia Curriculum Regarding Chronic Pain on Practice Patterns in Primary Care
methods
Medscape, LLC utilized a 4-stage process, Figure 2, to develop a CME curriculum model based on identifi ed learning objectives. The table lists primary domains by which the assessment items and the reporting metrics are organized in line with the learning objectives of the curriculum.
Chi-square tests were conducted to detect signifi cant differences between the baseline and the post-education assessment results. A mean score and standard deviation, computed for each post-education assessment question, were used to calculate the educational effect size using Cohen’s d formula to determine the average amount of difference between baseline responses and post-education responses.1 To provide an accurate effect size that accounts for the differences in sample sizes for each post-education question, due to the response rates for the individual post-education activities and associated questions, each question was weighted using the inverse ratio of the standard error for that question. The numerator within the applied formula was then calculated by determining the sum of each question’s weight multiplied by the corresponding effect size. The formula denominator consisted of the sum of the individual question weights.
resultsOverall, PCPs (N = 2755) who participated in this educational curriculum were 8% (actual effect size of 0.10) more likely to make evidence-based choices than clinicians participating in the baseline clinical practice assessment, which was conducted prior to the launch of the educational curriculum. Following is a summary of the fi ndings, organized by the assessment domains.
DEFINITIONS AND PATHOPHYSIOLOGY• Compared with baseline, signifi cantly more post-education PCPs
recognized that the diagnosis of postherpetic neuralgia (PHN) is made when pain persists for 2 months beyond the rash resolution (59%75%, P < .001, Figure 3). Fewer physicians are delaying diagnosis post-education, which may enable earlier treatment and resolution of symptoms.
DIAGNOSIS AND ASSESSMENT • Signifi cantly more post-education physicians (33%43%, P = .002,
Figure 4) recognized the use of the Brief Pain Inventory for patient pain assessment over the last 24 hours.
• In assessing for potential opioid abuse in a patient, two-thirds of physicians would appropriately use a validated risk assessment questionnaire. However, a third would not use these risk tools and would instead conduct no risk assessment or just assess pain levels alone.
• Most physicians would order appropriate tests when assessing a patient’s diffuse pain.
• The majority of physicians report limited confi dence in diagnosing peripheral neuropathies or assessing risk of pain medication abuse.
PAIN TREATMENTS: PHARMACOLOGIC• For a patient with chronic low back pain (LBP), after CME more than
three-fourths of physicians would add a tricyclic antidepressant to the medical therapy, a statistically signifi cant increase from baseline (56%76%, P < .001, Figure 5).
• Post-education PCPs are signifi cantly less likely to choose a short-acting as-needed opioid for a patient’s initial opioid therapy. One-fi fth of PCPs post-education would instead opt for a daily long-acting opioid.
• While nearly a third of PCPs chose an anticonvulsant as appropriate therapy for fi bromyalgia (23%29%, P = .11, data not shown), many were still not aware of the benefi ts of these agents, specifi cally pregabalin, for this type of patient.
• PCPs were signifi cantly less likely post-education to recognize that, of the given options, an opioid would be the least favorable therapy for a patient with fi bromyalgia (80%70%, P = .006, Figure 6), indicating more education on the treatment of patients with fi bromyalgia is needed.
• For a patient with PHN and known adverse reaction to gabapentin, less than a third of physicians selected the next most reasonable treatment option of nortriptyline. Most (60%) instead would opt for pregabalin, although this medication is not recommended due to the history of adverse event with gabapentin.
• For a patient with knee osteoarthritis, PCPs post-education were more likely to initiate self-help and patient-driven treatments (37%50%) but less likely to aspirate the effusion (22%18%) or inject with
corticosteroid (57%47%). Post-education participants were signifi cantly more likely, compared with baseline, to choose one of the appropriate responses (P = .002, Figure 7).
• PCPs had little consensus on pharmacologic therapy choice for a patient with osteoarthritis.
• Many physicians lack confi dence in their ability to alter treatment when fi rst-line pain treatment is inadequate.
PAIN TREATMENTS: NONPHARMACOLOGIC• Over half of respondents would appropriately recommend low-impact
aerobic exercises for a patient presenting with chronic low back pain, a signifi cant increase from baseline (42%52%, P = .05, Figure 8). The other half of physicians would instead order further diagnostic imaging, although guidance states this imaging should not be routinely obtained.
• Signifi cantly more PCPs post-education recognized that cardiovascular exercise has been demonstrated to be an effective treatment for patients with fi bromyalgia (18%34%, P < .001, Figure 9).
TREATMENT MONITORING• When asked about follow-up assessments of opioid use, post-
education physicians assessed the 4 “As” of pain medicine (analgesia, activity, adverse effects, and aberrant drug-related behaviors) less than baseline.
PATIENT EDUCATION• Discussions of goal-setting (81% 87%) and safe opioid storage
(56%66%) increased post education, while discussions of exit strategy decreased, compared with baseline (76%68%).
• PCPs post-education were less likely to recognize the purpose of establishing an exit strategy with a patient.
• Only 19% of physicians, pre- and post-education, were aware that the goal for pain relief is to return to previous function.
conclusion
IMPACT OF EDUCATIONEvidence-based treatment choices by PCPs who completed the case-based post-education assessment demonstrate the impact of the education. Such curricula can show improvement in PCP knowledge and competency in assessing and managing chronic pain. These results support those from recent research that case vignettes, compared with chart review and standardized patients, provide a valid, cost-effective, and noninvasive method to measure a physician’s processes of care.2,3
IMPLICATIONS FOR FUTURE EDUCATIONBased on the clinical practice gaps identifi ed within the post-education assessment responses, future educational activities should focus on the following:• Using validated questionnaires for initial pain assessment as well as risk assessment;• Choosing a short-acting vs long-acting opioid for initial opioid therapy;• Choosing the most appropriate treatment regimens for patients with chronic pain, including fi bromyalgia and
osteoarthritis;• Recognizing the value of aerobic exercise as a treatment choice for patients with chronic pain;• Using exit strategies when starting a patient on an opioid; and• Understanding the goals of pain treatment and patient function.
References
1. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, New Jersey: Lawrence Earlbaum Associates; 1988.
2. Peabody JW, Luck J, Glassman P, Dresselhaus TR, Lee M. Comparison of vignettes, standardized patients, and chart abstraction: a prospective validation study of 3 methods for measuring quality. JAMA. 2000; 283:1715-1722.
3. Peabody JW, Luck J, Glassman P, et al. Measuring the quality of physician practice by using clinical vignettes: a prospective validation study. Ann Intern Med. 2004; 141:771-780.
Acknowledgements
The CPA and educational curriculum was funded through an independent educational grant from Eli Lilly and Company.
Poster layout was provided by Irina Kogan of Medscape, LLC.
For more information, contact Anne Roc, PhD, Director, Clinical Strategy, Medscape, LLC, [email protected].
figure 1 Customized webpage of PainTV educational curriculum that includes host prologue and 12 episodes.
The Impact of a 12-Part Online CME Multimedia Curriculum Regarding Chronic Pain on Practice Patterns in Primary Care
figure 2 Medscape’s curriculum model for PainTV
stage 1 stage 2 stage 3 stage 4
A 25 item Clinical Practice Assessment (CPA) is created by CE Outcomes and posted on Medscape. It includes case vignettes and questions based on the LOs of the curriculum, as well as barrier and confi dence questions.
User data are collected by Medscape and analyzed by CE Outcomes to determine current clinical practice patterns.
Educational content for PainTV is developed by Medscape: 12 activities, 15-25 minutes each, are posted over 12 months. Each activity contains 3-5 post-activity questions aligned with the CPA.
The impact of the education was assessed by comparing post-activity questions responses with the baseline CPA responses.
Table Assessment domains and corresponding learning objectives of the curriculum
Assessment Domain Learning Objectives
Defi nitions and pathophysiology Recognize the different presentations of chronic pain and its impact on patient functioning and quality of life.
Diagnosis and assessment Conduct an effective pain assessment and diagnosis using validated tools.
Pain treatments: pharmacologic Select appropriate pain treatments for different pain and non-pharmacologic conditions based on pain pathophysiologies and the mechanisms of action of pain therapies.
Treatment monitoring Provide a follow-up and monitoring plan for chronic pain therapies.
Patient education Communicate and educate patients on treatment expectations and instructions on safe use.
figure 3
Pain that persists for 2 months beyond
resolution of the herpes zoster rash *
Pain that persists for 6 months beyond
resolution of the herpes zoster rash
Lack of pain relief after intradermal
injection of lidocaine
Varicella zoster titler 1:16
Post-education Primary Care Physicians (n=349)Baseline Primary Care Physicians (n=290)
P<.001*
PHN Case: A 59-year-old man had acute herpes zoster 9 months ago in the area of his left forehead and eye. The rash resolved; however, pain has continued in the affected area and is disrupting his sleep. A trial of gabapentin was discontinued due to severe dizziness. On exam, there is scarring along his left forehead and associated loss of light touch and temperature sensation.
100%
80%
60%
40%
20%
0%
59%
37%
2%2%
75%
20%
4%1%
Which of the following criteria are necessary to diagnose this patient with postherpetic neuralgia?
figure 4
Brief Pain Inventory*
McGill Pain Questionnaire
I would rely on patient history alone
Oswestry Disability Index
Pain Anxiety Symptoms Scale - 20
Post-education Primary Care Physicians (n=750)Baseline Primary Care Physicians (n=290)
P =.002*
PHN Case: A 35-year-old man presents with a 6-month history of lower back pain which began after a work injury. No fracture was found on exam, and he was treated with 4000 mg acetaminophen and physical therapy. He continues to experience frequent episodes of lower back pain which cause him to miss work. His pain is constant, and he indicates it is currently 2-3 out of 10. His pain increases to 7-8 out of 10 when he tries to exercise. Physical exam fi nds an antalgic gait, pain with lumbar fl exion and extension, and paraspinous spasms and tenderness.
100%
80%
60%
40%
20%
0%
33%
20%
30%
10%7%
43%
22% 18%6%
11%
Which of the following tools would you use to assess the impact of this patient’s pain on his physical functioning, emotional status, and sleep over the last 24 hours?
figure 5
Increase acetaminophen
Tricyclic antidepressant*
Long-acting opioid Systemic corticosteroid
Post-education Primary Care Physicians (n=464)Baseline Primary Care Physicians (n=290)
P <.001*
100%
80%
60%
40%
20%
0%
7%
56%
17%21%
6%
76%
8%10%
Which of the following pharmacological therapies would you add to this patient’s regimen? This question is related to the LBP case.
figure 6
Anticonvulsant Tricyclic antidepressant
Opioid* NSAID or selective COX-2 inhibitor
Post-education Primary Care Physicians (n=320)Baseline Primary Care Physicians (n=290)
P=.006*
Fibromyalgia Case: A 45-year-old woman sustained a whiplash injury in a motor vehicle accident approximately 5 years ago. Radiographs did not reveal any fractures. After the accident, she complained of diffuse muscle soreness that has continued on an intermittent basis. She presents to your offi ce with the complaint of constant, diffuse muscle aches, with a pain score of 6 out of 10. She reports that her pain ranges from 3-9 out of 10 and worsens with activity. The patient also complains of accompanying depression, for which her primary care physician is treating her with a selective serotonin reuptake inhibitor. She also suffers from fatigue, sleep disturbance, and cognitive impairment. She has not found any relief with either over-the-counter nonsteroidal anti-infl ammatory drugs (NSAIDs) or acetaminophen. On exam, her gait is normal, and she has multiple tender points throughout her body. Laboratory testing reveals that all results are within normal limits. The patient’s history, physical exam fi ndings, and laboratory results bring you to the diagnosis of fi bromyalgia.
100%
80%
60%
40%
20%
0%
11%4% 5%
80%
10% 7% 12%
70%
Which of the following therapies would be the least favorable for this patient?
figure 7
Initiate self-help and patient-driven
treatments*
Aspirate the effusion*
Inject the joint with corticosteroid*
Refer the patient to a physical therapist
Refer the patient to a surgeon for joint
replacement surgery
Post-education Primary Care Physicians (n=245)Baseline Primary Care Physicians (n=290)P=.002*
Osteoarthritis Case: An 81-year-old retired teacher with mild hypertension and obesity reports a progressive history of left knee pain over the past 10 years. She enjoys gardening but has had to limit her activity due to increasing pain in her left knee. She has found some improvement with acetaminophen 4000 mg/day, supplemented with over-the-counter ibuprofen. Radiographs show marked joint space narrowing, sclerosis, and periarticular osteophyte formation. Examination of the left knee reveals that her range of motion is reduced due to pain, and there is some mild swelling, with a small effusion.
For this question, if any of the 3 correct answers were selected by the respondent, the question is coded as correct. Forty-eight percent of baseline participants and 61% of post-education participants selected evidence-based responses (answer 1, 2, or 3).
100%
80%
60%
40%
20%
0%
37%
22%
44%
12%
57%50%
18%
35%
6%
47%
Which of the following would be your next course of action in the management of this patient?
figure 8
Encourage low-impact aerobic exercises such
as water therapy or recumbent bicycle*
Order an MRI of the lumbar spine
Refer for an epidural steroid injection
Refer immediately for a surgical consultation
Post-education Primary Care Physicians (n=162)Baseline Primary Care Physicians (n=290)
P=.05*
100%
80%
60%
40%
20%
0%
42%54%
0%3%
52%46%
1%2%
Which of the following would you choose as the next course of action for this patient? This question is related to the LBP case.
figure 9
Cardiovascular exercise*
Chiropractic manipulation
Trigger point injections
Flexibility exercises
Post-education Primary Care Physicians (n=320)Baseline Primary Care Physicians (n=290)
P<.001*
100%
80%
60%
40%
20%
0%
18%
3%
58%
21%
34%
5%
45%
16%
Which of the following therapies has demonstrated the strongest evidence for effi cacy in the treatment of the type of pain that this patient is experiencing? This question is related to the fi bromyalgia case.
14 15

AbstractBackground: Chronic hepatitis B virus (HBV) infection is undertreated in the United States; only 10% to 15% of treatment-eligible patients receive antiviral therapy. Without changes in practice, the clinical and public health burden of untreated chronic HBV infection, including hepatocellular carcinoma and liver failure, will only increase. The US Department of Health and Human Services has prioritized clinician education in addressing the viral hepatitis epidemic. However, research indicates that healthcare providers (HCPs) often participate in education that reinforces what they already know vs activities that target their true needs. Educational interventions tailored to the needs of individual learners (Personalized Learning [PL]) may be more effective than generalized programs for achieving improvements in clinical practice.
Methods: To evaluate HCPs’ knowledge, attitudes, practice patterns, and barriers to patient evaluation, treatment, and long-term care, an Internet-based clinical practice self-assessment (SA) consisting of case-based questions was developed. A series of 6 distinct continuing medical education (CME) activities, each designed using proven educational strategies, was developed to address a range of practice gaps in the care of patients with chronic HBV infection. Each SA question was mapped to 1 of the 6 CME activities so that education could be targeted to the specific needs of individuals. HCPs in the intervention arm are directed to relevant activities based on their responses in the SA; the control arm comprises a matched cohort of HCPs who have completed the SA but have not participated in the educational interventions. Each CME activity includes a post-activity assessment that incorporates relevant questions from the SA. Statistical comparison of SA and post-assessment data from the intervention arm (and with SA data from the control arm) will measure educational effectiveness.
Results: Initial data suggest that the tailored learning approach provided by the PL model can improve clinician performance; further evaluation of the effect of PL on improving treatment of chronic HBV infection is underway.
Conclusion: The PL model provides customized learning by guiding HCPs through a defined sequence of education modules that address specific gaps in chronic HBV care identified through their own self-assessment.
IntroductionChronic HBV Infection in the United States• Chronic hepatitis B virus (HBV) infection is
estimated to affect >1.4 million persons in the United States,1,2 but it is estimated that <5% of affected/eligible individuals with chronic HBV infection are screened, linked into care, receive prescription drugs, and are successfully engaged in treatment3
Education of HCPs as a Tool for Change• The 2010 Institute of Medicine report and the
Department of Health and Human Services Action Plan for the Prevention, Care, and Treatment of Viral Hepatitis recommend education of healthcare providers (HCPs) as a critical component of controlling this epidemic2,4
• Continued professional development (CPD) for HCPs is a life-long endeavor that addresses patient-related practice-based needs as well as maintenance of licensure and board certification requirements
• The goal of CME activities is to foster continued professional development among all HCPs not only by promoting clinician learning, but through: — Increasing clinician competency — Influencing and, where appropriate,
changing behavior — Positively affecting patient outcomes
• However, data suggest that HCPs do not always critically and/or accurately evaluate their own learning needs and therefore often participate in educational programs that reinforce what they already know vs participating in programs that target their unmet needs5,6
MethodsAdult Learning Theory and Tailored Education• CME developed in accordance with adult
learning theories can increase the likelihood that education will achieve the desired outcomes
• Changes in practice are more likely to occur if learners evaluate their own practice and commit to change following participation in CME7
• Accordingly, CME interventions that create cognitive dissonance, combined with timely and convenient methods to address the areas of identified need for each individual, are proposed to have greater impact than more traditional self-directed educational approaches
Personalized Learning • Medscape and CE Outcomes collaborated
to develop Personalized Learning, a needs-driven, targeted, and personalized educational solution
• The PL model leverages Medscape’s unique structured instructional methodology to assess learners’ individual competencies related to practicing evidence-based medicine and, subsequently, to deliver tailored educational plans and resources (Figure 1)
A Personalized Learning Initiative in Chronic HBV Infection (Figure 2)• Performance gaps were identified among
HCPs, including gastroenterologists, hepatologists, and primary care providers (PCPs) who treat patients with chronic HBV infection (Section A)
• Identified gaps were used to inform development of a collection of 6 CME activities (Section C), each of which address a discrete gap/educational need (Section B)
• A clinical practice self-assessment (SA) was used to identify gaps in an individual learner’s knowledge, skills, or performance as related to managing patients with chronic HBV infection and retaining them in care — The SA contained a series of case vignettes
and 19 associated questions, and was validated using cognitive interviews with practicing physicians
— Questions from the SA were aligned to individual PL activities (Figure 3)
• Learners’ specific responses in the SA indicate individual gaps in knowledge, skill, or performance and inform a personalized learning plan that directs learners to a customized grouping of Internet-based educational activities — CME activities include multimedia,
interactive formats that incorporate instructional principles specifically selected to align with the gaps and educational needs being addressed (Figure 3)
• A tailored communication and educational reinforcement plan ensures continued learner engagement through the completion of the program
• A pre-specified comprehensive education effectiveness evaluation plan will analyze the following:
— Percentage of learners receiving an educational plan with 1 or more activities
— Percentage of learners completing recommended activities
— Aggregate improvement in scores between SA and post-assessment for all learners completing each recommended course at a matched individual-to-individual level
— Aggregate differences between prescribed post-assessment scores and scores of a demographically similar control group
Data Collection and Analysis• The SA is available at: http://www.medscape.
org/prescribed-learning/6004101 • Participant response data were gathered
by Medscape and provided electronically 30 days after the SA posted online to CE Outcomes for analysis
• Nonpracticing HCPs and HCPs reporting that they see zero patients with chronic HBV infection were excluded from the analysis
• Data extraction, transformation, and statistical analyses were performed using a statistical analysis package for the social sciences (IBM SPSS Statistics 20)
• Learner responses were scored according to their concordance with the evidence-based measurement indicators and overall mean scores were calculated
• All participants in the sample were required to complete 100% of the case vignette survey questions
Results: Clinical Practice Self-Assessment Baseline Sample
Gap 1: Initial patient evaluation and assessment• While the majority (93%) of specialists were
able to appropriately interpret serologic tests to determine the phase of HBV infection, only 33% of PCPs were able to do so
• Similarly, a greater proportion of specialists vs PCPs (93% vs 73%) were aware of potential side effects associated with antiviral agents
• Both specialists (19%) and PCPs (60%) exhibited gaps in differentiating among antiviral agents with a high vs low barrier to genetic resistance
Gap 2: Awareness and application of evidence-based treatment strategies• Significant proportions of both specialists and
PCPs exhibited competence gaps with respect to the following: — Identifying treatment candidates and
determining when to initiate antiviral therapy — Developing management strategies for
patients •With a prior history of treatment •In the context of prior treatment failure•Who are pregnant and following childbirth•With HIV/HBV coinfection
— Recognizing and managing individuals at risk for HBV reactivation
Gap 3: Use of effective communication to facilitate patient adherence to treatment• The majority of both specialists (70%-76%)
and PCPs (65%-75%) did not recognize the importance of addressing cultural beliefs, health beliefs, and stigma prior to recommending antiviral therapy
• Monitoring of laboratory values was overlooked as a tool for assessing adherence by both specialists (55%) and PCPs (66%)
Discussion and Conclusion• Based upon the responses in the SA,
specialists were better able to interpret laboratory assessments and were more familiar with antiviral side effects than PCPs
• Both specialists and PCPs exhibited competence gaps with respect to treatment initiation and developing management strategies for “special” populations
• Responses to the SA confirm previously identified gaps/educational needs; CME activities developed as part of this PL initiative have been designed to improve clinician performance and bridge the identified gaps
• This PL initiative tailors access to educational activities and materials that address individual educational needs and supports continued participation; future analyses will evaluate educational effectiveness of the initiative through measurement of changes in learning efficiency and likelihood of enhanced performance outcomes
AcknowledgementsThis Personalized Learning initiative in chronic HBV infection was funded through an independent educational grant from Gilead Sciences Medical Affairs. For more information contact Simi T. Hurst, PhD, Director Clinical Strategy, Infectious Disease, Medscape, LLC, [email protected].
Reference1. Centers for Disease Control and Prevention. Viral Hepatitis Surveillance
– United States, 2010. www.cdc.gov/hepatitis/Statistics/index.htm. Accessed September 1, 2012.
2. Colvin HM, Mitchell AE, eds. Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C. Washington, DC: Institute of Medicine; 2010; 252.
3. Cohen C, Holmberg SD, McMahon BJ, et al. Is chronic hepatitis B being undertreated in the United States? J Viral Hepat. 2008;18(6):377-383.
4. Combating the silent epidemic of viral hepatitis: action plan for the prevention, care, and treatment of viral hepatitis. Department of Health and Human Services. www.hhs.gov/ash/initiatives/hepatitis/actionplan_viralhepatitis2011.pdf. Accessed September 1, 2012.
5. Davis DA, Mazmanian PE, Fordis M, Harrison VR, Thorpe KE, Perrier L. Accuracy of physician self-assessment compared with observed measures of competence: a systematic review. JAMA. 2006;296(9):1094-1102.
6. Hawkins R, Kreuter M, Resnicow K, Fishbein M, Dijkstra A. Understanding tailoring in communicating about health. Health Educ Res. 2008;23:454-466.
7. Mazmanian PE, Daffron SR, Johnson RE, Davis DA, Kantrowitz MP. Information about barriers to planned change: a randomized controlled trial involving continuing medical education lectures and commitment to change. Acad Med. 1998;73(8):882-886.
Figure 1. The Personalized Learning pathway
Figure 2. Performance gaps/educational needs in chronic HBV infection and alignment with CME activities
Figure 3. Baseline assessment questions map to specific CME activities to provide each learner with a personalized educational plan
Table 1. Demographics
A. Multisource assessment of professional practice gaps and educational needs
• CDC, DHHS, WHO• Clinical practice
guidelines• Published literature• Expert perspectives/
interviews• Medscape and AGA
membership survey data• Data from prior HBV-
related CME activities, including — Responses to pre-,
post-, and interactivity questions
— Education effectiveness/outcomes analysis
— Learner feedback
Initial patient evaluation and assessment, including interpretation and application of clinical and laboratory data to inform clinical decision making
1. Managing HBV Infection: A Clinician’s Handbook
2. After the Diagnosis: Next Steps in the Care of the Patient with Chronic HBV Infection
3. HBV Reactivation: What It Is, Why We Should Be Concerned, and What We Can Do About It
4. Care of the HBV/HIV Coinfected Patient: Management and Treatment
5. Chronic HBV and Pregnancy: Addressing the Needs of Mother and Child
6. The Art of Communication: A Team Approach to Adherence in Patients with Chronic HBV Infection
Awareness and application of evidence-based treatment strategies, including those for special populations
Use of effective communication to facilitate patient adherence to treatment
B. Identified practice gaps and educational needs in chronic HBV infection
C. CME activity topics
Self-Assessment
1.
2.
3.
4.
5.
Number of patients diagnosed with chronic HBV seen each week 1-10 73% 81% 11-20 9% 5% 21-30 10% 6% 31-40 0% 3% > 40 7% 5%
Practice location Urban 64% 59% Suburban 27% 27% Rural 9% 14%
Present Employment Solo practice 13% 21% Group practice 46% 34% Medical school 16% 13% HMO 1% 4% Nongovernment hospital 9% 15% Government 13% 13%
Major professional activity Direct patient care activities 88% 85% Administrative activities 1% 4% Medical education 7% 9% Medical research 3% 1%
Specialists Primary Care (n=67) (n=168)
Nancy Reau, MD1; Susan L. Smith, MN, PhD2; Wendy Cerenzia, MS3; Simi T. Hurst, PhD2
1Center for Liver Diseases, University of Chicago Medical Center, Chicago, IL, USA; 2Medscape, LLC, New York, NY, USA; 3CE Outcomes, Birmingham, AL, USA
• 225 physicians were included in the participant sample• Specialists included gastroenterologists, hepatologists, and infectious disease physicians; PCPs included
internists, family physicians, and obstetrician/gynecologists
1025
Personalized Learning: A Novel Educational Model to Bridge Clinical Practice Gaps in Chronic HBV Infection
4
P O S T E R
Presented at ID Week in 2012; Poster contained data on baseline assessment and interim analysis.
“ Personalized Learning: A Novel Educational Model to Bridge Clinical Practice Gaps in Chronic HBV Infection”
16 17

F O R M A T
HBV Personalized Learning Initiative. The personalized learning program, Breaking Down the Barriers in Hepatitis B: Treatment and Retention in Care, consisting of the baseline assessment, 6 educational interventions, and post-test assessment, was posted online by Medscape on June 26, 2012. This educational grant was awarded to Medscape by Gilead Sciences Medical Affairs to develop continuing medical education (CME) using a personalized learning model and to report metrics on the effect of the educational curriculum.
O V E R A L L I M P A C T S T A T E M E N T
G A P 1 : U S E O F C L I N I C A L A N D L A B O R A T O R Y D A T A T O I N F O R M C L I N I C A L D E C I S I O N - M A K I N G
G A P 3 : E F F E C T I V E C O M M U N I C A T I O N T O F A C I L I T A T E P A T I E N T A D H E R E N C E T O T R E A T M E N T
G A P 2 : U S E O F E V I D E N C E - B A S E D T R E A T M E N T R E C O M M E N D A T I O N S
• Following participation in the education, PCPs (69%) were signifi cantly more likely to recognize the laboratory values that characterized chronic HBV infection than before the education (57%, P=.02).
• Following participation in the education, PCPs (69%) were signifi cantly more likely to recognize the laboratory values that characterized chronic HBV infection than PCP nonparticipants (54%, P=.04).
• Following participation in the education, specialists (82%) were signifi cantly more likely to select the antiviral agent that provides the highest genetic barrier to resistance after participating in the education compared with before the education (50%, P=.002).
• Following participation in the education, PCPs (75%) were signifi cantly more likely to select the antiviral agent that provides the highest genetic barrier to resistance after participating in the education compared with before the education (25%, P<.001) and with PCP nonparticipants (42%, P<.001).
• Following participation in the education, specialists (95%) were signifi cantly more likely to recognize that nephrotoxicity is a potential side eff ect of tenofovir and adefovir than before the education (79%, P=.03).
• Following participation in the education, PCPs (88%) were signifi cantly more likely to recognize that nephrotoxicity is a potential side eff ect of tenofovir and adefovir than before the education (56%, P<.001) and then PCP nonparticipants (63%, P<.001).
• Following participation in the education specialists (78%) were signifi cantly more likely to start a patient who is HBV positive and pregnant on antiviral medication at 32 weeks of pregnancy to prevent maternal-fetal transmission than before the education (19%, P<.001) and compared with specialist nonparticipants (34%, P<.001).
• Following participation in the education, specialists (72%) were signifi cantly more aware that antiviral medication for an HBeAg-positive pregnant patient with chronic HBV infection should be started at an HBV DNA level > 108 copies/mL, compared with before the education (8%, P<.001) and compared with specialist nonparticipants (23%, P<.001).
• Following participation in the education, specialists (89%) were more likely to reassure a patient with HBV who stopped antiviral therapy to breastfeed and to continue to monitor her for rebound hepatitis fl are with liver transaminase levels compared with before the education (56%, P=.002) and compared with specialist nonparticipants (40%, P<.001).
• Following participation in the education, specialists (83%) were signifi cantly more likely to follow the AASLD’s “Chronic Hepatitis B: Update 2009” recommendations for a patient who is HBeAg negative with rising ALT and HBV DNA levels compared with before the education (64%, P=.01).
• Following participation in the education, specialists (64%) were signifi cantly more likely to follow the AASLD’s “Chronic Hepatitis B: Update 2009” recommendations for a patient who is HBeAg negative with an elevated ALT and HBV DNA 15000 IU/mL compared with before the education (26%, P<.01) and with specialist nonparticipants (37%, P=.01).
• Following participation in the education, specialists (89%) were signifi cantly more likely to appropriately address an ALT > 2X ULN in an HIV/HBV infected patient who is being treated with a HAART regimen including zidovudine/lamivudine than before the education (59%, P=.02) and compared with specialist nonparticipants (57%, P=.006).
• Following participation in the education, specialists (93%) were signifi cantly more likely to recognize the appropriate next step for a patient with HIV-HBV coinfection that has developed resistance to lamivudine is to switch the patient to tenofovir/emtricitabine as HIV regimen backbone than before the education (52%, P<.001) and compared to specialist nonparticipants (57%, P=.002).
• Following participation in the education, specialists (78%) were signifi cantly more likely to recognize that IRIS occurs most often in patients with HIV-HBV coinfection when treatment for HBV is initiated when the patient’s CD4 cell count is < 200 cells/mm3, as compared to before the education (44%, P=.004).
• Following participation in the education, specialists (71%) were signifi cantly more likely to recognize that in a cancer patient about to begin chemotherapy, HBeAg-negative serostatus makes HBV reactivation less likely, compared with HBeAg positive status than before the education (43%, P=.02).
• Following participation in the education, specialists (89%) were signifi cantly more likely to appropriately start antiviral prophylaxis (to prevent HBV reactivation) in a patient with cancer who is about to start chemotherapy than they were prior to the education (71%, P=.02) and compared with specialist nonparticipants (57%, P=.005).
Specialists (gastroenterologists, infectious disease specialists, hepatologists) and PCPs (n = 359) who participated in this educational program are 49%
(eff ect size = 0.84) more likely to make evidence-based choices after participating in the personalized educational program.
EFFECTIVENESS OF COMPLETED OUTCOMES STUDY
4 “ Personalized Learning: A Novel Educational Model to Bridge Clinical Practice Gaps in Chronic HBV Infection”
AbstractBackground: Chronic hepatitis B virus (HBV) infection is undertreated in the United States; only 10% to 15% of treatment-eligible patients receive antiviral therapy. Without changes in practice, the clinical and public health burden of untreated chronic HBV infection, including hepatocellular carcinoma and liver failure, will only increase. The US Department of Health and Human Services has prioritized clinician education in addressing the viral hepatitis epidemic. However, research indicates that healthcare providers (HCPs) often participate in education that reinforces what they already know vs activities that target their true needs. Educational interventions tailored to the needs of individual learners (Personalized Learning [PL]) may be more effective than generalized programs for achieving improvements in clinical practice.
Methods: To evaluate HCPs’ knowledge, attitudes, practice patterns, and barriers to patient evaluation, treatment, and long-term care, an Internet-based clinical practice self-assessment (SA) consisting of case-based questions was developed. A series of 6 distinct continuing medical education (CME) activities, each designed using proven educational strategies, was developed to address a range of practice gaps in the care of patients with chronic HBV infection. Each SA question was mapped to 1 of the 6 CME activities so that education could be targeted to the specific needs of individuals. HCPs in the intervention arm are directed to relevant activities based on their responses in the SA; the control arm comprises a matched cohort of HCPs who have completed the SA but have not participated in the educational interventions. Each CME activity includes a post-activity assessment that incorporates relevant questions from the SA. Statistical comparison of SA and post-assessment data from the intervention arm (and with SA data from the control arm) will measure educational effectiveness.
Results: Initial data suggest that the tailored learning approach provided by the PL model can improve clinician performance; further evaluation of the effect of PL on improving treatment of chronic HBV infection is underway.
Conclusion: The PL model provides customized learning by guiding HCPs through a defined sequence of education modules that address specific gaps in chronic HBV care identified through their own self-assessment.
IntroductionChronic HBV Infection in the United States• Chronic hepatitis B virus (HBV) infection is
estimated to affect >1.4 million persons in the United States,1,2 but it is estimated that <5% of affected/eligible individuals with chronic HBV infection are screened, linked into care, receive prescription drugs, and are successfully engaged in treatment3
Education of HCPs as a Tool for Change• The 2010 Institute of Medicine report and the
Department of Health and Human Services Action Plan for the Prevention, Care, and Treatment of Viral Hepatitis recommend education of healthcare providers (HCPs) as a critical component of controlling this epidemic2,4
• Continued professional development (CPD) for HCPs is a life-long endeavor that addresses patient-related practice-based needs as well as maintenance of licensure and board certification requirements
• The goal of CME activities is to foster continued professional development among all HCPs not only by promoting clinician learning, but through: — Increasing clinician competency — Influencing and, where appropriate,
changing behavior — Positively affecting patient outcomes
• However, data suggest that HCPs do not always critically and/or accurately evaluate their own learning needs and therefore often participate in educational programs that reinforce what they already know vs participating in programs that target their unmet needs5,6
MethodsAdult Learning Theory and Tailored Education• CME developed in accordance with adult
learning theories can increase the likelihood that education will achieve the desired outcomes
• Changes in practice are more likely to occur if learners evaluate their own practice and commit to change following participation in CME7
• Accordingly, CME interventions that create cognitive dissonance, combined with timely and convenient methods to address the areas of identified need for each individual, are proposed to have greater impact than more traditional self-directed educational approaches
Personalized Learning • Medscape and CE Outcomes collaborated
to develop Personalized Learning, a needs-driven, targeted, and personalized educational solution
• The PL model leverages Medscape’s unique structured instructional methodology to assess learners’ individual competencies related to practicing evidence-based medicine and, subsequently, to deliver tailored educational plans and resources (Figure 1)
A Personalized Learning Initiative in Chronic HBV Infection (Figure 2)• Performance gaps were identified among
HCPs, including gastroenterologists, hepatologists, and primary care providers (PCPs) who treat patients with chronic HBV infection (Section A)
• Identified gaps were used to inform development of a collection of 6 CME activities (Section C), each of which address a discrete gap/educational need (Section B)
• A clinical practice self-assessment (SA) was used to identify gaps in an individual learner’s knowledge, skills, or performance as related to managing patients with chronic HBV infection and retaining them in care — The SA contained a series of case vignettes
and 19 associated questions, and was validated using cognitive interviews with practicing physicians
— Questions from the SA were aligned to individual PL activities (Figure 3)
• Learners’ specific responses in the SA indicate individual gaps in knowledge, skill, or performance and inform a personalized learning plan that directs learners to a customized grouping of Internet-based educational activities — CME activities include multimedia,
interactive formats that incorporate instructional principles specifically selected to align with the gaps and educational needs being addressed (Figure 3)
• A tailored communication and educational reinforcement plan ensures continued learner engagement through the completion of the program
• A pre-specified comprehensive education effectiveness evaluation plan will analyze the following:
— Percentage of learners receiving an educational plan with 1 or more activities
— Percentage of learners completing recommended activities
— Aggregate improvement in scores between SA and post-assessment for all learners completing each recommended course at a matched individual-to-individual level
— Aggregate differences between prescribed post-assessment scores and scores of a demographically similar control group
Data Collection and Analysis• The SA is available at: http://www.medscape.
org/prescribed-learning/6004101 • Participant response data were gathered
by Medscape and provided electronically 30 days after the SA posted online to CE Outcomes for analysis
• Nonpracticing HCPs and HCPs reporting that they see zero patients with chronic HBV infection were excluded from the analysis
• Data extraction, transformation, and statistical analyses were performed using a statistical analysis package for the social sciences (IBM SPSS Statistics 20)
• Learner responses were scored according to their concordance with the evidence-based measurement indicators and overall mean scores were calculated
• All participants in the sample were required to complete 100% of the case vignette survey questions
Results: Clinical Practice Self-Assessment Baseline Sample
Gap 1: Initial patient evaluation and assessment• While the majority (93%) of specialists were
able to appropriately interpret serologic tests to determine the phase of HBV infection, only 33% of PCPs were able to do so
• Similarly, a greater proportion of specialists vs PCPs (93% vs 73%) were aware of potential side effects associated with antiviral agents
• Both specialists (19%) and PCPs (60%) exhibited gaps in differentiating among antiviral agents with a high vs low barrier to genetic resistance
Gap 2: Awareness and application of evidence-based treatment strategies• Significant proportions of both specialists and
PCPs exhibited competence gaps with respect to the following: — Identifying treatment candidates and
determining when to initiate antiviral therapy — Developing management strategies for
patients •With a prior history of treatment •In the context of prior treatment failure•Who are pregnant and following childbirth•With HIV/HBV coinfection
— Recognizing and managing individuals at risk for HBV reactivation
Gap 3: Use of effective communication to facilitate patient adherence to treatment• The majority of both specialists (70%-76%)
and PCPs (65%-75%) did not recognize the importance of addressing cultural beliefs, health beliefs, and stigma prior to recommending antiviral therapy
• Monitoring of laboratory values was overlooked as a tool for assessing adherence by both specialists (55%) and PCPs (66%)
Discussion and Conclusion• Based upon the responses in the SA,
specialists were better able to interpret laboratory assessments and were more familiar with antiviral side effects than PCPs
• Both specialists and PCPs exhibited competence gaps with respect to treatment initiation and developing management strategies for “special” populations
• Responses to the SA confirm previously identified gaps/educational needs; CME activities developed as part of this PL initiative have been designed to improve clinician performance and bridge the identified gaps
• This PL initiative tailors access to educational activities and materials that address individual educational needs and supports continued participation; future analyses will evaluate educational effectiveness of the initiative through measurement of changes in learning efficiency and likelihood of enhanced performance outcomes
AcknowledgementsThis Personalized Learning initiative in chronic HBV infection was funded through an independent educational grant from Gilead Sciences Medical Affairs. For more information contact Simi T. Hurst, PhD, Director Clinical Strategy, Infectious Disease, Medscape, LLC, [email protected].
Reference1. Centers for Disease Control and Prevention. Viral Hepatitis Surveillance
– United States, 2010. www.cdc.gov/hepatitis/Statistics/index.htm. Accessed September 1, 2012.
2. Colvin HM, Mitchell AE, eds. Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C. Washington, DC: Institute of Medicine; 2010; 252.
3. Cohen C, Holmberg SD, McMahon BJ, et al. Is chronic hepatitis B being undertreated in the United States? J Viral Hepat. 2008;18(6):377-383.
4. Combating the silent epidemic of viral hepatitis: action plan for the prevention, care, and treatment of viral hepatitis. Department of Health and Human Services. www.hhs.gov/ash/initiatives/hepatitis/actionplan_viralhepatitis2011.pdf. Accessed September 1, 2012.
5. Davis DA, Mazmanian PE, Fordis M, Harrison VR, Thorpe KE, Perrier L. Accuracy of physician self-assessment compared with observed measures of competence: a systematic review. JAMA. 2006;296(9):1094-1102.
6. Hawkins R, Kreuter M, Resnicow K, Fishbein M, Dijkstra A. Understanding tailoring in communicating about health. Health Educ Res. 2008;23:454-466.
7. Mazmanian PE, Daffron SR, Johnson RE, Davis DA, Kantrowitz MP. Information about barriers to planned change: a randomized controlled trial involving continuing medical education lectures and commitment to change. Acad Med. 1998;73(8):882-886.
Figure 1. The Personalized Learning pathway
Figure 2. Performance gaps/educational needs in chronic HBV infection and alignment with CME activities
Figure 3. Baseline assessment questions map to specific CME activities to provide each learner with a personalized educational plan
Table 1. Demographics
A. Multisource assessment of professional practice gaps and educational needs
• CDC, DHHS, WHO• Clinical practice
guidelines• Published literature• Expert perspectives/
interviews• Medscape and AGA
membership survey data• Data from prior HBV-
related CME activities, including — Responses to pre-,
post-, and interactivity questions
— Education effectiveness/outcomes analysis
— Learner feedback
Initial patient evaluation and assessment, including interpretation and application of clinical and laboratory data to inform clinical decision making
1. Managing HBV Infection: A Clinician’s Handbook
2. After the Diagnosis: Next Steps in the Care of the Patient with Chronic HBV Infection
3. HBV Reactivation: What It Is, Why We Should Be Concerned, and What We Can Do About It
4. Care of the HBV/HIV Coinfected Patient: Management and Treatment
5. Chronic HBV and Pregnancy: Addressing the Needs of Mother and Child
6. The Art of Communication: A Team Approach to Adherence in Patients with Chronic HBV Infection
Awareness and application of evidence-based treatment strategies, including those for special populations
Use of effective communication to facilitate patient adherence to treatment
B. Identified practice gaps and educational needs in chronic HBV infection
C. CME activity topics
Self-Assessment
1.
2.
3.
4.
5.
Number of patients diagnosed with chronic HBV seen each week 1-10 73% 81% 11-20 9% 5% 21-30 10% 6% 31-40 0% 3% > 40 7% 5%
Practice location Urban 64% 59% Suburban 27% 27% Rural 9% 14%
Present Employment Solo practice 13% 21% Group practice 46% 34% Medical school 16% 13% HMO 1% 4% Nongovernment hospital 9% 15% Government 13% 13%
Major professional activity Direct patient care activities 88% 85% Administrative activities 1% 4% Medical education 7% 9% Medical research 3% 1%
Specialists Primary Care (n=67) (n=168)
Nancy Reau, MD1; Susan L. Smith, MN, PhD2; Wendy Cerenzia, MS3; Simi T. Hurst, PhD2
1Center for Liver Diseases, University of Chicago Medical Center, Chicago, IL, USA; 2Medscape, LLC, New York, NY, USA; 3CE Outcomes, Birmingham, AL, USA
• 225 physicians were included in the participant sample• Specialists included gastroenterologists, hepatologists, and infectious disease physicians; PCPs included
internists, family physicians, and obstetrician/gynecologists
1025
Personalized Learning: A Novel Educational Model to Bridge Clinical Practice Gaps in Chronic HBV Infection
18 19

Cyndi Grimes, CCMEP, and Jane Lowers, Medscape, LLC, New York, NY
AbstractSince the American Medical Association (AMA) created Performance Improvement Continuing Medical Education (PI CME), a new format for AMA Physician’s Recognition Award (PRA) Category 1 CreditTM that recog-nizes CME credit for physicians who engage in self-evaluation and improvement activities related to their clinical performance, differ-ent approaches to this process have been implemented by accredited providers. Many factors must be considered in the design of the PI CME system to ensure optimal participation and performance improvement. Medscape, LLC, designed a PI CME platform that leverages the self-directed nature of its membership and included other key factors seen as beneficial to participants. Insights gathered during the development, implemen-tation, and evaluation of PI CME programs within this system will help other providers design future effective PI CME programs.
OverviewThe AMA asked accredited providers to cre-ate a structured, long-term staged process for PI CME in which physicians learn about specific performance measures, assess their practices based on those measures, imple-ment interventions to improve performance related to the measures over a period of time, and then reassess their practices using the same performance measures. • A performance measure is a mechanism
that enables the user to quantify a selected aspect of care by comparing it to a criterion.1
• The AMA requires that the performance measures are evidenced based and na-tionally recognized, with clear specific data elements for data collection.
Medscape (accredited with commendation by the Accreditation Council for CME in 2010) designed an innovative online platform leveraging our expertise in delivering online CME education and our understanding of our membership usage of the Medscape Educa-tion Website. The goal of this presentation is to share our experience in developing the platform and demonstrate the result of physi-cians participating in and completing PI CME initiatives. MethodsMedscape designed a structured PI CME framework that allows physicians to as-sess their practice against evidence-based performance measures and see how these measures relate to the 6 core competen-cies adopted by the Accreditation Council for Graduate Medical Education (ACGME) and the American Board of Medical Specialties (ABMS). The PI CME platform allows members to ac-cess specific PI CME initiatives on perfor-mance measures across multiple specialties; each offers a consistent format for self-direc-tion and reflection. • Medscape uses performance measures
validated by the AMA’s Physician Consor-tium for Performance Improvement (PCPI), the Physician Quality Reporting System (PQRS) measure set used by the Centers for Medicare & Medicaid Services, and the Healthcare Effectiveness Data and Information set (HEDIS).
In order for physicians to focus their clinical need for improvement, every question in the self-assessment and chart data collection in Stage A is linked to 1 performance measure
and 1 core competency. Table 1 provides an example of how self-assessment questions are linked to performance measures and the core competencies. • Physicians receive results of their Stage A self-assessment grouped by the ACGME/ABMS core competencies. • From this information, they can determine what area or areas of improvement they would like to ad-dress and are then provided tools and resources to support their personal PI CME improvement plan.
ResultsMedscape launched 3 PI CME activities in the areas of depression, diabetes, and osteoporosis starting in March 2011 that were supported by independent educational grants from Lilly USA, LLC. • Participation results as of April 2012 are listed in
Table 2. (Note that many physicians are still in the process of completing their PI CME and may not be eligible to start Stage C yet.)
• Additional PI CME programs on pain (supported by Lilly USA, LLC), on rheumatoid arthritis (supported by Abbott and UCB Pharma), and on HIV (support-ed by Gilead) are in progress.
Key Learning and Considerations• Design a PI CME initiative that will allow physicians
to self-direct their performance improvement spe-cific to their clinical needs based on performance measures
• Link core competencies to performance measures to enhance physicians’ ability to address key areas of improvement in practice
• Define the patient population to allow for ease of chart selection and input
• Recommend multiple interventions based on a physician’s customized improvement plan
AcknowledgementsAnne Le, PharmD, and Shari Weisenfeld, MD, of Medscape served as scientific directors on the diabetes and osteoporosis PI CME initiatives. Larry Culpepper, MD, MPH; Bradley Gaynes, MD, MPH; Michael Lewiecki, MD; Michael McClung, MD; and Anne Peters, MD, CDE served as faculty for the three initiatives. Medscape’s PI CME initiatives were funded, in part, through independent educational grants from Lilly USA, LLC, Abbott, ucbPharma and Gilead.For more information contact Cyndi Grimes, CME Director, Medscape, LLC at [email protected]
Reference1. Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Cen-
tury. Washington DC: National Academy Press; 2001.
Stage AThe PI CME platform includes 2 compo-nents at Stage A and Stage C: a self-assessment and a chart review. • The chart review is intended to help
participants determine how their clinical practice matches up against specific performance measures.
• The self-assessment is intended to help participants identify individual barriers to improvement.
Self-Assessment: Each question in the self-assessment is tied to a single perfor-mance measure and 1 of the 6 ACGME/ABMS core competencies. • Questions range from simple evalua-
tion (According to the ADA Standards of Medical Care in Diabetes-2010, how often should patients with type 2 diabetes without high-risk foot condi-tions undergo a comprehensive foot examination?) to case-based sce-narios designed to assess participants’ medical knowledge or patient-care habits related to a given performance measure.
• The self-assessment also includes questions to address the full range of barriers to care that can be addressed by clinicians in practice.
Chart Review: Questions in the chart re-view correlate to individual performance measures for the PI CME activity. The platform requires:• That measures evaluated in the chart
review relate to a single patient popu-lation (ie, patients 18 years and older with a diagnosis of type 2 diabetes).
• A minimum of 10 chart entries each to complete Stages A and C.
Feedback: Stage A completers receive scoring that combines their chart review results for each performance measure being evaluated with their self-assessment results (Figure 1) for that measure, grouped by ACGME/ABMS competency. These results become the basis for self-directed learning and improvement in Stage B.
Stage BStage B is available to participants imme-diately upon completion of Stage A. • During Stage B participants establish
a learning plan specific to their needs (Figure 2), with a minimum require-
ment to choose to work on at least 1 performance measure and 1 compe-tency for that measure.
• For example, a participant may review results for 3 measures related to treat-ment of diabetes but decide to focus only on improving foot examinations.
• Participants may see that they scored fairly well in terms of medical knowl-edge and patient care principles related to, for example, foot examina-tions, but the self-assessment reveals room for improvement in communica-tion skills and systems-based practice barriers, such as having an established referral network.
Learning Plan and Learning Record: Once participants have selected 1 or more areas of focus, the PI CME platform recommends resources specific to that identified need (Figure 3.). • These resources are drawn from a
broader collection of CME activities, evidence-based guidelines, practice tools, or other materials selected by the Medscape scientific director and faculty; all participants have access to the full collection of support resources.
• Participants must complete at least 1 required CME activity as part of their Stage B activities.
• Participants check off each resource that they have used as part of their self-directed improvement during this stage.
• Participants may also add their own improvement efforts outside of the provider’s recommendations; for example, attending a local live event on diabetes.
• Stage B lasts a minimum of 3 months before participants can progress to Stage C to allow sufficient time for participants to plan and enact changes in their practice; however, participants have up to 12 months before they must complete Stage C.
Stage CStage C mirrors Stage A. • Participants re-take the self-assess-
ment and enter data for another set of 10 charts.
• Upon completion, participants receive feedback showing changes in score on each performance measure and by chart review between Stages A and C (Figure 4).
• To complete the PI CME activity partici-pants also must complete an evalua-tion and write a personal reflection on their PI CME process.
Cyndi Grimes, CCMEP, and Jane Lowers, Medscape, LLC, New York, NY
Elements to Consider in the Development, Implementation, and Evaluation of Performance Improvement CME
User Experience
and 1 core competency. Table 1 provides an example of how self-assessment questions are linked to performance measures and the core competencies.
Stage A self-assessment grouped by the ACGME/ABMS core competencies.
determine what area or areas of improvement they would like to address and are then provided tools and resources to support their personal PI CME improvement plan.
Table 1. Sample Distribution of Self-Assessment Questions Based on ACGME/ABMS Core Competencies and Performance Measures for PI CME Program on Diabetes Care
ACGME Core Competencies
Performance Measure
Patient Care
Medical Knowledge
Interpersonal and
Communication Skills Professionalism
Systems-‐based Practice
Practice-‐based
Learning and Improvement*
≥ 1 A1c testing
3, 5 , 6, 7 1, 2 11, 28 4
LDL-‐C screening
10, 13 12 27
Foot examination
8, 9, 24, 25 14, 15, 16, 17, 18, 19, 20, 21, 22,
23
26
*Because PI CME itself is practice-based learning, questions generally do not target this competency.
Table 2. Medscape PI CME Completers as of April 2012
Participant Completers by Stage/Element
PI CME Program Topic Stage A
Learning Plan Stage B Stage C
% Completed to Date
Diabetes 2861 2605 2118 632 24
Depression 3159 2846 2361 897 30
Osteoporosis 2657 2360 1937 423 20
Figure 1. Stage A Sample Self-Assessment Results
Self Assessment Results
Please review the detailed results below for a comprehensive analysis of each question, plus an over-view of how your colleagues responded. Overall results: You answered 24 questions correctly
1. Based on the 2011 American Diabetes Association (ADA) position statement, which of the following is not considered to be one of the primary techniques used by healthcare providers and patients to assess glycemic control in patients with type 2 diabetes?
Response Choices Your Colleagues Responded:Self-monitoring of blood glucose 30%Postprandial glucose Best Answer 54%A1c 17%
Explanation:The 2 primary techniques available to healthcare providers and patients to assess the effectiveness of the management plan on glycemic control is patient self-monitoring of blood glucose (SMBG) and A1c. Measurement of postprandial SMBG may be appropriate to achieve postprandial glucose targets.
2. I am familiar with the ADA Standards of Medical Care in Diabetes-2011 for type 2 diabetes.
Response Choices Your Colleagues Responded:Yes Best Answer 73%No 27%
Explanation:The ADA Standards of Medical Care in Diabetes, which are updated annually, are based on a comprehensive review of the relevant literature by a group of highly trained clinicians. The resulting clinical recommendations are intended to provide healthcare professionals with treatment goals and screening, diagnostic, and therapeutic actions known to favorably affect health outcomes of patients with diabetes.
Stage A Stage B Stage C
From Medscape Education Diabetes & Endocrinology
Closing the Gaps in Comprehensive Diabetes Care: PerformanceImprovement PI CME
The self-assessment also includes
Figure 2. Stage B Sample Completed Learning Plan
Learning Plan
Below are your results from stage A, sorted by performance measure and relevant improvement criteria, to help guide your choices for your performance improvement program.
To create your Learning Plan, please select 1 or more choices below.
Performance Measure 1. A1c testPercentage of patients who received ≥ 1 A1c tests in the past year. Secondary measure: trend of A1c values (distribution of number of tests done [0, 1, 2, ≥ 3] and distribution of most recent A1c value by range: < 6.0%, 6.0%-6.9%, 7.0%-7.9%, 8.0%-8.9%, 9.0%-9.9%, ≥ 10%, undocumented). (Source: Physician Consortium on Practice Improvement)
Chart Review Results 40% eligible patients screened
If you would like to improve your results for this performance measure, add one or more of the following criteria to your Learning Plan.
Patient Care and Procedural Skills 50% correctMedical Knowledge 75% correctInterpersonal and Communication Skills 50% correctSystems-Based Practice 100% correct
✓
✓
Stage A Stage B Stage C
From Medscape Education Diabetes & Endocrinology
Closing the Gaps in Comprehensive Diabetes Care: PerformanceImprovement PI CME
Figure 4. Sample Summary Comparison of Stage A and Stage C Results
Stages A & C Results Summary and ComparisonStage C Completed. Credits awarded: 10 Total credits: 20
Performance Measure 1. Ac test
Stage A Stage C50% Chart Review: Eligible Patients Screened 80%
75% Patient Care and Procedural Skills 75%
50% Medical Knowledge 70%
100% Interpersonal and Communication Skills 100%
0% Systems-Based Practice 100%
Performance Measure 2: Lipid Assessment
Stage A Stage C60% Chart Review: Eligible Patients Screened 90%
50% Patient Care and Procedural Skills 100%
70% Medical Knowledge 90%
100% Interpersonal and Communication Skills 100%
Stage A Stage B Stage C
From Medscape Education Diabetes & Endocrinology
Closing the Gaps in Comprehensive Diabetes Care: PerformanceImprovement PI CME
ment to choose to work on at least 1
Figure 3. Stage B Sample Completed Learning Record
Completed Actions for Performance ImprovementStage B Completed. Credits awarded: 5 Total credits: 10
Required Action
Closing the Gaps in Type 2 Diabetes Mellitus: A Focus on Improving Key Performance Measures
Recommended for You
Guideline Adherence Improves Diabetes Care
Comprehensive Diabetes Care -- Are You Up to the Challenge?
American Diabetes Association: Standards of Medical Care in Diabetes - 2010
U.S. Preventive Services Task Force: Screening for Type 2 Diabetes Mellitus in Adults
Physician Consortium for Performance Improvement (AMA-PCPI). Clinical Performance Measures: Adult Diabetes.
American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice for the Management of Diabetes Mellitus
American Association of Diabetes Educators
American Diabetes Association
National Diabetes Information Clearinghouse
View/Print Certificate
✓
✓
✓
✓
✓
✓
Stage A Stage B Stage C
From Medscape Education Diabetes & Endocrinology
Closing the Gaps in Comprehensive Diabetes Care: PerformanceImprovement PI CME
5
P O S T E R
Presented at CME Congress 2012.
“ Elements to Consider in the Development, Implementation, and Evaluation of Performance Improvement CME”
20 21

F O R M A T
PI CME (supported by an educational grant from Lilly USA, LLC). Medscape designed a PI CME platform that leverages the self-directed nature of its membership and included other key factors seen as beneficial to participants. Insights gathered during the development, implementation, and evaluation of PI CME programs within this system will help other providers design future effective PI CME programs.
R E S U L T S
K E Y L E A R N I N G A N D C O N S I D E R A T I O N S
• Design a PI CME initiative that will allow physicians to self-direct their performance improvement specifi c to their clinical needs based on performance measures
• Link core competencies to performance measures to enhance physicians’ ability to address key areas of improvement in practice
• Defi ne the patient population to allow for ease of chart selection and input
• Recommend multiple interventions based on a physician’s customized improvement plan
• Medscape launched 3 PI CME activities in the areas of depression, diabetes, and osteoporosis starting in March 2011 that were supported by independent educational grants from Lilly USA, LLC.
• Participation results as of April 2012 are listed in Table 2. (Note that many physicians are still in the process of completing their PI CME and may not be eligible to start Stage C yet.)
• Additional PI CME programs on pain (supported by Lilly USA, LLC), on rheumatoid arthritis (supported by Abbott and UCB Pharma), and on HIV (supported by Gilead) are in progress.
5 “ Elements to Consider in the Development, Implementation, and Evaluation of Performance Improvement CME”
Cyndi Grimes, CCMEP, and Jane Lowers, Medscape, LLC, New York, NY
AbstractSince the American Medical Association (AMA) created Performance Improvement Continuing Medical Education (PI CME), a new format for AMA Physician’s Recognition Award (PRA) Category 1 CreditTM that recog-nizes CME credit for physicians who engage in self-evaluation and improvement activities related to their clinical performance, differ-ent approaches to this process have been implemented by accredited providers. Many factors must be considered in the design of the PI CME system to ensure optimal participation and performance improvement. Medscape, LLC, designed a PI CME platform that leverages the self-directed nature of its membership and included other key factors seen as beneficial to participants. Insights gathered during the development, implemen-tation, and evaluation of PI CME programs within this system will help other providers design future effective PI CME programs.
OverviewThe AMA asked accredited providers to cre-ate a structured, long-term staged process for PI CME in which physicians learn about specific performance measures, assess their practices based on those measures, imple-ment interventions to improve performance related to the measures over a period of time, and then reassess their practices using the same performance measures. • A performance measure is a mechanism
that enables the user to quantify a selected aspect of care by comparing it to a criterion.1
• The AMA requires that the performance measures are evidenced based and na-tionally recognized, with clear specific data elements for data collection.
Medscape (accredited with commendation by the Accreditation Council for CME in 2010) designed an innovative online platform leveraging our expertise in delivering online CME education and our understanding of our membership usage of the Medscape Educa-tion Website. The goal of this presentation is to share our experience in developing the platform and demonstrate the result of physi-cians participating in and completing PI CME initiatives. MethodsMedscape designed a structured PI CME framework that allows physicians to as-sess their practice against evidence-based performance measures and see how these measures relate to the 6 core competen-cies adopted by the Accreditation Council for Graduate Medical Education (ACGME) and the American Board of Medical Specialties (ABMS). The PI CME platform allows members to ac-cess specific PI CME initiatives on perfor-mance measures across multiple specialties; each offers a consistent format for self-direc-tion and reflection. • Medscape uses performance measures
validated by the AMA’s Physician Consor-tium for Performance Improvement (PCPI), the Physician Quality Reporting System (PQRS) measure set used by the Centers for Medicare & Medicaid Services, and the Healthcare Effectiveness Data and Information set (HEDIS).
In order for physicians to focus their clinical need for improvement, every question in the self-assessment and chart data collection in Stage A is linked to 1 performance measure
and 1 core competency. Table 1 provides an example of how self-assessment questions are linked to performance measures and the core competencies. • Physicians receive results of their Stage A self-assessment grouped by the ACGME/ABMS core competencies. • From this information, they can determine what area or areas of improvement they would like to ad-dress and are then provided tools and resources to support their personal PI CME improvement plan.
ResultsMedscape launched 3 PI CME activities in the areas of depression, diabetes, and osteoporosis starting in March 2011 that were supported by independent educational grants from Lilly USA, LLC. • Participation results as of April 2012 are listed in
Table 2. (Note that many physicians are still in the process of completing their PI CME and may not be eligible to start Stage C yet.)
• Additional PI CME programs on pain (supported by Lilly USA, LLC), on rheumatoid arthritis (supported by Abbott and UCB Pharma), and on HIV (support-ed by Gilead) are in progress.
Key Learning and Considerations• Design a PI CME initiative that will allow physicians
to self-direct their performance improvement spe-cific to their clinical needs based on performance measures
• Link core competencies to performance measures to enhance physicians’ ability to address key areas of improvement in practice
• Define the patient population to allow for ease of chart selection and input
• Recommend multiple interventions based on a physician’s customized improvement plan
AcknowledgementsAnne Le, PharmD, and Shari Weisenfeld, MD, of Medscape served as scientific directors on the diabetes and osteoporosis PI CME initiatives. Larry Culpepper, MD, MPH; Bradley Gaynes, MD, MPH; Michael Lewiecki, MD; Michael McClung, MD; and Anne Peters, MD, CDE served as faculty for the three initiatives. Medscape’s PI CME initiatives were funded, in part, through independent educational grants from Lilly USA, LLC, Abbott, ucbPharma and Gilead.For more information contact Cyndi Grimes, CME Director, Medscape, LLC at [email protected]
Reference1. Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Cen-
tury. Washington DC: National Academy Press; 2001.
Stage AThe PI CME platform includes 2 compo-nents at Stage A and Stage C: a self-assessment and a chart review. • The chart review is intended to help
participants determine how their clinical practice matches up against specific performance measures.
• The self-assessment is intended to help participants identify individual barriers to improvement.
Self-Assessment: Each question in the self-assessment is tied to a single perfor-mance measure and 1 of the 6 ACGME/ABMS core competencies. • Questions range from simple evalua-
tion (According to the ADA Standards of Medical Care in Diabetes-2010, how often should patients with type 2 diabetes without high-risk foot condi-tions undergo a comprehensive foot examination?) to case-based sce-narios designed to assess participants’ medical knowledge or patient-care habits related to a given performance measure.
• The self-assessment also includes questions to address the full range of barriers to care that can be addressed by clinicians in practice.
Chart Review: Questions in the chart re-view correlate to individual performance measures for the PI CME activity. The platform requires:• That measures evaluated in the chart
review relate to a single patient popu-lation (ie, patients 18 years and older with a diagnosis of type 2 diabetes).
• A minimum of 10 chart entries each to complete Stages A and C.
Feedback: Stage A completers receive scoring that combines their chart review results for each performance measure being evaluated with their self-assessment results (Figure 1) for that measure, grouped by ACGME/ABMS competency. These results become the basis for self-directed learning and improvement in Stage B.
Stage BStage B is available to participants imme-diately upon completion of Stage A. • During Stage B participants establish
a learning plan specific to their needs (Figure 2), with a minimum require-
ment to choose to work on at least 1 performance measure and 1 compe-tency for that measure.
• For example, a participant may review results for 3 measures related to treat-ment of diabetes but decide to focus only on improving foot examinations.
• Participants may see that they scored fairly well in terms of medical knowl-edge and patient care principles related to, for example, foot examina-tions, but the self-assessment reveals room for improvement in communica-tion skills and systems-based practice barriers, such as having an established referral network.
Learning Plan and Learning Record: Once participants have selected 1 or more areas of focus, the PI CME platform recommends resources specific to that identified need (Figure 3.). • These resources are drawn from a
broader collection of CME activities, evidence-based guidelines, practice tools, or other materials selected by the Medscape scientific director and faculty; all participants have access to the full collection of support resources.
• Participants must complete at least 1 required CME activity as part of their Stage B activities.
• Participants check off each resource that they have used as part of their self-directed improvement during this stage.
• Participants may also add their own improvement efforts outside of the provider’s recommendations; for example, attending a local live event on diabetes.
• Stage B lasts a minimum of 3 months before participants can progress to Stage C to allow sufficient time for participants to plan and enact changes in their practice; however, participants have up to 12 months before they must complete Stage C.
Stage CStage C mirrors Stage A. • Participants re-take the self-assess-
ment and enter data for another set of 10 charts.
• Upon completion, participants receive feedback showing changes in score on each performance measure and by chart review between Stages A and C (Figure 4).
• To complete the PI CME activity partici-pants also must complete an evalua-tion and write a personal reflection on their PI CME process.
Cyndi Grimes, CCMEP, and Jane Lowers, Medscape, LLC, New York, NY
Elements to Consider in the Development, Implementation, and Evaluation of Performance Improvement CME
User Experience
and 1 core competency. Table 1 provides an example of how self-assessment questions are linked to performance measures and the core competencies.
Stage A self-assessment grouped by the ACGME/ABMS core competencies.
determine what area or areas of improvement they would like to address and are then provided tools and resources to support their personal PI CME improvement plan.
Table 1. Sample Distribution of Self-Assessment Questions Based on ACGME/ABMS Core Competencies and Performance Measures for PI CME Program on Diabetes Care
ACGME Core Competencies
Performance Measure
Patient Care
Medical Knowledge
Interpersonal and
Communication Skills Professionalism
Systems-‐based Practice
Practice-‐based
Learning and Improvement*
≥ 1 A1c testing
3, 5 , 6, 7 1, 2 11, 28 4
LDL-‐C screening
10, 13 12 27
Foot examination
8, 9, 24, 25 14, 15, 16, 17, 18, 19, 20, 21, 22,
23
26
*Because PI CME itself is practice-based learning, questions generally do not target this competency.
Table 2. Medscape PI CME Completers as of April 2012
Participant Completers by Stage/Element
PI CME Program Topic Stage A
Learning Plan Stage B Stage C
% Completed to Date
Diabetes 2861 2605 2118 632 24
Depression 3159 2846 2361 897 30
Osteoporosis 2657 2360 1937 423 20
Figure 1. Stage A Sample Self-Assessment Results
Self Assessment Results
Please review the detailed results below for a comprehensive analysis of each question, plus an over-view of how your colleagues responded. Overall results: You answered 24 questions correctly
1. Based on the 2011 American Diabetes Association (ADA) position statement, which of the following is not considered to be one of the primary techniques used by healthcare providers and patients to assess glycemic control in patients with type 2 diabetes?
Response Choices Your Colleagues Responded:Self-monitoring of blood glucose 30%Postprandial glucose Best Answer 54%A1c 17%
Explanation:The 2 primary techniques available to healthcare providers and patients to assess the effectiveness of the management plan on glycemic control is patient self-monitoring of blood glucose (SMBG) and A1c. Measurement of postprandial SMBG may be appropriate to achieve postprandial glucose targets.
2. I am familiar with the ADA Standards of Medical Care in Diabetes-2011 for type 2 diabetes.
Response Choices Your Colleagues Responded:Yes Best Answer 73%No 27%
Explanation:The ADA Standards of Medical Care in Diabetes, which are updated annually, are based on a comprehensive review of the relevant literature by a group of highly trained clinicians. The resulting clinical recommendations are intended to provide healthcare professionals with treatment goals and screening, diagnostic, and therapeutic actions known to favorably affect health outcomes of patients with diabetes.
Stage A Stage B Stage C
From Medscape Education Diabetes & Endocrinology
Closing the Gaps in Comprehensive Diabetes Care: PerformanceImprovement PI CME
The self-assessment also includes
Figure 2. Stage B Sample Completed Learning Plan
Learning Plan
Below are your results from stage A, sorted by performance measure and relevant improvement criteria, to help guide your choices for your performance improvement program.
To create your Learning Plan, please select 1 or more choices below.
Performance Measure 1. A1c testPercentage of patients who received ≥ 1 A1c tests in the past year. Secondary measure: trend of A1c values (distribution of number of tests done [0, 1, 2, ≥ 3] and distribution of most recent A1c value by range: < 6.0%, 6.0%-6.9%, 7.0%-7.9%, 8.0%-8.9%, 9.0%-9.9%, ≥ 10%, undocumented). (Source: Physician Consortium on Practice Improvement)
Chart Review Results 40% eligible patients screened
If you would like to improve your results for this performance measure, add one or more of the following criteria to your Learning Plan.
Patient Care and Procedural Skills 50% correctMedical Knowledge 75% correctInterpersonal and Communication Skills 50% correctSystems-Based Practice 100% correct
✓
✓
Stage A Stage B Stage C
From Medscape Education Diabetes & Endocrinology
Closing the Gaps in Comprehensive Diabetes Care: PerformanceImprovement PI CME
Figure 4. Sample Summary Comparison of Stage A and Stage C Results
Stages A & C Results Summary and ComparisonStage C Completed. Credits awarded: 10 Total credits: 20
Performance Measure 1. Ac test
Stage A Stage C50% Chart Review: Eligible Patients Screened 80%
75% Patient Care and Procedural Skills 75%
50% Medical Knowledge 70%
100% Interpersonal and Communication Skills 100%
0% Systems-Based Practice 100%
Performance Measure 2: Lipid Assessment
Stage A Stage C60% Chart Review: Eligible Patients Screened 90%
50% Patient Care and Procedural Skills 100%
70% Medical Knowledge 90%
100% Interpersonal and Communication Skills 100%
Stage A Stage B Stage C
From Medscape Education Diabetes & Endocrinology
Closing the Gaps in Comprehensive Diabetes Care: PerformanceImprovement PI CME
ment to choose to work on at least 1
Figure 3. Stage B Sample Completed Learning Record
Completed Actions for Performance ImprovementStage B Completed. Credits awarded: 5 Total credits: 10
Required Action
Closing the Gaps in Type 2 Diabetes Mellitus: A Focus on Improving Key Performance Measures
Recommended for You
Guideline Adherence Improves Diabetes Care
Comprehensive Diabetes Care -- Are You Up to the Challenge?
American Diabetes Association: Standards of Medical Care in Diabetes - 2010
U.S. Preventive Services Task Force: Screening for Type 2 Diabetes Mellitus in Adults
Physician Consortium for Performance Improvement (AMA-PCPI). Clinical Performance Measures: Adult Diabetes.
American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice for the Management of Diabetes Mellitus
American Association of Diabetes Educators
American Diabetes Association
National Diabetes Information Clearinghouse
View/Print Certificate
✓
✓
✓
✓
✓
✓
Stage A Stage B Stage C
From Medscape Education Diabetes & Endocrinology
Closing the Gaps in Comprehensive Diabetes Care: PerformanceImprovement PI CME
TABLE 2: Medscape PI CME Completers as of April 2012
PI CME Program Topic
Diabetes
Depression
Osteoporosis
Stage A
2861
3159
2657
Learning Plan
2605
2846
2360
Stage B
2118
2361
1937
Stage C
632
897
423
% Completed to Date
24
30
20
PARTICIPANT COMPLETERS BY STAGE/ELEMENT
22 23

Grounded in science, fueled by innovation, driven to impact healthcare quality