opioid information package...opioid information package afn special chiefs assembly gatineau, qc...
TRANSCRIPT
Opioid Information Package
AFN Special Chiefs Assembly Gatineau, QC
December 2016

Community-basedbuprenorphinetreatmentforopioidusedisorders:AguideforIndigenouscommunities
Thisguidediscussesopioidaddictionanditstreatment,anddescribeshowcommunitybuprenorphineprogramswork.
Background:Opioidusedisordersandtreatment
WhyaresomanypeopleinIndigenouscommunitiesaddictedtoopioids?
Intergenerationaltrauma,likeotherformsoftrauma,isoftenacontributingfactorinsubstanceuse.Peoplewhohaveenduredpsychologicaltraumaduringchildhoodoftenexperiencelong-lastingsymptomsofpost-traumaticstressdisorder:nightmares,depression,anxiety,troubleformingrelationships,andlowself-esteem.Whenpeoplefirststartusingopioids,thesefeelingsvanishforafewhours,replacedbyfeelingsofconfidence,enthusiasm,energy,andcomfort.Unfortunately,thenervoussystemquicklyadaptstothesepositivefeelings,sothepersonmusttakeahigherdosetoachievethesameeffect(thisiscalledtolerance).Withinacoupleofweeksofdailyopioiduse,peoplebegintoexperiencefrighteningwithdrawalsymptoms,andmustnowtaketheopioideverydayjusttowardoffthesesymptoms.Apersonwhoendsupinthiscyclehasanopioidusedisorder:theiropioidusehastakenovertheirlife.
Insmallcommunities,substanceuseandsubsequentaddictioncanquicklyspreadfromoneortwopeopletotheircircleoffriends,usewithinthefamily,andsometimeseventothewholecommunity.InsomeIndigenouscommunitiesinCanada,almosteveryfamilyhasatleastonememberwithanaddiction.
Whyisitsodifficultforpeopletostopusingopioids?
Peoplewhotakeopioidsdailyexperiencewithdrawalsymptomswhentheygowithoutthemedication:muscleaches,nausea,insomnia,anxiety,depression,andstrongcravings.Withdrawalcancauseterribledistress–somepatientsattemptsuicideiftheycannotobtainopioidstorelievetheirsymptoms.Theconstantfearofwithdrawalisoftenwhatkeepspeoplefromquitting,evenwhentheyknowthattheiropioiduseisruiningtheirlife.
Whataremethadoneandbuprenorphine?
Methadoneandbuprenorphineareopioidsusedasmedicationstotreataddiction.Methadoneistakeninorangejuice,whilebuprenorphineisdissolvedunderthetongue.Unlikeotheropioids,whichreachthebrainveryquicklyandcauseanimmediate,short-lastinghigh,methadoneandbuprenorphineonlyreachtheirfulleffectaftertwoorthreehours,andtheseeffectslastfor24hours.Asaresult,methadoneandbuprenorphinemedicationsrelievecravingsandsymptomsofwithdrawalfortheentiredaywithoutcausingthesamehighthatotheropioidsdo.
Atthebeginningoftreatment,methadoneandbuprenorphinearedispenseddaily,undertheobservationofastaffmember.Thismakesithardforpatientstousethemedicationinawayotherthanasprescribed,ortosharethemedicationwithothers.Take-homedosescanbegivenwhennecessaryformedicaltrips,work,orfamilyobligations.Patientsonmethadoneorbuprenorphineare

requiredtoleaveregularurinesamples,whicharetestedformethadoneorbuprenorphine,illicitopioids,andotherdrugs.
What’sthedifferencebetweenmethadoneandbuprenorphine?
Methadoneisaverypowerfulopioid,whilebuprenorphineisonlyapartialopioid.Bothmethadoneandbuprenorphineareextremelyeffectiveatrelievingwithdrawalsymptomsandcravings,butmethadonemayhavemoresideeffectsthanbuprenorphine,suchassedationandriskofoverdose.Becauseitissuchastrongopioid,peoplecanoverdoseiftheytakeevenaslightlyhigherdoseofmethadonethantheyareprescribed.Forthisreason,doctorsmusthavespecialtrainingtoprescribemethadone.Buprenorphineissaferthanmethadone;itcancausedrowsinessandeuphoriaifitismisused,butfataloverdosesareveryrare.Becauseofitssafety,familydoctorsdon’tneedanyextratraininginordertoprescribeit,butobserveddailydosesarestillbestuntilthepatientisstableanddoingwell.
Isn’tgivingpeoplebuprenorphineormethadonejustswitchingoneaddictingdrugforanother?
Wheninjected,heroin,morphine,hydromorphone,andfentanylreachthebrainwithinseconds,producinganintensehigh.Thesesubstancesleavethebrainafterafewhours,triggeringseverewithdrawalsymptoms.Mostpeoplewithopioidusedisordersareunabletowork,gotoschool,orlookaftertheirfamily,becausetheyspendthewholedaygettingandtakingthedruginadesperateefforttofeelnormalandavoidwithdrawal.
Incontrast,peopledonotexperienceeuphoria,sedation,orwithdrawalaftertakingmethadoneorbuprenorphine,becausethemedicationstakehourstoreachtheirfulleffect,andtheeffectslastthroughoutthedayuntilthenextday’sdose.Patientsonthesemedicationscanreturntowork,school,ortheirfamilywithoutanyimpairmentintheirthinkingorfunctioning.
Aren’tmethadoneandbuprenorphinejustband-aids?Shouldn’ttreatmentbebasedoncounsellingthataddressestherootcausesofaddiction–trauma,poverty,anddespair?
Psychologicalcounsellingisessentialforlong-termrecovery.Itismosteffective,however,whenusedincombinationwithmethadoneorbuprenorphinetreatment,whichenablepeopletoparticipateincounsellingandtreatmentactivitieswithoutbeingtormentedbycravingsandwithdrawalsymptoms.
Howwelldobuprenorphineandmethadonetreatmentswork?
Extensiveresearchhasshownthatmethadoneandbuprenorphinetreatmentprogramsdramaticallyreduceopioiduse,overdosedeaths,andcrime,comparedtotreatmentsthatonlyprovidecounselling.Thesymptomsofopioidwithdrawalcanbesointenseandfrighteningthatiftheyarenottreatedmedically,mostpatientsrelapsequickly,eveniftheyreceiveexcellentcounsellingandsupport.
Whydopeoplehavetogotospecialclinicstogetmethadone?
Asmentionedabove,doctorsneedtohavespecialtraininginordertoprescribemethadone.Thereareonlyabout300doctorsinOntariowhohavethisspecialtraining,andalmostallofthemworkincitiesinthesouth.Manyofthesedoctorsworkinspecializedmethadoneclinics,whicharemoreefficientthangeneralclinicsforthespecifickindsofservicesthatmethadonedoctorsgive,likesupervisedurinedrugscreeningandobserveddailydispensing.Mostpatientsreceivemethadoneintheseclinics,whichareusuallyseparatefromprimarycareandmentalhealthservices.Manymethadoneclinicsoffer

buprenorphinetreatmentaswell;however,becausedoctorsdonotneedspecialtrainingtoprescribebuprenorphine,itcanbeprescribedinanysetting,notjustinurbanmethadoneclinics:ingeneralfamilymedicineclinics,hospitals,prisons,emergencydepartments,andbysolopractitionersinsmallruralcommunities.
Methadoneclinicskeeppatientsonmethadoneforyears,andsometimesforlife.Doesn’titmakemoresenseforpatientstoonlybeonmethadoneorbuprenorphineforaweekortwowhiletheyrecoverfromtheirwithdrawalsymptoms?
Mostpeoplerelapseiftheyaretaperedoffmethadoneorbuprenorphinetooquickly.Thisisbecausewithdrawalsymptoms–insomnia,anxiety,cravings–canlastformonthsafterthelastdoseofopioids.Also,addictedpatientshavelearnedthatdrugsgiveinstantandcompletereliefwhentheyfeelstressed,lonely,bored,angry,orupset;itcantakemanymonthsofcounsellingandhardworktolearnnewwaysofcopingwiththesefeelings,tomakenewfriendswhoaren’tdrugusers,andtotakeonnewresponsibilitieswithfamily,workorschoolthatkeeppeopleactiveandbusyawayfromdruguse.
Manypeopleareabletotaperoffmethadoneorbuprenorphinewhentheyhaven’tuseddrugsforatleastsixmonthsandthey’releadingproductive,busylivessurroundedbysupportivefamilyandfriends.
Somepeopleinmycommunityareattendingamethadoneclinicinanearbytown.HowdoIknowifthisclinicisprovidinggoodcare?
Bandleaders,addictioncounsellors,andfamilymembersofaddictedpatientsshouldaskthefollowingquestionsabouttheirlocalmethadoneclinic.
Doestheclinicprovideprimarycare?Agoodprogramshouldprovidepatientswithprimarycare–immunizations,screeningforcancerandheartdisease,andmanagementofchronicdiseasessuchasasthmaanddiabetes.Ifpatientshaveaccesstoprimarycareintheirowncommunities,thenthemethadonephysicianshouldcommunicateregularlywiththeprimarycarephysiciansornurses.
Doestheclinicprovidecounselling?Asmentionedabove,counsellingisanessentialpartofaddictiontreatment.Patientsarenotlikelytofullyrecoveriftheydon’treceivecounsellingandsupportfortheunderlyingmentaldisorderthatcausedtheaddiction,suchaspost-traumaticstressdisorder,anxiety,ordepression.
Doestheclinichelporhinderpatients’returntoanactiveandfulllife?Thegoalofaddictiontreatmentistohelppatientsliveafullandactivelife.Somemethadoneclinicsrequirepatientstoattendthecliniconceortwiceperweektoleaveaurinedrugscreenandgetaprescription.Thesevisitscaninterferewithpatients’workandfamilylives,becausetheyofteninvolve4-8hoursoftravellingandwaitingattheclinic.
Theeasiestwaytoanswerthesequestionsistotalktopatientsinyourcommunityabouttheirexperiencesattheclinic.Howoftendotheyhavetoattendtheclinic,andhowlongdoeseachvisittake?Howmuchtimedoesthephysicianspendwiththem?Dotheygetcounselling?Doesanyoneattheclinictalktothemabouttheiremotions,concernsordailylives?Aretheirfamilymembersallowedtoattendappointmentsandparticipateintheircare?Cantheygethelpformedicalproblemsattheclinic?Overall,dotheyfeelthatthephysiciansandotherclinicalstaffcareaboutthem?Aretheysatisfiedwiththecaretheyhavereceived?

WhatshouldIdoifmycommunitydoesn’thaveaccesstoaclinicthatprovidesgoodaddictioncare?
Iftherearemembersofyourcommunitywhowouldbenefitfrommethadoneorbuprenorphinetreatmentbutthereisnoaccesstoconvenient,high-qualitycare,youandothermembersofyourcommunityshouldconsidersettingupyourownbuprenorphinetreatmentprogram.SiouxLookoutcommunitieshavesetupanumberofbuprenorphineprogramsoverthepastseveralyears,andtheseprogramscanbeusedasamodelforyourcommunity.
SiouxLookoutprograms:Description
Priorto2010,ChiefandBandCouncilsandcommunityleadersinnorthwesternOntariobegantobringattentiontotheseriousissuesandimpactsofPrescriptionDrugAbuse(PDA)intheircommunities.In2010,theChiefsofOntariodeclaredPDAanepidemicandtheyreleasedtheFinalReportsonaPDAStrategy.By2012,atripartiteagreementbetweenprovincial,federalandSiouxLookoutHealthauthoritiesproducedaworkplan.CommunitiesintheSiouxLookoutFirstNationHealthAuthority(SLFNHA)regionbegantoplan,develop,mobilize,andgoverncommunity-basedtreatmentprogramsforPDA.Currentlythereare22buprenorphineprogramsintheSiouxLookoutregion,treatingapproximately1300patients.SimilarprogramsalsoexistinotherTreaty9communities.Whileeveryprogramisdifferent,theysharethefollowingcommonelements:
Theprogramteam:Eachprogramteamconsistsofamentalhealthandaddictionworker,afamilydoctor,amedicationdispenser,andanadministratorfromtheBandCouncil.Theteammeetsregularly,sometimesinconsultationwithanaddictiondoctor,tomakeclinicalandadministrativedecisionsabouttheprogram.
Assessment:Eachpatientisindividuallyassessedbyadoctor(eitheralocalfamilydoctororavisitingdoctorwithexpertiseinaddictions),inordertodeterminewhetherthepatienthasanopioidusedisorderand/orothermentalandphysicalconditions.Theassessmentconsistsofalonginterviewwiththepatient,aphysicalexam,andbloodwork.
Buprenorphineprescribing:Aftertheassessment,ifthedoctordeterminesthatthepatienthasanopioidusedisorder,theyprescribeadailydoseofbuprenorphine,adjustingthedoseuntilthepatient’scravingsandwithdrawalsymptomshaveresolved.
DispensingbuprenorphineDailydispensingofmedicationisdonebycommunitymemberdispensersthathavebeenhiredbytheBandCounciltoworkinthetreatmentprograms.Insomecommunities,nursingstationstaffornursesdispensebuprenorphine.
Urinedrugtesting:Urinesamplesareregularlytestedforbuprenorphine,opioids,andotherdrugs,usingsmalldisposablesticksthataredippedintotheurine.Nursesandphysicianscanconductthesetests,ascantrainedcommunitymembers.
Counselling:Theclinicdoctorprovidescounsellingduringtheassessmentandduringeachclinicvisit.MentalhealthandNationalNativeAlcoholandDrugAbuseProgram(NNADAP)workersprovidecounsellingandcasemanagement.Somecommunitieshavechosentosupportandfundcounsellingprograms,whichpatientsattenddailyforthefirstfewweeksoftreatment.Aftercareworkersengageclientsincounsellingandrecoveryactivities.Manypatientsalsobenefitfromtraditionalhealers,supportfromthechurch,orland-basedactivitiessuchasgardening.Informalsupportisalsoprovided

byelders,familymembers,thebandcouncil,friends,andpeerswhoarealsointreatment.Insomecommunities,apublicceremonyisheldforpatientsontheirfirstdayofbuprenorphinetreatment;thepatientsaregreetedandcongratulatedbycommunityleadersandfamilymembersforbeginningtheirjourneytowardrecovery.
Taperinganddiscontinuingtreatment:Patientsaredischargedfromtheprogramiftheyviolateprogramrules(forexample,iftheyarecaughtsellingtheirbuprenorphinetablets).Thebuprenorphinedoseistaperedwhenthepatientandthetreatmentteamfeelthatthepatientisready.
Funding:Themedicationsarecoveredbytheprovincialandfederaldrugplans.HealthCanadafundedstaff,suchasnurses,mentalhealthworkersandtheNNADAPworkersthatsupporttheprograms.ThreefundingcyclesfromHealthCanadaforPDAtreatmentsupportthedeliveryoftheprogram,includinghiringofdispensingandaftercarestaff.OutsideaddictiondoctorsthatvisitthecommunityhavetheirtravelexpensescoveredbytheCollegeofPhysiciansandSurgeonsofOntario,andtheyarepaidadailyratebytheSiouxLookoutRegionalHealthAuthority.Thecoststothebandsareoffsetbysavingsintravelcostsforpatientswhowouldhavehadtotravelbybustoattendamethadoneclinicinanearbycity.
HowwelldotheSiouxLookoutprogramswork?
TwopaperswererecentlypublishedintheCanadianFamilyPhysicianjournalonthebuprenorphineprogramsinSiouxLookout(seeenclosed).Thefirstpaperlookedattheimpactofbuprenorphinetreatmentononecommunity.Itreportedthatoneyearaftertheintroductionofbuprenorphinetreatment,“policecriminalchargeshadfallenby61.1%,childprotectioncaseshadfallenby58.3%,schoolattendancehadincreasedby33.3%,andseasonalinfluenzaimmunizationshaddramaticallygoneupby350.0%.Attendanceatcommunityeventsisnowrobust,andsalesatthelocalgeneralstorehavegoneupalmost20%.”Onecommunitymembersaidthattheprogram“hasbroughtlifebacktoourcommunity,[which]isbeingrestoredtothewayitusedtobebeforeeveryonegotstuckinaddiction.”Thesecondpaperlookedatindividualpatientresultsinsixcommunities.Itreportedthat78%ofthepatientswerestillintreatmentafteroneyear.Thiscomparesfavourablywithaprovincialaverageofonly50%.Intwoseparateanalyses,88%and90%ofurinedrugscreenswerenegativeforillicitdrugs.ThesuccessoftheSiouxLookoutprogramsisprobablyduetoseveralfactors.Thewholecommunityparticipatesinandsupportstheprogram,patientshaveagoodrelationshipwiththetreatmentteam,andtheprogramsaredeeplyfocusedonhelpingpatientsreturntotheircommunityactivitiesandresponsibilities.Perhapsmostimportantly,patientsgettreatmentintheirhomecommunity,withouthavingtotraveltoattendanoutsideclinic.Ifourcommunitysetupacommunitybuprenorphineprogram,whatshouldbedoneaboutpatientswhoarealreadyonmethadoneinanoutsidemethadoneclinic?
Methadonedoctorsshouldhelppatientsswitchfrommethadonetobuprenorphineiftheyrequestitanditisintheirbestinterests.Thedoctorprescribingmethadoneandthecommunitydoctorprescribingbuprenorphinehavetoworktogethertoorganizetheswitch.Switchingfrommethadonetobuprenorphineisnoteasy,butitcanbedonesuccessfullyinmostcases.
Howcanourcommunitysetupanewbuprenorphineprogram?

CommunitiesthatwishtoestablishtheirowntreatmentprogramshouldconsultwithpeoplewhoworkintheSiouxLookoutprograms.SiouxLookoutdoctorsandnursepractitionerscanassistwithrecruiting,trainingandmentoringthefamilydoctorsinyourcommunity,andSiouxLookoutprogramstaffcanhelptrainyourcommunity’smentalhealthandaddictionworkersanddispensers.Administratorscanassistwithfundingandplanning.

OPIOIDSUMMITFirstNationsActionPlanforOpioidMisuse
CarolHopkins,[email protected]
AbstractThisbriefprovidesanoutlinetoguidetheapplicationofHealthCanada’sActionPlanforOpioid
MisusewithFirstNationsinCanada.
1
“Itissaid,theGreatSpiritworkedtoensurewhatwewouldneedtolivelife,foreverandalltime,nomatterthecircumstances,wasthoughtofandputintoCreation”ElderJimDumont
IntroductionThisquoteisanindigenousteachingthatconveysabeliefthatsolutionstothechallengeswefaceareaccessiblethroughanindigenousworldviewandpracticesfromthatworldview.Wehaveacollectiveresponsibilityasindigenouspeoplestoensurewefacilitateaccesstosolutionsthataremeaningful.FirstNationsinCanadahavearticulatedthesesolutions,theirneedsandstrengthsintheHonouringOurStrengths:ARenewedFrameworktoAddressSubstanceUseIssuesAmongFirstNationsinCanada(HealthCanada2010)andmorerecently,FirstNationshavearticulatedacomprehensiveapproachtoachievingmentalwellnessforFirstNationspeopleandcommunitiesthroughtheFirstNationsMentalWellnessContinuumFramework(HealthCanada2015).TheFirstNationsMentalWellnessContinuumFrameworkdescribesthevisionforFirstNationsmentalwellness,withcultureasthefoundation.ItemphasizesFirstNationsstrengthsandcapacities.ItprovidesadviceonpolicyandprogramchangesthatshouldbemadetoimproveFirstNationsmentalwellnessoutcomes.AchievingmeaningfuloutcomesforFirstNationspeopleinCanadaisthevisionforaddressingtheopioidcrisisandongoingopioidmisuse;thatis,actiontoaddressopioidmisusemustbemeasuredbytheextenttowhichthoseactionscreatementalwellnessamongFirstNations.Theseindigenousbasedoutcomesmeasuresare:Hope,Belonging,MeaningandPurpose.Toachievesomemeasureoftheseindigenousdefinedmentalwellnessoutcomesrequireschangeinthewaygovernmentsdobusiness.Weneedmorehorizontalworkacrossgovernmentsandbetweendepartments/ministriesandwithacommitmenttoFirstNationsaspartnersingoverningmentalwellness.
HealthCanada’sActionPlanforOpioidMisuse(HealthCanada,2016)
1. BetterinformingCanadiansabouttherisksofopioids:newwarningstickers,patientinformationsheets,reviewofbestpractices
2. Supportingbetterprescribingpractices:promoteprescriptionmonitoringprograms,examinepharmacyrecords,shareinformationwithPTlicensingbodies,CanadaHealthInfowaye-prescribingsolution
3. Reducingeaseaccesstounnecessaryopioids:contraindicationsforapprovedopioids,requiringaprescriptionforlow-dosecodeineproducts,mandatoryriskmanagementplansforcertainopioids
4. Supportingbettertreatmentoptionsforpatients:better&fasteraccesstonaloxone,expeditingthereviewofnon-opioidpainrelievers,re-examiningspecialrequirementsformethadone
5. Improvingtheevidencebase:bringingtogetherexpertsinthefieldtodiscusshowtoimprovedatacollectionandtheCanadianevidencebase

2
FirstNationswithintheActionPlanforOpioidMisuse
1. Better informing Canadians about the risks of opioids:
GreatercapacityisrequiredwithinFirstNationsgovernedorganizationstodevelopculturallyrelevantinformationonBestPracticesthatareinclusiveofthefollowing:
a. UseofsocialmediaandeHealthsolutionsforpreventionandearlyinterventionaimedatyouthandwomenofchildbearingyearsonthefollowing:
i. Educationonfentanyl,Carfentanyl,thechemicalW-18anditsanalogsii. Naloxoneiii. Youthshouldhaveaccesstoservicesspecifictotheirdevelopmentalneedsand
youthneedtobeincludedindesigningthesestrategies.} Thereareveryfewprovidersofaddictiontreatmentservicesandspecifically
medicaltreatmentofOpioidUseDisorderswhoprovideyouthspecificservices,orattheveryleastintegrateservicesadaptedtotheneedsofyoungpeople.
} Themajorityofyoungpeoplewhoareactivelymisusingopioidshaveconcurrentmentalhealthissues,suchasanxietyandmooddisorderslinkedtointergenerationaltrauma.
} Homeless,streetinvolvedandmarginalizedyouthoftenhavecomplexpsychologicalandsocialissues.
} Twoexcellentexamplesofservicesadaptedtotheneedsofyouthare:o SchoolbasedprogramatDennisFranklynCromartyHighSchoolin
ThunderBayo TheBreakawayTorontoOpiateSupportTeam
} AnearlyinterventionprogramthathasalsohadgoodsuccessistheBuffaloRidersprogram.
} Supportforyouthcareerplanningandmentoringisrequiredinthefollowing:mentorshipintranslatingindigenousknowledgeintopractice,medicine,pharmacy,counselling,communitydevelopmentandharmreductionarenecessarytoensureFirstNationshavethenecessarycapacitytomeettheever-increasingdemandforculturallyrelevantandmeaningfulstrategiesforopioidmisuse.
iv. Prenatalcare–promotionofharmreduction(Buprenorphine-naloxone)andwarningsagainstwithdrawalofopioidriskstofetus
v. SupportinBirthing–rightsto“mother”andrightstocontinuityofhealthcarefornewbornandmothertogether.Attentioninaddressingneonatalabstinencesyndromefocusedondestigmatizingtreatmentforopioidaddictionandfocusonsupportforcontinuityoftreatment.RequireseducationwithChildWelfare.
vi. SupportinMothering–lactationsupport,FNculturespecificDoulacare

3
b. PromotionofCommunityBasedTreatmentasaBestPracticei. LandBasedServiceDeliveryModel&Buprenorphine-Naloxone(In
development)ii. Supportisrequiredtodecolonizeapproachestoaddictionsandmentalhealth
caretoincludeIndigenousculturalknowledgeandpracticesbyensuringappropriatefundingisinplacetocontractculturalpractitioners,providetrainingforstafftoensurearespectfulmulti-disciplinaryapproachinclusiveofculturalpractices,andtosupportindigenouspractitionersinunderstandingthenatureofaddictivesubstances.
c. HarmReductionStrategyrequiresmoreeducationandsupporttobuildcapacityinFirstNationscommunitiesandtosupportcommunityhealthplanning.Oneexampleofacommunity-basedharmreductionapproachisTsuTinaFirstNationlocatedjustoutsideCalgaryABwhohasinvesteditsownsourcerevenueinacommunitywideharmreductionstrategyandishavingsuccessstemmingthetideoftheopioidcrisis.
2. Supporting better prescribing practices:a. Buprenorphine-NaloxoneasfirstlineoftreatmentforFirstNationsb. PromoteGuidelinesforFirstNationscommunitybasedopioidtreatmentwith
physicianstosupportthemineffectivelysupportingFirstNationspeopleinaddressingopioidaddictioninatrauma-informedandstrengths-basedmanner(indevelopment)
c. SupportforimplementationofanationalprescriptiondrugusesurveyforFirstNationsCommunities(indevelopment)
d. CapacitydevelopingwithinFirstNationscommunitiestoengageingoverningopioidmisusetreatmentandprevention
3. Supporting better treatment options for patients:a. InvestindevelopingprimarycarewithinFirstNationscommunitiessuchas
supportingnursesinFirstnationscommunitiestotransitiontoastrength-basedapproachtoprimarycareandbecomemoreinvolvedinsupportingcommunitiesintheiropioidmisusestrategies.
b. CorefundingforFirstNationsgovernedharmreductionstrategiesandLandBasedOpioidTreatmentprograms
c. FundcapacitydevelopmentwithinFirstNationsCommunitiestosupportpeopleinopioidagonisttreatmenttohaveanactiveroleincommunityandforthecommunitythroughemploymentandskilldevelopment
d. Thatprogramfundingbeflexibleenoughtoallowcommunitiestoadjusttodynamicandchangingneedsandpriorities(e.g.,diversionofsuboxone),
e. Fundingtosupport“communityofpractice”forhealthdirectorsandprogramstaffengagedinaddressingopioidmisusetogettogetheratleasttwiceperyeartoshare/collaborate/discussdifficultiesandsuccesses.
4
4. Improving the evidence base:a. Ifwewanttomeasurethedifferencewewillmakeinaddressingtheopioidcrisis
amongIndigenouspeopleinCanada,thenthiswillrequireustomeasureculturallymeaningfuloutcomes.TheNativeWellnessAssessment(NWA)isaninstrumentthatmeasureswellness.WeneedtoknowwhatwellnessisachievedamongFirstNationsinadditiontothenumberofoverdoses,ratesofneonatalabstinencesyndrome,childrenplacedinchild-welfareduetoaddictions,andtheincreaseinaccesstoopioidagonisttherapies.Thisinstrumentmeasureswellnessashope,belonging,meaningandpurposeusingindigenousculture.ThedevelopmentofcapacitywithinFirstNationscommunitiestomeasureHopeBelongingMeaningandPurposeisrequired.
b. Weneedcapacitytosupportimplementationofanationalprescriptiondrugusesurveycurrentlyindevelopment.ThissurveyisstructuredinmodulessothatFNcommunitiescanchoosethedatatheyneedandthesurveywillbeavailableinanationaldatabaseforFirstNationsaddictionsandmentalwellness.FundingisrequiredtoimplementthissurveywhichwillprovideuswithanecessaryresourcetomeasurechangeovertimeontheimplementationoftheOpioidActionPlan.
c. AnationaladdictionsinformationmanagementsystemhasbeendevelopedandimplementedamongtheNationalNativeAlcoholandDrugAbuseprogramandtheNationalYouthSolventAbuseProgram.Fundingisrequiredtoenhancethisnationaldatabaseforincreasedcommunityaccessandtosupportrelevantdatasharingbetweensystemsforamorecomprehensiveanalysisofthechangewecanachieveinaddressingopioidmisuse.
d. Opioidsurveillanceprogramsarerequired.Forexample,supportisrequiredforFirstNationsinOntariobyprovidingacomprehensivepictureandbaselinedataonopiateprescriptiontrendsfortheeffectiveplanningofappropriateservicesandsupportsforaffectedcommunities.
e. Dooleyet.al(Dooley,2016)demonstratedpositiveresultsforinfantswhosemotherswereinopioidagonisttreatmentusingBuprenorphine-naloxone.Furtherresearchisneededtoexploresthelong-termimpactofmethadoneandbuprenorphine-naloxoneinuteroonFirstNationschildren’smentalwellnessisneeded.

5
FirstNationspeopleinCanadahavedemonstratedmeaningfulsolutionstotheopioidcrisis,wenowneedsupporttobuildcapacitytoeffectchangeanddelivermeaningfuldatathattellsthestoryofthedifferencewecanmake.

OVERVIEWOFFENTANYLBriefforAFN
October17,2016
AbstractThisdocumentprovidesabriefoverviewoffentanylandoutlinescurrentstrategiestoaddress
theissue.ItconcludeswithabroaderissueandthatisthatFirstNationsgovernmentsarechallengedwithaccesstoresourcestosupporttreatmentforopioidaddiction,andaccessto
naloxoneasonemethodforpreventingoverdoseforfentanyl.Therearemanymoresystemicissuesthatarenotaddressedinthisbriefing,includingfundingtosupportcommunitybased
opioidtreatment,consistentprogramsforpreventionaimedatwomenofchildbearingyears,increasedcommitmenttowardseffectivetreatmentthatfocusesonpreservationofamothers
righttoparentwhileengagedintreatmentforopioiddependence.

1|P a g e
OverviewofFentanyl
Canadaisnowthehighestpercapitaconsumerofopioidsintheworld,1andOntariohasthehighestrateofprescriptionopioiduseinthecountry.2
Fentanylisasyntheticopioid(narcotic)thatis50to100timesmoretoxicthanotherdrugssuchasmorphineand50timesmorepowerfulthanheroin.Illicitfentanylcanbefoundinliquid,powderandpillform.3MostillicitfentanyloriginatesfromlabsinChina,whichcopychemicalformulasfrompatentsfiledbypharmaceuticalcompanies.DrugtraffickerscanalsoimportthechemicalW-18oritsanalogs,whicharen'tcurrentlyillegal,despitetheirabilitytocauseasimilaropiateeffecttofentanyl.Eitherway,drugtraffickerswillthenusepharmaceutical-gradeequipmenttopressandcoatthechemicalstocreatetheirfakeoxycodonepills.ThepharmaceuticalcompanythatmanufacturesoxycodoneinCanadachangeditsformulaanditsstampbecauseofillicitmarketingwhichmeansthateverypillstampedwithCDN80actuallycontainsfentanyl.Alethaldoseoffentanyl—justtwomilligrams—isnearlytoosmalltosee,andcanbeabsorbedthroughtheskinandcanbelethal.4Fentanylisreportedbypolicetobemixedwithotherdrugssuchascocaine5andis commonlycutintootherstreetdrugs—includingheroin,oxycontinandmethamphetamine—tomakethemmorepotent.6
Inrecentyears’fentanylpopularitygrewduetothescarcityofanotheropiatebasedpainkiller,Oxycodone.Variationsinfentanylhaveincreasedinnumberandpotencyoverthelastyear,alongwithnon-fentanylopioidslikeW-18thathaveemerged,andwillcontinuetogrowforthenext12to18monthsaccordingtoaRCMPreport.“Whilefentanylcontinuestoposeahigh-levelthreat,theillicitopioidmarketwritlargeisevolvingatanalarmingrateandsignificantlyraisingtherisk/threatlevel.”Thereportsaysthatmeasureslikeincreasingaccesstonaloxone,increasedopioidreportingandearly-warningsystemswillhelpstemtheincreaseinfentanyldistribution,butwon’tstopthemarketforthedrugfromincreasing.7
Carfentanil,isanewsyntheticdruggroupedwithheroin,fentanyl,andoxycodone.Whatisknownasthe“superdrug”isheroinlacedwithelephanttranquilizers,and100timesmorepotentthanfentanyl.8
1PatentedMedicinePricesReviewBoard(2014).UtilizationofprescriptionopioidsinCanada'spublicdrugplans,2006/07to2012/13.Retrievedfromhttp://www.pmprb-cepmb.gc.ca/view.asp?ccid=1033#overview2UnitedNationsOfficeonDrugsandCrime(2014).WorldDrugReport2014.https://www.unodc.org/documents/wdr2014/World_Drug_Report_2014_web.pdf3BCRCMPWarningAboutRecentDrugOverdoses.May19,2015http://bc.rcmp-grc.gc.ca/ViewPage.action?siteNodeId=2130&languageId=1&contentId=420354RCMPreport.June24,2016.http://www.rcmp-grc.gc.ca/en/gazette/were-dead5OttawaPolicefindfentanylmixedinseizedcocaine.CBCNews.Oct.13,2016http://www.cbc.ca/news/canada/ottawa/fentanyl-in-cocaine-ottawa-police-1.38039366HealthCanadaCrackingDownonFentanylChemicals.Aug31,2016.http://www.cbc.ca/news/canada/british-columbia/health-canada-cracking-down-fentanyl-chemicals-1.37430847FentanylinCanadawillgetworsebeforeitgetsbetter:RCMPreport.ByTaniaKohutandRebeccaJosephGlobalNews.http://globalnews.ca/news/2960798/fentanyl-in-canada-will-get-worse-before-it-gets-better-rcmp-report/.Sept.24,20168Whatiscarfentanil.DeadlystreetdrugiscausingmassoverdosesintheUS.Sept.14,2016http://globalnews.ca/news/2939935/what-is-carfentanil-deadly-street-drug-is-causing-mass-overdoses-in-the-us/
2|P a g e
Legitimateuseoffentanylhasnotbeenwithoutconcerns.Accordingtoone2003study,fentanylpatchesareusedbypatientsinamannerthatisinconsistentwiththestandardrecommendationinthemanufacturers'PIbutitwasstillnotaspronouncedaswasoxycodoneHClcontrolled-release.9Fentanylisprescribedaspatchesforchronicpain.ApproachestoAddressingPublicHealthEmergency:Overdose
LastApril,apublichealthemergencywasdeclaredinB.C.becauseoftheoverdosespikeandtheincreaseoffenantyl.“FromJanuarytoJune,therehasbeena74percentincreaseinfentanyldeaths,”saidClark.“Thatis371liveslost.”inBC.10TheBCgovernmentestablishedataskforcewiththepurposeto:
A. establishatestingserviceforpeopletodetermineifdrugscontainfentanyl.B. ItwillalsocallontheFederalGovernmenttohelprestrictaccesstopillpressesand
tabletmachines,aswellastheopeningofmoresupervisedconsumptionorinjectionsights.
C. ThegovernmentwouldalsoliketoseeescalatingchargesfortheimportationandtraffickingoffentanylandwillrequestthatCanadaBorderServicesAgencyhastherighttoolstokeepillicitopioidsfromreachingB.C.streets.
BillS-225isinits3rdreadingandisaimedatmaking6chemicalsusedintheproductionoffentanylillegal.These6chemicalswerepreviouslyunregulatedbutnowwillfallundertheControlledDrugsandSubstancesAct.HealthCanadaalsoannouncedan“OpioidActionPlan”inJuneof2016:
1. BetterinformingCanadiansabouttherisksofopioids:newwarningstickers,patientinformationsheets,reviewofbestpractices
2. Supportingbetterprescribingpractices:promoteprescriptionmonitoringprograms,examinepharmacyrecords,shareinformationwithPTlicensingbodies,CanadaHealthInfowaye-prescribingsolution
3. Reducingeasyaccesstounnecessaryopioids:contraindicationsforapprovedopioids,requiringaprescriptionforlow-dosecodeineproducts,mandatoryriskmanagementplansforcertainopioids
4. Supportingbettertreatmentoptionsforpatients:better&fasteraccesstonaloxone,expeditingthereviewofnon-opioidpainrelievers,re-examiningspecialrequirementsformethadone
5. Improvingtheevidencebase:bringingtogetherexpertsinthefieldtodiscusshowtoimprovedatacollectionandtheCanadianevidencebase
9Patient-ReportedUtilizationPatternsofFentanylTransdermalSystemandOxycodoneHydrochlorideControlled-ReleaseAmongPatientsWithChronicNonmalignantPain.STACEYJ.ACKERMAN,MSE,PhD;MARGARETMORDIN,MS;JOSEPHREBLANDO,MPH;XIAOXU,PhD;JEFFSCHEIN,DRPh,MPh;SUEVALLOW,MBA,MA;andMICHAELBRENNAN,MD.www.amcp.orgVol.9,No.3May/June2003JMCPJournalofManagedCarePharmacy10B.C.Governmenttotacklecrisisoffentanyldrugoverdosedeaths.ByAmyJudd.OnlineNews,ProducerGlobalNews.http://globalnews.ca/news/2851474/b-c-government-to-tackle-crisis-of-fentanyl-drug-overdose-deaths/July27,2016
3|P a g e
AlthoughaccesstoNaloxonetopreventoverdoseisgrowing,itisnotwithoutlimitations.NaloxoneisnotpartofthepublicformularyeverywhereinCanada.Forexample,inNewfoundland,becausenaloxoneisnotpartofthepublicformulary,thegovernmentislookingforfundstoprovideasmanykitsaspossiblebutintheshorttermhascommittedtoatotalof24kitsinSt.JohnsbyChristmasandnotesthecostas35$perkit!11Inotherprovinces,naloxonewasoriginallyprovidedtoparamedicsandspecifichealthcareprovidersbutthisstrategyhasnotgonefarenoughtoreachvulnerablepopulationsathighriskforoverdose.Someprovinces,suchasOntario,12arecontemplatingwaystomakeNaloxoneandnaloxoneeducationmorewidelyavailable,forfreeandwithoutprescriptionatallpharmaciesalongwithexpandingdistributionmorebroadlythroughavarietyofhealth,socialandjusticesettings.
WhileNaloxonerequiresaprescription,theBCgovernmentexpectedthatthelifesavingdrugwouldbecomederegulated,alsomakingitmorewidelyavailable.TheMinisterofHealthforManitobahasindicatedthatthedistributionofnaloxonehastobeimproveddespiteensuringnaloxoneiscarriedbypolice,firedepartments,andsomepilotsitesaroundthecity.13Fentanylismakingitswayintocontrolledenvironmentssuchasjails/remandcentersandprovincialhealthauthoritiesarereportingtheuseofnaloxonetopreventoverdose.14Therearealsoreportedconcernsbyaddictionsspecialiststhatopioidmisuseisnotadequatelyassessedoraddressedthroughtreatmentforpeopleenteringjails/remandcenterswhichalsoincreasesriskforpeopleinwithdrawalandforaccessingillicitdrugs.Thisisespeciallyconcerninggiventhatindigenouspeoplemakeupatleast25%ofthoseincarcerated.
Thereisgrowingevidencethatonedoseofnaloxonewillnotworkinallsituationsoffentanyloverdosebecauseofthevaryinggradesoffentanyl.Mostnaloxonekitsprovide2dosesandithasbeenreportedthatthe2dosesandeven4dosesarenotenoughontheirowntosavesomeonefromoverdose.15Thismeansthateducationontheuseofnaloxonehasincludedwarningmessagestoseekmedicalattentionimmediatelyfollowingtheadministrationofnaloxone.Furtheremphasisandeducationisrequired.
WhiletheDeclarationpassedattheApril2016UnitedNationsSpecialSessionontheWorldDrugproblempromotesahumanrightsapproachfordrugrelatedissuesthroughthe“righttohealthcareincludingpreventionandtreatment”overthelongstandingparadigmof“warondrugs”thatcriminalizedpeoplefordrugrelatedissuesmorethanitsolvedtheworlddrugproblem,thecourtsinCanadaarewrestlingwithappropriatesentencingforfentanylrelatedcrimes.InCanada,drugcasesinvolvingfentanylhaveseenjudgesweighwhetherthepresenceoffentanyl–adruginthesamecategoryasheroinandcocaine–increasestheseverityorculpabilityofacriminalact,suchas
11SaintJohnlookstobringfentanylantidotenaloxonetocommunity.ByAndrewCromwellVideoJournalistGlobalNews.http://globalnews.ca/news/2998863/saint-john-looks-to-bring-fentanyl-antidote-naloxone-to-community/Oct13,201612MethadoneTreatmentServicesAdvisoryCommittee.June2016.MinistryofHealthandLongTermCareOntario.13 Naloxonedistribution'notadequate'inManitoba,healthministersays.Oct.13,2016http://www.cbc.ca/news/canada/manitoba/naloxone-manitoba-goertzen-1.3802953?cmp=rss14DeathsatEdmontonRemandCenterRaiseFearsofFentanylOverdoseAmongInmates.Oct.13,2016https://ca.news.yahoo.com/deaths-edmonton-remand-centre-raise-211636719.html15Fentanyltoopotentforoverdosekits.Oct.13,2016.http://ottawacitizen.com/news/local-news/fentanyl-too-potent-for-overdose-kits

4|P a g e
trafficking,inlightoftherecentsurgeinfentanyl-relateddeaths.Whileparliamentprescribeswhattodoaboutdrugtraffickingitissilentonassessingtheconsequencesofsellingfentanylordrugscontainingfentanyl.16Someprovincialjudgesareencouragingthatsentencesbebasedontheconsequencesforsellingfentanylandfentanylproductstomatchtheimpactofoverdosescausedbysuchdrugs.AnOntariocourtjudgedrecentlysentencedamanto10yearsinprisonforsellingfentanylandwillserve6yearsofthissentence.Thissentenceisreflectiveoftraffickingandforgingdocumentstogainaccesstofentanyl.Thissentencedoesnotconsidertheconsequencesforsellingfentanyl.
AccesstonaloxonewillbeakeyconversationamonghealthministersinOctober2016.
ProvincialgovernmentsareintheprocessofdevelopingstrategiestoaddresstheopioidcrisisbyfocusingeffortsonaddressingtheHealthCanada’s5-pointOpioidActionPlan.Somefirstnationshavealsodevelopedplansandresponses,suchasAlbertaMentalHealthandAddictionscommittee.TheChiefsofOntarioTakeaStandReporthasbeenusedasthefoundationforOntarioFirstNationandsomeAlbertaFirstNationcommunityplans.FirstNationPDAcommitteesinManitobaandSaskatchewanareworkingtogetherwithprovincialcollegesoffamilyphysiciansandcoronerstodevelopastrategicplanforaddressingopioidissues.Thesearebroadbasedinitiativestoaddressopioidissuesmorebroadly.
Conclusion
AddressingthefentanylcrisishasbeenchallengingforFirstNationscommunitiesespeciallyingainingaccesstonaloxone.Thisisrepresentativeofanoverallissuerelatedtoopioidmisusegenerally,andthatis,primarilywithhavingconsistentaccesstotreatmentandcapacityofFirstNationsgovernmentstoensureeffectiveprevention,healthpromotionandeducationrelatedtoopioidswithinthecontextinsocialinequality,intergenerationaltraumaandpoverty.
Fentanyllikeotheropioidshaveahistoryofnotbeingusedaccordingtomanufacturersspecificationandinoverprescribing.IllicitfentanylisabiggerissueanditsanissuethatrequiresthefederalgovernmenttoensurethatFirstNationsgovernmentshavesupportandcapacityforthe“OpioidActionPlan”.Inadditiontothis5pointplan,FirstNationsalsohaveotherneedsrelatedtoopioidmisuseandthesearearticulatedintheactionplansubmittedtothePrescriptionDrugAbuseCoordinatingCommittee(attachedhereasanappendix).
Someoftheshorttermandimmediateneedsrelatedtoopioidsmoregenerallyareasfollows:
1. Educationandsupportforcommunitybasedharmreductionisrequired,firstlybyensuringnaloxoneisimmediatelyandbroadlyavailablewithinFirstNationscommunitiestoallthosewhocanbenefitfromitandsecondly,byensuringfirstnationscommunitiesareprovidednecessaryresourcestoexploreculturallyrelevantstrategiesforreducingharmsofopioidmisuse.
2. Thatacommitmenttofundingcommunitybasedopioidagonisttreatmentprogramsbeassessedandincorporatedintocommunityhealthenvelopes,andfurtherthatNNADAPand
16Legalsystemadaptingtoriseoffentanylrelateddrugoffences.Oct11,2016http://www.theglobeandmail.com/news/british-columbia/legal-system-adapting-to-rise-of-fentanyl-related-drug-offences/article32325979/?cmpid=rss1&click=sf_globe

5|P a g e
NYSAPtreatmentcentersbesupportedforbuildingcapacityformanagingclientsalreadyparticipatinginopioidagonisttreatment.
3. Thatacommitmenttofundingcommunitybasedopioidpreventionprogramsthatsupportwomenofchildbearingyearsbeestablished.
4. Thatacommitmenttofundingcommunitybased,culturalbasedprogrammingformothersandinfantswhohaveexperienceneonatalabstinencesyndromebeestablished.
5. ThatthepriorityactionssubmittedtoPDACforthemanagementofPDAbeadoptedandthatadetailedbudgetandplanforaccomplishingsamebedevelopedandimplemented.
6|P a g e
APPENDIXA:ThunderbirdPartnershipFoundation:PDAPriorityActions
(SubmittedtoPDACC,May2016.Preparedby:MaeKattLPN,Dr.SharonCirone,Dr.ClaudetteChaseandCarolHopkins)
PrioritiesforAction1. GovernanceandCoordinationofCaremustsupportFirstNationsgovernanceofservices.
} StronggovernanceandcoordinationamongandwithinsystemsarevitaltodevelopingandmaintainingculturallyresponsivecareinaFirstNationscommunity.
} Keycomponentsthatsupportboththegovernanceandcoordinationofsystemsinclude:
•Community-drivenaddictionservices;
•Inter-jurisdictionalrelationshipsandcollaboration;
•Systemlevelpartnershipsandlinkages.
(HonouringOurStrengths:ARenewedFrameworktoAddressSubstanceUseAmongFirstNationsinCanada,p72)
2. FirstNationshealthcareprovidersandaddictionmedicineinstitutionsshoulddevelopanon-linetrainingcourseandlongdistanceclinicalsupportsystemonbuprenorphineforprimarycarephysiciansworkinginFirstNationscommunities.} Thereareanumberofphysicians,nursepractitionersandnursesinSiouxLookoutwith
manyyearsofexperienceinprescribinganddispensingbuprenorphineinFirstNationscommunities.
} Thesepractitionersarecapableofdeliveringtrainingandclinicalsupportthroughalong-distancementorshipnetwork.
3. Wheninvitedtodoso,addictionphysiciansshouldbesupportedtoassistinbuprenorphinetreatmentinFirstNationcommunitybasedprograms.
} Currently,agroupofaddictionphysiciansfromTorontoandSudburyregularlyflytoisolatedSiouxLookoutcommunitiestodobuprenorphineinductions.
} Supportisnecessarybecausefamilyphysicianssimplydonothavethetimeforbuprenorphineinductionsduringtheirfly-invisits.
} TheprogramisfundedbytheCPSO,whichcoverstravelcostsfromTorontotoThunderBay,andbytheSiouxLookoutRegionalHealthAuthority,whichprovidesdailystipendsfortheaddictionphysicians).
4. Nursepractitionersshouldbeallowedtoprescribebuprenorphine.} Currently,manynursepractitionersworkinisolatedruralandnortherncommunities
withveryhighratesofaddictionandlimitedaccesstoaddictionphysicians.} Buprenorphineismuchsaferthanmethadoneorotherpotentopioids.} PermittingNPstoprescribebuprenorphinewillsignificantlyenhancetreatmentcapacity
inthenorth.

7|P a g e
5. NIHBandFNIH,HealthCanadaneedstoensuresustainable,stableoperationalfundingforPrescriptionDrugAbuse(PDA)programs,includingtreatmentwithbuprenorphine,addictionsrecovery,relapsepreventioncounselling,cultureandlandbasedprogramming.
} Currently,HealthCanadalimitsthenumberofdays,perpatientthatnursesmaybeinvolvedinbuprenorphinedispensingtolessthanonemonth
} HealthCanadafundingforcommunitybasedPDAprogramswasrecentlytransitionedfromoneyeargrantstothreeyeargrantcycles.
} Sustainableprogramfundingisrequiredtobuildsustainableprogramsforcomplexchronicillnesses,suchasprescriptiondrugaddiction.
6. HealthCanadashouldprovidetrainingandsupportforrecoveryfromintergenerational/HistoricalTraumaandPTSD.Thereshouldbefundedsupportfor:
} WellnessretreatsforChiefandCouncilleadership(arequestforfundinghascomedirectlyfromGrandChiefIsadoreDay);
} TrainingofPrescriptionDrugAbuseprogramworkersinTraumaInformedCare;and} Aftercareprogramsthatsupportindividual,familyandcommunityhealingfromPTSD
andHistoricalTraumaTransmission.} PrescriptionDrugAbuseandotheraddictionsbeforethisrecentepidemic,including
alcoholusedisorders,areasymptomofunderlyingissues,sorrowandpain.7. Indigenouscommunitiesshouldbeofferedsupportinestablishinglocal,community-based
treatmentprograms.} Buprenorphineisemergingasaneffectiveandfeasiblealternativetomethadone
treatmentinindigenouscommunities.} AccordingtoregulationsoftheNon-InsuredHealthBenefitsprogram,physicians
requestingbuprenorphineforFirstNationspatientsmustconfirmthatbuprenorphinewillbedispensedthroughacommunitytreatmentprogramthatisabletostorebuprenorphineinasecurelocation.
} Thisensuresthatpatientsreceiveappropriatecounsellingandsupport,andthatsafeandstandardprescribinganddispensingprotocolsareinplace.
} IntheSiouxLookoutarea,approximately1500patientslivinginremoteFirstNationscommunitieshavebeentreatedincommunity-basedbuprenorphinetreatmentprograms,withstrongsupportfromthecommunities’leaders.
} Buprenorphinetreatmentisinitiatedeitherbythecommunity’sprimarycarephysicianorbyurbanaddictionphysiciansthroughtelemedicineorfly-inlocums.
} Theprimarycarephysiciancontinuesprescribingoncethepatientisstable.} Buprenorphineisdispenseddailyundertheobservationofnurses,nursepractitioners
orcommunityworkers.} Eachofthesecommunitieshasestablishedarecoveryprogramthatinvolvescommunity
mentalhealthworkerswhoprovidebothconventionalcounsellingandculturallyappropriate,traditionalhealingpractices.
i. Thiscomprehensiveapproachhasenabledmanypatientstostoptheiropioiduseandreturntowork,schoolandfamily.
ii. Kanateandcolleagues(2015),documentedremarkableresultsforabuprenorphineprograminNorthCaribouLakeFirstNation.

8|P a g e
iii. Ayearafterprograminitiation,criminalchargesandMedevactransfersdecreased,theneedledistributionprogramdispensedlessthanhalfitspreviousvolumeandratesofschoolattendanceincreased.
References:
1. Kanate,D.Folk,D.,Cirone,S.,Gordon,J.,Kirlew,M.,Veale,T.,Bocking,N.,Rea,S.,&Kelly,L.(2015).Community-widemeasuresofwellnessinaremoteFirstNationscommunityexperiencingopioiddependence.Evaluatingoutpatientbuprenorphine-naloxonesubstitutiontherapyinthecontextofaFirstNationshealingprogram.CanFamPhys,61(2):160-165.
2. WorldHealthOrganization.Dept.ofMentalHealth,SubstanceAbuse,WorldHealthOrganization,InternationalNarcoticsControlBoard,UnitedNationsOfficeonDrugs,&Crime(2009).Guidelinesforthepsychosociallyassistedpharmacologicaltreatmentofopioiddependence.
8. FirstNationspatientslivingonreservewhoareattendingoffreserveOpioidSubstitutionPrograms,shouldbeofferedtoentercommunitybasedPDArecoveryprograms.AllpatientsrequestingtoreturntoorenterPDAprogramsintheircommunitiesshouldbesupportedtotransitionfromMethadoneMaintenanceTreatment(MMT)tobuprenorphine.ThecollegeofphysicianandsurgeonsshouldencourageallMMTproviderstosupporttransitiontobuprenorphineprescribingwhererequested,byFirstNationspatients.
Patientchoiceshouldbesupported,patient-centredcareshouldbemandated.
} ManyFirstNationspatientsonMMTfacesignificantbarrierseithertravellingtotheirhomecommunitiesorreturningtoliveintheircommunitiesbecauseofmaintenanceonmethadone.
i. SomepatientsreportencounteringresistancefromMMTproviderstotransitiontobuprenorphineprescribing.
} Manycommunitiesarefinanciallysupportingexpensivetransportationfortheircommunitymemberstotravelfromthecommunitytooffreserve‘methadoneclinics’andpharmacies.
i. TheFirstNationsthatdevelopandmaintaincommunitybasedprogramscanrepatriatetheircommunitymemberstotheirownbuprenorphineprescribingprograms.
9. Youthshouldhaveaccesstoservicesspecifictotheirdevelopmentalneeds.} Thereareveryfewprovidersofaddictiontreatmentservicesandspecificallymedical
treatmentofOpioidUseDisorderswhoprovideyouthspecificservices,orattheveryleastintegrateservicesadaptedtotheneedsofyoungpeople.
} Youngpeople,uptotheageof25,havechallengesuniquetotheadultpopulation.o “thehumanbraindoesnotreachfullmaturityuntilatleastthemid-20s…”

9|P a g e
} Themajorityofyoungpeoplewithsubstanceusedisordershaveconcurrentmentalhealthissues,suchasanxietyandmooddisorders.
} Homeless,streetinvolvedandmarginalizedyouthoftenhavecomplexpsychologicalandsocialissues.
} Twoexcellentexamplesofservicesadaptedtotheneedsofyouthare:o SchoolbasedprogramatDennisFranklynCromartyHighSchoolinThunderBayo TheBreakawayTorontoOpiateSupportTeam
10. FamilyPhysicians,NursePractitioners,andanyothercliniciansprovidingOpioidSubstitution
Therapyshouldbeprescribingbuprenorphine/naloxoneandhaveaccesstoeducationinprovidingyouthspecificservices.
} YouthoftendonotseekservicesthroughtheirFamilyPhysiciansorotherhealthcareprovidersbecausethey:
} haveconcernsaboutconfidentialityorstigmatization;} donothaveaprimarycareproviderorhavelostcontactwiththeirusualprovider;and} areoftennotawareoftreatmentoptions.} FamilyPhysiciansandotherprovidersoftendonotfeelconfidentprovidingclinicalcare
toadolescentsandyouthwithalcoholandsubstanceusedisordersandtheconcurrentmentalhealthdisorders.
} Manyprimarycareprovidersworkinenvironmentsthatdonotpurposefullyprovideyouthspecificservices.
11. Anyadolescentoryoungperson,particularlythoseunder25yearsofage,especiallywhosehomecommunityisaFirstNation,seekingcareforOpioidUseDisorders,shouldbeofferedafullrangeoftreatmentoptions,includingabstinencebasedtreatmentand/orOpioidSubstitutionTherapy.AllthoseconsentingtoOpioidSubstitutionTherapyshouldbecounselledintheexpectationsofdurationoftreatment,andbeofferedtheopportunitytotaperdownandoffofOST,throughoutthecourseoftreatment.TheadvantagesofbuprenorphineversusmethadoneforOSTinyoungpeopleshouldbediscussed.
} Thereareanincreasingnumberofclinicaltrialsontreatmentinterventionsforadolescentsandyouthwithopioidusedisorders.
} Therearemanyinstanceshowever,wherepatientspreferbuprenorphine,wheretheirexpectationsoftreatmentorwheretheirlivingcircumstances,orgeographiclocationwouldsuggestthatbuprenorphineispreferableovermethadone.
} Manyyoungpeopleareconcernedaboutthelongdurationoftreatmentthatistypicalofmethadone,theyexpressconcernaboutsideeffects,includingsedationand/ortheyareworriedaboutthestigmaandregulationofmethadoneversusbuprenorphine.
} ThereisanecdotalevidenceandapharmacologicbasisforsupportingtheuseofbuprenorphineovermethadoneforpatientsanticipatingtaperingoffofanddiscontinuingOST.
} ManyyoungpeopleseekingtreatmentforPrescriptionDrugAbuse(PDA)havehadshorterdurationsofuse,withlessprogressiontohighriskuse(IVuse,highdoseuse,dailyuse).
} ItisagreatconcernwhenthedurationofOSTtreatmentisexponentiallylongerthanthedurationofillicitopioiduse.

10|P a g e
} AllyouthonOSTshouldbeofferedandsupportedineffortstotaperdownandoffofOST.
12. BuprenorphineshouldbedesignatedasfirstlineoftreatmentforAboriginalwomenwhoarepregnant.
} Womencanreturnhomemoreeasilytobewiththeirfamiliesandreceivesupportfromtheircommunities.
} Treatmenthasthesameoutcomesasothermonitoredopioidsforpregnantpatients.} Studiesshowlessintenseandshorterdurationofneonatalabstinencesyndrome(NAS)
withbuprenorphineovermethadone.13. Treatmenthastohaveagenderlens.
} Socialcontrolthroughsocialserviceagenciesandmedicalprovidersarepunitivedrugpoliciesandeffectwomenasdoubleandtriplepunishment.Isimpossibletoprotectchildrenbylockinguptheirmothersfortheirdruguseandit'simpossibletoensurethewellbeingofchildrenbydetachingthematbirthfromtheirmothers.
} Treatmentmustattendtotheneedsofwomenthroughtheprovisionofchildcare,removalofdisqualifyingcriteriaforpregnantwomen,supportbreastfeedingwomen,andmeettheneedsfortransgenderpopulations
} Treatmentformothersandtheirnewbornbabiesmustaccommodateaccesstohealthcarewhilegivingattentiontopoverty

160 Canadian Family Physician • Le Médecin de famille canadien | Vol 61: february • féVrier 2015
Research
Community-wide measures of wellness in a remote First Nations community experiencing opioid dependenceEvaluating outpatient buprenorphine-naloxone substitution therapy in the context of a First Nations healing programDinah Kanate David Folk MD CCFP Sharon Cirone MD CCFP Janet Gordon RN Mike Kirlew MD CCFP Terri Veale RN(EC) Natalie Bocking MD CCFP Sara Rea Len Kelly MD MClSc FCFP FRRM
AbstractObjective To document the development of unique opioid-dependence treatment in remote communities that combines First Nations healing strategies and substitution therapy with buprenorphine-naloxone.
Design Quantitative measurements of community wellness and response to community-based opioid- dependence treatment.
Setting Remote First Nations community in northwestern Ontario.
Participants A total of 140 self-referred opioid-dependent community members.
Intervention Community-developed program of First Nations healing, addiction treatment, and substitution therapy.
Main outcome measures Community-wide measures of wellness: number of criminal charges, addiction-related medical evacuations, child protection agency cases, school attendance, and attendance at community events.
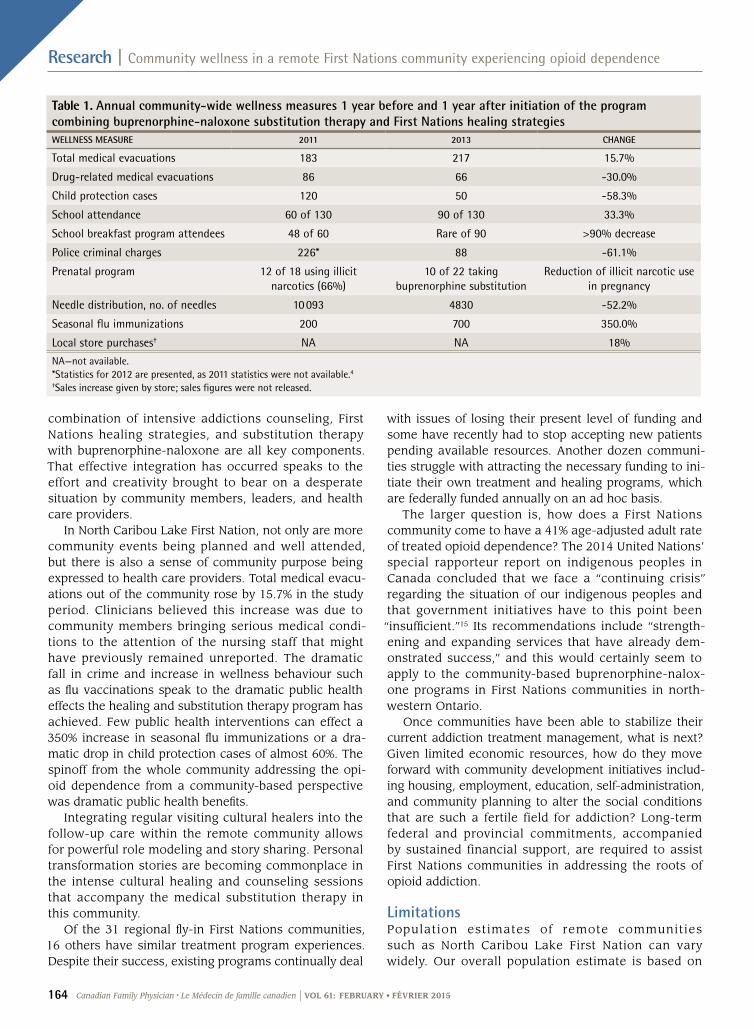
Results The age-adjusted adult rate of opioid-dependence treatment was 41%. One year after the development of the in-community healing and substitution therapy program for opioid dependence, police criminal charges had fallen by 61.1%, child protection cases had fallen by 58.3%, school attendance had increased by 33.3%, and seasonal influenza immunizations had dramatically gone up by 350.0%. Attendance at community events is now robust, and sales at the local general store have gone up almost 20%.
Conclusion Community-wide wellness measures have undergone dramatic public health changes since the development of a First Nations healing program involving opioid substitution therapy with buprenorphine-naloxone. Funding for such programs is ad hoc and temporary, and this threatens the survival of the described program and other such programs developing in this region, which has been strongly affected by an opioid-dependence epidemic.
EDITOR’S KEY POINTS• Opioid dependence has become a widespread issue in northwestern Ontario, particularly in remote First Nations communities, with some communities reporting prevalences of prescription opioid abuse between 35% and 50%.
• North Caribou Lake First Nation had an age-adjusted adult rate of treated opioid dependence of 41%. Opioid addiction affects the whole fabric of a community, so North Caribou Lake First Nation developed a community-based treatment program that combined substitution therapy and intensive, culturally appropriate counseling.
• The program has received strong community support, and considerable improvements in community-wide measures of wellness have been documented, including decreases in child protection cases, criminal charges, and drug-related medical evacuations, and increases in school attendance, participation in community events and vaccination programs, and spending at the local store.
This article has been peer reviewed. Can Fam Physician 2015;61:160-5

Vol 61: february • féVrier 2015 | Canadian Family Physician • Le Médecin de famille canadien 161
Recherche
Évaluation des indices de mieux-être pour la communauté d’un village éloigné des Premières Nations aux prises avec la dépendance aux opiacésÉvaluation d’un traitement de substitution à la buprénorphine-naxolone dans le contexte d’un programme de guérison des Premières NationsDinah Kanate David Folk MD CCFP Sharon Cirone MD CCFP Janet Gordon RN Mike Kirlew MD CCFP Terri Veale RN(EC) Natalie Bocking MD CCFP Sara Rea Len Kelly MD MClSc FCFP FRRM
RésuméObjectif Documenter le développement d’un traitement unique de la dépendance aux opiacés au sein de communautés éloignées à l’aide de stratégies de traitement propres aux Premières Nations, combinées à un traitement de substitution à la buprénorphine-naxolone.
Type d’étude On a fait une mesure quantitative du niveau de mieux-être dans la communauté et de la réponse au traitement propre à la communauté pour la dépendance aux opiacés.
Contexte Une communauté éloignée des Premières Nations, dans le nord-ouest de l’Ontario.
Participants Un total de 140 membres de la communauté souffrant de dépendance aux opiacés ont choisi de participer.
Intervention Un programme de guérison des Premières Nations développé au sein de la communauté, un traitement de la dépendance et un traitement de substitution.
Principaux paramètres à l’étude Des indices de mesure du bien-être pour l’ensemble de la communauté, soient le nombre d’accusations criminelles, les évacuations médicales liées à la dépendance, les cas de protection de l’enfance, l’assiduité à l’école et la présence aux activités communautaires.
Résultats Le taux ajusté pour l’âge du traitement de la dépendance aux opiacés chez les adultes était de 41 %. Un an après la création du programme de guérison intra-communautaire et du programme de traitement de substitution pour la dépendance aux opiacés, les accusations criminelles des policiers avaient diminué de 61,1 % et les cas de protection de l’enfance de 58,3 %, l’assiduité à l’école avait augmenté de 33, 3 % alors que la vaccination saisonnière contre la grippe avait connu une augmentation dramatique de 350,0 %. La présence aux activités communautaires est maintenant considérable et les ventes au magasin général local ont augmenté de près de 20 %.
Conclusion Les indices de mesure du bien-être de la communauté ont connu des changements dramatiques sur le plan de la santé publique depuis l’instauration d’un programme de guérison des Premières Nations comprenant un traitement de substitution à la buprénorphine-naloxone pour la dépendance aux opiacés. Comme ce programme jouissait d’un financement ad hoc temporaire, il risque de ne pas survivre, à l’instar d’autres programmes semblables qui se développent dans une région aux prises avec une grave épidémie de dépendance aux opiacés.
POINTS DE REPèRE Du RéDacTEuR• La dépendance aux opiacés est devenue un problème dans l’ensemble du nord-ouest de l’Ontario, particulièrement dans les communautés éloignées des Premières Nations, certaines de ces communautés rapportant une prévalence de prescription d’opiacés atteignant 35 % et 50 %.
• La Première Nation de North Caribou Lake avait un taux ajusté en fonction de l’âge, pour les cas adultes de dépendance aux opiacés traités, de 41 %. La dépendance aux opiacés ébranle l’ensemble de la structure de la communauté, et c’est pourquoi ce village a développé un programme de traitement propre à la communauté qui combine un traitement de substitution et un counseling intensif culturellement approprié.
• Le programme a reçu un très bon appui de la communauté et on a observé des améliorations considérables dans les indices de mieux-être, tels qu’une diminution des cas liés à la protection de l’enfance, des accusations criminelles et des évacuations médicales liées à la drogue, mais aussi une diminution des absences à l’école, une meilleure participation aux activités communautaires et aux programmes de vaccination, et une augmentation des achats au magasin local.
Cet article a fait l’objet d’une révision par des pairs. Can Fam Physician 2015;61:160-5

162 Canadian Family Physician • Le Médecin de famille canadien | Vol 61: february • féVrier 2015
Research | Community wellness in a remote First Nations community experiencing opioid dependence
Opioid dependence has become a widespread issue in northwestern Ontario, particularly in remote First Nations communities. In 2009, the north-
western Ontario First Nations chiefs declared a state of emergency regarding “prescription drug abuse” related to the epidemic of abuse of long-acting oxycodone prep-arations.1 This was in response to mounting concerns about the social, health, and economic consequences of opioid abuse among many remote First Nations commu-nities: increasing crime, family dysfunction, unemploy-ment, and increasing rates of hepatitis C and neonatal abstinence syndrome.1
In Ontario between 1991 and 2007, the number of prescriptions for oxycodone increased by 850%.2 While the proportion of First Nations people in Ontario receiv-ing opioids through Non-Insured Health Benefits, the responsible federal medical insurance agency, remained steady between 1999 and 2009, the quantity and propor-tion of oxycodone dispensed increased substantially.3
Concurrent with opioid prescribing among First Nations patients,3 diversion of prescription opioids and trafficking of oxycodone products from larger centres appears to have played an important role in their avail-ability in First Nations communities.4 The 2008 to 2010 First Nations Regional Health Survey reported that 6.8% of Ontario on-reserve respondents used opioids with-out a prescription.5 However, community-led surveys in several Nishnawbe Aski Nation communities reported prevalences of prescription opioid abuse between 35% and 50%.6,7 In addition, a 3-fold increase in the number of aboriginal people (mostly First Nations) seeking treat-ment for addiction to prescription opioids in Ontario occurred from 2004 to 2009.8
Remote communities need and have developed unique solutions to address the crisis of opioid drug abuse. In northwestern Ontario, the relatively inaccessi-ble geography of remote First Nations communities lim-its travel for most of the population. Thirty-one remote First Nations communities, which vary in size from a few hundred to several thousand in population, are sit-uated across a vast area accessible primarily only by small planes. Primary care clinics are staffed by nurses and supported by regular fly-in or in-community family physicians. North Caribou Lake First Nation (estimated population 1100) is one such community, as its regional health care centre and the closest hospital are located in Sioux Lookout, Ont, which is a 1-hour flight away. In 2012, in response to the urgent need for a workable opioid-dependence program, the community leadership in conjunction with health care providers developed a unique buprenorphine-naloxone opioid substitution and maintenance program, including in-community after-care counseling by First Nations healers. A pilot project in a neighbouring community in 2012 had demonstrated the effectiveness and safety of buprenorphine-naloxone
for substitution therapy in this setting.9 This medication combines an opioid agonist (buprenorphine) with an opioid antagonist (naloxone) and resists diversion from its intended sublingual route. The naloxone compo-nent, which is inactivated by first-pass effect when taken mucosally, precipitates withdrawal if used intravenously.
Primary care settingsThe safety and efficacy of buprenorphine-naloxone induction in primary care settings (including “home” or unobserved inductions) is well established.10-14 In fact, primary care delivery of buprenorphine-naloxone programs have success rates similar (50%) to those of more resource-intensive clinical settings.10-14 Treating addicted patients in a primary care setting allows for more cost-effective delivery of medical services for concurrent illnesses, development of therapeutic relationships, and surveillance for addiction-related complications and infections.
The program in North Caribou Lake First Nation is unique in the scope of community participation in treat-ment and its remote setting, far from hospital services.
METHODS
Setting and participantsA written request for program evaluation was provided by the Chief and Band Council of North Caribou Lake First Nation. Ethics approval was granted by the Sioux Lookout Meno Ya Win Health Centre Research and Review and Ethics Committee. All program participants signed a narcotic treatment contract, and no individual patient information was used in this study.
Program descriptionAs of May 2014, 140 self-referred community mem-bers of North Caribou Lake First Nation in northwestern Ontario had participated in the outpatient healing and buprenorphine-naloxone substitution program since the first intake in July 2012; 8 groups of up to 20 partic-ipants went through the induction and maintenance program. All patients met the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, criteria for sub-stance dependence. Medication inductions (and sublin-gual administration) are undertaken in the community clinic by the visiting family physicians or addiction spe-cialists. Initially the program runs daily for each patient for 28 days and is managed by the community nurses and mental health workers. Following that initial month, buprenorphine-naloxone dispensing and daily follow-up is managed by community-trained health aides. First Nations counselors and healers deliver group and indi-vidual daily sessions several weeks per month during and after the month-long initiation of the program. They

Vol 61: february • féVrier 2015 | Canadian Family Physician • Le Médecin de famille canadien 163
Community wellness in a remote First Nations community experiencing opioid dependence | Research
focus on addiction recovery, relapse prevention, under-standing early-life trauma, grief counseling, and tra-ditional healing teachings. Land-based activities were used, along with individual and group education and counseling sessions.
Study designStatistics from community programs and health-related data were collected and compared for time peri-ods 1 year before and 1 year after the initiation of the buprenorphine-naloxone program. Community-wide measures that are routinely monitored by their respec-tive agencies were collected, as they could be easily fol-lowed for changes in incidence.
Main outcomesData on community-wellness measures were collected to assess the effectiveness of the program on the com-munity as a whole. The community-wellness measures included the number of emergency air ambulance med-ical evacuations out of the community, seasonal influ-enza immunization rate, number of child protection apprehensions, local community policing calls, num-ber of needles given out by the needle distribution pro-gram, school attendance rates, and sales at local stores. Personal observations of manifestations of commu-nity spirit were contributed by community and visiting health care professionals and local community mental health workers.
RESuLTS
The 140 patients enrolled in the opioid-dependence treatment program were all between 20 and 50 years of age. Using local medical record population statis-tics, this accounts for a 41% age-adjusted rate of adult community members in that age group receiving opioid- substitution therapy, including a rate of 48% for patients in their 20s.
Medical evacuations are emergency evacuations to hospital by paramedics in a fixed-wing aircraft (supplied by the provincial air ambulance service). Drug-related medical evacuations were grouped as the total of drug-related assaults, suicide attempts, overdoses, and sexual assaults believed to be directly related to drugs or addic-tion. This subset of medical evacuations fell by 30.0%, while the total number of medical evacuations rose by 15.7% (Table 1).4
In the year following program initiation, police crimi-nal charges fell by 61.1%, including a 94.1% drop in rob-bery and arson charges (from 17 in 2011 to 1 related charge in 2013). Young offender criminal or drug charges fell by 66.3%. The needle distribution program dispensed less than half its previous volume, and in
2013, 700 used needles were returned, a rare occurrence in earlier years. The nursing station noted that children and elderly patients were being brought in for medical care at earlier stages of illness. They also noticed that the community clinic became more of a primary care centre than a trauma centre, as they were now caring for less drug-related violence and its medical sequelae. School attendance had increased and most children now arrived having had breakfast at home.
Public support of the program is integrated into the community. The community leadership is strongly sup-portive and donated a building to house the program called New Horizons. Clients proudly wear T-shirts attest-ing to their participation both in the substitution program and in the ongoing aftercare counseling. The chief and band councilors take a keen interest in the success of the program and maintain supportive relationships with clients and the medical, nursing, clerical, and counsel-ing program staff. Accepted community health indicators, such as increased planning of and participation in com-munity events and activities for youth and elders, were also evident but not systematically measured. Both the pervasiveness of the issue and the positive, holistic com-munity response have served to lessen the stigma typi-cally associated with substance abuse, perhaps rendering it more amenable to treatment.
Community members strongly endorsed the program: “It has brought life back to our community, [which] is being restored to the way it used to be before everyone got stuck in addiction.” Practical benefits include more disposable income:
When I am on Facebook, I see a lot of people writ-ing that they are so happy they joined the program because now that they are not using, their cupboards always have food in [them] and they have money in their pockets and they can buy what they need for them or their children.
DIScuSSION
We have documented, for the first time, an accurate measure of the scope of the problem in one of our regional communities. The age-adjusted rate of 41% of the adult population participating in the treatment program gives credence to the regional chief’s 2009 description of an “epidemic” of opioid dependence.1 This figure informs the community-wide scope of the prob-lem occurring in northwestern Ontario.
Given the depth of the issue, the successful com-munity-based development of this opioid-dependence program is even more remarkable. North Caribou Lake First Nation is effectively dealing with the community-wide opioid abuse it has experienced. The novel
164 Canadian Family Physician • Le Médecin de famille canadien | Vol 61: february • féVrier 2015
Research | Community wellness in a remote First Nations community experiencing opioid dependence
combination of intensive addictions counseling, First Nations healing strategies, and substitution therapy with buprenorphine-naloxone are all key components. That effective integration has occurred speaks to the effort and creativity brought to bear on a desperate situation by community members, leaders, and health care providers.
In North Caribou Lake First Nation, not only are more community events being planned and well attended, but there is also a sense of community purpose being expressed to health care providers. Total medical evacu-ations out of the community rose by 15.7% in the study period. Clinicians believed this increase was due to community members bringing serious medical condi-tions to the attention of the nursing staff that might have previously remained unreported. The dramatic fall in crime and increase in wellness behaviour such as flu vaccinations speak to the dramatic public health effects the healing and substitution therapy program has achieved. Few public health interventions can effect a 350% increase in seasonal flu immunizations or a dra-matic drop in child protection cases of almost 60%. The spinoff from the whole community addressing the opi-oid dependence from a community-based perspective was dramatic public health benefits.
Integrating regular visiting cultural healers into the follow-up care within the remote community allows for powerful role modeling and story sharing. Personal transformation stories are becoming commonplace in the intense cultural healing and counseling sessions that accompany the medical substitution therapy in this community.
Of the 31 regional fly-in First Nations communities, 16 others have similar treatment program experiences. Despite their success, existing programs continually deal
with issues of losing their present level of funding and some have recently had to stop accepting new patients pending available resources. Another dozen communi-ties struggle with attracting the necessary funding to ini-tiate their own treatment and healing programs, which are federally funded annually on an ad hoc basis.
The larger question is, how does a First Nations community come to have a 41% age-adjusted adult rate of treated opioid dependence? The 2014 United Nations’ special rapporteur report on indigenous peoples in Canada concluded that we face a “continuing crisis” regarding the situation of our indigenous peoples and that government initiatives have to this point been “insufficient.”15 Its recommendations include “strength-ening and expanding services that have already dem-onstrated success,” and this would certainly seem to apply to the community-based buprenorphine-nalox-one programs in First Nations communities in north-western Ontario.
Once communities have been able to stabilize their current addiction treatment management, what is next? Given limited economic resources, how do they move forward with community development initiatives includ-ing housing, employment, education, self-administration, and community planning to alter the social conditions that are such a fertile field for addiction? Long-term federal and provincial commitments, accompanied by sustained financial support, are required to assist First Nations communities in addressing the roots of opioid addiction.
LimitationsPopulation estimates of remote communities such as North Caribou Lake First Nation can vary widely. Our overall population estimate is based on
Table 1. Annual community-wide wellness measures 1 year before and 1 year after initiation of the program combining buprenorphine-naloxone substitution therapy and First Nations healing strategiesWELLNESS MEASuRE 2011 2013 ChANGE
Total medical evacuations 183 217 15.7%
Drug-related medical evacuations 86 66 -30.0%
Child protection cases 120 50 -58.3%
School attendance 60 of 130 90 of 130 33.3%
School breakfast program attendees 48 of 60 Rare of 90 >90% decrease
Police criminal charges 226* 88 -61.1%
Prenatal program 12 of 18 using illicit narcotics (66%)
10 of 22 taking buprenorphine substitution
Reduction of illicit narcotic use in pregnancy
Needle distribution, no. of needles 10 093 4830 -52.2%
Seasonal flu immunizations 200 700 350.0%
Local store purchases† NA NA 18%
NA—not available.*Statistics for 2012 are presented, as 2011 statistics were not available.4†Sales increase given by store; sales figures were not released.

Vol 61: february • féVrier 2015 | Canadian Family Physician • Le Médecin de famille canadien 165
Community wellness in a remote First Nations community experiencing opioid dependence | Research
community-generated numbers used in recent fire evac-uation planning in 2011, as well as age ranges derived from community medical records.
Data were gathered as available and markers were chosen by community members and health care pro-viders that highlighted the most important changes experienced by community members and health care providers, as the community moved from crisis to sta-bility of addiction treatment. Future measures of com-munity wellness will need to proceed systematically and involve community-based indicators of wellness using more subtle indicators of health.16 Our study was not intentionally limited to 20- to 50-year-olds, that was the actual age range of present participants. Program retention rates and urine drug screening values are also being collected and will be available in the future.
Before-and-after studies are limited in their ability to infer causality; however, in the small isolated commu-nity of North Caribou Lake First Nation, there were no other such programs or economic or social changes in the community during the observed time frame.
ConclusionOpioid addiction affects the whole fabric of a commu-nity. The combination of substitution therapy and inten-sive, culturally appropriate counseling appears to be immensely effective.
Long-term funding is required to sustain these community-based health and social initiatives around addiction management. They are hallmarks of success in treating opioid dependence within communities. Ms Kanate is Chief of North Caribou Lake First Nation and oversees the New Horizon Program in Round Lake, Ont. Dr Folk is a regional physician in Sioux Lookout, Ont, and regularly visits the community in North Caribou Lake as a family physician. Dr Cirone is an addiction specialist at St Joseph’s Health Centre in Toronto, Ont, and visits the North Caribou Lake community regularly for addictions work. Ms Gordon is Director of Health Services at the Sioux Lookout First Nations Health Authority. Dr Kirlew is Assistant Professor at the Northern Ontario School of Medicine in Sioux Lookout. Ms Veale is a commu-nity nurse in Round Lake. Dr Bocking was a resident in community medicine at the University of Toronto at the time of the study. Ms Rea was a research intern at the Anishinaabe Bimaadiziwin Research Unit in Sioux Lookout at the time of the study. Dr Kelly is Professor at the Northern Ontario School of Medicine in Sioux Lookout.
acknowledgmentThis study was supported by the Northern Ontario Academic Medicine Association Clinical Innovation Opportunities Fund award.
ContributorsAll authors contributed to concept and design of the study; data gathering, analysis, and interpretation; and preparing the manuscript for submission.
Competing interestsNone declared
CorrespondenceDr Len Kelly, Northern Ontario School of Medicine, Division of Clinical Sciences, Box 489, Sioux Lookout, ON P8T 1A8; telephone 807 737-3803; fax 807 737-1771; e-mail [email protected]
references1. Nishnawbe Aski Nation. Resolution: 09/92. Prescription drug abuse state of
emergency. Thunder Bay, ON: Nishnawbe Aski Nation; 2009.2. Dhalla IA, Mamdani MM, Sivilotti ML, Kopp A, Qureshi O, Juurlink DN.
Prescribing of opioid analgesics and related mortality before and after the introduction of long-acting oxycodone. CMAJ 2009;181(12):891-6.
3. First Nations Inuit Health Branch. NIHB Ontario region prescription drug trends: a ten-year analysis. Ottawa, ON: Health Canada; 2010.
4. Nishnawbe-Aski Police Service. Annual report 2011/2012. Thunder Bay, ON: Nishnawbe-Aski Police Service; 2012. Available from: www.naps.ca/media/NAPS_2011_2012_Annual_Report.pdf. Accessed 2013 Jun 4.
5. First Nations Information Governance Centre. First Nations Regional Health Survey (RHS) 2008/10: national report on adults, youth and children living in First Nations communities. Ottawa, ON: Assembly of First Nations; 2012.
6. Chiefs of Ontario. Prescription drug abuse strategy: take a stand. Toronto, ON: Chiefs of Ontario; 2010.
7. Expert Working Group on Narcotic Addiction. The way forward: stewardship for prescription narcotics in Ontario. Toronto, ON: Ministry of Health and Long-Term Care; 2012.
8. Calverson R. Prescription opioid-related issues in northern Ontario: “from benefit to harm to crisis.” Toronto, ON: Centre for Addiction and Mental Health; 2010.
9. Katt M, Chase C, Samokhvalov AV, Argento E, Rehm J, Fischer B. Feasibility and outcomes of a community-based taper-to-low-dose-maintenance Suboxone treatment program for prescription opioid dependence in a remote First Nations community in northern Ontario. Int J Indigenous Health 2012;9(1):52-9.
10. Fudala PJ, Bridge TP, Herbert S, Willeford WO, Chiang CN, Jones K, et al. Office-based treatment of opiate addiction with a sublingual-tablet formula-tion of buprenorphine and naloxone. N Engl J Med 2003;349(10):949-58.
11. Mintzer IL, Eisenberg M, Terra M, MacVane C, Himmelstein DU, Woolhandler S. Treating opioid addiction with buprenorphine-naloxone in community-based primary care settings. Ann Fam Med 2007;5(2):146-50.
12. Lee JD, Grossman E, DiRocco D, Gourevitch MN. Home buprenorphine/ naloxone induction in primary care. J Gen Intern Med 2009;24(2):226-32.
13. Sohler NL, Li X, Kunins HV, Sacajiu G, Giovanniello A, Whitley S, et al. Home- versus office-based buprenorphine inductions for opioid-dependent patients. J Subst Abuse Treat 2010;38(2):153-9. Epub 2009 Oct 3.
14. Doolittle B, Becker W. A case series of buprenorphine/naloxone treatment in a primary care practice. Subst Abus 2011;32(4):262-5.
15. United Nations. Report of the special rapporteur on the rights of indige-nous peoples, James Anaya, on the situation of indigenous peoples in Canada. Geneva, Switz: United Nations; 2014. Available from: http://unsr. jamesanaya.org/docs/countries/2014-report-canada-a-hrc-27-52- add-2-en-auversion.pdf. Accessed 2014 May 29.
16. Jeffery B, Abonyi S, Hamilton C, Bird S, Denechezhe M, Lidguerre T, et al. Community health indicators toolkit. Regina, SK: University of Regina and University of Saskatchewan Saskatchewan Population Health and Evaluation Research Unit; 2006.

ReviewCMAJ CME
©2015 8872147 Canada Inc. or its licensors CMAJ, January 6, 2015, 187(1) E41
Nonmedical use of prescription opioids is a growing problem in Canada; in 2011, it had the highest per capita consump-
tion of oxycodone in the world.1 When a woman with opioid dependence becomes pregnant, ade-quate management of the addiction is of critical importance for the well-being of both mother and child. Untreated opioid addiction has been associated with risk-taking behaviour, preterm delivery, low birth weight and stillbirth.2,3 Ide-ally, antenatal care for women with opioid dependence is accomplished with multidisci-plinary care, including treatment of the addic-tion.4,5 However, women who live in rural and remote communities may not have access to such care or may have challenges accessing it.6
Comprehensive guidelines to manage the care of pregnant women with opioid dependence who live in rural or remote communities do not cur-rently exist. This absence, in addition to a lack of resources, a lack of training in the treatment of addiction in pregnancy and providers’ discom-fort with opiate substitution therapy in preg-nancy, has contributed to wide variations in the quality of care these women receive.
We evaluate strategies for the treatment of opioid dependency in pregnancy applicable to rural and remote settings, including methadone maintenance therapy, buprenorphine mainte-nance, slow-release morphine maintenance and opioid detoxification (Box 1).7 Special consider-ation is given to members of Canada’s Aborig inal population. Very little literature exists re garding the management of polysubstance use in pregnancy, and a full discussion of the issue is beyond the scope of this review.
What are the patterns of opioid dependence in rural and remote areas of Canada?
Statistics Canada defines a rural community as having less than 10 000 people, with less than 30% of the population commuting to a city of 100 000 people or more for work.8 However, the Canadian Medical Association defines rural as
areas in which physicians have high call require-ments, there are long distances to secondary and tertiary care centres, there is a lack of specialist care and there are insufficient health care providers.9
Given these differing definitions, the descrip-tions of pregnant women with opioid dependence who reside in these areas vary widely in terms of socioeconomic status, ethnic diversity and proxim-ity to urban resources.10 Heroin is the most com-monly reported opioid used by pregnant women living in rural and remote communities,2,10,11 but the nonmedical use of prescription opioids is increas-ing.10,11 Regardless of the opioid in use, treatment strategies for pregnant women in these communi-ties primarily involve methadone maintenance.2,3
What is the recommended treatment for opioid dependence during pregnancy?
The management of opioid dependence in preg-nancy in rural and remote settings requires spe-cial consideration (Boxes 2 and 3).
Methadone maintenance therapy is the gold standard for treating opioid dependence in pregnancy.12,13 Numerous studies have shown that, in pregnant women who use heroin, meth-adone is associated with more visits for ante-natal care, longer gestations, higher birth weights, lower rates of HIV infection, higher rates of infant discharge home in care of the mother and lower rates of relapse compared
The management of opioid dependence during pregnancy in rural and remote settings
Naana Afua Jumah MD DPhil, Lisa Graves MD, Meldon Kahan MD MHSc
Competing interests: Meldon Kahan has received nonfinancial support from Reckitt Benckiser. No other competing interests were declared.
This article has been peer reviewed.
Correspondence to: Naana Afua Jumah, [email protected]
CMAJ 2015. DOI:10.1503 /cmaj.131723
• Nonmedical use of prescription opioids during pregnancy is becoming more common, and members of Canada’s Aboriginal population are disproportionately affected.
• Methadone maintenance therapy has logistic limitations in rural and remote settings, but buprenorphine and slow-release morphine maintenance therapies are feasible alternatives.
• Opioid detoxification in pregnancy is associated with high rates of relapse and should only be offered if a comprehensive rehabilitation program is available.
• Treatment of opioid dependence and rehabilitation services should be provided to all women during pregnancy and the postpartum period.
Key points

Review
E42 CMAJ, January 6, 2015, 187(1)
with no treatment or detoxification.4,5
Methadone has important logistical limita-tions that prohibit its use in resource-limited locations. Methadone can only be prescribed by physicians who hold a special license.14 Because of the high risk of overdose at the start of treat-ment, methadone must be dispensed daily and ingested under the observation of a licensed pharmacist at a registered pharmacy.15 Because many rural and remote communities are unable to provide this service, methadone is not offered.
What are the alternatives to methadone maintenance therapy?
Observational studies have shown buprenorphine maintenance therapy to be a safe and efficacious alternative to methadone for the treatment of opi-oid dependence in pregnant women.16,17 Recent randomized controlled trials have shown that buprenorphine and methadone cause similar reductions in maternal opioid use and similar
birth and neonatal outcomes, and that buprenor-phine is associated with decreased severity of symptoms of neonatal abstinence syndrome.18,19 A case series describing 10 women who took buprenorphine plus naloxone maintenance ther-apy showed outcomes similar to those of buprenorphine alone.20
Buprenorphine is a partial μ-opioid receptor agonist that has a lower risk of fatal overdose than full μ-opioid agonists such as methadone. Buprenorphine may precipitate withdrawal if caution is not exercised at the start of treatment. The drug may also incompletely treat withdrawal symptoms, putting patients at risk for ongoing use of illicit drugs to manage their symptoms. Furthermore, buprenorphine may be less effec-tive than methadone at retaining patients in treat-ment if they used opioids intravenously.21,22 Unlike methadone, Health Canada does not require an exemption to prescribe buprenorphine; however, outside of Ontario and Quebec, public funding of buprenorphine is restricted to physi-cians with a methadone license.23
The buprenorphine formulation now includes naloxone, which is intended to deter misuse. Addiction literature often cites naloxone as a possible teratogen and warns against its use in pregnancy.24 However, the United States Food and Drug Administration classifies naloxone as a pregnancy category B drug, meaning that there have been no reports of teratogenicity in humans or animals.25 The greater concern in pregnant women with opioid dependence is naloxone’s ability to precipitate withdrawal if taken intra-venously or intranasally. Naloxone has minimal buccal or sublingual absorption.26,27 As pre-viously described, acute opioid withdrawal is associated with morbidity for both the woman and her fetus.
What if methadone and buprenorphine are not available?
Slow-release morphine maintenance therapy has been proposed as an alternative to methadone when the latter is not available.28 In resource-limited areas, slow-release morphine may be more accessible because a special license to prescribe it is not required, and it is readily available in pharmacies. Accessibility is also the most notable drawback of morphine because it is more easily acquired and diverted than methadone. In addition, morphine is more easily injected than methadone, and it cannot be distinguished from heroin in a urine screening, limiting the usefulness of urine screens during treatment.
We identified one prospective, randomized
Box 1: Evidence used in this review
We conducted a literature search of PubMed, Embase and JSTOR between July 2013 and September 2013 for the following terms: “pregnancy,” “pregnant,” “rural,” “remote,” “non-urban,” “nonurban,” “Aboriginal,” “Indigenous,” “First Nations,” “Inuit,” “opiate,” “opioid,” “methadone,” “buprenorphine,” “slow release,” “morphine,” “detoxification,” “taper” and “wean.” We did not limit our search to a specific period or language. In addition, we searched government and nongovernmental organization sources including Statistics Canada, Health Canada, First Nations and Inuit Health Branch, National Aboriginal Health Organization and Nishnawbe-Aski Nation. If an abstract was deemed to be relevant, the article was read in full. We reviewed the references in each article to identify additional relevant papers. The details of our search strategies and retrieved articles are available on request. We reported the quality of the evidence according to criteria set forth by the Canadian Task Force on Preventive Health Care.7
Box 2: Applying the results of this review in clinical practice
• Methadone maintenance therapy should be started for all women with opioid dependence in pregnancy (I-A).
• If methadone is not available, maintenance therapy should be started with buprenorphine (I-A).
• If methadone and buprenorphine are not available, maintenance therapy should be start with slow-release morphine (I-A).
• If a woman is already receiving buprenorphine plus naloxone maintenance therapy before pregnancy, she may continue to do so during pregnancy (II-2B) or change to buprenorphine alone if available (I-A).
• Detoxification should only be used at the patient’s request (II-2A). The patient should be counselled about the high failure rate of detoxification (II-2A), the risks of overdose with failure of detoxification and the option to start maintenance therapy at any point should she relapse (III-B).
• All pregnant women with opioid dependence should be offered maintenance therapy and rehabilitation services postpartum (III-B).
• Methadone, buprenorphine (Subutex), buprenorphine + naloxone (Suboxone) and slow-release morphine (Kadian) are all available in Canada.

Review
CMAJ, January 6, 2015, 187(1) E43
study that compared methadone with slow-release morphine maintenance that included 24 women in each arm.29 No difference in neo-natal outcomes, including neonatal abstinence syndrome, was seen between the two groups. Mothers taking slow-release morphine had a sig-nificant decrease in the use of benzodiazepines and other opiates. Two smaller observational studies showed that pregnant women taking slow-release morphine were significantly less likely to use benzodiazepines or additional opi-oids while undergoing treatment.30,31 A hypothe-sized advantage of morphine is a decreased dura-tion of neonatal abstinence syndrome owing to its shorter half-life compared with methadone.30
Is neonatal abstinence syndrome a problem?
Neonatal abstinence syndrome has not been associated with long-term neurodevelopmental harms in children, whereas ongoing maternal substance use is associated with poor develop-mental outcomes in children.32 The syndrome is time-limited as the infant withdraws from in utero exposure to an opioid. No association has been found between a mother’s methadone dose and the severity of symptoms of neonatal abstinence syndrome.33,34 Furthermore, pharma-codynamic studies show that escalations in dose are needed to maintain the therapeutic effect as pregnancy progresses owing to changes in meth-adone metabolism.35
Is there a role for detoxification in pregnancy?
An early observational study showed similar out-comes among pregnant women who used heroin and had undergone medical detoxification com-pared with a control group consisting of preg-nant women with no opioid dependency.36 How-ever, medical detoxification was deemed a failure because of its inability to provide durable abstinence. This study was contrasted by two early case reports documenting adverse preg-nancy outcomes in women undergoing acute heroin withdrawal rather than medically man-aged detoxification.37,38 This contrasting evi-dence led to a resurgence of interest in medical detoxification in pregnancy in the 1990s. Com-plete opioid detoxification was recommended in a 2002 publication, with the aim of eliminating neonatal abstinence syndrome.39
Among the five retrospective case series involving women with heroin addiction, there is
no consensus on the rate of methadone taper or the superiority of inpatient versus outpatient detoxification (Box 4).40–44 Although the litera-ture cites concerns for increased rates of mis-carriage with detoxification during the first tri-mester and increased rates of preterm labour with detoxification during the third trimes-ter,45,46 this effect was not shown.40,43 Neonatal outcomes, when reported, were inconsistent. In addition, maternal heroin use postpartum and ongoing addiction treatment postpartum were not reported.
We recommend that acute detoxification in pregnancy should be abandoned, given the evi-dence, with the exception of women who decline opioid substitution therapy. In this cir-cumstance, a woman should be given the oppor-tunity to transfer into an opioid substitution pro-gram at any time if she elects to do so or if she is unable to successfully taper off of opioids. Postpartum rehabilitation services must be pro-vided for all women, particularly those who have chosen abstinence.
How does opioid dependence in pregnancy affect rural or remote Aboriginal populations?
Canada’s Aboriginal communities are predomi-nantly in rural and remote areas and are dispro-portionately affected by opioid dependence, with rates between 50% and 80%.47 Nonmedical use of prescription opioids is more common than heroin use,47,48 and the route of exposure is more often oral than intravenous.48 A 2012 descriptive report from Northwestern Ontario questioned whether the benefits seen with methadone in people who use heroin are applicable in remote Aboriginal communities where women engage in binge use of prescription opioids owing to
Box 3: Resources for clinicians
• Wong S, Ordean A, Kahan M. Substance abuse in pregnancy. J Obstet Gynaecol Can 2011;33:367-84.12
• American College of Obstetricians and Gynecologists. Opioid abuse, dependence and addiction in pregnancy. Committee opinion 254. Obstet Gynecol 2012;119:1070-71.13
• Chase C. Supporting women using opiates in pregnancy: a guideline for primary care providers. Toronto: The Centre for Addiction and Mental Health Knowledge Exchange; 2011. Available: http://knowledgex.camh .net/opioid_alert/2012/Documents/supporting_women_opiates_pregnancy511.pdf28
• Methadone program. Ottawa: Health Canada; 2011. Available: www.hc -sc.gc.ca/hc-ps/substancontrol/exemptions/methadone-eng.php14
• Hanford C. Buprenorphine/naloxone for opioid dependence: clinical practice guideline. Toronto: Centre for Addiction and Mental Health; 2012.23

Review
E44 CMAJ, January 6, 2015, 187(1)
intermittent drug availability rather than daily use of heroin.49 No evidence supports or refutes this claim.
A prevalence study involving First Nations women receiving antenatal care in Sioux Look-out, Ontario, showed that opioid use increased from 8% to 18% during the 18-month study. Neonatal abstinence syndrome in infants exposed to opioids was 30% overall and 66% among infants born to women who used opioids daily.48 Of the children affected, only 7% required pharmacologic treatment, whereas the remainder received supportive care.48 Pilot stud-ies are in progress in First Nations communities in Northwestern Ontario to investigate community-based provision of buprenorphine maintenance therapy where methadone is not available50 and to provide locally trained mater-nal support workers for women with opioid
dependence during pregnancy and continuing until the child reaches 3 years of age.51
Conclusion
Although methadone is the gold standard for treatment of opioid dependency in pregnancy, methadone therapy is often not feasible in rural and remote settings. Proposed alternatives to methadone, such as opioid detoxification and slow-release morphine substitution, have limited evidence to support their use in pregnancy. Stronger evidence exists to support buprenor-phine maintenance therapy.
A fundamental flaw of each study is the choice of birth as an end point. This enables reporting of nominal success rates in terms of abstinence at the time of delivery and neonatal abstinence syndrome. However, the true end
Box 4: Summary of retrospective case series describing methadone detoxification in pregnancy
Reference Protocol
Outcomes at delivery
Maternal Neonatal
Maas et al. 199042 n = 58
• Outpatient detoxification lasting 2–8 wk
• Individualized taper of 0.2–1 mg of methadone daily
• Abstinence: 17/58• MMT taper: 8/58• MMT taper with illicit drug use:
32/58• Lost to follow-up: 1/58
• Fewer NAS symptoms, lower PTD rate, higher body weight, longer pregnancies among women who abstained, followed by women who underwent MMT, compared with women who continued to use heroin
Dashe et al. 199840 n = 34
Stabilization• Clonidine: mild withdrawal• Methadone: moderate to
severe withdrawalTaper• No more than 20% every 3 d• 3–39 d, median 12-d inpatient
stay
• Abstinence: 59%• MMT: 12%• Illicit drug use: 29%
• NAS: 44% of infants showed symptoms, 15% required treatment
• PTD: no deliveries before 36 wk• Stillbirth: none
Luty et al. 200343 n = 101
• 21-d inpatient methadone taper
• 51 women lost to follow-up• Complete records for 24
women and 22 infants
• Abstinence: 1/24• MMT and opiate use: not
documented• Rehabilitation program
postpartum: none
• NAS: Not documented• PTD: 7/22 infants for whom
records were available• Stillbirth: None
Jones et al. 200844 n = 123
3-d methadone taper (n = 75)• Day 1, 20 mg; day 2, 10 mg;
day 3, 10 mg7-d methadone taper (n = 48)• Day 1, 30 mg; dose reduced by
5 mg each day thereafter
• Abstinence: 47% (3-d taper) and 43% (7-d taper)
• MMT: 11% (3-d taper) and 42% (7-d taper)
• Illicit drug use: 53% (3-d taper) and 57% (7-d taper) vs. 23% in control group receiving MMT
• No difference between case and control groups for NAS, low birth weight or APGAR scores
Stewart et al. 201341 n = 95
Stabilization• Methadone dose based on
history of use and titrated up based on withdrawal symptoms
Taper• No more than 20% every 1–3 d
• Abstinence: 56%• MMT: 18%• Illicit drug use: 44%
• NAS: Lower Finnegan scores, shorter stays in hospital and less treatment
• PTD: No difference• Stillbirth: 2 (mothers were
actively using heroin)
Note: APGAR = appearance, pulse, grimace, activity, respiration; MMT = methadone maintenance therapy; NAS = neonatal abstinence syndrome; PTD = preterm delivery.

Review
CMAJ, January 6, 2015, 187(1) E45
point is either sustained abstinence or stable opi-oid substitution therapy that would enable the new mother to parent her child. In this regard, the literature suggests that postpartum treatment is generally not provided to women in rural and remote communities, which contributes to high rates of relapse and apprehension of infants into custody.2,13,44
Despite knowledge of harm and rising rates of opioid dependence in pregnancy, there is a paucity of high-quality evidence in this area and none that specifically addresses the needs of rural and remote communities or Aboriginal communities, polysubstance use or postpartum management. There is an overwhelming need for training in opioid dependence therapy, regulatory changes to ensure pregnant women have access to appropriate medications and greater access to comprehensive treatment both during pregnancy and postpartum in rural and remote settings.
References 1. International Narcotics Control Board. Narcotic drugs techni-
cal report: estimated world requirements for 2013 — statistics for 2011. New York: United Nations; 2013.
2. Kaltenbach K, Berghella V, Finnegan L. Opioid dependence during pregnancy: effects and management. Obstet Gynecol Clin North Am 1998;25:139-51.
3. Fajemirokun-Odudeyi O, Sinha C, Tutty S, et al. Pregnancy out-come in women who use opiates. Eur J Obstet Gynecol Reprod Biol 2006;126:170-5.
4. Jones HE, Martin PR, Heil SH, et al. Treatment of opioid-dependent pregnant women: clinical and research issues. J Subst Abuse Treat 2008;35:245-59.
5. Winklbaur B, Kopf N, Ebner N, et al. Treating pregnant women dependent on opioids is not the same as treating pregnancy and opioid dependence: a knowledge synthesis for better treatment for women and neonates. Addiction 2008;103:1429-40.
6. Borders TF, Booth BM. Research on rural residence and access to drug abuse services: Where are we and where do we go? J Rural Health 2007;23(Suppl):79-83.
7. Canadian Task Force on Preventive Health Care. New grades for recommendations from the Canadian Task Force on Pre-ventive Health Care. CMAJ 2003;169:207-8.
8. What’s urban? What’s rural? Ottawa: Statistics Canada. Available: www41 .statcan.ca/2006/3119/ceb3119_002-eng.htm (accessed 2014 Apr. 21].
9. Buske L. Rural reality: analyzing medical life outside Canada’s cities. Ottawa: Canadian Medical Association; 2008.
10. Shannon LM, Havens JR, Hays L. Examining differences in sub-stance use among rural and urban pregnant women. Am J Addict 2010;19:467-73.
11. Heil SH, Sigmon SC, Jones HE, et al. Comparison of charac-teristics of opioid-using pregnant women in rural and urban settings. Am J Drug Alcohol Abuse 2008;34:463-71.
12. Wong S, Ordean A, Kahan M. Substance abuse in pregnancy. J Obstet Gynaecol Can 2011;33:367-84.
13. American College of Obstetricians and Gynecologists. Opioid abuse, dependence and addiction in pregnancy. Committee opinion 254. Obstet Gynecol 2012;119:1070-71.
14. Methadone program. Ottawa: Health Canada; 2011. Available: www.hc-sc.gc.ca/hc-ps/substancontrol/exemptions/methadone-eng .php (accessed 2013 July 29).
15. Section 56 class exemption for pharmacists. Ottawa: Health Canada; 2011. Available: www.hc-sc.gc.ca/hc-ps/substancontrol /pol/pol-docs/exemp_pharm-eng.php (accessed2013 July 29).
16. Lacroix I, Berrebi A, Garipuy D, et al. Buprenorphine versus methadone in pregnant opioid-dependent women: a prospec-tive multicenter study. Eur J Clin Pharmacol 2011;67:1053-9.
17. Welle-Strand GK, Skurtveit S, Jones HE, et al. Neonatal out-comes following in utero exposure to methadone or buprenor-phine: a national cohort study of opioid-agonist treatment of preg-nant women in Norway from 1996 to 2009. Drug Alcohol Depend 2013;127:200-6.
18. Fischer G, Ortner R, Rohrmeister K, et al. Methadone versus buprenorphine in pregnant addicts: a double-blind, double-dummy comparison study. Addiction 2006;101:275-81.
19. Jones HE, Kaltenbach K, Heil SH, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N Engl J Med 2010;363:2320-31.
20. Debelak K, Morrone WR, O’Grady KE, et al. Buprenorphine + naloxone in the treatment of opioid dependence during preg-nancy-initial patient care and outcome data. Am J Addict 2013;22:252-4.
21. Potter JS, Marino EN, Hillhouse MP, et al. Buprenorphine/nal-oxone and methadone maintenance treatment outcomes for opioid analgesic, heroin, and combined users: findings from starting treatment with agonist replacement therapies (START). J Stud Alcohol Drugs 2013;74:605-13.
22. Hser YI, Saxon AJ, Huang D, et al. Treatment retention among patients randomized to buprenorphine/naloxone compared to methadone in a multi-site trial. Addiction 2014; 109:79-87.
23. Hanford C. Buprenorphine/naloxone for opioid dependence: clinical practice guideline. Toronto: Centre for Addiction and Mental Health; 2012.
24. Lund IO, Fischer G, Welle-Strand GK, et al. A comparison of buprenorphine + naloxone to buprenorphine and methadone in the treatment of opioid dependence during pregnancy: maternal and neonatal outcomes. Subst Abuse 2013;7:61-74.
25. Daily Med. Naloxone hydrochloride [product monograph]. Bethesda (MD): National Institutes of Health; 2013. Available: http://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid =d524c0e5 -a7c2 -40b2-9eed-2caf71c787dc (accessed 2013 Aug. 23).
26. Daily Med. Suboxone tablet [product monograph]. Bethesda (MD): National Institutes of Health; 2013. Available: http://dailymed .nlm .nih.gov/dailymed/lookup.cfm?setid=4b9b43c4-293e-4323-a1a1 -9a2f6a16ac39. (accessed 2013 Aug. 23)
27. Daily Med. Suboxone soluble film [product monograph]. Bethesda (MD): National Institutes of Health; 2013. Available: http://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid =8a5edcf9 -828c-4f97-b671-268ab13a8ecd(accessed 2013 Aug. 23)
28. Chase C. Supporting women using opiates in pregnancy: a guideline for primary care providers. Toronto: The Centre for Addiction and Mental Health Knowledge Exchange; 2011. (accessed 2013 Aug. 11). Available: http://knowledgex.camh .net/opioid_alert/2012/Documents/supporting_women_opiates _pregnancy511.pdf
29. Fischer G, Jagsch R, Eder H, et al. Comparison of methadone and slow-release morphine maintenance in pregnant addicts. Addiction 1999;94:231-9.
30. Schneider C, Fischer G, Diamant K, et al. Pregnancy and Drug Dependence. Wien Klin Wochenschr 1996;108:611-4.
31. Etzersdorfer P, Fischer G, Eder H, et al. Comparison of mor-phine and methadone maintenance in pregnant opiate addicts. NIDA Res Monogr 1997;178:343.
32. Ornoy A, Michailevskaya V, Lukashov I, et al. The develop-mental outcome of children born to heroin-dependent mothers, raised at home or adopted. Child Abuse Negl 1996;20:385-96.
33. McCarthy JJ, Leamon MH, Parr MS, et al. High-dose metha-done maintenance in pregnancy: maternal and neonatal out-comes. Am J Obstet Gynecol 2005;193:606-10.
34. Cleary BJ, Eogan M, O’Connell MP, et al. Methadone and peri-natal outcomes: a prospective cohort study. Addiction 2012; 107:1482-92.
35. Albright B, de la Torre L, Skipper B, et al. Changes in metha-done maintenance therapy during and after pregnancy. J Subst Abuse Treat 2011;41:347-53.
36. Blinick G, Wallach RC, Jerez E. Pregnancy in narcotics addicts treated by medical withdrawal. The methadone detoxification program. Am J Obstet Gynecol 1969;105:997-1003.
37. Rementeriá JL, Nunag NN. Narcotic withdrawal in pregnancy: stillbirth incidence with a case report. Am J Obstet Gynecol 1973; 116:1152-6.
38. Stern R. The pregnant addict: a study of 66 case histories, 1950–1959. Am J Obstet Gynecol 1966;94:253-7.
39. Dashe JS, Sheffield JS, Olscher DA, et al. Relationship between maternal methadone dosage and neonatal withdrawal. Obstet Gynecol 2002;100:1244-9.
40. Dashe JS, Jackson GL, Olscher DA, et al. Opioid detoxification in pregnancy. Obstet Gynecol 1998;92:854-8.
41. Stewart RD, Nelson DB, Adhikari EH, et al. The obstetrical and neonatal impact of maternal opioid detoxification in preg-nancy. Am J Obstet Gynecol 2013;209:267.e1-5.
42. Maas U, Kattner E, Weingart-Jesse B, et al. Infrequent neona-tal opiate withdrawal following maternal methadone detoxifi-cation during pregnancy. J Perinat Med 1990;18:111-8.
43. Luty J, Nikolaou V, Bearn J. Is opiate detoxification unsafe in pregnancy? J Subst Abuse Treat 2003;24:363-7.

Review
E46 CMAJ, January 6, 2015, 187(1)
44. Jones HE, O’Grady KE, Malfi D, et al. Methadone mainte-nance vs. methadone taper during pregnancy: maternal and neonatal outcomes. Am J Addict 2008;17:372-86.
45. Finnegan LP. Treatment issues for opioid-dependent women during the perinatal period. J Psychoactive Drugs 1991;23: 191-201.
46. Kaltenbach K, Berghella V, Finnegan L. Opioid dependence dur-ing pregnancy. Effects and management. Obstet Gynecol Clin North Am 1998;25:139-51.
47. Uddin F. Hope in Fort Hope: First Nations community is winning the battle against prescription drug abuse. Can Fam Physician 2013;59:391-3.
48. Kelly L, Dooley J, Cromarty H, et al. Narcotic-exposed neonates in a First Nations population in Northwestern Ontario: incidence and implications. Can Fam Physician 2011;57:e441-7.
49. Kiepek N, Hancock L, Toppozini D, et al. Facilitating medical withdrawal from opiates in rural Ontario. Rural Remote Health 2012; 12:2193.
50. Webster PC. Indigenous Canadians confront prescription opi-oid misuse. Lancet 2013;381:1447-8.
51. First Nations maternal support worker program first of its kind. Meno Ya Win News [Sioux Lookout (ON)] 2013;11:1-2.
Affiliations: Thunder Bay Regional Research Institute, Thun-der Bay, Ont., and Department of Obstetrics and Gynaecol-ogy (Jumah), University of Toronto, Toronto, Ont.; Depart-ment of Family Medicine (Graves), Northern Ontario School of Medicine, Sudbury, Ont.; Department of Family and Com-munity Medicine, University of Toronto, and Substance Use Service, Women’s College Hospital (Kahan), Toronto, Ont.
Contributors: Naana Afua Jumah was responsible for the pri-mary literature review, the analysis and interpretation of data and the drafting and revising of the article. Lisa Graves and Meldon Kahan contributed to the analysis and interpretation of the data and revised the article for important intellectual con-tent. All of the authors approved the final version submitted for publication and agree to act as guarantors of the work.







