opioid harm reduction
TRANSCRIPT
Opioid Harm Reduction Strategies
Paul C. Coelho, MDBoard Certified PM&R
Subspecialty Certified Pain Medicine
Sunday, August 30, 15
Table Of Contents
1. General Principles
2. Reducing Harms to High Dose Patients
3. Preventing Harms to Opioid Naive Patients
Sunday, August 30, 15
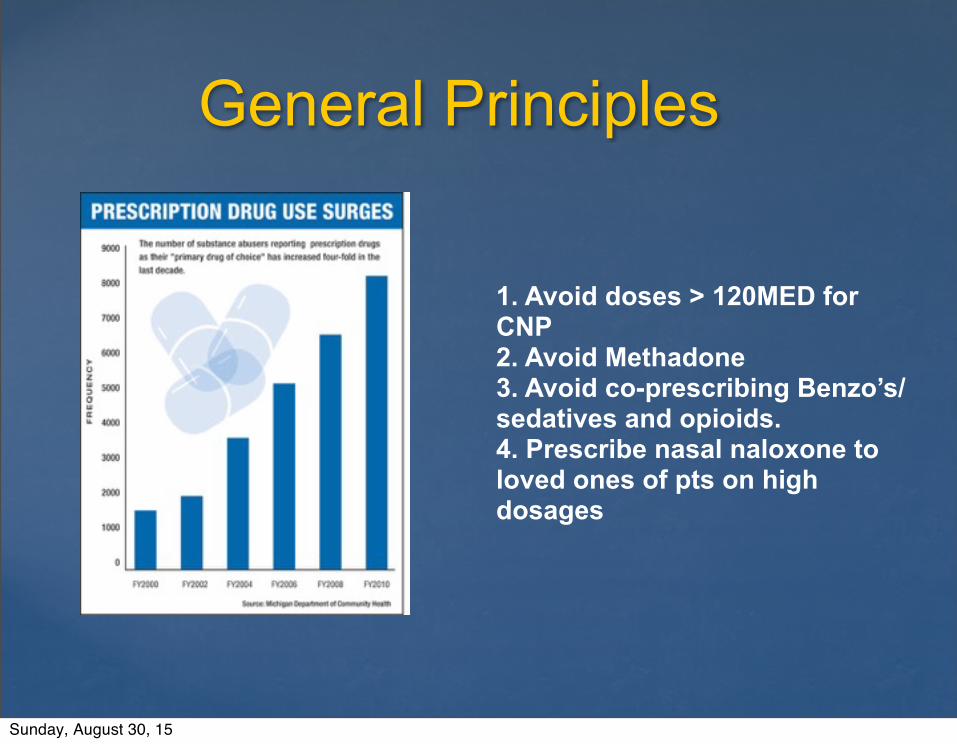
General Principles
1. Avoid doses > 120MED for CNP2. Avoid Methadone3. Avoid co-prescribing Benzo’s/ sedatives and opioids.4. Prescribe nasal naloxone to loved ones of pts on high dosages
Sunday, August 30, 15
High Dose (>120MED)Patients
1. Identify the high risk patients.
2. Explain to the patients that their dose has become dangerously
high and it will need to change.
3. Prescribe nasal naloxone and train a loved one in the
patient’s household on administration.
4. If the MED is < 240 offer the patient a 6mo taper.
5. If the MED is > 240 consider a taper or conversion to
buprenorphine for PAIN.
Sunday, August 30, 15
Example 1: Teresa
68y/o retired missionary with diffuse OA. Lives in Mennonite Village. Uses Oxycodone-APAP 10/325, six per day (MED 80). No aberrant behavior.
Sunday, August 30, 15
Example 1: Teresa
1. Teresa reports the medications give her comfort.
2. She was started on them years ago by a doctor long since retired.
3. Leave Teresa alone. She is not who we are worried about for the purposes of this talk.
Sunday, August 30, 15
Example 2: Cleatus
68y/o retired millwright with failed back syndrome. Lives with spouse Rx’d MS04 ER 60mg QID (MED 240). No aberrant behavior.
Sunday, August 30, 15
Example 2: Cleatus
1. Call Cleatus & Mabel into clinic to explain that new literature has suggests that Cleatus’ dose has become unsafe and it will need to change.
2. Rx nasal naloxone and train Mabel in it’s administration.
3. Offer a 15mg/mo taper over 8mo to 120MED.
Sunday, August 30, 15
Example 3: Loretta
52y/o disabled woman with FMS and chronic Hep C, on Transplant List @ OHSU. Medications include a Fentanyl patch 100ucg/hr Q48, Soma 350mg QID, and Xanax .5mg QID. Has an OMMP card. (MED 360)
Sunday, August 30, 15
Example 3: Loretta1. Call Loretta and her adult daughter/care-giver
into clinic to explain that new literature has suggests that Loretta’s dose has become unsafe and it will need to change.
2. Consider an addiction medicine consult given the complex PMH, Hep C, & Transplant status.
3. Rx nasal naloxone and train Frisbee - her daughter- in it’s administration.
4. Load with Gabapentin over 1mo to 1200mg/day5. Convert from alprazolam to clonazepam - 1:1
conversion and begin a 6mo taper. Consider non-addictive alternatives for anxiety (citalopram).
Sunday, August 30, 15

Example 3: Loretta
6. Stop the Soma - it is an addictive barbiturate - and offer a conventional muscle relaxant.7. Consider a conversion to Buprenophine for pain : Induction, stabilization, maintenance.7a. Or offer a 12ucg/mo taper to 50ucg/hr.8. Explain that our clinic policy is either THC or opioids but not both and let her choose.
Sunday, August 30, 15
Addiction Services In Oregon By County
Drug & Alcohol Services by County: http://www.oregon.gov/oha/amh/publications/provider-directory.pdf
Sunday, August 30, 15
Nasal Naloxone
1. SB 384 legalized for lay administration in 2013.
2. Stock in your pharmacies.3. Some patients must pay out of
pocket ($25.00.)4. http://www.prescribetoprevent.org/
wp-content/uploads/2012/11/naloxone-one-pager-in-nov-2012.pdf
Sunday, August 30, 15
Buprenorphine
1. Schedule III opioid.2. Morphine Equivalence 30:1.3. FDA approved for pain - Butrans & addiction - Suboxone.4. Ceiling effect for respiratory
suppression.5. Follow the QTc.6. Contra-indications: coprescribing
benzo’s, sedatives,or alcohol use.
Sunday, August 30, 15

Pain or Fear of Withdrawal?
Sunday, August 30, 15
It’s Easier Not to Start Opioids, Than to Stop Em.
Sunday, August 30, 15
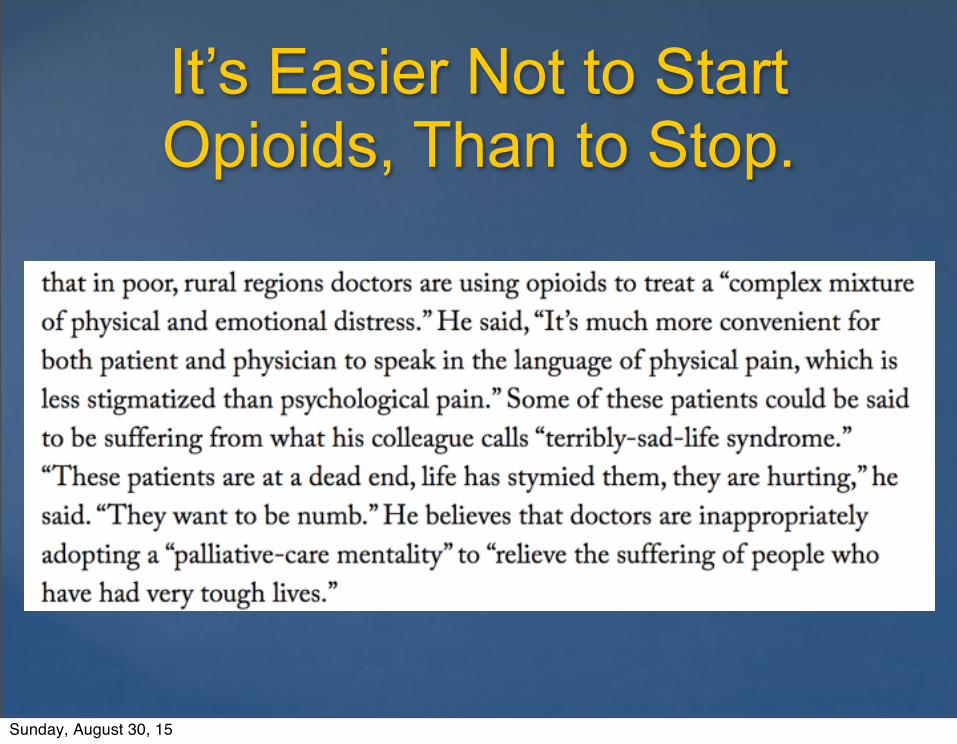
It’s Easier Not to Start Opioids, Than to Stop.
Sunday, August 30, 15
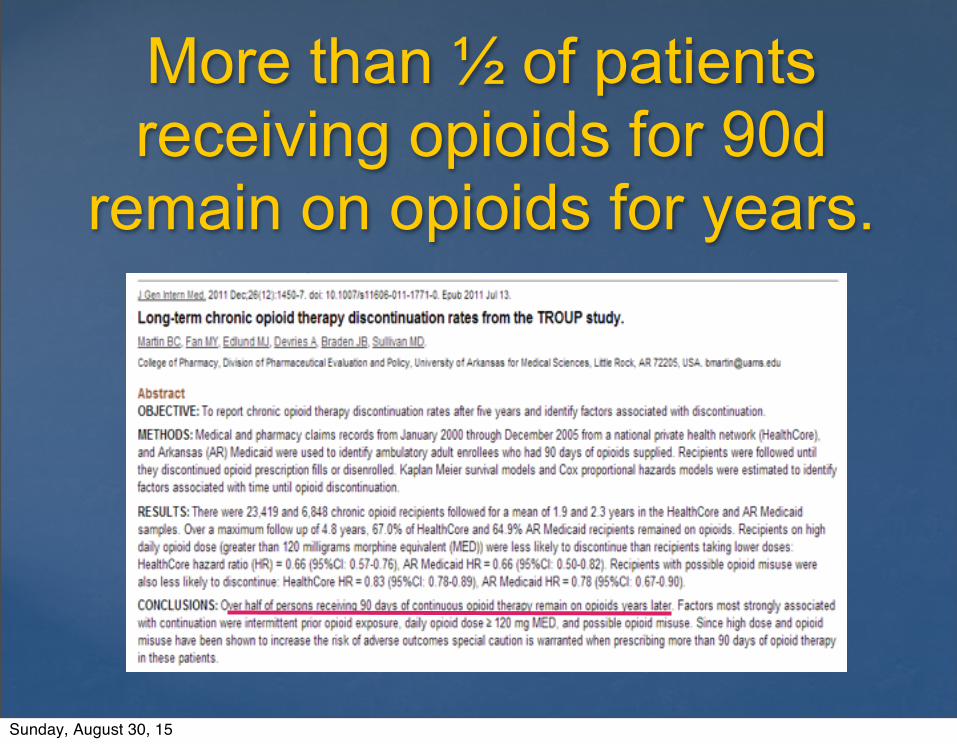
More than ½ of patients receiving opioids for 90d
remain on opioids for years.
Sunday, August 30, 15
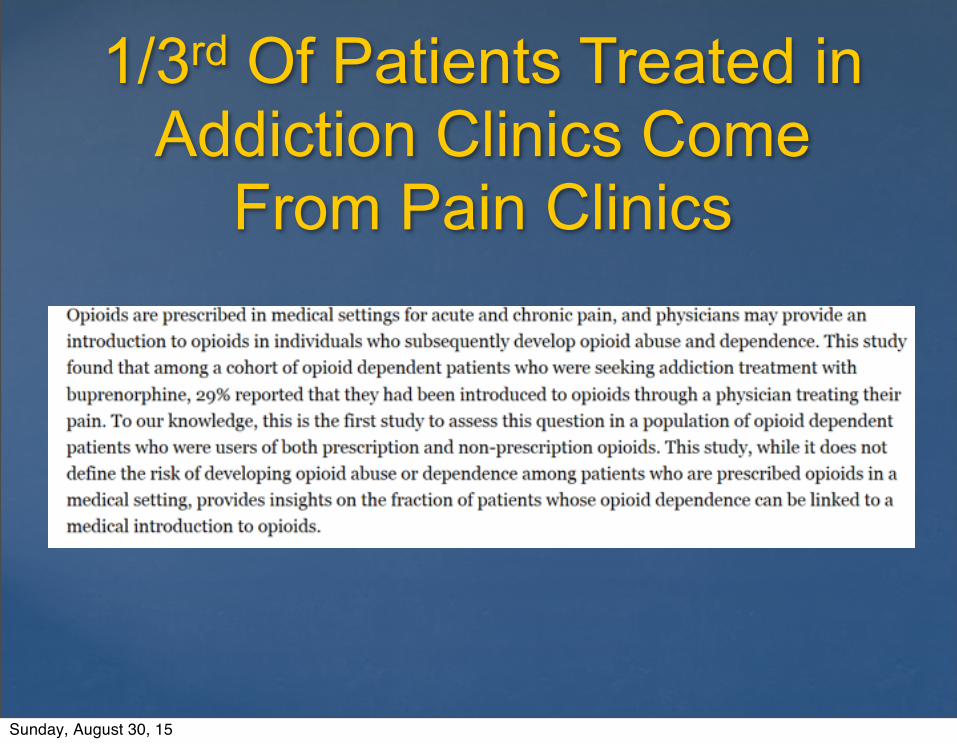
1/3rd Of Patients Treated in Addiction Clinics Come
From Pain Clinics
Sunday, August 30, 15
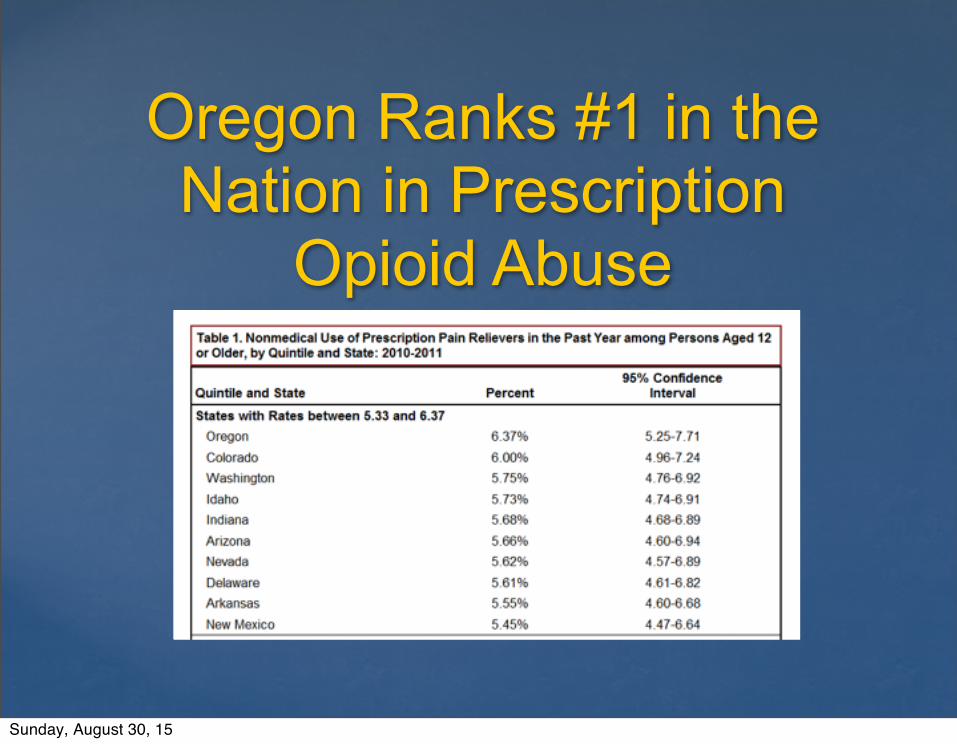
Oregon Ranks #1 in the Nation in Prescription
Opioid Abuse
Sunday, August 30, 15
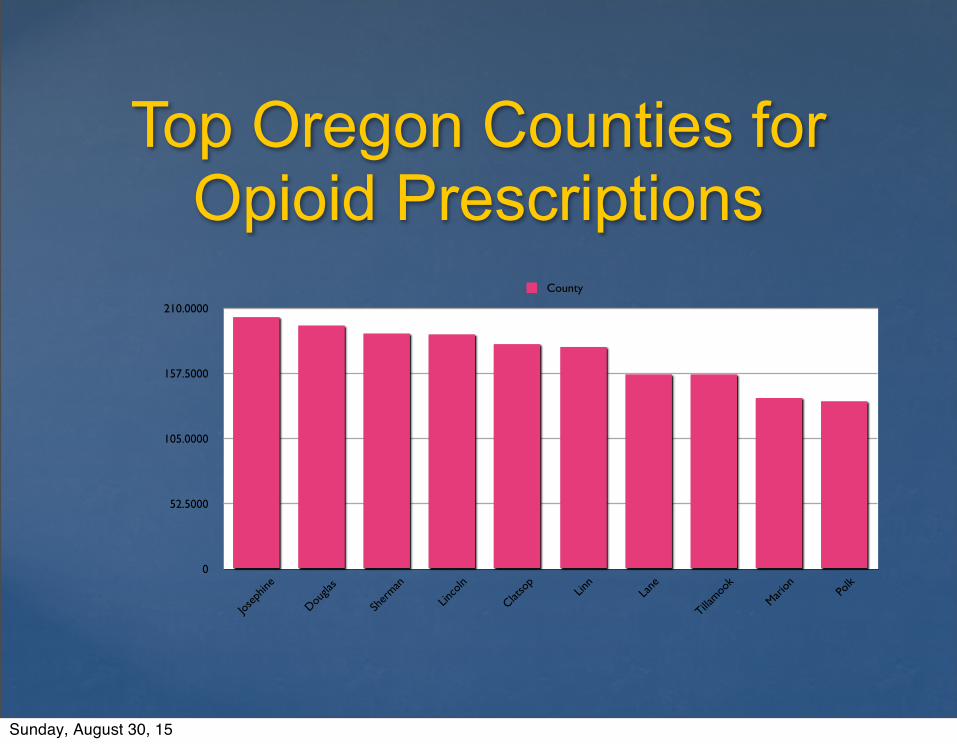
Top Oregon Counties for Opioid Prescriptions
0
52.5000
105.0000
157.5000
210.0000
Josep
hine
Dougla
s
Sher
man
Linco
ln
Clatso
pLin
nLa
ne
Tillamoo
k
Marion Po
lk
County
Sunday, August 30, 15

Prescription Opioid Deaths In Oregon 2000-2011
Sunday, August 30, 15
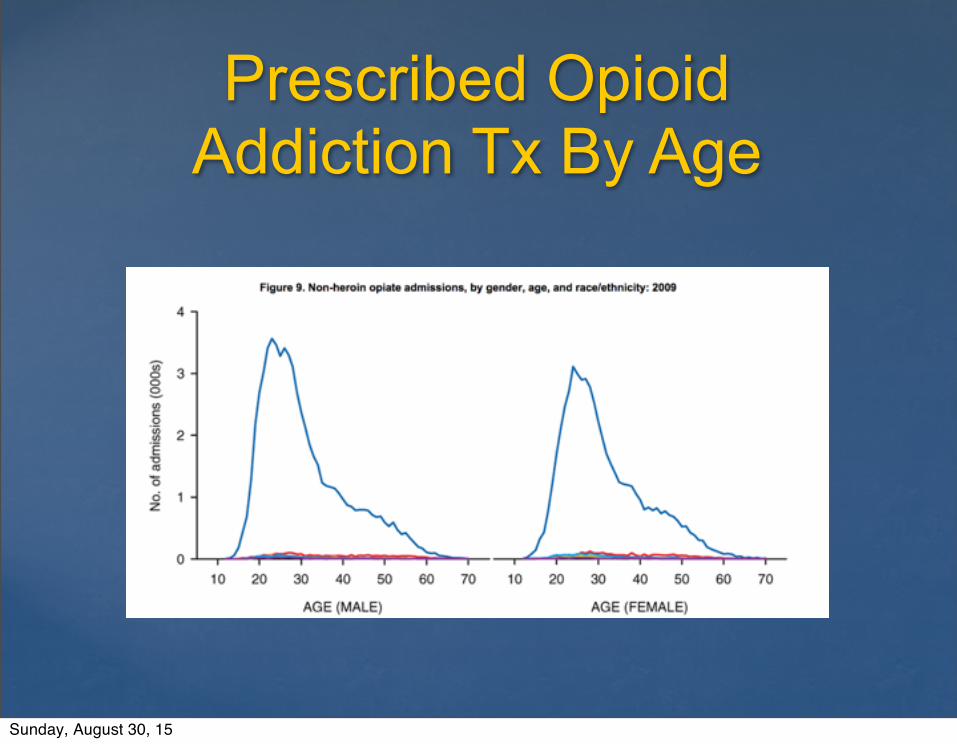
Prescribed Opioid Addiction Tx By Age
Sunday, August 30, 15

Age of Opioid ODD
Sunday, August 30, 15
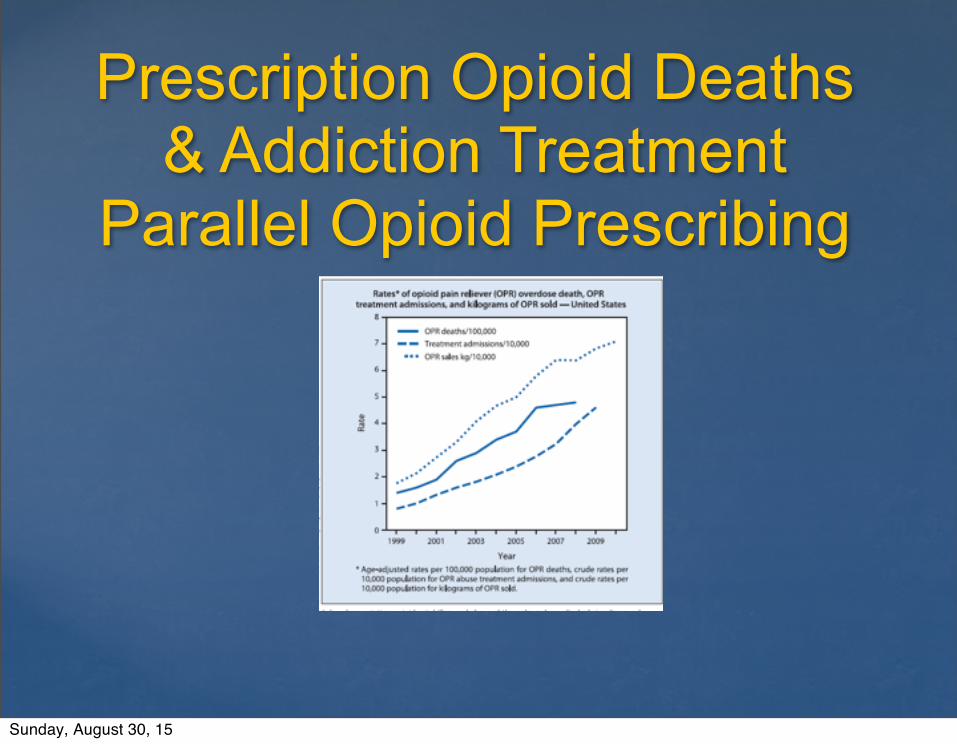
Prescription Opioid Deaths & Addiction Treatment
Parallel Opioid Prescribing
Sunday, August 30, 15
Special Thanks To:
• Andrew Kolodny, MD, Chief Medical OfficerPhoenix House
• Jim Shames, MD, Medical Director Jackson County, OR Health & Human Services
• Andrew Mendenhall, MD, Medical DirectorHazelden, Beaverton, OR
Sunday, August 30, 15

Thank You
www.supportprop.org
Sunday, August 30, 15