operationalizing healthy timing and spacing of pregnancy (htsp) in child health services: basics...
TRANSCRIPT

Operationalizing Healthy Timing and
Spacing of Pregnancy (HTSP) in Child Health
Services: BASICS Experience in Rwanda
Gloria Ekpo, MD, MPHIssakha Diallo, MD, MPH, DrPH
Diana Silimperi, MD, MPHMathias Yameogo, MD, MPH
Moses Ahabwe, MD MPHMay 24, 2008

Infants are twice as likely to survive if the previous birth interval is at least 2 years
177
104
7161
162
79
59
112
7154
29
78
149
88
71 71
< 2years 2 years 3 years 4year +
Mali Rwanda Cambodia Timor Leste
Source: Rwanda, Mali, Cambodia, Timor Leste DHS data
Infa
nt
Mor
talit
y R
ate
per
100
0Justification for On-going Advocacy and
Implementation of HTSP

Population: 8,648,248 (PGR: 2.43%)
Fertility Rate: 6.1
Knowledge of a method of FP: 98%
Contraceptive Prevalence:10%
Unmet Need for pregnancy spacing: 41%
HIV Prevalence: 3.6% (women and 2.3% in men)
Life Expectancy at birth: 47.3 years
RWANDA: BACKGROUND
Source: Rwanda DHS III 2005

Week in Review
After So Many Deaths, Too Many Births
Laura Hoemeke/Twubakane Decentralization and Health Program
BABIES, NOT GHOSTS A crowd at a health campaign rally in northern Rwanda. Population control has been controversial because survivors of the genocide have felt it was a family’s right to replenish what was lost. By STEPHEN KINZER Published: February 11, 2007
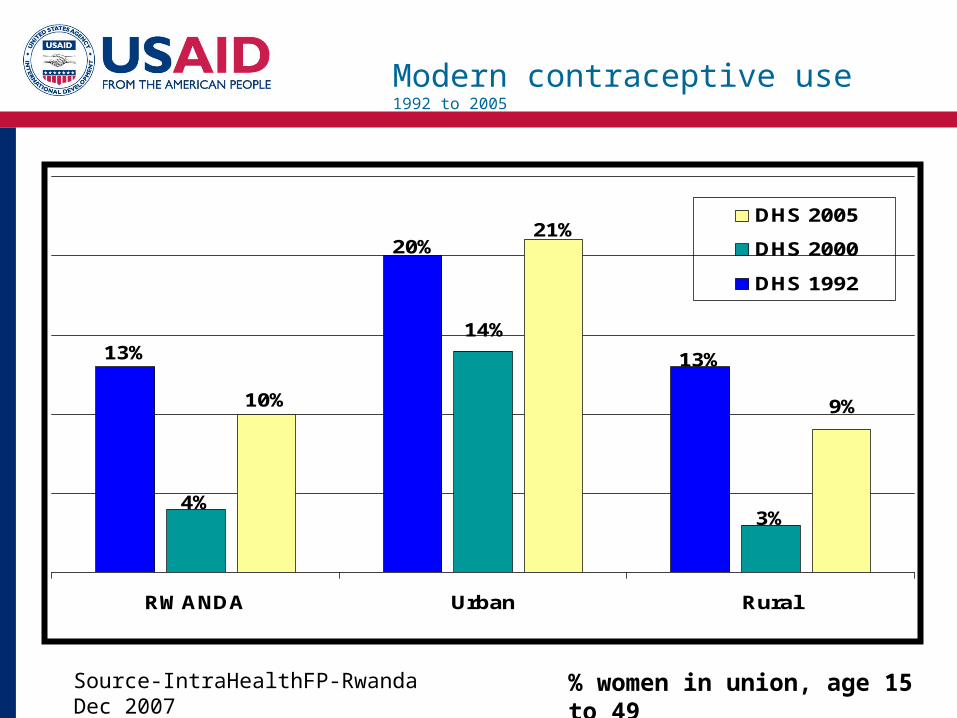
Modern contraceptive use 1992 to 2005
10%
13%
21%
9%
14%
3%4%
20%
13%
RuralUrbanRWANDA
DHS 2005
DHS 2000
DHS 1992
% women in union, age 15 to 49Source-IntraHealthFP-Rwanda Dec 2007

Important proportion of women have short birth intervals – case of Rwanda
Source: Rwanda DHS-III, 2005
23% Birth Interval < 2 years
41% 2 < Birth Interval < 3 years
36% Birth Interval ≥ 3 years

Children are paying the Highest Toll from the Short Birth Intervals In Rwanda
Source: Rwanda DHS-III, 2005
7953 48 47
149
8871 78
11390
72 71
245
170138 143
< 2 years 2 years 3 years 4 years +
Post Neonatal Mortality Rate Infant Mortality Rate
Child Mortality Rate Under five Mortality Rate
Mortality ratio per 1000

Pregnancies in 132 Women After Testing HIV+
GoR managedFaith-based
managedTotal
Intended 24 (35%) 10 (16%) 34 (26%)
Unintended 45 (65%) 52 (84%) 97 (74%)
Total 69 (100%) 62 (100%) 131* (100%)
* Excluding one case of no reply
p=.02 Source; Livinus Bangendanye, FHI/Rwanda Pregnancy, Pregnancy Desires, and Contraceptive Use Among HIV-infected Women 3rd Pediatric HIV Conference Dec 2007
Integrating HTSP into HIV Programs

Reported Contraceptive Use in 97 Cases of Unintended Pregnancy
GoR managedFaith-based
managedTotal
Modern 25 (56%) 17 (33%) 42 (43%)
Natural 2 (4%) 10 (19%) 12 (12%)
None 18 (40%) 25 (48%) 43 (44%)
Total 45 (100%) 52 (100%) 97 (100%)

Context of Family Planning in Rwanda
• 365 (81%) out of 450 health facilities offer Family Planning services
• FBOs own 133 (30%) health facilities of which 47% (62) of these offer FP services (i.e 17% of total FP facilities are owned by FBOs)
• FP services are not offered daily in most health facilities
• FBO facilities willing to counsel clients for FP but may not offer full package for FP at their facilities
• Secondary FP Post erected to accommodate clients needs from FBO facilities
• High client demand for long-term methods (Implants and injectables)
• Most services are free
• Incentive-Motivation: Performance-based Financing for FP services

449
365
133
62
0
50
100
150
200
250
300
350
400
450
Number of Health Facilities
1Category of FP Facility
Health Facilities and Family Planning Services in Rwanda
Total number of Health Facilities Number of Health Facilities with FP servicesNumber of Health Facilities owned by FBOs Number of FBO facilities providing FP services

Rwanda Government Objectives and Targets
for Family Planning 2006-2020
Indicator Baseline 2000
2005 2010 2020
Contraceptive Prevalence Rate-All Methods 13.2% 15.1% 26.3% 45.2%
Contraceptive Prevalence Rate-Modern Methods
4.3% 7.1% 18.5% 36.1%
Infant Mortality Rate(deaths/1000 live births) 107 - 70 25
Maternal Mortality Ratio 1071 - 700 350
Number of HIV +ve women counseled on FP - 113,000 - -
Number of HIV +ve women using modern methods
146,000
Women’s Total Fertility Rate 5.8 - 5.5 4.5
Population Growth Rate - 2.6 2.3 2.2

Enabling environment for a successful Integration: the Case of Rwanda
– Readily available quality and complete data from the DHS III 2005
– Functional PHC activities with increasing performance for the essential MCH package
– Political will and Partnership in management and leadership functional structures
– Partnership and collaboration in HTSP activities
– Appropriate tools and approaches for quality assurance
– Training and capacity building of health care workers on HTSP integration
– Supportive supervision, mentorship and monitoring

Programmatic HTSP Integration Strategies
• Advocacy: Encouraging governments and partners to adopt integration strategy, guidelines, or policy;
• Integration: Development/Strengthening of guidelines in HTSP, development of tools, dissemination of revised guidelines, policies, tools to relevant officials and partners;
• Implementation: Training of trainers and on-the-job-training of service providers on integration of HTSP in child health at central and district levels;
• Supervision, mentorship and Monitoring: Supportive supervision and mentoring of HTSP service providers;
• Expansion and Scale-up: To improve coverage in additional districts and provinces in the countries.
• Partnership and Collaboration: Global and Country level
USAID, ESD, ACCESS-FP, IMMbasics Ministry of Health and Maternal and Child Health department of ; Intrahealth/Twubakane project; Intrahealth/Capacity project; Extended Impact Project (EIP: IRC, WorldRelief, Concern), EGPAF, Population Council

Platforms for HTSP integration in child health programs
– IMNCI-Sick baby clinics at MCH (Rwanda, Malawi)
– Immunization and Well baby clinics (Rwanda)
– Essential newborn and postnatal care (Swaziland, East Timor, Cambodia)
– PMTCT programs (Malawi)
– Pediatric HIV care and support services (Rwanda)
– Pre-service and In-service training curriculum (Rwanda, Malawi)

1. Advocacy and Capacity Building in HTSP
2. Methodological guide for HTSP integration at child health entry points to care
3. Rapid Facility Functionality Assessment Guide
4. Supervision and Mentorship checklist
5. Framework for monitoring and evaluation at global and country level of HTSP results
6. Training Manual for integration of HTSP into child health programs
Tools in Support of HTSP Programming

HTSP Key Messages at Immunization Sites
HTSP:
• You have just given birth, waiting at least 24 months before trying to become pregnant again, but not more than five years is better for your health and your children’s health;
• Choosing a secure and effective contraceptive method that you can easily use is the best way to prevent unplanned pregnancy;
• This facility provides support for healthy timing and spacing of pregnancy and for more information about how you can access these services, please meet with our counselors before you leave this facility today.

Rwanda: Preliminary integration process at Immunization sites
• Key messages developed for use at group education sessions for women/parents/guardian
• 5 Pilot sites identified for the implementation of HTSP integrated messages
• Explore holding Immunization and FP services on same days
• Use of Secondary FP posts for close to FBO health facilities• Conduct mobile FP clinic during community immunization
outreaches and campaigns • Expectations:
– One-stop shop for child and maternal health needs in IMM and FP– Mothers looking forward to immunization days– Access FP services in addition to child immunization– Increased in uptake and retention of services

ADVOCACY
Policy Makers
Program Planners
Men
Civil Society,

ADVOCACY
Couples
Grand-mothers/fathers
Women Health Care Workers

On-The-Job-Training on HTSP
Accomplishment at Country Level
Rwanda:1. Integration and strengthening HTSP in:
• IMCI Training Manual, • pre-service nursing curriculum, • pediatric HIV job aids and tools• Comprehensive referral form for health facilities
2. Development of key HTSP messages for utilization at immunization sites
3. Training of trainers on IMNCI-HIV -HTSP integrated manual• 275 HCWs and 25 Supervisors• 42 Health Facilities• 15/30 Districts in the country
4. Supervision and quality assurance visits to monitor integrated services
5. Partners: MOH, TRAC, MCH, EPI, IntraHealth Twubakane, CAPCITY project.

Exit Interview results from clients visiting health centers in two districts in Rwanda
28% 31% 31% 34%
21%
100%
0%
20%
40%
60%
80%
100%
120%
HCW talked to Client onHTSP
Clients could identify 2benefits of HTSP
Clients could state 2methods of FP
Clients could stateadequate birth interval
Clients on modern FPmethod on day of
survey
Clients could identifywhere to go for FP
services
Responses from clients
Clien
ts in
terv
iewed
Rwanda: Exit Interview results from clients visiting health centers in two districts

Rwanda: Entry points to care where HTSP messages are delivered at health facilities.
38%
25% 25%
12.50%
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
Percentage of clients interviewed
FP ART/PMTCT IMCI Admission Ward
Sites where clients received HTSP messages
Result of Exit Interview on HTSP messages to clients at health facilities

Challenges
Constraints & Issues:
– Engaging child health providers to integrate preventive measures such as HTSP activity into their daily busy child survival activities
– Limited human resources for implementation of activities- Point person is required to facilitate program implementation, data collection and supervision of HTSP activities at all levels of care in the country
– Limited funds for expansion and scale up of HTSP integration in child health programs
– Monitoring impact of activities through partners who have other multiple activities and programs

Conclusion
• Integration of HTSP in child health services is crucial to reinforcing child and maternal health services
• HTSP in child health contributes to expand the access and use of FP services by reducing the missed opportunities to educate women/couples in contraception for birth spacing
• HTSP is an essential component of the Repositioning FP Initiative and should receive more attention and commitment from the FP program managers, policy makers and donors

Acknowledgement
USAID Washington
USAID Mission-Rwanda
MCH/MOH Rwanda
BASICS HTSP Partners- ESD, IMMbasics, ACCESS-FP
Implementing Partners:
Intrahealth Twubakane, CAPACITY Project
BASICS Country and HQ HTSP Team

Photo credit: Intrahealth/Twubakane