operating framework for the nhs in england 2011/12
DESCRIPTION
The operating framework for the NHS in England 2011/12 describes the tasks facing the health service in its first full year of transition to the system outlined in the White Paper, Equity and excellence: liberating the NHS. Our short briefing summarises the details and explores the implications.TRANSCRIPT

Contents
Introduction and implications .............1
Setting up the new structure .............2
Finance matters .............................4
Maintaining accountability ................6
Developing quality ..........................7
Commissioning transition timetable .....7
Performance measures .....................9
The operatingframeworkfor the NHS in England 2011/12
wellards.co.uk
Wellards briefi ng on...

The operating framework for the NHS in England 2011/12 describes the tasks facing the health service in its fi rst full year of transition to the system outlined in the White Paper, Equity and excellence: liberating the NHS.
In the coming months the NHS must establish the building blocks of the reorganisation while maintaining service quality, keeping tight control of fi nance and remaining accountable for its decisions.
The operating framework confi rms that the government intends to press ahead with the proposals announced in the Liberating the NHS White Paper, despite disquiet from some professional groups and wider concerns about the burden imposed by structural changes and management cuts at a time of unprecedented fi nancial restraint.
Growth in primary care trust (PCT) allocations is welcome, especially given the extent of cuts elsewhere in the public sector, but the fi nancial environment remains
extremely challenging. Major effi ciency gains will be required on an unprecedented scale.
It is vital that PCTs remain viable organisations until they are dissolved. Forming clusters may help them to do so, although it may risk disrupting existing local plans.
While it is helpful that GP consortia now have an idea of what they will be allowed for running costs, more precise detail is still needed on the duties they will be expected to perform. They will be relieved to fi nd they will not be responsible for PCT debt originating before 2011/12, but some PCTs may fi nd it diffi cult to eradicate this debt before 2013.
Introduction and implications
Key points
• England's NHS priorities are set out at the end of each year in the NHS operating framework
• The annual management guidance published by the Department of Health (DH) identifies the strategic goals for the coming year and describes how the performance of NHS organisations will be monitored
1wellards.co.uk

At national level:
The NHS Commissioning Board will be established in shadow form as a special health authority, overseeing development of GP consortia and systems for their authorisation and accountability. It will become fully operational in April 2012, when its responsibilities will include:
• supporting improvements in NHS-funded services • promoting public and patient involvement and choice • ensuring a comprehensive system of GP consortia and holding them to account• directly commissioning some services including primary medical care, other family health services, prison healthcare and aspects of military healthcare • allocating and accounting for NHS resources• promoting equality and reducing inequalities in access to healthcare along with Public Health England
A provider development authority will be set up by April 2012 as a special health authority to support transition of all remaining NHS trusts to foundation trust status, providing governance and performance management. It will be wound down once this has been achieved by April 2014.
At regional level:
Strategic health authorities (SHAs) will remain accountable for operational delivery and transition arrangements, fostering relationships between GP consortia pathfi nders and local health and wellbeing boards.
At local level:
Primary care trusts will have a critical role until 2013, but instead of maintaining all 150-odd PCTs they will form clusters in each region to fulfi l their statutory duties. Clusters will have a single executive team and be in place by June 2011. They will oversee:
• local and regional planning for 2012/13 and into 2013/14, handing increasing leadership to GP consortia• medium-term quality, innovation, productivity and prevention (QIPP) plans• the closedown of PCTs• services not delegated to consortia, such as commissioning primary care
Clusters will support GP consortia by providing:
• a £2 per head development fund resourced mainly from cost savings released from the mutually agreed resignation scheme (MARS) scheme. This can be used to pay for training and organisational development• delegated budgets with a dedicated management resource• a senior fi nance manager• an organisational development expert
Setting up the new structureKey points
• The NHS Commissioning Board will provide national leadership of commissioning; extend public and patient involvement and choice; and ensure the development of GP consortia
• A provider development authority will support the transition of remaining NHS trusts in becoming foundation trusts
• PCTs will form clusters in each region to support GP consortia
• By April 2012 health and wellbeing boards must formulate plans across the NHS, public health, social care and children's services
2 wellards.co.uk

• an expert in governance arrangements• a commissioning expert• support teams to provide technical functions• help to understand and participate in joint strategic needs assessment (JSNA) — where PCTs traditionally worked with local authorities to fi nd out the health, wellbeing and needs of their local communities
All general practices should consider how best to group together in consortia, ensuring they engage with their local communities.
Health and wellbeing boards will be the main vehicle for councils to lead on integrated working and commissioning across the NHS, public health and social care. A network of 'early implementer' boards will link closely to GP consortia
pathfi nders. By April 2012 boards must carry out a JSNA and devise a joint health and wellbeing strategy across NHS, public health, social care and children's services.
All NHS trusts will become foundation trusts (FTs) by April 2014, including those newly formed from PCT provider arms. SHAs are responsible for developing the 'FT pipeline', led by the national director for provider development.
Divestment of PCT directly provided community services must be completed or substantially progressed by April 2011, using the 'any willing provider' of services policy to encourage social enterprises (businesses that deliver services or goods in the pursuit of primarily social objectives) and others to take over these services.
Setting up the new structure
Department of Health (including public health England) - Overall responsibilty for health, public
health and social care policy
Local authorities(including health and
wellbeing boards)
NHSCommisioning Board
GP consortia
Publichealth
Socialcare
Department for Communities and Local Government
Service delivery
NHS
Accountability to patients, service users and the public(underpinned by regulators and Healthwatch England)
Subject to Parliamentary scrutiny
Public health
delivery
The Liberating the NHS system
3wellards.co.ukCrown copyright

Guiding principles:
Any surplus achieved in 2010/11 will be available to SHAs and PCTs in 2011/12, up to a maximum of £150m and subject to DH approval of how it is distributed.
No PCT may plan for an operating defi cit in 2011/12; NHS trust defi cits will be accepted only if part of an agreed recovery plan.
Every PCT must ensure 2 per cent of their recurrent funding is committed non-recurrently — more if they wish; the 2 per cent will be held by SHAs, and PCTs must submit a business case to access it.
GP consortia will not inherit any debt from PCTs arising before 2011/12, and will have their own budgets from 2013/14; until then, consortia and PCTs must work together to 'reduce the risk for GP consortia that they could have responsibility for any post 2010/11 PCT defi cit unresolved at the point of PCT abolition'.
Total PCT allocations increase by 3 per cent
(£2.6bn), with a minimum increase of 2.5 per cent and a maximum of 4.9 per cent. Average growth in recurrent allocations is 2.2 per cent, with a minimum growth of 2 per cent. Recurrent allocations are based on a revised weighted capitation formula.
PCTs and SHAs will have to report their running costs, which must decrease by a third by 2014/15, including a 45 per cent cut in management costs. GP consortia will have an allowance for running costs possibly between £25 to £35 per head of population by 2014/15, depending on further work with the pathfi nders. As with FTs, NHS trusts will no longer be required to report their running costs.
The main source of capital will continue to be internally generated cash with additional fi nance provided by interest-bearing loans. No unspent capital from 2010/11 will be carried forward. No central capital budget programme for the NHS will exist in 2011/12. Capital for PCTs will be allocated on a case-by-case basis.
PCTs will be allocated £648m for social care, with an indicative allocation of £622m for 2012/13. This is in addition to £150m for reablement services included in PCTs' recurrent allocations for 2011/12 rising to £300m in 2012/13. They must transfer this to local authorities.
The NHS must continue its search for £20bn savings by 2014/15, but it now has until the end of that fi nancial year to do so.
Tariff:
A 2 per cent effi ciency requirement has been embedded in the tariff by:
• expanding the use of best practice tariffs to new service areas
Finance matters
Key points
• Any PCT debt from before 2011/12 will not be passed to GP consortia. The consortia will receive their own budgets from 2013/14
• PCTs’ allocations for 2011/12, which are published alongside the framework, have increased by 3 per cent
• A 2 per cent effi ciency requirement has been added to the national tariff
4 wellards.co.uk

• setting all tariffs at 1 per cent below the average• ensuring short hospital stays do not attract long-stay payments
Overall, 2011/12 tariff prices refl ect a 4 per cent effi ciency requirement: the embedded 2 per cent plus 2 per cent offsetting pay and price increases. This results in a 1.5 per cent tariff reduction between 2010/11 and 2011/12. This reduction will also apply to non-tariff services. Pay and price infl ation is assumed to be 2.5 per cent.
Hospitals will not be reimbursed for emergency readmissions within 30 days of discharge following an elective admission. All other readmissions within 30 days of discharge will be subject to locally agreed thresholds, set to deliver a 25 per cent reduction.
Among other changes:
• adult renal services will be brought under payment by results by mandating a transition path to national prices• currencies (units of care for which providers are funded) — but not prices — for adult and neonatal critical care will be mandated• currencies for smoking cessation will be introduced• a national currency for cystic fi brosis services will be mandated• a local currency for podiatry services will be developed• spinal and neurosciences will become eligible for top-up payments• providers may offer services at less than the mandatory tariff price where they and commissioners agree
Finance matters
5wellards.co.uk

The NHS outcomes framework will be used by the Health Secretary from 2012/13 to hold the NHS Commissioning Board to account for improving quality. It will comprise 'a small set of outcome goals or domains', with overarching indicators and a small set of improvement areas. Each domain will be supported by National Institute for Health and Clinical Excellence quality standards. The framework will not set ambitions for 2011/12, but NHS organisations should 'take heed of the direction of travel towards focusing on outcomes, collecting data and establishing baselines for all indicators'.
Current guidance on patient reported outcome measures (PROMs) will be revised, and proposals issued for extending their use, collection and validity across the NHS.
An information strategy will be published in early 2011.
Measures to strengthen patient choice by April 2011 include:
• enabling all patients referred for an outpatient appointment to choose a named consultant-led team• obliging all providers to accept patients referred to a named consultant-led team if clinically appropriate• providers' services being listed on choose and book in a way that enables them to book appointments with named consultant-led teams • from April 2011, patients should be offered greater choice of treatment and provider in some mental health services• during 2011, patients should be offered greater choice in diagnostic testing and post- diagnosis care• during 2011, choice should be introduced in care for long-term conditions as part of personalised care planning
Allowing patients to choose any willing provider for most NHS-funded services will be introduced 'in a phased manner'. PCTs will need to work with GP practices to prepare for introducing choice of GP practice from April 2012.
The pilot programme for personal health budgets will be continued and extended, with sites invited to express an interest.
The government is committed to upholding the NHS Constitution, which remains 'at the heart of the NHS system'.
Maintaining accountability
Key point
• An NHS outcomes framework will hold the NHS Commissioning Board to account for improving quality of commissioning health services
6 wellards.co.uk

Developing quality
Key point
• The framework pledges a number of clinical improvements, including the publication of a mental health strategy
Now-March 2011 PCTs to involve GP practices and
emerging consortia, with other
clinicians, in the 2011/12 contracting
round and the broader commissioning
cycle from 2011/12 onwards
December 2010 Initial GP consortia pathfi nders
identifi ed
January-March 2011 Delegated responsibilities of pathfi nder
consortia confi rmed with PCTs
January 2011-March 2012
Further pathfi nders identifi ed and
emerging consortia encouraged to
become increasingly involved in
commissioning and take on increasing
delegated responsibilities
In 2011/12NHS Commissioning Board set up in
shadow form as special health authority
June 2011 PCT clustering arrangements in place
April 2012 All GP practices in GP consortia and start of NHS Commissioning Board authorisation of consortia
NHS Commissioning Board established, takes over relevant responsibilities
SHAs abolished
April 2012-March 2013 NHS Commissioning Board to work with GP consortia that need further support to be ready to take on full statutory responsibilities
April 2013 Authorised GP consortia take on full statutory responsibilities
PCTs abolished
7wellards.co.uk
Commissioning transition timetable
Important commitments include:
• an expanded and stronger health visiting service, increasing numbers by 4,200 by April 2015• expanding the family nurse partnership programme for the most vulnerable fi rst-time teenage mothers and their children, more than doubling capacity to at least 13,000 by April 2015• assessing the needs of people with autism,
then planning and commissioning services to meet them• for people with dementia, early diagnosis and intervention, improved care in general hospitals and care homes and less use of antipsychotic medication
Measures intended to maintain quality improvements include:
• an expectation that providers should offer maximum waiting times to patients, with their compliance monitored• an expectation of improvement in A&E and ambulance trust indicators• all providers must eliminate mixed-sex accommodation and from April 2011 report any breaches, which will attract contract sanctions

• ensuring all stroke patients are admitted directly to a stroke unit, access timely scanning, are assessed for thrombolysis, receiving it if clinically indicated, plus development of early supported discharge arrangements and community specialist stroke rehabilitation• a mental health strategy will be published in early 2011• development of a new dental contract
Areas for improvement include:
• offering all people with diabetes screening for early detection of — and prompt treatment for — retinopathy, with commissioners and providers doing more to ensure availability of insulin pumps; PCTs should commission structured patient education for people newly diagnosed with diabetes, while providers must shorten length of stay, improve experience of care and ensure patients’ blood glucose is managed safely whilst foot complications are avoided• all regions should be moving trauma service provision into regional trauma
network confi gurations in 2010/11, with designated major trauma centres planning continuous provision of consultant-led trauma teams, immediate computerised tomography (CT) scan options and access to interventional radiology services for haemorrhage• developing chronic obstructive pulmonary disease (COPD) services in line with the recommendations from the consultation on a national strategy• NHS organisations should continue to maintain and develop pharmaceutical services, including local enhanced services to meet pharmaceutical needs; SHAs and PCTs should actively optimise use of medicines in people with newly diagnosed long-term conditions and target medicines use reviews, while evidence continues to build for providing public health services through community pharmacies• continuing implementation of the NHS abdominal aortic aneurysm national screening programme due for completion by the end of 2012/13
Developing quality
8 wellards.co.uk
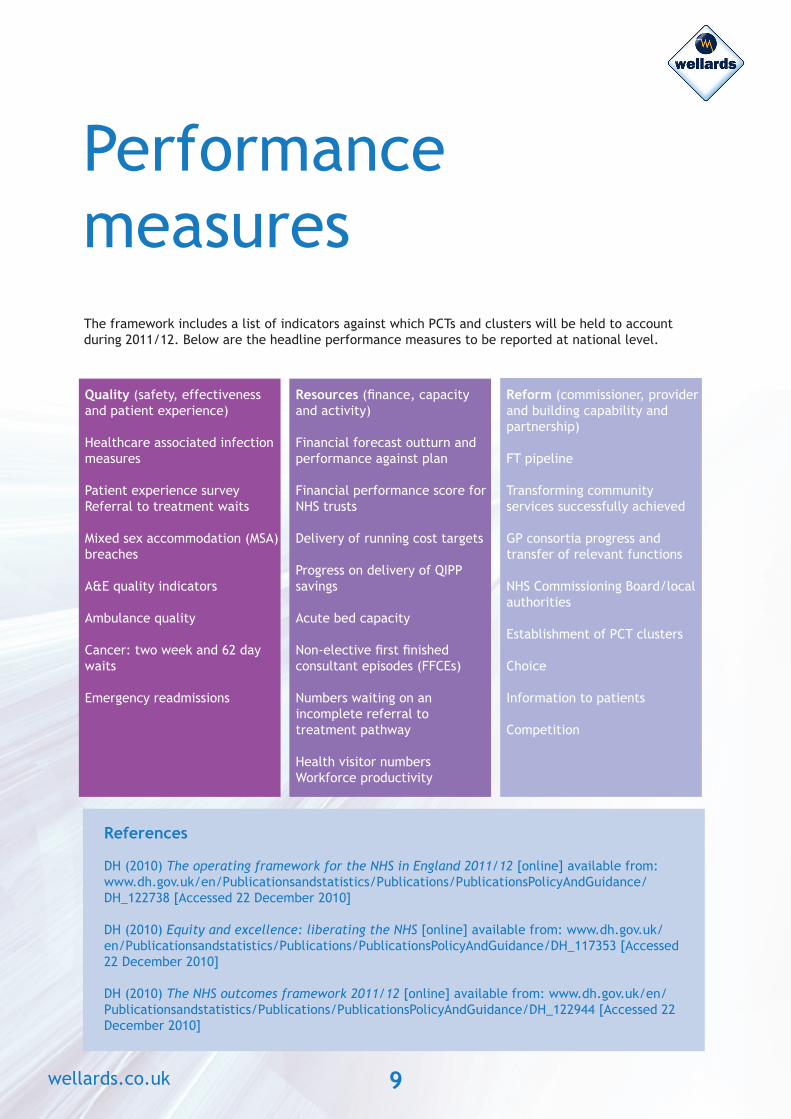
The framework includes a list of indicators against which PCTs and clusters will be held to account during 2011/12. Below are the headline performance measures to be reported at national level.
Performance measures
Quality (safety, effectiveness and patient experience)
Healthcare associated infection measures
Patient experience surveyReferral to treatment waits
Mixed sex accommodation (MSA) breaches
A&E quality indicators
Ambulance quality
Cancer: two week and 62 day waits
Emergency readmissions
Resources (fi nance, capacity and activity)
Financial forecast outturn and performance against plan
Financial performance score for NHS trusts
Delivery of running cost targets
Progress on delivery of QIPP savings
Acute bed capacity
Non-elective fi rst fi nished consultant episodes (FFCEs)
Numbers waiting on an incomplete referral to treatment pathway
Health visitor numbersWorkforce productivity
Reform (commissioner, provider and building capability and partnership)
FT pipeline
Transforming community services successfully achieved
GP consortia progress and transfer of relevant functions
NHS Commissioning Board/local authorities
Establishment of PCT clusters
Choice
Information to patients
Competition
References
DH (2010) The operating framework for the NHS in England 2011/12 [online] available from: www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_122738 [Accessed 22 December 2010]
DH (2010) Equity and excellence: liberating the NHS [online] available from: www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_117353 [Accessed 22 December 2010]
DH (2010) The NHS outcomes framework 2011/12 [online] available from: www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_122944 [Accessed 22 December 2010]
9wellards.co.uk