opening keynote “population management: the caremore experience" david ramirez, md, chief...
TRANSCRIPT
Population Management: The CareMore Experience
David Ramirez
Chief Quality Officer
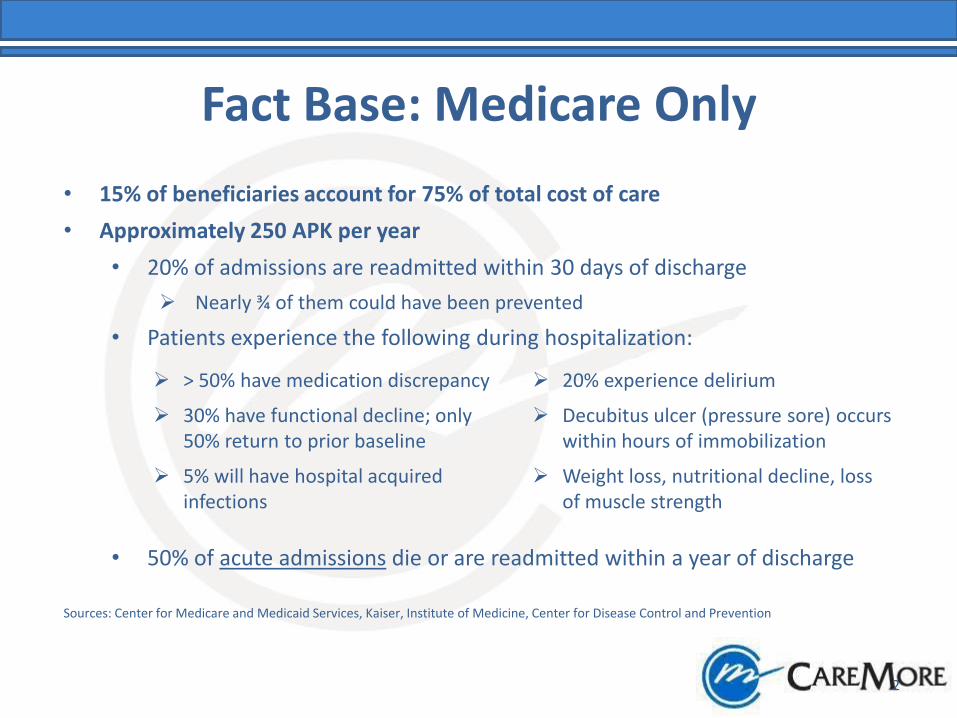
Fact Base: Medicare Only
2
• 15% of beneficiaries account for 75% of total cost of care
• Approximately 250 APK per year
• 20% of admissions are readmitted within 30 days of discharge
Nearly ¾ of them could have been prevented
• Patients experience the following during hospitalization:
• 50% of acute admissions die or are readmitted within a year of discharge
Sources: Center for Medicare and Medicaid Services, Kaiser, Institute of Medicine, Center for Disease Control and Prevention
> 50% have medication discrepancy 20% experience delirium
30% have functional decline; only 50% return to prior baseline
Decubitus ulcer (pressure sore) occurs within hours of immobilization
5% will have hospital acquired infections
Weight loss, nutritional decline, loss of muscle strength

Health Spending & Chronic Disease
• 15% of the population spends 70% of the dollars (Kaiser Permanente)
• 70% of all healthcare dollars are spent on chronic diseases (Agency for Healthcare Research and Quality)
• Five chronic diseases make up the vast majority of this category* - Diabetes - Congestive Heart Failure - Coronary Artery Disease - Asthma - Depression * Hypertension contributes to complications
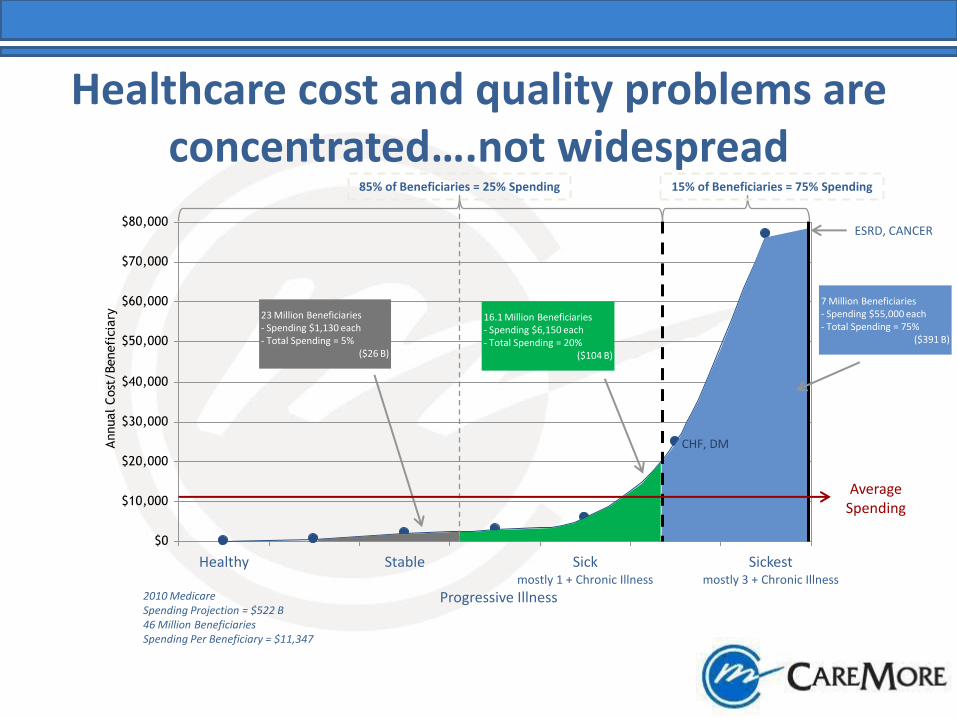
Healthcare cost and quality problems are concentrated….not widespread
Healthy Stable Sick Sickest mostly 1 + Chronic Illness mostly 3 + Chronic Illness
Progressive Illness 2010 Medicare Spending Projection = $522 B 46 Million Beneficiaries Spending Per Beneficiary = $11,347
$0
$10,000
$20,000
$30,000
$40,000
$50,000
$60,000
$70,000
$80,000
Annual
Cost
/Benefi
ciary 23 Million Beneficiaries
- Spending $1,130 each - Total Spending = 5%
($26 B)
16.1 Million Beneficiaries - Spending $6,150 each - Total Spending = 20%
($104 B)
7 Million Beneficiaries - Spending $55,000 each - Total Spending = 75%
($391 B)
Average Spending
CHF, DM
85% of Beneficiaries = 25% Spending 15% of Beneficiaries = 75% Spending
ESRD, CANCER

Community physicians work in parallel with CareMore Extensivists to provide a cohesive,
comprehensive solution
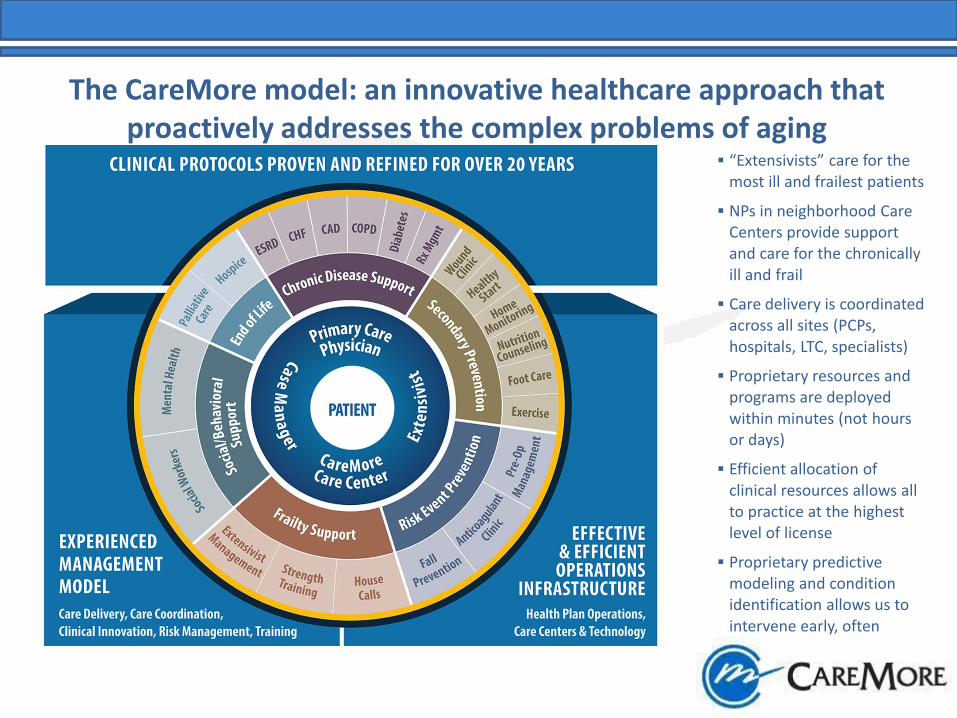
The CareMore model: an innovative healthcare approach that proactively addresses the complex problems of aging
“Extensivists” care for the most ill and frailest patients
NPs in neighborhood Care Centers provide support and care for the chronically ill and frail
Care delivery is coordinated across all sites (PCPs, hospitals, LTC, specialists)
Proprietary resources and programs are deployed within minutes (not hours or days)
Efficient allocation of clinical resources allows all to practice at the highest level of license
Proprietary predictive modeling and condition identification allows us to intervene early, often

CareMore’s operating principles and enabling capabilities coalesce to form a highly effective model of care
Operating Principles
Clinical Control - CareMore Extensivists determine when a patient requires proprietary services and programs
Speedy Deployment – Proprietary resources and programs must be available to adequately intervene and be deployed within minutes (not hours or days)
Efficient Allocation of Clinical Resources – Some types of physician labor is replaced with skilled, allied health professionals such as NPs, MAs, therapists and dieticians
Early, Proactive Intervention - Proprietary predictive modeling and condition identification resources allow us intervene early and often to prevent acute episodes and sentinel events
Intimacy of Contact – Management of complexity requires constant knowledge of the health condition
Key Enabling Capabilities
7
Predictive Modeling
Integrated IT Infrastructure
Longitudinal Patient Record
Point-of-care Decision Support
Evidence-based Protocols
Advanced Training

CareMore offers a broad range of SNPs geared toward the frail and elderly
ESRD
Chronic SNP
DIABETES
Chronic SNP
CONNECT Dual Eligible
SNP
TOUCH Institutional
SNP
BREATHE Pulmonary
Chronic SNP
HEART Cardiovascular
Chronic SNP

CareMore COPD Program
• Dedicated Nurse Practitioner lead
• Team approach coordinated with other providers
• Holistic management and education
• Protocols based on national clinical practice guidelines
9%
16%
18%
CareMore In Program
CareMore Not In Program
Medicare Average
COPD Readmissions

CareMore Wireless Monitoring Present State
• CHF: Wireless Scales
• HTN: Wireless BP Cuffs
• Benefits: Patient Compliance, Data Acquisition, Rapid Intervention
• Challenges: Patient Selection, False Alerts, Data Volume, Segmented Care

CareMore Wireless Monitoring Future State
• Integrated monitoring across disease states
• Selection of optimal patients
• Data management
• Provider alert management

CareMore – Sentrian COPD Program
• Identify-Monitor-Analyze-Act Model
• 1000 intervention patients over 12 months
• Use existing data to select optimal patients and wireless monitoring options
• Integrate monitoring across chronic diseases
• Continuous risk stratification
• Create rules for alerts

10,000 Member Initiative
• Goal = Proactively manage top 10% highest risk CareMore members
• Intervention = Early identification and referral to CareMore programs
• Approach = Develop inclusion/exclusion criteria, generate list from EDW, apply risk stratification criteria, prioritize outreach

Technology
EDW
FACETS
Rules Engine
(SAS, SQL, etc)
Criteria, Diagnostic Codes, Risk factors, Episodes, etc.
Criteria
Trigger List
Data Analytics
Analytics Overview

Population Management Overview
Chronic: Care Management Disease Management
Preventative: Member Services Clinical Outreach Pharmacy Outreach Med Therapy Mgmt CCC/ PCP visit Sales/Marketing/ Townhalls Patient Education
Episodic: PCP visit CCC visit ER/Inpatient visit Meds Reconciliation
Oversight: HEDIS QM submission STARs submission CAHPS HOS surveys Appeals Grievances
ACTIVITIES
Coordination
1. 2. 3
Prioritize 1. 2. 3
Categorize 1. 2. 3
Analyze Departments
Programs
Mu
ltip
le T
ou
chp
oin
ts
CRM
Integration Coordination
Risk
Patient Experience
Resource Management
Service Coordination List

CareMore Values
• Accountability
• Coordination
• Urgency to match care desired with care received