open wedge high tibial osteotomy with distal tubercle osteotomy...
TRANSCRIPT

Clinical StudyOpen Wedge High Tibial Osteotomy with Distal TubercleOsteotomy Lessens Change in Patellar Position
Hoon Park1 HyunWoo Kim2 Jin Hwa Kam2 and Dong Hoon Lee2
1Department of Orthopaedic Surgery Gangnam Severance Hospital Yonsei University College of Medicine 211 Eonju-roGangnam-gu Seoul 06273 Republic of Korea2Division of Orthopaedic Surgery Severance Childrenrsquos Hospital Yonsei University College of Medicine 50 Yonsei-roSeodaemun-gu Seoul 03722 Republic of Korea
Correspondence should be addressed to Dong Hoon Lee orthopaedeenavercom
Received 20 April 2017 Revised 8 June 2017 Accepted 14 June 2017 Published 18 July 2017
Academic Editor Magali Cucchiarini
Copyright copy 2017 Hoon Park et al This is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
The purpose of this study was to investigate the change in patellar position after open wedge high tibial osteotomy (OWHTO)with distal tubercle osteotomy (DTO) comparing outcomes of conventional OWHTO in young adults with proximal tibia varusdeformity but no arthritic manifestations Thirty-three patients (mean age 318 years) subjected to OWHTODTO were matchedwith 30 patients (mean age 335 years) undergoing conventional OWHTO Patellar position as measured in pre- and postoperativestanding lateral radiographs was compared Patellar height was assessed via Insall-Salvati ratio modified Insall-Salvati ratioBlackburne-Peel (BP) index Caton-Deschamps (CD) index and modified Miura-Kawamura index Computed tomography wasused to measure lateral patellar tilt and shift In the OWHTO group all patellar height indices decreased significantly followingsurgery Although mean values of BP and CD indices decreased significantly in the OWHTODTO group other determinantsof patellar height showed no significant postoperative differences Significant postoperative declines in average lateral patellar tiltwere also evident in both groups but pre- and postoperative lateral patellar shift did not differ significantly OWHTODTO can beperformed without significant changes in patellar height The results obtained support that OWHTODTO is suitable for relativelyyoung patients with proximal tibia vara but no arthritic change
1 Introduction
Genu varum deformity of the lower extremity results inabnormal load distribution across the knee joint andmay leadtomedial compartment joint osteoarthritis [1] Although var-iousmethods of osteotomy have emerged to correct proximaltibial varus deformities open wedge high tibial osteotomy(OWHTO) has gained popularity in recent years as thepreferred approach in relatively young patients with varusmalalignment and medial compartment knee osteoarthritis[2 3] Unfortunately change in patellofemoral indices (iepatellar height tilt and shift) is a potential postoperativecomplication of OWHTO [4ndash7] Such deviations resultingfrom distalization of the tibial tuberosity [6 8] may alterpatellofemoral biomechanics to culminate in patellofemoraljoint problems and difficulty in later total knee arthroplasty[9ndash12]
Technical modifications of OWHTO have been exten-sively studied in efforts to prevent change in patellar heightWhereas OWHTO undertaken below the tibial tuberosity isone option tomitigate the risk of patella infera this techniquehas the disadvantage of cortical bone involvement and slowhealing rate [13] Alternatively OWHTO with distal tubercleosteotomy (OWHTODTO) has been proposed to minimizeany impact on patellar height [8] Using this techniquewhich incorporates the tibial tubercle into the proximalplateau fragment patellar position is less vulnerable Previousstudies have proven that compared with OWHTO aloneOWHTODTO is effective in minimizing patellar height loss[8 14 15]
In active young adults with proximal tibial vara butno pain or arthritic change on medial side of knee it isparticularly important to minimize patellar position aftercorrecting the deformity To the best of our knowledge
HindawiBioMed Research InternationalVolume 2017 Article ID 4636809 10 pageshttpsdoiorg10115520174636809
2 BioMed Research International
however there have been no studies evaluating lateral incli-nation and deviation in patellar indices after OWHTO usingcomputed tomography (CT) Hence the purpose of thisstudy was to investigate the change in patellar positionafter corrective surgery comparing outcomes of these twosurgical techniques (OWHTO versus OWHTODTO) Weanticipated that OWHTODTO would prove superior toOWHTO in this regard
2 Materials and Methods
21 Study Patients This study was a retrospective compara-tive investigation approved by the Institutional Review Boardat our institution A total of 155 consecutive patients whohad undergone bilateral OWHTO or OWHTODTO foridiopathic proximal tibial vara between January 2011 andJune 2015 were identified by electronic search of medicalrecords Patients with available preoperative CT images andfollow-up CT images after index surgeries were includedAt our institution preoperative CT scans are done routinelyas part of surgical planning typically with follow-up CTimaging 6 months after surgery to evaluate locations andangles of osteotomies Both preoperative and follow-up CTscans were performed as dictated by patient managementprotocols of referring surgeons and were not confined tosymptomatic patients Inclusion criteria were as follows (1)skeletally mature patients younger than 40 years of age withcosmetic purpose (2) idiopathic proximal tibia vara withoutpain or arthritic change and (3) no history of fracture orligamentous injury congenital bony deformities or infec-tions of the lower extremity Patientswith patellofemoral jointsymptoms rheumatoid arthritis or limited range of motionwere excluded from the study
Ultimately 63 patients (126 tibias) were enrolled andstratified by surgical technique All patients underwent bilat-eral surgery but only the right tibia of each patient wasanalyzed to limit the number of variables A single surgeonperformed all surgeries The surgeon switched the surgicaltechnique during the study period Group 1 consisted of30 patients (30 tibias) who underwent OWHTO betweenJanuary 2011 and February 2013 Group 2 consisted of 33patients (33 tibias) who were treated with OWHTODTOfromMarch 2013 and June 2015 Preoperative data includingage sex and body mass index (BMI) were recorded in eachinstance
22 Surgical Technique Fixator-assisted high tibial osteot-omy was performed by one senior surgeon [16] All patientswere operated on in supine position using a conventionaloperating table and general anesthesia Initially a 25-cmoblique incision was made midway between the center ofthe tibial tuberosity and the posteromedial border of theproximal tibia starting 1 cm below the upper margin of thepes anserinus tendon then continuing proximally and inparallel with the posteromedial border of the tibia Carefuldissection is needed to expose the deep fascia over the pesanserinus and superficial fibers at the anterior margin ofthe medial collateral ligament (MCL) Once completing asharp L-shaped incision along anterior border of the MCL
and upper margin of the semitendinosus tendon the MCLwas raised and peeled off using a periosteal elevator Thefirst guide wire was then inserted toward a ldquosafe zonerdquowith a starting point 3mm below the upper margin of thesemitendinosus tendon and anterior one-third of the medialtibial surface [17] A second guide wire was also inserted 1 cmposterior to the first guide wire and advanced parallel to itunder fluoroscopic guidance so the osteotomy plane couldmirror the posterior tibial slope Finally a Mini-Hohmannretractor was inserted beneath MCL and multiple drill holeswere made along the superior margins of both guide wires
The first tibial osteotomy started at the center of themedial cortex and ran obliquely upward toward the fibularhead to about 2 cm below the lateral joint line The secondosteotomy involved a complete transverse cut of the posteriorcortex extending from the posteromedial to posterolateralborder The last osteotomy of anterior cortex was directedproximal to the tibial tuberosity in group 1 using a biplanarapproach in group 2 for technical reasons The latter com-menced at the anterior third of the main osteotomy makinga short beak distally screw fixation was not required distally(beneath pes anserinus tendon) unless the beak fracturedduring osteotomy (Figure 1)
After completing the osteotomy two 6-mm half-pinswere inserted at the medial aspect of the proximal tibia fortemporary fixation The half-pin inserted proximally wasplaced 1ndash15 cm distal to the joint line and parallel to theposterior cortex of the tibial shaft The distally inserted pinwas placed just anterior to the posterior tibial cortex Awedge-shaped spreader was then gently inserted into theosteotomy site and the gap was widened to correct the varusdeformity It is imperative to keep the knee fully extendedduring thismaneuver to avoid unwanted changes in posteriortibial slope Additionally these half-pins can also be usedto check on the changes in rotational alignment after varuscorrection The spreader was locked when sufficient varuscorrectionwas evident grossly A 15-cm carbon rodwith threeSchanz pin clamps was used to connect the two tibial half-pins
Keeping the fixator in place gaps were filled with hy-droxyapatite or szlig-tricalcium phosphate (Bongros CGBioSeongnam-si SouthKorea) or allograft cancellous bone chips(OSG-DualPor OssGen Gyungsan-si South Korea) A plate(TomoFix TomoFix Medial High Tibial Plate DePuy Syn-thes Raynham MA USA) inserted into anteromedial tibialsurface was then fixed in a less invasive manner using 50-mm locking screws In patients of group 2 (OWHTODTO)sustaining tibial tuberosity fractures tibial tubercle wascompressed against the distal tibia by anteroposterior coun-tersinking of a 45-mm cortical lag screw (Figure 2) Thewounds were irrigated and suction drains inserted
Postoperative management was the same for both groupsof patients From postoperative day 1 gentle active range-of-motion knee regimens and full weight bearing were allowedas tolerated
23 Radiographic Measures All radiologic measurementswere performed by two orthopedic residents who wereblinded to the study The measurements were independently
BioMed Research International 3
(a) (b) (c)
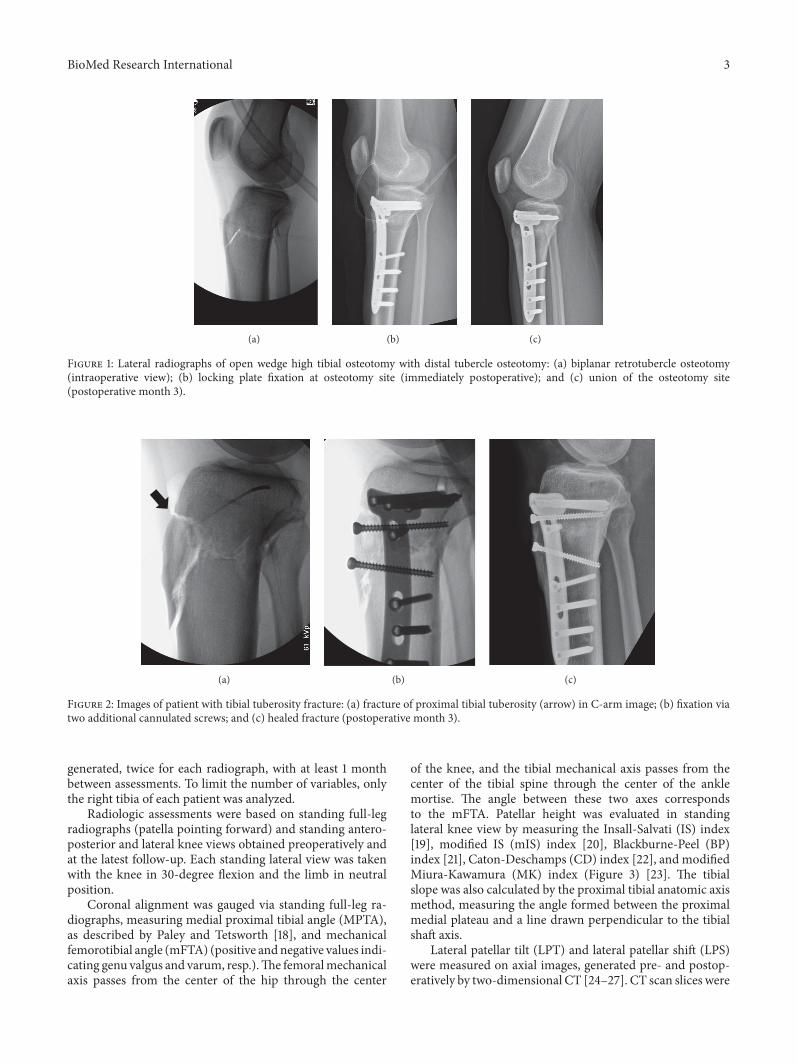
Figure 1 Lateral radiographs of open wedge high tibial osteotomy with distal tubercle osteotomy (a) biplanar retrotubercle osteotomy(intraoperative view) (b) locking plate fixation at osteotomy site (immediately postoperative) and (c) union of the osteotomy site(postoperative month 3)
(a) (b) (c)
Figure 2 Images of patient with tibial tuberosity fracture (a) fracture of proximal tibial tuberosity (arrow) in C-arm image (b) fixation viatwo additional cannulated screws and (c) healed fracture (postoperative month 3)
generated twice for each radiograph with at least 1 monthbetween assessments To limit the number of variables onlythe right tibia of each patient was analyzed
Radiologic assessments were based on standing full-legradiographs (patella pointing forward) and standing antero-posterior and lateral knee views obtained preoperatively andat the latest follow-up Each standing lateral view was takenwith the knee in 30-degree flexion and the limb in neutralposition
Coronal alignment was gauged via standing full-leg ra-diographs measuring medial proximal tibial angle (MPTA)as described by Paley and Tetsworth [18] and mechanicalfemorotibial angle (mFTA) (positive andnegative values indi-cating genu valgus and varum resp)The femoralmechanicalaxis passes from the center of the hip through the center
of the knee and the tibial mechanical axis passes from thecenter of the tibial spine through the center of the anklemortise The angle between these two axes correspondsto the mFTA Patellar height was evaluated in standinglateral knee view by measuring the Insall-Salvati (IS) index[19] modified IS (mIS) index [20] Blackburne-Peel (BP)index [21] Caton-Deschamps (CD) index [22] and modifiedMiura-Kawamura (MK) index (Figure 3) [23] The tibialslope was also calculated by the proximal tibial anatomic axismethod measuring the angle formed between the proximalmedial plateau and a line drawn perpendicular to the tibialshaft axis
Lateral patellar tilt (LPT) and lateral patellar shift (LPS)were measured on axial images generated pre- and postop-eratively by two-dimensional CT [24ndash27] CT scan slices were
4 BioMed Research International
a
b
Insall-Salvati ba
(a)
c
b
Modified Insall-Salvati bc
(b)
c
d
Blackburne-Peel dc
(c)
c
e
Caton-Deschamps ec
(d)
c
f
Modified Miura-Kawamura fc
(e)
Figure 3 Radiographic diagrams showing five indices measured to assess patellar height (a) Insall-Salvati (b) modified Insall-Salvati (c)Blackburne-Peel (d) Caton-Deschamps and (e) modified Miura-Kawamura 119886 diagonal patellar length 119887 patellar length 119888 length of thepatellar articular surface 119889 perpendicular distance between the proximal tibial articular surface and the inferior tip of patellar articularsurface 119890 distance from the anterosuperior border of the tibial plateau to the inferior tip of the patellar articular surface 119891 distance from aline perpendicular to the tibial diaphyseal line to the inferior tip of the patellar articular surface
focused on the central patella with hips flexed at 45 degreesand knees flexed at 30 degrees (Figure 4)
24 Statistical Analysis All statistical calculations reliedon standard software (SPSS v190 SPSS Inc Chicago ILUSA) All continuous variables were tested for normality viaShapiro-Wilk test and did not violate the normal distribu-tion assumption Studentrsquos paired 119905-test was used to assessdifferences between pre- and postoperative measures in eachgroup To compare changes in patellar position by operativegroup Studentrsquos independent 119905-test was applied Statisticalsignificance was set at 119901 lt 005 Changes in patellar heightand tibial slope and degrees of correction angle in the coronalplane (MPTA) were analyzed using Pearsonrsquos correlationcoefficient Inter- and intraobserver reliabilities were gaugedas well through intraclass correlation coefficients (ICCs)ICCs were interpreted as follows poor lt04 marginal gt04but lt075 and good gt075
3 Results
Baseline demographics as well as pre- and postoperativeMPTA and mFTA data are reported by operative method inTable 1 The two groups did not differ significantly in termsof age gender BMI or follow-up period There were nosignificant between-group differences with respect to meanpreoperative MPTA andmFTA or mean extent of correction
Pre- and postoperative patellar height indices tibial slopeand lateral patellar tilt and shift are shown by group inTable 2 None of the pre- and postoperative variables differedsignificantly
Patellar height and tibial slope measurements before andafter surgery for both groups are tabulated in Figure 5 Ingroup 1 (OWHTO) all patellar height indices including IS(119901 = 0003) mIS (119901 = 0007) BP (119901 lt 0001) CD (119901 lt0001) and MK index (119901 lt 0001) declined significantlyAlthough mean BP (119901 = 0023) and CD (119901 = 0009)
BioMed Research International 5
(a)
L M
(b)
L M
p
c
p
c
(c)
Figure 4 Methods of assessing lateral patellar tilt (LPT) and lateral patellar shift (LPS) (a) patient positioned for computed tomographyimaging with knee in 30 degrees of flexion (b) LPT defined as the angle between a line intersecting the widest bony structure of the patellaand a line tangential to the anterior femoral condylar surfaces (c) LPS defined as the ratio of distances 11990111990110158401198881198881015840 where 1198881198881015840 is the distancebetween the summits of the medial and lateral femoral condyles and 1199011199011015840 is the distance between the summit of the lateral femoral condyleand the point where a line from the lateral edge of the patella perpendicular to the line that passed through the summits of the femoralcondyles crosses that line L lateral M medial
Table 1 Demographics and correction angles by operative group
Variables OWHTO (119899 = 30) OWHTODTO (119899 = 33) 119901 valueAge (years) 328 plusmn 75 305 plusmn 80 018Gender (male female) 8 22 13 20 023Body mass index (kgm2) 233 plusmn 52 245 plusmn 50 052Preoperative MPTA (degrees) 818 plusmn 19 823 plusmn 23 030Postoperative MPTA (degrees) 881 plusmn 20 883 plusmn 24 063Correction of MPTA (degrees) 62 plusmn 21 60 plusmn 27 064Preoperative mFTA (degrees) minus60 plusmn 18 minus64 plusmn 30 044Postoperative mFTA (degrees) 08 plusmn 15 03 plusmn 18 024Correction of mFTA (degrees) 68 plusmn 23 77 plusmn 31 024Follow-up period (months) 324 plusmn 87 331 plusmn 29 068Values expressed as mean plusmn SD OWHTO open wedge high tibial osteotomy DTO distal tubercle osteotomy MPTA medial proximal tibial angle mFTAmechanical femorotibial angle
Table 2 Pre- and postoperative radiographic measurements by operative group
Variables OWHTO (119899 = 30) OWHTODTO (119899 = 33) 119901 valuePreoperative Insall-Salvati 102 plusmn 013 101 plusmn 023 0932Postoperative Insall-Salvati 097 plusmn 012 100 plusmn 014 0353Preoperative modified Insall-Salvati 148 plusmn 013 146 plusmn 016 0701Postoperative modified Insall-Salvati 140 plusmn 015 147 plusmn 017 0072Preoperative Blackburne-Peel 080 plusmn 011 079 plusmn 011 0800Postoperative Blackburne-Peel 071 plusmn 015 076 plusmn 015 0138Preoperative Caton-Deschamps 093 plusmn 008 090 plusmn 012 0237Postoperative Caton-Deschamps 083 plusmn 011 086 plusmn 014 0265Preoperative modified Miura-Kawamura 089 plusmn 008 084 plusmn 012 0077Postoperative modified Miura-Kawamura 081 plusmn 012 083 plusmn 016 0552Preoperative tibial slope (degrees) 83 plusmn 35 87 plusmn 39 0655Postoperative tibial slope (degrees) 111 plusmn 323 112 plusmn 416 0943Preoperative lateral patella tilt (degrees) 141 plusmn 247 145 plusmn 369 0582Postoperative lateral patella tilt (degrees) 121 plusmn 218 131 plusmn 398 0249Preoperative lateral patella shift 014 plusmn 003 015 plusmn 047 0493Postoperative lateral patella shift 013 plusmn 004 014 plusmn 005 0450Values expressed as mean plusmn SD OWHTO open wedge high tibial osteotomy DTO distal tubercle osteotomy
6 BioMed Research International
PreoperativePostoperative
PreoperativePostoperative
0
02
04
06
08
1
12
14In
sall-
Salv
ati
0
02
04
06
08
1
12
Cato
n-D
esch
amps
0
02
04
06
08
1
12
14
16
18
Mod
ified
Insa
ll-Sa
lvat
i
0
2
4
6
8
10
12
14
Tibi
al sl
ope (
degr
ees)
OWHTO OWHTODTOOWHTO OWHTODTO0
010203040506070809
1
Blac
kbur
ne-P
eel
0
02
04
06
08
1
12
Miu
ra-K
awam
ura
lowast lowast lowast
lowast
lowast
lowast lowast
Figure 5 Patellar height indices and tibial slope pre- and postoperatively charted by operative group OWHTO open wedge high tibialosteotomy DTO distal tubercle osteotomy lowastSignificant change after surgery (119901 lt 005)
indices decreased significantly in group 2 (OWHTODTO)other patellar height indices were not significantly altered bysurgery Neither group showed significant change in meantibial slope
Average LPT decreased significantly after surgery inboth groups However no statistical differences between pre-operative and postoperative LPS were evident (Figure 6)
We compared the amount of change between group 1 andgroup 2 (Table 3) The amount of change of mIS BP CDand MK indices significantly differed between two groupsBecause of the small number of subjects independent 119905-testpower calculation was carried out using Power Analysis andSample Size 11 for Windows software package (NCSS IncLLC Kaysville UT USA) and the power was 076 for mIS
index 041 for BP index 064 for CD index and 073 for MKindex between group 1 and group 2
There were no significant correlations in either groupwith respect to patellar height or tibial slope changes ordegree of correction angle in coronal plane (MPTA)
Bone union at osteotomy sites was achieved at an averageof 3 months in all patients A total of two complicationsoccurred in group 2 In these two patients the tibialtuberosity fractured during tuberosity osteotomy Remediedby fixation screws these fractures healed in 3 months Noother complications such as wound infection delayed unionor nonunion were seen
Interrater reliability of all patellar indices measuredwas confirmed using (ICCs) based on radiographs before
BioMed Research International 7
Table 3 The amount of change for radiographic measurements by operative group
Variables OWHTO (119899 = 30) OWHTODTO (119899 = 33) 119901 valueInsall-Salvati minus005 plusmn 008 minus002 plusmn 020 0408Modified Insall-Salvati minus008 plusmn 014 000 plusmn 009 0002Blackburne-Peel minus009 plusmn 009 minus004 plusmn 013 0037Caton-Deschamps minus010 plusmn 009 minus004 plusmn 011 0008Modified Miura-Kawamura minus008 plusmn 009 minus001 plusmn 012 0010Tibial slope (degrees) 078 plusmn 306 047 plusmn 395 0705Lateral patella tilt (degrees) minus206 plusmn 176 minus141 plusmn 214 0218Lateral patella shift minus001 plusmn 003 minus001 plusmn 003 0661Values expressed as mean plusmn SD OWHTO open wedge high tibial osteotomy DTO distal tubercle osteotomy
and after surgery ICC ranges for intraobserver (075ndash091)and interobserver (072ndash09) reliabilities were comparable tothose of previous studies [14 28]
4 Discussion
Introduction of OWHTODTO was fueled by efforts tominimize surgery-related loss in patellar height and preventsubsequent patellofemoral problems [8] Several studiesoffer proof that this technique is effective in minimizingpostoperative patellar height change citing clinical out-comes comparable to conventional OWHTO in patients withosteoarthritis of the medial tibiofemoral compartment andvarus malalignment [8 14 15 29ndash31] However there wasno study investigating the surgical results of OWHTODTOin patients with normal knee Special concerns in this pop-ulation include unsightly aesthetics and pain or discomfortupon kneeling after surgery Therefore we have used thistechnique to correct proximal tibial varus deformities inyoung patients without pain or arthritic joints provingthat diminished patellar height is avoidable through thisapproach Considering the positional changes of the patellafollowing conventionalOWHTOmay induce new symptomsthese concerns will be addressed by OWHTODTO
In the present study we found significant postoperativedecreases in IS and mIS indices of the OWHTO groupwhereas these ratios were unchanged in the OWHTODTOgroup Outcomes herein were aligned with previous studiesthat similarly utilized these ratios to evaluate patellar height[14 15 29] Both IS and mIS are indirect measures of patellarheight any change reflecting altered patellar tendon length[14 32] Any slackening or shortening of patellar tendon thusimplied may be explained by intratendinous fibrosis or adhe-sions of proximal tuberosity following OWHTO whereas theextensor mechanism remains intact after OWHTODTO
Although there were significant postoperative declines inBP and CD indices of both groups the MK index of theOWHTODTO group was unchanged Still only one otherstudy corroborates our results [14]Most earlier investigationshave recorded no significant changes in BP and CD indicesafter OWHTODTO [8 15 29 30] This discrepancy may bedue to the method of measurement Both BP and CD indiceshave been viewed as highly reliable gauges of patellar height[28 33] but their dependency on joint line is disadvanta-geous given tibial plateau as a reference Because tibial slope
OWHTO OWHTODTO
PreoperativePostoperative
0
005
01
015
02
025
Late
ral p
atel
la sh
ift
0
2
4
6
8
10
12
14
16
18
20
Late
ral p
atel
la ti
lt (d
egre
es)
lowast
lowast
Figure 6 Lateral patellar tilt and lateral patellar shift pre- andpostoperatively charted by operative group OWHTO open wedgehigh tibial osteotomy DTO distal tubercle osteotomy lowastSignificantchange after surgery (119901 lt 005)
decreased postoperatively in both arms of our study evenminimal deviations in tibial slope may thus have bearing Weagree with other investigators that BP and CD indices shouldnot be relied upon in surgical procedures involving proximaltibia [23 32] In our opinion the decrease seen in MK index
8 BioMed Research International
reflects a true reduction in patellar height because MK indexis independent with the change of tibial slope
Although various radiographic techniques (based onaxial radiography CT or MRI) have been described forevaluating patellar inclination [34] use of LPT and LPSafter OWHTODTO has not previously been investigatedPrevious publications studying changes in LPT and LPS afterOWHTO have relied on axial radiography of load-bearingpatellofemoral joints (Delgado-Martins method) [7 24 3536] However determinations rendered by axial radiographymay be not accurate due to overlapping of images difficultyin positioning the leg and incidental angles of X-ray beams[37 38] CT imaging of contracted quadriceps muscle mayserve better in confirming patellar position [25 34 37 39]Consequently we used axial CT images in supine positionwith the knee in 30 degrees of flexion to measure LPT andLPS
Ultimately we found that LPT declined significantlyfor both procedures but the reductions did not differsignificantly by operative group Our findings followingOWHTO were consistent with those of previous stud-ies [35 36] whereby lessening of LPT was attributed toincreased lateral pull on the patella Although we expectedthat OWHTODTO would prevent any changes in LPTand LPS LPT surprisingly showed significant decline afterOWHTODTO as well One possible explanation for this isthat a change in mechanical axis may affect the inclinationof patella For another reason the change of tibial rotationafter OWHTOmay affect the LPT Previous studies reportedOWHTO made significant internal axial rotation of the tibia[40 41] However there was no change on tibial rotation aftervarus correction because we used two half-pins to check thechange of rotational alignment in the operating room
In our analysis no significant correlations emerged withrespect to change in patellar height change in tibial slopeor correction angle degree Prior reports have indicated thatOWHTODTO ismore effective than conventional OWHTOin patients requiring large (gt10-degree) angular corrections[8 14 15 30] However we could provide corroborationbecause correction angles for most of our patients werelt10 degrees and the surgical goal was to restore neutralalignment Hence the protective effect of OWHTODTO onpatellar height after large angular correction (gt10 degrees)could not be fully evaluated by this study
There were two tibial tuberosity fractures in OWHTODTO group Only one previous literature reported samesurgical complications [8]Therewas no such complication inother reports using OWHTODTO [14 15 29 30]Thereforeit seems that tibial tuberosity fracture is related to mistakeof surgical procedure not the degrees of correction angleAdditionally in our study such fractures occurred at an earlystage in our learning curve and healed well with additionalscrew fixation Eventually we think that tibial tuberosityfracture is easily preventable with caution leaving at least a1-cm thickness on the proximal tuberosity fragment
Our study has some limitations First it is a retrospectiveinvestigation and not a randomized trial Also the twooperative groups reflected a shift in surgical technique ratherthan pure randomization Nevertheless the two groups were
well matched at baseline in terms of preoperative variablesAnother limitation was that blinding of the OWHTODTOarm was not feasible when measuring radiologic param-eters postoperatively even if two independent orthopedicresidents participated Finally radiographic parameters werethe primary focus To investigate the relationship betweenradiologic findings and clinical outcomes a well-plannedfuture prospective study is needed
There are various methods for correcting proximal tibialvara deformity and best surgical techniquemust be individu-alized Compared to conventional OWHTO OWHTODTOdid not influence patella height associated with the procedureand was considered an useful method to preserve patellaheight
Ethical Approval
This study was conducted following the approval of Institu-tional Review Board of Severance Hospital Yonsei UniversityCollege of Medicine (IRB number 4-2015-0796)
Conflicts of Interest
The authors declare that there are no conflicts of interest toreport regarding the work and publication of this study
Acknowledgments
The authors thank Dr Sung Min Kim and Jung Woo Lee forthe data measurement of the patients
References
[1] W Strecker ldquoPlanning Analysis of Knee-Adjacent DeformitiesrdquoEuropean Journal of Trauma and Emergency Surgery vol 33 no6 pp 662ndash668 2007
[2] R Rossi D E Bonasia and A Amendola ldquoThe Role of HighTibial Osteotomy in the Varus Kneerdquo American Academy ofOrthopaedic Surgeon vol 19 no 10 pp 590ndash599 2011
[3] R K Marti R A W Verhagen G M M J Kerkhoffs andT M Moojen ldquoProximal tibial varus osteotomy Indicationstechnique and five to twenty-one-year resultsrdquo Journal of Boneand Joint Surgery - Series A vol 83 no 2 pp 164ndash170 2001
[4] H El-Azab P Glabgly J Paul A B Imhoff and S Hinterwim-mer ldquoPatellar height and posterior tibial slope after open- andclosed-wedge high tibial osteotomy A radiological study on 100patientsrdquoAmerican Journal of Sports Medicine vol 38 no 2 pp323ndash329 2010
[5] B P Kaper R B Bourne C H Rorabeck and S J MacDonaldldquoPatellar infera after high tibial osteotomyrdquo Journal of Arthro-plasty vol 16 no 2 pp 168ndash173 2001
[6] D Tigani D Ferrari P Trentani G Barbanti-Brodano and FTrentani ldquoPatellar height after high tibial osteotomyrdquo Interna-tional Orthopaedics vol 24 no 6 pp 331ndash334 2001
[7] J-H Yang S-H Lee K S Nathawat S-H Jeon and K-JOh ldquoThe effect of biplane medial opening wedge high tibialosteotomy on patellofemoral joint indicesrdquo Knee vol 20 no 2pp 128ndash132 2013
[8] R D A Gaasbeek H Sonneveld R J Van Heerwaarden W CH Jacobs and A B Wymenga ldquoDistal tuberosity osteotomy in
BioMed Research International 9
open wedge high tibial osteotomy can prevent patella infera Anew techniquerdquo Knee vol 11 no 6 pp 457ndash461 2004
[9] C M Rodner D J Adams V Diaz-Doran et al ldquoMedialopeningwedge tibial osteotomy and the sagittal planeThe effectof increasing tibial slope on tibiofemoral contact pressurerdquoAmerican Journal of SportsMedicine vol 34 no 9 pp 1431ndash14412006
[10] R E Windsor J N Insall and K G Vince ldquoTechnicalconsiderations of total knee arthroplasty after proximal tibialosteotomyrdquo Journal of Bone and Joint Surgery - Series A vol 70no 4 pp 547ndash555 1988
[11] H E Figgie III V M Goldberg K G Heiple H S MollerIII and N H Gordon ldquoThe influence of tibial-patellofemorallocation on function of the knee in patients with the posteriorstabilized condylar knee prosthesisrdquo Journal of Bone and JointSurgery - Series A vol 68 no 7 pp 1035ndash1040 1986
[12] K Kim D Kim S Song S Lee and D Bae ldquoMedialOpen-Wedge High Tibial Osteotomy May Adversely Affect thePatellofemoral Jointrdquo Arthroscopy The Journal of Arthroscopicamp Related Surgery vol 33 no 4 pp 811ndash816 2017
[13] J S Shim S H Lee H J Jung and H I Lee ldquoHightibial open wedge osteotomy below the tibial tubercle Clinicaland radiographic resultsrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 1 pp 57ndash63 2013
[14] P D Longino T B Birmingham W J Schultz R F Moyerand J R Giffin ldquoCombined tibial tubercle osteotomy withmedial openingwedge high tibial osteotomyminimizes changesin patellar height A prospective cohort study with historicalcontrolsrdquo American Journal of Sports Medicine vol 41 no 12pp 2849ndash2857 2013
[15] S Keyhani M R Abbasian S M Kazemi et al ldquoModifiedretro-tubercle opening-wedge versus conventional high tibialosteotomyrdquo Orthopedics vol 34 no 2 2011
[16] D H Lee K J Ryu H H Kim S Soung and S Shin ldquoFixator-assisted Technique Enables Less Invasive Plate Osteosynthesisin Medial Opening-wedge High Tibial Osteotomy A NovelTechniquerdquo Clinical Orthopaedics and Related Research vol473 no 10 pp 3133ndash3142 2015
[17] S B Han D H Lee G M Shetty D J Chae J G Songand K W Nha ldquoA ldquosafe zonerdquo in medial open-wedge hightibia osteotomy to prevent lateral cortex fracturerdquoKnee SurgerySports Traumatology Arthroscopy vol 21 no 1 pp 90ndash95 2013
[18] D Paley and K Tetsworth ldquoMechanical axis deviation ofthe lower limbs Preoperative planning of uniapical angulardeformities of the tibia or femurrdquo Clinical Orthopaedics andRelated Research no 280 pp 48ndash64 1992
[19] J Insall and E Salvati ldquoPatella position in the normal kneejointrdquo Radiology vol 101 no 1 pp 101ndash104 1971
[20] R P Grelsamer and S Meadows ldquoThe modified Insall-Salvatiratio for assessment of patellar heightrdquo Clinical Orthopaedicsand Related Research no 282 pp 170ndash176 1992
[21] J S Blackburne and T E Peel ldquoA new method of measuringpatellar heightrdquo J Bone Joint Surg Br vol 59 no 2 pp 241-2421977
[22] J Caton G Deschamps P Chambat J L Lerat and HDejour ldquoPatella infera Apropos of 128 casesrdquo Rev Chir OrthopReparatrice Appar Mot vol 68 no 5 pp 317ndash325 1982
[23] H Miura H Kawamura R Nagamine K Urabe and YIwamoto ldquoIs patellar height really lower after high tibialosteotomyrdquo Fukuoka igaku zasshi = Hukuoka acta medica vol88 no 6 pp 261ndash266 1997
[24] H Delgado-Martins ldquoThe bicondylo-patellar angle as a mea-sure of patellar tiltingrdquo Archives of Orthopaedic and TraumaticSurgery vol 96 no 4 pp 303-304 1980
[25] V Vahasarja P Lanning S Lahde and W Serlo ldquoAxialradiography or CT in the measurement of patellofemoralmalalignment indices in children and adolescentsrdquo ClinicalRadiology vol 51 no 9 pp 639ndash643 1996
[26] U M Kujala K Osterman M Kormano M Komu and DSchlenzka ldquoPatellar motion analyzed by magnetic resonanceimagingrdquo Acta Orthopaedica vol 60 no 1 pp 13ndash16 1989
[27] C A Laurin R Dussault and H P Levesque ldquoThe tan-gential X-ray investigation of the patellofemoral joint X-raytechnique diagnostic criteria and their interpretationrdquo ClinicalOrthopaedics and Related Research no 144 pp 16ndash26 1979
[28] R Seil B Muller T Georg D Kohn and S Rupp ldquoReliabilityand interobserver variability in radiological patellar heightratiosrdquo Knee Surgery Sports Traumatology Arthroscopy vol 8no 4 pp 231ndash236 2000
[29] N Elmali I Esenkaya M Can and M Karakaplan ldquoMono-planar versus biplanar medial open-wedge proximal tibialosteotomy for varus gonarthrosis A comparison of clinicaland radiological outcomesrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 12 pp 2689ndash2695 2013
[30] S Hinterwimmer K Beitzel J Paul et al ldquoControl of posteriortibial slope and patellar height in open-wedge valgus high tibialosteotomyrdquo American Journal of Sports Medicine vol 39 no 4pp 851ndash856 2011
[31] S Hopwood W Khan and S Agarwal ldquoThe biplanar openwedge high tibial osteotomy preserving the tibial tuberclerdquoJournal of Orthopaedic Science vol 21 no 6 pp 786ndash790 2016
[32] H Kesmezacar R Erginer T Ogut A Seyahi M Babacan andY Tenekecioglu ldquoEvaluation of patellar height and measure-ment methods after valgus high tibial osteotomyrdquo Knee SurgerySports Traumatology Arthroscopy vol 13 no 7 pp 539ndash5442005
[33] B A Rogers P Thornton-Bott S R Cannon and T W RBriggs ldquoInterobserver variation in the measurement of patellarheight after total knee arthroplastyrdquo Journal of Bone and JointSurgery - Series B vol 88 no 4 pp 484ndash488 2006
[34] R P Grelsamer C H Weinstein J Gould and A DubeyldquoPatellar tilt The physical examination correlates with MRimagingrdquo Knee vol 15 no 1 pp 3ndash8 2008
[35] R Gaasbeek R Welsing M Barink N Verdonschot andA Van Kampen ldquoThe influence of open and closed hightibial osteotomy on dynamic patellar tracking A biomechanicalstudyrdquo Knee Surgery Sports Traumatology Arthroscopy vol 15no 8 pp 978ndash984 2007
[36] H Bito R Takeuchi K Kumagai et al ldquoOpening wedge hightibial osteotomy affects both the lateral patellar tilt and patellarheightrdquo Knee Surgery Sports Traumatology Arthroscopy vol 18no 7 pp 955ndash960 2010
[37] T Sasaki and T Yagi ldquoSubluxation of the patella - Investigationby computerized tomographyrdquo International Orthopaedics vol10 no 2 pp 115ndash120 1986
[38] F Boven M-A Bellemans J Geurts and R PotvliegeldquoA comparative study of the patello-femoral joint on axialroentgenogram axial arthrogram and computed tomographyfollowing arthrographyrdquo Skeletal Radiology vol 8 no 3 pp179ndash181 1982
[39] A D Delgado-Martınez C Estrada E C Rodrıguez-MerchanM Atienza and J M Ordonez ldquoCT scanning of the
10 BioMed Research International
patellofemoral joint The quadriceps relaxed or contractedrdquoInternational Orthopaedics vol 20 no 3 pp 159ndash162 1996
[40] S Hinterwimmer M J Feucht J Paul et al ldquoAnalysis of theeffects of high tibial osteotomy on tibial rotationrdquo InternationalOrthopaedics vol 40 no 9 pp 1849ndash1854 2016
[41] K-M Jang J-H Lee H-J Park J L Kim and S-B HanldquoUnintended Rotational Changes of the Distal Tibia AfterBiplane Medial Open-Wedge High Tibial Osteotomyrdquo Journalof Arthroplasty vol 31 no 1 pp 59ndash63 2016
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 BioMed Research International
however there have been no studies evaluating lateral incli-nation and deviation in patellar indices after OWHTO usingcomputed tomography (CT) Hence the purpose of thisstudy was to investigate the change in patellar positionafter corrective surgery comparing outcomes of these twosurgical techniques (OWHTO versus OWHTODTO) Weanticipated that OWHTODTO would prove superior toOWHTO in this regard
2 Materials and Methods
21 Study Patients This study was a retrospective compara-tive investigation approved by the Institutional Review Boardat our institution A total of 155 consecutive patients whohad undergone bilateral OWHTO or OWHTODTO foridiopathic proximal tibial vara between January 2011 andJune 2015 were identified by electronic search of medicalrecords Patients with available preoperative CT images andfollow-up CT images after index surgeries were includedAt our institution preoperative CT scans are done routinelyas part of surgical planning typically with follow-up CTimaging 6 months after surgery to evaluate locations andangles of osteotomies Both preoperative and follow-up CTscans were performed as dictated by patient managementprotocols of referring surgeons and were not confined tosymptomatic patients Inclusion criteria were as follows (1)skeletally mature patients younger than 40 years of age withcosmetic purpose (2) idiopathic proximal tibia vara withoutpain or arthritic change and (3) no history of fracture orligamentous injury congenital bony deformities or infec-tions of the lower extremity Patientswith patellofemoral jointsymptoms rheumatoid arthritis or limited range of motionwere excluded from the study
Ultimately 63 patients (126 tibias) were enrolled andstratified by surgical technique All patients underwent bilat-eral surgery but only the right tibia of each patient wasanalyzed to limit the number of variables A single surgeonperformed all surgeries The surgeon switched the surgicaltechnique during the study period Group 1 consisted of30 patients (30 tibias) who underwent OWHTO betweenJanuary 2011 and February 2013 Group 2 consisted of 33patients (33 tibias) who were treated with OWHTODTOfromMarch 2013 and June 2015 Preoperative data includingage sex and body mass index (BMI) were recorded in eachinstance
22 Surgical Technique Fixator-assisted high tibial osteot-omy was performed by one senior surgeon [16] All patientswere operated on in supine position using a conventionaloperating table and general anesthesia Initially a 25-cmoblique incision was made midway between the center ofthe tibial tuberosity and the posteromedial border of theproximal tibia starting 1 cm below the upper margin of thepes anserinus tendon then continuing proximally and inparallel with the posteromedial border of the tibia Carefuldissection is needed to expose the deep fascia over the pesanserinus and superficial fibers at the anterior margin ofthe medial collateral ligament (MCL) Once completing asharp L-shaped incision along anterior border of the MCL
and upper margin of the semitendinosus tendon the MCLwas raised and peeled off using a periosteal elevator Thefirst guide wire was then inserted toward a ldquosafe zonerdquowith a starting point 3mm below the upper margin of thesemitendinosus tendon and anterior one-third of the medialtibial surface [17] A second guide wire was also inserted 1 cmposterior to the first guide wire and advanced parallel to itunder fluoroscopic guidance so the osteotomy plane couldmirror the posterior tibial slope Finally a Mini-Hohmannretractor was inserted beneath MCL and multiple drill holeswere made along the superior margins of both guide wires
The first tibial osteotomy started at the center of themedial cortex and ran obliquely upward toward the fibularhead to about 2 cm below the lateral joint line The secondosteotomy involved a complete transverse cut of the posteriorcortex extending from the posteromedial to posterolateralborder The last osteotomy of anterior cortex was directedproximal to the tibial tuberosity in group 1 using a biplanarapproach in group 2 for technical reasons The latter com-menced at the anterior third of the main osteotomy makinga short beak distally screw fixation was not required distally(beneath pes anserinus tendon) unless the beak fracturedduring osteotomy (Figure 1)
After completing the osteotomy two 6-mm half-pinswere inserted at the medial aspect of the proximal tibia fortemporary fixation The half-pin inserted proximally wasplaced 1ndash15 cm distal to the joint line and parallel to theposterior cortex of the tibial shaft The distally inserted pinwas placed just anterior to the posterior tibial cortex Awedge-shaped spreader was then gently inserted into theosteotomy site and the gap was widened to correct the varusdeformity It is imperative to keep the knee fully extendedduring thismaneuver to avoid unwanted changes in posteriortibial slope Additionally these half-pins can also be usedto check on the changes in rotational alignment after varuscorrection The spreader was locked when sufficient varuscorrectionwas evident grossly A 15-cm carbon rodwith threeSchanz pin clamps was used to connect the two tibial half-pins
Keeping the fixator in place gaps were filled with hy-droxyapatite or szlig-tricalcium phosphate (Bongros CGBioSeongnam-si SouthKorea) or allograft cancellous bone chips(OSG-DualPor OssGen Gyungsan-si South Korea) A plate(TomoFix TomoFix Medial High Tibial Plate DePuy Syn-thes Raynham MA USA) inserted into anteromedial tibialsurface was then fixed in a less invasive manner using 50-mm locking screws In patients of group 2 (OWHTODTO)sustaining tibial tuberosity fractures tibial tubercle wascompressed against the distal tibia by anteroposterior coun-tersinking of a 45-mm cortical lag screw (Figure 2) Thewounds were irrigated and suction drains inserted
Postoperative management was the same for both groupsof patients From postoperative day 1 gentle active range-of-motion knee regimens and full weight bearing were allowedas tolerated
23 Radiographic Measures All radiologic measurementswere performed by two orthopedic residents who wereblinded to the study The measurements were independently
BioMed Research International 3
(a) (b) (c)
Figure 1 Lateral radiographs of open wedge high tibial osteotomy with distal tubercle osteotomy (a) biplanar retrotubercle osteotomy(intraoperative view) (b) locking plate fixation at osteotomy site (immediately postoperative) and (c) union of the osteotomy site(postoperative month 3)
(a) (b) (c)
Figure 2 Images of patient with tibial tuberosity fracture (a) fracture of proximal tibial tuberosity (arrow) in C-arm image (b) fixation viatwo additional cannulated screws and (c) healed fracture (postoperative month 3)
generated twice for each radiograph with at least 1 monthbetween assessments To limit the number of variables onlythe right tibia of each patient was analyzed
Radiologic assessments were based on standing full-legradiographs (patella pointing forward) and standing antero-posterior and lateral knee views obtained preoperatively andat the latest follow-up Each standing lateral view was takenwith the knee in 30-degree flexion and the limb in neutralposition
Coronal alignment was gauged via standing full-leg ra-diographs measuring medial proximal tibial angle (MPTA)as described by Paley and Tetsworth [18] and mechanicalfemorotibial angle (mFTA) (positive andnegative values indi-cating genu valgus and varum resp)The femoralmechanicalaxis passes from the center of the hip through the center
of the knee and the tibial mechanical axis passes from thecenter of the tibial spine through the center of the anklemortise The angle between these two axes correspondsto the mFTA Patellar height was evaluated in standinglateral knee view by measuring the Insall-Salvati (IS) index[19] modified IS (mIS) index [20] Blackburne-Peel (BP)index [21] Caton-Deschamps (CD) index [22] and modifiedMiura-Kawamura (MK) index (Figure 3) [23] The tibialslope was also calculated by the proximal tibial anatomic axismethod measuring the angle formed between the proximalmedial plateau and a line drawn perpendicular to the tibialshaft axis
Lateral patellar tilt (LPT) and lateral patellar shift (LPS)were measured on axial images generated pre- and postop-eratively by two-dimensional CT [24ndash27] CT scan slices were
4 BioMed Research International
a
b
Insall-Salvati ba
(a)
c
b
Modified Insall-Salvati bc
(b)
c
d
Blackburne-Peel dc
(c)
c
e
Caton-Deschamps ec
(d)
c
f
Modified Miura-Kawamura fc
(e)
Figure 3 Radiographic diagrams showing five indices measured to assess patellar height (a) Insall-Salvati (b) modified Insall-Salvati (c)Blackburne-Peel (d) Caton-Deschamps and (e) modified Miura-Kawamura 119886 diagonal patellar length 119887 patellar length 119888 length of thepatellar articular surface 119889 perpendicular distance between the proximal tibial articular surface and the inferior tip of patellar articularsurface 119890 distance from the anterosuperior border of the tibial plateau to the inferior tip of the patellar articular surface 119891 distance from aline perpendicular to the tibial diaphyseal line to the inferior tip of the patellar articular surface
focused on the central patella with hips flexed at 45 degreesand knees flexed at 30 degrees (Figure 4)
24 Statistical Analysis All statistical calculations reliedon standard software (SPSS v190 SPSS Inc Chicago ILUSA) All continuous variables were tested for normality viaShapiro-Wilk test and did not violate the normal distribu-tion assumption Studentrsquos paired 119905-test was used to assessdifferences between pre- and postoperative measures in eachgroup To compare changes in patellar position by operativegroup Studentrsquos independent 119905-test was applied Statisticalsignificance was set at 119901 lt 005 Changes in patellar heightand tibial slope and degrees of correction angle in the coronalplane (MPTA) were analyzed using Pearsonrsquos correlationcoefficient Inter- and intraobserver reliabilities were gaugedas well through intraclass correlation coefficients (ICCs)ICCs were interpreted as follows poor lt04 marginal gt04but lt075 and good gt075
3 Results
Baseline demographics as well as pre- and postoperativeMPTA and mFTA data are reported by operative method inTable 1 The two groups did not differ significantly in termsof age gender BMI or follow-up period There were nosignificant between-group differences with respect to meanpreoperative MPTA andmFTA or mean extent of correction
Pre- and postoperative patellar height indices tibial slopeand lateral patellar tilt and shift are shown by group inTable 2 None of the pre- and postoperative variables differedsignificantly
Patellar height and tibial slope measurements before andafter surgery for both groups are tabulated in Figure 5 Ingroup 1 (OWHTO) all patellar height indices including IS(119901 = 0003) mIS (119901 = 0007) BP (119901 lt 0001) CD (119901 lt0001) and MK index (119901 lt 0001) declined significantlyAlthough mean BP (119901 = 0023) and CD (119901 = 0009)
BioMed Research International 5
(a)
L M
(b)
L M
p
c
p
c
(c)
Figure 4 Methods of assessing lateral patellar tilt (LPT) and lateral patellar shift (LPS) (a) patient positioned for computed tomographyimaging with knee in 30 degrees of flexion (b) LPT defined as the angle between a line intersecting the widest bony structure of the patellaand a line tangential to the anterior femoral condylar surfaces (c) LPS defined as the ratio of distances 11990111990110158401198881198881015840 where 1198881198881015840 is the distancebetween the summits of the medial and lateral femoral condyles and 1199011199011015840 is the distance between the summit of the lateral femoral condyleand the point where a line from the lateral edge of the patella perpendicular to the line that passed through the summits of the femoralcondyles crosses that line L lateral M medial
Table 1 Demographics and correction angles by operative group
Variables OWHTO (119899 = 30) OWHTODTO (119899 = 33) 119901 valueAge (years) 328 plusmn 75 305 plusmn 80 018Gender (male female) 8 22 13 20 023Body mass index (kgm2) 233 plusmn 52 245 plusmn 50 052Preoperative MPTA (degrees) 818 plusmn 19 823 plusmn 23 030Postoperative MPTA (degrees) 881 plusmn 20 883 plusmn 24 063Correction of MPTA (degrees) 62 plusmn 21 60 plusmn 27 064Preoperative mFTA (degrees) minus60 plusmn 18 minus64 plusmn 30 044Postoperative mFTA (degrees) 08 plusmn 15 03 plusmn 18 024Correction of mFTA (degrees) 68 plusmn 23 77 plusmn 31 024Follow-up period (months) 324 plusmn 87 331 plusmn 29 068Values expressed as mean plusmn SD OWHTO open wedge high tibial osteotomy DTO distal tubercle osteotomy MPTA medial proximal tibial angle mFTAmechanical femorotibial angle
Table 2 Pre- and postoperative radiographic measurements by operative group
Variables OWHTO (119899 = 30) OWHTODTO (119899 = 33) 119901 valuePreoperative Insall-Salvati 102 plusmn 013 101 plusmn 023 0932Postoperative Insall-Salvati 097 plusmn 012 100 plusmn 014 0353Preoperative modified Insall-Salvati 148 plusmn 013 146 plusmn 016 0701Postoperative modified Insall-Salvati 140 plusmn 015 147 plusmn 017 0072Preoperative Blackburne-Peel 080 plusmn 011 079 plusmn 011 0800Postoperative Blackburne-Peel 071 plusmn 015 076 plusmn 015 0138Preoperative Caton-Deschamps 093 plusmn 008 090 plusmn 012 0237Postoperative Caton-Deschamps 083 plusmn 011 086 plusmn 014 0265Preoperative modified Miura-Kawamura 089 plusmn 008 084 plusmn 012 0077Postoperative modified Miura-Kawamura 081 plusmn 012 083 plusmn 016 0552Preoperative tibial slope (degrees) 83 plusmn 35 87 plusmn 39 0655Postoperative tibial slope (degrees) 111 plusmn 323 112 plusmn 416 0943Preoperative lateral patella tilt (degrees) 141 plusmn 247 145 plusmn 369 0582Postoperative lateral patella tilt (degrees) 121 plusmn 218 131 plusmn 398 0249Preoperative lateral patella shift 014 plusmn 003 015 plusmn 047 0493Postoperative lateral patella shift 013 plusmn 004 014 plusmn 005 0450Values expressed as mean plusmn SD OWHTO open wedge high tibial osteotomy DTO distal tubercle osteotomy
6 BioMed Research International
PreoperativePostoperative
PreoperativePostoperative
0
02
04
06
08
1
12
14In
sall-
Salv
ati
0
02
04
06
08
1
12
Cato
n-D
esch
amps
0
02
04
06
08
1
12
14
16
18
Mod
ified
Insa
ll-Sa
lvat
i
0
2
4
6
8
10
12
14
Tibi
al sl
ope (
degr
ees)
OWHTO OWHTODTOOWHTO OWHTODTO0
010203040506070809
1
Blac
kbur
ne-P
eel
0
02
04
06
08
1
12
Miu
ra-K
awam
ura
lowast lowast lowast
lowast
lowast
lowast lowast
Figure 5 Patellar height indices and tibial slope pre- and postoperatively charted by operative group OWHTO open wedge high tibialosteotomy DTO distal tubercle osteotomy lowastSignificant change after surgery (119901 lt 005)
indices decreased significantly in group 2 (OWHTODTO)other patellar height indices were not significantly altered bysurgery Neither group showed significant change in meantibial slope
Average LPT decreased significantly after surgery inboth groups However no statistical differences between pre-operative and postoperative LPS were evident (Figure 6)
We compared the amount of change between group 1 andgroup 2 (Table 3) The amount of change of mIS BP CDand MK indices significantly differed between two groupsBecause of the small number of subjects independent 119905-testpower calculation was carried out using Power Analysis andSample Size 11 for Windows software package (NCSS IncLLC Kaysville UT USA) and the power was 076 for mIS
index 041 for BP index 064 for CD index and 073 for MKindex between group 1 and group 2
There were no significant correlations in either groupwith respect to patellar height or tibial slope changes ordegree of correction angle in coronal plane (MPTA)
Bone union at osteotomy sites was achieved at an averageof 3 months in all patients A total of two complicationsoccurred in group 2 In these two patients the tibialtuberosity fractured during tuberosity osteotomy Remediedby fixation screws these fractures healed in 3 months Noother complications such as wound infection delayed unionor nonunion were seen
Interrater reliability of all patellar indices measuredwas confirmed using (ICCs) based on radiographs before
BioMed Research International 7
Table 3 The amount of change for radiographic measurements by operative group
Variables OWHTO (119899 = 30) OWHTODTO (119899 = 33) 119901 valueInsall-Salvati minus005 plusmn 008 minus002 plusmn 020 0408Modified Insall-Salvati minus008 plusmn 014 000 plusmn 009 0002Blackburne-Peel minus009 plusmn 009 minus004 plusmn 013 0037Caton-Deschamps minus010 plusmn 009 minus004 plusmn 011 0008Modified Miura-Kawamura minus008 plusmn 009 minus001 plusmn 012 0010Tibial slope (degrees) 078 plusmn 306 047 plusmn 395 0705Lateral patella tilt (degrees) minus206 plusmn 176 minus141 plusmn 214 0218Lateral patella shift minus001 plusmn 003 minus001 plusmn 003 0661Values expressed as mean plusmn SD OWHTO open wedge high tibial osteotomy DTO distal tubercle osteotomy
and after surgery ICC ranges for intraobserver (075ndash091)and interobserver (072ndash09) reliabilities were comparable tothose of previous studies [14 28]
4 Discussion
Introduction of OWHTODTO was fueled by efforts tominimize surgery-related loss in patellar height and preventsubsequent patellofemoral problems [8] Several studiesoffer proof that this technique is effective in minimizingpostoperative patellar height change citing clinical out-comes comparable to conventional OWHTO in patients withosteoarthritis of the medial tibiofemoral compartment andvarus malalignment [8 14 15 29ndash31] However there wasno study investigating the surgical results of OWHTODTOin patients with normal knee Special concerns in this pop-ulation include unsightly aesthetics and pain or discomfortupon kneeling after surgery Therefore we have used thistechnique to correct proximal tibial varus deformities inyoung patients without pain or arthritic joints provingthat diminished patellar height is avoidable through thisapproach Considering the positional changes of the patellafollowing conventionalOWHTOmay induce new symptomsthese concerns will be addressed by OWHTODTO
In the present study we found significant postoperativedecreases in IS and mIS indices of the OWHTO groupwhereas these ratios were unchanged in the OWHTODTOgroup Outcomes herein were aligned with previous studiesthat similarly utilized these ratios to evaluate patellar height[14 15 29] Both IS and mIS are indirect measures of patellarheight any change reflecting altered patellar tendon length[14 32] Any slackening or shortening of patellar tendon thusimplied may be explained by intratendinous fibrosis or adhe-sions of proximal tuberosity following OWHTO whereas theextensor mechanism remains intact after OWHTODTO
Although there were significant postoperative declines inBP and CD indices of both groups the MK index of theOWHTODTO group was unchanged Still only one otherstudy corroborates our results [14]Most earlier investigationshave recorded no significant changes in BP and CD indicesafter OWHTODTO [8 15 29 30] This discrepancy may bedue to the method of measurement Both BP and CD indiceshave been viewed as highly reliable gauges of patellar height[28 33] but their dependency on joint line is disadvanta-geous given tibial plateau as a reference Because tibial slope
OWHTO OWHTODTO
PreoperativePostoperative
0
005
01
015
02
025
Late
ral p
atel
la sh
ift
0
2
4
6
8
10
12
14
16
18
20
Late
ral p
atel
la ti
lt (d
egre
es)
lowast
lowast
Figure 6 Lateral patellar tilt and lateral patellar shift pre- andpostoperatively charted by operative group OWHTO open wedgehigh tibial osteotomy DTO distal tubercle osteotomy lowastSignificantchange after surgery (119901 lt 005)
decreased postoperatively in both arms of our study evenminimal deviations in tibial slope may thus have bearing Weagree with other investigators that BP and CD indices shouldnot be relied upon in surgical procedures involving proximaltibia [23 32] In our opinion the decrease seen in MK index
8 BioMed Research International
reflects a true reduction in patellar height because MK indexis independent with the change of tibial slope
Although various radiographic techniques (based onaxial radiography CT or MRI) have been described forevaluating patellar inclination [34] use of LPT and LPSafter OWHTODTO has not previously been investigatedPrevious publications studying changes in LPT and LPS afterOWHTO have relied on axial radiography of load-bearingpatellofemoral joints (Delgado-Martins method) [7 24 3536] However determinations rendered by axial radiographymay be not accurate due to overlapping of images difficultyin positioning the leg and incidental angles of X-ray beams[37 38] CT imaging of contracted quadriceps muscle mayserve better in confirming patellar position [25 34 37 39]Consequently we used axial CT images in supine positionwith the knee in 30 degrees of flexion to measure LPT andLPS
Ultimately we found that LPT declined significantlyfor both procedures but the reductions did not differsignificantly by operative group Our findings followingOWHTO were consistent with those of previous stud-ies [35 36] whereby lessening of LPT was attributed toincreased lateral pull on the patella Although we expectedthat OWHTODTO would prevent any changes in LPTand LPS LPT surprisingly showed significant decline afterOWHTODTO as well One possible explanation for this isthat a change in mechanical axis may affect the inclinationof patella For another reason the change of tibial rotationafter OWHTOmay affect the LPT Previous studies reportedOWHTO made significant internal axial rotation of the tibia[40 41] However there was no change on tibial rotation aftervarus correction because we used two half-pins to check thechange of rotational alignment in the operating room
In our analysis no significant correlations emerged withrespect to change in patellar height change in tibial slopeor correction angle degree Prior reports have indicated thatOWHTODTO ismore effective than conventional OWHTOin patients requiring large (gt10-degree) angular corrections[8 14 15 30] However we could provide corroborationbecause correction angles for most of our patients werelt10 degrees and the surgical goal was to restore neutralalignment Hence the protective effect of OWHTODTO onpatellar height after large angular correction (gt10 degrees)could not be fully evaluated by this study
There were two tibial tuberosity fractures in OWHTODTO group Only one previous literature reported samesurgical complications [8]Therewas no such complication inother reports using OWHTODTO [14 15 29 30]Thereforeit seems that tibial tuberosity fracture is related to mistakeof surgical procedure not the degrees of correction angleAdditionally in our study such fractures occurred at an earlystage in our learning curve and healed well with additionalscrew fixation Eventually we think that tibial tuberosityfracture is easily preventable with caution leaving at least a1-cm thickness on the proximal tuberosity fragment
Our study has some limitations First it is a retrospectiveinvestigation and not a randomized trial Also the twooperative groups reflected a shift in surgical technique ratherthan pure randomization Nevertheless the two groups were
well matched at baseline in terms of preoperative variablesAnother limitation was that blinding of the OWHTODTOarm was not feasible when measuring radiologic param-eters postoperatively even if two independent orthopedicresidents participated Finally radiographic parameters werethe primary focus To investigate the relationship betweenradiologic findings and clinical outcomes a well-plannedfuture prospective study is needed
There are various methods for correcting proximal tibialvara deformity and best surgical techniquemust be individu-alized Compared to conventional OWHTO OWHTODTOdid not influence patella height associated with the procedureand was considered an useful method to preserve patellaheight
Ethical Approval
This study was conducted following the approval of Institu-tional Review Board of Severance Hospital Yonsei UniversityCollege of Medicine (IRB number 4-2015-0796)
Conflicts of Interest
The authors declare that there are no conflicts of interest toreport regarding the work and publication of this study
Acknowledgments
The authors thank Dr Sung Min Kim and Jung Woo Lee forthe data measurement of the patients
References
[1] W Strecker ldquoPlanning Analysis of Knee-Adjacent DeformitiesrdquoEuropean Journal of Trauma and Emergency Surgery vol 33 no6 pp 662ndash668 2007
[2] R Rossi D E Bonasia and A Amendola ldquoThe Role of HighTibial Osteotomy in the Varus Kneerdquo American Academy ofOrthopaedic Surgeon vol 19 no 10 pp 590ndash599 2011
[3] R K Marti R A W Verhagen G M M J Kerkhoffs andT M Moojen ldquoProximal tibial varus osteotomy Indicationstechnique and five to twenty-one-year resultsrdquo Journal of Boneand Joint Surgery - Series A vol 83 no 2 pp 164ndash170 2001
[4] H El-Azab P Glabgly J Paul A B Imhoff and S Hinterwim-mer ldquoPatellar height and posterior tibial slope after open- andclosed-wedge high tibial osteotomy A radiological study on 100patientsrdquoAmerican Journal of Sports Medicine vol 38 no 2 pp323ndash329 2010
[5] B P Kaper R B Bourne C H Rorabeck and S J MacDonaldldquoPatellar infera after high tibial osteotomyrdquo Journal of Arthro-plasty vol 16 no 2 pp 168ndash173 2001
[6] D Tigani D Ferrari P Trentani G Barbanti-Brodano and FTrentani ldquoPatellar height after high tibial osteotomyrdquo Interna-tional Orthopaedics vol 24 no 6 pp 331ndash334 2001
[7] J-H Yang S-H Lee K S Nathawat S-H Jeon and K-JOh ldquoThe effect of biplane medial opening wedge high tibialosteotomy on patellofemoral joint indicesrdquo Knee vol 20 no 2pp 128ndash132 2013
[8] R D A Gaasbeek H Sonneveld R J Van Heerwaarden W CH Jacobs and A B Wymenga ldquoDistal tuberosity osteotomy in
BioMed Research International 9
open wedge high tibial osteotomy can prevent patella infera Anew techniquerdquo Knee vol 11 no 6 pp 457ndash461 2004
[9] C M Rodner D J Adams V Diaz-Doran et al ldquoMedialopeningwedge tibial osteotomy and the sagittal planeThe effectof increasing tibial slope on tibiofemoral contact pressurerdquoAmerican Journal of SportsMedicine vol 34 no 9 pp 1431ndash14412006
[10] R E Windsor J N Insall and K G Vince ldquoTechnicalconsiderations of total knee arthroplasty after proximal tibialosteotomyrdquo Journal of Bone and Joint Surgery - Series A vol 70no 4 pp 547ndash555 1988
[11] H E Figgie III V M Goldberg K G Heiple H S MollerIII and N H Gordon ldquoThe influence of tibial-patellofemorallocation on function of the knee in patients with the posteriorstabilized condylar knee prosthesisrdquo Journal of Bone and JointSurgery - Series A vol 68 no 7 pp 1035ndash1040 1986
[12] K Kim D Kim S Song S Lee and D Bae ldquoMedialOpen-Wedge High Tibial Osteotomy May Adversely Affect thePatellofemoral Jointrdquo Arthroscopy The Journal of Arthroscopicamp Related Surgery vol 33 no 4 pp 811ndash816 2017
[13] J S Shim S H Lee H J Jung and H I Lee ldquoHightibial open wedge osteotomy below the tibial tubercle Clinicaland radiographic resultsrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 1 pp 57ndash63 2013
[14] P D Longino T B Birmingham W J Schultz R F Moyerand J R Giffin ldquoCombined tibial tubercle osteotomy withmedial openingwedge high tibial osteotomyminimizes changesin patellar height A prospective cohort study with historicalcontrolsrdquo American Journal of Sports Medicine vol 41 no 12pp 2849ndash2857 2013
[15] S Keyhani M R Abbasian S M Kazemi et al ldquoModifiedretro-tubercle opening-wedge versus conventional high tibialosteotomyrdquo Orthopedics vol 34 no 2 2011
[16] D H Lee K J Ryu H H Kim S Soung and S Shin ldquoFixator-assisted Technique Enables Less Invasive Plate Osteosynthesisin Medial Opening-wedge High Tibial Osteotomy A NovelTechniquerdquo Clinical Orthopaedics and Related Research vol473 no 10 pp 3133ndash3142 2015
[17] S B Han D H Lee G M Shetty D J Chae J G Songand K W Nha ldquoA ldquosafe zonerdquo in medial open-wedge hightibia osteotomy to prevent lateral cortex fracturerdquoKnee SurgerySports Traumatology Arthroscopy vol 21 no 1 pp 90ndash95 2013
[18] D Paley and K Tetsworth ldquoMechanical axis deviation ofthe lower limbs Preoperative planning of uniapical angulardeformities of the tibia or femurrdquo Clinical Orthopaedics andRelated Research no 280 pp 48ndash64 1992
[19] J Insall and E Salvati ldquoPatella position in the normal kneejointrdquo Radiology vol 101 no 1 pp 101ndash104 1971
[20] R P Grelsamer and S Meadows ldquoThe modified Insall-Salvatiratio for assessment of patellar heightrdquo Clinical Orthopaedicsand Related Research no 282 pp 170ndash176 1992
[21] J S Blackburne and T E Peel ldquoA new method of measuringpatellar heightrdquo J Bone Joint Surg Br vol 59 no 2 pp 241-2421977
[22] J Caton G Deschamps P Chambat J L Lerat and HDejour ldquoPatella infera Apropos of 128 casesrdquo Rev Chir OrthopReparatrice Appar Mot vol 68 no 5 pp 317ndash325 1982
[23] H Miura H Kawamura R Nagamine K Urabe and YIwamoto ldquoIs patellar height really lower after high tibialosteotomyrdquo Fukuoka igaku zasshi = Hukuoka acta medica vol88 no 6 pp 261ndash266 1997
[24] H Delgado-Martins ldquoThe bicondylo-patellar angle as a mea-sure of patellar tiltingrdquo Archives of Orthopaedic and TraumaticSurgery vol 96 no 4 pp 303-304 1980
[25] V Vahasarja P Lanning S Lahde and W Serlo ldquoAxialradiography or CT in the measurement of patellofemoralmalalignment indices in children and adolescentsrdquo ClinicalRadiology vol 51 no 9 pp 639ndash643 1996
[26] U M Kujala K Osterman M Kormano M Komu and DSchlenzka ldquoPatellar motion analyzed by magnetic resonanceimagingrdquo Acta Orthopaedica vol 60 no 1 pp 13ndash16 1989
[27] C A Laurin R Dussault and H P Levesque ldquoThe tan-gential X-ray investigation of the patellofemoral joint X-raytechnique diagnostic criteria and their interpretationrdquo ClinicalOrthopaedics and Related Research no 144 pp 16ndash26 1979
[28] R Seil B Muller T Georg D Kohn and S Rupp ldquoReliabilityand interobserver variability in radiological patellar heightratiosrdquo Knee Surgery Sports Traumatology Arthroscopy vol 8no 4 pp 231ndash236 2000
[29] N Elmali I Esenkaya M Can and M Karakaplan ldquoMono-planar versus biplanar medial open-wedge proximal tibialosteotomy for varus gonarthrosis A comparison of clinicaland radiological outcomesrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 12 pp 2689ndash2695 2013
[30] S Hinterwimmer K Beitzel J Paul et al ldquoControl of posteriortibial slope and patellar height in open-wedge valgus high tibialosteotomyrdquo American Journal of Sports Medicine vol 39 no 4pp 851ndash856 2011
[31] S Hopwood W Khan and S Agarwal ldquoThe biplanar openwedge high tibial osteotomy preserving the tibial tuberclerdquoJournal of Orthopaedic Science vol 21 no 6 pp 786ndash790 2016
[32] H Kesmezacar R Erginer T Ogut A Seyahi M Babacan andY Tenekecioglu ldquoEvaluation of patellar height and measure-ment methods after valgus high tibial osteotomyrdquo Knee SurgerySports Traumatology Arthroscopy vol 13 no 7 pp 539ndash5442005
[33] B A Rogers P Thornton-Bott S R Cannon and T W RBriggs ldquoInterobserver variation in the measurement of patellarheight after total knee arthroplastyrdquo Journal of Bone and JointSurgery - Series B vol 88 no 4 pp 484ndash488 2006
[34] R P Grelsamer C H Weinstein J Gould and A DubeyldquoPatellar tilt The physical examination correlates with MRimagingrdquo Knee vol 15 no 1 pp 3ndash8 2008
[35] R Gaasbeek R Welsing M Barink N Verdonschot andA Van Kampen ldquoThe influence of open and closed hightibial osteotomy on dynamic patellar tracking A biomechanicalstudyrdquo Knee Surgery Sports Traumatology Arthroscopy vol 15no 8 pp 978ndash984 2007
[36] H Bito R Takeuchi K Kumagai et al ldquoOpening wedge hightibial osteotomy affects both the lateral patellar tilt and patellarheightrdquo Knee Surgery Sports Traumatology Arthroscopy vol 18no 7 pp 955ndash960 2010
[37] T Sasaki and T Yagi ldquoSubluxation of the patella - Investigationby computerized tomographyrdquo International Orthopaedics vol10 no 2 pp 115ndash120 1986
[38] F Boven M-A Bellemans J Geurts and R PotvliegeldquoA comparative study of the patello-femoral joint on axialroentgenogram axial arthrogram and computed tomographyfollowing arthrographyrdquo Skeletal Radiology vol 8 no 3 pp179ndash181 1982
[39] A D Delgado-Martınez C Estrada E C Rodrıguez-MerchanM Atienza and J M Ordonez ldquoCT scanning of the
10 BioMed Research International
patellofemoral joint The quadriceps relaxed or contractedrdquoInternational Orthopaedics vol 20 no 3 pp 159ndash162 1996
[40] S Hinterwimmer M J Feucht J Paul et al ldquoAnalysis of theeffects of high tibial osteotomy on tibial rotationrdquo InternationalOrthopaedics vol 40 no 9 pp 1849ndash1854 2016
[41] K-M Jang J-H Lee H-J Park J L Kim and S-B HanldquoUnintended Rotational Changes of the Distal Tibia AfterBiplane Medial Open-Wedge High Tibial Osteotomyrdquo Journalof Arthroplasty vol 31 no 1 pp 59ndash63 2016
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
BioMed Research International 3
(a) (b) (c)
Figure 1 Lateral radiographs of open wedge high tibial osteotomy with distal tubercle osteotomy (a) biplanar retrotubercle osteotomy(intraoperative view) (b) locking plate fixation at osteotomy site (immediately postoperative) and (c) union of the osteotomy site(postoperative month 3)
(a) (b) (c)
Figure 2 Images of patient with tibial tuberosity fracture (a) fracture of proximal tibial tuberosity (arrow) in C-arm image (b) fixation viatwo additional cannulated screws and (c) healed fracture (postoperative month 3)
generated twice for each radiograph with at least 1 monthbetween assessments To limit the number of variables onlythe right tibia of each patient was analyzed
Radiologic assessments were based on standing full-legradiographs (patella pointing forward) and standing antero-posterior and lateral knee views obtained preoperatively andat the latest follow-up Each standing lateral view was takenwith the knee in 30-degree flexion and the limb in neutralposition
Coronal alignment was gauged via standing full-leg ra-diographs measuring medial proximal tibial angle (MPTA)as described by Paley and Tetsworth [18] and mechanicalfemorotibial angle (mFTA) (positive andnegative values indi-cating genu valgus and varum resp)The femoralmechanicalaxis passes from the center of the hip through the center
of the knee and the tibial mechanical axis passes from thecenter of the tibial spine through the center of the anklemortise The angle between these two axes correspondsto the mFTA Patellar height was evaluated in standinglateral knee view by measuring the Insall-Salvati (IS) index[19] modified IS (mIS) index [20] Blackburne-Peel (BP)index [21] Caton-Deschamps (CD) index [22] and modifiedMiura-Kawamura (MK) index (Figure 3) [23] The tibialslope was also calculated by the proximal tibial anatomic axismethod measuring the angle formed between the proximalmedial plateau and a line drawn perpendicular to the tibialshaft axis
Lateral patellar tilt (LPT) and lateral patellar shift (LPS)were measured on axial images generated pre- and postop-eratively by two-dimensional CT [24ndash27] CT scan slices were
4 BioMed Research International
a
b
Insall-Salvati ba
(a)
c
b
Modified Insall-Salvati bc
(b)
c
d
Blackburne-Peel dc
(c)
c
e
Caton-Deschamps ec
(d)
c
f
Modified Miura-Kawamura fc
(e)
Figure 3 Radiographic diagrams showing five indices measured to assess patellar height (a) Insall-Salvati (b) modified Insall-Salvati (c)Blackburne-Peel (d) Caton-Deschamps and (e) modified Miura-Kawamura 119886 diagonal patellar length 119887 patellar length 119888 length of thepatellar articular surface 119889 perpendicular distance between the proximal tibial articular surface and the inferior tip of patellar articularsurface 119890 distance from the anterosuperior border of the tibial plateau to the inferior tip of the patellar articular surface 119891 distance from aline perpendicular to the tibial diaphyseal line to the inferior tip of the patellar articular surface
focused on the central patella with hips flexed at 45 degreesand knees flexed at 30 degrees (Figure 4)
24 Statistical Analysis All statistical calculations reliedon standard software (SPSS v190 SPSS Inc Chicago ILUSA) All continuous variables were tested for normality viaShapiro-Wilk test and did not violate the normal distribu-tion assumption Studentrsquos paired 119905-test was used to assessdifferences between pre- and postoperative measures in eachgroup To compare changes in patellar position by operativegroup Studentrsquos independent 119905-test was applied Statisticalsignificance was set at 119901 lt 005 Changes in patellar heightand tibial slope and degrees of correction angle in the coronalplane (MPTA) were analyzed using Pearsonrsquos correlationcoefficient Inter- and intraobserver reliabilities were gaugedas well through intraclass correlation coefficients (ICCs)ICCs were interpreted as follows poor lt04 marginal gt04but lt075 and good gt075
3 Results
Baseline demographics as well as pre- and postoperativeMPTA and mFTA data are reported by operative method inTable 1 The two groups did not differ significantly in termsof age gender BMI or follow-up period There were nosignificant between-group differences with respect to meanpreoperative MPTA andmFTA or mean extent of correction
Pre- and postoperative patellar height indices tibial slopeand lateral patellar tilt and shift are shown by group inTable 2 None of the pre- and postoperative variables differedsignificantly
Patellar height and tibial slope measurements before andafter surgery for both groups are tabulated in Figure 5 Ingroup 1 (OWHTO) all patellar height indices including IS(119901 = 0003) mIS (119901 = 0007) BP (119901 lt 0001) CD (119901 lt0001) and MK index (119901 lt 0001) declined significantlyAlthough mean BP (119901 = 0023) and CD (119901 = 0009)
BioMed Research International 5
(a)
L M
(b)
L M
p
c
p
c
(c)
Figure 4 Methods of assessing lateral patellar tilt (LPT) and lateral patellar shift (LPS) (a) patient positioned for computed tomographyimaging with knee in 30 degrees of flexion (b) LPT defined as the angle between a line intersecting the widest bony structure of the patellaand a line tangential to the anterior femoral condylar surfaces (c) LPS defined as the ratio of distances 11990111990110158401198881198881015840 where 1198881198881015840 is the distancebetween the summits of the medial and lateral femoral condyles and 1199011199011015840 is the distance between the summit of the lateral femoral condyleand the point where a line from the lateral edge of the patella perpendicular to the line that passed through the summits of the femoralcondyles crosses that line L lateral M medial
Table 1 Demographics and correction angles by operative group
Variables OWHTO (119899 = 30) OWHTODTO (119899 = 33) 119901 valueAge (years) 328 plusmn 75 305 plusmn 80 018Gender (male female) 8 22 13 20 023Body mass index (kgm2) 233 plusmn 52 245 plusmn 50 052Preoperative MPTA (degrees) 818 plusmn 19 823 plusmn 23 030Postoperative MPTA (degrees) 881 plusmn 20 883 plusmn 24 063Correction of MPTA (degrees) 62 plusmn 21 60 plusmn 27 064Preoperative mFTA (degrees) minus60 plusmn 18 minus64 plusmn 30 044Postoperative mFTA (degrees) 08 plusmn 15 03 plusmn 18 024Correction of mFTA (degrees) 68 plusmn 23 77 plusmn 31 024Follow-up period (months) 324 plusmn 87 331 plusmn 29 068Values expressed as mean plusmn SD OWHTO open wedge high tibial osteotomy DTO distal tubercle osteotomy MPTA medial proximal tibial angle mFTAmechanical femorotibial angle
Table 2 Pre- and postoperative radiographic measurements by operative group
Variables OWHTO (119899 = 30) OWHTODTO (119899 = 33) 119901 valuePreoperative Insall-Salvati 102 plusmn 013 101 plusmn 023 0932Postoperative Insall-Salvati 097 plusmn 012 100 plusmn 014 0353Preoperative modified Insall-Salvati 148 plusmn 013 146 plusmn 016 0701Postoperative modified Insall-Salvati 140 plusmn 015 147 plusmn 017 0072Preoperative Blackburne-Peel 080 plusmn 011 079 plusmn 011 0800Postoperative Blackburne-Peel 071 plusmn 015 076 plusmn 015 0138Preoperative Caton-Deschamps 093 plusmn 008 090 plusmn 012 0237Postoperative Caton-Deschamps 083 plusmn 011 086 plusmn 014 0265Preoperative modified Miura-Kawamura 089 plusmn 008 084 plusmn 012 0077Postoperative modified Miura-Kawamura 081 plusmn 012 083 plusmn 016 0552Preoperative tibial slope (degrees) 83 plusmn 35 87 plusmn 39 0655Postoperative tibial slope (degrees) 111 plusmn 323 112 plusmn 416 0943Preoperative lateral patella tilt (degrees) 141 plusmn 247 145 plusmn 369 0582Postoperative lateral patella tilt (degrees) 121 plusmn 218 131 plusmn 398 0249Preoperative lateral patella shift 014 plusmn 003 015 plusmn 047 0493Postoperative lateral patella shift 013 plusmn 004 014 plusmn 005 0450Values expressed as mean plusmn SD OWHTO open wedge high tibial osteotomy DTO distal tubercle osteotomy
6 BioMed Research International
PreoperativePostoperative
PreoperativePostoperative
0
02
04
06
08
1
12
14In
sall-
Salv
ati
0
02
04
06
08
1
12
Cato
n-D
esch
amps
0
02
04
06
08
1
12
14
16
18
Mod
ified
Insa
ll-Sa
lvat
i
0
2
4
6
8
10
12
14
Tibi
al sl
ope (
degr
ees)
OWHTO OWHTODTOOWHTO OWHTODTO0
010203040506070809
1
Blac
kbur
ne-P
eel
0
02
04
06
08
1
12
Miu
ra-K
awam
ura
lowast lowast lowast
lowast
lowast
lowast lowast
Figure 5 Patellar height indices and tibial slope pre- and postoperatively charted by operative group OWHTO open wedge high tibialosteotomy DTO distal tubercle osteotomy lowastSignificant change after surgery (119901 lt 005)
indices decreased significantly in group 2 (OWHTODTO)other patellar height indices were not significantly altered bysurgery Neither group showed significant change in meantibial slope
Average LPT decreased significantly after surgery inboth groups However no statistical differences between pre-operative and postoperative LPS were evident (Figure 6)
We compared the amount of change between group 1 andgroup 2 (Table 3) The amount of change of mIS BP CDand MK indices significantly differed between two groupsBecause of the small number of subjects independent 119905-testpower calculation was carried out using Power Analysis andSample Size 11 for Windows software package (NCSS IncLLC Kaysville UT USA) and the power was 076 for mIS
index 041 for BP index 064 for CD index and 073 for MKindex between group 1 and group 2
There were no significant correlations in either groupwith respect to patellar height or tibial slope changes ordegree of correction angle in coronal plane (MPTA)
Bone union at osteotomy sites was achieved at an averageof 3 months in all patients A total of two complicationsoccurred in group 2 In these two patients the tibialtuberosity fractured during tuberosity osteotomy Remediedby fixation screws these fractures healed in 3 months Noother complications such as wound infection delayed unionor nonunion were seen
Interrater reliability of all patellar indices measuredwas confirmed using (ICCs) based on radiographs before
BioMed Research International 7
Table 3 The amount of change for radiographic measurements by operative group
Variables OWHTO (119899 = 30) OWHTODTO (119899 = 33) 119901 valueInsall-Salvati minus005 plusmn 008 minus002 plusmn 020 0408Modified Insall-Salvati minus008 plusmn 014 000 plusmn 009 0002Blackburne-Peel minus009 plusmn 009 minus004 plusmn 013 0037Caton-Deschamps minus010 plusmn 009 minus004 plusmn 011 0008Modified Miura-Kawamura minus008 plusmn 009 minus001 plusmn 012 0010Tibial slope (degrees) 078 plusmn 306 047 plusmn 395 0705Lateral patella tilt (degrees) minus206 plusmn 176 minus141 plusmn 214 0218Lateral patella shift minus001 plusmn 003 minus001 plusmn 003 0661Values expressed as mean plusmn SD OWHTO open wedge high tibial osteotomy DTO distal tubercle osteotomy
and after surgery ICC ranges for intraobserver (075ndash091)and interobserver (072ndash09) reliabilities were comparable tothose of previous studies [14 28]
4 Discussion
Introduction of OWHTODTO was fueled by efforts tominimize surgery-related loss in patellar height and preventsubsequent patellofemoral problems [8] Several studiesoffer proof that this technique is effective in minimizingpostoperative patellar height change citing clinical out-comes comparable to conventional OWHTO in patients withosteoarthritis of the medial tibiofemoral compartment andvarus malalignment [8 14 15 29ndash31] However there wasno study investigating the surgical results of OWHTODTOin patients with normal knee Special concerns in this pop-ulation include unsightly aesthetics and pain or discomfortupon kneeling after surgery Therefore we have used thistechnique to correct proximal tibial varus deformities inyoung patients without pain or arthritic joints provingthat diminished patellar height is avoidable through thisapproach Considering the positional changes of the patellafollowing conventionalOWHTOmay induce new symptomsthese concerns will be addressed by OWHTODTO
In the present study we found significant postoperativedecreases in IS and mIS indices of the OWHTO groupwhereas these ratios were unchanged in the OWHTODTOgroup Outcomes herein were aligned with previous studiesthat similarly utilized these ratios to evaluate patellar height[14 15 29] Both IS and mIS are indirect measures of patellarheight any change reflecting altered patellar tendon length[14 32] Any slackening or shortening of patellar tendon thusimplied may be explained by intratendinous fibrosis or adhe-sions of proximal tuberosity following OWHTO whereas theextensor mechanism remains intact after OWHTODTO
Although there were significant postoperative declines inBP and CD indices of both groups the MK index of theOWHTODTO group was unchanged Still only one otherstudy corroborates our results [14]Most earlier investigationshave recorded no significant changes in BP and CD indicesafter OWHTODTO [8 15 29 30] This discrepancy may bedue to the method of measurement Both BP and CD indiceshave been viewed as highly reliable gauges of patellar height[28 33] but their dependency on joint line is disadvanta-geous given tibial plateau as a reference Because tibial slope
OWHTO OWHTODTO
PreoperativePostoperative
0
005
01
015
02
025
Late
ral p
atel
la sh
ift
0
2
4
6
8
10
12
14
16
18
20
Late
ral p
atel
la ti
lt (d
egre
es)
lowast
lowast
Figure 6 Lateral patellar tilt and lateral patellar shift pre- andpostoperatively charted by operative group OWHTO open wedgehigh tibial osteotomy DTO distal tubercle osteotomy lowastSignificantchange after surgery (119901 lt 005)
decreased postoperatively in both arms of our study evenminimal deviations in tibial slope may thus have bearing Weagree with other investigators that BP and CD indices shouldnot be relied upon in surgical procedures involving proximaltibia [23 32] In our opinion the decrease seen in MK index
8 BioMed Research International
reflects a true reduction in patellar height because MK indexis independent with the change of tibial slope
Although various radiographic techniques (based onaxial radiography CT or MRI) have been described forevaluating patellar inclination [34] use of LPT and LPSafter OWHTODTO has not previously been investigatedPrevious publications studying changes in LPT and LPS afterOWHTO have relied on axial radiography of load-bearingpatellofemoral joints (Delgado-Martins method) [7 24 3536] However determinations rendered by axial radiographymay be not accurate due to overlapping of images difficultyin positioning the leg and incidental angles of X-ray beams[37 38] CT imaging of contracted quadriceps muscle mayserve better in confirming patellar position [25 34 37 39]Consequently we used axial CT images in supine positionwith the knee in 30 degrees of flexion to measure LPT andLPS
Ultimately we found that LPT declined significantlyfor both procedures but the reductions did not differsignificantly by operative group Our findings followingOWHTO were consistent with those of previous stud-ies [35 36] whereby lessening of LPT was attributed toincreased lateral pull on the patella Although we expectedthat OWHTODTO would prevent any changes in LPTand LPS LPT surprisingly showed significant decline afterOWHTODTO as well One possible explanation for this isthat a change in mechanical axis may affect the inclinationof patella For another reason the change of tibial rotationafter OWHTOmay affect the LPT Previous studies reportedOWHTO made significant internal axial rotation of the tibia[40 41] However there was no change on tibial rotation aftervarus correction because we used two half-pins to check thechange of rotational alignment in the operating room
In our analysis no significant correlations emerged withrespect to change in patellar height change in tibial slopeor correction angle degree Prior reports have indicated thatOWHTODTO ismore effective than conventional OWHTOin patients requiring large (gt10-degree) angular corrections[8 14 15 30] However we could provide corroborationbecause correction angles for most of our patients werelt10 degrees and the surgical goal was to restore neutralalignment Hence the protective effect of OWHTODTO onpatellar height after large angular correction (gt10 degrees)could not be fully evaluated by this study
There were two tibial tuberosity fractures in OWHTODTO group Only one previous literature reported samesurgical complications [8]Therewas no such complication inother reports using OWHTODTO [14 15 29 30]Thereforeit seems that tibial tuberosity fracture is related to mistakeof surgical procedure not the degrees of correction angleAdditionally in our study such fractures occurred at an earlystage in our learning curve and healed well with additionalscrew fixation Eventually we think that tibial tuberosityfracture is easily preventable with caution leaving at least a1-cm thickness on the proximal tuberosity fragment
Our study has some limitations First it is a retrospectiveinvestigation and not a randomized trial Also the twooperative groups reflected a shift in surgical technique ratherthan pure randomization Nevertheless the two groups were
well matched at baseline in terms of preoperative variablesAnother limitation was that blinding of the OWHTODTOarm was not feasible when measuring radiologic param-eters postoperatively even if two independent orthopedicresidents participated Finally radiographic parameters werethe primary focus To investigate the relationship betweenradiologic findings and clinical outcomes a well-plannedfuture prospective study is needed
There are various methods for correcting proximal tibialvara deformity and best surgical techniquemust be individu-alized Compared to conventional OWHTO OWHTODTOdid not influence patella height associated with the procedureand was considered an useful method to preserve patellaheight
Ethical Approval
This study was conducted following the approval of Institu-tional Review Board of Severance Hospital Yonsei UniversityCollege of Medicine (IRB number 4-2015-0796)
Conflicts of Interest
The authors declare that there are no conflicts of interest toreport regarding the work and publication of this study
Acknowledgments
The authors thank Dr Sung Min Kim and Jung Woo Lee forthe data measurement of the patients
References
[1] W Strecker ldquoPlanning Analysis of Knee-Adjacent DeformitiesrdquoEuropean Journal of Trauma and Emergency Surgery vol 33 no6 pp 662ndash668 2007
[2] R Rossi D E Bonasia and A Amendola ldquoThe Role of HighTibial Osteotomy in the Varus Kneerdquo American Academy ofOrthopaedic Surgeon vol 19 no 10 pp 590ndash599 2011
[3] R K Marti R A W Verhagen G M M J Kerkhoffs andT M Moojen ldquoProximal tibial varus osteotomy Indicationstechnique and five to twenty-one-year resultsrdquo Journal of Boneand Joint Surgery - Series A vol 83 no 2 pp 164ndash170 2001
[4] H El-Azab P Glabgly J Paul A B Imhoff and S Hinterwim-mer ldquoPatellar height and posterior tibial slope after open- andclosed-wedge high tibial osteotomy A radiological study on 100patientsrdquoAmerican Journal of Sports Medicine vol 38 no 2 pp323ndash329 2010
[5] B P Kaper R B Bourne C H Rorabeck and S J MacDonaldldquoPatellar infera after high tibial osteotomyrdquo Journal of Arthro-plasty vol 16 no 2 pp 168ndash173 2001
[6] D Tigani D Ferrari P Trentani G Barbanti-Brodano and FTrentani ldquoPatellar height after high tibial osteotomyrdquo Interna-tional Orthopaedics vol 24 no 6 pp 331ndash334 2001
[7] J-H Yang S-H Lee K S Nathawat S-H Jeon and K-JOh ldquoThe effect of biplane medial opening wedge high tibialosteotomy on patellofemoral joint indicesrdquo Knee vol 20 no 2pp 128ndash132 2013
[8] R D A Gaasbeek H Sonneveld R J Van Heerwaarden W CH Jacobs and A B Wymenga ldquoDistal tuberosity osteotomy in
BioMed Research International 9
open wedge high tibial osteotomy can prevent patella infera Anew techniquerdquo Knee vol 11 no 6 pp 457ndash461 2004
[9] C M Rodner D J Adams V Diaz-Doran et al ldquoMedialopeningwedge tibial osteotomy and the sagittal planeThe effectof increasing tibial slope on tibiofemoral contact pressurerdquoAmerican Journal of SportsMedicine vol 34 no 9 pp 1431ndash14412006
[10] R E Windsor J N Insall and K G Vince ldquoTechnicalconsiderations of total knee arthroplasty after proximal tibialosteotomyrdquo Journal of Bone and Joint Surgery - Series A vol 70no 4 pp 547ndash555 1988
[11] H E Figgie III V M Goldberg K G Heiple H S MollerIII and N H Gordon ldquoThe influence of tibial-patellofemorallocation on function of the knee in patients with the posteriorstabilized condylar knee prosthesisrdquo Journal of Bone and JointSurgery - Series A vol 68 no 7 pp 1035ndash1040 1986
[12] K Kim D Kim S Song S Lee and D Bae ldquoMedialOpen-Wedge High Tibial Osteotomy May Adversely Affect thePatellofemoral Jointrdquo Arthroscopy The Journal of Arthroscopicamp Related Surgery vol 33 no 4 pp 811ndash816 2017
[13] J S Shim S H Lee H J Jung and H I Lee ldquoHightibial open wedge osteotomy below the tibial tubercle Clinicaland radiographic resultsrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 1 pp 57ndash63 2013
[14] P D Longino T B Birmingham W J Schultz R F Moyerand J R Giffin ldquoCombined tibial tubercle osteotomy withmedial openingwedge high tibial osteotomyminimizes changesin patellar height A prospective cohort study with historicalcontrolsrdquo American Journal of Sports Medicine vol 41 no 12pp 2849ndash2857 2013
[15] S Keyhani M R Abbasian S M Kazemi et al ldquoModifiedretro-tubercle opening-wedge versus conventional high tibialosteotomyrdquo Orthopedics vol 34 no 2 2011
[16] D H Lee K J Ryu H H Kim S Soung and S Shin ldquoFixator-assisted Technique Enables Less Invasive Plate Osteosynthesisin Medial Opening-wedge High Tibial Osteotomy A NovelTechniquerdquo Clinical Orthopaedics and Related Research vol473 no 10 pp 3133ndash3142 2015
[17] S B Han D H Lee G M Shetty D J Chae J G Songand K W Nha ldquoA ldquosafe zonerdquo in medial open-wedge hightibia osteotomy to prevent lateral cortex fracturerdquoKnee SurgerySports Traumatology Arthroscopy vol 21 no 1 pp 90ndash95 2013
[18] D Paley and K Tetsworth ldquoMechanical axis deviation ofthe lower limbs Preoperative planning of uniapical angulardeformities of the tibia or femurrdquo Clinical Orthopaedics andRelated Research no 280 pp 48ndash64 1992
[19] J Insall and E Salvati ldquoPatella position in the normal kneejointrdquo Radiology vol 101 no 1 pp 101ndash104 1971
[20] R P Grelsamer and S Meadows ldquoThe modified Insall-Salvatiratio for assessment of patellar heightrdquo Clinical Orthopaedicsand Related Research no 282 pp 170ndash176 1992
[21] J S Blackburne and T E Peel ldquoA new method of measuringpatellar heightrdquo J Bone Joint Surg Br vol 59 no 2 pp 241-2421977
[22] J Caton G Deschamps P Chambat J L Lerat and HDejour ldquoPatella infera Apropos of 128 casesrdquo Rev Chir OrthopReparatrice Appar Mot vol 68 no 5 pp 317ndash325 1982
[23] H Miura H Kawamura R Nagamine K Urabe and YIwamoto ldquoIs patellar height really lower after high tibialosteotomyrdquo Fukuoka igaku zasshi = Hukuoka acta medica vol88 no 6 pp 261ndash266 1997
[24] H Delgado-Martins ldquoThe bicondylo-patellar angle as a mea-sure of patellar tiltingrdquo Archives of Orthopaedic and TraumaticSurgery vol 96 no 4 pp 303-304 1980
[25] V Vahasarja P Lanning S Lahde and W Serlo ldquoAxialradiography or CT in the measurement of patellofemoralmalalignment indices in children and adolescentsrdquo ClinicalRadiology vol 51 no 9 pp 639ndash643 1996
[26] U M Kujala K Osterman M Kormano M Komu and DSchlenzka ldquoPatellar motion analyzed by magnetic resonanceimagingrdquo Acta Orthopaedica vol 60 no 1 pp 13ndash16 1989
[27] C A Laurin R Dussault and H P Levesque ldquoThe tan-gential X-ray investigation of the patellofemoral joint X-raytechnique diagnostic criteria and their interpretationrdquo ClinicalOrthopaedics and Related Research no 144 pp 16ndash26 1979
[28] R Seil B Muller T Georg D Kohn and S Rupp ldquoReliabilityand interobserver variability in radiological patellar heightratiosrdquo Knee Surgery Sports Traumatology Arthroscopy vol 8no 4 pp 231ndash236 2000
[29] N Elmali I Esenkaya M Can and M Karakaplan ldquoMono-planar versus biplanar medial open-wedge proximal tibialosteotomy for varus gonarthrosis A comparison of clinicaland radiological outcomesrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 12 pp 2689ndash2695 2013
[30] S Hinterwimmer K Beitzel J Paul et al ldquoControl of posteriortibial slope and patellar height in open-wedge valgus high tibialosteotomyrdquo American Journal of Sports Medicine vol 39 no 4pp 851ndash856 2011
[31] S Hopwood W Khan and S Agarwal ldquoThe biplanar openwedge high tibial osteotomy preserving the tibial tuberclerdquoJournal of Orthopaedic Science vol 21 no 6 pp 786ndash790 2016
[32] H Kesmezacar R Erginer T Ogut A Seyahi M Babacan andY Tenekecioglu ldquoEvaluation of patellar height and measure-ment methods after valgus high tibial osteotomyrdquo Knee SurgerySports Traumatology Arthroscopy vol 13 no 7 pp 539ndash5442005
[33] B A Rogers P Thornton-Bott S R Cannon and T W RBriggs ldquoInterobserver variation in the measurement of patellarheight after total knee arthroplastyrdquo Journal of Bone and JointSurgery - Series B vol 88 no 4 pp 484ndash488 2006
[34] R P Grelsamer C H Weinstein J Gould and A DubeyldquoPatellar tilt The physical examination correlates with MRimagingrdquo Knee vol 15 no 1 pp 3ndash8 2008
[35] R Gaasbeek R Welsing M Barink N Verdonschot andA Van Kampen ldquoThe influence of open and closed hightibial osteotomy on dynamic patellar tracking A biomechanicalstudyrdquo Knee Surgery Sports Traumatology Arthroscopy vol 15no 8 pp 978ndash984 2007
[36] H Bito R Takeuchi K Kumagai et al ldquoOpening wedge hightibial osteotomy affects both the lateral patellar tilt and patellarheightrdquo Knee Surgery Sports Traumatology Arthroscopy vol 18no 7 pp 955ndash960 2010
[37] T Sasaki and T Yagi ldquoSubluxation of the patella - Investigationby computerized tomographyrdquo International Orthopaedics vol10 no 2 pp 115ndash120 1986
[38] F Boven M-A Bellemans J Geurts and R PotvliegeldquoA comparative study of the patello-femoral joint on axialroentgenogram axial arthrogram and computed tomographyfollowing arthrographyrdquo Skeletal Radiology vol 8 no 3 pp179ndash181 1982
[39] A D Delgado-Martınez C Estrada E C Rodrıguez-MerchanM Atienza and J M Ordonez ldquoCT scanning of the
10 BioMed Research International
patellofemoral joint The quadriceps relaxed or contractedrdquoInternational Orthopaedics vol 20 no 3 pp 159ndash162 1996
[40] S Hinterwimmer M J Feucht J Paul et al ldquoAnalysis of theeffects of high tibial osteotomy on tibial rotationrdquo InternationalOrthopaedics vol 40 no 9 pp 1849ndash1854 2016
[41] K-M Jang J-H Lee H-J Park J L Kim and S-B HanldquoUnintended Rotational Changes of the Distal Tibia AfterBiplane Medial Open-Wedge High Tibial Osteotomyrdquo Journalof Arthroplasty vol 31 no 1 pp 59ndash63 2016
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
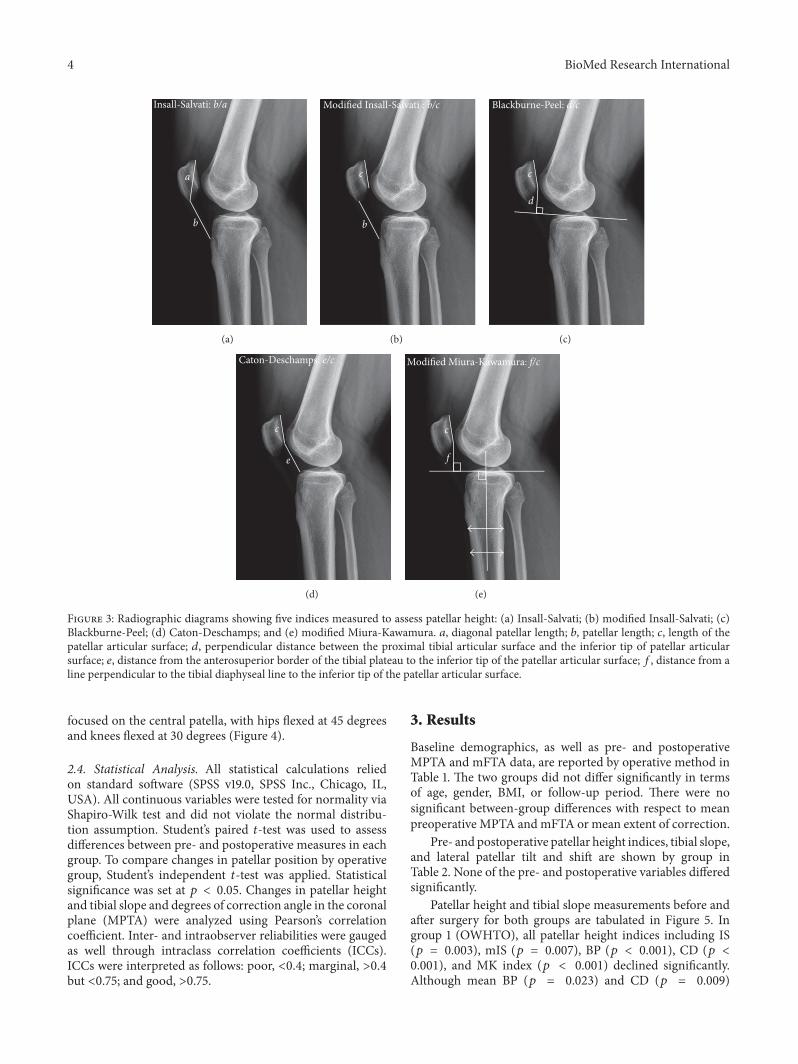
4 BioMed Research International
a
b
Insall-Salvati ba
(a)
c
b
Modified Insall-Salvati bc
(b)
c
d
Blackburne-Peel dc
(c)
c
e
Caton-Deschamps ec
(d)
c
f
Modified Miura-Kawamura fc
(e)
Figure 3 Radiographic diagrams showing five indices measured to assess patellar height (a) Insall-Salvati (b) modified Insall-Salvati (c)Blackburne-Peel (d) Caton-Deschamps and (e) modified Miura-Kawamura 119886 diagonal patellar length 119887 patellar length 119888 length of thepatellar articular surface 119889 perpendicular distance between the proximal tibial articular surface and the inferior tip of patellar articularsurface 119890 distance from the anterosuperior border of the tibial plateau to the inferior tip of the patellar articular surface 119891 distance from aline perpendicular to the tibial diaphyseal line to the inferior tip of the patellar articular surface
focused on the central patella with hips flexed at 45 degreesand knees flexed at 30 degrees (Figure 4)
24 Statistical Analysis All statistical calculations reliedon standard software (SPSS v190 SPSS Inc Chicago ILUSA) All continuous variables were tested for normality viaShapiro-Wilk test and did not violate the normal distribu-tion assumption Studentrsquos paired 119905-test was used to assessdifferences between pre- and postoperative measures in eachgroup To compare changes in patellar position by operativegroup Studentrsquos independent 119905-test was applied Statisticalsignificance was set at 119901 lt 005 Changes in patellar heightand tibial slope and degrees of correction angle in the coronalplane (MPTA) were analyzed using Pearsonrsquos correlationcoefficient Inter- and intraobserver reliabilities were gaugedas well through intraclass correlation coefficients (ICCs)ICCs were interpreted as follows poor lt04 marginal gt04but lt075 and good gt075
3 Results
Baseline demographics as well as pre- and postoperativeMPTA and mFTA data are reported by operative method inTable 1 The two groups did not differ significantly in termsof age gender BMI or follow-up period There were nosignificant between-group differences with respect to meanpreoperative MPTA andmFTA or mean extent of correction
Pre- and postoperative patellar height indices tibial slopeand lateral patellar tilt and shift are shown by group inTable 2 None of the pre- and postoperative variables differedsignificantly
Patellar height and tibial slope measurements before andafter surgery for both groups are tabulated in Figure 5 Ingroup 1 (OWHTO) all patellar height indices including IS(119901 = 0003) mIS (119901 = 0007) BP (119901 lt 0001) CD (119901 lt0001) and MK index (119901 lt 0001) declined significantlyAlthough mean BP (119901 = 0023) and CD (119901 = 0009)
BioMed Research International 5
(a)
L M
(b)
L M
p
c
p
c
(c)
Figure 4 Methods of assessing lateral patellar tilt (LPT) and lateral patellar shift (LPS) (a) patient positioned for computed tomographyimaging with knee in 30 degrees of flexion (b) LPT defined as the angle between a line intersecting the widest bony structure of the patellaand a line tangential to the anterior femoral condylar surfaces (c) LPS defined as the ratio of distances 11990111990110158401198881198881015840 where 1198881198881015840 is the distancebetween the summits of the medial and lateral femoral condyles and 1199011199011015840 is the distance between the summit of the lateral femoral condyleand the point where a line from the lateral edge of the patella perpendicular to the line that passed through the summits of the femoralcondyles crosses that line L lateral M medial
Table 1 Demographics and correction angles by operative group
Variables OWHTO (119899 = 30) OWHTODTO (119899 = 33) 119901 valueAge (years) 328 plusmn 75 305 plusmn 80 018Gender (male female) 8 22 13 20 023Body mass index (kgm2) 233 plusmn 52 245 plusmn 50 052Preoperative MPTA (degrees) 818 plusmn 19 823 plusmn 23 030Postoperative MPTA (degrees) 881 plusmn 20 883 plusmn 24 063Correction of MPTA (degrees) 62 plusmn 21 60 plusmn 27 064Preoperative mFTA (degrees) minus60 plusmn 18 minus64 plusmn 30 044Postoperative mFTA (degrees) 08 plusmn 15 03 plusmn 18 024Correction of mFTA (degrees) 68 plusmn 23 77 plusmn 31 024Follow-up period (months) 324 plusmn 87 331 plusmn 29 068Values expressed as mean plusmn SD OWHTO open wedge high tibial osteotomy DTO distal tubercle osteotomy MPTA medial proximal tibial angle mFTAmechanical femorotibial angle
Table 2 Pre- and postoperative radiographic measurements by operative group
Variables OWHTO (119899 = 30) OWHTODTO (119899 = 33) 119901 valuePreoperative Insall-Salvati 102 plusmn 013 101 plusmn 023 0932Postoperative Insall-Salvati 097 plusmn 012 100 plusmn 014 0353Preoperative modified Insall-Salvati 148 plusmn 013 146 plusmn 016 0701Postoperative modified Insall-Salvati 140 plusmn 015 147 plusmn 017 0072Preoperative Blackburne-Peel 080 plusmn 011 079 plusmn 011 0800Postoperative Blackburne-Peel 071 plusmn 015 076 plusmn 015 0138Preoperative Caton-Deschamps 093 plusmn 008 090 plusmn 012 0237Postoperative Caton-Deschamps 083 plusmn 011 086 plusmn 014 0265Preoperative modified Miura-Kawamura 089 plusmn 008 084 plusmn 012 0077Postoperative modified Miura-Kawamura 081 plusmn 012 083 plusmn 016 0552Preoperative tibial slope (degrees) 83 plusmn 35 87 plusmn 39 0655Postoperative tibial slope (degrees) 111 plusmn 323 112 plusmn 416 0943Preoperative lateral patella tilt (degrees) 141 plusmn 247 145 plusmn 369 0582Postoperative lateral patella tilt (degrees) 121 plusmn 218 131 plusmn 398 0249Preoperative lateral patella shift 014 plusmn 003 015 plusmn 047 0493Postoperative lateral patella shift 013 plusmn 004 014 plusmn 005 0450Values expressed as mean plusmn SD OWHTO open wedge high tibial osteotomy DTO distal tubercle osteotomy
6 BioMed Research International
PreoperativePostoperative
PreoperativePostoperative
0
02
04
06
08
1
12
14In
sall-
Salv
ati
0
02
04
06
08
1
12
Cato
n-D
esch
amps
0
02
04
06
08
1
12
14
16
18
Mod
ified
Insa
ll-Sa
lvat
i
0
2
4
6
8
10
12
14
Tibi
al sl
ope (
degr
ees)
OWHTO OWHTODTOOWHTO OWHTODTO0
010203040506070809
1
Blac
kbur
ne-P
eel
0
02
04
06
08
1
12
Miu
ra-K
awam
ura
lowast lowast lowast
lowast
lowast
lowast lowast
Figure 5 Patellar height indices and tibial slope pre- and postoperatively charted by operative group OWHTO open wedge high tibialosteotomy DTO distal tubercle osteotomy lowastSignificant change after surgery (119901 lt 005)
indices decreased significantly in group 2 (OWHTODTO)other patellar height indices were not significantly altered bysurgery Neither group showed significant change in meantibial slope
Average LPT decreased significantly after surgery inboth groups However no statistical differences between pre-operative and postoperative LPS were evident (Figure 6)
We compared the amount of change between group 1 andgroup 2 (Table 3) The amount of change of mIS BP CDand MK indices significantly differed between two groupsBecause of the small number of subjects independent 119905-testpower calculation was carried out using Power Analysis andSample Size 11 for Windows software package (NCSS IncLLC Kaysville UT USA) and the power was 076 for mIS
index 041 for BP index 064 for CD index and 073 for MKindex between group 1 and group 2
There were no significant correlations in either groupwith respect to patellar height or tibial slope changes ordegree of correction angle in coronal plane (MPTA)
Bone union at osteotomy sites was achieved at an averageof 3 months in all patients A total of two complicationsoccurred in group 2 In these two patients the tibialtuberosity fractured during tuberosity osteotomy Remediedby fixation screws these fractures healed in 3 months Noother complications such as wound infection delayed unionor nonunion were seen
Interrater reliability of all patellar indices measuredwas confirmed using (ICCs) based on radiographs before
BioMed Research International 7
Table 3 The amount of change for radiographic measurements by operative group
Variables OWHTO (119899 = 30) OWHTODTO (119899 = 33) 119901 valueInsall-Salvati minus005 plusmn 008 minus002 plusmn 020 0408Modified Insall-Salvati minus008 plusmn 014 000 plusmn 009 0002Blackburne-Peel minus009 plusmn 009 minus004 plusmn 013 0037Caton-Deschamps minus010 plusmn 009 minus004 plusmn 011 0008Modified Miura-Kawamura minus008 plusmn 009 minus001 plusmn 012 0010Tibial slope (degrees) 078 plusmn 306 047 plusmn 395 0705Lateral patella tilt (degrees) minus206 plusmn 176 minus141 plusmn 214 0218Lateral patella shift minus001 plusmn 003 minus001 plusmn 003 0661Values expressed as mean plusmn SD OWHTO open wedge high tibial osteotomy DTO distal tubercle osteotomy
and after surgery ICC ranges for intraobserver (075ndash091)and interobserver (072ndash09) reliabilities were comparable tothose of previous studies [14 28]
4 Discussion
Introduction of OWHTODTO was fueled by efforts tominimize surgery-related loss in patellar height and preventsubsequent patellofemoral problems [8] Several studiesoffer proof that this technique is effective in minimizingpostoperative patellar height change citing clinical out-comes comparable to conventional OWHTO in patients withosteoarthritis of the medial tibiofemoral compartment andvarus malalignment [8 14 15 29ndash31] However there wasno study investigating the surgical results of OWHTODTOin patients with normal knee Special concerns in this pop-ulation include unsightly aesthetics and pain or discomfortupon kneeling after surgery Therefore we have used thistechnique to correct proximal tibial varus deformities inyoung patients without pain or arthritic joints provingthat diminished patellar height is avoidable through thisapproach Considering the positional changes of the patellafollowing conventionalOWHTOmay induce new symptomsthese concerns will be addressed by OWHTODTO
In the present study we found significant postoperativedecreases in IS and mIS indices of the OWHTO groupwhereas these ratios were unchanged in the OWHTODTOgroup Outcomes herein were aligned with previous studiesthat similarly utilized these ratios to evaluate patellar height[14 15 29] Both IS and mIS are indirect measures of patellarheight any change reflecting altered patellar tendon length[14 32] Any slackening or shortening of patellar tendon thusimplied may be explained by intratendinous fibrosis or adhe-sions of proximal tuberosity following OWHTO whereas theextensor mechanism remains intact after OWHTODTO
Although there were significant postoperative declines inBP and CD indices of both groups the MK index of theOWHTODTO group was unchanged Still only one otherstudy corroborates our results [14]Most earlier investigationshave recorded no significant changes in BP and CD indicesafter OWHTODTO [8 15 29 30] This discrepancy may bedue to the method of measurement Both BP and CD indiceshave been viewed as highly reliable gauges of patellar height[28 33] but their dependency on joint line is disadvanta-geous given tibial plateau as a reference Because tibial slope
OWHTO OWHTODTO
PreoperativePostoperative
0
005
01
015
02
025
Late
ral p
atel
la sh
ift
0
2
4
6
8
10
12
14
16
18
20
Late
ral p
atel
la ti
lt (d
egre
es)
lowast
lowast
Figure 6 Lateral patellar tilt and lateral patellar shift pre- andpostoperatively charted by operative group OWHTO open wedgehigh tibial osteotomy DTO distal tubercle osteotomy lowastSignificantchange after surgery (119901 lt 005)
decreased postoperatively in both arms of our study evenminimal deviations in tibial slope may thus have bearing Weagree with other investigators that BP and CD indices shouldnot be relied upon in surgical procedures involving proximaltibia [23 32] In our opinion the decrease seen in MK index
8 BioMed Research International
reflects a true reduction in patellar height because MK indexis independent with the change of tibial slope
Although various radiographic techniques (based onaxial radiography CT or MRI) have been described forevaluating patellar inclination [34] use of LPT and LPSafter OWHTODTO has not previously been investigatedPrevious publications studying changes in LPT and LPS afterOWHTO have relied on axial radiography of load-bearingpatellofemoral joints (Delgado-Martins method) [7 24 3536] However determinations rendered by axial radiographymay be not accurate due to overlapping of images difficultyin positioning the leg and incidental angles of X-ray beams[37 38] CT imaging of contracted quadriceps muscle mayserve better in confirming patellar position [25 34 37 39]Consequently we used axial CT images in supine positionwith the knee in 30 degrees of flexion to measure LPT andLPS
Ultimately we found that LPT declined significantlyfor both procedures but the reductions did not differsignificantly by operative group Our findings followingOWHTO were consistent with those of previous stud-ies [35 36] whereby lessening of LPT was attributed toincreased lateral pull on the patella Although we expectedthat OWHTODTO would prevent any changes in LPTand LPS LPT surprisingly showed significant decline afterOWHTODTO as well One possible explanation for this isthat a change in mechanical axis may affect the inclinationof patella For another reason the change of tibial rotationafter OWHTOmay affect the LPT Previous studies reportedOWHTO made significant internal axial rotation of the tibia[40 41] However there was no change on tibial rotation aftervarus correction because we used two half-pins to check thechange of rotational alignment in the operating room
In our analysis no significant correlations emerged withrespect to change in patellar height change in tibial slopeor correction angle degree Prior reports have indicated thatOWHTODTO ismore effective than conventional OWHTOin patients requiring large (gt10-degree) angular corrections[8 14 15 30] However we could provide corroborationbecause correction angles for most of our patients werelt10 degrees and the surgical goal was to restore neutralalignment Hence the protective effect of OWHTODTO onpatellar height after large angular correction (gt10 degrees)could not be fully evaluated by this study
There were two tibial tuberosity fractures in OWHTODTO group Only one previous literature reported samesurgical complications [8]Therewas no such complication inother reports using OWHTODTO [14 15 29 30]Thereforeit seems that tibial tuberosity fracture is related to mistakeof surgical procedure not the degrees of correction angleAdditionally in our study such fractures occurred at an earlystage in our learning curve and healed well with additionalscrew fixation Eventually we think that tibial tuberosityfracture is easily preventable with caution leaving at least a1-cm thickness on the proximal tuberosity fragment
Our study has some limitations First it is a retrospectiveinvestigation and not a randomized trial Also the twooperative groups reflected a shift in surgical technique ratherthan pure randomization Nevertheless the two groups were
well matched at baseline in terms of preoperative variablesAnother limitation was that blinding of the OWHTODTOarm was not feasible when measuring radiologic param-eters postoperatively even if two independent orthopedicresidents participated Finally radiographic parameters werethe primary focus To investigate the relationship betweenradiologic findings and clinical outcomes a well-plannedfuture prospective study is needed
There are various methods for correcting proximal tibialvara deformity and best surgical techniquemust be individu-alized Compared to conventional OWHTO OWHTODTOdid not influence patella height associated with the procedureand was considered an useful method to preserve patellaheight
Ethical Approval
This study was conducted following the approval of Institu-tional Review Board of Severance Hospital Yonsei UniversityCollege of Medicine (IRB number 4-2015-0796)
Conflicts of Interest
The authors declare that there are no conflicts of interest toreport regarding the work and publication of this study
Acknowledgments
The authors thank Dr Sung Min Kim and Jung Woo Lee forthe data measurement of the patients
References
[1] W Strecker ldquoPlanning Analysis of Knee-Adjacent DeformitiesrdquoEuropean Journal of Trauma and Emergency Surgery vol 33 no6 pp 662ndash668 2007
[2] R Rossi D E Bonasia and A Amendola ldquoThe Role of HighTibial Osteotomy in the Varus Kneerdquo American Academy ofOrthopaedic Surgeon vol 19 no 10 pp 590ndash599 2011
[3] R K Marti R A W Verhagen G M M J Kerkhoffs andT M Moojen ldquoProximal tibial varus osteotomy Indicationstechnique and five to twenty-one-year resultsrdquo Journal of Boneand Joint Surgery - Series A vol 83 no 2 pp 164ndash170 2001
[4] H El-Azab P Glabgly J Paul A B Imhoff and S Hinterwim-mer ldquoPatellar height and posterior tibial slope after open- andclosed-wedge high tibial osteotomy A radiological study on 100patientsrdquoAmerican Journal of Sports Medicine vol 38 no 2 pp323ndash329 2010
[5] B P Kaper R B Bourne C H Rorabeck and S J MacDonaldldquoPatellar infera after high tibial osteotomyrdquo Journal of Arthro-plasty vol 16 no 2 pp 168ndash173 2001
[6] D Tigani D Ferrari P Trentani G Barbanti-Brodano and FTrentani ldquoPatellar height after high tibial osteotomyrdquo Interna-tional Orthopaedics vol 24 no 6 pp 331ndash334 2001
[7] J-H Yang S-H Lee K S Nathawat S-H Jeon and K-JOh ldquoThe effect of biplane medial opening wedge high tibialosteotomy on patellofemoral joint indicesrdquo Knee vol 20 no 2pp 128ndash132 2013
[8] R D A Gaasbeek H Sonneveld R J Van Heerwaarden W CH Jacobs and A B Wymenga ldquoDistal tuberosity osteotomy in
BioMed Research International 9
open wedge high tibial osteotomy can prevent patella infera Anew techniquerdquo Knee vol 11 no 6 pp 457ndash461 2004
[9] C M Rodner D J Adams V Diaz-Doran et al ldquoMedialopeningwedge tibial osteotomy and the sagittal planeThe effectof increasing tibial slope on tibiofemoral contact pressurerdquoAmerican Journal of SportsMedicine vol 34 no 9 pp 1431ndash14412006
[10] R E Windsor J N Insall and K G Vince ldquoTechnicalconsiderations of total knee arthroplasty after proximal tibialosteotomyrdquo Journal of Bone and Joint Surgery - Series A vol 70no 4 pp 547ndash555 1988
[11] H E Figgie III V M Goldberg K G Heiple H S MollerIII and N H Gordon ldquoThe influence of tibial-patellofemorallocation on function of the knee in patients with the posteriorstabilized condylar knee prosthesisrdquo Journal of Bone and JointSurgery - Series A vol 68 no 7 pp 1035ndash1040 1986
[12] K Kim D Kim S Song S Lee and D Bae ldquoMedialOpen-Wedge High Tibial Osteotomy May Adversely Affect thePatellofemoral Jointrdquo Arthroscopy The Journal of Arthroscopicamp Related Surgery vol 33 no 4 pp 811ndash816 2017
[13] J S Shim S H Lee H J Jung and H I Lee ldquoHightibial open wedge osteotomy below the tibial tubercle Clinicaland radiographic resultsrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 1 pp 57ndash63 2013
[14] P D Longino T B Birmingham W J Schultz R F Moyerand J R Giffin ldquoCombined tibial tubercle osteotomy withmedial openingwedge high tibial osteotomyminimizes changesin patellar height A prospective cohort study with historicalcontrolsrdquo American Journal of Sports Medicine vol 41 no 12pp 2849ndash2857 2013
[15] S Keyhani M R Abbasian S M Kazemi et al ldquoModifiedretro-tubercle opening-wedge versus conventional high tibialosteotomyrdquo Orthopedics vol 34 no 2 2011
[16] D H Lee K J Ryu H H Kim S Soung and S Shin ldquoFixator-assisted Technique Enables Less Invasive Plate Osteosynthesisin Medial Opening-wedge High Tibial Osteotomy A NovelTechniquerdquo Clinical Orthopaedics and Related Research vol473 no 10 pp 3133ndash3142 2015
[17] S B Han D H Lee G M Shetty D J Chae J G Songand K W Nha ldquoA ldquosafe zonerdquo in medial open-wedge hightibia osteotomy to prevent lateral cortex fracturerdquoKnee SurgerySports Traumatology Arthroscopy vol 21 no 1 pp 90ndash95 2013
[18] D Paley and K Tetsworth ldquoMechanical axis deviation ofthe lower limbs Preoperative planning of uniapical angulardeformities of the tibia or femurrdquo Clinical Orthopaedics andRelated Research no 280 pp 48ndash64 1992
[19] J Insall and E Salvati ldquoPatella position in the normal kneejointrdquo Radiology vol 101 no 1 pp 101ndash104 1971
[20] R P Grelsamer and S Meadows ldquoThe modified Insall-Salvatiratio for assessment of patellar heightrdquo Clinical Orthopaedicsand Related Research no 282 pp 170ndash176 1992
[21] J S Blackburne and T E Peel ldquoA new method of measuringpatellar heightrdquo J Bone Joint Surg Br vol 59 no 2 pp 241-2421977
[22] J Caton G Deschamps P Chambat J L Lerat and HDejour ldquoPatella infera Apropos of 128 casesrdquo Rev Chir OrthopReparatrice Appar Mot vol 68 no 5 pp 317ndash325 1982
[23] H Miura H Kawamura R Nagamine K Urabe and YIwamoto ldquoIs patellar height really lower after high tibialosteotomyrdquo Fukuoka igaku zasshi = Hukuoka acta medica vol88 no 6 pp 261ndash266 1997
[24] H Delgado-Martins ldquoThe bicondylo-patellar angle as a mea-sure of patellar tiltingrdquo Archives of Orthopaedic and TraumaticSurgery vol 96 no 4 pp 303-304 1980
[25] V Vahasarja P Lanning S Lahde and W Serlo ldquoAxialradiography or CT in the measurement of patellofemoralmalalignment indices in children and adolescentsrdquo ClinicalRadiology vol 51 no 9 pp 639ndash643 1996
[26] U M Kujala K Osterman M Kormano M Komu and DSchlenzka ldquoPatellar motion analyzed by magnetic resonanceimagingrdquo Acta Orthopaedica vol 60 no 1 pp 13ndash16 1989
[27] C A Laurin R Dussault and H P Levesque ldquoThe tan-gential X-ray investigation of the patellofemoral joint X-raytechnique diagnostic criteria and their interpretationrdquo ClinicalOrthopaedics and Related Research no 144 pp 16ndash26 1979
[28] R Seil B Muller T Georg D Kohn and S Rupp ldquoReliabilityand interobserver variability in radiological patellar heightratiosrdquo Knee Surgery Sports Traumatology Arthroscopy vol 8no 4 pp 231ndash236 2000
[29] N Elmali I Esenkaya M Can and M Karakaplan ldquoMono-planar versus biplanar medial open-wedge proximal tibialosteotomy for varus gonarthrosis A comparison of clinicaland radiological outcomesrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 12 pp 2689ndash2695 2013
[30] S Hinterwimmer K Beitzel J Paul et al ldquoControl of posteriortibial slope and patellar height in open-wedge valgus high tibialosteotomyrdquo American Journal of Sports Medicine vol 39 no 4pp 851ndash856 2011
[31] S Hopwood W Khan and S Agarwal ldquoThe biplanar openwedge high tibial osteotomy preserving the tibial tuberclerdquoJournal of Orthopaedic Science vol 21 no 6 pp 786ndash790 2016
[32] H Kesmezacar R Erginer T Ogut A Seyahi M Babacan andY Tenekecioglu ldquoEvaluation of patellar height and measure-ment methods after valgus high tibial osteotomyrdquo Knee SurgerySports Traumatology Arthroscopy vol 13 no 7 pp 539ndash5442005
[33] B A Rogers P Thornton-Bott S R Cannon and T W RBriggs ldquoInterobserver variation in the measurement of patellarheight after total knee arthroplastyrdquo Journal of Bone and JointSurgery - Series B vol 88 no 4 pp 484ndash488 2006
[34] R P Grelsamer C H Weinstein J Gould and A DubeyldquoPatellar tilt The physical examination correlates with MRimagingrdquo Knee vol 15 no 1 pp 3ndash8 2008
[35] R Gaasbeek R Welsing M Barink N Verdonschot andA Van Kampen ldquoThe influence of open and closed hightibial osteotomy on dynamic patellar tracking A biomechanicalstudyrdquo Knee Surgery Sports Traumatology Arthroscopy vol 15no 8 pp 978ndash984 2007
[36] H Bito R Takeuchi K Kumagai et al ldquoOpening wedge hightibial osteotomy affects both the lateral patellar tilt and patellarheightrdquo Knee Surgery Sports Traumatology Arthroscopy vol 18no 7 pp 955ndash960 2010
[37] T Sasaki and T Yagi ldquoSubluxation of the patella - Investigationby computerized tomographyrdquo International Orthopaedics vol10 no 2 pp 115ndash120 1986
[38] F Boven M-A Bellemans J Geurts and R PotvliegeldquoA comparative study of the patello-femoral joint on axialroentgenogram axial arthrogram and computed tomographyfollowing arthrographyrdquo Skeletal Radiology vol 8 no 3 pp179ndash181 1982
[39] A D Delgado-Martınez C Estrada E C Rodrıguez-MerchanM Atienza and J M Ordonez ldquoCT scanning of the
10 BioMed Research International
patellofemoral joint The quadriceps relaxed or contractedrdquoInternational Orthopaedics vol 20 no 3 pp 159ndash162 1996
[40] S Hinterwimmer M J Feucht J Paul et al ldquoAnalysis of theeffects of high tibial osteotomy on tibial rotationrdquo InternationalOrthopaedics vol 40 no 9 pp 1849ndash1854 2016
[41] K-M Jang J-H Lee H-J Park J L Kim and S-B HanldquoUnintended Rotational Changes of the Distal Tibia AfterBiplane Medial Open-Wedge High Tibial Osteotomyrdquo Journalof Arthroplasty vol 31 no 1 pp 59ndash63 2016
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
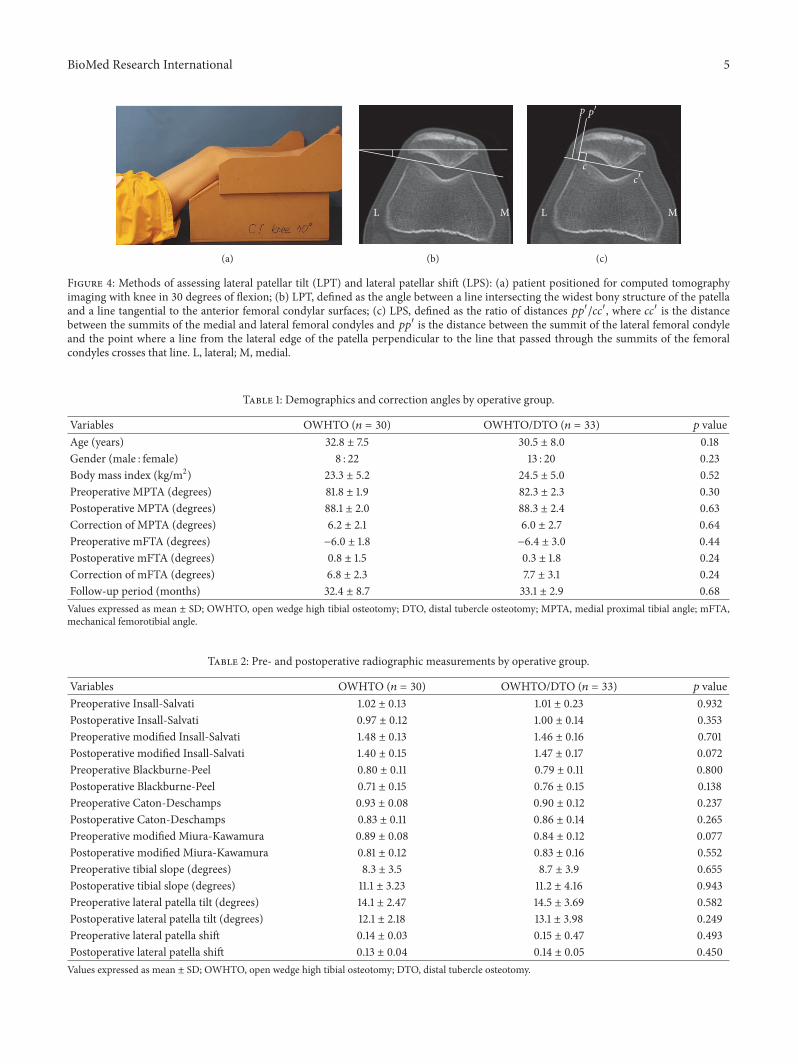
BioMed Research International 5
(a)
L M
(b)
L M
p
c
p
c
(c)
Figure 4 Methods of assessing lateral patellar tilt (LPT) and lateral patellar shift (LPS) (a) patient positioned for computed tomographyimaging with knee in 30 degrees of flexion (b) LPT defined as the angle between a line intersecting the widest bony structure of the patellaand a line tangential to the anterior femoral condylar surfaces (c) LPS defined as the ratio of distances 11990111990110158401198881198881015840 where 1198881198881015840 is the distancebetween the summits of the medial and lateral femoral condyles and 1199011199011015840 is the distance between the summit of the lateral femoral condyleand the point where a line from the lateral edge of the patella perpendicular to the line that passed through the summits of the femoralcondyles crosses that line L lateral M medial
Table 1 Demographics and correction angles by operative group
Variables OWHTO (119899 = 30) OWHTODTO (119899 = 33) 119901 valueAge (years) 328 plusmn 75 305 plusmn 80 018Gender (male female) 8 22 13 20 023Body mass index (kgm2) 233 plusmn 52 245 plusmn 50 052Preoperative MPTA (degrees) 818 plusmn 19 823 plusmn 23 030Postoperative MPTA (degrees) 881 plusmn 20 883 plusmn 24 063Correction of MPTA (degrees) 62 plusmn 21 60 plusmn 27 064Preoperative mFTA (degrees) minus60 plusmn 18 minus64 plusmn 30 044Postoperative mFTA (degrees) 08 plusmn 15 03 plusmn 18 024Correction of mFTA (degrees) 68 plusmn 23 77 plusmn 31 024Follow-up period (months) 324 plusmn 87 331 plusmn 29 068Values expressed as mean plusmn SD OWHTO open wedge high tibial osteotomy DTO distal tubercle osteotomy MPTA medial proximal tibial angle mFTAmechanical femorotibial angle
Table 2 Pre- and postoperative radiographic measurements by operative group
Variables OWHTO (119899 = 30) OWHTODTO (119899 = 33) 119901 valuePreoperative Insall-Salvati 102 plusmn 013 101 plusmn 023 0932Postoperative Insall-Salvati 097 plusmn 012 100 plusmn 014 0353Preoperative modified Insall-Salvati 148 plusmn 013 146 plusmn 016 0701Postoperative modified Insall-Salvati 140 plusmn 015 147 plusmn 017 0072Preoperative Blackburne-Peel 080 plusmn 011 079 plusmn 011 0800Postoperative Blackburne-Peel 071 plusmn 015 076 plusmn 015 0138Preoperative Caton-Deschamps 093 plusmn 008 090 plusmn 012 0237Postoperative Caton-Deschamps 083 plusmn 011 086 plusmn 014 0265Preoperative modified Miura-Kawamura 089 plusmn 008 084 plusmn 012 0077Postoperative modified Miura-Kawamura 081 plusmn 012 083 plusmn 016 0552Preoperative tibial slope (degrees) 83 plusmn 35 87 plusmn 39 0655Postoperative tibial slope (degrees) 111 plusmn 323 112 plusmn 416 0943Preoperative lateral patella tilt (degrees) 141 plusmn 247 145 plusmn 369 0582Postoperative lateral patella tilt (degrees) 121 plusmn 218 131 plusmn 398 0249Preoperative lateral patella shift 014 plusmn 003 015 plusmn 047 0493Postoperative lateral patella shift 013 plusmn 004 014 plusmn 005 0450Values expressed as mean plusmn SD OWHTO open wedge high tibial osteotomy DTO distal tubercle osteotomy
6 BioMed Research International
PreoperativePostoperative
PreoperativePostoperative
0
02
04
06
08
1
12
14In
sall-
Salv
ati
0
02
04
06
08
1
12
Cato
n-D
esch
amps
0
02
04
06
08
1
12
14
16
18
Mod
ified
Insa
ll-Sa
lvat
i
0
2
4
6
8
10
12
14
Tibi
al sl
ope (
degr
ees)
OWHTO OWHTODTOOWHTO OWHTODTO0
010203040506070809
1
Blac
kbur
ne-P
eel
0
02
04
06
08
1
12
Miu
ra-K
awam
ura
lowast lowast lowast
lowast
lowast
lowast lowast
Figure 5 Patellar height indices and tibial slope pre- and postoperatively charted by operative group OWHTO open wedge high tibialosteotomy DTO distal tubercle osteotomy lowastSignificant change after surgery (119901 lt 005)
indices decreased significantly in group 2 (OWHTODTO)other patellar height indices were not significantly altered bysurgery Neither group showed significant change in meantibial slope
Average LPT decreased significantly after surgery inboth groups However no statistical differences between pre-operative and postoperative LPS were evident (Figure 6)
We compared the amount of change between group 1 andgroup 2 (Table 3) The amount of change of mIS BP CDand MK indices significantly differed between two groupsBecause of the small number of subjects independent 119905-testpower calculation was carried out using Power Analysis andSample Size 11 for Windows software package (NCSS IncLLC Kaysville UT USA) and the power was 076 for mIS
index 041 for BP index 064 for CD index and 073 for MKindex between group 1 and group 2
There were no significant correlations in either groupwith respect to patellar height or tibial slope changes ordegree of correction angle in coronal plane (MPTA)
Bone union at osteotomy sites was achieved at an averageof 3 months in all patients A total of two complicationsoccurred in group 2 In these two patients the tibialtuberosity fractured during tuberosity osteotomy Remediedby fixation screws these fractures healed in 3 months Noother complications such as wound infection delayed unionor nonunion were seen
Interrater reliability of all patellar indices measuredwas confirmed using (ICCs) based on radiographs before
BioMed Research International 7
Table 3 The amount of change for radiographic measurements by operative group
Variables OWHTO (119899 = 30) OWHTODTO (119899 = 33) 119901 valueInsall-Salvati minus005 plusmn 008 minus002 plusmn 020 0408Modified Insall-Salvati minus008 plusmn 014 000 plusmn 009 0002Blackburne-Peel minus009 plusmn 009 minus004 plusmn 013 0037Caton-Deschamps minus010 plusmn 009 minus004 plusmn 011 0008Modified Miura-Kawamura minus008 plusmn 009 minus001 plusmn 012 0010Tibial slope (degrees) 078 plusmn 306 047 plusmn 395 0705Lateral patella tilt (degrees) minus206 plusmn 176 minus141 plusmn 214 0218Lateral patella shift minus001 plusmn 003 minus001 plusmn 003 0661Values expressed as mean plusmn SD OWHTO open wedge high tibial osteotomy DTO distal tubercle osteotomy
and after surgery ICC ranges for intraobserver (075ndash091)and interobserver (072ndash09) reliabilities were comparable tothose of previous studies [14 28]
4 Discussion
Introduction of OWHTODTO was fueled by efforts tominimize surgery-related loss in patellar height and preventsubsequent patellofemoral problems [8] Several studiesoffer proof that this technique is effective in minimizingpostoperative patellar height change citing clinical out-comes comparable to conventional OWHTO in patients withosteoarthritis of the medial tibiofemoral compartment andvarus malalignment [8 14 15 29ndash31] However there wasno study investigating the surgical results of OWHTODTOin patients with normal knee Special concerns in this pop-ulation include unsightly aesthetics and pain or discomfortupon kneeling after surgery Therefore we have used thistechnique to correct proximal tibial varus deformities inyoung patients without pain or arthritic joints provingthat diminished patellar height is avoidable through thisapproach Considering the positional changes of the patellafollowing conventionalOWHTOmay induce new symptomsthese concerns will be addressed by OWHTODTO
In the present study we found significant postoperativedecreases in IS and mIS indices of the OWHTO groupwhereas these ratios were unchanged in the OWHTODTOgroup Outcomes herein were aligned with previous studiesthat similarly utilized these ratios to evaluate patellar height[14 15 29] Both IS and mIS are indirect measures of patellarheight any change reflecting altered patellar tendon length[14 32] Any slackening or shortening of patellar tendon thusimplied may be explained by intratendinous fibrosis or adhe-sions of proximal tuberosity following OWHTO whereas theextensor mechanism remains intact after OWHTODTO
Although there were significant postoperative declines inBP and CD indices of both groups the MK index of theOWHTODTO group was unchanged Still only one otherstudy corroborates our results [14]Most earlier investigationshave recorded no significant changes in BP and CD indicesafter OWHTODTO [8 15 29 30] This discrepancy may bedue to the method of measurement Both BP and CD indiceshave been viewed as highly reliable gauges of patellar height[28 33] but their dependency on joint line is disadvanta-geous given tibial plateau as a reference Because tibial slope
OWHTO OWHTODTO
PreoperativePostoperative
0
005
01
015
02
025
Late
ral p
atel
la sh
ift
0
2
4
6
8
10
12
14
16
18
20
Late
ral p
atel
la ti
lt (d
egre
es)
lowast
lowast
Figure 6 Lateral patellar tilt and lateral patellar shift pre- andpostoperatively charted by operative group OWHTO open wedgehigh tibial osteotomy DTO distal tubercle osteotomy lowastSignificantchange after surgery (119901 lt 005)
decreased postoperatively in both arms of our study evenminimal deviations in tibial slope may thus have bearing Weagree with other investigators that BP and CD indices shouldnot be relied upon in surgical procedures involving proximaltibia [23 32] In our opinion the decrease seen in MK index
8 BioMed Research International
reflects a true reduction in patellar height because MK indexis independent with the change of tibial slope
Although various radiographic techniques (based onaxial radiography CT or MRI) have been described forevaluating patellar inclination [34] use of LPT and LPSafter OWHTODTO has not previously been investigatedPrevious publications studying changes in LPT and LPS afterOWHTO have relied on axial radiography of load-bearingpatellofemoral joints (Delgado-Martins method) [7 24 3536] However determinations rendered by axial radiographymay be not accurate due to overlapping of images difficultyin positioning the leg and incidental angles of X-ray beams[37 38] CT imaging of contracted quadriceps muscle mayserve better in confirming patellar position [25 34 37 39]Consequently we used axial CT images in supine positionwith the knee in 30 degrees of flexion to measure LPT andLPS
Ultimately we found that LPT declined significantlyfor both procedures but the reductions did not differsignificantly by operative group Our findings followingOWHTO were consistent with those of previous stud-ies [35 36] whereby lessening of LPT was attributed toincreased lateral pull on the patella Although we expectedthat OWHTODTO would prevent any changes in LPTand LPS LPT surprisingly showed significant decline afterOWHTODTO as well One possible explanation for this isthat a change in mechanical axis may affect the inclinationof patella For another reason the change of tibial rotationafter OWHTOmay affect the LPT Previous studies reportedOWHTO made significant internal axial rotation of the tibia[40 41] However there was no change on tibial rotation aftervarus correction because we used two half-pins to check thechange of rotational alignment in the operating room
In our analysis no significant correlations emerged withrespect to change in patellar height change in tibial slopeor correction angle degree Prior reports have indicated thatOWHTODTO ismore effective than conventional OWHTOin patients requiring large (gt10-degree) angular corrections[8 14 15 30] However we could provide corroborationbecause correction angles for most of our patients werelt10 degrees and the surgical goal was to restore neutralalignment Hence the protective effect of OWHTODTO onpatellar height after large angular correction (gt10 degrees)could not be fully evaluated by this study
There were two tibial tuberosity fractures in OWHTODTO group Only one previous literature reported samesurgical complications [8]Therewas no such complication inother reports using OWHTODTO [14 15 29 30]Thereforeit seems that tibial tuberosity fracture is related to mistakeof surgical procedure not the degrees of correction angleAdditionally in our study such fractures occurred at an earlystage in our learning curve and healed well with additionalscrew fixation Eventually we think that tibial tuberosityfracture is easily preventable with caution leaving at least a1-cm thickness on the proximal tuberosity fragment
Our study has some limitations First it is a retrospectiveinvestigation and not a randomized trial Also the twooperative groups reflected a shift in surgical technique ratherthan pure randomization Nevertheless the two groups were
well matched at baseline in terms of preoperative variablesAnother limitation was that blinding of the OWHTODTOarm was not feasible when measuring radiologic param-eters postoperatively even if two independent orthopedicresidents participated Finally radiographic parameters werethe primary focus To investigate the relationship betweenradiologic findings and clinical outcomes a well-plannedfuture prospective study is needed
There are various methods for correcting proximal tibialvara deformity and best surgical techniquemust be individu-alized Compared to conventional OWHTO OWHTODTOdid not influence patella height associated with the procedureand was considered an useful method to preserve patellaheight
Ethical Approval
This study was conducted following the approval of Institu-tional Review Board of Severance Hospital Yonsei UniversityCollege of Medicine (IRB number 4-2015-0796)
Conflicts of Interest
The authors declare that there are no conflicts of interest toreport regarding the work and publication of this study
Acknowledgments
The authors thank Dr Sung Min Kim and Jung Woo Lee forthe data measurement of the patients
References
[1] W Strecker ldquoPlanning Analysis of Knee-Adjacent DeformitiesrdquoEuropean Journal of Trauma and Emergency Surgery vol 33 no6 pp 662ndash668 2007
[2] R Rossi D E Bonasia and A Amendola ldquoThe Role of HighTibial Osteotomy in the Varus Kneerdquo American Academy ofOrthopaedic Surgeon vol 19 no 10 pp 590ndash599 2011
[3] R K Marti R A W Verhagen G M M J Kerkhoffs andT M Moojen ldquoProximal tibial varus osteotomy Indicationstechnique and five to twenty-one-year resultsrdquo Journal of Boneand Joint Surgery - Series A vol 83 no 2 pp 164ndash170 2001
[4] H El-Azab P Glabgly J Paul A B Imhoff and S Hinterwim-mer ldquoPatellar height and posterior tibial slope after open- andclosed-wedge high tibial osteotomy A radiological study on 100patientsrdquoAmerican Journal of Sports Medicine vol 38 no 2 pp323ndash329 2010
[5] B P Kaper R B Bourne C H Rorabeck and S J MacDonaldldquoPatellar infera after high tibial osteotomyrdquo Journal of Arthro-plasty vol 16 no 2 pp 168ndash173 2001
[6] D Tigani D Ferrari P Trentani G Barbanti-Brodano and FTrentani ldquoPatellar height after high tibial osteotomyrdquo Interna-tional Orthopaedics vol 24 no 6 pp 331ndash334 2001
[7] J-H Yang S-H Lee K S Nathawat S-H Jeon and K-JOh ldquoThe effect of biplane medial opening wedge high tibialosteotomy on patellofemoral joint indicesrdquo Knee vol 20 no 2pp 128ndash132 2013
[8] R D A Gaasbeek H Sonneveld R J Van Heerwaarden W CH Jacobs and A B Wymenga ldquoDistal tuberosity osteotomy in
BioMed Research International 9
open wedge high tibial osteotomy can prevent patella infera Anew techniquerdquo Knee vol 11 no 6 pp 457ndash461 2004
[9] C M Rodner D J Adams V Diaz-Doran et al ldquoMedialopeningwedge tibial osteotomy and the sagittal planeThe effectof increasing tibial slope on tibiofemoral contact pressurerdquoAmerican Journal of SportsMedicine vol 34 no 9 pp 1431ndash14412006
[10] R E Windsor J N Insall and K G Vince ldquoTechnicalconsiderations of total knee arthroplasty after proximal tibialosteotomyrdquo Journal of Bone and Joint Surgery - Series A vol 70no 4 pp 547ndash555 1988
[11] H E Figgie III V M Goldberg K G Heiple H S MollerIII and N H Gordon ldquoThe influence of tibial-patellofemorallocation on function of the knee in patients with the posteriorstabilized condylar knee prosthesisrdquo Journal of Bone and JointSurgery - Series A vol 68 no 7 pp 1035ndash1040 1986
[12] K Kim D Kim S Song S Lee and D Bae ldquoMedialOpen-Wedge High Tibial Osteotomy May Adversely Affect thePatellofemoral Jointrdquo Arthroscopy The Journal of Arthroscopicamp Related Surgery vol 33 no 4 pp 811ndash816 2017
[13] J S Shim S H Lee H J Jung and H I Lee ldquoHightibial open wedge osteotomy below the tibial tubercle Clinicaland radiographic resultsrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 1 pp 57ndash63 2013
[14] P D Longino T B Birmingham W J Schultz R F Moyerand J R Giffin ldquoCombined tibial tubercle osteotomy withmedial openingwedge high tibial osteotomyminimizes changesin patellar height A prospective cohort study with historicalcontrolsrdquo American Journal of Sports Medicine vol 41 no 12pp 2849ndash2857 2013
[15] S Keyhani M R Abbasian S M Kazemi et al ldquoModifiedretro-tubercle opening-wedge versus conventional high tibialosteotomyrdquo Orthopedics vol 34 no 2 2011
[16] D H Lee K J Ryu H H Kim S Soung and S Shin ldquoFixator-assisted Technique Enables Less Invasive Plate Osteosynthesisin Medial Opening-wedge High Tibial Osteotomy A NovelTechniquerdquo Clinical Orthopaedics and Related Research vol473 no 10 pp 3133ndash3142 2015
[17] S B Han D H Lee G M Shetty D J Chae J G Songand K W Nha ldquoA ldquosafe zonerdquo in medial open-wedge hightibia osteotomy to prevent lateral cortex fracturerdquoKnee SurgerySports Traumatology Arthroscopy vol 21 no 1 pp 90ndash95 2013
[18] D Paley and K Tetsworth ldquoMechanical axis deviation ofthe lower limbs Preoperative planning of uniapical angulardeformities of the tibia or femurrdquo Clinical Orthopaedics andRelated Research no 280 pp 48ndash64 1992
[19] J Insall and E Salvati ldquoPatella position in the normal kneejointrdquo Radiology vol 101 no 1 pp 101ndash104 1971
[20] R P Grelsamer and S Meadows ldquoThe modified Insall-Salvatiratio for assessment of patellar heightrdquo Clinical Orthopaedicsand Related Research no 282 pp 170ndash176 1992
[21] J S Blackburne and T E Peel ldquoA new method of measuringpatellar heightrdquo J Bone Joint Surg Br vol 59 no 2 pp 241-2421977
[22] J Caton G Deschamps P Chambat J L Lerat and HDejour ldquoPatella infera Apropos of 128 casesrdquo Rev Chir OrthopReparatrice Appar Mot vol 68 no 5 pp 317ndash325 1982
[23] H Miura H Kawamura R Nagamine K Urabe and YIwamoto ldquoIs patellar height really lower after high tibialosteotomyrdquo Fukuoka igaku zasshi = Hukuoka acta medica vol88 no 6 pp 261ndash266 1997
[24] H Delgado-Martins ldquoThe bicondylo-patellar angle as a mea-sure of patellar tiltingrdquo Archives of Orthopaedic and TraumaticSurgery vol 96 no 4 pp 303-304 1980
[25] V Vahasarja P Lanning S Lahde and W Serlo ldquoAxialradiography or CT in the measurement of patellofemoralmalalignment indices in children and adolescentsrdquo ClinicalRadiology vol 51 no 9 pp 639ndash643 1996
[26] U M Kujala K Osterman M Kormano M Komu and DSchlenzka ldquoPatellar motion analyzed by magnetic resonanceimagingrdquo Acta Orthopaedica vol 60 no 1 pp 13ndash16 1989
[27] C A Laurin R Dussault and H P Levesque ldquoThe tan-gential X-ray investigation of the patellofemoral joint X-raytechnique diagnostic criteria and their interpretationrdquo ClinicalOrthopaedics and Related Research no 144 pp 16ndash26 1979
[28] R Seil B Muller T Georg D Kohn and S Rupp ldquoReliabilityand interobserver variability in radiological patellar heightratiosrdquo Knee Surgery Sports Traumatology Arthroscopy vol 8no 4 pp 231ndash236 2000
[29] N Elmali I Esenkaya M Can and M Karakaplan ldquoMono-planar versus biplanar medial open-wedge proximal tibialosteotomy for varus gonarthrosis A comparison of clinicaland radiological outcomesrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 12 pp 2689ndash2695 2013
[30] S Hinterwimmer K Beitzel J Paul et al ldquoControl of posteriortibial slope and patellar height in open-wedge valgus high tibialosteotomyrdquo American Journal of Sports Medicine vol 39 no 4pp 851ndash856 2011
[31] S Hopwood W Khan and S Agarwal ldquoThe biplanar openwedge high tibial osteotomy preserving the tibial tuberclerdquoJournal of Orthopaedic Science vol 21 no 6 pp 786ndash790 2016
[32] H Kesmezacar R Erginer T Ogut A Seyahi M Babacan andY Tenekecioglu ldquoEvaluation of patellar height and measure-ment methods after valgus high tibial osteotomyrdquo Knee SurgerySports Traumatology Arthroscopy vol 13 no 7 pp 539ndash5442005
[33] B A Rogers P Thornton-Bott S R Cannon and T W RBriggs ldquoInterobserver variation in the measurement of patellarheight after total knee arthroplastyrdquo Journal of Bone and JointSurgery - Series B vol 88 no 4 pp 484ndash488 2006
[34] R P Grelsamer C H Weinstein J Gould and A DubeyldquoPatellar tilt The physical examination correlates with MRimagingrdquo Knee vol 15 no 1 pp 3ndash8 2008
[35] R Gaasbeek R Welsing M Barink N Verdonschot andA Van Kampen ldquoThe influence of open and closed hightibial osteotomy on dynamic patellar tracking A biomechanicalstudyrdquo Knee Surgery Sports Traumatology Arthroscopy vol 15no 8 pp 978ndash984 2007
[36] H Bito R Takeuchi K Kumagai et al ldquoOpening wedge hightibial osteotomy affects both the lateral patellar tilt and patellarheightrdquo Knee Surgery Sports Traumatology Arthroscopy vol 18no 7 pp 955ndash960 2010
[37] T Sasaki and T Yagi ldquoSubluxation of the patella - Investigationby computerized tomographyrdquo International Orthopaedics vol10 no 2 pp 115ndash120 1986
[38] F Boven M-A Bellemans J Geurts and R PotvliegeldquoA comparative study of the patello-femoral joint on axialroentgenogram axial arthrogram and computed tomographyfollowing arthrographyrdquo Skeletal Radiology vol 8 no 3 pp179ndash181 1982
[39] A D Delgado-Martınez C Estrada E C Rodrıguez-MerchanM Atienza and J M Ordonez ldquoCT scanning of the
10 BioMed Research International
patellofemoral joint The quadriceps relaxed or contractedrdquoInternational Orthopaedics vol 20 no 3 pp 159ndash162 1996
[40] S Hinterwimmer M J Feucht J Paul et al ldquoAnalysis of theeffects of high tibial osteotomy on tibial rotationrdquo InternationalOrthopaedics vol 40 no 9 pp 1849ndash1854 2016
[41] K-M Jang J-H Lee H-J Park J L Kim and S-B HanldquoUnintended Rotational Changes of the Distal Tibia AfterBiplane Medial Open-Wedge High Tibial Osteotomyrdquo Journalof Arthroplasty vol 31 no 1 pp 59ndash63 2016
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
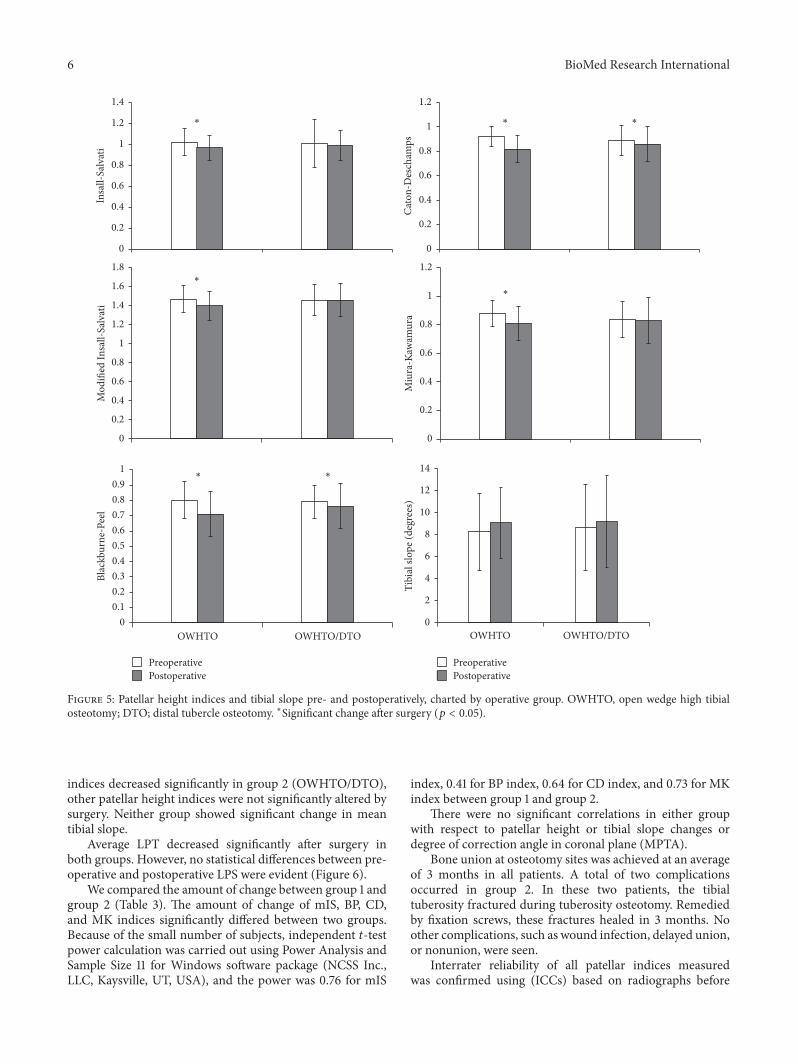
6 BioMed Research International
PreoperativePostoperative
PreoperativePostoperative
0
02
04
06
08
1
12
14In
sall-
Salv
ati
0
02
04
06
08
1
12
Cato
n-D
esch
amps
0
02
04
06
08
1
12
14
16
18
Mod
ified
Insa
ll-Sa
lvat
i
0
2
4
6
8
10
12
14
Tibi
al sl
ope (
degr
ees)
OWHTO OWHTODTOOWHTO OWHTODTO0
010203040506070809
1
Blac
kbur
ne-P
eel
0
02
04
06
08
1
12
Miu
ra-K
awam
ura
lowast lowast lowast
lowast
lowast
lowast lowast
Figure 5 Patellar height indices and tibial slope pre- and postoperatively charted by operative group OWHTO open wedge high tibialosteotomy DTO distal tubercle osteotomy lowastSignificant change after surgery (119901 lt 005)
indices decreased significantly in group 2 (OWHTODTO)other patellar height indices were not significantly altered bysurgery Neither group showed significant change in meantibial slope
Average LPT decreased significantly after surgery inboth groups However no statistical differences between pre-operative and postoperative LPS were evident (Figure 6)
We compared the amount of change between group 1 andgroup 2 (Table 3) The amount of change of mIS BP CDand MK indices significantly differed between two groupsBecause of the small number of subjects independent 119905-testpower calculation was carried out using Power Analysis andSample Size 11 for Windows software package (NCSS IncLLC Kaysville UT USA) and the power was 076 for mIS
index 041 for BP index 064 for CD index and 073 for MKindex between group 1 and group 2
There were no significant correlations in either groupwith respect to patellar height or tibial slope changes ordegree of correction angle in coronal plane (MPTA)
Bone union at osteotomy sites was achieved at an averageof 3 months in all patients A total of two complicationsoccurred in group 2 In these two patients the tibialtuberosity fractured during tuberosity osteotomy Remediedby fixation screws these fractures healed in 3 months Noother complications such as wound infection delayed unionor nonunion were seen
Interrater reliability of all patellar indices measuredwas confirmed using (ICCs) based on radiographs before
BioMed Research International 7
Table 3 The amount of change for radiographic measurements by operative group
Variables OWHTO (119899 = 30) OWHTODTO (119899 = 33) 119901 valueInsall-Salvati minus005 plusmn 008 minus002 plusmn 020 0408Modified Insall-Salvati minus008 plusmn 014 000 plusmn 009 0002Blackburne-Peel minus009 plusmn 009 minus004 plusmn 013 0037Caton-Deschamps minus010 plusmn 009 minus004 plusmn 011 0008Modified Miura-Kawamura minus008 plusmn 009 minus001 plusmn 012 0010Tibial slope (degrees) 078 plusmn 306 047 plusmn 395 0705Lateral patella tilt (degrees) minus206 plusmn 176 minus141 plusmn 214 0218Lateral patella shift minus001 plusmn 003 minus001 plusmn 003 0661Values expressed as mean plusmn SD OWHTO open wedge high tibial osteotomy DTO distal tubercle osteotomy
and after surgery ICC ranges for intraobserver (075ndash091)and interobserver (072ndash09) reliabilities were comparable tothose of previous studies [14 28]
4 Discussion
Introduction of OWHTODTO was fueled by efforts tominimize surgery-related loss in patellar height and preventsubsequent patellofemoral problems [8] Several studiesoffer proof that this technique is effective in minimizingpostoperative patellar height change citing clinical out-comes comparable to conventional OWHTO in patients withosteoarthritis of the medial tibiofemoral compartment andvarus malalignment [8 14 15 29ndash31] However there wasno study investigating the surgical results of OWHTODTOin patients with normal knee Special concerns in this pop-ulation include unsightly aesthetics and pain or discomfortupon kneeling after surgery Therefore we have used thistechnique to correct proximal tibial varus deformities inyoung patients without pain or arthritic joints provingthat diminished patellar height is avoidable through thisapproach Considering the positional changes of the patellafollowing conventionalOWHTOmay induce new symptomsthese concerns will be addressed by OWHTODTO
In the present study we found significant postoperativedecreases in IS and mIS indices of the OWHTO groupwhereas these ratios were unchanged in the OWHTODTOgroup Outcomes herein were aligned with previous studiesthat similarly utilized these ratios to evaluate patellar height[14 15 29] Both IS and mIS are indirect measures of patellarheight any change reflecting altered patellar tendon length[14 32] Any slackening or shortening of patellar tendon thusimplied may be explained by intratendinous fibrosis or adhe-sions of proximal tuberosity following OWHTO whereas theextensor mechanism remains intact after OWHTODTO
Although there were significant postoperative declines inBP and CD indices of both groups the MK index of theOWHTODTO group was unchanged Still only one otherstudy corroborates our results [14]Most earlier investigationshave recorded no significant changes in BP and CD indicesafter OWHTODTO [8 15 29 30] This discrepancy may bedue to the method of measurement Both BP and CD indiceshave been viewed as highly reliable gauges of patellar height[28 33] but their dependency on joint line is disadvanta-geous given tibial plateau as a reference Because tibial slope
OWHTO OWHTODTO
PreoperativePostoperative
0
005
01
015
02
025
Late
ral p
atel
la sh
ift
0
2
4
6
8
10
12
14
16
18
20
Late
ral p
atel
la ti
lt (d
egre
es)
lowast
lowast
Figure 6 Lateral patellar tilt and lateral patellar shift pre- andpostoperatively charted by operative group OWHTO open wedgehigh tibial osteotomy DTO distal tubercle osteotomy lowastSignificantchange after surgery (119901 lt 005)
decreased postoperatively in both arms of our study evenminimal deviations in tibial slope may thus have bearing Weagree with other investigators that BP and CD indices shouldnot be relied upon in surgical procedures involving proximaltibia [23 32] In our opinion the decrease seen in MK index
8 BioMed Research International
reflects a true reduction in patellar height because MK indexis independent with the change of tibial slope
Although various radiographic techniques (based onaxial radiography CT or MRI) have been described forevaluating patellar inclination [34] use of LPT and LPSafter OWHTODTO has not previously been investigatedPrevious publications studying changes in LPT and LPS afterOWHTO have relied on axial radiography of load-bearingpatellofemoral joints (Delgado-Martins method) [7 24 3536] However determinations rendered by axial radiographymay be not accurate due to overlapping of images difficultyin positioning the leg and incidental angles of X-ray beams[37 38] CT imaging of contracted quadriceps muscle mayserve better in confirming patellar position [25 34 37 39]Consequently we used axial CT images in supine positionwith the knee in 30 degrees of flexion to measure LPT andLPS
Ultimately we found that LPT declined significantlyfor both procedures but the reductions did not differsignificantly by operative group Our findings followingOWHTO were consistent with those of previous stud-ies [35 36] whereby lessening of LPT was attributed toincreased lateral pull on the patella Although we expectedthat OWHTODTO would prevent any changes in LPTand LPS LPT surprisingly showed significant decline afterOWHTODTO as well One possible explanation for this isthat a change in mechanical axis may affect the inclinationof patella For another reason the change of tibial rotationafter OWHTOmay affect the LPT Previous studies reportedOWHTO made significant internal axial rotation of the tibia[40 41] However there was no change on tibial rotation aftervarus correction because we used two half-pins to check thechange of rotational alignment in the operating room
In our analysis no significant correlations emerged withrespect to change in patellar height change in tibial slopeor correction angle degree Prior reports have indicated thatOWHTODTO ismore effective than conventional OWHTOin patients requiring large (gt10-degree) angular corrections[8 14 15 30] However we could provide corroborationbecause correction angles for most of our patients werelt10 degrees and the surgical goal was to restore neutralalignment Hence the protective effect of OWHTODTO onpatellar height after large angular correction (gt10 degrees)could not be fully evaluated by this study
There were two tibial tuberosity fractures in OWHTODTO group Only one previous literature reported samesurgical complications [8]Therewas no such complication inother reports using OWHTODTO [14 15 29 30]Thereforeit seems that tibial tuberosity fracture is related to mistakeof surgical procedure not the degrees of correction angleAdditionally in our study such fractures occurred at an earlystage in our learning curve and healed well with additionalscrew fixation Eventually we think that tibial tuberosityfracture is easily preventable with caution leaving at least a1-cm thickness on the proximal tuberosity fragment
Our study has some limitations First it is a retrospectiveinvestigation and not a randomized trial Also the twooperative groups reflected a shift in surgical technique ratherthan pure randomization Nevertheless the two groups were
well matched at baseline in terms of preoperative variablesAnother limitation was that blinding of the OWHTODTOarm was not feasible when measuring radiologic param-eters postoperatively even if two independent orthopedicresidents participated Finally radiographic parameters werethe primary focus To investigate the relationship betweenradiologic findings and clinical outcomes a well-plannedfuture prospective study is needed
There are various methods for correcting proximal tibialvara deformity and best surgical techniquemust be individu-alized Compared to conventional OWHTO OWHTODTOdid not influence patella height associated with the procedureand was considered an useful method to preserve patellaheight
Ethical Approval
This study was conducted following the approval of Institu-tional Review Board of Severance Hospital Yonsei UniversityCollege of Medicine (IRB number 4-2015-0796)
Conflicts of Interest
The authors declare that there are no conflicts of interest toreport regarding the work and publication of this study
Acknowledgments
The authors thank Dr Sung Min Kim and Jung Woo Lee forthe data measurement of the patients
References
[1] W Strecker ldquoPlanning Analysis of Knee-Adjacent DeformitiesrdquoEuropean Journal of Trauma and Emergency Surgery vol 33 no6 pp 662ndash668 2007
[2] R Rossi D E Bonasia and A Amendola ldquoThe Role of HighTibial Osteotomy in the Varus Kneerdquo American Academy ofOrthopaedic Surgeon vol 19 no 10 pp 590ndash599 2011
[3] R K Marti R A W Verhagen G M M J Kerkhoffs andT M Moojen ldquoProximal tibial varus osteotomy Indicationstechnique and five to twenty-one-year resultsrdquo Journal of Boneand Joint Surgery - Series A vol 83 no 2 pp 164ndash170 2001
[4] H El-Azab P Glabgly J Paul A B Imhoff and S Hinterwim-mer ldquoPatellar height and posterior tibial slope after open- andclosed-wedge high tibial osteotomy A radiological study on 100patientsrdquoAmerican Journal of Sports Medicine vol 38 no 2 pp323ndash329 2010
[5] B P Kaper R B Bourne C H Rorabeck and S J MacDonaldldquoPatellar infera after high tibial osteotomyrdquo Journal of Arthro-plasty vol 16 no 2 pp 168ndash173 2001
[6] D Tigani D Ferrari P Trentani G Barbanti-Brodano and FTrentani ldquoPatellar height after high tibial osteotomyrdquo Interna-tional Orthopaedics vol 24 no 6 pp 331ndash334 2001
[7] J-H Yang S-H Lee K S Nathawat S-H Jeon and K-JOh ldquoThe effect of biplane medial opening wedge high tibialosteotomy on patellofemoral joint indicesrdquo Knee vol 20 no 2pp 128ndash132 2013
[8] R D A Gaasbeek H Sonneveld R J Van Heerwaarden W CH Jacobs and A B Wymenga ldquoDistal tuberosity osteotomy in
BioMed Research International 9
open wedge high tibial osteotomy can prevent patella infera Anew techniquerdquo Knee vol 11 no 6 pp 457ndash461 2004
[9] C M Rodner D J Adams V Diaz-Doran et al ldquoMedialopeningwedge tibial osteotomy and the sagittal planeThe effectof increasing tibial slope on tibiofemoral contact pressurerdquoAmerican Journal of SportsMedicine vol 34 no 9 pp 1431ndash14412006
[10] R E Windsor J N Insall and K G Vince ldquoTechnicalconsiderations of total knee arthroplasty after proximal tibialosteotomyrdquo Journal of Bone and Joint Surgery - Series A vol 70no 4 pp 547ndash555 1988
[11] H E Figgie III V M Goldberg K G Heiple H S MollerIII and N H Gordon ldquoThe influence of tibial-patellofemorallocation on function of the knee in patients with the posteriorstabilized condylar knee prosthesisrdquo Journal of Bone and JointSurgery - Series A vol 68 no 7 pp 1035ndash1040 1986
[12] K Kim D Kim S Song S Lee and D Bae ldquoMedialOpen-Wedge High Tibial Osteotomy May Adversely Affect thePatellofemoral Jointrdquo Arthroscopy The Journal of Arthroscopicamp Related Surgery vol 33 no 4 pp 811ndash816 2017
[13] J S Shim S H Lee H J Jung and H I Lee ldquoHightibial open wedge osteotomy below the tibial tubercle Clinicaland radiographic resultsrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 1 pp 57ndash63 2013
[14] P D Longino T B Birmingham W J Schultz R F Moyerand J R Giffin ldquoCombined tibial tubercle osteotomy withmedial openingwedge high tibial osteotomyminimizes changesin patellar height A prospective cohort study with historicalcontrolsrdquo American Journal of Sports Medicine vol 41 no 12pp 2849ndash2857 2013
[15] S Keyhani M R Abbasian S M Kazemi et al ldquoModifiedretro-tubercle opening-wedge versus conventional high tibialosteotomyrdquo Orthopedics vol 34 no 2 2011
[16] D H Lee K J Ryu H H Kim S Soung and S Shin ldquoFixator-assisted Technique Enables Less Invasive Plate Osteosynthesisin Medial Opening-wedge High Tibial Osteotomy A NovelTechniquerdquo Clinical Orthopaedics and Related Research vol473 no 10 pp 3133ndash3142 2015
[17] S B Han D H Lee G M Shetty D J Chae J G Songand K W Nha ldquoA ldquosafe zonerdquo in medial open-wedge hightibia osteotomy to prevent lateral cortex fracturerdquoKnee SurgerySports Traumatology Arthroscopy vol 21 no 1 pp 90ndash95 2013
[18] D Paley and K Tetsworth ldquoMechanical axis deviation ofthe lower limbs Preoperative planning of uniapical angulardeformities of the tibia or femurrdquo Clinical Orthopaedics andRelated Research no 280 pp 48ndash64 1992
[19] J Insall and E Salvati ldquoPatella position in the normal kneejointrdquo Radiology vol 101 no 1 pp 101ndash104 1971
[20] R P Grelsamer and S Meadows ldquoThe modified Insall-Salvatiratio for assessment of patellar heightrdquo Clinical Orthopaedicsand Related Research no 282 pp 170ndash176 1992
[21] J S Blackburne and T E Peel ldquoA new method of measuringpatellar heightrdquo J Bone Joint Surg Br vol 59 no 2 pp 241-2421977
[22] J Caton G Deschamps P Chambat J L Lerat and HDejour ldquoPatella infera Apropos of 128 casesrdquo Rev Chir OrthopReparatrice Appar Mot vol 68 no 5 pp 317ndash325 1982
[23] H Miura H Kawamura R Nagamine K Urabe and YIwamoto ldquoIs patellar height really lower after high tibialosteotomyrdquo Fukuoka igaku zasshi = Hukuoka acta medica vol88 no 6 pp 261ndash266 1997
[24] H Delgado-Martins ldquoThe bicondylo-patellar angle as a mea-sure of patellar tiltingrdquo Archives of Orthopaedic and TraumaticSurgery vol 96 no 4 pp 303-304 1980
[25] V Vahasarja P Lanning S Lahde and W Serlo ldquoAxialradiography or CT in the measurement of patellofemoralmalalignment indices in children and adolescentsrdquo ClinicalRadiology vol 51 no 9 pp 639ndash643 1996
[26] U M Kujala K Osterman M Kormano M Komu and DSchlenzka ldquoPatellar motion analyzed by magnetic resonanceimagingrdquo Acta Orthopaedica vol 60 no 1 pp 13ndash16 1989
[27] C A Laurin R Dussault and H P Levesque ldquoThe tan-gential X-ray investigation of the patellofemoral joint X-raytechnique diagnostic criteria and their interpretationrdquo ClinicalOrthopaedics and Related Research no 144 pp 16ndash26 1979
[28] R Seil B Muller T Georg D Kohn and S Rupp ldquoReliabilityand interobserver variability in radiological patellar heightratiosrdquo Knee Surgery Sports Traumatology Arthroscopy vol 8no 4 pp 231ndash236 2000
[29] N Elmali I Esenkaya M Can and M Karakaplan ldquoMono-planar versus biplanar medial open-wedge proximal tibialosteotomy for varus gonarthrosis A comparison of clinicaland radiological outcomesrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 12 pp 2689ndash2695 2013
[30] S Hinterwimmer K Beitzel J Paul et al ldquoControl of posteriortibial slope and patellar height in open-wedge valgus high tibialosteotomyrdquo American Journal of Sports Medicine vol 39 no 4pp 851ndash856 2011
[31] S Hopwood W Khan and S Agarwal ldquoThe biplanar openwedge high tibial osteotomy preserving the tibial tuberclerdquoJournal of Orthopaedic Science vol 21 no 6 pp 786ndash790 2016
[32] H Kesmezacar R Erginer T Ogut A Seyahi M Babacan andY Tenekecioglu ldquoEvaluation of patellar height and measure-ment methods after valgus high tibial osteotomyrdquo Knee SurgerySports Traumatology Arthroscopy vol 13 no 7 pp 539ndash5442005
[33] B A Rogers P Thornton-Bott S R Cannon and T W RBriggs ldquoInterobserver variation in the measurement of patellarheight after total knee arthroplastyrdquo Journal of Bone and JointSurgery - Series B vol 88 no 4 pp 484ndash488 2006
[34] R P Grelsamer C H Weinstein J Gould and A DubeyldquoPatellar tilt The physical examination correlates with MRimagingrdquo Knee vol 15 no 1 pp 3ndash8 2008
[35] R Gaasbeek R Welsing M Barink N Verdonschot andA Van Kampen ldquoThe influence of open and closed hightibial osteotomy on dynamic patellar tracking A biomechanicalstudyrdquo Knee Surgery Sports Traumatology Arthroscopy vol 15no 8 pp 978ndash984 2007
[36] H Bito R Takeuchi K Kumagai et al ldquoOpening wedge hightibial osteotomy affects both the lateral patellar tilt and patellarheightrdquo Knee Surgery Sports Traumatology Arthroscopy vol 18no 7 pp 955ndash960 2010
[37] T Sasaki and T Yagi ldquoSubluxation of the patella - Investigationby computerized tomographyrdquo International Orthopaedics vol10 no 2 pp 115ndash120 1986
[38] F Boven M-A Bellemans J Geurts and R PotvliegeldquoA comparative study of the patello-femoral joint on axialroentgenogram axial arthrogram and computed tomographyfollowing arthrographyrdquo Skeletal Radiology vol 8 no 3 pp179ndash181 1982
[39] A D Delgado-Martınez C Estrada E C Rodrıguez-MerchanM Atienza and J M Ordonez ldquoCT scanning of the
10 BioMed Research International
patellofemoral joint The quadriceps relaxed or contractedrdquoInternational Orthopaedics vol 20 no 3 pp 159ndash162 1996
[40] S Hinterwimmer M J Feucht J Paul et al ldquoAnalysis of theeffects of high tibial osteotomy on tibial rotationrdquo InternationalOrthopaedics vol 40 no 9 pp 1849ndash1854 2016
[41] K-M Jang J-H Lee H-J Park J L Kim and S-B HanldquoUnintended Rotational Changes of the Distal Tibia AfterBiplane Medial Open-Wedge High Tibial Osteotomyrdquo Journalof Arthroplasty vol 31 no 1 pp 59ndash63 2016
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
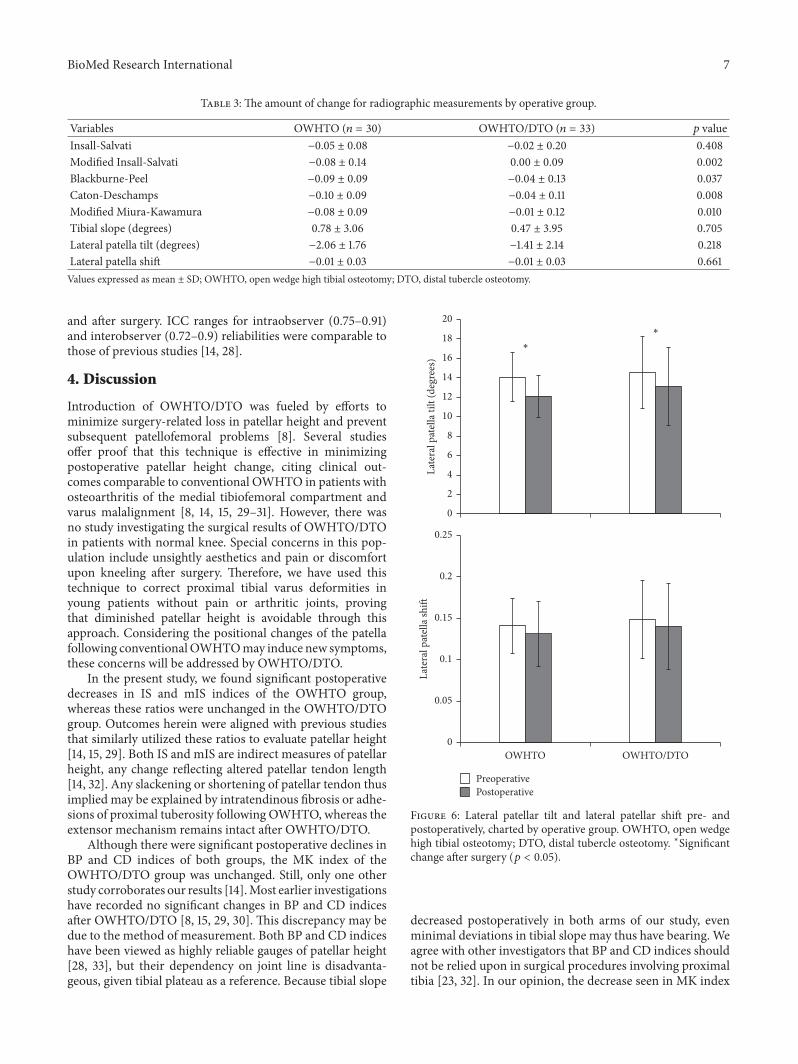
BioMed Research International 7
Table 3 The amount of change for radiographic measurements by operative group
Variables OWHTO (119899 = 30) OWHTODTO (119899 = 33) 119901 valueInsall-Salvati minus005 plusmn 008 minus002 plusmn 020 0408Modified Insall-Salvati minus008 plusmn 014 000 plusmn 009 0002Blackburne-Peel minus009 plusmn 009 minus004 plusmn 013 0037Caton-Deschamps minus010 plusmn 009 minus004 plusmn 011 0008Modified Miura-Kawamura minus008 plusmn 009 minus001 plusmn 012 0010Tibial slope (degrees) 078 plusmn 306 047 plusmn 395 0705Lateral patella tilt (degrees) minus206 plusmn 176 minus141 plusmn 214 0218Lateral patella shift minus001 plusmn 003 minus001 plusmn 003 0661Values expressed as mean plusmn SD OWHTO open wedge high tibial osteotomy DTO distal tubercle osteotomy
and after surgery ICC ranges for intraobserver (075ndash091)and interobserver (072ndash09) reliabilities were comparable tothose of previous studies [14 28]
4 Discussion
Introduction of OWHTODTO was fueled by efforts tominimize surgery-related loss in patellar height and preventsubsequent patellofemoral problems [8] Several studiesoffer proof that this technique is effective in minimizingpostoperative patellar height change citing clinical out-comes comparable to conventional OWHTO in patients withosteoarthritis of the medial tibiofemoral compartment andvarus malalignment [8 14 15 29ndash31] However there wasno study investigating the surgical results of OWHTODTOin patients with normal knee Special concerns in this pop-ulation include unsightly aesthetics and pain or discomfortupon kneeling after surgery Therefore we have used thistechnique to correct proximal tibial varus deformities inyoung patients without pain or arthritic joints provingthat diminished patellar height is avoidable through thisapproach Considering the positional changes of the patellafollowing conventionalOWHTOmay induce new symptomsthese concerns will be addressed by OWHTODTO
In the present study we found significant postoperativedecreases in IS and mIS indices of the OWHTO groupwhereas these ratios were unchanged in the OWHTODTOgroup Outcomes herein were aligned with previous studiesthat similarly utilized these ratios to evaluate patellar height[14 15 29] Both IS and mIS are indirect measures of patellarheight any change reflecting altered patellar tendon length[14 32] Any slackening or shortening of patellar tendon thusimplied may be explained by intratendinous fibrosis or adhe-sions of proximal tuberosity following OWHTO whereas theextensor mechanism remains intact after OWHTODTO
Although there were significant postoperative declines inBP and CD indices of both groups the MK index of theOWHTODTO group was unchanged Still only one otherstudy corroborates our results [14]Most earlier investigationshave recorded no significant changes in BP and CD indicesafter OWHTODTO [8 15 29 30] This discrepancy may bedue to the method of measurement Both BP and CD indiceshave been viewed as highly reliable gauges of patellar height[28 33] but their dependency on joint line is disadvanta-geous given tibial plateau as a reference Because tibial slope
OWHTO OWHTODTO
PreoperativePostoperative
0
005
01
015
02
025
Late
ral p
atel
la sh
ift
0
2
4
6
8
10
12
14
16
18
20
Late
ral p
atel
la ti
lt (d
egre
es)
lowast
lowast
Figure 6 Lateral patellar tilt and lateral patellar shift pre- andpostoperatively charted by operative group OWHTO open wedgehigh tibial osteotomy DTO distal tubercle osteotomy lowastSignificantchange after surgery (119901 lt 005)
decreased postoperatively in both arms of our study evenminimal deviations in tibial slope may thus have bearing Weagree with other investigators that BP and CD indices shouldnot be relied upon in surgical procedures involving proximaltibia [23 32] In our opinion the decrease seen in MK index
8 BioMed Research International
reflects a true reduction in patellar height because MK indexis independent with the change of tibial slope
Although various radiographic techniques (based onaxial radiography CT or MRI) have been described forevaluating patellar inclination [34] use of LPT and LPSafter OWHTODTO has not previously been investigatedPrevious publications studying changes in LPT and LPS afterOWHTO have relied on axial radiography of load-bearingpatellofemoral joints (Delgado-Martins method) [7 24 3536] However determinations rendered by axial radiographymay be not accurate due to overlapping of images difficultyin positioning the leg and incidental angles of X-ray beams[37 38] CT imaging of contracted quadriceps muscle mayserve better in confirming patellar position [25 34 37 39]Consequently we used axial CT images in supine positionwith the knee in 30 degrees of flexion to measure LPT andLPS
Ultimately we found that LPT declined significantlyfor both procedures but the reductions did not differsignificantly by operative group Our findings followingOWHTO were consistent with those of previous stud-ies [35 36] whereby lessening of LPT was attributed toincreased lateral pull on the patella Although we expectedthat OWHTODTO would prevent any changes in LPTand LPS LPT surprisingly showed significant decline afterOWHTODTO as well One possible explanation for this isthat a change in mechanical axis may affect the inclinationof patella For another reason the change of tibial rotationafter OWHTOmay affect the LPT Previous studies reportedOWHTO made significant internal axial rotation of the tibia[40 41] However there was no change on tibial rotation aftervarus correction because we used two half-pins to check thechange of rotational alignment in the operating room
In our analysis no significant correlations emerged withrespect to change in patellar height change in tibial slopeor correction angle degree Prior reports have indicated thatOWHTODTO ismore effective than conventional OWHTOin patients requiring large (gt10-degree) angular corrections[8 14 15 30] However we could provide corroborationbecause correction angles for most of our patients werelt10 degrees and the surgical goal was to restore neutralalignment Hence the protective effect of OWHTODTO onpatellar height after large angular correction (gt10 degrees)could not be fully evaluated by this study
There were two tibial tuberosity fractures in OWHTODTO group Only one previous literature reported samesurgical complications [8]Therewas no such complication inother reports using OWHTODTO [14 15 29 30]Thereforeit seems that tibial tuberosity fracture is related to mistakeof surgical procedure not the degrees of correction angleAdditionally in our study such fractures occurred at an earlystage in our learning curve and healed well with additionalscrew fixation Eventually we think that tibial tuberosityfracture is easily preventable with caution leaving at least a1-cm thickness on the proximal tuberosity fragment
Our study has some limitations First it is a retrospectiveinvestigation and not a randomized trial Also the twooperative groups reflected a shift in surgical technique ratherthan pure randomization Nevertheless the two groups were
well matched at baseline in terms of preoperative variablesAnother limitation was that blinding of the OWHTODTOarm was not feasible when measuring radiologic param-eters postoperatively even if two independent orthopedicresidents participated Finally radiographic parameters werethe primary focus To investigate the relationship betweenradiologic findings and clinical outcomes a well-plannedfuture prospective study is needed
There are various methods for correcting proximal tibialvara deformity and best surgical techniquemust be individu-alized Compared to conventional OWHTO OWHTODTOdid not influence patella height associated with the procedureand was considered an useful method to preserve patellaheight
Ethical Approval
This study was conducted following the approval of Institu-tional Review Board of Severance Hospital Yonsei UniversityCollege of Medicine (IRB number 4-2015-0796)
Conflicts of Interest
The authors declare that there are no conflicts of interest toreport regarding the work and publication of this study
Acknowledgments
The authors thank Dr Sung Min Kim and Jung Woo Lee forthe data measurement of the patients
References
[1] W Strecker ldquoPlanning Analysis of Knee-Adjacent DeformitiesrdquoEuropean Journal of Trauma and Emergency Surgery vol 33 no6 pp 662ndash668 2007
[2] R Rossi D E Bonasia and A Amendola ldquoThe Role of HighTibial Osteotomy in the Varus Kneerdquo American Academy ofOrthopaedic Surgeon vol 19 no 10 pp 590ndash599 2011
[3] R K Marti R A W Verhagen G M M J Kerkhoffs andT M Moojen ldquoProximal tibial varus osteotomy Indicationstechnique and five to twenty-one-year resultsrdquo Journal of Boneand Joint Surgery - Series A vol 83 no 2 pp 164ndash170 2001
[4] H El-Azab P Glabgly J Paul A B Imhoff and S Hinterwim-mer ldquoPatellar height and posterior tibial slope after open- andclosed-wedge high tibial osteotomy A radiological study on 100patientsrdquoAmerican Journal of Sports Medicine vol 38 no 2 pp323ndash329 2010
[5] B P Kaper R B Bourne C H Rorabeck and S J MacDonaldldquoPatellar infera after high tibial osteotomyrdquo Journal of Arthro-plasty vol 16 no 2 pp 168ndash173 2001
[6] D Tigani D Ferrari P Trentani G Barbanti-Brodano and FTrentani ldquoPatellar height after high tibial osteotomyrdquo Interna-tional Orthopaedics vol 24 no 6 pp 331ndash334 2001
[7] J-H Yang S-H Lee K S Nathawat S-H Jeon and K-JOh ldquoThe effect of biplane medial opening wedge high tibialosteotomy on patellofemoral joint indicesrdquo Knee vol 20 no 2pp 128ndash132 2013
[8] R D A Gaasbeek H Sonneveld R J Van Heerwaarden W CH Jacobs and A B Wymenga ldquoDistal tuberosity osteotomy in
BioMed Research International 9
open wedge high tibial osteotomy can prevent patella infera Anew techniquerdquo Knee vol 11 no 6 pp 457ndash461 2004
[9] C M Rodner D J Adams V Diaz-Doran et al ldquoMedialopeningwedge tibial osteotomy and the sagittal planeThe effectof increasing tibial slope on tibiofemoral contact pressurerdquoAmerican Journal of SportsMedicine vol 34 no 9 pp 1431ndash14412006
[10] R E Windsor J N Insall and K G Vince ldquoTechnicalconsiderations of total knee arthroplasty after proximal tibialosteotomyrdquo Journal of Bone and Joint Surgery - Series A vol 70no 4 pp 547ndash555 1988
[11] H E Figgie III V M Goldberg K G Heiple H S MollerIII and N H Gordon ldquoThe influence of tibial-patellofemorallocation on function of the knee in patients with the posteriorstabilized condylar knee prosthesisrdquo Journal of Bone and JointSurgery - Series A vol 68 no 7 pp 1035ndash1040 1986
[12] K Kim D Kim S Song S Lee and D Bae ldquoMedialOpen-Wedge High Tibial Osteotomy May Adversely Affect thePatellofemoral Jointrdquo Arthroscopy The Journal of Arthroscopicamp Related Surgery vol 33 no 4 pp 811ndash816 2017
[13] J S Shim S H Lee H J Jung and H I Lee ldquoHightibial open wedge osteotomy below the tibial tubercle Clinicaland radiographic resultsrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 1 pp 57ndash63 2013
[14] P D Longino T B Birmingham W J Schultz R F Moyerand J R Giffin ldquoCombined tibial tubercle osteotomy withmedial openingwedge high tibial osteotomyminimizes changesin patellar height A prospective cohort study with historicalcontrolsrdquo American Journal of Sports Medicine vol 41 no 12pp 2849ndash2857 2013
[15] S Keyhani M R Abbasian S M Kazemi et al ldquoModifiedretro-tubercle opening-wedge versus conventional high tibialosteotomyrdquo Orthopedics vol 34 no 2 2011
[16] D H Lee K J Ryu H H Kim S Soung and S Shin ldquoFixator-assisted Technique Enables Less Invasive Plate Osteosynthesisin Medial Opening-wedge High Tibial Osteotomy A NovelTechniquerdquo Clinical Orthopaedics and Related Research vol473 no 10 pp 3133ndash3142 2015
[17] S B Han D H Lee G M Shetty D J Chae J G Songand K W Nha ldquoA ldquosafe zonerdquo in medial open-wedge hightibia osteotomy to prevent lateral cortex fracturerdquoKnee SurgerySports Traumatology Arthroscopy vol 21 no 1 pp 90ndash95 2013
[18] D Paley and K Tetsworth ldquoMechanical axis deviation ofthe lower limbs Preoperative planning of uniapical angulardeformities of the tibia or femurrdquo Clinical Orthopaedics andRelated Research no 280 pp 48ndash64 1992
[19] J Insall and E Salvati ldquoPatella position in the normal kneejointrdquo Radiology vol 101 no 1 pp 101ndash104 1971
[20] R P Grelsamer and S Meadows ldquoThe modified Insall-Salvatiratio for assessment of patellar heightrdquo Clinical Orthopaedicsand Related Research no 282 pp 170ndash176 1992
[21] J S Blackburne and T E Peel ldquoA new method of measuringpatellar heightrdquo J Bone Joint Surg Br vol 59 no 2 pp 241-2421977
[22] J Caton G Deschamps P Chambat J L Lerat and HDejour ldquoPatella infera Apropos of 128 casesrdquo Rev Chir OrthopReparatrice Appar Mot vol 68 no 5 pp 317ndash325 1982
[23] H Miura H Kawamura R Nagamine K Urabe and YIwamoto ldquoIs patellar height really lower after high tibialosteotomyrdquo Fukuoka igaku zasshi = Hukuoka acta medica vol88 no 6 pp 261ndash266 1997
[24] H Delgado-Martins ldquoThe bicondylo-patellar angle as a mea-sure of patellar tiltingrdquo Archives of Orthopaedic and TraumaticSurgery vol 96 no 4 pp 303-304 1980
[25] V Vahasarja P Lanning S Lahde and W Serlo ldquoAxialradiography or CT in the measurement of patellofemoralmalalignment indices in children and adolescentsrdquo ClinicalRadiology vol 51 no 9 pp 639ndash643 1996
[26] U M Kujala K Osterman M Kormano M Komu and DSchlenzka ldquoPatellar motion analyzed by magnetic resonanceimagingrdquo Acta Orthopaedica vol 60 no 1 pp 13ndash16 1989
[27] C A Laurin R Dussault and H P Levesque ldquoThe tan-gential X-ray investigation of the patellofemoral joint X-raytechnique diagnostic criteria and their interpretationrdquo ClinicalOrthopaedics and Related Research no 144 pp 16ndash26 1979
[28] R Seil B Muller T Georg D Kohn and S Rupp ldquoReliabilityand interobserver variability in radiological patellar heightratiosrdquo Knee Surgery Sports Traumatology Arthroscopy vol 8no 4 pp 231ndash236 2000
[29] N Elmali I Esenkaya M Can and M Karakaplan ldquoMono-planar versus biplanar medial open-wedge proximal tibialosteotomy for varus gonarthrosis A comparison of clinicaland radiological outcomesrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 12 pp 2689ndash2695 2013
[30] S Hinterwimmer K Beitzel J Paul et al ldquoControl of posteriortibial slope and patellar height in open-wedge valgus high tibialosteotomyrdquo American Journal of Sports Medicine vol 39 no 4pp 851ndash856 2011
[31] S Hopwood W Khan and S Agarwal ldquoThe biplanar openwedge high tibial osteotomy preserving the tibial tuberclerdquoJournal of Orthopaedic Science vol 21 no 6 pp 786ndash790 2016
[32] H Kesmezacar R Erginer T Ogut A Seyahi M Babacan andY Tenekecioglu ldquoEvaluation of patellar height and measure-ment methods after valgus high tibial osteotomyrdquo Knee SurgerySports Traumatology Arthroscopy vol 13 no 7 pp 539ndash5442005
[33] B A Rogers P Thornton-Bott S R Cannon and T W RBriggs ldquoInterobserver variation in the measurement of patellarheight after total knee arthroplastyrdquo Journal of Bone and JointSurgery - Series B vol 88 no 4 pp 484ndash488 2006
[34] R P Grelsamer C H Weinstein J Gould and A DubeyldquoPatellar tilt The physical examination correlates with MRimagingrdquo Knee vol 15 no 1 pp 3ndash8 2008
[35] R Gaasbeek R Welsing M Barink N Verdonschot andA Van Kampen ldquoThe influence of open and closed hightibial osteotomy on dynamic patellar tracking A biomechanicalstudyrdquo Knee Surgery Sports Traumatology Arthroscopy vol 15no 8 pp 978ndash984 2007
[36] H Bito R Takeuchi K Kumagai et al ldquoOpening wedge hightibial osteotomy affects both the lateral patellar tilt and patellarheightrdquo Knee Surgery Sports Traumatology Arthroscopy vol 18no 7 pp 955ndash960 2010
[37] T Sasaki and T Yagi ldquoSubluxation of the patella - Investigationby computerized tomographyrdquo International Orthopaedics vol10 no 2 pp 115ndash120 1986
[38] F Boven M-A Bellemans J Geurts and R PotvliegeldquoA comparative study of the patello-femoral joint on axialroentgenogram axial arthrogram and computed tomographyfollowing arthrographyrdquo Skeletal Radiology vol 8 no 3 pp179ndash181 1982
[39] A D Delgado-Martınez C Estrada E C Rodrıguez-MerchanM Atienza and J M Ordonez ldquoCT scanning of the
10 BioMed Research International
patellofemoral joint The quadriceps relaxed or contractedrdquoInternational Orthopaedics vol 20 no 3 pp 159ndash162 1996
[40] S Hinterwimmer M J Feucht J Paul et al ldquoAnalysis of theeffects of high tibial osteotomy on tibial rotationrdquo InternationalOrthopaedics vol 40 no 9 pp 1849ndash1854 2016
[41] K-M Jang J-H Lee H-J Park J L Kim and S-B HanldquoUnintended Rotational Changes of the Distal Tibia AfterBiplane Medial Open-Wedge High Tibial Osteotomyrdquo Journalof Arthroplasty vol 31 no 1 pp 59ndash63 2016
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

8 BioMed Research International
reflects a true reduction in patellar height because MK indexis independent with the change of tibial slope
Although various radiographic techniques (based onaxial radiography CT or MRI) have been described forevaluating patellar inclination [34] use of LPT and LPSafter OWHTODTO has not previously been investigatedPrevious publications studying changes in LPT and LPS afterOWHTO have relied on axial radiography of load-bearingpatellofemoral joints (Delgado-Martins method) [7 24 3536] However determinations rendered by axial radiographymay be not accurate due to overlapping of images difficultyin positioning the leg and incidental angles of X-ray beams[37 38] CT imaging of contracted quadriceps muscle mayserve better in confirming patellar position [25 34 37 39]Consequently we used axial CT images in supine positionwith the knee in 30 degrees of flexion to measure LPT andLPS
Ultimately we found that LPT declined significantlyfor both procedures but the reductions did not differsignificantly by operative group Our findings followingOWHTO were consistent with those of previous stud-ies [35 36] whereby lessening of LPT was attributed toincreased lateral pull on the patella Although we expectedthat OWHTODTO would prevent any changes in LPTand LPS LPT surprisingly showed significant decline afterOWHTODTO as well One possible explanation for this isthat a change in mechanical axis may affect the inclinationof patella For another reason the change of tibial rotationafter OWHTOmay affect the LPT Previous studies reportedOWHTO made significant internal axial rotation of the tibia[40 41] However there was no change on tibial rotation aftervarus correction because we used two half-pins to check thechange of rotational alignment in the operating room
In our analysis no significant correlations emerged withrespect to change in patellar height change in tibial slopeor correction angle degree Prior reports have indicated thatOWHTODTO ismore effective than conventional OWHTOin patients requiring large (gt10-degree) angular corrections[8 14 15 30] However we could provide corroborationbecause correction angles for most of our patients werelt10 degrees and the surgical goal was to restore neutralalignment Hence the protective effect of OWHTODTO onpatellar height after large angular correction (gt10 degrees)could not be fully evaluated by this study
There were two tibial tuberosity fractures in OWHTODTO group Only one previous literature reported samesurgical complications [8]Therewas no such complication inother reports using OWHTODTO [14 15 29 30]Thereforeit seems that tibial tuberosity fracture is related to mistakeof surgical procedure not the degrees of correction angleAdditionally in our study such fractures occurred at an earlystage in our learning curve and healed well with additionalscrew fixation Eventually we think that tibial tuberosityfracture is easily preventable with caution leaving at least a1-cm thickness on the proximal tuberosity fragment
Our study has some limitations First it is a retrospectiveinvestigation and not a randomized trial Also the twooperative groups reflected a shift in surgical technique ratherthan pure randomization Nevertheless the two groups were
well matched at baseline in terms of preoperative variablesAnother limitation was that blinding of the OWHTODTOarm was not feasible when measuring radiologic param-eters postoperatively even if two independent orthopedicresidents participated Finally radiographic parameters werethe primary focus To investigate the relationship betweenradiologic findings and clinical outcomes a well-plannedfuture prospective study is needed
There are various methods for correcting proximal tibialvara deformity and best surgical techniquemust be individu-alized Compared to conventional OWHTO OWHTODTOdid not influence patella height associated with the procedureand was considered an useful method to preserve patellaheight
Ethical Approval
This study was conducted following the approval of Institu-tional Review Board of Severance Hospital Yonsei UniversityCollege of Medicine (IRB number 4-2015-0796)
Conflicts of Interest
The authors declare that there are no conflicts of interest toreport regarding the work and publication of this study
Acknowledgments
The authors thank Dr Sung Min Kim and Jung Woo Lee forthe data measurement of the patients
References
[1] W Strecker ldquoPlanning Analysis of Knee-Adjacent DeformitiesrdquoEuropean Journal of Trauma and Emergency Surgery vol 33 no6 pp 662ndash668 2007
[2] R Rossi D E Bonasia and A Amendola ldquoThe Role of HighTibial Osteotomy in the Varus Kneerdquo American Academy ofOrthopaedic Surgeon vol 19 no 10 pp 590ndash599 2011
[3] R K Marti R A W Verhagen G M M J Kerkhoffs andT M Moojen ldquoProximal tibial varus osteotomy Indicationstechnique and five to twenty-one-year resultsrdquo Journal of Boneand Joint Surgery - Series A vol 83 no 2 pp 164ndash170 2001
[4] H El-Azab P Glabgly J Paul A B Imhoff and S Hinterwim-mer ldquoPatellar height and posterior tibial slope after open- andclosed-wedge high tibial osteotomy A radiological study on 100patientsrdquoAmerican Journal of Sports Medicine vol 38 no 2 pp323ndash329 2010
[5] B P Kaper R B Bourne C H Rorabeck and S J MacDonaldldquoPatellar infera after high tibial osteotomyrdquo Journal of Arthro-plasty vol 16 no 2 pp 168ndash173 2001
[6] D Tigani D Ferrari P Trentani G Barbanti-Brodano and FTrentani ldquoPatellar height after high tibial osteotomyrdquo Interna-tional Orthopaedics vol 24 no 6 pp 331ndash334 2001
[7] J-H Yang S-H Lee K S Nathawat S-H Jeon and K-JOh ldquoThe effect of biplane medial opening wedge high tibialosteotomy on patellofemoral joint indicesrdquo Knee vol 20 no 2pp 128ndash132 2013
[8] R D A Gaasbeek H Sonneveld R J Van Heerwaarden W CH Jacobs and A B Wymenga ldquoDistal tuberosity osteotomy in
BioMed Research International 9
open wedge high tibial osteotomy can prevent patella infera Anew techniquerdquo Knee vol 11 no 6 pp 457ndash461 2004
[9] C M Rodner D J Adams V Diaz-Doran et al ldquoMedialopeningwedge tibial osteotomy and the sagittal planeThe effectof increasing tibial slope on tibiofemoral contact pressurerdquoAmerican Journal of SportsMedicine vol 34 no 9 pp 1431ndash14412006
[10] R E Windsor J N Insall and K G Vince ldquoTechnicalconsiderations of total knee arthroplasty after proximal tibialosteotomyrdquo Journal of Bone and Joint Surgery - Series A vol 70no 4 pp 547ndash555 1988
[11] H E Figgie III V M Goldberg K G Heiple H S MollerIII and N H Gordon ldquoThe influence of tibial-patellofemorallocation on function of the knee in patients with the posteriorstabilized condylar knee prosthesisrdquo Journal of Bone and JointSurgery - Series A vol 68 no 7 pp 1035ndash1040 1986
[12] K Kim D Kim S Song S Lee and D Bae ldquoMedialOpen-Wedge High Tibial Osteotomy May Adversely Affect thePatellofemoral Jointrdquo Arthroscopy The Journal of Arthroscopicamp Related Surgery vol 33 no 4 pp 811ndash816 2017
[13] J S Shim S H Lee H J Jung and H I Lee ldquoHightibial open wedge osteotomy below the tibial tubercle Clinicaland radiographic resultsrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 1 pp 57ndash63 2013
[14] P D Longino T B Birmingham W J Schultz R F Moyerand J R Giffin ldquoCombined tibial tubercle osteotomy withmedial openingwedge high tibial osteotomyminimizes changesin patellar height A prospective cohort study with historicalcontrolsrdquo American Journal of Sports Medicine vol 41 no 12pp 2849ndash2857 2013
[15] S Keyhani M R Abbasian S M Kazemi et al ldquoModifiedretro-tubercle opening-wedge versus conventional high tibialosteotomyrdquo Orthopedics vol 34 no 2 2011
[16] D H Lee K J Ryu H H Kim S Soung and S Shin ldquoFixator-assisted Technique Enables Less Invasive Plate Osteosynthesisin Medial Opening-wedge High Tibial Osteotomy A NovelTechniquerdquo Clinical Orthopaedics and Related Research vol473 no 10 pp 3133ndash3142 2015
[17] S B Han D H Lee G M Shetty D J Chae J G Songand K W Nha ldquoA ldquosafe zonerdquo in medial open-wedge hightibia osteotomy to prevent lateral cortex fracturerdquoKnee SurgerySports Traumatology Arthroscopy vol 21 no 1 pp 90ndash95 2013
[18] D Paley and K Tetsworth ldquoMechanical axis deviation ofthe lower limbs Preoperative planning of uniapical angulardeformities of the tibia or femurrdquo Clinical Orthopaedics andRelated Research no 280 pp 48ndash64 1992
[19] J Insall and E Salvati ldquoPatella position in the normal kneejointrdquo Radiology vol 101 no 1 pp 101ndash104 1971
[20] R P Grelsamer and S Meadows ldquoThe modified Insall-Salvatiratio for assessment of patellar heightrdquo Clinical Orthopaedicsand Related Research no 282 pp 170ndash176 1992
[21] J S Blackburne and T E Peel ldquoA new method of measuringpatellar heightrdquo J Bone Joint Surg Br vol 59 no 2 pp 241-2421977
[22] J Caton G Deschamps P Chambat J L Lerat and HDejour ldquoPatella infera Apropos of 128 casesrdquo Rev Chir OrthopReparatrice Appar Mot vol 68 no 5 pp 317ndash325 1982
[23] H Miura H Kawamura R Nagamine K Urabe and YIwamoto ldquoIs patellar height really lower after high tibialosteotomyrdquo Fukuoka igaku zasshi = Hukuoka acta medica vol88 no 6 pp 261ndash266 1997
[24] H Delgado-Martins ldquoThe bicondylo-patellar angle as a mea-sure of patellar tiltingrdquo Archives of Orthopaedic and TraumaticSurgery vol 96 no 4 pp 303-304 1980
[25] V Vahasarja P Lanning S Lahde and W Serlo ldquoAxialradiography or CT in the measurement of patellofemoralmalalignment indices in children and adolescentsrdquo ClinicalRadiology vol 51 no 9 pp 639ndash643 1996
[26] U M Kujala K Osterman M Kormano M Komu and DSchlenzka ldquoPatellar motion analyzed by magnetic resonanceimagingrdquo Acta Orthopaedica vol 60 no 1 pp 13ndash16 1989
[27] C A Laurin R Dussault and H P Levesque ldquoThe tan-gential X-ray investigation of the patellofemoral joint X-raytechnique diagnostic criteria and their interpretationrdquo ClinicalOrthopaedics and Related Research no 144 pp 16ndash26 1979
[28] R Seil B Muller T Georg D Kohn and S Rupp ldquoReliabilityand interobserver variability in radiological patellar heightratiosrdquo Knee Surgery Sports Traumatology Arthroscopy vol 8no 4 pp 231ndash236 2000
[29] N Elmali I Esenkaya M Can and M Karakaplan ldquoMono-planar versus biplanar medial open-wedge proximal tibialosteotomy for varus gonarthrosis A comparison of clinicaland radiological outcomesrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 12 pp 2689ndash2695 2013
[30] S Hinterwimmer K Beitzel J Paul et al ldquoControl of posteriortibial slope and patellar height in open-wedge valgus high tibialosteotomyrdquo American Journal of Sports Medicine vol 39 no 4pp 851ndash856 2011
[31] S Hopwood W Khan and S Agarwal ldquoThe biplanar openwedge high tibial osteotomy preserving the tibial tuberclerdquoJournal of Orthopaedic Science vol 21 no 6 pp 786ndash790 2016
[32] H Kesmezacar R Erginer T Ogut A Seyahi M Babacan andY Tenekecioglu ldquoEvaluation of patellar height and measure-ment methods after valgus high tibial osteotomyrdquo Knee SurgerySports Traumatology Arthroscopy vol 13 no 7 pp 539ndash5442005
[33] B A Rogers P Thornton-Bott S R Cannon and T W RBriggs ldquoInterobserver variation in the measurement of patellarheight after total knee arthroplastyrdquo Journal of Bone and JointSurgery - Series B vol 88 no 4 pp 484ndash488 2006
[34] R P Grelsamer C H Weinstein J Gould and A DubeyldquoPatellar tilt The physical examination correlates with MRimagingrdquo Knee vol 15 no 1 pp 3ndash8 2008
[35] R Gaasbeek R Welsing M Barink N Verdonschot andA Van Kampen ldquoThe influence of open and closed hightibial osteotomy on dynamic patellar tracking A biomechanicalstudyrdquo Knee Surgery Sports Traumatology Arthroscopy vol 15no 8 pp 978ndash984 2007
[36] H Bito R Takeuchi K Kumagai et al ldquoOpening wedge hightibial osteotomy affects both the lateral patellar tilt and patellarheightrdquo Knee Surgery Sports Traumatology Arthroscopy vol 18no 7 pp 955ndash960 2010
[37] T Sasaki and T Yagi ldquoSubluxation of the patella - Investigationby computerized tomographyrdquo International Orthopaedics vol10 no 2 pp 115ndash120 1986
[38] F Boven M-A Bellemans J Geurts and R PotvliegeldquoA comparative study of the patello-femoral joint on axialroentgenogram axial arthrogram and computed tomographyfollowing arthrographyrdquo Skeletal Radiology vol 8 no 3 pp179ndash181 1982
[39] A D Delgado-Martınez C Estrada E C Rodrıguez-MerchanM Atienza and J M Ordonez ldquoCT scanning of the
10 BioMed Research International
patellofemoral joint The quadriceps relaxed or contractedrdquoInternational Orthopaedics vol 20 no 3 pp 159ndash162 1996
[40] S Hinterwimmer M J Feucht J Paul et al ldquoAnalysis of theeffects of high tibial osteotomy on tibial rotationrdquo InternationalOrthopaedics vol 40 no 9 pp 1849ndash1854 2016
[41] K-M Jang J-H Lee H-J Park J L Kim and S-B HanldquoUnintended Rotational Changes of the Distal Tibia AfterBiplane Medial Open-Wedge High Tibial Osteotomyrdquo Journalof Arthroplasty vol 31 no 1 pp 59ndash63 2016
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
BioMed Research International 9
open wedge high tibial osteotomy can prevent patella infera Anew techniquerdquo Knee vol 11 no 6 pp 457ndash461 2004
[9] C M Rodner D J Adams V Diaz-Doran et al ldquoMedialopeningwedge tibial osteotomy and the sagittal planeThe effectof increasing tibial slope on tibiofemoral contact pressurerdquoAmerican Journal of SportsMedicine vol 34 no 9 pp 1431ndash14412006
[10] R E Windsor J N Insall and K G Vince ldquoTechnicalconsiderations of total knee arthroplasty after proximal tibialosteotomyrdquo Journal of Bone and Joint Surgery - Series A vol 70no 4 pp 547ndash555 1988
[11] H E Figgie III V M Goldberg K G Heiple H S MollerIII and N H Gordon ldquoThe influence of tibial-patellofemorallocation on function of the knee in patients with the posteriorstabilized condylar knee prosthesisrdquo Journal of Bone and JointSurgery - Series A vol 68 no 7 pp 1035ndash1040 1986
[12] K Kim D Kim S Song S Lee and D Bae ldquoMedialOpen-Wedge High Tibial Osteotomy May Adversely Affect thePatellofemoral Jointrdquo Arthroscopy The Journal of Arthroscopicamp Related Surgery vol 33 no 4 pp 811ndash816 2017
[13] J S Shim S H Lee H J Jung and H I Lee ldquoHightibial open wedge osteotomy below the tibial tubercle Clinicaland radiographic resultsrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 1 pp 57ndash63 2013
[14] P D Longino T B Birmingham W J Schultz R F Moyerand J R Giffin ldquoCombined tibial tubercle osteotomy withmedial openingwedge high tibial osteotomyminimizes changesin patellar height A prospective cohort study with historicalcontrolsrdquo American Journal of Sports Medicine vol 41 no 12pp 2849ndash2857 2013
[15] S Keyhani M R Abbasian S M Kazemi et al ldquoModifiedretro-tubercle opening-wedge versus conventional high tibialosteotomyrdquo Orthopedics vol 34 no 2 2011
[16] D H Lee K J Ryu H H Kim S Soung and S Shin ldquoFixator-assisted Technique Enables Less Invasive Plate Osteosynthesisin Medial Opening-wedge High Tibial Osteotomy A NovelTechniquerdquo Clinical Orthopaedics and Related Research vol473 no 10 pp 3133ndash3142 2015
[17] S B Han D H Lee G M Shetty D J Chae J G Songand K W Nha ldquoA ldquosafe zonerdquo in medial open-wedge hightibia osteotomy to prevent lateral cortex fracturerdquoKnee SurgerySports Traumatology Arthroscopy vol 21 no 1 pp 90ndash95 2013
[18] D Paley and K Tetsworth ldquoMechanical axis deviation ofthe lower limbs Preoperative planning of uniapical angulardeformities of the tibia or femurrdquo Clinical Orthopaedics andRelated Research no 280 pp 48ndash64 1992
[19] J Insall and E Salvati ldquoPatella position in the normal kneejointrdquo Radiology vol 101 no 1 pp 101ndash104 1971
[20] R P Grelsamer and S Meadows ldquoThe modified Insall-Salvatiratio for assessment of patellar heightrdquo Clinical Orthopaedicsand Related Research no 282 pp 170ndash176 1992
[21] J S Blackburne and T E Peel ldquoA new method of measuringpatellar heightrdquo J Bone Joint Surg Br vol 59 no 2 pp 241-2421977
[22] J Caton G Deschamps P Chambat J L Lerat and HDejour ldquoPatella infera Apropos of 128 casesrdquo Rev Chir OrthopReparatrice Appar Mot vol 68 no 5 pp 317ndash325 1982
[23] H Miura H Kawamura R Nagamine K Urabe and YIwamoto ldquoIs patellar height really lower after high tibialosteotomyrdquo Fukuoka igaku zasshi = Hukuoka acta medica vol88 no 6 pp 261ndash266 1997
[24] H Delgado-Martins ldquoThe bicondylo-patellar angle as a mea-sure of patellar tiltingrdquo Archives of Orthopaedic and TraumaticSurgery vol 96 no 4 pp 303-304 1980
[25] V Vahasarja P Lanning S Lahde and W Serlo ldquoAxialradiography or CT in the measurement of patellofemoralmalalignment indices in children and adolescentsrdquo ClinicalRadiology vol 51 no 9 pp 639ndash643 1996
[26] U M Kujala K Osterman M Kormano M Komu and DSchlenzka ldquoPatellar motion analyzed by magnetic resonanceimagingrdquo Acta Orthopaedica vol 60 no 1 pp 13ndash16 1989
[27] C A Laurin R Dussault and H P Levesque ldquoThe tan-gential X-ray investigation of the patellofemoral joint X-raytechnique diagnostic criteria and their interpretationrdquo ClinicalOrthopaedics and Related Research no 144 pp 16ndash26 1979
[28] R Seil B Muller T Georg D Kohn and S Rupp ldquoReliabilityand interobserver variability in radiological patellar heightratiosrdquo Knee Surgery Sports Traumatology Arthroscopy vol 8no 4 pp 231ndash236 2000
[29] N Elmali I Esenkaya M Can and M Karakaplan ldquoMono-planar versus biplanar medial open-wedge proximal tibialosteotomy for varus gonarthrosis A comparison of clinicaland radiological outcomesrdquo Knee Surgery Sports TraumatologyArthroscopy vol 21 no 12 pp 2689ndash2695 2013
[30] S Hinterwimmer K Beitzel J Paul et al ldquoControl of posteriortibial slope and patellar height in open-wedge valgus high tibialosteotomyrdquo American Journal of Sports Medicine vol 39 no 4pp 851ndash856 2011
[31] S Hopwood W Khan and S Agarwal ldquoThe biplanar openwedge high tibial osteotomy preserving the tibial tuberclerdquoJournal of Orthopaedic Science vol 21 no 6 pp 786ndash790 2016
[32] H Kesmezacar R Erginer T Ogut A Seyahi M Babacan andY Tenekecioglu ldquoEvaluation of patellar height and measure-ment methods after valgus high tibial osteotomyrdquo Knee SurgerySports Traumatology Arthroscopy vol 13 no 7 pp 539ndash5442005
[33] B A Rogers P Thornton-Bott S R Cannon and T W RBriggs ldquoInterobserver variation in the measurement of patellarheight after total knee arthroplastyrdquo Journal of Bone and JointSurgery - Series B vol 88 no 4 pp 484ndash488 2006
[34] R P Grelsamer C H Weinstein J Gould and A DubeyldquoPatellar tilt The physical examination correlates with MRimagingrdquo Knee vol 15 no 1 pp 3ndash8 2008
[35] R Gaasbeek R Welsing M Barink N Verdonschot andA Van Kampen ldquoThe influence of open and closed hightibial osteotomy on dynamic patellar tracking A biomechanicalstudyrdquo Knee Surgery Sports Traumatology Arthroscopy vol 15no 8 pp 978ndash984 2007
[36] H Bito R Takeuchi K Kumagai et al ldquoOpening wedge hightibial osteotomy affects both the lateral patellar tilt and patellarheightrdquo Knee Surgery Sports Traumatology Arthroscopy vol 18no 7 pp 955ndash960 2010
[37] T Sasaki and T Yagi ldquoSubluxation of the patella - Investigationby computerized tomographyrdquo International Orthopaedics vol10 no 2 pp 115ndash120 1986
[38] F Boven M-A Bellemans J Geurts and R PotvliegeldquoA comparative study of the patello-femoral joint on axialroentgenogram axial arthrogram and computed tomographyfollowing arthrographyrdquo Skeletal Radiology vol 8 no 3 pp179ndash181 1982
[39] A D Delgado-Martınez C Estrada E C Rodrıguez-MerchanM Atienza and J M Ordonez ldquoCT scanning of the
10 BioMed Research International
patellofemoral joint The quadriceps relaxed or contractedrdquoInternational Orthopaedics vol 20 no 3 pp 159ndash162 1996
[40] S Hinterwimmer M J Feucht J Paul et al ldquoAnalysis of theeffects of high tibial osteotomy on tibial rotationrdquo InternationalOrthopaedics vol 40 no 9 pp 1849ndash1854 2016
[41] K-M Jang J-H Lee H-J Park J L Kim and S-B HanldquoUnintended Rotational Changes of the Distal Tibia AfterBiplane Medial Open-Wedge High Tibial Osteotomyrdquo Journalof Arthroplasty vol 31 no 1 pp 59ndash63 2016
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
10 BioMed Research International
patellofemoral joint The quadriceps relaxed or contractedrdquoInternational Orthopaedics vol 20 no 3 pp 159ndash162 1996
[40] S Hinterwimmer M J Feucht J Paul et al ldquoAnalysis of theeffects of high tibial osteotomy on tibial rotationrdquo InternationalOrthopaedics vol 40 no 9 pp 1849ndash1854 2016
[41] K-M Jang J-H Lee H-J Park J L Kim and S-B HanldquoUnintended Rotational Changes of the Distal Tibia AfterBiplane Medial Open-Wedge High Tibial Osteotomyrdquo Journalof Arthroplasty vol 31 no 1 pp 59ndash63 2016
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom