ontology-based convergence of medical terminologies: snomed ct and icd-11 institute for medical...
TRANSCRIPT

Ontology-based Convergence of Medical Terminologies: SNOMED CT and ICD-11
Institute for Medical Informatics, Statistics and Documentation, Medical University of Graz, Austria Institute of Medical Biometry and Medical Informatics, University Medical Center Freiburg, Germany
University of Manchester, UK
University of Saint Etienne, CHU, FranceINSERM UMR 872 Eq 20, Paris, France
Mayo Clinic, Minnesota, US
World Health Organization, Geneva
International Health Terminology Standard Development Organisation, Copenhagen, Denmark
Stefan Schulz
Alan Rector
Jean-Marie Rodrigues
Christopher Chute
Bedirhan Üstün
Kent Spackman
WHO – IHTSDO Joint Advisory Group (JAG) for the harmonisation between ICD-10, ICD-11 and SNOMED CT

ICD-11 – SNOMED CT Harmonization
• Background:– ICD: disease classification maintained by WHO (World Health Organization)
ICD-11 revision process ongoing– SNOMED CT: ontology-based clinical terminology maintained by IHTSDO
(International Health Terminology Standards Development Organisation)– Size: SNOMED CT >> ICD, – Coverage: ICD only diseases, SNOMED CT: all EHR content
• Institutional agreement between WHO and IHTSDO:– Goal: common ontological basis for both the
ICD-11 foundation component (FC) and SNOMED CT– Practical implications:
• Each class in the ICD-11 foundation component will correspond to exactly one class in SNOMED CT.
• The transitive closure of taxonomic (subclass) relations in ICD-11-FC is included in the transitive closure of these relations in SNOMED CT.

ICD - SNOMED CT Mapping principle
• Taxonomies are main construction principle for both terminologies• Edges correspond to subclass links. Each ICD class corresponds to
exactly one SNOMED class (same letter). • Subclass links contained in ICD but not SNOMED must be obtained
by transitive closure.
SNOMED CTICD 11 Foundation
Component(multihierarchical)

Two Principles of ontology-based mapping of SNOMED CT and ICD-11
1. The semantics of the subclass relation is shared
2. Classes to be aligned denote the same types of entities
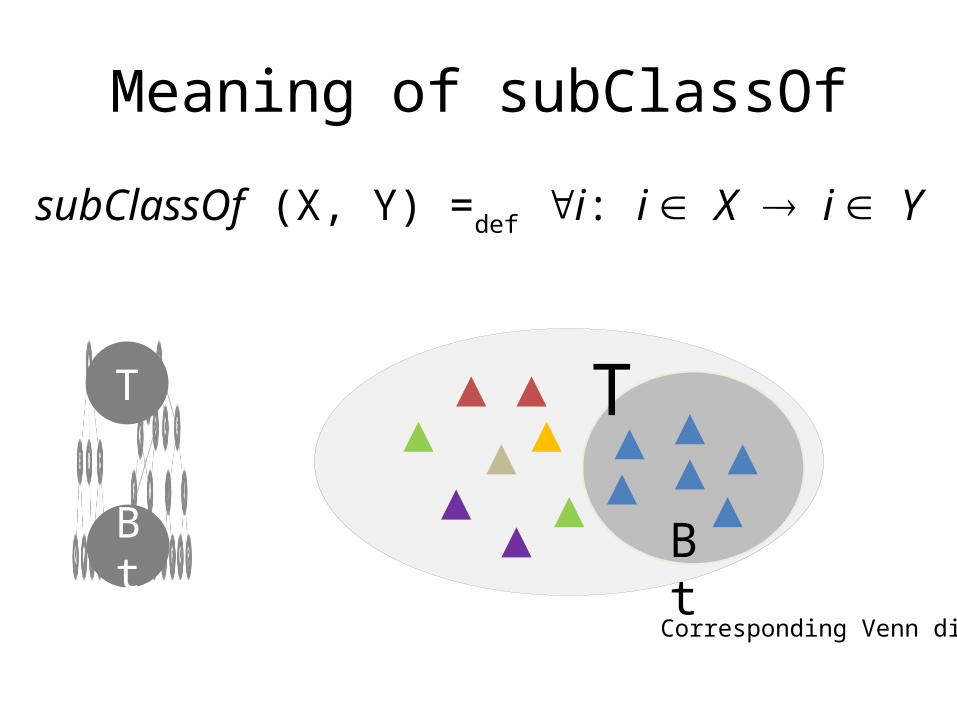
Meaning of subClassOf
Graph Corresponding Venn diagram
T
Bt
T
Bt
subClassOf (X, Y) =def i: i X i Y

Two Principles of ontology-based alignment of SNOMED CT and ICD-11
1. The semantics of the subclass relation is shared
2. Classes to be aligned denote the same types of entities
?

Is this correct?Fracture of
UlnaFracture of
Radius
Fracture ofRadius and Ulna
subClassOf subClassOf
Fracture
FractureSNOMED CT Example

Is this correct?Fracture of
UlnaFracture of
Radius
Fracture ofRadius and Ulna
subClassOf subClassOf
Fracture
FractureSNOMED CT Example
• No, if “clinical condition”: the combined fracture is composed by the two single fractures, not a subtype
• Yes, if “clinical situation”: “situation with X” or “patient having X”

Clinical condition viewFractured ulnaFractured radius
Fractured radius + ulna
No overlap / inclusion of classes

Clinical situation view
Clinical situation with fractured ulna
U
URU
RUU
RUR
R
R
Clinical situation with fractured radius

Current axiomatization in SNOMED CT
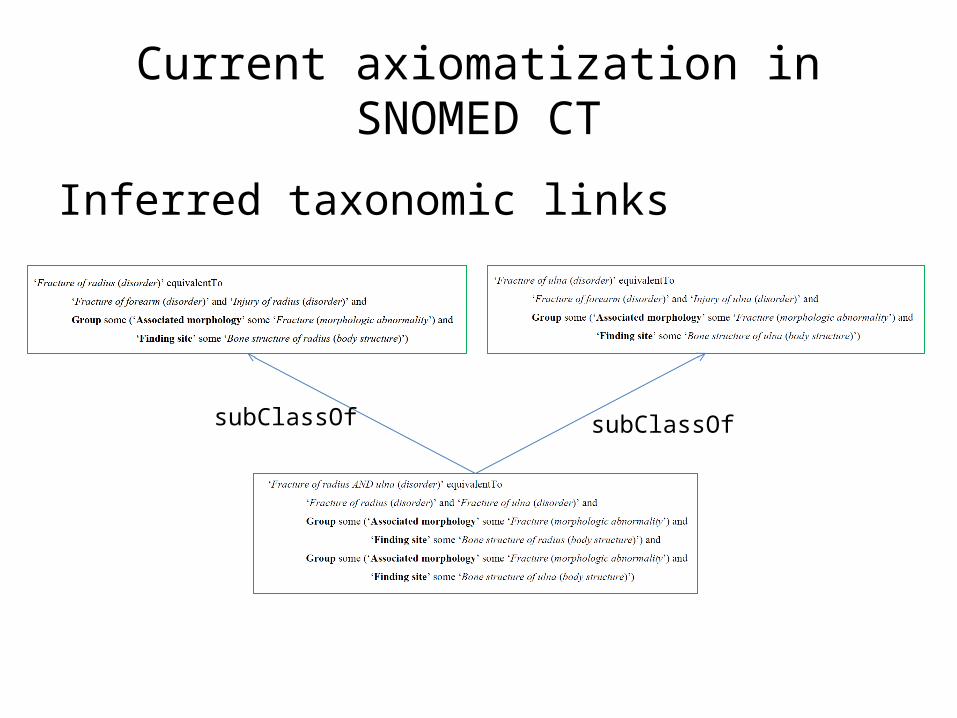
Current axiomatization in SNOMED CT
Inferred taxonomic links
subClassOf subClassOf

Facts / Hypotheses
• “Problematic” subclass links between SNOMED CT classes result from formal (description logics) definitions
• It can be shown:
Acond subClassOf Bcond entails:
Asit subClassOf Bsit
Acond subClassOf hasPart Bcond entails:
Asit subClassOf Bsit
More subClassOf relations between situation classes

Review of 400 sample SNOMED CT disorder concepts
• Four experts: K. Spackman, A. Rector, J.-M. Rodrigues, S. Schulz
• Assessment of a sample of 400 SNOMED disorder concepts – Fully specified names– Formal definitions– Parent classes– Child classes
• Evidence for “clinical situation” readingSchulz S, Rector A, Rodrigues JM, Spackman K. Competing Interpretations of Disorder Codes in SNOMED CT and ICD. Submitted to AMIA 2012

Results
• ~ 11% of disorder evidence that they represent situations and not conditions (such as Fracture of radius and ulna)
• For the rest, both interpretations are possible• Agreement difficult – fuzzy boundary between
what should be interpreted as a clinical condition and what as a clinical situation .

Possible actions
1. Redesigning the SNOMED CT disorder hierarchy to exclude interpretation a clinical situations: huge effort, difficult boundary decisions
2. Leaving disorder classes uncommitted: should support condition interpretation: many existing subclass relations wrong
3. Considering all SNOMED CT disorder codes as denoting clinical situations: – more robust– consistent with current state of the disorder hierarchy– agreement with ICD view on the meaning of the code– compatible with clinical use cases

Foundations of ontology-based alignment of SNOMED CT and ICD-11
1. The semantics of the subclass relation is shared
2. Classes to be aligned denote the same types of entities
subClassOf (X, Y) =def i: i X i Y
SNOMED CT disorder codes andICD-11 classes denote:Clinical Situations


Example 2

Example 2Extension of “Pulmonic Valve Stenosis” includes extension of “Tetralogy of Fallot”: FALSE

Example 2
F
P
P
P
P
FF
P
F
P
P
Extension of “Situation with Pulmonic Valve Stenosis” includes extension of “Situation with Tetralogy of Fallot”: TRUE

Two diverging interpretations of disorder terms in SNOMED CT and ICD:
• They denote patient-borne Conditions such as body processes, states, dispositions, or (patho-) anatomical structures, which are reportable in the context of medical records
• They denote Clinical Situations, which are defined as phases of a patient’s life, during which he/she is bearer of (some combination of) pathological conditions.

Situations, conditions and role groups

Facts / Hypotheses
• Most SNOMED CT disorder concepts contain role groups
• The role group link can be interpreted as a relation that links a situation with a condition
• It can be shown:– ‘A_cond subClass of B_cond’ entails:
‘A_sit subClass of B_sit’– ‘A_cond subClass of hasPart B_cond’ entails:
‘A_sit subClass of B_sit’Schulz S, Rector A , Rodrigues JM ,Chute C , Üstün B , Spackman K . ONTOLOGY-BASED CONVERGENCE OF MEDICAL TERMINOLOGIES: SNOMED CT AND ICD-11. In: Schreier G, Hayn D, Hörbst A, Ammenwerth E, editors. Proceedings of the eHealth2012. 2012 Mai 10-11; Vienna, Austria. OCG; 2012.

Proper parts or taxonomic parents ?
is-a is-a is-a is-a is-a is-a is-a
Tetralogy of Fallot Traffic Light
Red Light Yellow Light Green LightVSD PVS RVH OA
Example from Harold Solbrig

Proper parts or taxonomic parents ?
subClassOf
Combined fracture Traffic Light
Red Light Yellow Light Green Light
Example from Harold Solbrig
subClassOf