older adult survivorship
TRANSCRIPT
Older Adult Survivorship Meghan Routt, MSN ANP/GNP-BC, AOCNP
• I have no financial conflict of interest
Objectives
• At the end of this session the participant will be able to: • Describe some of the main barriers to treatment in the older adult population
• Identify common side effects of cancer treatment and specific challenges of treatment in the older adult
• Identify four common geriatric syndromes

The “Silver Tsunami”
• By the year 2050, the number of adults over the age of 65 will double (to approximately 89 million people) and will contribute a 45% increase in the number of people developing cancer 1
• Adults over the age of 65 account for 54% of all cancer patients and 69.5% of all cancer deaths occur in this age group2
• Aging is the biggest risk factor for developing cancer

Why do we care?
• Older adults have certain changes in their physiology which providers need to keep in mind when prescribing medications or other therapy
Body system Changes in the older adult
Skin Loses elasticity, loses ability to keep moisture in, thins, more apt for injury
Renal function Decreases with age, lose 1ml/min/year of GFR after the age of 30. Renal blood flow decreases by 50%
Urinary Incontinence is NEVER normal, increased frequency of urinary tract infections due to impaired bladder emptying
Gastrointestinal Constipation: due to medication, due to inactivity, due to decreased peristalsis Diarrhea: more prone to dehydration, increased risk for falls
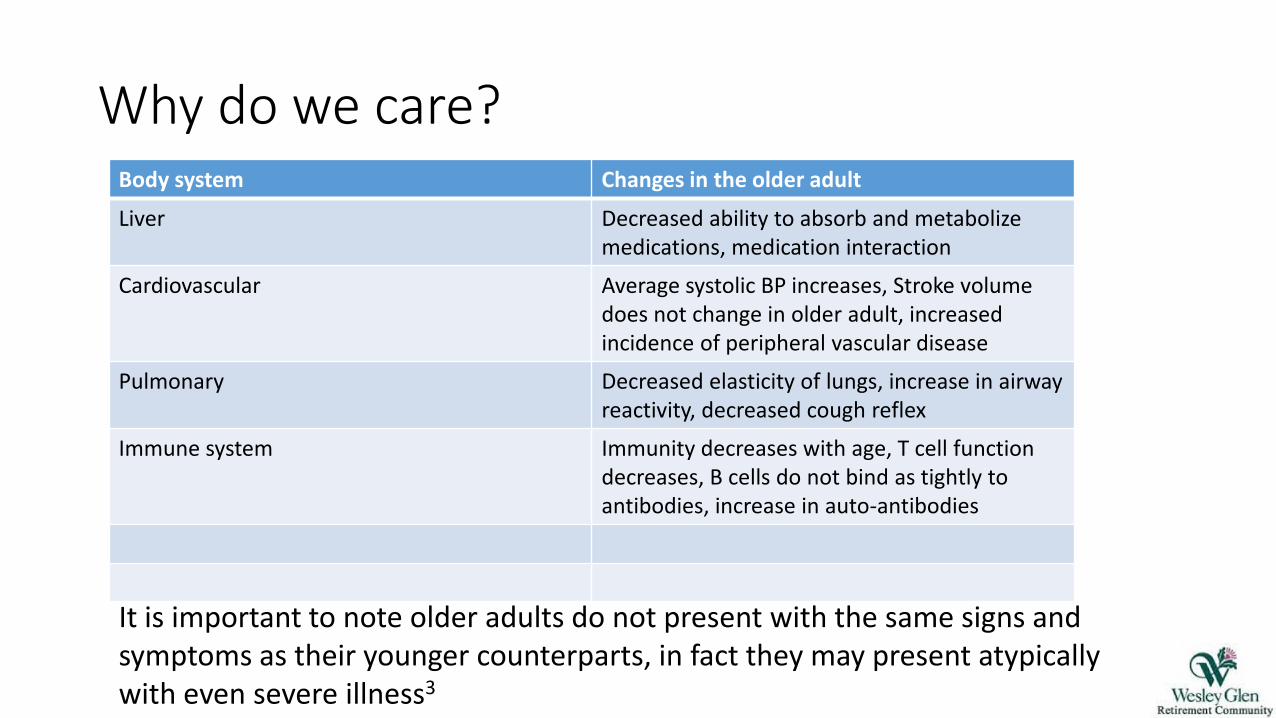
Why do we care? Body system Changes in the older adult
Liver Decreased ability to absorb and metabolize medications, medication interaction
Cardiovascular Average systolic BP increases, Stroke volume does not change in older adult, increased incidence of peripheral vascular disease
Pulmonary Decreased elasticity of lungs, increase in airway reactivity, decreased cough reflex
Immune system Immunity decreases with age, T cell function decreases, B cells do not bind as tightly to antibodies, increase in auto-antibodies
It is important to note older adults do not present with the same signs and symptoms as their younger counterparts, in fact they may present atypically with even severe illness3
Guidelines to treat older adults with cancer

NCCN Clinical Practice Guidelines
• It is important to note, treatment is based on the patient’s goals and age is not considered a primary risk factor for surgical or medical treatment3
• Unfortunately, studies have shown older adults do not receive “standard of care” treatment for many diseases including breast cancer, colon cancer, kidney, bladder
• Comprehensive Geriatric Assessments (CGA) should be done prior to any treatment • Includes assessments in all domains of health • Nutrition, Activities of daily living, Depression, Dementia, Health
related quality of life, Physical exertion

NCCN Clinical Practice Guidelines
• Mucositis • Early hospitalization is needed for patients who develop dysphagia/diarrhea • Provide nutritional support
• Bone marrow suppression • Prophylactic colony-stimulating factors are needed when dose intensity is required for
response
• Neurotoxicity • Monitor hearing loss, peripheral neuropathy and cognitive dysfunction
• Cardiac toxicity • Monitor for symptomatic or asymptomatic heart failure, especially with the use of
anthracyclines and trastuzumab
• Renal toxicity • Adjust dose for glomerular filtration rate to reduce systemic toxicity
• Insomnia • Nonpharmacologic methods are recommended • Do not use hypnotics, Benadryl or benzodiazepenes as first line treatment for insomnia

Surgery and the older adult

Chemotherapy and the Older Adult
• Two specific tools for the older adult in monitoring chemotherapy risk assessment and toxicity:
• Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) Score: http://eforms.moffitt.org/crashScore.aspx
• Cancer and Aging Research Group (CARG) Chemo toxicity Calculator http://www.mycarg.org
A cancer survivor story…

Tom’s story
• Diagnosed with metastatic prostate cancer to bone (right hip and sacrum)
• Previously underwent a total prostatectomy
• Now receiving Lupron q6 months and Xjeva monthly
• Tom’s major issues:
• Transportation/Family Dynamics
• Pain
Tom’s Survivorship issues
• Transportation and family dynamics
• His ex-wife Dottie was his primary means of transportation as well as picked up him controlled substances as he no longer drives
• Dottie is not his healthcare power of attorney
• Dottie has had issues with alcoholism
• Dottie recently diagnosed with a brain tumor
• Pain • Treating urologist did not assess Tom’s pain
• His primary care provider has him on MS Contin 30mg BID with norco for breakthrough
Older adult pain management
• Pain is one of the most frequently reported symptom in this age group regardless of survivorship stage5
• Furthermore, at least 42% of older adult patients with cancer report unrelieved pain6
• This is due to many factors but primarily:
• Older adults’ believe that pain is a normal part of aging
• They do not want to become “addicted”
• Clinicians do not adequately assess their pain (occurs a lot in patients who have cognitive impairment)
Older Adult Cancer Pain Management
• Unrelieved pain can lead to depression, sleep, appetite disturbances and an increase in healthcare utilization and cost7
• Pain is often nociceptive and neuropathic pain
• Older adults may achieve pain relief at lower doses than younger people who report the same severity8
• Acetaminophen or other non-steroidal anti-inflammatories is first line treatment for nociceptive pain
• Narcotics often provide good pain relief and methadone is a good long acting agent in older adults due to minimal renal clearance.

Older adult cancer pain management
Retrieved from: http://www.who.int/cancer/palliative/painladder/en/

Other Geriatric Survivorship Issues
• Polypharmacy • Defined as the use of 9 or more medications • It is estimated that all people age 65 and above take two to nine
prescriptions each day • Additionally, 50% take two to four over the counter medications
daily and 47-59% ingest vitamins or minerals daily9 • Biggest issue occurs when a medication is prescribed to counteract
a side effect of another medication • Significant risk factor in the exacerbation of common geriatric
syndromes such as dementia, delirium, depression, malnutrition, falls or urinary incontinence9

Wait…what are geriatric syndromes?
• The term geriatric syndromes incorporate unique features of common health conditions in older adults
• Include: Dementia, Failure to thrive, delirium, Falls, urinary incontinence
• People can have one, some, or none of these]

Risk for Falls
• Thirty percent of older adults who live at home experience at least one fall annually11
• Injurious falls are also the primary cause of accidental deaths in this age group11
• It is imperative older adult cancer survivors be asked about whether they have fallen or not as well as be screened at every appointment1

Questions?
References • 1. US Department of Commerce Census Bureau (2012). Population projections. Retrieved February 15, 2016 from
http://www.census.gov/population/projections/data/national/2012/summarytables.html.
• 2. Howlader N, Noone AM, Krapcho M, Garshell J, Miller D, Altekruse SF…& Cronin KA (eds). (2013). SEER Cancer Statistics Review, 1975-2011, National Cancer Institute. Bethesda, MD retrieved February 15, 2016 from: http://seer.cancer.gov/csr/1975_2011/ .
• 3. Walker, M., Spivak, M., & Sebastian, M. (2014). The impact of aging physiology in critical care. Critical Care Nursing Clinics of North America, 26, 7-14.
• 4. National Comprehensive Cancer Network. (2016). NCCN guidelines: Older Adult Oncology. Version 1. 2016. Retrieved from: https://www.nccn.org/professionals/physician_gls/pdf/senior.pdf
• 5. Mohanty, S., Rosethal, B.A., Russell, M.M., Neuman, M.D, Ko, B.Y & Esanola, N.F. (2012) Optimal perioperative management of the geriatric patient: Best practices guideline from ACS NSQIP/American Geriatrics Society. Retrieved from: https://www.facs.org/~/media/files/quality%20programs/geriatric/acs%20nsqip%20geriatric%202016%20guidelines.ashx
• 6. Beck, S., Towsley, G., Caserta, M., Lindau, K. & Dudley, W. (2009). Symptom experiences and quality of life of rural and urban older adult cancer survivors. Cancer Nursing, 32, 359-369.
• 7. Barford, K. & D’Olimpio, J.T. (2008). Symptom management in geriatric oncology: Practical treatment considerations and current challenges. Current Treatment Options in Oncology, 9, 204-214.
• 8. Sutton, L.M., Denmark-Wahnefried, W., & Clipp, E.C. (2003). Management of terminal cancer in elderly patients, Lancet Oncology, 4, 149-157.
• 9. Mercadante, S. & Arcuri, E. (2007). Pharmacological management of cancer pain in the elderly. Drugs and Aging, 24, 761-776
• 10. Flood, K.L., Carrol, M.B., Le, C.V. & Brown, C.J. (2009). Polypharmacy in hospitalized older adult cancer patients: Experience from a prospective, observational study of an oncology-acute care for elders unit. American Journal of Geriatric Pharmacotherapy, 7, 151-158.
• 11. Day., L., Fildes, B., Gordon, I., Fitzharris, M., Flamer, H., & Lord, S. (2002). Randomised factorial trial of falls prevention among older people living in their own homes. BMJ, 325, 128.