offloading: how and why? the ransart boot - jscimed central · offloading: how and why? the ....
TRANSCRIPT
CentralBringing Excellence in Open Access
JSM Foot and Ankle
Cite this article: Dumont I (2017) Offloading: How and Why? The Ransart boot. JSM Foot Ankle 2(3): 1028.
*Corresponding authorIsabelle Dumont, Department of Internal Medicine, Vrije Universiteit Brussel, rue du Melon 1190 Bruxelles, Belgium, Tel: 32475433970; Fax: 323443970; Email: [email protected]
Submitted: 28 May 2018
Accepted: 17 May 2017
Published: 19 May 2017
ISSN: 2475-9112
Copyright© 2017 Dumont
OPEN ACCESS
Keywords•Diabetic Foot Ulcer (DFU)•Offloading•Ransart boot•Total Contact Cast (TCC)•Half shoe•Healing•Amputation
Review Article
Offloading: How and Why? The Ransart bootIsabelle Dumont*Department of Internal Medicine, Vrije Universiteit Brussel, Belgium
Abstract
Plantar ulcers are one of the most common complications of diabetes. It is difficult to treat and leads, still today, to too many amputations. The decrease in the number of these amputations remains the goal, apparently easy and yet so difficult in practice, to reach of all diabetic foot specialists. Offloading is the basis of the treatment of Diabetic Foot Ulcer (DFU), we will begin by demonstrating this in detail. There are numerous methods of offloading of different effectiveness and simplicity of use, non removable or removable and also other modalities often used and yet poorly effective. We will describe them briefly and summarize the results reported in the literature. Among all these devices, we will be particularly interested by the Ransart boot. This means of offloading is a lightweight, removable, quickly made and easy-to-use windowed resin cast which enable patients to continue their everyday life activities while unloading their wound. We report the results of two open, retrospective and multicenter studies evaluating the efficacy and safety of this boot in the treatment of diabetic foot ulcers. The Ransart boot appears to be an effective, safe and inexpensive offloading technique for all types of ulcers, whether infected and / or ischemic, as well as for ulcers on Charcot feet that are not active.
ABBREVIATIONSUT: University of Texas Classification; TCC: Total Contact
Cast; RCT: Randomized Controlled Trial
INTRODUCTIONMore than 15% of diabetics will suffer from a foot ulcer
during their lifetime [1] and up to 84% of all major amputations in diabetic are preceded by an ulcer [1].
Offloading
Offload the ulcer: why?: Abnormal forces applied to the skin play a key role in the pathogenesis of the majority of foot ulcers. When an ulcer appears, it is therefore fundamental to minimize these forces [2]. The purpose of offloading is to redistribute these forces from the ulcerated zone and the pressure points at risk to a wider area.
University of Texas or Armstrong Classification (UT): This classification is a double-entry table that takes into account both the depth of the wound (grade) and the presence or absence of infection and / or ischemia (stage) . This classification has a predictive value for healing and has been validated for DFU in diabetic patients. The percentage in each cell corresponds to the amputation rate in the Armstrong validation study [3].
Effectiveness and evidence
Histological changes and offloading: 20 diabetic patients with UT class 1A and 2A ulcers has been randomized to 2 groups:
one treated with ulcerrectomy and the other with a TCC (Total Contact Cast) for 20 Days followed by ulcerectomy [4,5]. After offloading, the wound of the diabetic foot resembles in many points to an acute wound and thus heals more easily Table 1. Without effective debridement and adequate offloading, no other modality, however promising or revolutionary, will help to heal these wounds more quickly and ultimately prevent many unnecessary amputations of the lower limbs Table 2.
Dressings: No dressing proved to be superior to the physiological saline impregnated compress in terms of healing [6]. One RCT compared TCC versus traditional dressing. 40 patients were followed for 12 weeks [7]. TCC significantly increased healing (91% healed with TCC versus 32% treated only with a dressing after 12 weeks). It reduces occurence of infection compared with traditional dressings [7].
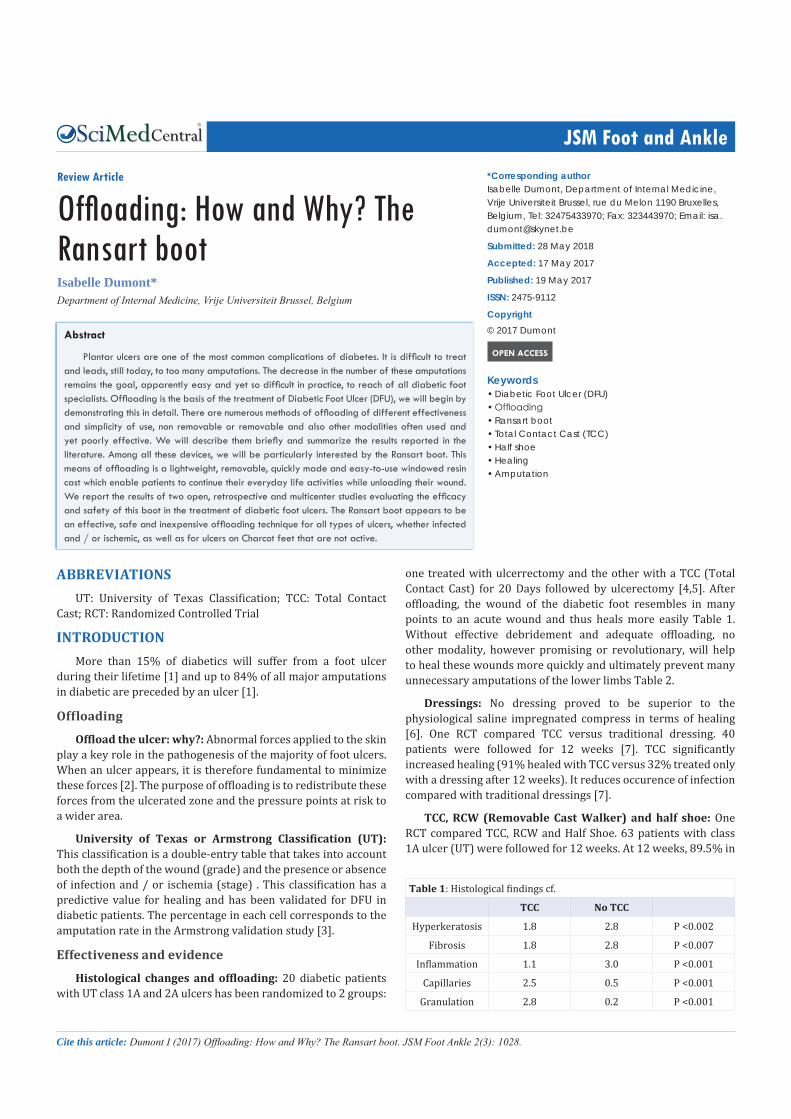
TCC, RCW (Removable Cast Walker) and half shoe: One RCT compared TCC, RCW and Half Shoe. 63 patients with class 1A ulcer (UT) were followed for 12 weeks. At 12 weeks, 89.5% in
Table 1: Histological findings cf.
TCC No TCC
Hyperkeratosis 1.8 2.8 P <0.002
Fibrosis 1.8 2.8 P <0.007
Inflammation 1.1 3.0 P <0.001
Capillaries 2.5 0.5 P <0.001
Granulation 2.8 0.2 P <0.001
CentralBringing Excellence in Open Access
Proietti et al. (2017)Email:
JSM Foot Ankle 2(3): 1028 (2017) 2/7
the TCC group had healed, 65% in the RCW group and 58% in the Half Shoe group (8). The lower the plantar pressure, the faster the healing process [8] Figure 1, Offloading is the treatment that gives the best results in terms of rate and healing time.
Offloading: How?
In thinking “offloading” we intuitively want to put something on the foot a very thick dressing, padding or device. And yet the first and most important thing to do to unload a wound is actually removing something [5]. “It’s Not What You Put On, But What You Take Off ....”.
A good offloading “device” should
• Be usable by all patients
• Do not cause side effects
• Be easily set up and inexpensive
• Encourage compliance: (patient mobility and usual activities should be taken into account when choosing the type of device)
• Causes effective reduction of pressure on the ulcer at any time
And depends on:
• The general condition of the wound (localization etc ...)
• Frequency of wound and foot control required
• The infrastructure available
• A large number of offloading device are available, ranging from the simplest to the most complex, from the non-removable to the removable through the insoles and other orthotics
Non Removable Devices
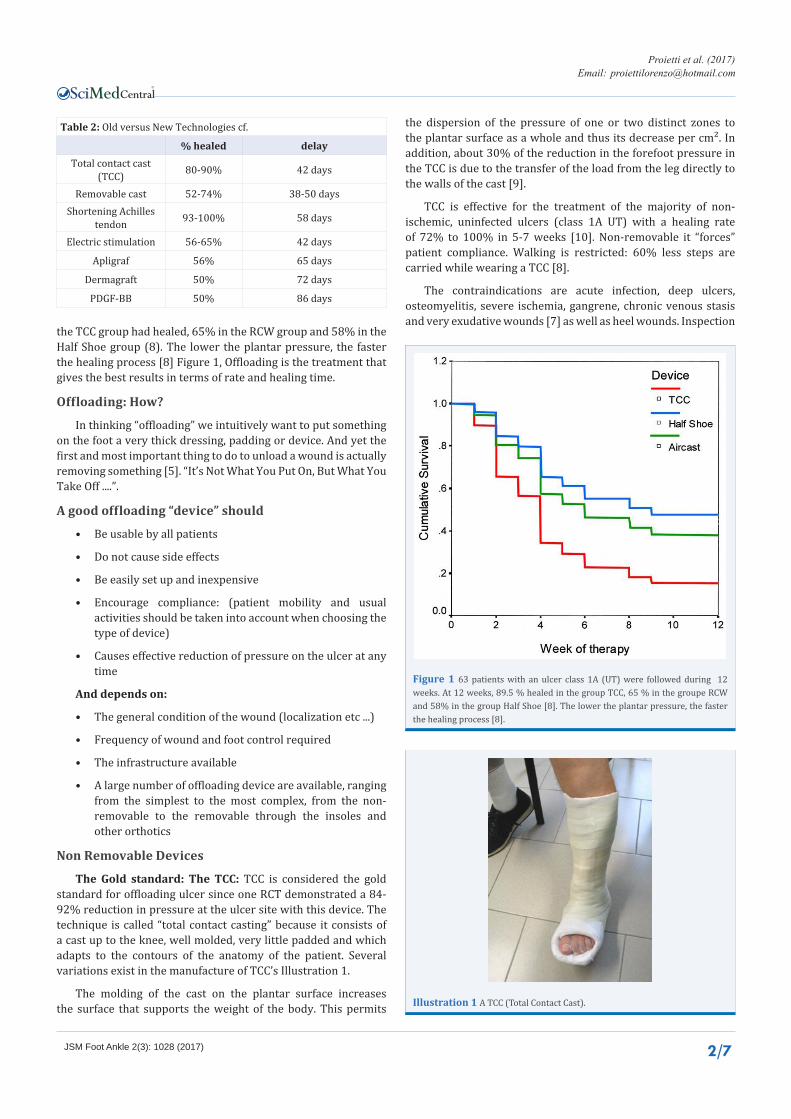
The Gold standard: The TCC: TCC is considered the gold standard for offloading ulcer since one RCT demonstrated a 84-92% reduction in pressure at the ulcer site with this device. The technique is called “total contact casting” because it consists of a cast up to the knee, well molded, very little padded and which adapts to the contours of the anatomy of the patient. Several variations exist in the manufacture of TCC’s Illustration 1.
The molding of the cast on the plantar surface increases the surface that supports the weight of the body. This permits
the dispersion of the pressure of one or two distinct zones to the plantar surface as a whole and thus its decrease per cm². In addition, about 30% of the reduction in the forefoot pressure in the TCC is due to the transfer of the load from the leg directly to the walls of the cast [9].
TCC is effective for the treatment of the majority of non-ischemic, uninfected ulcers (class 1A UT) with a healing rate of 72% to 100% in 5-7 weeks [10]. Non-removable it “forces” patient compliance. Walking is restricted: 60% less steps are carried while wearing a TCC [8].
The contraindications are acute infection, deep ulcers, osteomyelitis, severe ischemia, gangrene, chronic venous stasis and very exudative wounds [7] as well as heel wounds. Inspection
Table 2: Old versus New Technologies cf.
% healed delayTotal contact cast
(TCC) 80-90% 42 days
Removable cast 52-74% 38-50 daysShortening Achilles
tendon 93-100% 58 days
Electric stimulation 56-65% 42 days
Apligraf 56% 65 days
Dermagraft 50% 72 days
PDGF-BB 50% 86 days
Figure 1 63 patients with an ulcer class 1A (UT) were followed during 12 weeks. At 12 weeks, 89.5 % healed in the group TCC, 65 % in the groupe RCW and 58% in the group Half Shoe [8]. The lower the plantar pressure, the faster the healing process [8].
Illustration 1 A TCC (Total Contact Cast).
CentralBringing Excellence in Open Access
Proietti et al. (2017)Email:
JSM Foot Ankle 2(3): 1028 (2017) 3/7
of the wound and foot daily is impossible. Inadequate application may result in new ulcers. A special skill is required. Its realization takes time and is costly. Daily activities are limited.
Less than 2% of specialized centres in the US use TCC [11]. Why? Because its application takes longer than other methods and requires a skilled technician and it is poorly accepted by patients!
Removable devices
Crutches, walkers and wheelchairs: In absolute terms these techniques may seem very effective, but: the majority of patients lack strength especially in the upper limbs to use crutches. Crutches and walkers are difficult to use because of the balance problems associated with neuropathy. The contralateral limb is at risk of ulceration due to increase in pressure on the “healthy” side. Most homes are not suitable for wheelchairs. Rest in bed is rarely respected and can lead to pressure sores and phlebitis Illustration 2. Compared to TCC and RCW, Half Shoe is ranked 3rd in terms ofreduction in pressure at the forefoot [12-14] cf. Figure 1. Compliance is a problem because they are removable. Half Shoe has a significantly less good healing rate at 12 weeks compared with TCC and RCW [12].
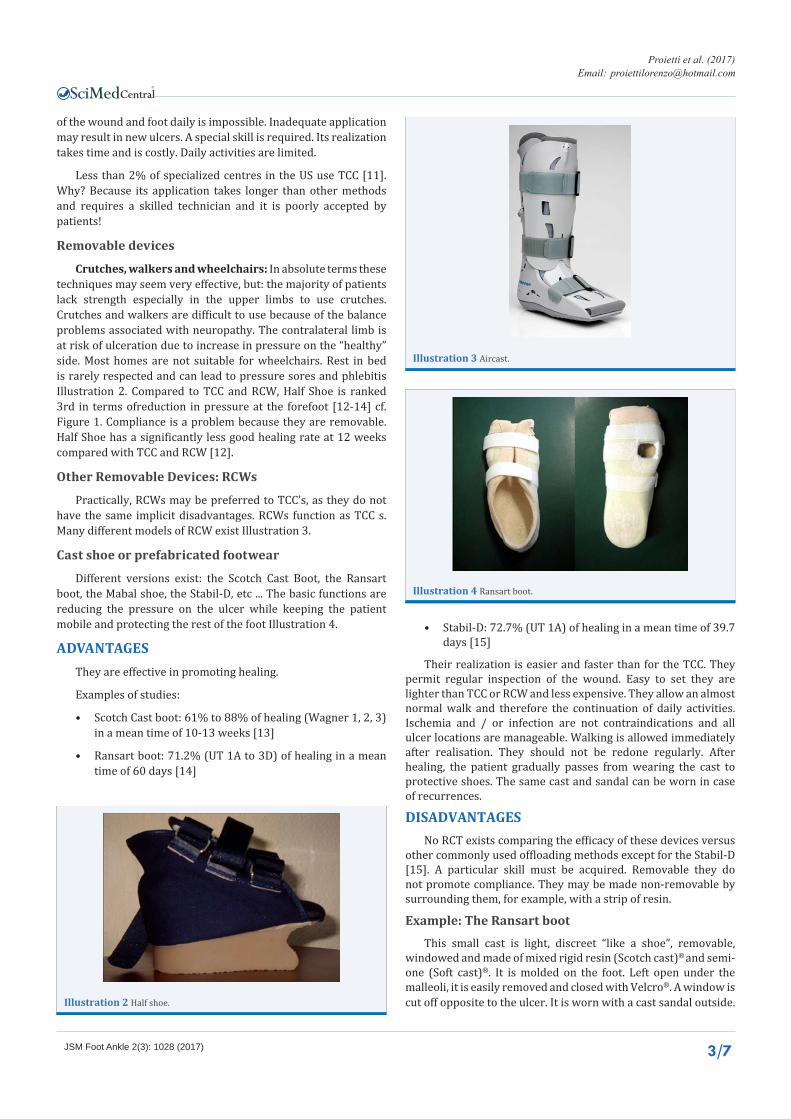
Other Removable Devices: RCWs
Practically, RCWs may be preferred to TCC’s, as they do not have the same implicit disadvantages. RCWs function as TCC s. Many different models of RCW exist Illustration 3.
Cast shoe or prefabricated footwear
Different versions exist: the Scotch Cast Boot, the Ransart boot, the Mabal shoe, the Stabil-D, etc ... The basic functions are reducing the pressure on the ulcer while keeping the patient mobile and protecting the rest of the foot Illustration 4.
ADVANTAGESThey are effective in promoting healing.
Examples of studies:
• Scotch Cast boot: 61% to 88% of healing (Wagner 1, 2, 3) in a mean time of 10-13 weeks [13]
• Ransart boot: 71.2% (UT 1A to 3D) of healing in a mean time of 60 days [14]
• Stabil-D: 72.7% (UT 1A) of healing in a mean time of 39.7 days [15]
Their realization is easier and faster than for the TCC. They permit regular inspection of the wound. Easy to set they are lighter than TCC or RCW and less expensive. They allow an almost normal walk and therefore the continuation of daily activities. Ischemia and / or infection are not contraindications and all ulcer locations are manageable. Walking is allowed immediately after realisation. They should not be redone regularly. After healing, the patient gradually passes from wearing the cast to protective shoes. The same cast and sandal can be worn in case of recurrences.
DISADVANTAGESNo RCT exists comparing the efficacy of these devices versus
other commonly used offloading methods except for the Stabil-D [15]. A particular skill must be acquired. Removable they do not promote compliance. They may be made non-removable by surrounding them, for example, with a strip of resin.
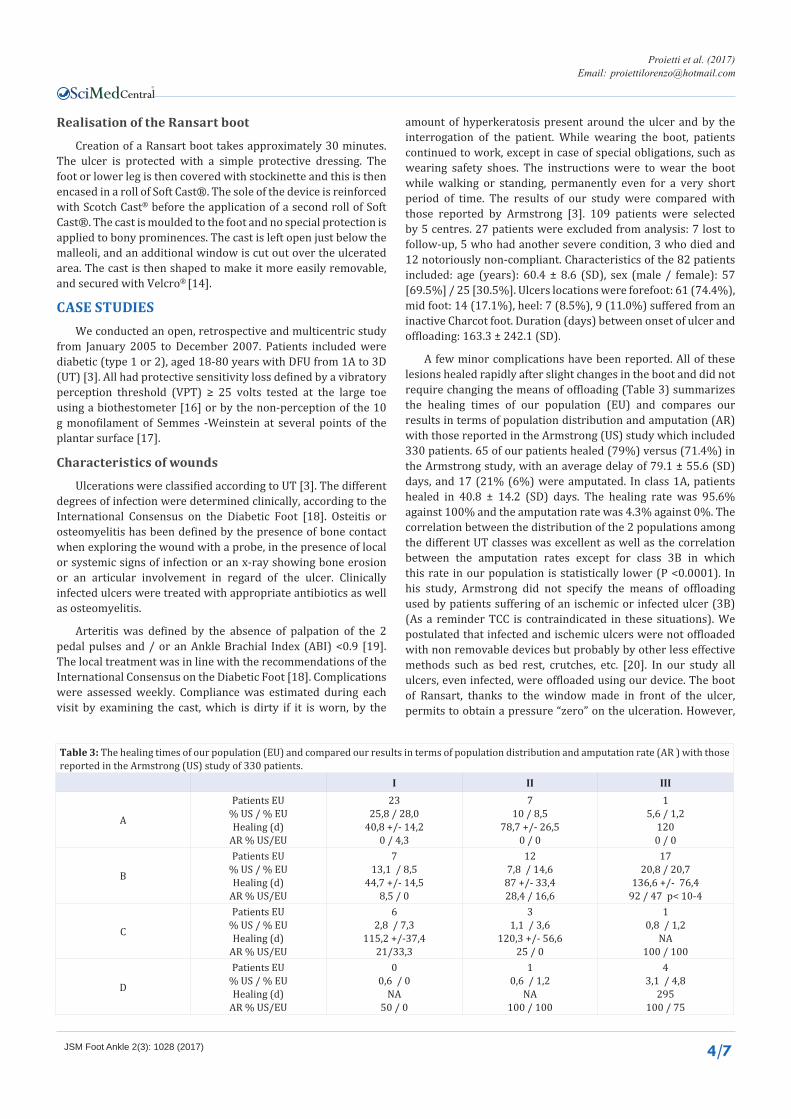
Example: The Ransart bootThis small cast is light, discreet “like a shoe”, removable,
windowed and made of mixed rigid resin (Scotch cast)® and semi- one (Soft cast)®. It is molded on the foot. Left open under the malleoli, it is easily removed and closed with Velcro®. A window is cut off opposite to the ulcer. It is worn with a cast sandal outside.Illustration 2 Half shoe.
Illustration 3 Aircast.
Illustration 4 Ransart boot.
CentralBringing Excellence in Open Access
Proietti et al. (2017)Email:
JSM Foot Ankle 2(3): 1028 (2017) 4/7
Realisation of the Ransart boot
Creation of a Ransart boot takes approximately 30 minutes.The ulcer is protected with a simple protective dressing. The foot or lower leg is then covered with stockinette and this is then encased in a roll of Soft Cast®. The sole of the device is reinforced with Scotch Cast® before the application of a second roll of Soft Cast®. The cast is moulded to the foot and no special protection is applied to bony prominences. The cast is left open just below the malleoli, and an additional window is cut out over the ulcerated area. The cast is then shaped to make it more easily removable, and secured with Velcro® [14].
CASE STUDIESWe conducted an open, retrospective and multicentric study
from January 2005 to December 2007. Patients included were diabetic (type 1 or 2), aged 18-80 years with DFU from 1A to 3D (UT) [3]. All had protective sensitivity loss defined by a vibratory perception threshold (VPT) ≥ 25 volts tested at the large toe using a biothestometer [16] or by the non-perception of the 10 g monofilament of Semmes -Weinstein at several points of the plantar surface [17].
Characteristics of wounds
Ulcerations were classified according to UT [3]. The different degrees of infection were determined clinically, according to the International Consensus on the Diabetic Foot [18]. Osteitis or osteomyelitis has been defined by the presence of bone contact when exploring the wound with a probe, in the presence of local or systemic signs of infection or an x-ray showing bone erosion or an articular involvement in regard of the ulcer. Clinically infected ulcers were treated with appropriate antibiotics as well as osteomyelitis.
Arteritis was defined by the absence of palpation of the 2 pedal pulses and / or an Ankle Brachial Index (ABI) <0.9 [19]. The local treatment was in line with the recommendations of the International Consensus on the Diabetic Foot [18]. Complications were assessed weekly. Compliance was estimated during each visit by examining the cast, which is dirty if it is worn, by the
amount of hyperkeratosis present around the ulcer and by the interrogation of the patient. While wearing the boot, patients continued to work, except in case of special obligations, such as wearing safety shoes. The instructions were to wear the boot while walking or standing, permanently even for a very short period of time. The results of our study were compared with those reported by Armstrong [3]. 109 patients were selected by 5 centres. 27 patients were excluded from analysis: 7 lost to follow-up, 5 who had another severe condition, 3 who died and 12 notoriously non-compliant. Characteristics of the 82 patients included: age (years): 60.4 ± 8.6 (SD), sex (male / female): 57 [69.5%] / 25 [30.5%]. Ulcers locations were forefoot: 61 (74.4%), mid foot: 14 (17.1%), heel: 7 (8.5%), 9 (11.0%) suffered from an inactive Charcot foot. Duration (days) between onset of ulcer and offloading: 163.3 ± 242.1 (SD).
A few minor complications have been reported. All of these lesions healed rapidly after slight changes in the boot and did not require changing the means of offloading (Table 3) summarizes the healing times of our population (EU) and compares our results in terms of population distribution and amputation (AR) with those reported in the Armstrong (US) study which included 330 patients. 65 of our patients healed (79%) versus (71.4%) in the Armstrong study, with an average delay of 79.1 ± 55.6 (SD) days, and 17 (21% (6%) were amputated. In class 1A, patients healed in 40.8 ± 14.2 (SD) days. The healing rate was 95.6% against 100% and the amputation rate was 4.3% against 0%. The correlation between the distribution of the 2 populations among the different UT classes was excellent as well as the correlation between the amputation rates except for class 3B in which this rate in our population is statistically lower (P <0.0001). In his study, Armstrong did not specify the means of offloading used by patients suffering of an ischemic or infected ulcer (3B) (As a reminder TCC is contraindicated in these situations). We postulated that infected and ischemic ulcers were not offloaded with non removable devices but probably by other less effective methods such as bed rest, crutches, etc. [20]. In our study all ulcers, even infected, were offloaded using our device. The boot of Ransart, thanks to the window made in front of the ulcer, permits to obtain a pressure “zero” on the ulceration. However,
Table 3: The healing times of our population (EU) and compared our results in terms of population distribution and amputation rate (AR ) with those reported in the Armstrong (US) study of 330 patients.
I II III
A
Patients EU% US / % EUHealing (d)
AR % US/EU
2325,8 / 28,0
40,8 +/- 14,20 / 4,3
710 / 8,5
78,7 +/- 26,50 / 0
15,6 / 1,2
1200 / 0
B
Patients EU% US / % EUHealing (d)
AR % US/EU
713,1 / 8,5
44,7 +/- 14,58,5 / 0
127,8 / 14,6
87 +/- 33,428,4 / 16,6
1720,8 / 20,7
136,6 +/- 76,492 / 47 p< 10-4
C
Patients EU% US / % EUHealing (d)
AR % US/EU
62,8 / 7,3
115,2 +/-37,421/33,3
31,1 / 3,6
120,3 +/- 56,625 / 0
10,8 / 1,2
NA100 / 100
D
Patients EU% US / % EUHealing (d)
AR % US/EU
00,6 / 0
NA50 / 0
10,6 / 1,2
NA100 / 100
43,1 / 4,8
295100 / 75
CentralBringing Excellence in Open Access
Proietti et al. (2017)Email:
JSM Foot Ankle 2(3): 1028 (2017) 5/7
any pressure exerted on a wound increases the risk of developing or aggravating an infection [21]. It is probable that the absence of any pressure minimized the development or aggravation of infection and therefore favoures healing and decrease the amputation rate, which would explain our advantage in terms of AR for Class 3B ulcers.
The wandering activity in this study does not alter the healing time. Indeed, the healing time of class 1A ulcers treated by our device, a situation where the ambulation remains quasi-normal, are equivalent to those obtained with the TCC, in which the usual ambulation activity is reduced by 60% [22]. The rate of patients completely adhering to the offloading may vary from 10% when the apparatus is removable to 98% when it is irremovable [23]. We report a compliance rate of 11%. This surprisingly high rate of “non-forced” compliance is probably related to the characteristics of our device, small, light, discreet, windowed, removable and allowing the pursuit of everyday activities. This model has been created by following the feedback of users. The Ransart boot is an offloading technique that seems effective and safe for all types of ulcers, even infected and / or ischemic ones, as well as for non-active Charcot foot ulcers and could be even more effective for class 3B if we compare our results with those published by Armstrong.
The second study was a proof-of-concept study. This observational study of the Ransart boot in the treatment of diabetic foot ulcers was carried out in 7 centres. They included class 1A to 3D ulcers (UT). The methodology applied was the same as in the previous study, diagnosis, treatment, use of the Ransart boot ... 135 patients were included in 7 participating centres. 20 were excluded from the analysis (14 erroneously recruited and 6 who underwent surgery other than amputation during the study). Population demographics and characteristics of inclusion ulcers: mean age 60.3 ± 11.4 years (range 23-85), median duration of diabetes 15.2 ± 0.6 years (range 0-42). 118 (87.4%) patients had Type 2 diabetes. 96 (71.1%) were men. The glycosylated hemoglobin (HbA1c) was 7.7 ± 1.8%. The mean duration of ulcer at baseline was 90 [interquartile range (IQR) 30-1825] days. 97 ulcers were on the forefoot, 20 on the mid-foot
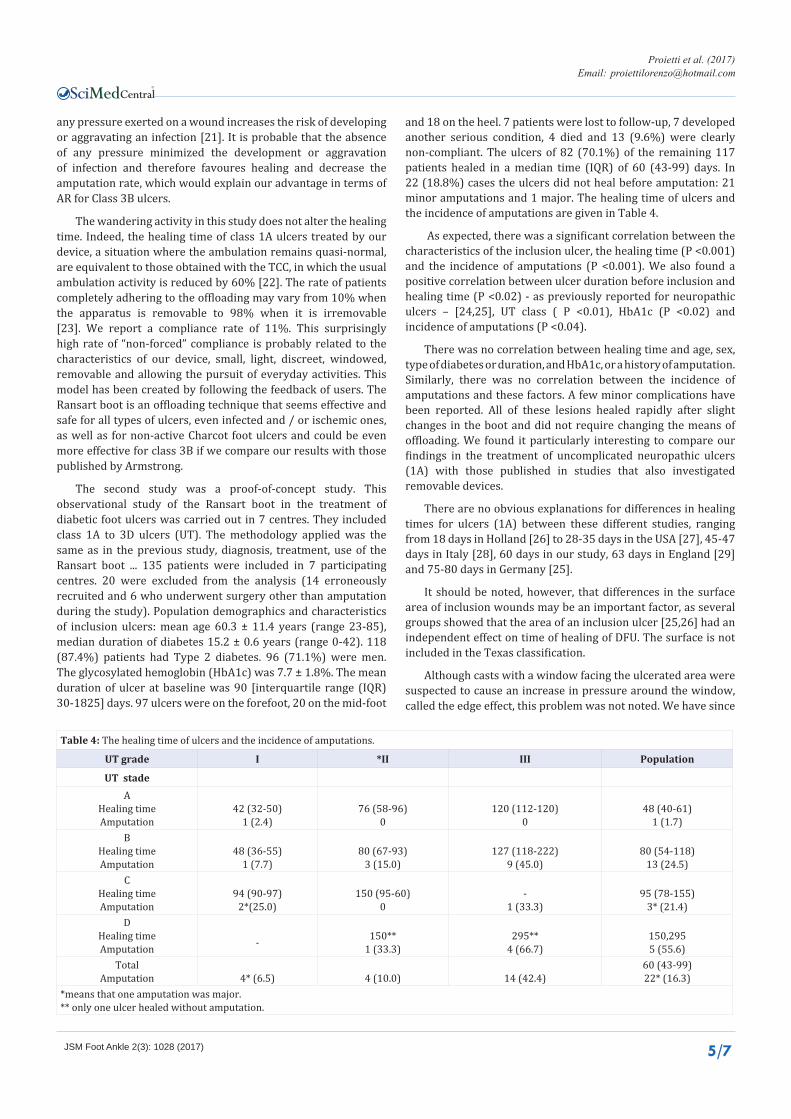
and 18 on the heel. 7 patients were lost to follow-up, 7 developed another serious condition, 4 died and 13 (9.6%) were clearly non-compliant. The ulcers of 82 (70.1%) of the remaining 117 patients healed in a median time (IQR) of 60 (43-99) days. In 22 (18.8%) cases the ulcers did not heal before amputation: 21 minor amputations and 1 major. The healing time of ulcers and the incidence of amputations are given in Table 4.
As expected, there was a significant correlation between the characteristics of the inclusion ulcer, the healing time (P <0.001) and the incidence of amputations (P <0.001). We also found a positive correlation between ulcer duration before inclusion and healing time (P <0.02) - as previously reported for neuropathic ulcers – [24,25], UT class ( P <0.01), HbA1c (P <0.02) and incidence of amputations (P <0.04).
There was no correlation between healing time and age, sex, type of diabetes or duration, and HbA1c, or a history of amputation. Similarly, there was no correlation between the incidence of amputations and these factors. A few minor complications have been reported. All of these lesions healed rapidly after slight changes in the boot and did not require changing the means of offloading. We found it particularly interesting to compare our findings in the treatment of uncomplicated neuropathic ulcers (1A) with those published in studies that also investigated removable devices.
There are no obvious explanations for differences in healing times for ulcers (1A) between these different studies, ranging from 18 days in Holland [26] to 28-35 days in the USA [27], 45-47 days in Italy [28], 60 days in our study, 63 days in England [29] and 75-80 days in Germany [25].
It should be noted, however, that differences in the surface area of inclusion wounds may be an important factor, as several groups showed that the area of an inclusion ulcer [25,26] had an independent effect on time of healing of DFU. The surface is not included in the Texas classification.
Although casts with a window facing the ulcerated area were suspected to cause an increase in pressure around the window, called the edge effect, this problem was not noted. We have since
Table 4: The healing time of ulcers and the incidence of amputations.
UT grade I *II III Population
UT stadeA
Healing timeAmputation
42 (32-50)1 (2.4)
76 (58-96)0
120 (112-120)0
48 (40-61)1 (1.7)
BHealing timeAmputation
48 (36-55)1 (7.7)
80 (67-93)3 (15.0)
127 (118-222)9 (45.0)
80 (54-118)13 (24.5)
CHealing timeAmputation
94 (90-97)2*(25.0)
150 (95-60)0
-1 (33.3)
95 (78-155)3* (21.4)
DHealing timeAmputation - 150**
1 (33.3)295**
4 (66.7)150,2955 (55.6)
TotalAmputation 4* (6.5) 4 (10.0) 14 (42.4)
60 (43-99)22* (16.3)
*means that one amputation was major.** only one ulcer healed without amputation.
CentralBringing Excellence in Open Access
Proietti et al. (2017)Email:
JSM Foot Ankle 2(3): 1028 (2017) 6/7
demonstrated in a study the non-existence of this supposed edge effect [30]. As observed in the first study, we again have a surprisingly high rate of “non-forced” compliance. The purpose of this paper is to summarize our experience about the efficacy and the safety of this boot, based on our practice reported in 2 studies.
CONCLUSIONThe healing time and incidence of amputations were
comparable to those reported for non-removable devices. This suggests that a removable and user-friendly offloading device - which probably increases compliance - could be as effective as a non-removable and restrictive device. Non-compliance may be less related to being removable than to other features of the device itself. Walking, if the ulcer is at rest, does not slow the healing time. The effectiveness, cost and acceptability of removable devices, such as Ransart, should be compared to non removable devices in a randomized study.
Post-op or temporary or dressing shoes
Many different models and appellations exist: post-op shoes, dressing shoes, extra wide shoes ... ..It is difficult to compare looking at the literature because the appellations differ from one country to another. Very few serious studies have been carried out and the few results obtained with respect to the healing time are poor.
Shoes and insoles
Even the most optimistic studies of shoes as a means of offloading suggest that only 1/2 of uninfected, non-ischemic, superficial ulcers class 1A UT will heal at 12 weeks [31]. We can therefore affirm that the true value of therapeutic shoes and insoles lies in the prevention of ulcers and not in their treatment.
The gold standard is TCC: short healing time, forced compliance and decreased patient activity. But is forced compliance and decreased activity so attractive for the patient? Compliance
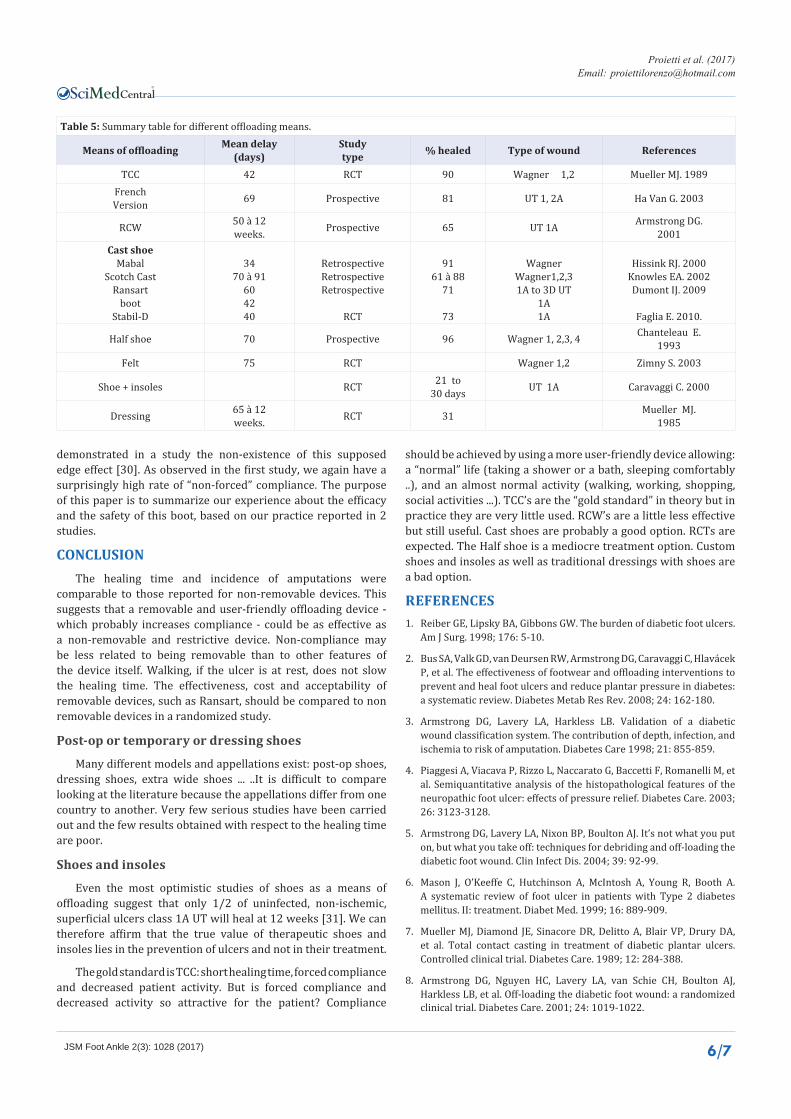
Table 5: Summary table for different offloading means.
Means of offloading Mean delay(days)
Studytype % healed Type of wound References
TCC 42 RCT 90 Wagner 1,2 Mueller MJ. 1989FrenchVersion 69 Prospective 81 UT 1, 2A Ha Van G. 2003
RCW 50 à 12weeks. Prospective 65 UT 1A Armstrong DG.
2001Cast shoe
MabalScotch Cast
Ransartboot
Stabil-D
3470 à 91
604240
RetrospectiveRetrospectiveRetrospective
RCT
9161 à 88
71
73
WagnerWagner1,2,31A to 3D UT
1A1A
Hissink RJ. 2000Knowles EA. 2002Dumont IJ. 2009
Faglia E. 2010.
Half shoe 70 Prospective 96 Wagner 1, 2,3, 4 Chanteleau E.1993
Felt 75 RCT Wagner 1,2 Zimny S. 2003
Shoe + insoles RCT 21 to30 days UT 1A Caravaggi C. 2000
Dressing 65 à 12weeks. RCT 31 Mueller MJ.
1985
should be achieved by using a more user-friendly device allowing: a “normal” life (taking a shower or a bath, sleeping comfortably ..), and an almost normal activity (walking, working, shopping, social activities ...). TCC’s are the “gold standard” in theory but in practice they are very little used. RCW’s are a little less effective but still useful. Cast shoes are probably a good option. RCTs are expected. The Half shoe is a mediocre treatment option. Custom shoes and insoles as well as traditional dressings with shoes are a bad option.
REFERENCES1. Reiber GE, Lipsky BA, Gibbons GW. The burden of diabetic foot ulcers.
Am J Surg. 1998; 176: 5-10.
2. Bus SA, Valk GD, van Deursen RW, Armstrong DG, Caravaggi C, Hlavácek P, et al. The effectiveness of footwear and offloading interventions to prevent and heal foot ulcers and reduce plantar pressure in diabetes: a systematic review. Diabetes Metab Res Rev. 2008; 24: 162-180.
3. Armstrong DG, Lavery LA, Harkless LB. Validation of a diabetic wound classification system. The contribution of depth, infection, and ischemia to risk of amputation. Diabetes Care 1998; 21: 855-859.
4. Piaggesi A, Viacava P, Rizzo L, Naccarato G, Baccetti F, Romanelli M, et al. Semiquantitative analysis of the histopathological features of the neuropathic foot ulcer: effects of pressure relief. Diabetes Care. 2003; 26: 3123-3128.
5. Armstrong DG, Lavery LA, Nixon BP, Boulton AJ. It’s not what you put on, but what you take off: techniques for debriding and off-loading the diabetic foot wound. Clin Infect Dis. 2004; 39: 92-99.
6. Mason J, O’Keeffe C, Hutchinson A, McIntosh A, Young R, Booth A. A systematic review of foot ulcer in patients with Type 2 diabetes mellitus. II: treatment. Diabet Med. 1999; 16: 889-909.
7. Mueller MJ, Diamond JE, Sinacore DR, Delitto A, Blair VP, Drury DA, et al. Total contact casting in treatment of diabetic plantar ulcers. Controlled clinical trial. Diabetes Care. 1989; 12: 284-388.
8. Armstrong DG, Nguyen HC, Lavery LA, van Schie CH, Boulton AJ, Harkless LB, et al. Off-loading the diabetic foot wound: a randomized clinical trial. Diabetes Care. 2001; 24: 1019-1022.
CentralBringing Excellence in Open Access
Proietti et al. (2017)Email:
JSM Foot Ankle 2(3): 1028 (2017) 7/7
Dumont I (2017) Offloading: How and Why? The Ransart boot. JSM Foot Ankle 2(3): 1028.
Cite this article
9. Shaw JE, Hsi WL, Ulbrecht JS, Norkitis A, Becker MB, Cavanagh PR, et al. The mechanism of plantar unloading in total contact casts: implications for design and clinical use. Foot Ankle Int. 1997; 18: 809-817.
10. Sinacore DR, Mueller MJ, Diamond JE, Blair VP, Drury D, Rose SJ, et al. Diabetic plantar ulcers treated by total contact casting. A clinical report.. Phys Ther. 1987; 67: 1543-1547.
11. Wu SC, Jensen JL, Weber AK, Robinson DE, Armstrong DG. Use of pressure offloading devices in diabetic foot ulcers: do we practice what we preach? Diabetes Care. 2008; 31: 2118-2119.
12. Fleischli JG, Lavery LA, Vela SA, Ashry H, Lavery DC. 1997 William J. Stickel Bronze Award. Comparison of strategies for reducing pressure at the site of neuropathic ulcers. J Am Podiatr Med Assoc. 1997; 87: 466-472.
13. Knowles A, Armstrong DG, Hayat SA, Khawaja KI, Malik RA, Boulton AJ. Offloading diabetic foot wounds using the Scotchcast boot: a retrospective study. Ostomy Wound Manage. 2002; 48: 50-53.
14. Dumont IJ, Lepeut MS, Tsirtsikolou DM, Popielarz SM, Cordonnier MM, Fayard AJ, et al. A proof-of-concept study of the effectiveness of a removable device for offloading in patients with neuropathic ulceration of the foot: the Ransart boot. Diabet Med. 2009; 26: 778-782.
15. Faglia E, Caravaggi C, Clerici G, Sganzaroli A, Curci V, Vailati W, et al. Effectiveness of removable walker cast versus nonremovable fiberglass off-bearing cast in the healing of diabetic plantar foot ulcer: a randomized controlled trial. Diabetes Care. 2010; 33: 1419-1423.
16. Miranda-Palma B, SosenkoJM, Bowker JH, Mizel MS, BoultonAJ. A comparison of the monofilament with other testing modalities for foot ulcer susceptibility. Diabetes Res Clin Pract. 2005; 70: 8-12.
17. Kumar S, Fernando DJ, Veves A, Knowles EA, Young MJ, Boulton AJ, et al. Semmes-Weinstein monofilaments: a simple, effective and inexpensive screening device for identifying diabetic patients at risk of foot ulceration. Diabetes Res Clin Pract. 1991; 13: 63-67.
18. International Working Group on the Diabetic Foot. International consensus on the diabetic foot [CDROM]. Brussels: Interna tional Diabetes Foundation, 2003.
19. National Agency for Accreditation and Evaluation in Sant. Doppler ultrasonography in obliterative arthritis of the lower limbs. Journal des maladies vasculaires. 2003; 28: 36-41.
20. Richard JL, Ha Van G, Dumont I. The discharge of chronic wounds from
the diabetic foot: why and how? J Plaies Cicatrisations. 2008; 66: 14-19.
21. Mueller MJ, Diamond JE, Sinacore DR, Delitto A, Blair VP, Drury DA, et al. Total contact casting in treatment of diabetic plantar ulcers. Controlled clinical trial. Diabetes Care. 1989; 12: 384-388.
22. Armstrong DG, Lavery LA, Kimbriel HR, Nixon BP, Boulton AJ. Activity patterns of patients with diabetic foot ulceration: patients with active ulceration may not adhere to a standard pressure off-loading regimen. Diabetes Care. 2003; 26: 2595-2597.
23. Ha Van G, Siney H, Hartmann-Heurtier A, Jacqueminet S, Greau F, Grimaldi A, et al. Nonremovable, windowed, fiberglass cast boot in the treatment of diabetic plantar ulcers: efficacy, safety, and compliance. Diabetes Care. 2003; 26: 2848-2852.
24. Ince P, Game FL, Jeffcoate WJ. Rate of healing of neuropathic ulcers of the foot in diabetes and its relationship to ulcer duration and ulcer area. Diabetes Care. 2007; 30: 660-663.
25. Margolis DJ, Allen-Taylor L, Hoffstad O, Berlin JA. Diabetic neuropathic foot ulcers: the association of wound size, wound duration, and wound grade on healing. Diabetes Care. 2002; 25: 1835-1839.
26. Nabuurs-Franssen MH, Huijberts MS, Sleegers R, Schaper NC. Casting of recurrent diabetic foot ulcers: effective and safe? Diabetes Care. 2005; 28: 1493-1494.
27. Katz IA, Harlan A, Miranda-Palma B, Prieto-Sanchez L, Armstrong DG, Bowker JH , et al. A randomized trial of two irremovable off-loading devices in the management of plantar neuropathic diabetic foot ulcers. Diabetes Care. 2005; 28: 555-559.
28. Piaggesi A, Macchiarini S, Rizzo L, Palumbo F, Tedeschi A, Nobili LA, et al. An off-the-shelf instant contact casting device for the management of diabetic foot ulcers: a randomized prospective trial versus traditional fiberglass cast. Diabetes Care. 2007; 30: 586-590.
29. Ince P, Kendrick D, Game F, Jeffcoate W. The association between baseline characteristics and the outcome of foot lesions in a UK population with diabetes. Diabet Med. 2007; 24: 977-981.
30. Dumont I. Do windows in removable casts increase local pressure? The Diabetic Foot Journal. 2013; 1: 24-28.
31. Caravaggi C, Faglia E, De Giglio R, Mantero M, Quarantiello A, Sommariva E, et al. Effectiveness and safety of a non removable fiberglass off-bearing cast versus a therapeutic shoe in the treatment of neuropathic foot ulcers: a randomized study. Diabetes Care. 2000; 23:1746-1751.