“off-pump” (“beating-heart”) coronary...
TRANSCRIPT

Page 1 of 41
“OFF-PUMP” (“BEATING-HEART”)CORONARY ARTERY BYPASS SURGERY
ISSUE
Blue Shield has received requests for coverage of off-pump coronary arterybypass surgery in the treatment of coronary artery disease. The Medical PolicyCommittee on Quality and Technology is asked to review the published dataregarding the efficacy and safety of this new technology in clinical practice.
CURRENT BLUE SHIELD POLICY
Current Blue Shield policy (2/25/98) states that, “Post-access coronary arterybypass (PACAB/Port CAB) is investigational and not eligible for coverage.Minimally invasive direct coronary artery bypass (MID CAB) isinvestigational and not eligible for coverage.” There is currently no policy on“off-pump” coronary artery bypass (OPCAB) surgery.
BACKGROUND
Coronary artery disease, which affects 1.5 million Americans and causesapproximately 500,000 deaths every year, is a result of atherosclerosis.Annually, more than 1 million coronary angiograms and more than 600,000coronary artery bypass graft operations are performed in the U.S.
Conventional coronary artery bypass grafting (CCABG) is a routine and safeprocedure with a mortality of 2-3% in elective cases (Ascione et al, 1999c).CCABG with cardiopulmonary bypass (CPB) is a safe, time-honoredprocedure yielding excellent and highly reproducible results in surgicalcoronary revascularization (Baumgartner et al, 2000).
Although “off-pump” (“beating heart”) coronary artery bypass (OPCAB)surgery may seem to be a new procedure, in fact, some of the earliest attemptsat surgical myocardial revascularization were performed without use ofcardioplegia and CPB pumps. Sabiston’s original saphenous veinaortocoronary bypass was performed in this manner (Sabiston, 1974), as wasKolessov’s early use of the left internal mammary artery bypass to the leftanterior descending coronary artery (Kolessov, 1967). But, with the advent ofcardiopulmonary bypass and cardioplegic arrest, “off-pump” coronary arterybypass (OPCAB) surgery through a full sternotomy was abandoned (Arom etal, 2000).

Page 2 of 41
BACKGROUND, continued
The development of cardioplegia and cardiopulmonary bypass pumps enabledfull access to the coronary arteries and allowed CABG surgery to be performedin a quiescent, bloodless field (Koutlas et al, 2000; Kshettry et al, 2000).
Benetti (1985) and Buffolo and colleagues (1985) in the mid-1980s began therevival of OPCAB. Initially, the desire to reduce morbidity and mortalityassociated with CPB resulted in renewed interest in OPCAB procedures(Hernandez et al, 2000). For example, CPB can cause physiologicalderangements such as activation of the systemic inflammatory response anddetrimental effects on hemostasis (Lancey et al, 2000). Subsequently, withintroduction and improvements in retractor-stabilizer systems and techniquesthat enable exposure of all surfaces of the heart, it became technically possibleto perform multi-vessel coronary artery bypass grafting on the beating heart(Arom et al, 2000).
Off-Pump Coronary Artery Bypass
Off pump coronary artery bypass operations are carried out through a standardmedian sternotomy incision (Gundry et al, 1998) or sometimes a leftposterolateral thoracotomy (Baumgartner et al, 2000). Thus, OPCAB surgerymust be differentiated from so-called minimally invasive coronary arterybypass (MIDCAB) surgery, in which the surgeon is operating through a“keyhole” or “port.”
In OPCAB, surgeons use stabilizers to steady the heart and intracoronaryshunts to permit continued myocardial perfusion during construction of thedistal anastomoses (Yeatman et al, 2001). Stabilization of the target arteries isaccomplished with stabilizing retractors such as the CTS tissue stabilizer(Guidant Cardiac Surgery, Cupertino CA), Octopus Tissue StabilizationSystem (Medtronic Inc., Minneapolis, MN), and the Cohn Stabilizer (GenzymeCorp, Cambridge, MA) (Arom et al, 2000; Koutlas et al, 2000).
OPCAB is a more demanding procedure than CCABG. Constant heart motion,hemodynamic derangements during manipulation and elevation of the heart,regional ischemia, bleeding, and difficulties with access to the coronaries,especially to the left circumflex coronary artery, remain concerns (Arom et al,2000; Kshettry et al, 2000; Rama et al, 2001). Despite local tissue stabilizationand induced bradycardia, the heart’s natural motion and the potential forhemodynamic compromise during elevation of the heart raise concernregarding the quality of anastomoses.

Page 3 of 41
Off-Pump Coronary Artery Bypass, continued
To achieve technically adequate anastomoses requires more attention to detail(Kshettry et al, 2000). The quality of anastomoses can be assessed at the timeof operation by utilizing transonic flow meters (Arom et al, 2000) or post-operatively by coronary angiography (Bull et al, 2001).
Potential advantages of OPCAB include: decreased operative mortality,reduced peri-operative morbidity, decreased incidence of myocardialinfarction, shorter hospital stays, and hastened recovery times (Gundry et al,1998; Arom et al, 2000; Kshettry et al, 2000). The avoidance of aortic cross-clamping might minimize the risk of global myocardial ischemia, myocardialstunning, and potential neurological complications.
Potential disadvantages of OPCAB include: operating on a moving field,potentially resulting in inferior quality of anastomoses; problems accessing allareas of the heart, potentially limiting the number of vessels that can bebypassed resulting in fewer bypass grafts per patient and incompleterevascularization; and uncertainty regarding long-term functional results (long-term graft patency, recurrence of angina, and need for repeat interventions)(Jegaden et al, 2001).
TECHNOLOGY ASSESSMENT (TA)
TA Criterion 1
The Octopus Tissue Stabilization System (Medtronic Inc., Minneapolis, MN);Genzyme-OPCAB Stabilization System (Genzyme Surgical Products,Cambridge, MA); and the CTS Retractor and Stabilizer (Guidant CardiacSurgery, Cupertino, CA) received device class 1 exemption per Sec. 870.4500:Cardiovascular surgical instruments which states (a) Cardiovascular surgicalinstruments are surgical instruments that have special features for use incardiovascular surgery. These devices include, e.g., forceps, retractors, andscissors and (b) Classification. Class I. The devices are exempt from thepremarket notification procedures in subpart E of part 807 or this chapter. TACriterion 1 is met.
TA Criterion 2
The main inclusion criterion for OPCAB procedures is the same as forCCABG: symptomatic, bypassable coronary artery disease. Exclusion criteriafor OPCAB procedures include small or diffusely diseased target vessels.Patients with hemodynamic instability, massive cardiomegaly, or small,intramyocardial, or heavily calcified coronary arteries are considered poorcandidates for OPCAB (Baumgartner et al, 2000).

Page 4 of 41
TA Criterion 2, continued
Location of target vessels has become less of an obstacle to OPCAB. Initialstudies included fewer patients with circumflex coronary artery lesions becauseaccess to such lesions was more difficult, but presently exposure is usuallysufficient, except for obtuse marginal branches that require grafting close to theatrioventricular groove. Some surgeons consider morbid obesity a relativecontraindication to OPCAB (Koutlas et al, 2000). Other exclusion criteria inthe various trials include: ejection fractions of <30, recent (<1 month)myocardial infarction, severe renal and pulmonary disease, diabetes mellitus,previous stroke or TIA, and coagulopathy (Ascione et al, 1999b; Ascione et al,1999c).
Outcomes assessed in the various clinical trials summarized below include:(1) Intraoperative factors, such as number of arteries bypassed,
procedure time, and blood loss;(2) Immediate postoperative factors, such as blood loss, transfusion
requirement, duration of ventilatory support, length of ICU stay,length of hospitalization, reoperations for bleeding or graftocclusion; morbidity, including peri-operative myocardialinfarction, TIA or stroke, renal failure, and atrial fibrillation;and mortality;
and(3) Long-term follow-up factors, such as frequency and intensity of
recurrent angina, need for repeat cardiac interventions such asPTCA or CABG, and long-term mortality (Kshettry et al, 2000).
Published studies have included: uncontrolled clinical series of patientsundergoing OPCAB; non-randomized retrospective and prospectivecomparisons between OPCAB and CCABG; and prospective randomizedcomparisons of OPCAB and CCABG.
In most of the non-randomized comparisons, the selection of “off-pump”versus “on-pump” approach was the surgeon’s decision, and most oftendepended on patient factors, such as location and adequacy of target vessels aswell as co-morbid illnesses present (Koutlas et al, 2000; Kshettry et al, 2000).In such nonrandomized trials, there is always the possibility of selection bias.In many of the published studies, the preoperative coronary angiogram playedan important role in patient selection: patients requiring 4 or more grafts weremore likely to undergo CABG with CPB.

Page 5 of 41
TA Criterion 2, continued
For example, in one study, 90% of CCABG patients had circumflex graftsplaced, while only 70% of OPCAB patients had circumflex grafts (Bull et al,2001). This makes direct comparison of results of the two procedures difficult.
Other limitations of published trials include data limitations imposed byretrospective analyses, and the inability to conduct a reliable multivariateanalysis of predictor variables of early mortality because of the small numberof deceased patients. The short period of clinical follow-up in most trials isanother limitation, along with the absence of angiographic follow-up thatwould enable a comparison of the early and late graft patency between the twogroups. Further, the number of patients in the two groups is often too small toallow a valid statistical comparison between the OPCAB and CCABG groups(Stamou et al, 2000).
Published studies regarding OPCAB have varied in whether they excludedpatients undergoing emergency or reoperative (“redo”) CABG procedures orconcomitant valve surgery (Koutlas et al, 2000). Some trials exclude patientsrequiring grafts to the distal circumflex (Ascione et al, 1999a) or two or moregrafts per patient (Stamou et al, 2000). Others have included patientsundergoing other “beating heart” procedures, such as MIDCAB (minimallyinvasive coronary artery bypass) procedures (Stamou et al, 2000; Hirose et al,2000) with or without PTCA (Koutlas et al, 2000). Some have involvedhistorical comparison groups (Puskas et al, 1998; Lancey et al, 2000;Hernandez et al, 2000). Studies have also varied in whether the surgeonsattempt to achieve full revascularization. Each of these factors leads tocomparison of disparate patient groups. For example, conventional reoperative(“redo”) CABG has been associated with a relatively high early mortality rate(3.4% to 12.5%) compared with first-time CABG (Stamou et al, 2000).
Many of the published series have small numbers (< 100) of patients. Withsuch small numbers, data regarding safety may be unreliable, especially forinfrequent complications. With a low incidence of complications in bothgroups, power analysis would indicate the necessity of a large study group todemonstrate differences between the two groups. Because the rates of manycomplications are very low (in the range of 1% to 5%), a sample size of morethan 1000 patients would be needed to show a significant difference betweengroups (Bull et al, 2001).

Page 6 of 41
TA Criterion 2, continued
Therefore, the best available evidence derives from the randomizedcomparative trials. To date, five groups of investigators have publishedrandomized comparisons of OPCAB and CCABG. Ascione and colleagues(1999a; 1999b; 1999c; 2000; 2001) have published 5 manuscripts, all derivingfrom one randomized trial in which 100 patients from the Bristol HeartInstitute were randomized to OPCAB and 100 to CCABG, but each reportingon one or more different outcomes. Covino and colleagues (2001) havepublished one manuscript from a randomized trial in which 21 patients withsevere lung disease were randomized to OPCAB and 16 to CCABG. Guler andcolleagues (2001) also randomized patients with severe COPD to OPCAB(n=19) or CCABG (n=18 patients). Czerny and colleagues (2001) randomizedelective low-risk patients with multivessel disease to OPCAB with CCABG.van Dijk et al (2001) have published preliminary (1 month) results fromrandomized trial in which 142 patients were randomized to OPCAB and 139 toCCABG.
Given the large number of non-randomized and randomized comparative trials,TA Criterion 2 is met.
Level of Evidence: 1, 3, 4, 5
TA Criterion 3
Uncontrolled Series
Many uncontrolled series of OPCAB have been published (Buffolo et al, 1996;Moshkovitz et al, 1997; Jansen et al, 1998; Spooner et al, 1998; Tasdemir et al,1998; Hart et al, 1999; Turner et al, 1999; Hernandez et al, 2000; Rama et al,2001; Al-Ruzzeh et al 2001; Dewey et al, 2001; Lima et al, 2001; Zehr et al,2001). Because these series do not compare OPCAB to CCABG, they do notallow us to determine whether OPCAB outcomes are equal to or better thanthose achieved with CCABG while subjecting the patients to risks that are thesame or less than the risks of patients undergoing CCABG (Hernandez et al,2000). Consequently, the individual uncontrolled case series will not beconsidered further here.

Page 7 of 41
Meta-Analysis
Stanbridge et al (1999) reported a meta-analysis of 3060 off-pump sternotomyprocedures performed in 21 centers. The operative and postoperative mortalityrate was 2.2%. Complications included myocardial infarctions in 1.45% andatrial fibrillation in 9%. In the total series, 5% of patients undergoing OPCABrequired conversion to CCABG with CPB. The graft occlusion and stenosisrates were 4.9% and 1.4%, respectively.
Nonrandomized Comparative Trials
Tables 1, 2 and 3 display intraoperative, immediate postoperative and long-term follow-up results of non-randomized studies comparing OPCAB versusCCABG operation.
In 15/20 of the nonrandomized comparative trials, the number of grafts perpatient were significantly fewer in the OPCAB than in the CCABG patients.This clearly indicates some pre-selection among those undergoing OPCAB forpatients with fewer diseased vessels.
a. Operative outcomes
Table 1 presents the operative outcomes in 22 non-randomized comparativestudies of OPCAB and CCABG. Operative mortality was significantly lowerafter OPCAB in 2/17 studies and not significantly different than after CCABGin the remaining 15/17 studies. Operation duration was shorter after OPCAB in8/9 studies and not significantly different in the remaining 1/9 studies.Reoperations for bleeding were less common after OPCAB in 1/13 studies andnot significantly different in the remaining 12/13 studies. Reoperations forgraft occlusion were less common after OPCAB in 1/3 studies and notsignificantly different in the remaining 2/3 studies. Duration of intubation wassignificantly less after OPCAB in 9/12 studies and not significantly different inthe remaining 3/12 studies. Length of stay in the ICU was less after OPCAB in7/14 studies and not significantly different in the remaining 7/14 studies. Post-operative hospital length of stay was less after OPCAB in 10/16 studies and notsignificantly different in the remaining 6/16 studies. Thus, in all of the non-randomized comparative studies, OPCAB produced similar or better operativeresults to CCABG.

Page 8 of 41
Nonrandomized Comparative Trials, continued
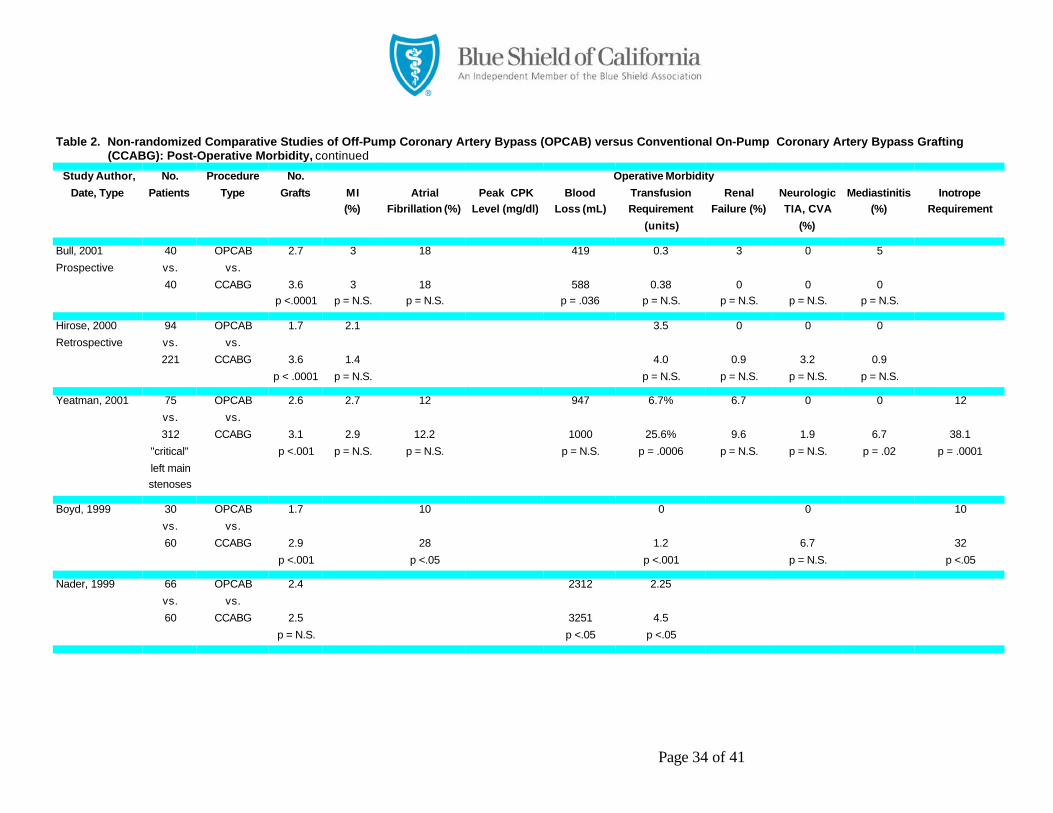
b. Post-operative morbidity outcomes
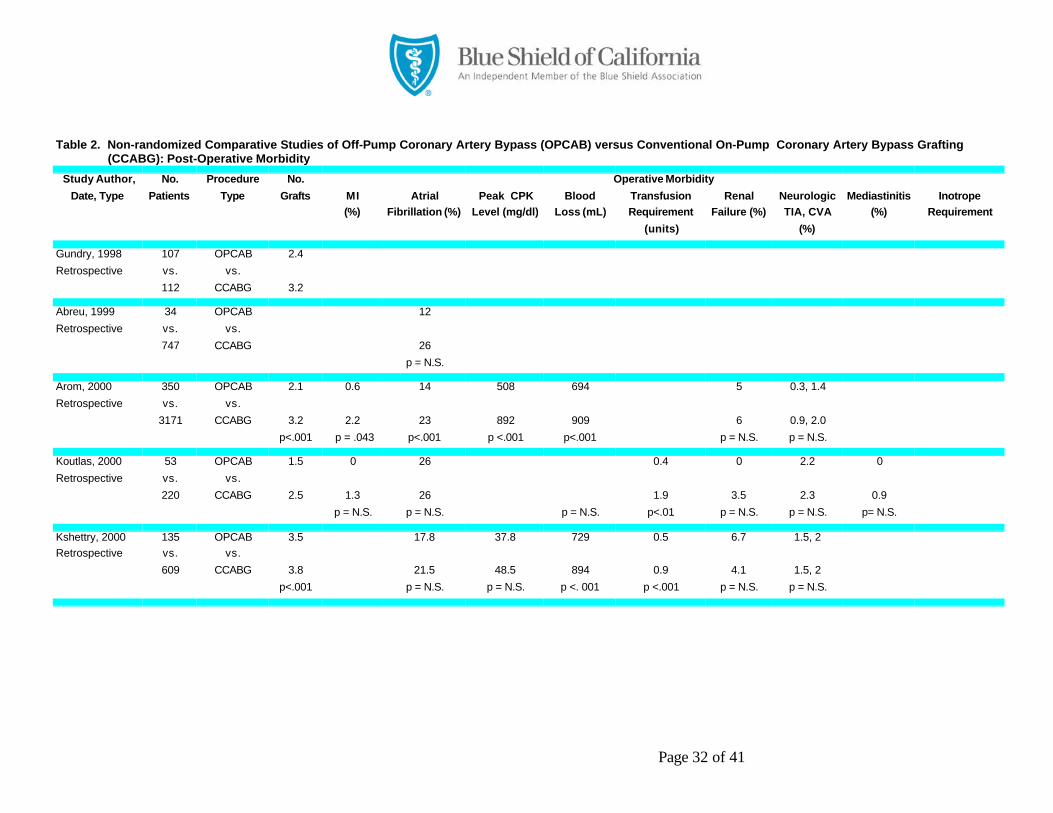
Table 2 presents the post-operative morbidity outcomes in 21 non-randomizedcomparative studies of OPCAB and CCABG. Myocardial infarctions were lesscommon after OPCAB in 2/14 studies and not significantly different in theremaining 12/14 studies. Atrial fibrillation occurred less commonly afterOPCAB in 4/13 studies and not significantly different in the remaining 9/13studies. Peak CPK levels were less after OPCAB in ¾ studies and notsignificantly different in the remaining 1/4 studies. Blood loss was less afterOPCAB in 6/9 studies and not significantly different in the remaining 3/9studies. Transfusion was required less often in 12/16 studies and was notsignificantly different in the remaining 4/16 studies. Renal failure occurredless often in 1/13 studies and was not significantly different in the remaining12/13 studies. Neurological complications of transient ischemic attack orstroke occurred less often in 2/15 studies and were not significantly different inthe remaining 13/15 studies. Mediastinitis occurred less often in 1/8 studiesand not significantly different in the remaining 7/8 studies. Inotropic supportwas required less often in 3/6 studies and was not significantly different in theremaining 3/6 studies. Thus, in all of the non-randomized comparative studies,OPCAB produced similar or better post-operative morbidity results toCCABG.
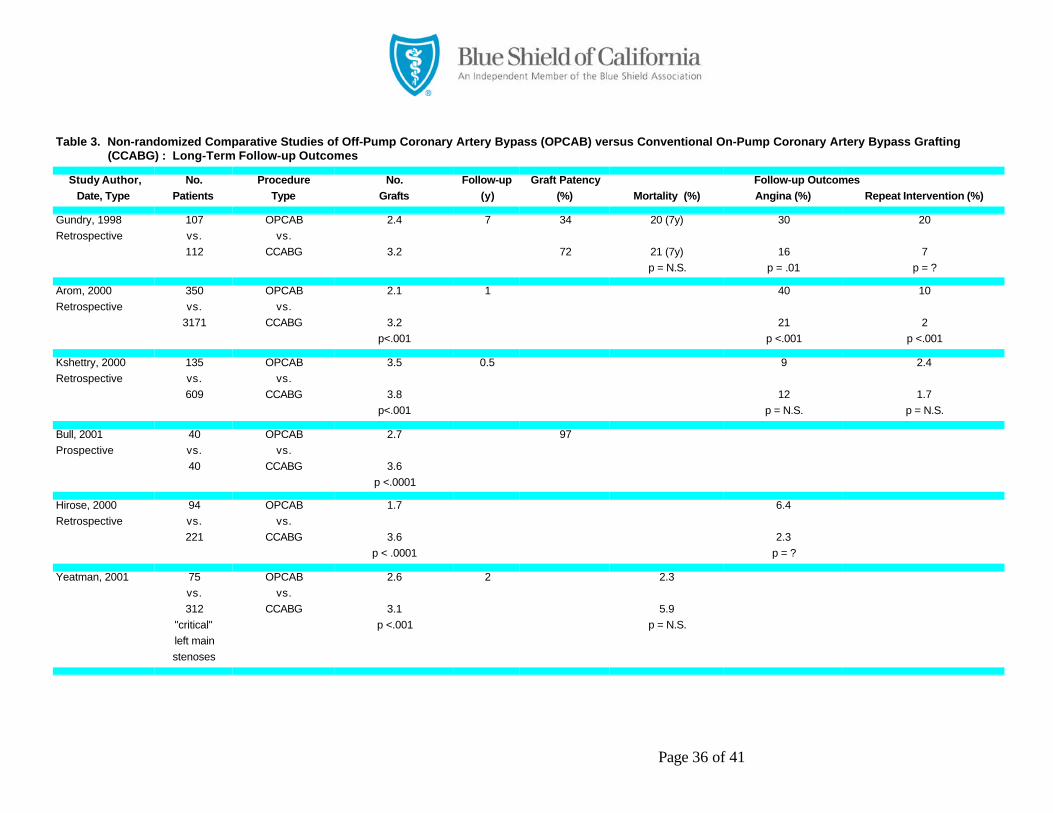
c. Long-term follow-up outcomes
Table 3 summarizes four long-term follow-up outcomes in 10 non-randomizedcomparative studies of OPCAB and CCABG.
(1) Graft patency: With the exception of the early study by Gundry et al (1998)who found a 34% of graft patency at 7 years, rates of graft patency by post-operative angiography or Doppler flow in 5 studies have varied between 97%and 100% at 1 month to 1 year post-OPCAB (Boyd et al, 1999; Calafiore et al,1999; Hirose et al, 2000; Bull et al, 2001). Improvement in early graft patencyoccurred once the use of a mechanical stabilizer became routine (Puskas et al,1998; Jansen et al, 1998). Some investigators have used intraoperative Dopplerto assess immediate graft patency; in one study, Doppler flow data led toimmediate anastomotic revisions in about 8% of cases (Boyd et al, 1999).Such an approach could enhance long-term graft patency.

Page 9 of 41
Nonrandomized Comparative Trials, continued
(2) Mortality: Long-term mortality after OPCAB was not significantly differentthan after CCABG in 3/3 studies.
(3) Angina recurrence: Rates of recurrent angina were higher after OPCABthan CCABG in 3/4 studies, and not significantly different in the remaining 1/4studies.
(4) Repeat intervention: Rates of repeat intervention were higher after OPCABthan CCABG in 2/3 studies, and not significantly different in the remaining 1/3 studies.
Thus, in the non-randomized comparative studies, long-term outcomesfollowing OPCAB compared to CCABG were favorable for two of the fouroutcomes reported (graft patency and mortality) and unfavorable for two of thefour outcomes reported (angina recurrence and need for repeat intervention).
In the early non-randomized trial by Gundry et al (1998), a total of 107 patientsunderwent OPCAB and 112 patients underwent CCABG. Results showedsimilar mortality rates: at 7-year follow-up, 80% of OPCAB patients were aliveversus 79% of CCABG patients. However, 30% of the OPCAB patients neededsubsequent coronary angiography for anginal symptoms versus 16% of theCCABG patients (p = .01). In addition, 20% of patients in the OPCAB groupneeded PTCA (angioplasty) or a second coronary artery bypass procedureversus only 7% of CCABG patients. In the trial by Arom et al (2000), at oneyear follow-up, OPCAB patients had more angina than CCABG patients (40%versus 21%, p < .001) and required more repeat cardiac (angioplasty or stent)interventions (10% versus 2%, p<.001).
Randomized Comparative Trials
In 4/6 of the randomized, comparative trials, the number of grafts per patientwas generally the same in OPCAB and CCABG, indicating adequaterandomization and no pre-selection for patients with fewer diseased vessels inthe OPCAB group.

Page 10 of 41
Randomized Comparative Trials, continued
a. Operative outcomes
Table 4 presents the operative outcomes in 8 randomized comparative studiesof OPCAB and CCABG. Operative mortality was not significantly differentafter OPCAB than after CCABG in 7/7 studies. Operation duration was longerafter OPCAB than after CCABG in 1/4 studies, not significantly different in1/4 studies, and shorter in 2/4 studies. Reoperations for bleeding were notsignificantly different after OPCAB than after CCABG in 4/4 studies.Reoperations for graft occlusion were not significantly different in 3/3 studies.Duration of intubation was significantly less after OPCAB in 5/5 studies.Length of stay in the ICU was less after OPCAB in 5/7 studies and notsignificantly different in the remaining 2/7 studies. Post-operative hospitallength of stay was less after OPCAB in 4/6 studies and not significantlydifferent in the remaining 2/6 studies. Thus, in virtually all of the randomizedcomparative studies, OPCAB produced similar or better operative results toCCABG.
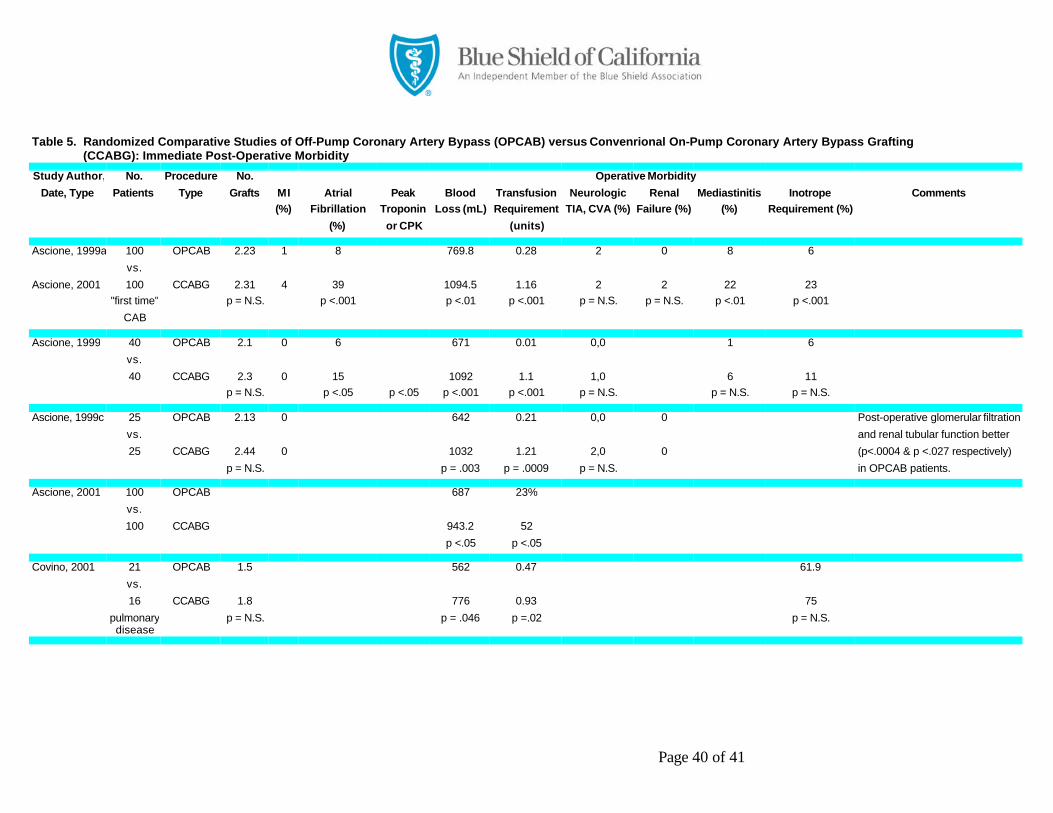
b. Post-operative morbidity outcomes
Table 5 presents the post-operative morbidity outcomes in 7 randomizedcomparative studies of OPCAB and CCABG. Myocardial infarctions were lesscommon after OPCAB in 5/5 studies. Atrial fibrillation occurred lesscommonly after OPCAB in 2/4 studies and not significantly different in theremaining 2/4 studies. Peak CPK levels were less after OPCAB in 2/2 studies.Blood loss was less after OPCAB in 6/6 studies. Transfusion was requiredless often OPCAB in 6/7 studies, and the same in 1/7 studies. Renal failureoccurred less often in 2/2 studies. Neurological complications of transientischemic attack or stroke occurred less often in 5/5 studies. Mediastinitisoccurred less often in 1/3 studies and not significantly different in theremaining 2/3 studies. Inotropic support was required less often in 1/4 studiesand was not significantly different in the remaining 3/4 studies. Thus, in all ofthe non-randomized comparative studies, OPCAB produced similar or betterpost-operative morbidity results to CCABG.
c. Long-term follow-up outcomes
Unfortunately, none of the published randomized comparative trials provideslong-term follow-up data on angina recurrence, need for re-intervention, graftpatency, or mortality. The long-term graft patency rate is a major unansweredquestion in the current OPCAB literature (Plomodon et al, 2001).

Page 11 of 41
Randomized Comparative Trials, continued
The 8 published randomized comparative trials are summarized below.
Ascione and colleagues (1999a, 1999b, 1999c, 2000, 2001) have published aseries of reports from the same randomized trial. In the first, they reportprospectively randomizing 200 patients undergoing first-time coronary arterybypass surgery to either OPCAB or CCABG. There was no difference betweenthe groups with respect to pre- and intraoperative patient variables. Patientsundergoing off-pump surgery had significantly less bed occupancy andtransfusion requirement than conventional on-pump surgery. There were nodeaths or intraoperative myocardial infarctions in either group. However,morbidity was significantly lower in the OPCAB group (Ascione et al, 1999b,1999c). Troponin I release at 1, 2, 12, and 24 hours postoperatively wassignificantly lower in the OPCAB patients than in the CCABG patients(Ascione et al, 1999b). There was a decreased incidence of atrial fibrillation inthe OPCAB patients (Ascione et al, 1999b; Ascione et al, 2000). Theseinvestigators also showed a significant decrease in postoperative blood loss andtransfusion requirement with OPCAB compared to CCABG (p<.001) (Ascioneet al, 1999c). Less than one quarter of the OPCAB patients requiredtransfusion compared with over one half of the CCABG patients (Ascione etal, 2001). The authors also documented shorter length of stays in the intensivecare unit (1.2 vs. 1.0 days) and in the hospital (5.3 vs. 7.3 days) in the OPCABpatients (p<.05) (Ascione et al, 1999c).
A second set of investigators reported a small randomized, controlled trial ofOPCAB (n=21) versus CCABG (n=16) in a group of patients with chronicobstructive pulmonary disease (COPD) and/or restrictive lung disease (Covinoet al, 2001). Results showed that there were significant differences favoringOPCAB in duration of surgery (p=.014), postoperative bleeding (p=.046),transfusion requirement (p=.02), duration of ventilatory support (p=.03), lengthof stay in the ICU. Duration of hospitalization did not differ significantly. NoOPCAB patients developed respiratory failure; 2 CCABG patients developedrespiratory failure, 1 of whom died from it. The authors concluded thatOPCAB allowed a better postoperative clinical course than CCABG in patientswith advanced lung disease.
Page 12 of 41
Randomized Comparative Trials, continued
Guler and colleagues (2001) also randomized patients with severe COPD toOPCAB (n=19) or CCABG (n=18 patients). Results showed that the averageICU stay was significantly shorter in OPCAB than CCABG patients (1.4 vs.2.6 days, p < .05). The most prevalent respiratory morbidity was atelectasis,which postoperatively, there were no significant differences in FEV1,FEV1/FVC, or FVC. The authors concluded that OPCAB procedures are moreadvantageous than on-pump methods for patients with COPD.
Czerny and colleagues (2001) studying elective low-risk patients withmultivessel disease, randomly assigned them by age, sex, and left ventricularejection fraction to receive OPCAB (n=40) or CCABG (n = 40).
Short- and mid-term clinical outcomes were monitored during a mean 13.4month period. Complete revascularization was achieved in 65% of OPCABpatients and 85% of CCABG patients. Mean number of bypass grafts was 2.6with OPCAB and 3.1 with CCABG techniques (p=.043). Clinical outcome andhospital stay were comparable in both groups. There were no myocardialinfarctions or patient deaths in either group. The authors concluded thatOPCAB was effective for complete revascularization in the majority ofselected low-risk patients, but noted that the rate of incompleterevascularization was higher with OPCAB.
A final randomized, controlled trial of OPCAB (n = 142) versus CCABG ( n =139) reports immediate and one-month outcomes (van Dijk et al, 2001).OPCAB patients had fewer vessels bypassed than CCABG (2.4 vs. 2.6, p =.05). Results showed that OPCAB patients compared to CCABG patientsrequired blood products less often (3% vs. 13%, p < . 01), and released CPKless often (p <. 01). OPCAB patients were extubated sooner (3h vs. 9h, p <.01) and discharged home sooner (6d vs. 7d, p < .01) than CCABG patients.Otherwise, there were no significant differences in post-operative outcomes,including atrial fibrillation, TIAs or CVAs, requirement for inotropic support,or length of stay in the ICU. At one month, there were no differences inmortality (0% vs. 0%), stroke (0.7% vs. 1.4%), MI (4.9% vs. 4.3%), repeatCABG (0% vs. 0%). Two OPCAB patients (1.4%) required PTCA; noCCABG patients required PTCA. The authors concluded that, in selectedpatients, off-pump CABG is safe and yields a short-term cardiac outcomecomparable to that of on-pump CABG.

Page 13 of 41
Multicenter Comparison
In a large multicenter comparison, Plomodon et al (2001), using clinicalrecords from the Department of Veterans Affairs from 1997 to 1999, comparedresults obtained for 680 patients receiving OPCAB in 9 centers with 1,733patients receiving CCABG in 34 other centers. The major outcomes studiedwere morbidity and mortality within 30 days of operation. Morbidity includedthe perioperative complications of stroke, coma, ventilator use >48 hours, renalfailure requiring dialysis, endocarditis, mediastinitis, reoperation for bleeding,cardiac arrest requiring CPR, and repeat operation requiring CPB. Thoughthere was no evidence of overall hospital selection bias in the data, the 9 studycenters providing OPCAB were “experienced,” defined as those that performedat least 8% of all CABGs off-pump. Results showed that OPCAB patients,compared to CCABG patients, had slightly lower mortality (2.7% vs. 4.0%,p=N.S.) and significantly lower complication rates (8.8% vs. 14.0%, p<.001).Risk-adjusted morbidity and mortality rates (0.52 and 0.56, respectively) werealso significantly lower for OPCAB vs. CCABG patients (p<.05 for both).These findings were observed despite the fact that, preoperatively, the OPCABpopulation that had higher estimated risks of both death and complicationsbecause of more emergent operations, higher frequency of COPD and diureticuse, and worse ratings for angina and CHF. This study did not examine graftpatency rates following either CABG technique.
Summary Balance Sheet
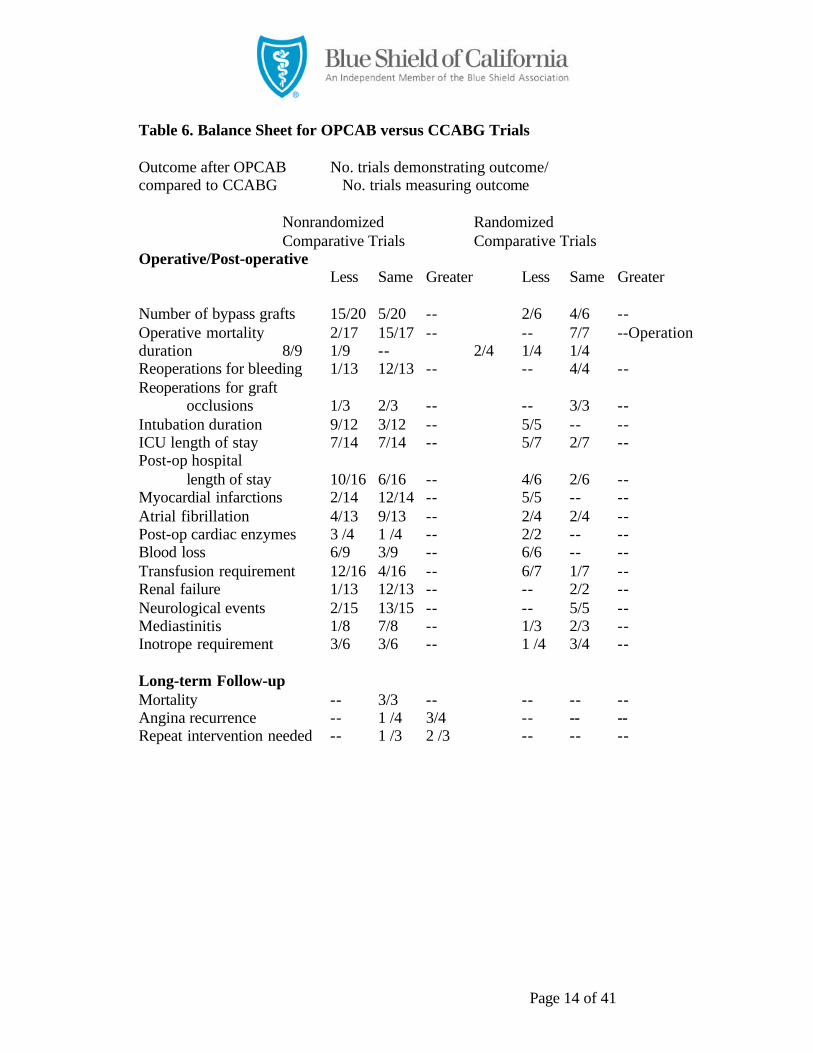
The summary balance sheet in Table 6 suggests that operative and post-operative morbidity outcomes of OPCAB are generally comparable to or betterthan those of CCABG in both non-randomized and randomized trials.However, in the non-randomized trials, long-term follow-up of patientsundergoing OPCAB finds significantly more frequent recurrence of anginathan in CCABG patients in 2/3 trials; and more frequent need for repeat cardiacinterventional procedures (PTCA or CABG) in 2/3 trials (Arom et al, 2000;Gundry et al 1998). In none of 3 trials was there a significant difference inlong-term mortality rates. Graft patency rates appear excellent in 6/7rials.Unfortunately, none of the randomized trials comparing OPCAB with CCABGreports long-term follow-up of patients with respect to angina recurrence, needfor re-intervention, or mortality.
Page 14 of 41
Table 6. Balance Sheet for OPCAB versus CCABG Trials
Outcome after OPCAB No. trials demonstrating outcome/compared to CCABG No. trials measuring outcome
Nonrandomized RandomizedComparative Trials Comparative Trials
Operative/Post-operativeLess Same Greater Less Same Greater
Number of bypass grafts 15/20 5/20 -- 2/6 4/6 --Operative mortality 2/17 15/17 -- -- 7/7 --Operationduration 8/9 1/9 -- 2/4 1/4 1/4Reoperations for bleeding 1/13 12/13 -- -- 4/4 --Reoperations for graft
occlusions 1/3 2/3 -- -- 3/3 --Intubation duration 9/12 3/12 -- 5/5 -- --ICU length of stay 7/14 7/14 -- 5/7 2/7 --Post-op hospital
length of stay 10/16 6/16 -- 4/6 2/6 --Myocardial infarctions 2/14 12/14 -- 5/5 -- --Atrial fibrillation 4/13 9/13 -- 2/4 2/4 --Post-op cardiac enzymes 3 /4 1 /4 -- 2/2 -- --Blood loss 6/9 3/9 -- 6/6 -- --Transfusion requirement 12/16 4/16 -- 6/7 1/7 --Renal failure 1/13 12/13 -- -- 2/2 --Neurological events 2/15 13/15 -- -- 5/5 --Mediastinitis 1/8 7/8 -- 1/3 2/3 --Inotrope requirement 3/6 3/6 -- 1 /4 3/4 --
Long-term Follow-upMortality -- 3/3 -- -- -- --Angina recurrence -- 1 /4 3/4 -- -- --Repeat intervention needed -- 1 /3 2 /3 -- -- --

Page 15 of 41
Neurological Events and Cognitive Dysfunction
OPCAB appears to reduce but not eliminate neurological complications(CVAs, TIAs) in a few series (Baumgartner et al, 2000). However, thenonrandomized trials found fewer neurological events in only 2/15 trials, andnone of the randomized trials showed that OPCAB patients had fewerneurological events.
An important related question is whether OPCAB can reduce cognitivedysfunction after bypass grafting compared with CABG with CPB (McKhannet al, 1997; Roach et al, 1997; Bull et al, 2001). Elderly patients frequentlyexhibit adverse cerebral outcomes after CCABG, with as many as 16% of thoseover age 80 suffering strokes, TIAs, or severe confusion (Roach et al, 1996).A pooled analysis of 6 highly comparable studies found that neurocognitivedysfunction occurs frequently after CABG with CPB. Overall, an estimated22.5% (95% confidence interval, 18.7%-26.4%) of patients had a cognitivedeficit (a decrease of at least 1 standard deviation in at least 2 of 9 or 10 tests)2 months after CPB (van Dijk et al, 2000b). Newman et al have documentedthat over half (53%) of patients undergoing CCABG have cognitive declines atdischarge compared to preoperative tests, and that this decline is a significantpredictor of long-term cognitive function at 5 years (Newman et al, 2001).Cognitive changes after CCABG are believed largely to be due to CPB andaortic manipulation (Baumgartner et al, 2000).
Over time, refinements in CPB techniques, especially use of membraneoxygenators and arterial line microfilters, have lowered the incidence ofpostoperative neurological dysfunction (Pugsley et al, 1994; Kshettry et al,2000). Other factors besides use and duration of CPB contribute toneurological dysfunction after CABG, including age >70, pre-existingatherosclerosis of the aorta and cerebrovascular circulation, and other medicalvariables (Selnes et al, 1999; Kshettry et al, 2000). One recent study showedsimilar patterns of early decline and late recovery of cognitive function inpatients undergoing CABG with and without CPB, suggesting that CPB maynot be the major cause of postoperative cognitive impairment (Taggart et al,1999). Others disagree, however (Murkin et al, 1999).
In a retrospective review of 10 years of OPCAB, Trehan et al (2001) reported areduction in expected stroke/TIA incidence and deaths. Neurologicalcomplications occurred in only 0.14% and deaths in 0.07% of 2,800 patientsundergoing OPCAB.

Page 16 of 41
Neurological Events and Cognitive Dysfunction, continued
In a non-randomized comparative trial using intraoperative transcranial pulsedwave Doppler ultrasound, BhaskerRao et al (1998) provided evidence ofsignificantly fewer high-intensity transient signals (HITS) over the middlecerebral artery in 17 patients undergoing OPCAB compared to 305 patientshaving CCABG. Postoperatively, patients in the OPCAB group scoredsignificantly better on the antisaccadic eye movement test, a sensitive indicatorof neurocognitive deficits secondary to frontal lobe dysfunction. Diegler et al(2000) reported similar results from a randomized trial involving 40 patients(20 OPCAB and 20 CCABG). The median number of perioperative HITS was11 in the OPCAB group versus 394.5 in the CCABG group (p<.0001).Postoperative cognitive testing also showed markedly different results (0%versus 90% rates of impairment by the Syndrom Kurtz Test SKT).Furthermore, there was a correlation between the decrease in postoperativeneurocognitive performance and the number of HITS.
Thus, there is some clinical evidence in a very small number of patients(totaling 37 patients) suggesting less cognitive dysfunction following OPCAB,than after CCABG. However, the etiologic contribution of CPB toneurocognitive dysfunction will remain unclear until a randomized trial thatdirectly compares off-pump and on-pump bypass surgery is completed (vanDijk et al, 2000b). A large randomized trial examining this outcome is stillunderway (see Pending Trials, below).
Other Issues with OPCAB
a. Patient selection criteria
Patient selection criteria for OPCAB have yet to be defined. Two of therandomized trials suggest benefits for high-risk patients with severe lungdisease (Covino et al, 2001; Guler et al, 2001). Arom et al (2000) reported aretrospective series of 350 OPCAB patients, divided into 3 groups on the basisof the Society of Thoracic Surgeons predicted risk model estimate. They foundthat higher-risk patients (>10% predicted risk) fared better with OPCAB thanCCABG. They reported an operative mortality of 7.7% in the high-riskOPCAB group compared to 29% in the high-risk CCABG group.

Page 17 of 41
Other Issues with OPCAB, continued
b. Conversion to CCABG
Conversion to standard CABG with CPB occurs sometimes due either todifficult access to the coronary artery (e.g., an intramyocardial vessel) or a poorquality vessel (Koutlas et al, 2000). Conversion to CPB occurs in about 5% ofOPCAB operations (Stanbridge et al, 1999; Baumgartner et al, 2000), thoughconversion rates as high as 25% have been noted (Soltoski et al, 1998).Conversion is in general well tolerated except when it is instituted for graftmalfunction combined with hemodynamic instability or collapse (Soltoski etal, 1998).
a. Learning curve
The evolution of surgical experience and instrumentation for a multivesselOPCAB is evident both in the gradual rise in the mean number of arteriesbypassed and the increasing proportion of multivessel to single vesselprocedures performed over time, and in the greater number of circumflexcoronary arteries bypassed in OPCAB patients over time. In addition, assurgeons gain familiarity with OPCAB techniques, rates of conversion toCCABG with CPB decline (Soltoski et al, 1998). In groups active in off-pumpsurgery, the rate of conversion to on-pump surgery ranges from 0% to 2.5%,instead of the 5% seen in many series (Bull et al, 2001).
Pending Trials
van Dijk et al (2000a, 2001) report that two multicenter randomized clinicaltrial of OPCAB are underway. The first RCT compares OPCAB tointracoronary stent implantation; the second compares OPCAB to CCABG.The primary endpoint in the comparison of off-pump to conventional CABG,is cerebral safety (i.e., absence of cognitive deficits and fatal or nonfatalstroke). Secondary endpoints will include presence and severity of angina,quality of life, and exercise capacity. The study will enroll a total of 560patients, and a random sample of 210 of them will undergo repeat angiographyat 1 year to reassess angiographic restenosis rate and graft patency. Finalresults at 1 year of this trial are still pending, but preliminary results at 1 monthhave recently been published (van Dijk et al, 2001).
TA Criterion 3 is met.

Page 18 of 41
TA Criterion 4
The established alternative to OPCAB is CCABG. CABG with CPB is a safe,time-honored procedure giving excellent and highly reproducible results insurgical myocardial revascularization (Baumgartner et al, 2000), with amortality rate of 2-3% in elective cases (Ascione et al, 1999b).
The nonrandomized and randomized comparative studies summarized inTables 1-6 above suggest that OPCAB produces similar, or sometimes better,operative, post-operative morbidity and long-term outcomes as CCABG.Therefore, it may be concluded that OPCAB for coronary artery disease meetsCriterion 4 of improving net health outcomes as much as or more than theavailable alternatives.
TA Criterion 4 is met.
TA Criterion 5
OPCAB has recently been successfully used in multiple centers in the U.S. andabroad, including 9 centers in the V.A. system participating in a multicentertrial (Plomodon et al, 2001). Provided that surgeons performing OPCAB areexperienced in off-pump surgery, results similar to those in the published trialssummarized above should be attainable when used to treat individuals withcoronary artery disease in the community setting under conditions of usualmedical practice. TA Criterion 5 is met.
RECOMMENDATIONS OF OTHERS
Blue Cross Blue Shield Association (BCBSA)
The BCBSA has not yet reviewed this topic.
American College of Cardiology (ACC) (California)
The ACC does not have a position specific to this procedure.
CONCLUSION
The selection criteria (indications and contraindications) for OPCABprocedures have yet to be rigorously defined.

Page 19 of 41
CONCLUSION, continued
Recent studies, including retrospective and prospective nonrandomizedcomparative trials, and prospective randomized comparative trials, suggest thatOPCAB results in similar or reduced postoperative morbidity compared withCCABG with CPB. Concerns remain, however, that OPCAB procedures maybe associated with increased angina, and increased need for repeated cardiacinterventions over long-term (1-7 year) follow-up.
In non-randomized trials, but not randomized trials, OPCAB patients havegenerally had fewer grafts placed per patient than CCABG patients, makingdirect comparisons of the techniques somewhat problematic.
In 22 non-randomized comparative studies of OPCAB and CCABG, OPCABproduced similar or better operative, post-operative morbidity, and mortalityresults to CCABG. Long-term outcomes following OPCAB compared toCCABG were favorable for two of the four outcomes reported (graft patencyand mortality) and unfavorable for two others (angina recurrence and need forrepeat intervention).
In virtually all of 8 randomized comparative studies of OPCAB and CCABG,OPCAB produced similar or better operative, post-operative morbidity, andmortality results to CCABG. Unfortunately, none of the published randomizedcomparative trials provides long-term follow-up data on angina recurrence,need for re-intervention, graft patency, or mortality.
There is some published clinical evidence in a small number of patientssuggesting less cognitive dysfunction following OPCAB than CCABG.
Whether OPCAB will result in less neurological compromise on the one hand,and in more subsequent angina or cardiac events or greater need for re-intervention such as PTCA or CABG on the other hand, remains to bedetermined.
In summary, in a majority of patients, off-pump complete coronary arteryrevascularization appears to be an acceptable alternative to conventionalCABG operations, yielding good results given adequate surgeon experienceand rigorous technique, and adequate coronary artery stabilization.
TA criteria 1-5 are met.

Page 20 of 41
RECOMMENDATION
It is recommended that “off-pump” coronary artery bypass graft surgerymeets Blue Shield TA criteria.
Committee approval as recommended
February 13, 2002
This assessment is the property of, and is published by permission of,Blue Shield of California. Any unauthorized use or reproduction of thisassessment is strictly prohibited. This assessment was current as of thedate it was prepared and may not be current as of any later date. Thisassessment may not represent current Blue Shield of California policy.

Page 21 of 41
REFERENCES
Abreu JE; Reilly J; Salzano RP; et al. Comparison of frequencies of atrialfibrillation after coronary artery bypass grating with and without the use ofcardiopulmonary bypass. American Journal of Cardiology, 1999;83:775-6.
Al-Ruzzeh S; George S; Bustami M; et al. The early clinical and angiographicoutcome of the sequential coronary artery bypass grafting using the off pumptechnique. Journal of Thoracic and Cardiovascular Surgery, 2001: in press.
Arom KV; Flavin TF; Emery RW; Kshettry VR; Janey PA; Petersen RJ. Safetyand efficacy of off-pump coronary artery bypass grafting. Annals of ThoracicSurgery, 2000 Mar, 69(3):704-10.
Arom KV; Flavin TF; Emery RW; Kshettry VR; Petersen RJ; Janey PA. Islow ejection fraction safe for off-pump coronary bypass operation? AnnThorac Surg. 2000;70:1021-5.
Ascione R; Lloyd CT; Underwood MJ; et al. On pump versus off pumpcoronary revascularization: evaluation of renal function. Annals of ThoracicSurgery 1999a;68:493-8.
Ascione R, et al. Beating versus arrested heart revascularization: evaluation ofmyocardial function in prospective randomized study. Eur J Cardio-thoracSurg 1999b;15:685-690.
Ascione R; Lloyd CT; Underwood MJ; Lotto AA; Pitsis AA; Angelini GD.Economic outcome of off-pump coronary artery bypass surgery: a prospectiverandomized study. Annals of Thoracic Surgery, 1999c Dec, 68(6):2237-42.
Ascione R; Caputo M; Calori G; et al. Predictors of atrial fibrillation afterconventional and beating heart coronary surgery: a prospective, randomizedstudy. Circulation, 2000;102(13):1530-1535.
Ascione R; William S; Lloyd CT; et al. Reduced postoperative blood loss andtransfusion requirement after beating-heart coronary operations: a prospectiverandomized study. Journal of Thoracic Cardiovascular Surgery, 2001;121:689-96.
Page 22 of 41
REFERENCES, continued
Baumgartner FJ; Yokoyama T; Gheissari A; Capouya ER; Panagiotides GP;Declusin RJ. Effect of off-pump coronary artery bypass grafting on morbidity.American Journal of Cardiology, 2000 Nov 1, 86(9):1021-2, A10.
Benetti FJ. Direct coronary surgery with saphenous vein bypass without eithercardiopulmonary bypass or cardiac rest. Journal of Cardiovascular Surgery,1985;26:217-22.
BhaskerRao B, et al. Evidence for improved cerebral function after minimallyinvasive bypass surgery. J Card Surg, 1998;13:27-31.
Boyd WD et al. Off-pump surgery decreases postoperative complications andresource utilization in the elderly. Annals of Thoracic Surgery,1999;68(4):1490-93.
Buffolo, et al. Coronary artery bypass grafting without cardiopulmonarybypass. Ann Thorac Surg 1996; 61:63-66.
Bull DA; Neumayer LA; Stringham JC; Meldrum P; Affleck DG; KarwandeSV. Coronary artery bypass grafting with cardiopulmonary bypass versus off-pump cardiopulmonary bypass grafting: does eliminating the pump reducemorbidity and cost? Annals of Thoracic Surgery, 2001 Jan, 71(1):170-3;discussion 173-5.
Calafiore AM, Di Giammarco G, Teodori G, Mazzei V, Vitolla G. Recentadvances in multivessel coronary grafting without cardiopulmonary bypass.Heart Surg Forum. 1998;1(1):20-5.
Calafiore AM; Teodori G; Di Giammarco G; et al. Multiple arterial conduitswithout cardiopulmonary bypass: early angiographic results. Annals ofThoracic Surgery 1999;57:450-6.
Cartier R; Brann S; Dagennairs F; Martineau R; Couturier A. Systematic off-pump coronary artery revascularization in multivessel disease: an experiencewith 300 cases. Journal of Thoracic and Cardiovascular Surgery2000;199:221-9.
Covino E; Santise G; DiLello F; et al. Surgical myocardial revascularization(CABG) in patients with pulmonary disease: beating heart versuscardiopulmonary bypass. Journal of Cardiovascular Surgery, 2001;42:23-6.
Page 23 of 41
REFERENCES, continued
Czerny M, Baumer H, Kilo J, Zuckermann A, Grubhofer G, Chevtchik O,Wolner E, Grimm M. Complete revascularization in coronary artery bypassgrafting with and without cardiopulmonary bypass. Ann Thorac Surg. 2001Jan;71(1):165-9.
Dewey TM, Magee M, Edgerton J, Vela R, Prince SL, Acuff T, Mack MJ.Leftmini-thoracotomy for beating heart bypass grafting: a safe alternative to high-risk intervention for selected grafting of the circumflex artery distribution.Circulation. 2001 Sep 18;104(12 Suppl 1):I99-101.
Dewey TM, Magee M, Edgerton J, Mathison M; Tinnison D; Mack MJ. Off-pump bypass grafting is safe in patients with left main coronary disease . AnnThorac Surg. 2001;72:788-92.
Diegler A, et al. Neuromonitoring and neurocognitive outcome in off-pump vs.conventional coronary bypass operation. Annals of Thoracic Surgery2000;69:1162-1166.
Gamoso MG; Phillips-Bute B; Landolfo KP; Newman MF; Stafford-Smith M.Off-pump versus on-pump coronary artery bypass surgery and postoperativerenal dysfunction. Anesthesia and Analgesia, 2000 Nov, 91(5):1080-4.
Guler M, Kirali K, Toker ME, Bozbuga N, Omeroglu SN, Akinci E, Yakut C.Different CABG methods in patients with chronic obstructive pulmonarydisease. Ann Thorac Surg. 2001 Jan;71(1):152-7.
Gundry SR; Romano MA; Shattuck OH; Razzouk AJ; Bailey LL.. Seven-yearfollow-up of coronary artery bypasses performed with and withoutcardiopulmonary bypass. J Thoracic Cardiovasc Surg, 1998; 115:1273-78.
Hart JC; Spooner T; Edgerton J; Milsteen SA. Off-pump multivessel coronaryartery bypass utilizing the Octopus tissue stabilization system: initialexperience in 374 patients from three separate centers. Heart Surg Forum,1999, 2(1):15-28.
Hernandez F; Clough RA; Klemperer JD; Blum JM. Off-pump coronary arterybypass grafting: initial experience at one community hospital. Annals ofThoracic Surgery, 2000 Sep, 70(3):1070-2.
Jansen WE; Borst C; Lahpor JR; et al. Coronary artery bypass grafting withoutcardiopulmonary bypass using the octopus method: results in the first onehundred patients. J Thorac Cardiovasc Surg, 1998;116:60-67.

Page 24 of 41
REFERENCES, continued
Jegaden O; Mikaeloff P. Off-pump coronary artery bypass surgery. Thebeginning of the end? [editorial] European Journal of Cardio-Thoracic Surgery,2001 Mar, 19(3):237-8.
Kolessov VI. Mammary artery-coronary artery anastomosis as a method oftreatment for angina pectoris. Journal of Thoracic and Cardiovascular Surgery,1967;54:534-44.
Koutlas TC; Elbeery JR; Williams JM; Moran JF; Francalancia NA; ChitwoodWR Jr. Myocardial revascularization in the elderly using beating heartcoronary artery bypass surgery. Annals of Thoracic Surgery, 2000 Apr,69(4):1042-7.
Kshettry VR; Flavin TF; Emery RW; Nicoloff DM; Arom KV; Petersen RJ.Does multivessel, off-pump coronary artery bypass reduce postoperativemorbidity? Annals of Thoracic Surgery, 2000 Jun, 69(6):1725-30; discussion1730-1.
Lancey RA; Soller BR; Vander Salm TJ. Off-pump versus on-pump coronaryartery bypass surgery: a case-matched comparison of clinical outcomes andcosts. Heart Surg Forum, 2000, 3(4):277-81.
Lima LE, Jatene F, Buffolo E, Vanky F, Casimir-Ahn E, Lohn U, Leprince PPavie, A, Laczkovics AM, Reichenspurner H, Calafiore A, Nataf P, Mack M.Amulticenter initial clinical experience with right heart support and beating heartcoronary surgery. Heart Surg Forum. 2001;4(1):60-4.
McKhann GM; Goldsborough MA; Borowitz LM; et al. Cognitive outcomeafter coronary artery bypass: a one year prospective study. Annals of ThoracicSurgery, 1997;63:510-5.
Meharwal ZS, Trehan N. Is off-pump coronary artery bypass surgery safe forleft main coronary artery stenosis? Indian Heart J. 2001 May-Jun;53(3):314-8.
Moshkovitz Y; Sternik L; Paz Y; et al. Primary coronary artery bypassgrafting without cardiopulmonary bypass in impaired left ventricular function.Ann Thorac Surg. 1997;63:S44-7.
Murkin JM; Boyd WD; Ganapathy S; et al. Beating heart surgery: why expectless central nervous system morbidity? Annals of Thoracic Surgery,1999;68;1498-501.
Page 25 of 41
REFERENCES, continued
Nader ND; Khadra WZ; Reich NT; et al. Blood product use in cardiacrevascularization: comparison of on- and off-pump techniques. Annals ofThoracic Surgery, 1999;68:1640-43.
Newman M, et al. Longitudinal assessment of neurocognitive function aftercoronary artery bypass surgery. NEJM, 2001; 344(6):395-402.
Plomodon ME; Cleveland JC Jr; Ludwig ST; et al. Off-pump coronary arterybypass is associated with improved risk-adjusted outcomes. Ann Thorac Surg.2001;72:114-9.
Pugsley W; Klinger L; Paschalis C; et al. The impact of micro-emboli duringcardiopulmonary bypass on neuropsychological functioning. Stroke,1994;25:1393-9.
Puskas JD; Wright CE; Ronson RS; et al. Off-pump multivessel coronaryartery bypass via sternotomy is safe and effective. Annals of Thoracic Surgery,1998;66:1068-72.
Puskas JD, Thourani VH, Marshall JJ, Dempsey SJ, Steiner MA, SammonsBH,Brown WM 3rd, Gott JP, Weintraub WS, Guyton RA. Clinical outcomes,angiographic patency, and resource utilization in 200 consecutive off-pumpcoronary bypass patients. Ann Thorac Surg. 2001 May;71(5):1477-83;discussion 1483-4.
Rama A; Mohammadi S; Leprince P; Gandjbakhch I. A simple method forheart stabilization during off-pump multi-vessel coronary artery bypassgrafting: surgical technique and short term results. European Journal of Cardio-Thoracic Surgery, 2001 Jan, 19(1):105-7.
Roach GW; Kanchuger M; Mangano CM; et al. Adverse cerebral outcomesafter coronary artery bypass surgery. N Engl J Med, 1996;335:1857-63.
Sabiston DC, Jr. The coronary circulation. Johns Hopkins Medical Journal,1974;134:314-29.
Selnes OA; Goldsborough MA; Borowicz LM; et al. Determinants ofcognitive change after coronary artery bypass surgery: a multifactorialproblem. Annals of Thoracic Surgery, 1999;67:1669-76.
Page 26 of 41
REFERENCES, continued
Society of Thoracic Surgeons Cardiac Registry Eighth Annual Report,December 1998; 195.
Soltoski P; Salerno T; Levinsky L; Schmid S; Hasnain S; Diesfeld T; Huang C;Akhter M; Alnoweiser O; Bergsland J. Conversion to cardiopulmonary bypassin off-pump coronary artery bypass grafting: its effect on outcome. Journal ofCardiac Surgery, 1998 Sep-Oct, 13(5):328-34.
Spooner TH; Dyrud PE; Monson BK; et al. Coronary artery bypass on thebeating heart with the octopus: a North American experience. Annals ofThoracic Surgery, 1998;66:1032-35.
Stamou SC; Pfister AJ; Dangas G; Dullum MK; Boyce SW; Bafi AS; GarciaJM; Corso PJ. Beating heart versus conventional single-vessel reoperativecoronary artery bypass. Annals of Thoracic Surgery, 2000 May, 69(5):1383-7.
Stanbridge RDL; Hadjinikolaou LK. Technical adjuncts in beating heartsurgery. Comparison of MIDCAB to off-pump sternotomy: a meta-analysis.Eur J Cardio-thorac Surg, 1999;16(Suppl 2):S24-33.
Sternik L; Moshkovitz Y; Hod H; Mohr R. Comparison of myocardialrevascularization without cardiopulmonary bypass to standard open hearttechnique in patients with left ventricular dysfunction. Eur J Cardio-thoracSurg, 1997;11:1213-28.
Stump DA; Rorie KD; Jones TJ. Does off-pump coronary artery bypasssurgery reduce the risk of brain injury? Heart Surg Forum, 2001, 4 Suppl1:S14-8.
Taggart DP; Browne SM; Halligan PW; Wade DT. Is cardiopulmonary bypassstill the cause of cognitive dysfunction after cardiac operations? Journal ofThoracic and Cardiovascular Surgery, 1999;118;414-21.
Tasdemir O; Vural KM; Karagoz H; Bayazit K. Coronary artery bypassgrafting on the beating heart without the use of extracorporeal circulation:review of 2052 cases. Journal of Thoracic and Cardiovascular Surgery, 1998Jul, 116(1):68-73.
Trehan N; Mishra M; Sharma OP; Mishra A; Kasliwal RR. Further reductionin stroke after off-pump coronary artery bypass grafting: a 10-year experience.Ann Thorac Surg. 2001;72:S1026-32.
Page 27 of 41
REFERENCES, continued
Turner WF Jr. "Off-pump" coronary artery bypass grafting: the first onehundred cases of the Rose City experience. Annals of Thoracic Surgery, 1999Oct, 68(4):1482-5.
van Dijk D; Nierich AP; Eefting FD; et al. The Octopus Study: Rationale anddesign of two randomized trials on medical effectiveness, safety, and costeffectiveness of bypass surgery on the beating heart. Controlled Clinical Trials,2000a; 21: 595-609.
van Dijk D, Keizer AM, Diephuis JC, Durand C, Vos LJ, Hijman R.Neurocognitive dysfunction after coronary artery bypass surgery: a systematicreview. J Thorac Cardiovasc Surg 2000b Oct;120(4):632-9.
van Dijk D, Nierich AP, Jansen EW, Nathoe HM, Suyker WJ, Diephuis JC,van Boven WJ, Borst C, Buskens E, Grobbee DE, Robles De Medina EO, deJaegere PP; Octopus Study Group. Early outcome after off-pump versus on-pump coronary bypass surgery: results from a randomized study. Circulation2001 Oct 9;104(15):1761-6.
Yeatman M; Caputo M; Ascione R; Ciulli F; Angelini GD. Off-pump coronaryartery bypass surgery for critical left main stem disease: safety, efficacy andoutcome. European Journal of Cardio-Thoracic Surgery, 2001 Mar, 19(3):239-44.
Zehr KJ, Handa N, Bonilla LF, Abel MD, Holmes DR Jr.Pitfalls and results of immediate angiography after off-pump coronary arterybypass grafting. Heart Surg Forum. 2000; 3(4): 293-9.

Page 28 of 41
Table 1. Non-randomized Comparative Studies of Off-Pump Coronary Artery Bypass (OPCAB) versus Conventional On-Pump Coronary Artery Bypass Grafting(CCABG) : Operative Outcomes
Study Author, No. Procedure No. Operative Operation Reoperation Intubation ICU Post -op HospitalDate, Type Patients Type Grafts Mortality (%) Duration (mins) Bleeding (%) Occlusion (%) Duration (h) LOS LOS (days)
Gundry, 1998 107 OPCAB 2.4Retrospective vs. vs.
112 CCABG 3.2
Abreu, 1999 34 OPCABRetrospective vs. vs.
747 CCABG
Arom, 2000 350 OPCAB 2.1 3.4 231 1.4 1.4 9 33 h 6.1Retrospective vs. vs.
3171 CCABG 3.2 3.4 306 2.2 0.1 19 42 7.1
p<.001 p = N.S. p < .001 p = .003 p <.001 p <.001 p <.001 p <.001
Koutlas, 2000 53 OPCAB 1.5 0 0 4.4Retrospective vs. vs.
220 CCABG 2.5 7.6 3.1 8.4p = .04 p = N.S. p <.05
Kshettry, 2000 135 OPCAB 3.5 0.7 202 0 0 7.1 7.0Retrospective vs. vs.
609 CCABG 3.8 2.1 194 3 0 14.8 7.3p<.001 p = N.S. p = N.S. p = N.S. p = .02 p = N.S. p = N.S.
Lancey, 2000 76 OPCAB 2.8 1.3 0 0.26 d 1.8 d 5.17case-matched vs. vs.Historical controls 76 CCABG 3.7 3.9 1.3 0.77 2.4 6.24
p = .00001 p = N.S. p = N.S. p = .007 p = N.S. p = N.S.
Gamoso, 2000 55 OPCABRetrospective vs. vs.
635 CCABG

Page 29 of 41
Table 1. Non-randomized Comparative Studies of Off-Pump Coronary Artery Bypass (OPCAB) versus Conventional On-Pump Coronary Artery Bypass Grafting(CCABG) : Operative Outcomes, continued
Study Author, No. Procedure No. Operative Operation Reoperation Intubation ICU Post -op HospitalDate, Type Patients Type Grafts Mortality (%) Duration (mins) Bleeding (%) Occlusion (%) Duration (h) LOS LOS (days)
Baumgarten, 2000 303 OPCAB 3.1 0.7 "prolonged":3%
2.0 d 6.6
vs. vs.483 CCABG 4 2.7 6.6 2.3 6.8
p = N.S. p <.05 p = N.S. p = N.S.
Hernandez, 2000 332 OPCAB 3.03 2.11 153 3.01 < 5 d:Prospective,historical
vs. vs. 39.2%
Controls 445 CCABG 3.45 3.38 164.7 4.73 7.4p<.001 p = N.S. p <.001 p = N.S. p <.001
Stamou, 2000 91 OPCAB 1 1 180 0 "prolonged":4%
1 d 5
Retrospective vs. vs.41 CCABG 1 10 240 2 17 2 8
"redo"single
p = .03 p <.04 p = N.S. p = .03 p = N.S. p <.001
vessel
Bull, 2001 40 OPCAB 2.7 3 188 3 7.5h 24 h 3.6Prospective vs. vs.
40 CCABG 3.6 0 210 0 8.6 26 3.7p <.0001 p = N.S. p <.0001 p = N.S. p = N.S. p = N.S. p = N.S.
Hirose, 2000 94 OPCAB 1.7 0 224 0 6.1 1.8 d 14.2Retrospective vs. vs.
221 CCABG 3.6 0.9 312 0.9 12.2 2.9 16.8p < .0001 p = N.S. p <.0001 p = N.S. p <.0001 p <.0001 p <.005

Page 30 of 41
Table 1. Non-randomized Comparative Studies of Off-Pump Coronary Artery Bypass (OPCAB) versus Conventional On-Pump Coronary Artery Bypass Grafting(CCABG) : Operative Outcomes, continued
Study Author, No. Procedure No. Operative Operation Reoperation Intubation ICU Post -op HospitalDate, Type Patients Type Grafts Mortality (%) Duration (mins) Bleeding (%) Occlusion (%) Duration (h) LOS LOS (days)
Yeatman, 2001 75 OPCAB 2.6 1.3 2.7 13.7 1.5 d 7.9vs. vs.312 CCABG 3.1 2.6 6.1 18.7 1.7 8.3
"critical" p <.001 p = N.S. p = N.S. p = .03 p = N.S. p = .01left mainstenoses
Boyd, 1999 30 OPCAB 1.7 0 8 24 h 6.3vs. vs.60 CCABG 2.9 1 16 37 7.7
p <.001 p = N.S. p <.001 p <.05 p <.05
Nader, 1999 66 OPCAB 2.4vs. vs.60 CCABG 2.5
p = N.S.
Calafiore, 1999 122 OPCAB 2.5 0 1 4.5 14.1 h 4.1vs. vs.105 CCABG 2.8 1 0 3.8 27.3 5.4
p = N.S. p = N.S. p = N.S. p = N.S. p <.001 p <.001
Cartier, 2000 300 OBCAB 2.92 1.3 29.8vs. vs.
1870 CCABG 2.84 2 45p = N.S. p = N.S. p <.05
Meharwal, 2001 174 OPCAB 2.9 1.1 178 0.6 15 23 h 6vs. vs.991 CCABG 3.1 1.4 238 2.4 22 36 h 9
left main p = .002 p= N. S. p <.001 p = N.S. p = .001 p < .001 p <.001

Page 31 of 41
Table 1. Non-randomized Comparative Studies of Off-Pump Coronary Artery Bypass (OPCAB) versus Conventional On-Pump Coronary Artery Bypass Grafting(CCABG) : Operative Outcomes, continued
Study Author, No. Procedure No. Operative Operation Reoperation Intubation ICU Post -op HospitalDate, Type Patients Type Grafts Mortality (%) Duration (mins) Bleeding (%) Occlusion (%) Duration (h) LOS LOS (days)
Puskas, 2001 200 OPCAB 2.5 1 1.5 3.9vs. vs.
1000 CCABG 3.7 0.8 1.5 5.7p < .001 p = N.S. p = N.S. p < .001
Calafiore, 1999 122 OPCAB 1.6 16.8 4.1high-risk
vs. vs.158 OPCAB 1.9good
anatomyvs. vs.114 CCABG 2.6 26.3 5.5
p = N.S. p = .007 p < .001
Dewey, 2001 100 OPCAB 2.87 1 7.8vs. vs.723 CCABG 3.4 4.7 7.2
left main p = .001 p = .059 p = N.S.
Arom, 2000 45 OPCAB 2.7 4.4 174 0 0 23.5 60.5 8.2
vs. vs.
132 CCABG 3.3 7.5 235 3.8 0.8 33.2 58 7.9
lowejection
p = .001 p = N.S. p < .001 p = N.S. p = N.S. p = N.S. p = N.S. p = N.S.
fraction
Page 32 of 41
Table 2. Non-randomized Comparative Studies of Off-Pump Coronary Artery Bypass (OPCAB) versus Conventional On-Pump Coronary Artery Bypass Grafting(CCABG): Post-Operative Morbidity
Study Author, No. Procedure No. Operative Morbidity
Date, Type Patients Type Grafts MI Atrial Peak CPK Blood Transfusion Renal Neurologic Mediastinitis Inotrope(%) Fibrillation (%) Level (mg/dl) Loss (mL) Requirement Failure (%) TIA, CVA (%) Requirement
(units) (%)
Gundry, 1998 107 OPCAB 2.4
Retrospective vs. vs.
112 CCABG 3.2
Abreu, 1999 34 OPCAB 12
Retrospective vs. vs.
747 CCABG 26
p = N.S.
Arom, 2000 350 OPCAB 2.1 0.6 14 508 694 5 0.3, 1.4
Retrospective vs. vs.
3171 CCABG 3.2 2.2 23 892 909 6 0.9, 2.0
p<.001 p = .043 p<.001 p <.001 p<.001 p = N.S. p = N.S.
Koutlas, 2000 53 OPCAB 1.5 0 26 0.4 0 2.2 0
Retrospective vs. vs.
220 CCABG 2.5 1.3 26 1.9 3.5 2.3 0.9
p = N.S. p = N.S. p = N.S. p<.01 p = N.S. p = N.S. p= N.S.
Kshettry, 2000 135 OPCAB 3.5 17.8 37.8 729 0.5 6.7 1.5, 2Retrospective vs. vs.
609 CCABG 3.8 21.5 48.5 894 0.9 4.1 1.5, 2
p<.001 p = N.S. p = N.S. p <. 001 p <.001 p = N.S. p = N.S.

Page 33 of 41
Table 2. Non-randomized Comparative Studies of Off-Pump Coronary Artery Bypass (OPCAB) versus Conventional On-Pump Coronary Artery Bypass Grafting(CCABG): Post-Operative Morbidity, continued
Study Author, No. Procedure No. Operative Morbidity
Date, Type Patients Type Grafts MI Atrial Peak CPK Blood Transfusion Renal Neurologic Mediastinitis Inotrope(%) Fibrillation (%) Level (mg/dl) Loss (mL) Requirement Failure (%) TIA, CVA (%) Requirement
(units) (%)
Lancey, 2000 76 OPCAB 2.8 1.2 23.9 565 0.25 1.3
case-matched vs. vs.
Historical controls 76 CCABG 3.7 1.3 26.3 834 0.88 0p =
.00001p = N.S. p = N.S. p = .009 p = .00001 p = N. S.
Gamoso, 2000 55 OPCAB 8.9Retrospective vs. vs.
635 CCABG 7.7p = N.S.
Baumgarten,2000
303 OPCAB 3.1 10% 3.3 1.3
vs. vs.483 CCABG 4 45% 5.4 5
p <.001 p <.05 p <.02
Hernandez, 2000 332 OPCAB 3.03 0.3 19 30.2% 9.6 0.9 0.3
Prospective,historical
vs. vs.
Controls 445 CCABG 3.45 7.2 22.9 40 6.3 1.13 0.9
p<.001 p <.001 p = N.S. p = N.S. p = N.S p = N.S. p = N.S.
Stamou, 2000 91 OPCAB 1 1 14 27% 5 2 12
Retrospective vs. vs.
41 CCABG 1 2 29 58 10 12 24
"redo"single
p = N.S. p = .04 p = .001 p = N.S. p = .03 p = N.S.
vessel
Page 34 of 41
Table 2. Non-randomized Comparative Studies of Off-Pump Coronary Artery Bypass (OPCAB) versus Conventional On-Pump Coronary Artery Bypass Grafting(CCABG): Post-Operative Morbidity, continued
Study Author, No. Procedure No. Operative Morbidity
Date, Type Patients Type Grafts MI Atrial Peak CPK Blood Transfusion Renal Neurologic Mediastinitis Inotrope(%) Fibrillation (%) Level (mg/dl) Loss (mL) Requirement Failure (%) TIA, CVA (%) Requirement
(units) (%)
Bull, 2001 40 OPCAB 2.7 3 18 419 0.3 3 0 5
Prospective vs. vs.
40 CCABG 3.6 3 18 588 0.38 0 0 0p <.0001 p = N.S. p = N.S. p = .036 p = N.S. p = N.S. p = N.S. p = N.S.
Hirose, 2000 94 OPCAB 1.7 2.1 3.5 0 0 0
Retrospective vs. vs.
221 CCABG 3.6 1.4 4.0 0.9 3.2 0.9
p < .0001 p = N.S. p = N.S. p = N.S. p = N.S. p = N.S.
Yeatman, 2001 75 OPCAB 2.6 2.7 12 947 6.7% 6.7 0 0 12
vs. vs.
312 CCABG 3.1 2.9 12.2 1000 25.6% 9.6 1.9 6.7 38.1
"critical" p <.001 p = N.S. p = N.S. p = N.S. p = .0006 p = N.S. p = N.S. p = .02 p = .0001
left mainstenoses
Boyd, 1999 30 OPCAB 1.7 10 0 0 10
vs. vs.
60 CCABG 2.9 28 1.2 6.7 32
p <.001 p <.05 p <.001 p = N.S. p <.05
Nader, 1999 66 OPCAB 2.4 2312 2.25
vs. vs.
60 CCABG 2.5 3251 4.5
p = N.S. p <.05 p <.05

Page 35 of 41
Table 2. Non-randomized Comparative Studies of Off-Pump Coronary Artery Bypass (OPCAB) versus Conventional On-Pump Coronary Artery Bypass Grafting(CCABG): Post-Operative Morbidity, continued
Study Author, No. Procedure No. Operative Morbidity
Date, Type Patients Type Grafts MI Atrial Peak CPK Blood Transfusion Renal Neurologic Mediastinitis Inotrope(%) Fibrillation (%) Level (mg/dl) Loss (mL) Requirement Failure (%) TIA, CVA (%) Requirement
(units) (%)
Calafiore, 1999 122 OPCAB 2.5 0 9.8 403 14.7 0 0 0
vs. vs.
105 CCABG 2.8 1 12.3 697 23.8 1.9 0.9 6p = N.S. p = N.S p = N.S. p = N.S. p = N.S. p = N.S. p = N.S. p = N.S.
Cartier, 2000 300 OPCAB 2.92 3.6 34%
vs. vs.
1870 CCABG 2.84 4.2 66%
p = N.S. p = N.S. p > .005
Meharwal, 2001 174 OPCAB 2.9 0.6 9.7 365 36.2% 0.6 0 0.6 12.6vs. vs.991 CCABG 3.1 1.4 15.8 582 48.0% 1.2 0.3 0.7 18.6
left main p = .002 p = N.S. p = .05 p < .001 p =.05 p = N.S. p = N.S. p = N.S. p = N.S.
Puskas, 2001 200 OPCAB 2.5 1 33.0% 1.5 0vs. vs.
1000 CCABG 3.7 0.8 70.0% 2.3 2.2p <.001 p = N.S. p < .001 p = N.S. p = N.S.
Dewey, 2001 100 OPCAB 2.87 1 35% 23vs. vs.723 CCABG 3.4 1.4 67% 63
p = .001 p = N.S. p = .001 p < .001
Arom, 2000 45 OPCAB 2.7 0 13.3 233 379 11.1 0 0vs. vs.132 CCABG 3.3 0 23 790 713 9 2.3 0low
ejectionp = .001 p = N.S. p = N.S. p < .001 p <.001 p = N.S. p = N.S. p = N.S.
fraction
Page 36 of 41
Table 3. Non-randomized Comparative Studies of Off-Pump Coronary Artery Bypass (OPCAB) versus Conventional On-Pump Coronary Artery Bypass Grafting(CCABG) : Long-Term Follow-up Outcomes
Study Author, No. Procedure No. Follow-up Graft Patency Follow-up OutcomesDate, Type Patients Type Grafts (y) (%) Mortality (%) Angina (%) Repeat Intervention (%)
Gundry, 1998 107 OPCAB 2.4 7 34 20 (7y) 30 20Retrospective vs. vs.
112 CCABG 3.2 72 21 (7y) 16 7p = N.S. p = .01 p = ?
Arom, 2000 350 OPCAB 2.1 1 40 10Retrospective vs. vs.
3171 CCABG 3.2 21 2p<.001 p <.001 p <.001
Kshettry, 2000 135 OPCAB 3.5 0.5 9 2.4Retrospective vs. vs.
609 CCABG 3.8 12 1.7p<.001 p = N.S. p = N.S.
Bull, 2001 40 OPCAB 2.7 97Prospective vs. vs.
40 CCABG 3.6p <.0001
Hirose, 2000 94 OPCAB 1.7 6.4Retrospective vs. vs.
221 CCABG 3.6 2.3p < .0001 p = ?
Yeatman, 2001 75 OPCAB 2.6 2 2.3vs. vs.312 CCABG 3.1 5.9
"critical" p <.001 p = N.S.left mainstenoses

Page 37 of 41
Table 3. Non-randomized Comparative Studies of Off-Pump Coronary Artery Bypass (OPCAB) versus Conventional On-Pump Coronary Artery Bypass Grafting(CCABG) : Long-Term Follow-up Outcomes, continued
Study Author, No. Procedure No. Follow-up Graft Patency Follow-up OutcomesDate, Type Patients Type Grafts (y) (%) Mortality (%) Angina (%) Repeat Intervention (%)
Boyd, 1999 30 OPCAB 1.7 100vs. vs.60 CCABG 2.9
p <.001
Calafiore, 1999 122 OPCAB 2.5 98.9 0vs. vs.105 CCABG 2.8 0.9
p = N.S. p = N.S.
Puskas, 2001 200 OPCAB 98.8vs. vs.
1000 CCABG
Calafiore, 1999 280 OPCAB 98.6 1.8vs. vs.114 CCABG 2.6
p = N.S.

Page 38 of 41
Table 4. Randomized Comparative Studies of Off-Pump Coronary Artery Bypass (OPCAB) versus Conventional On-Pump Coronary Artery Bypass Grafting(CCABG): Operative Outcomes
Study Author, No. Procedure No. Operative Mortality Operation Reoperation Intubation ICU Post -op Hospital Comments
Date, Type Patients Type Grafts (%) Duration (mins) Bleeding (%) Occlusion (%) Duration (h) LOS LOS (days)
Ascione, 1999a 100 OPCAB 2.23 0 176.7 0 7.16 1.09 6.28 2% of OPCAB patients
vs. required conversionAscione, 2001 100 CCABG 2.31 2 186.2 1 12.72 1.35 7.17 to CPB
"first time" p = N.S. p = N.S. p = N.S. p <.05 p <.05 p <.05CAB
Ascione, 1999 40 OPCAB 2.1 0 0 1 5.8vs.40 CCABG 2.3 0 4 1.2 7.3
p = N.S. p = N.S. p <.05 p <.05
Ascione, 1999c 25 OPCAB 2.13 0 0 1 5.84
vs.25 CCABG 2.44 0 3 1 7.36
p = N.S. p = N.S. p <.04 p = .03
Ascione, 2001 100 OPCAB 2 0vs.100 CCABG 8 1
p = N.S. p = N.S.
Covino, 2001 21 OPCAB 1.5 0 196 13.1 33.8 7.2
vs.16 CCABG 1.8 6.2 235 19.1 53.6 8.25
pulmonarydisease
p = N.S. p = N.S. p = .014 p = .03 p = .01 p = N.S.
Van Dijk, 2001 142 OPCAB 2.4 0 4.2 3 22 6 7.7 % of OPCAB patientsvs. required conversion
139 CCABG 2.6 0 3.8 9 22 7 to CPB.p = .05 p < .01 p <.01 p = N.S. p < .01

Page 39 of 41
Table 4. Randomized Comparative Studies of Off-Pump Coronary Artery Bypass (OPCAB) versus Conventional On-Pump Coronary Artery Bypass Grafting (CCABG): Operative Outcomes, continued
Study Author, No. Procedure No. Operative Mortality Operation Reoperation Intubation ICU Post -op Hospital Comments
Date, Type Patients Type Grafts (%) Duration (mins) Bleeding (%) Occlusion (%) Duration (h) LOS LOS (days)
Guler, 2001 19 OPCAB 0 4.5 1.4 No difference in
vs. postoperative18 CCABG 0 8.65 2.6 FEV 1 , FEV1 / FVC, and
p < .001 p <.05 FVC between groups.
Czerny, 2001 40 OPCAB 2.6 0 178 2.5 2.5 4.8 1.2 13.5vs.40 CCABG 3.1 0 254 5 0 17.7 2 12.6
p = .04 p = .001 p = N.S. p = N.S. p = .003 p = N.S. p = N.S.
Page 40 of 41
Table 5. Randomized Comparative Studies of Off-Pump Coronary Artery Bypass (OPCAB) versus Convenrional On-Pump Coronary Artery Bypass Grafting (CCABG): Immediate Post-Operative Morbidity
Study Author, No. Procedure No. Operative Morbidity
Date, Type Patients Type Grafts MI Atrial Peak Blood Transfusion Neurologic Renal Mediastinitis Inotrope Comments(%) Fibrillation Troponin Loss (mL) Requirement TIA, CVA (%) Failure (%) (%) Requirement (%)
(%) or CPK (units)
Ascione, 1999a 100 OPCAB 2.23 1 8 769.8 0.28 2 0 8 6
vs.
Ascione, 2001 100 CCABG 2.31 4 39 1094.5 1.16 2 2 22 23"first time" p = N.S. p <.001 p <.01 p <.001 p = N.S. p = N.S. p <.01 p <.001
CAB
Ascione, 1999 40 OPCAB 2.1 0 6 671 0.01 0,0 1 6
vs.
40 CCABG 2.3 0 15 1092 1.1 1,0 6 11p = N.S. p <.05 p <.05 p <.001 p <.001 p = N.S. p = N.S. p = N.S.
Ascione, 1999c 25 OPCAB 2.13 0 642 0.21 0,0 0 Post-operative glomerular filtration
vs. and renal tubular function better
25 CCABG 2.44 0 1032 1.21 2,0 0 (p<.0004 & p <.027 respectively)
p = N.S. p = .003 p = .0009 p = N.S. in OPCAB patients.
Ascione, 2001 100 OPCAB 687 23%
vs.
100 CCABG 943.2 52
p <.05 p <.05
Covino, 2001 21 OPCAB 1.5 562 0.47 61.9
vs.
16 CCABG 1.8 776 0.93 75
pulmonarydisease
p = N.S. p = .046 p =.02 p = N.S.

Page 41 of 41
Table 5. Randomized Comparative Studies of Off-Pump Coronary Artery Bypass (OPCAB) versus Convenrional On-Pump Coronary Artery Bypass Grafting (CCABG): Immediate Post-Operative Morbidity, continued
Study Author, No. Procedure No. Operative Morbidity
Date, Type Patients Type Grafts MI Atrial Peak Blood Transfusion Neurologic Renal Mediastinitis Inotrope Comments(%) Fibrillation Troponin Loss (mL) Requirement TIA, CVA (%) Failure (%) (%) Requirement (%)
(%) or CPK (units)
Van Dijk, 2001 142 OPCAB 2.4 4.9 20 0.5 3 0.7 27 At one month, PTCA required in
vs. 1.4% of OPCAB versus
139 CCABG 2.6 4.3 21 0.4 13 1.4 28 0% of CCABG patients. Nop = .05 p =
N.S.p = N.S. p < .01 p < .01 p <.01 p = N.S. p = N.S. repeat CABGs in either group.
Czerny, 2001 40 OPCAB 2.6 0 12.5 1.1 0 2.5 By 3 months, PTCA required invs. 7.5% of OPCAB versus 0% of40 CCABG 3.1 0 17.5 1.7 0 5 CCABG patients. Graft patency
p = .04 p = N.S. p = N.S. p = N.S. was 89% at 3 months in 9patients.