oecd review of quality of health care raising standards: czech republic francesca colombo acting...
TRANSCRIPT

OECD REVIEW OF QUALITY OF HEALTH CARERAISING STANDARDS: CZECH REPUBLIC
Francesca Colombo
Acting HeadOECD Health Division25 June 2014

Where is the Czech Republic today?
• Significant progress in improving quality.• Czech Health Services Act (2012) contains
requirements linked to quality of care.• Stakeholders have developed mechanisms to
improve effectiveness, safety and patient-centredness.
• Strong emphasis on preventive health care• Ambitious screening programmes, including one of
the first for colorectal cancer in the world. • More focus on patients’ rights.

But the quality agenda is narrowly oriented and still poorly enforced…
• Only 20% of hospitals report adverse events.
• One-time mandatory hospital accreditation rather than continuous monitoring.
• Lack of incentives to drive quality improvement on the ground
• Uncertain whether current preventive health initiatives are effective and good value for money.
Underpinning all of this -
more effective data collection, analysis and dissemination

A HEALTH SYSTEM THAT HAS MADE GOOD
PROGRESS

Strong improvement in case-fatality rate after a heart attack

… and significant decline in deaths after stroke

A focus on preventive health care and early diagnosis
• Breast cancer screening since 2002.• Cervical cancer screening since
2008• Colorectal cancer screening since
2009 – one of the first in the world.• Bi-annual health checks for all
adults

THE NEXT CHALLENGES TO TACKLE WILL BE…

Population aged over 65 … and % reporting good health
Increasing demands
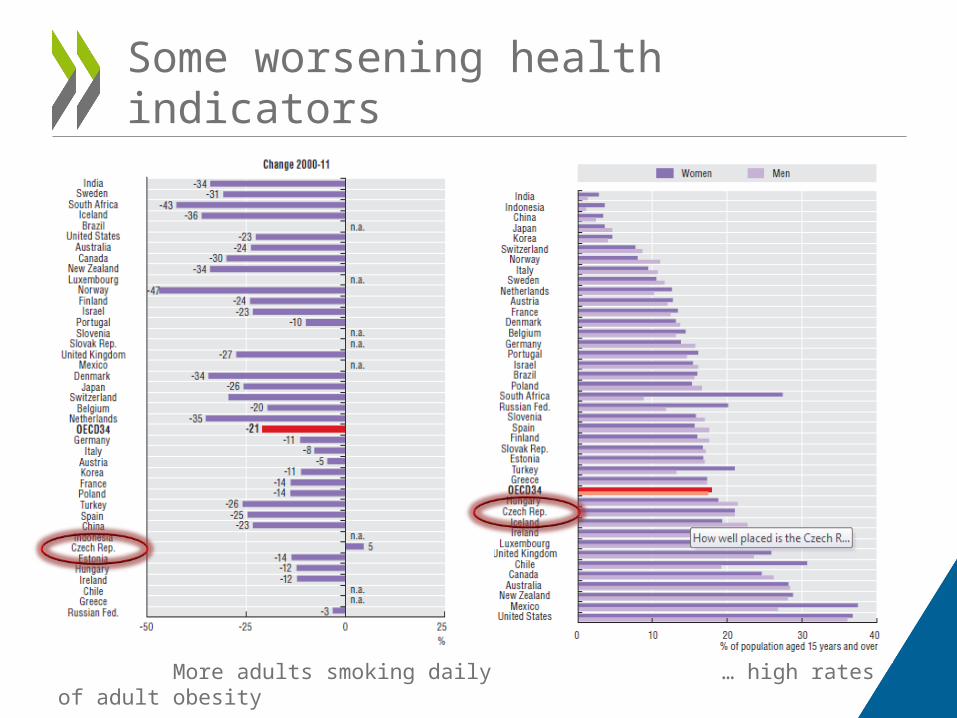
More adults smoking daily … high rates of adult obesity
Some worsening health indicators
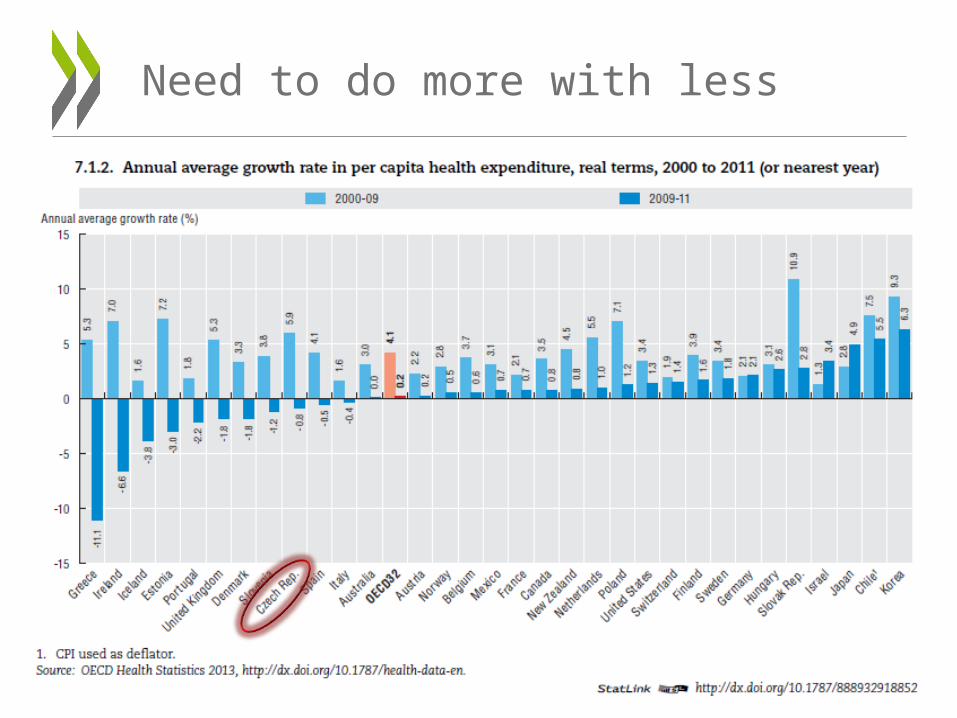
Need to do more with less

… and reduce dependence on the hospital sector

HOW WELL PLACED IS THE CZECH REPUBLIC TO MEET
THESE CHALLENGES ?

Governance:
How well placed is the Czech Republic to meet these challenges?
• The Czech Republic trails other OECD countries in moving towards a systemic and continuous focus on quality of care.
• Governance around quality depends largely on one-time accreditation of minimum standards.
• Lack of a coherent governance structure, many split responsibilities.

Information:
How well placed is the Czech Republic to meet these challenges?
• Data infrastructure is weak and fragmented.
• A substantial amount of information is gathered across the health system, but most of it is used for billing and is focused on volumes of care and resources – not quality.
• The openness of the data infrastructure is low and patients have very limited access to information on performance. This makes it difficult for patients to make informed choices.

• Data is narrowly used. For example, although the Czech Republic has one of the longest-established national cancer registers in the OECD, it is mostly used for epidemiological analysis.
• Data doesn’t yield the full picture because it doesn’t link-up. For example, a much richer assessment of cancer screening programmes could be achieved if clinical outcomes in the cancer register were linked to screening histories.
• Important data gaps persist. For example, there is a national register for type I diabetes, but not for the much more common type II diabetes.
Examples of weaknesses in the information infrastructure

Services:
How well placed is the Czech Republic to meet these challenges?
• Primary prevention efforts are failing.
• Prevention efforts and programmes for people with diabetes need to be strengthened.
• Cancer screening remains opportunistic, rather than population-based.

• High avoidable hospital admissions – High diabetes hospitalisation rate of 221 per
100,000 population (OECD 164.4 per 100,000). – Asthma and COPD hospital admissions lower than
OECD average.
• Care is not always patient centred – 97.2% of patients report doctors spend enough
time with them during consultations, and 94% report doctors give an opportunity to ask questions.
– BUT only 81.8% report doctor involves patient in decision making (OECD 86.1%)
Primary care seems weak
• Significant risk factors: Obesity– Adult obesity rose from 14% in 2000 to 21% in 2011,
and is higher than the OECD average of 17.2%. – Overweight and obesity among Czech 15-year-olds
rose from 9% to 15%.
• Smoking rates are rising, contrary to other OECD
– Daily adult tobacco consumption increased by 5% between 2000 and 2011, compared to an OECD average reduction of 21%.
– 24.6% of Czech adults smoke daily, compared to 20.9% across the OECD.
Programs to prevent chronic disease don’t appear to be effective

Cervical cancer screening is low in women aged 20 to 69
Source: OECD Health Statistics 2013, http://dx.doi.org/10.1787/health-data-en.

• Prevalence in Czech Republic of 8%, compared to OECD average of 6.9%.
• Burden of disease rising with increasing rates of obesity and ageing population.
• Mortality and some complication rates have fallen, but diabetic retinopathy incidence rising.
Mixed outcomes on diabetes care

WHAT THE CZECH REPUBLIC COULD DO…

•Shift from the current emphasis on ensuring basic minimum standards are met, to continuous monitoring and improvement
•Shift from a voluntary approach to quality assurance, to an approach underpinned by tougher requirements and stronger incentives
•Open up quality and performance data to the public scrutiny
Improve quality-based governance

• Streamline whilst developing the data infrastructure - to make it less fragmented and enable more data sharing.
• Produce more sophisticated analyses giving a detailed picture of health needs and outcomes, to inform the policy-making process.
• Ensure analysis and reporting is patient-oriented as well
Strengthen data collection, analysis and dissemination

• Promote the role of primary care professionals in co-ordinating care for patients with diabetes, by giving GPs incentives and training to take on more complex patients.
• Establish a patient register for type 2 diabetes, and strengthen the existing type 1 and gestational diabetes registers.
• Explore the introduction of Disease Management Programmes to promote well co-ordinated care.
Strengthen primary care in diabetes management

Encourage GPs to adopt a leading role in assuring quality and outcomes
Coordination
GovernanceInformation

• Move to a population-based cancer screening program. Particular attention should be paid to screening rates of socially disadvantaged people.
• Place an emphasis on preventive health, particularly aimed at children.
• Evaluate its comprehensive health check, and abandon it if it is not good value for money.
• Link screening data to clinical outcomes to gain a richer picture of gaps in coverage.
Improve screening and prevention

TO CONCLUDE…

Key policy recommendations
1. Shift governance toward continuous quality improvement.
2. Strengthen data collection, analysis and reporting.
3. Promote prevention of chronic disease.
4. Give primary care practitioners incentives to manage complex patients.
30
OECD Reviews of Health Care QualityOECD Reviews of Health Care Qualitywww.oecd.org/health/qualityreviews

Contact: [email protected]
Read more about our work Follow us on Twitter: @OECD_Social
Website: www.oecd.org/health
Newsletter: http://www.oecd.org/health/update
Thank you