october 12, 2010 approval code: in1070 ingenix insite user group
TRANSCRIPT

October 12, 2010
Approval Code: IN1070
Ingenix InSite User
Group

© Ingenix, Inc. 2
Ingenix InSite User Group: Welcome
Administrative Reminders: This call is hosted in a listen only mode for participants until our Q&A
segment. Questions you may want to ask prior to the Q&A segment can be typed in
our chat panel for the host to address Please keep your phones on mute during Q&A.
The webex login password for this call is ‘insite’. When logging into the webex please enter in your first and last name. The user group presentation materials will be sent with the meeting minutes. Ingenix InSite User Group Questions or Product Enhancement requests?
Email [email protected]. Ingenix InSite Website Questions? Call or email the Ingenix Helpdesk 1-866-
818-7503 or [email protected].
© Ingenix, Inc. 3
Ingenix InSite User Group: Agenda
10:00 AM – 10:05 AM Welcome 10:05 AM – 10:10 AM InSite Operations Announcements 10:10 AM – 10:20 AM Report Selection Tool 10:20 AM – 10:30 AM Changes to the CMS-HCC Payment Model and Impact on RAF 10:30 AM – 10:45 AM Focus on: Peripheral Vascular (Arterial) Disease 10:45 AM – 11:00 AM Q & A

InSite Operations Announcements
Presented BySusan RickInSite Business Operations Manager
© Ingenix, Inc. 5
InSite Operations Announcements
Data Refresh Update– InSite Mid-month data refreshed September 20th
• Data refresh may not impact all InSite users• Mid-month data refresh will not replace the normal monthly data
refresh– Next monthly data refresh is targeted for October 18th
October 8th, 2010 – InSite Updates– October Ingenix Insider
– Report Selection Tool

InSite Report Selection Tool
Presented By Francesca SicilianoInSite Business Analyst

© Ingenix, Inc. 7
InSite Report Selection Tool
Report Selection Tool

Changes to CMS-HCC Payment Model for 2011 and Impact on RAF
Presented By Loren Maddy Director, Analytics

© Ingenix, Inc. 9
Overview
Medicare Advantage Reimbursement is a Function of Bid (Ratebook) and RAF
– Estimated 2011 Net Impact: -1.6%• Ratebook:
– No Ratebook changes for 2011• RAF:
– Impact of CMS Changes on Otherwise Equal RAF is -1.6%
» FFS Normalization: -1.6%» No other CMS changes for 2011 Pmt
Yr
© Ingenix, Inc. 10
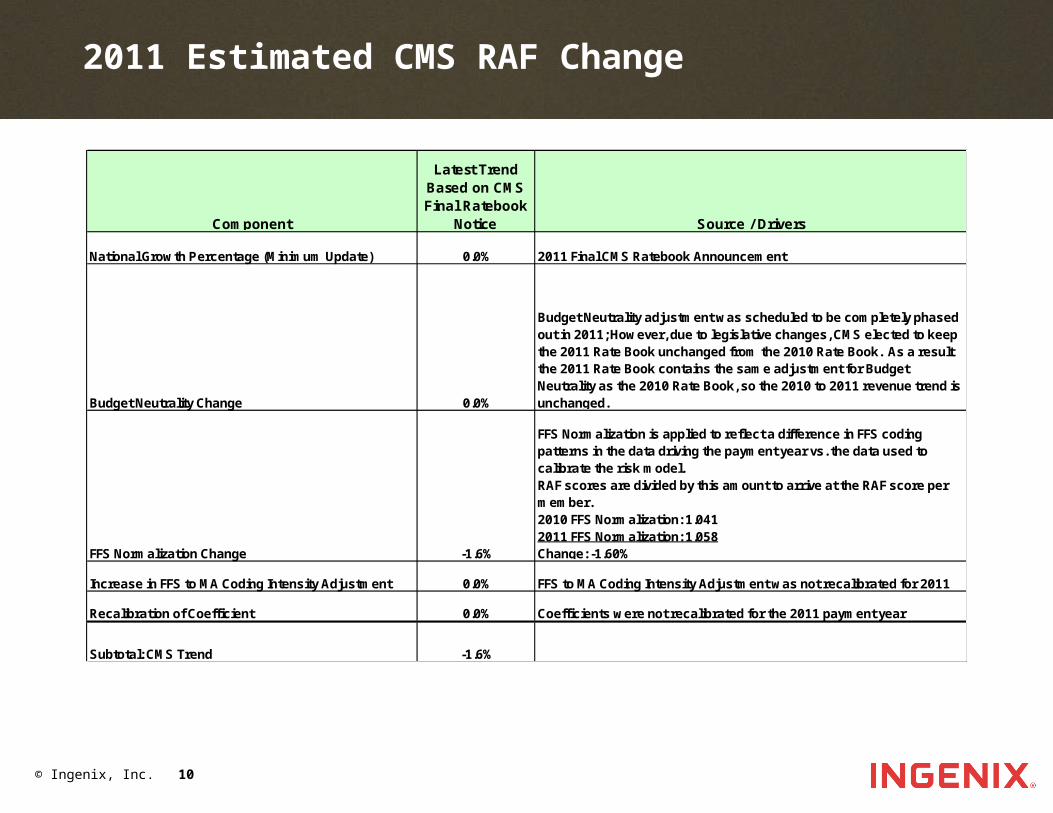
2011 Estimated CMS RAF Change
Component
Latest Trend Based on CMS Final Ratebook
Notice Source / Drivers
National Growth Percentage (Minimum Update) 0.0% 2011 Final CMS Ratebook Announcement
Budget Neutrality Change 0.0%
Budget Neutrality adjustment was scheduled to be completely phased out in 2011; However, due to legislative changes, CMS elected to keep the 2011 Rate Book unchanged from the 2010 Rate Book. As a result the 2011 Rate Book contains the same adjustment for Budget Neutrality as the 2010 Rate Book, so the 2010 to 2011 revenue trend is unchanged.
FFS Normalization Change -1.6%
FFS Normalization is applied to reflect a difference in FFS coding patterns in the data driving the payment year vs. the data used to calibrate the risk model.RAF scores are divided by this amount to arrive at the RAF score per member.2010 FFS Normalization: 1.0412011 FFS Normalization: 1.058Change: -1.60%
Increase in FFS to MA Coding Intensity Adjustment 0.0% FFS to MA Coding Intensity Adjustment was not recalibrated for 2011
Recalibration of Coefficient 0.0% Coefficients were not recalibrated for the 2011 payment year
Subtotal: CMS Trend -1.6%

© Ingenix, Inc. 11
Impact of CMS Changes on RAF: FFS Normalization & MA Coding Pattern Differences
2008 Pmt Yr 2009 Pmt Yr 2010 Pmt Yr 2011 Pmt Yr
Age/Sex RAF component1 0.520 0.517 0.517 0.517
Special Status RAF component1 0.202 0.166 0.166 0.166
CHF (HCC 080) 0.395 0.410 0.410 0.410 Vascular Disease (HCC 105) 0.324 0.316 0.316 0.316 COPD (HCC 108) 0.398 0.399 0.399 0.399 CHF/COPD Interaction 0.216 0.219 0.219 0.219
HCC RAF component 1.333 1.344 1.344 1.344
Total RAF 2.055 2.027 2.027 2.027
FFS Normalization factor 1.040 1.030 1.041 1.058 FFS to MA Coding Intensity Adj % - - -3.41% -3.41%
Adjusted Total RAF 1.976 1.968 1.881 1.851
1Assumes member is a 75 year old Community male w ho is Medicaid eligible
New ICD-9 Codes added to CMS-HCC Payment Model
Presented By Pam Holt Manager, SoCal Market Consultation
© Ingenix, Inc. 13
CMS Announces New Codes for Model
On October 1st each year, new ICD-9 codes are effective
CMS evaluates which codes will be included in the CMS-HCC and Rx Models
CMS posted a new crosswalk including new codes effective Oct 1st
8 codes were added to the CMS-HCC model
https://www.cms.gov/MedicareAdvtgSpecRateStats/06_Risk_adjustment.asp
– Zip File Name: “2011 Model Diagnoses”– File Name: “Risk Model Diagnoses for 2011.xls”

Mary Jo Groome, CCS-P, CPC-HSr. Provider Training & Development Consultant
Peripheral Vascular (Arterial) Disease
© Ingenix, Inc. 15
What is Peripheral Artery Disease (P.A.D.)?
P.A.D. occurs when plaque builds up in the arteries that carry blood to your head, organs, and limbs. Plaque is made up of a fat, cholesterol, calcium, fibrous tissue and other substances in the blood.
When plaque builds up in the arteries, the condition is called atherosclerosis. Over time, plaque can harden and narrow the arteries. This limits the flow of oxygen-rich blood to the organs and other parts of the body.
P.A.D. usually affects the legs, but also can affect the arteries that carry blood from the heart to the head, arms, kidneys and stomach.
Today’s comments will focus on P.A.D. that affects blood flow to the legs.

© Ingenix, Inc. 16
Peripheral Arterial Disease (PAD)
Clinical description of PAD Present in approximately 8 to 12 million individuals in the
U.S. Estimated to be present in 29% of those
– Age 70 or over; or– Age 50 to 69 with a history of smoking 10 pack years or those
with diabetes.1
History and physical examination may not be reliable for the detection of lower extremity PAD8
– Presents with classic claudication 10% to 35% of cases– Many individuals have no symptoms or non-classic
symptoms– Poor recognition (under-diagnosis) results in under-
treatment (estimated only 25% of those with PAD are treated)2

© Ingenix, Inc. 17
Peripheral Arterial Disease (PAD)
Clinical description of PAD Often caused by atherosclerosis Identifies risk for myocardial infarction
(also referred to as a heart attack) and stroke3
Causes poor blood supply to extremities
Symptoms worsen when demand increases (exercise)
As disease progresses, less exercise causes symptoms; if severe – symptoms at rest (with no movement)
May result in pain (disability), skin and tissue damage (ulcers) and infection (gangrene)
Can worsen diabetic complications such as slow healing foot ulcers
© Ingenix, Inc. 18
Peripheral Vascular (Arterial) Disease
PAD Facts:
Most major cardiovascular events occur in those without a prior diagnosis of vascular disease.
Over 50% with PAD will not have previous vascular symptoms; 40% have atypical symptoms.
It is estimated that only 25% of afflicted individuals receive care

© Ingenix, Inc. 19
There are two types of PAD
– Arteriosclerotic: Involves medium to large vessels and is amenable to bypass.
– Diabetic: Involves medium to small vessels and is not typically helped by bypass.
Workup can be done by Ankle Brachial Index (ABI)
– Can be used to diagnose PAD and can be performed in any doctor’s office
– Reveals a comparison of the systolic blood pressure between the lower and upper extremities and is measured using a Doppler.
– An ABI of less than or equal to 0.90 is abnormal and is considered evidence of lower extremity PAD.
• Prompt investigation and risk-reducing treatments are then warranted
Peripheral Vascular (Arterial) Disease
© Ingenix, Inc. 20
Peripheral arterial disease, peripheral vascular disease, and claudication are coded to 443.9
– It is important to note that this code excludes atherosclerosis of the arteries of the extremities.
Atherosclerosis of native arteries of the extremities, Category 440, is further classified as such:
– With intermittent claudication 440.21– With rest pain 440.22– With ulceration 440.23 (see ulcer coding rules)– With gangrene 440.24 (see ulcer coding rules)– Unspecified 440.20
Documentation & Coding PAD / PVD
© Ingenix, Inc. 21
Diagnostic statements that do not impact severity adjustment as theyare coded to:
440.9: Generalized and unspecified atherosclerosis
– Arteriosclerotic (vascular) disease– Generalized arteriosclerosis– Arteriosclerotic endarteritis– Arteriosclerosis obliterans– Arteriosclerosis with calcification
PAD Documentation & Coding

© Ingenix, Inc. 22
Vascular diseases often occur as a manifestation of diabetes: Diabetic Peripheral Circulatory Disorders
250.70-250.73
– If the PVD is due to diabetes mellitus, codes 250.7x and 443.81 would be assigned.
– The specificity of the PVD changes to 443.81, Peripheral Angiopathy in diabetes mellitus.
– Code 443.81 provides a more comprehensive picture of the patient’s PAD/PVD condition in regard to DM as an underlying cause.
– Provide the appropriate linkage for the diabetes with Peripheral Circulatory Manifestations (250.7x)
American Hospital Association, AHA Coding Clinic for ICD-9-CM. 3rd Qtr. 1991. p. 10World Health Organization, 2009 Ingenix ICD-9-CM Professional for Physicians, Volumes 1&2. 6th ed.
2008. pp. 8&27
Documentation & Coding PAD / PVD

© Ingenix, Inc. 23
Underlying Disease – Diabetes Mellitus
A patient with Type II controlled Diabetes that has treatment for a manifestation of the disease should have both conditions coded:
– PVD due to Diabetes Mellitus• 250.70 Diabetes with peripheral circulatory disorder• 443.81 Peripheral angiopathy in disease classified
elsewhere The underlying disease is coded first, followed by the
manifestation code. The linkage has been documented with “due to” and
the 4th digit is properly assigned on the 250.

© Ingenix, Inc. 24
Peripheral Vascular diseases as a result of atherosclerosis of extremities: Atherosclerosis of Native arteries of the Extremities
(440.2 subcategory).
– For coding purposes, the physician must document that the PVD is due to atherosclerosis (ASPVD) before a code from 440.2 may be assigned.
– In fact, Coding Clinic advises to query the physician for further specification if the physician documents vague diagnoses as peripheral vascular disease or intermittent claudication.
American Hospital Association, AHA Coding Clinic for ICD-9-CM. 4th Qtr. 1992. p. 25
3M Health Information Systems (2008, April). Coding for peripheral vascular disease. In, For The Record, Vol. 20 No.8 P. 28. Retrieved March 10, 2009 from: http://www.fortherecordmag.com/archives/ftr_04142008p28.shtml
PAD Diagnosis Coding
© Ingenix, Inc. 25
Peripheral Vascular diseases as a result of atherosclerosis of extremities ICD-9-CM Coding: 440.2 (Atherosclerosis of Native Arteries of the Extremities)
– 440.20 Atherosclerosis of extremities, unspecified– 440.21 Atherosclerosis of extremities w/ intermittent claudication– 440.22 Atherosclerosis of extremities w/ rest pain– 440.23 Atherosclerosis of extremities w/ gangrene– 440.24 Atherosclerosis of extremities w/ ulceration
443 category (Other Peripheral Vascular Disease) - Without additional documentation regarding the type or manifestationof PVD/PAD, code 443.9 would be assigned.
– 443.9 Peripheral Vascular Disease, unspecified
PAD Diagnosis Coding

© Ingenix, Inc. 26
When Assigning Atherosclerosis of Arteries of the Extremities (440 Category)
All patients documented as atherosclerosis with gangrene are coded to 440.24
– If gangrene is documented without mention of atherosclerosis, only code 785.4
All patients documented as atherosclerosis without gangrene, but with ulceration are coded to 440.23 *
– If ulceration is documented without mention of atherosclerosis, only code 707.9
Patients documented as atherosclerosis with neither gangrene nor ulceration, but with rest pain are coded to 440.22
– If rest pain is documented without mention of atherosclerosis, only code 729.5
Patients documented as atherosclerosis with intermittent claudication due to atherosclerosis are coded to 440.21
– If claudication is documented without mention of atherosclerosis, only code 443.9
Rules of Coding PAD / PVD
* Ulcers: Codes from subcategory 707.1x (Ulcer of lower limb) should be assigned in addition to 440.23
© Ingenix, Inc. 27
Rules of Coding PAD / PVD: Ischemic Ulcers
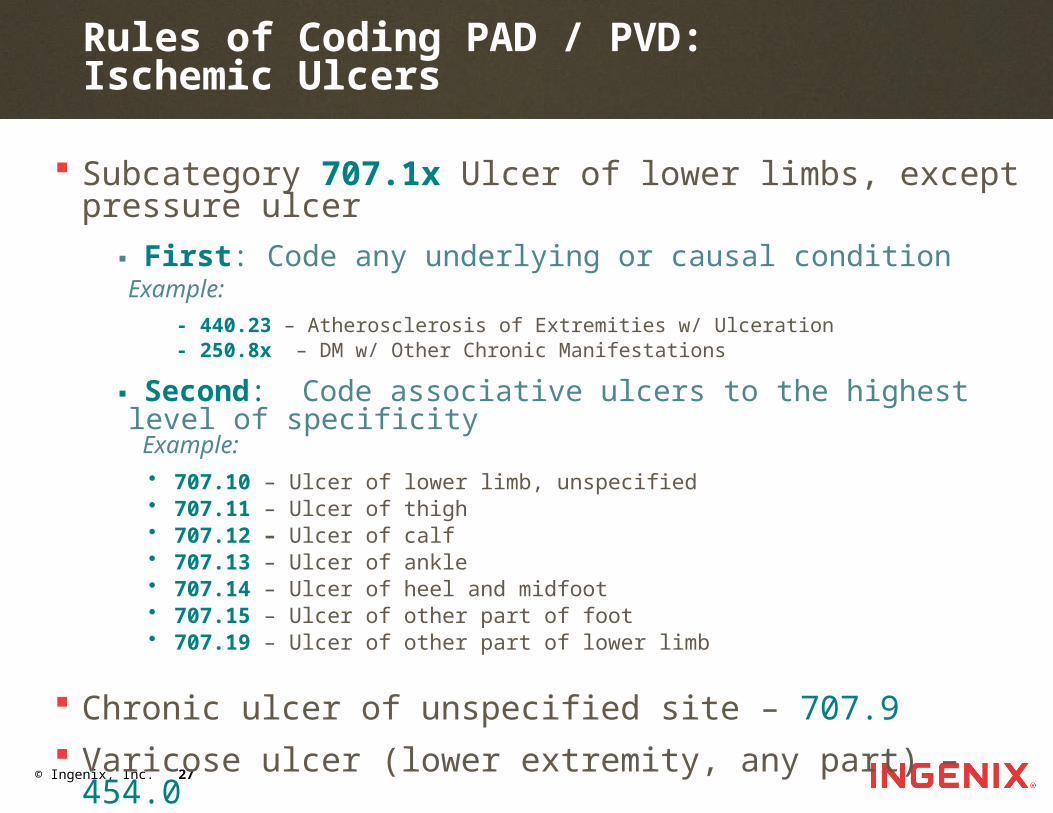
Subcategory 707.1x Ulcer of lower limbs, exceptpressure ulcer
▪ First: Code any underlying or causal conditionExample:
- 440.23 – Atherosclerosis of Extremities w/ Ulceration - 250.8x – DM w/ Other Chronic Manifestations
▪ Second: Code associative ulcers to the highest level of specificity Example:
• 707.10 – Ulcer of lower limb, unspecified• 707.11 – Ulcer of thigh• 707.12 – Ulcer of calf• 707.13 – Ulcer of ankle• 707.14 – Ulcer of heel and midfoot• 707.15 – Ulcer of other part of foot• 707.19 – Ulcer of other part of lower limb
Chronic ulcer of unspecified site – 707.9
Varicose ulcer (lower extremity, any part) – 454.0

© Ingenix, Inc. 28
Exam: S1S2 no murmur or gallop with regular rhythm. Radial pulses 2+. Feet cool with left pedal faint and absent rt pedal pulse. No edema. Hemosiderin stain of both anterior LE.
Dx: 443.9 A/P Stable PVD.
Comments: “Stable PVD.” represents a definitive diagnosis. This is correct coding.
Clinical Example
© Ingenix, Inc. 29
HISTORY OF PRESENT ILLNESS: L ankle wound: Had ankle fx 12/07, with small open area on medial aspect of her ankle that heals over and then reopens.
REVIEW OF SYSTEMS VASCULAR: ULCER: Inner left malleolus has non-healing wound. POSITIVE FOR: Ulcer
PHYSICAL EXAM VASCULAR: 1+ pedal pulse on R. Foot warm w/sensation. No reddened or open areas.
Clinical Example
© Ingenix, Inc. 30
ASSESSMENT AND PLAN Diagnosis : 440.23 - Atherosclerosis of native arteries
of the extremities with ulceration – Treatment Plan : STATUS: Has open area on inner aspect of
left malleolus. very difficult to heal with probable osteomyelitis. Will continue wound healing measures and conservative interventions if wound worsens.
Diagnosis : 707.13 - Ulcer of ankle – Treatment Plan : STATUS: Chronic, PLAN: Had ankle fracture
12'07. has had an open area on the medial aspect of her left ankle that heals over, opens up, heals over, etc. 6'08 has open area 1 cm that has a pinpoint hole in the center. a shiny metal piece is visible which is probably a plate or screw that was used to fix the ankle fracture. xray ordered to r/o osteo.
Clinical Example
© Ingenix, Inc. 31
Comments:
ROS documentation states: VASCULAR: ULCER: Inner left malleolus has non-healing wound. POSITIVE FOR: Ulcer
Is this an ulcer or a non-healing surgical wound?
– The code for ulcer of the ankle is 707.13. It maps to HCC 149 with a RAF of 0.241.
– The code for non-healing surgical wound is 998.83. It does not risk adjust.
Clinical Example

© Ingenix, Inc. 32
Atherosclerosis is never mentioned in the documentation. In order to code 440.23 - Atherosclerosis of native arteries of the extremities with ulceration, the documentation must state atherosclerosis, ASPVD or atherosclerotic PVD, etc.
– 440.23 maps to HCC 104 with a RAF of 0.482.
An argument could be made that the documentation does not support the codes reported.
According to the documentation, the correct codes for this scenario would be 998.83, and 443.9.
– 998.83 does not risk adjust.– 443.9 maps to HCC 105 with a RAF of 0.165.
Specific documentation can make a big difference!
Clinical Example

© Ingenix, Inc. 33
References
1 Hirsch, A.T., et al. Peripheral Artery Disease Detection , Awareness, and Treatment in Primary Care. JAMA; Sept 19 2001; 286(11):1317-24
2 Bhatt DL, Steg PG, Ohman EM, Hirsch AT, Ikeda Y, Mas JL, Goto S, Liau CS, Richard AJ, Rother J, Wilson PW; REACH Registry Investigators. International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis. JAMA. 2006;295:180–189
3 Hirsch, A.T., et al. (October 2005). ACC/AHA Practice Guidelines. Journal of the American College of Cardiology, 2006; 47; e1-e192, Retrieved February 12, 2009, from http://content.onlinejacc.org/cgi/content/full/47/6/e1
4 Hiatt, WR. Medical Treatment of Peripheral Arterial Disease and Claudication. N Engl J Med 2001; 344:1608
5 McDermott, MM, Kerwin, DR, Liu, K, et al. Prevalence and significance of unrecognized lower extremity peripheral arterial disease in general medical practice. J Gen Intern Med 2001; 16:384
6 Norgren, L, Hiatt, WR, Dormandy, JA, et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASCII). J Vasc Surgery 2007; 45: Suppl S:S5
7 "Executive Summary: Standards of medical care in diabetes—2009". Diabetes Care 32: S6–S12. 2009.
8 PAD Peripheral Arterial Disease. March 22, 2010. <www.padcoalition.org>.
© Ingenix, Inc. 34
Future InSite Coding Topics:
◘ November -Diabetes, Linda Farrington, CPC, CPC-I
◘ December- Ulcers, Mary Jo Groome, CCS-P, CPC-H

© Ingenix, Inc. 35
User Group Feedback Survey
We want your feedback!
Survey is to be sent immediately after this call

© Ingenix, Inc. 36
Question and Answer