occupational exposures and the co-occurrence of work ... · occupational exposures and the...
TRANSCRIPT

Occupational Exposures and the Co-Occurrence of Work-Related Skin and Respiratory Symptoms
by
Victoria Helen Arrandale
A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy
Institute of Medical Science
University of Toronto
© Copyright by Victoria Helen Arrandale (2012)

ii
Occupational Exposures and the Co-Occurrence of Work-
Related Skin and Respiratory Symptoms
Victoria Helen Arrandale
Doctor of Philosophy
Institute of Medical Science
University of Toronto
2012
Abstract
Occupational skin and respiratory symptoms, and disease, are common problems. Workers
can develop new disease or aggravate existing disease as a result of exposures at work.
Many workers are exposed to chemicals that can cause both respiratory and skin responses
and there is evidence that some workers experience symptoms in both systems. There is
also evidence that skin exposure may lead to sensitization and the development of
respiratory disease. There is very little research that has examined both airborne and skin
exposures together with lung and skin outcomes. The purpose of this thesis was to further
investigate the relationships between occupational exposures, skin symptoms and disease,
and respiratory symptoms and disease. Four studies were undertaken to improve our
understanding of these complex relationships. Results from a study of clinical patch test
data determined that seven of the ten most common occupational contact allergens are also
capable of causing occupational asthma and that these common occupational exposures
may not be recognized as sensitizers in common reference materials. Exposure-response
relationships for skin symptoms were modeled in bakery workers and auto body shop
workers using historical data; significant exposure-response relationships were found for
auto body workers. In two separate studies of concurrent skin and respiratory symptoms,

iii
workers did report concurrent skin and respiratory symptoms. In predictive models, subjects
reporting a history of eczema were more likely to report concurrent skin and respiratory
symptoms. Overall, the results from this thesis provide more evidence that the skin and
respiratory systems are associated. This body of work suggests that: (1) several common
occupational exposures can cause disease in both the skin and respiratory system; (2) a
portion of workers report both skin and respiratory symptoms; and (3) exposure-response
relationships do exist for skin symptoms, both work-related and non-work-related. Future
studies need to gather detailed information about exposure and response in both systems in
order to better determine the role of exposure(s) in the development of skin and respiratory
symptoms. Improved understanding of these relationships will allow for more targeted and
effective exposure prevention strategies and will ultimately reduce the burden of
occupational disease.

iv
Acknowledgments
First and foremost I would like to thank my committee members, Dr. Jeremy Scott, Dr.
Susan Tarlo, Dr. Frances Silverman and especially Dr. Linn Holness for their support,
guidance and feedback throughout his process.
I would like to extend thanks to Dr. Dick Heederik for his warm welcome in Utrecht, The
Netherlands, and for allowing me to explore the occupational data that his group has
collected. I am also very thankful to Dr. Carrie Redlich and Dr. Allen Kraut for their
feedback on several key aspects of this thesis.
I must thank the staff at the St Michael’s Hospital Occupational Health Clinic for their help
in data collection, especially their sense of humour when things didn’t go exactly as
planned. I’m also grateful to the staff at the Gage Occupational and Environmental Health
Unit, my academic home for the last five years.
I would also like to thank the Massey College community that has served as my home away
from home. I am forever grateful for the friendships that I know will endure, and the
memories that I will carry with me.
I am grateful to the North American Contact Dermatitis Group (NACDG) for providing
data access and both the Research Advisory Council of the Ontario Workplace Safety and
Insurance Board as well as the Workers’ Compensation Board of Manitoba for providing
operating grant support for the research studies.
Both the Canadian Institutes of Health Research and the Centre for Research Expertise in
Occupational Disease supported my stipend and this financial support made this thesis
possible.
I would also like to thank Nigel, Carole and Samantha. We may have rendezvoused in San
Francisco, New York, and Paris but nothing beats being together, fireside, at 1088. And
finally, thank you to Taylor for your patience, love and fierce editing skills.

v
Table of Contents
Acknowledgments.......................................................................................................................... iv
Table of Contents ............................................................................................................................ v
List of Abbreviations ...................................................................................................................... x
List of Tables ................................................................................................................................ xv
List of Figures ............................................................................................................................ xviii
List of Appendices ....................................................................................................................... xix
Chapter 1 Literature Review.................................................................................................... 1
1.1 Background ......................................................................................................................... 1
1.2 Asthma ................................................................................................................................ 1
1.2.1 Work-Related Asthma (WRA) ............................................................................... 2
1.2.2 Diagnosis of WRA.................................................................................................. 3
1.2.3 Prevalence of WRA ................................................................................................ 4
1.2.4 Causes of WRA....................................................................................................... 6
1.2.5 Epidemiological Evidence: Relationship Between Symptoms and
Disease .................................................................................................................... 8
1.3 Contact Dermatitis .............................................................................................................. 9
1.3.1 Occupational Contact Dermatitis (OCD)................................................................ 9
1.3.2 Diagnosis of OCD................................................................................................. 10
1.3.3 Prevalence of OCD ............................................................................................... 10
1.3.4 Causes of OCD ..................................................................................................... 11
1.3.5 Epidemiological Evidence: Relationship between Symptoms and Disease ......... 13
1.4 Occupational Exposure ..................................................................................................... 15
1.4.1 Exposure-Response Relationships ........................................................................ 16
1.5 Connecting the Skin and Respiratory Systems ................................................................. 18
1.5.1 Occupational Exposure ......................................................................................... 18

vi
1.5.2 Mechanisms of Effect ........................................................................................... 21
1.5.3 Concurrent Skin and Respiratory Disease in Individuals ..................................... 22
1.5.4 Epidemiological Evidence Linking Skin and Respiratory Outcomes................... 24
1.5.5 Possible Cross-System Sensitization .................................................................... 25
1.5.6 Cross-System Interaction in Other Disease Models ............................................. 30
1.5.7 Additional Considerations .................................................................................... 30
1.6 Framework ........................................................................................................................ 32
Chapter 2 Research Aims and Hypotheses............................................................................ 34
2.1 Knowledge Gaps............................................................................................................... 34
2.2 Research Aims .................................................................................................................. 34
2.2.1 Specific Research Aims ........................................................................................ 34
2.3 Hypotheses ........................................................................................................................ 35
Chapter 3 Occupational Contact Allergens: Are They Also Associated With
Occupational Asthma? ............................................................................................................. 38
3.1 Abstract ............................................................................................................................. 39
3.2 Introduction....................................................................................................................... 40
3.3 Methods............................................................................................................................. 41
3.3.1 Diagnosis of Occupational Allergic Contact Dermatitis ...................................... 41
3.3.2 Determination of Occupationally-Relevant Positive Patch Test
Responses.............................................................................................................. 42
3.3.3 Determination of Whether OCAs May Also Cause OA....................................... 42
3.3.4 Determination of Skin Sensitizer Notation Status ................................................ 43
3.4 Results............................................................................................................................... 44
3.4.1 Common Occupational Contact Allergens ........................................................... 44
3.4.2 Occupational Contact Allergens as a Cause of Occupational Asthma ................. 46
3.4.3 Sensitizer Notations .............................................................................................. 47
3.5 Discussion ......................................................................................................................... 48

vii
3.5.1 Limitations ............................................................................................................ 51
Chapter 4 Co-existing Skin and Respiratory Symptoms in Four Occupational
Groups........ .............................................................................................................................. 53
4.1 Abstract ............................................................................................................................. 54
4.2 Introduction....................................................................................................................... 55
4.3 Methods............................................................................................................................. 55
4.4 Results............................................................................................................................... 56
4.5 Discussion ......................................................................................................................... 59
Chapter 5 Skin Symptoms in Bakery and Auto Body Shop Workers: Associations
with Exposure and Respiratory Symptoms .............................................................................. 61
5.1 Abstract ............................................................................................................................. 62
5.2 Introduction....................................................................................................................... 63
5.3 Methods............................................................................................................................. 65
5.3.1 Exposure ............................................................................................................... 65
5.3.2 Specific IgE and Atopy......................................................................................... 66
5.3.3 Symptoms ............................................................................................................. 66
5.3.4 Additional Variables ............................................................................................. 66
5.3.5 Analyses ................................................................................................................ 67
5.4 Results............................................................................................................................... 67
5.5 Discussion ......................................................................................................................... 75
Chapter 6 Skin and Respiratory Symptoms Among Workers with Suspected Work-
Related Disease ........................................................................................................................ 79
6.1 Abstract ............................................................................................................................. 80
6.2 Introduction....................................................................................................................... 81
6.3 Methods............................................................................................................................. 82
6.3.1 Outcome Variables................................................................................................ 83
6.3.2 Predictor Variables................................................................................................ 83

viii
6.3.3 Statistical Analyses ............................................................................................... 84
6.4 Results............................................................................................................................... 84
6.4.1 Concurrent Symptoms .......................................................................................... 89
6.5 Discussion ......................................................................................................................... 90
6.5.1 Limitations ............................................................................................................ 93
6.5.2 Conclusions........................................................................................................... 93
Chapter 7 General Discussion ............................................................................................... 94
7.1 Revisiting Research Aims and Hypotheses ...................................................................... 94
7.2 Methodological Considerations ........................................................................................ 96
7.3 Causes of Occupational Skin and Respiratory Disease .................................................... 99
7.3.1 Surveillance of OCD and OA ............................................................................. 100
7.3.2 Knowledge Translation and Communication ..................................................... 101
7.4 Modeling Exposure-Response Relationships ................................................................. 104
7.5 Workers Do Report Concurrent Skin and Respiratory Symptoms ................................. 105
7.6 Symptom Progression ..................................................................................................... 107
7.7 Predictors of Concurrent Skin and Respiratory Symptoms ............................................ 108
7.7.1 Barrier Function and Concurrent Skin and Respiratory Symptoms ................... 108
7.7.2 Personal Protective Equipment ........................................................................... 109
7.7.3 Smoking .............................................................................................................. 110
7.7.4 Mechanism of Effect........................................................................................... 111
7.8 Strengths & Limitations .................................................................................................. 112
7.8.1 Strengths ............................................................................................................. 112
7.8.2 Limitations .......................................................................................................... 114
7.9 Contribution to the Literature ......................................................................................... 116
Chapter 8 Conclusions......................................................................................................... 119
Chapter 9 Future Directions ................................................................................................ 120

ix
References................................................................................................................................... 124
Appendices.................................................................................................................................. 144
Copyright Acknowledgements.................................................................................................... 181

x
List of Abbreviations
AA Allergy/Asthma
ACD Allergic Contact Dermatitis
ACGIH American Conference of Governmental Industrial Hygiene
AD Atopic Dermatitis
ANOVA Analysis of Variance
AOCD Allergic Occupational Contact Dermatitis
ATS American Thoracic Society
ATSQ American Thoracic Society Questionnaire
BADGE Bisphenol A Diglycidyl Ether
BEI Biological Exposure Indices
BMRC British Medical Research Questionnaire
CD Contact Dermatitis
CI Confidence Intervals
Conc Concurrent
Derm Dermatology
Df Degrees of Freedom
DGEBA Diglycidyl Ether of Bisphenol A
DNCB Dinitrochlorobenzene
DREAM Dermal Exposure Assessment Method

xi
ECCS European Community of Coal and Steel
ECRHS European Community Respiratory Health Survey
EPIDERM Occupational Skin Surveillance (UK)
ESSCA European Surveillance System on Contact Allergies
FEV1 Forced Expiratory Volume in One Second
FROD Finnish Register of Occupational Disease
FVC Forced Vital Capacity
GCV Generalized Cross Validation
HDI Hexamethylene diisocyanate
HDM House Dust Mite
HEMA Hydroxyethyl Methacrylate
HMW High Molecular Weight
HSE Health and Safety Executive (UK)
ICD Irritant Contact Dermatitis
IgE Immunoglobin E
IQR Inter-quartile Range
IUATLD International Union Against Tuberculosis and Lung Disease
kDa Kilodalton
LMW Low Molecular Weight
MDI Methylene Diphenyl Diisocyanate

xii
MRC Medical Research Council
MSDS Material Safety Data Sheet
NACDG North American Contact Dermatitis Group
NCO Isocyanate Functional Group (Nitrogen, Carbon, Oxygen)
NIH National Institutes of Health
NIOSH National Institute of Occupational Safety and Health (USA)
NLM National Library of Medicine
NOCS National Occupational Classification System
NPG NIOSH Pocket Guide to Chemical Hazards
NR Not Reported
NS Not Significant
OA Occupational Asthma
OCA Occupational Contact Allergen
OCD Occupational Contact Dermatitis
OH Occupational Hygiene
OHIP Ontario Health Insurance Plan
OPRA Occupational Physicians Reporting Activity (UK)
OR Odds Ratio
OSD Occupational Skin Disease
PAC Polycyclic Aromatic Compounds

xiii
PPD P-phenylenediamine
PPE Personal Protective Equipment
PPT Positive Patch Test
PR Prevalence Ratio
Pred. Predicted
PT Patch Test
RADS Reactive Airways Dysfunction Syndrome
Resp Respiratory
SABRE Surveillance of Australian Workplace Based Respiratory Events
SAS Statistical Analysis Software (program)
sd Standard Deviation
SEN Sensitizer Notation
Sens Sensitivity
SIC Specific Inhalation Challenge
SLS Sodium Laurel Sulfate
Spec Specificity
Sx Symptom(s)
SWORD Surveillance of Work-Related and Occupational Respiratory Disease (UK)
TDI Toluene Diisocyanate
TEWL Transepidermal Water Loss

xiv
THOR The Health and Occupation Research Network (UK)
TLV Threshold Limit Value
TMA Trimellitic Anhydride
VITAE Video Imaging Technique for Assessing Occupational Skin Exposure
WEA Work-Exacerbated Asthma
WRA Work-Related Asthma
WR Work-Related
WSIB Workplace Safety and Insurance Board (of Ontario)

xv
List of Tables
Table 1 Agents Potentially Causing Work-Related Asthma (WRA)...................................... 7
Table 2 Common Agents Causing Occupational Contact Dermatitis, Both Irritant and
Allergic.. ............................................................................................................................... 13
Table 3 Summary of Literature Investigating the Relationship between Symptom
Reporting and Skin Disease Diagnoses. ............................................................................... 15
Table 4 Correlation Coefficients for the Association Between Skin and Airborne
Exposures in Various Occupational Studies. ........................................................................ 21
Table 5 Exposures Reported in Published Case Studies to Cause Both Occupational
Asthma and Occupational Contact Dermatitis...................................................................... 23
Table 6 Summary of Experimental Animal Studies Demonstrating Skin Exposure
Resulting in Sensitization and an Asthma-like Response on First Inhalation Challenge. .... 27
Table 7 Basic Descriptive Statistics for the Entire Study Population, Subjects with an
Allergic Contact Dermatitis (ACD) Diagnoses and ACD Cases Stratified by
Occupational Relatedness. .................................................................................................... 45
Table 8 Ten Most Common Occupational Contact Allergens (OCAs). ............................... 45
Table 9 Summary of the Ten Most Frequent Occupational Contact Allergens (OCAs)
and the Evidence Linking Each to OA in Asthma in the Workplace and the UK HSE
Asthmagen. ........................................................................................................................... 46
Table 10 Categorization of Whether Each Common Occupational Contact Allergen
(OCA) Has the Potential To Cause OA Based on Reference Sources and Systematic
Literature Review, Where Necessary. .................................................................................. 47
Table 11 Summary of Sensitizer Notations for the Ten Most Common OCAs in
Common Occupational Hygiene Reference Documents. ..................................................... 48

xvi
Table 12 Skin and Respiratory Symptom Group Distribution (Work-Related and Non-
Work-Related) Across Studies and Description of Groups by Age, Sex, Smoking and
Pulmonary Function Variables.. ........................................................................................... 58
Table 13 Demographics and Symptom Frequencies for Both Auto Body Repair and
Bakery Workers. ................................................................................................................... 69
Table 14 Results of Generalized Linear Models Describing the Simple Relationship
Between Exposure, Skin Symptoms, Atopy and Specific IgE. ............................................ 73
Table 15 Prevalence Ratio (PR) of Symptoms per Inter-Quartile Range (IQR) Increase
in Average Exposure............................................................................................................. 74
Table 16 Association Between Skin Symptoms and Respiratory Symptoms in Both
Bakery and Auto Body Repair Workers. .............................................................................. 74
Table 17 Demographic Description of Study Population, Stratified by Subjects Who
Reported Both Skin and Respiratory Symptoms. ................................................................. 86
Table 18 Skin and Respiratory Symptom Prevalence, Stratified by Clinical Stream........... 87
Table 19 Self-Reported Workplace Characteristics, Stratified by Subjects Who
Reported Both Skin and Respiratory Symptoms. ................................................................. 88
Table 20 Self-Reported Workplace Exposures, Stratified by Subjects Who Reported
Both Skin and Respiratory Symptoms.. ................................................................................ 89
Table 21 Multiple Logistic Regression Model Results for Predictors of Reporting
Concurrent Skin and Respiratory Symptom Outcomes. ....................................................... 90
Table 22 Description of Possible Outcome Groups when Considering Both Skin and
Respiratory Symptom Outcomes and their Individual Work-Relatedness. .......................... 98
Table 23 Results of Generalized Linear Models Describing the Simple Relationship
Between Exposure, Respiratory Symptoms, Atopy and Specific IgE. ............................... 148

xvii
Table 24 Comparison Between Participants and Patients Who Refused Study
Participation. ....................................................................................................................... 174
Table 25 Comparison Between Dermatology (Derm) Strem and Asthma/Allergy (AA)
Stream Subjects................................................................................................................... 175
Table 26 Comparison Between Public Insurance Subjects (OHIP) and Workplace
Insurance Subjects (ODSP)................................................................................................. 176
Table 27 Comparison Between Participants and Non-Participants in the Reliability
Testing Study.. .................................................................................................................... 177
Table 28 Test-Retest Reliability Statistics for Workplace Characteristics Questionnaire . 178
Table 29 Test-Retest Reliability Statistics for Workplace Exposure Questionnaire Items.179
Table 30 Multiple Logistic Regression Model Results for Predictors of Reporting
Work-Related Concurrent Skin and Respiratory Symptom Outcomes. ............................. 180

xviii
List of Figures
Figure 1 Schematic Describing the Relationships Between Work-Related Asthma
(WRA), Work-Exacerbated Asthma (WEA) and Occupational Asthma (OA) ...................... 3
Figure 2 A Proposed Framework for Conceptualizing the Connections Between Skin
and Respiratory Symptoms and Disease............................................................................... 33
Figure 3 Auto Body Shop Workers: Associations Between Average Diisocyanate
Exposure and Skin Symptoms, Shown in Smoothed Plots, Stratified by Atopy.. ................ 70
Figure 4 Bakery Workers: Associations Between Average Wheat Exposure and Skin
Symptoms, Shown in Smoothed Plots, Stratified by Atopy ................................................. 71
Figure 5 Flow Chart of Study Progression, Including Sample Sizes at Each Stage. ............ 85
Figure 6 Modified Framework for Conceptualizing the Connections Between Skin and
Respiratory Symptoms in Occupational Disease. ............................................................... 118
Figure 7 Auto Body Shop Workers Associations Between Average Isocyanate Exposure
and Respiratory Symptoms, Shown In Smoothed Plots Stratified by Atopy. .................... 146
Figure 8 Bakery Workers Associations Between Average Wheat Exposure and
Respiratory Symptoms, Shown in Smoothed Plots Stratified by Atopy ............................ 147

xix
List of Appendices
Appendix 1: Supplemental Figures for Chapter 5 “Skin Symptoms in Bakery and Auto
Body Shop Workers: Associations with Exposure and Respiratory Symptoms”............... 145
Appendix 2: Interviewer-Administered Questionnaire for Chapter 6 “Skin and
Respiratory Symptoms Among Workers with Suspected Work-Related Disease.............. 149
Appendix 3: Supplemental Tables for Chapter 6 “Skin and Respiratory Symptoms
Among Workers with Suspected Work-Related Disease ................................................... 173

1
Chapter 1 Literature Review
1.1 Background
Occupational lung disease and occupational skin disease are common problems. Many workers
are exposed to chemicals that are thought to cause respiratory and/or skin responses as a result of
either airborne or skin exposure. Historically, there has been a significant amount of work
focused on individual respiratory or skin outcomes and their association with particular (route
specific) exposures, but there has been very little work done examining both airborne and skin
exposures together with lung and skin outcomes.
This lack of evidence creates a problem for recognition, diagnosis, and prevention of disease.
Clinically, disease in the other system may be under-recognized when workers are assessed by
either skin or respiratory physicians. From a prevention standpoint, opportunities for exposure
control and disease prevention may be missed if research continues to focus only on airborne or
skin exposure.
There is a need to better understand the relationships between skin and airborne exposures,
between skin and respiratory outcomes, and also the complicated relationships between both
routes of exposure and outcomes in both systems.
1.2 Asthma
Asthma is a heterogeneous inflammatory disorder characterized by variable airflow limitation
and/or airway hyper-responsiveness [Holgate. 2008, Lombardo and Balmes. 2000]. The
mechanisms that can cause an asthmatic response are varied: antigen induced hypersensitivity,
pharmacologic effect, nonspecific inflammation and direct irritation of the airways [Lombardo
and Balmes. 2000].
In the general population, approximately 7.7% of adults have asthma [Akinbami et al. 2011]. A
review by Toren and Blanc suggests that between 15-20% of all adult asthma (new-onset and
exacerbation) is attributable to work-place exposures [Toren and Blanc. 2009].

2
1.2.1 Work-Related Asthma (WRA)
Work-related asthma (WRA) is one of the most common occupational lung diseases [Lombardo
and Balmes. 2000]. WRA describes all asthma that is caused or made worse by one’s work.
Under the umbrella of work-related asthma (WRA) there is both occupational asthma (OA) and
work-exacerbated asthma (WEA) [Tarlo et al. 2008].
1.2.1.1 Work-Exacerbated Asthma (WEA)
Workers who have pre-existing asthma (either current, or quiescent) may experience aggravation
of their asthma symptoms, or re-development of asthma, in response to workplace exposures
[Banks and Jalloul. 2007, Goe et al. 2004, Pelissier et al. 2006].
1.2.1.2 Occupational Asthma (OA)
Occupational asthma (OA) can be defined as asthma “due to causes and conditions attributable to
a particular occupational environment and not to stimuli encountered outside the workplace”
[Bernstein et al. 2006b]. Within OA there are two possible mechanisms of response: allergic and
irritant. Allergic and irritant OA differ in latency and mechanism of effect.
1.2.1.2.1 Allergic Occupational Asthma
Allergic asthma is characterized by a latency period between the onset of exposure and the onset
of symptoms, which allows time for the characteristic development of an immunological
response [Bernstein et al. 2006b]. Two types of sensitizers are described as causative agents in
occupational allergic asthma, high and low molecular weight proteins and chemicals [Toren et al.
2000]. High molecular weight biologic proteins (e.g., animal or plant proteins) stimulate the
production of specific IgE antibodies. Some low molecular weight agents (e.g., complex
platinum salts and epoxy compounds) act as haptens, binding with a protein to form an antigen,
and inducing occupational asthma via a specific IgE-mediated mechanism. Other low molecular
weight sensitizers, including diisocyanates and plicatic acid (Western red cedar) act through
mechanisms that are not yet fully understood [Tarlo et al. 2006].
1.2.1.2.2 Irritant Occupational Asthma
Historically, irritant induced asthma was thought to occur after a single exposure to irritant
agents and was described as reactive airways dysfunction syndrome (RADS) [Bernstein et al.

3
2006b, Brooks et al. 1985] but there is increased understanding and recognition of the chronic
lung effects of irritant exposures. There is now consensus that irritant asthma may result from
repeated exposures, and there may also be a latency period between exposure and symptoms in
irritant-induced asthma. Common exposures that can cause RADS include chlorine gas,
anhydrous ammonia and fire smoke [Gautrin et al. 1999]. Lime, welding fumes and hydrochloric
acid are potential causes of irritant induced asthma [Burge et al. 2011].
Figure 1 Schematic Describing the Relationships Between Work-Related Asthma (WRA),
Work-Exacerbated Asthma (WEA) and Occupational Asthma (OA) As Described by Tarlo
et al. [Tarlo et al. 2008]
1.2.2 Diagnosis of WRA
The diagnosis of OA is made based on a combination of work history and clinical evaluation
[Tarlo et al. 2008, Tarlo et al. 1998]. The American College of Chest Physicians Consensus
Statement outlines the following steps in diagnosis [Tarlo et al. 2008]:
1. Confirm Asthma and Onset: Using medical history, reported symptoms, spirometry results,
and medications

4
2. Assess Exposures that Cause/Exacerbate Asthma: Using the occupational history,
environmental history, reported/confirmed allergies, and atopy.
3. Assess Relationship of Asthma to Work: Based on reported symptoms (onset, severity and
timing), physiological findings (peak flows, spirometry, methacholine challenge, specific
inhalation challenge), and results of immunologic tests
4. Decide Whether the Asthma is Primary OA or WEA.
In order to assess the relationship between asthma and work, clinical investigations may use
several diagnostic tools. Repeated peak expiratory flow measures throughout the day (at work
and at home), and over several days, will provide a measure of variability in airflow limitation.
Nonspecific bronchial hyper-responsiveness can be measured using methacholine challenge, and
spirometry can measure standard lung function parameters including the forced expiratory
volume in one second (FEV1). Both spirometry and methacholine challenge can be repeated
before and after a work shift to measure changes over the course of the workday, providing the
subject is still in the workplace and not off due to illness. Where the experimental equipment is
available, the patient can also undergo a specific inhalation challenge (SIC), the gold standard in
the diagnosis of occupational asthma.
In a SIC the patient is exposed to the workplace agent suspected of causing asthma in a
controlled environment. A positive response (i.e., decreased FEV1, decreased peak flow,
classical “asthmatic reaction”) following the exposure confirms it as causative. The limitations of
the SIC include the time and complexity of the testing set-up, but also the fact that only one
exposure can be tested at a time; most workplaces have mixed exposures which can make
identifying the causal exposure via SIC challenging.
1.2.3 Prevalence of WRA
The burden of work-related asthma is difficult to assess. The criteria for compensation differ by
country or region; some regions compensate for work-exacerbated asthma while others do not. In
regions where compensation exists, detailed data are generally collected only for cases that are
accepted for compensation. There are surveillance schemes that collect information on cases of
occupational asthma, but the organization of each scheme differs. Often, participation in

5
surveillance or reporting schemes for occupational asthma (and other occupational diseases) is
voluntary, leading to under-reporting of disease.
In Finland, physicians are required to report any known or suspected occupational diseases to the
Finnish Registry of Occupational Disease (FROD). The requirement for mandatory reporting
makes the FROD one of the best occupational surveillance systems. From 1989-1995, over 2600
cases of OA were reported to FROD, corresponding to a mean annual incidence rate of 17.4
cases per 100,000 workers [Karjalainen et al. 2000, Karjalainen et al. 2000]. The most recent
data available (2002) permits the calculation of an incidence rate for OA of 12.9 cases per
100,000 workers across all industries and occupations [Riihimäki et al. 2004].
In the United Kingdom (UK), chest and occupational physicians voluntarily report cases of
occupational asthma to both SWORD (Surveillance of Work-Related and Occupational
Respiratory Disease) and OPRA (Occupational Physicians Reporting Activity). In 2001 these
schemes were subsumed into a larger program, The Health and Occupational Research Network
(THOR). From 1992-2000, 897 reports of occupational asthma were received; the estimated
average incidence of occupational asthma was 28 cases per million people (men) and 14 cases
per million people (women) [McDonald et al. 2005].
In Australia, the Surveillance of Australian workplace Based Respiratory Events (SABRE) is
voluntary reporting scheme that began 1997 and involves both thoracic and occupational
physicians [Hannaford-Turner et al. 2010]. From June 2001 to December 2008 the New South
Wales region of SABRE received 3856 reports including 89 cases of OA; the majority of reports
were made up by pleural plaques (32%), mesothelioma (24%), diffuse pleural plaques (22%),
asbestosis (10%) and lung cancer (5%). The prevalence of OA can be converted to a rate of 18
cases per million people, based on approximately 4.8 million NSW Australians of working age
[Australian Bureau of Statistics. 2011].
The difference in the population estimates between Finland, the UK and Australia – the Finnish
estimates are an order of magnitude larger than the UK and Australia - is likely due to the
mandatory nature of the Finnish system, compared with the voluntary system in the UK and
Australia.

6
It is also useful to look to population studies that have attempted to estimate the portion of new
onset adult asthma that may be work-related as another measure of the burden of work-related
asthma. Blanc and Toren have comprehensively reviewed reports since 1966 in two successive
publications, one in 1999 and the other in 2009. [Toren and Blanc. 2009, Blanc and Toren.
1999]. The most recent summary included seventeen published studies of adult onset asthma and
estimated the median population attributable fraction (PAR) of all asthma due to occupation to
be 17% [Toren and Blanc. 2009]. This suggests that almost one-fifth of all adult asthma may
occur as a result of occupational exposures.
1.2.4 Causes of WRA
More than 300 causes of OA have been reported around the world [Mapp et al. 2005]. Two
publications stand out for the thoroughness of their summary: the Appendix compiled by Malo
and Chan-Yeung within the text book “Asthma in the Workplace”, edited by Dr. L. I. Bernstein
[Bernstein et al. 2006a] and the publication from van Kampen et al. [van Kampen et al. 2000].
Both provide a thorough list of exposures that have been shown to cause occupational asthma,
including the clinical, symptom and diagnostic information reported in each case. Malo and
Chan-Yeung published an appended version of their list in 2009, which identifies the most
common agents associated with occupational asthma separated into low molecular weight
(LMW) (<5 kDa) and high molecular weight (HMW) (≥5 kDa) antigens.
The common LMW agents include anhydrides, metals, diisocyanates, cleaning agents, wood
dusts, soldering fluxes, pesticides, pharmaceuticals and reactive dyes. HMW agents include
enzymes, cereals, flour, animals and latex [Malo and Chan-Yeung. 2009]. Mapp et al. identify a
similar list, but also include epoxy compounds and persulfate as common workplace sensitizers
that may cause occupational asthma [Mapp et al. 2005]. Mapp also published a more detailed list
that also included the HMW agents of crustacean, arthropods, moulds and plants as well as the
LMW agents anhydrides, aliphatic amines, biocides, fungicides, acrylates, metal working fluids,
perfumes, and general irritants [Mapp. 2001]. Known causes of occupational asthma are
summarized in Table 1 and separated into three categories: LMW, HMW, and Irritant.
Using reported surveillance data, previous studies have attempted to identify which of the known
causes of OA are the most common. The published studies have presented very similar common
causes of OA. Hannaford-Turner et al. reported that the most common agents causing

7
occupational asthma in an Australian surveillance program were flour, diisocyanates, and
solvents [Hannaford-Turner et al. 2010]. In the UK, diisocyanates, flour, wood dust, metals,
solder/colophony, glutaraldehyde, and epoxy were the most common agents reported by
physicians as causing OA [McDonald et al. 2005]. Animals, flour, mites, diisocyanates, and
welding fumes are the five most common causative agents in the Finnish data from 1989-95
[Karjalainen et al. 2000].
Table 1 Agents Potentially Causing Work-Related Asthma (WRA) Based on Peer-
Reviewed Publications [Mapp et al. 2005, Malo and Chan-Yeung. 2009, Mapp. 2001].
LMW HMW Irritant
Acrylates
Aliphatic amines
Anhydrides
Biocides
Cleaning agents
Diisocyanates
Drugs/Pharmaceuticals
Epoxy compounds
Fungicides
Hardeners
Metals
Persulfate
Pesticides
Reactive dyes
Solder fluxes
Synthetic materials
Wood dust or bark
Animal derived allergens
Arthropods
Biological enzymes
Crustaceans, seafood, fish
Moulds
Plants (Latex)
General Irritants
Perfumes

8
1.2.5 Epidemiological Evidence: Relationship Between Symptoms and Disease
There is a detailed body of literature that has examined the inter-relationships between self-
reported symptoms, bronchial hyper-responsiveness, and asthma diagnoses.
One important goal of these studies has been to determine if, and how, population studies can
measure asthma using questionnaire items rather than expensive and time-consuming diagnostic
testing. The result is a better understanding of which symptom questions, or combination of
symptom questions, can serve as a reasonable proxy for an asthma diagnosis among study
subjects. For the most part, these studies have focused on general asthma, and not occupational
asthma.
Among adults in an Australian study physician diagnosis was the gold standard. Self-reported
asthma with a reported attack in the last 12 months had a higher Youden’s index (combination of
sensitivity and specificity) than measured bronchial hyper-reactivity [Jenkins et al. 1996]. In
New Zealand adults, all of self-reported wheeze, wheeze with dyspnea, and wheeze without cold
had better performance (measured as a higher Youden’s Index) than non-specific bronchial
hyper-responsiveness when compared with self-reported doctor-diagnosed asthma [Sistek et al.
2006]. Pekkanen et al. looked at the same symptoms questions in relation to self-reported “ever-
asthma” (not necessarily doctor-diagnosed) in the European Community Respiratory Health
Study (ECRHS) [Pekkanen et al. 2005]. Though results suggested worse performance (lower
Youden’s indices) than Sistek et al., the wheeze questions were still more highly associated with
asthma than measured non-specific bronchial hyper-responsiveness [Pekkanen et al. 2005].
Vandenplas et al. focused on the ability of symptoms to predict occupational asthma (diagnosed
by specific inhalation challenge) and showed that wheezing at work was the strongest single
questionnaire item for predicting occupational asthma [Vandenplas et al. 2005]. This association
between wheeze at work and occupational asthma diagnosis was even stronger when the
population was limited to workers with HMW exposures [Vandenplas et al. 2005].
The research addressing the relationship between questionnaire responses and diagnosis of
asthma provides occupational health and population researchers with a methodological

9
alternative to diagnostic testing, particularly in large studies. This literature also allows for better
understanding of the implications of using a questionnaire tool for identifying subjects with
asthma, or occupational asthma.
1.3 Contact Dermatitis
Contact dermatitis is defined as “an inflammatory skin reaction to direct contact with noxious
agents in our environment” [Lachapelle. 1995]. Clinical contact dermatitis presents as itching,
redness, scaling, erythema, vesiculation, and papulovesicles [Diepgen and Coenraads. 1999].
Causes of contact dermatitis can be grouped into three categories: physical, biological, and
chemical [Lushniak. 2004]. For contact dermatitis to be considered as work-related the exposure
to the causal agent must occur in the workplace. As in the case of occupational asthma there are
two major types of contact dermatitis - irritant and allergic contact dermatitis.
Although the mechanisms underlying the development of allergic contact dermatitis and irritant
contact dermatitis are different, the physical appearances of the two inflammatory responses are
similar in many aspects [Marks et al. 1992]. A number of industrial agents are classified as both
irritants and allergens. Individuals who have underlying atopic dermatitis may also develop
aggravation of their disease related to workplace exposures [Marks et al. 1992].
1.3.1 Occupational Contact Dermatitis (OCD)
1.3.1.1 Allergic Contact Dermatitis (ACD)
Allergic contact dermatitis (ACD) is the result of a delayed, cell-mediated (Type IV)
immunologic response [Kimber et al. 2002]. Similar to allergic asthma, ACD is characterized by
a latency period between the onset of exposure and the onset of symptoms. This latency allows
for the induction of sensitization, prior to the elicitation of the allergic response upon subsequent
exposure [Kimber et al. 2002].
1.3.1.2 Irritant Contact Dermatitis (ICD)
Irritant contact dermatitis (ICD) is the direct toxic effect of a chemical agent on the skin,
following either a single application (e.g., an acute response such as a chemical burn) or repeated
applications [English. 2004].

10
1.3.1.3 Work-Exacerbated Dermatitis
Workers who have a history of atopic dermatitis (AD) may develop aggravation of their
dermatitis from exposure to physical or chemical irritants in the workplace leading to work-
aggravated atopic dermatitis. Unlike WEA, there is very little published research on work
aggravation of atopic dermatitis.
1.3.2 Diagnosis of OCD
The diagnosis of occupational contact dermatitis is based on the occupational exposure history,
the temporal relationships between exposure and disease, physical examination, and patch testing
[Mathias. 1994].
Patch testing is a specialized technique that involves applying a small amount of a chemical with
a known concentration, to the upper back for at least 48 hours [Zug et al. 2009]. The site where
the exposure patch has been placed is occluded for 48 hours, at which time the occlusion is
removed and the skin is examined. The exposure site then remains un-occluded for at least an
additional 24-72 hours, when the skin is examined a second time. The skin responses at both
time points are considered when determining if any reaction has occurred, and whether the
reaction is allergic or irritant. In contrast to specific inhalation challenge in the diagnosis of OA,
which is complicated and can only be completed for one exposure at a time, the use of patch
testing in the diagnosis of contact dermatitis (CD) permits the examination of an individual’s
reactivity to a large number, often 65 or more, agents at one time [Zug et al. 2009].
1.3.3 Prevalence of OCD
As in the case of OA, the population burden of OCD is challenging to estimate. Estimates of
incidence and prevalence are hampered by under-reporting of disease to practitioners, and a lack
of mandatory surveillance schemes in many jurisdictions. Some estimates suggest that
occupational skin disease (not just contact dermatitis) may represent up to 30% of all
occupational disease worldwide [Diepgen and Coenraads. 1999].
Under the mandatory reporting scheme in Finland (FROD) 643 cases of occupational contact
dermatitis (OCD) were reported in 2002 [Riihimäki et al. 2004]. The cases were evenly split
between irritant (313) and allergic (330) CD. The 2002 incidence rate for CD in Finland was

11
estimated at 27.3 cases per 100,000 workers – more than double the rate for OA [Riihimäki et al.
2004].
The Netherlands began a voluntary reporting scheme for occupational skin disease in 2002.
Under this program, 4516 cases of occupational skin disease were reported from 2001-2005;
3603 (80%) of cases reported were contact dermatitis (CD) [Pal et al. 2009]. The mean annual
incidence rate for CD in the Netherlands was 8.7 cases per 100,000 workers [Pal et al. 2009,
United States Department of Labor Bureau of Labor Statistics. 2011].
From 1999-2001 the UK surveillance programs (OPRA, THOR) reported an annual average of
2191 cases of CD reported by dermatologists and 1427 cases by occupational physicians
[McDonald et al. 2006]. McDonald et al. estimate an annual incidence rate of 74 cases per
million for dermatologists, and 510 per million for occupational physicians [McDonald et al.
2006]. A more recent report suggests incidence rates may have decreased; 68 cases per million
among dermatologists and 260 cases per million from occupational physicians [Turner et al.
2007].
Based on studies from the 1990s, Diepgen and Coenraads estimate the annual incidence rate in
most countries to be around 0.5-1.9 cases per 1000 full-time workers, or approximately 50-190
cases per 100,000 workers, significantly higher than even the mandatory surveillance scheme in
Finland [Diepgen and Coenraads. 1999]. As in the case of WRA we see discrepancies between
the reporting schemes with mandatory surveillance programs reporting higher incidence rates
than voluntary programs. But compared with WRA, there is much less research focused on
estimating the population incidence (or prevalence) of occupational contact dermatitis.
1.3.4 Causes of OCD
The surveillance schemes that provide estimates of population incidence of CD can also provide
insight into the most common causal factors. Turner et al. reported the top ten suspected agents
causing CD in EPIDERM and OPRA for 2002-2005 to be latex, soaps/cleansers, wet work,
personal protective equipment (PPE), nickel, preservatives, resin and acrylics, foods,
chromes/chromates, and cobalt [Turner et al. 2007]. This list of common causes of CD is
relatively unchanged from 1996-2001, except for differences with petroleum products, cutting
oils and coolants, solvents and alcohol [McDonald et al. 2006].

12
It is also possible to standardize the diagnostic procedure (patch testing) so that data can be
compared within and between clinical centers. The North American Contact Dermatitis Group
(NACDG) is one consortium that pools patch test results for both occupational and
environmental (non-occupational) patients. Among the thirteen contributing members, the ten
most common occupational patch test positive allergens in 1997-1998 were: nickel, thiuram,
carba mix, formaldehyde, quaternium-15, neomycin, cobalt, thimerosol, bacitracin, and balsam
of Peru [Rietschel et al. 2002].
A similar group, the European Surveillance System on Contact Allergens (ESSCA) has reported
on the common agents in positive patch tests, for all patients, both occupational and non-
occupational across Europe [Uter et al. 2009]. In 2005/2006 the most common contact allergens
resulting in positive patch tested included: fragrance mix, nickel sulfate, cobalt chloride,
potassium dichromate, colophonium, p-phenylenediamine, and formaldehyde, among others
[Uter et al. 2009].
Table 2 summarizes the exposures commonly associated with occupational contact dermatitis,
and demonstrates the troubles when comparing different reporting schemes. The UK surveillance
schemes for CD (THOR, EPIDERM, OPRA) have grouped causal agents in to chemical groups
(likely to ease reporting burden on physicians), while the patch test results from the NACDG are
allergen specific. This prevents direct comparison, but still allows for similarities to be identified
(i.e., rubber chemicals in THOR, EPIDERM and OPRA and thiuram and carba mix in the
NACDG data).

13
Table 2 Common Agents Causing Occupational Contact Dermatitis, Both Irritant and
Allergic. As Reported by Peer-Reviewed Studies as Cited.
NACDG (US)
[Rietschel et al. 2002]
THOR (UK)
[Turner et al. 2007]
EPIDERM and OPRA (UK)
[McDonald et al. 2006]
No Irritants Includes Irritants
Includes Allergens
Carba Mix
Cobalt Chloride
Epoxy Resin
Formaldehyde
Glutaraldehyde
Glyceryl Thioglycolate
Mercaptobenzothiazole
Nickel Sulfate
Potassium Dichromate
Quaternium 15
Thiuram
Chromes/chromates
Cobalt
Foods
Latex materials
Nickel
PPE
Preservative
Resins and acrylics
Soaps/cleansers
Wet work
Cutting oils and coolants
Foods and flour
Nickel
Petroleum and products
Preservatives
Resins and acrylics
Rubber chemicals and
materials
Soaps and cleaners
Solvents and alcohols
Wet work
1.3.5 Epidemiological Evidence: Relationship between Symptoms and Disease
The research examining the relationship between symptoms and skin disease is far less thorough
than the equivalent body of literature relating to respiratory symptoms and disease. The
standardization of questionnaire items is also, arguably, less advanced than in studies of
respiratory health. There are a few studies that have specifically addressed the relationships
between reported symptoms and doctor-diagnosed skin disease; these studies are summarized in
Table 3.
Svensson et al. found that asking patients if they had hand eczema had better sensitivity and
specificity than asking about specific skin symptoms (fissures, scaling, vesicles, papules,
erythema) when compared with the gold standard of dermatologist examination and diagnosis
[Svensson et al. 2002]. A study of hand dermatitis in nurses showed high sensitivity and
specificity for both a symptom questionnaire-based diagnosis as well as a self-reported diagnosis
when compared with the gold standard of physician diagnosis [Smit and Coenraads. 1993].

14
In an occupational setting, Meding et al. compared self-reported hand eczema with doctor-
diagnosed hand eczema among car mechanics, dentists, and office workers and found similar
sensitivities (range 53-59%) and specificities (range 96-99%) across the three groups [Meding
and Barregard. 2001]. However in another occupational study Carstensen et al. found lower
sensitivities (range 22-33%) and specificities (range 76-89%) for both self-reported diagnosis
and symptom based diagnosis when compared with doctor diagnosis [Carstensen et al. 2006].
The lack of consistent results in the use of questionnaire-based diagnoses when compared with
physician diagnosis may be partly due to the lack of a standardized questionnaire for skin
symptoms. Independently, Vermeulen et al. and Carstensen et al. noted that the differences in
occupational environments may also require that skin symptom questionnaires be validated in the
specific occupational setting prior to large-scale epidemiological use [Carstensen et al. 2006,
Vermeulen et al. 2000]. It may also be partly due to the number of terms used to describe skin
conditions: eczema, hand dermatitis, atopic dermatitis, skin rash, and others. More information
on the study population, as well as more detailed and/or self-explanatory questions may help to
clarify the relationship of skin symptom reporting to specific diagnoses. And, as the examination
by a dermatologist is more straightforward and less labour intensive than spirometry and specific
inhalation challenges, this task should be less daunting than the work already completed in
respiratory epidemiology.

15
Table 3 Summary of Literature Investigating the Relationship between Symptom
Reporting and Skin Disease Diagnoses.
Population Ref Gold Standard Outcome Sen Spec
Symptom based 1.00 0.64 Nurses [Smit et al.
1992]
Doctor-diagnosed
hand dermatitis Self-reported hand
dermatitis
0.65 0.93
Symptom based 0.86 0.64 Metal workers [de Joode et
al. 2007]
Doctor-diagnosed
hand dermatitis Picture based
questionnaire
0.36 0.84
Symptom based 0.64 0.87 Clinical [Svensson et
al. 2002]
Doctor-diagnosed
hand eczema Patient reported hand
eczema
0.87 0.79
Wind turbine
production
workers
[Carstensen
et al. 2006]
Doctor-diagnosed
current dermatitis
Self-reported skin rash 0.22 0.89
Self-reported one or
more symptoms, lasting
more than 3 weeks
0.46 0.83
Self-reported one or
more symptoms
0.63 0.75
Rubber
manufacturing
[Vermeulen
et al. 2000]
Doctor-diagnosed
hand dermatitis
Self-reported two or
more symptoms, lasting
more than 3 weeks
0.23 0.89
Car
Mechanics
Self-reported hand
eczema
0.59 0.96
Dentists Self-reported hand
eczema
0.58 0.99
Office
Workers
[Meding and
Barregard.
2001]
Doctor-diagnosed
hand eczema
Self-reported hand
eczema
0.53 0.96
1.4 Occupational Exposure
Over time, the recognition, assessment, and control of occupational exposures has evolved and
grown into the science of occupational, or industrial, hygiene. Historically, exposure assessment
has focused on airborne exposure rather than skin exposure, and rarely a combination of the two.
This may be due in part to the relative complexity of sampling skin exposure when compared
with the air samples required for determining potential inhalation exposure.

16
It may also be due in part to the reality that exposure limits have focused on airborne exposure;
in some cases a biological marker is suggested to monitor systemic burden as a result of uptake
from all exposure routes (inhalation, ingestion, skin absorption), but a quantitative skin exposure
limit is almost unheard of, and rarely suggested [Bos et al. 1998].
The emphasis on airborne hazards is important because it has resulted in fundamental differences
in the approach to prevention of skin and airborne hazards. The American Conference of
Governmental Industrial Hygienists (ACGIH) publishes a handbook of exposure limits called
threshold limit values (TLVs) [American Conference of Governmental Industrial Hygienists
(ACGIH). 2008]. These values have been adopted by many jurisdictions as the regulated
occupational exposure limits, including Ontario.
In the ACGIH TLVs, quantitative airborne exposure limits are listed in up to three formats per
substance: (1) a time weighted average concentration for a conventional 8-hour work day, (2) a
short term exposure limit intended as a 15-minute time weighted average, and (3) a ceiling limit
which should not be exceeded at any point in work day. In comparison, substances that have
relevant skin exposures are given a qualitative ‘skin’ notation, which denotes a “potential
significant contribution to the overall exposure by the cutaneous route” [American Conference of
Governmental Industrial Hygienists (ACGIH). 2008]. The ‘skin’ notation is not intended to
denote chemicals that have only a dermatological effect [Boeniger. 2003]. The qualitative nature
of this ‘skin’ notation and the resulting lack of a measurable exposure limit make it near
impossible to declare dermal exposure too high without the use of biological exposure indices
(BEIs) which take into account systemic burden integrated over all exposure routes.
1.4.1 Exposure-Response Relationships
The relationship between airborne exposure and respiratory disease has been studied in
numerous workplaces for a wide variety of exposures and outcomes ranging from reported
symptoms to confirmed clinical diagnoses of respiratory disease [Jaakkola et al. 2009, Heldal et
al. 2010, Lillienberg et al. 2010, Smit et al. 2008, Pronk et al. 2007, Jacobs et al. 2008, Cox-
Ganser et al. 2009].
Comparatively, studies focusing on skin exposure or on exposure-response studies for skin
symptoms and/or disease are rare. This lack of research makes it challenging to identify causal

17
links between skin exposure and skin symptoms/disease, and may ultimately hamper efforts to
better control skin exposure in the workplace. The few exposure-response studies completed to
date suggest that there are observable exposure-response relationships for skin exposure and skin
symptoms/disease.
In 2009, Sripaiboonkij et al. published two studies that included exposure-response analysis for
skin symptoms. The first was a study of glass microfiber production workers, which
demonstrated that workers in the factory areas had increased odds (OR 3.89, 95% CI 1.70–8.90)
of reporting skin symptoms (dryness or flaking of skin, itchy skin, irritation, smarting or redness
of skin, sore or tender skin, or urticaria) [Sripaiboonkij et al. 2009b]. When the workers were
classified into high and low microfiber exposure groups (airborne exposure), those with high
exposures also had greater odds of reporting skin symptoms (OR 4.82 1.89–12.33) compared
with office workers, suggesting a dose-response relationship [Sripaiboonkij et al. 2009b].
The second study by Sripaiboonkij et al. reported on similar relationships, this time among
employees in a wood furniture factory [Sripaiboonkij et al. 2009a]. There were no associations
between factory work (vs. office work) and skin symptoms or between a high/low categorization
of airborne wood dust levels and skin symptoms. But, workers who reported exposures to
chemicals on a questionnaire had increased odds of reporting skin symptoms (OR 2.53, 95% CI
1.24 to 5.17); it is unclear whether the questionnaire asked about route of exposure to the
chemicals [Sripaiboonkij et al. 2009a].
An earlier study (2007) by Van Wendel do Joode et al. investigated the association between skin
symptoms and exposure to semi-synthetic metalworking fluids [de Joode et al. 2007]. Skin
exposure was measured in two ways: first by a semi-quantitative dermal exposure assessment
tool, DREAM [Van-Wendel-de-Joode et al. 2003], and second using a quantitative tracer
method, VITAE [Fenske et al. 1986a, Fenske et al. 1986b]. Skin outcomes were also measured in
two ways: first a standard symptoms questionnaire and second, a picture based screening list. In
separate models, exposure (yes/no) and workers with high exposure (none/low/high) had
increased prevalence ratios (PR) for reporting skin symptoms on their hands, forearms or face
(PR range 2.3-2.4) [de Joode et al. 2007].

18
Chapter 5 of this thesis further contributes to the developing body of knowledge on exposure-
response relationships for skin symptoms in two occupational populations: bakery workers and
auto body shop workers.
1.5 Connecting the Skin and Respiratory Systems
1.5.1 Occupational Exposure
1.5.1.1 Exposure Recognition
Together, Table 1 and Table 2 provide a summary of workplace exposures that may cause
occupational asthma and occupational contact dermatitis, respectively. There is some evident
overlap between these two lists (i.e., metals causing OA and cobalt/nickel/chromate causing
OCD) but a review of the overlap among these causal agents has never been formally completed.
Chapter 3 of this thesis will identify common occupational contact allergens in recent Canadian
data, and investigate whether these known occupational contact allergens are also capable of
causing occupational asthma.
1.5.1.2 Exposure Assessment
The measurement of airborne exposure is well established. Air samples are collected, usually by
drawing a known amount of air through a filter and weighing or analyzing the filter for the
contaminant of interest. The pathway from airborne contamination inhaled into the respiratory
system is reasonably straightforward and well understood. The contaminants enter the upper
respiratory system, deposit at various depths (depending on particle aerodynamic diameter)
within the airways, and the smallest particles, gases and vapours deepest into the lung.
The pathway from environmental contaminant onto, into, and through the skin is seen to be more
complicated. The exposure agent can be deposited directly onto the skin during work tasks,
picked up by the skin when touching surfaces (settled airborne exposure), deposited from the
airborne compartment directly on to the skin or onto surfaces, or deposited onto a clothing layer
covering the skin [Schneider et al. 1999]. From here, the contamination can be transferred
between the compartments, ultimately reaching the skin surface where it may or may not
penetrate depending on the chemical composition of the exposure and the integrity of the skin
barrier. Much of the recent work focusing on dermal exposure and dermal exposure assessment

19
has stemmed from the conceptual model published in 1999 by Schneider et al. [Schneider et al.
1999].
In this model, Schneider et al. acknowledge the interaction between the source of contamination,
the air component and surface contamination. Additionally, the model acknowledges the
complexity that exists due to the exchange of contaminant between the outer clothing layer, the
inner clothing layer and the skin itself. All of these layers can receive contaminant from either
the airborne component or the surface contaminant layer, and can also exchange contaminant
between each other.
Given the interconnectedness of the surface and air compartments in the Schneider model, it is
likely that when the contribution from the airborne contaminant to the surface contamination
layer is high, that skin and airborne exposures in the workplace may be correlated. Previous
studies have investigated this question. In 2004, McClean et al. studied highway construction
workers’ exposure to pyrene and polycyclic aromatic compounds (PACs) and found that among
paver operators, screedmen, and roller operators skin and airborne exposures to both pyrene (r =
0.58, p = 0.04) and PACs (r = 0.45, p = 0.01) were significantly correlated [McClean et al.
2004]. Burstyn et al. found similar, though not statistically significant, results for correlation
between bitumen fume among a small group (n = 7) of Dutch paving workers (r = 0.71, p = 0.08)
[Burstyn et al. 2002].
Studies of both skin and airborne exposure in spray painters have measured exposure to xylene,
ethyl benzene, 1,6-hexamethylene diisocyanate (HDI) monomers, and isocyanurate. Chang et al.
found significant correlation between full shift skin and airborne exposure to both xylene and
ethylbenzene [Chang et al. 2007a, Chang et al. 2007b]. Fent et al. collected task based samples
for both HDI monomers and isocyanurate and also observed significant correlation between skin
and airborne exposure in both cases (HDI r = 0.79, p < 0.0001; isocyanurate r = 0.71, p =
<0.0001) [Fent et al. 2008]. A similar correlation relationship (r = 0.98) for methylene bisphenyl
diisocyanate (MDI) exposure was also observed iron foundry workers [Liljelind et al. 2010].
The correlation between skin and airborne exposure to nickel in foundry workers varied
depending on the anatomical site of skin exposure assessment, but ranged from 0.46 to 0.57 (all
p-values <0.001) [Hughson et al. 2010]. Though the actual Pearson coefficient was not given,

20
there was a significant association between skin and airborne exposure to fentanyl reported in a
recent study of pharmaceutical workers [Van Nimmen et al. 2006].
In studies of pesticide exposure, the results have not been consistent. Two studies, Flack et al.
studying propiconazole exposure in workers applying the pesticide to peach crops, and Aprea et
al. studying imidacloprid exposure in greenhouse workers, both found no correlation between
measured skin and airborne exposures [Flack et al. 2008, Aprea et al. 2009]. However,
Tsakirakis et al. recently reported skin and airborne exposures that suggest a high level of
correlation between skin and airborne exposure to malathion in pesticide applicators [Tsakirakis
et al. 2011]. Aprea et al. suggest that the lack of correlation between skin and airborne exposure
in the greenhouse workers may indicate that “exposed skin was contaminated by a different
mechanism, possible accidental contact of the face with contaminated hands, clothes or surfaces”
and not through deposition of airborne contamination onto exposed skin [Aprea et al. 2009].
It would appear that skin and airborne exposure are correlated in many, but not all exposure
scenarios. When the airborne contaminant portion is contributing highly to the skin exposure, the
two exposure measurements are likely to be correlated. This may be especially relevant with low
vapour pressure (low volatility) substances, but is likely to be dynamic in all scenarios,
dependent on exposure, tasks performed, and personal protective equipment utilized. The
mechanisms of airborne and skin exposure are complex. Exposures can be correlated and
exposure can occur in one system or both (simultaneously or concurrently). The results of studies
reporting on the correlation between skin and airborne exposure are summarized in Table 4.

21
Table 4 Correlation Coefficients for the Association Between Skin and Airborne Exposures
in Various Occupational Studies. NR = Not reported, *=Pearson Correlation Coefficient
Was Calculated Based On Published Exposure Data
Occupation Exposure Ref. r p
Paving Workers Bitumen [Burstyn et al. 2002] 0.71 0.08
Polycyclic Aromatic
Compounds (PACs)
0.15 0.5 Highway Construction -
Rakers
Pyrene 0.69 0.06
Polycyclic Aromatic
Compounds (PACs)
0.45 0.01 Highway Construction –
Non-Rakers
Pyrene
[McClean et al. 2004]
0.58 0.04
Iron Foundry Workers MDI [Liljelind et al. 2010] 0.69*
Nickel Refinery
Workers
Nickel [Hughson et al. 2010] 0.46-
0.57
<0.001
Ship Spray Painters Xylene [Chang et al. 2007b] 0.64*
Xylene NR <0.001 Ship Spray Painters
Ethylbenzene
[Chang et al. 2007a]
NR <0.001
HDI monomer 0.79 <0.0001 Auto Spray Painters
Isocyanurate
[Fent et al. 2008]
0.71 <0.0001
Farm Workers Propiconazole [Flack et al. 2008] 0.11 0.52
Pesticide Applicators Malathion [Tsakirakis et al. 2011] 0.82*
Greenhouse Workers Imidacloprid [Aprea et al. 2009] NR NS
Pharmaceutical
Production
Fentanyl [Van Nimmen et al.
2006]
NR 0.013
1.5.2 Mechanisms of Effect
Traditionally the clinical and research communities have investigated disease in silos;
respirologists diagnose and treat asthma, while dermatologists diagnose and treat dermatitis. The
outcome of this isolated approach is that thorough clinical research into the mechanisms of
disease in each system occurs individually, and investigations into occupational exposures and
pre-clinical outcomes (i.e., self-reported symptoms) address either respiratory illness or skin
illness; rarely, if ever, are both examined together.

22
As outlined in sections 1.2 and 1.3, the diagnostic categories within asthma and contact
dermatitis are similar; in both cases allergic and irritant forms of the diseases are recognized. In
contact dermatitis the irritant form is more prevalent, whereas in the case of asthma the allergic
form is considered more prevalent [English. 2004, Maestrelli et al. 2009].
The mechanisms of immune response for occupational contact dermatitis, and for most cases of
occupational asthma, are known and are accepted to be different. In the case of allergic asthma
the mechanism is usually a Type I (IgE) hypersensitivity response, while in allergic contact
dermatitis it is a Type IV (cell-mediated) delayed hypersensitivity reaction.
1.5.3 Concurrent Skin and Respiratory Disease in Individuals
Case reports in the literature indicate that workers do present with concurrent contact dermatitis
and asthma that are both work-related in a variety of occupations including manufacturing,
construction, and animal work [Moulin et al. 2009, Valks et al. 2003, De Raeve et al. 1998,
Kanerva et al. 1995, Estlander et al. 1993, Paggiaro et al. 1979]. Table 5 summarizes case reports
of concurrent asthma and contact dermatitis, stratified by cases where results of specific
inhalation challenge (SIC) testing and patch testing were reported, and those where one, or both,
of SIC or PT results were not reported.

23
Table 5 Exposures Reported in Published Case Studies to Cause Both Occupational
Asthma and Occupational Contact Dermatitis. Limited to Case Reports Where OA was
Diagnosed Using Specific Inhalation Challenge (SIC) and Occupational Contact Dermatitis
(OCD) was Diagnosed Using Patch Testing (PT).
Exposure Occupation Ref.
Diagnosed OA (SIC) and OCD (Patch Test):
2-hydroxyethyl methacrylate
(HEMA)
Beautician [Moulin et al. 2009]
Diglycidyl Ether of Bisphenol
A (DGEBA)
Resin applier [Moulin et al. 2009]
Diphenylmethane-4,4’-
diisocyanate (MDI)
Manufacturing (Automotive
Industry)
[Valks et al. 2003]
Potassium Dichromate Cement Floorer [De Raeve et al. 1998]
Aziridine Hardener Painter and varnisher [Kanerva et al. 1995]
Onion Homemaker [Valdivieso et al. 1994]
Nickel Manual grinding of metal
castings
[Estlander et al. 1993]
Spiramycin Poultry breeder [Paggiaro et al. 1979]
Diagnosed OA and OCD (No SIC and/or No Patch Test):
Nematode (Anisakis simplex) Fish processing [Barbuzza et al. 2009]
Limolene Labourer [Guarneri et al. 2008]
Peptide Coupling Reagents Laboratory workers [Vandenplas et al. 2008]
Ortho-phthalaldehyde Nurse [Fujita et al. 2006]
Sapele Wood Carpenter [Alvarez-Cuesta et al. 2004]
Ammonium Persulfate Hairdresser [Krautheim et al. 2004]
Compositae Florist [Uter et al. 2001]
Leek Agricultural worker [Cadot et al. 2001]
Aziridine Cross Linker Spray painter [Leffler and Milton. 1999]
Sodium Metabisulfite Photographic technician [Jacobs and Rycroft. 1995]
Green Bean Homemaker [Igea et al. 1994]
Diglycidyl Ether of Bisphenol
A (DGEBA)
Insulation manufacturing [Kanerva et al. 1991]

24
1.5.4 Epidemiological Evidence Linking Skin and Respiratory Outcomes
Despite the case reports of co-occurring skin and respiratory disease (Table 5) attributed to
occupational exposures, there is still very limited research in working populations regarding the
co-existence of these outcomes. As mentioned previously, there are many studies of respiratory
symptoms in working populations [Jaakkola et al. 2009, Heldal et al. 2010, Lillienberg et al.
2010, Smit et al. 2008, Pronk et al. 2007, Jacobs et al. 2008, Cox-Ganser et al. 2009] but a
comparatively small body of literature on dermal symptoms [de Joode et al. 2007, Sripaiboonkij
et al. 2009a, Sripaiboonkij et al. 2009b].
There are several population level studies that have collected and reported information on both
skin and lung symptoms individually [Sripaiboonkij et al. 2009b, Sripaiboonkij et al. 2009a,
Lindgren et al. 2002, Fantuzzi et al. 2010, Nettis et al. 2002, Kujala and Reijula. 1995, Holter et
al. 2002, Friis et al. 1999, Holness and Nethercott. 1989, Holness et al. 1989, Nethercott and
Holness. 1988, Huusom et al. 2011]. However, there are surprisingly few published studies that
have reported on co-existing skin and respiratory symptoms. A clinical study by Moulin et al.
reported on 234 patients with diagnosed WR contact dermatitis (CD) in an occupational health
clinic. When the CD patients were asked about both their respiratory symptoms only 10 (4%)
reported work-related respiratory symptoms [Moulin et al. 2009].
Lynde et al. focused on skin and respiratory symptoms in a group of professional cleaners
[Lynde et al. 2009]. Of the 549 cleaners, 460 (84%) were male. Among male cleaners, 43 (9.3%)
had a current rash and 86 (18.6%) reported having a rash in the last 12 months. In total, 33
(7.2%) male cleaners had a current rash and also reported three or more respiratory symptoms;
17 (3.7%) had skin rash plus three or more work-related respiratory symptoms. In logistic
regression models, those cleaners with a current rash and those reporting a rash in the last twelve
months were at significantly increased odds of reporting work-related respiratory symptoms
compared with cleaners who did not have a rash [Lynde et al. 2009].
These two studies were the only studies that commented on the prevalence in concurrent skin
and respiratory symptoms in populations. Though Lynde et al. reported on a working population
and Moulin et al. on a clinical population, the prevalence of concurrent symptoms in both groups
was similar. This thesis will further contribute to the literature on concurrent skin and respiratory
symptoms. Data from historical occupational studies in a variety of workplaces will be pooled

25
and analyzed to determine if there is a group of workers who report concurrent symptoms
(Chapter 4).
Additionally, this thesis will consider how workers (or patients) with concurrent skin and
respiratory symptoms may be different from those with only one symptom, or those who are
asymptomatic. This thesis will be the first study to investigate the differences in personal,
environmental and occupational factors between subjects with concurrent skin and respiratory
symptoms and those with symptoms only in one system in a clinical study population (Chapter
6).
1.5.5 Possible Cross-System Sensitization
1.5.5.1 Animal Studies
As previously stated, the mechanisms of immunologic (allergic) response differ between the skin
and the respiratory systems. Allergic contact dermatitis occurs through a Type IV T-cell
mediated response whereas allergic asthma most often through a Type I IgE mediated response.
Despite these differences in mechanisms of action, there is an increasing interest in examining
whether each route of exposure is capable of inducing sensitization and immune response(s) in
the other system.
It has been demonstrated in animal models of occupational asthma that skin sensitization may be
relevant to respiratory outcomes in the case of exposure to some chemical agents (Table 6).
These experiments generally follow structured sensitization (induction) and elicitation
(challenge) exposure protocols. The skin of naive experimental animals is exposed to the agent
in order to develop sensitization, and upon subsequent (first) inhalation challenge to the same
agent, an asthma-like response is measured in the study animals.
This skin induction and inhalation challenge experimental system has been demonstrated for
various exposures relevant to occupational asthma including: TDI [Tarkowski et al. 2007,
Vanoirbeek et al. 2004], MDI [Pauluhn. 2008, Rattray et al. 1994], TMA [Vanoirbeek et al.
2006, Arts et al. 2004, Zhang et al. 2004, Arts et al. 1998], and latex [Woolhiser et al. 1999,
Woolhiser et al. 2000].

26
Table 6 summarizes the published studies where animal models were used to determine whether
topical skin exposure can cause sensitization that results in an asthma-like response on first
respiratory challenge (intratracheal, intranasal or inhalation). Each study reported in Table 6
measured a ventilatory response to determine whether the experimental animals were having a
physiological asthma-like ventilatory response; Table 6 does not summarize experiments that
included only cellular outcomes.
The experimental animal studies reported in Table 6 involve the use of genetically identical
animals in controlled exposure scenarios. Despite the high degree of control, the different studies
still follow slightly different protocols. There are between-study differences in the location of the
dermal exposure (e.g., flank vs. ear), the preparation of the exposure site (e.g., hair removal
methods), the number of exposures in the sensitization period, and the delay between
sensitization and challenge.
This lack of standardization in the animal studies has been noted by other researchers who have
attempted to summarize a large body of evidence [Arts et al. 2006]. The lack of standardization
will be amplified when moving from animal studies into humans, as there will be an exponential
increase in variability. Human populations are genetically diverse, with large variability in both
exposure (within and between individuals) and physiological response (symptoms and diagnosed
disease).

27
Tab
le 6
Su
mm
ary
of
Exp
erim
enta
l A
nim
al
Stu
die
s D
em
on
stra
tin
g S
kin
Exp
osu
re R
esu
ltin
g i
n S
ensi
tiza
tion
an
d a
n A
sth
ma
-lik
e
Res
pon
se o
n F
irst
In
hala
tion
Ch
all
enge.
Ref
eren
ce
Ex
posu
re
Spec
ies
Sen
siti
zati
on
Chal
lenge
Ast
hm
a
resp
onse
[Kuper
et
al. 2011]
Ox
azolo
ne
Norw
ay r
ats
day
0, 7:
topic
al a
ppli
cati
on
to f
lank O
R
day
0, 4, 11, 14:
topic
al
appli
cati
on a
lter
nat
ing f
lank
and e
ar
day
21:
inhal
atio
n c
hal
lenge
+
[Tar
kow
ski
et a
l. 2
007]
Tolu
ene
dii
socy
anat
e (T
DI)
Bal
b/c
mic
e day
1, 7:
der
mal
appli
cati
on
on e
ar
day
10:
intr
anas
al c
hal
lenge
+
[Van
oir
bee
k e
t al
.
2004]
TD
I B
alb/c
mic
e day
1, 2, 3, 7:
der
mal
appli
cati
on o
n e
ar
day
10:
intr
anas
al c
hal
lenge
+
[Pau
luhn. 2008]
Met
hyle
ne
dip
hen
yl
dii
socy
anat
e (M
DI)
Norw
ay r
ats
day
0, 7:
topic
al a
ppli
cati
on
to f
lank
day
20, 35, 50, 65:
inhal
atio
n
chal
len
ge
+
[Rat
tray
et
al. 1994]
MD
I G
uin
ea P
igs
day
1:
topic
al, in
trad
erm
al o
r
inhal
atio
n a
ppli
cati
on
day
21:
inhal
atio
n c
hal
lenge
+
[Van
oir
bee
k e
t al
.
2006]
Tri
mel
liti
c
anh
yd
ride
(TM
A)
Bal
b/c
mic
e day
1, 7:
der
mal
appli
cati
on
on e
ar
day
10:
intr
anas
al c
hal
lenge
+
[Art
s et
al.
2004]
TM
A
Norw
ay r
ats
day
0, 7:
topic
al a
ppli
cati
on
to f
lank
day
21:
inhal
atio
n c
hal
lenge
+
[Zhan
g e
t al
. 2004]
TM
A
Norw
ay r
ats
day
0, 7, 14, 21:
topic
al
appli
cati
on o
n d
ors
um
day
28:
chal
len
ge
wit
h c
lean
air
;
day
35, 42:
intr
anas
al c
hal
lenge
+
[Art
s et
al.
1998]
TM
A
Norw
ay r
ats
day
0, 7:
der
mal
appli
cati
on
on f
lank
day
21 o
r 22:
resp
irat
or
chal
lenge
+
[Fra
nko e
t al
. 2011]
Furf
ury
l A
lcohol
Bal
b/c
mic
e D
ay 1
-4:
der
mal
appli
cati
on
on e
ar, in
crea
sin
g d
ose
Day 5
, 9, 13, 17:
phar
yn
gea
l
aspir
atio
n
+

28
Ref
eren
ce
Ex
posu
re
Spec
ies
Sen
siti
zati
on
Chal
lenge
Ast
hm
a
resp
onse
[Woolh
iser
et
al. 1999,
Woolh
iser
et
al. 2000]
Lat
ex
Bal
b/c
mic
e 5 d
ays
a w
eek, fo
r 7 w
eeks:
topic
al a
ppli
cati
on t
o d
ors
um
or
lum
bar
reg
ion
day
28:
inhal
atio
n c
hal
lenge
+
[Kli
nk a
nd M
eade.
2003]
3-a
min
o-5
-
mer
capto
-1,2
,4-
tria
zole
(A
MT
)
Bal
b/c
mic
e 35 c
onse
cuti
ve
days:
topic
al
appli
cati
on o
n d
ors
um
day
28, 35:
intr
atra
chea
l
chal
len
ge
+
[Las
tbom
et
al. 1998,
Las
tbom
et
al. 2000]
3-c
aren
e G
uin
ea P
igs
four
der
mal
ex
posu
res
day
21
-28:
per
fuse
d l
un
g
chal
len
ge
+
[Art
s et
al.
2004]
TM
A
Wis
tar
rats
day
0, 7:
topic
al a
ppli
cati
on
to f
lank
day
21:
inhal
atio
n c
hal
lenge
-
[Art
s et
al.
1998]
TM
A
Wis
tar
rats
day
0, 7:
der
mal
appli
cati
on
on f
lank
day
21 o
r 22:
resp
irat
or
chal
lenge
-
[van
Tri
el e
t al
. 2010]
Din
itro
chlo
ro-
ben
zene
(DN
CB
)
Wis
tar
rats
day
0:
topic
al a
ppli
cati
on
on
flan
k;
day
7:
topic
al a
ppli
cati
on
on
ear
day
21, 24, 27, 30, 34, 37
, 41, 43:
inhal
atio
n c
hal
len
ge
-
[Kuper
et
al. 2008]
DN
CB
N
orw
ay r
ats
day
0:
topic
al a
ppli
cati
on
on
flan
k;
day
7:
topic
al a
ppli
cati
on
on
ear
day
21:
inhal
atio
n c
hal
lenge
-
[Van
oir
bee
k e
t al
.
2006]
DN
CB
B
alb/c
mic
e day
1, 7:
der
mal
appli
cati
on
on e
ar
day
10:
intr
anas
al c
hal
lenge
-
[Art
s et
al.
1998]
DN
CB
N
orw
ay r
ats
day
0, 7:
der
mal
appli
cati
on
on f
lank
day
21 o
r 22:
resp
irat
or
chal
lenge
-
[Art
s et
al.
1998]
DN
CB
W
ista
r ra
ts
day
0, 7:
der
mal
appli
cati
on
on f
lank
day
21 o
r 22:
resp
irat
or
chal
lenge
-
[Lee
et
al. 1984]
Form
aldeh
yd
e G
uin
ea P
igs
day
0, 2:
topic
al a
ppli
cati
on
to d
ors
um
day
7, 22, 29:
inhal
atio
n
chal
len
ge
-

29
1.5.5.2 Human Studies & Epidemiological Evidence
Perhaps due to the challenges of large exposure and response variability in humans, but also due
to ethical considerations, there is very little experimental evidence of skin sensitization leading to
respiratory disease in humans. De Zotti reported on a latex challenge test in a health care worker
where the wearing of a latex glove on one hand was followed by an immediate decrease in peak
flow and FEV1 as well as welts and flares on the head and neck [De Zotti et al. 1992]. In a
population study Kujala et al. reported that among 534 Finnish health care workers, wearing
gloves for ≥ two hours per day was associated with having at least one respiratory disorder
(p<0.001) [Kujala and Reijula. 1995]. In the case of health care workers, there was clearly a skin
exposure to the gloves, but there may have also been an airborne exposure to the glove powder,
containing latex. However, no quantitative exposure measurements were collected as part of this
study.
Two human studies have tested experimentally whether inhalation challenges can elicit a skin
response. Tupker et al. exposed twenty subjects with confirmed atopic dermatitis (AD) to
airborne house dust mite (HDM) allergen to determine whether this exposure could exacerbate
existing dermatitis or induce new dermatitis lesions [Tupker et al. 1996]. In nine subjects (45%)
a skin reaction was observed; in eight patients the skin symptoms were preceded by a reaction in
the respiratory system (decreased FEV1). Isaksson et al. attempted to reactivate positive patch
test responses to budesonide with an inhalation challenge (budesonide) six weeks after the initial
positive patch test [Isaksson and Bruze. 2002]. Fifteen subjects with a positive patch test to
budesonide were enrolled. Seven subjects were given an inhalation challenge with budesonide,
eight received a control inhalation challenge. Of the seven who received the experimental
challenge, four exhibited a reactivation of the positive patch test response.
In working populations there is less work examining the role of skin exposure in the
development of occupational asthma. In 1993, Nemery and Laenerts commented on the use of
methylene diphenyl isocyanate (MDI) use in coal mines and the potential for skin exposure to
cause respiratory complaints [Nemery and Lenaerts. 1993]. More recently, Petsonk et al.
completed a longitudinal study of workers in a wood products plant that had exposure to MDI. In
these workers, those who reported skin staining or clothing staining (a possible marker of skin

30
exposure) were significantly more likely to report new onset asthma symptoms at the follow-up
visits (after reporting no asthma symptoms at the initial visit) [Petsonk et al. 2000].
1.5.6 Cross-System Interaction in Other Disease Models
The concept of cross-system interaction, particularly between the skin and the lungs is not
limited to occupational asthma. There are other examples of cross-system interaction in human
disease. The experiment by Tupker et al. was previously mentioned. In this case, subjects allergic
to dust mites were exposed to house dust mite allergen by inhalation, and skin responses were
observed in 45% of the subjects [Tupker et al. 1996]. In the case of chronic beryllium disease (a
respiratory disease) there is evidence that the skin is an important route of exposure for
sensitization and disease progression [Tinkle et al. 2003, Day et al. 2007, Day et al. 2006].
Additionally, respiratory symptoms have been observed in cases of food allergy in both children
and adults [Chiang et al. 2010, Bjorksten. 1996]. Cullinan et al. reported increased respiratory
symptoms in sensitized subjects after a blind food challenge test (bread containing enzymes),
compared with a control test (bread without enzymes) [Cullinan et al. 1997].
1.5.7 Additional Considerations
1.5.7.1 The Skin as a Barrier
When thinking about the role of skin exposure in the development of sensitization and
potentially the development of subsequent respiratory disease, the role of the skin barrier must be
considered. It is possible that damage to the skin either through physical, chemical, or biological
processes may hamper the skin’s ability to block penetration of allergens.
Nielsen chemically damaged human skin samples with known concentrations of sodium laurel
sulfate (SLS), a known skin irritant. The penetration of five pesticides was tested on a series of
skin samples with varying levels of SLS induced damage. Results suggested the penetration rate,
total penetration, and lag-time were all greater in the damaged skin samples compared with
control (undamaged) skin samples [Nielsen. 2005]. The ability of the SLS treatment to disrupt
the barrier function was confirmed by measuring the penetration of tritiated water across SLS
treated skin samples. Skin treated with higher concentrations of SLS had greater overall
penetration and a greater rate of penetration compared with undamaged skin [Nielsen. 2005].

31
An in vivo study of penetration in human skin demonstrated that the normal skin barrier can be
disrupted using physical (tape stripping) and chemical (sodium laurel sulfate) treatment, and also
showed that the penetration of salicylic acid is greater in skin with the most severely disrupted
barrier [Benfeldt et al. 1999].
Jakasa et al. studied volunteer subjects with atopic dermatitis (AD) and healthy skin (controls) to
test whether the skin penetration of sodium laurel sulfate differed between the two groups
[Jakasa et al. 2006]. Results suggested that the penetration was greater among subjects with
active AD compared with healthy controls, but there were no differences between subjects with
inactive AD and the healthy controls [Jakasa et al. 2006].
In an epidemiological study of dermal and airborne exposure to potentially carcinogenic
substances in rubber workers, Vermeulen et al. collected information on the skin condition of the
exposed workers [Vermeulen et al. 2003]. A dermatologist assessed the skin of each subjects and
recorded the presence of active hand dermatitis, minor dermatitis, and skin injuries. The results
from Vermeulen et al. suggested that workers who were observed to have minor skin aberrations
(mild dermatitis) had higher levels of urine mutagenicity (measured using a Salmonella
typhimurium assay) than subjects with normal skin, implying that the subjects with skin disease
had great uptake of occupational exposure [Vermeulen et al. 2003]. This result suggests a role
for barrier function in modifying the uptake of dermal exposure.
Similarly, Hino et al. studied toluene and xylene exposure in auto body painters. They found no
correlation between airborne exposure levels and urinary biomarkers for either toluene or xylene
[Hino et al. 2008]. However, they did find a strong and significant correlation between the
urinary biomarkers of toluene and xylene exposure and poor skin condition (toluene: r = 0.61, p
< 0.0001; xylene: r = 0.34, p = 0.004) as measured by a dermatologist on a skin severity index
[Hino et al. 2008].
A clinical study by Bremmer et al. examined 491 patients with atopic dermatitis (AD) and
ichthyosis vulgaris (IV), those with higher severity of IV were more likely to report asthma, even
after adjustment for AD severity, age, sex, and season of symptom reporting [Bremmer et al.
2008]. Bremmer suggests that the presence of severe IV could be used as a marker for patients
who are more likely to develop allergic respiratory disease. These findings lend more support to

32
the hypothesis that skin barrier dysfunction influences the degree of allergic sensitization, though
this mechanism remains unclear [Bremmer et al. 2008].
Together, these studies suggest that a compromised skin barrier is a modifying factor in the
uptake of skin exposure into the human body. These results also suggest that the barrier function
is not an innate, static characteristic within an individual. The application of physical stress (tape
stripping) or chemical stress (SLS) can induce a change in barrier function. It is possible that
some workplace exposures will act to disrupt the skin barrier, increasing the permeability of
workers’ skin and, in turn, the uptake of workplace exposures through the skin.
1.6 Framework
A simple framework for conceptualizing the possible connection between skin and respiratory
outcomes in terms of both exposure and response is proposed in Figure 2. Figure 2 uses the
common exposure to health effects pathway and incorporates the exposures, intermediate health
effects, and specific outcomes of interest for this thesis.
In four separate studies, this thesis will further investigate three of the relationships outlined in
Figure 2. The results from this thesis will contribute to knowledge of each of these relationships
individually and more broadly to the understanding of the framework as a whole. The three
specific relationships that this thesis seeks to investigate are:
• Relationship between airborne exposure and skin exposure,
• Relationship between skin symptoms and respiratory symptoms,
• Relationship between exposure (airborne) and skin symptoms.

33
Figure 2 A Proposed Framework for Conceptualizing the Connections Between Skin and
Respiratory Symptoms and Disease. With Contributions from V.H. Arrandale, J. Cherrie
and D. Heederik.

34
Chapter 2 Research Aims and Hypotheses
2.1 Knowledge Gaps
Occupational contact dermatitis and occupational asthma are common problems in the
workplace. Workers can develop new disease, or aggravate existing disease, as a result of
exposures at work. Both diseases have an allergic and an irritant form, and both are associated
with symptoms reported by the workers. Though we have a good understanding of exposure–
response relationships in relation to respiratory symptoms and occupational asthma, we do not
understand exposure-response relationships for skin symptoms and skin disease to the same
extent.
We also do not have a good understanding of which exposures may be risks to both the skin and
respiratory symptoms, nor have we evaluated our current systems of identifying potential skin
and/or respiratory allergens in the workplace.
Additionally, there is evidence that some workers experience symptoms in both systems, and
these symptoms may be a result of workplace exposures. There is mounting evidence that skin
exposure may lead to sensitization that is relevant to the development of respiratory disease.
Neither of these two areas, concurrent symptoms and cross-system sensitization, have been
explored thoroughly in occupational studies.
2.2 Research Aims
The overarching purpose of this thesis is to further investigate the relationships between
occupational exposures, skin symptoms and disease, and respiratory symptoms and disease.
There is particular focus on the interaction between the two systems in terms of co-existing
exposures and concurrent symptoms.
2.2.1 Specific Research Aims
The specific research aims of this thesis are as follows, arranged by thesis chapter:
Chapter 3: “Occupational Contact Allergens: Are They Also Associated With Occupational
Asthma?”

35
Aim 1. To identify the most common occupational contact allergens in the available
Canadian patch test data.
Aim 2. To identify which of the most common occupational contact allergens in Canadian
data are also associated with causing occupational asthma.
Chapter 4: “Co-existing Skin and Respiratory Symptoms in Four Occupational Groups”
Aim 3. To determine whether workers report symptoms in both their skin and respiratory
systems.
Chapter 5: “Skin Symptoms in Bakery and Auto Body Shop Workers: Associations With
Exposure and Respiratory Symptoms”
Aim 4. To determine whether exposure-response relationships can be observed for skin
symptoms in two separate occupational groups: bakery workers and auto body shop
workers.
Chapter 6: “Predictors of Concurrent Skin and Respiratory Symptoms among Workers with
Suspected Work-Related Skin or Respiratory Disease”
Aim 5. To determine how many patients with suspected work-related skin or respiratory
disease report symptoms in both systems, and whether or not these symptoms are
work-related.
Aim 6. To identify predictors of reporting both skin and respiratory symptoms among a
clinical population with suspected work-related skin or respiratory disease.
2.3 Hypotheses
A. There is significant overlap in agents/exposures that cause occupational asthma and
occupational contact dermatitis.
Previous research has studied the causes of occupational contact dermatitis and occupational
asthma separately. Results from these studies show that there are similarities in the type of
exposure that cause these two outcomes, however differences in the way these exposures are
identified hamper the comparison. This thesis will identify recent common occupational contact

36
allergens in Canadian patch test data and systematically review the literature to determine
whether they are also capable of causing occupational asthma.
B. Exposure-response relationships exist for occupational exposures and skin symptoms in a
similar manner to those observed for occupational exposures and respiratory symptoms.
In general, the exposure-response relationships for respiratory symptoms are studied more often,
and are better understood, than exposure-response relationships for skin symptoms. Exposure-
response relationships for respiratory symptoms have been previously described in two working
populations, bakery workers and auto body shop workers. The data describing skin symptoms in
these two groups has not been examined. This thesis will examine whether exposure-response
relationships for skin symptoms exists in these two working populations.
C. Some workers are experiencing and will report both skin and respiratory symptoms.
Very few studies have examined the prevalence of concurrent skin and respiratory symptoms and
disease. We know that skin and airborne exposures are likely to occur in the workplace and that
these exposures can be correlated. Despite this, it is not know whether concurrent symptoms are
rare or common, or whether they occur in some occupations or all occupations. This thesis will
pool data from historical occupational studies and analyze the data to determine what portion of
workers (form a variety of workplaces) report concurrent skin and respiratory symptoms. This
thesis will also measure the prevalence of concurrent skin and respiratory symptoms in a clinical
population of patients with suspected work-related disease.
D. Patients with concurrent skin and respiratory symptoms will differ from patients with
symptoms in only one system based on exposure, occupation and/or personal protective
equipment use.
It is suspected that a clinical population with suspected work-related disease (either skin or
respiratory) will have higher symptom prevalence than healthy working populations. The
increased prevalence in the clinical population will permit for analyses to identify predictors of
concurrent symptoms. This analysis will allow for the identification of occupations and
workplaces that are at higher risk of concurrent skin and respiratory symptoms. This thesis will

37
explore whether patients with concurrent symptoms differ from patients with symptom(s) only in
one system based on occupation, exposure and personal protective equipment use.

38
Chapter 3 Occupational Contact Allergens: Are They Also Associated With Occupational Asthma?
Victoria H. Arrandale1; Gary M. Liss
1,2; Susan M. Tarlo
1,3,6; Melanie Pratt
4; Denis Sasseville
5;
Irena Kudla6; D. Linn Holness
1, 6
1 University of Toronto, Toronto, Canada
2 Ontario Ministry of Labour, Toronto, Canada
3 Toronto Western Hospital, Toronto, Canada
4 University of Ottawa, Ottawa, Canada
5 McGill University, Montreal, Canada
6 St. Michaels Hospital, Toronto, ON
This manuscript was published in the American Journal of Industrial Medicine (Am J Ind
Med. 2012 Apr; 55 (4):353-60). Copyright permission has been granted (see Copyright
Acknowledgements).

39
3.1 Abstract
Background: Workplace exposures that can potentially cause both allergic occupational contact
dermatitis (AOCD) and occupational asthma (OA) are not clearly identified.
Methods: Occupational contact allergens (OCAs) were identified using North American Contact
Dermatitis Group (NACDG) data. Reference documents and systematic reviews were used to
determine whether each OCA had been reported to potentially cause OA. The presence or
absence of a sensitizer notation in occupational hygiene reference documents was also examined.
Results: The 10 most common OCAs were: epoxy resin systems*, thiuram, carba mix, nickel
sulfate*, cobalt chloride*, potassium dichromate*, glyceryl thioglycolate, p-phenylenediamine*,
formaldehyde* and glutaraldehyde*. Seven (indicated by *) were determined to be possible
causes of OA. Information on sensitizing potential from OH reference materials contained
conflicting information.
Conclusions: Several common OCAs can also potentially cause OA. Inhalation and dermal
exposures to these agents should be controlled and both OA and AOCD should be considered as
possible health outcomes. Increased consistency in sensitizer notations is needed.

40
3.2 Introduction
Traditionally, research related to occupational contact dermatitis (OCD) and occupational asthma
(OA) has been done in separate organ system silos, with the work focusing on either lung disease
or skin disease, but rarely the two together. In the workplace, workers are exposed to chemicals
that may cause both irritant and allergic effects, in the skin and lung, by both dermal and
inhalation routes of exposure. Agents causing responses in both systems are not well
documented, and are not always recognized in the occupational or clinical settings.
In addition, there is an emerging body of research that examines whether each route (dermal and
inhalation) of exposure is capable of inducing sensitization and response in the other system. It
has been shown in animal models that dermal exposure can cause sensitization that upon first
inhalation exposure (in a naïve animal) results in an asthma-like response [Vanoirbeek et al.
2004, Zhang et al. 2004, Klink and Meade. 2003, Herrick et al. 2002, Lehto et al. 2005]. There
are also case reports in the literature of workers having both AOCD and OA in response to the
same chemical [Moulin et al. 2009, De Raeve et al. 1998, Guarneri et al. 2008].
The evidence from animal models and human case reports shows that there is a need to better
understand the inter-relationships between inhalation and dermal routes of exposure, and
between respiratory and skin responses, to workplace chemicals in order to develop appropriate
prevention strategies.
Patch testing is an important clinical tool in the diagnosis of allergic contact dermatitis (ACD).
The North American Contact Dermatitis Group (NACDG) is a group of dermatologists across
the United States and Canada who have agreed to patch test patients to standard sets of allergens
according to a standardized protocol and pool their data for surveillance and research purposes
[Zug et al. 2009]. Members are dermatologists trained in patch testing and experienced in the
diagnosis of occupational skin disease; two of the thirteen members of the NACDG are located
in Canada. The group uses standardized methods for patch testing and interpretation of results
and regularly reviews the results of the pooled patch test results from their clinics
The NACDG database offers an opportunity to examine contact allergens in a large clinical
population. There is no equivalent database containing data on airway sensitizers.

41
The aim of this study was to first identify the most common OCAs in the Canadian portion of the
NACDG data, and to determine whether these agents were also airway sensitizers using the peer-
reviewed occupational asthma literature. The secondary aim was to identify whether or not the
common OCAs were noted as skin or respiratory sensitizers in common occupational hygiene
(OH) reference documents.
3.3 Methods
De-identified patient data were obtained for the two Canadian NACDG sites for the period
January 1, 2001 to December 31, 2006. This data represented three 2-year cycles of NACDG
data collection. All patients were patch tested with a standard screening series of 65 allergens
(“standard tray”); a standardized technique was followed in all cases [Pratt et al. 2004]. Informed
consent was obtained from all patients as required by each study center’s human research
committee. This study was approved by the St. Michael’s Research Ethics Board.
During each 2-year study period the standard patch test tray included sixty-five (65) allergens;
changes to this standard tray are made between cycles. Generally, the allergens removed have
low rates of positive response, and the allergens added are emerging as more common allergens.
Fifty-eight (58) allergens were common to all three NACDG cycles included in this analysis.
None of the fourteen allergens excluded were known, common occupational allergens.
For each patient, the physician assigned up to three diagnostic codes, which indicate the
diagnosis. The work-relatedness of the diagnosis was also recorded by the physician as a
separate variable (yes, no, unsure or not tested). For all patients, their response to each of the
individual 58 allergens was recorded as allergic, unknown, negative or not tested. The work-
relatedness for each individual allergen (separate from the diagnosis) was recorded as yes, no,
unsure or not tested. Additional information on the subjects’ age, sex and race was included in
the data.
3.3.1 Diagnosis of Occupational Allergic Contact Dermatitis
Subjects were considered to have allergic contact dermatitis (ACD) if any of the three diagnostic
codes were “allergic dermatitis”. Subjects were considered to have occupational-related ACD
(AOCD) if there was a diagnostic code of “allergic dermatitis” and if the overall diagnosis was

42
coded as occupationally-related (“yes”). Subjects where the overall occupationally-related
variable was coded as “unsure” were not included as cases of AOCD for this analysis.
3.3.2 Determination of Occupationally-Relevant Positive Patch Test Responses
Occupational contact allergens (OCAs) were identified using the response code (“allergic”) and
the work-relatedness code (“yes”) assigned to the individual allergens tested. The number of
individual positive patch test (PPT) responses that were coded both as occupational (allergen
specific) and allergic (allergen specific) were counted for each allergen. As the OCAs were
determined based on individual allergen responses, it was possible for a single subject to
contribute multiple times to the OCA frequency table.
Differences between occupational and non-occupational ACD cases were tested using ANOVA
(continuous variables) and chi-square (categorical variables) tests. All analyses were conducted
using SAS v9.2 [SAS Institute Inc. 2008].
3.3.3 Determination of Whether OCAs May Also Cause OA
Whether each of the ten most common OCAs was also a potential cause of work-related asthma
was determined using two reference documents that are considered authoritative sources of
information among the occupational asthma research community. Where no information was
available in the reference sources, the peer-reviewed literature was searched systematically.
The first source for determining whether an OCA has been associated with OA was “Asthma in
the Workplace”, edited by Bernstein et al. (2006). If the allergen was listed in “Appendix –
Agents Causing Occupational Asthma with Key References” (p.825), the allergen was
considered to have been associated with OA.
Second, the United Kingdom Health and Safety Executive’s 2001 publication “Asthmagen?” was
consulted [UK Health and Safety Executive,. 2001]. “Asthmagen?” reported on all substances
that were suspected of being respiratory sensitizers under the European Union’s (EU) 1996
criteria. If the allergen was listed as meeting the criteria it was considered to be associated with
OA.
43
In cases where a search of the peer-reviewed literature was required, a systematic review strategy
was followed. All alternate names for the allergen listed in the manufacturer’s documentation
(Chemotechnique® Diagnostics, Vellinge, Sweden) as well as alternate names listed in the
HazMap on-line database [National Institutes of Health. 2009] were used. Searches were
completed for each allergen (all alternate names) combined with occupational asthma. Searches
were limited to human studies published on or before December 31, 2010. The systematic search
strategy was completed in three separate databases: Ovid MEDLINE, TOXLINE and EMBASE.
Results from the three database searches were combined for each OCA and all articles were
reviewed.
Based on data gathered from the two reference materials and the systematic review of the peer-
reviewed literature, each of the ten most common OCAs was classified into one of four
categories describing the level of evidence linking the agent with OA:
• Established, the OCA is listed in either Asthma in the Workplace or Asthmagen as a
potential cause of OA;
• Possible, the OCA is not listed in either Asthma in the Workplace or Asthmagen, but there
is some evidence in the peer-reviewed literature (e.g. case reports), OR the evidence in
Asthma in the Workplace and Asthmagen is conflicting;
• Negative, studies have investigated the OCA in OA aetiology and found negative results;
• No evidence located, no evidence of the role of the OCA in the aetiology of OA was
located.
3.3.4 Determination of Skin Sensitizer Notation Status
Three sources of information available to practicing occupational hygienists were reviewed to
assess whether the 10 most common OCAs identified were listed as possible sensitizers. The
sources reviewed were the American Conference of Governmental Industrial Hygienists
(ACGIH) Threshold Limit Value (TLV) handbook [American Conference of Governmental
Industrial Hygienists (ACGIH),. 2008], the National Library of Medicine’s HazMap
Occupational Exposure to Hazardous Chemical database [National Institutes of Health. 2009]
and the NIOSH Pocket Guide to Chemical Hazards [National Institute for Occupational Safety
and Health. 2007].

44
The notations indicating sensitizing potential differed between the OH reference documents. In
some cases sensitizing potential was not explicitly noted. The notations that were accepted to
indicate the possibility of sensitization resulting from exposure were as follows:
• NLM HazMap Database: adverse effects ‘Skin’ and ‘Asthma’ as well as potential disease
outcomes of ‘Asthma’ and ‘Contact Dermatitis’.
• ACGIH TLV Handbook: specific sensitizer notation, ‘SEN’, though this does not
differentiate between the systems in which sensitization may occur.
• NIOSH Pocket Guide: possible symptoms as ‘Respiratory sensitizer’, ‘Asthma’ or ‘Skin
Sensitizer’.
3.4 Results
Data received from the NACDG contained 3676 patch test records for the period January 1, 2001
– December 31, 2006. In total 1808 (49%) subjects had a diagnosis of allergic contact dermatitis
and 619 (17%) subjects had a diagnosis of work-related dermatitis. Overall, 397 subjects (11% of
all subjects) met the definition of AOCD.
The ACD and overall population were not observed to have any striking differences in the
demographic variables (Table 7). There were 354 (10%) subjects who had both an irritant and an
allergic diagnosis (data not shown). Among the occupational cases, 20% had both an allergic and
an irritant diagnosis (n=120) (data not shown). Among the ACD cases, occupational cases were
more likely to be male (p<0.0001) and to be younger (p<0.0001) than the non-occupational cases
(Table 7).
3.4.1 Common Occupational Contact Allergens
The ten most frequent OCAs (PPT reactions coded as occupational and allergic) were: epoxy
resin, thiuram, carba mix, nickel sulfate, cobalt chloride, potassium dichromate, glyceryl
thioglycolate, p-phenylenediamine (PPD), glutaraldehyde, and formaldehyde (Table 8). In total
forty-one allergens were coded as both work-related and allergic in at least one subject.

45
Table 7 Basic Descriptive Statistics for the Entire Study Population, Subjects with an
Allergic Contact Dermatitis (ACD) Diagnoses and ACD Cases Stratified by Occupational
Relatedness. ACD Frequencies Reported as n (%) of All Patients. AOCD and Non-
Occupational ACD Reported as n (%) of ACD Cases. P-values Shown for Comparison
Between AOCD and Non-Occupational ACD Groups.
All Patients ACD AOCD
Non-Occup.
ACD
n (%) n (%) n (%) n (%) p-value
Overall 3676 (100%) 1808 (49%) 397 (22%) 1411 (78%) -
A 2167 (59%) 1286 (59%) 244 (19%) 1042 (81%) Physician
B 1509 (41%) 522 (35%) 153 (29%) 369 (71%) <0.0001
Yes 619 (17%) 397 (64%) - -
No 2854 (78%) 1321 (46%) - -
Work-
Related
Unsure 203 (5.5%) 90 (44%) - -
-
Male 1155 (31%) 554 (48%) 200 (36%) 354 (64%) Sex
Female 2521 (69%) 1254 (50%) 197 (16%) 1057 (84%) <0.0001
White 3265 (89%) 1601 (49%) 339 (21%) 1262 (79%)
Black 88 (2.4%) 45 (51%) 15 (33%) 30 (67%)
Asiatic 205 (5.6%) 105 (51%) 27 (26%) 78 (74%)
Hispanic 35 (1.0%) 11 (31%) 4 (36%) 7 (64%)
Race
Other 83 (2.3%) 46 (55%) 12 (26%) 34 (74%)
NS
Age (mean, sd) 45.5 (15.9) 45.4 (15.9) 39.3 (11.2) 47.1 (16.6) <0.0001
Table 8 Ten Most Common Occupational Contact Allergens (OCAs). (Frequency That
Individual Responses to the Allergen Were Coded Both as Work-Related and Allergic.)
# Allergen n
1 Epoxy Resin 49
2 Thiuram 39
3 Carba Mix 36
4 Nickel Sulfate 22
5 Cobalt Chloride 21
6 Potassium Dichromate 20
6 Glyceryl Thioglycolate 20
8 P-phenylenediamine (PPD) 19
8 Formaldehyde 19
10 Glutaraldehyde 16

46
3.4.2 Occupational Contact Allergens as a Cause of Occupational Asthma
Of the ten most frequent OCAs in our patient population, seven were listed in Asthma in the
Workplace (all except thiuram, carba mix and glyceryl thioglycolate) and five were listed in the
HSE Asthmagen document (some components of epoxy resin systems, nickel sulfate, cobalt
chloride, potassium dichromate, and glutaraldehyde) as exposures capable of causing OA (Table
9).
Three of the ten most common OCAs in our patient population were not listed in either
document: thiuram, carba mix and glyceryl thioglycolate; the systematic review strategy was
completed for each of these agents. The systematic search strategy retrieved the following
number of citations: carba mix - 9 articles; thiuram mix -19 articles; and glyceryl thioglycolate -
1 article. After review (VA, ST, GL, LH), none of the retrieved articles contained objective
diagnostic test results that supported an association between exposure to the OCA and
occupational asthma.
Table 9 Summary of the Ten Most Frequent Occupational Contact Allergens (OCAs) and
the Evidence Linking Each to OA in Asthma in the Workplace and the UK HSE
Asthmagen.
Asthma in Workplace HSE Asthmagen
1 Components of Epoxy
Resin Systems
Yes* Yes*
2 Thiuram Not Listed Not Listed
3 Carba Mix Not Listed Not Listed
4 Nickel Sulfate Yes Yes
5 Cobalt Chloride Yes Yes
6 Potassium Dichromate Yes Yes
7 Glyceryl Thioglycolate Not Listed Not Listed
8 P-phenylenediamine (PPD) Yes Watch List
9 Formaldehyde Yes No
10 Glutaraldehyde Yes Yes
* Epoxy resin systems contain epoxy monomers and polymers (e.g., bisphenol A, bisphenol F) as well as
hardeners (e.g., acid anhydrides and amines). The hardeners are confirmed causes of OA, some epoxy
monomers, such as bisphenol A have been associated with OA in a few cases [Moulin et al. 2009, Hannu et
al. 2009, Kanerva et al. 2000].

47
Table 10 Categorization of Whether Each Common Occupational Contact Allergen (OCA)
Has the Potential To Cause OA Based on Reference Sources and Systematic Literature
Review, Where Necessary.
Asthma Causing Agent?
Establ. Possible Negative
No Current
Evidence
1 Components of Epoxy
Resin Systems X*
2 Thiuram X
3 Carba Mix X
4 Nickel Sulfate X
5 Cobalt Chloride X
6 Potassium Dichromate X
7 Glyceryl Thioglycolate X
8 P-phenylenediamine (PPD) X
9 Formaldehyde X
10 Glutaraldehyde X
* Epoxy resin systems contain epoxy monomers and polymers (e.g., bisphenol A, bisphenol F) as well as
hardeners (e.g., acid anhydrides and amines). The hardeners are confirmed causes of OA, some epoxy
monomers, such as bisphenol A have been associated with OA in a few cases [Moulin et al. 2009, Hannu et al.
2009, Kanerva et al. 2000].
Epoxy resin, nickel sulfate, cobalt chloride, potassium dichromate, and glutaraldehyde were
classified as having established associations with OA. P-phenylenediamine (PPD) and
formaldehyde were classified as possibly associated with OA due to discrepancies between the
two reference documents. Thiuram, carba mix and glyceryl thioglycolate were classified as
having no current evidence of causing OA. These categorizations are summarized in Table 10.
3.4.3 Sensitizer Notations
Lastly, the presence or absence of a sensitizer notation, or a reasonable equivalent as described in
the Methods, was determined for each of the ten most common OCAs in the three OH reference
documents (Table 11). The NLM HazMap data base was the only source to assign all of the
OCAs a skin or contact dermatitis notation (indicating sensitizing or irritant effects); seven were
assigned an asthma notation (Table 11). All three sources agreed that epoxy resin (or

48
components of epoxy resin systems) and glutaraldehyde were potential sensitizers (either skin or
respiratory) but for all other OCAs there was disagreement between the sources.
Table 11 Summary of Sensitizer Notations for the Ten Most Common OCAs in Common
Occupational Hygiene Reference Documents.
ACGIH
TLVs
NLM HazMap
Health Effects NIOSH Pocket Guide
Sensitizer
Notation Asthma
Skin OR
Contact
Dermatitis
Resp
Sensitizer
OR Asthma
Skin
Sensitizer
Hardener Yes Yes Yes Yes No Components of
Epoxy Resin
Systems Monomer No Yes Yes No No
Thiuram Not listed No Yes No No
Carba Mix Not listed No Yes Not listed
Nickel Sulfate No Yes Yes Yes Yes
Cobalt Chloride No Yes Yes Not listed
Potassium Dichromate No Yes Yes No Yes
Glyceryl Thioglycolate Not listed No Yes Not listed
p-phenylenediamine (PPD) No Yes Yes Not listed
Formaldehyde Yes Yes Yes No No
Glutaraldehyde Yes Yes Yes Yes Yes
Not listed = Agent not listed in the reference material.
3.5 Discussion
This study generated a list of the ten most common OCAs in the Canadian portion of the 2001-
2006 NACDG population. In 2002 Rietschel et al published an analysis of the complete NACDG
data from 1998-2000 and reported that the most common occupational contact allergens in this
period were, in descending frequency: thiuram, epoxy resin, carba mix, nickel sulfate,
formaldehyde, potassium dichromate, quaternium 15, cobalt chloride, glutaraldehyde, glyceryl
thioglycolate and mercaptobenzothiazole [Rietschel et al. 2002]. With the exception of
quaternium 15 and mercaptobenzothiazole, the results presented here are strikingly similar to

49
those of Rietschel et al. This suggests that the results from the 2001-06 Canadian data are at least
somewhat representative of the NACDG data as a whole.
A second comparison can be made with the UK’s surveillance system data: EPIDERM and the
Occupational Physicians Reporting Activity (OPRA). These surveillance schemes group
allergens into more holistic groups but results from both indicate that the most common OCAs in
the Canadian NACDG population map well to the published EPIDERM and OPRA data
[McDonald et al. 2006]. For example, “rubber chemicals and materials”, which would include
thiuram and carba mix, were the materials most frequently reported as causing cases of contact
dermatitis in both OPRA and EPIDERM from 1996 to 2001 [McDonald et al. 2006]. “Resins and
acrylics”, “nickel” and “preservatives” were also in the ten most common agents reported as
causes of contact dermatitis during this period. OPRA and EPIDERM do not differentiate
between irritant and allergic contact dermatitis; this both explains why “wet work” appears as the
second leading cause of dermatitis, and suggests why more of the agents identified in the current
study were not more highly ranked in the OPRA/ EPIDERM results.
These comparisons suggest that, although the small sample size may have caused the results to
be influenced by local industry and case clusters, the most common agents observed in the
Canadian NACDG data are common occupational contact allergens in other parts of the world.
Determining whether an OCA is related to occupational asthma presented a few challenges,
specifically in the case of epoxy resin. The epoxy resin on the NACDG standard tray contains
epichlorhydrin and bisphenol A that react to form the epoxy resin monomer diglycidyl ether of
bisphenol A (DGEBA or BADGE). However, a worker using epoxy resin systems in the
workplace will likely have exposure to both the epoxy resin (DGEBA or BADGE) as well as at
least one hardener to ‘cure’ the epoxy. Several common hardeners, including amine and acid
anhydride formulas are known to cause occupational asthma; these agents were listed in both
reference texts [Bernstein et al. 2006a, UK Health and Safety Executive,. 2001] as known causes
of OA. Epoxy resin monomer, specifically DGEBA, has also been associated with asthma in the
peer-review literature [Moulin et al. 2009, Hannu et al. 2009, Kanerva et al. 2000] but was not
listed as a cause of OA in either text. It is clear that components of epoxy resin systems are
capable of causing AOCD and OA, and that a worker using epoxy resins systems may be at risk
for both OCD and OA from separate chemical exposures during the use of epoxy resin systems.

50
For this reason we included both the epoxy resin monomer and the hardeners in our review of the
reference documents and literature.
When the common OCAs were cross-referenced with the OA literature, seven of the ten OCAs
were determined to be established or possible causes of OA (epoxy resin, nickel sulfate, cobalt
chloride, potassium dichromate, PPD, formaldehyde and glutaraldehyde). A wide variety of
workers may be exposed to these common OCAs in various occupational settings [National
Institutes of Health. 2009]. Epoxy resins are commonly used in coatings for metal, wood,
concrete, or plastic, but are also found in adhesives, castings and electrical components. Nickel
sulfate is used as a dye and in the process of electroplating; it can also be found in both coatings
and ceramics and is commonly used in the production of other nickel compounds. Cobalt
chloride is found in a wide variety of applications including as a laboratory reagent, in the
process of electroplating, and as a glass or porcelain pigment. Potassium dichromate can be used
in the processes of dyeing, bleaching and leather tanning and can also be found in some types of
cement. It can also be present in the health care setting as an antiseptic or astringent, as well as in
painting, printing, coating or staining. P-phenylenediamine (PPD) is present in dark hair dyes
used by hairdressers, but can also be used in photographic development. Formaldehyde is used in
the production of formaldehyde resins, plywood, particle board and urea-formaldehyde foam.
Glutaraldehyde is used for sterilization purposes in health care settings. Embalmers and
laboratory workers may have exposure to both formaldehyde and glutaraldehyde.
Three OCAs were found to have no evidence of an association with OA: thiuram, carba mix and
glyceryl thioglycolate. Glyceryl thioglycolate is found in permanent wave solution used by
hairdressers. Thiuram and carba mix are accelerants used in rubber manufacturing, and can be
present in the final manufactured rubber product (i.e. rubber elastic components, rubber gloves,
rubber tool hand grips). Components of the carba mix allergen can also be found in carbamate
pesticides.
The results suggesting an association between epoxy resin and OA are largely based on the link
between amine and anhydride hardeners (used to cure the epoxy resin) with OA (rather than
from the epoxy monomers themselves, though BADGE (or DGEBA) has been shown in three
case studies to be related to OA [Moulin et al. 2009, Hannu et al. 2009, Kanerva et al. 2000].

51
When the ten most common OCAs identified in the Canadian NACDG data were cross-
referenced in the occupational hygiene resources only the NLM NIH HazMap database identified
all ten as causing skin effects. The ACGIH TLV Hand Book reported only epoxy resin
hardeners, formaldehyde and glutaraldehyde as potential sensitizing agents, but does not specify
the system of effect. The NIOSH Pocket Book identified epoxy resin hardeners, nickel sulfate
and glutaraldehyde as potential respiratory sensitizers as well as nickel sulfate, potassium
dichromate and glutaraldehyde as possible dermal sensitizers.
In the ACGIH TLV Hand Book the sensitizer (SEN) notation does not distinguish between the
respiratory, dermal or conjunctival organ systems. In both the NLM NIH HazMap database and
the NIOSH Pocket Book respiratory and dermal effects are separate notations. However, the
HazMap database does not differentiate between sensitizing and irritant, thus a limitation is that
the notations could refer to either allergic or irritants exposure effects.
Though each OH reference document has a slightly different purpose and scope, the
contradictory information provided by these sources is problematic. Neither a practicing
occupational hygienist nor occupational physician should be required to reference multiple
sources for comprehensive information on an occupational exposure. More work is needed to
ensure consistency in the application of sensitizer notations if workers are to be sufficiently
protected; this process has been proposed in other jurisdictions [Schnuch et al. 2002].
This study analyzed six years of patient data from the two Canadian contributors to the NACDG.
The results could reflect local clusters of exposure as one of the centers has a large
telecommunications industry with known epoxy exposure. Due to the small number of AOCD
cases, the data is perhaps more sensitive to these regional clusters. However, the common OCAs
that were identified in this study have previously been reported as some of the most frequent
OCAs [Rietschel et al. 2002].
3.5.1 Limitations
There are some limitations with our study to be noted. It must be emphasized that the basis for
the list of common OCAs was a database of patch test data focused exclusively on contact
sensitizers. The OCAs identified as possible causes of OA should not be interpreted as common
causes of OA, but rather as common contact sensitizers (or common causes of ACD) that are

52
also capable of causing OA. No inference on each OCA’s likelihood of causing OA, or
frequency of cases, can be made from this study.
There is no source of information on occupational respiratory sensitizers that is comparable to
the North American Contact Dermatitis Group database, making it challenging to identify the
most common asthmagens at the population level. Although the agents discussed in this study
are common contact sensitizers they are not necessarily the most common respiratory sensitizers,
they are simply capable of causing OA in some workers.
The practical importance of the current findings are 2-fold: first, there are many OCAs that can
also cause OA. Awareness of this by occupational hygienists and clinicians alike needs to be
improved. Second, the designation of workplace chemicals as potential skin and/or lung
sensitizers is lacking in consistency across databases and agencies.
Results from this study highlight the importance of considering both dermal and inhalation
routes of exposure. Analysis of the 2001-06 data from the NACDG Canadian data showed that of
the ten most common OCAs, seven have been associated with OA in the literature. Unrecognized
or uncontrolled exposure to these agents through either dermal or inhalation routes of exposure
can potentially lead to work-related allergic disease in both the skin and the respiratory system.

53
Chapter 4 Co-existing Skin and Respiratory Symptoms in Four Occupational Groups
Victoria H. Arrandale1 and D. Linn Holness
1,2
1 University of Toronto, Toronto, ON, Canada
2 St. Michael’s Hospital, Toronto, ON, Canada
This short report manuscript was peer-reviewed and ultimately rejected. This manuscript is
currently under revision in preparation for re-submission.

54
4.1 Abstract
Background: There is evidence in animals of an interaction between the skin and respiratory
system in the development of allergic skin and respiratory disease. The evidence supporting a
similar association in humans is limited. The goal of this study was to determine if workers
report both skin and respiratory symptoms related to their work.
Methods: Data from four studies were pooled. Information on self-reported skin and respiratory
symptoms was obtained using an interviewer-administered questionnaire; pulmonary function
was measured in all subjects.
Results: A total of 113 (46%) workers reported at least one respiratory symptom; 42 (17%)
reported a skin rash. Overall, 26 (11%) workers reported both skin and respiratory symptoms
(range 6-17% across groups). Only 2 workers reported both work-related skin and work-related
respiratory symptoms.
Conclusions: As the potential interaction between the skin and the respiratory system is further
investigated thorough information about exposure and response in both systems must be
collected.

55
4.2 Introduction
There is some evidence in animals of an interaction between the skin and respiratory system with
respect to the development of allergic skin and respiratory disease. Results from animal studies
have shown that the skin is a viable route of sensitization for some exposures [Rattray et al.
1994, Zhang et al. 2004]. The evidence that there is a similar association in humans is still quite
limited, however there are case reports of co-existing work-related allergic contact dermatitis and
allergic asthma [Lockman. 2002]. Occupational disease researchers are beginning to consider the
skin and the lungs as important routes of exposure [Redlich and Herrick. 2008].
In the case of experimental animal models, if dermal exposure is the route of sensitization, an
inhalation exposure is still required to trigger an asthma-like response. However, once sensitized,
the inhalation exposure required to trigger an asthma-like response may be much lower than the
exposure level required to sensitize the airways [Arts et al. 2006]. We hypothesize that if dermal
and airborne exposures do occur in the workplace there will be a portion of the working
population that experiences symptoms in both systems. These symptoms could be irritant or
allergic in nature. The goal of this study was to use previously collected data from four
occupational groups to determine if, and how many, workers experience both skin and
respiratory symptoms that they relate to their work.
4.3 Methods
Previously collected data from four cross-sectional studies were pooled for this analysis. The
four studies included workers from a soda ash production facility [Holness et al. 1989]
(exposure: ammonia), a softwood planing mill (exposure: softwood dust), embalming [Holness
and Nethercott. 1989] (exposure: formaldehyde and glutaraldehyde) and cabinet making [Sass-
Kortsak et al. 1986] (exposure: hardwood dust). All studies were initially designed to study
work-related skin problems and/or work-related lung problems. The study of respiratory effects
in softwood planing mill workers has not been previously published. Briefly, this was a cross-
sectional study of fifty softwood sawmill workers. The workers’ respiratory and cutaneous
statuses were evaluated and dust exposure was measured over a work-week, allowing exposure-
effect relationships to be assessed. The research ethics board at St Michael’s Hospital in Toronto,
Canada, approved all original studies.

56
In each study, information on self-reported skin and respiratory symptoms was obtained using an
interviewer-administered questionnaire. Data on basic demographics (e.g., age, sex, smoking) as
well as self-reported symptoms were collected. Pulmonary function was measured and is
reported as percent of predicted forced expiratory volume in one second (FEV1) based on the
equations of Crapo et al. [Crapo et al. 1981]. Respiratory symptom questions were based on the
American Thoracic Society Questionnaire (ATSQ). The question employed for skin rash was as
follows, “Do you have a skin rash?”. A subject was considered to have at least one respiratory
symptom if they said yes to any of the cough, wheeze, shortness of breath or phlegm questions.
In order to determine the respiratory symptom’s relation to the subjects’ work, subjects were
asked “Is your [cough/wheeze/shortness of breath/phlegm] better, worse, unchanged when
you’re at work?” For skin rash, subjects were asked “Is your [skin] rash better, worse, unchanged
when you’re [at work/on holiday/on layoff]?”
Differences between occupational groups were investigated using chi-square tests and ANOVA
with post-hoc Scheffe. The prevalence of self-reported respiratory and skin symptoms was
determined using basic descriptive statistics. Subjects were divided into four possible symptom
groups: no symptoms, only skin symptoms, only respiratory symptoms and both skin and
respiratory symptoms. Between group differences in age, sex, pulmonary function and smoking
were examined. All analyses were completed using SAS v.9.2.
4.4 Results
A total of 247 workers were included in this analysis (Table 12). The individual studies had
sample sizes ranging from 50 to 86 (average 62). The entire population was male, except for 9
female embalmers. The mean age of subjects was 36.4 years (sd 12.7). Cabinet makers were
significantly older than all other groups (p<0.0001). There was no difference in the proportion of
ever smokers between the studies though among smokers, cabinet makers had more pack-years
of smoking (p=0.0023), likely due to their older age. Pulmonary function, reported as percent-
predicted FEV1, was approximately normal for all groups; there were no differences between
studies in measures FEV1 percent predicted.
A total of 113 (46%) workers reported at least one respiratory symptom; 42 (17%) reported a
skin rash. Overall, dyspnea was the least common self-reported symptom (n=33, 13%) and

57
phlegm was the most common (n=65, 26%). Cabinet makers were more likely than other
workers to report a cough (p=0.0444); no other differences were observed between study groups.
Of the 113 workers who reported at least one respiratory symptom, 34 (30%) reported at least
one respiratory symptom that was work-related. Wheeze was the most common work-related
symptom reported (n=15, 35% of self-reported wheeze). Overall, embalmers were significantly
less likely to report work-related respiratory symptoms compared with the other study groups
(p=0.0002).
Overall, 26 (11%) workers reported both skin and respiratory symptoms (range 6-17% across
occupational groups). Embalmers were the most likely to report both skin and respiratory
symptoms. Soda ash production workers had the highest prevalence of reporting skin symptoms
only and the lowest of respiratory symptoms only, however, these differences did not reach
statistical significance.
Subjects reporting both skin and respiratory symptoms were more likely to be female
(p<0.0001). No differences between the symptom groups were observed in age, smoking or
FEV1 percent predicted (Table 12).
There were four workers who reported work-related skin symptoms but no work-related
respiratory symptoms while 32 workers reported work-related respiratory symptoms and no
work-related skin symptoms. Only 2 workers reported both work-related skin and work-related
respiratory symptoms. These two workers were both male and worked in the Soda Ash
Production facility; neither reported allergies or asthma. One of the two workers was a smoker
with 21 pack years of smoking history; the other had never smoked. One worker was 36 years
old with normal lung function results (FEV1 92% pred., FVC 95% pred.), the other was 56 years
old with below predicted lung function (FEV1 71% pred., FVC 64% pred.).

58
Table 12 Skin and Respiratory Symptom Group Distribution (Work-Related and Non-
Work-Related) Across Studies and Description of Groups by Age, Sex, Smoking and
Pulmonary Function Variables. Symptom Frequencies Given as Row n (%). Demographic
Variables Given as Column n (%).
None Skin only
Respiratory
only
Both skin &
respiratory p-value
Symptoms
Overall 116 (47%) 16 (6%) 87 (35%) 26 (11%)
Soda Ash Prod 32 (55%) 7 (12%) 14 (24%) 5 (9%)
Cabinet 25 (50%) 2 (4%) 20 (40%) 3 (6%)
Softwood 23 (43%) 3 (6%) 23 (43%) 4 (8%)
Embalming 36 (43%) 4 (5%) 30 (36%) 14 (17%)
NS
Female 2 (2%) 0 (0%) 0 (0%) 7 (27%) <0.0001
Age (yrs), mean (sd) 36.2 (12.3) 35.2 (14.0) 37.0 (13.0) 36.3 (13.1) NS
Ever Smokers 75 (64%) 11 (68%) 64 (74%) 22 (84%) NS
Pack-yrs, mean (sd) 16.6 (18.2) 16.9 (19.7) 20.2 (18.8) 14.5 (18.3) NS
FEV1 % pred., mean (sd) 95.5 (12.8) 91.5 (16.6) 93.6 (11.7) 90.8 (12.6) NS
Work-Related Symptoms
Overall 207 (84%) 4 (1.6%) 32 (13%) 2 (0.8%) -
Soda Ash Prod 47 (81%) 1 (1.7%) 8 (14%) 2 (3.4%)
Cabinet 39 (78%) 1 (2.0%) 10 (20%) 0 (0%)
Softwood 41 (77%) 1 (1.9%) 11 (21%) 0 (0%)
Embalming 80 (95%) 1 (1.2%) 3 (3.6%) 0 (0%)
0.0301
Female 8 (3.8%) 1 (25%) 0 (0%) 0 (0%) NS b
Age, mean yr (sd) 35.3 (12.2) a 42.8 (13.5) 42.1 (14.3)
a 46.0 (14.1) 0.0179
Ever Smokers 145 (70%) 4 (100%) 22 (69%) 1 (5%) NS
Pack-yrs, mean (sd) 17.1 (18.5) 22.8 (14.8) 20.8 (19.8) 21.6 (-) NS
FEV1, % pred., mean (sd) 94.2 (12.4) 80.9 (3.9) 95.8 (13.4) 79.4 (22.1) NS b
a significantly different groups in post hoc comparisons;
b 0.05 < p < 0.10

59
4.5 Discussion
Among workers in four different occupational groups the prevalence of co-existing skin and
respiratory symptoms was 11%. These subjects were more likely to work in embalming and be
female, though these variables were highly correlated. No differences in smoking, age or FEV1
percent predicted were observed between symptom groups.
The prevalence of skin symptoms (14%) and respiratory symptoms (range 18-35%) is similar to
other studies in occupational populations by the same research group [Nethercott and Holness.
1988, Holness et al. 1984]. Very few studies have reported the prevalence of co-existing skin and
respiratory symptoms. A recent study by Lynde et al. among professional cleaners reported a
much higher prevalence of co-existing skin and respiratory symptoms. In this study, among
workers with a current rash almost two-thirds reported two or more work-related respiratory
symptoms [Lynde et al. 2009].
The reported prevalence of co-existing symptoms in the dermal and respiratory systems does not
indicate whether the symptoms are related to the same exposure, nor does it provide an
indication of whether the symptoms are due to allergic or irritant mechanisms. The reported
prevalence simply indicates that in working populations that have demonstrated airborne and/or
dermal exposure to agents capable of causing allergic and/or irritant responses there exists a
group of workers who report symptoms in both systems, and a small portion of these workers
identify these symptoms as being associated with their jobs.
The workers with co-existing skin and respiratory symptoms make up a small portion (11%) of
the workers in this sample. This group of workers is important because they demonstrate that in
workplaces where one route of exposure may be recognized as the most hazardous, some
workers still report symptoms in other systems. However, of these workers only a small number
reported that their symptoms were related to their work.
The hypotheses of how the skin and the lung may interact in terms of exposure and outcomes are
complex. If a worker is sensitized due to dermal exposure, a respiratory response may be
triggered by relatively low airborne exposure. This has implications for exposure control because
airborne exposure limits may prevent airways sensitization but may not be protective for
elicitation in the airways of a sensitized worker.

60
This study shows that there is a portion of workers who experience both skin and respiratory
symptoms that they attribute to their work. As we continue to further investigate the potential
interaction between the skin and the respiratory system in terms of exposure and disease we need
to ensure that we collect thorough information about exposure and response in both systems,
using quantitative measurements in addition to self-reported symptoms where possible.
Although there is a need to understand how the skin and respiratory exposure routes contribute to
occupational respiratory disease, it is clear that both dermal and airborne exposures must be
minimized in the occupational setting. The techniques for achieving reduction and elimination of
occupational exposures are well understood and should be applied in the workplace.

61
Chapter 5 Skin Symptoms in Bakery and Auto Body Shop Workers: Associations with Exposure and Respiratory Symptoms
Victoria H. Arrandale1, Tim Meijster
2, Anjoeka Pronk
2, Gert Doekes
3, Carrie A. Redlich
4, D.
Linn Holness1, Dick Heederik
3
1 Centre for Research Expertise in Occupational Disease, University of Toronto, Canada
2 TNO Quality and Safety, Zeist, The Netherlands
3 Environmental Epidemiology Department, Institute for Risk Assessment Sciences, Utrecht
University, The Netherlands
4 Yale University School of Medicine, New Haven, CT USA
This manuscript was e-published ahead of print by the International Archives of Occupational
and Environmental Health on March 13, 2012. Copyright permission has been granted (see
Copyright Acknowledgements).

62
5.1 Abstract
Background: Despite the importance of skin exposure, studies of skin symptoms in relation to
exposure and respiratory symptoms are rare. The goals of this study were to describe exposure-
response relationships for skin symptoms, and to investigate associations between skin and
respiratory symptoms in bakery and auto body shop workers.
Methods: Data from previous studies of bakery and auto body shop workers were analyzed.
Average exposure estimates for wheat allergen and diisocyanates were used. Generalized linear
models were constructed to describe the relationships between exposure and skin symptoms, as
well as between skin and respiratory symptoms.
Results: Data from 723 bakery and 473 auto body shop workers were analyzed. In total, 5.3% of
bakery and 6.1% of auto body shop workers were female; subjects’ mean age was 39 and 38
years, respectively. Exposure-response relationships were observed in auto body shop workers
for itchy or dry skin (PR 1.55, 95% CI 1.2-2.0) and work-related itchy skin (PR 1.97, 95% CI
1.2-3.3). A possible exposure-response relationship for work-related itchy skin in bakery workers
did not reach statistical significance. In both groups reporting skin symptoms was strongly and
significantly associated with reporting respiratory symptoms, both work-related and non-work-
related.
Conclusions: Exposure-response relationships were observed for skin symptoms in auto body
shop workers. The lack of significant exposure-response associations in bakery workers should
be interpreted cautiously. Workers who reported skin symptoms were up to four times more
likely to report respiratory symptoms. Improved awareness of both skin and respiratory
outcomes in exposed workers is needed.

63
5.2 Introduction
The connection between skin and respiratory systems in occupational disease is a growing area
of research interest [Redlich and Herrick. 2008]. Specifically, there is interest in determining
whether the skin can be an important route of sensitization for occupational allergens and
subsequent development of occupational respiratory symptoms, including asthma. Research in
this area is challenging, in part due to the organ system silos that have historically existed in
medicine and epidemiological research.
Recent evidence from animal models suggests that after sensitization through skin exposure to
some high (e.g., latex) and low (e.g., trimellitic anhydride, toluene diisocyanate (TDI)) molecular
weight agents, an asthma-like response can be elicited upon inhalation exposure [Vanoirbeek et
al. 2004, Zhang et al. 2009]. Evidence of possible cross-system sensitization and elicitation in
humans is scarce. Among methylene diphenyl diisocyanate (MDI) exposed workers, Petsonk et
al. observed that subjects reporting skin staining (a proxy for skin exposure) were more likely to
report asthma-like symptoms [Petsonk et al. 2000].
Despite the possibility that skin exposures can contribute to the burden of respiratory disease,
studies focusing on skin exposure, and specifically on exposure-response studies for skin
symptoms and/or sensitization, are rare. This lack of evidence limits the ability to infer causality
between skin exposure and response, and may ultimately hamper efforts to better control both
skin exposure as well as skin and respiratory symptoms in the workplace. Studies on skin
symptoms in relation to exposure do exist [de Joode et al. 2007, Sripaiboonkij et al. 2009b,
Sripaiboonkij et al. 2009a], but even less information is available on the associations between
exposure, skin and respiratory symptoms as well as the relationship between skin and respiratory
effects. Many occupational studies report the prevalence of both skin and respiratory symptoms
but rarely explore the relationship between the two, or the prevalence of these symptoms
coexisting. Lynde et al. reported that among male cleaners, those with skin symptoms were more
likely to report respiratory symptoms [Lynde et al. 2009].
The mechanisms of airborne and skin exposure are complex. Airborne and skin exposures can be
related if they share sources, but these associations are so far poorly studied [Schneider et al.
1999]. Associations between skin and airborne exposures have been reported for bitumen and

64
pyrene in road pavers, 1,6-hexamethylene diisocyanate (HDI) in spray painters, methylene
bisphenyl isocyanate (MDI) in foundry works, solvents in spray painters and nickel exposure in
primary industries [McClean et al. 2004, Burstyn et al. 2002, Chang et al. 2007a, Fent et al.
2008, Liljelind et al. 2010, Hughson and Cherrie. 2005]. In two other studies, both involving
pesticide exposure, there was no association found between skin and airborne exposure. The
authors attribute this lack of association to the fact that the primary source of skin exposure was
likely contact with contaminated foliage rather than the settling of airborne pesticide [Flack et al.
2008, Aprea et al. 2009].
Bakery and auto body shop workers have both skin and respiratory exposures to known
occupational allergens, making them good candidates for further study of exposure-response
relationships for skin symptoms, as well as the relationship between skin and respiratory
symptoms. Bakery and auto body shop workers are at increased risk of occupational asthma
(OA) as well as occupational skin disease (OSD) due to their workplace exposures: flour dust
and diisocyanates , respectively [McDonald et al. 2005, McDonald et al. 2006]. Flour dust is a
common cause of occupational asthma in bakers. Flour dust, which includes wheat and α-
amylase allergens among others, contains high molecular weight (HMW) antigens which act
through an IgE mediated (Type I) immunological pathway to cause OA and contact urticaria, and
can also cause contact dermatitis through a Type IV (cell-mediated) mechanism [Nethercott and
Holness. 1989]. Isocyanates are a heterogeneous group of compounds, including monomers and
oligomers, categorized as low molecular weight (LMW) antigens. The mechanism of action
leading to isocyanate-induced OA is not yet fully understood and though IgE (Type I) mediated
processes appear to play a role in some cases, other unrevealed mechanisms play a role in
respiratory sensitization [Maestrelli et al. 2009, Wisnewski. 2007]. Similar to flour dust,
diisocyanates can also cause contact dermatitis (Type IV) [Donovan et al. 2009, Frick et al.
2003].
The goals of this study are to describe the exposure-response relationships for skin symptoms in
both bakery workers and auto body shop workers, and to investigate the association between skin
and respiratory symptoms in these two groups.

65
5.3 Methods
Reports on respiratory outcomes in both the bakery and auto body shop workers studies have
been published previously [Pronk et al. 2007, Jacobs et al. 2008]. Workers were asked to
complete a questionnaire on respiratory and skin symptoms, an exposure questionnaire and also
to provide a blood sample for analysis. For this analysis subjects were required to have complete
data for both respiratory and skin symptoms, as well as atopy and workplace allergen specific
IgE. In total, 723 bakery workers and 472 auto body shop workers were included in this analysis,
which is a slightly different study population than previous publications [Pronk et al. 2007,
Jacobs et al. 2008].
5.3.1 Exposure
In both groups (bakery and auto body shop workers), exposure was estimated based on existing
data sets of personal airborne exposure measurements [Pronk et al. 2006a, Meijster et al. 2007].
Cumulative monthly hexamethylene diisocyanate (HDI) exposure was estimated using task-
based measurements of airborne diisocyanates combined with self-reported monthly frequencies
of task completion as was described previously [Pronk et al. 2007]. This exposure metric was
then divided by the self reported average number of hours worked per month to determine the
long-term average diisocyanate exposure of these workers (µg-NCO*m-3), which facilitated
comparison with the bakery workers. Average wheat exposure for bakery workers was estimated
using subjects’ work characteristics (exposure determinants) reported on the questionnaire
combined with an exposure model constructed by Meijster et al., to predict average wheat
exposures (µg-dust*m-3) for each subject [Meijster et al. 2007].
A relatively small number of task based skin exposure measurements were available for
diisocyanate exposure in auto body shops, but no comparable exposure measurements were
available in bakery workers. As a result this study investigates the exposure-response
relationships for skin symptoms, using airborne exposure as a proxy for skin exposure in both
working populations. In auto body shop workers, airborne exposure was not significantly
associated with having a detectable skin diisocyanate exposure (OR 1.34, 0.97-1.84), but the
analysis was limited by small number of samples and a direct correlation was not calculated
[Pronk et al. 2006b].

66
5.3.2 Specific IgE and Atopy
Specific IgE was measured using commercially available kits as previously described [Pronk et
al. 2007, Jacobs et al. 2008]. In bakery workers specific IgE was measured for wheat protein
(Bakery, Pharmacia, Unicap System, Pharmacia Diagnostics, Uppsala, Sweden); in auto body
shop workers specific IgE to HDI oligomers (N100-HSA) was measured (Diisocyanates: Phadia,
Uppsala Sweden). All samples were also tested for specific IgE to common aeroallergens (house
dust mite, cat, dog, grass or birch pollen) [Doekes et al. 1996]. Analytical results were
dichotomized and IgE (work-related or common allergens) was considered elevated if above
0.35kU/L. Subjects were classified atopic if they had elevated IgE in response to at least one of
the common aeroallergens.
5.3.3 Symptoms
Respiratory symptoms and skin symptoms were reported on a self-completed questionnaire
derived from the International Union Against Tuberculosis and Lung Disease (IUATLD) and the
Medical Research Council - European Community of Coal and Steel (MRC-ECCS) for the
bakery workers, and from the British Medical Research Council (BMRC) respiratory
questionnaire for auto body shop workers [Burney et al. 1989, van der Lende and Orie. 1972,
Medical Research Council on the Aetiology of Chronic Bronchitis. 1960]. Information on cough,
phlegm, wheeze, chest tightness, shortness of breath and self reported asthma were included. A
variable describing asthma-like symptoms (wheezing, chest tightness, current/previous asthma)
was constructed using the individual symptom responses. Skin itch and dry skin were reported
on the questionnaire; a dichotomous variable describing the presence of either itchy or dry skin
was constructed. Work-related symptoms were explicit items on the questionnaire. Subjects were
asked directly whether they have itchy skin at work and whether they experience asthma-like
symptoms at work. No work-related symptom variables were constructed post-hoc.
5.3.4 Additional Variables
Age, sex, smoking (current and historical) as well as years working were self-reported on the
questionnaire.

67
5.3.5 Analyses
Iterative non-parametric regression models (smoothing splines) with generalized additive models
(PROC GAM) were first used to explore the shape of the exposure-response relationships for
skin outcomes at the population level. These models were used to explore unadjusted non-linear
relationships between estimated exposure and symptoms outcomes. Generalized cross validation
(GCV) was used to select the smoothing parameter degrees of freedom (df); the df selected were
limited to four to avoid large fluctuations that are likely not biologically relevant [Hastie. 1990].
Generalized linear models (SAS PROC GENMOD) with a log function were used to estimate
unadjusted and adjusted prevalence ratios (PR) for the associations between exposure, atopy,
specific sensitization and symptoms. Adjusted models included atopy, work-related specific IgE
sensitization, age and sex; respiratory symptom models were additionally adjusted for smoking
status. Sensitivity analyses were completed to explore whether atopy and specific sensitization
were modifying the exposure-response relationships. Exposure-response relationships were
investigated in models where atopic and specific sensitized subjects were excluded. All PR
estimates for exposure effects are reported as the PR associated with an inter-quartile range
(IQR) increase in exposure.
Additionally, relationships between skin and respiratory symptoms were explored using
generalized linear models (PROC GENMOD) as described above with the same covariates and
including sensitivity analyses to explore the effect of atopy and work-related specific
sensitization. All analyses were completed in SAS v.9 software (SAS Institute Inc., Cary, NC,
USA).
5.4 Results
Both the auto body shop and bakery workers were predominantly male with an average age of
approximately 38 and 39 years respectively (Table 13). The distribution of smoking status was
similar between the two groups, though there were more never-smokers among the bakery
workers.
The prevalence of atopy among bakery and auto body shop workers was similar (34% vs. 36%,
respectively) but the prevalence of specific sensitization to workplace allergens was higher

68
among bakery workers (Table 13). Eleven percent of bakery workers had wheat-specific IgE;
only 2% of auto body shop workers had HDI-specific IgE.
Differences between the bakery and auto body shop workers were observed in symptom
frequencies (Table 13). We observed slightly more respiratory symptoms in auto body shop
workers and more skin symptoms in bakery workers. Estimated average exposure among auto
body repair shop workers ranged from 0 – 353µg-NCO*m-3 (IQR 21.4), and among bakery
workers from 0.35 – 95.6µg-wheat*m-3 (IQR 32.9) based on the previously collected exposure
measures.
Smoothing splines (Figure 3 and Figure 4) show the shape of the exposure-response distribution
for skin symptoms at a population level, stratified by atopy. Among bakers the exposure-
response relationship for skin symptoms appears to be linear in both the atopic and non-atopic
groups. However, in auto body shop workers a bell-shaped distribution is supported (df=3.7;
p<0.05) in non-atopic subjects. Similar analyses for respiratory symptoms have been previously
reported for both the bakery and auto body shop workers [Pronk et al. 2007, Jacobs et al. 2008].
Graphs for respiratory symptom models directly comparable to the skin symptom models
presented here are provided for comparison in Appendix 1 (Figure 7 and Figure 8).

69
Table 13 Demographics and Symptom Frequencies for Both Auto Body Repair and Bakery
Workers. All Frequencies Given as Column n (%).
Auto Body Repair
Workers
Bakery Workers
Demographics
Overall, n 473 723
Female, n (%) 29 (6.1%) 38 (5.3%)
Age, years, mean (sd) 38.0 (11) 39.0 (11)
Current smoker, n (%) 173 (37%) 238 (33%)
Former smoker, n (%) 130 (28%) 157 (22%)
Never smoker, n (%) 170 (36%) 328 (45%)
Years working, mean (sd) 17.6 (11%) 14.4 (11%)
Symptoms, n (%)
Cough 65 (14%) 83 (12%)
Wheeze, ever 111 (24%) 111 (15%)
Asthma, ever 72 (15%) 71 (9.8%)
Asthma Symptoms 134 (28%) 174 (24%)
Work-related asthma symptoms 20 (4.2%) 15 (2.1%)
Dry Skin in the last 12 months 113 (24%) 188 (26%)
Itchy Skin in the last 12 months 50 (11%) 208 (29%)
Either itchy or dry skin in the last 12 months 134 (28%) 265 (37%)
Work-related itchy skin 40 (8.5%) 122 (17%)
Atopy and Specific IgE, n (%)
Atopy 169 (36%) 245 (34%)
HDI specific IgE 10 (2.1%) -
Wheat specific IgE - 82 (11%)

70
Figure 3 Auto Body Shop Workers: Associations Between Average Diisocyanate Exposure
and Skin Symptoms, Shown in Smoothed Plots, Stratified by Atopy. Data rug indicates the
distribution of observations by exposure level. (a) Itchy or dry skin in atopic subjects
(linear: NS; spline: NS), (b) Work-related itchy skin in atopic subjects (linear: NS; spline:
NS), (c) Itchy or dry skin in non-atopic subjects (linear: NS; spline: df=1.05, p<0.05), (d)
Work-related itchy skin in non-atopic subjects (linear: NS; spline: df=3.71, p<0.05).

71
Figure 4 Bakery Workers: Associations Between Average Wheat Exposure and Skin
Symptoms, Shown in Smoothed Plots, Stratified by Atopy. Data rug indicates the
distribution of observations by exposure level. (a) Itchy or dry skin in atopic subjects
(linear: NS; spline: NS), (b) Work-related itchy skin in atopic subjects (linear: NS; spline:
NS), (c) Itchy or dry skin in non-atopic subjects (linear: NS; spline: NS), (d) Work-related
itchy skin in non-atopic subjects (linear: NS; spline: NS).

72
In auto body shop workers (Table 14), statistically significant exposure-response relationships
were observed for itchy or dry skin (PR 1.56, 95% CI 1.2-2.0) and work-related itchy skin (PR
1.97, 95% CI 1.2-3.3); a similar trend was observed in the bakery workers for work-related skin
symptoms but this did not reach significance (Table 14).
In auto body shop workers (Table 14), exposure was significantly related to specific HDI
sensitization (PR 10.0, 95% CI 1.4-73), with wide confidence limits likely due to the small
number of sensitized subjects. HDI specific sensitization was associated with itchy or dry skin
(PR 1.86, 95% CI 1.1-3.2) but not work-related itchy skin. Atopy predicted itchy or dry skin in
auto body shop workers (PR 1.26, 95% CI 1.0-1.7) but not work-related itchy skin.
Among bakery workers (Table 14), wheat exposure was not related to having wheat specific
sensitization, but wheat specific sensitization was associated with work-related itchy skin (PR
2.17, 95% CI 1.5-3.1). Atopy was associated with both itchy or dry skin (PR 1.45, 95% CI 1.2-
1.8) and work-related itchy skin (PR 1.67, 95% CI 1.2-2.3).
In both groups, exposure was negatively associated with atopy, though this relationship only
reached significance in the auto body shop workers (Table 14).
When atopy and specific sensitization were added to exposure-response models for skin
symptoms, the effect on prevalence ratios due to exposure remained relatively unchanged in both
groups (Table 15). Removing the atopic and sensitized (work-related specific IgE) subjects also
did not change the exposure relative risk estimates (results not shown).
The association between reporting skin symptoms and reporting respiratory symptoms was
investigated separately (Table 16). In both auto body shop and bakery workers, reporting
itchy/dry skin and work-related itchy skin was significantly associated with reporting wheeze
and asthma-like symptoms. Both work-related and non-work-related skin symptoms were
significantly associated with work-related chest tightness in auto body shop workers. In bakery
workers, work-related itchy skin was not significantly associated with work-related chest
tightness.

73
Table 14 Results of Generalized Linear Models Describing the Simple Relationship
Between Exposure, Skin Symptoms, Atopy and Specific IgE. Each Reported Prevalence
Ratio (PR) Was Estimated From a Separate Model. Models Adjusted for Age and Sex.
(WR=Work-related)
Independent Variable Dependant Variable PR (95% CI)
Auto Body Repair Workers (n=473):
Itchy or Dry Skin 1.56 (1.2-2.0)
WR Itchy Skin 1.97 (1.2-3.3)
Atopy 0.83 (0.7-1.0)
Average Diisocyanate Exposure (µg-
NCO*m-3)
HDI-Specific IgE 10.0 (1.4-73)
Atopy Itchy or Dry Skin 1.26 (1.0-1.7)
WR Itchy Skin 0.80 (0.4-1.5)
HDI-Specific IgE Itchy or Dry Skin 1.86 (1.1-3.2)
WR Itchy Skin 1.03 (0.2-6.8)
Bakery Workers (n=723):
Average Wheat Exposure (µg*m-3) Itchy or Dry Skin 0.96 (0.8-1.1)
WR Itchy Skin 1.16 (0.9-1.5)
Atopy 0.91 (0.8-1.1)
Wheat-Specific IgE 1.12 (0.8-1.5)
Atopy Itchy or Dry Skin 1.45 (1.2-1.8)
WR Itchy Skin 1.67 (1.5-3.1)
Wheat -Specific IgE Itchy or Dry Skin 1.22 (0.9-1.6)
WR Itchy Skin 2.17 (1.5-3.1)

74
Table 15 Prevalence Ratio (PR) of Symptoms per Inter-Quartile Range (IQR) Increase in
Average Exposure. Multivariate Models Adjusted for Atopy and Specific Sensitization in
Addition to Age, Sex and Smoking As Described.
Outcome Covariates PR (95% CI)
Auto Body Repair Workers (n=473)
Either itchy or dry skin in last 12 months A, S, Atp, IgE 1.55 (1.2-2.0)
Work-related itchy skin A, Atp, IgE 1.97 (1.2-3.3)
Bakery Workers (n=723)
Either itchy or dry skin in last 12 months A, S, Atp, IgE 0.96 (0.8-1.1)
Work-related itchy skin A, S, Atp, IgE 1.14 (0.9-1.5)
A=Age, S=Sex, Atp=Atopy, IgE=Work-related Specific IgE
Table 16 Association Between Skin Symptoms and Respiratory Symptoms in Both Bakery
and Auto Body Repair Workers. Reported as Prevalence Ratio of Respiratory Symptoms,
Adjusted for Age, Sex, Smoking and Atopy with 95% Confidence Intervals.
Auto Body Repair
Workers
Bakery Workers
Predictor Outcome PR (95% CI) PR (95% CI)
Wheeze, ever 2.01 (1.5-2.8) 1.94 (1.4-2.7)
Asthma-like symptoms 1.83 (1.4-2.4) 1.78 (1.4-2.3) Itchy or dry skin
in last 12 months WR asthma symptoms 4.06 (1.6-10) 3.90 (1.2-12)
Wheeze, ever 2.50 (1.7-3.6) 1.60 (1.1-2.3)
Asthma-like symptoms 2.12 (1.5-3.0) 1.54 (1.2-2.0) Work-related
itchy skin WR asthma symptoms 3.61 (1.4-9.4) 2.15 (0.7-6.3)

75
5.5 Discussion
Significant exposure-response relationships were observed between estimated exposure to
diisocyanates (µg-NCO*m-3) and skin symptoms in auto body shop workers. Such associations
have not been previously reported. Though similar trends were observed between wheat
exposure and work-related skin symptoms in bakery workers, the associations did not reach
statistical significance.
Both auto body repair and bakery workers who reported skin symptoms were consistently and
significantly more likely to report work-related and non-work-related respiratory symptoms.
These findings are comparable with results of Lynde et al. who showed that male cleaners with a
skin rash were more likely to report respiratory symptoms, particularly work-related respiratory
symptoms [Lynde et al. 2009].
The prevalence of skin symptoms reported in auto body shop workers and bakery workers is
similar to previous studies of skin outcomes in these populations. Randolph et al. reported that
32% of HDI exposed spray painters reported hand dermatitis, while Daftarian found 35% of TDI
exposed workers to have skin symptoms [Randolph et al. 1997, Daftarian et al. 2002]. Cullinan
et al. found that 11% of bakery and flour mill workers had skin symptoms [Cullinan et al. 2001].
Steiner et al. reported that 19% of all bakers and 31% of high-risk (higher likelihood of
exposure) bakers reported at least one skin symptom in the last 12 months [Steiner et al. 2011].
Previous research supports that self-reported skin symptoms are predictive of skin disease.
However, some results suggest that self-reported skin symptoms may over estimate [Smit et al.
1992, Lynde et al. 2009] or underestimate [Holness et al. 1995] the prevalence of disease when
compared with a physician examination. The use of picture based questionnaires and self-
reported doctor-diagnosed dermatitis may provide a prevalence estimate closer to that of
physician diagnoses, but may also underestimate prevalence [Smit et al. 1992].
Skin symptoms may be due to irritant or different immunologic (Type I or Type IV)
mechanisms. Though it is possible to differentiate between these outcomes in the clinical setting,
it is not possible to differentiate using symptoms reported on the questionnaire alone. The strong
relationship between wheat specific IgE and work-related itchy skin supports a role for the IgE
mediated (Type I) allergy in the development of work-related skin symptoms in bakery workers.

76
Parallel results for respiratory symptoms (Supplemental Material) also demonstrate strong
relationships between wheat specific IgE and both asthma-like symptoms and work-related chest
tightness. It is not possible to model the potential role of Type IV allergy or irritant mechanisms
in symptom development in this study.
The bell shaped (non-linear) distribution observed for non-atopic auto body shop workers in the
smoothing splines (Figure 3) may be the result of a healthy worker effect, with fewer
symptomatic subjects at the higher exposure levels. The negative association between exposure
and atopy in both the auto body shop and bakery workers also suggests a healthy worker effect
(Table 14).
The prevalence of work-related allergen specific sensitization was five times higher in bakery
workers (11%) compared to auto body shop workers (2%). The low prevalence of HDI specific-
IgE sensitization is well documented in other studies and is commonly interpreted as indicating
mechanisms other than IgE sensitization are responsible for the development of symptoms in
exposed workers [Maestrelli et al. 2009, Wisnewski. 2007].
Atopy and work-related sensitization were strongly associated in both auto body shop workers
(PR 13.8, 95% CI 1.7-109) and bakery workers (PR 2.62, 95% CI 1.9-3.6).
The correlation between these two variables necessitated caution when offering both variables to
the same model. Models where adjustment for atopy and specific sensitization was desired were
first constructed separately and estimates were compared with those from models including both
variables. In the end, estimates from the separate models were comparable and both variables
were offered into all of the combined models.
In general, auto body shop workers tended to report more respiratory symptoms, while bakery
workers tended to report more skin symptoms. This could be due, in part, to differences in
exposure prevention activities. Unfortunately self-reported use of personal protective equipment
was only available for auto body shop workers, preventing a comparison of this effect.
Observations by the researchers in the field suggest that differences did exist between the two
populations, specifically that bakery workers did not use hand or respiratory protection while
auto body shop workers tended to use both. A significant exposure-response relationship was

77
observed in the auto body shop workers, the group observed to use PPE, suggesting that in these
workers PPE use did not reduce exposure to a level that was trivial with respect to health effects.
Estimates of airborne exposure were used in the exposure-response models as a crude proxy for
skin exposure, so results should be interpreted as airborne exposure-skin symptom associations.
It is plausible that the airborne exposure estimates provide a good surrogate of skin exposure.
Results from previous studies have shown a relatively strong association between skin and
airborne exposures in auto body shop workers [Fent et al. 2008, Liljelind et al. 2010]. No reports
comparing skin and airborne exposures in bakery workers were located. It is possible that
airborne exposure may be a better surrogate for skin exposure in the auto body shops, resulting
in less exposure misclassification among auto body shop workers compared to bakery workers. It
may also be that average diisocyanate exposure (µg-NCO*m-3), or another exposure which was
correlated with diisocyanates, was the causal exposure for skin symptoms in auto body shop
workers, but that an exposure other than average wheat exposure (µg-wheat*m-3) was
responsible for skin symptoms among bakery workers (i.e., wet work, oils etc.).
Despite the observed associations between atopy, specific sensitization and skin symptoms the
exposure-response relationships remained unchanged in sensitivity analyses. When atopic and
specifically sensitized subjects were excluded from the models the exposure-response
relationships for skin symptoms in auto body shop workers persisted and the effect estimates
were not attenuated. This provides support for the existence of an exposure-response relationship
between NCO exposure and skin symptoms (work-related and non-work-related) in auto body
shop workers.
In the second analysis, reported skin symptoms were predictive of reporting respiratory
symptoms in both occupational groups regardless of the symptom combination, an association
that has rarely been investigated [Lynde et al. 2009]. Results were unchanged after adjustment
for age, sex, smoking and atopy. The persistence of the association after adjustment for these
variables suggests that there are other factors that lead to the co-existing skin and respiratory
symptoms (i.e., exposure). These results highlight the importance of considering both skin and
respiratory outcomes in exposed workers as well as the importance of properly assessing both
skin and airborne exposure in the workplace.

78
In conclusion, reporting skin symptoms was strongly and consistently associated with reporting
respiratory symptoms in both bakery and auto body shop workers. Additionally, exposure-
response relationships for skin symptoms were observed in auto body shop workers, similar
relationships for work-related skin symptoms in bakery workers did not reach statistical
significance. There are several reasons why an association may have been missed in bakery
workers, including poor correlation between airborne and skin exposure for the particulate
exposure and the lack of information on other, potentially causal, exposures in the workplace.
The lack of observed association in bakery workers should be interpreted cautiously; exposure-
response relationships for skin symptoms require more investigation in all occupations. These
relationships must be better understood before more complex relationships are investigated,
however the overall goal remains the reduction of both airborne and skin exposure.

79
Chapter 6 Skin and Respiratory Symptoms Among Workers with Suspected Work-Related Disease
Victoria H. Arrandale1, Irena Kudla
2, Allen G. Kraut
3, Jeremy A. Scott
1, Susan M. Tarlo
1,2,4,
Carrie A. Redlich5, D. Linn Holness
1,2
1 University of Toronto, Toronto, Ontario, CANADA
2 St. Michael’s Hospital, Toronto, Ontario, CANADA
3 Faculty of Medicine, University of Manitoba, Winnipeg, Manitoba, CANADA
4 Toronto Western Hospital, Toronto, Ontario, CANADA
5 Yale University School of Medicine, New Haven, Connecticut, USA
This manuscript is currently under review by Occupational Medicine (Oxford).

80
6.1 Abstract
Background: Many workers are exposed to chemicals that can cause both respiratory and skin
responses. Although there has been much work on respiratory and skin outcomes individually,
there are few published studies examining lung and skin outcomes together. The objective of this
study was to identify predictors of reporting concurrent skin and respiratory symptoms in a
clinical population.
Methods: Patients with possible work-related skin or respiratory disease were recruited. An
interviewer-administered questionnaire collected data on skin and respiratory symptoms, health
history, smoking habits, workplace characteristics and occupational exposures. Predictors of
concurrent skin and respiratory symptoms were identified using multiple logistic models.
Results: In total, 204 subjects participated; 46% of the subjects were female and the mean age
was 45.4 years (sd 10.5). Most subjects (n=167, 82%) had possible work-related skin disease,
compared to only 37 (18%) subjects with possible work-related respiratory disease. Subjects
with a history of eczema (OR 3.68, 95% CI 1.7-7.8), those from larger (>499 employees)
workplaces (OR 2.82, 95% 1.8-7.4) and those reporting respirator use at work (OR 2.44, 95% CI
1.2-4.8) had significantly greater odds of reporting both work-related skin and respiratory
symptoms. Current smoking was also associated with reporting concurrent skin and respiratory
symptoms (OR 2.57, 95% CI 1.2-5.8).
Conclusions: Workers do report symptoms in both systems; this may be under-recognized both
in the workplace and in the clinic. The association between history of doctor-diagnosed eczema
and concurrent skin and respiratory symptoms suggests role for impaired barrier function and
this finding needs further investigation.

81
6.2 Introduction
Many workers are exposed to chemicals that can cause lung and skin responses as a result of
both inhalation and skin exposure. Although there has been significant work focused on
individual lung or skin outcomes and their association with exposures, there are few published
studies examining both airborne and skin exposures with lung and skin outcomes together. This
is important clinically, as disease in the one system may be under-recognized when workers are
assessed by physicians who are specialist in the other system. It is also important from a
prevention standpoint, because opportunities for exposure control and prevention may be missed
if research focuses on either airborne or skin exposure.
There is also increasing interest in the role that skin exposure may play in sensitization and the
development of respiratory symptoms and/or disease [Day et al. 2006, Redlich. 2010]. In
humans, the role of skin exposure in the development of occupational asthma has been examined
almost exclusively in diisocyanate exposure scenarios [Petsonk et al. 2000, Bello et al. 2008]
though studies in animal models suggest this pathway may exist for other exposures [Vanoirbeek
et al. 2006, Arts et al. 2004]. Animal studies demonstrate that in order for the skin to act as a
relevant route of sensitization in the development of occupational asthma, both a skin and an
inhalation exposure are required [Vanoirbeek et al. 2004, Kuper et al. 2011].
It is also known that occupational airborne and skin exposures may be correlated [Fent et al.
2008, Liljelind et al. 2010]. The skin exposure model proposed by Schneider et al. suggests that
there is a compartmental connection between airborne and skin exposure based on contribution
of one to the other (and vice versa) [Schneider et al. 1999]. This connection means it is plausible
that when the contribution of airborne exposure to skin exposure via deposition is high, the two
exposures (airborne and skin) will be correlated. In addition to correlations between skin and
airborne exposure levels, there is evidence that several common contact sensitizers are also
associated with occupational asthma [Arrandale et al. 2012].
Individually, exposure-response relationships have been reported between occupational exposure
and skin symptoms [de Joode et al. 2007, Sripaiboonkij et al. 2009a], though studies of
exposure-response for respiratory symptoms are far more common. There has been little research
on causal exposures or risk factors for reporting concurrent skin and respiratory symptoms,

82
despite a number of case studies of workers with allergic contact dermatitis and occupational
asthma in response to the same occupational exposure [Moulin et al. 2009, De Raeve et al.
1998].
Given that some workers are likely to have both skin and inhalation exposures, and that these
exposures may be correlated, it is plausible that some workers may experience both skin and
respiratory symptoms. Aside from one clinical study and one occupational study, this issue has
received little attention in previous research [Moulin et al. 2009, Lynde et al. 2009].
The primary objective of this study was to estimate the prevalence of concurrent skin and
respiratory symptoms in a clinical population, and to determine how workers with concurrent
skin and respiratory symptoms differ from those with symptoms in only one system (skin or
respiratory).
6.3 Methods
Subjects were recruited consecutively from a hospital-based outpatient occupational health clinic
between July 2009 and June 2010. Patients with possible work-related respiratory disease were
seen through the Allergy/Asthma (AA) clinical stream and those with possible work-related skin
disease were seen through the Dermatology (Derm) clinical stream; both were eligible to
participate. In both streams, patients were either referred through the public health care insurance
system (Ontario Health Insurance Plan - OHIP), or through the workers’ compensation insurance
system (Workplace Safety Insurance Board - WSIB).
Patients provided written informed consent. An interviewer-administered questionnaire was
completed during the clinic visit by one of two trained interviewers. If there was insufficient time
to complete the questionnaire, subjects were given the option of completing the questionnaire via
telephone. The questionnaire contained questions on respiratory symptoms (modified ATS
questionnaire [Ferris. 1978]), skin symptoms, health history, smoking history, workplace
characteristics and workplace exposures. Following the clinic visit(s), the final physician
diagnosis was abstracted from the subjects’ medical chart.

83
6.3.1 Outcome Variables
The main outcome of interest was concurrent, skin and respiratory symptoms. This was
conceptualized as subjects who reported any respiratory symptom (any of cough, phlegm,
wheeze, shortness of breath, or chest tightness) as well as current skin rash. The portion of
subjects reporting concurrent skin and respiratory symptoms that were both work-related was
also determined. In descriptive analysis, both the prevalence of current hand or arm rash as well
as the prevalence of asthma symptoms (defined as wheeze accompanied by shortness of breath
but without a cold/flu occurring in the last 12 months [Pekkanen et al. 2005]) were also
investigated.
6.3.2 Predictor Variables
Variables considered as possible predictors of concurrent symptoms included: history of asthma,
history of eczema, workplace size, use of gloves at work, use of a respirator at work, occupation,
insurance scheme (workers’ compensation vs. public system), clinical stream (asthma/allergy vs.
dermatology), presence of a union in the workplace, workplace education on personal protective
equipment, workplace education on occupational disease(s) and a series of possible workplace
exposures (cement, dander, dust, fumes, isocyanates, paints, pesticides, wet work and others).
Age and sex were reported on the questionnaire. Smoking included any reported tobacco
smoking. Atopy was defined based on subjects’ positive responses to having allergies to dust,
dust mites or other animals, or having had doctor-diagnosed hay fever [Lakwijk et al. 1998].
Previous asthma and eczema were recorded as a positive response to both “have you ever had
asthma/eczema?” and, “was it confirmed by a doctor?”
Workplace size was categorized into four groups based on the number of employees (<20, 20-
99,100-499 and >500) [Industry Canada. 2011]. Self-reported job title and industry information
was coded using the National Occupational Classification System (NOCS) [Statistics Canada.
2011]. Occupations were further condensed into 6 groups (trades, sales/service, office,
manufacturing, health, other) due to small sample sizes in the major NOCS groupings.
Workplace education variables included education on skin and/or respiratory personal protective
equipment and occupational disease.

84
6.3.2.1 Reliability Testing
We also measured the test-retest reliability of the workplace characteristics and workplace
exposure sections of a detailed occupational hygiene questionnaire that was already used in the
clinic setting. Subjects who consented to participate in further research were selected randomly
and contacted by telephone. Subjects were required to have no significant changes at their job
since first completing the questionnaire in order to participate. Results of the test-retest reliability
portion of this study are shown in Appendix 3.
6.3.3 Statistical Analyses
Differences between participants and patients who refused to participate were tested using chi
square for categorical variables and Student’s t-test continuous variables. Cohen’s Kappa,
percent observed agreement, percent positive agreement and percent negative agreements were
calculated to assess the reliability of the workplace questionnaire.
Possible predictors of concurrent symptoms were first investigated using simple logistic
regression. The outcome in these models was concurrent skin and respiratory symptoms; the
comparison group was subjects who reported either skin or respiratory symptoms but not both.
Predictors where the parameter estimate in simple logistic regression results had a p < 0.20 were
offered into multiple logistic models. Multiple logistic regression models were adjusted for age,
sex, smoking, atopy and interviewer. A nested model comparing subjects with respiratory
symptoms only to subjects with skin symptoms only was also constructed in the same manner.
All analyses were completed in SAS v.9 software (SAS Institute Inc., Cary, NC, USA). The
study was approved by the St Michael’s Hospital Research Ethics Board (Toronto, ON, Canada).
6.4 Results
In total, 218 subjects were successfully recruited with a response rate of 81%. Figure 5 shows a
flow chart of the study progression with the sample sizes at each stage. Thirty-three patients were
not approached at the discretion of the staff/physician or due to higher than usual activity in the
clinic. Fourteen subjects were excluded from analyses as they reported neither skin nor
respiratory symptoms. The sample size for the reported analysis is 204 subjects.

85
Figure 5 Flow Chart of Study Progression, Including Sample Sizes at Each Stage.
Patients who refused study participation did not differ from the participants in terms of age or
sex (Appendix 3) but those who declined participation were more likely to be from the AA
clinical stream (32% vs. 13%, p = 0.0007) (Appendix 3). Patients who declined participation also
tended to be referred more often through the provincial worker’s compensation system rather
than the main public health care system (21% vs. 13%, p = 0.07) though this difference did not
reach statistical significance.
Of the total 204 subjects, most (n = 167, 82%) had possible work-related skin disease and were
seen through the dermatology (Derm) stream; only 37 (18%) subjects were seen in the
asthma/allergy (AA) stream with possible work-related respiratory disease. This distribution of
participants between the Derm and AA streams is reflective of the overall patient breakdown in
the clinic. The participation rates were 86% and 68% for the Derm and AA streams, respectively.
Twenty-two (59%) AA subjects and 117 (70%) Derm subjects were diagnosed with work-related
disorders after their assessment. An additional 4 (11%) AA subjects and 31 (19%) Derm subjects
were diagnosed with a possible work-related disorder. Just under half (46%) of the subjects were
female and the mean age was 45.4 years (sd 10.5) (Table 17). Fifty-one percent of subjects had a
smoking history, either former or current. Almost one-quarter of the study population self-
reported doctor-diagnosed asthma (Table 17), though asthma was more common in the AA
stream (40% vs. 11%, p < 0.0001).

86
Table 17 Demographic Description of Study Population, Stratified by Subjects Who
Reported Both Skin and Respiratory Symptoms. Overall Values Reported as Column n
(%), Symptom Values Reported as the Row n (%). Comparison between ‘Both Skin and
Respiratory Symptoms’ and ‘Skin Symptoms Only or Respiratory Symptoms Only’. NS
Not Significant (p > 0.05).
Overall
Skin Symptoms
Only or
Respiratory
Symptoms
Only
Both Skin and
Respiratory
Symptoms p-value
n 204 121 83
Female 94 (46%) 59 (63%) 35 (37%)
Male 110 (54%) 62 (56%) 48 (44%)
NS
Age in years, mean (sd) 45.4 (10.5) 45.7 (10.0) 45.1 (11.2) NS
Age <35 years 38 (19%) 20 (53%) 18 (47%)
Age 35-49 years 88 (43%) 55 (62%) 33 (38%)
Age ≥50 years 78 (38%) 46 (59%) 32 (41%)
NS
Never Smoker 98 (48%) 64 (65%) 34 (35%)
Former Smoker 50 (24%) 31 (62%) 19 (38%)
Current Smoker 56 (27%) 26 (46%) 30 (54%)
NS
Interviewer 1 115 (56%) 69 (60%) 46 (40%)
Interviewer 2 89 (44%) 52 (58%) 37 (42%)
NS
Telephone Questionnaire 5 (2%) 2 (40%) 3 (60%)
In Clinic Questionnaire 198 (98%) 118 (60%) 80 (40%)
NS
AA Clinical Stream 37 (18%) 31 (84%) 6 (16%)
Derm Clinical Stream 167 (82%) 90 (54%) 77 (46%)
0.0008
Workplace Insurance 91 (45%) 59 (65%) 32 (35%)
Public Insurance 113 (55%) 62 (55%) 51 (45%)
NS
Atopy 68 (33%) 42 (62%) 26 (38%) NS
History of Asthma 50 (24%) 29 (58%) 21 (42%) NS
History of Eczema 54 (26%) 20 (37%) 34 (63%) 0.0001

87
Among the study subjects, symptom prevalence was high, as expected in a clinical population
(Table 18). General concurrent skin and respiratory symptoms were reported by approximately
one-third of the subjects (Table 18) but work-related concurrent symptoms were only reported by
18% of subjects.
Among the subjects being assessed for possible work-related skin disease (Derm stream), 30%
reported at least one work-related respiratory symptoms and 6% reported work-related asthma
symptoms. Work-related skin symptoms were less common in the AA stream, but were still
reported (11% work-related rash, 8% work-related hand/arm rash) (Table 18).
Table 18 Skin and Respiratory Symptom Prevalence, Stratified by Clinical Stream. All
Frequencies Reported as Column n (%).
Clinical Stream
Overall Dermatology Asthma/Allergy
n 204 167 37
General Symptoms:
Current Skin Rash 146 (72%) 140 (84%) 6 (16%)
Hand/Arm Rash 134 (66%) 130 (78%) 4 (11%)
Any Respiratory Symptom 141 (69%) 104 (62%) 37 (100%)
Asthma-like Symptoms 48 (24%) 24 (14%) 24 (65%)
Work-Related Symptoms:
Current Skin Rash 129 (63%) 125 (75%) 4 (11%)
Hand/Arm Rash 120 (59%) 117 (70%) 3 (8%)
Any Respiratory Symptom 83 (41%) 50 (30%) 33 (89%)
Asthma-like Symptoms 33 (16%) 11 (6%) 22 (59%)
Concurrent Skin and Respiratory Symptoms 83 (41%) 77 (46%) 6 (16%)
Concurrent Work-Related Skin and
Respiratory Symptoms 40 (20%) 36 (22%) 4 (11%)

88
Reported glove use at work was higher (90%) than the reported use of a respirator (39%) (Table
19). More than half of the subjects (53%) reported having had workplace education about
personal protective equipment, but only 14% reported having education that addressed the topic
of work-related disease.
Dust was the most commonly reported occupational exposure (68%); exposure to wet work
(65%), fumes (55%) and paint (41%) were also common exposures (Table 20). None of the self-
reported exposures were associated with reporting concurrent skin and respiratory symptoms.
Table 19 Self-Reported Workplace Characteristics, Stratified by Subjects Who Reported
Both Skin and Respiratory Symptoms. Overall Values Reported as Column n (%),
Symptom Values Reported as the Row n (%). Comparison between ‘Both Skin and
Respiratory Symptoms’ and ‘Skin Symptoms Only or Respiratory Symptoms Only’. NS
Not Significant (p > 0.05).
Overall
Skin Symptoms
Only or
Respiratory
Symptoms Only
Both Skin and
Respiratory
Symptoms p-value
Unionized 98 (48%) 62 (63%) 36 (37%) NS
< 20 Employees 52 (25%) 31 (60%) 21 (40%)
20-99 Employees 57 (28%) 38 (67%) 19 (33%)
100-499 Employees 52 (25%) 34 (65%) 18 (35%)
>499 Employees 43 (21%) 18 (42%) 25 (58%)
NS
Gloves Use 183 (90%) 105 (57%) 78 (43%) NS
Respirator Use 80 (39%) 39 (49%) 41 (51%) 0.0136
Trades 49 (24%) 28 (57%) 21 (43%)
Sales and Service 42 (20%) 25 (60%) 17 (40%)
Manufacturing 38 (19%) 25 (66%) 13 (34%)
Health Related 30 (15%) 12 (40%) 18 (60%)
Office Workers 27 (13%) 19 (70%) 8 (30%)
Other Occupations 18 (9%) 12 (67%) 6 (33%)
NS
PPE Education 108 (53%) 59 (55%) 49 (45%) NS
WR Disease
Education 28 (14%) 14 (50%) 14 (50%)
NS

89
Table 20 Self-Reported Workplace Exposures, Stratified by Subjects Who Reported Both
Skin and Respiratory Symptoms. Overall Values Reported as Column n (%), Symptom
Values Reported as the Row n (%). Comparison between ‘Both Skin and Respiratory
Symptoms’ and ‘Skin Symptoms Only or Respiratory Symptoms Only’. NS Not Significant
(p > 0.05).
Overall
Skin Symptoms Only
or Respiratory
Symptoms Only
Both Skin and
Respiratory
Symptoms p-value
Cement 41 (20%) 21 (51%) 20 (49%) NS
Animal Dander 25 (12%) 14 (56%) 11 (44%) NS
Dust 139 (68%) 85 (61%) 54 (39%) NS
Fume 113 (55%) 69 (61%) 44 (39%) NS
Isocyanate 32 (16%) 17 (53%) 15 (47%) NS
Paint 84 (41%) 52 (62%) 32 (38%) NS
Pesticide 22 (11%) 13 (59%) 9 (41%) NS
Wet Work 133 (65%) 78 (59%) 55 (41%) NS
6.4.1 Concurrent Symptoms
Models were constructed to compare subjects with concurrent skin and respiratory symptoms to
those with symptoms in only one system. Larger than acceptable variance inflation factors for
occupation variable meant that occupation did not remain into the multiple logistic regression
models.
The results of the multiple logistic regression models are shown in Table 21. Results showed
that subjects with a history of eczema (OR 3.68, 95% CI 1.73-7.83) had significantly greater
odds of reporting both work-related skin and respiratory symptoms. Additionally, subjects from
larger (>499 employees) workplaces (OR 2.82, 95% 1.08-7.35) and those who reported wearing
a respirator while at work (OR 2.44, 95% CI 1.2-4.8) were more likely to report concurrent skin
and respiratory symptoms. Current smoking was found to be associated with reporting
concurrent skin and respiratory symptoms (OR 2.57, 95% CI 1.15-5.76).
In the nested model comparing subjects with respiratory symptoms only to subjects with skin

90
symptoms only smoking was not significantly associated with reporting respiratory symptoms
(Table 21). In this model a history of doctor-diagnosed eczema was associated with reporting
skin symptoms only (OR 0.28, 95% CI 0.09-0.87).
Table 21 Multiple Logistic Regression Model Results for Predictors of Reporting
Concurrent Skin and Respiratory Symptom Outcomes. Models Adjusted for Age, Sex and
Interviewer.
Model Description
Predictor↓
Both Skin and Respiratory
Symptoms
Respiratory Symptoms Only
vs. Skin Symptoms Only
Never Smoker 1.00 1.00
Former Smoker 1.22 (0.52-2.85) 1.36 (0.49-3.77)
Current Smoker 2.57 (1.15-5.76) 1.25 (0.46-3.34)
Atopy 0.86 (0.41-1.77) 2.49 (1.05-5.88)
Doctor-diagnosed Eczema 3.68 (1.73-7.83) 0.28 (0.09-0.87)
< 20 Employees 0.96 (0.39-2.34) -
20-99 Employees 1.00 -
100-499 Employees 1.00 (0.40-2.48) -
>499 Employees 2.82 (1.08-7.35) -
AA Clinical Stream (vs. Derm) 0.25 (0.09-0.70) -
Respirator Worn at Work 2.44 (1.25-4.77) -
Isocyanate Exposure at Work - 2.29 (0.72-7.31)
# Outcomes 83 58
Model n 204 121
6.5 Discussion
Concurrent symptoms were more common among the Derm stream subjects (46%) compared
with the AA stream subjects (16%), but both groups had a higher prevalence of concurrent skin
and respiratory symptoms than previous studies [Moulin et al. 2009, Lynde et al. 2009]. In
another clinical study, Moulin et al. reported on 234 patients with diagnosed contact dermatitis,
of whom 10 (4%) had both work-related contact dermatitis and respiratory symptoms [Moulin et
al. 2009]. This is one-fourth the prevalence observed here in the Derm patients; 88% of whom

91
were diagnosed with contact dermatitis. Lynde et al. studied working professional cleaners but
required more than one respiratory symptom to be reported [Lynde et al. 2009]. Lynde et al.
found that 7.2% reported both a current skin rash and two or more respiratory symptoms; 5.9%
reported current skin rash as well as two or more work-related respiratory symptoms [Lynde et
al. 2009].
Work-related symptoms were common, as would be expected in a clinical population being
assessed for possible work-related disease. A large proportion of workers also reported work-
related symptoms in the system other than the one they were being assessed for; 30% of Derm
stream subjects reported work-related respiratory symptoms and 11% of AA subjects reported
work-related skin rash.
In models exploring the difference between subjects with concurrent symptoms (both skin and
respiratory symptoms) and those with only one symptom (either skin or respiratory symptoms)
none of the specific exposures investigated were significant risk factors for concurrent
symptoms. A history of doctor-diagnosed eczema was a risk factor for reporting concurrent skin
and respiratory symptoms, but a history of asthma was not. Childhood eczema has been reported
as a risk-factor for developing adult onset asthma [Martin et al. 2011], but the relationship
between eczema and concurrent symptoms is less clear.
Studies by Vermeulen et al. in rubber workers and Hino et al. in car spray painters found that
subjects with abnormal skin (mild dermatitis or hand eczema) had elevated biomarkers of
exposure, suggesting that they had greater uptake of exposure through their skin [Vermeulen et
al. 2003, Hino et al. 2008]. In a clinical population with atopic dermatitis, Bremmer et al.
reported that patients who also had ichthyosis vulgaris, a skin disease that disrupts the barrier
function of the skin, were significantly more likely to report asthma symptoms [Bremmer et al.
2008].
The reported association between eczema and concurrent skin and respiratory symptoms
suggests that impaired barrier function may play a role in modifying the uptake of exposures
through the skin, and potentially also in the development of both skin and respiratory symptoms
[Nielsen. 2005]. However, the data available in this study does not address the extent (if any) of
barrier function impairment in the current study subjects, or the location of the eczema and its
relevance to occupational exposures.

92
Atopy was considered a possible confounder in the relationship between eczema and symptoms
and was included in all models. The observed association between a history of eczema and
concurrent skin and respiratory symptoms persists in the model after adjusting for atopy,
suggesting that the association is not a result of confounding.
The association between large workplaces and reporting concurrent skin and respiratory
symptoms is more challenging. There may be social factors (i.e., a lack of a personal relationship
with their employer) that make workers from larger workplaces more likely to report symptom as
associated with their work, but these underlying factors cannot be determined from this study.
Neither having a union in the workplace nor receiving occupational health and safety education
(PPE or work-related disease) was associated with reporting concurrent skin and respiratory
symptoms, though both were more likely in larger workplaces (results not shown).
No associations between workplace exposures and reporting concurrent skin and respiratory
symptoms were observed. This was a small study population with diverse occupations and
exposures that lacked power to explore the relationship between single exposures and the
concurrent symptom outcome. However, subjects reporting respirator use at work were observed
to have significantly greater odds of reporting concurrent skin and respiratory symptoms. In this
case, the use of a respirator at work may serve as proxy for general exposure at work. The
observed association may suggest an association between higher exposure, or perhaps higher risk
exposure, and concurrent symptoms. It is also possible that, regardless of the other workplace
exposures, the respirator is actually an important exposure. In cases of contact dermatitis and
patch testing, gloves, and the chemical components of gloves, are often implicated as causal
occupational exposures, this is less common in the case of respirators but it is still plausible
[Warshaw et al. 2008].
Current smokers had increased odds of concurrent skin and respiratory symptoms. Interestingly
in the nested model, which compared subjects with respiratory symptoms only to subjects with
skin symptoms only, smoking was not associated with reporting respiratory symptoms. This is
surprising because the association between smoking and respiratory symptoms is well
established [Higgins. 1959]. In this nested model subjects with atopy were more likely to report
respiratory symptoms while subjects with a history of eczema were more likely to report skin
symptoms.

93
6.5.1 Limitations
The main limitation of this study is that it was cross-sectional and able only to describe
association rather than causation. Secondly, this study was completed in a selective clinical
population of patients with suspected work-related disease and may not be generalizable to all
workers. The aim of this study was to determine if workers who have concurrent skin and
respiratory symptoms are different from those with symptoms only in one system that was more
easily addressed in a population with higher symptom prevalence. The mechanism(s) underlying
the reported symptoms cannot be ascertained from this study. The reported symptoms could be
due to either allergic or irritant mechanisms; in the case of concurrent symptoms it is possible
that one symptom is allergic in nature, while the other is irritant. Additionally the relative
infancy of dermatological epidemiology is a limitation of this research area. Respiratory
epidemiology is well-developed, with established questionnaire tools and an accepted
understanding of which reported symptoms relate to formal diagnoses [Pekkanen et al. 2005,
Ferris. 1978]. The epidemiology of skin disease is significantly less developed; much work
remains to be done.
6.5.2 Conclusions
In conclusion, while no specific exposures were found to predict the reporting of concurrent skin
and respiratory symptoms, workers who reported respirator use at work and those who worked in
larger workplaces had increased odds of reporting concurrent skin and respiratory symptoms, as
did current smokers and subjects with a history of eczema. The association between a history of
doctor-diagnosed eczema and concurrent skin and respiratory symptoms, including the potential
role of impaired barrier function in the development of concurrent symptoms is interesting and
needs further investigation. Future occupational research should aim to include measures of both
skin and respiratory exposures and outcomes, particularly in studies of occupational exposures
that are known to cause effects in both systems.

94
Chapter 7 General Discussion
The broad aim of this thesis, as stated in Section 2.2, was to “further investigate the relationships
between occupational exposures, skin symptoms and disease, and respiratory symptoms and
disease.” This overarching purpose was achieved through four studies, which investigated the
connection between the skin and respiratory systems in terms of exposure, response (symptoms
or disease), and exposure-response relationships.
7.1 Revisiting Research Aims and Hypotheses
Data available from surveillance reporting schemes (both mandatory and voluntary) provides
information on the causes of occupational contact dermatitis and occupational asthma in reported
cases [Karjalainen et al. 2000, Riihimäki et al. 2004, McDonald et al. 2005, Hannaford-Turner et
al. 2010, Pal et al. 2009, McDonald et al. 2006, Turner et al. 2007]. We hypothesized that in a
systematic review of common occupational contact allergens there would be many that could
also cause work-related asthma. Results from the North American Contact Dermatitis Group
(NACDG) patch test data and the subsequent systematic literature review demonstrated that this
hypothesis was supported (Chapter 3).
Seven of the ten most common contact allergens from the NACDG data (2001-2006) were also
found to be associated with OA. Though the hypothesis was shown to be correct, there is still an
important gap in knowledge, as this study reported only on the ability for contact allergens to
potentially also cause asthma. It did not address the potential for the most common causes of
occupational asthma to also cause contact dermatitis. Identifying the common causes of
occupational asthma in the same general population is more challenging as there is no structure
in place for collecting information on causes of occupational asthma in Canada. Additionally, the
diagnosis of occupational asthma is not as clear-cut as the diagnosis of occupational contact
allergy. The need for better surveillance and record keeping around causes of occupational
asthma will be addressed in this discussion.
While investigating the common occupational contact allergens in the NACDG data, conflicting
notations regarding the sensitization potential of the common contact allergens was discovered in
three common sources of occupational hygiene information. This discordance will also be
described in further detail.

95
The proposed framework for conceptualizing possible connections between the skin and
respiratory systems (Figure 1) led to the hypothesis that, when asked, some workers would report
both skin and respiratory symptoms. And, that a portion of these workers (with concurrent skin
and respiratory symptoms) would report both symptoms as being associated with their job
(work-related). Results from a small data pooling study suggested that this hypothesis was also
supported (Chapter 4). Historical data from four occupational studies (n=247) that focused on
skin or respiratory symptoms (or both) were pooled and the prevalence of concurrent skin and
respiratory symptoms was calculated. The mean prevalence of concurrent symptoms was 11%
(range by occupation: 6-17%) though only two subjects (<1%) reported both skin and respiratory
symptoms that were both work-related.
There is little work on underlying exposure-response relationships that lead to skin symptoms
despite that fact that exposure-response is considered to be one of the necessary conditions for
demonstrating causation [Hill. 1965]. In order to better understand the exposure-response
relationships for skin symptoms, the fourth research aim was to determine whether exposure-
response relationships could be observed in two different occupational groups: bakery workers
and auto body shop workers (Chapter 5). Both groups have occupational exposures that are
known to cause asthma and contact dermatitis. In both cases there has been research into the
prevalence of skin symptoms, but little research into exposure-response relationships. The
hypothesis was that exposure-response relationships for skin symptoms would be observed in
both of these occupational groups. Results from the analyses suggested that the hypothesis was
not supported; exposure-response relationships were observed in auto body shop workers, but
not in bakery workers. There are many explanations for why an exposure-response relationship
among the bakery workers may not have been observed, if in fact one exists. Wheat exposure
was the exposure estimated in the study of bakery workers, but wheat may not have been the
causal exposure. The study also used airborne exposure as a proxy for skin exposure, which may
have led to exposure misclassification if there was low correlation between skin and airborne
exposure to wheat. These limitations will be discussed further.
The final section (Chapter 6) of this thesis investigated the prevalence and predictors of
concurrent skin and respiratory symptoms in a clinical population with suspected occupational
disease. The first hypothesis investigated in this study was the same as in the data pooling study
(Chapter 4), namely that subjects would report concurrent skin and respiratory symptoms and

96
that a portion would associate these symptoms with their job (work-related). We expected that
the prevalence of concurrent symptoms would be higher in the clinical population than in the
pooled occupational studies (Chapter 4). With this group we were able to explore possible
predictors of concurrent symptoms, including health history, workplace characteristics,
prevention practices, and occupational exposures. We hypothesized that there would be
differences between subjects who reported only one symptom (either skin or respiratory), and
those who reported both skin and respiratory symptoms in these variables.
Results from the study of workers with suspected disease (n=204) confirmed that a relatively
large portion, 41%, reported both skin and respiratory symptoms, and that 20% reported both
skin and respiratory symptoms that were work-related. Workers with a history of eczema as well
as workers from larger workplaces and those who reported wearing a respirator at work had
increased odds of reporting concurrent skin and respiratory symptoms. No specific occupational
exposures were associated with reporting concurrent skin and respiratory symptoms. The
importance of the observed relationship between eczema and concurrent symptoms will be
discussed in greater detail.
There were a series of research aims that guided the work contained in this thesis. These aims
were simple in nature, reasonable, and manageable. Individually, they each contribute a small
piece of knowledge to an incomplete picture of possible connections and interactions between
the skin and respiratory systems in occupational disease. Specifically, these results confirm that
some workplace exposures can cause both skin and respiratory disease, that workers do
experience both skin and respiratory symptoms at the same time, and that there are observable
exposure-response relationships for skin symptoms in some working populations. Together the
findings from this thesis support the broad hypothesis that there are connections between the skin
and respiratory systems in terms of occupational exposure and disease, and that this area of
research both needs and deserves further attention.
7.2 Methodological Considerations
Beyond the specific research findings from this thesis, there were two main themes that emerged
from the work. The first theme was the existence of silos in respiratory research and
dermatology/skin research. Second was the challenge in bridging this gap in studies where the
outcome was actually two different, yet concurrent outcomes.

97
At a basic level there were differences in the history and body of literature on occupational skin
and respiratory disease. There has been a large amount of effort in the past to standardize the
questionnaire tools related to respiratory symptoms and disease [Jenkins et al. 1996, Sistek et al.
2006, Pekkanen et al. 2005, Vandenplas et al. 2005, Medical Research Council on the Aetiology
of Chronic Bronchitis. 1960, Ferris. 1978]. Researchers have also spent a considerable amount of
time investigating the relationships between specific symptoms and respiratory diagnoses (e.g.,
wheeze, asthma and bronchial hyper-responsiveness) which permits the use of questionnaire
items in place of diagnostic testing in research studies [Jenkins et al. 1996, Sistek et al. 2006,
Pekkanen et al. 2005, Vandenplas et al. 2005, Medical Research Council on the Aetiology of
Chronic Bronchitis. 1960, Ferris. 1978].
There is currently no equivalent body of literature relating skin symptoms to skin diagnoses.
Several studies have confirmed that skin symptoms are positively related to physician diagnosis
of skin disease. However, these studies used different questionnaire items to predict different
clinical outcomes [Svensson et al. 2002, Meding and Barregard. 2001, Carstensen et al. 2006,
Smit et al. 1994]. There is a need for more methodological work to better determine if specific
skin symptoms questions are predictive of dermatological diagnoses, and if it is possible to use
questionnaire items to differentiate between different dermatological diagnoses (i.e.,
irritant/allergic contact dermatitis).
As the studies of concurrent skin and respiratory symptoms and disease were undertaken, it
became clear that conceptualizing the concurrent outcomes (skin and respiratory), and addressing
the work-relatedness of two outcomes at once, was more complicated than originally considered.
The outcomes of interest were two separate reported symptoms, but either, both or neither could
be work-related. This resulted in nine possible outcomes groups that are described with respect
to each symptom and its work-relatedness in Table 22.
Separating subjects who had concurrent symptoms (skin and respiratory) was a straightforward
task, but when the layer of work-relatedness was added this forced a decision about whether one
work-related symptom (of two reported) was sufficient, or whether both reported symptoms
needed to be work-related. In either case, when selecting a definition of work-related concurrent
symptoms, there was always a group of subjects (group 6 from Table 22) who were placed in the
reference group despite having concurrent skin and respiratory symptoms. This meant that any

98
comparison between work-related concurrent symptoms and those without was no longer a
comparison between concurrent symptoms and symptoms only in one system as was originally
described in the research objectives.
It was decided that both symptoms were required to be work-related for membership in the
work-related concurrent symptom group (Appendix 3, Table 30). This decision was made in part
because the difference between the group with both symptoms (n=83) and the group with both
symptoms where only one symptom was work-related (n=77) were small (Table 18) and because
the interpretation was simply more straightforward when the concurrent symptoms were both
required to be work-related. In the end the models that were included in Chapter 6 focused only
on general concurrent symptoms.
Table 22 Description of Possible Outcome Groups when Considering Both Skin and
Respiratory Symptom Outcomes and their Individual Work-Relatedness. Under
Symptoms, ‘X’ = Symptom is Present in the Symptom Group. Under Model A and Model
B, ‘Yes= Symptom Groups are Considered to Have the Outcome of Interest and ‘No =
Symptom Groups are Considered Not to Have the Outcome of Interest. Conc =
Concurrent, WR = Work-Related, Resp = Respiratory.
Symptoms
Symptom Group n Skin
WR
Skin Resp
WR
Resp
Model A:
Conc Sx
Model B:
Both WR
Conc Sx
(1) No Symptoms (Sx) 14 No No
(2) Skin Sx, No Respiratory Sx 7 X No No
(3) Work-related Skin Sx, No
Respiratory Sx
19 X X No No
(4) No Skin Sx, Respiratory Sx 56 X No No
(5) No Skin Sx, Work-Related
Respiratory Sx
39 X X No No
(6) Skin Sx, Respiratory Sx 6 X X Yes No
(7) Work-Related Skin Sx,
Respiratory Sx
33 X X X Yes No
(8) Skin Sx, Work-Related
Respiratory Sx
4 X X X Yes No
(9) Work-Related Skin Sx, Work-
Related Respiratory Sx
40 X X X X Yes Yes

99
7.3 Causes of Occupational Skin and Respiratory Disease
The results from Chapter 3 demonstrate that seven of the top ten contact allergens were also
associated with occupational asthma in the literature or reference materials investigated
(“Asthma in the Workplace”, UK HSE “Asthmagen?”, MEDLINE, TOXNET, EMBASE). As
emphasized in Chapter 3, it is important to reiterate that we started with a list of contact allergens
and investigated their association with OA. The result is a list of contact sensitizers that may also
be respiratory sensitizers. Due to the structure of this process there are some common respiratory
sensitizers that are missing from the list (e.g., isocyanates, animals, flour).
The seven common occupational contact allergens that were found to be capable of causing
occupational asthma were: epoxy resin, nickel sulfate, cobalt chloride, potassium dichromate,
glutaraldehyde p-phenylenediamine (PPD), and formaldehyde. Thiuram, carba mix, and glyceryl
thioglycolate were classified as having no current evidence of causing OA (Table 10).
The ten most common occupational contact allergens were similar to previously published
studies that reported on the common contact allergens in other regions, including the UK
[McDonald et al. 2006], Finland [Riihimäki et al. 2004] and the entire NACDG database
[Rietschel et al. 2002]. Though the UK and Finnish surveillance systems use chemical groupings
rather than the specific chemical names that are tested in the patch testing process, the
similarities between all of the findings is evident. The Canadian NACDG contained carba mix
and thiuram, while rubber chemicals were listed in the UK data [McDonald et al. 2006].
Aliphatic aldehydes were in the top ten chemical groups causing allergic contact dermatitis in
Finland [Riihimäki et al. 2004]; similarly, formaldehyde and glutaraldehyde were present in the
Canadian NACDG data. The consistency of the common allergens among the Canadian centres
in the NACDG with the entire NACDG, as well as with other countries suggests that the results
from the Canadian centres are not overly sensitive to local industry or case clusters and are good
indicators of trends in contact allergy.
Additionally, some of the common contact allergens identified in Chapter 3 were the same casual
agents implicated in cases studies of workers with both occupational asthma and occupational
contact dermatitis (Table 5). There have been reports in the literature of workers with exposure
to diglycidyl ether of bisphenol A (DGEBA) a component in epoxy resin systems [Moulin et al.
2009, Kanerva et al. 1991], potassium dichromate [De Raeve et al. 1998], and nickel [Estlander

100
et al. 1993]. The combination of peer-reviewed literature supporting the causal link between
these contact allergens and occupational asthma, combined with the case studies of occupational
contact dermatitis and occupational asthma from the same exposures, provide a good direction
for future research of concurrent skin and respiratory outcomes.
It would be ideal to complete the reverse process, and investigate common respiratory sensitizers
and their association with contact dermatitis. However, there is currently no equivalent to the
NACDG patch test data for respiratory sensitizers.
7.3.1 Surveillance of OCD and OA
The history of clinical standardization and data pooling amongst dermatologists specializing in
contact dermatitis and patch testing has resulted in a large amount of standardized diagnostic
data from the USA, Canada, and Europe that allow for surveillance studies of common contact
allergens (both work-related and non-work-related) within these regions [Zug et al. 2009, Uter et
al. 2009]. The studies are valuable, and their existence is due in part to the large number of
allergens that can be tested at one time in one subject. The North America Contact Dermatitis
Group (NACDG) tests a standard tray of 65 allergens, in addition to any occupation-specific
allergens the physician deems necessary, including custom allergens in some cases [Zug et al.
2009].
It would be beneficial to have a similar pooling of information on the diagnostic tests used in
occupational asthma, but the relative infrequency of specific inhalation challenge testing and the
fact that only one allergen is tested at a time in a SIC means that a database would likely contain
a fraction of the information.
The best data potentially available in Ontario would be workers’ compensation claims data from
the Workplace Safety and Insurance Board (WSIB), but this would limit the exposures to those
cases of OA that were accepted for compensation, rather than all work-related asthma at a clinic
or population level, which is likely a significantly larger group. A data pooling scheme for SIC
testing may be more feasible in jurisdictions where SIC is more common (i.e., the province of
Quebec, Canada) but very few workers’ compensation claims for OA undergo SIC testing in
other jurisdictions.

101
The development of a system that permitted pooling among the few physicians who complete
SIC test would be a huge asset to occupational asthma research in Canada. A voluntary system in
the province of Ontario was recently tested for feasibility but the future of this endeavor is
“unknown” [To et al. 2011]. The lessons learned from this experience should be applied to any
future attempts to improve the system, or launch a similar program in another jurisdiction.
Further to this, the two Canadian centres whose data were utilized in Chapter 3 are part of an
American-based organization, the NACDG. An idea championed by Dr. Holness is the
development of a Canadian patch test pooling group, similar to the NACDG and the European
Surveillance System on Contact Allergies (ESSCA). There are many clinics across the country
that offer patch testing, together their pooled data would be a huge asset for skin research, both
occupational and non-occupational, in Canada.
7.3.2 Knowledge Translation and Communication
Results from Chapter 3 demonstrated that among identified occupational contact allergens there
was significant discordance in how these known sensitizers are described and annotated in
common occupational hygiene references materials.
Practicing occupational hygienists, occupational physicians, and nurses, as well as other health
practitioners often look to the NIOSH pocket guide, the ACGIH TLV book and/or the HazMap
database for guidance on the handling of specific chemicals [American Conference of
Governmental Industrial Hygienists (ACGIH). 2008, National Institutes of Health. 2009,
National Institute for Occupational Safety and Health. 2007]. When the ten most common
occupational contact allergens were referenced in each of the three documents, only the HazMap
database identified them all as possibly having skin effects.
The major issue in interpretation of these results is that the notations provided by the three
sources of information are fundamentally different. The NLM HazMap database uses notations
for the adverse effects ‘Skin’ and ‘Asthma’ as well as potential disease outcomes of ‘Asthma’
and ‘Contact Dermatitis’ [National Institutes of Health. 2009]. The ACGIH TLV Handbook
includes a specific sensitizer notation, ‘SEN,’ but this notation does not include information on
the route of sensitization through which sensitization may occur [American Conference of
Governmental Industrial Hygienists (ACGIH). 2008]. Thirdly, the NIOSH Pocket Guide

102
includes possible symptoms as ‘Dermatitis’ or ‘Asthma’ as well as notations that are specific to
sensitization, ‘Respiratory sensitizer’ or ‘Skin Sensitizer’ [National Institute for Occupational
Safety and Health. 2007].
To better understand the differences in the notations, the purpose or guiding statement for each
document was investigated. The US National Library of Medicine states that:
“HazMap … is an occupational health database designed for health and safety
professionals and for consumers seeking information about the health effects of
exposure to chemicals and biologicals at work. HazMap links jobs and hazardous
tasks with occupational diseases and their symptoms” [National Institutes of
Health. 2009].
The ACGIH writes that the TLVs are:
“…guidelines designed for use by industrial hygienists in making decisions
regarding safe levels of exposure to various chemical substances and physical
agents found in the workplace. In using these guidelines, industrial hygienists are
cautioned that the TLVs® and BEIs® are only one of multiple factors to be
considered in evaluating specific workplace situations and conditions” [American
Conference of Governmental Industrial Hygienists (ACGIH). 2008].
Thirdly, the CDC states that the:
“NIOSH Pocket Guide to Chemical Hazards (NPG) is intended as a source of
general industrial hygiene information on several hundred chemicals/classes for
workers, employers, and occupational health professionals. The NPG does not
contain an analysis of all pertinent data, rather it presents key information and
data in abbreviated or tabular form for chemicals or substance groupings … that
are found in the work environment” [National Institute for Occupational Safety
and Health. 2007].
Both the ACGIH and the NIOSH pocket guide state that they do not contain all of the relevant
data, and should be used in concert with other sources of information when evaluating workplace
exposure scenarios. The NLM HazMap database makes no such statement but also employs the

103
broadest notations in the reference materials. The broad notation used by the HazMap database
does not specify sensitization, rather just specifies skin (skin or contact dermatitis) or respiratory
effects (asthma).
It is unknown how these reference documents are used in practice; whether occupational
hygienists consult only one, or a selection, of the sources of information on hazards. What is
clear is that a practitioner who only consulted one of these documents would likely receive an
incomplete picture of the exposure hazard. Even though the HazMap database would be more
likely to identify a potential hazard, further research and investigation would be required to
better identify the specific type of hazard.
In Table 28 and Table 29 the reliability statistics for workplace characteristics questionnaire
items are reported. It is relevant to this discussion of sensitizer notations to note that in the small
reliability study, the least reliable (lowest Kappa) questions were the two asking about allergens
or irritants in the workplace. The majority of questionnaire items asking about specific
occupational exposures (Table 28 and Table 29) had better reliability than the general questions
about allergens and irritants. This suggests that workers may have struggled to categorize their
exposures as either allergic or irritants. This may be a result of not understanding the meaning of
allergen or irritant when asked during the questionnaire procedure, but also may be due to a lack
of knowledge about which exposures are allergens and which are irritants.
Given the differing information in the three occupational hygiene documents, it is possible that
there is confusion even among the health and safety professionals, and that this confusion and
misinformation has trickled down to workers and managers. Workers on the job, occupational
hygienists in the field, and health practitioners in the clinic all need to be aware of the potential
health hazards associated with a workplace exposure. These groups cannot be required to learn
and retain all of this information, but instead need a source of information that provides an up-to-
date description of workplace exposures, and directs the reader to other sources when necessary.
In this digital age, it seems that there should be a way to merge information from multiple
sources into one interface, perhaps even one that can be accessed on mobile devices that would
allow for on-demand access to health and safety information.

104
7.4 Modeling Exposure-Response Relationships
Historically, occupational studies of health outcomes have tended to measure either skin or
airborne exposures. Studies in which skin and airborne exposures were measured in parallel
(Table 4) focused only on exposure assessment and not on potential health outcomes.
Many studies have collected information about both skin and respiratory symptoms, but have not
reported on the prevalence of these symptoms co-existing [Sripaiboonkij et al. 2009b,
Sripaiboonkij et al. 2009a, Lindgren et al. 2002, Fantuzzi et al. 2010, Nettis et al. 2002, Kujala
and Reijula. 1995, Holter et al. 2002, Friis et al. 1999, Holness and Nethercott. 1989, Holness et
al. 1989, Nethercott and Holness. 1988, Huusom et al. 2011]. Compared with collecting
exposure measurements of two routes, including questions on both outcomes is relatively simple
and may explain why there is such a wealth of data on symptoms, and a lack of exposure data.
As a first step in determining whether there may be a connection between skin and respiratory
systems, previously collected data was analyzed to determine whether there was a group of
workers who reported concurrent skin and respiratory symptoms. These analyses (Chapter 4)
benefitted from a series of previous studies that had asked about both skin and respiratory
symptoms but had never analyzed the two together.
When the exposure-response relationships for skin symptoms were explored in bakery workers
(exposure: wheat allergen) and auto body shop workers (exposure: diisocyanates), again the
symptom data had been collected for both skin and respiratory outcomes but there was
incomplete skin exposure information in both groups. For this reason the airborne exposures
were used as a proxy of skin exposure in both groups (Chapter 5)
The use of airborne exposure as a proxy for skin exposure was justified based on the evidence in
the literature that skin and airborne exposures are correlated in many occupational exposure
scenarios (Table 4). Specifically there was evidence of correlation between skin and airborne
diisocyanate exposure in an auto body shop population [Fent et al. 2008]. However, there was no
evidence located to support or refute a correlation between skin and airborne exposures in bakery
workers. In fact, there were no located studies of measured skin exposure in bakery workers.
The lack of skin exposure measures in bakery workers may be due to the particulate nature of
flour dust, a major exposure in bakeries. The measurement of skin exposure to particulates

105
introduces unique challenges. A dermal sampling strategy for particulate exposures has been
developed but does not appear in any published studies of bakery workers to date [Lundgren et
al. 2006, Ashley et al. 2007].
The results in Chapter 5 showed that there were exposure-response relationships for skin
symptoms in auto body shop workers; the same relationships were not observed in bakery
workers. There may not be an exposure-response relationship in bakery workers. But, if one does
exist, the lack of an observed relationship in this study may be due to any of several factors. The
first possibility is that the exposure investigated (wheat allergen) may not have been the causal
exposure for skin symptoms. Other possible exposures in the bakery environment include flour
dust, enzymes, preservatives, oils, and wet work. The relationships of total dust and α-amylase
with skin symptoms were investigated separately and neither showed a significant exposure-
response relationship (results not shown). A second possibility is that the measured airborne
exposures to wheat allergen may have been a poor proxy for skin exposure in this exposure
scenario. The study by Hughson et al. was the only study in Table 4 to examine skin and airborne
exposure to a particulate exposure (nickel). In this case they found strong correlation (r = 0.46-
0.57) between inhalable nickel concentrations and the amount of nickel on skin (using skin wipes
as a removal method).
Further understanding of exposure-response relationships for skin symptoms in a wider variety
of occupational settings under different exposure scenarios is needed.
7.5 Workers Do Report Concurrent Skin and Respiratory Symptoms
Results reported in this thesis (Chapter 4, Chapter 5 and Chapter 6) demonstrate that a portion of
workers in a variety of occupations do report both skin and respiratory symptoms. The small data
pooling study in Chapter 4 was a pilot study designed to determine whether or not workers from
a variety of occupations (ammonia processing, cabinet making, softwood planing, and
embalming) reported concurrent skin and respiratory symptoms. Among this group, 26 workers
(11%) did report concurrent skin and respiratory symptoms, though few (n=2, < 1%) associated
both their skin and their lung symptoms as being caused by work. This study confirmed our
hypothesis that concurrent symptoms would exist among workers, but suggested that the

106
prevalence of concurrent work-related symptoms was much lower than either work-related skin
symptoms or work-related respiratory symptoms alone.
In Chapter 6, concurrent skin and respiratory symptoms were examined in a clinical population
where the prevalence of both symptoms and work-related symptoms was expected to be higher
than in the data used in Chapter 4. This hypothesis was supported; 38% of subjects reported
concurrent skin and respiratory symptoms and 18% reported that they had both skin and
respiratory symptoms that were work-related.
In Chapter 5 the primary goal was to identify exposure-response relationships for skin symptoms
among bakery and auto body shop workers. Additionally, the relationships between skin
symptoms and respiratory symptoms were also investigated in these two populations. Results
suggested that workers who reported skin symptoms were at significantly greater risk of
reporting respiratory symptoms. This result was true for both bakery and auto body shop
workers, for both work-related and non-work-related symptoms.
The results from Chapter 4, Chapter 5, and Chapter 6 are similar to the findings of two previous
studies on concurrent skin and respiratory symptoms. Moulin et al. briefly reported on subjects
with diagnosed occupational contact dermatitis, 4% of these patients also reported work-related
respiratory symptoms [Moulin et al. 2009]. In an occupational study of professional cleaners,
Lynde et al. reported than 7.2% of subjects reported a skin rash as well as three or more
respiratory symptoms; 3.7% of subjects reported a rash plus two or more work-related
respiratory symptoms [Lynde et al. 2009]. The clinical study from Moulin et al. has a low
prevalence of work-related respiratory symptoms among a group of occupational contact
dermatitis patients. Few details about this population are available, but the fact that they all have
occupational contact dermatitis suggests that they are all exposed (via contact) at work. Lynde et
al. report similar prevalence of work-related respiratory symptoms (3.7%) among professional
cleaners with a current rash. There is no clinical diagnosis of the rash, so this group may contain
subjects with contact dermatitis, atopic eczema, or other skin conditions that may or may not be
work-related. Comparing between these two studies is difficult as they were conducted in
different environments (clinical vs. occupational) with different groups of subjects (patients with
varied exposures vs. workers with similar exposures) and different symptom definitions.

107
The prevalence of work-related concurrent skin and lung symptoms among the four occupational
groups in Chapter 4 are lower than those reported by both Moulin et al. and Lynde et al. [Moulin
et al. 2009, Lynde et al. 2009]. Reasons for this are not entirely clear. The data that was used in
Chapter 4 were historical (1980s) data collected in the occupational setting.
The clinical population in Chapter 6 can be reasonably compared to the study by Moulin et al.
Among the Derm (possible work-related skin disease) subjects in Chapter 6, 88% were
diagnosed with contact dermatitis and 69% with work-related contact dermatitis. Among all
Derm subjects, 28% reported work-related respiratory symptoms and 6% reported work-related
asthma-like symptoms. These rates of work-related respiratory symptoms are much higher than
those reported my Moulin et al. There may be differences in the clinical population that we
cannot determine from the information reported, including occupational distribution, exposures
at work, or prevention strategies employed at work, among others.
With so few studies, we do not yet have a good estimate of the prevalence of concurrent
symptoms among workers or among patients. But it is clear that a portion of subjects in all
studies did report concurrent symptoms. There is a need to at least consider the possibility of
concurrent symptom outcomes and the mechanisms that might be leading to these outcomes in
workers. It would be beneficial if future research considering either skin or respiratory outcomes
could collect information on outcomes in both systems, as well as the work-relatedness of both
symptoms, and if possible collect information (or measurements) to estimate exposure in both
systems.
7.6 Symptom Progression
When considering the concurrent skin and respiratory symptom outcomes in Chapter 4, Chapter
5 and Chapter 6 it would have been interesting to be able to group subjects based on which
symptom was experienced first. This information was not collected as part of these studies.
The clinical stream was initially considered as a proxy for the first, or at least more serious,
symptom. But upon further consideration this was deemed inappropriate. The clinical stream
under which a patient was seen at the clinic is highly variable and depends in large part on the
referring physician. In addition, it is possible that some subjects would have underlying disease
(i.e., asthma or dermatitis) that is long-standing and under management by another physician. If

108
the primary symptom could not be determined from the clinical stream, and subjects were not
asked about the timing of symptoms in the questionnaire, it was not possible to determine the
temporality of symptom onset. Though the order that symptoms are experienced in workers may
not matter, it cannot be determined without investigation. In future studies it would be beneficial
for the timing or order of symptoms onset to be investigated and included in greater depth in the
questionnaire items.
7.7 Predictors of Concurrent Skin and Respiratory Symptoms
Chapter 6, the final thesis data chapter, investigated the specific predictors of reporting
concurrent skin and respiratory symptoms among the clinical subjects. Contrary to our
hypotheses, results from the clinic-based study suggested that none of the specific workplace
exposures or occupational groups were strong predictors of concurrent skin and respiratory
symptoms. In this population, workers with a history of eczema, current smokers and workers
from larger workplaces were at higher risk of reporting concurrent symptoms. Despite the fact
that these results did not support our hypotheses, they are, nonetheless, interesting.
7.7.1 Barrier Function and Concurrent Skin and Respiratory Symptoms
The finding that workers with a history of eczema had increased odds of reporting concurrent
skin and respiratory symptoms suggests a role for impaired barrier function in the development
of the concurrent symptoms. The hypothesis is that workers with an impaired barrier function
may be more likely to report concurrent symptoms because they have increased uptake of skin
exposure through a compromised skin barrier.
Previous studies have shown that workers with impaired skin barrier function have increased
uptake of exposure. In a study of carcinogen exposed rubber workers, Vermeulen et al. reported
that those workers with hand dermatitis had higher levels of mutagenicity in their urine
[Vermeulen et al. 2003]. Hino et al. found a better correlation between skin condition and urine
biomarkers of exposure than between airborne exposure and urine levels of the biomarkers of
exposure [Hino et al. 2008]. Evidence from Bremmer et al. suggested that the presence of
ichthyosis vulgaris in patients with atopic dermatitis (AD) is predictive of subsequent
development of respiratory symptoms [Bremmer et al. 2008]. Results presented in Chapter 6

109
showed that subjects with a history of eczema (doctor-diagnosed) were more likely to report
concurrent skin and respiratory symptoms (both work-related and non-work-related).
The subjects in Chapter 6 reported whether they ever had eczema, and also reported current skin
rash. Jakasa et al. showed that the uptake of SLS (a strong irritant) was greater among subjects
with active AD, compared with subjects with normal skin and those with inactive AD [Jakasa et
al. 2006]. In this case, the AD had to be active in order for the increased permeation to be
observed. Jakasa et al. also measured the penetration of a strong irritant, one that has itself been
known to disrupt barrier function even in healthy skin [Nielsen. 2005]. As the subjects in
Chapter 6 reported current skin symptoms, it is plausible that they did have current barrier
dysfunction, but no objective measure of skin condition was collected as part of this study.
There was no association with having a history of asthma and reporting concurrent skin and
respiratory symptoms. In univariate analyses there was no significant relationship between a
history of asthma and a history of eczema, suggesting there was no confounding between these
variables. Additionally, the multiple logistic regression models were adjusted for atopy, and the
effect of eczema remained significant after adjustment for atopy, suggesting that this relationship
was also not confounded by atopy.
Beyond having (or having had) eczema, there are other factors that could disrupt the skin barrier
in a manner meaningful for the uptake of occupational exposures. Impaired skin barrier function
can result from disease (eczema or atopic dermatitis [Jakasa et al. 2006]), genetics (filaggrin
mutations [Nemoto-Hasebe et al. 2008]), exposure effects (irritant exposures [Nielsen. 2005]), or
a combination of these factors.
The measurement of skin condition and barrier function deserves attention in future studies of
skin exposure and both skin and respiratory outcomes. This could take the form of
dermatological examination, the use of pictorial questionnaires for identification of skin disease
or the direct measurement of skin condition using transepidermal water loss (TEWL) and other
physiological measures of skin integrity (i.e., hydration and pH).
7.7.2 Personal Protective Equipment
In the first two studies of symptom outcomes (Chapter 4 and Chapter 5) there was not consistent
information on the use of personal protective equipment (PPE) to be able to consider its use in
110
pooled analyses or exposure-response models. As a result, any effect of wearing PPE (i.e., gloves
or respirator) was missed in these studies.
It is possible that PPE use results in lower exposure and in turn a lower probability of reporting
symptoms. However is it also possible that symptoms could result as an effect of wearing PPE.
Thirdly, from the progression perspective it is possible that workers did not wear PPE, were
consequently exposed and went on to developed symptoms, and then, after the onset of
symptoms, began wearing PPE.
In Chapter 6 subjects were explicitly asked about their use of PPE, both yes/no use and
frequency of use, however no information was collected on the temporal relationship between
symptoms and PPE use. The result is that, in the same way that the timing and order of symptom
onset cannot be determined, neither can the order of PPE use in relation to symptom onset.
Models describing the predictors of reporting both skin and respiratory symptoms indicated that
workers who wore respirators at work were more likely to report general skin and respiratory
symptoms (Table 21). Several explanations are possible. It is possible that workers who are
more highly exposed, or are exposed to higher risk compounds are more likely to report
symptoms. In this case, respirator use would be acting as a proxy for exposures. However, it is
also possible that the subjects who had symptoms were more likely to wear a respirator at work.
As in the case of the symptom timing, we are unable to determine which came first (the
symptoms or the PPE use) with the data collected in this cross-sectional study.
It would be ideal if future studies of occupational exposure-response relationships could include
questions directly about the role of PPE in symptoms development, and the temporality of
symptom onset with respect to PPE use (or changes in PPE) in the workplace. This will allow for
better understanding of the role of PPE in the pathway from exposure to response.
7.7.3 Smoking
In Chapter 6 , current smoking was a significant predictor of reporting concurrent skin and
respiratory symptoms (not work-related) in multiple logistic regression models (Table 21). The
differences between subjects reporting respiratory symptoms only and subjects reporting skin
symptoms only were explored in models nested within the concurrent symptom models (Table

111
21). Results from the nested models indicated that smoking was not a significant predictor of
reporting respiratory symptoms only (Table 21).
This result from the nested model was surprising because the association between smoking and
respiratory symptoms is established [Higgins. 1959], and in some cases, most commonly with
asbestos exposures and lung cancer, occupational exposures and smoking are known to act in a
synergistic manner [Frost et al. 2011]. The lack of an association suggests that the risk of
respiratory symptoms among smokers is not statistically different than the risk of skin symptoms.
In previous studies of skin symptoms, some researchers have chosen to adjust for smoking
[Sripaiboonkij et al. 2009b, Sripaiboonkij et al. 2009a] while others have not [de Joode et al.
2007]. The former studies also examined exposure-response relationships that may explain why
they included smoking as a covariate, but there is no explicit discussion of leaving the variable in
models that described exposure-response relationships for skin symptoms.
Models exploring the exposure-response relationships for skin symptoms in bakery and auto
body shop workers in Chapter 5 did not include smoking as a covariate. Smoking was included
in the models presented in Chapter 6 due to the known association between smoking and
respiratory symptoms, which were part of the outcome variable. The result that smoking was
associated with concurrent symptoms and not with respiratory symptoms (in the nested model)
was surprising. This result suggests that the relationships between smoking, skin symptoms, and
respiratory symptoms may be more complicated than anticipated, and that smokers may be at
higher risk of skin symptoms than previously thought. This association deserves further attention
in future studies. Researchers investigating skin symptoms should be sure to include smoking, at
least in preliminary analyses, to ensure that there is not an unrecognized association.
7.7.4 Mechanism of Effect
As noted in each of Chapter 4, Chapter 5, and Chapter 6 the mechanisms of self-reported
symptoms (skin or respiratory) cannot be determined without immunological testing. Without
this information it is not possible to differentiate between symptoms resulting from irritant and
allergic mechanisms.
Despite this limitation in studies of self-reported symptoms, it is important to recognize that
when considering the prevention of concurrent skin and respiratory symptom outcomes the

112
specific mechanism(s) underlying the symptom may not be as relevant. In the case of workers
with concurrent symptoms there may be unrecognized or uncontrolled exposures in either/both
systems. These simultaneous exposures may be to the same exposure agent, or to different (and
multiple) exposure agents that may act independently to cause concurrent symptoms in the
separate systems. In the workplace, the primary concern should be exposure control regardless of
the agent or route of exposures.
Additionally, many occupational allergens can also act as irritants. And, workers with exposures
to sensitizing agents in the workplace will also likely have exposure to irritants (i.e., hand
washing and wet work). As seen in previous studies [Vermeulen et al. 2003, Hino et al. 2008],
co-existing exposures to irritants and allergens can interact to potentially increase the uptake of
exposure.
Work from Nielsen et al. mentioned previously shows that irritant exposures (SLS) can disrupt
skin barrier function and that the penetration of pesticides is increased in the irritant disrupted
skin [Nielsen. 2005]. Benfeldt et al. showed similar effects for the uptake of salicylic acid
through skin damaged by tape stripping [Benfeldt et al. 1999].
Together with the results from Vermeulen et al. and Hino et al. which demonstrate increased
uptake of occupational exposures in workers with compromised skin barrier [Vermeulen et al.
2003, Hino et al. 2008], there is good reason to believe that damaged skin barrier leads to an
increase in subsequent occupational exposures through the skin. The potential for exposure to
skin damaging irritants to increase the uptake of occupational sensitizers has not been
investigated. There are many interesting studies of allergen and irritant exposure, skin barrier
integrity, and sensitization that could be undertaken as a starting point for exploring these
relationships.
7.8 Strengths & Limitations
7.8.1 Strengths
The biggest strength of this thesis is that it investigated the connections between skin and
respiratory systems from several different perspectives: the similarities in causal exposures, the
association between skin and respiratory symptoms, and exposure-response relationships for skin
symptoms. In all of these cases, the results support that there is a connection between the skin

113
and the respiratory system in terms of exposure and outcome. These results provide strong
evidence that there is a need for further study of these connections.
The research aims of this thesis outlined a plan that involved the study of multiple research
questions, each approaching a slightly different aspect of the possible connection between the
skin and respiratory systems. The results provide some insight into a number of the relationships
described in the proposed framework (Figure 2).
Overall, the series of papers that make up this thesis are part of small body of research that has
considered the skin and respiratory systems together in human studies. Two of the studies
included in this thesis were able to take advantage of existing data to explore skin and respiratory
symptoms in working populations. The availability of quality previously unanalyzed data
relevant to the research questions provided an opportunity to confirm that there was a portion of
workers with skin and respiratory symptoms (Chapter 4).
The work presented in Chapter 3, the study of common occupational contact allergens and their
possible associations with occupational asthma, shed light on workplace exposures that may be
able to cause both skin and respiratory disease in workers. Prior to this study there were no
systematic comparisons of exposures causing occupational asthma and exposures causing
occupational contact dermatitis located in the literature. Secondarily this study provided a review
of occupational hygiene notations for each of the common occupational contact allergens. The
review on the notations highlighted important differences in the purpose of the three
occupational hygiene reference documents, and also clearly demonstrated discrepancies in the
information that is acquired from each of the different sources. The dissemination of these results
will ideally lead to more informed interpretation of these notations and perhaps even more
thorough consideration of skin effects in future versions of these documents.
In Chapter 5 the study modeled exposure-response for skin symptom in two working
populations, bakery workers and auto body shop workers. Specifically, this study contributes to a
relatively small body of literature on exposure-response relationships for skin symptoms in
working populations. The results from this study add to previous findings that exposure-response
relationships exist for skin symptoms in wood workers, glass microfiber workers and metal
workers [de Joode et al. 2007, Sripaiboonkij et al. 2009b, Sripaiboonkij et al. 2009a].

114
In addition, this study demonstrated that both bakery workers and auto body shop workers who
reported skin symptoms were more likely to report respiratory symptoms than those who did not
report skin symptoms. This finding confirmed previous work by Lynde et al. in professional
cleaners [Lynde et al. 2009]. Together these studies suggest that concurrent symptoms may be a
significant issue in some working populations.
Chapter 6 described the first study of co-existing skin and respiratory symptoms among a clinical
population of workers with suspected work-related disease. In this study there was a very high
response rate (81%) for eligible subjects. Among workers being assessed for work-related skin or
respiratory disease, a surprising portion also reported work-related symptoms in the other
system. This is an important finding as the majority of clinical investigations are siloed and tend
to focus on one problem at a time. This study broke down the silos and demonstrated a need to
inquire about exposure and symptoms in other systems, particularly in cases where the exposures
are known to cause disease in more than one system.
7.8.2 Limitations
All of the studies reported in this thesis were cross-sectional in nature. Due to the limitations of
the cross-sectional design, no temporal relationships were investigated and causality cannot be
inferred from any reported associations. In hindsight, it may have been possible to address some
of the temporality issues that were raised in the discussion (i.e., order of symptom onset, use of
PPE before or after symptom onset) with carefully designed questionnaires. Unfortunately this
was not possible in studies using historical data, and was unfortunately not incorporated into
tools used for collecting new data.
Another aspect of this thesis that might be perceived as a limitation is the strong focus on
reported symptoms rather than clinical diagnoses. The lack of reliance on diagnostic testing is
due in large part to the fact that subjects were being clinically investigated for either skin or
respiratory disease, or had previously participated in a research that was focused on either skin or
respiratory symptoms, and therefore only received the diagnostic testing associated with one
system. In addition, the studies focused on concurrent symptoms were not particularly concerned
with the mechanism of action. Instead the goal was to determine the prevalence and predictors of
concurrent symptoms regardless of underlying mechanism. Thus it is possible that the concurrent
symptoms we observed arose from simultaneous exposure through both the skin and the

115
respiratory routes and that these potential simultaneous exposures may have included multiple
different exposure agents.
It would be interesting to undertake complete diagnostic testing for both biological systems of
interest (i.e., spirometry, methacholine, and patch testing) in all subjects in a future study, but the
cost is high and recruiting subjects for a significant amount of time and additional testing might
decrease the response rate.
A large limitation of studying concurrent symptoms is the lack of accepted methods for
investigating these two concurrent outcomes. In addition, the merging of data on respiratory and
skin data proved more challenging than anticipated.
The limitations of individual studies were described in each chapter. Briefly, the study in Chapter
6 included subjects from a wide variety of occupations and exposures that resulted in low power
for investigating predictors of interest and also issues of data sparseness. It was known a priori
that the group of patients seen in the clinic was varied, but the true extent of variety in exposures
and occupation had never been described. In future it may be preferable to limit the recruitment
of subjects by occupation or industry to reduce this variability.
The much discussed limitation within Chapter 5 is the use of airborne exposure as a proxy for
skin exposure. This choice may have resulted in exposure misclassification for skin exposure,
and may have contributed to the lack of an observed exposure-response for skin symptoms in
bakery workers. In studies utilizing historical data, the limitations of the data are inescapable.
Prospective studies of skin and respiratory outcomes should consider measuring, or at least
estimating, both skin and airborne exposure wherever possible.
Chapter 4 was again limited by the historical data utilized. No detailed analysis on exposures in
these groups was undertaken as it was not feasible to combine the exposures measured in the
individual occupational groups into a single exposure metric. Additionally, the health outcomes
and diagnostic testing completed were different between the four groups, which again limited the
ability to pool these results. Currently, further research into the group of embalmers is underway.
The workers in this group are exposed to both glutaraldehyde and formaldehyde, exposure was
measured for both the skin and inhalation routes, and subjects were clinically investigated for
both skin and respiratory outcomes.

116
The main limitation of the study identifying common contact allergens and their ability to also
cause OA (Chapter 3) was that this process was not completed for the opposite scenario:
common causes of OA that can also cause CD. This additional work was not undertaken due to
the inability to access sufficient data for the causes of occupational asthma cases. This limitation
could potentially be resolved through the development of a surveillance system for OA, or by
identifying the common causes of OA from workers’ compensation claims on a province-by-
province effort, though both of these may be limited by under-reporting of occupational asthma.
7.9 Contribution to the Literature
Overall, the results from this thesis provide evidence from several perspectives that the skin and
respiratory systems are more closely related in the occupational setting than previously realized.
The exact nature of this connection is not fully understood, and will likely differ depending on
the exposure hazard and exposure scenario, but clearly needs to be investigated in future
research.
This body of work provides evidence that several common occupational exposures can cause
disease in both the skin and respiratory system as a result of skin and airborne exposures,
respectively. In general, there is a need to better communicate the risks of both skin and
respiratory exposure to workers, occupational health and safety practitioners, and clinicians so
that occupational disease does not continue to be under-recognized and under-reported.
The results from this thesis demonstrate that among working populations and clinical
populations, a portion of workers do report both skin and respiratory symptoms, though a smaller
portion report concurrent skin and respiratory symptoms that are work-related. These symptoms
may be due to a single exposure agent or to multiple exposure agents, perhaps even a different
exposure in each system; more work is needed to answer these questions. The study of bakery
workers and auto body shop workers confirms previous research results that workers with skin
symptoms are more likely to report respiratory symptoms. Future studies need to gather detailed
exposure information about both skin and airborne exposures into order to better determine the
role of allergen and irritants exposures in the development of skin and respiratory symptoms.
The study of auto body shop workers also provides support that exposure-response relationships
do exist for skin symptoms, both work-related and non-work-related. The potential importance of

117
skin exposures in the development of occupational isocyanate-induced asthma is currently being
studied by a handful of research groups. Results from these ongoing studies are sure to shed
more light on the role of skin exposure in the development of occupational isocyanate-induced
asthma.
Models constructed to identify predictors of concurrent symptom suggested that subjects with a
history of eczema had great odds of reporting concurrent symptoms. This finding supports
previous occupational research that showed a relationship between skin disease or skin damage
and both the uptake of exposure and the likelihood of reporting respiratory symptoms. The role
for skin barrier function in modifying the uptake of skin exposure and potentially contributing to
the development of respiratory symptoms should continue to be investigated in occupational
studies.
After synthesizing the results from this thesis, the proposed framework from Figure 2 has been
modified to include the additional factors of co-morbid disease, personal characteristics, and PPE
use. These factors, along with the previously included genetic factors, have been added to the
framework with dotted lines to indicate potential associations, not necessarily causal
relationships.

118
Figure 6 Modified Framework for Conceptualizing the Connections Between Skin and
Respiratory Symptoms in Occupational Disease.

119
Chapter 8 Conclusions
This thesis is made up of four studies that explore the connection between skin and airborne
exposures as well as between skin and respiratory symptoms and disease. The studies included in
this thesis contribute to the collective understanding of the connection between the skin and
respiratory systems in terms of exposure, response (symptoms), and exposure-response
relationships.
Overall, the results of this thesis demonstrate that the skin and respiratory systems are associated
more closely in terms of occupational exposure and health outcomes than previously considered.
This thesis offers four main findings on the potential connection between the skin and respiratory
systems in terms of occupational exposures and health outcomes:
1. Common occupational contact allergens are also capable of causing occupational asthma,
but may not be recognized correctly as sensitizers in common reference materials.
2. Exposure-response relationships exist for skin symptoms in auto-body workers, and these
relationships deserve further study in all occupations with potential skin exposure.
3. Workers in the workplace, as well as workers with suspected occupational disease in a
clinical setting, report concurrent skin and respiratory symptoms. A portion of these
symptomatic workers associates both of their concurrent symptoms with their work.
4. Subjects who report a history of eczema, are current smokers, wear a respirator at work
and work in large workplaces are more likely to report concurrent skin and respiratory
symptoms (both work-related and non-work-related). The relationship between eczema
and concurrent symptoms lends support to previous findings that skin barrier function in
pathway from exposure to symptoms.

120
Chapter 9 Future Directions
The results from this thesis have generated many new research questions across a variety of
disciplines - exposure assessment, occupational hygiene, disease surveillance and mechanistic
research - that could, and should, be the subject of future study.
Additionally, there are many research questions that remain to be answered within the data
collected for Chapter 6. This data collected as part of the study described in Chapter 6 contains a
large amount of data on prevention of occupational exposures. Prevention was not a focus of this
thesis but is an important consideration in the study of skin and respiratory outcomes. Future
analyses will include a description of personal protective equipment (PPE) use and prevention
training in the workplace. The goal will be to identify the predictors of PPE use within this
population of workers.
The results from Chapter 3 identified seven exposures, which are capable of causing both
occupational contact dermatitis and occupational asthma. This list of seven exposures will help
identify workplaces and workers for in-depth studies of exposure and response in both the skin
and respiratory systems together. Workers exposure to these agents may be at risk of both skin
and respiratory symptoms.
Smaller studies with carefully planned exposure assessment that includes both skin and airborne
exposure measurements will help clarify whether there are significant skin and inhalation
exposure hazards for workers. If both exposures exist, this type of data will allow for the
investigation of correlation between theses exposures, and exposure-response associations with
both skin and respiratory outcomes. These analyses will provide exposure (and exposure
scenario) specific insight into whether workers are at risk of skin and/or respiratory outcomes,
and the relative importance of each route of exposure with respect to the individual outcomes.
Within future studies it will be important to better record the use and protection factors of PPE
among participants. The role of PPE in modifying exposure, as well as the potential for PPE use
(and PPE protection factors) to differ between the skin and respiratory systems will need to be
considered. This task could be undertaken in several ways: self-reported use of PPE (e.g.,
frequency, duration), direct observation of PPE use in the workplace, or perhaps even biomarkers
of exposure that measure the internal dose taking into consideration the effects of PPE.

121
The results that demonstrated a lack of agreement across the occupational hygiene reference
materials show that there is a need for researchers to better collaborate with occupational
hygienists. There is a need to integrate research knowledge with practical field reference
documents. This work may not take the form of formal research projects, but could involve
improved collaboration of researchers and hygienists in the decision making process around
sensitizer and skin notations. This knowledge transfer and exchange between disciplines is
crucial for effective and efficient risk communication and the protection of workers.
In this age of technology and mobile devices it seems plausible that the information from
multiple occupational hygiene or occupational health and safety applications could be merged
into a master application which allows workers on-site access to a variety of different documents
summarizing relevant health and safety information. A few individual organizations have put
their documents into a mobile application format (e.g., NIOSH Handbook, WHIMS) but a
merging of information does not appear to have been attempted. Though the overall task would
be a large one, it might be possible to undertake the development of a mobile application and
linkage of data and for one industry as a pilot/feasibility study.
This thesis has highlighted the discrepancy between our understanding of skin exposure-response
and our understanding of exposure-response in the respiratory system. There is a basic need to
better understand the burden of dermatitis, including occupational dermatitis, in the general
population. These estimates could be obtained through the analysis of administrative and
workers’ compensation data for skin disease claims, as has been done successfully for
occupational asthma in several Canadian jurisdictions.
There is also a need for methodological studies to better determine if, and which, skin symptoms
and questionnaire items are predictive of dermatological diagnoses. Studies designed to identify
symptoms (or symptoms combinations) that identify cases of allergic contract dermatitis, or that
differentiate between irritant and allergic contact dermatitis, would permit the use of
questionnaires in place of physician diagnosis in subsequent studies. A study of this nature will
require a large data set that includes information on reported skin symptoms as well as physician
diagnoses. Within a group that has a history of research standardization, such as the NACDG,
this may be feasible.

122
We also need to further our understanding of skin exposure and exposure-response relationships
for skin symptoms. These studies can be undertaken in workplaces with known skin hazards,
identified either through the results presented in Chapter 3, or from other surveillance data on
common causes of contact dermatitis. These studies of skin exposure should be accompanied by
measurements of skin barrier function, either through direct measurement or a questionnaire tool
(question or picture based). The incorporation of skin barrier measurement in studies of
exposure, biomarkers of exposure and exposure-response will allow for better understanding of
how and if the skin barrier modifies exposure-response relationships.
Beyond the exposure-response relationships within the skin, there is also a need to better
understand the role of skin exposure in the development of respiratory sensitization and disease.
As airborne exposure continues to be the focus of research and control strategies, airborne
exposures will continue to decrease and the relative importance of skin exposure will increase.
This shift is already occurring in the cases of isocyanate and beryllium exposure, and there will
likely be other examples in the future.
Despite the challenges, these complicated pathways can only be fully addressed in studies where
both skin and airborne exposures are measured, and both skin and respiratory outcomes are
considered. This design would allow for the relative importance of each route of exposure to be
considered; the tendencies for correlation between skin and airborne exposure will complicate
this task but it is a challenge that should be overcome.
There are also general themes that are highlighted in the limitations of this work. There is a need
for well designed, prospective studies that allow for repeated measurements and the study of
temporality of the exposure-sensitization-symptom-disease pathway. Though prospective studies
are the ideal approach to these problems, careful questionnaire design could also result in rich
data that allows for retrospective construction of exposure and response patterns. It seems likely
that in order to address the complex relationships between exposure and response in the skin and
respiratory symptoms it will be fruitful to focus on studies of one exposure in a more
homogenous working population where the variability within and between workers can be
accurately assessed.

123
The results of this study have contributed to the basic understanding on the relationship between
the skin and respiratory systems in terms of exposure and disease, but there is an overwhelming
amount of work yet to be done.

124
References
Akinbami LJ, Moorman JE, Liu X. 2011. Asthma prevalence, health care use, and mortality:
United states, 2005–2009 National Health Statistics Reports 32.
Alvarez-Cuesta C, Gala Ortiz G, Rodriguez Diaz E, Blanco Barrios S, Galache Osuna C, Raya
Aguado C, Pineda F. 2004. Occupational asthma and IgE-mediated contact dermatitis from
sapele wood. Contact Dermatitis 51(2):88-98.
American Conference of Governmental Industrial Hygienists (ACGIH). 2008. 2008 TLVs and
BEIs threshold limit values for chemical substances and physical agents. .
Aprea C, Lunghini L, Banchi B, Peruzzi A, Centi L, Coppi L, Bogi M, Marianelli E, Fantacci M,
Catalano P, Benvenuti A, Miligi L, Sciarra G. 2009. Evaluation of inhaled and cutaneous doses
of imidacloprid during stapling ornamental plants in tunnels or greenhouses. J Expo Sci Environ
Epidemiol 19(6):555-569.
Arrandale VH, Liss GM, Tarlo SM, Pratt MD, Sasseville D, Kudla I, Holness DL. 2012.
Occupational contact allergens: Are they also associated with occupational asthma? Am J Ind
Med .
Arts J, de Koning M, Bloksma N, Kuper C. 2004. Respiratory allergy to trimellitic anhydride in
rats: Concentration-response relationships during elicitation. Inhal Toxicol 16(5):259-269.
Arts JH, Kuper CF, Spoor SM, Bloksma N. 1998. Airway morphology and function of rats
following dermal sensitization and respiratory challenge with low molecular weight chemicals.
Toxicol Appl Pharmacol 152(1):66-76.
Arts JH, Mommers C, de Heer C. 2006. Dose-response relationships and threshold levels in skin
and respiratory allergy. Crit Rev Toxicol 36(3):219-251.
Ashley K, Applegate GT, Wise TJ, Fernback JE, Goldcamp MJ. 2007. Evaluation of a
standardized micro-vacuum sampling method for collection of surface dust. J Occup Environ
Hyg 4(3):215-223.

125
Australian Bureau of Statistics. 2011, 3235.0 population by age and sex, regions of Australia
2010. (October 18, 2011).
Banks DE, Jalloul A. 2007. Occupational asthma, work-related asthma and reactive airways
dysfunction syndrome. Curr Opin Pulm Med 13(2):131-136.
Barbuzza O, Guarneri F, Galtieri G, Gangemi S, Vaccaro M. 2009. Protein contact dermatitis
and allergic asthma caused by Anisakis simplex. Contact Dermatitis 60(4):239-240.
Bello D, Redlich CA, Stowe MH, Sparer J, Woskie SR, Streicher RP, Hosgood HD, Liu Y.
2008. Skin exposure to aliphatic polyisocyanates in the auto body repair and refinishing industry:
II. A quantitative assessment. Ann Occup Hyg 52(2):117-124.
Benfeldt E, Serup J, Menne T. 1999. Effect of barrier perturbation on cutaneous salicylic acid
penetration in human skin: In vivo pharmacokinetics using microdialysis and non-invasive
quantification of barrier function. Br J Dermatol 140(4):739-748.
Bernstein IL, Chan-Yeung M, Malo J, Bernstein DI. 2006a. Asthma in the workplace, and
related conditions. .
Bernstein IL, Chan-Yeung M, Malo J, Bernstein DI. 2006b. Definition and classification of
asthma in the workplace (Chapter 1). In: Bernstein IL, Chan-Yeung M, Malo J, Bernstein DI,
editors. 3rd ed. New York: Taylor & Francis. p 1-8.
Bjorksten B. 1996. The role of the gastrointestinal tract in the development of respiratory
hypersensitivities. Toxicol Lett 86(2-3):85-88.
Blanc PD, Toren K. 1999. How much adult asthma can be attributed to occupational factors? Am
J Med 107(6):580-587.
Boeniger MF. 2003. The significance of skin exposure. Ann Occup Hyg 47(8):591-593.
Bos PM, Brouwer DH, Stevenson H, Boogaard PJ, de Kort WL, van Hemmen JJ. 1998. Proposal
for the assessment of quantitative dermal exposure limits in occupational environments: Part 1.
Development of a concept to derive a quantitative dermal occupational exposure limit. Occup
Environ Med 55(12):795-804.

126
Bremmer SF, Hanifin JM, Simpson EL. 2008. Clinical detection of ichthyosis vulgaris in an
atopic dermatitis clinic: Implications for allergic respiratory disease and prognosis. J Am Acad
Dermatol 59(1):72-78.
Brooks SM, Weiss MA, Bernstein IL. 1985. Reactive airways dysfunction syndrome (RADS).
Persistent asthma syndrome after high level irritant exposures. Chest 88(3):376-384.
Burney PG, Laitinen LA, Perdrizet S, Huckauf H, Tattersfield AE, Chinn S, Poisson N, Heeren
A, Britton JR, Jones T. 1989. Validity and repeatability of the IUATLD (1984) bronchial
symptoms questionnaire: An international comparison. Eur Respir J 2(10):940-945.
Burstyn I, Ferrari P, Wegh H, Heederik D, Kromhout H. 2002. Characterizing worker exposure
to bitumen during hot mix paving and asphalt mixing operations. AIHA J (Fairfax, VA)
63(3):293-299.
Cadot P, Tits G, Bussels L, Ceuppens JL. 2001. Asthma and hand dermatitis to leek. Allergy
56(2):192-193.
Carstensen O, Rasmussen K, Ponten A, Gruvberger B, Isaksson M, Bruze M. 2006. The validity
of a questionnaire-based epidemiological study of occupational dermatosis. Contact Dermatitis
55(5):295-300.
Chang FK, Chen ML, Cheng SF, Shih TS, Mao IF. 2007a. Dermal absorption of solvents as a
major source of exposure among shipyard spray painters. J Occup Environ Med 49(4):430-436.
Chang FK, Chen ML, Cheng SF, Shih TS, Mao IF. 2007b. Evaluation of dermal absorption and
protective effectiveness of respirators for xylene in spray painters. Int Arch Occup Environ
Health 81(2):145-150.
Chiang WC, Pons L, Kidon MI, Liew WK, Goh A, Wesley Burks A. 2010. Serological and
clinical characteristics of children with peanut sensitization in an Asian community. Pediatr
Allergy Immunol 21(2 Pt 2):e429-38.
Cox-Ganser JM, Rao CY, Park JH, Schumpert JC, Kreiss K. 2009. Asthma and respiratory
symptoms in hospital workers related to dampness and biological contaminants. Indoor Air
19(4):280-290.

127
Crapo RO, Morris AH, Gardner RM. 1981. Reference spirometric values using techniques and
equipment that meet ATS recommendations. Am Rev Respir Dis 123(6):659-664.
Cullinan P, Cook A, Jones M, Cannon J, Fitzgerald B, Taylor AJ. 1997. Clinical responses to
ingested fungal alpha-amylase and hemicellulase in persons sensitized to Aspergillus fumigatus?
Allergy 52(3):346-349.
Cullinan P, Cook A, Nieuwenhuijsen MJ, Sandiford C, Tee RD, Venables KM, McDonald JC,
Newman Taylor AJ. 2001. Allergen and dust exposure as determinants of work-related
symptoms and sensitization in a cohort of flour-exposed workers; a case-control analysis. Ann
Occup Hyg 45(2):97-103.
Daftarian HS, Lushniak BD, Reh CM, Lewis DM. 2002. Evaluation of self-reported skin
problems among workers exposed to toluene diisocyanate (TDI) at a foam manufacturing
facility. J Occup Environ Med 44(12):1197-1202.
Day GA, Dufresne A, Stefaniak AB, Schuler CR, Stanton ML, Miller WE, Kent MS, Deubner
DC, Kreiss K, Hoover MD. 2007. Exposure pathway assessment at a copper-beryllium alloy
facility. Ann Occup Hyg 51(1):67-80.
Day GA, Stefaniak AB, Weston A, Tinkle SS. 2006. Beryllium exposure: Dermal and
immunological considerations. Int Arch Occup Environ Health 79(2):161-164.
de Joode BW, Vermeulen R, Heederik D, van Ginkel K, Kromhout H. 2007. Evaluation of 2
self-administered questionnaires to ascertain dermatitis among metal workers and its relation
with exposure to metalworking fluids. Contact Dermatitis 56(6):311-317.
De Raeve H, Vandecasteele C, Demedts M, Nemery B. 1998. Dermal and respiratory
sensitization to chromate in a cement floorer. Am J Ind Med 34(2):169-176.
De Zotti R, Larese F, Fiorito A. 1992. Asthma and contact urticaria from latex gloves in a
hospital nurse. Br J Ind Med 49(8):596-598.
Diepgen TL, Coenraads PJ. 1999. The epidemiology of occupational contact dermatitis. Int Arch
Occup Environ Health 72(8):496-506.

128
Doekes G, Douwes J, Wouters I, de Wind S, Houba R, Hollander A. 1996. Enzyme
immunoassays for total and allergen specific IgE in population studies. Occup Environ Med
53(1):63-70.
Donovan JC, Kudla I, DeKoven JG. 2009. Rapid development of allergic contact dermatitis from
dicyclohexylmethane-4,4'-diisocyanate. Dermatitis 20(4):214-217.
English JS. 2004. Current concepts of irritant contact dermatitis. Occup Environ Med 61(8):722-
6, 674.
Estlander T, Kanerva L, Tupasela O, Keskinen H, Jolanki R. 1993. Immediate and delayed
allergy to nickel with contact urticaria, rhinitis, asthma and contact dermatitis. Clin Exp Allergy
23(4):306-310.
Fantuzzi G, Righi E, Predieri G, Giacobazzi P, Mastroianni K, Aggazzotti G. 2010. Prevalence
of ocular, respiratory and cutaneous symptoms in indoor swimming pool workers and exposure
to disinfection by-products (DBPs). Int J Environ Res Public Health 7(4):1379-1391.
Fenske RA, Leffingwell JT, Spear RC. 1986a. A video imaging technique for assessing dermal
exposure. I. Instrument design and testing. Am Ind Hyg Assoc J 47(12):764-770.
Fenske RA, Wong SM, Leffingwell JT, Spear RC. 1986b. A video imaging technique for
assessing dermal exposure. II. Fluorescent tracer testing. Am Ind Hyg Assoc J 47(12):771-775.
Fent KW, Jayaraj K, Ball LM, Nylander-French LA. 2008. Quantitative monitoring of dermal
and inhalation exposure to 1,6-hexamethylene diisocyanate monomer and oligomers. J Environ
Monit 10(4):500-507.
Ferris BG. 1978. Epidemiology standardization project (American Thoracic Society). Am Rev
Respir Dis 118(6):1-120.
Flack S, Goktepe I, Ball LM, Nylander-French LA. 2008. Development and application of
quantitative methods for monitoring dermal and inhalation exposure to propiconazole. J Environ
Monit 10(3):336-344.

129
Franko J, Jackson LG, Hubbs A, Kashon M, Meade BJ, Anderson SE. 2011. Evaluation of
furfuryl alcohol sensitization potential following dermal and pulmonary exposure: Enhancement
of airway responsiveness. Toxicol Sci .
Frick M, Bjorkner B, Hamnerius N, Zimerson E. 2003. Allergic contact dermatitis from
dicyclohexylmethane-4,4'-diisocyanate. Contact Dermatitis 48(6):305-309.
Friis L, Norback D, Edling C. 1999. Self-reported asthma and respiratory symptoms in sewage
workers. Journal of Occupational Health 41(2):87-90.
Frost G, Darnton A, Harding AH. 2011. The effect of smoking on the risk of lung cancer
mortality for asbestos workers in Great Britain (1971-2005). Ann Occup Hyg 55(3):239-247.
Fujita H, Ogawa M, Endo Y. 2006. A case of occupational bronchial asthma and contact
dermatitis caused by ortho-phthalaldehyde exposure in a medical worker. J Occup Health
48(6):413-416.
Gautrin D, Bernstein IL, Brooks SM, Henneberger PK. 1999. Ch. 25 reactive airways
dysfunction syndrome and irritant induced asthma. In: Bernstein IL, Bernstein DI, Chan-Yeung
M, Malo J, editors. Asthma in the workplace. 2nd ed. New York: M. Dekker.
Goe SK, Henneberger PK, Reilly MJ, Rosenman KD, Schill DP, Valiante D, Flattery J, Harrison
R, Reinisch F, Tumpowsky C, Filios MS. 2004. A descriptive study of work aggravated asthma.
Occup Environ Med 61(6):512-517.
Guarneri F, Barbuzza O, Vaccaro M, Galtieri G. 2008. Allergic contact dermatitis and asthma
caused by limonene in a labourer handling citrus fruits. Contact Dermatitis 58(5):315-316.
Hannaford-Turner K, Elder D, Sim MR, Abramson MJ, Johnson AR, Yates DH. 2010.
Surveillance of Australian workplace Based Respiratory Events (SABRE) in New South Wales.
Occup Med (Lond) .
Hannu T, Frilander H, Kauppi P, Kuuliala O, Alanko K. 2009. IgE-mediated occupational
asthma from epoxy resin. Int Arch Allergy Immunol 148(1):41-44.
Hastie T. 1990. Generalized additive models. London: Chapman and Hall. .

130
Heldal KK, Madso L, Huser PO, Eduard W. 2010. Exposure, symptoms and airway
inflammation among sewage workers. Ann Agric Environ Med 17(2):263-268.
Herrick CA, Xu L, Wisnewski AV, Das J, Redlich CA, Bottomly K. 2002. A novel mouse model
of diisocyanate-induced asthma showing allergic-type inflammation in the lung after inhaled
antigen challenge. J Allergy Clin Immunol 109(5):873-878.
Higgins IT. 1959. Tobacco smoking, respiratory symptoms, and ventilatory capacity; studies in
random samples of the population. Br Med J 1(5118):325-329.
Hill AB. 1965. The environment and disease: Association or causation? Proc R Soc Med 58:295-
300.
Hino R, Nishio D, Kabashima K, Tokura Y. 2008. Percutaneous penetration via hand eczema is
the major accelerating factor for systemic absorption of toluene and xylene during car spray
painting. Contact Dermatitis 58(2):76-79.
Holgate ST. 2008. The airway epithelium is central to the pathogenesis of asthma. Allergol Int
57(1):1-10.
Holness DL, Broder I, Corey PN, Booth N, Mozzon D, Nazar MA, Guirguis S. 1984.
Respiratory variables and exposure-effect relationships in isocyanate-exposed workers. J Occup
Med 26(6):449-455.
Holness DL, Nethercott JR. 1989. Health status of funeral service workers exposed to
formaldehyde. Arch Environ Health 44(4):222-228.
Holness DL, Purdham JT, Nethercott JR. 1989. Acute and chronic respiratory effects of
occupational exposure to ammonia. Am Ind Hyg Assoc J 50(12):646-650.
Holness DL, Tarlo SM, Sussman G, Nethercott JR. 1995. Exposure characteristics and cutaneous
problems in operating room staff. Contact Dermatitis 32(6):352-358.
Holter G, Irgens A, Nyfors A, Aasen TB, Florvaag E, Overa KB, Elsayed S, Naerheim J. 2002.
Self-reported skin and respiratory symptoms related to latex exposure among 5,087 hospital
employees in Norway. Dermatology 205(1):28-31.

131
Hughson GW, Cherrie JW. 2005. Comparison of measured dermal dust exposures with predicted
exposures given by the EASE expert system. Ann Occup Hyg 49(2):111-123.
Hughson GW, Galea KS, Heim KE. 2010. Characterization and assessment of dermal and
inhalable nickel exposures in nickel production and primary user industries. Ann Occup Hyg
54(1):8-22.
Huusom AJ, Agner T, Backer V, Ebbehoj N, Jacobsen P. 2011. Skin and respiratory disorders
following the identification of disaster victims in Thailand. Forensic Sci Med Pathol.
Igea JM, Fernandez M, Quirce S, de la Hoz B, Diez Gomez ML. 1994. Green bean
hypersensitivity: An occupational allergy in a homemaker. J Allergy Clin Immunol 94(1):33-35.
Industry Canada. 2011. Canadian industry statistics - glossary of terms. .
Isaksson M, Bruze M. 2002. Allergic contact dermatitis in response to budesonide reactivated by
inhalation of the allergen. J Am Acad Dermatol 46(6):880-885.
Jaakkola MS, Suuronen K, Luukkonen R, Jarvela M, Tuomi T, Alanko K, Makela EA, Jolanki
R. 2009. Respiratory symptoms and conditions related to occupational exposures in machine
shops. Scand J Work Environ Health 35(1):64-73.
Jacobs JH, Meijster T, Meijer E, Suarthana E, Heederik D. 2008. Wheat allergen exposure and
the prevalence of work-related sensitization and allergy in bakery workers. Allergy 63(12):1597-
1604.
Jacobs MC, Rycroft RJ. 1995. Contact dermatitis and asthma from sodium metabisulfite in a
photographic technician. Contact Dermatitis 33(1):65-66.
Jakasa I, de Jongh CM, Verberk MM, Bos JD, Kezic S. 2006. Percutaneous penetration of
sodium lauryl sulphate is increased in uninvolved skin of patients with atopic dermatitis
compared with control subjects. Br J Dermatol 155(1):104-109.
Jenkins MA, Clarke JR, Carlin JB, Robertson CF, Hopper JL, Dalton MF, Holst DP, Choi K,
Giles GG. 1996. Validation of questionnaire and bronchial hyperresponsiveness against
respiratory physician assessment in the diagnosis of asthma. Int J Epidemiol 25(3):609-616.

132
Kanerva L, Estlander T, Keskinen H, Jolanki R. 2000. Occupational allergic airborne contact
dermatitis and delayed bronchial asthma from epoxy resin revealed by bronchial provocation
test. Eur J Dermatol 10(6):475-477.
Kanerva L, Jolanki R, Tupasela O, Halmepuro L, Keskinen H, Estlander T, Sysilampi ML. 1991.
Immediate and delayed allergy from epoxy resins based on diglycidyl ether of bisphenol A.
Scand J Work Environ Health 17(3):208-215.
Kanerva L, Keskinen H, Autio P, Estlander T, Tuppurainen M, Jolanki R. 1995. Occupational
respiratory and skin sensitization caused by polyfunctional aziridine hardener. Clin Exp Allergy
25(5):432-439.
Karjalainen A, Kurppa K, Virtanen S, Keskinen H, Nordman H. 2000. Incidence of occupational
asthma by occupation and industry in Finland. Am J Ind Med 37(5):451-458.
Kimber I, Basketter DA, Gerberick GF, Dearman RJ. 2002. Allergic contact dermatitis. Int
Immunopharmacol 2(2-3):201-211.
Klink KJ, Meade BJ. 2003. Dermal exposure to 3-amino-5-mercapto-1,2,4-triazole (AMT)
induces sensitization and airway hyperreactivity in BALB/c mice. Toxicol Sci 75(1):89-98.
Krautheim AB, Jermann TH, Bircher AJ. 2004. Chlorhexidine anaphylaxis: Case report and
review of the literature. Contact Dermatitis 50(3):113-116.
Kujala VM, Reijula KE. 1995. Glove-induced dermal and respiratory symptoms among health
care workers in one Finnish hospital. Am J Ind Med 28(1):89-98.
Kuper CF, Radonjic M, van Triel J, Stierum R, de Groot RJ, Arts JH. 2011. Oxazolone (OXA) is
a respiratory allergen in brown Norway rats. Toxicology 290(1):59-68.
Kuper CF, Stierum RH, Boorsma A, Schijf MA, Prinsen M, Bruijntjes JP, Bloksma N, Arts JH.
2008. The contact allergen dinitrochlorobenzene (DNCB) and respiratory allergy in the Th2-
prone brown Norway rat. Toxicology 246(2-3):213-221.
Lachapelle J. 1995. Historical aspects. In: Frosch PJ, Menné T, Rycroft RJG, editors. Textbook
of contact dermatitis. 2nd ed. New York: Springer-Verlag.

133
Lakwijk N, Van Strien RT, Doekes G, Brunekreef B, Gerritsen J. 1998. Validation of a screening
questionnaire for atopy with serum IgE tests in a population of pregnant Dutch women. Clin Exp
Allergy 28(4):454-458.
Lastbom L, Boman A, Camner P, Ryrfeldt A. 2000. Increased airway responsiveness after skin
sensitisation to 3-carene, studied in isolated guinea pig lungs. Toxicology 147(3):209-214.
Lastbom L, Boman A, Camner P, Ryrfeldt A. 1998. Does airway responsiveness increase after
skin sensitisation to 3-carene: A study in isolated guinea pig lungs. Toxicology 125(1):59-66.
Lee HK, Alarie Y, Karol MH. 1984. Induction of formaldehyde sensitivity in guinea pigs.
Toxicol Appl Pharmacol 75(1):147-155.
Leffler CT, Milton DK. 1999. Occupational asthma and contact dermatitis in a spray painter after
introduction of an aziridine cross-linker. Environ Health Perspect 107(7):599-601.
Lehto M, Haapakoski R, Wolff H, Majuri ML, Makela MJ, Leino M, Reunala T, Turjanmaa K,
Palosuo T, Alenius H. 2005. Cutaneous, but not airway, latex exposure induces allergic lung
inflammation and airway hyperreactivity in mice. J Invest Dermatol 125(5):962-968.
Liljelind I, Norberg C, Egelrud L, Westberg H, Eriksson K, Nylander-French LA. 2010. Dermal
and inhalation exposure to methylene bisphenyl isocyanate (MDI) in iron foundry workers. Ann
Occup Hyg 54(1):31-40.
Lillienberg L, Andersson EM, Jarvholm B, Toren K. 2010. Respiratory symptoms and exposure-
response relations in workers exposed to metalworking fluid aerosols. Ann Occup Hyg
54(4):403-411.
Lindgren T, Andersson K, Dammstrom BG, Norback D. 2002. Ocular, nasal, dermal and general
symptoms among commercial airline crews. International Archives of Occupational &
Environmental Health 75(7):475-483.
Lockman LE. 2002. Case report: Allergic contact dermatitis and new-onset asthma. Chromium
exposure during leather tanning. Can Fam Physician 48:1907-1909.

134
Lombardo LJ, Balmes JR. 2000. Occupational asthma: A review. Environ Health Perspect 108
Suppl 4:697-704.
Lundgren L, Skare L, Liden C. 2006. Measuring dust on skin with a small vacuuming sampler--a
comparison with other sampling techniques. Ann Occup Hyg 50(1):95-103.
Lushniak BD. 2004. Occupational contact dermatitis. Dermatol Ther 17(3):272-277.
Lynde CB, Obadia M, Liss GM, Ribeiro M, Holness DL, Tarlo SM. 2009. Cutaneous and
respiratory symptoms among professional cleaners. Occup Med (Lond) 59(4):249-254.
Maestrelli P, Boschetto P, Fabbri LM, Mapp CE. 2009. Mechanisms of occupational asthma. J
Allergy Clin Immunol 123(3):531-542.
Malo JL, Chan-Yeung M. 2009. Agents causing occupational asthma. J Allergy Clin Immunol
123(3):545-550.
Mapp CE. 2001. Agents, old and new, causing occupational asthma. Occup Environ Med
58(5):354-60, 290.
Mapp CE, Boschetto P, Maestrelli P, Fabbri LM. 2005. Occupational asthma. Am J Respir Crit
Care Med 172(3):280-305.
Marks JG, Elsner P, DeLeo VA. 1992. Allergic and irritant contact dermatitis. In: Contact and
occupational dermatology. St. Louis: Mosby Year Book.
Martin PE, Matheson MC, Gurrin L, Burgess JA, Osborne N, Lowe AJ, Morrison S, Meszaros
D, Giles GG, Abramson MJ, Walters EH, Allen KJ, Dharmage SC. 2011. Childhood eczema and
rhinitis predict atopic but not non-atopic adult asthma: A prospective cohort study over 4
decades. J Allergy Clin Immunol 127(6):1473-9.e1.
Mathias CGT. 1994. Occupational dermatoses. In: Dickerson OB, Horvath EP, Zenz C, editors.
Occupational medicine. 3rd ed. ed. St. Louis: Mosby.
McClean MD, Rinehart RD, Ngo L, Eisen EA, Kelsey KT, Herrick RF. 2004. Inhalation and
dermal exposure among asphalt paving workers. Ann Occup Hyg 48(8):663-671.

135
McDonald JC, Beck MH, Chen Y, Cherry NM. 2006. Incidence by occupation and industry of
work-related skin diseases in the united kingdom, 1996-2001. Occup Med (Lond) 56(6):398-405.
McDonald JC, Chen Y, Zekveld C, Cherry NM. 2005. Incidence by occupation and industry of
acute work related respiratory diseases in the UK, 1992-2001. Occup Environ Med 62(12):836-
842.
Medical Research Council on the Aetiology of Chronic Bronchitis. 1960. Standardised
questionnaire on respiratory symptoms. Br Med J 2:1665.
Meding B, Barregard L. 2001. Validity of self-reports of hand eczema. Contact Dermatitis
45(2):99-103.
Meijster T, Tielemans E, de Pater N, Heederik D. 2007. Modelling exposure in flour processing
sectors in the Netherlands: A baseline measurement in the context of an intervention program.
Ann Occup Hyg 51(3):293-304.
Moulin P, Magnan A, Lehucher-Michel MP. 2009. Occupational allergic contact dermatitis and
asthma due to a single low molecular weight agent. J Occup Health 51(1):91-96.
National Institute for Occupational Safety and Health. 2007. NIOSH pocket guide to chemical
hazards. DHHS (NIOSH) Publication No. 2005-149.
National Institutes of Health. 2009. Haz-Map: Occupational exposures to hazardous agents. .
Nemery B, Lenaerts L. 1993. Exposure to methylene diphenyl diisocyanate in coal mines. Lancet
341(8840):318.
Nemoto-Hasebe I, Akiyama M, Nomura T, Sandilands A, McLean WI, Shimizu H. 2008.
Clinical severity correlates with impaired barrier in filaggrin-related eczema. J Invest Dermatol.
Nethercott JR, Holness DL. 1989. Occupational dermatitis in food handlers and bakers. J Am
Acad Dermatol 21(3 Pt 1):485-490.
Nethercott JR, Holness DL. 1988. Health status of a group of sewage treatment workers in
Toronto, Canada. Am Ind Hyg Assoc J 49(7):346-350.

136
Nettis E, Assennato G, Ferrannini A, Tursi A. 2002. Type I allergy to natural rubber latex and
type IV allergy to rubber chemicals in health care workers with glove-related skin symptoms.
Clin Exp Allergy 32(3):441-447.
Nielsen JB. 2005. Percutaneous penetration through slightly damaged skin. Arch Dermatol Res
296(12):560-567.
Paggiaro PL, Loi AM, Toma G. 1979. Bronchial asthma and dermatitis due to spiramycin in a
chick breeder. Clin Allergy 9(6):571-574.
Pal TM, de Wilde NS, van Beurden MM, Coenraads PJ, Bruynzeel DP. 2009. Notification of
occupational skin diseases by dermatologists in the Netherlands. Occup Med (Lond) 59(1):38-
43.
Pauluhn J. 2008. Brown Norway rat asthma model of diphenylmethane-4,4'-diisocyanate (MDI):
Analysis of the elicitation dose-response relationship. Toxicol Sci 104(2):320-331.
Pekkanen J, Sunyer J, Anto JM, Burney P, European Community Respiratory Health Study.
2005. Operational definitions of asthma in studies on its aetiology. Eur Respir J 26(1):28-35.
Pelissier S, Chaboillez S, Teolis L, Lemiere C. 2006. Outcome of subjects diagnosed with
occupational asthma and work-aggravated asthma after removal from exposure. J Occup Environ
Med 48(7):656-659.
Petsonk EL, Wang ML, Lewis DM, Siegel PD, Husberg BJ. 2000. Asthma-like symptoms in
wood product plant workers exposed to methylene diphenyl diisocyanate. Chest 118(4):1183-
1193.
Pratt MD, Belsito DV, DeLeo VA, Fowler Jr. JF, Fransway AF, Maibach HI, Marks JG, Mathias
CG, Rietschel RL, Sasseville D, Sherertz EF, Storrs FJ, Taylor JS, Zug K. 2004. North American
Contact Dermatitis Group patch-test results, 2001-2002 study period. Dermatitis 15(4):176-183.
Pronk A, Preller L, Raulf-Heimsoth M, Jonkers IC, Lammers JW, Wouters IM, Doekes G,
Wisnewski AV, Heederik D. 2007. Respiratory symptoms, sensitization, and exposure response
relationships in spray painters exposed to isocyanates. Am J Respir Crit Care Med 176(11):1090-
1097.

137
Pronk A, Tielemans E, Skarping G, Bobeldijk I, VAN Hemmen J, Heederik D, Preller L. 2006a.
Inhalation exposure to isocyanates of car body repair shop workers and industrial spray painters.
Ann Occup Hyg 50(1):1-14.
Pronk A, Yu F, Vlaanderen J, Tielemans E, Preller L, Bobeldijk I, Deddens JA, Latza U, Baur X,
Heederik D. 2006b. Dermal, inhalation, and internal exposure to 1,6-HDI and its oligomers in
car body repair shop workers and industrial spray painters. Occup Environ Med 63(9):624-631.
Randolph BW, Lallooug, Gouws E, Colvin MS. 1997. An evaluation of the respiratory health
status of automotive spray-painters exposed to paints containing hexamethylene di-isocyanates in
the greater Durban area. S Afr Med J 87(3):318-323.
Rattray NJ, Botham PA, Hext PM, Woodcock DR, Fielding I, Dearman RJ, Kimber I. 1994.
Induction of respiratory hypersensitivity to diphenylmethane-4,4'-diisocyanate (MDI) in guinea
pigs. influence of route of exposure. Toxicology 88(1-3):15-30.
Redlich CA. 2010. Skin exposure and asthma: Is there a connection? Proc Am Thorac Soc
7(2):134-137.
Redlich CA, Herrick CA. 2008. Lung/skin connections in occupational lung disease. Curr Opin
Allergy Clin Immunol 8(2):115-119.
Rietschel RL, Mathias CG, Fowler Jr. JF, Pratt M, Taylor JS, Sherertz EF, Marks Jr. JG, Belsito
DV, Storrs FJ, Maibach HI, Fransway AF, Deleo VA, North American Contact Dermatitis G.
2002. Relationship of occupation to contact dermatitis: Evaluation in patients tested from 1998 to
2000. Am J Contact Dermat 13(4):170-176.
Riihimäki H, Kurppa K, Karjalainen A, Palo L, Jolanki R, Keskinen H, Mäkinen I, Saalo A,
Kauppinen T. 2004. Occupational diseases in Finland in 2002: New cases of occupational
diseases reported to the Finnish register of occupational disease. .
SAS Institute Inc. . 2008. SAS v.9.2. Version 9.2.
Sass-Kortsak AM, Holness DL, Pilger CW, Nethercott JR. 1986. Wood dust and formaldehyde
exposures in the cabinet-making industry. Am Ind Hyg Assoc J 47(12):747-753.

138
Schneider T, Vermeulen R, Brouwer DH, Cherrie JW, Kromhout H, Fogh CL. 1999. Conceptual
model for assessment of dermal exposure. Occup Environ Med 56(11):765-773.
Schnuch A, Lessmann H, Schulz KH, Becker D, Diepgen TL, Drexler H, Erdmann S, Fartasch
M, Greim H, Kricke-Helling P, Merget R, Merk H, Nowak D, Rothe A, Stropp G, Uter W,
Wallenstein G. 2002. When should a substance be designated as sensitizing for the skin ('sh') or
for the airways ('sa')? Hum Exp Toxicol 21(8):439-444.
Sistek D, Wickens K, Amstrong R, D'Souza W, Town I, Crane J. 2006. Predictive value of
respiratory symptoms and bronchial hyperresponsiveness to diagnose asthma in New Zealand.
Respir Med 100(12):2107-2111.
Smit HA, Coenraads PJ. 1993. A retrospective cohort study on the incidence of hand dermatitis
in nurses. Int Arch Occup Environ Health 64(8):541-544.
Smit HA, Coenraads PJ, Lavrijsen AP, Nater JP. 1992. Evaluation of a self-administered
questionnaire on hand dermatitis. Contact Dermatitis 26(1):11-16.
Smit HA, van Rijssen A, Vandenbroucke JP, Coenraads PJ. 1994. Susceptibility to and incidence
of hand dermatitis in a cohort of apprentice hairdressers and nurses. Scand J Work Environ
Health 20(2):113-121.
Smit LA, Heederik D, Doekes G, Blom C, van Zweden I, Wouters IM. 2008. Exposure-response
analysis of allergy and respiratory symptoms in endotoxin-exposed adults. Eur Respir J
31(6):1241-1248.
Sripaiboonkij P, Phanprasit W, Jaakkola MS. 2009a. Respiratory and skin effects of exposure to
wood dust from the rubber tree Hevea brasiliensis. Occup Environ Med 66(7):442-447.
Sripaiboonkij P, Sripaiboonkij N, Phanprasit W, Jaakkola MS. 2009b. Respiratory and skin
health among glass microfiber production workers: A cross-sectional study. Environ Health 8:36.
Statistics Canada. 2011. National occupational classification - statistics (NOC-S) 2006. 2011.
Steiner MF, Dick FD, Scaife AR, Semple S, Paudyal P, Ayres JG. 2011. High prevalence of skin
symptoms among bakery workers. Occup Med (Lond) 61(4):280-282.

139
Svensson A, Lindberg M, Meding B, Sundberg K, Stenberg B. 2002. Self-reported hand eczema:
Symptom-based reports do not increase the validity of diagnosis. Br J Dermatol 147(2):281-284.
Tarkowski M, Vanoirbeek JA, Vanhooren HM, De Vooght V, Mercier CM, Ceuppens J, Nemery
B, Hoet PH. 2007. Immunological determinants of ventilatory changes induced in mice by
dermal sensitization and respiratory challenge with toluene diisocyanate. Am J Physiol Lung
Cell Mol Physiol 292(1):L207-14.
Tarlo SM, Balmes J, Balkissoon R, Beach J, Beckett W, Bernstein D, Blanc PD, Brooks SM,
Cowl CT, Daroowalla F, Harber P, Lemiere C, Liss GM, Pacheco KA, Redlich CA, Rowe B,
Heitzer J. 2008. Diagnosis and management of work-related asthma: American college of chest
physicians consensus statement. Chest 134(3 Suppl):1S-41S.
Tarlo SM, Boulet LP, Cartier A, Cockcroft D, Cote J, Hargreave FE, Holness L, Liss G, Malo
JL, Chan-Yeung M. 1998. Canadian Thoracic Society guidelines for occupational asthma. Can
Respir J 5(4):289-300.
Tarlo SM, Malo JL, ATS/ERS. 2006. An ATS/ERS report: 100 key questions and needs in
occupational asthma. Eur Respir J 27(3):607-614.
Tinkle SS, Antonini JM, Rich BA, Roberts JR, Salmen R, DePree K, Adkins EJ. 2003. Skin as a
route of exposure and sensitization in chronic beryllium disease. Environ Health Perspect
111(9):1202-1208.
To T, Tarlo SM, McLimont S, Haines T, Holness DL, Lougheed MD, Liss GM, Cicutto L. 2011.
Feasibility of a provincial voluntary reporting system for work-related asthma in Ontario. Can
Respir J 18(5):275-277.
Toren K, Blanc PD. 2009. Asthma caused by occupational exposures is common - A systematic
analysis of estimates of the population-attributable fraction. BMC Pulm Med 9(1):7.
Toren K, Brisman J, Olin AC, Blanc PD. 2000. Asthma on the job: Work-related factors in new-
onset asthma and in exacerbations of pre-existing asthma. Respir Med 94(6):529-535.
Tsakirakis A, Kasiotis KM, Arapaki N, Charistou A, Tsatsakis A, Glass CR, Machera K. 2011.
Determination of operator exposure levels to insecticide during bait applications in olive trees:

140
Study of coverall performance and duration of application. International Journal of Hygiene &
Environmental Health 214(1):71-78.
Tupker RA, De Monchy JG, Coenraads PJ, Homan A, van der Meer JB. 1996. Induction of
atopic dermatitis by inhalation of house dust mite. J Allergy Clin Immunol 97(5):1064-1070.
Turner S, Carder M, van Tongeren M, McNamee R, Lines S, Hussey L, Bolton A, Beck MH,
Wilkinson M, Agius R. 2007. The incidence of occupational skin disease as reported to the
health and occupation reporting (THOR) network between 2002 and 2005. Br J Dermatol
157(4):713-722.
UK Health and Safety Executive,. 2001. Asthmagen? Critical assessment of the evidence for
agents implicated in occupational asthma. .
United States Department of Labor Bureau of Labor Statistics. 2011. International comparisons
of annual labor force statistics, adjusted to U.S. concepts, 10 countries, 1970-2010. .
Uter W, Nohle M, Randerath B, Schwanitz HJ. 2001. Occupational contact urticaria and late-
phase bronchial asthma caused by compositae pollen in a florist. Am J Contact Dermat
12(3):182-184.
Uter W, Ramsch C, Aberer W, Ayala F, Balato A, Beliauskiene A, Fortina AB, Bircher A,
Brasch J, Chowdhury MM, Coenraads PJ, Schuttelaar ML, Cooper S, Corradin MT, Elsner P,
English JS, Fartasch M, Mahler V, Frosch PJ, Fuchs T, Gawkrodger DJ, Gimenez-Arnau AM,
Green CM, Horne HL, Jolanki R, King CM, Krecisz B, Kiec-Swierczynska M, Ormerod AD,
Orton DI, Peserico A, Rantanen T, Rustemeyer T, Sansom JE, Simon D, Statham BN, Wilkinson
M, Schnuch A. 2009. The European baseline series in 10 European countries, 2005/2006--
Results of the European Surveillance System on Contact Allergies (ESSCA). Contact Derm
61(1):31-38.
Valdivieso R, Subiza J, Varela-Losada S, Subiza JL, Narganes MJ, Martinez-Cocera C, Cabrera
M. 1994. Bronchial asthma, rhinoconjunctivitis, and contact dermatitis caused by onion. J
Allergy Clin Immunol 94(5):928-930.

141
Valks R, Conde-Salazar L, Barrantes OL. 2003. Occupational allergic contact urticaria and
asthma from diphenylmethane-4,4'-diisocyanate. Contact Dermatitis 49(3):166-167.
van der Lende R, Orie NG. 1972. The MRC-ECCS questionnaire on respiratory symptoms (use
in epidemiology). Scand J Respir Dis 53(4):218-226.
van Kampen V, Merget R, Baur X. 2000. Occupational airway sensitizers: An overview on the
respective literature. Am J Ind Med 38(2):164-218.
Van Nimmen NF, Poels KL, Veulemans HA. 2006. Identification of exposure pathways for
opioid narcotic analgesics in pharmaceutical production workers. Ann Occup Hyg 50(7):665-
677.
van Triel JJ, Arts JH, Muijser H, Kuper CF. 2010. Allergic inflammation in the upper respiratory
tract of the rat upon repeated inhalation exposure to the contact allergen dinitrochlorobenzene
(DNCB). Toxicology 269(1):73-80.
Vandenplas O, Ghezzo H, Munoz X, Moscato G, Perfetti L, Lemiere C, Labrecque M,
L'Archeveque J, Malo JL. 2005. What are the questionnaire items most useful in identifying
subjects with occupational asthma? Eur Respir J 26(6):1056-1063.
Vandenplas O, Hereng MP, Heymans J, Huaux F, Lilet-Leclercq C, Dezfoulian B, Grand JL,
Thimpont J. 2008. Respiratory and skin hypersensitivity reactions caused by a peptide coupling
reagent. Occup Environ Med 65(10):715-716.
Vanoirbeek JA, Tarkowski M, Ceuppens JL, Verbeken EK, Nemery B, Hoet PH. 2004.
Respiratory response to toluene diisocyanate depends on prior frequency and concentration of
dermal sensitization in mice. Toxicol Sci 80(2):310-321.
Vanoirbeek JA, Tarkowski M, Vanhooren HM, De Vooght V, Nemery B, Hoet PH. 2006.
Validation of a mouse model of chemical-induced asthma using trimellitic anhydride, a
respiratory sensitizer, and dinitrochlorobenzene, a dermal sensitizer. J Allergy Clin Immunol
117(5):1090-1097.

142
Van-Wendel-de-Joode B, Brouwer DH, Vermeulen R, Van Hemmen JJ, Heederik D, Kromhout
H. 2003. DREAM: A method for semi-quantitative dermal exposure assessment. Ann Occup
Hyg 47(1):71-87.
Vermeulen R, Bos RP, Pertijs J, Kromhout H. 2003. Exposure related mutagens in urine of
rubber workers associated with inhalable particulate and dermal exposure. Occup Environ Med
60(2):97-103.
Vermeulen R, Kromhout H, Bruynzeel DP, de Boer EM. 2000. Ascertainment of hand dermatitis
using a symptom-based questionnaire; applicability in an industrial population. Contact
Dermatitis 42(4):202-206.
Warshaw EM, Schram SE, Maibach HI, Belsito DV, Marks JG,Jr, Fowler JF,Jr, Rietschel RL,
Taylor JS, Mathias CG, DeLeo VA, Zug KA, Sasseville D, Storrs FJ, Pratt MD. 2008.
Occupation-related contact dermatitis in North American health care workers referred for patch
testing: Cross-sectional data, 1998 to 2004. Dermatitis 19(5):261-274.
Wisnewski AV. 2007. Developments in laboratory diagnostics for isocyanate asthma. Current
Opinion in Allergy and Clinical Immunology 7(2):138-145.
Woolhiser MR, Munson AE, Meade BJ. 2000. Immunological responses of mice following
administration of natural rubber latex proteins by different routes of exposure. Toxicol Sci
55(2):343-351.
Woolhiser MR, Munson AE, Meade BJ. 1999. Role of sensitization routes in the development of
type I hypersensitivity to natural rubber latex in mice. Am J Ind Med Suppl 1:139-141.
Zhang XD, Fedan JS, Lewis DM, Siegel PD. 2004. Asthma-like biphasic airway responses in
brown Norway rats sensitized by dermal exposure to dry trimellitic anhydride powder. J Allergy
Clin Immunol 113(2):320-326.
Zhang XD, Hubbs AF, Siegel PD. 2009. Changes in asthma-like responses after extended
removal from exposure to trimellitic anhydride in the brown Norway rat model. Clin Exp
Allergy 39(11):1746-1753.

143
Zug KA, Warshaw EM, Fowler JF,Jr, Maibach HI, Belsito DL, Pratt MD, Sasseville D, Storrs
FJ, Taylor JS, Mathias CG, Deleo VA, Rietschel RL. 2009. Patch-test results of the North
American Contact Dermatitis Group 2005-2006. Dermatitis 20(3):149-160.

144
Appendices

145
Appendix 1: Supplemental Figures for Chapter 5 “Skin Symptoms in Bakery and Auto
Body Shop Workers: Associations with Exposure and Respiratory Symptoms”

146
Figure 7 Auto Body Shop Workers Associations Between Average Isocyanate Exposure
and Respiratory Symptoms, Shown In Smoothed Plots Stratified by Atopy. Data rugs
indicate the distribution of observations by exposure level. (a) Asthma-like symptoms in
atopic subjects (linear: NS; spline: NS), (b) Work-related chest tightness in atopic subjects
(linear: NS; spline: df=3, p<0.05), (c) Asthma-like symptoms in non-atopic subjects (linear:
p<0.05; spline: NS), (d) Work-related chest tightness in non-atopic subjects (linear: p<0.05;
spline: df=3, p<0.05).
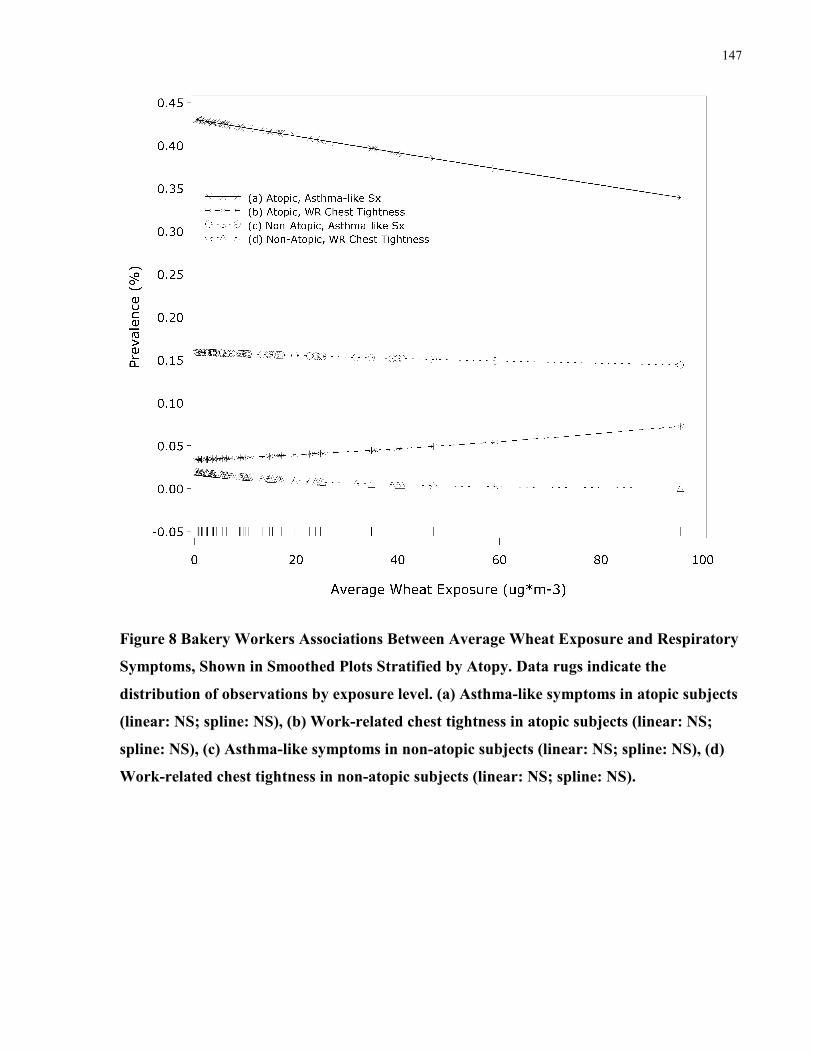
147
Figure 8 Bakery Workers Associations Between Average Wheat Exposure and Respiratory
Symptoms, Shown in Smoothed Plots Stratified by Atopy. Data rugs indicate the
distribution of observations by exposure level. (a) Asthma-like symptoms in atopic subjects
(linear: NS; spline: NS), (b) Work-related chest tightness in atopic subjects (linear: NS;
spline: NS), (c) Asthma-like symptoms in non-atopic subjects (linear: NS; spline: NS), (d)
Work-related chest tightness in non-atopic subjects (linear: NS; spline: NS).

148
Table 23 Results of Generalized Linear Models Describing the Simple Relationship
Between Exposure, Respiratory Symptoms, Atopy and Specific IgE. Each Reported
Prevalence Ratio (PR) was Estimated From a Separate Model. Models Adjusted for Age
and Sex. Symptom Models Additionally Adjusted for Smoking. (WR=Work-related)
Independent Variable Dependant Variable PR (95% CI)
Auto Body Repair Workers (n=473):
Average Isocyanate Exposure Asthma-like Symptoms 1.12 (0.9-1.4)
(µg-NCO*m-3
) WR Chest Tightness 1.71 (0.8-3.5)
Atopy 0.83 (0.7-1.0)
HDI-Specific IgE 10.0 (1.6-72)
Atopy Asthma-like Symptoms 1.40 (1.1-1.9)
WR Chest Tightness 2.61 (1.1-6.3)
HDI-Specific IgE Asthma-like Symptoms 1.13 (0.4-3.0)
WR Chest Tightness 4.89 (1.3-18)
Bakery Workers (n=723):
Average Wheat Exposure (µg*m-3
) Asthma-like Symptoms 0.89 (0.7-1.1)
WR Chest Tightness 0.92 (0.4-1.9)
Atopy 0.91 (0.8-1.1)
Wheat-Specific IgE 1.12 (0.8-1.5)
Atopy Asthma-like Symptoms 2.67 (2.1-3.4)
WR Chest Tightness 4.11 (1.4-12)
Wheat -Specific IgE Asthma-like Symptoms 2.6 (2.0-3.4)
WR Chest Tightness 15.7 (5.5-45)

149
Appendix 2: Interviewer-Administered Questionnaire for Chapter 6 “Skin and Respiratory
Symptoms Among Workers with Suspected Work-Related Disease”

“Work-related skin and respiratory symptoms and disease”
Last updated 05/12/2009
Part 1. Demographic Information
1. Study ID __________
2. Name _____________________________________________________________ (first) (mi) (last)
3. Address __________________________________________________
__________________________________________________
4. City ____________________ 5. Province __________ 6. Postal Code _________________
7. Interviewer Initials __________
8. Interview Date _______________________ MM DD YY
9. Birth Date ____________________
10. Place of Birth ____________________
11. Sex Male
Female

151
*********TTThhhiiisss pppaaagggeee wwwaaasss iiinnnttteeennntttiiiooonnnaaallllllyyy llleeefffttt bbblllaaannnkkk *********

152
Part 2. Symptoms The following questions are about lung and skin symptoms as well as related conditions. If you are in
doubt whether the answer is yes or no, please answer no.
2.1 COUGH
Row # [01]
1. Do you usually have a cough? (count cough with first smoke
or first going out of doors. Exclude clearing throat.)
1.Yes ___ 0. No ___ [ ] 1
IF YES TO ‘1’, ask:
A. Do you usually cough as much as 4 times a day, 4 or more
days out of the week?
1. Yes ___ 0. No ___ [ ] 2
IF NO TO 'A', ask:
B. Do you usually cough at all on getting up or first thing in
the morning?
1.Yes ___ 0. No ___ [ ] 3
C. Do you usually cough at all during the rest of the day or
night?
1.Yes ___ 0. No ___ [ ] 4
IF YES TO ANY OF ABOVE, ask:
D. Do you usually cough like this most days for 3
consecutive months or more during the year?
1.Yes ___ 0. No ___ [ ] 5
E. For how many years have you had this cough? ______________
number of years
[ ] [ ]
6-7
F. Does the cough improve:
on days off?
on long holidays?
1.Yes ___
1.Yes ___
0. No ___
0. No ___
[ ] 8
[ ] 9
G. Is there anything or situation which makes your cough
worse?
Specify: _______________________________
1.Yes ___ 0. No ___ [ ] 10
[ ][ ]
11-12

153
2.2 PHLEGM
1. Do you usually bring up phlegm from your chest?
(count phlegm with first smoke or first going out of doors.
Count swallowed phlegm. Exclude phlegm from the nose.)
1.Yes ___ 0. No ___ [ ] 13
IF YES TO ‘1’, ask:
A. Do you usually bring up phlegm like this as much as
twice a day, 4 or more days out of the week?
1. Yes ___
0. No ___
[ ] 14
IF NO TO 'A', ask:
B. Do you usually bring up phlegm at all on getting up or
first thing in the morning?
1.Yes ___ 0. No ___ [ ] 15
C. Do you usually bring up phlegm at all during the rest of
the day or night?
1.Yes ___ 0. No ___ [ ] 16
IF YES TO ANY OF ABOVE, ask:
D. Do you usually bring up phlegm like this most days for 3
consecutive months or more during the year?
1.Yes ___ 0. No ___ [ ] 17
E. For how many years have you had trouble with phlegm?
______________
number of years
[ ][ ]
18-19
F. Does the phlegm improve:
on days off?
on long holidays?
1.Yes ___
1.Yes ___
0. No ___
0. No ___
[ ] 20
[ ] 21
G. Is there any thing or situation which makes you bring up
phlegm?
Specify: __________________________________
1.Yes ___ 0. No ___ [ ] 22
[ ][ ]
23-24

154
2.3 WHEEZING
1. Have you ever had wheezing or whistling in your chest? 1. Yes ___ 0. No ___ [ ] 25
IF YES TO ‘1’, ask:
Did you have wheezing or whistling in your chest when you we:
A. Younger than 2 years old? 1. Yes ___ 0. No ___ [ ] 26
B. 2 to 18 years old? 1. Yes ___ 0. No ___ [ ] 27
C. Older than 18 years old? 1. Yes ___ 0. No ___ [ ] 28
2. In the last 12 months, have you had wheezing or whistling in
your chest at any time?
1. Yes ___ 0. No ___ [ ] 29
IF YES TO ‘2’, ask:
A. In the last 12 months, how often have you had this wheezing or whistling?
1. Most Days or Nights ________
2. A few days or nights a week ________
3. A few days or nights a month ________
4. A few days or nights a year, or less ________
[ ] 30
B. In the last 12 months, have you had this wheezing or
whistling in the chest when you had a cold?
1. Yes ___ 0. No ___ [ ] 31
C. In the last 12 months, have you had this wheezing or
whistling in the chest apart from colds?
1. Yes ___ 0. No ___ [ ] 32
D. In the last 12 months have you had an attack of wheezing
or whistling in the chest that has made you feel short of
breath?
1. Yes ___ 0. No ___ [ ] 33
E. In the last 12 months, has this wheezing or whistling
improved:
On days off?
On long holidays?
1. Yes ___
1. Yes ___
0. No ___
0. No ___
[ ] 34
[ ] 35
F. Is there any thing or situation which makes the wheezing
worse?
Specify: __________________________________
1.Yes ___ 0. No ___ [ ] 36
[ ][ ]
37 - 38
G. When does the wheeze occur MOST frequently? (choose one)
1. at work ________ 2. on return home ________
3. during sleep ________ 4. no difference ________
5. upon waking up _______
[ ] 39

155
2.4 SHORTNESS OF BREATH
1. Do you get short of breath with exertion more easily than
others of your own age?
1. Yes ___ 0. No ___ [ ] 40
IF YES TO ‘1’, ask:
A. Are you troubled by shortness of breath when hurrying on
level ground or walking up a slight hill?
1. Yes ___ 0. No ___ [ ] 41
B. Do you have to walk slower than people of your age on
level ground because of shortness of breath?
1. Yes ___ 0. No ___ [ ] 42
C Do you ever have to stop for breath when walking at your
own pace on level ground?
1. Yes ___ 0. No ___ [ ] 43
D. Do you ever have to stop for breath after walking about
100 yards (or a few minutes) on level ground?
1. Yes ___ 0. No ___ [ ] 44
E. Is there any thing or situation which makes you short of
breath?
Specify: __________________________________
1. Yes ___ 0. No ___ [ ] 45
[ ] 46
F. Does it improve:
On days off?
On long holidays?
1. Yes ___
1. Yes ___
0. No ___
0. No ___
[ ] 47
[ ] 48
2.4 CHEST TIGHTNESS
1. Do you usually have any chest tightness 1.Yes ___ 0. No ___ [ ] 49
2. Do you get attacks of chest tightness 1.Yes ___ 0. No ___ [ ] 50
If YES to ‘1 or 2’ then ask:
A. How many years have you had the chest tightness? 1.Yes ___ 0. No ___ [ ] 51
B. Does the chest tightness improve:
on days off?
on long holidays?
1.Yes ___
1.Yes ___
0. No ___
0. No ___
[ ] 52
[ ] 53
C. Is there any thing or situation which makes the chest
tightness worse?
Specify: __________________________________
1.Yes ___ 0. No ___ [ ] 54
[ ][ ]
55-56
D. In the last 12 months, have you been awakened from
sleep by shortness of breath or a feeling of tightness in your
chest?
1.Yes ___ 0. No ___ [ ] 57

156
If ‘YES’ to ‘D’, ask:
E. In the last 12 months, how often have you been awakened by shortness of breath
or a feeling of tightness in your chest?
1. Most Days or Nights ________
2. A few days or nights a week ________
3. A few days or nights a month ________
4. A few days or nights a year, or less ________
5. Not Applicable ________
[ ] 58
F. Do you associate your chest tightness with:
Muscular pain or injury?
Heart problems?
Breathing problems?
1.Yes ___
1.Yes ___
1.Yes ___
0. No ___
0. No ___
0. No ___
[ ] 59
[ ] 60
[ ] 61
If you feel that this chest tightness is associated with heart troubles, you should contact your family
physician immediately.
2.5 OVERALL RESPIRATORY HEALTH
1. Which of the following statements best describes your breathing?
1. I rarely get trouble with my breathing _______ [ ] 62
2. I do get regular trouble with my breathing
but it always gets completely better _______
3. My breathing is never quite right _______
2.6 SKIN SYMPTOMS Row # [02]
1. Do you presently have a skin rash? 1. Yes ___ 0. No ___ [ ] 1
IF YES to ‘1’, ask:
A. How many years have you had this rash? ________ [ ] 2
B. Is the rash located: Generalized
Hands/Arms
Feet
Face
Arms
Legs
Truck
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
0. No ___
0. No ___
0. No ___
0. No ___
0. No ___
0. No ___
0. No ___
[ ] 3
[ ] 4
[ ] 5
[ ] 6
[ ] 7
[ ]8
[ ] 9
C. Has the rash caused you to miss work? 1. Yes ___ 0. No ___ [ ] 10
D. Have you consulted a doctor about the rash? 1. Yes ___ 0. No ___ [ ] 11

157
If YES to ‘D’ then ask:
Which type of doctor have
you seen?
Family doctor
Dermatologist
Other ____________
1. Yes ___
1. Yes ___
1. Yes ___
0. No ___
0. No ___
0. No ___
[ ] 12
[ ] 13
[ ] 14
What was the diagnosis?
________________________________________
[ ] 15
C. Is the rash better when you are on vacation? 1. Yes ___ 0. No ___ [ ] 16
D. Is the rash worse in the: Winter
Summer
No difference
1. Yes ___
1. Yes ___
1. Yes ___
0. No ___
0. No ___
0. No ___
[ ] 17
[ ] 18
[ ] 19
E. Is the rash worse at work? 1. Yes ___ 0. No ___ [ ] 20
If YES to ‘E’ then ask:
Do you associate this with any particular operation? 1. Yes ___ 0. No ___ [ ] 21
What operations? _______________________________________ [ ] 22
2. Have you previously had a skin rash? 1. Yes ___ 0. No ___ [ ] 23
IF YES to ‘1’, ask:
A. How many years have you had this rash? ________ [ ] 24
B. Is the rash located: Generalized
Hands/Arms
Feet
Face
Arms
Legs
Truck
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
0. No ___
0. No ___
0. No ___
0. No ___
0. No ___
0. No ___
0. No ___
[ ] 25
[ ] 26
[ ] 27
[ ] 28
[ ] 29
[ ] 30
[ ] 31
C. Has the rash caused you to miss work? 1. Yes ___ 0. No ___ [ ] 32
D. Have you consulted a doctor about the rash? 1. Yes ___ 0. No ___ [ ] 33
If YES to ‘D’ then ask:
Which type of doctor have
you seen?
Family doctor
Dermatologist
Other ____________
1. Yes ___
1. Yes ___
1. Yes ___
0. No ___
0. No ___
0. No ___
[ ] 34
[ ] 35
[ ] 36
What was the diagnosis?
________________________________________
[ ] 37

158
C. Is the rash better when you are on vacation? 1. Yes ___ 0. No ___ [ ] 38
D. Is the rash worse in the: Winter
Summer
No difference
1. Yes ___
1. Yes ___
1. Yes ___
0. No ___
0. No ___
0. No ___
[ ] 39
[ ] 40
[ ] 41
E. Is the rash worse at work? 1. Yes ___ 0. No ___ [ ] 42
If YES to ‘E’ then ask:
Do you associate this with any particular operation? 1. Yes ___ 0. No ___ [ ] 43
What operations? _______________________________________ [ ] 44
3. Do you get a rash from metal buttons, metal fasteners, metal
jewellery or other metal objects next to your skin?
1. Yes ___ 0. No ___ [ ] 45
4. Do you have dry skin? 1. Yes ___ 0. No ___ [ ] 46
5. Does your skin itch when you sweat? 1. Yes ___ 0. No ___ [ ] 47
6. Have you ever had a rash as a result of contact with any of the following:
Metals
Leather
Plants
Rubber
Adhesive
Cosmetics
Medicines
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
0. No ___
0. No ___
0. No ___
0. No ___
0. No ___
0. No ___
0. No ___
[ ] 48
[ ] 49
[ ] 50
[ ] 51
[ ] 52
[ ] 53
[ ] 54
7. Have you had any of the following skin symptoms during the past 12 months?
Redness 1. Yes ___ 0. No ___ [ ] 55
Dry skin with scaling/flaking 1. Yes ___ 0. No ___ [ ] 56
Fissures or crack 1. Yes ___ 0. No ___ [ ] 57
weeping or crusts 1. Yes ___ 0. No ___ [ ] 58
Tiny water blisters (vesicles) 1. Yes ___ 0. No ___ [ ] 59
Papules (red bumps) 1. Yes ___ 0. No ___ [ ] 60
Rapidly appearing itchy wheal/welts 1. Yes ___ 0. No ___ [ ] 61
Itching 1. Yes ___ 0. No ___ [ ] 62
Burning, prickling or stinging 1. Yes ___ 0. No ___ [ ] 63
Tenderness 1. Yes ___ 0. No ___ [ ] 64
Aching or pain 1. Yes ___ 0. No ___ [ ] 65
Something else: _____________________________ 1. Yes ___ 0. No ___ [ ] 66
No symptoms during the past 12 months 1. Yes ___ 0. No ___ [ ] 67

159
2.7 NASAL SYMPTOMS
Row # [03]
1. In the last 12 months, have you had a problem with sneezing,
runny or blocked nose when you did not have a cold or the flu?
1.Yes ___ 0. No ___ [ ] 1
IF YES TO '1', ask:
A. Was the problem with sneezing, runny, or blocked nose related to the time of year?
1. No, Present all year long (skip to question Next Section) _____
2. No, comes and goes but does not relate to time of
year (skip to question Next Section) _____
3. Yes, worse at certain times of year _____
[ ] 2
B. In which of the past 12 months did this nose problem occur? (Please check all
months in which this occurred.)
Jan Feb Mar Apr May Jun Jul Aug Sept Oct Nov Dec
___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___
3 4 5 6 7 8 9 10 11 12 13 14
C. Does this improve:
on days off?
on long holidays?
1.Yes ___
1.Yes ___
0. No ___
0. No ___
[ ] 15
[ ] 16
2.8 EYE SYMPTOMS
1. In the last 12 months, have you had watery, itchy, or burning
eyes when you did not have a cold or the flu?
1.Yes ___ 0. No ___ [ ] 17
IF YES TO '1', ask:
A. Were the watery, itchy, or burning eyes related to the time of year?
1. No, Present all year long (skip to question Next Section) _____
2. No, comes and goes but does not relate to time of
year (skip to question Next Section) _____
3. Yes, worse at certain times of year _____
[ ] 18
B. In which of the past 12 months did the watery, itchy, or burning eyes occur? (Please
check all months in which this occurred.)
Jan Feb Mar Apr May Jun Jul Aug Sept Oct Nov Dec
___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___
19 20 21 22 23 24 25 26 27 28 29 30
C. Does this improve:
on days off?
on long holidays?
1.Yes ___
1.Yes ___
0. No ___
0. No ___
[ ] 31
[ ] 32

160
2.9 GENERAL HEALTH QUESTIONS
1. When you are near animals (such as cats, dogs, or horses) or
near feathers (including pillows, quilts or comforters) or in a
dusty or moldy part of the house, do you ever:
A. start to cough?
B. start to wheeze?
C. start to feel short of breath?
D. get a feeling of tightness in your chest?
E. get a runny or stuffy nose or start to sneeze?
F. get itching or watering eyes?
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
0. No ___
0. No ___
0. No ___
0. No ___
0. No ___
0. No ___
[ ] 33
[ ] 34
[ ] 35
[ ] 36
[ ] 37
[ ] 38
2. When you are near trees, grass, or flowers, or when there is a
lot of pollen in the air, do you ever:
A. start to cough?
B. start to wheeze?
C. start to feel short of breath?
D. get a feeling of tightness in your chest?
E. get a runny or stuffy nose or start to sneeze?
F. get itching or watering eyes?
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
0. No ___
0. No ___
0. No ___
0. No ___
0. No ___
0. No ___
[ ] 39
[ ] 40
[ ] 41
[ ] 42
[ ] 43
[ ] 44
3. When you are at your current job, do you ever:
A. start to cough?
B. start to wheeze?
C. start to feel short of breath?
D. get a feeling of tightness in your chest?
E. get a runny or stuffy nose or start to sneeze?
F. get itching or watering eyes?
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
0. No ___
0. No ___
0. No ___
0. No ___
0. No ___
0. No ___
[ ] 45
[ ] 46
[ ] 47
[ ] 48
[ ] 49
[ ] 50
4. When you are near strong odors such as perfume or bleach or
near smoke, do you ever:
A. start to cough?
B. start to wheeze?
C. start to feel short of breath?
D. get a feeling of tightness in your chest?
1. Yes ___
1. Yes ___
1. Yes ___
1. Yes ___
0. No ___
0. No ___
0. No ___
0. No ___
[ ] 51
[ ] 52
[ ] 53
[ ] 54
5. What would you say your overall health, as compared to
others of your own age is?
1. Excellent ___
2. Very Good ___
3. Good ___
4. Fair ___
5. Poor ___
[ ] 55

161
2.10 GENERAL ALLERGY SYMPTOMS
1. Has a doctor ever diagnosed you with an allergy? 1. Yes ___ 0. No ___ [ ] 56
IF YES TO '1', ask:
A. What allergies have you been diagnosed with?
________________________________________________ Year: _______ [ ] 57 [ ] [ ] 58-59
________________________________________________ Year: _______ [ ] 60 [ ] [ ] 61-62
________________________________________________ Year: _______ [ ] 63 [ ] [ ] 64-65
________________________________________________ Year: _______ [ ] 66 [ ] [ ] 67-68
________________________________________________ Year: _______ [ ] 69 [ ] [ ] 70-71
________________________________________________ Year: _______ [ ] 72 [ ] [ ] 73-74
________________________________________________ Year: _______ [ ] 75 [ ] [ ] 76-77
2.11 HEALTH HISTORY QUESTIONS
1. Have you ever had attacks of Bronchitis? 1. Yes ___ 0. No ___ [ ] 78
IF YES TO '1', ask:
A. Was it confirmed by a doctor? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 79
B. At what age was your first attack? __________ 8. N/A ___ [ ] 80
2. Have you ever had Hay Fever? 1. Yes ___ 0. No ___ [ ] 81
IF YES TO '2', ask:
A. Was it confirmed by a doctor? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 82
B. At what age did it start? __________ 8. N/A ___ [ ] 83
3. Have you ever had Chronic Bronchitis? 1. Yes ___ 0. No ___ [ ] 84
IF YES TO '3', ask:
A. Was it confirmed by a doctor? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 85
B. At what age did it start? __________ 8. N/A ___ [ ] 86
4. Have you ever had Asthma? 1. Yes ___ 0. No ___ [ ] 87
IF YES TO '4', ask:
A. Was it confirmed by a doctor? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 88
B. At what age did it start? __________ 8. N/A ___ [ ] 89
C. If you no longer have it, at what age did it
stop?
__________ 8. N/A ___ [ ] 90

162
5. Have you ever had Eczema? 1. Yes ___ 0. No ___ [ ] 91
IF YES TO '5', ask:
A. Was it confirmed by a doctor? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 92
B. At what age did it start? __________ 8. N/A ___ [ ] 93
C. If you no longer have it, at what age did it
stop?
__________ 8. N/A ___ [ ] 94
6. Have you ever had Hives? 1. Yes ___ 0. No ___ [ ] 95
IF YES TO '6', ask:
A. Was it confirmed by a doctor? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 96
B. At what age did it start? __________ 8. N/A ___ [ ] 97
C. If you no longer have it, at what age did it
stop?
__________ 8. N/A ___ [ ] 98
7. Have you ever had Psoriasis? 1. Yes ___ 0. No ___ [ ] 99
IF YES TO '7', ask:
A. Was it confirmed by a doctor? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 100
B. At what age did it start? __________ 8. N/A ___ [ ] 101
C. If you no longer have it, at what age did it
stop?
__________ 8. N/A ___ [ ] 102

163
Part 3. Smoking History Row # [04]
1. Have you ever smoked cigarettes? (Yes, means more than 1
cigarette per day for 1 year)
1. Yes ___ 0. No ___ [ ] 1
IF YES TO '1', ask:
A. Do you now smoke cigarettes? (as of 1 month ago) 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 2
B. How old were you when you first started smoking? __________ 8. N/A ___ [ ] 3
C. If you have stopped smoking, at what age did you
stop?
__________ 8. N/A ___ [ ] 4
D. How many cigarettes do you smoke per day now? __________ 8. N/A ___ [ ] 5
E. On the average of the entire time you smoked, how
many cigarettes did you smoke per day?
__________ 8. N/A ___ [ ] 6
F. Do you, or did you, inhale the cigarette smoke? 1. Not at all
2. Slightly
3. Moderately
4. Deeply
8. N/A [ ] 7
2. Have you ever smoked a pipe regularly? (Yes, means more
than 12 oz tobacco in a lifetime)
1. Yes ___ 0. No ___ [ ] 8
IF YES TO '2', ask:
A. Do you now smoke a pipe? (as of 1 month ago) 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 9
B. How old were you when you first started smoking a
pipe regularly?
__________ 8. N/A ___ [ ] 10
C. If you have stopped smoking a pipe, at what age did
you stop?
__________ 8. N/A ___ [ ] 11
D. How much tobacco do you smoke per day now? __________ oz per
week (std pouch = 1.5
oz)
8. N/A ___ [ ] 12
E. On the average of the entire time you smoked a pipe,
how much tobacco did you smoke per week?
__________ oz per
week (std pouch = 1.5
oz)
8. N/A ___ [ ] 13
F. Do you, or did you, inhale the pipe smoke? 1. Not at all
2. Slightly
3. Moderately
4. Deeply
8. N/A [ ] 14

164
3. Have you ever smoked cigars regularly? (Yes, means more
than 1 cigar a week for 1 year)
1. Yes ___ 0. No ___ [ ] 15
IF YES TO '3', ask:
A. Do you now smoke cigars? (as of 1 month ago) 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 16
B. How old were you when you first started smoking
cigars regularly?
__________ 8. N/A ___ [ ] 17
C. If you have stopped smoking cigars, at what age did
you stop?
__________ 8. N/A ___ [ ] 18
D. How many cigars do you smoke per week now? __________ oz per
week (std pouch = 1.5
oz)
8. N/A ___ [ ] 19
E. On the average of the entire time you smoked cigars,
how many cigars did you smoke per week?
__________ oz per
week (std pouch = 1.5
oz)
8. N/A ___ [ ] 20
F. Do you, or did you, inhale the cigar smoke? 1. Not at all
2. Slightly
3. Moderately
4. Deeply
8. N/A [ ] 21

165
Part 4. Workplace Characteristics
4.1 EMPLOYMENT STATUS
Row # [05]
1. What is your current employment status? 1. Employed
2. Unemployed
3. Self employed/Private contractor
4. Student
5. Apprentice/Trainee
6. Maternity/Paternity leave
7. Other _________________
[ ] 1
2. How would you describe your current work
schedule?
1. Full time
2. Part time
3. Casual
4. Other: _____________________
5. N/A
[ ] 2
3. If you are not working, why are you not at work? 1. Temporarily stopped due to
health problem
2. Been laid off
3. Been terminated/fired
4. Retired
5. Quit Job
6. Returned to school
7. Maternity/Paternity leave
8. Other: _____________________
9. N/A
[ ] 3
4. Have you submitted a WSIB claim related to your doctors
appointment today?
1. Yes ___ 0. No ___ [ ] 4
If YES to ‘4’ then ask:
A. Has it been accepted? 1. Yes ___ 0. No ___ 2. Pending ___ 8. N/A ___ [ ] 5
If they are employed, then ask:
A. On average how many hours do you work each week? __________ 8. N/A ___ [ ] 6
B. On average how many hours of overtime do you work each
week?
__________ 8. N/A ___ [ ] 7
B. What is your job title? ________________________________________ 8. N/A ___ [ ] 8
C. In which industry? 1. Manufacturing
2. Construction
3. Transportation
4. Food & Beverage
5. Chemical
6. Electrical
7. Service
8. Government
9. Mining
10. Automotive
11. Health Care
12. Agricultural
13. Pulp & Paper
14. Forestry
15. Education
16. Primary Metals
17. Other
_________________
88. N/A
[ ] 9

166
4.2 GENERAL WORK ENVIRONMENT
A. How many employees are in the workplace? __________ 8. N/A ___ [ ] 10
B. Is your workplace unionized? 1. Yes ___ 0. No ___ 2. Don’t Know___ 8. N/A __ [ ] 11
C. Is there a Joint Health & Safety
Committee in your workplace?
1. Yes ___ 0. No ___ 2. Don’t Know___ 8. N/A __ [ ] 12
D. Are skin problems an issue in the workplace? 1. Yes ___ 0. No ___ 2. Don’t Know___ [ ] 13
E. Is there a skin protection program in the
workplace?
1. Yes ___ 0. No ___ 2. Don’t Know___ [ ] 14
F. Are there known skin allergens in the workplace? 1. Yes ___ 0. No ___ 2. Don’t Know___ [ ] 15
G. Are there known skin irritants in the workplace? 1. Yes ___ 0. No ___ 2. Don’t Know___ [ ] 16
H. Are breathing problems an issue in the
workplace?
1. Yes ___ 0. No ___ 2. Don’t Know___ [ ] 17
I. Is there a breathing protection program in the
workplace?
1. Yes ___ 0. No ___ 2. Don’t Know___ [ ] 18
J Are there known lung allergens in the workplace? 1. Yes ___ 0. No ___ 2. Don’t Know___ [ ] 19
K. Are there known lung irritants in the workplace? 1. Yes ___ 0. No ___ 2. Don’t Know___ [ ] 20
L. Is there a hearing conservation program in your
workplace (regular hearing testing)?
1. Yes ___ 0. No ___ 2. Don’t Know___ [ ] 21
M. Is your breathing tested (pulmonary function) in
the workplace?
1. Yes ___ 0. No ___ 2. Don’t Know___ [ ] 22
N. Are washing facilities readily available in the
workplace?
1. Yes ___ 0. No ___ 2. Don’t Know___ [ ] 23
O. Do you shower at work? 1. Yes ___ 0. No ___ 2. Don’t Know___ [ ] 24
P. Are there separate eating facilities in the
workplace?
1. Yes ___ 0. No ___ 2. Don’t Know___ [ ] 25
Q. Do you eat at your work station? 1. Yes ___ 0. No ___ 2. Don’t Know___ [ ] 26
R. Do you launder your work clothes at home? 1. Yes ___ 0. No ___ 2. Don’t Know___ [ ] 27
S. Are MSDSs available in the workplace? 1. Yes ___ 0. No ___ 2. Don’t Know___ [ ] 28
T. Are MSDSs accessible to workers when
required?
1. Yes ___ 0. No ___ 2. Don’t Know___ [ ] 29
U. Have you ever accessed an MSDS in the
workplace?
1. Yes ___ 0. No ___ 2. Don’t Recall___ [ ] 30
V. Have you ever given an MSDS from your
workplace to a health care professional?
1. Yes ___ 0. No ___ 2. Don’t Recall___ [ ] 31

167
4.3 PREVENTION ACTIVITIES
1. Please indicate whether you have received training on each type of Personal Protective Equipment, and
whether you use each in your current job.
2. How would you rate the overall effectiveness of ventilation in removing
contaminants from the workplace (1 = not at all effective; 5 = very
effective)?
_________ [ ] 46
3. How would you rate the overall state of housekeeping in the workplace?
1. Inadequate
2. Adequate
3. Excellent
[ ] 47
4. Are processes and equipment equipped with
local exhaust ventilation?
1. Yes ___ 0. No ___ 2. Don’t Know ___ [ ] 48
5. Do you wear a respirator at work? 1. Yes ___ 0. No ___ [ ] 49
If YES to ‘5’ then ask:
A. How often do you wear a respirator? 1. Rarely ___
2. Sometimes ___
3. Often ___
4. Always ___
8. N/A
[ ] 50
B. Were you trained on how to use and maintain your
respirator?
1. Yes ___ 0. No ___ 8. N/A ___ [ ] 51
C. Have you received fit testing for your respirator? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 52
D. Do you re-use the respirator? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 53
E. Is the respirator disposable? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 54
F. Do you share the respirator with others? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 55
G. Do you experience any of the following when wearing the respirator?
Hot and sweaty face 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 56
Work is difficult to complete with the respirator on 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 57
The respirator does not provide adequate protection 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 58
I forget to wear it 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 59
It irritates your skin 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 60
Other ___________________________________ 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 61
TYPE OF PROTECTION Training? Use?
A. Hand protection 1. Yes ___ 1. Yes ___ [ ] 32 [ ] 33
B. Hearing protection 1. Yes ___ 1. Yes ___ [ ] 34 [ ] 35
C. Respiratory protection 1. Yes ___ 1. Yes ___ [ ] 36 [ ] 37
D. Face protection (face shield, etc.) 1. Yes ___ 1. Yes ___ [ ] 38 [ ] 39
E. Eye protection (safety goggles, etc.) 1. Yes ___ 1. Yes ___ [ ] 40 [ ] 41
F. Foot protection 1. Yes ___ 1. Yes ___ [ ] 42 [ ] 43
G. Protective Clothing (gown, coveralls, tyvek etc.)
G. Other? ________________________________ 1. Yes ___ 1. Yes ___ [ ] 44 [ ] 45

168
H. Which kind of respirator do you most
commonly use:
1. Disposable (N95)
2. Powered Air Purifying Respirator (PAPR)
3. Negative pressure air-purifying respirator
(cartridges, canister)
4. Self-contained breathing apparatus (SCBA)
5. Air-line respirator
6. Combination air-line/air purifying
7. Don’t know
8. N/A
[ ] 62
If NO to ‘5’ then ask:
6. Why do you not wear a respirator at work? 1. They are not provided
2. They are unsuitable for the work
3. They are not needed for the job
4. They irritate your skin
5. They are uncomfortable to wear
6. Other _________________
7. N/A
[ ] 63
7. Do you wear gloves at work? 1. Yes ___ 0. No ___ [ ] 64
If YES to ‘7’ then ask:
A. How often do you wear gloves? 1. Rarely ___
2. Sometimes ___
3. Often ___
4. Always ___
8. N/A
[ ] 65
B. Were you trained on how to use the gloves? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 66
C. What type of gloves do you use? 1. Cloth
2. Rubber
3. Leather
4. Synthetic rubber
5. Plastic
6. Cotton Liners
7. Combination of
materials
8. Don’t Know
7. N/A
[ ] 67
D. Do you use disposable gloves? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 68
E. If they are disposable, are they powdered? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 69
F. Are the gloves the correct size? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 70
G. Are the gloves suitable for the work task? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 71
H. Is there an adequate supply of gloves in the workplace? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 72
I. Do you supply your own gloves? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 73
J. Do you take off your gloves for breaks or lunch? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 74
K. Do you obtain a clean pair of gloves at the start of each
shift?
1. Yes ___ 0. No ___ 8. N/A ___ [ ] 75
L. If gloves are reusable, does the employer send them out
for cleaning?
1. Yes ___ 0. No ___ 8. N/A ___ [ ] 76
M. Do you wear cotton liners under your gloves? 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 77

169
N. Do you experience any of the following when wearing gloves?
Hot and sweaty hands 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 78
Work is difficult to complete with gloves on 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 79
The gloves do not provide adequate protection 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 80
You forget to wear them 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 81
They irritate your skin 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 82
Other ___________________________________ 1. Yes ___ 0. No ___ 8. N/A ___ [ ] 83
If NO to ‘7’ then ask:
8. Why do you not wear gloves at work? 1. They are not provided
2. They are unsuitable for the work
3. They are not needed for the job
4. They irritate your skin
5. They are uncomfortable to wear
6. Other _________________
7. N/A
[ ] 84
4.4 PREVENTION TRAINING
1. Has skin health education been provided in the
workplace, including how to identify the early
signs and symptoms of skin disease?
1. Yes ___ 0. No ___ 8. Don’t Recall
___
[ ] 85
If YES to ‘1’ then ask:
A. How was this information delivered? 1. Individual instruction
2. Information meeting
3. Posters/books/videos (multimedia)
4. Written guidelines
5. Other ______________________________
6. N/A
[ ] 86
2. Has education on skin exposure prevention
been provided in the workplace, including proper
use of personal protective equipment?
1. Yes ___ 0. No ___ 8. Don’t Recall
___
[ ] 87
If YES to ‘2’ then ask:
A. How was this information delivered? 1. Individual instruction
2. Information meeting
3. Posters/books/videos (multimedia)
4. Written guidelines
5. Other ______________________________
6. N/A
[ ] 88

170
3. Has lung health education been provided in the
workplace, including how to identify the early
signs and symptoms of lung disease?
1. Yes ___ 0. No ___ 8. Don’t Recall
___
[ ] 89
If YES to ‘3’ then ask:
A. How was this information delivered? 1. Individual instruction
2. Information meeting
3. Posters/books/videos (multimedia)
4. Written guidelines
5. Other ______________________________
6. N/A
[ ] 90
4. Has education on breathing exposure
prevention been provided in the workplace,
including proper use of personal protective
equipment?
1. Yes ___ 0. No ___ 8. Don’t Recall
___
[ ] 91
If YES to ‘4’ then ask:
A. How was this information delivered? 1. Individual instruction
2. Information meeting
3. Posters/books/videos (multimedia)
4. Written guidelines
5. Other ______________________________
6. N/A
[ ] 92

171
4.5 OCCUPATIONAL EXPOSURES
1. Thinking about the job that you think caused the problems that you are being seen for, are you exposed
to any of the following materials at work? If yes, how often?
Row # [06]
Exposure
(0)
Never
(1)
Rarely
(2)
Some Days
(3)
Most Days
animal dander (farm, lab, shellfish,
lanolin)
[ ] 1
beauty care products [ ] 2
bleaching agents [ ] 3
bodily fluids (blood, etc.) [ ] 4
cement or concrete [ ] 5
corrosives (acids/alkalis) [ ] 6
detergent and soaps [ ] 7
disinfectants [ ] 8
dusts (wood, rock, manufacturing) [ ] 9
dyes/pigments [ ] 10
foods/flavours/spices [ ] 11
fumes (eg., welding, plastic fume) [ ] 12
glues/adhesives/sealants/fillers/resins [ ] 13
isocyanates [ ] 14
mechanical irritation (contact with
sharp particles, heavy use of hands)
[ ] 15
metals (sheeting, parts, elemental) [ ] 16
oils and coolants (incl. metalworking) [ ] 17
oils, greases and lubricants [ ] 18
paint/varnish/degreasers [ ] 19
pesticides/herbicides/fungicides [ ] 20
pharmaceuticals [ ] 21
photographic chemicals [ ] 22
plastics, resins, epoxies [ ] 23
preservatives (eg., glutaraldehyde,
formaldehyde)
[ ] 24
printing inks [ ] 25
rubber compounds [ ] 26
second-hand smoke [ ] 27
silica [ ] 28
solvents (degreasers, thinners, etc) [ ] 29
textiles [ ] 30
wet work [ ] 31
asbestos [ ] 32

172
2. Thinking about all the jobs you have held, have you EVER been exposed to any of the following materials at work?
Exposure (0) No (1) Yes
animal dander (farm, lab, shellfish,
lanolin)
[ ] 33
beauty care products [ ] 34
bleaching agents [ ] 35
bodily fluids (blood, etc.) [ ] 36
cement or concrete [ ] 37
corrosives (acids/alkalis) [ ] 38
detergent and soaps [ ] 39
disinfectants [ ] 40
dusts (wood, rock, manufacturing) [ ] 41
dyes/pigments [ ] 42
foods/flavours/spices [ ] 43
fumes (eg., welding, plastic fume) [ ] 44
glues/adhesives/sealants/fillers/resins [ ] 45
isocyanates [ ] 46
mechanical irritation (contact with sharp
particles, heavy use of hands)
[ ] 47
metals (sheeting, parts, elemental) [ ] 48
oils and coolants (incl. metalworking) [ ] 49
oils, greases and lubricants [ ] 50
paint/varnish/degreasers [ ] 51
pesticides/herbicides/fungicides [ ] 52
pharmaceuticals [ ] 53
photographic chemicals [ ] 54
plastics, resins, epoxies [ ] 55
preservatives (eg., glutaraldehyde,
formaldehyde)
[ ] 56
printing inks [ ] 57
rubber compounds [ ] 58
second-hand smoke [ ] 59
silica [ ] 60
solvents (degreasers, thinners, etc) [ ] 61
textiles [ ] 62
wet work [ ] 63
asbestos [ ] 64

173
Appendix 3: Supplemental Tables for Chapter 6 “Skin and Respiratory Symptoms Among
Workers with Suspected Work-Related Disease”

174
Table 24 Comparison Between Participants and Patients Who Refused Study Participation.
All Frequencies Reported as n (%).
Total Refused Participant p-value
Overall 262 44 218
Female 117 (45%) 16 (36%) 101 (46%) 0.2251
Age <35 years 49 (19%) 6 (14%) 43 (20%)
Age 35-49 years 118 (45%) 24 (54%) 94 (43%)
Age ≥50 years 95 (36%) 14 (32%) 81 (37%)
0.3544
Doctor A 44 (17%) 6 (14%) 38 (17%)
Doctor B 67 (26%) 9 (20%) 58 (27%)
Doctor C 26 (10%) 9 (20%) 17 (8%)
Doctor D 32 (12%) 10 (23%) 22 (20%)
Doctor E 88 (34%) 10 (23%) 78 (36%)
Doctor F 5 (2%) 0 (0%) 5 (2%)
0.0132
Dermatology 205 (78%) 26 (59%) 179 (82%)
Asthma/Allergy 57 (22%) 18 (41%) 39 (18%)
0.0007
OHIP 140 (53%) 18 (41%) 122 (56%)
ODSP 122 (47%) 26 (59%) 96 (44%)
0.0678

175
Table 25 Comparison Between Dermatology (Derm) Stream and Asthma/Allergy (AA)
Stream Subjects. All Frequencies Reported as n (%).
Total Derm AA p-value
Overall 218 179 39
Interviewer 1 96 (44%) 81 (45%) 15 (38%)
Interviewer 2 122 (56%) 98 (55%) 24 (62%)
0.4389
In Clinic 212 (98%) 174 (98%) 38 (97%)
Telephone 5 (2%) 4 (2%) 1 (3%)
0.9049
Male 117 (54%) 97 (54%) 20 (51%)
Female 101 (46%) 82 (46%) 19 (49%)
0.7414
Age <35 years 43 (2%) 39 (22%) 4 (10%)
Age 35-49 years 94 (43%) 75 (42%) 19 (49%)
Age ≥50 years 81 (37%) 65 (36%) 16 (41%)
0.2598
Doctor A 38 (17%) 38 (21%) 0 (0%)
Doctor B 58 (27%) 58 (32%) 0 (0%)
Doctor C 17 (8%) 0 (0%) 17 (44%)
Doctor D 22 (11%) 0 (0%) 22 (56%)
Doctor E 78 (36%) 78 (44%) 0 (0%)
Doctor F 5 (2%) 5 (3%) 0 (0%)
<.0001
Never Smoker 106 (49%) 89 (50%) 17 (44%)
Former Smoker 54 (25%) 41 (23%) 13 (33%)
Current Smoker 58 (27%) 49 (27%) 9 (23%)
0.3915
OHIP 122 (56%) 116 (65%) 6 (15%)
ODSP 96 (44%) 63 (35%) 33 (85%)
<.0001
No Cross Referral 207 (95%) 176 (98%) 31 (79%)
Cross Referral Made 11 (5%) 3 (2%) 8 (21%)
<.0001

176
Table 26 Comparison Between Public Insurance Subjects (OHIP) and Workplace
Insurance Subjects (ODSP). All Frequencies Reported as n (%).
Total OHIP ODSP p-value
Overall 218 122 96
Interviewer 1 96 (44%) 50 (41%) 46 (48%)
Interviewer 2 122 (56%) 72 (59%) 50 (52%)
0.3060
In Clinic 212 (98%) 117 (96%) 95 (99%)
Telephone 5 (2%) 4 (3%) 1 (1%)
0.2696
Male 117 (54%) 60 (49%) 57 (59%)
Female 101 (46%) 62 (51%) 39 (41%)
0.1340
Age <35 years 43 (20%) 28 (23%) 15 (16%)
Age 35-49 years 94 (43%) 53 (43%) 41 (43%)
Age ≥50 years 81 (37%) 41 (34%) 40 (42%)
0.3000
Doctor A 38 (17%) 11 (9%) 27 (28%)
Doctor B 58 (27%) 24 (20%) 34 (35%)
Doctor C 17 (8%) 0 (0%) 17 (18%)
Doctor D 22 (11%) 6 (5%) 16 (17%)
Doctor E 78 (36%) 76 (62%) 2 (2%)
Doctor F 5 (2%) 5 (4%) 0 (0%)
<.0001
Never Smoker 106 (49%) 64 (52%) 42 (44%)
Former Smoker 54 (25%) 29 (24%) 25 (26%)
Current Smoker 58 (27%) 29 (24%) 29 (30%)
0.4093
Dermatology 179 (82%) 116 (95%) 63 (66%)
Asthma/Allergy 39 (18%) 6 (5%) 33 (34%)
<.0001
No Cross Referral 207 (95%) 119 (98%) 88 (92%)
Cross Referral Made 11 (5%) 3 (2%) 8 (8%)
0.0492

177
Table 27 Comparison Between Participants and Non-Participants in the Reliability Testing
Study. All Frequencies Reported as n (%).
Total No
Reliability
Reliability p-value
Overall 218 199 19
Interviewer 1 96 (44%) 94 (47%) 2 (11%)
Interviewer 2 122 (56%) 106 (53%) 16 (89%)
0.0033
In Clinic 212 (98%) 194 (97%) 18 (100%)
Telephone 5 (2%) 5 (3%) 0 (0%)
0.4963
Male 117 (54%) 108 (54%) 9 (50%)
Female 101 (46%) 92 (46%) 9 (50%)
0.7444
Age <35 years 43 (20%) 42 (21%) 1 (6%)
Age 35-49 years 94 (43%) 87 (43%) 7 (39%)
Age ≥50 years 81 (37%) 71 (35%) 10 (55%)
0.1447
Doctor A 38 (17%) 35 (18%) 3 (17%)
Doctor B 58 (27%) 51 (26%) 7 (39%)
Doctor C 17 (8%) 16 (8%) 1 (5%)
Doctor D 22 (11%) 21 (11%) 1 (5%)
Doctor E 78 (36%) 72 (36%) 6 (33%)
Doctor F 5 (2%) 5 (3%) 0 (0%)
0.8311
Never Smoker 106 (49%) 100 (50%) 6 (33%)
Former Smoker 54 (25%) 49 (24%) 5 (28%)
Current Smoker 58 (27%) 51 (26%) 7 (39%)
0.3451
Dermatology 179 (82%) 163 (81%) 16 (89%)
Asthma/Allergy 39 (18%) 37 (19%) 2 (11%)
0.4334
OHIP 122 (56%) 113 (56%) 9 (50%)
ODSP 96 (44%) 87 (44%) 9 (50%)
0.5947
No Cross Referral 207 (95%) 190 (95%) 17 (94%)
Cross Referral Made 11 (5%) 10 (5%) 1 (6%)
0.9179

178
Table 28 Test-Retest Reliability Statistics for Workplace Characteristics Questionnaire
Kappa
% Observed
Agreement
% Positive
Agreement
% Negative
Agreement
Union 1.00 100% 100% 100%
Breathing Protection Program 0.79 89% 91% 88%
Education on Skin PPE 0.69 84% 84% 84%
Education on Respiratory PPE 0.67 84% 87% 80%
Gloves Worn at Work 0.64 95% 97% 67%
Skin Protection Program 0.58 79% 78% 80%
Education on Respiratory Disease 0.48 84% 57% 90%
Respirator Worn at Work 0.48 74% 74% 74%
Skin Problems in the Workplace 0.46 74% 78% 67%
MSDS available at work 0.46 89% 94% 50%
Joint Health and Safety Committee 0.44 89% 94% 50%
Education on Skin Disease 0.44 89% 50% 94%
Lung Allergens in the Workplace 0.37 68% 70% 67%
Skin Allergens in the Workplace 0.36 68% 73% 63%
Breathing Problems in the Workplace 0.36 68% 63% 73%
Lung Irritants in the Workplace 0.27 74% 83% 44%
Skin Irritants in the Workplace 0.11 63% 74% 36%

179
Table 29 Test-Retest Reliability Statistics for Workplace Exposure Questionnaire Items.
Variable Kappa
% Observed
Agreement
% Positive
Agreement
% Negative
Agreement
Dusts 0.88 95% 96% 92%
Body Care Products 0.78 89% 88% 91%
Silica 0.78 89% 88% 91%
Pesticides 0.77 95% 80% 97%
Solvents 0.69 84% 82% 86%
Printing Inks 0.68 89% 75% 93%
Corrosives 0.68 84% 82% 86%
Paints 0.68 84% 82% 86%
Food, Flavors or Spices 0.62 84% 73% 89%
Glues, adhesives, sealants 0.62 84% 89% 73%
Oils, greases, Lubricants 0.58 79% 80% 78%
Wet Work 0.52 79% 85% 67%
Disinfectants 0.51 79% 85% 67%
Fumes 0.49 74% 78% 67%
Oils and Coolants 0.47 74% 71% 76%
Textiles 0.46 79% 60% 86%
Bodily Fluids 0.44 89% 50% 94%
Mechanical Irritation 0.41 79% 87% 50%
Pharmaceuticals 0.41 79% 50% 87%
Plastics 0.37 68% 70% 67%
Cement 0.36 74% 55% 81%
Photographic Chemicals 0.31 84% 40% 91%
Asbestos 0.31 84% 40% 91%
Preservatives 0.28 68% 50% 77%
Bleaching Agents 0.18 63% 46% 72%
Dyes/Pigments 0.16 58% 56% 60%
Environmental Tobacco Smoke 0.14 58% 64% 50%
Dander 0.13 74% 29% 84%
Metals 0.10 53% 47% 57%
Detergents 0.05 68% 80% 25%
Rubber Compounds 0.03 53% 40% 61%
Isocyanates -0.06 89% 0% 94%

180
Table 30 Multiple Logistic Regression Model Results for Predictors of Reporting Work-
Related Concurrent Skin and Respiratory Symptom Outcomes. Models Adjusted for Age,
Sex, and Interviewer.
Model Description
Predictor↓
Both Work-Related Skin and
Work-Related Respiratory
Symptoms
Work-Related Respiratory
Symptoms Only vs. Work-
Related Skin Symptoms Only
Never Smoker 1.00 1.00
Former Smoker 0.74 (0.26-2.06) 1.46 (0.49-4.37)
Current Smoker 0.97 (0.38-2.49) 0.65 (0.23-1.83)
Atopy 1.00 (0.44-2.24) 2.37 (0.98-5.72)
Doctor-diagnosed Eczema 2.93 (1.33-6.44) 0.31 (0.10-0.94)
< 20 Employees 0.94 (0.31-2.85) 0.29 (0.09-1.02)
20-99 Employees 1.00 1.00
100-499 Employees 0.69 (0.22-2.14) 1.02 (0.33-3.12)
>499 Employees 3.25 (1.13-9.28) 1.92 (0.504-6.83)
Education: PPE - 0.26 (0.11-0.64)
# Outcomes 40 43
Model n 204 132

181
Copyright Acknowledgements
1. Permission from John Wiley and Sons to use Figure 1. Relationships of asthma to the
workplace, from “Diagnosis and Management of Work-Related Asthma: American
College of Chest Physicians Consensus Statement” published in Chest (Chest September
2008 134:3 suppl 1S-41S) by Susan M. Tarlo, John Balmes, Ronald Balkissoon, Jeremy
Beach, William Beckett, David Bernstein, Paul D. Blanc, Stuart M. Brooks, Clayton T.
Cowl, Feroza Daroowalla, Philip Harber, Catherine Lemiere, Gary M. Liss, Karin A.
Pacheco, Carrie A. Redlich, Brian Rowe, and Julia Heitzer. This copyright permission
pertains to Figure 1 in this thesis.
2. Permission from John Wiley and Sons to use the entire article “Occupational contact
allergens: Are they also associated with occupational asthma?” published in the
American Journal of Industrial Medicine by V.H. Arrandale, G.M. Liss, S.M. Tarlo,
M.D. Pratt, D. Sasseville, I. Kudla, and D.L. Holness. This copyright permission pertains
to all of Chapter 3 in this thesis.
3. Permission from Springer to use the entire article “Skin Symptoms in Bakery and Auto
Body Shop Workers: Associations with Exposure and Respiratory Symptoms” published
in the International Archives of Occupational and Environmental Health by V.H.
Arrandale, T. Meijster, A. Pronk, G. Doekes, C.A. Redlich, D.L. Holness, D. Heederik.
This copyright permission pertains to all of Chapter 5 in this thesis.