objectives 1.identify purpose of documentation. 2.identify legal issues of a patient care report....
TRANSCRIPT

Documentation
Skills
OBJECTIVES
1. Identify purpose of documentation.
2. Identify legal issues of a patient care report.
3. Identify special circumstances.
4. Explain types of patient care reports.
5. Discuss refusal of care reporting.
6. Discuss PCR record.
7. Explain errors and falsification.
8. Identify correction of errors.

Introduction• EMS documentation is important.
1. Only written record of the call
2. Legal record
3. Becomes part of the:Patient’s medical record
Emergency department chart
• Know:I. What shape a report.
II. Who might read the report.
III. When it must be completed.
IV. What terminology may be used.
Definition of Documentation
Documentation defined as : Recording patient findings,
following principles of medical documentation and report writing.
• For every call, the PCR should include:
A. Objective information.
B. Subjective information.
C. Details of patient care
Documentation

PURPOSE OF DOCUMENTATION
• The PCR is a record of:
1. The patient’s condition upon arrival.
2. The care provided.
3. Any changes in the patient’s condition.
Legal Issues of a Patient Care Report
• PCRs may be written or computerized.
• Reports should be:
A. Complete.
B. Well written.
C. Legible (clear)
D. Professional.
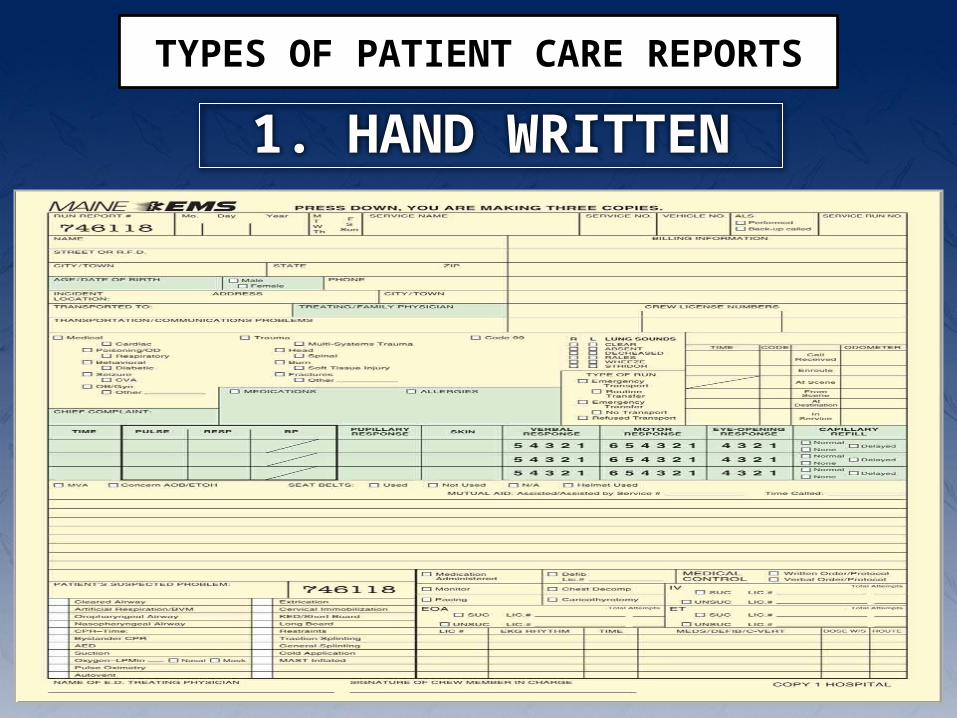
1. HAND WRITTEN
TYPES OF PATIENT CARE REPORTS

Elements of Written Report
Information should be comprehensive and concise.
Complete all sections, even if not applicable to call.
Handwritten reports should be:
1. Legible.
2. Written in ink
3. Neat and easy to read
4. Respect patient privacy.
5. Complete in a timely manner.
Types of Patient Care Reports
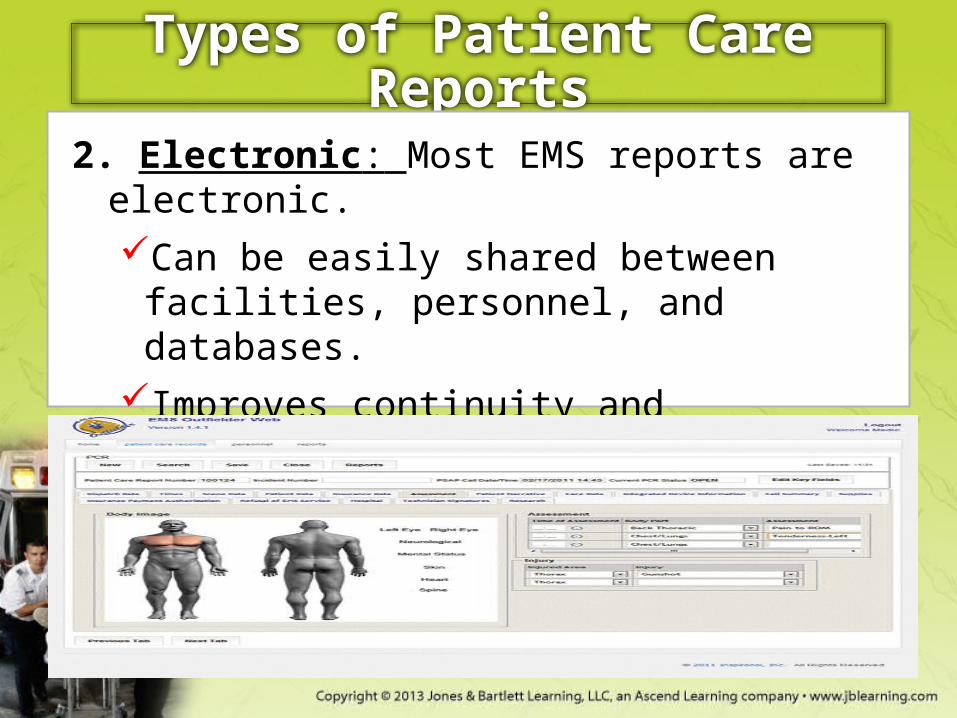
2. Electronic: Most EMS reports are electronic.
Can be easily shared between facilities, personnel, and databases.
Improves continuity and efficiency of care.
Advances evidence-based practice

Documentation for Every EMS Call
• Standard items documented on every call
1. Agency name.
2. Unit number.
3. Date.
4. Times.
5. Run or call number.
6. Crew members’ names, licensure levels, and numbers.
1. Run data

Patient data1. Patient’s name, address, date of birth, age, sex.
2. Billing and insurance inform.
3. Nature of call.
4. Location where patient was found.
5. Signs and symptoms.
6. Baseline vital signs.
7. Investigation
8. Care administered and the effect on the patient.
9. Changes in condition throughout the call.
10. History

Errors and Falsification
• Avoid errors.– If they occur, know how to address them.
• If a revision must be made:– Note the date and time of revision.– Include purpose for correction.– Never discard the original.
Only the person who wrote the report can revise it.
Routine reviews are necessary.
Follow protocol for making corrections.
The PCR is a legal document.
Correction of Errors
Use a different color of ink.
Draw a single horizontal line through the error.
Write the correct information beside it.
Do not obliterate the error.
Initial and date the correction.
Refusal of Care Reporting
adult patients have the right to refuse care.
Know and understand patient rights.
The patient should know:
His or her current situation
Consequences of refusal of care
Evaluate the patient’s mental status.

Refusal of Care Reporting
Information must be:Given in a language the patient
understandsDocumented on the PCRsigned by the patient
Unresponsive patients may be treated under implied consent.
Be familiar with individual state laws related to consent.

Refusal of Care Reporting
Remind patient he or she can call EMS later.
Two main types of refusals:
Person who is not seriously injured and does not
want to go to the hospital.
The patient refuses even though you feel he
needs it.
Patients may agree to some treatments and
refuse others.

THANK YOU