nutrition support for the critically ill infant - kintera.org1cb444df-77c3-4d94-82fa... · •can...
TRANSCRIPT

Nutrition Support for the
Critically Ill Infant
June Garrett Hatfield MS, RD, CNSC

Objectives
By the end of this lecture, you should be able to :
1. Understand impact of maternal/prenatal factors on
neonatal nutrition status
2. Explain three reasons why premature infants are at
increased nutritional risk
3. Expand knowledge and understanding of critical
illnesses and the impact to nutrition status
4. Name the three parameters used to assess growth for
infants

Outline
• Overall Goals of Nutrition Assessment and Support
• Nutrition Assessment Considerations
• Nutrition Support
• Nutrition Requirements – Parenteral
– Enteral
• Nutrition Implications of Prematurity, Common Critical Illnesses
• Growth, Nutrition Intervention Monitoring
3

Goals of Nutrition Support
• Ensure growth rates consistent with standards for
intrauterine growth or postnatal growth
• Protect lean body mass and function
• Provide adequate amounts of substrates including
vitamins, minerals and trace elements
• Marker of nutrition adequacy is GROWTH

Nutrition Support
Considerations in Nutrition Care Process:
– Prenatal and maternal factors/fetal nutrition
– Gestational age and weight
– Route of feeding: enteral or parenteral or both
– Baseline protein, energy, fluid, micronutrient needs
– Nutritional implications of prematurity and common critical illnesses
– Growth expectations and monitoring

Mother Placenta
Fetus
Fetal Nutrition
• Fetus depends on maternal supply of nutrients
through placenta into umbilical circulation
• Glucose, amino acids, fatty acids=most
important nutrients in fetal life
• Mom, placenta, fetus
each w/own metabolism
while interacting with
each other
6

Fetal Nutrition
• During rapid growth, cell differentiation,
both mother and fetus are very susceptible
to alterations in dietary supply
• Micronutrients are essential at every stage
in fetal growth & development
• Maternal concentration main determinant
for fetus glucose, AA, FA concentrations—but
placenta acts to determine composition of
fetal diet
7

Prenatal and Maternal
Considerations
• ISAM—Infant of substance abusing mother
• IDDM—Infant of diabetic mother
• Hypertension/preeclampsia
• Polyhydraminos
• Infections, illnesses
• Medications
• Trauma
8

Classification of Infants By Gestational Age
• Preterm: ≤36+6/7 wks
• Late Preterm: 34-36 6/7 wks
• Early/Near term: 37-38 6/7 wks
• Full Term: 39-40 6/7 wks
• Late Term: 41-41 6/7 wks
• Post Term: 42 wks and beyond
The American College of Obstetrics and Gynecologists 2013 Acog.org, Definition Of Term Pregnancy - ACOG '. N. p., 2015

Correcting for Prematurity
[Baby’s actual age in weeks] – [# of weeks
premature at birth, out of 40] = Baby’s CGA
Ex: pt is DOL 168, ex-24 week infant
[24] – [16] = 8 weeks CGA
Patients should be corrected for
prematurity until 2 years CGA
10

Classification of Infants By weight
• LBW <2500g
• VLBW <1500g
• ELBW <1000g
• SGA <10th %ile
• AGA >10th %ile & <90th %ile
• LGA >90th %ile

IUGR vs SGA
• IUGR: – Reduction from physiological fetal growth rate
– Generally prenatal, longitudinal measure based on multiple u/s
• SGA: – Refers to size of infant at birth, not fetal growth
– Associated w/maternal, fetal, placental factors
• Constitutionally small infants: – 70% of pt w/BW <10%ile
– Well proportioned, normal development
– Small 2/2 constitutional reasons
12

Impact of IUGR • Symmetrical IUGR <32 weeks
– Associated w/genetic or congenital problem/infection
– Proportional reduction in soft tissue growth (muscle, fat, organs), length, HC • Normal Ponderal Index, wt/length/HC all <10%
• Asymmetrical IUGR >32 weeks – Associated w/uteroplacental insufficiency
– Brain growth relatively spared in relation to weight, length of fetus
– Fetus often hypoxic, hypoglycemic, decreased subcutaneous fat, reduced abd circumference, disproportionately large head • Low Ponderal Index, normal length/HC, wt <10th%ile
13

Impact of IUGR/SGA
• Blood flow to muscle, liver, gut decreased
• Increased risk of hypoglycemia d/t decreased glycogen stores, decreased glucose production in liver from alanine/lactate via gluconeogenesis
• At risk for neonatal hypocalcemia d/t decreased transfer of Ca across placenta
• Decreased fat mass, may not oxidize FFAs, TG
• Decreased skeletal muscle—increased insulin receptors present but inactive signaling molecules
• In severe cases, potential for refeeding syndrome
14

Impact of LGA • Macrosomia—common in IDM (primarily GDM)
• Can also be r/t Beckwith-Wiedermann, hydrops fetalis, post-term, constitutionally large, ethnicity
• Maternal hyperglycemia=fetal hyperglycemia promotes fetal insulin production, secretion increased fat production from glucose, glycerol, FAs, TG
• Increased glycogen content of organs organomegaly
• Infants have high insulin levels that prevent glycogenolysis, gluconeogenesis, prevents FA release from adipose tissue – Hypoglycemia
15

Initiating Nutrition Support
• Use the gut if possible
• Promote the use of breastmilk and skin-to-skin contact
• Promote early postnatal nutrition: use combination of enteral and parenteral if necessary
• If unable to use the GI tract within 48-72hours, consider parenteral nutrition for protein delivery – Protein should be should be provided DOL 0 if
possible
16

Initiating Nutrition Support
• Specific to preemies:
– promote early enteral nutrition
– prevent catabolism with immediate protein
provision
– prevent development of nutrition-related
common diseases
• Additionally, specific to critically ill infant:
– Understand how the condition affects nutrition
delivery and prevent rather than treat growth
failure (whenever possible)

Fluid Management
Fluid Requirements (mL/kg/d) by Age
Birth Wt (g) 1-2 days 3-7 days 7-30 days
<750 100-250 150-300 120-180
750-1000 80-150 100-150 120-180
1000-1500 60-100 80-150 120-180
<1500 60-80 100-150 120-180
18
Harriet Lane; Data from Taesuch HW, Ballard RA 1998

Fluid Management
• Take into account all fluids—TPN, IL,
medications, PRNs, boluses, continuous
drips
– Dextrose as carrier fluid? Increased GIR?
– Concentrations of drugs
– Room to combine/condense?
• Typically do not count blood/plasma,
replacement fluids
19

Dextrose: Glucose Infusion
Rate (GIR) Start
mg/kg/min
Advancement
mg/kg/min
Goals
mg/kg/min
Infant: 5-7 1-2 10-12.5
LBW & VLBW: 5-7 1-2 11-13
ELBW: 5-7 0.5-1 12-13
Minimum: 5 mg/kg/min
Maximum: depends on protein and fat delivery; > 13 mg/kg/min or
>18gm/kg/d may lead to conversion of glucose to fat leading to
increased energy expenditure, increased O2 consumption and C02
production.

Energy Requirements
• Energy requirements are based on:
– basal metabolic rate
– temperature control
– excretion and digestion (use of GI tract)
– activity
– expected placental delivery

Energy Needs
• PN can support growth at lower energy intakes
because energy is not lost in absorption and
digestion
• PN needs during critical illness vary
– REE increases during recovery phase ; not
septic phase
– REE of septic newborns based on metabolic
capabilities.
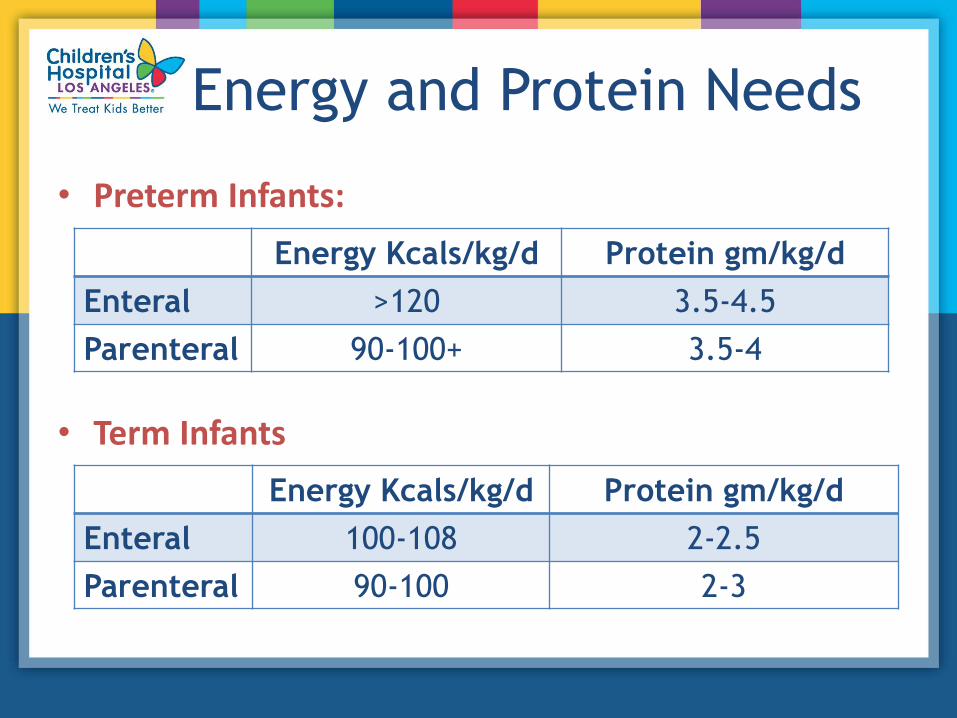
Energy and Protein Needs
• Preterm Infants:
• Term Infants
Energy Kcals/kg/d Protein gm/kg/d
Enteral >120 3.5-4.5
Parenteral 90-100+ 3.5-4
Energy Kcals/kg/d Protein gm/kg/d
Enteral 100-108 2-2.5
Parenteral 90-100 2-3

Protein Needs
• Protein delivery reduces protein breakdown and
helps to improve negative nitrogen balance
• In ELBW infants, amino acids serve as a significant
energy source beyond needs for protein accretion
– an elevated BUN may reflect acceptable metabolic
byproduct vs. protein intolerance
24

Fat (Intralipids)
Start Advancement Goal
Infant: 2.5-10 kg 1.0 g/kg 1.0 g/kg 2.0-3.0 g/kg
LBW, VLBW:
(1-2.499 kg) 1.0 g/kg 1.0 g/kg 3.0 g/kg
ELBW:(< 1 kg) 0.5 g/kg 0.5 g/kg 3.0 g/kg
Minimum: 0.5-1.0 g/kg/d of IL is necessary to prevent EFA deficiency
Infants w/ sepsis, liver disease or severely compromised oxygenation
may need lower IL rate d/t impaired lipid clearance

Parenteral Calcium and
Phosphorus Recommendations
Ca Infant: 2 mEq/kg
ELBW/LBW: 4 mEq/kg
P Infant: 1 mmol/kg
ELBW/LBW: 1.5-2 mmol/kg
Ca:P ratio Infant: 1.3:1
ELBW/LBW: 1.7:1*
*in face of hypophosphatemia, ok to give reduced
ratio to replete phos

Trace Elements
• Zinc:
– Increased needs with rapid growth, increased stool
and ostomy output, GI disease.
– Deficiency can lead to poor growth
• Standard trace elements include Mn, Se, Cu, Cr
• Involved in many enzymatic reactions as cofactors and
coenzymes

• Changes in metabolic demand and energy
expenditure
– Ventilation and sedation changes
– Impact of inflammatory process
– Post operative clinical status changes
– Transition from an isolette to an open crib
– Transition from feeding tube to oral feeds
• Understand the medical picture as it relates to
nutrition support
Changes in Metabolic
Demand

Parenteral Nutrition
• Parenteral nutrition is a medication
• Required to meet the nutrition needs of rapidly growing
premature infants…life saving therapy
• PN can support growth at lower energy intakes because
energy is not lost in absorption and digestion
• PN needs during critical illness vary
• Specific PN considerations in the NICU:
– Early/high protein
– Ca:Phos
– Carnitine
– Long term complications w/out close monitoring

Enteral Nutrition
How/Where do we start? 1. Trophic feeds
2. Gastric
3. Q3hr bolus
What do we start with? 1. Breastmilk
2. Donor breastmilk
- when appropriate, per institution
3. Formula
Goal: avoid over/underfeeding and maintain nutrition status while transitioning from PN to EN

Trophic Feeds
Trophics = gut priming, minimal enteral nutrition (MEN)
What: • 10-20ml/kg ml/kg for 5-7days
• Stimulating the enteric system
Why: • Structural, functional integrity of GI tract
depends on enteral nutrition
• Lack of enteral use leads to
intestinal mucosal atrophy and
flattening of the villi
• Affects absorption
31

Trophic Feeds
Benefits of Trophic Feeds: • Stimulation of GI hormonal response
• Improved maturation of GI motor patterns
• Earlier progression to enteral feeds
• Improved feeding tolerance
• Improved wt gain
• Fewer days on PN
32

Managing Enteral Nutrition
• Increase caloric density before reaching full volume
• Use modulars
– protein powder or other forms of liquid protein
– medium chained triglyceride oil or other liquid
forms of enteral fat
– premature and transitional infant formulas
– use high protein options
– liquid concentrates
• Incorporate breastmilk and donor breastmilk

Micronutrient
Supplementation Iron:
• Preterm infant iron needs higher: 2-4mg/kg
• Fe-fortified formula provides ~ 1.8-2.1 mg/kg/d of iron
• Formula-fed ex-preemies need additional 2 mg/kg
Vitamin D:
• ALL infants need at least 400 IU per day
• Vitamin D needs not met with current formula
• Breastmilk contains <6 IU/100cals of Vitamin D
• Give cholecalciferol (Vit D3) or infant multivitamin

Vitamin Dosing
35
Suggested Vitamin Supplementation for all Neonates:
Premature Infants Full Term Infants
Breastmilk 20cal/oz 1 mL/d Poly-vi-sol 1 mL/d Poly-vi-sol
Breastmilk + HMF 400 IU/d Vit D N/A
Breastmilk + Transitional Preterm Formula
1 mL/d Poly-vi-sol N/A
Breastmilk + Term Infant Formula 1 mL/d Poly-vi-sol 1 mL/d Poly-vi-sol
24cal/oz Premature Formula 400 IU/d Vit D N/A
Transitional Preterm Formula 400 IU/d Vit D N/A
Term Infant Formula 1 mL/d Poly-vi-sol 400 IU/d Vit D
Infants w/TPN Cholestasis (D. Bili >2) 1 mL/d AquaDEKs 1 mL/d AquaDEKs

Nutritional Implications
of Prematurity Nutritional Emergency:
Limited nutrient reserves
Increased nutritional demands
Common critical illnesses
Immature organ function
Nutritional Implications
of Prematurity Limited nutrient reserves: lack of 3rd trimester nutrient
accretion Low stores of glycogen, fat, protein, fat-soluble vitamins, Ca,
Ph, Mg, and trace elements
Higher risk for nutrient deficiencies
Increased nutritional demands:
rapid growth phase
tissue development
temperature control
Altered feeding abilities and patterns: suck/swallow/ breath mechanism develops after 32wks

Nutritional Implications
of Prematurity
Common Critical Illnesses:
• Some directly related to alteration or imbalance of
nutrition
• Some indirectly affect how or how much nutrition is
provided

Nutritional Implications: Common Critical Illnesses
• RDS: respiratory distress syndrome
– PO status; altered GI motility
• PDA: patent ductus arteriosis
– fluid restriction; Indocin use
• NEC: necrotizing enterocolitis
– requires bowel rest
– complications from bowel resection and longterm
parenteral nutrition

Nutritional Implications: Common Critical Illnesses
• CLD: chronic lung disease
– fluid restriction, steroids, diuretics; affects bone
growth and energy needs
• IVH: intraventricular hemorrhage
– impact on oral feeding skills or intakes
• Sepsis:
– can affect mesenteric blood flow; increases risk of
NEC; feeding issues with holding of feeds

Nutritional Implications: Common Critical Illnesses
Osteopenia of Prematurity:
– Decreased bone density
and mineralization
– Impairs linear growth
– Increases energy and
protein needs
– Impact on other systems

Nutritional Implications: Common Critical Illnesses
Direct hyperbilirubinemia from lack of gut use
and prolonged PN:
– Increases energy needs
– Higher incidence of feeding intolerance
– Altered fat-soluble vitamin absorption
– Altered fat absorption
– Impairs growth
– Can lead to trace element deficiencies/toxicities

Nutritional Implications: Common Critical Illnesses
Growth Failure/Extrauterine Growth
Restriction (EUGR):
– Lack of strength
– Reduced endurance
– Altered linear growth
– Increased risk of infection
– Prolonged hospitalization

• Feeding intolerance
• Frequent holding of feeds for tests or other
reasons
• Access limitations
• Volume restriction
• Metabolic complications
• Overshooting nutrition goals
Nutrition Support Barriers

Growth
• Fenton growth curves, updated 2013, male/female
• WHO growth curves
• Weight loss during the first week of life is expected and
acceptable
– Premature infants can lose up to 20% of birth weight
and should regain within 2 weeks
– Term infants can lose 7-10% of BW and should regain
within 7-10 days

Growth Parameters
CLASSIFICATION WEIGHT
GAIN
LENGTH
(cm/week)
HEAD CIRC.
(cm/week)
Preterm <2.0 kg 15-20
gm/kg/d 0.8-1.1 0.8-1
Preterm >2.0 kg 25-35
gm/d 0.8-1.1 0.8-1
Term 23-34
gm/d 0.8-0.93 0.38-0.48
General recommendations, not absolute
Who.int,(2015). WHO | Weight velocity. http://www.who.int/childgrowth/standards/w_velocity/en/

Impaired Growth Velocity
Premature and critically ill infants at increased risk for
suboptimal nutrition delivery and impaired growth d/t:
• Fluid restriction
• PN compounding limitations
• Feeding intolerance and feeding immaturity
• Holding of feeds for tests, residuals, sepsis, etc.
• Acidosis
• Prolonged electrolyte abnormalities

Monitoring Nutrition Status
48
- Growth =main indicator of adequate nutritional status - Follow growth trends, not just numbers - Postnatal nutrition is INTEGRAL for success

Monitoring Nutrition Status
• Labs/gasses – BUN
– ALK
– Vitamin D
– Chronic nutrition labs
• Appearance – Adiposity
– Coloring
• Progress – Endurance, thermoregulation, strength
49

Closing Considerations
• Prenatal nutrition status is important consideration—sets foundation for infant
• Nutrition support plays critical role in acute and long-term success of critically ill infants
• Growth is best evidence of appropriate nutrition support—but growth should not be solely assessed based on wt gain alone
50

Questions?
51