nutrition support for adults oral nutrition support, enteral tube
TRANSCRIPT

National Collaborating Centrefor Acute Care
Nutrition Support for AdultsOral Nutrition Support, Enteral TubeFeeding and Parenteral Nutrition
METHODS, EVIDENCE & GUIDANCE
FEBRUARY 2006Commissioned by the National Institute for
Clinical Excellence

1
Nutrition support in adultsOral nutrition support, enteral tubefeeding and parenteral nutrition
METHODS, EVIDENCE & GUIDANCE
Published by the National Collaborating Centre for Acute Care at The Royal College of Surgeons of England, 35-43 Lincoln’s Inn Fields, London, WC2A 3PE
First published 2006
© National Collaborating Centre for Acute Care 2006
Apart from any fair dealing for the purposes of research or private study, criticism or review, as permitted under the Copyright, Designsand Patents Act, 1988, no part of this publication may be reproduced, stored or transmitted in any form or by any means, without theprior written permission of the publisher or, in the case of reprographic reproduction, in accordance with the terms of licences issued bythe Copyright Licensing Agency in the UK. Enquiries concerning reproduction outside the terms stated here should be sent to thepublisher at the UK address printed on this page.
The use of registered names, trademarks, etc. in this publication does not imply, even in the absence of a specific statement, that suchnames are exempt from the relevant laws and regulations and therefore for general use.
The rights of National Collaborating Centre for Acute Care to be identified as Author of this work have been asserted by them inaccordance with the Copyright, Designs and Patents Act, 1988.
ISBN 0-9549760-2-9Citing this document: National Collaborating Centre for Acute Care, February 2006. Nutrition support in adults Oral nutrition support,enteral tube feeding and parenteral nutrition.National Collaborating Centre for Acute Care, London. Available from www.rcseng.ac.uk

FOREWORD
Malnutrition is both a cause and a consequence of ill-health. It is surprisingly common in the UK, especially inthose who are unwell. Many older people and those with any long-term medical or psycho-social problems arechronically underweight and so are vulnerable to acute illness. Even people who are well-nourished eat and drinkless if they are ill or injured and although this may only be short-lived as part of an acute problem, if it persists the person can become undernourished to an extent that may impair recovery or precipitate other medical conditions.
The consequences of malnutrition include vulnerability to infection, delayed wound healing, impaired function ofheart and lungs, decreased muscle strength and depression. People with malnutrition consult their generalpractitioners more frequently, go to hospital more often and for longer, and have higher complication andmortality rates. Surgical patients, who have malnutrition for example, have around three times as many post-operative complications and four times greater risk of death than well nourished patients having similaroperations. If poor dietary intake or complete inability to eat persists for weeks, the resulting malnutrition can belife-threatening in itself.
The provision of normal food and drink along with physical help to eat if necessary, when unwell will often suffice.However, if this fails, is impractical or is unsafe, measures to provide nutrition support may be indicated. Theseinclude, either alone or in combination: extra oral intake such as extra food and special drinks ; feeding via a tubeinto the gastro-intestinal tract (enteral tube feeding - ETF); or giving nutrients intravenously (parenteral nutrition -PN). Choosing the most effective and safest route is essential, yet current knowledge of nutrition support amongstmost UK health professionals is poor.
The need for nutrition support is essentially absolute if patients are unable to meet the majority of their nutrientneeds for prolonged periods (e.g. in complete dysphagia or intestinal failure). However, when nutritional intakesare closer to meeting needs, or when the likely period of inadequate intake is uncertain, decisions are morecomplex, especially as providing nutrition support is not without risk. Oral supplementation can cause pneumoniain dysphagic patients, while ETF and PN can cause gastrointestinal problems, infections, metabolic upset andtrauma. ‘These risks will need to be discussed with patients and even in those instances where they are able toprovide informed consent, difficult clinical and ethical issues can arise particularly where such patients do notwant to ‘artificially’ prolong their life. Likewise with patients who are unable to express a wish either becausethey are unconscious and thus unable to communicate but in need of immediate nutritional support or becausethey lack capacity to provide informed consent, in which case clinicians will need to act in accordance with whatthey determine to be in the best interests of the patient.’
NUTRITION SUPPORT IN ADULTS2

FOREWORD 3
The aim of these guidelines is to improve the practice of nutrition support by providing evidence and informationfor all healthcare professionals, patients and their carers so that malnutrition whether in hospital or in thecommunity, is recognized and treated by the best form of nutrition support at the appropriate time. However,although the recommendations have been systematically developed and based on trial evidence wherever possible,the Guideline Development Group (GDG) have met with some difficulties: the breadth of our remit was enormous;time and resources were finite; and the evidence base for nutrition support is difficult to interpret. The last of thesewas most problematic. Most of the evidence consists of many small trials, applying different interventions andoutcome measures, to very variable populations. This not only leads to individual trials being statisticallyunderpowered but makes combining them into meta-analyses more difficult. The varied study settings also createdifficulties in making firm recommendations for patients in the community when most research was conducted inhospitals. Furthermore, in the case of the more ‘invasive’ ETF and PN techniques, problems with the evidence arenear insurmountable. It is unethical to include patients who are unable to eat at all for significant periods in anyrandomized trial of ETF or PN (where feeding may be withheld). The scientific trials therefore examine ‘elective’supplementary usage of ETF and PN rather than their use in patients with an absolute need for such support andso the results do not necessarily apply to routine clinical practice.
In the light of the problems above, many of the recommendations in this guideline are derived from a combinationof clinical evidence, clinical experience and expertise. Many are also quite general, applying to all patients withmalnutrition whatever their disease or care setting. However, all healthcare professionals who have contact withpatients should find the recommendations relevant for we believe that they contain an obvious, simple message:
‘Do not let your patients starve and when you offer them nutrition support, do so by the safest, most simplest,effective route.’
This is essential to good patient care,
Mike StroudChair, Guideline Development Group.

3. Organisation of Nutrition Support in
hospital and the community 56
3.1. Introduction 563.2. Nutrition support in the community 563.3. Nutrition support in Hospital 563.4. Methods 583.5. Clinical evidence 583.6. Cost effectiveness evidence 603.7. Conclusion 603.8. Recommendations for clinical practice 613.9. Research recommendations 62
4. Screening for malnutrition and the risk
of malnutrition in hospital and
the community 63
4.1. Nutritional assessment 634.2. Why and how to screen 634.3. Methods 644.4. Studies considered for this review 654.5. Clinical evidence 654.6. Cost-effectiveness evidence 654.7. Consensus development methods 664.8. Impact of nutritional assessment on
the patient 684.9. Recommendations for clinical practice 694.10. Research recommendations 69
5. Indications for nutrition support 70
5.1. Introduction 705.2. Methodology 705.3. Appropriate Nutrition Support and
ethical/legal issues 715.4. Rationale for recommendations 725.4.1 Recommendations for clinical practice 725.5. Algorithms 74 - 76
6. What to give in hospital and
the community 77
6.1. Background 776.2. General Principles 776.3. Calculating requirements 78
NUTRITION SUPPORT IN ADULTS4
Contents
Guideline Development Group membership
and acknowledgments 6
Stakeholder Involvement 8
Abbreviations 10
Glossary of Terms 12
1. Introduction and methods 27
1.1. The need for guidelines in nutrition support 27
1.2. What is a guideline? 281.3. Remit of the guideline 281.4. What the guideline covers 291.5. What the guideline does not cover 291.6. Who the guideline is for 301.7. Who developed the guideline? 301.8. Methodology 301.9. Hierarchy of clinical evidence 331.10. Health economics methods 331.11. Forming and grading the recommendations 351.12. Specific problems with evidence relating
to the development of nutrition support guidelines 36
1.13. Patient-centred care 371.14. Summary of the recommendations 371.14.3 Research recommendations 51
2. Malnutrition and the principles
of nutrition support 53
2.1. Introduction 532.2. The causes of malnutrition 532.3. The effects of malnutrition 542.4. The prevalence of malnutrition 542.5. Principles underlying intervention 55

6.4. Concerns with prescribing levels 796.5. Recommendations for clinical practice 806.6. Re-feeding Problems 806.7. Recommendations for research 83
7. Monitoring of nutrition support in
hospital and the community 84
7.1. Introduction 847.2. Methods 847.3. Recommendations for clinical practice 857.4. Research Recommendations 90
8. Oral Nutrition Support in hospital
and the community 91
8.1. Introduction 918.2. Oral nutritional support versus standard
care in malnourished patients 918.3. Dietary advice versus standard care 968.4. Oral nutritional supplements versus
dietary advice 978.5. Recommendations for clinical practice 988.6. Oral nutrition support in surgical patients 988.7. Recommendations for clinical practice 1038.8. Oral nutrition support in pancreatitis patients 1038.9. Oral multivitamin and mineral
supplementation in malnourished patients 1038.10. Nutrition support in patients with dysphagia1068.11. Recommendations for clinical practice 1088.12. Research recommendations 108
9. Enteral tube feeding in hospital and
the community 110
9.1. Introduction 1109.2. General Indications for Enteral Tube Feeding1109.3. Recommendations for clinical practice 1119.4. Enteral tube feeding versus standard care 1119.5. Recommendations for clinical practice 1159.6. Enteral tube feeding routes of access 1159.7. Recommendations for clinical practice 1179.8. Percutaneous Endoscopic Gastrostomy
(PEG) versus Nasogastric (NG) Feeding 1179.9 Recommendations for clinical practice 1199.10. Commencing enteral tube feeding after
insertion of a percutaneous endoscopicgastrostomy 119
9.11. Recommendations for clinical practice 1199.12. Types of enteral feeds 1199.13. Mode of delivering Enteral Tube Feeding 1219.14. Recommendations for clinical practice 1229.15. Motility Agents 1229.16. Recommendations for clinical practice 1239.17. Complications of enteral tube feeding 1239.18. Recommendations for clinical practice 1249.19. Research recommendations 124
10. Parenteral nutrition in hospital
and the community 125
10.1. Introduction 12510.2. PN versus no PN 12510.2.3Elective PN in surgical patients 12710.3. Recommendations for clinical practice 12810.4. Parenteral versus enteral tube feeding 12910.5. Recommendations for clinical practice 13210.6. Venous access for PN 13210.7. Recommendations for clinical practice 13410.8. Peripheral PN versus central PN 13410.9. PN via a tunnelled catheter versus
PN via a non-tunnelled catheter 13610.10. Tailored PN preparations versus
standard PN preparations 13710.11. Recommendations for clinical practice 13710.12. Delivery of PN cyclically versus continuously 13810.13. Recommendations for clinical practice 13910.14. Complications from PN 13910.15. Recommendations for clinical practice 14010.16. Research recommendations 140
11. Supporting patients in the community 141
11.1 Home enteral tube feeding 14111.2 Recommendations for clinical practice 14111.3 Home parenteral nutrition 14211.4 Recommendations for clinical practice 14211.5 Working in partnership with patients,
families and carers 14311.6 Recommendations for clinical practice 14611.7 Research recommendations 146
12. Audit criteria 147
12. Bibliography 153
CONTENTS 5

NUTRITION SUPPORT IN ADULTS6
Guideline Development Group membershipand acknowledgments
GGuuiiddeelliinnee DDeevveellooppmmeenntt GGrroouupp
DDrr MMiikkee SSttrroouudd ((CChhaaiirr)) Institute of Human Nutrition, Southampton General Hospital; British Association of Parenteraland Enteral Nutrition (BAPEN)
MMss CChhrriissttiinnee BBaallddwwiinn Dietitian, Department of Medicine and Therapeutics, Imperial College, London; British DieteticAssociation (BDA)
MMrrss VViicckkyy BBrraaddnnaamm Chief Pharmacist, Bromley Hospitals NHS Trust, Bromley. Royal Pharmaceutical Society of GreatBritain
MMrrss AAnnddrreeaa CCaarrttwwrriigghhtt Senior Nutrition Nurse Specialist, Basildon University Hospital; National Nurses Nutrition Group(NNNG)
MMiissss GGwweenn CCoolleemmaann Manager, Food for Thought, Patient representative for Alzheimer’s Society
MMrrss LLiinnddaa DDiittcchhbbuurrnn Community Nutrition Nurse Specialist, Fernbank Medical Centre, Birmingham; National NursesNutrition Group (NNNG)
PPrrooffeessssoorr MMaarriinnooss EElliiaa Professor of Clinical Nutrition & Metabolism, Institute of Human Nutrition, Southampton GeneralHospital; Royal College of Physicians/Malnutrition Action Group (BAPEN)
PPrrooffeessssoorr RRiicchhaarrdd GGrriiffffiitthhss Professor of Medicine (Intensive Care), Division of Metabolic and Cellular Medicine, School ofClinical Science, University of Liverpool, and the Intensive Care Society (UK)
MMss JJuuddiitthh JJaacckkssoonn Principal Speech and Language Therapist, Islington PCT based at Whittington Hospital; RoyalCollege of Speech and Language Therapists Advisor in dysphagia
PPrrooffeessssoorr PPaauull LLiittttllee Professor of Primary Care Research, University of Southampton; Royal College of GeneralPractitioners
MMrr BBrruuccee MMccEEllrrooyy Associate Director of Pharmacy, University Hospital Birmingham Foundation Trust, Birmingham,Royal Pharmaceutical Society of Great Britain,
DDrr JJeerreemmyy NNiigghhttiinnggaallee Consultant Gastroenterologist, Digestive Disease Centre, Leicester Royal Infirmary; British Societyof Gastroenterology
MMiissss JJooaannnnaa PPrriicckkeetttt Chief Dietitian, Department Nutrition and Dietetics, North Bristol NHS Trust, British DieteticAssociation
PPrrooffeessssoorr AAllaann SShheennkkiinn Professor of Clinical Chemistry and Hon Consultant Chemical Pathologist, Department of ClinicalChemistry, University of Liverpool; Intercollegiate Group for Nutrition
MMrrss CCaarroollyynn WWhheeaattlleeyy Chairman, Patients on Intravenous and Nasogastric Nutrition Therapy (PINNT); PatientRepresentative for PINNT

NNCCCC--AACC ssttaaffff oonn tthhee GGuuiiddeelliinnee DDeevveellooppmmeenntt GGrroouupp
Ms Susan Murray Project Manager
Ms Louise Thomas Research Associate/Assistant Project Manager
Dr Funsho Akinluyi Research Associate
Ms Rifna Aktar Research Associate
Ms Leticia Barcena Research Associate
Dr John Browne Advisor on methodological issues
Mr Peter B Katz Information Specialist
Ms Veena Mazarello Paes Research Associate
Ms Guldem Okem Health Economist
Dr Arash Rashidian Advisor on methodological issues
Mr Carlos Sharpin Information Specialist and Reviewer
Ms Rachel Southon Information Specialist
Mr David Wonderling Health Economist
AAcckknnoowwlleeddggeemmeennttss
• The development of this guideline was greatly assisted by the following people:
From the NCC-AC: Jennifer Wood, Jacqueline Rainsbury, Sally Williams, Jennifer Hill, Sophie Capo-Bianco
• Annette Kelly, Specialist Speech and Language Therapist (ENT) – The Royal National Throat Nose and Ear HospitalLondon; Paula Leslie – Dysphagia Research Speech and Language Therapist, North Tees & Hartlepool PCT and CourseDirector MSc Speech & Swallowing Research, University of Newcastle and Heulwen Sheldrick Senior Lecturer,Manchester Metropolitan University and Senior Speech and Language Therapist, Halton Primary Care Trust
• Karen Harris- St Jean, Patient Representative for Samantha Dickson Research Trust ‡
• Barry Jones, Consultant Gastroenterologist, Dudley Hospital
CCoonnfflliicctt ooff IInntteerreessttss
The Guideline Development Group was asked to declare any possible conflict of interest and none that could interfere withtheir work on the guideline were declared. All documentation is held by the National Collaborating Centre for Acute Care.
GGuuiiddeelliinnee RReevviieeww PPaanneell
The Guideline Review Panel is an independent panel that oversees the development of the guideline and takes responsibilityfor monitoring its quality. The members of the Guideline Review Panel were as follows.
MMrr PPeetteerr RRoobbbb ((CChhaaiirr)) Consultant ENT Surgeon, Epsom and St Helier University Hospitals and the Royal SurreyCounty NHS Trusts
MMrrss JJooyyccee SSttrruutthheerrss Patient Representative, Bedford
DDrr PPeetteerr DDuunnccaann ((DDeeppuuttyy CChhaaiirr)) Consultant in Anaesthetics and Intensive Care Medicine, Royal Preston Hospital
MMrr MMiikkee BBaallddwwiinn Head of Health Technology Appraisals, Sanofi-Aventis
MMrrss AAnnnnee WWiilllliiaammss Deputy Director of Clinical Governance, Kettering General Hospital NHS Trust,Northamptonshire
GUIDELINE DEVELOPMENT GROUP MEMBERSHIP AND ACKNOWLEDGMENTS 7

CCoollllaabboorraattiinngg CCeennttrreess
Patient Involvement Unit for NICE
CCoommmmeerrcciiaall CCoommppaannyy
Abbott Laboratories Limited (BASF/Knoll)Bard LimitedBaxter OncologyBritannia Pharmaceuticals LtdClinovia LtdEnglish Community Care AssociationFresenius Kabi LtdImmogenics LimitedInfant and Dietetic Foods AssociationIntra-Tech Healthcare LtdMerck PharmaceuticalsNestle Clinical NutritionNovartis Consumer Health (Novartis Medical Nutrition)Nutricia Ltd (UK)Oxford Nutrition LtdPaines and Byrne LimitedProprietary Association of Great Britain (PAGB)SHS International LtdSyner-Med (PP) LtdVitaline Pharmaceuticals UK LtdVygon (UK) Ltd
HHeeaalltthh AAuutthhoorriittyy
Hampshire & Isle of Wight Strategic Health Authority
NNHHSS TTrruusstt
Addenbrookes NHS TrustAiredale General Hospital - Acute TrustAnglesey Local Health BoardAshfield and Mansfield District PCTsAvon and Wiltshire Mental Health Partnership NHS TrustBarnet PCTBolton Hospitals NHS TrustCarlisle and District Primary Care Trust
City and Hackney Primary Care TrustColchester Primary Care TrustCroydon Primary Care TrustDepartment of Academic Psychiatry - Guy’s HospitalDerby Hospitals NHS Foundation TrustGedling Primary Care TrustGreater Peterborough Primary Care Partnership-North Guys & St Thomas NHS TrustHammersmith Hospitals NHS TrustHertfordshire Partnership NHS TrustKing’s College Hospital NHS TrustKingston Primary Care TrustLeeds Teaching Hospitals NHS TrustManchester Royal InfirmaryMid Essex Hospitals NHS TrustMiddlesbrough Primary Care TrustNational Nurses Nutrition GroupNorth Glamorgan NHS Trust - Merthyr TydfilNorth West Wales NHS TrustOxfordshire Mental Healthcare NHS TrustPowys Local Health BoardPrincess Alexandra Hospital NHS TrustQueen Victoria Hospital NHS Foundation TrustRoyal Liverpool Children’s NHS TrustRoyal United Hospital Bath NHS TrustSandwell General Hospital Sheffield South West Primary Care TrustSheffield Teaching Hospitals NHS TrustSouth & Central Huddersfield PCTsSouth Birmingham Primary Care TrustSouth East Sheffield Primary Care TrustSouth Tees Hospitals NHS TrustTameside and Glossop Acute Services NHS TrustThe National Implementation Board for Modernisation ofNHS Medicines Manufacturing & PreparationThe Royal West Sussex TrustTrafford Primary Care TrustsUniversity College Londons Hospital NHS Trust
NUTRITION SUPPORT IN ADULTS8
Stakeholder Involvement
TThhee ffoolllloowwiinngg ssttaakkeehhoollddeerrss rreeggiisstteerreedd wwiitthh NNIICCEE aanndd wweerree iinnvviitteedd ttoo ccoommmmeenntt oonn ddrraafftt vveerrssiioonnss ooff tthheessee gguuiiddeelliinneess::

University Hospital Birmingham NHSFTVale of Aylesbury Primary Care TrustVale of Glamorgan Local Health Board
PPaattiieenntt//CCaarreerr OOrrggaanniissaattiioonn
Age Concern EnglandAlzheimer’s SocietyBritish Dyslexia AssociationBritish Liver TrustChildren’s Liver Disease FoundationDepression AllianceDiabetes UKEating Disorders Association, TheFibroid Network CharityHelp the AgedHelp the HospicesL’Arche UKMotor Neurone Disease AssociationNational Council for Disabled People, Black, Minority and National Kidney Federation (NFK)Parkinson’s Disease SocietyPatients on Intravenous and Nasogastric Nutrition Therapy(PINNT)Relatives and Residents AssociationSamantha Dickson Research Trust, TheSue Ryder CareThe Stroke AssociationWomen’s Health Concern
PPrrooffeessssiioonnaall OOrrggaanniissaattiioonn
All Wales Dietetic Advisory CommitteeAll Wales Senior Nurses Advisory Group (Mental Health)Association of Clinical Biochemists, TheAssociation of Surgeons of Great Britain and IrelandBritish Association for Parenteral & Enteral Nutrition(BAPEN)British Association of Head and Neck OncologistsBritish Association of Oral and Maxillofacial SurgeonsBritish Association of Otolaryngologists, Head & Neck British Association of Paediatric SurgeonsBritish Association of Perinatal MedicineBritish Dietetic AssociationBritish Geriatrics SocietyBritish Pharmaceutical Nutrition GroupBritish Psychological Society, TheBritish Society of GastroenterologyBritish Society of Paediatric Gastroenterology,Hepatology &NutritionCollege of Occupational Therapists
Co-operative Pharmacy AssociationFaculty of Dental SurgeryFaculty of Public HealthFood Standards AgencyInfection Control Nurses Association of the British IslesInstitute of Sport and Recreation ManagementIntensive Care SocietyMalnutrition Advisory Group (MAG)National Care Standards CommissionNutrition SocietyRoyal College of AnaesthetistsRoyal College of General PractitionersRoyal College of General Practitioners WalesRoyal College of Nursing (RCN)Royal College of Paediatrics and Child HealthRoyal College of PathologistsRoyal College of Physicians of EdinburghRoyal College of Physicians of LondonRoyal College of RadiologistsRoyal College of Speech and Language TherapistsRoyal Pharmaceutical Society of Great BritainSociety of Cardiothoracic SurgeonsThe British Psychological SocietyThe Royal Society of MedicineUniversity of Liverpool - Department of Child HealthWest Midlands Specialised Services Agency
RReesseeaarrcchh BBooddyy ((ddooiinngg rreesseeaarrcchh))
GeneWatch UKKeele UniversityMRC Human Nutrition Research
SSoocciiaall CCaarree OOrrggaanniissaattiioonn
The Disabilities Trust
SSttaattuuttoorryy BBooddyy
British National Formulary (BNF)Department of HealthHealthcare CommissionMedicines and Healthcare Products Regulatory Agency National Institute for Health and Clinical ExcellenceNational Patient Safety AgencyNational Public Health Service - WalesNHS Health and Social Care Information CentreNHS Quality Improvement ScotlandPerigon (formerly The NHS Modernisation Agency)Scottish Intercollegiate Guidelines Network (SIGN)Welsh Assembly Government (formerly National Assemblyfor Wales
STAKEHOLDER INVOLVEMENT 9

NUTRITION SUPPORT IN ADULTS10
Abbreviations
aaaa Amino acid
AAPPRR Acute phase reaction
AASSPPEENN American Society for Parenteral and Enteral Nutrition
BBAAPPEENN British Association for Parenteral and Enteral Nutrition
BBDDAA British Dietetic Association
BBMMII Body Mass Index
CCEEAA Cost-effectiveness analysis
CCII Confidence interval
CCOO22 Carbon dioxide
CCOOPPDD Chronic obstructive pulmonary disorder
CCVVAA Cerebrovascular disease
CCUUAA Cost-utility analysis
CCVVCC Central venous catheter
DDEEAALLEE Declining Exponential Approximation of Life Expectancy
DDHH Department of Health
EENN Enteral nutrition
EESSPPEENN European Society of Parenteral and Enteral Nutrition
(European Society for Clinical Nutrition and Metabolism)
EETTFF Enteral tube feeding
GGDDGG Guideline Development Group
GGII Gastrointestinal
GGPP General Practitioner
GGPPPP Good practice point
GGRRAADDEE Guidelines Recommendations Assessment Development Evaluation
GGRRPP Guideline Review Panel (formerly known as the Guidelines Advisory Committee, from which Designated Committee Members were selected)
HHEETTFF Home enteral tube feeding
HHIIVV Human Immunodeficiency Virus
HHPPNN Home parenteral nutrition
HHRRQQLL Health Related Quality of Life
HHTTAA Health technology assessment
HHTTBBSS Health Technology Board for Scotland

ABBREVIATIONS 11
IICCEERR Incremental cost-effectiveness ratio
IIPP Inpatient
IIVV Intravenous
LLOOSS Length of Stay
LLYY Life-year
MMAACC Mid arm circumference
MMAAMMCC Mid arm muscle circumference
MMDDTT Multidisciplinary team
MMNNAA Mini Nutritional Assessment
MMNNAA--SSFF Mini Nutritional Assessment-Short Form
MMNNDD Motor neuron disease
MMRRCC Medical Research Council
MMSS Multiple sclerosis
‘‘MMUUSSTT’’ ‘Malnutrition Universal Screening Tool’
NNCCCC National Collaborating Centre
NNCCCC--AACC National Collaborating Centre for Acute Care
NNCCEEPPOODD National Confidential Enquiry into Patient Outcome and Death
NNDD Nasoduodenal
NNGG Nasogastric
NNHHSS National Health Service
NNII Nutrition intake
NNIICCEE National Institute for Health and Clinical Excellence (formerly National Institute for Health and Clinical Excellence)
NNJJ Nasojejunal
NNNNTT Number needed to treat
OO22 Oxygen
OONNSS Oral Nutritional Supplement
PPEEGG Percutaneous endoscopic gastrostomy
PPEEJJ Percutaneous endoscopic jejunostomy
PPIICCCC Peripherally inserted central catheters
PPIICCOO Framework incorporating patients, interventions, comparisons, outcomes
PPIIUU Patient Involvement Unit (formerly known as the National Guidelines and Audit Patient Involvement Unit)
PPNN Parenteral nutrition
PPPPIIPP Patient and Public Involvement Programme
QQAALLYY Quality-adjusted life year
RRCCTT Randomised controlled trial
RRDDAA Recommended Dietary Allowance
RRQQ Respiratory quotient
SSIIGGNN Scottish Intercollegiate Guidelines Network
SSRR Systematic review
TTPPNN Total parenteral nutrition
TTSSFF Tricep skinfold

Glossary of Terms
Amended from a glossary produced by the Patient Involvement Unit, NICE.
AAbbssoolluuttee rriisskk rreedduuccttiioonn ((RRiisskk ddiiffffeerreennccee)) The difference in event rates between two groups (one subtracted from the other)in a comparative study.
AAbbssttrraacctt Summary of a study, which may be published alone or as an introduction to a fullscientific paper.
AAccuuttee PPhhaassee RReessppoonnssee ((AAPPRR)) A group of physiologic processes occurring soon after the onset of infection,trauma, inflammatory processes, and some malignant conditions. The mostprominent change is a dramatic increase of acute phase proteins, especially C-reactive protein, in the serum. Also seen are fever, increased vascular permeability,
and a variety of metabolic and pathologic changes2.
AAddjjuussttmmeenntt A statistical procedure in which the effects of differences in composition of thepopulations being compared (or treatment given at the same time) have beenminimised by statistical methods.
AAllggoorriitthhmm ((iinn gguuiiddeelliinneess)) A flow chart of the clinical decision pathway described in the guideline, wheredecision points are represented with boxes, linked with arrows.
AAllllooccaattiioonn ccoonncceeaallmmeenntt The process used to prevent advance knowledge of group assignment in a RCT.The allocation process should be impervious to any influence by the individualmaking the allocation, by being administered by someone who is not responsiblefor recruiting participants.
AAnncciillllaarriieess The equipment and consumables required for enteral and parenteral nutrition.
AApppplliiccaabbiilliittyy The degree to which the results of an observation, study or review are likely tohold true in a particular clinical practice setting.
AApppprraaiissaall ooff GGuuiiddeelliinneess,, RReesseeaarrcchh aanndd An international collaboration of researchers and policy makers whose aim is toimprove the quality and effectiveness of clinical practice guidelines(http://www.agreecollaboration.org). The AGREE instrument, developed by thegroup, is designed to assess the quality of clinical guidelines.
AApppprraaiissaall CCoommmmiitttteeee A standing advisory committee of the Institute. Its members are drawn from theNHS, patient/carer organisations, relevant academic disciplines and thepharmaceutical and medical devices industries.
AArrmm ((ooff aa cclliinniiccaall ssttuuddyy)) Sub-section of individuals within a study who receive one particular intervention,for example placebo arm.
AAsssseessssmmeenntt pprroottooccooll Written instructions for the conduct and analysis of the assessment of a technology.
NUTRITION SUPPORT IN ADULTS12
EEvvaalluuaattiioonn ((AAGGRREEEE))

AAsssseessssmmeenntt RReeppoorrtt In technology appraisals, a critical review of the clinical and cost effectiveness ofa health technology/technologies. It is prepared by the Assessment Group. Toprepare the report, the Assessment Group carries out a review of the publishedliterature and the submissions from manufacturers and sponsors.
AAssssoocciiaattiioonn Statistical relationship between two or more events, characteristics or othervariables. The relationship may or may not be causal.
AAuuddiitt See ‘Clinical audit’.
AAuuddiitt ttrraaiill Records of action to assess practice against standards. Also a record of actions,for example changes to a draft guideline so that reasons can be apparent to athird party.
BBaasseelliinnee The initial set of measurements at the beginning of a study (after run-in periodwhere applicable), with which subsequent results are compared.
BBiiaass Influences on a study that can lead to invalid conclusions about a treatment orintervention. Bias in research can make a treatment look better or worse than itreally is. Bias can even make it look as if the treatment works when it actuallydoesn’t. Bias can occur by chance or as a result of systematic errors in the designand execution of a study. Bias can occur at different stages in the researchprocess, e.g. in the collection, analysis, interpretation, publication or review ofresearch data.
BBlliinnddiinngg ((mmaasskkiinngg)) Keeping the study participants, caregivers, researchers and outcome assessors unawareabout the interventions to which the participants have been allocated in a study
BBooddyy MMaassss IInnddeexx A measure of body weight relative to height used to determine whether peopleare underweight, at a healthy weight, over weight or obese.
BBoolluuss//iinntteerrmmiitttteenntt ffeeeeddiinngg The administration of a feed through an enteral tube delivered as a single portionover a short period of time.
CCaappiittaall ccoossttss Costs of purchasing major capital assets (usually land, buildings or equipment).Capital costs represent investments at one point in time.
CCaarree hhoommeess This refers to residential and nursing care.
CCaarreerr ((ccaarreeggiivveerr)) Someone other than a health professional who is involved in caring for a personwith a medical condition.
CCaassee--ccoonnttrrooll ssttuuddyy Comparative observational study in which the investigator selects individuals whohave experienced an event (for example, developed a disease) and others whohave not (controls), and then collects data to determine previous exposure to apossible cause
CCaassee rreeppoorrtt ((oorr ccaassee ssttuuddyy)) Detailed report on one patient (or case), usually covering the course of thatperson’s disease and their response to treatment.
CCaassee sseerriieess Report of a number of cases of a given disease, usually covering the course of the disease and the response to treatment. There is no comparison (control) groupof patients.
GLOSSARY 13

CCllaassssiiffiiccaattiioonn ooff rreeccoommmmeennddaattiioonnss A code (such as A, B, C, D) given to a guideline recommendation, indicating thestrength of the evidence supporting that recommendation.
CClliinniiccaall aauuddiitt A quality improvement process that seeks to improve patient care and outcomesthrough systematic review of care against explicit criteria and the implementationof change.
CClliinniiccaall eeffffiiccaaccyy The extent to which an intervention is active when studied under controlledresearch conditions.
CClliinniiccaall eeffffeeccttiivveenneessss The extent to which an intervention produces an overall health benefit in routineclinical practice.
CClliinniiccaall iimmppaacctt The effect that a guideline recommendation is likely to have on the treatment ortreatment outcomes, of the target population.
CClliinniiccaall qquueessttiioonn In guideline development, this term refers to the questions about treatment and carethat are formulated to guide the development of evidence-based recommendations.
CClliinniicciiaann A healthcare professional providing direct patient care, for example doctor, nurseor physiotherapist.
CClluusstteerr A closely grouped series of events or cases of a disease or other related healthphenomena with well-defined distribution patterns, in relation to time or place orboth. Alternatively, a grouped unit for randomisation.
CCoocchhrraannee LLiibbrraarryy A regularly updated electronic collection of evidence-based medicine databases,including the Cochrane Database of Systematic Reviews.
CCoocchhrraannee RReevviieeww A systematic review of the evidence from randomised controlled trials relating toa particular health problem or healthcare intervention, produced by the CochraneCollaboration. Available electronically as part of the Cochrane Library.
CCoohhoorrtt ssttuuddyy A retrospective or prospective follow-up study. Groups of individuals to befollowed up are defined on the basis of presence or absence of exposure to asuspected risk factor or intervention. A cohort study can be comparative, in whichcase two or more groups are selected on the basis of differences in their exposureto the agent of interest.
CCoommbbiinneedd mmooddaalliittyy Use of different treatments in combination (for example surgery, chemotherapyand radiotherapy used together).
CCoommmmeennttaattoorr Organisations that engage in the appraisal process but that are not asked toprepare a submission dossier, and that receive the Final Appraisal Determination(FAD) for information only, without right of appeal. These organisations aremanufacturers of comparator technologies, NHS Quality Improvement Scotland;the relevant National Collaborating Centre; other related research groups andother groups where appropriate.
CCoommmmeennttss ttaabbllee Table compiled by NICE to show all the comments and responses generated aspart of the consultation process.
CCoommmmeerrcciiaall iinn ccoonnffiiddeennccee See ‘In confidence’
NUTRITION SUPPORT IN ADULTS14

CCoommmmuunniittyy This may refer to care homes (including residential care and nursing care),domiciliary care (also known as ‘home’ care) and primary care.
CCoo--mmoorrbbiiddiittyy Co-existence of more than one disease or an additional disease (other than thatbeing studied or treated) in an individual.
CCoommppaarraabbiilliittyy Similarity of the groups in characteristics likely to affect the study results (such ashealth status or age).
CCoommpplliiaannccee The extent to which a person adheres to the health advice agreed with healthcareprofessionals. May also be referred to as ‘adherence’.
CCoonnffeerreennccee pprroocceeeeddiinnggss Compilation of papers presented at a conference.
CCoonnffiiddeennccee iinntteerrvvaall ((CCII)) A range of values for an unknown population parameter with a stated ‘confidence’(conventionally 95%) that it contains the true value. The interval is calculated fromsample data, and generally straddles the sample estimate. The ‘confidence’ valuemeans that if the method used to calculate the interval is repeated many times, thenthat proportion of intervals will actually contain the true value.
CCoonnffoouunnddiinngg In a study, confounding occurs when the effect of an intervention on an outcomeis distorted as a result of an association between the population or interventionor outcome and another factor (the ‘confounding variable’) that can influence theoutcome independently of the intervention under study.
CCoonnsseennssuuss mmeetthhooddss Techniques that aim to reach an agreement on a particular issue. Formalconsensus methods include Delphi and nominal group techniques, and consensusdevelopment conferences. In the development of clinical guidelines, consensusmethods may be used where there is a lack of strong research evidence on aparticular topic. Expert consensus methods will aim to reach agreement betweenexperts in a particular field.
CCoonnssuullttaattiioonn The process that allows stakeholders and individuals to comment on initialversions of NICE guidance and other documents so their views can be taken intoaccount when producing the final version.
CCoonnssuulltteeee An organisation that accepts an invitation to participate in the appraisal. Consulteescan participate in the consultation on the draft scope, the Assessment Report and theAppraisal Consultation Document; consultee organisations representing patient/carersand professionals can nominate clinical specialists and patient experts to present theirpersonal views to the Appraisal Committee, AND are given the opportunity to appealagainst the Final Appraisal Determination (FAD).
CCOONNSSOORRTT ssttaatteemmeenntt Recommendations for improving the reporting of randomised controlled trials injournals. A flow diagram and checklist allow readers to understand the conduct ofthe study and assess the validity of the results.
CCoonnttrrooll ggrroouupp A group of patients recruited into a study that receives no treatment, a treatmentof known effect, or a placebo (dummy treatment) - in order to provide acomparison for a group receiving an experimental treatment, such as a new drug.
GLOSSARY 15
((CCoonnssoolliiddaatteedd rreeppoorrttiinngg ooff cclliinniiccaall ttrriiaallss))

CCoonnttrroolllleedd cclliinniiccaall ttrriiaall ((CCCCTT)) A study testing a specific drug or other treatment involving two (or more) groups ofpatients with the same disease. One (the experimental group) receives the treatmentthat is being tested, and the other (the comparison or control group) receives analternative treatment, a placebo (dummy treatment) or no treatment. The two groupsare followed up to compare differences in outcomes to see how effective theexperimental treatment was. A CCT where patients are randomly allocated totreatment and comparison groups is called a randomised controlled trial.
CCoosstt bbeenneeffiitt aannaallyyssiiss A type of economic evaluation where both costs and benefits of healthcaretreatment are measured in the same monetary units. If benefits exceed costs, theevaluation would recommend providing the treatment.
CCoosstt--ccoonnsseeqquueenncceess aannaallyyssiiss ((CCCCAA)) A type of economic evaluation where various health outcomes are reported inaddition to cost for each intervention, but there is no overall measure of health gain.
CCoosstt--eeffffeeccttiivveenneessss aannaallyyssiiss ((CCEEAA)) An economic study design in which consequences of different interventions aremeasured using a single outcome, usually in ‘natural’ units (for example, life-yearsgained, deaths avoided, heart attacks avoided, cases detected). Alternativeinterventions are then compared in terms of cost per unit of effectiveness.
CCoosstt--eeffffeeccttiivveenneessss mmooddeell An explicit mathematical framework, which is used to represent clinical decisionproblems and incorporate evidence from a variety of sources in order to estimatethe costs and health outcomes.
CCoosstt--uuttiilliittyy aannaallyyssiiss ((CCUUAA)) A form of cost-effectiveness analysis in which the units of effectiveness arequality-adjusted life-years (QALYs).
CCoonntteenntt eexxppeerrtt An individual with skills or knowledge relating to the subject being investigated.
CCrriitteerriioonn ((iinn aauuddiitt)) An explicit statement that defines the appropriateness of healthcare decisions,services and outcomes, and that can be measured.
CCrroossss--sseeccttiioonnaall ssttuuddyy The observation of a defined set of people at a single point in time or time period– a snapshot. (This type of study contrasts with a longitudinal study which followsa set of people over a period of time).
DDeecciissiioonn aannaallyyssiiss A systematic way of reaching decisions, based on evidence from research. Thisevidence is translated into probabilities, and then into diagrams or decision treeswhich direct the clinician through a succession of possible scenarios, actions and outcomes.
DDeecciissiioonn aannaallyyttiicc tteecchhnniiqquueess A way of reaching decisions, based on evidence from research. This evidence istranslated into probabilities, and then into diagrams or decision trees that directthe clinician through a succession of possible scenarios, actions and outcomes.
DDeecciissiioonn pprroobblleemm A clear specification of the interventions, patient populations and outcomemeasures and perspective adopted in an evaluation, with an explicit justification,relating these to the decision which the analysis is to inform.
DDiieettaarryy aaddvviiccee The provision of instructions on modifying food intake to improve nutritional intake.
NUTRITION SUPPORT IN ADULTS16
DDiissccoouunnttiinngg Costs and perhaps benefits incurred today have a higher value than costs andbenefits occurring in the future. Discounting health benefits reflects individualpreference for benefits to be experienced in the present rather than the future.Discounting costs reflects individual preference for costs to be experienced in thefuture rather than the present.
DDoommiinnaannccee An intervention is said to be dominated if there is an alternative intervention thatis both less costly and more effective.
DDoossaaggee The prescribed amount of a drug to be taken, including the size and timing of the doses.
DDoouubbllee bblliinndd ssttuuddyy A study in which neither the subject (patient) nor the observer(investigator/clinician) is aware of which treatment or intervention the subject isreceiving. The purpose of blinding is to protect against bias.
DDrroopp--oouutt A participant who withdraws from a clinical trial before the end.
DDyysspphhaaggiiaa Any impairment of eating, drinking and swallowing.
EEccoonnoommiicc eevvaalluuaattiioonn Comparative analysis of alternative health strategies (interventions orprogrammes) in terms of both their costs and consequences.
EEffffiiccaaccyy See ‘Clinical efficacy’.
EEffffeecctt ((aass iinn eeffffeecctt mmeeaassuurree,, ttrreeaattmmeenntt The observed association between interventions and outcomes or a statistic tosummarise the strength of the observed association.
EEffffeeccttiivveenneessss See ‘Clinical effectiveness’.
EElleeccttiivvee Name for clinical procedures that are regarded as advantageous to the patientbut not urgent.
EElleeccttrroollyytteess Anions and cations in the blood, tissue fluids and cells e.g. sodium, potassiumand chlorine.
EEnntteerraall nnuuttrriittiioonn see enteral tube feeding
EEnntteerraall ttuubbee ffeeeeddiinngg Nutrition support directly into the gut via a tube (the term as used in theseguidelines does not include oral intake).
EEppiiddeemmiioollooggiiccaall ssttuuddyy The study of a disease within a population, defining its incidence and prevalenceand examining the roles of external influences (for example, infection, diet) andinterventions
EEvviiddeennccee Information on which a decision or guidance is based. Evidence is obtained froma range of sources including randomised controlled trials, observational studies,expert opinion (of clinical professionals and/or patients).
EEvviiddeennccee ttaabbllee A table summarising the results of a collection of studies which, taken together,represent the evidence supporting a particular recommendation or series ofrecommendations in a guideline.
GLOSSARY 17
eeffffeecctt,, eessttiimmaattee ooff eeffffeecctt,, eeffffeecctt ssiizzee))

EExxcclluussiioonn ccrriitteerriiaa ((lliitteerraattuurree rreevviieeww)) Explicit standards used to decide which studies should be excluded fromconsideration as potential sources of evidence.
EExxcclluussiioonn ccrriitteerriiaa ((cclliinniiccaall ssttuuddyy)) Criteria that define who is not eligible to participate in a clinical study.
EExxppeerrtt ccoonnsseennssuuss See ‘Consensus methods’.
EExxtteennddeedd ddoommiinnaannccee If Option A is both more clinically effective than Option B and has a lower costper unit of effect, when both are compared with a do-nothing alternative thenOption A is said to have extended dominance over Option B. Option A istherefore more efficient and should be preferred, other things remaining equal.
EExxttrraappoollaattiioonn In data analysis, predicting the value of a parameter outside the range ofobserved values.
FFaacciilliittaattoorr An individual whose function is to promote the effective functioning of thegroup.
FFooccuuss ggrroouupp A qualitative research technique. It is a method of group interview or discussionof between 6–12 people focused around a particular issue or topic. The methodexplicitly includes and uses the group interaction to generate data.
FFoollllooww uupp Observation over a period of time of an individual, group or initially definedpopulation whose appropriate characteristics have been assessed in order toobserve changes in health status or health-related variables.
GGaanntttt CChhaarrtt A project planning tool showing the timing of tasks within a project. Dates runfrom left to right and each task is represented by a horizontal bar, the left end ofwhich marks the expected beginning of the task and the right end of whichmarks the planned completion date.
GGaassttrroojjeejjuunnoossttoommyy ttuubbee Enteral tube inserted through the abdominal wall which passes through thestomach into the jejunum for the purpose of nutrition support.
GGaassttrroossttoommyy Enteral tube inserted through the abdominal wall into the stomach for thepurpose of nutrition support.
GGeenneerraalliissaabbiilliittyy The extent to which the results of a study based on measurement in a particularpatient population and/or a specific context hold true for another populationand/or in a different context. In this instance, this is the degree to which theguideline recommendation is applicable across both geographical and contextualsettings. For instance, guidelines that suggest substituting one form of labour foranother should acknowledge that these costs might vary across the country.
GGeenneerriicc nnaammee The general non-proprietary name of a drug or device.
GGoolldd ssttaannddaarrdd A method, procedure or measurement that is widely accepted as being the bestavailable.
GGooooddnneessss--ooff--ffiitt How well a statistical model or distribution compares with the observed data.
GGoooodd PPrraaccttiiccee PPooiinnttss Recommended good practice based on the clinical experience of the GuidelineDevelopment Group.
NUTRITION SUPPORT IN ADULTS18

GGrraaddiinngg eevviiddeennccee A code given to a study or other evidence, indicating the quality andgeneralisability of the research. The highest grade evidence will usually beobtained from randomised controlled trials.
GGrreeyy lliitteerraattuurree Reports that are unpublished or have limited distribution, and are not included inthe common bibliographic retrieval systems.
HHaarrmmss Adverse effects of an intervention.
HHeeaalltthh eeccoonnoommiiccss The study of the allocation of scarce resources among alternative healthcaretreatments. Health economists are concerned with both increasing the averagelevel of health in the population and improving the distribution of health.
HHeeaalltthh rreellaatteedd qquuaalliittyy ooff lliiffee A combination of an individual’s physical, mental and social well-being; notmerely the absence of disease.
HHeeaalltthh tteecchhnnoollooggyy Any method used by those working in health services to promote health, preventand treat disease, and improve rehabilitation and long-term care. Technologies inthis context are not confined to new drugs or pieces of sophisticated equipment.
HHeetteerrooggeenneeiittyy Or lack of homogeneity. The term is used in meta-analyses and systematic reviewswhen the results or estimates of effects of treatment from separate studies seem to bevery different – in terms of the size of treatment effects or even to the extent thatsome indicate beneficial and others suggest adverse treatment effects. Such resultsmay occur as a result of differences between studies in terms of the patientpopulations, outcome measures, definition of variables or duration of follow-up.
HHoommee eenntteerraall ttuubbee ffeeeeddiinngg The practice of enteral tube feeding in the community.
HHoommee ppaarreenntteerraall NNuuttrriittiioonn The practice of parenteral nutrition in the community.
HHoommooggeenneeiittyy This means that the results of studies included in a systematic review or meta-analysis are similar and there is no evidence of heterogeneity. Results are usuallyregarded as homogeneous when differences between studies could reasonably beexpected to occur by chance.
HHyyppootthheessiiss A supposition made as a starting point for further investigation.
IImmpplleemmeennttaattiioonn Introducing the use of the guidance recommendations in practice.
IInn ccoonnffiiddeennccee mmaatteerriiaall Information (for example, the findings of a research project) defined as‘confidential’ as its public disclosure could have an impact on the commercialinterests of a particular company or the academic interests of a research orprofessional organisation.
IInncclluussiioonn ccrriitteerriiaa ((lliitteerraattuurree rreevviieeww)) Explicit criteria used to decide which studies should be considered as potentialsources of evidence.
IInnccrreemmeennttaall aannaallyyssiiss The comparison of the costs and effects of one intervention compared with thenext best alternative.
IInnccrreemmeennttaall ccoosstt eeffffeeccttiivveenneessss rraattiioo ((IICCEERR)) The difference in the mean costs in the population of interest divided by thedifferences in the mean outcomes in the population of interest.
GLOSSARY 19

IInnddeexx In epidemiology and related sciences, this word usually means a rating scale, forexample, a set of numbers derived from a series of observations of specifiedvariables. Examples include the various health status indices, and scoring systemsfor severity or stage of cancer.
IInnddiiccaattiioonn ((ssppeecciiffiicc)) The defined use of a technology as licensed by the Medicines and Healthcareproducts Regulatory Agency (MHRA).
IInntteennttiioonn--ttoo--ttrreeaatt aannaallyyssiiss ((IITTTT aannaallyyssiiss)) An analysis of the results of a clinical study in which the data are analysed for allstudy participants as if they had remained in the group to which they wererandomised, regardless of whether or not they remained in the study until theend, crossed over to another treatment or received an alternative intervention
IInntteerrmmeeddiiaattee oouuttccoommeess Outcomes that are related to the outcome of interest but may be more easilyassessed within the context of a clinical study: for example, blood pressurereduction is related to the risk of a stroke.
IInntteerrnnaall vvaalliiddiittyy The degree to which the results of a study are likely to approximate the ‘truth’ forthe participants recruited in a study (that is, are the results free of bias?). It refersto the integrity of the design and is a prerequisite for applicability (externalvalidity) of a study’s findings. See ‘External validity’.
IInntteerrvveennttiioonn Healthcare action intended to benefit the patient, for example, drug treatment,surgical procedure, psychological therapy.
JJeejjuunnoossttoommyy Enteral tube inserted through the abdominal wall directly into the jejunum forthe purpose of nutrition support.
LLeennggtthh ooff ssttaayy The total number of days a participant stays in hospital.
LLiicceennccee See ‘Product licence’.
LLiiffee yyeeaarr A measure of health outcome which shows the number of years of remaining lifeexpectancy.
LLiiffee--yyeeaarrss ggaaiinneedd Average years of life gained per person as a result of the intervention.
LLoonnggiittuuddiinnaall ssttuuddyy A study of the same group of people at more than one point in time. (This type ofstudy contrasts with a cross sectional study which observes a defined set ofpeople at a single point in time).
LLuummeenn Cavity or channel within a tube
MMaallnnuuttrriittiioonn A state of nutrition in which a deficiency of energy, protein and/or othernutrients causes measurable adverse effects on tissue/body form, composition,
function or clinical outcome94 (in these guidelines we do not use the term tocover excess nutrient provision). For the purposes of this guideline we haveconsidered that malnutrition is likely to be significant if a person has a
BMI <18.5 kg/m2, or unintentional weight loss >10% within the previous 3-6
months, or a BMI<20 kg/m2 and unintentional weight loss >5% within theprevious 3-6 months.
NUTRITION SUPPORT IN ADULTS20

MMaallnnuuttrriittiioonn,, aatt rriisskk has eaten little or nothing for more than 5 days and/or is likely to eat little ornothing for the next 5 days or longer
MMeeddiicciinneess aanndd HHeeaalltthhccaarree PPrroodduuccttss The Executive Agency of the Department of Health protecting and promotingpublic health and patient safety by ensuring that medicines, healthcare productsand medical equipment meet appropriate standards of safety, quality,performance and effectiveness, and are used safely.
MMeettaa--aannaallyyssiiss Results from a collection of independent studies (investigating the sametreatment) are pooled, using statistical techniques to synthesise their findingsinto a single estimate of a treatment effect. Where studies are not compatible e.g.because of differences in the study populations or in the outcomes measured, itmay be inappropriate or even misleading to statistically pool results in this way.See also Systematic review & Heterogeneity.
MMoottiilliittyy aaggeenntt A medication used to aid the movement of food from the stomach into theintestine.
NNaassoodduuooddeennaall ((ttuubbee)) ffeeeeddiinngg Nutrition support provided via a tube inserted via the nose, oesophagus andstomach into the duodenum.
NNaassooggaassttrriicc ((ttuubbee)) ffeeeeddiinngg Nutrition support provided through a tube inserted through the nose via theoesophagus into the stomach.
NNaassoojjeejjuunnaall ((ttuubbee)) ffeeeeddiinngg Nutrition support provided through a tube inserted through the nose via theoesophagus, stomach and duodenum into the jejunum.
NNIICCEE TTeecchhnnoollooggyy AApppprraaiissaallss Recommendations on the use of new and existing medicines and othertreatments within the NHS in England and Wales, such as: medicines (forexample, drugs), medical devices (for example, hearing aids and inhalers),diagnostic techniques (tests used to identify diseases), surgical procedures (forexample, repair of hernias), health promotion activities (for example, patienteducation models for diabetes).
NNoonn--eexxppeerriimmeennttaall ssttuuddyy A study based on subjects selected on the basis of their availability, with noattempt having been made to avoid problems of bias.
NNuummbbeerr nneeeeddeedd ttoo ttrreeaatt ((NNNNTT)) The number of patients that who on average must be treated to prevent a singleoccurrence of the outcome of interest.
NNuuttrriittiioonn aasssseessssmmeenntt A comprehensive evaluation to define nutrition status, including medical history,dietary history, physical examination, anthropometric measurements andlaboratory data, by a health professional with skills and tanning in nutrition andnutrition support. For example dietitian, nutrition nurse.
NNuuttrriittiioonn ssccrreeeenniinngg A rapid, simple and general procedure used by nursing, medical or other staff,often at first contact with the patient, to detect those who have significantnutritional problems or significant risks of such problems, in order that clearguidelines for action can be implemented, e.g. simple dietary measures or referral
for expert help94.
GLOSSARY 21
RReegguullaattoorryy AAggeennccyy ((MMHHRRAA))

NNuuttrriittiioonn ssuuppppoorrtt The provision of nutrients and any necessary adjunctive therapeutic agents topatients orally and/or enterally by administration into the stomach or intestineand/or by intravenous infusion (parenterally) for the purpose of improving ormaintaining a patient’s nutrition status’
NNuuttrriittiioonn SSuuppppoorrtt TTeeaamm A multidisciplinary team with dietetic, nursing, pharmacy and medical expertiseto provide safe nutrition support.
OObbsseerrvvaattiioonnaall ssttuuddyy Retrospective or prospective study in which the investigator observes the naturalcourse of events with or without control groups; for example, cohort studies andcase–control studies.
OOllddeerr ppeeooppllee People over the age of 65 years.
OOppeerraattiinngg ccoossttss Ongoing costs of carrying out an intervention, excluding capital costs.
OOrraall NNuuttrriittiioonnaall SSuupppplleemmeenntt A product for use in oral nutrition support given with the aim to increasenutritional intake.
OOrraall nnuuttrriittiioonn ssuuppppoorrtt The modification of food and fluid by: fortifying food with protein, carbohydrateand/or fat plus minerals and vitamins; the provision snacks and/or oralnutritional supplements as extra nutrition to regular meals, changing mealpatterns or the provision of dietary advice to patients on how to increase overallnutrition intake by the above.
OOrrooggaassttrriicc ((ttuubbee)) ffeeeeddiinngg Nutrition support provided by a tube inserted through the mouth via theoesophagus into the stomach
OOppppoorrttuunniittyy ccoosstt The opportunity cost of investing in a healthcare intervention is the otherhealthcare programmes that are displaced by its introduction. This may be bestmeasured by the health benefits that could have been achieved had the moneybeen spent on the next best alternative healthcare intervention.
OOuuttccoommee Measure of the possible results that may stem from exposure to a preventive ortherapeutic intervention. Outcome measures may be intermediate endpoints orthey can be final endpoints. See ‘Intermediate outcome’.
PP vvaalluuee The probability that an observed difference could have occurred by chance,assuming that there is in fact no underlying difference between the means of theobservations. If the probability is less than 1 in 20, the P value is less than 0.05;a result with a P value of less than 0.05 is conventionally considered to be‘statistically significant’.
PPaalllliiaattiivvee ccaarree Active holistic care of patients with advanced progressive illness, focusing on themanagement of pain and other symptoms and provision of psychological, socialand spiritual support. The goal of palliative care is the achievement of the best
quality of life for patients and their families.378
PPaarreenntteerraall nnuuttrriittiioonn The provision of nutrition support through intravenous administration of nutrientssuch as amino acids, glucose, fat, electrolytes, vitamins and trace elements.
NUTRITION SUPPORT IN ADULTS22

PPeerriiooppeerraattiivvee The period from admission through surgery until discharge, encompassing pre-operative and post-operative periods. Studies included in this guideline for surgicalpatients sometimes start or end their intervention outside this period. However, theyalways include nutrition support during some of the perioperative phase.
PPeeeerr rreevviieeww A process where research is scrutinised by experts that have not been involved inthe design or execution of the studies.
PPiilloott ssttuuddyy A small scale ‘test’ of the research instrument. For example, testing out (piloting)a new questionnaire with people who are similar to the population of the study,in order to highlight any problems or areas of concern, which can then beaddressed before the full scale study begins.
PPllaacceebboo An inactive and physically identical medication or procedure used as acomparator in controlled clinical trials.
PPllaacceebboo eeffffeecctt A beneficial (or adverse) effect produced by a placebo and not due to anyproperty of the placebo itself.
PPoowweerr See ‘Statistical power’.
PPrriimmaarryy ccaarree Healthcare delivered to patients outside hospitals. Primary care covers a range ofservices provided by GPs, nurses and other healthcare professionals, dentists,pharmacists and opticians.
PPrriimmaarryy rreesseeaarrcchh Study generating original data rather than analysing data from existing studies(which is called secondary research).
PPrroodduucctt lliicceennccee An authorisation from the MHRA to market a medicinal product.
PPrrooggnnoossiiss A probable course or outcome of a disease. Prognostic factors are patient ordisease characteristics that influence the course. Good prognosis is associatedwith low rate of undesirable outcomes; poor prognosis is associated with a highrate of undesirable outcomes.
PPrroopprriieettaarryy nnaammee The brand name given by the manufacturer to a drug or device it produces.
PPrroossppeeccttiivvee ssttuuddyy A study in which people are entered into the research and then followed up overa period of time with future events recorded as they happen. This contrasts withstudies that are retrospective.
QQuuaalliittaattiivvee rreesseeaarrcchh Research concerned with subjective outcomes relating to social, emotional andexperiential phenomena in health and social care.
QQuuaalliittyy aaddjjuusstteedd lliiffee yyeeaarrss ((QQAALLYYSS)) An index of survival that is adjusted to account for the patient’s quality of lifeduring this time. QALYs have the advantage of incorporating changes in bothquantity (longevity/mortality) and quality (morbidity, psychological, functional,social and other factors) of life. Used to measure benefits in cost-utility analysis.
QQuuaalliittyy ooff lliiffee See ‘Health related quality of life’
GLOSSARY 23

QQuuaannttiittaattiivvee rreesseeaarrcchh Research that generates numerical data or data that can be converted intonumbers, for example clinical trials or the national Census which counts peopleand households.
QQuuiicckk RReeffeerreennccee GGuuiiddee An abridged version of NICE guidance, which presents the key priorities forimplementation and summarises the recommendations for the core clinical audience.
RRaannddoomm aallllooccaattiioonn oorr RRaannddoommiissaattiioonn Allocation of participants in a research study to two or more alternative groups usinga chance procedure, such as computer-generated random numbers. This approach isused in an attempt to ensure there is an even distribution of participants withdifferent characteristics between groups and thus reduce sources of bias.
RRaannddoommiisseedd ccoonnttrroolllleedd ttrriiaall ((RRCCTT)) A comparative study in which participants are randomly allocated to interventionand control groups and followed up to examine differences in outcomes betweenthe groups.
RRaappiidd uuppddaattee Review of existing guidance carried out sooner than originally planned becausenew data have become available.
RReeffeerreennccee ssttaannddaarrdd ((oorr ggoolldd ssttaannddaarrdd)) An agreed standard, for example for a test or treatment, against which otherinterventions can be compared.
RReellaattiivvee rriisskk ((RRRR)) The number of times more likely or less likely an event is to happen in one groupcompared with another (calculated as the risk of the event in group A/the risk ofthe event in group B).
RReelliiaabbiilliittyy//rreeppeeaattaabbiilliittyy The degree of agreement exhibited when a measurement is repeated underidentical conditions. Reliability refers to the degree to which the results obtainedby a measurement procedure can be replicated.
RReemmiitt The brief given by the Department of Health and Welsh Assembly Government atthe beginning of the guideline development process. This defines core areas ofcare that the guideline needs to address.
RReesseeaarrcchh EEtthhiiccss CCoommmmiitttteeee An independent committee that scrutinises proposals for research to ensure theyare ethically acceptable.
RReessoouurrccee iimmpplliiccaattiioonn The likely impact in terms of finance, workforce or other NHS resources.
RReettrroossppeeccttiivvee ssttuuddyy A retrospective study deals with the present/ past and does not involve studyingfuture events. This contrasts with studies that are prospective.
RReevviieeww ooff tthhee lliitteerraattuurree An article that summarises the evidence contained in a number of differentindividual studies and draws conclusions about their findings. It may or may notbe systematically researched and developed.
SSeeccoonnddaarryy bbeenneeffiittss Benefits resulting from a treatment in addition to the primary, intended outcome.
SSeeccoonnddaarryy ccaarree Care provided in hospitals.
SSeelleeccttiioonn bbiiaass ((aallssoo aallllooccaattiioonn bbiiaass)) A systematic bias in selecting participants for study groups, so that the groupshave differences in prognosis and/or therapeutic sensitivities at baseline.Randomisation (with concealed allocation) of patients protects against this bias.
NUTRITION SUPPORT IN ADULTS24
((ffoorr aa gguuiiddeelliinnee oorr aapppprraaiissaall))

SSeelleeccttiioonn ccrriitteerriiaa Explicit standards used by guideline development groups to decide which studiesshould be included and excluded from consideration as potential sources ofevidence.
SSeennssiittiivviittyy aannaallyyssiiss A means of representing uncertainty in the results of economic evaluations.Uncertainty may arise from missing data, imprecise estimates or methodologicalcontroversy. Sensitivity analysis also allows for exploring the generalisability ofresults to other settings. The analysis is repeated using different assumptions toexamine the effect on the results. One-way simple sensitivity analysis (univariateanalysis): each parameter is varied individually in order to isolate theconsequences of each parameter on the results of the study. Multi-way simplesensitivity analysis (scenario analysis): two or more parameters are varied at thesame time and the overall effect on the results is evaluated. Threshold sensitivityanalysis: the critical value of parameters above or below which the conclusions ofthe study will change are identified. Probabilistic sensitivity analysis: probabilitydistributions are assigned to the uncertain parameters and are incorporated intoevaluation models based on decision analytical techniques (for example, MonteCarlo simulation).
SSeerrvviiccee ddeelliivveerryy gguuiiddaannccee Recommendations on service delivery primarily aimed at health servicecommissioners. Service delivery guidance focuses on the broad configuration andprovision of clinical services and addresses only those interventions that are likelyto have implications for the configuration of services.
SSppeecciiaalliisseedd nnuuttrriittiioonn ssuuppppoorrtt
SSppeecciiffiicciittyy ((ooff aa tteesstt)) The proportion of individuals classified as negative by the gold (or reference)standard, who are correctly identified by the study test.
SSttaannddaarrdd ccaarree The situation in which a patient is given no supplementary nutrition support butstill eats meals and snacks as appropriate for their clinical status and usualpractice.
SSttaannddaarrddiisseedd PPaarreenntteerraall NNuuttrriittiioonn Admixtures containing fixed formulations of nutrients, such as amino acids,glucose, fat emulsion and electrolytes in a single sterile container system.Additions of other nutrients such as vitamins and trace elements and occasionallysupplemental electrolytes are required to ensure complete admixtures areadministered.
SSttaakkeehhoollddeerr Those with an interest in the use of a technology under appraisal or a guidelineunder development. Stakeholders include manufacturers, sponsors, healthcareprofessionals, and patient and carer groups.
SSttaattiissttiiccaall ppoowweerr The ability to demonstrate an association when one exists. Power is related tosample size; the larger the sample size, the greater the power and the lower therisk that a possible association could be missed.
SSyynntthheessiiss ooff eevviiddeennccee A generic term to describe methods used for summarising (comparing andcontrasting) evidence into a clinically meaningful conclusion in order to answer adefined clinical question. This can include systematic review (with or withoutmeta-analysis), qualitative and narrative summaries.
GLOSSARY 25

SSyysstteemmaattiicc rreevviieeww Research that summarises the evidence on a clearly formulated questionaccording to a pre-defined protocol using systematic and explicit methods toidentify, select and appraise relevant studies, and to extract, collate and reporttheir findings. It may or may not use statistical meta-analysis.
SSyysstteemmiicc IInnffllaammmmaattoorryy RReessppoonnssee A systemic inflammatory response to at least two criteria leukocytosis, fever,tachycardia, and tachypnea.
TTeecchhnniiccaall LLeeaadd Appraisals team member who has responsibility for the technical aspects of theappraisal including liaising with the Assessment Group, scoping the appraisal,preparing drafts of consultation documents and advising the AppraisalCommittee on technical aspects of the appraisal. There may be more than oneTechnical Lead for an appraisal.
TTeecchhnnoollooggyy aasssseessssmmeenntt The process of evaluating the clinical, economic and other evidence relating touse of a technology in order to formulate guidance on its most efficient use.
TTeesstt--aanndd--ttrreeaatt ssttrraatteeggyy Testing all individuals presenting with suspected of having a condition, andtreating only those with a particular test result.
TTiimmee hhoorriizzoonn The time span used in the NICE appraisal which reflects the period over whichthe main differences between interventions in health effects and use ofhealthcare resources are expected to be experienced, and taking into account thelimitations of supportive evidence.
TTrreeaattmmeenntt aallllooccaattiioonn Assigning a participant to a particular arm of the trial.
TTrreeaattmmeenntt ooppttiioonnss The choices of intervention available.
UUttiilliittyy A measure of the strength of an individual’s preference for a specific health statein relation to alternative health states. The utility scale assigns numerical valueson a scale from 0 (death) to 1 (optimal or ‘perfect’ health). Health states can beconsidered worse than death and thus have a negative value.
NUTRITION SUPPORT IN ADULTS26
SSyynnddrroommee ((SSIIRRSS))

11..11 TThhee nneeeedd ffoorr gguuiiddeelliinneess iinn nnuuttrriittiioonn ssuuppppoorrtt
Malnutrition is a state in which a deficiency ofenergy, protein and/or other nutrients causesmeasurable adverse effects on tissue/body form,
composition, function or clinical outcome 94 (inthese guidelines we do not use the term to coverexcess nutrient provision). It is both a cause anda consequence of ill-health and is common in theUK. Since malnutrition increases a patient’svulnerability to ill-health, providing nutritionsupport to patients with malnutrition shouldimprove outcomes but decisions on the mosteffective and safe means to do so are complex.Currently, knowledge of the causes, effects andtreatment of malnutrition amongst UK healthprofessionals is poor. Guidelines are thereforeneeded to emphasise the following:
1. Malnutrition is common - many people whoare unwell in hospital or the community, arelikely to eat and drink less than they need. Thisimpairment of food and fluid intake may beshort-lived as part of an acute illness, orprolonged if there are chronic medical or socialproblems. If impaired food intake persists foreven a few days, a patient can becomemalnourished to a degree that may impairrecovery or precipitate other medical problems.This is especially true if the patient wasmalnourished before they became unwell dueto other longstanding medical or psycho-socialproblems, or a generally poor diet. Tocompound any disease related reduction infood intake, many patients also have no helpwith obtaining or preparing meals when theyare ill at home, while those in hospital mayhave further problems relating to poorstandards of catering, inappropriate or
interrupted meal times, incorrect foodconsistencies, and inappropriate eating aidsand/or staff to help them eat and drink for
themselves. The ‘Better Hospital Food’248 and
the ‘Protected Mealtimes’249 plans are welcomegovernment initiatives which try to improve theprovision of hospital meals and snacks.
2. Malnutrition increases vulnerability to ill-health - The consequences of malnutritioninclude vulnerability to infections, delayedwound healing, impaired function of heartand lungs, muscle weakness and
depression353. As a consequence people whoare malnourished consult their generalpractitioners (GPs) more frequently, go tohospital more often for longer periods, andhave higher complication and mortality ratesfor similar conditions. If poor dietary intakepersists for weeks, the resulting malnutritionmay be life-threatening in itself.
3. Decisions on providing nutrition support arecomplex - Although it is clear that clinicaloutcomes in malnourished groups are poorcompared to the better nourished (e.g.malnourished surgical patients havecomplication rates 2-3 times higher than theirbetter nourished counterparts), the indicationsfor active nutrition support using dietarysupplementation, enteral tube feeding orparenteral nutrition are debatable. Whenindividuals are unable or unlikely to meet themajority of their nutrient needs for prolongedperiods (e.g. patients with dysphagia orintestinal failure) the need for appropriatesupport is necessary unless there are concernsaround ethical issues. However, if nutritionalintake is closer to meeting a patient’s needs or
INTRODUCTION AND METHODS 27
1. Introduction and methods
NUTRITION SUPPORT IN ADULTS28
the likely period of impaired intake isuncertain, decisions on providing nutritionsupport and the best means to do so are moredifficult with multiple criteria for choosingoral, enteral or parenteral modalities whichvary with both individual patient needs andthe clinical expertise available to ensure thatany intervention can be undertaken safely.
4. Understanding of malnutrition and nutritionsupport amongst many healthcareprofessionals is poor – The many difficultiesrelating to the need and best mode ofnutrition support are compounded by a lack ofknowledge about malnutrition and itstreatment amongst many healthcareprofessionals. There has been little emphasison nutrition education in eitherundergraduate medical or nursing courses.This has led to poor recognition of bothnutritional risks and the dangers of poorlymanaged nutrition support. Along with thelack of agreed national guidelines, this hasalso led to wide variation in nutritional care
standards. Heyland et al 151 highlighted thedifference between evidence in nutritionalhealthcare and practice when stating that:
‘Approximately 30-40% of patients do notreceive care according to present scientificevidence and about 20-25% of care is notneeded or is potentially harmful’.
The objective of these guidelines is therefore toimprove the practice of nutrition support byproviding guidance to assist all healthcareprofessionals to correctly identify patients inhospital or the community who requirenutritional intervention, and to help themchoose and deliver the most appropriate form ofnutrition support at the appropriate time. Assuch, they are in keeping with other recentpublications highlighting the importance ofgood nutritional care e.g. the Department of
Health’s Essence of Care document82, the WelshAssembly Government’s Fundamentals of
Care370 and the Royal College of Physicians’report ‘Nutrition and patients: a doctor’s
responsibility’297. They are also about improving
people’s quality of life by making them feelbetter through adequate nutrition, and theyhave been developed with a significantcontribution from patient representatives.
11..22 WWhhaatt iiss aa gguuiiddeelliinnee??
Guidelines are recommendations for the care ofindividuals in specific clinical conditions orcircumstances – from prevention and self-carethough primary and secondary care to morespecialised services. Clinical guidelines are basedon the best available evidence, and are producedto assist healthcare professionals and patientsmake informed choices about appropriatehealthcare. While guidelines assist the practice ofhealthcare professionals, they do not replace theirknowledge and skills.
Clinical guidelines for the NHS in England andWales are produced as a response to a request fromthe Department of Health and the Welsh AssemblyGovernment. They select topics for guidelinedevelopment and before deciding whether to refer aparticular topic to the National Institute for Healthand Clinical Excellence (NICE) they consult with therelevant patient bodies, professional organisationsand companies. Once a topic is referred, NICE thencommissions one of seven National CollaboratingCentres to produce a guideline. The CollaboratingCentres are independent of government andcomprise partnerships between a variety ofacademic institutions, health profession bodies and patient groups.
11..33 RReemmiitt ooff tthhee gguuiiddeelliinnee
The following remit was received from theDepartment of Health and National Assembly forWales in as part of NICE’s 7th wave programmeof work:“To prepare a guideline on appropriate methodsof feeding people whoare still capable of deriving at least some of theirnutritional requirements by conventional feedingand/orhave difficulty in swallowingincluding the use of nutritional supplements andenteral and parenteral nutrition methods.”

INTRODUCTION AND METHODS 29
11..44 WWhhaatt tthhee gguuiiddeelliinnee ccoovveerrss
These guidelines cover most aspects of nutritionsupport in adult patients (>18 years) who areeither malnourished or are at ‘risk’ of malnutrition.In some cases specific guidance related topatients in specific care settings or with specificdiseases has been provided but in general theguidance is applicable to patients whatever theirsetting (hospital or community) or disease. Theguideline therefore includes:
• Information on the prevalence of malnutritionand the benefits of good nutrition
• Guidance on the appropriate forums for theorganisation of nutrition support in all settings
• Guidance on who should be screened formalnutrition and when, along with the criteriafor consideration when assessing patients’nutritional status.
• The general indications for nutrition supporttogether with ethical and legal considerationsthat may arise.
• Guidance on the process and specialconsiderations required to prescribe nutritionsupport and details information on theimportant parameters to monitor for patientsreceiving nutrition support.
• Detailed guidance on the administration oforal, enteral and parenteral nutritionincluding; the appropriate types of access forenteral and parenteral nutrition and theoptimum mode of delivering these.
• Specific guidance on the management ofproviding nutrition support to patients withdysphagia
• Issues to consider for patients receivingenteral and parenteral nutrition support in thecommunity
• Issues arising for patients and their carers.
For more detailed information please see the fullscope of this guideline Appendix One: scope..
11..55 WWhhaatt tthhee gguuiiddeelliinnee ddooeess nnoott ccoovveerr
The guideline does not provide guidance on:
• The provision of normal food and drinks
• Patients requiring specific specialisttherapeutic or maintenance nutrition regimensin the context of diseases such as inbornerrors of metabolism, diabetes and chronicrenal or liver failure.
• Pregnant women, since the nutritionaldemands on the mother and baby requirespecialist considerations
• Patients with eating disorders. This is covered
in the NICE guideline on eating disorders244.
• People who are obese. This will be covered bythe NICE obesity guidelines expected to bepublished in 2007.
• Primary prevention of malnutrition in healthyindividuals in the general population.
• Children and adolescents under the age of 18 years.
• The guideline also provides norecommendations on:
• The suitability of individually named oralsupplements or enteral and parenteralnutrition solutions.
• The use of novel substrates such as glutamineor arginine (we are aware that there is someevidence suggesting potential benefit fromthe use of these substrates and believe thatthis should be addressed by NICE in theformat of a health technology assessment).
• Types of tubing and receptacles used forenteral and parenteral nutrition support.
• The management of infections and infectioncontrol related to enteral and parenteralnutrition support although reference is madeto the existing NICE guidance on InfectionControl where appropriate.

11..66 WWhhoo tthhee gguuiiddeelliinnee iiss ffoorr
This guideline does not include recommendationscovering every detail of nutrition support. Insteadthey seek to ensure that all healthcare professionalsconsider every patient’s nutritional status and thelength of time the patient has or will have aninadequate food intake, whatever the disease stateor care setting. They are therefore relevant to allhealthcare professionals who come into contact withpatients, as well as to the patients themselves andtheir carers. It is also expected that the guideline willalso be of value to those involved in clinicalgovernance in both primary and secondary care tohelp ensure that arrangements are in place toidentify, treat and audit malnutrition and the use ofnutrition support within their organisations.
11..77 WWhhoo ddeevveellooppeedd tthhee gguuiiddeelliinnee??
A multidisciplinary Guideline Development Group(GDG) comprising professional group members andconsumer representatives of the main stakeholdersdeveloped this guideline (see Guideline DevelopmentGroup Membership and acknowledgements).
The National Institute for Health and ClinicalExcellence funds the National Collaborating Centrefor Acute Care and thus supported the developmentof this guideline. The GDG was convened by theNational Collaborating Centre for Acute Care (NCC-AC) and chaired by Dr Mike Stroud in accordancewith guidance from the National Institute for Healthand Clinical Excellence (NICE).
The Group met every 6-8 weeks during thedevelopment of the guideline. At the start of theguideline development process all GDG members’interests were recorded on a standard declarationform that covered consultancies, fee-paid work,share-holdings, fellowships and support from thehealthcare industry. At all subsequent GDGmeetings, members declared arising conflicts ofinterest which were recorded.
Staff from the NCC-AC provided methodologicalsupport and guidance for the development process.They undertook systematic searches, retrieval andappraisal of the evidence and drafted the guideline.The Glossary to the guideline contains definitions ofterms used by staff and the GDG.
11..88 MMeetthhooddoollooggyy
11..88..11 OOuuttlliinnee ooff mmeetthhooddss uusseedd
The guideline was commissioned by NICE. Theguideline development process involved several stepsand was developed in accordance with the guidelinedevelopment process outlined in Guidelinedevelopment methods: information for National
Collaborating Centres and guideline developers245 .
11..88..22 DDeevveellooppmmeenntt ooff cclliinniiccaall qquueessttiioonnss
The Guideline Development Group proposed a listof clinical questions (Appendix Two) related to theinitiation and administration of oral, enteral andparenteral nutrition support. With the exception ofthe nutrition screening, monitoring and refeedingsyndrome questions, the remaining questions weredeveloped to investigate the benefit of one type ormode of intervention with another.
11..88..33 TTyyppeess ooff ssttuuddyy iinntteerrvveennttiioonnss
The Guideline Development Group agreed on thedefinition of terms and the inclusion and exclusioncriteria for oral, enteral and parenteral interventions.These were included in the search strategies andconsidered throughout the process of systematicreviewing.
11..88..44 TTyyppeess ooff ssttuuddyy ppooppuullaattiioonn
The search strategies were not restricted tospecific patient/population groups since the GDGwished to determine the likely benefit or risks ofnutrition support to all patient groups. Papers onchildren, pregnant mothers and people witheating disorders were excluded since they wereout of the scope of this guideline.)
11..88..55 TTyyppeess ooff oouuttccoommeess
The Guideline Development Group requested thatall outcomes should be recorded, with theexception of biochemical outcomes which werenot clearly associated with clinical benefit (forexample changes in nitrogen balance or plasmaprotein concentrations).
11..88..66 TTyyppeess ooff ssttuuddiieess
Study design was restricted to systematic reviews,meta-analyses of randomised controlled trials andrandomised controlled trials. No other study designs
NUTRITION SUPPORT IN ADULTS30
were considered because of the potential biasassociated with observational study designs. Also, the wide inclusion criteria agreed forpopulations, interventions and outcomes would havemade the task of including observational studiesin the systematic reviews too great for the resources available.
11..88..77 LLiitteerraattuurree sseeaarrcchh
A literature review was conducted to identify andsynthesise relevant evidence from the publishedliterature. Three main search strategies weredeveloped for oral, enteral and parenteral nutritioninterventions. Four other search strategies weredeveloped for nutritional screening, monitoring,dysphagia and patient issues.
Search filters to identify systematic reviews (SRs) andrandomised controlled trials (RCTs) were applied tothe search strategies. No language restrictions wereapplied to the search; however, foreign languagepapers were not requested or reviewed.
The following databases were included in theliterature search:
• The Cochrane Library up to 2005 (Issue 1)
• Medline (Dialog Datastar) 1966-2005 (week)
• Embase (Dialog Datastar) 1980-2005 (week)
• Cinahl (Dialog Datastar) 1982-2005
• Allied & Complementary Medicine (DialogDatastar) 1985-2005
• British Nursing Index (Dialog Datastar) 1994-2005
Although literature searching was started in 2003update searches were run for each search toensure all reviews included literature up to thesame cut-off date. Therefore, each database was
searched from its start date up to 3rd March2005. Papers identified after this date were notconsidered, with the exception of the draft BAPENreport on ‘The cost of malnutrition in the UK andthe economic case for the use of oral supplements
(ONS) in adults’91, which the GDG had beenanticipating but which was received shortly afterthe cut-off date. Search strategies can be foundin Appendix Three.
There was no systematic attempt to search for allthe ‘grey literature’ (conferences, abstracts, thesesand unpublished literature). We searched forguidelines and reports from relevant websites,including the following listed below. Bibliographiesof identified reports and guidelines were alsochecked to identify relevant literature.
• National Institute for Health and ClinicalExcellence (NICE) (www.nice.org.uk)
• National electronic Library for Health (NeLH)(http://www.nelh.nhs.uk/)
• National Institutes of Health ConsensusDevelopment Program (consensus.nih.gov)
• New Zealand Guidelines Development Group(NZGG) (http://www.nzgg.org.nz/)
• Scottish Intercollegiate Guideline Network(SIGN) (www.sign.ac.uk)
• US National Guideline Clearing House(www.guidelines.gov)
• Web sites of relevant members of theGuidelines International Network(http://www.g-i-n.net/)
• Google (www.google.com)
11..88..88 SSttuuddyy sseelleeccttiioonn
One reviewer independently scanned the titlesand abstracts of the literature searches. Fullpublications were obtained for any studiesconsidered relevant or where there wasinsufficient information from the title andabstract to make a decision.
11..88..99 DDaattaa eexxttrraaccttiioonn aanndd qquuaalliittyy aasssseessssmmeenntt
A team of reviewers individually applied theinclusion/exclusion criteria to determine allpotentially relevant studies. The reviewers alsoassessed the quality of eligible studies byreferring to the SIGN quality checklists forsystematic reviews/meta-analyses andrandomised control trials. Of all the relevantstudies data on the type of population,intervention, comparator and outcomes wassummarised onto evidence tables (AppendixFour). In the instances where there was missing
INTRODUCTION AND METHODS 31

data we did not attempt to contact the authorsbecause of limited resources.
11..88..1100 MMeettaa--aannaallyyssiiss
For some of our results we were able to produce ameta-analysis using Review Manager version 4.2,the software used by the Cochrane Collaboration.For some studies we approximated the meanlength of stay using the median and estimatedthe standard deviation as a weighted mean of thestandard deviations of the other studies.
11..88..1111 AAbbsseennccee ooff lliitteerraattuurree
The recommendations in this guideline have beensystematically developed with as much scientificrigour as possible. However for a number of theclinical questions there was an absence of RCTevidence either because the clinical questions didnot lend themselves to controlled trials andsystematic reviewing, or for which there were toofew trials identified to make substantiverecommendations. Invariably, we needed to useadditional approaches such as surveys orinformal/formal consensus development to assistwith some areas of the guidance. Below is adescription of the areas of the guideline thatrequired additional approaches in addition tosystematic searching and reviewing of RCTs.
Nutritional screening: because of weaknesses inthe methodologies and designs of the studiesidentified, no firm conclusions could be made. Amodified Delphi approach for consensusdevelopment was used, consisting of two roundsof Delphi questionnaire surveys and then anominal group technique meeting. See ScreeningChapter 4.7 Consensus development methods.
Indications for oral, enteral and parenteralinterventions: the guidance could not be derivedfrom controlled trials thus the recommendationswere drafted by the technical team at the NCC-AC and modified and agreed by informalconsensus with the GDG.
Ethical and Legal issues: The brief importantcomments on the ethical and legal issues ofnutrition support contained within theseGuidelines were derived from GDG expertise andprevious expert treatises on these topics
Dysphagia: No RCT’s were found to provideguidance on options of nutrition support forpatients with Dysphagia. A specialist sub group ofspeech and language therapists’ with a specialinterest in dysyphagia was convened to developand propose suitable recommendations. Thesewere agreed by informal consensus with the GDG.
Prescription of nutrients: recommendations wereproposed by GDG members with relevantexpertise and agreed by informal consensusamong all GDG members.
Refeeding syndrome: recommendations wereformulated by members of the group based onprevious published reviews and their ownexpertise, and agreed by informal consensusamong all GDG members.
Monitoring: The GDG were sent questionnaireselectronically asking them to determine how oftencertain nutritional and biochemical parametersare and should be measured. Two GDG memberswith expertise in this area considered theoutcomes of the survey and proposed theguidance/recommendations which the GDGagreed by informal consensus.
Nutritional assessment: two GDG members withexpertise in this area proposed theguidance/recommendations to the whole GDGwho agreed on these by informal consensus.
Nutrition support teams: both randomised andnon-randomised trials were considered for thissection as some observational study designs werealso appropriate for this question.
Patients’ and carers’ views: We sent lettersrequesting evidence on patients’ and carers’ viewsof nutrition support to twenty stakeholders. A literature search was conducted to identifyrelevant evidence for any study design. The following databases were included:
• Medline (1951-2005)
• Embase (1980-2005)
• Cinahl (1982-2005)
Three sub-group meetings with patientrepresentatives on the GDG were held. Patient
NUTRITION SUPPORT IN ADULTS32

representatives were involved in the sifting of theabstracts retrieved from the literature search. A systematic reviewer summarised the evidencefrom the studies. The text was included indiscussion with patient representatives at sub-group meetings and in consultation with GDGmembers at GDG meetings.
11..99 HHiieerraarrcchhyy ooff cclliinniiccaall eevviiddeennccee
There are many different methods of ranking theevidence and there has been considerable debateabout what system is best. A number ofinitiatives are currently under way to find aninternational consensus on the subject, but until adecision is reached on the most appropriatesystem for the NICE guidelines, the Instituteadvises the National Collaborating Centres to usethe system for evidence shown in Table 1.
TTaabbllee 11:: LLeevveellss ooff eevviiddeennccee ffoorr iinntteerrvveennttiioonn ssttuuddiieess((rreepprroodduucceedd wwiitthh ppeerrmmiissssiioonn ooff tthhee SSccoottttiisshhIInntteerrccoolllleeggiiaattee GGuuiiddeelliinneess NNeettwwoorrkk))
LLeevveell ooff eevviiddeennccee TTyyppee ooff eevviiddeennccee
1++ High-quality meta-analyses, systematic reviewsof RCTs, or RCTs with a very low risk of bias
1+ Well-conducted meta-analyses, systematicreviews of RCTs, or RCTs with a low risk of bias
1- Meta-analyses, systematic reviews of RCTs, orRCTs with a high risk of bias
2++ High-quality systematic reviews of case-controlor cohort studies
High-quality case-control or cohort studies with a very low risk of confounding, bias, orchance and a high probability that therelationship is causal
2+ Well-conducted case-control or cohort studies with a low risk of confounding, bias, orchance and a moderate probability that therelationship is causal
2- Case-control or cohort studies with a high risk of confounding bias, or chance and a significantrisk that the relationship is not causal
3 Non-analytic studies (for example, case reports,case series)
4 Expert opinion
The ranking system described above coversstudies of treatment effectiveness and is lessappropriate for studies reporting diagnostic testsof accuracy.
11..1100 HHeeaalltthh eeccoonnoommiiccss mmeetthhooddss
It is important to investigate whether healthservices are both clinically effective and cost-effective (that is, value for money). If a particulardiagnostic or treatment strategy was found to yieldlittle health gain relative to the resources used, thenit could be advantageous to re-deploy resources toother activities that yield greater health gain.
To assess the cost-effectiveness of eachrecommendation, a comprehensive systematicreview of the economic literature was conducted.In addition an original cost-effectiveness analysiswas performed for malnutrition screening.
The primary criteria applied for an intervention tobe considered cost-effective were either:
a) the intervention dominated other relevantstrategies (that is, it is both less costly interms of resource use and more clinicallyeffective compared with the other relevantalternative strategies); or
b) the intervention cost less than £20,000 perquality-adjusted life-year (QALY) gainedcompared with the next best strategy (andcompared with best supportive care).Between £20,000 and £30,000 per QALY,judgments about the acceptability of theintervention as an effective use of NHSresources have to make more explicit referenceto such factors as the degree of uncertaintysurrounding the calculation of cost-effectiveness, the innovative nature of theintervention and the particular features of thecondition and the population receiving it.
11..1100..11 LLiitteerraattuurree rreevviieeww ffoorr hheeaalltthh eeccoonnoommiiccss
We obtained published economic evidence from asystematic search of the following databases:
• Medline (Dialog Datastar) (1966-2005)
• Embase (Dialog Datastar) (1980-2005)
INTRODUCTION AND METHODS 33

• Health Economic Evaluations Database (HEED)
• NHS Economic Evaluations Database (NHS EED)
For those clinical areas we reviewed, theinformation scientists used a similar searchstrategy as used for the review of clinicalevidence. However, an economics filter was usedin the place of a systematic review orrandomised controlled trial filter. Althoughliterature searching was started in 2003 updatesearches were run for each search to ensure allreviews included literature up to the same cut-off date. Therefore, each database wassearched from its start date up to 3rd March2005. Papers identified after this date werenot considered. Search strategies can be foundin Appendix Three.
Each search strategy was designed to find anyapplied study estimating the cost or cost-effectiveness of some aspect of nutritionsupport. A health economist reviewedabstracts. Relevant references in thebibliographies of reviewed papers were alsoidentified and reviewed.
Given the diversity of economic studies, it wasnot possible to determine a general exclusioncriterion based on study quality. Hence, allstudies were included in the evidence tablesand study quality and applicability arediscussed in the review. Papers were onlyexcluded from the evidence tables and review if:
• The study did not contain any original data oncost or cost-effectiveness (i.e. it was a reviewor a clinical paper).
• The analysis was not incremental and was notdescribed adequately to allow incrementalanalysis (so studies reporting only averagecost-effectiveness ratios [the cost for onetreatment divided by the health outcome]were excluded unless they provided data toallow the calculation of incremental cost-effectiveness ratios [the change in costdivided by the change in health outcome]).Only incremental cost-effectiveness ratios caninform us about value for money.
• Cost analyses were excluded if the resultswere not presented in a way that would allowthe incremental cost per patient to beextracted or derived. The total hospital cost isdifficult to interpret unless we know howmany patients are being treated.
For one topic – nutrition support teams – it wasdecided to exclude studies which had only asingle cohort and used conjecture to assess theincremental cost. These studies were excludedsince there was other evidence that was deemedto be more rigorous – the included studies allcompared two cohorts, and one of them was arandomised controlled trial.
Included papers were reviewed by a healtheconomist. In the text, costs have beenconverted to £ sterling using the relevantpurchasing power parity for the study year. Inthe evidence tables costs are reported as givenin the paper. However, where costs were in acurrency other than pounds sterling, US dollars or euros, the results were converted topounds sterling.
Each study was categorised as one of thefollowing: cost analysis, cost-effectivenessanalysis, cost-utility analysis or costconsequences analysis (see glossary). Many ofthe studies in this review were labelled ‘costconsequences analyses’ because they presentmany different health outcomes (in addition tocost) without a single overall measure healthgain. Often these studies report complications.Where complications averted appears to be themain clinical outcome we have estimated cost-effectiveness by calculating the incrementalcost per complication averted. We did not findany ‘cost benefit analyses’ (studies that put amonetary value on health gain).
11..1100..22 CCoosstt--eeffffeeccttiivveenneessss mmooddeelllliinngg
Screening was selected for original economicanalysis because it was likely that therecommendations under consideration wouldsubstantially change clinical practice in the NHSand have important consequences for resource use.
NUTRITION SUPPORT IN ADULTS34

The details of the model are reported in chapter 4and Appendix Five: Cost-Effectiveness Analysis ofMalnutrition Screening. The following generalprinciples were adhered to:
• The GDG was consulted during theconstruction and interpretation of the model.
• The model was based on the best evidencefrom the systematic review.
• Model assumptions were reported fully andtransparently.
• The results were subject to thoroughsensitivity analysis and limitations discussed.
• Costs were calculated from a health servicesperspective.
11..1111 FFoorrmmiinngg aanndd ggrraaddiinngg tthhee rreeccoommmmeennddaattiioonnss
NICE guideline recommendations are gradedaccording to the strength of the supportingevidence, which is assessed from the design ofeach study (see Table 1). The grading systemcurrently used is presented in Table 2.
The Guideline Development Group was presentedwith summaries (text and evidence tables) of thebest available research evidence to answer theclinical questions. Recommendations were basedon and explicitly linked to the evidence thatsupported them. With the exception of thenutrition screening recommendations the Groupworked on an informal consensus basis toformulate and grade recommendations accordingto the level of evidence upon which they werebased. In the final stages of the guidelinedevelopment process, the recommendations werefurther revised at a number of meetings wherethe GDG members agreed by informal theconsensus the final wording and meaning of therecommendations as a round table discussion.
TTaabbllee 22:: GGrraaddiinngg ooff rreeccoommmmeennddaattiioonnss
Grade Evidence
A • At least one meta-analysis, systematic review,or RCT rated as 1++, and directly applicable tothe target population, or
• A systematic review of RCTs or a body ofevidence consisting principally of studies ratedas 1+, directly applicable to the targetpopulation, and demonstrating overallconsistency of results
• Evidence drawn from a NICE technologyappraisal
B • A body of evidence including studies rated as2++, directly applicable to the targetpopulation, and demonstrating overallconsistency of results, or
• Extrapolated evidence from studies rated as1++ or 1+
C • A body of evidence including studies rated as2+, directly applicable to the target populationand demonstrating overall consistency ofresults, or
• Extrapolated evidence from studies ratedmmas 2++
D • Evidence level 3 or 4, or
• Extrapolated evidence from studies rated as2+, or
• Formal consensus
D (GPP) A good practice point (GPP) is a recommendation forbest practice based on the experience of theGuideline Development Group
The usefulness of a classification system basedsolely on the level of evidence has beenquestioned because it does not take intoconsideration the importance of therecommendation in changing practice andimproving patient care. It is worth noting thatNICE is currently assessing the best way ofpresenting recommendations for future guidelines.
INTRODUCTION AND METHODS 35

11..1122 SSppeecciiffiicc pprroobblleemmss wwiitthh eevviiddeennccee rreellaattiinngg ttoo tthhee ddeevveellooppmmeenntt ooff nnuuttrriittiioonn ssuuppppoorrtt gguuiiddeelliinneess
Literature searching, appraising the evidence anddeveloping recommendations for this guidelineproved to be particularly challenging. In part, thiswas due to a shortage of randomised controlledtrials relating to some of the clinical questions,but the GDG also observed problems with thetypes of patients entered into many of theselected controlled trials. Providing adequatenutrition is usually seen as a part of basic care,and this creates obstacles to good qualityresearch in nutrition support. For example,although it is obvious that inadequate provisionof nutrition for prolonged periods eventually leadsto death, no randomised trials support thisstatement and any recommendation that patientsshould not be allowed to die of starvation istherefore grade D.
Other fundamental problems with availableevidence include:
a) In trials of nutritional intervention it is oftenneither feasible nor ethical to have ‘nonutrition’ as the control.
b) Patients who are malnourished and thereforeeligible to be recruited for trials of nutritionsupport have very variable diagnoses andcome from a wide variety of settings. Trialpopulations are therefore very heterogeneouswith wide potential variation in outcomes ofinterest. Large scale studies are thereforeneeded to demonstrate any potential benefitson outcome but most nutritional trials havebeen small.
c) When performing trials on invasive means ofnutrition support such as enteral andparenteral nutrition, it is usually consideredunethical to randomise patients who have an‘undoubted’ need for such support. Trialstherefore recruit patients who are at lowernutritional risk than those conventionally fedby these methods and so their results may beinapplicable to normal clinical practice.
d) Developments in the formulations anddelivery of enteral and parenteral nutrition
support and consequent reductions in riskhave made many older studies less relevant.For instance, in recent years it has beenrecognised that too much additional nutrientprovision can sometimes be more harmfulthan no nutrition support, yet much of theliterature pre-dates this change in thinking.
The GDG also encountered methodologicalproblems with the available nutritional research,including:
a) Significant heterogeneity in the outcomesreported e.g. for one type of intervention, 5separate studies may use 5 different indicatorsto report change in nutritional status.
b) Lack of information on the period prior tostarting nutrition support despite the fact thatthe duration and intensity of starvation beforeintervention is clearly pertinent to any outcome.
c) Study periods which were often too short todetermine the true effect of any intervention(e.g. reporting change in body weight twoweeks after prescribing a oral nutritionalsupplement may not be long enough toestablish whether the patient benefits in thelong term).
d) Weak characterisation of patient populationsin terms of underlying diagnosis, illnessseverity or degree of malnutrition.
e) Lack of information on the amount of feedactually received by patients and/ or the widevariation in the amount received (a particularweakness of older enteral feeding studies).
f) The presence of many potentially confoundingissues when reporting outcomes attributed byauthors to nutritional intervention in smalltrials (e.g. infection rates and mortality).
g) The predominance of evidence from limitedacute or chronic care settings with completeabsence of evidence from other settings makesgeneralisation of conclusions difficult.
In view of the above, many questions related tonutrition support may be better addressed bystudy designs other than RCTs but the broad
NUTRITION SUPPORT IN ADULTS36

scope of these Guidelines and the difficulties withhandling the biases associated with observationalstudies prevented the GDG from formallysearching for sources of non-RCT evidence. In theabsence of evidence from Rat’s many of theclinical questions have therefore been addressedusing expert opinion and consensus techniques.
11..1133 PPaattiieenntt--cceennttrreedd ccaarree
This guideline offers best practice advice on thecare of adults who are malnourished or at risk ofmalnutrition.
Treatment and care should take into accountpatients’ needs and preferences. People withmalnutrition should have the opportunity to makeinformed decisions about their care andtreatment, in partnership with their healthprofessionals. When patients do not have thecapacity to make decisions, healthcareprofessionals should follow the Department ofHealth guidelines – Reference guide to consentfor examination or treatment (2001) (availablefrom www.dh.gov.uk).
Good communication between healthcareprofessionals and patients is essential. It shouldbe supported by evidence-based writteninformation tailored to the patient’s needs.Treatment and care, and the information patientsare given about it, should be culturallyappropriate. It should also be accessible to peoplewith additional needs such as physical, sensory orlearning disabilities, and to people who do notspeak or read English.
Carers and relatives should have the opportunityto be involved in decisions about the patient’scare and treatment, if the patient agrees to this.Carers and relatives should also be given theinformation and support they need.
Recommendations in this guideline apply to allpatients with malnutrition or at risk ofmalnutrition, whether they are in hospital or athome. Good coordination between the hospitaland the home or community is needed whenpatients are transferred between settings.
11..1144 SSuummmmaarryy ooff tthhee rreeccoommmmeennddaattiioonnss
11..1144..11 KKeeyy pprriioorriittiieess ffoorr iimmpplleemmeennttaattiioonn
The following recommendations have beenselected from the full list (section 1.14.2) aspriorities for implementation.
1.14.1.1 Key clinical priorities
• Screening for malnutrition and the risk ofmalnutrition should be carried out by healthcareprofessionals with appropriate skills andtraining. [Chapter 4]
• All hospital inpatients on admission and alloutpatients at their first clinic appointmentshould be screened. [Chapter 4] Screeningshould be repeated weekly for inpatients andwhen there is clinical concern for outpatients.People in care homes should be screened onadmission and when there is clinical concern.[Chapter 4]
• Hospital departments who identify groups ofpatients with low risk of malnutrition may optout of screening these groups. Opt-outdecisions should follow an explicit process viathe local clinical governance structureinvolving experts in nutrition support.[Chapter 4]
• Nutrition support should be considered inpeople who are malnourished, as defined byany of the following:
– a body mass index (BMI) of less than 18.5kg/m2
– unintentional weight loss greater than10% within the last 3–6 months
– a BMI of less than 20 kg/m2 andunintentional weight loss greater than 5%within the last 3–6 months. [Chapter 5]
• Nutrition support should be considered inpeople at risk of malnutrition, defined asthose who have:
– eaten little or nothing for more than 5days and/or are likely to eat little ornothing for 5 days or longer
INTRODUCTION AND METHODS 37
– a poor absorptive capacity and/or highnutrient losses and/or increasednutritional needs from causes such ascatabolism. [Chapter 5]
• Healthcare professionals should consider usingoral, enteral or parenteral nutrition support,alone or in combination, for people who areeither malnourished or at risk of malnutrition, asdefined above. Potential swallowing problemsshould be taken into account.
1.14.1.2 Key organisational priorities
• All healthcare professionals who are directlyinvolved in patient care should receiveeducation and training, relevant to their post,on the importance of providing adequatenutrition. [Chapter 3]
• Healthcare professionals should ensure thatall people who need nutrition support receivecoordinated care from a multidisciplinaryteam . [Chapter 3]
• All acute hospital trusts should employ atleast one specialist nutrition support nurse.[Chapter 3]
• All hospital trusts should have a nutritionsteering committee working within the clinicalgovernance framework. [Chapter 3]
11..1144..22 CClliinniiccaall pprraaccttiiccee rreeccoommmmeennddaattiioonnss
11..1144..22..11 OOrrggaanniissaattiioonn ooff nnuuttrriittiioonn ssuuppppoorrtt iinn hhoossppiittaall aanndd tthhee ccoommmmuunniittyy
All healthcare professionals who are directly involvedin patient care should receive education and training,relevant to their post, on the importance of providingadequate nutrition. [[DD((GGPPPP))]]
Education and training should cover:
• nutritional needs and indications for nutritionsupport
• options for nutrition support (oral, enteral andparenteral)
• ethical and legal concepts
• potential risks and benefits
• when and where to seek expert advice. [[DD((GGPPPP))]]
Healthcare professionals should ensure that careprovides:
• food and fluid of adequate quantity andquality in an environment conducive to eating
• appropriate support, for example, modifiedeating aids, for people who can potentiallychew and swallow but are unable to feed themselves. [[DD((GGPPPP))]]
Healthcare professionals should ensure that allpeople who need nutrition support receive
coordinated care from a multidisciplinary team1.[[DD((GGPPPP))]]
All acute hospital trusts should have amultidisciplinary nutrition support team which mayinclude: doctors (for example gastroenterologists,gastrointestinal surgeons, intensivists or others witha specific interest in nutrition support), dietitians, aspecialist nutrition nurse, other nurses, pharmacists,biochemistry and microbiology laboratory supportstaff, and other allied healthcare professionals (forexample, speech and language therapists). [[DD((GGPPPP))]]
All hospital trusts should have a nutrition steeringcommittee working within the clinical governanceframework. [[DD((GGPPPP))]]
Members of the nutrition steering committee shouldbe drawn from trust management, and includesenior representation from medical staff, catering,nursing, dietetics, pharmacy and other healthcareprofessionals as appropriate, for example, speechand language therapists. [[DD((GGPPPP))]]
All acute hospital trusts should employ at leastone specialist nutrition support nurse. [[DD((GGPPPP))]]
The specialist nutrition support nurse should workalongside nursing staff, as well as dietitians andother experts in nutrition support, to:
• minimise complications related to enteral tubefeeding and parenteral utrition
• ensure optimal ward-based training of nurses
• ensure adherence to nutrition support protocols
• support coordination of care between thehospital and the community. [[DD((GGPPPP))]]
NUTRITION SUPPORT IN ADULTS38
1 The composition of this team may differ according to setting and local arrangements.

1.14.2.2 Screening for malnutrition and the risk
of malnutrition in hospital and the community
Screening for malnutrition and the risk ofmalnutrition should be carried out by healthcareprofessionals with appropriate skills and training.[[DD((GGPPPP))]]
All hospital inpatients on admission and alloutpatients at their first clinic appointmentshould be screened. Screening should be repeatedweekly for inpatients and when there is clinicalconcern for outpatients. [[DD((GGPPPP))]]
Hospital departments who identify groups ofpatients with low risk of malnutrition may opt outof screening these groups. Opt-out decisionsshould follow an explicit process via the localclinical governance structure involving experts innutrition support. [[DD((GGPPPP))]]
People in care homes should be screened onadmission and when there is clinical concern.[[DD((GGPPPP))]]
Screening should take place on initial registrationat general practice surgeries and when there is
clinical concern2. Screening should also beconsidered at other opportunities (for example,health checks, flu injections). [[DD((GGPPPP))]]
Screening should assess body mass index (BMI)3
and percentage unintentional weight loss andshould also consider the time over which nutrientintake has been unintentionally reduced and/or thelikelihood of future impaired nutrient intake. TheMalnutrition Universal Screening Tool (MUST), forexample, may be used to do this. [[DD((GGPPPP))]]
1.14.2.3 Indications for nutrition support in hospital
and the community
Nutrition support should be considered in peoplewho are malnourished, as defined by any of thefollowing:
• a BMI of less than 18.5 kg/m2
• unintentional weight loss greater than 10%within the last 3–6 months
• a BMI of less than 20 kg/m2 andunintentional weight loss greater than,5% within the last 3–6 months. [[DD((GGPPPP))]]
Nutrition support should be considered in peopleat risk of malnutrition who, as defined by any ofthe following:
• have eaten little or nothing for more than 5days and/or are likely to eat little or nothingfor the next 5 days or longer
• have a poor absorptive capacity, and/or havehigh nutrient losses and/or have increasednutritional needs from causes such ascatabolism. [[DD((GGPPPP))]]
Healthcare professionals should consider usingoral, enteral or parenteral nutrition support, aloneor in combination, for people who are either
malnourished4 or at risk of malnutrition5.Potential swallowing problems should be takeninto account. [[DD((GGPPPP))]]
Healthcare professionals involved in starting orstopping nutrition support should:
• obtain consent from the patient if he or she is competent
• act in the patient’s best interest if he or she isnot competent to give consent
• be aware that the provision of nutrition supportis not always appropriate. Decisions onwithholding or withdrawing of nutrition support require a consideration of both ethicaland legal principles (both at common law andstatute including the Human Rights Act 1998).
When such decisions are being made guidance
issued by the General Medical Council6 and the
Department of Health7 should be followed. [[DD((GGPPPP))]]
Healthcare professionals should ensure thatpeople having nutrition support, and their carers,are kept fully informed about their treatment.They should also have access to appropriateinformation and be given the opportunity todiscuss diagnosis and treatment options. [[DD((GGPPPP))]]
INTRODUCTION AND METHODS 39
2Clinical concern includes, for example, unintentional weight loss, fragile skin, poor wound healing, apathy, wasted muscles, poor appetite, alteredtaste sensation, impaired swallowing, altered bowel habit, loose fitting clothes or prolonged intercurrent illness. 3BMI is weight (kg)/height(m2) (weight in kilograms divided by height in metres squared).4Malnourished: BMI <18.5 kg/m2, unintentional weight loss >10% within the last 3-6 months, a BMI<20 kg/m2 and unintentional weight loss>5% within the last 3-6 months.5At risk of malnutrition: eaten little or nothing for more than 5 days and/or likely to eat little or nothing for the next 5 days or longer or poorabsorptive capacity, and or high nutrient losses and or increased nutritional needs from causes such as catabolism.
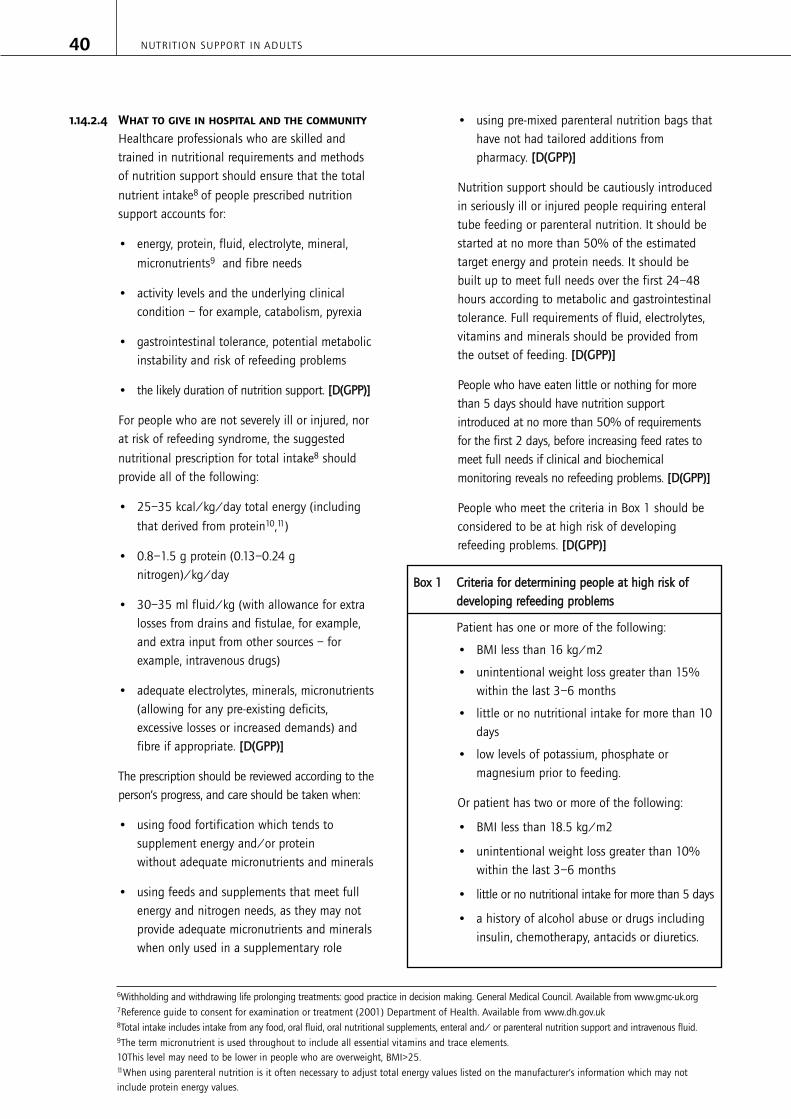
1.14.2.4 What to give in hospital and the community
Healthcare professionals who are skilled andtrained in nutritional requirements and methodsof nutrition support should ensure that the total
nutrient intake8 of people prescribed nutritionsupport accounts for:
• energy, protein, fluid, electrolyte, mineral,
micronutrients9 and fibre needs
• activity levels and the underlying clinicalcondition – for example, catabolism, pyrexia
• gastrointestinal tolerance, potential metabolicinstability and risk of refeeding problems
• the likely duration of nutrition support. [[DD((GGPPPP))]]
For people who are not severely ill or injured, norat risk of refeeding syndrome, the suggested
nutritional prescription for total intake8 shouldprovide all of the following:
• 25–35 kcal/kg/day total energy (including
that derived from protein10,11)
• 0.8–1.5 g protein (0.13–0.24 gnitrogen)/kg/day
• 30–35 ml fluid/kg (with allowance for extralosses from drains and fistulae, for example,and extra input from other sources – forexample, intravenous drugs)
• adequate electrolytes, minerals, micronutrients(allowing for any pre-existing deficits,excessive losses or increased demands) andfibre if appropriate. [[DD((GGPPPP))]]
The prescription should be reviewed according to theperson’s progress, and care should be taken when:
• using food fortification which tends tosupplement energy and/or protein without adequate micronutrients and minerals
• using feeds and supplements that meet fullenergy and nitrogen needs, as they may notprovide adequate micronutrients and mineralswhen only used in a supplementary role
• using pre-mixed parenteral nutrition bags thathave not had tailored additions frompharmacy. [[DD((GGPPPP))]]
Nutrition support should be cautiously introducedin seriously ill or injured people requiring enteraltube feeding or parenteral nutrition. It should bestarted at no more than 50% of the estimatedtarget energy and protein needs. It should bebuilt up to meet full needs over the first 24–48hours according to metabolic and gastrointestinaltolerance. Full requirements of fluid, electrolytes,vitamins and minerals should be provided fromthe outset of feeding. [[DD((GGPPPP))]]
People who have eaten little or nothing for morethan 5 days should have nutrition supportintroduced at no more than 50% of requirementsfor the first 2 days, before increasing feed rates tomeet full needs if clinical and biochemicalmonitoring reveals no refeeding problems. [[DD((GGPPPP))]]
People who meet the criteria in Box 1 should beconsidered to be at high risk of developingrefeeding problems. [[DD((GGPPPP))]]
BBooxx 11 CCrriitteerriiaa ffoorr ddeetteerrmmiinniinngg ppeeooppllee aatt hhiigghh rriisskk ooff ddeevveellooppiinngg rreeffeeeeddiinngg pprroobblleemmss
Patient has one or more of the following:
• BMI less than 16 kg/m2
• unintentional weight loss greater than 15%within the last 3–6 months
• little or no nutritional intake for more than 10days
• low levels of potassium, phosphate ormagnesium prior to feeding.
Or patient has two or more of the following:
• BMI less than 18.5 kg/m2
• unintentional weight loss greater than 10%within the last 3–6 months
• little or no nutritional intake for more than 5 days
• a history of alcohol abuse or drugs includinginsulin, chemotherapy, antacids or diuretics.
NUTRITION SUPPORT IN ADULTS40
6Withholding and withdrawing life prolonging treatments: good practice in decision making. General Medical Council. Available from www.gmc-uk.org7Reference guide to consent for examination or treatment (2001) Department of Health. Available from www.dh.gov.uk8Total intake includes intake from any food, oral fluid, oral nutritional supplements, enteral and/ or parenteral nutrition support and intravenous fluid.9The term micronutrient is used throughout to include all essential vitamins and trace elements.10This level may need to be lower in people who are overweight, BMI>25.11When using parenteral nutrition is it often necessary to adjust total energy values listed on the manufacturer’s information which may notinclude protein energy values.

People at high risk of developing refeedingproblems (Box 1) should be cared for byhealthcare professionals who are appropriatelyskilled and trained and have expert knowledge ofnutritional requirements and nutrition support.[[DD((GGPPPP))]]
The prescription for people at high risk ofdeveloping refeeding problems should consider:
• starting nutrition support at a maximum of 10kcal/kg/day, increasing levels slowly to meetor exceed full needs by 4–7 days
• using only 5 kcal/kg/day in extreme cases(for example, BMI less than 14 kg/m2 ornegligible intake for more than 15 days) andmonitoring cardiac rhythm continually in thesepeople and any others who already have ordevelop any cardiac arrythmias
• restoring circulatory volume and monitoringfluid balance and overall clinical status closely
• providing immediately before and during thefirst 10 days of feeding: oral thiamin 200–300mg daily, vitamin B co strong 1 or 2 tablets,three times a day (or full dose daily intravenousvitamin B preparation, if necessary) and abalanced multivitamin/trace elementsupplement once daily.
• providing oral, enteral or intravenoussupplements of potassium (likely requirement2–4 mmol/kg/day), phosphate (likelyrequirement 0.3–0.6 mmol/kg/day) andmagnesium (likely requirement 0.2mmol/kg/day intravenous, 0.4 mmol/kg/dayoral) unless pre-feeding plasma levels arehigh. Pre-feeding correction of low plasmalevels is unnecessary. [[DD((GGPPPP))]]
1.14.2.5 Monitoring of nutrition support in hospital
and the community
Healthcare professionals should review theindications, route, risks, benefits and goals ofnutrition support at regular intervals. The timebetween reviews depends on the patient, caresetting and duration of nutrition support.Intervals may increase as the patient is stabilisedon nutrition support. [[DD((GGPPPP))]]
People having nutrition support in hospital shouldbe monitored by healthcare professionals with therelevant skills and training in nutritionalmonitoring. [[DD((GGPPPP))]]
Healthcare professionals should refer to theprotocols for nutritional, anthropometric andclinical monitoring, shown in Table 3, whenmonitoring people having nutrition support inhospital. [[DD((GGPPPP))]]
Healthcare professionals should refer to theprotocols for laboratory monitoring, shown in Table4, when monitoring people having nutrition supportin hospital. Table 4 is particularly relevant toparenteral nutrition. It could also be selectivelyapplied when enteral or oral nutrition support isused, particularly for people who are metabolicallyunstable or at risk of refeeding syndrome. Thefrequency and extent of the observations given mayneed to be adapted in acutely ill or metabolicallyunstable people. [[DD((GGPPPP))]]
People having parenteral nutrition in thecommunity need regular assessment andmonitoring. This should be carried out by homecare specialists and by experienced hospitalteams (initially at least weekly), usingobservations marked * in Table 3. In addition,they should be reviewed at a specialist hospitalclinic every 3–6 months. Monitoring should bemore frequent during the early months of homeparenteral nutrition, or if there is a change inclinical condition, when the full range of testsin Tables 3 and 4 should be performed. Some ofthe clinical observations may be checked bypatients or carers. [[DD((GGPPPP))]]
People having oral nutrition support and/orenteral tube feeding in the community should bemonitored by healthcare professionals with therelevant skills and training in nutritionalmonitoring. This group of people should bemonitored every 3–6 months or more frequently ifthere is any change in their clinical condition. Alimited number of observations and tests fromTable 3 should be performed. Some of the clinicalobservations may be checked by patients orcarers. If clinical progress is satisfactory,laboratory tests are rarely needed. [[DD((GGPPPP))]]
INTRODUCTION AND METHODS 41

If long-term nutrition support is needed patientsand carers should be trained to recognise andrespond to adverse changes in both their well-being and in the management of their nutritionaldelivery system. [[DD((GGPPPP))]]
NUTRITION SUPPORT IN ADULTS42
TTaabbllee 33 PPrroottooccooll ffoorr nnuuttrriittiioonnaall,, aanntthhrrooppoommeettrriicc aanndd cclliinniiccaall mmoonniittoorriinngg ooff nnuuttrriittiioonn ssuuppppoorrtt
PPaarraammeetteerr
NNuuttrriittiioonnaall
Nutrient intake from oral, enteral orparenteral nutrition (including anychange in conditions that areaffecting food intake)
Actual volume of feed delivered*
Fluid balance charts (enteral andparenteral)
AAnntthhrrooppoommeettrriicc
Weight*
BMI*
Mid-arm circumference*
Triceps skinfold thickness
GGII ffuunnccttiioonn
Nausea/vomiting*
Diarrhoea*
Constipation*
Abdominal distension
EEnntteerraall ttuubbee –– nnaassaallllyy iinnsseerrtteedd
Gastric tube position (pH less than orequal to 5.5 using pH paper – or notingposition of markers on tube once initialposition has been confirmed)
FFrreeqquueennccyy
Daily initially, reducing to twiceweekly when stable
Daily initially, reducing to twiceweekly when stable
Daily initially, reducing to twiceweekly when stable
Daily if concerns regarding fluidbalance, otherwise weekly reducing tomonthly
Start of feeding and then monthly
Monthly, if weight cannot beobtained or is difficult to interpret
Monthly, if weight cannot beobtained or is difficult to interpret
Daily initially, reducing to twice weekly
Daily initially, reducing to twice weekly
Daily initially, reducing to twice weekly
As necessary
Before each feed begins
RRaattiioonnaallee
To ensure that patient is receivingnutrients to meet requirements andthat current method of feeding isstill the most appropriate. To allowalteration of intake as indicated
To ensure that patient is receivingcorrect volume of feed. To allowtroubleshooting
To ensure patient is not becomingover/under hydrated
To assess ongoing nutritionalstatus, determine whethernutritional goals are beingachieved and take into accountboth body fat and muscle
To ensure tolerance of feed
To rule out any other causes ofdiarrhoea and then assess toleranceof feeds
To rule out other causes ofconstipation and then assesstolerance of feeds
Assess tolerance of feed
To ensure tube in correct position
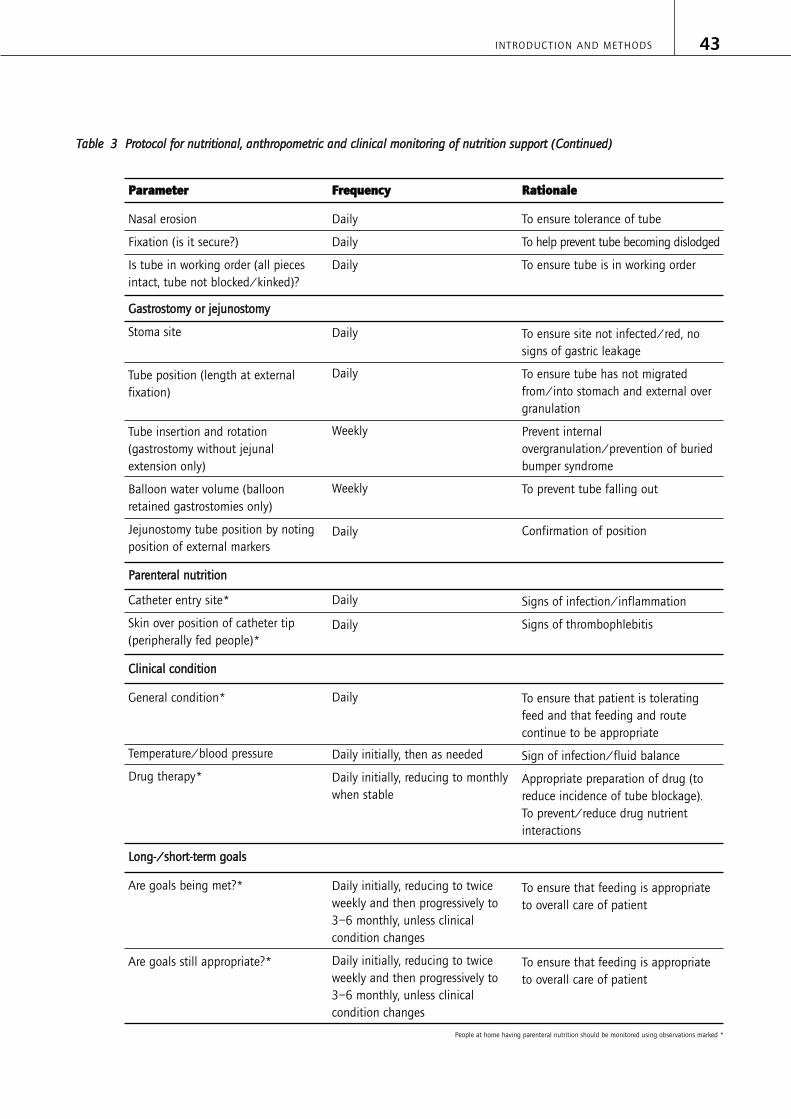
INTRODUCTION AND METHODS 43
PPaarraammeetteerr
Nasal erosion
Fixation (is it secure?)
Is tube in working order (all piecesintact, tube not blocked/kinked)?
GGaassttrroossttoommyy oorr jjeejjuunnoossttoommyy
Stoma site
Tube position (length at externalfixation)
Tube insertion and rotation(gastrostomy without jejunalextension only)
Balloon water volume (balloonretained gastrostomies only)
Jejunostomy tube position by notingposition of external markers
PPaarreenntteerraall nnuuttrriittiioonn
Catheter entry site*
Skin over position of catheter tip(peripherally fed people)*
CClliinniiccaall ccoonnddiittiioonn
General condition*
Temperature/blood pressure
Drug therapy*
LLoonngg--//sshhoorrtt--tteerrmm ggooaallss
Are goals being met?*
Are goals still appropriate?*
FFrreeqquueennccyy
Daily
Daily
Daily
Daily
Daily
Weekly
Weekly
Daily
Daily
Daily
Daily
Daily initially, then as needed
Daily initially, reducing to monthlywhen stable
Daily initially, reducing to twice weekly and then progressively to 3–6 monthly, unless clinical condition changes
Daily initially, reducing to twice weekly and then progressively to 3–6 monthly, unless clinical condition changes
RRaattiioonnaallee
To ensure tolerance of tube
To help prevent tube becoming dislodged
To ensure tube is in working order
To ensure site not infected/red, nosigns of gastric leakage
To ensure tube has not migratedfrom/into stomach and external overgranulation
Prevent internalovergranulation/prevention of buriedbumper syndrome
To prevent tube falling out
Confirmation of position
Signs of infection/inflammation
Signs of thrombophlebitis
To ensure that patient is toleratingfeed and that feeding and routecontinue to be appropriate
Sign of infection/fluid balance
Appropriate preparation of drug (toreduce incidence of tube blockage). To prevent/reduce drug nutrientinteractions
To ensure that feeding is appropriateto overall care of patient
To ensure that feeding is appropriateto overall care of patient
TTaabbllee 33 PPrroottooccooll ffoorr nnuuttrriittiioonnaall,, aanntthhrrooppoommeettrriicc aanndd cclliinniiccaall mmoonniittoorriinngg ooff nnuuttrriittiioonn ssuuppppoorrtt ((CCoonnttiinnuueedd))
People at home having parenteral nutrition should be monitored using observations marked *

NUTRITION SUPPORT IN ADULTS44
TTaabbllee 44 PPrroottooccooll ffoorr llaabboorraattoorryy mmoonniittoorriinngg ooff nnuuttrriittiioonn ssuuppppoorrtt
PPaarraammeetteerr
Sodium, potassium, urea,creatinine
Glucose
Magnesium, phosphate
Liver function tests includingInternational NormalisedRatio (INR)
Calcium, albumin
C-reactive protein
Zinc, copper
FFrreeqquueennccyy
BaselineDaily until stableThen 1 or 2 times a week
Baseline
1 or 2 times a day (or moreif needed) until stable
Then weekly
Baseline
Daily if risk of refeedingsyndrome
Three times a week untilstable
Then weekly
Baseline
Twice weekly until stable
Then weekly
Baseline
Then weekly
Baseline
Then 2 or 3 times a weekuntil stable
Baseline
Then every 2–4 weeks,depending on results
RRaattiioonnaallee
Assessment of renal function,fluid status, and Na and Kstatus
Glucose intolerance iscommon
Depletion is common andunder recognised
Abnormalities commonduring parenteral nutrition
Hypocalcaemia orhypercalcaemia may occur
Assists interpretation ofprotein, trace element andvitamin results
Deficiency common,especially when increasedlosses
IInntteerrpprreettaattiioonn
Interpret with knowledgeof fluid balance andmedication
Urinary sodium may behelpful in complex caseswith gastrointestinal fluid loss
Good glycaemic control isnecessary
Low concentrations indicatepoor status
Complex. May be due tosepsis, other disease ornutritional intake
Correct measured serumcalcium concentration foralbumin
Hypocalcaemia may besecondary to Mg deficiency
Low albumin reflects diseasenot protein status
To assess the presence of anacute phase reaction (APR).The trend of results isimportant
People most at risk whenanabolic
APR causes Zn ↓ and
Cu ↑

INTRODUCTION AND METHODS 45
PPaarraammeetteerr
Seleniuma
Full blood count and MCV
Iron, ferritin
Folate, B12
Manganeseb
25-OH Vit Db
Bone densitometryb
FFrreeqquueennccyy
Baseline if risk of depletion
Further testing dependenton baseline
Baseline
1 or 2 times a week untilstable
Then weekly
Baseline
Then every 3–6 months
Baseline
Then every 2–4 weeks
Every 3–6 months if onhome parenteral nutrition
6 monthly if on long-termsupport9
On starting home parenteralnutrition
Then every 2 years
RRaattiioonnaallee
Se deficiency likely in severeillness and sepsis, or long-term nutrition support
Anaemia due to iron orfolate deficiency is common
Iron deficiency common inlong-term parenteralnutrition
Iron deficiency is common
Excess provision to beavoided, more likely if liverdisease
Low if housebound
Metabolic bone diseasediagnosis
IInntteerrpprreettaattiioonn
APR causes Se ↓
Long-term status betterassessed by glutathioneperoxidase
Effects of sepsis may beimportant
Iron status difficult if APR(Fe ↓, ferritin ↑)
Serum folate/B12 sufficient,with full blood count
Red blood cell or wholeblood better measure ofexcess than plasma
Requires normal kidneyfunction for effect
Together with lab tests formetabolic bone disease
TTaabbllee 44 PPrroottooccooll ffoorr llaabboorraattoorryy mmoonniittoorriinngg ooff nnuuttrriittiioonn ssuuppppoorrtt ((CCoonnttiinnuueedd))
a These tests are needed primarily for people having parenteral nutrition in the community.
b These tests are rarely needed for people having enteral tube feeding (in hospital or in the community), unless there is cause for concern.

1.14.2.6 Oral nutrition support in hospital and
the community
PPeeooppllee wwiitthh ddyysspphhaaggiiaa
People who present with any obvious or lessobvious indicators of dysphagia listed in Box 2should be referred to healthcare professionalswith relevant skills and training in the diagnosis,assessment and management of swallowingdisorders. [[DD((GGPPPP))]]
BBooxx 22 IInnddiiccaattoorrss ooff ddyysspphhaaggiiaaOObbvviioouuss iinnddiiccaattoorrss ooff ddyysspphhaaggiiaa
Difficult, painful chewing or swallowingRegurgitation of undigested foodDifficulty controlling food or liquid in the mouthDroolingHoarse voiceCoughing or choking before, during or afterswallowingGlobus sensationNasal regurgitationFeeling of obstruction Unintentional weight loss – for example, inpeople with dementia
LLeessss oobbvviioouuss iinnddiiccaattoorrss ooff ddyysspphhaaggiiaa
Change in respiration patternUnexplained temperature spikesWet voice qualityTongue fasciculation (may be indicative of motor neurone disease)XerostomiaHeartburnChange in eating habits – for example, eatingslowly or avoiding social occasionsFrequent throat clearingRecurrent chest infectionsAtypical chest pain
Healthcare professionals should recognise thatpeople with acute and chronic neurologicalconditions and those who have undergonesurgery or radiotherapy to the upper aero-digestive tract are at high risk of developingdysphagia. [[DD((GGPPPP))]]
When managing people with dysphagia, healthcareprofessionals with relevant skills and training in thediagnosis, assessment and management ofswallowing disorders should consider:
• the risks and benefits of modified oralnutrition support and/or enteral tube feeding
• the factors listed in Box 3. [[DD((GGPPPP))]]
BBooxx 33 FFaaccttoorrss ttoo bbee ccoonnssiiddeerreedd bbeeffoorree mmooddiiffiiccaattiioonn ooff nnuuttrriittiioonn ssuuppppoorrtt aanndd hhyyddrraattiioonn iinn ppeeooppllee wwiitthh ddyysspphhaaggiiaa
• Recurrent chest infections
• Mobility
• Dependency on others for assistance to eat
• Perceived palatability and appearance of foodor drink
• Level of alertness
• Compromised physiology
• Poor oral hygiene
• Compromised medical status
• Metabolic and nutritional requirements
• Vulnerability (for example,immunocompromised)
• Comorbidities
People with dysphagia should have a drug reviewto ascertain if the current drug formulation, routeand timing of administration remains appropriateand is without contraindications for the feedingregimen or swallowing process. [[DD((GGPPPP))]]
Healthcare professionals with relevant skills andtraining in the diagnosis, assessment andmanagement of swallowing disorders shouldregularly monitor and reassess people withdysphagia who are having modified food andliquid until they are stable. [[DD((GGPPPP))]]
IInnddiiccaattiioonnss ffoorr oorraall nnuuttrriittiioonn ssuuppppoorrtt
Healthcare professionals should consider oral
nutrition support12 to improve nutritional intakefor people who can swallow safely and are
malnourished13 or at risk of malnutrition14. [[AA]]
NUTRITION SUPPORT IN ADULTS46
12 Oral nutrition support includes any of the following methods to improve nutritional intake: fortified food with protein, carbohydrate and/or fat,plus minerals and vitamins; snacks; oral nutritional supplements; altered meal patterns; the provision of dietary advice.13 Malnourished: BMI <18.5 kg/m2, unintentional weight loss >10% within the last 3-6 months, a BMI<20 kg/m2 and unintentional weight loss>5% within the last 3-6 months.14 At risk of malnutrition: eaten little or nothing for more than 5 days and/or likely to eat little or nothing for the next 5 days or longer or poorabsorptive capacity, and or high nutrient losses and or increased nutritional needs from causes such as catabolism.

Healthcare professionals should ensure that theoverall nutrient intake of oral nutrition supportoffered contains a balanced mixture of protein,energy, fibre, electrolytes, vitamins and minerals.[[DD((GGPPPP))]]
If there is concern about the adequacy ofmicronutrient intake, a complete oralmultivitamin and mineral supplement providingthe reference nutrient intake for all vitaminsand trace elements should be considered byhealthcare professionals with the relevant skillsand training in nutrition support who are ableto determine the nutritional adequacy of apatient’s dietary intake. [[DD((GGPPPP))]]
Oral nutrition support should be stopped whenthe patient is established on adequate oral intakefrom normal food. [[DD((GGPPPP))]]
OOrraall nnuuttrriittiioonn ssuuppppoorrtt ffoorr ssuurrggiiccaall ppaattiieennttss
Peri-operative oral nutrition support should beconsidered for surgical patients who can swallow
safely and are malnourished15. [[BB]]
Healthcare professionals should consider givingpost-caesarean or gynaecological surgical patientswho can swallow safely, some oral intake within24 hours of surgery. [[AA]]
Healthcare professionals should consider givingpost-abdominal surgery patients who can swallowsafely, and in whom there are no specific concernsabout gut function or integrity, some oral intakewithin 24 hours of surgery. The patient should bemonitored carefully for any signs of nausea orvomiting. [[AA]]
1.14.2.7 Enteral tube feeding in hospital and the
community
In this guideline, enteral tube feeding refers tothe delivery of a nutritionally complete feed (asspecified in Chapter 9) via a tube into thestomach, duodenum or jejunum.
IInnddiiccaattiioonnss ffoorr eenntteerraall ttuubbee ffeeeeddiinngg
Healthcare professionals should consider enteral
tube feeding in people who are malnourished15 or
at risk of malnutrition16, respectively, and have:
• inadequate or unsafe oral intake, and
• a functional, accessible gastrointestinal tract.[[DD((GGPPPP))]]
Enteral tube feeding should not be given to
people unless they are malnourished15 or at risk
of malnutrition16 and have; inadequate or unsafeoral intake and a functional, accessiblegastrointestinal tract, or they are taking part in aclinical trial. [[AA]]
Enteral tube feeding should be stopped when thepatient is established on adequate oral intake.[[DD((GGPPPP))]]
EEnntteerraall ttuubbee ffeeeeddiinngg ffoorr ssuurrggiiccaall ppaattiieennttss
Surgical patients who are: malnourished17, andhave; inadequate or unsafe oral intake and afunctional, accessible gastrointestinal tract andare due to undergo major abdominal procedures,should be considered for pre-operative enteraltube feeding. [[BB]]
General surgical patients should not have enteraltube feeding within 48 hours post-surgery unless
they are malnourished17 or at risk of
malnutrition18 and have; inadequate or unsafeoral intake and a functional, accessiblegastrointestinal tract. [[AA]]
RRoouuttee ooff aacccceessss
People in general medical, surgical and intensive
care wards who are malnourished17 or at risk of
malnutrition18 and have; inadequate or unsafeoral intake and a functional, accessiblegastrointestinal tract should be fed via a tube intothe stomach unless there is upper gastrointestinaldysfunction. [[AA]]
INTRODUCTION AND METHODS 47
15 Malnourished: BMI <18.5 kg/m2, unintentional weight loss >10% within the last 3-6 months, a BMI<20 kg/m2 and unintentional weight loss>5% within the last 3-6 months.16 At risk of malnutrition: eaten little or nothing for more than 5 days and/or likely to eat little or nothing for the next 5 days or longer or poorabsorptive capacity, and or high nutrient losses and or increased nutritional needs from causes such as catabolism.

People who are malnourished17 or at risk of
malnutrition18 and have; inadequate or unsafe oralintake and a functional, accessible gastrointestinaltract, with upper gastrointestinal dysfunction (or aninaccessible upper gastrointestinal tract) should beconsidered for post-pyloric (duodenal or jejunal)feeding. [[DD((GGPPPP))]]
Gastrostomy feeding should be considered inpeople likely to need long-term (4 weeks or more)enteral tube feeding. [[DD((GGPPPP))]]
Percutaneous endoscopic gastrostomy (PEG) tubeswhich have been placed without apparentcomplications can be used for enteral tubefeeding 4 hours after insertion. [[AA]]
PPeeooppllee wwiitthh ddyysspphhaaggiiaa
In the acute setting, for example following stroke,people unable to swallow safely or take sufficientenergy and nutrients orally should have an initial2–4 week trial of nasogastric enteral tubefeeding. Healthcare professionals with relevantskills and training in the diagnosis, assessmentand management of swallowing disorders shouldassess the prognosis and options for futurenutrition support. [[AA]]
MMooddee ooff ddeelliivveerryy
For people being fed into the stomach, bolus orcontinuous methods should be considered, takinginto account patient preference, convenience anddrug administration. [[BB]]
For people in intensive care, nasogastric tubefeeding should usually be delivered continuouslyover 16–24 hours daily. If insulin administration isneeded it is safe and more practical to administerfeeding continuously over 24 hours. [[DD((GGPPPP))]]
MMoottiilliittyy aaggeennttss
For people in intensive care with delayed gastricemptying who are not tolerating enteral tubefeeding, a motility agent should be considered,unless there is a pharmacological cause that canbe rectified or suspicion of gastrointestinalobstruction. [[AA]]
People in other acute care settings who havedelayed gastric emptying and are not toleratingenteral tube feeding should also be offered amotility agent unless there is a pharmacologicalcause that can be rectified or suspicion ofgastrointestinal obstruction. [[DD((GGPPPP))]]
If delayed gastric emptying is severely limitingfeeding into the stomach, despite the use ofmotility agents, post-pyloric enteral tube feedingand/or parenteral nutrition should be considered.[[DD((GGPPPP))]]
MMaannaaggeemmeenntt ooff ttuubbeess
People requiring enteral tube feeding should havetheir tube inserted by healthcare professionalswith the relevant skills and training. [[DD((GGPPPP))]]
The position of all nasogastric tubes should beconfirmed after placement and before each useby aspiration and pH graded paper (with X-ray ifnecessary) as per the advice from the NationalPatient Safety Agency (NPSA 2005). Localprotocols should address the clinical criteria thatpermit enteral tube feeding. These criteria includehow to proceed when the ability to make repeatchecks of the tube position is limited by theinability to aspirate the tube, or the checking ofpH is invalid because of gastric acid suppression.[[DD((GGPPPP))]]
The initial placement of post-pyloric tubes shouldbe confirmed with an abdominal X-ray (unlessplaced radiologically). Agreed protocols settingout the necessary clinical checks need to be inplace before this procedure is carried out.[[DD((GGPPPP))]]
NUTRITION SUPPORT IN ADULTS48
17 Malnourished: BMI <18.5 kg/m2, unintentional weight loss >10% within the last 3-6 months, a BMI<20 kg/m2 and unintentional weight loss>5% within the last 3-6 months.18 At risk of malnutrition: eaten little or nothing for more than 5 days and/or likely to eat little or nothing for the next 5 days or longer or poorabsorptive capacity, and or high nutrient losses and or increased nutritional needs from causes such as catabolism.

1.14.2.8 Parenteral nutrition in hospital and
the community
Indications for parenteral nutrition
Healthcare professionals should consider parenteral
nutrition in people who are malnourished19 or at
risk of malnutrition20, respectively, and meet eitherof the following criteria:
• inadequate or unsafe oral and/or enteralnutritional intake
• a non-functional, inaccessible or perforated(leaking) gastrointestinal tract. [[DD((GGPPPP))]]
PPrreessccrriippttiioonn
Parenteral nutrition should be introducedprogressively and closely monitored, usuallystarting at no more than 50% of estimated needsfor the first 24–48 hours. Parenteral nutrition canbe withdrawn once adequate oral or enteralnutrition is tolerated and nutritional status isstable. Withdrawal should be planned andstepwise with a daily review of the patient’sprogress. [[DD((GGPPPP))]]
Patients who need parenteral nutrition shouldhave their nutritional requirements determined byhealthcare professionals with the relevant skillsand training in the prescription of nutritionsupport. Before using most parenteral nutritionproducts, micronutrients and trace elementsshould be added and additional electrolytes andother nutrients may also be needed. Additionsshould be made under appropriatepharmaceutically controlled environmentalconditions before administration. [[DD((GGPPPP))]]
Parenteral nutrition should be stopped when thepatient is established on adequate oral and/orenteral support. There is no minimum length of time for the duration of parenteral nutrition.[[DD((GGPPPP))]]
PPaarreenntteerraall nnuuttrriittiioonn ffoorr ssuurrggiiccaall ppaattiieennttss
Healthcare professionals should considersupplementary peri-operative parenteral nutrition
in malnourished19 surgical patients who have aninadequate or unsafe oral and/or enteralnutritional intake or a non-functional, inaccessibleor perforated (leaking) gastrointestinal tract. [[BB]]
Peri-operative supplementary parenteral nutritionshould not be given to surgical patients unless
they are malnourished19 or at risk of
malnutrition20 and have an inadequate or unsafeoral and/or enteral nutritional intake or a non-functional, inaccessible or perforated (leaking)gastrointestinal tract. [[BB]]
If intestinal tolerance persistently limits enteraltube feeding in surgical or critical care patients,parenteral nutrition should be used tosupplement or replace enteral tube feeding. [[BB]]
RRoouuttee ooff aacccceessss
In hospital, parenteral nutrition can be given via adedicated peripherally inserted central catheter as analternative to a dedicated centrally placed centralvenous catheter. A free dedicated lumen in a multi-lumen centrally placed catheter may also be used. [[BB]]
Administration of parenteral nutrition via aperipheral venous catheter should be consideredfor patients who are likely to need short-termparenteral nutrition (less than 14 days) who haveno need for central access for other reasons. Careshould be taken in catheter choice, and inattention to pH, tonicity and long-termcompatibility of the parenteral nutritionformulations in order to avoid administration orstability problems. [[BB]]
Tunnelling subclavian lines is recommended forlong-term use (more than 30 days). [[DD((GGPPPP))]]
Catheters do not have to be tunnelled for short-term use (less than 30 days). [[BB]]
MMooddee ooff ddeelliivveerryy
Continuous administration of parenteral nutritionshould be offered as the preferred method ofinfusion in severely ill people who requireparenteral nutrition. [[BB]]
INTRODUCTION AND METHODS 49
19Malnourished: BMI <18.5 kg/m2, unintentional weight loss >10% within the last 3-6 months, a BMI<20 kg/m2 and unintentional weight loss>5% within the last 3-6 months.20At risk of malnutrition: eaten little or nothing for more than 5 days and/or likely to eat little or nothing for the next 5 days or longer or poorabsorptive capacity, and or high nutrient losses and or increased nutritional needs from causes such as catabolism.

Cyclical delivery of parenteral nutrition should beconsidered when using peripheral venous cannulaewith planned routine catheter change. [[BB]]
A gradual change from continuous to cyclicaldelivery should be considered in patientsrequiring parenteral nutrition for more than 2weeks. [[DD((GGPPPP))]]
MMaannaaggeemmeenntt ooff ccaatthheetteerrss
Only healthcare professionals competent incatheter placement should be responsible for theplacement of catheters and they should be awareof the importance of monitoring and managing
these safely21. [[DD((GGPPPP))]]
1.14.2.9 Supporting patients in the community
Healthcare professionals should ensure thatpatients having enteral or parenteral nutrition inthe community and their carers:
• are kept fully informed and have access toappropriate sources of information in formats,languages and ways that are suited to anindividual’s requirements. Consideration shouldbe given to cognition, gender, physical needs,culture and stage of life of the individual
• have the opportunity to discuss diagnosis,treatment options and relevant physical,psychological and social issues
• are given contact details for relevant supportgroups, charities and voluntary organisations.[[DD((GGPPPP))]]
EEnntteerraall ttuubbee ffeeeeddiinngg
All people in the community having enteral tubefeeding should be supported by a coordinatedmultidisciplinary team, which includes dietitians,district, care home or homecare company nurses, GPs,community pharmacists and other allied healthcareprofessionals (for example, speech and languagetherapists) as appropriate. Close liaison between themultidisciplinary team and patients and carersregarding diagnoses, prescription, arrangements andpotential problems is essential. [[DD((GGPPPP))]]
Patients in the community having enteral tubefeeding and their carers should receive anindividualised care plan which includes overallaims and a monitoring plan. [[DD((GGPPPP))]]
Patients in the community having enteral tubefeeding and their carers, should receive trainingand information from members of themultidisciplinary team on:
• the management of the tubes, deliverysystems and the regimen, outlining allprocedures related to setting up feeds, usingfeed pumps, the likely risks and methods fortroubleshooting common problems and beprovided with an instruction manual (andvisual aids if appropriate)
• both routine and emergency telephonenumbers to contact a healthcare professionalwho understands the needs and potentialproblems of people on home enteral tubefeeding
• the delivery of equipment, ancillaries and feedwith appropriate contact details for anyhomecare company involved. [[DD((GGPPPP))]]
PPaarreenntteerraall nnuuttrriittiioonn
All people in the community having parenteralnutrition should be supported by a co-ordinatedmultidisciplinary team, which includes input fromspecialist nutrition nurses, dietitians, GPs,pharmacists and district and/or homecarecompany nurses. Close liaison between themultidisciplinary team and patients and carersregarding diagnoses, prescription, arrangementsand potential problems is essential. [[DD((GGPPPP))]]
People in the community having parenteralnutrition and their carers should receive anindividualised care plan which includes overallaims and a monitoring plan. [[DD((GGPPPP))]]
People in the community having parenteralnutrition and their carers should receive trainingand information from members of themultidisciplinary team on:
NUTRITION SUPPORT IN ADULTS50
21Infection control: prevention of healthcare – associated infection in primary and community care. NICE clinical guideline No.2 (2003).Available from www.nice.org.uk/CG002

• the management of the delivery systems andthe regimen, outlining all procedures relatedto setting up feeds, using feed pumps, thelikely risks and methods for troubleshootingcommon problems and be provided with aninstruction manual (and visual aids ifappropriate)
• routine and emergency telephone numbers tocontact a healthcare professional with therelevant competencies (specialist nutritionnurse, pharmacist)
• the arrangements for the delivery ofequipment, ancillaries and feed withappropriate contact details for any homecarecompany involved. [[DD((GGPPPP))]]
11..1144..33 RReesseeaarrcchh rreeccoommmmeennddaattiioonnss
The Guideline Development Group has made thefollowing recommendations for research, on the basisof its review of the evidence. The Group regards theserecommendations as the most important researchareas to improve NICE guidance and patient care inthe future. The Guideline Development Group’s fullset of research recommendations are detailed furtherin the guideline.
11.. RReesseeaarrcchh qquueessttiioonn
Further research is needed to ascertain whetheran educational intervention (for example, three 1-week modular courses, over 6 months) for allhealthcare professionals, in particular medical andnursing staff including those who work withpeople with dementia would have an affect onpatient care (that is, affect on nutritional status,length of hospital stay, frequency of GP visits,complications and quality of life) compared to noformal education?
WWhhyy tthhiiss iiss iimmppoorrttaanntt
It is known that healthcare professionals in boththe hospital and community setting have a poorknowledge of nutrition. This is partly due toreceiving a minimal amount of education innutrition during their undergraduate or basictraining. It is therefore essential to determinewhether an organised nutrition support educationprogramme to healthcare professionals wouldimprove the choice made about nutrition supportand the consequent care of patients prescribednutrition support.
22.. RReesseeaarrcchh qquueessttiioonn
What are the benefits to patients of a nutritionalscreening programme (using a simple tool such asthe ‘Malnutrition Universal Screening Tool’[MUST]) compared with not screening people in:a) primary care (attending GP clinics); b) carehomes; c) hospital inpatients; d) hospitaloutpatients; e) patients with dementia in terms ofdetermining the number of people at risk ofmalnutrition, complications, survival, hospitaladmission rates, length of stay, quality of life andcost effectiveness?
INTRODUCTION AND METHODS 51

WWhhyy tthhiiss iiss iimmppoorrttaanntt
There is no clear evidence available as to whetherscreening is really beneficial or how it should becarried out. With the lack of evidence the GDGhave considered in detail this problem and haveinstead carefully developed consensus statementsto support recommendations for screening. As apriority it is important that we determine theneed for screening and intervention in particularprimary care and the wider community.
33.. RReesseeaarrcchh qquueessttiioonn
Further research is needed to identify whichcomponents of nutrition monitoring are clinicallyand cost effective.
WWhhyy tthhiiss iiss iimmppoorrttaanntt
There is no clear evidence available regarding thelong- and short-term benefits of clinicalmonitoring in terms of prevention ofcomplications and survival. With the lack ofevidence the GDG have considered in detail thisproblem and have instead carefully developed theguidance for monitoring by expert clinical practiceand consensus opinion.
44.. RReesseeaarrcchh qquueessttiioonn
What are the benefits of patients (in hospital or thecommunity, including older people) identified as athigh risk of malnutrition by a screening tool such asMUST being offered either oral nutritionalsupplements compared with a) dietary modificationand/or food fortification, or b) dietary modificationand/or food fortification together with dietarycounselling, in terms of determining complications,survival, length of hospital stay, quality of life andcost effectiveness?
WWhhyy tthhiiss iiss iimmppoorrttaanntt
This is an essential recommendation for researchsince there is insufficient evidence on the benefitsof intervention used for oral nutrition support – inparticular, the benefits of often first linetreatment, for example food fortification and ordietary counselling. It is essential to know this sothat the indications on how to treat can befurther supported.
55.. RReesseeaarrcchh qquueessttiioonn
What are the benefits of enteral tube feeding topatients compared with no enteral tube feeding inpeople with dysphagia and early to mid-stagedementia in terms of reduced complicationsassociated with swallowing, improved nutritionalstatus, delayed onset of advanced stage dementia,hospital admissions, cost effectiveness and survival?
WWhhyy tthhiiss iiss iimmppoorrttaanntt
Much of the research tends to focus orconcentrate on tube feeding people withadvanced dementia or those who may be interminal stages of the disease. Depending on thetype of dementia, swallowing disorders may occurat an earlier stage in the disease, for examplevascular dementia. The benefits and complicationsof tube feeding may be quite different in peoplein the earlier stages than those who are in theadvanced stage of dementia.
NUTRITION SUPPORT IN ADULTS52
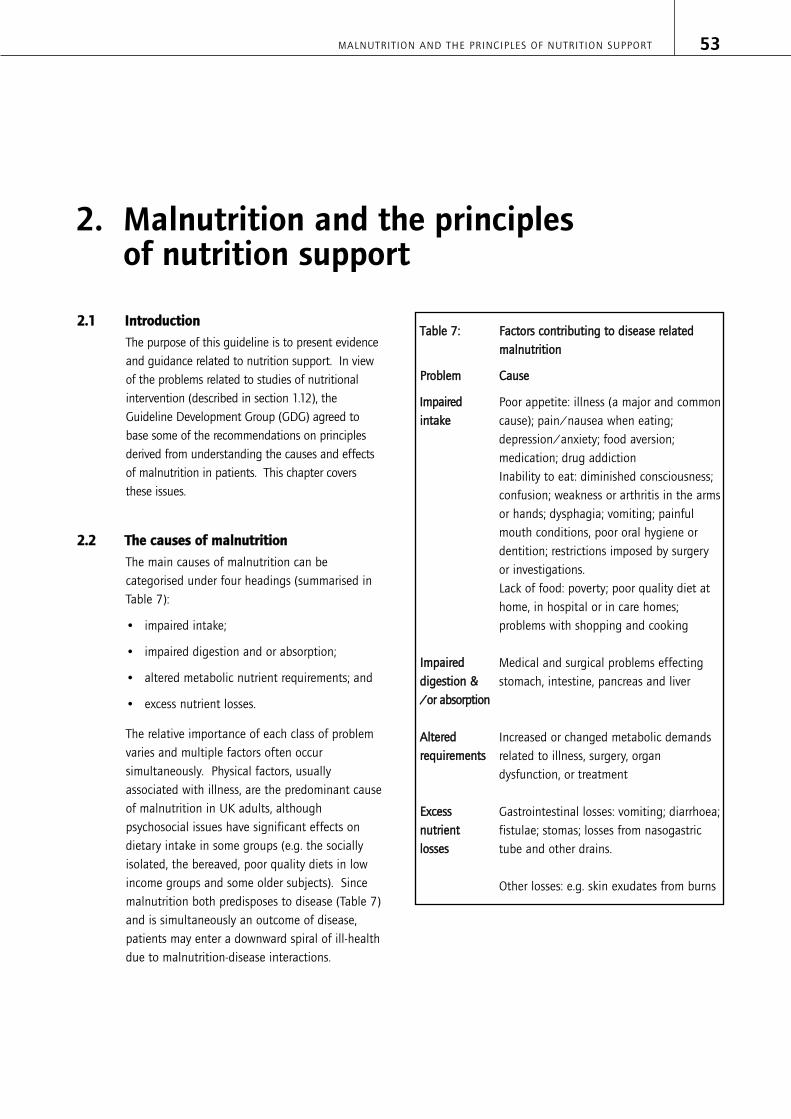
22..11 IInnttrroodduuccttiioonn
The purpose of this guideline is to present evidenceand guidance related to nutrition support. In viewof the problems related to studies of nutritionalintervention (described in section 1.12), theGuideline Development Group (GDG) agreed tobase some of the recommendations on principlesderived from understanding the causes and effectsof malnutrition in patients. This chapter coversthese issues.
22..22 TThhee ccaauusseess ooff mmaallnnuuttrriittiioonn
The main causes of malnutrition can becategorised under four headings (summarised inTable 7):
• impaired intake;
• impaired digestion and or absorption;
• altered metabolic nutrient requirements; and
• excess nutrient losses.
The relative importance of each class of problemvaries and multiple factors often occursimultaneously. Physical factors, usuallyassociated with illness, are the predominant causeof malnutrition in UK adults, althoughpsychosocial issues have significant effects ondietary intake in some groups (e.g. the sociallyisolated, the bereaved, poor quality diets in lowincome groups and some older subjects). Sincemalnutrition both predisposes to disease (Table 7)and is simultaneously an outcome of disease,patients may enter a downward spiral of ill-healthdue to malnutrition-disease interactions.
TTaabbllee 77:: FFaaccttoorrss ccoonnttrriibbuuttiinngg ttoo ddiisseeaassee rreellaatteeddmmaallnnuuttrriittiioonn
PPrroobblleemm CCaauussee
IImmppaaiirreedd Poor appetite: illness (a major and common iinnttaakkee cause); pain/nausea when eating;
depression/anxiety; food aversion;medication; drug addictionInability to eat: diminished consciousness;confusion; weakness or arthritis in the armsor hands; dysphagia; vomiting; painfulmouth conditions, poor oral hygiene ordentition; restrictions imposed by surgeryor investigations. Lack of food: poverty; poor quality diet athome, in hospital or in care homes; problems with shopping and cooking
IImmppaaiirreedd Medical and surgical problems effectingddiiggeessttiioonn && stomach, intestine, pancreas and liver//oorr aabbssoorrppttiioonn
AAlltteerreedd Increased or changed metabolic demands rreeqquuiirreemmeennttss related to illness, surgery, organ
dysfunction, or treatment
EExxcceessss Gastrointestinal losses: vomiting; diarrhoea; nnuuttrriieenntt fistulae; stomas; losses from nasogastric lloosssseess tube and other drains.
Other losses: e.g. skin exudates from burns
MALNUTRITION AND THE PRINCIPLES OF NUTRITION SUPPORT 53
2. Malnutrition and the principles of nutrition support

22..33.. TThhee eeffffeeccttss ooff mmaallnnuuttrriittiioonn
Malnutrition detrimentally effects physicalfunction, psychosocial well-being and theoutcome of disease. It can affect every system
and tissue of the body 185,335, see Table 8.
NUTRITION SUPPORT IN ADULTS54
TTaabbllee 88:: SSoommee pphhyyssiiccaall aanndd ppssyycchhoo--ssoocciiaall eeffffeeccttss ooff mmaallnnuuttrriittiioonn
AAddvveerrssee eeffffeecctt CCoonnsseeqquueennccee
IImmppaaiirreedd iimmmmuunnee rreessppoonnsseess Predisposes to infection and impairs recovery when infected
IImmppaaiirreedd wwoouunndd hheeaalliinngg Surgical wound dehiscence, anastamotic breakdowns, development of post-surgical fistulae, failure of fistulae to close, increased risk of wound infection and un-united fractures. All can then lead to prolonged recovery from illness,increased length of hospital stay and delayed return to work
RReedduucceedd mmuussccllee ssttrreennggtthh Inactivity, inability to work effectively, and poor self care. Abnormal muscle aanndd ffaattiigguuee (or neuromuscular) function may also predispose to falls or other accidents
RReedduucceedd rreessppiirraattoorryy mmuussccllee Poor cough pressure, predisposing to and delaying recovery from chest infection. ssttrreennggtthh Difficulty weaning malnourished patients from ventilators
IInnaaccttiivviittyy,, eessppeecciiaallllyy iinn bbeedd Predisposes to pressure sores and thromboembolism, and muscle wasting.bboouunndd ppaattiieenntt
WWaatteerr aanndd eelleeccttrroollyyttee ddiissttuurrbbaanncceess Malnourished individuals are usually depleted in whole body potassium,magnesium and phosphate, while simultaneously overloaded in whole bodysodium and water. They also have reduced renal capacity to excrete a sodiumand water load. This leads to vulnerability to re-feeding syndrome (see section6.6) and iatrogenic sodium and water overload.
IImmppaaiirreedd tthheerrmmoorreegguullaattiioonn Hypothermia and falls, especially in older people
VViittaammiinn aanndd ootthheerr ddeeffiicciieenncciieess Specific vitamin deficiency states e.g. scurvy and vitamin related re-feeding riskse.g. Wernike-Korsakoff syndrome (see section 6.6.3). Mineral deficiencies includeiron deficiency anaemia, and magnesium deficiency, which can cause tetany (see also above for electrolyte disturbances). A lack of trace elements can also
be a cause of range of problems.290.
MMeennssttrruuaall iirrrreegguullaarriittiieess//aammeennoorrrrhhooeeaa Infertility and osteoporosis
IImmppaaiirreedd ppssyycchhoo--ssoocciiaall ffuunnccttiioonn Even when uncomplicated by disease, patients who are malnourished mayexperience apathy, depression, self-neglect, hypochondriasis, lack of self esteem, poor body image, possible confusion about slow recovery, lack of interest in food,
loss of libido and deterioration in social interactions185,335. Malnutrition may alsoaffect behaviour and attitude.
22..44.. TThhee pprreevvaalleennccee ooff mmaallnnuuttrriittiioonn
There are many different anthropometric, clinicaland biochemical criteria that have been used toassess malnutrition and these have resulted in
widely varying reports of its prevalence. One ofthe simplest criteria is current weight status (e.g.body mass index; BMI). The proportion of
underweight adults (BMI<20 kg/m2) in the UK

varies considerably according to care setting: 10-40% in hospitals and care homes; < 5% in thegeneral population at home, and >10% in thoseat home with chronic diseases of the lung andgastrointestinal tract, or those who have hadsurgery in the previous 6 weeks. The
‘Malnutrition Universal Screening Tool’ (‘MUST’)94,which incorporates both current weight status andunintentional weight loss, has identified morethan 10% of the general population aged 65years and over as being at medium or high risk of
malnutrition92-94,336. In hospitalised patients, thesame degree of risk is seen in 10-60% dependingon medical condition and patients’ age. Similarvery high prevalence’s of nutritional risk are seenin residents of care homes but although mostmalnutrition is found in the community (>95%),most malnutrition related expenditure occurs in
hospital9,87. However, both care settings make asubstantial contribution to total costs.
The prevalence of individual nutrient deficienciesis also disturbing, especially in older subjects. For
example, in people aged 65 years and over109,folate deficiency affects 29% of those who are“free living” (8% in severe form) and 35% ofthose in institutions (16% in severe form).Similarly, vitamin C deficiency in such peopleaffects 14% of those who are free living (5% in asevere form) and 40% of those in institutions(16% in severe form). Nutrient deficiencies and
protein-energy malnutrition commonly coexist335.
22..55.. PPrriinncciipplleess uunnddeerrllyyiinngg iinntteerrvveennttiioonn
The difficulties inherent in nutrition support meanthat there is little hard evidence to assist withdecisions on how and when to treat patients whoare either malnourished or at risk of becoming so.However, sensible approaches can be derived fromunderstanding 3 types of observations:
1. Cross-sectional studies suggest thatnutritionally related problems are likely tooccur in individuals who are thin or who have
recently lost weight94,335,336 e.g. those withBMIs of <20 kg/m2 and especially <18.5kg/m2 and/or those who have recently lost>5% of their usual body weight, especiallythose who have lost >10%.
2. Studies in healthy volunteers show that
measures such as muscle function203,335
decline within a few days of completestarvation, and after more than 5 -7 days oflittle or no intake there is significantdetriment in several bodily functions includingmany of those listed in Table 8. These illeffects reverse promptly with the provision ofadequate feeding.
3. Studies in malnourished patients show rapidfunctional benefits when adequate feeding isprovided. These changes can occur well beforethe weight lost has been regained (e.g.malnourished patients have low collagendeposition rates in surgical wounds but showimproved deposition within days of receiving
nutrition support374).
With these observations in mind, good nutritionshould benefit both those who are already overtlymalnourished in terms of BMI or recentunintentional weight loss and those who aredeveloping nutritional risks by having eaten littleor nothing or be likely to eat little or nothing forover 5 days. In addition, nutrition support canoften provide simple direct benefits by:
• Keeping patients who are eating inadequately,alive for long enough for specific medical orsurgical interventions to take effect.
• Making malnourished patients feel better,improving their ability to cope with ill-health.
• Maintaining strength through patients’illnesses so that their recuperation isshortened and they are less susceptible tofurther problems.
• Providing long-term support for those patientswith chronic inability to eat, drink or absorbadequately.
The principles above underlie many of therecommendations proposed in these Guidelines.They are also in keeping with physical,psychological and social improvements that occur
during repletion185.
MALNUTRITION AND THE PRINCIPLES OF NUTRITION SUPPORT 55
33..11.. IInnttrroodduuccttiioonn
Patients requiring nutrition support need helpfrom a range of healthcare professionals includingdietitians, pharmacists, laboratory specialists,nurses, care assistants, speech and languagetherapists, occupational therapists,physiotherapists, GPs and hospital doctors. It istherefore important that all healthcare workersinvolved in direct patient care should appreciatethe value of providing their patients withadequate nutrition and be familiar with thepossibilities for providing nutrition support ifneeded. The composition and organisation ofmultidisciplinary teams for nutrition support willdiffer in community and hospital settings.
33..22.. NNuuttrriittiioonn ssuuppppoorrtt iinn tthhee ccoommmmuunniittyy
All healthcare professionals should try to ensurethat coordinated nutritional care is provided forpatients with or at risk of malnutrition in thecommunity. A multi-disciplinary ‘communitynutrition team’ approach is valuable, comprisingdietitians, district nurses and care home staff withother allied healthcare professionals such as speechand language therapists, physiotherapists andoccupational therapists as necessary. The teamshould then work with patients, relatives, carers,caterers, and GPs to prevent or treat malnutritionas appropriate. They should also develop protocolsand care pathways for nutrition support, along witheducational initiatives to ensure that all healthcareprofessionals understand the importance ofnutrition in patient care.
Although guidance on the provision of meals incare homes is beyond the scope of theseGuidelines, it is clear that care homes should
provide adequate quantities of good quality foodif the use of unnecessary nutrition support is tobe avoided. The food should be served in anenvironment conducive to eating, with help givento those patients who can potentially eat but whoare unable to feed themselves.
Patients having home enteral tube feeding orhome parenteral nutrition have particularlycomplex needs with demands for a coordinatedsupply of feeds and ancillaries, and the need forregular expert review (see Chapter 11).
Although the GDG were unaware of any RCTsexamining the benefits of introducing communitynutrition support teams, observational work hassuggested benefit e.g. audits following theintroduction of expert review for home ETFpatients have suggested overall cost savingsrelated to identification of significant numbers ofsuch patients whose condition had improvedenough to allow them to return to normal ormodified oral intake.
33..33.. NNuuttrriittiioonn ssuuppppoorrtt iinn HHoossppiittaall
The organisation of nutrition support in hospitalneeds to ensure that all patients’ nutritionalneeds are met whenever possible. This requirescoordinated activity by catering, dieteticdepartments and multi-disciplinary nutritionsupport teams (NSTs), working with all ward-based nurses and care assistants. Other alliedhealthcare professionals such as speech andlanguage therapists, occupational therapists andphysiotherapists may also need to be involved.The GDG agree with recommendations made byBAPEN (BAPEN1994) and the Royal College of
NUTRITION SUPPORT IN ADULTS56
3. Organisation of nutrition support in hospital and the community

Physicians in London297 that such coordination isbest achieved by hospitals having a NutritionSteering Committee with members which includesenior representation from Trust management,catering, pharmacy, dietetics, nursing and thenutrition support team. The Committee shouldwork within the Governance framework, reportingdirectly to the Chief Executive or Trust Board.
The departments or clinicians involved in theprovision of adequate nutrition for patients havediffering roles:
33..33..11.. CCaatteerriinngg
There are numerous good reasons for hospitals toprovide adequate quantities of good quality food,of which one is the need to limit unnecessary useof nutrition support. The food should also beserved in an environment conducive to eating,with help given to those who can potentially eatbut who are unable to feed themselves. Theseissues are given proper consideration in the
Government ‘Better Hospital Food’248 and
‘Protected Mealtimes’ 249.
33..33..22.. DDiieettiittiiaannss
Although there are no relevant RCTs, dietitians areclearly central to the provision of nutritionsupport for patients who cannot derive enoughnourishment from food. Dietitians are involved innutritional screening and assessment, as well aswith the provision of supplementary nutritionthrough oral, enteral and parenteral routes. Allhospitals should therefore ensure that patientswho are either at risk of or have malnutritionshould have access to a dietitian if necessary.
The relatively small number of dietitians in mosthospitals, means that some of their roles must bedelegated to other ward staff. The dietitianstherefore need to develop hospital protocols andcare pathways on nutrition support, and toparticipate in the nutritional education of theentire clinical workforce. The aim should be thatall hospital healthcare professionals shouldunderstand the importance of nutrition in patientcare and the means available to provide it safelyand effectively.
33..33..33.. WWaarrdd nnuurrsseess
Although there are no relevant scientific studies,all ward nurses should be fully aware of theimportance of patients meeting their nutritionalneeds and should understand the likely benefitsand risks of nutrition support by oral, enteral andparenteral routes. Furthermore, nurses lookingafter patients other than those explicitly excludedfrom nutritional screening (section 4.9) will oftenneed to undertake the screening process and toinstigate associated care pathways.
33..33..44.. SSppeecciiaalliisstt nnuuttrriittiioonn ssuuppppoorrtt nnuurrsseess
Many hospitals employ specialist nurses or nurseconsultants to take responsibility for ensuring thatnutrition support is delivered as safely andeffectively as possible. Such nurses will trainother healthcare professionals, will monitoradherence to protocols for enteral and parenteralnutrition and will usually coordinate thenutritional care of patients in hospitals andbetween hospitals and the community.
33..33..55 NNuuttrriittiioonn ssuuppppoorrtt tteeaammss
The aim of a hospital NST is to ensure thatspecialised nutrition support is given safely andeffectively to those patients who need it. The NSTshould be formally recognised and shouldcomprise dietitians, nutrition nurses, pharmacistsand clinicians with good biochemistry andmicrobiology laboratory support. NST cliniciansare often gastroenterologists, GI surgeons orintensivists or chemical pathologists with aspecific interest in nutritional problems butwhatever their background, they should have alsoreceived specific training in nutrition support.
Hospital NSTs may take on total responsibility forthe nutritional care of patients, particularly thoseon PN, or act in an advisory (consultative) role.The potential advantages of NSTs include:
• reduction of unnecessary treatments
• prevention of complications (mechanical,infective and metabolic)
• pharmaceutical advice on stability andcompatibility of drugs and PN regimens
ORGANISATIONS OF NUTRITION SUPPORT IN HOSPITAL AND THE COMMUNIT Y 57

• production or support of existing guidelines
• education and training of other staff, patientsand carers
• audit/research
• acting as advocates for patients
• point of contact for patients and carers,especially for those on home parenteralnutrition (HPN) or home enteral tube feeding(HETF) (see Chapter 11)
The scale of these benefits is open to debate, andwe therefore conducted a review of studiesinvestigating these issues, recognising while doingso, and the many difficulties inherent inconducting RCTs on service interventions.
33..44.. MMeetthhooddss
Our review included randomised and non-randomised controlled trials, since we were awarethat this type of question is not easily addressedby controlled trials. The studies included patientscared for by a NST and patients receiving thestandard regimen used in the care setting withoutan NST. In the intervention arm patients had tobe receiving nutrition support (oral, ETF or PNexcluding home nutrition support) and had tohave nutritional management from a NSTcomposed of two or more relevant healthcareprofessionals. In the comparison arm patients hadno intervention from nutrition support teams.
33..44..11.. SSttuuddiieess ccoonnssiiddeerreedd ffoorr tthhiiss rreevviieeww
The literature search identified two RCTs170,170,312
and four non-randomised comparative studies:
two on ETF48,280 and two on PN 107,182 one of
which was a systematic review 107 including 11studies (Table 83,Table 84,Table 85). All studieswere set within hospitals. A number of studieswere excluded due to poor methodologicalquality, the main reason being the studies had nocontrol group.
33..55 CClliinniiccaall eevviiddeennccee
33..55..11 RRaannddoommiisseedd ccoonnttrroolllleedd ttrriiaallss
One RCT included 212 patients at nutritional
risk170 (Table 85). Three Danish hospitalsparticipated in the study. The NST consisted ofa nurse and a dietitian. Patients wererandomised to receive nutrition supportmanaged by the NST (n= 108) or by usualdepartmental procedures (n= 104). The NSTprovided motivation for patients and staff,detailed a nutritional plan, assured delivery ofprescribed food and gave advice on ETF and PNwhen appropriate.
The primary outcome was length of stayconsidered to be sensitive to nutrition support.When a patient fulfilled the following threecriteria, hospital stay was no longer considered tobe sensitive to nutrition support:
• patient is able to manage toilet visit withoutassistance
• absence of fever (temperature < 38oC)
• patient is without intravenous access
Other outcomes reported were total length of staywith a maximum of 28 days (LOS28), minor and
major complications and quality of life (QoL).
There were no statistically significantdifferences between the two groups in any ofthe outcomes. In a subgroup analysis, patientswith complications but no operation hadshorter length of stay sensitive to nutritionsupport (p=0.015) and shorter overall LOS28
(p=0.028) if managed by the NST. The otherRCT included 101 patients referred and
accepted for a PEG312 (NST group n= 47,Control group n= 54) (Table 84). The NSTconsisted of a nurse and a dietitian. Patientswere followed up for 12 months. The teamprovided weekly visits while in acute hospitaland at least monthly after discharge, regularliaison with ward and primary careprofessionals and counselling to patients andcarers including telephone contact for support.There were no statistically significantdifferences between the two groups in
NUTRITION SUPPORT IN ADULTS58

mortality, complications, time to removal ofPEG, LOS or readmissions. For QoL there was animprovement in the social functioning elementof the SF36 with NST group over control group(p=0.05). There were no differences in otherelements of the SF36.
33..55..22.. NNoonn--rraannddoommiisseedd ccoonnttrroolllleedd ttrriiaallss
3.5.2.1 Enteral tube feeding
Two studies from the same American universityteaching hospital looked at the effect of a NST insurgical, medical and ICU patients who were
started on ETF support (n= 101280; n= 10248).The comparative group were concurrent controlsmanaged by their primary physician (Table 83).
In both studies patients in the NST group hadfewer untreated metabolic complications (p<0.05)such as hyperglycaemia (p<0.05) andhypophosphataemia (p<0.05). More NST grouppatients also attained adequate feeding (p<0.05)
One study280 reported fewer total complications(pulmonary, mechanical, GI and metabolic) in the
NST group (p<0.05) but in the other study48 thedifference was not significant. Neither studyfound significant differences in mortality.
3.5.2.2 Parenteral Nutrition
One systematic review107 looked at the effect of aNST in patients receiving PN (Table 84). Thereview included 11 studies but there was a lot ofheterogeneity in study methodology, patientsincluded, the members and roles of the NSTs andoutcome measures and length of follow up. Infour of the studies the NST groups were compared
with concurrent controls75,108,119,354 whilst in seventhe NST groups were compared with historical
patients64,111,155,166,257,278,357. Sample sizes in thestudies were generally small ranging from 28 to285 and five studies had unequal sample sizesbetween the groups. Both medical and surgicalpatients were included.
In most studies the NST was composed of aphysician, pharmacist, nurse and a dietitian. Two
studies included a gastroenterologist108,111,
another included a biochemist108 and another
surgeon278. In some studies the NST provided a
consultative service whilst in others it assumedtotal responsibility for the nutritionalmanagement of the patient.
Due to the heterogeneity of the studies it was notpossible to pool the results, however, a generalsummary of outcomes reported is provided below:
Catheter related complications:
There were no significant differences inmechanical complications between the groupsalthough there was a trend towards fewerpneumothoraces in the NST group.
Most studies reported no significant differences inseptic complications between the groups.
However a retrospective study182 which reporteddata on 54 medical and surgical patients whoreceived PN before the NST was formed,compared with 75 who received PN after, foundthat patients in the NST group had significantlyfewer incidents of catheter related sepsis: 29%compared to 71% (p<0.05) (Table 85). Due to theway that this clinical question was defined, theeffect of a nutrition support nurse on patientoutcomes was not specifically considered.However, the GDG were aware of findings from
several observational studies50,102,103,130,167,183 thathave demonstrated much reduced rates ofcatheter related sepsis following the introductionof specialist nutrition nurses in a variety ofhospital settings.
Metabolic complications:
NST groups had significantly fewer metabolic
complications in five studies75,108,111,119,357.
Mortality
Most studies reported no significant differences in
mortality but the retrospective study182 whichreported lower catheter sepsis rates also reportedlower mortality in the NST managed patients:24% compared to 43% (p<0.05).
ORGANISATIONS OF NUTRITION SUPPORT IN HOSPITAL AND THE COMMUNIT Y 59

33..66.. CCoosstt eeffffeeccttiivveenneessss eevviiddeennccee
It has been hypothesised that NSTs can achievecost savings through:
• Reduced complications associated with PNsuch as catheter-related sepsis and metabolicdisturbance
• Reduced use of inappropriate PN
• Reduced length of stay
• Reduced PN wastage
• Use of lower cost materials
We found a number of studies that evaluated thecost of nutrition support teams(Table 86 and Table
87). One was based on an RCT312 and five were
based on comparisons of cohorts1,64,182,357,368. Twostudies were excluded because the NST existedduring the control period and therefore the nature
of the comparison was unclear 67,254. One study wasexcluded because it was poorly reported and used
an obscure method of controlling for severity 146. Afurther eight studies were not included becausethey used a hypothecated comparison
arm18,101,123,232,233,253,295,316 and two were excludedbecause they reported total costs only and the
denominator was not stated 22,174.
One RCT312 evaluated the follow-up of patientsafter insertion of a PEG (as reported in section3.5.1 above). All hospital and community carecosts were measured over 12 months. There were(non-significant) incremental cost savings perpatient of £3,538 (95% CI: -£2,790, £9,847) butthere were no apparent differences incomplication rates.
A US evaluation based on a prospective cohort
study 64 compared automatic referral to NST withad hoc referral for patients who were on PN for atleast two days. They estimated hospital pharmacyand biochemistry costs although NST costs werenot included. They found incremental costsavings (p=0.41): £930 vs. £1100.
A retrospective cohort study 368 evaluated NSTs inthe management of patients referred for seriousburns compared with physician management.They found hospital costs savings (£9,300 vs.
£12,700). There were statistically significantreductions in minor complications but nodifferences in major complications.
A second US retrospective cohort study 357
compared an NST (metabolic support service)consultation with no NST consultation forinpatients beginning PN. For both cohorts theyestimated avoidable PN charges using the ASPENguidelines. They found incremental cost savings(the statistical significance of which was notclearly reported): £180 vs. £540. And there was asubstantial reduction in complications: 34% vs.66% (p=0.004). However, it is possible thatpatients referred to NST could be very different tothose not referred and it is unclear who wasdeciding which costs were avoidable. NST costswere also not included.
A UK-based retrospective cohort study 182
estimated cost savings of £227 per patientreferred for PN due to prevention of catheter-related sepsis (cost of staff time and bedoccupancy costs not included). Substantial costsavings were also estimated through theavoidance of unnecessary PN (£777 per patientreferred). However this does not take into accountthe observation that total PN days were increased,and the authors were unable to determine theextent to which this was due to the presence ofthe NST or due to changing workload andpractices within the hospital. Nor did the studyestimate the health gain associated with thisincrease in PN usage.
A UK study1 estimated cost savings from areduced incidence of catheter-related sepsisattributable to the presence of an NST. Using theaggregated infection rate from seven cohortstudies, they estimated cost savings of between£400 (best case scenario) and £1200 (worst case)per patient receiving PN.
33..77.. CCoonncclluussiioonn
As expected for studies relating to serviceinterventions, those identified by our review wereof limited quality in terms of the scientific rigourof their design and all were small andheterogeneous. Nevertheless, the evidence
NUTRITION SUPPORT IN ADULTS60
suggests that NSTs decrease complications andcosts through reductions in unnecessarytreatments and prevention of complications.
33..88.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
All healthcare professionals who are directlyinvolved in patient care should receive educationand training, relevant to their post, on theimportance of providing adequate nutrition.[[DD((GGPPPP))]]
Education and training should cover:
• nutritional needs and indications for nutritionsupport
• options for nutrition support (oral, enteral andparenteral)
• ethical and legal concepts
• potential risks and benefits
• when and where to seek expert advice.[[DD((GGPPPP))]]
Healthcare professionals should ensure that care provides:
• food and fluid of adequate quantity andquality in an environment conducive to eating
• appropriate support, for example, modifiedeating aids, for people who can potentiallychew and swallow but are unable to feedthemselves. [[DD((GGPPPP))]]
Healthcare professionals should ensure that allpeople who need nutrition support receive
coordinated care from a multidisciplinary team22.[[DD((GGPPPP))]]
All acute hospital trusts should have amultidisciplinary nutrition support team whichmay include: doctors (for examplegastroenterologists, gastrointestinal surgeons,intensivists or others with a specific interest innutrition support), dietitians, a specialist nutritionnurse, other nurses, pharmacists, biochemistryand microbiology laboratory support staff, andother allied healthcare professionals (for example,speech and language therapists). [[DD((GGPPPP))]]
All hospital trusts should have a nutrition steeringcommittee working within the clinical governanceframework. [[DD((GGPPPP))]]
Members of the nutrition steering committee shouldbe drawn from trust management, and includesenior representation from medical staff, catering,nursing, dietetics, pharmacy and other healthcareprofessionals as appropriate, for example, speechand language therapists. [[DD((GGPPPP))]]
All acute hospital trusts should employ at leastone specialist nutrition support nurse. [[DD((GGPPPP))]]
The specialist nutrition support nurse should workalongside nursing staff, as well as dietitians andother experts in nutrition support, to:
• minimise complications related to enteral tubefeeding and parenteral nutrition
• ensure optimal ward-based training of nurses
• ensure adherence to nutrition support protocols
• support coordination of care between thehospital and the community. [[DD((GGPPPP))]]
ORGANISATIONS OF NUTRITION SUPPORT IN HOSPITAL AND THE COMMUNIT Y 61
22 The composition of this team may differ according to setting and local arrangements.

33..99.. RReesseeaarrcchh rreeccoommmmeennddaattiioonnss
FFuurrtthheerr rreesseeaarrcchh iiss rreeqquuiirreedd ttoo aasscceerrttaaiinn wwhheetthheerraann eedduuccaattiioonnaall iinntteerrvveennttiioonn ((ee..gg.. 33 oonnee wweeeekkmmoodduullaarr ccoouurrsseess,, oovveerr 66 mmoonntthhss)) ffoorr aallll hheeaalltthhccaarreepprrooffeessssiioonnaallss,, iinn ppaarrttiiccuullaarr mmeeddiiccaall aanndd nnuurrssiinnggssttaaffff iinncclluuddiinngg tthhoossee wwhhoo wwoorrkk wwiitthh ppeeooppllee wwiitthhddeemmeennttiiaa aanndd tthhee iimmppaacctt tthhaatt tthhiiss wwoouulldd hhaavvee oonnppaattiieenntt ccaarree ((ii..ee.. aaffffeecctt oonn nnuuttrriittiioonnaall ssttaattuuss,,lleennggtthh ooff hhoossppiittaall ssttaayy,, ffrreeqquueennccyy ooff GGPP vviissiittss,,ccoommpplliiccaattiioonnss aanndd qquuaalliittyy ooff lliiffee)) ccoommppaarreedd ttoo nnooffoorrmmaall eedduuccaattiioonn??
It is known that healthcare professionals in boththe hospital and community setting have a poorknowledge of nutrition. This is partly due toreceiving a minimal amount of education innutrition during their undergraduate or basictraining. It is therefore essential to determinewhether an organised nutrition support educationprogramme to healthcare professionals wouldimprove the choice made about nutrition supportand the consequent care of patients prescribednutrition support.
NUTRITION SUPPORT IN ADULTS62

44..11.. NNuuttrriittiioonnaall aasssseessssmmeenntt
Early identification of patients who arenutritionally depleted (or likely to become so) isvital if you are to provide help and achieve themost effective use of resources. Althoughbiochemical measurements can contribute tonutritional assessment, none are always a reliablemeasure of nutritional risk e.g. a low serumalbumin is almost always a marker of an acutephase response or saline overload rather than amarker of malnutrition. There is therefore noalternative to measurements of weight andheight, along with other anthropometric measuresin specialist circumstances. These measurementsare then used in conjunction with considerationof the following:
• Has the patient been eating a normal andvaried diet in the last few weeks?
• Has the patient experienced intentional orunintentional weight loss recently? Obesity orfluid balance changes and oedema may maskloss of lean tissue. Rapid weight loss is aconcern in all patients whether obese or not.
• Can the patient eat, swallow, digest and absorbenough food safely to meet their likely needs?
• Does the patient have an unusually high needfor all or some nutrients? Surgical stress,trauma, infection, metabolic disease, wounds,bedsores or history of poor intake may allcontribute to such a need.
• Does any treatment, disease, physicallimitation or organ dysfunction limit thepatient’s ability to handle the nutrientsneeded to meet current or futurerequirements?
• Does the patient have excessive nutrientlosses through vomiting, diarrhoea, surgicaldrains etc.?
• Does a global assessment of the patientsuggest under nourishment? Low body weight,loose fitting clothes, fragile skin, poor woundhealing, apathy, wasted muscles, poorappetite, altered taste sensation, alteredbowel habit. Discussion with relatives may beimportant.
• In the light of all of the above, can the patientmeet all of their requirements by voluntarychoice from the food available?
Considering all the above takes time andexpertise and so simple, repeatable screeningtools designed to be used by non-experts havebeen developed to identify those in need of morecareful assessment.
44..22.. WWhhyy aanndd hhooww ttoo ssccrreeeenn
Several studies have found that malnutrition iswidespread among hospital in-patients and
common in some community settings 94,337. Manyscreening tools have been developed to help
identify such individuals 105,173 and given the highprevalence of malnutrition and lack of propermanagement of patients in various settings,routine nutritional ‘screening’ should result inearly identification of patients who might haveotherwise been missed.
Nutritional screening in this context is not a standalone procedure since the assessments of heightand weight are arguably useful clinicalmeasurements which provide a reliable baselinefor reference in future episodes of care - enabling
SCREENING FOR MALNUTRITION AND THE RISK ,OF MALNUTRITION IN HOSPITAL AND THE COMMUNIT Y 63
4. Screening for malnutrition and the risk of malnutrition in hospital and the community

the clinician to reliably document changes inweight with intercurrent acute illness or chronicillness. Thus, although clinicians must ask patientswhether their height and weight can be measured(and where this is declined the patient’s wishesmust be respected), it is probably not necessaryfor the normal requirements of screening to bemet (e.g. formal consent and explanation ofdifferent possible pathways of care that mightresult from measurement). ‘Screening’ asdiscussed in this document therefore refers tocombined initial clinical assessment and screeningfor risk of malnutrition.
If patients agree to ‘screening’, then the outcomeshould be documented - including whereappropriate decisions on how to pursue thediagnosis underlying any malnutrition or risk ofmalnutrition, intervention plans to combat themalnutrition and timelines for review and or remeasurement. The ‘screening’ should thereforehelp to establish reliable pathways of care forpatients with malnutrition including provision ofsupport, advice for junior clinicians, access todietitians, provision of adequate follow-up, andattention to continuity of care across sectorboundaries (e.g. malnourished patients dischargedto the community).
Routine assessment of weight and height inhospitals as well as in high-risk groups in thecommunity has been recommended by many
expert panels 94,202,217,297,322. However, despitethese efforts and publicity, recent studies suggestthat weight and height of patients are still notsystematically recorded in hospitals, making itdifficult to estimate BMI, change in weight and
risk of malnutrition 56. It is also known that manynutritional screening tools were developed withno reference to defined methodological criteria11,173. Recently, however, an easy to use, validnutritional screening tool with clear criteria, the‘Malnutrition Universal Screening tool’ (MUST)
was developed 94 and this or an equivalent hasbeen widely recommended in an attempt toimprove quality of nutritional care in hospitals
and other care settings 252. MUST can be used forthe screening of both malnutrition and obesity.MUST has limitations – for example the
measurement of height may not always bepossible in order to calculate BMI, but in suchcases alternative measurements are suggested.
Other tools can also be used 105,173 but MUSThas been shown to be simple and easy toimplement with initial training requirements ofless than one hour. It has also had some
validation 94.
Introducing any programme, however, can invokecosts to health systems (personnel time andtreatment costs) and problems for patients (e.g.because of false negatives, false positives, andside effects from potential treatments). It istherefore important to try and assess theeffectiveness of nutritional ‘screening’ similar to
other areas of care 300.
A nutritional screening programme refers to theapplication of a screening tool in a group ofpatients or apparently healthy individuals, forwhom the level of malnutrition risk is unknown, inorder to establish the level of risk.
44..33.. MMeetthhooddss
In view of the above, a systematic review ofevidence for the benefits of screening formalnutrition was conducted, taking care to try todistinguish between screening and assessment(assessment is more detailed and targets patientsalready considered to be ‘at risk’ of malnutrition,whilst screening targets patients for whom therisk of under-nourishment is unknown). Inpractice, however, the line between the two isoften blurred and so careful attention is neededwhen examining the relevant literature.Furthermore, nutritional screening can be offeredas a stand alone intervention or as part of a widerstrategy (e.g. a multi-component screeningand/or interventional strategy for qualityimprovement). Such a ‘multiple screening andintervention package’ has been reported inprimary care settings for older people.
NUTRITION SUPPORT IN ADULTS64

44..44.. SSttuuddiieess ccoonnssiiddeerreedd ffoorr tthhiiss rreevviieeww
The systematic review aimed to examine the (cost)effectiveness of nutritional screening in improvingquality of care (professional practice) and patientoutcomes compared with usual care.
Because of a perceived lack of good qualityevidence it was decided a priori that allexperimental and quasi-experimental studies inwhich nutritional screening is compared with acontrol intervention (e.g. usual care) would beeligible for inclusion in the review. In line withthe guideline scope, studies from the hospital andcommunity setting were considered eligible.
44..55.. CClliinniiccaall eevviiddeennccee
Three primary studies were considered eligible forinclusion (Table 24). The studies wereheterogeneous in their designs, settings,interventions and outcomes. Therefore, noquantitative synthesis was conducted.
One study, a cluster randomised trial, had been
conducted in a US primary care setting 237. Theintervention practices offered screening for eightailments (including malnutrition) to patients olderthan 70 years on their first visits to the practices.The study found participating physicians werereceptive to the intervention; but it did not resultin any improvement in detection rate, nutritionalintervention rate or patients’ quality of life.However, the study was underpowered and therewere concerns about the quality of the screeningtool used in the study.
The other two studies had been conducted inhospitals. One UK controlled study offerednutritional screening to patients admitted totwo hospital wards and used a further two
wards as controls177. The control wards receivedusual care. The mean age of the hospitalisedpatients was 67. As a result of the intervention,patients’ weight recording in the interventionwards increased from 26% to 72% while itdecreased in the control wards. The studyobserved no change in meal-time observationfor the ‘at risk’ patients, and referral to thedietitians decreased in both intervention andcontrol wards. The study did not report patient
outcomes. This study suffered from weak design and lack of measurement of appropriateoutcomes.
The third study was conducted in three hospitals
in the Netherlands 299. The intervention wasscreening patients older than 60 years formalnutrition (using the MNA-sf), dysphagia anddehydration followed by immediate treatment,including menu modification or supplements. Theintervention was offered in one hospital and theother two acted as controls. The study reportedstatistically significant weight gain and reductionin hospital acquired infection rate in theintervention hospital. It observed no change inpressure ulcer rates and length of hospital stay.The study concluded that targeted nutritionalscreening improved quality of care for olderpatients. For some of the outcomes (e.g. lengthof stay, hospital infection rate) the study did notreport the ‘before’ rates.
44..66.. CCoosstt--eeffffeeccttiivveenneessss eevviiddeennccee
Only one of the above studies evaluated cost or
cost-effectiveness 299. The study found asignificant reduction in complications and asignificant weight gain in the intervention arm(Table 25 and Table 26). In their base case theyfound that the weight gain was achieved at a costof £39 per kg gained. As a sensitivity analysis,hospital costs associated with length of stay wereincluded and the result was that screening wascost-saving; however, length of stay was highlyvariable and not statistically significant.Alternatively, the worst case scenario suggested acost of £369 per kg gained.
It is difficult to judge whether this representsgood value for money since weight gain is noteasily converted into patient outcomes and sincethere is no accepted threshold of cost per kggained and the impact on health-related qualityof life is unclear. Cost-effectiveness modelling onthis topic could provide a clearer answer andcould utilise broader evidence on theeffectiveness of oral nutritional interventions. Anoriginal model was therefore developed for theseguidelines to explore the cost-effectiveness ofmalnutrition screening and intervention.
SCREENING FOR MALNUTRITION AND THE RISK ,OF MALNUTRITION IN HOSPITAL AND THE COMMUNIT Y 65

44..66..11.. CCoosstt--eeffffeeccttiivveenneessss mmooddeell
We conducted a cost-utility analysis, which weundertook from the perspective of the NHS andpersonal social services. Expected costs and healthoutcomes (quality-adjusted life-years) werecalculated using decision analysis, with lifeexpectancies being estimated by life-table analysis.Full details are given in Appendix Five: Cost-Effectiveness Analysis of Malnutrition Screening.
A screening strategy (‘Screen’) was compared witha strategy of ward nurses selecting patients fororal nutrition support using oral nutritionalsupplements with later dietetic input if this wasunsuccessful (‘Nurse’), and with a strategy of nooral nutrition intervention (‘Don’t Treat’). Thetarget population chosen for the base case wasolder inpatients. This population was chosenbecause it is known to have a high prevalence ofmalnutrition and because the majority of RCTsevaluating oral nutrition interventions havefocused on this group. We also conducted asensitivity analysis to explore how the cost-effectiveness of screening varies for otherinpatient populations.
Screening of older inpatients was more effectivebut more costly than the other two strategies.The Nurse strategy was excluded due to extendeddominance, that is to say that not only was it lesseffective than screening but also (when both werecompared with Don’t treat) it had a higher costper QALY gained. The incremental cost per QALYgained for Screen compared with Don’t Treat was£6,800. This would suggest that screening iscost-effective when compared to a threshold of£20,000 per QALY gained. We conducted one-way sensitivity analyses on each of the model’sparameters. In none of the scenarios was Nursethe optimal strategy. The Screen strategy was nolonger cost-effective compared with Don’t Treatonly when:
* the mortality relative risk was high (i.e. therelative risk reduction attributable to oral nutritionsupport was small), or
* the duration of the intervention was long(without a commensurate increase in health gain)
The observation that screening of older inpatientswould increase hospital costs (rather than creatingnet cost savings) is consistent with the findings ofthe one published cost-effectiveness analysis of
malnutrition screening described above299. Thatstudy showed that hospital costs might be reducedif length of stay is reduced. However, they did notfind a significant reduction in length of stay and ourmeta-analysis of the effects of oral nutrition support(Chapter 8) do not indicate significant reductions inlength of stay either.
Table 9 shows a two-way sensitivity analysis thatindicates the cost-effectiveness for Screen versusDon’t Treat, when the population characteristicsof malnutrition risk and mortality are varied. Thered (dark) shaded cells indicate the combinationof assumptions where Screen would NOT be cost-effective, when compared to a threshold of£20,000 per QALY gained. So for example, withan acute background mortality of 1.5%, aprevalence of malnutrition of 3% would beenough to make screening cost-effective. This ison the basis that the relative risk reductionassociated with oral nutrition support is the samefor all groups; all data and assumptions used aredetailed in Appendix Five: Cost-EffectivenessAnalysis of Malnutrition Screening. In hospitalinpatients generally the prevalence ofmalnutrition has been estimated to be around
25%336 and using HES data3 we estimate thatmortality in adult inpatients is around 4%, whichwould imply that screening will be very cost-effective in most hospital departments.
NUTRITION SUPPORT IN ADULTS66

The model’s base case assumptions weredeliberately conservative in the following ways.We assumed that the risk reduction observed inthe trials did not continue beyond the observationperiod. Also, we assumed that a proportion ofpatients would have enteral tube-feeding, eventhough this guideline does not advocate tube-feeding, except where oral nutrition is notpossible. As part of the Screen strategy weincluded the cost of nurse time for monitoringand assisting patients to eat, whereas it could beargued that these activities should already bepracticed as part of basic standards of care.
There are a few assumptions that might bias themodel in favour of screening. The level ofcompliance achieved and clinical effect observedin the trials might be greater than that achievablein normal clinical practice, where protocols mightbe less rigorously enforced and patients less wellselected. Certainly, it has been observed that thewastage of oral nutritional supplements in NHS
hospitals can be very high132, but this might wellbe reduced if proper screening protocols led tobetter selection of patients and more rigorousapplication of interventions.
In our model, we also estimated that the cost perpatient of training and quality assurance wasrather low; however, the published cost-
effectiveness analysis299 based on a realintervention showed these costs to be rather highbecause they were averaged over only 140patients. We would argue that such costs can be
kept low if screening is conducted at a hospital-wide level, and would urge implementers to takethis into consideration.
44..66..22 TTrraannssffeerraabbiilliittyy ttoo ootthheerr sseettttiinnggss
We believe that the model reflects with areasonable level of accuracy the costs andbenefits of screening, given the particularintervention strategies specified and thepopulations covered by the clinical trials included.However, with alternative strategies or alternativesettings/populations the cost-effectiveness couldbe quite different.
The nutrition intervention that was costed in ourmodel comprised of oral nutritional supplements,nurse time and dietitian time (and tube-feedingfor a small minority of patients). If alternativeintervention strategies are used the cost-effectiveness could be different – less labour-intensive interventions might be less costly butthey might also be less effective.
In general practice, screening could be less cost-effective than in hospital if patients at risk aremore likely to be identified without the use of ascreening tool because their co-morbidities areknown to practice staff or if the incidence ofmalnutrition is lower than in hospital.Furthermore, the paucity of evidence about riskreduction, and the likelihood that risk reductionfrom intervention would be less in a lower riskpopulation makes it even more difficult to assess.In the community, oral nutritional supplements
SCREENING FOR MALNUTRITION AND THE RISK ,OF MALNUTRITION IN HOSPITAL AND THE COMMUNIT Y 67
All-cause mortality in 60 days from admission Patients at moderate or
highmalnutrition
1.0% 1.5% 2.0% 2.5% 3.0% 3.5% 4.0%1% 65,300 44,400 33,900 27,600 23,400 20,400 18,200 2% 37,800 26,000 20,000 16,500 14,100 12,500 11,200 3% 28,600 19,800 15,400 12,800 11,100 9,800 8,900 4% 24,000 16,800 13,100 11,000 9,500 8,500 7,700 5% 21,200 14,900 11,700 9,800 8,600 7,700 7,000 6% 19,400 13,700 10,800 9,100 8,000 7,100 6,500 7% 18,100 12,800 10,200 8,600 7,500 6,800 6,200 8% 17,100 12,200 9,700 8,200 7,200 6,500 6,000
risk
TTaabbllee 99:: CCoosstt--eeffffeeccttiivveenneessss ((ccoosstt ppeerr QQAALLYY ggaaiinneedd)) ooff ssccrreeeenniinngg iinnppaattiieennttss,, bbyy mmaallnnuuttrriittiioonn rriisskk aanndd bbaasseelliinnee mmoorrttaalliittyy

would also be purchased at the full NHS list pricerather than the heavily discounted hospital price.
Similar arguments are likely to apply in carehomes, and residents in such settings may also beless amenable to intervention or to risk reductionfrom intervention (e.g. those with multiple andsevere co morbidities). In addition, screening maybe less cost-effective if the life expectancy ofpatients is low therefore the potential benefitsfrom intervention are less. There are alsoincreased costs of care with added days of life,which ought to be considered in the evaluation ofcost-effectiveness, along with improvements inquality of life.
Evidence that typical patients in the communitymay possibly benefit less for intervention (andhence less from screening) comes from the threestudies using more typical patients in thecommunity - the elderly malnourished, often in a
nursing home setting 87,195,379 . The estimatesfrom these studies suggest a benefit fromsupplements of increased weight but no mortalitybenefit, in contrast to the net overall mortalitybenefit identified by the meta-analysis.
Due to the difficulty of the generalising theevidence from hospital settings to primary caresettings, our recommendations for primary carecentre more around opportunistic clinicalmanagement rather than a systematic screeningprogramme - hence we advocate baseline‘screening’ at registration with the practice or carehome, and then with subsequent clinical concern.
44..66..33 CCoonncclluussiioonnss
Using the evidence from the literature and expertopinion, we found that malnutrition screening inolder hospital inpatients is likely to be cost-effective, although there is still some uncertainty,given the broad confidence intervals for theclinical effects associated with oral nutritionsupport. Screening is also likely to be cost-effective for other inpatient groups, except wheremalnutrition risk and acute background mortalityare very low. The cost-effectiveness of screeningin other settings is harder to determine.
44..77.. CCoonnsseennssuuss ddeevveellooppmmeenntt mmeetthhooddss
Because of weaknesses in the methodologies anddesigns of the identified studies, no firmconclusion could be made and the cost-effectiveness model also highlighted uncertaintiesin the value of screening. The group thereforeconducted a consensus development exercise toutilise the expertise of the GDG for makingrecommendations.
We used a modified Delphi approach for
consensus development33,242. It comprised threestages: two rounds of Delphi questionnaire surveys(plus an in-group discussion meeting), and then anominal group technique meeting. It was decideda priori that if 80% of the members agreed on arecommendation, then the consensus had beenachieved. After each Delphi round, the resultswere quantitatively summarised and fed back tothe group in meetings. The views expressed in thesurveys were anonymised and presented to all themembers. In the nominal group techniquemeeting, all the members expressed their views, inrounds, about all potential recommendations.Final votes were obtained privately. The results ofthe consensus development exercisesdemonstrated the existence of consensus for allfour pre-defined settings.
44..88.. IImmppaacctt ooff nnuuttrriittiioonnaall aasssseessssmmeenntt oonn tthhee ppaattiieenntt
Patient representatives on the GDG recognisedthe importance of nutritional assessment andscreening as being in the patient’s interest. Goodcommunication skills and a non-judgementalattitude by healthcare professionals will help tocreate a suitable environment in which thepatient will feel comfortable to be open andprovide accurate and helpful information.
Aspects of nutritional assessment and routinemeasurements of weight, height and otheranthropometric measurements may be perceivedby the patient as an invasion of personal spaceand information. Healthcare professionals shouldbe aware of this and respect the patient’s dignity:this information should be documented andstored both for future reference and to minimiseunnecessary repetition.
NUTRITION SUPPORT IN ADULTS68

44..99.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
Screening for malnutrition and the risk ofmalnutrition should be carried out by healthcareprofessionals with appropriate skills and training.[[DD((GGPPPP))]]
All hospital inpatients on admission and alloutpatients at their first clinic appointmentshould be screened. Screening should be repeatedweekly for inpatients and when there is clinicalconcern for outpatients. [[DD((GGPPPP))]]
Hospital departments who identify groups ofpatients with low risk of malnutrition may opt outof screening these groups. Opt-out decisionsshould follow an explicit process via the localclinical governance structure involving experts innutrition support. [[DD((GGPPPP))]]
People in care homes should be screened onadmission and when there is clinical concern.[[DD((GGPPPP))]]
Screening should take place on initial registrationat general practice surgeries and when there is
clinical concern23. Screening should also beconsidered at other opportunities (for example,health checks, flu injections). [[DD((GGPPPP))]]
Screening should assess body mass index (BMI)24
and percentage unintentional weight loss andshould also consider the time over which nutrientintake has been unintentionally reduced and/orthe likelihood of future impaired nutrient intake.The Malnutrition Universal Screening Tool(MUST), for example, may be used to do this.[[DD((GGPPPP))]]
44..1100.. RReesseeaarrcchh rreeccoommmmeennddaattiioonnss
WWhhaatt aarree tthhee bbeenneeffiittss ooff aa nnuuttrriittiioonnaall ssccrreeeenniinnggpprrooggrraammmmee ((uussiinngg aa ssiimmppllee ttooooll ssuucchh aass tthhee‘‘MMaallnnuuttrriittiioonn UUnniivveerrssaall SSccrreeeenniinngg TTooooll’’ ((‘‘MMUUSSTT’’))))ccoommppaarreedd ttoo nnoott ssccrreeeenniinngg ppaattiieennttss iinn;; aa))pprriimmaarryy ccaarree ((aatttteennddiinngg GGPP cclliinniiccss)),, bb)) ccaarreehhoommeess cc)) hhoossppiittaall iinnppaattiieennttss dd)) hhoossppiittaalloouuttppaattiieennttss ee))ppaattiieennttss wwiitthh ddeemmeennttiiaa iinn tteerrmmss ooffddeetteerrmmiinniinngg tthhee nnuummbbeerr ooff ppaattiieennttss aatt rriisskk ooffmmaallnnuuttrriittiioonn,, ccoommpplliiccaattiioonnss,, ssuurrvviivvaall,, hhoossppiittaallaaddmmiissssiioonn rraatteess,, lleennggtthh ooff ssttaayy,, qquuaalliittyy ooff lliiffeeaanndd ccoosstt eeffffeeccttiivveenneessss??
There is no clear evidence available as towhether screening is really beneficial or how itshould be carried out. With the lack of evidencethe GDG have considered in detail this problemand have instead carefully developed consensusstatements to support recommendations forscreening. As a priority it is important that wedetermine the need for screening andintervention in the community.
SCREENING FOR MALNUTRITION AND THE RISK ,OF MALNUTRITION IN HOSPITAL AND THE COMMUNIT Y 69
23 Clinical concern includes, for example, unintentional weight loss, fragile skin, poor wound healing, apathy, wasted muscles, poor appetite,altered taste sensation, impaired swallowing, altered bowel habit, loose fitting clothes or prolonged intercurrent illness.24 BMI is weight (kg)/height(m2) (weight in kilograms divided by height in metres squared).
.
55..11 IInnttrroodduuccttiioonn
Food and nutrition intake is fundamental to goodhealth and resistance to disease. There is apositive duty at common law to care for andprovide such treatment as is in the patient’s bestinterests and to take such reasonable steps as arenecessary to preserve life. Where nutrition asfood and fluid (including nutrition support) isnecessary to preserve life, the duty of care willnormally require the supply of such nutrition ornutrition support. There will be circumstances inwhich the provision of nutrition or nutritionsupport is not clinically indicated or where riskstrying to provide nutrition outweigh the potentialbenefits. Prolonging life will usually be in thebest interests of a patient provided that thetreatment is not excessively burdensome ordisproportionate to the expected benefits.
In the majority of cases an adequate dietaryintake can be achieved by providing good food, aslong as care is taken to ensure that theappropriate consistency of food is used andphysical help with eating is provided whennecessary. In hospitals, it is also important thatmeals are not missed and that restrictions onintake related to investigations or surgicalprocedures are minimized.
Nutrition support involves the provision ofnutrition beyond that provided by normal foodintake using oral supplementation, or enteral tubefeeding(ETF) and parenteral nutrition (PN). Theoverall aim of nutrition support is to try to ensurethat total nutrient intake (food + nutritionsupport) provides enough energy, protein, fluidand micronutrients to meet all the patients’needs. When feasible, it should be given via the
gastrointestinal (GI) tract, which is generallyeffective and relatively inexpensive. The followingmethods can be used:
• Modified food and menus
• Food fortification
• Proprietary oral nutritional supplement
• Enteral tube feeding (ETF)
Feeding via the GI tract is also relatively safealthough there are some risks if ETF is needed(Chapter 9).
If the GI tract cannot be accessed or there iseither partial or complete intestinal failure (e.g.with obstruction, ileus, extensive surgical resectionor malabsorption), some or all of a patient’snutritional needs may be met using anintravenous infusion of parenteral nutrition (PN).This entails risks (Chapter 10 Parenteral nutrition)and costs but should always be considered if it isthe only way to feed a patient effectively.
55..22.. MMeetthhooddoollooggyy
Decisions on when and to whom nutrition supportshould be offered can be difficult and requirecareful consideration. Oral, enteral and parenteralmethods of nutrition support are not mutuallyexclusive and although we carried out a number ofreviews on the benefits and risks of oral, enteraland parenteral interventions, the literature does notyield data that provide hard evidence on theindications for nutrition support for the reasonsoutlined in Section 1.12. The GDG therefore reliedon their expert knowledge through clinical practice
NUTRITION SUPPORT IN ADULTS70
5. Indications for nutrition support

to agree by informal consensus the generalguidance on indications for oral, enteral and orparenteral nutrition support (although morespecific guidance in circumstances where there isan evidence base is provided in the individualchapters or oral, enteral and parenteral feeding).The GDG agreed that consideration of thefollowing is needed when making decisions on theneed for nutrition support:
• The extent to which the patient’s nutritionalneeds are met through ordinary eating anddrinking.
• The length of time that intake has beeninadequate and/or is likely to remaininadequate.
• The patient’s current nutritional status interms of BMI, recent unintentional weight lossand evidence of any specific nutrientdeficiencies.
• The patient’s current medical conditions
• Whether nutrition support will serve thepatient’s best interests in terms of bothclinical outcomes and quality of life, havingregard to all relevant ethical and legal issues.
• The potential methods available to providenutrition support and whether these wouldentail any clinical risks.
• Difficulties arise when trying to define fixedcriteria on instigating nutrition support sincethe first of the three factors listed areinfinitely variable. Support may thus beneeded in patients who have had a mildnutritional deficit for a prolonged period, acomplete deficit for a short period, oranything in between.
55..33.. AApppprroopprriiaattee NNuuttrriittiioonn SSuuppppoorrtt aanndd eetthhiiccaall//lleeggaall iissssuueess
The provision of nutrition support is not alwaysappropriate. Decisions on withholding orwithdrawing nutrition support can be difficult.Decisions which involve the withholding orwithdrawing of nutrition support require aconsideration of both ethical and legal principles(both at common law and statute including theHuman Rights Act 1998). It is important to note:
• it is a general legal and ethical principle thatvalid consent must be obtained before startingtreatment for a patient. A health professionalwho does not respect this principle may beliable both to legal action by the patient andaction by their professional body.
• for consent to be valid it must be givenvoluntarily, by an appropriately informedperson who has the capacity to consent.
• for capacity the person must be able tocomprehend and retain the informationmaterial to the decision, the consequences ofhaving or not having the treatment and beable to use that information in the decisionmaking process.
• no one is able to consent to or refusetreatment on behalf of another competentadult where that adult cannot consent for himself;
• the competent adult has the absolute right todecide what treatment he does or does notwish to receive even where refusal may resultin the death of the patient;
• where the patient lacks the capacity to makea decision for himself, the law requires adoctor to provide such treatment and care asare in the patient’s best interests;
• ‘best interests’ are not confined to ‘medicalbest interests’ and are not necessarily thesame as the wishes of the patient;
• in considering what is in the ‘best interests’ ofthe patient the doctor should consult withfamily and carers and take their views intoaccount in the decision making process;
INDICATIONS FOR NUTRITION SUPPORT 71

• in respect of those patients detained underthe Mental Health Act 1983, healthcareprofessionals should not make the assumptionthat such patients lack the capacity to consentand as with all other patients, an assessmentshould be undertaken as to whether or notsuch patients retain the capacity to consent tothe treatment under consideration;
• regard should be had to communicationdifficulties with the help of relatives, carers,interpreters and speech and languagetherapists;
• patient autonomy and the right to selfdetermination do not extend to the patientinsisting on receipt of a particular treatmentregardless of its nature;
• a distinction has to be drawn between thosecases where a patient’s life can be prolongedindefinitely by treatment or provision ofnutrition, but only at a cost of great sufferingand those cases where the ‘incompetent’patient is in the final stages of life andalthough treatment would prolong the dyingprocess, this would be at the cost of comfortand dignity;
• each case must be considered individually anddecisions as to the provision, withholding orwithdrawal of nutrition reached objectively;
• decisions involving the withholding andwithdrawal of treatment can be particularlydifficult and at times contentious and in thesecircumstances consideration should be giventhe GMC guidance ‘Withholding andWithdrawing Life-prolonging Treatments:
Good Practice in Decision-making’122 andlegal advice sought if appropriate.
• if there is any doubt as to the patient’scapacity or what is or is not in their bestinterests, legal advice should be sought and ifappropriate the Court’s intervention sought.
Additionally:• if an illness is regarded as being in the
terminal phase and the treatment plan is toprovide only compassionate and palliativecare, an artificial supply of nutrients or fluidneed only be given to relieve symptoms andsuch provision should not necessarily be usedto prolong survival;
• in cases where the benefits of specialisednutrition or fluid support are in doubt, aplanned ‘time-limited’ trial may be useful; and
• treatment plans for patients should includedecisions on fluid and/or nutrient provision,especially when there are either existing orpossible future deficits in fluid or nutrient intake.
55..44.. RRaattiioonnaallee ffoorr rreeccoommmmeennddaattiioonnss
Since it is impossible to make firm recommendationsto cover all circumstances, decisions on instigatingnutrition support should ideally involve individualswith expertise in clinical nutrition such as dietitians,specialist nutrition nurses, and pharmacists andclinicians with relevant training (see Chapter 3).However, in reality there are many malnourishedpatients in both hospital and community settingsand hence it is important that all healthcareprofessionals understand the importance ofmalnutrition and its treatment in patient care. TheseGuidelines therefore provide broad recommendationson when to consider active nutritional interventionbased on the principles outlined in Chapter 2,combined with consideration of the ethical and legalprinciples involved.
55..44..11 RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
5.4.1.1 Indications
Nutrition support should be considered in peoplewho are malnourished, as defined by any of thefollowing:
• a BMI of less than 18.5 kg/m2
• unintentional weight loss greater than 10%within the last 3–6 months
• a BMI of less than 20 kg/m2 andunintentional weight loss greater than %within the last 3–6 months. [[DD((GGPPPP))]]
NUTRITION SUPPORT IN ADULTS72
Nutrition support should be considered in peopleat risk of malnutrition who, as defined by any ofthe following:
• have eaten little or nothing for more than 5days and/or are likely to eat little or nothingfor the next 5 days or longer
• have a poor absorptive capacity, and/or havehigh nutrient losses nd/or have increasednutritional needs from causes such as catabolism. [[DD((GGPPPP))]]
Healthcare professionals should consider usingoral, enteral or parenteral nutrition support, aloneor in combination, for people who are either
malnourished25 or at risk of malnutrition26.Potential swallowing problems should be takeninto account. [[DD((GGPPPP))]]
Healthcare professionals involved in starting orstopping nutrition support should:
• obtain consent from the patient if he or she iscompetent
• act in the patient’s best interest if he or she isnot competent to give consent
• be aware that the provision of nutritionsupport is not always appropriate. Decisionson withholding or withdrawing of nutrition support require a consideration of both ethical and legal principles (both at commonlaw and statute including the Human RightsAct 1998).
When such decisions are being made guidance
issued by the General Medical Council27 and the
Department of Health28 should be followed.[[DD((GGPPPP))]]
Healthcare professionals should ensure thatpeople having nutrition support, and their carers,are kept fully informed about their treatment.They should also have access to appropriateinformation and be given the opportunity todiscuss diagnosis and treatment options. [[DD((GGPPPP))]]
INDICATIONS FOR NUTRITION SUPPORT 73
25 Malnourished: BMI <18.5 kg/m2, unintentional weight loss >10% within the last 3-6 months, a BMI<20 kg/m2 and unintentional weight loss>5% within the last 3-6 months.26 At risk of malnutrition: eaten little or nothing for more than 5 days and/or likely to eat little or nothing for the next 5 days or longer or poorabsorptive capacity, and or high nutrient losses and or increased nutritional needs from causes such as catabolism.27 Witholding and withdrawing life prolonging treatments: good practice in decision making. General Medical Council. Available from www.gmc-uk.org28 Reference guide to consent for examination or treatment (2001) Department of Health. Available from www.dh.gov.uk

NUTRITION SUPPORT IN ADULTS74
55..55.. PPaattiieenntt PPaatthhwwaayy AAllggoorriitthhmm
Yes
Is the patient malnourished or at risk from malnutrition?
Repeat screening:
• weekly for inpatients
• where there is clinical concern for patients in the community
At all stages of care: • Consider cultural, ethical and legal issues of providing nutrition support • Provide patients with information about their treatment • Ensure that there is a care pathway with clear treatment goals
Screen: Hospital:
• inpatients on admission • all outpatients at their first clinic appointment
Community: • Residents or patients in care homes on admission • Patients registering at general practice• Patients where there is clinical concern
Consider appropriate form of nutrition
support
No
Enteralinterventions (algorithm 5.7)
Parenteralinterventions(algorithm 5.7)
And/ or
And/ or
Prescribenutritionsupport
Review
Monitor
Patient having long term nutrition support
Patient having short term nutrition support
Review Review
Oralinterventions(algorithm 5.6)

INDICATIONS FOR NUTRITION SUPPORT 75
55..66.. OOrraall AAllggoorriitthhmm
No
No
Yes
Yes
Patient is malnourished or at risk of malnutrition on screening
This patient should undergo a nutritional assessment by a suitably qualified health professional (e.g. Dietitian, NST), in line with local policies.
Does the patient have any of the obvious or less obvious indicators for
dysphagia?
Review indications for, route, risks, benefits and goals of nutrition support at regular intervals depending on the patient and care setting.
Nutritional intake may be improved by: • Treating contributory symptoms e.g.
nausea• Support/supervision at mealtimes • Expert assessment by a dietitian.
If further weight loss or BMI already <18.5kg/m2 and/or unintentional weight loss >10% within the last 3-6 months or BMI <20kg/m2 and unintentional weight loss >5% , within the last 3-6 months then options:• Increasing menu choice and provision of
snacks• Support/supervision at mealtimes • Food fortification • Oral nutritional supplements • Vitamin and mineral supplements to
meet dietary reference values (DRV).
(these options are not exclusive and canbe used in combination)
Continue modified food and liquids and to monitor intake, body weight, and severity of
dysphagia and review need for intervention monthly
Is nutritional intake satisfactory?
No
Patient is unable to meet nutritional needs through oral
route alone See Enteral and Parenteral
Support Algorithm
Yes
No
No
Is the patient’s GI tract accessible and
functioning and is the patient likely to meet
nutritional needs through the oral route alone?
Stop nutrition support if/when normal diet meets adequate nutritional needs and maintains nutritional status
Refer patient for assessment by a healthcare professional with specialist training in diagnosis, assessment and management of swallowing disorders (e.g. speech and language therapists).
No
Can oral intake be safely maintained by use of
modified food and liquids?
Yes
Stop nutrition support if/when normal diet meets adequate nutritional needs and maintains nutritional status.
Yes
Is nutrient intake adequate and is weight stable or
increasing?

NUTRITION SUPPORT IN ADULTS76
55..77.. EEnntteerraall aanndd PPaarreenntteerraall AAllggoorriitthhmm
No
Yes
Yes
Yes
Yes
Yes
No
No
No
No
Yes
No
NoYes
Patient unable to meet nutritional needs through oral route alone – seek expert advice (e.g. NST and/or dietitian)
Is the patient’s GI tract accessible and functioning?
Do you anticipate that intestinal absorptive function will meet all nutritional needs?
Consider parenteral nutrition
+/- enteral/ oral nutrition
Is the oesophagus and/ or stomach absent?
Is there impaired gastric emptying?
After consideration of risk vs benefit, is a
trial of NG tube feeding +/- oral
nutrition appropriate?
Is feeding likely to be short term
(e.g. <4 weeks)?
Are methods to improve gut
function (e.g. prokinetics)successful?
NG tube +/- oral nutrition
Gastrostomy +/- oral nutrition
Is adequate nutrient intake achieved and
tolerated ?
Review of the indications for, route, risks, benefits and goals of nutrition support at regular intervals depending on the patient, care setting and duration of nutrition support. Intervals between monitoring may increase as the patient is stabilised on nutrition support.
Review need to continue nutritional support
Jejunal feeding +/- oral nutrition
Is the GI tract obstructed?
No
Yes
No
Yes
Stop parenteral nutrition support if/when adequate oral and or enteral nutrition support meets nutritional needs and maintains nutritional status.Stop enteral tube feeding if/when oral intake meet adequate nutitionl needs and maintain nutritional status..

66..11.. BBaacckkggrroouunndd
Individual patients’ nutritional needs vary withtheir current and past nutritional history and thenature of their condition. It is therefore essentialto estimate nutritional requirements beforeinstigating nutrition support. Since eitherinadequate or excessive macronutrient ormicronutrient provision can be harmful,recommendations on appropriate levels wouldideally be based on large studies comparing theeffects of different levels of feeding on clinicaloutcomes e.g. complications, length of stay, andmortality. However, relatively few such studieshave been published and hence therecommendations in this part of the guidelinewere proposed by a number of GDG memberswho have expertise in this area and a knowledgeof other widely accepted levels of feeding
including those recommended by BAPEN39 and
the PEN Group345. These accepted levels evolvedover several decades from studies of metabolicrate and nitrogen balance along withmeasurements of electrolyte and micronutrientstatus in both healthy volunteers and patients.Nevertheless, members of the GDG have concernsabout some aspects of current practice,particularly the potential over provision ofnutrition in early feeding of severely ill or injuredpatients (see Section 6.6).
66..22 GGeenneerraall PPrriinncciipplleess
The overall aim when devising a prescription,whether for oral, enteral or parenteral nutrition, isto provide the patient with their completerequirements via single or combined routes. Theprescription of any supplementary nutritionsupport by enteral or parenteral routes should
therefore account for any current oral intake fromfood and/or oral nutritional supplements.
The usual approach to estimating nutritionalneeds is to estimate energy requirements fromcalculations of basal metabolic rate (usingequations accounting for age, sex and bodyweight) with the addition of increments to allowfor any physical activity and increases inmetabolism caused by illness and feeding itself(see Section 5.3). Protein requirements areestimated from body weight with additionalincrements dependent on likely metabolic stressand hence catabolism. A prescription is thendevised to meet the estimated energy and proteinrequirements. This can then be exceeded if bodyweight recovery is indicated or less can be given ifweight loss would be beneficial or there areconcerns about a patient’s ability to tolerate thefeed in terms of re-feeding risks (see Section 6.6)or metabolic instability (see Section 5.4). In allpatients, likely micronutrient, electrolyte and fluidneeds must also be met, taking into account anyunusual demands or losses.
The aims and objectives of nutrition supportshould be clearly defined at each stage of thepatient’s illness with nutrition support tailoredaccordingly e.g. limitation but not prevention oflean tissue loss in acutely ill patients,maintenance in stable patients who still haveincreased catabolism, and anabolism in patientsonce the catabolic phase has passed.Requirements and prescription must therefore beregularly reviewed to account for changes inactivity levels, goals of treatment, clinicalcondition and care setting.
WHAT TO GIVE IN HOSPITAL AND THE COMMUNIT Y 77
6 What to give in hospital and the community

In patients requiring long-term nutrition support,it is useful to decide on a ‘target weight’ and tomake adjustments to the level of nutritionprovided in order to achieve it. The target weightmay sometimes be lower than an optimal‘healthy’ weight since the latter may beimpossible or inappropriate to achieve in illpatients (especially those with gastrointestinaldysfunction). Occasionally, the target weightmay be higher than that considered optimal forhealth since it is not always reasonable to expectsevere weight reduction in obese patients withillness and eating problems.
66..33.. CCaallccuullaattiinngg rreeqquuiirreemmeennttss
66..33..11 EEnneerrggyy
A number of equations are available to calculate
basal metabolic rate (BMR) e.g. Schofield 1985309
to which increments are added to account forincreased energy requirements caused by themetabolic stress of disease and variations in activitylevels etc. Tables summarising these increments areused by experts in nutrition support to tailorrequirements to individual patients needs and
those recommended by the PEN Group345. Theyinclude guidance on the special requirements fordifferent patient groups such as the obese. Formost patients, however, 20-30 kcal/kg/day islikely to be adequate although patients who areseverely malnourished or severely ill might need tocommence feeding at lower levels (Section 6.6) andpatients who have reached an anabolic state mayhave greater requirements.
The energy delivered by nutrition support is notonly derived from metabolism of the carbohydrateand fat content of the feed but also, unless thepatient is anabolic, from metabolism of anamount of protein at least equivalent to all thatprovided within the feed. It is thereforeinappropriate in most cases of nutrition supportto consider matching estimated energyrequirements from ‘non-protein energy’ content offeeds, whatever the route of administration.
66..33..22 PPrrootteeiinn
For most patients in both hospital and communitysettings, 1g/kg/day will provide sufficientprotein (corresponding to approximately 0.15g Nfrom amino acids in intravenous nutrition).However in situations of metabolic stress,requirements may be higher although the GDGwould not recommend the provision of levelsgreater than 1.5 g/kg/day (0.24g nitrogen/kg).
66..33..33 FFlluuiidd
Fluid needs are usually a total of 30 - 35 ml/kgbody weight in both hospital and communitysetting with allowance for extra losses fromdrains, fistulae etc. All sources of fluid must beconsidered to stop over-prescription in patientsreceiving enteral/parenteral feeds including anyoral intake and other intravenous sourcesespecially the large amounts of fluid given withsome intravenous drugs. This is a particularproblem for surgical patients since excess fluidand sodium is a common cause of oedema,prolonged ileus and other complications.
66..33..44 EElleeccttrroollyytteess aanndd mmiinneerraallss
Most standard oral and enteral feeds containenough electrolytes and minerals to meet thedaily requirements of sodium, potassium,calcium, magnesium and phosphate, but only ifthe patient is having enough of the feed to meetall their energy needs. Since many patients areeither receiving less than full nutrition fromthese products or have pre-existing deficits, highlosses or increased demands, additional provisionis often required. However, care is needed toavoid excessive provision in some patients e.g.those with renal or liver impairment. Somespecialised feeds are designed specifically forpatients with low total energy needs to provideadequate electrolytes, vitamins and minerals inlower total calories. .
Pre-mixed PN bags contain very variable amountsof electrolyte and minerals and care is needed toavoid giving PN with either inadequate orexcessive electrolyte and/or mineral content.
NUTRITION SUPPORT IN ADULTS78

66..33..55 MMiiccrroonnuuttrriieennttss
Micronutrients are required for the prevention orcorrection of deficiency states and maintenance ofnormal metabolism and anti-oxidant status. Aswith electrolytes and minerals, most standard oraland enteral feeds contain enough vitamins andtrace elements to ensure that needs are met if thepatient is taking enough feed to meet their dailyenergy needs. However, when this is not the case,further balanced micronutrient supplementationmay be required especially in those with pre-existing deficits, poor absorption, increaseddemands or high losses. Food fortification withboth high-energy foodstuffs (e.g. cream or butter)or commercial products need to be used withparticular caution since they usually contain verylow and unbalanced levels of micronutrients.
Premixed PN bags invariably contain inadequatelevels of some micronutrients and therefore needadditions to be made prior to administration. Theprovision of PN without adequate micronutrientcontent must be avoided.
66..33..66 FFiibbrree
Oral and enteral feeds with added fibre should beconsidered for those on long term feeding.
66..44 CCoonncceerrnnss wwiitthh pprreessccrriibbiinngg lleevveellss
Although the levels of feeding suggested in Section6.4 are similar to those previously advocated bymany expert groups, including the BDA, BAPEN andESPEN, they often result in high levels of energy andprotein being prescribed for patients who areseverely ill. This concerned members of the GDGsince severe illness is associated with ‘metabolicinstability’ and poor tolerance of feeding.Furthermore, a number of clinical observations raisethe possibility that high levels of early feeding maycause problems. These observations include:
• feeding at levels above actual requirementsadvocated widely during the early developmentof PN, had adverse effects on clinical outcome.
• the very high, early energy requirements seenin the severely ill often decline swiftly so thatinitial estimates of nutritional needs canrapidly become over-estimates.
• most trials showing benefit from short-termnutrition support, do so despite ‘too littlenutrition’ being given for ‘too short a time’ forthe benefit to accrue from maintaining or
improving body energy and protein stores168
• higher levels of feeding increase oxygenconsumption and carbon dioxide production
and hence may worsen respiratory failure12,13.
• severely ill patients are often insulin resistantand so high levels of feeding will producerelative hyperglycaemia. This is of particularconcern since a large intensive care trialdemonstrated outcome benefits from tight
blood glucose control362.
• Although studies have shown that higherlevels of protein provision (e.g. 1.5gprotein/kg/day) may reduce net lean tissueloss, they have not shown better clinicaloutcomes. Furthermore, very high levels ofprotein provision (e.g. 2g protein/kg/day) donot yield additional lean tissue sparing.
• the amino acids (AAs) needed for synthesis ofacute-phase proteins differ from thoseprovided in either food or commerciallyavailable nutrition support products whichgenerally meet the needs for normal synthesis
of structural and transport proteins etc288.Excess nitrogen provision could therefore leadto an excess of free AAs which may havedetrimental effects unless they are eitheroxidised or metabolism is diverted away fromacute phase protein synthesis into more‘normal’ pathways.
• high protein and or/high energy feeding hasbeen shown to increase mortality in animal
models of sepsis (e.g. Peck et al, 1989274)
• the mortality of very malnourished,oedematous, severely ill adults in refeedingcamps following famine has been shown to beincreased by high protein provision comparedto those receiving low protein diets (e.g.
Collins et al, 199868) as has that of children
(Scherbaum et al, 2000307).
WHAT TO GIVE IN HOSPITAL AND THE COMMUNIT Y 79
• a retrospective observational study ofoutcomes in ICU patients showed that survivalwas best amongst patients receiving 33-66%of their nutrient needs compared to thosereceiving either <33% or >66% (although theGDG recognize that there are several possibleexplanations for such observations)
Meeting the high estimates of nutritional needsduring early feeding of the severely ill maytherefore cause problems and the practice ofcautious introduction of nutrition support (e.g. at50% of calculated requirement) is nowwidespread. The GDG therefore made thefollowing recommendations.
66..55.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
Healthcare professionals who are skilled andtrained in nutritional requirements and methodsof nutrition support should ensure that the total
nutrient intake29 of people prescribed nutritionsupport accounts for:
• energy, protein, fluid, electrolyte, mineral,
micronutrients30 and fibre needs
• activity levels and the underlying clinicalcondition – for example, catabolism, pyrexia
• gastrointestinal tolerance, potential metabolicinstability and risk of refeeding problems
• the likely duration of nutrition support.[[DD((GGPPPP))]]
For people who are not severely ill or injured, norat risk of refeeding syndrome, the suggested
nutritional prescription for total intake29 shouldprovide all of the following:
• 25–35 kcal/kg/day total energy (including
that derived from protein31 32)
• 0.8–1.5 g protein (0.13–0.24 gnitrogen)/kg/day
• 30–35 ml fluid/kg (with allowance for extralosses from drains and fistulae, for example,
and extra input from other sources – forexample, intravenous drugs)
• adequate electrolytes, minerals, micronutrients(allowing for any pre-existing deficits,excessive losses or increased demands) andfibre if appropriate. [[DD((GGPPPP))]]
The prescription should be reviewed according to theperson’s progress, and care should be taken when:
• using food fortification which tends tosupplement energy and/or protein withoutadequate micronutrients and minerals
• using feeds and supplements that meet fullenergy and nitrogen needs, as they may notprovide adequate micronutrients and mineralswhen only used in a supplementary role
• using pre-mixed parenteral nutrition bags thathave not had tailored additions frompharmacy. [[DD((GGPPPP))]]
66..66 RRee--ffeeeeddiinngg PPrroobblleemmss
66..66..11 BBaacckkggrroouunndd
Re-feeding problems encompass life-threateningacute micronutrient deficiencies, fluid andelectrolyte imbalance, and disturbances of organfunction and metabolic regulation that may resultfrom over-rapid or unbalanced nutrition support.They can occur in any severely malnourishedindividuals but are particularly common in thosewho have had very little or no food intake, evenincluding overweight patients who have eatennothing for protracted periods.
• The problems arise because starvation causesadaptive reductions in cellular activity andorgan function accompanied by micronutrient,mineral and electrolyte deficiencies.Abnormalities in malnourished individualsmay therefore include: deficiencies of vitaminsand trace elements;
• whole body depletion of intracellularpotassium, magnesium and phosphate;
NUTRITION SUPPORT IN ADULTS80
29 Total intake includes intake from any food, oral fluid, oral nutritional supplements, enteral and/ or parenteral nutrition support and intravenous fluid.30 The term micronutrient is used throughout the guideline to include all essential vitamins and trace elements.31 This level may need to be lower in people who are overweight, BMI >25.32 When using parenteral nutrition it is often necessary to adjust total energy values listed on the manufacturers information which may notinclude protein energy values.

• increased intracellular and whole body sodiumand water;
• low insulin levels and a partial switch fromcarbohydrate metabolism to ketonemetabolism to provide energy.
• impaired cardiac and renal reserve withdecreased ability to excrete an excess salt andwater load.
• abnormalities of liver function
Giving nutrients and fluid to malnourished patientswill reverse these changes but in doing so leads toan increase in demands for electrolytes andmicronutrients, and a simultaneous shift of sodiumand water out of cells. Over-rapid or unbalancednutrition support can therefore precipitate acutemicronutrient deficiencies and dangerous changesin fluid and electrolyte balance.
The problems of refeeding are less likely to arisewith oral feeding since starvation is usuallyaccompanied by a loss of appetite, however careshould be taken in the prescription of oral nutritionsupplements particularly in the area of eatingdisorders. Enteral tube or PN feeding can precipitatere-feeding problems since excessive feeding levelscan be achieved easily. The problem can also beexaggerated if the products do not includeadequate vitamins, phosphate or electrolytes.
The two widely recognized problems of re-feeding arethose of the classical ‘Re-Feeding Syndrome’ and the‘Wernicke-Korsakoff Syndrome’. Since the nature ofrefeeding precludes randomised trials of treatment,recommendations are derived from expert opinion.
66..66..22 TThhee ccllaassssiiccaall ‘‘RRee--FFeeeeddiinngg SSyynnddrroommee’’
6.6.2.1 Clinical description
‘Re-Feeding Syndrome’ occurs on feeding when arange of life-threatening clinical and biochemicalabnormalities arise:
• cardiac failure, pulmonary oedema anddysrhythmias
• acute circulatory fluid overload or circulatoryfluid depletion
• hypophosphataemia
• hypokalaemia
• hypomagnesaemia and occasionallyhypocalcaemia
• hyperglycaemia
Any patient who has had very little food intakefor >5 days is at some risk of re-feeding problems.Nutrition support for these patients shouldtherefore be introduced at a maximum of 50% ofrequirements for the first 2 days, before increasingto meet full needs if close clinical andbiochemical monitoring reveals no refeedingproblems. However, much greater care is neededin some patients, particularly those meeting anyof the following criteria:
• BMI <16 kg/m2
• unintentional weight loss of >15% within theprevious 3 – 6 months
• very little or no nutrient intake for >10 days
• low levels of potassium, phosphate ormagnesium prior to any feeding.
Patients with two or more of the following lesser criteria are also at high re-feeding risk:
• BMI <18.5 kg/m2
• unintentional weight loss >10% within theprevious 3-6 months
• very little or no intake for >5 days
• a history of alcohol abuse or some drugsincluding insulin, chemotherapy, antacids ordiuretics
6.6.2.2 Clinical management of patients at
high re-feeding risk
Patients at high risk of re-feeding syndromeshould commence feeding at very low levels ofenergy and protein but with generous provision ofthiamin and other B group vitamins, along with abalanced multi-vitamin and trace elementsupplement (since they are likely to have multipledeficits that cannot be met by low level oral,enteral or parenteral intake). Levels can then beincreased over the next few days as carefulmonitoring reveals no problems.
WHAT TO GIVE IN HOSPITAL AND THE COMMUNIT Y 81

Most patients at high re-feeding risk also needgenerous supplementation of potassium,magnesium and phosphate from the onset offeeding unless blood levels are already high (thismay be the case in patients who have renalimpairment). It is important to appreciate thatpatients with normal pre-feeding levels ofpotassium, magnesium and phosphate can still beat high risk, and that many of those with highplasma levels will still have whole body depletionand may therefore need supplementation as re-feeding progresses and renal function improves.
The GDG do not agree with previousrecommendations from some groups that allfeeding should be withheld in patients with lowlevels of potassium, magnesium or phosphateuntil these have been corrected. The rationaleunderlying this disagreement is that since the vastmajority of the deficits are intracellular, theycannot be corrected without commencing low-level energy provision. Any reassurance gainedfrom pre-feeding correction of plasma levels istherefore unlikely to reflect significant changes inwhole body status or significant reduction in risks.
66..66..33 TThhee WWeerrnniikkee--KKoorrssaakkooffff ssyynnddrroommee
6.6.3.1 Clinical description
The Wernike-Korsakoff syndrome is caused byacute thiamin deficiency when re-feeding ofmalnourished patients precipitates increasedthiamin demand as starving cells switch back tocarbohydrate metabolism. The syndrome of acuteneurological abnormalities comprises of one ormore of the following:
• apathy and disorientation
• nystagmus, opthgalmoplegia or other eyemovement disorders
• ataxia
• severe impairment of short-term memory oftenwith confabulation.
It is seen particularly frequently in alcoholics whomay have low liver stores of thiamin. It can alsooccur in any patient with chronic vomitingincluding those with hyperemesis gravidarum andgastric outlet obstruction.
6.6.3.1 Clinical management
Patients should be managed as for “re-feedingsyndrome” with particularly high doses of dailythiamin and other B vitamins intravenously for 3days (e.g. pabrinex 1 + 2 o.d + oral thiamin100mg every 6hrs + Vitamin B Co strong 1 b.d.).The eye signs and impairment of consciousnessusually resolve but the loss of short-term memorymay be permanent.
66..66..44.. OOtthheerr rree--ffeeeeddiinngg ssyynnddrroommeess
Other re-feeding issues may occur that are lesseasily characterized on clinical or biochemicalgrounds. Some experts believe that these mayarise in less obviously malnourished patientswhen significant metabolic stress, redirection ofmetabolic processes or organ dysfunction acutelyalters fluid distribution and the levels/demandsof vitamins and electrolytes.
66..66..55.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
Nutrition support should be cautiously introducedin seriously ill or injured people requiring enteraltube feeding or parenteral nutrition. It should bestarted at no more than 50% of the estimatedtarget energy and protein needs. It should bebuilt up to meet full needs over the first 24–48hours according to metabolic and gastrointestinaltolerance. Full requirements of fluid, electrolytes,vitamins and minerals should be provided fromthe outset of feeding. [[DD((GGPPPP))]]
People who have eaten little or nothing for morethan 5 days should have nutrition supportintroduced at no more than 50% of requirementsfor the first 2 days, before increasing feed rates tomeet full needs if clinical and biochemicalmonitoring reveals no refeeding problems. [[DD((GGPPPP))]]
People who meet the criteria in Box 4 should beconsidered to be at high risk of developingrefeeding problems. [[DD((GGPPPP))]]
NUTRITION SUPPORT IN ADULTS82

BBooxx 44 CCrriitteerriiaa ffoorr ddeetteerrmmiinniinngg ppeeooppllee aatt hhiigghh rriisskk ooffddeevveellooppiinngg rreeffeeeeddiinngg pprroobblleemmssPPaattiieenntt hhaass oonnee oorr mmoorree ooff tthhee ffoolllloowwiinngg::
• BMI less than 16 kg/m2
• unintentional weight loss greater than 15%within the last 3–6 months
• little or no nutritional intake for more than 10 days
• low levels of potassium, phosphate ormagnesium prior to feeding.
OOrr ppaattiieenntt hhaass ttwwoo oorr mmoorree ooff tthhee ffoolllloowwiinngg::
• BMI less than 18.5 kg/m2
• unintentional weight loss greater than 10%within the last 3–6 months
• little or no nutritional intake for more than 5 days
• a history of alcohol abuse or drugs includinginsulin, chemotherapy, antacids or diuretics.
People at high risk of developing refeedingproblems (Box 4) should be cared for byhealthcare professionals who are appropriatelyskilled and trained and have expert knowledge ofnutritional requirements and nutrition support.[[DD((GGPPPP))]]
The prescription for people at high risk ofdeveloping refeeding problems should consider:
• starting nutrition support at a maximum of 10kcal/kg/day, increasing levels slowly to meetor exceed full needs by 4–7 days
• using only 5 kcal/kg/day in extreme cases(for example, BMI less than 14 kg/m2 ornegligible intake for more than 15 days) andmonitoring cardiac rhythm continually in thesepeople and any others who already have ordevelop any cardiac arrythmias
• restoring circulatory volume and monitoringfluid balance and overall clinical status closely
• providing immediately before and during thefirst 10 days of feeding: oral thiamin200–300 mg daily, vitamin B co strong 1 or 2tablets, three times a day (or full dose dailyintravenous vitamin B preparation, ifnecessary) and a balanced multivitamin/traceelement supplement once daily.
• providing oral, enteral or intravenoussupplements of potassium (likely requirement2–4 mmol/kg/day), phosphate (likelyrequirement 0.3–0.6 mmol/kg/day) andmagnesium (likely requirement 0.2mmol/kg/day intravenous, 0.4 mmol/kg/dayoral) unless pre-feeding plasma levels arehigh. Pre-feeding correction of low plasmalevels is unnecessary. [[DD((GGPPPP))]]
66..77.. RReeccoommmmeennddaattiioonnss ffoorr rreesseeaarrcchh
FFuurrtthheerr rreesseeaarrcchh iinnvveessttiiggaattiinngg tthhee ooppttiimmaall lleevveellssooff eenneerrggyy aanndd nniittrrooggeenn pprroovviissiioonn ffoorr sseevveerreellyy iillll oorriinnjjuurreedd ppaattiieennttss dduurriinngg tthhee eeaarrllyy ppaarrtt ooff tthheeiirriillllnneessss iiss nneeeeddeedd uussiinngg cclliinniiccaall eennddppooiinnttss ssuucchh aassiinnffeeccttiioonn aanndd mmoorrttaalliittyy rraatteess rraatthheerr tthhaann cchhaannggeessiinn aanntthhrrooppoommeettrryy aanndd eessttiimmaatteedd nnuuttrriieenntt bbaallaannccee..
WHAT TO GIVE IN HOSPITAL AND THE COMMUNIT Y 83

77..11.. IInnttrroodduuccttiioonn
The main objectives of monitoring nutritionsupport are:
1. To ensure nutrition support is provided safely,and to detect and treat clinical complicationsas early and effectively as possible.
2. To assess the extent to which nutritionalobjectives have been reached.
3. To alter the type of nutrition support, or thecomponents of the regimen, to improve itseffectiveness and to minimise or preventmetabolic complications.
To achieve these objectives monitoring protocols(Table 10 and Table 11) which integrate a varietyof observations and measurements, are required.These will usually include:
• Basic clinical observations (temperature, pulse,oedema)
• Observations specifically relating to the feedingtechnique and its possible complications
• Measures of nutritional intake (appetite, oralfood intake and total intake, gastrointestinalfunction).
• Weight
• Fluid balance charts (in hospital)
• Laboratory data
• Outcome factors (complications, improvementsin aspects of nutritional status, length of stay)
• Change in socio-psychological state whichmight influence nutritional therapy
The type and frequency of monitoring will dependon the nature and severity of the underlyingdisease state, whether previous results wereabnormal, the type of nutrition support used, thetolerance of nutrition support, the setting of thenutritional care, and the expected duration ofnutrition support.
Laboratory tests usually involve analyses of serumor plasma, but may also require tests on wholeblood or blood cellular components. Tests ofurinary loss are rarely required (although urinarysodium may be useful in patients with complexelectrolyte problems). Most tests are non- specific,and abnormalities can be caused by factors otherthan the nutritional component of interest, andespecially by aspects of the disease process. Caremust therefore be exercised in interpretation ofresults, particularly when patients are subject tothe effects of the Acute Phase Reaction (APR), orSystemic Inflammatory Response Syndrome (SIRS)such as after surgery, trauma or infection, in thecritically ill, or if they have a chronic inflammatorydisease state.
77..22.. MMeetthhooddss
We conducted a literature search to identifystudies that looked at the impact of monitoringnutrition support compared with no monitoring.Since no trials that prospectively investigated thediagnostic efficacy or cost- effectiveness ofmonitoring could be identified, we conducted asurvey within the GDG to try to identify currentbest practice. The recommendations onmonitoring provided here were then developed bymembers of the GDG with specific clinicalexpertise in this area and were agreed by theGDG using informal consensus.
NUTRITION SUPPORT IN ADULTS84
7. Monitoring of nutrition support in hospital and the community

The above approach recognises that the guidelinesfor monitoring patients on nutrition support givenin Table 10 and Table 11 will need to be agreed bylocal Nutrition Support Teams or other experts innutritional care, and that final protocols willtherefore vary depending upon local clinicalexperience and local availability of particular tests.They will also be modified in individual casesaccording to clinical progress of the patient.
77..33.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
Healthcare professionals should review theindications, route, risks, benefits and goals ofnutrition support at regular intervals. The timebetween reviews depends on the patient, caresetting and duration of nutrition support.Intervals may increase as the patient is stabilisedon nutrition support. [[DD((GGPPPP))]]
People having nutrition support in hospital shouldbe monitored by healthcare professionals with therelevant skills and training in nutritionalmonitoring. [[DD((GGPPPP))]]
Healthcare professionals should refer to theprotocols for nutritional, anthropometric andclinical monitoring, shown in Table 10, whenmonitoring people having nutrition support inhospital. [[DD((GGPPPP))]]
Healthcare professionals should refer to theprotocols for laboratory monitoring, shown inTable 11, when monitoring people havingnutrition support in hospital. Table 11 isparticularly relevant to parenteral nutrition. Itcould also be selectively applied when enteral ororal nutrition support is used, particularly forpeople who are metabolically unstable or at riskof refeeding syndrome. The frequency and extentof the observations given may need to beadapted in acutely ill or metabolically unstablepeople. [[DD((GGPPPP))]]
People having parenteral nutrition in thecommunity need regular assessment andmonitoring. This should be carried out by homecare specialists and by experienced hospital teams(initially at least weekly), using observationsmarked * in Table 10. In addition, they should bereviewed at a specialist hospital clinic every 3–6months. Monitoring should be more frequentduring the early months of home parenteralnutrition, or if there is a change in clinicalcondition, when the full range of tests in Tables10 and 11 should be performed. Some of theclinical observations may be checked by patientsor carers. [[DD((GGPPPP))]]
People having oral nutrition support and/orenteral tube feeding in the community should bemonitored by healthcare professionals with therelevant skills and training in nutritionalmonitoring. This group of people should bemonitored every 3–6 months or more frequently ifthere is any change in their clinical condition. Alimited number of observations and tests fromTable 10 should be performed. Some of theclinical observations may be checked by patientsor carers. If clinical progress is satisfactory,laboratory tests are rarely needed. [[DD((GGPPPP))]]
If long-term nutrition support is needed patientsand carers should be trained to recognise andrespond to adverse changes in both their well-being and in the management of their nutritionaldelivery system. [[DD((GGPPPP))]]
MONITORING OF NUTRITION SUPPORT IN HOSPITAL AND THE COMMUNIT Y 85

NUTRITION SUPPORT IN ADULTS86
TTaabbllee 1100:: PPrroottooccooll ffoorr nnuuttrriittiioonnaall,, aanntthhrrooppoommeettrriicc aanndd cclliinniiccaall mmoonniittoorriinngg ooff nnuuttrriittiioonn ssuuppppoorrtt
Parameter
NNuuttrriittiioonnaall
Nutrient intake from oral,enteral or parenteral nutrition(including any change inconditions that are affectingfood intake)
Actual volume of feeddelivered*
Fluid balance charts (enteral and parenteral)
AAnntthhrrooppoommeettrriicc
Weight*
BMI*
Mid-arm circumference*
Triceps skinfold thickness
GGII ffuunnccttiioonn
Nausea/vomiting*
Diarrhoea*
Constipation*
Abdominal distension
EEnntteerraall ttuubbee –– nnaassaallllyy iinnsseerrtteedd
Gastric tube position (pH lessthan or equal to 5.5 using pHpaper – or noting position ofmarkers on tube once initialposition has been confirmed)
Nasal erosion
Fixation (is it secure?)
Is tube in working order (all pieces intact, tube notblocked/kinked)?
Frequency
Daily initially, reducing to twice weeklywhen stable
Daily initially, reducing to twice weeklywhen stable
Daily initially, reducing to twice weeklywhen stable
Daily if concerns regarding fluidbalance, otherwise weekly reducing tomonthly
Start of feeding and then monthly
Monthly, if weight cannot be obtainedor is difficult to interpret
Monthly, if weight cannot be obtainedor is difficult to interpret
Daily initially, reducing to twice weekly
Daily initially, reducing to twice weekly
Daily initially, reducing to twice weekly
As necessary
Before each feed begins
Daily
Daily
Daily
Rationale
To ensure that patient is receivingnutrients to meet requirements andthat current method of feeding is stillthe most appropriate. To allowalteration of intake as indicated
To ensure that patient is receivingcorrect volume of feed. To allowtroubleshooting
To ensure patient is not becomingover/under hydrated
To assess ongoing nutritional status,determine whether nutritional goalsare being achieved and take intoaccount both body fat and muscle
To ensure tolerance of feed
To rule out any other causes of diarrhoeaand then assess tolerance of feeds
To rule out other causes of constipationand then assess tolerance of feeds
Assess tolerance of feed
To ensure tube in correct position
To ensure tolerance of tube
To help prevent tube becomingdislodged
To ensure tube is in working order

MONITORING OF NUTRITION SUPPORT IN HOSPITAL AND THE COMMUNIT Y 87
TTaabbllee 1100:: PPrroottooccooll ffoorr nnuuttrriittiioonnaall,, aanntthhrrooppoommeettrriicc aanndd cclliinniiccaall mmoonniittoorriinngg ooff nnuuttrriittiioonn ssuuppppoorrtt ((CCoonnttiinnuueedd))
Parameter
GGaassttrroossttoommyy oorr jjeejjuunnoossttoommyy
Stoma site
Tube position (length at externalfixation)
Tube insertion and rotation(gastrostomy without jejunalextension only)
Balloon water volume (balloonretained gastrostomies only)
Jejunostomy tube position bynoting position of external markers
PPaarreenntteerraall nnuuttrriittiioonn
Catheter entry site*
Skin over position of catheter tip(peripherally fed people)*
CClliinniiccaall ccoonnddiittiioonn
General condition*
Temperature/blood pressure
Drug therapy*
LLoonngg--//sshhoorrtt--tteerrmm ggooaallss
Are goals being met?*
Are goals still appropriate?*
Frequency
Daily
Daily
Weekly
Weekly
Daily
Daily
Daily
Daily
Daily initially, then as needed
Daily initially, reducing to monthlywhen stable
Daily initially, reducing to twice weeklyand then progressively to 3–6 monthly,unless clinical condition changes
Daily initially, reducing to twice weeklyand then progressively to 3–6 monthly,unless clinical condition changes
Rationale
To ensure site not infected/red, nosigns of gastric leakage
To ensure tube has not migratedfrom/into stomach and external overgranulation
Prevent internalovergranulation/prevention of buriedbumper syndrome
To prevent tube falling out
Confirmation of position
Signs of infection/inflammation
Signs of thrombophlebitis
To ensure that patient is toleratingfeed and that feeding and routecontinue to be appropriate
Sign of infection/fluid balance
Appropriate preparation of drug (toreduce incidence of tube blockage). Toprevent/reduce drug nutrientinteractions
To ensure that feeding is appropriateto overall care of patient
To ensure that feeding is appropriateto overall care of patient
People at home having parenteral nutrition should be monitored using observations marked *

NUTRITION SUPPORT IN ADULTS88
TTaabbllee 1111 PPrroottooccooll ffoorr llaabboorraattoorryy mmoonniittoorriinngg ooff nnuuttrriittiioonn ssuuppppoorrtt
Parameter
Sodium, potassium,urea, creatinine
Glucose
Magnesium, phosphate
Liver function testsincluding InternationalNormalised Ratio (INR)
Calcium, albumin
C-reactive protein
Zinc, copper
Frequency
Baseline
Daily until stableThen 1 or 2 times a week
Baseline
1 or 2 times a day (or moreif needed) until stable
Then weekly
BaselineDaily if risk of refeedingsyndromeThree times a week untilstableThen weekly
Baseline
Twice weekly until stable
Then weekly
Baseline
Then weekly
Baseline
Then 2 or 3 times a weekuntil stable
Baseline
Then every 2–4 weeks,depending on results
Rationale
Assessment of renalfunction, fluid status, andNa and K status
Glucose intolerance iscommon
Depletion is common andunder recognised
Abnormalities commonduring parenteral nutrition
Hypocalcaemia orhypercalcaemia may occur
Assists interpretation ofprotein, trace element andvitamin results
Deficiency common,especially when increasedlosses
Interpretation
Interpret with knowledge offluid balance and medication
Urinary sodium may be helpfulin complex cases withgastrointestinal fluid loss
Good glycaemic control isnecessary
Low concentrations indicatepoor status
Complex. May be due tosepsis, other disease ornutritional intake
Correct measured serumcalcium concentration foralbumin
Hypocalcaemia may besecondary to Mg deficiency
Low albumin reflects diseasenot protein status
To assess the presence of anacute phase reaction (APR).The trend of results isimportant
People most at risk whenanabolic
APR causes Zn ↓ and
Cu ↑

MONITORING OF NUTRITION SUPPORT IN HOSPITAL AND THE COMMUNIT Y 89
TTaabbllee 1111 PPrroottooccooll ffoorr llaabboorraattoorryy mmoonniittoorriinngg ooff nnuuttrriittiioonn ssuuppppoorrtt ((CCoonnttiinnuueedd))
Parameter
Seleniuma
Full blood count and MCV
Iron, ferritin
Folate, B12
Manganeseb
25-OH Vit Db
Bone densitometryb
Frequency
Baseline if risk of depletion
Further testing dependenton baseline
Baseline
1 or 2 times a week untilstable
Then weekly
Baseline
Then every 3–6 months
Baseline
Then every 2–4 weeks
Every 3–6 months if onhome parenteral nutrition
6 monthly if on long-termsupport
On starting homeparenteral nutrition
Then every 2 years
Rationale
Se deficiency likely insevere illness and sepsis, orlong-term nutrition support
Anaemia due to iron orfolate deficiency is common
Iron deficiency common inlong-term parenteralnutrition
Iron deficiency is common
Excess provision to beavoided, more likely if liverdisease
Low if housebound
Metabolic bone diseasediagnosis
Interpretation
APR causes Se ↓
Long-term status betterassessed by glutathioneperoxidase
Effects of sepsis may beimportant
Iron status difficult if APR (Fe ↓, ferritin ↑)
Serum folate/B12 sufficient,with full blood count
Red blood cell or whole blood better measure of excessthan plasma
Requires normal kidneyfunction for effect
Together with lab tests formetabolic bone disease
a These tests are needed primarily for people having parenteral nutrition in the community.b These tests are rarely needed for people having enteral tube feeding (in hospital or in the community), unless there is cause for concern.

77..44 RReesseeaarrcchh RReeccoommmmeennddaattiioonnss
The following research recommendation wasproposed:
FFuurrtthheerr rreesseeaarrcchh iiss rreeqquuiirreedd ttoo iiddeennttiiffyy wwhhiicchhccoommppoonneennttss ooff nnuuttrriittiioonn mmoonniittoorriinngg aarree cclliinniiccaallllyyaanndd ccoosstt eeffffeeccttiivvee.
There is no clear evidence available in to the longand short term benefits of clinical monitoring interms of prevention of complications and survival.With the lack of evidence the GDG haveconsidered in detail this problem and haveinstead carefully developed the guidance formonitoring by expert clinical practice andconsensus opinion.
NUTRITION SUPPORT IN ADULTS90

88..11.. IInnttrroodduuccttiioonn
Options for oral nutrition support should beconsidered for any patients taking inadequatefood and fluid to meet their requirements,unless they cannot swallow safely or haveinadequate gastrointestinal function. Oraloptions include dietary counselling to facilitatethe addition of ingredients high in energyand/or protein (e.g. butter, cream, milk, sugar);adaptation of meal structures (e.g. 3 meals plus3 snacks); the inclusion of ‘nourishing fluids(milky drinks, fruit juices and smoothies) andthe use of proprietary oral nutritionalsupplements such as nutritionally complete pre-packed drinks or vitamin/mineral tablets.
Proprietary oral nutritional supplements can beprescribed for conditions laid down underBorderline substance guidance. Levels ofelectrolytes in oral and enteral feeds are governedby the EC Directive for Foods for Special MedicalPurposes (1999/21/EC) The aim of oralnutritional supplements is to improve thepatient’s overall food and fluid intake in order toimprove clinical outcomes. It is important thatthe total intake from normal food plus theadditional measures provides a balanced mix ofenergy, protein and micronutrients.
Dietary counselling and nutritional supplementsmay both be used to increase nutrient intakeeither individually or in combination. Dietarycounselling has potential advantages in that itoffers greater variety, can be tailored to individualneeds and may be associated with lower costs tothe health service. It has therefore beensuggested that it should precede the use of
nutritional supplements347. However, provision of
complete oral nutritional supplements is simpleand many are available on prescription although anumber of studies have highlighted problems
with compliance181,241,271. It is not known whetherthese two methods of nutrition support arecomplimentary to one another.
We conducted a number of reviews to investigatethe clinical and nutritional effects of one or moreoral interventions along with a review to identifypatients’ views on some of these interventions.Patient in all settings were included but there wasinsufficient evidence to make separaterecommendations for each setting. However, it islikely that if oral nutritional interventions provideoverall benefit for malnourished patients, thesebenefits will occur regardless of the setting inwhich the nutritional intervention is given. Alldiagnoses were also included in the reviews butonly three areas were identified with enoughspecific studies to warrant separate sectionsin this chapter: surgery, pancreatitis anddysphagic patients.
88..22.. OOrraall nnuuttrriittiioonnaall ssuuppppoorrtt vveerrssuuss ssttaannddaarrdd ccaarree iinn mmaallnnoouurriisshheedd ppaattiieennttss
88..22..11.. SSttuuddiieess ccoonnssiiddeerreedd ffoorr tthhiiss rreevviieeww
Since effects of oral nutritional interventions arelikely to be most evident in patients who aremalnourished or at risk of malnutrition, we onlyaimed to review studies undertaken in suchgroups in both hospital and community settings(Table 27). Ideally, the studies included wouldhave used the same or similar definitions formalnutrition and nutritional risk but unfortunatelyinclusion criteria were variable and in some cases
ORAL NUTRITION SUPPORT IN HOSPITAL AND THE COMMUNIT Y 91
8. Oral nutrition support in hospital and the community
unclear. Consequently, we included any study inwhich it appeared likely from either the reportedcriteria or the clinical setting that at least 50% ofall participants would have had a BMI less than
or equal to 21kg/m2, unintentional weight loss of5% in recent months, or had not been able to eator unlikely to eat for more than five days.
88..22..22 CClliinniiccaall eevviiddeennccee ffoorr oorraall nnuuttrriittiioonnaall ssuupppplleemmeennttssvveerrssuuss ssttaannddaarrdd ccaarree iinn mmaallnnoouurriisshheedd ppaattiieennttss
The review identified 40 RCTs10,19,23,26,31,36,62,79,86-
88,118,121,157,181,187,195,197,199,205,226,228,260,269,270,279,282,2
83,285,302,306,326,344,349,363-365,373,375,379 that lookedat the effectiveness of using an oral nutritionalsupplement. These included studies givingsupplements alone and in combination withdietary counselling. The supplements investigatedwere a combination of proprietary completesupplements (complete supplements contain abalanced mixture of protein, energy, vitamins andminerals), homemade supplements andincomplete supplements (incomplete supplementsdo not contain a complete balance of nutrients).
88..22..33 OOrraall nnuuttrriittiioonnaall ssuupppplleemmeennttss aalloonnee vveerrssuussssttaannddaarrdd ccaarree
Thirty two RCTs compared patients who receivedoral nutritional supplements with patients whoreceived standard care/no intervention19,26,36,62,79,86-88,121,157,181,187,195,197,199,205,226,228,
260,279,283,285,302,306,326,344,349,363-365,375,379. Therewas no form of dietary advice in either arm. Themost frequently reported outcomes were: death,anthropometric measurements (such as weightchange), length of hospital stay, wound healing orcomplications, quality of life and functional status.
Twenty studies19,36,62,79,86,87,121,157,187,197,199,226,279,
283,306,344,349,364,365,379 reported mortality.Although most of the studies showed lowermortality rates in the supplemented group noindividual study showed a significant difference.However, a meta-analysis (Table 13) of thesestudies showed a significant reduction inmortality for the proprietary completesupplements with no significant difference forhomemade or incomplete supplements (althoughonly three small studies reported mortality thistype of intervention).
Nineteen studies provided information on weight
change26,62,87,121,157,181,187,195,205,226,228,260,279,302,306,3
49,363,365,379. Eight showed a significant weightchange in favour of the supplemented
group62,181,195,226,228,260,279,379, although in one ofthese it was only evident in a severely
malnourished sub-group 279. The other studiesshowed no significant difference in weightchange.
Sixteen of the nineteen included studies withenough data to incorporate into a meta-
analysis26,62,87,121,157,181,195,226,260,279,302,306,349,363,365
,379 The meta-analysis showed that those takingproprietary complete supplements62,87,121,181,226,260,279,349,363,365,379 had significantweight gains whereas homemade or incomplete
supplements26,157,195,302,306 only showed a non-significant weight change in favour ofsupplements.
Change in BMI as an outcome was reported in 6
studies62,181,195,285,375,379. Two 62,379 documentedsignificant change favouring the supplementedgroup, one reported that the majority ofparticipants in both groups showed improved ormaintained BMI but did not document the
change285, one reported a significant increase inBMI of men that were supplemented compared tomale controls but no significant differences for
women375 and the last two showed no significant
difference in any groups181,195. Otheranthropometric measurements such as Triceps skinfold (TSF), Mid-arm muscle circumference (MAC),were not reported consistently in studies althoughwhere significant differences were shown theyfavoured the intervention groups.
Twelve studies provided data on length of
stay79,87,121,157,181,279,283,302,326,349,364,375. One showed
a significant reduction in the supplemented group79,four showed no significant difference between
groups181,279,283,326, and seven did not report thesignificance. Our meta-analysis (Appendix Six: Meta-Analyses Oral versus Standard Care) showed nosignificant difference overall for either completeproprietary supplements or non-complete/homemade supplements.
NUTRITION SUPPORT IN ADULTS92

Functional outcomes reported differed from studyto study but where benefit was identified, itfavoured the supplemented group.
Energy and/or protein intake was higher in thesupplemented group in some
studies36,121,181,187,205,228,302,326,363 and wheresignificant benefit was identified it was in favourof the intervention. No study demonstrated abetter intake in the control for this outcome.
Complications were reported in eight
studies36,79,121,181,283,302,326,349. All showed fewercomplications in the supplemented group, thedifference was significant in four
studies36,181,283,326.
88..22..44 OOrraall nnuuttrriittiioonnaall ssuupppplleemmeennttss pplluuss ddiieettaarryyccoouunnsseelllliinngg vveerrssuuss ssttaannddaarrdd ccaarree
Three studies compared oral supplements plus
dietary counselling with standard care31,269,270. All three of these showed a weight gain in thesupplement plus dietary counselling groupcompared to the standard care group, the gain
was significant in two of these studies269,270. Twostudies reported data on energy intake with one
showing no difference between the groups31 andthe other showing a significant increase in the
supplemented group270.
88..22..55 OOrraall nnuuttrriittiioonnaall ssuupppplleemmeennttss pplluuss ddiieettaarryyccoouunnsseelllliinngg vveerrssuuss ddiieettaarryy ccoouunnsseelllliinngg
The review identified five RCTs10,23,118,282,373 thatcompared oral supplements plus dietary
counselling with dietary counselling alone(although dietary counselling is not necessarilystandard care). There was no significantdifference in mortality for the three studies
reporting this outcome 10,23,118. The same threestudies also reported weight change with only
one of them showing a significant difference23,this was in favour of the supplemented group.
Length of stay was reported for two studies23,373,both reported shorter lengths of stay in the controlgroup than the supplemented group but neither
showed a significant difference. Beattie et al23 alsoreported complications, the supplement group hadsignificantly fewer than the control group.
88..22..66 MMeettaa--aannaallyyssiiss ssuummmmaarryy ooff oorraall ssuupppplleemmeennttss vvss..ssttaannddaarrdd ccaarree
Our meta-analysis (Appendix Six: Meta-AnalysesOral versus Standard Care) looked into fourcommonly reported outcomes for oral nutritionalsupplementation. It demonstrated that their useleads to statistically significant increases inweight and statistically significant reductions incomplications and mortality. There was nosignificant effect on length of hospital stayalthough some caution is required wheninterpreting both weight change and length of
stay data. In one study 26, we had to approximatemean weight change from median weight change,and estimate the standard deviation using theweighted mean of standard deviations in theother studies. Similar approaches were needed for
lengths of stay data in four studies79,121,279,349.
ORAL NUTRITION SUPPORT IN HOSPITAL AND THE COMMUNIT Y 93
TTaabbllee 1133:: SSuummmmaarryy ooff mmeettaa--aannaallyyssiiss ooff oorraall nnuuttrriittiioonnaall ssuupppplleemmeennttss vvss.. ssttaannddaarrdd ccaarree
NNoo.. ppaattiieennttss PP vvaalluuee ffrroomm((IInntteerrvveennttiioonn// PPoooolleedd eeffffeecctt tteesstt ffoorrssttaannddaarrdd ccaarree)) [[9955%% CCII]] hheetteerrooggeenneeiittyy
MMoorrttaalliittyy reported in 25 studies10,19,23,36,62,79,86,87,118,121,157,195,197,199,226,269,270,279,
RRRR ((ffiixxeedd))
283,306,344,349,364,365,379 1388/1480 0.82 [0.69, 0.98] 0.63
LLeennggtthh ooff ssttaayy ((ddaayyss)) reported in 14 studies WWMMDD ((rraannddoomm))23,79,87,121,157,181,279,283,302,326,349,364,373,375 760/746 -0.77 [-1.96, 0.41] 0.00001
CCoommpplliiccaattiioonnss reported in 9 studies RRRR ((ffiixxeedd)) 23,36,79,121,181,283,302,326,349 540/622 0.68 [0.59, 0.78] 0.06
WWeeiigghhtt ggaaiinn ((kkgg)) reported in 22 studies23,26,31,62,87,118,121,157,181,195,226,260,269,270,279,282,
WWMMDD ((rraannddoomm))
302,306,349,363,365,379 595/589 1.26 [0.79, 1.74] 0.00001

88..22..77 CCoosstt eeffffeeccttiivveenneessss ooff oorraall nnuuttrriittiioonnaall ssuupppplleemmeennttss
We found one UK and one French study thatcompared the cost of oral nutrition support withstandard care using data extracted from specificRCTs (Studies on the use of support in surgicalpatients rather than generally malnourishedpatients are dealt with separately – see section8.6). Both studies were performed on patients inthe community although in one case patients hadjust been discharged from hospital and in bothcases hospital admissions or readmissions werecosted outcomes.
The UK study was a cost-effectiveness analysis 87
was based on an RCT to determine whethernutritional supplementation reduced health carecosts and improved quality of life in oldermalnourished patients post-discharge. They foundno significant difference in quality of life ofpatients although, the short course of theintervention (8 weeks) made it relatively unlikelythat improvements would be evident. Patients inthe oral supplement arm had significantlyincreased cost (£3034 vs. £1854) due to longerlengths of stay for those who needed readmissionto hospital, even though the increases in lengthof stay were not significant. The reasons for theincreased length of stay were neither clear nordiscussed in the paper. However, although it ispossible that they were a result of theintervention, a misbalance between trial arms(although baseline characteristics of the patientswere similar) or chance within the small studywith varied diagnoses seems more likely.
The French study also evaluated the resource andcost implications of using supplements in older
patients9. It was based on a prospectivecomparison of patient cohorts with one cohort ina region with high rates of oral nutritionalsupplement prescription compared to anothercohort in a region with low prescription rates.Patients in the high frequency arm had asignificantly improved MNA scores, reducednumbers of admissions (in contrast to Edington2004) but no significant reduction in costs.There was no significant difference in mortalityand other patient outcomes, such as quality of lifewere not recorded.
In addition to the above, we also examined an
unpublished report 91 that estimated the costimpact of oral nutritional supplements from anNHS perspective using two separate analysesrelated to lengths of stay or complication rates.These were extracted by meta-analysis fromselected RCTs. The report found relatively fewstudies in the community on which to base anyestimates of cost impact and the majority ofrelevant RCTs identified in hospital settings, werein surgical patients and did not necessarily focuson patients that were malnourished. Both thelength of stay and complication rate showed thatthe use of oral nutritional supplements led toreduced in hospital costs. However, specificadditional costs associated with administeringand monitoring the supplements were notincluded, the bed day costs used did account forassociated nursing time etc. However, the studiesdid not claim to be full cost-benefit analyses andthey do not account for potential additional NHScosts of care related to added weeks of life in anyseriously ill patients and, furthermore, thedifferences in length of stay reported in this studydo not concord with either our meta-analysis or
that in the Cochrane review 231 (neither of whichshow significant reductions in length of stay withoral nutritional supplements).
We also estimated the cost-effectiveness of oralnutrition support in older inpatients in our modelof their use within the context of a malnutritionscreening programme (Section 4.6.1). Thissuggested that screening followed by interventionusing oral nutritional supplements would be cost-effective using the base case assumptionsalthough the results were sensitive to relativelysmall changes in some of the model’s parameters.
8.2.7.1 Conclusions
Overall, although the studies identified were smallwith marked heterogeneity in study populationsand outcomes, they do show improved outcomesfor malnourished patients given oral nutritionalsupplements. These benefits were somewhatinconsistent but our meta-analysis (Appendix Six:Meta-Analyses Oral versus Standard Care) showsthat the use of oral nutritional supplements insuch patients leads to statistically significant
NUTRITION SUPPORT IN ADULTS94
improvements in body weight along withreductions in complications and mortality.Economic modelling of the use of oral nutritionalsupplements within the context of a screeningprogramme undertaken in elderly hospitalpatients also suggests probable cost-effectivenessin terms of cost per QALY <£20,000. However,available RCTs provide too little information andare too underpowered to define these costs with confidence,
88..22..88 TThhee iinnfflluueennccee ooff ccaarree sseettttiinngg ffoorr oorraall nnuuttrriittiioonnaallssuupppplleemmeennttaattiioonn
As stated in the introduction to this section, toofew RCTs on the effects of on oral nutritionsupport in the community were identified to makeseparate recommendations for different patientsettings. Furthermore, we did find some evidencewhich suggests that caution is needed inextrapolating to typical malnourished groups inthe community from the evidence within hospital
studies. Three RCTs 87,195,379 examined the benefitsof oral nutrition support in typical elderlymalnourished patients in community settings(rather than community studies on more unusualpopulations such as those with locally advancedcancer or alcoholic liver disease). These studiessuggested a benefit from supplements in terms ofincreased weight but did not confirm the netmortality benefit in this setting that was identifiedby our meta-analysis. However, overall the paucityof evidence from community studies make it verydifficult to be confident in any real differencesrelated to setting and/or patient population, andmore detailed larger studies are required.
88..22..99 PPaattiieenntt’’ss ssaattiissffaaccttiioonn wwiitthh nnuuttrriittiioonnaall ssuupppplleemmeennttss
A literature search conducted to identify patient’sviews on nutrition support retrieved four studieswhich looked at patients’ preferences for
nutritional supplements 85,142,222,324.
In one US study 324 20 patients and 20 staffmembers of a large teaching hospital rated a varietyof brands of liquid nutritional supplements. Eachparticipant sampled four brands of vanilla productand four brands of an alternate flavour (eitherchocolate or strawberry, based on their personalpreference). The first round of sampling was blinded
(participants did not know the brand of thesupplements) and in the second round the brandwas disclosed. The results of the study indicated thatstaff member ratings of acceptability were lower (insome cases significantly lower) than ratings given bypatients. In general, staff member acceptabilityratings did not change significantly once the brandname was known. Patient acceptability ratingsappeared to be impacted to a much greater degreeby knowing brand name; significant increases wereseen in four ratings.
Another study 85 also looked at differences inpreferences of oral nutritional supplements betweenpatients and dietitians. There were significantdifferences between patients and dietitians in theirevaluation of 7 of their 13 products.
The palatability of sip-feed nutritional supplementsand other high-energy foods to older medical
inpatients was assessed in one study 142. 49malnourished subjects rated the taste of apreviously selected sip-feed supplement and fiveother high-energy foods: cheese biscuit, plain potatocrisps, chocolate, cherry-flavored cereal bar andstout beer. Subjects rated the taste of sip-feeds asfavourable as all other offered foods, with theexception of stout beer which had a lower rate.
Another study 222 examined whether sip-feeds areless preferred and less likely to be selected thanother energy-dense foods in healthy elders; andwhether eating alone further reduces intakerelative to eating in a social setting.
Twenty-one healthy older adults (aged 60-79)were included. Subjects rated six different flavoursof sip-feed (three fruit juice flavours: apple,orange and fruit punch and three milkshakeflavours: vanilla, strawberry and chocolate) andthen rated the pleasantness of the taste of theflavour against five other energy-dense familiarfoods/drinks (cheese cracker, cereal bar, potatochip, chocolate button, and beer). Two drinks, twosalty foods, and two sweet foods were offered tothe participants. Intake was measured whenparticipants ate alone or in a group. Pleasantnessratings were made on a 7-point Likert scale,where 1 represented ‘extremely unpleasant’ and 7represented ‘extremely pleasant’.
ORAL NUTRITION SUPPORT IN HOSPITAL AND THE COMMUNIT Y 95

The results from the study showed that the meanpleasantness of sip-feeds was above neutral(rating of 4) in all but one case (chocolate). Sip-feeds were rated as the third most pleasant (5.0+/- 0.3). The participants’ favourite flavours ofsip-feeds compared well with other more familiarfoods and were selected as part of a snack. Snackintake increased by 60% when consumed in agroup setting compared with eating alone.
8.2.9.1 Conclusions
Patients found oral nutritional supplements anacceptable form of nutrition support.
88..33 DDiieettaarryy aaddvviiccee vveerrssuuss ssttaannddaarrdd ccaarree
88..33..11 SSttuuddiieess ccoonnssiiddeerreedd ffoorr tthhiiss rreevviieeww
One systematic review 17 and one RCT113
investigated the impact of dietary advice. Thepurpose of dietary advice given by a dietitian orhealthcare professional was to provide instructionon modifying food intake (e.g. food fortification,meal plan adaptation) to improve nutritionalintake. ‘No dietary advice’ as used in this context meant patients received no other specificoral intervention.
Two of the sub-group comparisons were ofinterest; dietary advice versus no advice anddietary advice plus supplements (if required)versus no advice and no supplements.
88..33..22 CClliinniiccaall eevviiddeennccee ffoorr ddiieettaarryy aaddvviiccee vveerrssuuss nnooddiieettaarryy aaddvviiccee
The review considered 5 RCTs including 888 olderpeople, cancer and Crohn’s disease patients (Table28). However, only three of these studiesreported outcomes of interest; mortality, hospitaladmission, nutritional status and clinical function.No significant difference was found for mortalityat six months (two studies), hospital admission(one study), weight change and BMI (one study)or measures of clinical function (one study).
88..33..33 CClliinniiccaall eevviiddeennccee ffoorr ddiieettaarryy aaddvviiccee pplluuss oorraallnnuuttrriittiioonnaall ssuupppplleemmeennttss ((iiff rreeqquuiirreedd)) vveerrssuuss nnooddiieettaarryy aaddvviiccee aanndd nnoo oorraall nnuuttrriittiioonnaall ssuupppplleemmeennttss
The Baldwin et al. review 17 also compared patientsreceiving dietary advice plus oral nutritionalsupplements (if required) with those receiving noadvice and no oral nutritional supplements (Table28). Seven RCTs including 665 cancer, surgical andchronic obstructive pulmonary disease patients werecontained within the review although, only twoprovided data on the outcomes of interest whichwere mortality and change in nutritional status. The
separate small RCT 113 also looked at thiscomparison although it also included a third,normal weight group of patients, which we did notinclude in our analysis.
No significant differences for any of the outcomes
were found in either the systematic review 17 or
the small RCT 113.
88..33..44 PPaattiieenntt’’ss ssaattiissffaaccttiioonn wwiitthh ddiieettaarryy aaddvviiccee
We performed a literature search to assesspatient’s views on dietary advice which identified
two studies: one conducted in Canada 356 and the
other in Australia 106. The studies includedhospitalised patients for a minimum stay of 5
days 356 (n=55) and acute hospital patients 106
(n=49). Patients consumed a therapeutic diet andused dietary counselling during their hospitalstay. A survey questionnaire was used to evaluatepatients’ satisfaction with four components of
dietary counselling. One study 356 looked at thefollowing components:
• knowledge: “patient’s perception of thedietitian’s knowledge of his or her medicalcondition, dietary therapy, and foodcomposition of meals served in the hospital.”
• cognitive communication skills: “dietitian’s useof simple language in verbal and writtencommunications and in answering patient’squestions”
• affective communication skills: “interpersonalqualities of the dietitian (e.g., courtesy,warmth, and attentiveness) that help build apositive relationship with the patient”
NUTRITION SUPPORT IN ADULTS96

• facilitation skills: “dietitian customization ofthe diet, inclusion of the patient in decisionmaking, and dispensation of advice to thepatient about adapting the diet afterdischarge from the hospital”
• The other study 106 assessed the followingelements:
• Staff interpersonal skills: These included staffcommunication skills and understanding ofpatients’ needs.
• Nutrition supplements: Temperature, taste,smell and appearance of nutritionalsupplements
• Perceived health benefits of nutrition care:Effect of dietary advice on patient’s health
• Staff presentation skills: These includedwhether staff were polite, courteous andfriendly.
The result from the studies indicated that staff
facilitation skills, knowledge 356 and interpersonal
skills 106 were the most important factors ofpatient satisfaction with dietary advice.
8.3.4.1 Conclusions
Staff facilitation skills were the most importantdeterminant of patients’ satisfaction with dietaryadvice.
88..33..66 CCoosstt--eeffffeeccttiivveenneessss eevviiddeennccee ffoorr ddiieettaarryy aaddvviiccee
No study reporting cost or cost-effectiveness ofdietary advice was found.
88..33..77 CCoonncclluussiioonnss
We were unable to demonstrate any evidence ofeffect for dietary advice but studies were too smalland heterogeneous to allow any conclusions. Manyalso failed to report outcomes of interest and thereis no relevant economic evidence
88..44.. OOrraall nnuuttrriittiioonnaall ssuupppplleemmeennttss vveerrssuuss ddiieettaarryy aaddvviiccee
88..44..11.. SSttuuddiieess ccoonnssiiddeerreedd ffoorr tthhiiss rreevviieeww
We looked for studies that compared one type oforal nutrition support with another, for examplethree meals per day versus six meals per day, snacksor dietary advice to improve nutritional status versusoral nutritional supplement, oral nutritionalsupplement versus placebo multivitamin pills, inmalnourished patients or patients at risk ofmalnutrition (Table 29). One systematic review andone RCT met the inclusion criteria. The systematicreview compared the effects of dietary advice to no
advice or other oral interventions 17, and the RCTcompared dietary advice with oral supplements and
also standard care 285.
88..44..22 CClliinniiccaall eevviiddeennccee ffoorr ddiieettaarryy aaddvviiccee oorr ssnnaacckkssvveerrssuuss oorraall nnuuttrriittiioonnaall ssuupppplleemmeennttss
We identified one systematic review 17 whichincluded 4 RCTs covering 173 older, HIV and
cystic fibrosis patients, and one additional RCT 285
that included 111 colorectal cancer patientsundergoing radiotherapy treatment, compareddietary advice or snacks with oral nutritional
supplements. The Ravasco RCT 285 includedpatients regardless of nutritional status but didprovide some results for 42 patients consideredmalnourished. The reported outcomes weremortality, hospital admission, nutritional status,nutritional intake and clinical function.
There was no significant difference in mortality atthree months (5 studies), hospital admission (1study), or measures of clinical function at threemonths (1 study investigating older people livingat home). Energy intake at three months wassignificantly greater in the oral nutritionalsupplement group compared to the dietary advicegroup (4 studies) and although there werevariable effects on weight change, the systematicreview reported significantly greater gains in thesip fed patients.
ORAL NUTRITION SUPPORT IN HOSPITAL AND THE COMMUNIT Y 97

88..44..33 CCoosstt--eeffffeeccttiivveenneessss eevviiddeennccee
No study reporting cost or cost-effectiveness was found.
88..44..44 CCoonncclluussiioonnss
Oral nutritional supplements may be moreeffective in increasing energy intake andincreasing weight than dietary advice but studieshave been too small to determine whether thereare any differences in terms of mortality or clinicaloutcome, and there is little or no information oncost effectiveness.
Since oral nutritional supplements presumablyproduce clinical benefits through increasednutrient intake, a similar increase in nutrientintake achieved by dietary means, should lead tosimilar clinical benefits. It therefore seems logicalthat, until further evidence is available, peoplewith weight loss secondary to illness should eitherbe managed by referral to a dietitian or by staffusing protocols drawn up by dietitians withreferral as necessary.
88..55.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
88..55..11 IInnddiiccaattiioonnss ffoorr oorraall nnuuttrriittiioonn ssuuppppoorrtt
Healthcare professionals should consider oral
nutrition support33 to improve nutritional intakefor people who can swallow safely and are
malnourished34 or at risk of malnutrition35. [[AA]]
Healthcare professionals should ensure that theoverall nutrient intake of oral nutrition supportoffered contains a balanced mixture of protein,energy, fibre, electrolytes, vitamins and minerals.[[DD((GGPPPP))]]
Oral nutrition support should be stopped whenthe patient is established on adequate oral intakefrom normal food. [[DD((GGPPPP))]]
88..66.. OOrraall nnuuttrriittiioonn ssuuppppoorrtt iinn ssuurrggiiccaall ppaattiieennttss
88..66..11 IInnttrroodduuccttiioonn
Many surgical patients are malnourished prior totheir operation. During the period leading up todiagnosis, the underlying problem (especially ifgastrointestinal) may cause deterioration innutritional status and in some patients,coincidental illness or psycho-social issues alsocontribute. To add to these nutritional risks, manyinvestigations used to diagnose surgical problems,require patients to be ‘nil by mouth’.
Following surgery, any pre-operative problems canworsen. Many patients have some degree ofintestinal failure, usually due to ileus and most alsohave variable catabolic responses with increased orchanged nutrient demands. Some have abnormalnutrient losses via drains, stomas etc.
In view of the above, there are always somesurgical patients with an undoubted need fortemporary nutrition support (e.g. those withprolonged but potentially reversible intestinalfailure due to post-operative complications such assepsis, anastamotic leaks, or GI fistulae, will needit until recovery). There will also be occasionalpatients who end up with irreversible intestinalfailure due to extensive gut resection etc., andthese may need long-term enteral tube feeding orparenteral nutrition (see Chapter 11). In themajority of surgical cases, however, the need fornutrition support is less definite. Nevertheless,they might benefit from its elective use. Pre-operative nutrition support might reduce risks ofinfection or poor wound healing, whilst early post-operative intervention might limit the nutritionalrisks arising from the standard practice of keepingpatients ‘nil by mouth’ for several days (with aview to protecting gastro-intestinal anastomosesand allowing any ileus to resolve). Furthermore,there is some evidence that early post-operativeengagement of the GI tract might reduce themetabolic effects of injury and limit infectionscaused by the spread of gut organisms to otherparts of the body. We therefore reviewed studies oforal nutrition support around the time of surgery.
NUTRITION SUPPORT IN ADULTS98
33 Oral nutrition support includes any of the following methods to improve nutritional intake: fortified food with protein, carbohydrate and/or fat,plus minerals and vitamins; snacks; oral nutritional supplements; altered meal patterns; the provision of dietary advice.34 Malnourished: BMI <18.5 kg/m2, unintentional weight loss >10% within the last 3-6 months, a BMI<20 kg/m2 and unintentional weight loss>5% within the last 3-6 months.35 At risk of malnutrition: eaten little or nothing for more than 5 days and/or likely to eat little or nothing for the next 5 days or longer or poorabsorptive capacity, and or high nutrient losses and or increased nutritional needs from causes such as catabolism.

88..66..22.. MMeetthhooddoollooggyy
We conducted literature searches to identifystudies on the ‘elective’ use of nutrition supportaround the time of surgery. The studies identifiedwere grouped to examine the possible benefitsunder the following circumstances:
Pre-operative oral nutrition support versus noadditional pre-operative supplementary nutrition(i.e. normal hospital diet, placebo drink, fasting orsimple IV fluids)
Pre- and post-operative oral nutrition support vs. noadditional nutrition support (i.e. normal hospitaldiet, placebo drink, fasting or simple IV fluids)
Pre-operative oral nutrition support versus post-operative oral nutrition support
Early post-operative oral nutrition (<24 hrs aftersurgery) versus no additional post -operativenutrition (i.e. normal post-operative fasting withsimple IV fluids until clinically-judged return of GI function)
They were also grouped according to the type ofsurgery undertaken.
88..66..33.. EElleeccttiivvee pprree--ooppeerraattiivvee oorraall nnuuttrriittiioonn ssuuppppoorrtt vveerrssuussnnoo pprree-- ooppeerraattiivvee nnuuttrriittiioonn ssuuppppoorrtt
SSttuuddiieess ccoonnssiiddeerreedd ffoorr tthhiiss rreevviieeww
We identified 2 RCTs209,326 which examined pre-operative oral nutritional supplements versus nopre-operative nutrition support (Table 32).
8.6.3.1 Clinical evidence
One study326 reported a decrease in postoperativecomplications following pre-operative nutritional
supplementation while the other 209 reportedincreased problems.
88..66..44.. EElleeccttiivvee pprree-- aanndd ppoosstt--ooppeerraattiivvee oorraall nnuuttrriittiioonnssuuppppoorrtt vvss.. nnoo nnuuttrriittiioonn ssuuppppoorrtt
SSttuuddiieess ccoonnssiiddeerreedd ffoorr tthhiiss rreevviieeww
Two RCTs 209,326 were identified (Table 32).
8.6.4.1 Clinical evidence
One RCT 326 reported a decrease in the totalnumber of postoperative minor complications inpatients receiving pre- and post-operativenutrition support (p<0.05) and the fed group also
lost significantly less weight than controls
(p<0.05), however, the other RCT 209 found nosignificant differences between intervention andcontrol groups. Different systems of classificationof complications were used for the studies.
88..66..55.. EElleeccttiivvee pprree--ooppeerraattiivvee oorraall nnuuttrriittiioonn ssuuppppoorrtt vveerrssuussppoosstt--ooppeerraattiivvee oorraall nnuuttrriittiioonn ssuuppppoorrtt
SSttuuddiieess ccoonnssiiddeerreedd ffoorr tthhiiss rreevviieeww
Two RCTs 209,326 were identified (Table 32).
8.6.5.1 Clinical evidence
No significant differences were found in any ofthe outcomes.
88..66..66.. EElleeccttiivvee ppoosstt--ooppeerraattiivvee oorraall nnuuttrriittiioonn ssuuppppoorrttvveerrssuuss ssttaannddaarrdd ccaarree
88..66..66..11 PPoosstt--ooppeerraattiivvee oorraall nnuuttrriittiioonn ssuuppppoorrtt iinn GGII ssuurrggeerryy((aatt tthhee ttiimmee ooff oorr aafftteerr rreettuurrnn ooff GGII ffuunnccttiioonn))SSttuuddiieess ccoonnssiiddeerreedd ffoorr tthhiiss rreevviieeww
Five RCT’s 23,181,209,283,302,326 compared patientsundergoing abdominal surgery who receivedstandard care/no intervention with patients whoreceived oral supplements at or after the returngastrointestinal function judged clinically (Table33). One study included patients undergoing
elective and emergency GI surgery 302, fourstudies included patients undergoing elective GI
surgery only 181,209,283,326 and one study includedpatients undergoing elective GI and vascular
surgery 23. Three of these studies 23,283,302 arealso included in the oral vs. standard care sectionfor malnourished patients in general (section 8.2).
8.6.6.2 Clinical evidence
Post-operative oral supplements led to significantincrease in BMI and mid-arm circumference in 1
study 181 and weight gain in 3 studies 181,283,302.
In one study181 the intervention group hadsignificantly less complications than the control
group (p< 0.05), although in another326 thedifference was only significant for minorcomplications. Four studies reported no significant
difference for wound infections 23,209,283,302. . The
only study that reported pneumonia 283 showed alower incidence in the supplemented group(p<0.02). Quality of life was significantly higher
in the intervention group in one study 23.Postoperative anxiety was reported in one study
ORAL NUTRITION SUPPORT IN HOSPITAL AND THE COMMUNIT Y 99

and showed no significant difference 209. Therewere no significant changes in length of stay209,283,302 or mortality 23,209,283 in the studiesreporting these outcomes.
88..66..77.. PPoosstt ooppeerraattiivvee oorraall nnuuttrriittiioonn ssuuppppoorrtt iinnoorrtthhooppaaeeddiicc SSuurrggeerryy ((aatt tthhee ttiimmee ooff oorr aafftteerr rreettuurrnnooff GGII ffuunnccttiioonn))
A systematic review (8 RCT’s) 14 and 2
additional RCT’s 49,161 provided data on theeffects of elective post-operative oral nutritionsupport in patients following orthopaedicsurgery for hip fracture (Table 34). Thesystematic review reported on mortality,complications, and unfavourable outcomes butpotential biases resulting from inadequatesample size, allocation and concealment makethe results difficult to interpret.
Pooled data from for 3 RCTs 79,141,330 containedin the systematic review demonstrate that oralnutritional supplements led to a statisticallysignificant reduction in adverse outcomes in thesupplemented groups including reducedcomplications (borderline significance).However, none of the studies in the systematicreview demonstrated a difference between studygroups for functional outcomes and the 2
separate RCTs 49,161 did not show anydifferences in reported outcomes.
88..66..88.. EEaarrllyy ppoosstt--ooppeerraattiivvee oorraall nnuuttrriittiioonn ((<<2244 hhrrss aafftteerrssuurrggeerryy)) vveerrssuuss ppoosstt--ooppeerraattiivvee ‘‘nniill bbyy mmoouutthh’’..
Routine practice in most centres is for post-surgical patients to be kept nil by mouth untilthere are clinical signs of returning GI functione.g. for two to three days after a major abdominaloperation. This delayed nutrient intake could havesignificant consequences on nutritional state andpotential recovery but conversely, very early oralintake might cause problems with nausea andvomiting, or leakage from vulnerableanastomoses. We therefore conducted a review toinvestigate any benefits or harm related todelaying the start of food and fluid intake in post-surgical patients.
8.6.8.1 Studies considered for this review
We identified one systematic review 206 that lookedat early post-operative feeding (oral or enteral)versus post-operative ‘nil by mouth’. The oral studiesfrom this review were included as relevant in thissection (enteral tube studies were included in section9.4.5 on post-operative enteral tube feeding) to givea total of20 RCTs identified in which patients weregiven oral feeding within 1-24 hours post operativelycompared to no nutrition (i.e. intravenous dextroseand/or clear fluids only) until clinical evidence of
returning bowel function 32,51,73,104,127,128,137,140,144,
192,214,258, 268,272,286,291,308,331,334,369. Data wereextracted on seven outcomes: vomiting, anastomoticdehiscence, pneumonia, death, intra-abdominalabscess, wound infection and hospital length of stay(LOS) (Table 35,Table 36,Table 37). Whereappropriate we pooled the data for these outcomesbut we were unable to pool data for LOS as thestudies reported this in different units andinformation needed to convert these units waslacking. Studies fell into two groups, those includingpatients undergoing general abdominal surgery forgastrointestinal problems, vascular problems oftrauma, and those including patients undergoinggynaecological or obstetric surgery. One study ofearly oral intake in pancreatitis patients who did notundergo surgery is reported separately.
8.6.8.2 Clinical evidence
Abdominal surgery patientsWe identified eight studies. Six included patients
undergoing lower GI surgery 32,104,144,258,291,334, oneincluded patient undergoing lower GI and
transabdominal central vascular reconstruction 140
and one included emergency or elective intra-
peritoneal surgery of all types286 (Table 35). Acombined analysis of these eight studies showedthat patients in the early feeding group had astatistically higher incidence of vomiting comparedto patients in the later feeding group. There wereno statistically significant differences in any of theother outcomes in this pooled analysis (Table 14and Appendix Seven). LOS was reported in six
studies 32,104,140,144,291,334 with no statisticallysignificant differences between groups.
NUTRITION SUPPORT IN ADULTS100

Caesarean and gynaecological surgeryWe identified twelve studies in this group: sevenstudies included patients undergoing caesarean
section 51,127,128,137,192,268,369 and five studies73,214,272,308,331 included patients undergoinggynaecological surgery (Table 36,Table 37).Although pregnancy does not fall within thescope of the guideline the GDG decided toinclude patients who have undergone caesariansection as these patients are no longer pregnantat the start of oral feeding.
We initially analysed the two surgical groups(caesarean and gynaecology) separately. Theresults of the analyses showed no significant
differences between the groups in vomiting,pneumonia and wound infection in either surgicalgroup. The P value from test for heterogeneitywas greater than 0.1 for all outcomes in eithersurgical group. LOS was reported in 10 studies.The early feeding group spent fewer days in
hospital (p< 0.001) in two 128,268 out of six
studies51,127,128,192,268,369 on caesarean section and
four73,272,308,331 out of four studies ongynaecological surgery (p<0.05).
In an analysis there were no statistically significantdifferences in any of the outcomes extracted (Table15 and Appendix Seven: Meta-Analyses Oral versusNil Post Operative Nutrition Support).
ORAL NUTRITION SUPPORT IN HOSPITAL AND THE COMMUNIT Y 101
TTaabbllee 1144:: OOuuttccoommeess rreeppoorrtteedd iinn ssttuuddiieess ooff ppaattiieennttss uunnddeerrggooiinngg GGII ssuurrggeerryy
NNoo.. ppaattiieennttss ((eeaarrllyy RRRR ((ffiixxeedd))ffeeeeddiinngg//llaattee ffeeeeddiinngg)) 9955%% CCII
VVoommiittiinngg (reported in six studies 32,104,144,286,291,334 262/261 1.43 [1.07, 1.92]
P value from test for heterogeneity 0.52
AAnnaassttoommoottiicc ddeehhiisscceennccee (reported in five studies 140,144,258,291,334 300/294 0.74 [0.27, 2.06]
P value from test for heterogeneity 0.75
PPnneeuummoonniiaa (reported in five studies 140,144,258,291,334 300/294 0.98 [0.32, 3.00]
P value from test for heterogeneity 0.92
IInnttrraa--aabbddoommiinnaall aabbsscceessss (reported in four studies144,258,291,334 244/245 1.01 [0.14, 7.06]
P value from test for heterogeneity P=1.0
WWoouunndd iinnffeeccttiioonn (reported in six studies 104,140,144,258,291,334 350/344 0.62 [0.29, 1.34]
P value from test for heterogeneity P=0.48
DDeeaatthh (reported in six studies 104,140,144,258,291,334 350/344 1.21 [0.29, 4.96]
P value from test for heterogeneity P= 0.29
NNoo.. ppaattiieennttss ((eeaarrllyy ffeeeeddiinngg//llaattee ffeeeeddiinngg)) RRRR ((ffiixxeedd)) 9955%% CCII
VVoommiittiinngg (reported in five studies51,73,192,214,272) 361/395 1.07[0.73, 1.58]
P value from test for heterogeneity 0.71
WWoouunndd iinnffeeccttiioonn (reported in five studies 73,127,128,272,331 358/356 0.94 [0.58, 1.52]
P value from test for heterogeneity 0.65
PPnneeuummoonniiaa (reported in 4 studies 73,272,308,331) 249/260 0.42 [0.08,2.17]
P value from test for heterogeneity 0.74
TTaabbllee 1155:: OOuuttccoommeess ooff ssttuuddiieess ooff ppaattiieennttss uunnddeerrggooiinngg ccaaeessaarreeaann aanndd ggyynnaaeeccoollooggiiccaall ssuurrggeerryy

8.6.8.3 Cost effectiveness evidence in
surgical patients
We identified two studies and two cost analyseswhich examined the effects of perioperative oralnutrition support. An RCT (n=152), based in theUK compared four arms (preoperative,postoperative, perioperative and no nutritionalsupplementation) in patients undergoing elective
major to moderate lower GI surgery 326. Therewere significantly fewer minor complications inthe intervention arms and no significantdifferences with respect to major complications.Costs were lower by £300 per patient althoughthis was not significant. The results favourintervention but the trial was inadequatelypowered to detect differences in cost.
Another study198 looked at the effect of post-operative oral supplements on complication ratesand hospital costs in adult orthopaedic patients,using a cross-over trial. Despite low compliancewith the intervention there was a significantreduction in the complication rate in the oralsupplemented group (16.6 % vs. 35.1%,p=0.005). There were cost savings from thereductions in both length of stay and specifictreatment interventions (£2,068 vs. £2,199)although it was not stated whether this differencewas statistically significant.
An unpublished UK-based decision analysis 266
evaluated preoperative assessment, dietary adviceand oral intervention (mixture of fortificationand/or supplements) versus no preoperativeassessment or intervention in patients undergoingGI surgery. Data was elicited from the expertopinion of a sample of NHS consultants.Incremental cost per patient (excluding costsavings due to complications averted) wasestimated to be between £17 and £48. Theyfound that preoperative assessment and ONSwould be cost saving if averting a complicationsaves three or more bed-days.
An unpublished report 91 estimated the costimpact of oral nutritional supplements from anNHS perspective using two alternative methods:firstly by costing length of stay (as reported inselected RCTs) and secondly by costingcomplications (reported in those same RCTs). The
RCTs included were mainly in surgical patients butdid not all focus on patients that we wouldcategorise as being at risk of malnutrition. Foreach of the trials, and using both methods, theyestimated in hospital cost savings from oralnutritional supplements and although any specificadditional costs associated with administering andmonitoring the supplements were not included,the bed day costs used did account for associatednursing etc. The studies did not claim to be fullcost-benefit analyses and they did not account forthe potential additional NHS costs of care inadded weeks of life for critically ill patients.
Only one study was found that evaluated thecosts (and consequences) of early post-operative
oral nutrition versus nil by mouth 6. It wasperformed in Japanese patients undergoingoncological colorectal surgery and reported thatearly post-operative feeding significantly reducedlength of stay and hence medical costs with nosignificant differences in complication rates.However, the difference in length of stay in thisstudy was much greater than that observed instudies within the clinical review and patients didnot appear to be randomized. This, incombination with small sample size andconsiderable variation in the types of surgeryincluded within different arms, gave a largepotential for bias. Furthermore, the costs appearto be expressed as medians and hence might notreflect true differences in mean cost and thefeeding protocol was based on rice gruel, whichmay not be replicable in a UK setting.
88..66..99.. CCoonncclluussiioonnss -- oorraall nnuuttrriittiioonn ssuuppppoorrtt iinn ssuurrggiiccaall ppaattiieennttss
Some surgical patients need nutrition supporteither pre- and or post-operatively due to theseverity of their existing malnutrition or thepresence of post–operative complications andhence prolonged delay in recovery of normal foodintake. These patients should receive support bythe simplest method possible using oralsupplements, enteral tube feeding or PN alone orin combination as necessary.
For patients who are not malnourished , there islittle evidence that pre-operative oral nutrition
NUTRITION SUPPORT IN ADULTS102

support is of benefit although trials are small andunderpowered. A cost-benefit model doessuggest that pre-operative oral support might becost saving for some patient groups but themodels were sensitive to assumptions about thenumber of complications averted. Similarly, thereis also no evidence that the early introduction oforal intake following general abdominal surgery isof value although there is also no evidence ofharm other than a slight increased incidence ofnausea and vomiting. In caesarean orgynaecological surgery patients early oral intakeis generally well tolerated and may lead to earlierdischarge. Larger trials are needed to confirmthese points.
There is some evidence that post-operative oralnutritional supplements, introduced at or afterrecovery of GI function may reduce somecomplications in general surgery patients andpatients with hip fracture requiring orthopaedicsurgery but once again, studies have been smalland underpowered. Nutritional principles suggestthat giving post-operative oral supplements tomore malnourished patients might lead to greaterbenefits but larger, targeted trials are also neededto prove this point.
88..77.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
OOrraall nnuuttrriittiioonn ssuuppppoorrtt ffoorr ssuurrggiiccaall ppaattiieennttss
Peri-operative oral nutrition support should beconsidered for surgical patients who can swallow
safely and are malnourished36. [[BB]]
Healthcare professionals should consider givingpost-caesarean or gynaecological surgical patientswho can swallow safely, some oral intake within24 hours of surgery. [[AA]]
Healthcare professionals should consider givingpost-abdominal surgery patients who can swallowsafely, and in whom there are no specific concernsabout gut function or integrity, some oral intakewithin 24 hours of surgery. The patient should be monitored carefully for any signs of nausea or vomiting. [[AA]]
88..88.. OOrraall nnuuttrriittiioonn ssuuppppoorrtt iinn ppaannccrreeaattiittiiss ppaattiieennttss
Only one study included patients who had clinicalfeatures of acute pancreatitis and did not have
any surgical procedure 196 (Table 38). Fiftypatients were included in the study. Patients inthe early feeding group (n=50) were givenliquids, such as tea, water and juice, orallywithout restrictions immediately after admission.Patients in the late feeding group had anasogastric tube placed in the stomach forsuction. Continuous suction was applied andmaintained until the tube was removed.
Results were available for mortality and LOS.There were three deaths in the early feedinggroup and two deaths in the late feeding group.There were no statistically significant differencesin LOS.
88..88..11.. CCoonncclluussiioonn
There is insufficient data to conclude on thebenefits of early feeding for pancreatitis patients.
88..99.. OOrraall mmuullttiivviittaammiinn aanndd mmiinneerraall ssuupppplleemmeennttaattiioonn iinn mmaallnnoouurriisshheedd ppaattiieennttss
88..99..11.. IInnttrroodduuccttiioonn
Oral multivitamin and mineral supplementsshould help individuals who are eating poorly tomeet their vitamin and mineral requirements andin some circumstances, apparently healthy peoplemay also have sub-optimal multivitamin/mineralstatus. In the National Diet and Nutrition Survey,many older individuals living at home and a greatmany living in residential care were found to havebiochemical deficiencies of vitamins or mineralsdespite the fact that their food supply appearedto contain sufficient amounts. This raises thepossibility that vitamin/mineral supplementationmight be of value to patients with malnutritionand they might even be of value to individualswho are not overtly malnourished or ill, althoughthe latter fall outside the scope of this guideline.
ORAL NUTRITION SUPPORT IN HOSPITAL AND THE COMMUNIT Y 103
36 Malnourished: BMI <18.5 kg/m2, unintentional weight loss >10% within the last 3-6 months, a BMI<20 kg/m2 and unintentional weight loss>5% within the last 3-6 months.

88..99..22.. CClliinniiccaall eevviiddeennccee
Our review identified RCTs that studied the effectsof multivitamins/minerals on patients who werepotentially malnourished. The studies includedindividuals who were hospitalised, living in olderpersons care homes or were HIV infected
patients.124-126,159,275,364. The studies werecategorised into two groups according to the typeof supplement provided i.e. multivitamin and
mineral supplement v placebo124-126 (Table 30) or
multivitamin supplement only v placebo 159,275,364
(Table 31).
88..99..33.. MMuullttiivviittaammiinn aanndd mmiinneerraall vv ppllaacceebboo//ssttaannddaarrdd ccaarree
8.9.3.1 Studies considered for this review
Four studies were included in this category 8,124-
126,169 (one study was reported in two papers124,126). Three studies included older patients innursing homes and one study included HIVinfected patients.
8.9.3.2 Older patients in nursing homes
Two studies with identical methodology includedolder patients in nursing homes. One was a large
multi-centre study125 and the other reported in
two papers124,126 was a study in one of the centresin the multi-centre study but provided additionaldata. Patients in both studies were randomisedinto four groups: vitamin group (Vitamins A, Cand E) mineral group (zinc, selenium), vitaminand mineral group (vitamins A, C, E and zinc andselenium) and a placebo group (calciumphosphate). Immunological data were reported in
the large multi-centre study 125.
Clinical Evidence No differences were observed in delayedhypersensitivity responses. A sub-group of patientsreceived influenza vaccine towards the end of thetwo-year supplementation period and the humoralresponse to the vaccine strain was assessed beforeand after vaccination. Results overall for the threeinfluenza vaccines showed an improvement inantibody titre in trace element and traceelement/vitamin groups relative to placebo orvitamins alone, but the mineral group hadsignificantly higher numbers of serologicallyprotected patients compared to the vitamin,
vitamin/mineral, and placebo groups, for one of thethree vaccines (p<0.05). The authors concluded thatzinc and selenium supplementation improves thehumoral response, and that vitaminsupplementation led to a weaker response, butchance variation is another explanation.
Infectious morbidity, respiratory and urogenitalinfections were reported in both of these studies. In
the smaller study 124,126 (n=81) patients in themineral and (mineral/vitamin) groups hadsignificantly fewer respiratory and urogenitalinfections( p<0.01). In the larger multicentre study125 (n=725) no significant difference between thegroups was observed. However, there are somelimitations with this last result. A subgroup of140/725 patients in this study received influenzavaccine to assess immunological outcomes.Infections were reported for the total number ofpatients and not extracted for the group that
received the vaccine. These two trials 124-126 alsoreported mortality and both found no significantdifferences between the groups.
In a further small study in the UK 8, a two monthperiod of supplementation with a completevitamin/trace element mixture was not associatedwith any significant alteration in antibodyresponse to influenza vaccination.
8.9.3.3 HIV-infected patients
Studies considered for this review
A single study was identified 169 which included481 HIV-infected patients randomised to receiveeither a high dose multiple micronutrient or aplacebo for a period of 48 weeks. Patients wereexamined clinically 12-weekly and tested for CD4cell count 24-weekly.
Clinical Evidence There were no statistically significant differencesin overall mortality or changes in CD4 cell count.
88..99..44.. MMuullttiivviittaammiinn vv ppllaacceebboo//ssttaannddaarrdd ccaarree
8.9.4.1 Studies considered for this review
Three studies were included in this category159,275,364 and although there was a variation inthe content of the intervention supplement, mostwere composed of vitamins C,+/- A, B and E. One
included older long-stay stroke patients 275 and
NUTRITION SUPPORT IN ADULTS104

one included acute medical or surgical patients364 (Table 31). The other study 159 included oldermedical patients who received in addition to theintervention/placebo either a glucose energy orplacebo drink.
8.9.4.2 Clinical Evidence
One study 275 reported changes in absolutenumber of lymphocytes and T cells sub-types. Thisshowed a significant increase in the interventiongroup (p<0.05). Mental test score and Barthelscore (activity score) were reported in one study159 with no significant differences between thegroups. Change in body weight was reported in
two studies159,275. In one there was no significant
change whilst in the other 275, the supplementedgroup lost weight compared to placebo p<0.05).There were no significant differences reported for
mortality or length of stay 159,364 although thefindings in the Vlaming study did suggest thatlength of stay may be shorter in multivitaminsupplemented acute hospital patients and if thiswere the case, it would be a very importantfinding since the intervention is relatively low costand probably harmless. More research is thereforeneeded with a large multi—=centre trial to clarifythis point.
(Note: The most commonly reported outcome wasbiochemical assessment of plasma vitamins andminerals. This data was not extracted.)
8.9.4.3 Cost-effectiveness evidence
We did not find any relevant economic studies.
88..99..55.. TThhee NNaattiioonnaall DDiieett aanndd NNuuttrriittiioonn SSuurrvveeyy
The National Diet and Nutrition Survey presentedfindings on biochemical indices of nutritionalstatus and nutrient intake in older people living innursing homes. Results from the survey indicatethat although the food supply appears to containsufficient amounts of vitamins and traceelements, in general the status of vitamins andminerals is poor in this population, suggestingthat intake and absorption from food wasinadequate. The reasons for this are not clear, butpossibilities include the presentation and timingof the food, the need for assistance in eating,changes in absorptive function of the gut, andgeneral medical condition.
88..99..66.. CCoonncclluussiioonnss
There is no evidence to support the routine use ofvitamin and mineral supplements in either acutehospitalised patients or older residents of nursinghomes. However, in view of the National Diet andNutrition Survey findings, large scale trials areneeded and a vitamin/ mineral supplement maybe beneficial in older people when there isconcern about the adequacy of total food intake.
88..99..77.. RRaattiioonnaallee ffoorr rreeccoommmmeennddaattiioonn
The National Diet and Nutrition Survey has shownbiochemical deficiency of vitamins and orminerals is common in older people, particularlythose in residential care. Studies to determinewhether there is definite benefit of providingvitamin supplements to patients have beeninadequate, but balanced micronutrientsupplements providing the reference nutrientintake for all vitamins and trace elements, havebeen shown to improve biochemical deficiencies.
88..99..88.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
88..99..88..11 Oral multivitamin and mineral supplement
If there is concern about the adequacy ofmicronutrient intake, a complete oral multivitaminand mineral supplement providing the referencenutrient intake for all vitamins and trace elementsshould be considered by healthcare professionalswith the relevant skills and training in nutritionsupport who are able to determine the nutritionaladequacy of a patient’s dietary intake. [[DD((GGPPPP))]]
ORAL NUTRITION SUPPORT IN HOSPITAL AND THE COMMUNIT Y 105

88..1100.. NNuuttrriittiioonn ssuuppppoorrtt iinn ppaattiieennttss wwiitthh ddyysspphhaaggiiaa
88..1100..11 IInnttrroodduuccttiioonn
Dysphagia is the term used to describe anyimpairment of eating, drinking and swallowing. Itis …’ not a disease in itself, but rather a symptom
of one or more underlying pathologies…’ 194..Patients with dysphagia are seen in both hospitaland community settings, with varying degrees ofseverity and impact on individuals’ lives. Around50% of older people with dysphagia living ineither nursing homes or attending clinics reportedthat they ate less, whilst 44% reported weightloss and 41%, anxiety or panic attacks during
mealtimes90. There is therefore a close linkbetween dysphagia and nutritional compromise.Indeed, one study showed that by offeringswallowing therapy to dysphagic patients poststroke, they could improve nutritional parameters95. The cause of dysphagia can be either a singlemedical problem (e.g. acute cerebral conditions,progressive neurological disorders and trauma,disease or surgery to the mouth, pharynx, larynx
or oesophagus 204). It can also occur or worsenwith conditions such as sepsis, respiratoryimpairment and cognitive disorders.
If the dysphagia is not diagnosed, it can lead toinadequate food and fluid intake, impairednutritional status and problems such as chestinfections, sepsis, and pneumonia. Avoidance ofeating may also lead to social isolation andultimately dysphagia has a ‘high morbidity,
mortality and cost’69,255. As a result, particularlysince it is not always obvious that a patient hasdysphagia, the condition must be assessed andmanaged by a knowledgeable and skilled team.
88..1100..22 PPrreevvaalleennccee ooff ddyysspphhaaggiiaa
The prevalence of oropharyngeal dysphagia isestimated to be 60% in nursing home residents
and 12-13% of patients in hospital69. Theprevalence for the general population over 50
years is cited as 16-22% 194. , Specific examplesof conditions which may present with dysphagia
include 27 – 100% of stroke patients 194
depending on the time assessed post stroke,adults with learning disabilities (36% of peoplewith learning difficulties in hospital and 5.3% of
those in the community present with dysphagia156
and between 48-100% of patients with Motor
Neurone Disease (MND)194. However, there isconsiderable variation in prevalences cited,probably due to variation in the timing andcompleteness of assessments (e.g. in stroke theincidence of presentation with aspiration risk is51% on admission, 27% at day 7, 6.8% at 6
months, and 2.3% after 6 months)329.
88..1100..33.. IIddeennttiiffyyiinngg ppaattiieennttss wwiitthh ddyysspphhaaggiiaa
Patients with dysphagia may present with a rangeof symptoms which can be divided into obviousand less obvious indicators (Table 16)
Patients with any of the obvious or less obviousindicators for dysphagia should be referred forassessment by healthcare professionals withspecialist training in diagnosis, assessment andmanagement of swallowing disorders. A variety ofskills is needed including those of speech andlanguage therapists, gastroenterologists,radiologists and specialist nurses. Healthcareprofessionals should be aware that patients withacute cerebral conditions, degenerative disorders(e.g. MND, dementia), trauma, disease, or whohave undergone surgery or radiotherapy to theupper aero-digestive tract, are at high risk ofdeveloping dysphagia.
NUTRITION SUPPORT IN ADULTS106

88..1100..44.. NNuuttrriittiioonnaall iinntteerrvveennttiioonn ssttrraatteeggiieess
There are a number of possible treatmentstrategies that may help to maintain or improvethe nutritional status of patients with oro-pharyngeal dysphagia. These include modificationof the consistency, temperature and/or taste ofliquids and food. Factors to be considered beforeany modification is undertaken are listed in table21 but more detailed guidance can be found inspecialist documents (e.g. National descriptors for
Texture Modification in Adults, 200244) In somesituations, however, modification of texture andconsistency may compromise hydration status,nutritional intake, and swallowing
safety\efficiency for patients371 and so help fromappropriately trained healthcare professionalsshould always be sought and all oral and non-oral
options must be considered110.
88..1100..55.. MMeetthhooddss
We searched for systematic reviews and RCTsinvestigating either the effectiveness of modifiedfoods and fluids or the use of and enteral tubefeeding in dysphagic patients. No studies orsystematic reviews were found, probably becauseRCTS are not feasible in this patient group. TheGDG therefore appointed a sub-group of experts todevelop our recommendations which were ratified bythe whole GDG through informal consensus.
88..1100..66.. RRaattiioonnaallee ffoorr RReeccoommmmeennddaattiioonnss
Due to the complex nature of dysphagia and therange of its presentations our recommendationsoffer a framework upon which to make decisionsthat are based on individual patients’ symptomsrather than specific diagnoses. Therecommendations must take into account theappropriateness of intervention in individual casesand all ethical/legal issues (section 5.3) anddecisions should always involve the patient, familyand clinical teams. Dysphagia specialists shouldadvise the clinical teams.
ORAL NUTRITION SUPPORT IN HOSPITAL AND THE COMMUNIT Y 107
TTaabbllee 1166:: OObbvviioouuss aanndd lleessss oobbvviioouuss iinnddiiccaattoorrss ffoorr ddyysspphhaaggiiaa
Obvious Indicators
Patient reports difficulty and/ or painful chewingand/ or swallowing.
Regurgitation of undigested food stuffs
Difficulty controlling food and/ or liquid in themouth
Drooling
Hoarse voice
Coughing and/ or choking before, during, orafter swallowing
Globus sensation
Nasal regurgitation
Feeling of obstruction
Unexplained/ involuntary weight loss.
Less Obvious Indicators
Change in respiration pattern
Unexplained temperature spikes
Wet voice quality
Tongue fasciculation (may be indicative of motor neurone disease)
Xerostomia
Heartburn
Change in eating – for example, eating slowly or avoidingsocial occasions
Frequent throat clearing
Recurrent chest infections
Atypical chest pain

88..1111.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
88..1111..11 PPeeooppllee wwiitthh ddyysspphhaaggiiaa
People who present with any obvious or lessobvious indicators of dysphagia listed in Box 5should be referred to healthcare professionalswith relevant skills and training in the diagnosis,assessment and management of swallowingdisorders. [[DD((GGPPPP))]
Healthcare professionals should recognise thatpeople with acute and chronic neurologicalconditions and those who have undergonesurgery or radiotherapy to the upper aero-digestive tract are at high risk of developingdysphagia. [[DD((GGPPPP))]]
When managing people with dysphagia,healthcare professionals with relevant skills andtraining in the diagnosis, assessment andmanagement of swallowing disorders shouldconsider:
• the risks and benefits of modified oralnutrition support and/or enteral tube feeding
• the factors listed in Box 6. [[DD((GGPPPP))]]
BBooxx 66 FFaaccttoorrss ttoo bbee ccoonnssiiddeerreedd bbeeffoorree mmooddiiffiiccaattiioonn ooff nnuuttrriittiioonn ssuuppppoorrtt aanndd hhyyddrraattiioonn iinn ppeeooppllee wwiitthh ddyysspphhaaggiiaa
Recurrent chest infections
Mobility
Dependency on others for assistance to eat
Perceived palatability and appearance of food or drink
Level of alertness
Compromised physiology
Poor oral hygiene
Compromised medical status
Metabolic and nutritional requirements
Vulnerability (for example, immunocompromised)
Comorbidities
People with dysphagia should have a drug reviewto ascertain if the current drug formulation, routeand timing of administration remains appropriateand is without contraindications for the feedingregimen or swallowing process. [[DD((GGPPPP))]]
Healthcare professionals with relevant skills andtraining in the diagnosis, assessment andmanagement of swallowing disorders shouldregularly monitor and reassess people withdysphagia who are having modified food andliquid until they are stable. [[DD((GGPPPP))]]
NUTRITION SUPPORT IN ADULTS108
BBooxx 55 IInnddiiccaattoorrss ooff ddyysspphhaaggiiaaOObbvviioouuss iinnddiiccaattoorrss ooff ddyysspphhaaggiiaa
Difficult, painful chewing or swallowing
Regurgitation of undigested food
Difficulty controlling food or liquid in the mouth
Drooling
Hoarse voice
Coughing or choking before, during or afterswallowing
Globus sensation
Nasal regurgitation
Feeling of obstruction
Unintentional weight loss – for example, in people with dementia
LLeessss oobbvviioouuss iinnddiiccaattoorrss ooff ddyysspphhaaggiiaa
Change in respiration pattern
Unexplained temperature spikes
Wet voice quality
Tongue fasciculation (may be indicative of motorneurone disease)
Xerostomia
Heartburn
Change in eating habits – for example, eatingslowly or avoiding social occasions
Frequent throat clearing
Recurrent chest infections
Atypical chest pain

88..1122.. RReesseeaarrcchh rreeccoommmmeennddaattiioonnss
WWhhaatt aarree tthhee bbeenneeffiittss ooff ppaattiieennttss ((iinn hhoossppiittaall oorrtthhee ccoommmmuunniittyy,, iinncclluuddiinngg oollddeerr ppeeooppllee)) iiddeennttiiffiieeddaass hhiigghh rriisskk ooff mmaallnnuuttrriittiioonn bbyy aa ssccrreeeenniinngg ttoooollssuucchh aass tthhee ‘‘MMaallnnuuttrriittiioonn UUnniivveerrssaall SSccrreeeenniinnggTTooooll’’ ((‘‘MMUUSSTT’’)) bbeeiinngg ooffffeerreedd eeiitthheerr oorraall nnuuttrriittiioonnaallssuupppplleemmeennttss ccoommppaarreedd ttoo aa)) ddiieettaarryy mmooddiiffiiccaattiioonnaanndd oorr ffoooodd ffoorrttiiffiiccaattiioonn,, oorr bb)) ddiieettaarryymmooddiiffiiccaattiioonn aanndd oorr ffoooodd ffoorrttiiffiiccaattiioonn aanndd ddiieettaarryyccoouunnsseelllliinngg iinn tteerrmmss ooff ddeetteerrmmiinniinnggccoommpplliiccaattiioonnss,, ssuurrvviivvaall,, lleennggtthh ooff hhoossppiittaall ssttaayy,,qquuaalliittyy ooff lliiffee aanndd ccoosstt eeffffeeccttiivveenneessss??
This is an essential recommendation for researchsince there is insufficient evidence on the benefits ofintervention used for oral nutrition support inparticular the benefits of often first line treatmentfor example food fortification and or dietarycounselling. It is essential to know this so that theindications on who to treat can be further supported
.
WWhhaatt aarree tthhee bbeenneeffiittss ttoo ppaattiieennttss iinn hhoossppiittaalliiddeennttiiffiieedd aass aatt hhiigghh rriisskk ooff mmaallnnuuttrriittiioonn bbyy aassccrreeeenniinngg ttooooll ssuucchh aass tthhee ‘‘MMaallnnuuttrriittiioonn UUnniivveerrssaallSSccrreeeenniinngg TTooooll’’ ((‘‘MMUUSSTT’’)) bbeeiinngg ooffffeerreedd eeiitthheerr aa))ccoommpplleettee oorraall nnuuttrriittiioonnaall ssuupppplleemmeennttss bb))ccoommbbiinneedd mmiiccrroo aanndd mmaaccrroonnuuttrriieenntt ssuupppplleemmeennttssoorr cc)) mmiiccrroonnuuttrriieenntt ssuupppplleemmeennttaattiioonn iinn tteerrmmss ooffssuurrvviivvaall,, hhoossppiittaall aaddmmiissssiioonnss,, qquuaalliittyy ooff lliiffee aannddccoosstt eeffffeeccttiivveenneessss??
This is an essential recommendation for researchsince there is insufficient evidence on the benefits ofintervention using oral nutrition support and/ormicronutrients but indications that such interventionsmight decrease complications, mortality and lengthsof stay. Results will clarify indications on who to treatand the best means of doing so.
WWhhaatt aarree tthhee bbeenneeffiittss ttoo ppaattiieennttss iinn pprriimmaarryy ccaarreeiiddeennttiiffiieedd aass hhiigghh rriisskk ooff mmaallnnuuttrriittiioonn bbyy aassccrreeeenniinngg ttooooll ssuucchh aass tthhee ‘‘MMaallnnuuttrriittiioonn UUnniivveerrssaallSSccrreeeenniinngg TTooooll’’ ((‘‘MMUUSSTT’’)) bbeeiinngg ooffffeerreedd eeiitthheerr oorraallnnuuttrriittiioonnaall ssuupppplleemmeennttss ccoommppaarreedd ttoo bbeeiinnggooffffeerreedd;; aa)) ccoommbbiinneedd mmiiccrroo aanndd mmaaccrroonnuuttrriieennttssuupppplleemmeenntt oorr bb)) mmiiccrroonnuuttrriieenntt ssuupppplleemmeennttaattiioonnaalloonnee oorr cc)) ssttaannddaarrdd ccaarree ((nnoo ssppeecciiffiicc ddiieettaarryyiinntteerrvveennttiioonn)) iinn tteerrmmss ooff ssuurrvviivvaall,, hhoossppiittaallaaddmmiissssiioonnss,, qquuaalliittyy ooff lliiffee aanndd ccoosstt eeffffeeccttiivveenneessss??
This is an essential recommendation for researchsince there is insufficient evidence on the benefitsof intervention used for oral nutrition support. Itis essential to know this so that the indications onwho to treat can be further supported.
DDoo ppaattiieennttss wwiitthh oorroo--pphhaarryynnggeeaall ddyysspphhaaggiiaa ((aassaasssseesssseedd bbyy aa ttrraaiinneedd pprraaccttiittiioonneerr)) wwhhoo aarree ggiivveenntthhiicckkeenneedd lliiqquuiiddss ccoommppaarreedd ttoo ssttaannddaarrdd//uunntthhiicckkeenneedd lliiqquuiiddss bbeenneeffiitt iinn tteerrmmss ooff iimmpprroovveeddmmoooodd,, iinnccrreeaasseedd nnuuttrriittiioonnaall iinnttaakkee,, rreedduucceeddeehhyyddrraattiioonn,, lleessss aassppiirraattiioonn iinncciiddeennttss,, mmoorrttaalliittyyaanndd aavvooiiddaannccee ooff tthhee nneeeedd ffoorr eenntteerraall ffeeeeddiinngg??
This is an essential area for research. Thickeningliquids(and foods) is a major cost considerationwith no evidence to support it and increasingevidence to show it causes more harm than goodfor example dehydration.
DDoo ppaattiieennttss wwiitthh oorroo--pphhaarryynnggeeaall ddyysspphhaaggiiaa ((aassaasssseesssseedd bbyy aa ttrraaiinneedd pprraaccttiittiioonneerr)) wwhhoo aarree ggiivveennppuurreeeedd ffoooodd ccoommppaarreedd ttoo ssttaannddaarrdd// ssoofftt ffooooddbbeenneeffiitt iinn tteerrmmss ooff iimmpprroovveedd nnuuttrriittiioonnaall iinnttaakkee,,tthhee ssaaffeettyy aanndd eeffffiicciieennccyy ooff sswwaallllooww,, tthhee nnuummbbeerrooff aassppiirraattiioonn iinncciiddeennttss aanndd aavvooiiddaannccee ooff tthhee nneeeeddffoorr eenntteerraall ffeeeeddiinngg??
This is an essential area for research. Thickeningliquids or modifying foods for example liquidisedfoods) has cost implications with no evidence tosupport it and increasing evidence to show it causesmore harm, for example dehydration, than good.
ORAL NUTRITION SUPPORT IN HOSPITAL AND THE COMMUNIT Y 109

99..11.. IInnttrroodduuccttiioonn
For the purposes of these Guidelines, enteral tubefeeding (ETF) refers to the delivery of anutritionally complete feed (containing protein oramino acids, carbohydrate +/- fibre, fat, water,minerals and vitamins) directly into the gut via atube. The tube is usually placed into the stomach,duodenum or jejunum via either the nose, mouth
or the direct percutaneous route37. ETF is notexclusive and can be used in combination withoral and/or parenteral nutrition. Patientsreceiving ETF should be reviewed regularly toenable re-instigation of oral nutrition whenappropriate. Most enteral feeding tubes areintroduced at the bedside but some are placedsurgically, at endoscopy or using radiologicaltechniques,and some are inserted in thecommunity. Whenever possible the patient shouldbe aware of why this form of nutrition support isnecessary, how it will be given, for how long, andthe potential risks involved. There may beconsiderable ethical difficulties in deciding if it isin a patient’s best interests to start a tube feed.
Innumerable questions regarding best ETF practicecould be asked but for these guidelines, reviews wererestricted to studies providing potential guidance onthe indications for ETF, studies on the benefits of ETFcompared to oral or parenteral nutrition, and studieson some technical aspects of delivering enteral feeds. No studies on different types of enteral feed were reviewed.
99..22.. GGeenneerraall IInnddiiccaattiioonnss ffoorr EEnntteerraall TTuubbee FFeeeeddiinngg iinn hhoossppiittaall aanndd tthhee ccoommmmuunniittyy
99..22..11 IInnttrroodduuccttiioonn
Enteral tube feeding (ETF) is used to feed patientswho cannot attain an adequate oral intake fromfood and/or oral nutritional supplements, or whocannot eat/drink safely. The aim is to improvenutritional intake and so improve or maintainnutritional status. It is used most commonly inpatients with dysphagia either because theycannot meet their nutritional needs despitesupplements and/or modifications to foodtexture/consistency, or because they riskaspiration if they try to do so. The GI tract mustbe accessible and functioning sufficiently toabsorb the feed administered. Commonindications for ETF are listed in Table 18, althoughthis is not necessarily an exhaustive list. If ETF isunsafe or unlikely to be successful (e.g.inaccessible GI tract, severe malabsorption,excessive gastrointestinal losses), parenteralnutrition is likely to become the therapy of choice.
99..22..22 RReelleevvaanntt SSttuuddiieess
Most studies on indications for ETF (rather thantiming, type of tube, type/amounts of nutrientsetc) exclude all patients with the most commonclinical indication for ETF (i.e. those with afunctional GI tract but unsafe swallow, who wouldstarve or require PN if ETF were not used). Thefindings from these studies do not thereforeprovide help with decision making for routineclinical practice. The recommendations weretherefore derived using expert opinion.
NUTRITION SUPPORT IN ADULTS110
9. Enteral tube feeding in hospital and the community
37 Enteral feeding tubes may also be used for the administration of drugs, frequently on an unlicensed basis. Information and choice on suitable drugpreparations can be obtained from local pharmacy or Medicines Information Departments. Further information can also be obtained from ‘Guidance inadministering drugs via enteral feeding tubes’ from www.bapen.org
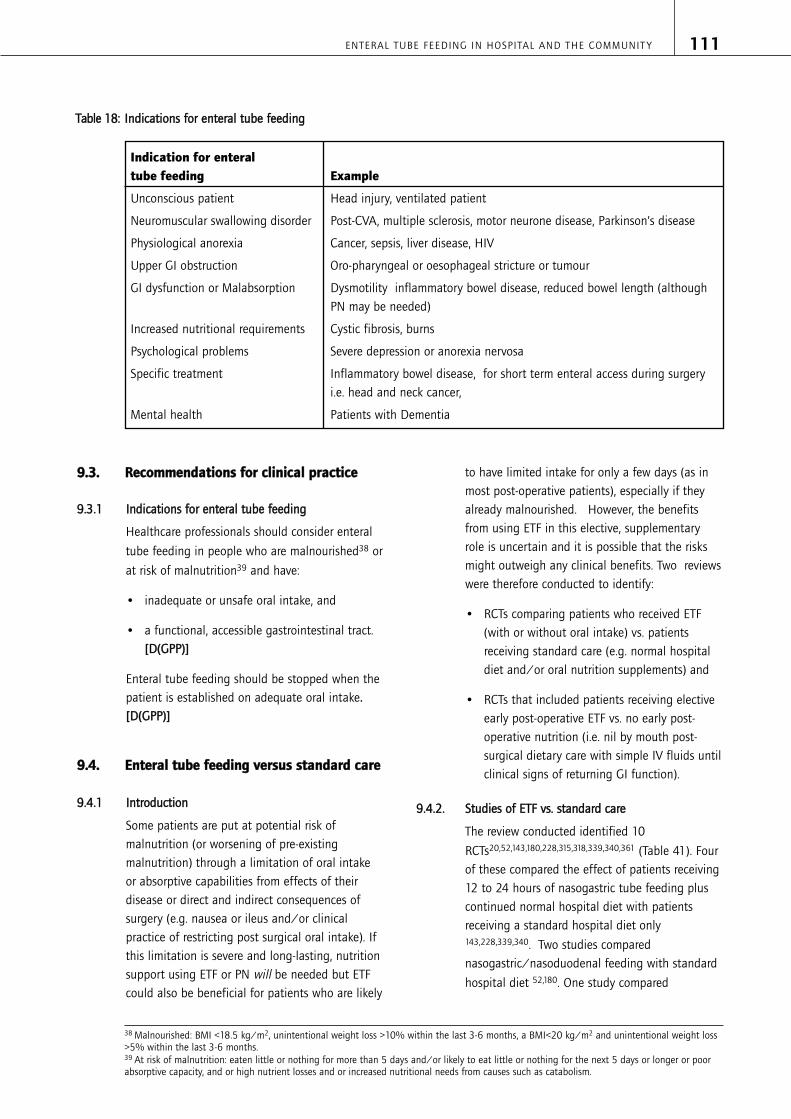
99..33.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
99..33..11 IInnddiiccaattiioonnss ffoorr eenntteerraall ttuubbee ffeeeeddiinngg
Healthcare professionals should consider enteral
tube feeding in people who are malnourished38 or
at risk of malnutrition39 and have:
• inadequate or unsafe oral intake, and
• a functional, accessible gastrointestinal tract.[[DD((GGPPPP))]]
Enteral tube feeding should be stopped when thepatient is established on adequate oral intake..[[DD((GGPPPP))]]
99..44.. EEnntteerraall ttuubbee ffeeeeddiinngg vveerrssuuss ssttaannddaarrdd ccaarree
99..44..11 IInnttrroodduuccttiioonn
Some patients are put at potential risk ofmalnutrition (or worsening of pre-existingmalnutrition) through a limitation of oral intakeor absorptive capabilities from effects of theirdisease or direct and indirect consequences ofsurgery (e.g. nausea or ileus and/or clinicalpractice of restricting post surgical oral intake). Ifthis limitation is severe and long-lasting, nutritionsupport using ETF or PN will be needed but ETFcould also be beneficial for patients who are likely
to have limited intake for only a few days (as inmost post-operative patients), especially if theyalready malnourished. However, the benefitsfrom using ETF in this elective, supplementaryrole is uncertain and it is possible that the risksmight outweigh any clinical benefits. Two reviewswere therefore conducted to identify:
• RCTs comparing patients who received ETF(with or without oral intake) vs. patientsreceiving standard care (e.g. normal hospitaldiet and/or oral nutrition supplements) and
• RCTs that included patients receiving electiveearly post-operative ETF vs. no early post-operative nutrition (i.e. nil by mouth post-surgical dietary care with simple IV fluids untilclinical signs of returning GI function).
99..44..22.. SSttuuddiieess ooff EETTFF vvss.. ssttaannddaarrdd ccaarree
The review conducted identified 10
RCTs20,52,143,180,228,315,318,339,340,361 (Table 41). Fourof these compared the effect of patients receiving12 to 24 hours of nasogastric tube feeding pluscontinued normal hospital diet with patientsreceiving a standard hospital diet only143,228,339,340. Two studies comparednasogastric/nasoduodenal feeding with standard
hospital diet 52,180. One study compared
ENTERAL TUBE FEEDING IN HOSPITAL AND THE COMMUNIT Y 111
38 Malnourished: BMI <18.5 kg/m2, unintentional weight loss >10% within the last 3-6 months, a BMI<20 kg/m2 and unintentional weight loss>5% within the last 3-6 months.39 At risk of malnutrition: eaten little or nothing for more than 5 days and/or likely to eat little or nothing for the next 5 days or longer or poorabsorptive capacity, and or high nutrient losses and or increased nutritional needs from causes such as catabolism.
TTaabbllee 1188:: IInnddiiccaattiioonnss ffoorr eenntteerraall ttuubbee ffeeeeddiinngg
Indication for enteral tube feeding Example
Unconscious patient Head injury, ventilated patient
Neuromuscular swallowing disorder Post-CVA, multiple sclerosis, motor neurone disease, Parkinson’s disease
Physiological anorexia Cancer, sepsis, liver disease, HIV
Upper GI obstruction Oro-pharyngeal or oesophageal stricture or tumour
GI dysfunction or Malabsorption Dysmotility inflammatory bowel disease, reduced bowel length (althoughPN may be needed)
Increased nutritional requirements Cystic fibrosis, burns
Psychological problems Severe depression or anorexia nervosa
Specific treatment Inflammatory bowel disease, for short term enteral access during surgeryi.e. head and neck cancer,
Mental health Patients with Dementia

nasogastric feeding with standard hospital diet
plus ad lib snacks 20, while another had twointervention arms in which patients received anasogastric feed with amino acids alone or anasogastric feed containing amino acids plus
carbohydrates 218. The control group continued ona normal hospital diet. A further study comparedoesophagostomy tube feeding with a clear liquid
diet, advancing to a normal diet as tolerated 315
and one investigated the benefits of pre-operativeETF (nasogastric tube feeding) compared with
routine hospital diet 318. The final study examinedthe effect of perioperative nutrition in
malnourished head and neck cancer patients 361
using three intervention arms: one group receivedno preoperative and standard postoperative ETF;another group received standard preoperative andpostoperative ETF; and the third group receivedarginine supplemented preoperative andpostoperative tube feeding.
The patients included in the studies wereorthopaedic hip fracture patients (four studies
covering 337 patients)20,143,339,340, people whowere generally malnourished (one study covering
86 patients)228, malnourished surgical patients
(one study covering 110 patients) 318, totallaryngectomy patients (one study covering 67
patients)315, malnourished patients undergoingsurgery because of a head and neck malignancy
(one study covering 49 patients) 361 and patientswith alcoholic liver disease (two studies covering
66 patients)52,180.
99..44..33.. CClliinniiccaall eevviiddeennccee EETTFF vvss.. ssttaannddaarrdd ccaarree
The main outcomes reported were nutritionalintake achieved, changes in nutritional status,mortality, length of stay and complicationsassociated with tube feeding (e.g. tolerance of thefeeding tube).
The difference in nutritional intake (usually reportedas energy and/or protein intake) between theenterally tube fed patients and those receivingstandard care was reported in six
studies52,143,180,228,339,340. In all six studies, theenterally fed group achieved a significantly greaternutritional intake (range p<0.0001 to 0.012).
Five studies reported changes in measures of
nutritional status 20,180,228,318,361 with three
showing improvement20,228,318 (range p=0.001 to
p=0.05) while two showed no differences 180,361.
Mortality was reported in 8 studies20,52,143,180,318,
339,340,361. Four showed no differences between
groups 20,339,340,361 but one 52 did showsignificantly lower mortality in the ETF group(p=0.02) and two further studies reported lowermortalities but with no significance values given180,318 . One study, 143 noted a higher mortalityrate for the patients who were tube fed but againno p-value was reported.
There were no significant differences in post-operative complications reported in four
studies315,339,340,361; nor in the incidence of
pressure sores in one study143; diarrhoea in one
study 180, or infection rates in one study 52. In one
study 318 the incidence of wound infection,nausea and vomiting were lower in the ETF groupalthough no p-value was reported.
Five studies reported that ETF had no influence
on length of hospital stay 180,315,339,340,361;
although in one study 20, median time toindependent mobility was lower in the ETF group(p 0.02 -0.04).
Three studies20,228,318 provided information onpatient’s tolerance of ETF but no p-values were
reported. In two studies 22%20 and 30%228 ofstudy participants experienced problemstolerating the nasogastric tube. In the third study318 7 out of 67 patients receiving ETF (10.5%)needed it to be discontinued due touncontrollable diarrhoea, vomiting or severeaversion to the smell and taste of the feed.
99..44..44.. CCoosstt--eeffffeeccttiivveenneessss eevviiddeennccee EETTFF vvss.. ssttaannddaarrdd ccaarree
Four studies were found that reported a cost
comparison104,210,234,256: two RCTs, oneretrospective cohort study and a study thatconstructed a simple model on the basis of twosmall trials (Table 56).
NUTRITION SUPPORT IN ADULTS112

One RCT210 evaluated insertion of double-lumengastrojejunostomy tube compared with routinecare by the surgeon after pancreatico-duodenectomy. Half the patients in the routinecare arm received PN; and the other groupprobably received NG feeding (but the route offeeding was unclear). The study found significantreductions in gastro-paresis and in costs. The
second RCT104 compared early nasogastric enteralfeeding with early oral feeding after colorectalresection in cancer patients. They found thatearly oral intervention was safe but there were nocost savings or improvements in clinical outcomes.
The aim of the retrospective study 234 was to testwhether there were cost savings in using tube-feeding rather than a carer manually feeding thepatient (which requires expensive staff time andrisks causing aspiration) for patients withadvanced dementia. The results showed that thetotal costs were higher for the patients withfeeding tubes compared with those without tubes(£5,600 vs. £3,100, p=0.04). The difference wasdue to tube feeding placement cost and hospitalcosts arising from complications directly related totube feeding. However, the sample size of thisstudy was small (11 patients in each group) andpotentially biased since it was a conveniencesample. Costing was also made using Medicaidand Medicare reimbursement rates, which maynot be applicable to the UK NHS setting.
The fourth cost-effectiveness study evaluated the
cost of preoperative enteral nutrition 256. ETF (10-21 days) was compared with no ETF. The studywas a sensitivity analysis based on the two smalltrials with the largest reduction in complicationrate. Incremental cost per complication avertedwas between £9,000 and £94,500 with hospitalpreoperative ETF, depending on the assumptionsmade. However, they found that homepreoperative ETF is more likely to be cost saving.
There were no economic studies evaluating preand post-operative ETF.
99..44..55.. SSttuuddiieess ooff eeaarrllyy ppoosstt--ooppeerraattiivvee EETTFF vvss.. nnoo eeaarrllyyppoosstt--ooppeerraattiivvee nnuuttrriittiioonn
We identified one systematic review206 thatlooked at early post-operative feeding (oral orenteral) versus post-operative ‘nil by mouth’.There were 11 studies included in this review: 6on early post-operative enteral feeding versus no
early post-operative nutrition 27,58,148,301,310,367 and5 on early post-operative oral feeding versus post-
operative ‘nil by mouth’ 32,144,258,291,334 (includedin the oral chapter 8). In this section we haveincluded the six studies from the systematicreview that looked at the effect of early post-operative ETF. In addition to the studies from thissystematic review, we identified 17 further studiesthat looked at the effect of early post-operativeETF versus no early post-operative nutrition. TheRCTs were analysed according to the type ofsurgical patients included in the studies.
Five studies included patients undergoing upper
GI surgery 45,148,263,341,367 (Table 51). Three studiesincluded patients undergoing lower GI surgery215,301,310 (Table 51). Six studies included both
upper and lower surgery 27,58,160,298,321,328 (Table53). Three studies included patients undergoing
hepatobiliary surgery 117,145,164 (Table 54). Sixstudies included acute trauma patients65,98,175,216,238,281 (Table 45).
We extracted data on seven outcomes: vomiting,anastomotic dehiscence, pneumonia, death, intra-abdominal abscess, wound infection and hospitallength of stay (LOS) where available. Whereappropriate we pooled the data for theseoutcomes. We were unable to pool the data forLOS as the studies reported the data in differentunits and information needed to convert theseunits was not available.
ENTERAL TUBE FEEDING IN HOSPITAL AND THE COMMUNIT Y 113

99..44..66.. CClliinniiccaall eevviiddeennccee:: eeaarrllyy ppoosstt--ooppeerraattiivvee EETTFF vvss.. nnoo eeaarrllyy ppoosstt--ooppeerraattiivvee nnuuttrriittiioonn
Analyses for each of the surgical subgroupsshowed no statistically significant differences inany of the outcomes extracted. The P value fromtests for heterogeneity was greater than 0.1 for alloutcomes in all the groups.
We also conducted a combined analysis whichincluded all the surgical studies (Appendix Eight:Meta-Analyses Enteral versus Nil Post OperativeNutrition Support). This also identified nostatistically significant differences in any of the
outcomes extracted which included vomiting,anastomotic dehiscence, pneumonia, intra-abdominal abscess, wound infection andmortality. The data on lengths of hospital stay
reported in fourteen studies 58,98,117,145,148,216,238,263
,281,301,321,328,341,367 were not adequate to permit acombined analysis but statistically significantdifferences were only detected in two studies withone showing that early feeding led to fewer days
in hospital (p< 0.05)301 whilst the other showed it
extended length of stay (p< 0.01)328.
NUTRITION SUPPORT IN ADULTS114
NNoo.. ppaattiieennttss RRRR ((ffiixxeedd)) ((eeaarrllyy ffeeeeddiinngg//llaattee ffeeeeddiinngg)) 9955%% CCII
VVoommiittiinngg (reported in four studies27,148,175,216 298/280 1.27 [0.92, 1.75]
P value from test for heterogeneity P= 0.21
AAnnaassttoommoottiicc ddeehhiisscceennccee (reported in 10 studies27,148,215,263,301,310,321,328,341,367
257/264 0.60 [0.33, 1.10]
P value from test for heterogeneity P= 0.79
PPnneeuummoonniiaa (reported in 9 studies27,98,148,216,238,263,310,321,328
355/361 0.76 [0.53, 1.08]
P value from test for heterogeneity P= 0.36
DDeeaatthh (reported in 10 studies27,98,148,216,263,281,301,310,321,328
368/375 0.72 [0.45, 1.15]
P value from test for heterogeneity P=0.37
IInnttrraa--aabbddoommiinnaall aabbsscceessss (reported in eight studies27,98,148,238,301,310,321,328
250/256 0.60 [0.32, 1.14]
P value from test for heterogeneity P=0.69
WWoouunndd iinnffeeccttiioonn (reported in 12 studies 27,98,117,148,163,216,263,281,301,321,328,341
402/408 0.92 [0.68, 1.23]
P value from test for heterogeneity P= 0.26
TTaabbllee 1199:: OOuuttccoommeess rreeppoorrtteedd iinn ssttuuddiieess ooff eeaarrllyy eenntteerraall ttuubbee ffeeeeddiinngg
99..44..77.. CCoosstt eeffffeeccttiivveenneessss eevviiddeennccee:: eeaarrllyy ppoosstt--ooppeerraattiivveeEETTFF vvss.. nnoo eeaarrllyy ppoosstt--ooppeerraattiivvee nnuuttrriittiioonn
We identified three cost-effectiveness analyses forETF compared to nil nutrition post-
operatively27,145,147, although all three were smalland potentially biased due to methodologicalweaknesses. Results were inconsistent although allreported a lower number of infections in the ETFgroups compared to the nil groups. Estimatedeffects on cost were as follows:
A non-randomised prospective US study of
patients undergoing bowel resection147 showed acost saving (the magnitude and statisticalsignificance is unclear due to poor reporting) withjejunal feeding tube placed during surgery andfeeding initiated within 12 hours of surgerycompared with usual care (which was notdetailed). The cost savings were due to areduction in infections.

A small Danish RCT27 reported a non-significantdifference in (median) cost of about £1,500 for a4 day nasoduodenal intervention compared withplacebo after major abdominal surgery. Meancosts, which are more relevant than median costs,were not reported.
A small US RCT comparing nasojejunal tubefeeding from 12 hours after surgery with
maintenance iv fluid after liver transplantation 145
found a non-significant incremental cost of£1,200, despite a 50% reduction in infections.Control patients that were moved to tube feedingwere excluded.
99..44..88.. CCoonncclluussiioonnss
ETF in patients where there is some doubt aboutthe adequacy of oral intake is effective inincreasing nutritional intake over and above theintake observed with standard care and/or oralsupplements and this usually leads to animprovement in nutritional status. However, thisdoes not seem to produce consistent benefit interms of length of stay or mortality rates and tubetolerance is sometimes a problem in thesepatients. The evidence of benefit related tocomplications, quality of life, costs and cost-effectiveness is very limited and ETF use in olderpeople with dementia could be more expensivethan oral feeding. The cost-effectiveness ofpreoperative enteral nutrition is unclear but mightbe improved if administered in the patients’home. However, oral nutrition support is likely tobe more cost-effective, when this can be toleratedby the patient.
The studies on early post-operative ETF comparedto standard practice of nil by mouth until returnof GI function, do not support the use of earlyETF although most did not focus on verymalnourished patients who might benefit fromthis approach. There may be cost benefitsassociated with the use of post-operativejejunostomy feeding in some circumstances butmore research is needed.
The studies that examined elective ETF inmalnourished patients prior to surgery suggestthat they benefit in terms of nutritional status.
However, much larger trials are needed todetermine whether there are any benefits inlengths of hospital stay or mortality.
99..44..99.. RRaattiioonnaallee ffoorr rreeccoommmmeennddaattiioonn((ss))
Although ETF does increase nutritional intakes in patients the evidence that this benefitsoutcomes such as length of hospital stay ormortality is not clear.
99..55.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
99..55..11 IInnddiiccaattiioonnss ffoorr eenntteerraall ttuubbee ffeeeeddiinngg
Enteral tube feeding should not be given to
people unless they are malnourished40 or at risk
of malnutrition41 and have; inadequate or unsafeoral intake and a functional, accessiblegastrointestinal tract, or they are taking part in aclinical trial. [[AA]]
EEnntteerraall nnuuttrriittiioonn ssuuppppoorrtt ffoorr ssuurrggiiccaall ppaattiieennttss::
Surgical patients who are: malnourished22 andhave; inadequate or unsafe oral intake and afunctional, accessible gastrointestinal tract andare due to undergo major abdominal procedures,should be considered for pre-operative enteraltube feeding. [[BB]]
General surgical patients should not have enteraltube feeding within 48 hours post-surgery unless
they are malnourished22 or at risk of
malnutrition23 and have; inadequate or unsafeoral intake and a functional, accessiblegastrointestinal tract. [[AA]]
99..66.. EEnntteerraall ttuubbee ffeeeeddiinngg rroouutteess ooff aacccceessss
99..66..11.. IInnttrroodduuccttiioonn
Many types of enteral feeding tubes can be usedto deliver nutrition into the stomach or uppersmall intestine. Choices depend on theproposed/expected period of feeding, clinicalcondition, and anatomy. Nasogastric (NG) tubesare used most frequently but others includenasoduodenal or nasojejunal tubes andgastrostomies or jejunostomies placed byendoscopic, radiological or surgical means.
ENTERAL TUBE FEEDING IN HOSPITAL AND THE COMMUNIT Y 115
40 Malnourished: BMI <18.5 kg/m2, unintentional weight loss >10% within the last 3-6 months, a BMI<20 kg/m2 and unintentional weight loss>5% within the last 3-6 months.41 At risk of malnutrition: eaten little or nothing for more than 5 days and/or likely to eat little or nothing for the next 5 days or longer or poorabsorptive capacity, and or high nutrient losses and or increased nutritional needs from causes such as catabolism.

9.6.1.1 Nasogastric tubes
NG tubes are used mainly for short-term supportin patients who do not have problems such asvomiting, gastro-oesophageal reflux, poor gastricemptying, ileus or intestinal obstruction, althoughthey can also be used for longer term supportwhere other enteral access is not possible orcarries a risk. NG tubes are potentially dangerousin patients with an unsafe swallow and those whoneed to be nursed prone or flat and a risk /benefit assessment should be carried out beforeplacement. Fine bore (5 – 8 FrG) NG tubesshould be used for ETF unless there is a need forrepeated large volume gastric aspiration i.e.gastric decompression. NG tubes should beplaced by appropriately trained staff.
There is a small risk that NG tubes can bemisplaced on insertion or move out of position ata later stage. Position of NG tubes should beverified on initial placement and before each use.Guidance from the National Patient Safety Agency246 advocates aspiration of gastric contents andthe use of pH graded indicator paper. It isrecommended that a pH <5.5 is consistent withgastric placement. If aspirate cannot be obtainedor the pH is >5.5 feeding should not commence.The NG tube should be left in place, the patient’sposition changed and the aspirate re-tested inone hour. The feed itself can increase the pH inthe stomach, so aspiration should take place atleast 1 hour after the feed has been stopped.Radiography (a chest x-ray) is not recommendedroutinely, but it is suggested that local policies bedeveloped for high risk groups (e.g. intensive careor neonatal units) or for where an aspirate is notobtained. Radiography in these circumstanceswould depend on the clinical situation and failureof aspiration checks. N.B. Gastric antisecretorydrugs can cause the gastric acid pH to be altered.Clinical judgement needs to be exercised in thissituation together with local guidance.
9.6.1.2 Nasoduodenal and nasojejunal tubes
Nasoduodenal (ND) and nasojejunal (NJ) tubesare those placed into the gastrointestinal tractwith the distal tip lying beyond the stomach inthe duodenum or jejunum respectively. Thesetubes can be placed at the bedside or withendoscopic/radiological assistance but the
position needs to be confirmed by abdominal X-ray after placement (unless placed underfluoroscopic guidance).
9.6.1.3 Gastrostomy and jejunostomy
Gastrostomy tubes pass through the abdominalwall directly into the stomach. They are usuallyused for patients who require medium to long-term feeding or where NG access is difficult.Gastrostomy tubes are usually placedendoscopically (Percutaneous EndoscopicGastrostomy - PEG) but they can also be placedradiologically or surgically
Jejunostomy tubes pass through the abdominalwall into the jejunum and are usually placedsurgically. However, many percutaneousjejunostomy tubes are placed endoscopically orradiologically via gastric puncture with anextension through the pylorus into the duodenumor jejunum (Percutaneous EndoscopicGastroJejunostomy PEGJ)
Gastrostomy feeding does not negate the risksassociated with reflux and aspiration, althoughrisks may be lower than with NG feeding. Inpatients at high risk of aspiration, jejunostomytubes or PEGJ tubes should be considered sincethey probably do reduce aspiration risks.
99..66..22.. NNaassooggaassttrriicc ((NNGG)) vveerrssuuss nnaassoodduuooddeennaall ((NNDD)) oorrnnaassoojjeejjuunnaall ((NNJJ)) ttuubbeess
9.6.2.1 Introduction
Patients receiving ETF via the naso/orogastricroute can have problems tolerating their enteralfeeding regimen due to gastro-oesophageal refluxor delayed gastric emptying. As a result, patientsmay experience reflux or vomiting which maycause aspiration pneumonia and also result in areduced nutrient intake. When these problemsoccur despite drug intervention, nasoduodenal ornasojejunal feeding should be considered.
9.6.2.2 Studies on Nasogastric (NG) versus
nasoduodenal (ND) or nasojejunal (NJ) tubes
We identified 14 RCTs (707 patients) thatcompared nasogastric feeding with nasoduodenal
or nasojejunal feeding (Table 42) 34,76,77,96,134,
149,153,179,191,200,235,236,247,338. Twelve studies
included intensive care patients34,76,77,96,134,149,
NUTRITION SUPPORT IN ADULTS116

153,179,191,235,236,247, one study malnourished
neurological patients338 and one study was in
healthy people 200. In five of these studies theintervention and comparison arms used thenaso/orogastric route but did not specify thenumber of patients for each.
The main outcomes reported included
aspiration96,153,179,247, pneumonia76,77,179,191,235,
236,338, vomiting77,235,236,247, diarrhoea76,77,179,
235,236 and percentage of target energy
received34,77,96,134,235. Other outcomes reportedincluded: length of stay in ICU and in hospital,mortality and change in nutritional status.
9.6.2.3 Clinical evidence
No significant differences were found formortality, length of stay in intensive care orhospital, incidence of pneumonia, vomiting ordiarrhoea. Two studies reported the mean weight
change, one showed no significant difference 179
while the other reported a significant weight gain
for the nasogastric group 251. However, theweight change for the latter study was onlyrecorded for 21 of the 38 patients entered intothe study. Four out of the five studies reportedno significant difference in the percent of
prescribed calorie intake34,77,96,134 but one showedthe nasojejunal patients achieving a significantlyhigher percent of their daily goal caloric intake
than the nasogastric patients235.
9.6.2.4 Cost-effectiveness
No study reporting cost or cost-effectiveness was found.
9.6.2.5 Conclusions
Feeding patients with a nasogastric tube isusually as effective as a post-pyloric tube(nasoduodenal/nasojejunal) for deliveringnutrients to patients (especially to patients onintensive care). The expected problems of gastricfeeding in patients with gastro oesophageal refluxand delayed gastric emptying are not apparent inthese studies.
It must be noted, however, that for ethical reasonsrandomised studies have not been performed inthe patient groups usually considered for postpyloric feeding, although some information aboutthe effectiveness and safety of post pyloricfeeding in these patients may be gained fromtrials that compare post-pyloric feeding toparenteral nutrition.
9.6.2.6 Rationale for recommendation(s)
The gastric route is usually technically simpler andin most circumstances achieves similar nutrientdelivery with similar risks. Clinical studies havefailed to show any clear advantage in feedingpost-pylorically.
99..77.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
9.7.0.1 Route of access
People in general medical, surgical and intensive
care wards who are malnourished42 or at risk of
malnutrition43 and have; inadequate or unsafeoral intake and a functional, accessiblegastrointestinal tract should be fed via a tube intothe stomach unless there is upper gastrointestinaldysfunction. [[AA]]
People who are malnourished42 or at risk of
malnutrition43 and have; inadequate or unsafe oralintake and a functional, accessible gastrointestinaltract with upper gastrointestinal dysfunction (or aninaccessible upper gastrointestinal tract) should beconsidered for post-pyloric (duodenal or jejunal)feeding. [[DD((GGPPPP))]]
99..88 PPeerrccuuttaanneeoouuss EEnnddoossccooppiicc GGaassttrroossttoommyy ((PPEEGG)) vveerrssuuss NNaassooggaassttrriicc ((NNGG)) FFeeeeddiinngg
9.8.1 Introduction
For some patients with acute or chronicconditions requiring enteral feeding there is theoption of feeding through a nasogastric tube or agastrostomy (usually a PEG). Nasogastric tubefeeding is usually successful but problems includedislodgement of the tube with the need forreplacement which can be invasive anduncomfortable. For some patients the locationand securing by tape of the nasogastric tube canalso be irritating and may raise ethical issues
ENTERAL TUBE FEEDING IN HOSPITAL AND THE COMMUNIT Y 117
42 Malnourished: BMI <18.5 kg/m2, unintentional weight loss >10% within the last 3-6 months, a BMI<20 kg/m2 and unintentional weight loss>5% within the last 3-6 months.43 At risk of malnutrition: eaten little or nothing for more than 5 days and/or likely to eat little or nothing for the next 5 days or longer or poorabsorptive capacity, and or high nutrient losses and or increased nutritional needs from causes such as catabolism.

surrounding patient restraint. For some patientsthe tube itself may also cause discomfort in the back of the throat and occasionallyswallowing problems
In contrast, a gastrostomy tube cannot bedislodged as easily and is more comfortable.However, there are potential difficulties and risksin placement; feed aspiration can still occur andthere can be greater difficulties surrounding anydecision to withdraw gastrostomy feedingcompared to NG/NJ feeding (although from theethical stand-point there is no distinction to bemade between short and long-term tubes, norbetween withdrawing feeding compared to notinstigating it in the first place (section 5.3). Sincegastrostomy feeding is increasingly considered forpatients likely to require long-term ETF weundertook a review of studies comparing the twoaccess techniques.
9.8.1.1 Studies considered for this review
Our review compared percutaneous endoscopicgastrostomy with nasogastric feeding (Table 43).
Three small published RCTs 15,251,267 and a large
multi-centre randomised controlled trial 343 metthe inclusion criteria. One study looked atneurological, surgical and ear, nose and throat
(ENT) patients 15, while the multi-centre study andthe other two studies focused on stroke patients
with accompanying dysphagia 251,267,343.
The main outcomes reported in the studies wereabsolute risk of death and risk of death or pooroutcome (using the Modified Rankin Scale - MRS),treatment failure, amount of feed received, weightchange, mortality, GI - haemorrhage and pressuresores. Other outcomes reported were: the timeneeded for tube insertion, length of hospital stay,convenience of care, quality of life, fixation oftube to patient and the incidence of aspiration or pneumonia.
9.8.1.2 Clinical evidence
There were some methodological problems with
two of the smaller studies. One15 had more sickpatients in the PEG group than did the NG groupsuggesting a possible allocation bias between
groups, while in another 267 most of the patientsin the NG arm crossed over to the PEG arm less
than halfway through so that by day 28 of thestudy period, 18 out of the 19 patients hadswitched to PEG feeding.
Two studies251,267 reported significantly greaterintake of prescribed feed and consequentlysignificantly greater weight gain in PEG patients.
In three studies15,251,267 there was a non-significant increase in treatment failure in thenasogastric group.
Mortality was reported for all of the trials. One of
them 267 showed no difference between studygroups, one showed significantly higher mortality
in the nasogastric arm than the PEG arm 251 and
two 15,343 reported higher mortality in the PEGgroup especially if inserted within the first twoweeks following a stroke. In addition to the smallincrease in risk of death demonstrated by the
large multi-centre randomised trial 343, this studyalso showed an increased risk of poor outcomes,although for secondary outcomes such as GIhaemorrhaging, PEG patients fared better.
9.8.1.3 Cost-effectiveness evidence
We did not find any study reporting cost or cost-effectiveness.
9.8.1.4 Conclusions
The results of the largest multi-centre trial showedthat significant benefit of a PEG over an NG tubeis very unlikely and there is a significantmortality/ morbidity from PEG insertion.However, patients generally prefer a PEG to a NGtube for long term treatment as it less likely todisplace, can remain unseen and is morecomfortable. A PEG should therefore beconsidered after a patient has been shown totolerate gastric feeding via a nasogastric tube for2-4 weeks or in patients unable to tolerate anasogastric tube despite the tube being wellsecured. After an acute neurological event such asa stroke, insertion of a PEG should be delayeduntil; the prognosis/QOL of the patient can bebetter predicted.
‘If the patient cannot decide for themselves, thedoctor must provide such treatment and care as arein the patient’s best interests including the durationfor which treatment is to be provided. Indetermining what constitutes best interests the
NUTRITION SUPPORT IN ADULTS118

doctor should have regard to the views expressed bycarers and the appropriate multidisciplinary healthteam (see Section 5.3).’ A similar group shoulddecide whether feeding should be stopped. Inclinical practice it is more difficult to stop feedingthrough a PEG than though an NG tube althoughthe same ethical/ moral considerations apply.
99..99.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
99..99..11 PPeeooppllee wwiitthh ddyysspphhaaggiiaa
In the acute setting, for example following stroke,people unable to swallow safely or take sufficientenergy and nutrients orally should have an initial2–4 week trial of nasogastric enteral tubefeeding. Healthcare professionals with relevantskills and training in the diagnosis, assessmentand management of swallowing disorders shouldassess the prognosis and options for futurenutrition support. [[AA]]
99..99..22 RRoouuttee ooff aacccceessss
Gastrostomy feeding should be considered inpeople likely to need long-term (4 weeks or more)enteral tube feeding. [[DD((GGPPPP))]]
99..1100.. CCoommmmeenncciinngg eenntteerraall ttuubbee ffeeeeddiinngg aafftteerr iinnsseerrttiioonn ooff aa ppeerrccuuttaanneeoouuss eennddoossccooppiicc ggaassttrroossttoommyy
99..1100..11 IInnttrroodduuccttiioonn
Percutaneous endoscopic gastrostomy (PEG) is arelatively common procedure but it has asignificant mortality/morbidity (NCEPOD report).The length of time one should wait beforecommencing feeding after insertion of the tubehas been subject to controversy. Many cliniciansbelieve that feeding should be delayed for at least24 hours post-insertion but others use PEGs muchearlier. Delays in starting PEG feeding may resultin unnecessary prolongation of hospital stay andcosts. A review was therefore performed to assessthe safety of early PEG feeding (within four hoursof installation) compared with delayed feeding(more than 24 hours after installation).
99..1100..22 SSttuuddiieess ccoonnssiiddeerreedd ffoorr tthhiiss rreevviieeww
Four published RCTs (including 290 patients) met
the inclusion criteria46,63,223,333 (Table 46). Themore recent studies were of highermethodological quality. The mean age of patientsin all studies was more than 60 years.
99..1100..33 CClliinniiccaall eevviiddeennccee
No significant differences were reported formortality (three studies) or complication rates (4studies), although two studies reported moregastric distension which had resolved by day threeafter insertion.
99..1100..44 CCoonncclluussiioonn
Since none of the studies detected a significantdifference or trend between the early or lategroups it can be assumed that in anuncomplicated patient there is no reason to delaythe start of feeding for more than 4 hours afterinsertion of a new PEG tube.
99..1111.. RReeccoommmmeennddaattiioonn ffoorr cclliinniiccaall pprraaccttiiccee
99..1111..11 RRoouuttee ooff aacccceessss
Percutaneous endoscopic gastrostomy (PEG) tubeswhich have been placed without apparentcomplications can be used for enteral tubefeeding 4 hours after insertion. [[AA]]
99..1122.. TTyyppeess ooff eenntteerraall ffeeeeddss
Most enteral feeds come as ready to use liquidmicrobial free preparations that contain energy,protein, vitamins, minerals, trace elements andfluid +/- fibre. They are usually nutritionallycomplete within a specific volume. A ready to usestandard feed will usually contain 1 kcal and0.04g protein per ml but many other types ofenteral feed preparations are available withdiffering energy: protein ratios and types of fat or protein.
The GDG did not undertake a formal review of theliterature related to different types of enteralfeed, however a summary is provided in Table 20.
ENTERAL TUBE FEEDING IN HOSPITAL AND THE COMMUNIT Y 119

TTaabbllee 2200:: TTyyppeess ooff eenntteerraall ffeeeedd
NUTRITION SUPPORT IN ADULTS120
Type of feed Usage
Standard 1kcal/ml – with or without fibre Suitable for the majority of patients. Combination ofsoluble and insoluble fibre added for use in patientson long term feeding.
High energy 1.2-2.0 kcal/ml – with or without fibre Used for patients on fluid restriction, or with increasednutritional requirements. Combination of soluble and insoluble fibre added for use in patients on longterm feeding.
Low energy formulas Contain 0.5 – 1 kcal/ml are complete for vitaminsand minerals in a lower volume. Usually used for longterm HETF patients with low energy requirements.
Elemental / Peptide feeds Provide nitrogen in the form of free amino acids orpeptides and may be used in the presence of severemaldigestion or malabsorption
Milk free feed Standard 1kcal/ml feed with a soya based protein source
Low Sodium feeds Standard feeds with the sodium content reduced toaround 10-15 mmol/litre
Renal feeds Contain reduced amounts of sodium, potassium andphosphate. The protein content is variable, providingsimilar or lower protein: calorie ratios compared tostandard feeds. Energy dense versions for fluidrestriction are available, with subtle modification ofother nutrients e.g. higher water soluble vitamincontent to allow for intradialytic losses
Respiratory feeds Contain a higher percentage energy content from fat,which may reduce the amount of carbon dioxideproduced from feed metabolism, and may be useful inpatients with respiratory failure
Immune feeds Contain variable amounts of specific amino acids orfats, together with altered levels of specificmicronutrients which have an immune benefitattributed to them
Jejunostomy/high output Ileostomy feeds These need to have an osomolality of 300 mOsm/Land a sodium content of 100 mmol/L.

99..1133.. MMooddee ooff ddeelliivveerriinngg EEnntteerraall TTuubbee FFeeeeddiinngg
99..1133..11 BBoolluuss vv ccoonnttiinnuuoouuss
Administering an enteral feed into the stomachrather than small intestine permits the use ofhypertonic feeds, higher feeding rates and bolusfeeding. Enteral feeding pumps are available toalter rates and in patients with doubtful GImotility, the stomach may be aspirated every 4hours. If aspirates are high (e.g. exceed 200 –300 mls depending upon local policy), the pumprate may be reduced and/or prokinetic drugsconsidered. This is usually recommended in thecritical care setting though an aspirate of under400 ml correlates poorly with the risk of
aspiration or pneumonia225. Enteral feedingdelivery is usually increased gradually over thefirst 24 hours (or slower in the very malnourished,see section 6.6).
When using NG feeding, enteral feeds can bedelivered continuously over a variable number ofhours or intermittently as boluses (or as acombination of both methods). There arepotential advantages and disadvantages to bothmethods. We therefore identified studies thatcompared different modes of delivering enteralfeeds. The RCTs found were categorised intocontinuous v bolus and continuous (24hr) vcontinuous (16-18hr). The rationale for non-continuous feeding is that it is more physiologicaland allows the stomach to completely empty andhence may reduce bacterial colonisation of thestomach which may be safer should an episode ofaspiration occur.
99..1133..22.. SSttuuddiieess oonn bboolluuss vvss.. ccoonnttiinnuuoouuss
Nine studies compared continuous v bolusregimens in neurological dysphagic patients,patients with injuries to the head, post-operative
cancer patients, critically ill patients314, older
patients and healthy adults24,35,66,154,188,201,276,332
(Table 44). Most regimens described in thestudies compared 24 hourly continuous feedingwith 3-6 hour bolus feeds (250 -500ml). Themain outcomes reported were: abdominaldiscomfort, aspiration pneumonia, change innutritional status, clogged tubes, nurse preferenceand biochemical changes.
99..1133..33.. CClliinniiccaall eevviiddeennccee oonn bboolluuss vvss.. ccoonnttiinnuuoouuss
For abdominal discomfort, aspiration pneumonia andnurse preference there was no evidence of benefitbetween the continuous and bolus fed
group54,66,201,332. However, in one study276 thecontinuous group were found to have a significantimprovement in nutritional status (body weight andarm circumference) compared to the bolus fed group
(p<0.01), while in another 66 there was less cloggingof nasogastric tubes with bolus feeding (p=0.01).
99..1133..44.. CCoonnttiinnuuoouuss vvss.. ccyycclleedd ccoonnttiinnuuoouuss
Five studies compared continuous ETF (24hours) vcycled continuous ETF (16 -18hours) with daily breaks(2 – 4 hours) or even intermittent ETF (e.g. 4-6 hoursfeeding then 2 hours rest). Studies were undertakenin critically ill, ventilated patients and post surgical
patients35,55,134,323,360. The main outcomes reportedwere; length of hospital stay, duration of enteralfeeding, mortality, ventilator associated pneumonia,gastric pH and rate of gastric colonisation.
99..1133..55.. CClliinniiccaall eevviiddeennccee:: ccoonnttiinnuuoouuss vvss.. ccyycclleedd ccoonnttiinnuuoouuss
There were no significant differences between the24 hour continuous feeding groups and the 16-18hour feeding groups in either mortality or
ventilator associated pneumonia; 35,134,360, andrates of gastric colonisation and levels of gastric
pH were also similar35,323. In one study however360 there was a significant reduction in hospitalstay for a 16 hour fed group compared to a 24hour continuous group (p=0.04).
99..1133..66.. CCoosstt--eeffffeeccttiivveenneessss
No study reporting cost or cost-effectiveness was found.
99..1133..77.. CCoonncclluussiioonnss
Bolus feeding is as effective as continuous (16-24hours) feeding. Overall, however, the mode of feeddelivery can be dictated by practical issues. Forexample, in patients who pull or dislodge nasogastrictubes regularly, bolus feeding can be used as apractical safe alternative to continuous feeding, whilein intensive care the severity of illness and issues ofgastric emptying, metabolic stability and control ofglucose levels favour continuous feed administration.
RUNNING HEAD 121

99..1144.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
99..1144..11 MMooddee ooff ddeelliivveerryy
For people being fed into the stomach, bolus orcontinuous methods should be considered, takinginto account patient preference, convenience anddrug administration. [[BB]]
For people in intensive care, nasogastric tubefeeding should usually be delivered continuouslyover 16–24 hours daily. If insulin administration isneeded it is safe and more practical to administerfeeding continuously over 24 hours. [[DD((GGPPPP))]]
99..1155.. MMoottiilliittyy AAggeennttss
99..1155..11 TThhee uussee ooff eenntteerraall mmoottiilliittyy aaggeennttss
If patients with impaired gastrointestinal motilityare fed enterally they may develop symptoms ofabdominal distension vomiting, gastrooesophageal reflux, pulmonary aspiration,pneumonia or sepsis. They may also have largegastric aspirates and impaired fluid andnutritional intakes. The administration ofprokinetic agents is used widely to help withthese problems by promoting gastric emptyingand improving intestinal motility. We conducted areview to identify studies comparing patientsreceiving enteral feeds with and without motilityagents to see whether this approach is of benefit.
99..1155..22 SSttuuddiieess oonn eenntteerraall mmoottiilliittyy aaggeennttss iinn EETTFF
Ten studies were identified and were categorisedinto 5 groups according to the type of prokineticagent administered; erythromycin,metaclopromide and or cisapride (Table 47 andTable 48). However, since cisapride has now beenwithdrawn, the studies using that drug are notreported here. Most of the studies includedpatients on intensive care in whomgastrointestinal feed intolerance is associatedwith a worse outcome and the development ofaspiration pneumonia. However, this associationis not considered to be causal and the inclusion ofthese high risk patients in the studies makesinterpretation difficult.
9.15.2.1 Erythromycin v placebo
5 studies were included in which erythromycinwas administered intravenously either as a single
dose 61,212 or every six hours for a minimum of five
days30,289,381 (Table 46). Four studies includedintensive care patients and one pancreatico-duodenectomy patients. In 2 studies patientswere only recruited if they demonstrated
intolerance to enteral feeding61,212. The outcomesassessed included mortality, pneumonia, length ofstay, complications, gastric emptying, residualgastric volume and feed tolerance.
One study30 detected no significant differences inmortality, pneumonia or length of stay between theintervention and control group and two studies30,381 reported similar complication rates. Gastricresidual volumes were lower with erythromycin in
one study289 but there were no differences
reported in another 381. Improved tolerance toenteral feeds in the intervention group, was
observed in one study30, p=0.001 during the first48 hours of feeding but there were no significantdifferences by the end of the study period. In
another study61 enteral feeding was moresuccessful in the intervention group after 1hour,p=0.05 and 12 hours, p=0.01 of a single initiatingdose of erythromycin but there were no significantdifferences 24 hours after the dose.
9.15.2.2 Metoclopramide v placebo
Three studies were included176,212,380 one of which
also had an additional arm for erythromycin212
(Table 47). All the studies included intensive care
patients who were tube fed, with one study 212
only recruiting patients who were not toleratingenteral feeds. The metoclopramide was
administered intravenously in one study176 and via
a naso/orogastric tube in the other two212,380. Nodifferences were found in intensive care mortalityor nosocomial pneumonia, however, this could bedue to the inadequate power of the studies.Gastric emptying rates were higher with
metaclopramide (p=0.04) in one study 176 but
similar in another 212.
NUTRITION SUPPORT IN ADULTS122

99..1155..33 CCoosstt--eeffffeeccttiivveenneessss
Motility agents could be cost-effective, if they getthe gut working without having to resort toparenteral nutrition in a substantial proportion ofpatients. No study reporting cost or cost-effectiveness was found.
99..1155..44 AAddddiittiioonnaall ccoonnssiiddeerraattiioonnss
Prior to administration of motility agents healthcareprofessionals should review the patient’s need fordrugs with known effects in delayed gastricemptying, such as opiates. A reduction in the doseof these drugs may itself improve intolerance toenteral feeds. Within intensive care elevating thehead of the patient above 30 degrees isrecommended at all times for ETF also turning onthe right side may improve gastric emptying.
Patients with moderate to mild gastric motilityproblems should be offered oral/enteral/IVerythromycin unless there is a high probability ofintolerance. Patients with severe gastric problemsand those who do not respond to oral agents after48 hours, should be offered IV motility agents andalternative methods of nutrition support such aspost-pyloric ETF or PN may be needed.
99..1155..55 CCoonncclluussiioonnss
Metaclopromide and erythromycin appear to beeffective in improving gastric motility and mayimprove tolerance to enteral feeds for a limitedperiod. However, the studies do not provideevidence of benefit for important long term clinicalend points. In the intensive care population careshould be taken to consider the risk of druginteractions and side-effects (e.g. dystonic reactions
in older people with metoclopramide).
99..1166.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
99..1166..11 MMoottiilliittyy aaggeennttss
For people in intensive care with delayed gastricemptying who are not tolerating enteral tubefeeding, a motility agent should be considered,unless there is a pharmacological cause that canbe rectified or suspicion of gastrointestinalobstruction. [[AA]]
People in other acute care settings who havedelayed gastric emptying and are not toleratingenteral tube feeding should also be offered amotility agent unless there is a pharmacologicalcause that can be rectified or suspicion ofgastrointestinal obstruction. [[DD((GGPPPP))]]
If delayed gastric emptying is severely limitingfeeding into the stomach, despite the use ofmotility agents, post-pyloric enteral tube feedingand/or parenteral nutrition should be considered.[[DD((GGPPPP))]]
99..1177.. CCoommpplliiccaattiioonnss ooff eenntteerraall ttuubbee ffeeeeddiinngg
99..1177..11 IInnttrroodduuccttiioonn
Although the GDG did not conduct a formalreview of the literature, it is important torecognize that Enteral Tube feeding is associatedwith a number of complications. These aresummarised in Table 21.
In view of the above, placement of all enteraltubes should only be undertaken by suitablytrained individuals. The position of all NG tubesshould be confirmed after placement and before
RUNNING HEAD 123
TTyyppee CCoommpplliiccaattiioonn
Insertion Nasal damage, intra-cranial insertion, pharyngeal/oesophageal pouch perforation,bronchial placement, precipitate variceal bleeding.
PEG/PEJ insertions – bleeding, intestinal/colonic perforation.
Post insertion trauma Discomfort, erosions, fistulae and strictures.
Displacement Tube falls out’, bronchial administration of feed
Reflux Oesophagitis, aspiration
GI intolerance Nausea, bloating, pain, diarrhoea
Metabolic Refeeding syndrome, hyper-glycaemia, fluid overload, electrolyte disturbance.
TTaabbllee 2211 CCoommpplliiccaattiioonnss ooff eenntteerraall ttuubbee ffeeeeddiinngg

each time of using aspiration and pH paper (withX-ray if necessary) as per the advice from the
National Patient Safety Agency 246. This adviceshould be incorporated in local protocols whichshould also address the clinical criteria (e.g.unchanged length of tube, absence of anyapparent ETF related problems) which will allowETF to proceed when the ability to repeat checksof position are limited (aspiration and pHchecking may be impossible or unhelpful due togastric acid suppression and repeated X-raysbefore every feed are not practical). The initialplacement of post-pyloric tubes requires X-raywith clinical checks before repeated use. Allpatients receiving ETF should be closelymonitored, particularly early after instigation.Monitoring allows quantification of losses toenable daily estimation of replacementrequirements, maintenance of metabolic balance,detection of toxicity/deficiency states, and earlydetection of complications (see Chapter 7). NGtubes should be replaced in the time framerecommended by the manufacturers.
99..1188.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
99..1188..11 MMaannaaggeemmeenntt ooff ttuubbeess
People requiring enteral tube feeding should havetheir tube inserted by healthcare professionalswith the relevant skills and training. [[DD((GGPPPP))]]
The position of all nasogastric tubes should beconfirmed after placement and before each use byaspiration and pH graded paper (with X-ray ifnecessary) as per the advice from the NationalPatient Safety Agency (NPSA 2005). Local protocolsshould address the clinical criteria that permitenteral tube feeding. These criteria include how toproceed when the ability to make repeat checks ofthe tube position is limited by the inability toaspirate the tube, or the checking of pH is invalidbecause of gastric acid suppression. [[DD((GGPPPP))]]
The initial placement of post-pyloric tubes should beconfirmed with an abdominal X-ray (unless placedradiologically). Agreed protocols setting out thenecessary clinical checks need to be in place beforethis procedure is carried out. [[DD((GGPPPP))]]
99..1199.. RReesseeaarrcchh rreeccoommmmeennddaattiioonnss
WWhhaatt aarree tthhee bbeenneeffiittss ttoo IInntteennssiivvee ccaarree ppaattiieennttsslliikkeellyy ttoo ssttaayy ffoorr >>55 ddaayyss,, wwhhoo aarree ooffffeerreedd EETTFFoonnllyy ccoommppaarreedd ttoo EETTFF aanndd PPNN iiff tthheeyy ffaaiill ttoottoolleerraattee >>6600%% ooff tthheeiirr ttaarrggeett nnuuttrriittiioonnaall nneeeeddss 22ddaayyss aafftteerr ssttaarrttiinngg EETTFF iinn tteerrmmss ooff ssuurrvviivvaall,,ccoommpplliiccaattiioonnss aanndd hhoossppiittaall ccoossttss??
This is an area of common practice but where thebenefits of these interventions are unclear andpoorly reported.
WWhhaatt aarree tthhee bbeenneeffiittss ttoo mmaallnnoouurriisshheedd ssuurrggiiccaallppaattiieennttss wwhhoo hhaavvee iinnddiiccaattiioonnss ffoorr EETTFF bbeeiinnggooffffeerreedd EETTFF oonnllyy ccoommppaarreedd ttoo EETTFF aanndd PPNN iiff tthheeyyffaaiill ttoo ttoolleerraattee >>6600%% ooff tthheeiirr ttaarrggeett nnuuttrriittiioonnaallnneeeeddss ttwwoo ddaayyss aafftteerr ssttaarrttiinngg EETTFF iinn tteerrmmss ooffssuurrvviivvaall,, ccoommpplliiccaattiioonnss aanndd hhoossppiittaall ccoossttss??
Currently patients who present with theindications for enteral feeding are being given PNearly when it seems that they are not toleratingenough enteral feed to meet requirements,however the benefits of fairly early interventionwith PN are unclear.
WWhhaatt aarree tthhee bbeenneeffiittss ooff eenntteerraall ttuubbee ffeeeeddiinnggccoommppaarreedd ttoo nnoo eenntteerraall ttuubbee ffeeeeddiinngg iinn ppeeoopplleewwiitthh ddyysspphhaaggiiaa aanndd eeaarrllyy ttoo mmiidd ssttaaggee ddeemmeennttiiaaiinn tteerrmmss ooff rreedduucceedd ccoommpplliiccaattiioonnss aassssoocciiaatteedd wwiitthhsswwaalllloowwiinngg,, iimmpprroovveedd nnuuttrriittiioonnaall ssttaattuuss,, ddeellaayyoonnsseett ooff aaddvvaanncceedd ssttaaggee ddeemmeennttiiaa,, hhoossppiittaallaaddmmiissssiioonnss,, ccoosstt eeffffeeccttiivveenneessss aanndd ssuurrvviivvaall??
Much of the research tends to tends to focus orconcentrate on tube feeding people with advanceddementia or those who may be in terminal stagesof the disease. Depending upon the types ofdementia a person has swallowing disorders mayoccur at an earlier stage in the disease, forexample vascular dementia. The benefits andcomplications of tube feeding may be quitedifferent in people in the earlier stages than thosewho are in the advanced stage of dementia.
NUTRITION SUPPORT IN ADULTS124

1100..11 IInnttrroodduuccttiioonn
Parenteral nutrition (PN) refers to theadministration of nutrients by the intravenousroute. It is usually administered via a dedicatedcentral or peripheral placed line and is generallyused where there is:
a. failure of gut function (e.g. with obstruction,ileus, dysmotility, fistulae, surgical resection orsevere malabsorption) to a degree thatdefinitely prevents adequate gastrointestinalabsorption of nutrients
and
b. the consequent intestinal failure has eitherpersisted for several days (e.g. >5 days) or islikely to persist for many days (e.g. 5 days orlonger) before significant improvement.
It may also be needed in patients with reasonablegut function who cannot eat when ETF isimpossible or impractical for reasons of tube access.
PN is an invasive and relatively expensive form ofnutrition support (equivalent to most ‘newgeneration’ IV antibiotics daily) and ininexperienced hands, can be associated with risksfrom line placement, line infections, thrombosisand metabolic disturbance. Careful considerationis therefore needed when deciding to who, whenand how this form of nutrition support should begiven. Whenever possible, patients should beaware of why this form of nutrition support isneeded and its potential risks and benefits.
In view of the complex issues surrounding PNadministration, we conducted a number ofreviews in an attempt to provide evidence basedguidance on the indications and benefits/risks ofPN versus enteral, oral and no nutritional
intervention. The reviews also aimed to provideguidance on some technical issues of deliveringparenteral feeds. The GDG, however, were acutelyaware of the limited relevance to normal clinicalpractice of studies examining indications for usingPN for two important reasons:
• RCTs of PN vs. alternative or no nutritionsupport have excluded on ethical groundspatients with a ‘definite’ indication for suchfeeding i.e. those with indications for nutritionsupport but who have intestinal failure to adegree prohibiting feeding by oral or enteraltube methods. Results may therefore beinapplicable to patients in whom PN is usuallyadministered.
• most studies comparing PN to ETF have beenundertaken in surgical and intensive caresettings in patients who can only toleratesmall amounts of enteral feed. The studiestherefore not only compare different routes ofnutrient provision but usually differentamounts, with these severely ill patientsgetting levels of PN support that raiseconcerns amongst GDG members.
The general recommendations for PN use aretherefore based upon the principles elucidated inChapter 2 of these guidelines, taking into accountthe results of the studies reviewed where possible.
1100..22.. PPNN vveerrssuuss nnoo PPNN
1100..22..11.. IInnttrroodduuccttiioonn
PN is generally started in order to prevent orminimize the adverse effects of malnutrition inpatients who would otherwise have no significantnutritional intake. However, the length of timethat a patient can tolerate complete or near
PARENTERAL NUTRITION IN HOSPITAL AND THE COMMUNIT Y 125
10.Parenteral nutrition in hospital and the community

complete starvation without harm is unknownand probably variable. In the well nourished it islikely to be many days before the outset ofproblems but even then, early ‘elective’ PNsupport may be beneficial. Indeed, pre-emptivePN support (e.g. PN for malnourished patientsbefore surgery likely to cause temporary intestinalfailure) might also be of value. We thereforeconducted reviews of studies that randomizedpatients to the elective use of PN versus standardcare of simple IV fluids with oral intake astolerated or as dictated by routine clinical practice(e.g. restricted for a few days after surgery).
1100..22..22.. SSttuuddiieess ccoonnssiiddeerreedd ffoorr tthhiiss rreevviieeww
One general review identified a systematic
analysis 190 that looked at the efficacy of PNcompared with no nutrition support on clinicallyimportant parameters such as mortality, morbidityand length of hospitalisation (Table 58). Thissystematic review included randomised studies inpatients with a variety of conditions such aspulmonary disease, liver disease, oncological,perioperative, acute pancreatitis, InflammatoryBowel Disease (IBD) and AcquiredImmunodeficiency Syndrome (AIDS). In addition
to the systematic review, four RCTs178,296,304,377
(Table 58) were identified: one 296 including 55well-nourished, females with stage II-IV breastcancer undergoing high-dose chemotherapy and
haematopoietic cell transplantation (HCT); one 377
including 122 patients following major thoracic-
abdominal procedures; one 304 including 300patients undergoing major general surgical
procedures; and one 178 including patients withgastric cancer undergoing total gastrectomy.
Independently from the above, a second reviewexamined the elective use of PN around the timeof surgery. These surgical patients could besubdivided into two further groups:
a. Pre-operative supplementary PN versus no pre-operative supplementary nutrition: Two RCTs29,327 (Table 76) studied the effect of pre-operative PN vs. no pre-operative nutritionsupport in malnourished GI surgical patientsdefined by weight loss (>10%) or a PrognosticNutritional Index (PNI score >30%).
b. Pre and post-operative PN versus nosupplementary perioperative nutrition. Seven
RCT’s42,99,100,240,346,348,366 (Table 76) examinedvarious periods of pre- and post-operative PNversus no perioperative nutrition support ingroups of surgical patients who were alsomalnourished at the time of surgery, mostwith gastro-intestinal malignancy.
1100..22..33.. CClliinniiccaall eevviiddeennccee
10.2.3.1 Elective PN in all patients
As stated above, the evidence from the studiesfound applies to the use of PN in circumstanceswhich are not common within UK practice i.e. inpatients who have no definite indication forintravenous support. The combined data from all
patient groups in the Koretz systematic review 190
showed no benefit for giving early PN comparedto no early nutrition support, and in the group ofoncology patients (including 19 trials of 1050patients) PN use resulted in an increase ininfectious complications, although there was nochange in mortality. However, all results from thisreview have a major limitation in that the RCTsexamined had all excluded severely malnourishedpatients from the studies. Furthermore, several ofthe studies came from a period when very highlevels of PN support were given to patients, oftenresulting in significant hyperglycaemia which isknown to increase risks. The findings are thereforeinapplicable to usual UK PN practice.
In addition to the overall findings of the Koretzreview, the studies within it and the other studieswe identified showed little or no benefit fromearly elective use of PN in various sub groups. PNusage did improve nutritional status and/ornitrogen balance in some cases but clinicaloutcomes were no better in most instances and insome they were worse. For example, in two trialsof patients with acute pancreatitis (subgroupanalysis within the Koretz review) and one trial in
gastric cancer resection patients 178, PN resultedin significantly more complications and longerhospitalisation compared to standard therapy ofIV fluids only.
NUTRITION SUPPORT IN ADULTS126

10.2.3.2 Elective PN in surgical patients
The studies in surgical patients receiving only pre-
operative PN 29,327 showed no significantdifferences in mortality or length of hospital staybetween PN fed and control groups, althoughBellatone reported increased septic complicationsin controls (p<0.05). However, studies in patientsreceiving both pre-and post-operative PN supportdid suggest benefits from this approach. Four
studies 42,100,240,346 showed lower mortality inpatients given PN compared to controls although
only in one240 did this reach significance
(p<0.05). The same four studies 42,100,240,346 alsoshowed reduced complications in severelymalnourished patients given perioperative PN,
although in only 2 studies42,240 this was not
significant. Two RCTs100,348 showed greater weightgain for patients receiving perioperative nutrition
with one 348 reaching significance (p<0.01). One
study 366 also reported lower intra-abdominalabscess rates in malnourished PN supportedpatients versus malnourished controls (p<0.05)
and another 346 found that whilst borderline ormildly malnourished patients given PN hadincreased rates of infections, severelymalnourished patients had reduced non-infectiouscomplications and no increase in infectiousproblems when given PN.
The beneficial effects of perioperative PN inmalnourished individuals identified in the last
mentioned study above 346 were only seen inpatients who received > 7 days PN. This has ledto a widespread belief that PN in normal clinicaluse (i.e. in those who really need it) is of no valueunless given for >7 days. The GDG believe thatthis is not true. Patients with definite indicationsfor PN support are not the same as those in thetrial and within the first few days of PNadministration to a malnourished patient withreversible gastro-intestinal failure, it is notuncommon to see rapid resolution of that failureas nutrient deficiencies and adverse changes inmetabolism and physiology are corrected. Thepatient is then able to resume feeding by the oralor enteral route.
10.2.3.3 Cost-effectiveness evidence
As with our other reviews of the use of PN indifferent circumstances, evaluation of cost-effectiveness studies was limited by the fact thatthey do not apply to the usage of PN within UKclinical settings. However, six cost studies andone cost-utility study were found (Table 76).Three were evaluating the preoperative use ofparenteral nutrition and four its postoperative use.
A US cost analysis 89 based on a relatively large
well-conducted RCT346 compared pre and post-opPN (16 days) vs. no pre-op and post-op PN atclinician’s discretion. The patients weremalnourished (mainly men) and were undergoinglaparotomy or thoracotomy. They found overallno difference in complications. For theintervention group, who were admitted early forpre-operative PN, there was a longer length ofstay and an incremental cost of £1,900 perpatient (significance not stated). However, forhigh-risk patients (identified using SubjectiveGlobal Assessment) there was a significantreduction in non-infectious complications with anassociated cost-effectiveness of £4,300 percomplication averted.
A smaller US RCT342 compared PN over 28 dayswith individualised oral, enteral parenteralnutrition support for patients in early recoverystage after bone marrow transplantation. PNpatients had a longer length of stay, increasedinfections and increased complications, but thepatients receiving PN were probably sicker thanthose in other groups. There was an incremental
cost of £850 per patient. A Spanish study53
based on a single cohort also estimated theincremental cost of PN in this patient group butcompared it with a programme of intensivemonitoring – it too found an incremental costassociated with the use of PN.
A Spanish RCT 57 compared early PN over fivedays with IV fluids alone in patients undergoingtotal gastrectomy for gastric cancer. This reportedsubstantial cost savings through the use of PN,
although a Japanese RCT178 in very similarpatients, found that early oral intake was lesscostly than early PN.
PARENTERAL NUTRITION IN HOSPITAL AND THE COMMUNIT Y 127

A decision analysis358, again in a US contextcompared 10 days preoperative PN with no PN forpatients undergoing surgery for gastrointestinalcancer. They assumed reductions in length of stayand complication rates and hence estimated anincremental cost saving of about £1000 perpatient. In contrast, a Canadian decision
analysis129 comparing PN (10 days) with bothselective PN and no PN in patients undergoingmajor upper GI surgery with and without cancer,suggested that both cancer and non-cancergroups would have increased life expectancy butat increased cost. The use of PN was relativelycost-effective (which they defined as <£30,000per QALY gained) in the following groups:
• Non cancer – high and moderate risk
• Localised stomach cancer - high risk andmoderate risk
• Regionalised stomach cancer - high risk
• Localised oesophageal cancer - high risk
Benefits of PN were small for patients with lowlife expectancy i.e. those with more advancedcancer. The fact that the US model assumed agreater reduction in major complications and agreater cost per complication was the reason whythe US model suggested cost savings whilst theCanadian model did not (Table 22).
NUTRITION SUPPORT IN ADULTS128
Goel129 Goel129
US study 358 Not cancer Cancer
Patients with a major complication averted (a) 19% 2% 11%
Cost per major complication (b) £26,000 £6,500 £6,500
Cost savings per patient (a x b) £5,000 £130 £740
TTaabbllee 2222:: CCoommppaarriissoonn ooff mmooddeell aassssuummppttiioonnss
10.2.3.4 Conclusions
Evidence from these reviews of elective PN use isdifficult to interpret since the use of PN in themajority of patients included in the trials was out ofline with routine UK clinical practice. The negativefindings in the reviews therefore have littlerelevance to PN use in patients who have been orare likely to be unable to feed by other means. PNshould therefore be considered in all such patients,taking into account whether likely benefitsoutweigh potential risks. There is no evidence tosupport the widely accepted idea that PN was inretrospect unnecessary if, in such patients, it provesto have been required for <7 days.
The evidence from the review does suggest that incertain groups elective, supplementary PN can reducecomplications and mortality. For well nourishedpatients there is no evidence that pre or post-operative PN support is of benefit but for severelymalnourished GI and thoracic surgical patientspreoperative/perioperative and postoperative PN
there is evidence of benefit. Similarly, although thereis no evidence that perioperative PN is cost-effectivein general (indeed if given to all general surgerypatients there would probably be increased healthservice costs with no health gain), the studies founddo not apply to PN as used in most UK practice andfor elective supplementary perioperative PN is cost-effective in severely malnourished surgical patients.
1100..33.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
1100..33..11 IInnddiiccaattiioonnss ffoorr ppaarreenntteerraall nnuuttrriittiioonn
Healthcare professionals should consider parenteral
nutrition in people who are malnourished44 or at risk
of malnutrition45, respectively, and meet either of thefollowing criteria:
• inadequate or unsafe oral and/or enteralnutritional intake
• a non-functional, inaccessible or perforated(leaking) gastrointestinal tract. [[DD((GGPPPP))]]
44 Malnourished: BMI <18.5 kg/m2, unintentional weight loss >10% within the last 3-6 months, a BMI<20 kg/m2 and unintentional weight loss>5% within the last 3-6 months.45 At risk of malnutrition: eaten little or nothing for more than 5 days and/or likely to eat little or nothing for the next 5 days or longer or poorabsorptive capacity, and or high nutrient losses and or increased nutritional needs from causes such as catabolism.

Parenteral nutrition should be introducedprogressively and closely monitored, usuallystarting at no more than 50% of estimated needsfor the first 24–48 hours. Parenteral nutrition canbe withdrawn once adequate oral or enteralnutrition is tolerated and nutritional status isstable. Withdrawal should be planned andstepwise with a daily review of the patient’sprogress. [[DD((GGPPPP))]]
Parenteral nutrition should be stopped when thepatient is established on adequate oral and/orenteral support. There is no minimum length of timefor the duration of parenteral nutrition. [[DD((GGPPPP))]]
1100..33..22 PPaarreenntteerraall nnuuttrriittiioonn ffoorr ssuurrggiiccaall ppaattiieennttss
Healthcare professionals should considersupplementary peri-operative parenteral nutrition
in malnourished46 surgical patients who have aninadequate or unsafe oral and/or enteralnutritional intake or a non-functional, inaccessibleor perforated (leaking) gastrointestinal tract. [[BB]]
Peri-operative supplementary parenteral nutritionshould not be given to surgical patients unless
they are malnourished46 or at risk of
malnutrition47 and have an inadequate or unsafeoral and/or enteral nutritional intake or a non-functional, inaccessible or perforated (leaking)gastrointestinal tract. [[BB]]
1100..44.. PPaarreenntteerraall vveerrssuuss eenntteerraall ttuubbee ffeeeeddiinngg
1100..44..11.. IInnttrroodduuccttiioonn
As mentioned above, PN is usually reserved forthose who need support but who have either anon-functioning or non-accessible GI tract. Thechoice of PN versus ETF is therefore not an issueand furthermore, there can be no means ofconducting meaningful RCTs to examine thisprimary indication for PN. Nevertheless, manypatients who are severely ill or who haveundergone major surgery are unable for manydays to meet much if any of their nutritionalneeds by mouth. They may therefore benefit fromelective nutrition support given by enteral and/orparenteral routes. In general, ETF is preferredsince it is perceived to be both cheaper and
perhaps erroneously safer than PN. However, insome patients there is debate about whether gutfunction is adequate to permit ETF and in thesecases, RCTs of PN versus ETF are possible.Nevertheless, a literature search identified only
one RCT 376 addressing this point directly (also
included in 2 systematic reviews152,320) and allother studies identified, examined the use of PNin patients whose GI tract was both accessibleand functional to a degree that at least made ETFfeasible. The use of PN in some patients in theseother studies was therefore ‘elective’ since suchpatients would NOT usually receive PN as either asupplementary or sole source of nutrition untilETF had been shown to fail.
1100..44..22.. SSttuuddiieess ccoonnssiiddeerreedd ffoorr tthhiiss rreevviieeww
In addition to the single study of ETF vs. PN in
patients of uncertain GI function376, we identifiedmany RCTs examining elective PN use (Table59,Table 60,Table 61,Table 62,Table 63,Table64,Table 65,Table 66,Table 67,Table 68,Table 69).These included 16
RCTs16,38,41,43,131,136,162,165,239,261,292, 303,313,317,382,383
and 3 systematic reviews152,219,320. The 3systematic reviews and 14 of the
RCTs16,38,41,43,131,136,150,152,162,165,219,292,303,313,317,383
compared patients who received PN alone withpatients on ETF alone(Table 59,Table 60,Table61,Table 62,Table 63,Table 64,Table 65), while 3RCTs compared the effects of PN alone vs. a
combination of PN and ETF239,261,382 (Table
67,Table 68,Table 69). One systematic review 152
(Table 66) compared ETF alone vs. a combinationof ETF and PN.
Studies were grouped into disease populationsand looked at patients with liver disease, Crohn’sdisease, ulcerative colitis, acute pancreatitis,abdominal trauma, bone marrow transplant,cancer, the critically ill and surgical patients.
1100..44..33.. CClliinniiccaall eevviiddeennccee
In the single study that selected patients for ETFor PN on the grounds of likely gastrointestinal
function 376, 237 patients were considered tohave GI function adequate to try enteral tubefeeding, 267 patients were felt to have intestinal
PARENTERAL NUTRITION IN HOSPITAL AND THE COMMUNIT Y 129
46 Malnourished: BMI <18.5 kg/m2, unintentional weight loss >10% within the last 3-6 months, a BMI<20 kg/m2 and unintentional weight loss>5% within the last 3-6 months.47 At risk of malnutrition: eaten little or nothing for more than 5 days and/or likely to eat little or nothing for the next 5 days or longer or poorabsorptive capacity, and or high nutrient losses and or increased nutritional needs from causes such as catabolism.

failure to a degree that required parenteralnutrition, and 64 were considered to havemarginal intestinal failure at a level which madethe decision of whether to use ETF or PNgenuinely equivocal. This last group wastherefore randomised to either ETF or PN support.The study showed that in the elective, nonrandomised ETF and PN groups there was nodifference in septic morbidity but a higher non-septic complication rate in the ETF groupassociated with a significant increase in mortality.A similar higher mortality was also seen in thegroup randomised to ETF within those withquestionable GI function. ETF patient groups,both randomized and selected also hadsignificantly lower nutritional intakes than thosewho were randomized or selected for PN.
The RCTs on elective PN use showed the followingresults in different patient groups.
10.4.3.1 Critically ill patients
Two systematic reviews 152,320 compared theeffects of ETF v PN in the critically ill (Table 65).
Heyland et al. 152 showed a significant reductionin infectious complications for the enteral group.There was no significant difference in mortalitybetween groups. However, the other systematic
review 320 which had a few studies in common
with Heyland et al. 152 concluded that there was agreater risk of mortality in the patients receivingETF although this was only evident in studieswhere initiation of ETF had been delayed.
10.4.3.2 Cancer patients
Many RCTs studied the use of supplementary PNvs. ETF in cancer patients, mostly in the
perioperative period. The six RCTs16,41,43,165,292,303
that we identified were classified into threegroups according to the nutritional status of thepatients included (Table 61).
Two studies 41,43 included GI cancer patientsundergoing elective surgery with a weight loss ≥10% of the usual body weight in the past 6
months. In one of these studies 41, 158 patientsreceived PN whilst 159 received ETF via ajejunostomy catheter or nasojejunal tube. Resultsshowed that overall post-operative complicationswere significantly fewer for patients in the ETF
group (p<0.005) 41. However, in a sub-group ofmalnourished patients analyzed separately within
the second study 43 (48 PN fed patients versus 43ETF patients fed by jejunostomy or nasojejunaltube), no significant differences were observed.Adverse effects of specialised nutrition(abdominal distension, cramps, diarrhoea and
vomiting) were reported in one study41 with theETF group showing a significantly higherincidence (p<0.0001). Both studies reported nosignificant difference in hospital length of stayand mortality.
Three studies included malnourished and non-malnourished GI cancer patients undergoing
surgery16,43,292, although only one 43 provideda definition of malnutrition - involuntaryweight loss > 10% with respect to their usualbody weight in the preceding 6 months).Patients were randomised to receive PN or ETFby jejunostomy catheter.
One study reported the number of patientsachieving their nutritional goal within four days
post-operatively43. There was a significantlygreater number of patients achieving this in the PNgroup than the ETF group (p<0.001). The same
study43 reported time to first flatus and bowelmovement. The first flatus and bowel movementoccurred earlier in the ETF group than the PNgroup (p=0.001). One study reported catheter-related complications and non-catheter related
complications16. For catheter-related complications,there was no significant difference between thegroups. However, the PN group had a significantlygreater number of non-catheter relatedcomplications (p<0.05). These included life-threatening and non-life threatening complications.
Length of hospital stay was reported in one study43
and there was no significant difference betweenthe groups. Mortality was reported in the threestudies and there were no significant differencesbetween the groups.
Two studies were included PN vs. ETF in cancerpatients with exclusion of those who were
severely malnourished 165,303. One study165
included patients undergoing total laryngectomy(n=48). Patients were randomised to receive
NUTRITION SUPPORT IN ADULTS130

PN (n=24) or ETF (n=24) by percutaneousendoscopic gastrostomy.
The ETF group had a significantly shorter hospitallength of stay than the PN group (p< 0.05). Therewere no significant differences between the groupsin wound infections and surgical complications.
The other study303 included patients undergoingcurative total gastrectomy (n= 29). Patients wererandomised to receive PN (n=16) or ETF bynasojejunal tube (n=13). The study did not reportthe patients’ nutritional status.
10.4.3.3 Pancreatitis
A systematic review of studies in patients with
acute pancreatitis219 (Table 59) showed significantreductions in length of hospital stay, infectionsand the need for surgical interventions in the ETFgroup, although in individual studies on this topicit is unclear whether the advantage is due to theroute of enteral tube feeding (nasojejunal) or dueto the PN fed patients receiving high levels ofsupport which made many of the PN fed patientshyperglycaemic.
10.4.3.4 Inflammatory bowel disease
Two studies on patients with Crohn’s disease or
ulcerative colitis 131,136 (Table 64)showed asignificant reduction in post-operative infectionsand complications from nutrition support in theulcerative colitis population only. There were noother significant differences in these studies.
A few studies have reported changes in nitrogenbalance with equivocal findings. A study of
patients undergoing major GI surgery 38
demonstrated significantly higher nitrogenbalance for the ETF group, whereas a study in
patients with abdominal trauma 313 showedsignificantly higher nitrogen balance in the PNgroup. The study reported no significantdifferences in postoperative complications andhospital length of stay.
1100..44..44.. CClliinniiccaall eevviiddeennccee PPNN vveerrssuuss ((PPNN++EETTFF))
Three studies compared the effects of PN versusthe combination of PN and ETF in differentpatient groups. One studying patients with
pancreatitis 382 (Table 67)showed that thosereceiving combined PN and ETF had greater
weight gains compared to those on PN alone. Asimilar study design, in patients having bone
marrow transplantation239 (Table 68) showed thatcombination feeding reduced the days ofdiarrhoea but no other significant differenceswere seen. A study in patients who had
abdominal surgery 261 (Table 69) demonstratedno differences between PN fed and combinationPN and ETF fed patients.
1100..44..55.. CClliinniiccaall eevviiddeennccee EETTFF vveerrssuuss ((PPNN++EETTFF))
The one systematic review152 comparing ETF toPN feeding with simultaneous commencement ofETF in critically ill patients contained data from 5RCTs. No significant differences for any outcomeswere demonstrated but all of the RCTS weresmall, low quality studies.
1100..44..66.. CCoosstt--eeffffeeccttiivveenneessss eevviiddeennccee
As with our other reviews of the use of PN indifferent circumstances, evaluation of cost-effectiveness studies was limited by the fact thatthey do not apply to the usage of PN within UKclinical settings. However, fifteen cost analyseswere found – ten from the USA and one each fromCanada, China, Finland, France and Italy (Table 79and Table 79). One study compared ETF and PNwith ETF and placebo and the rest compared totalPN with ETF. The studies varied in terms of bothsetting and patient group: post-operative (10),acute pancreatitis (2), home (1), ICU (2). Therewere also varied study designs: RCT (10),retrospective cohort (4), meta-analysis (1). A majorproblem was that ten studies only included thecost of nutrition therapy and support, with only fivestudies including the costs of treatingcomplications or extended hospitalisation. It isdoubtful if even these included all the costs. Directcomparison of the cost savings was alsocomplicated by the studies reporting in differentcurrencies, in different years, in different healthcaresystems and varied techniques were used toprovide ETF. Nevertheless, it is very likely that ETFis cheaper than PN and Table 23 indicates therelative size of the hospital cost savings.
PARENTERAL NUTRITION IN HOSPITAL AND THE COMMUNIT Y 131

1100..44..77.. CCoonncclluussiioonnss
Once again evidence from the enteral versusparenteral review is difficult to interpret since theuse of PN in the majority of patients included inthe trials was out of line with routine UK clinical
practice. In the one study that is relevant 376, PNin expert hands was found to be as safe andprobably safer than ETF, especially in patientswith gastrointestinal function that is so marginalthat the likelihood of tolerating ETF is uncertain(PN fed patients in this group had lower mortalityand achieved higher feeding rates with lower non-septic complication rates than ETF patients).
The other studies, examining the ‘elective’ use ofPN in circumstances when it was not absolutelynecessary, are much less relevant but the findingsdo support current UK thinking. PN provides nosignificant advantages when ETF can be used andETF patients tend to do better for outcomes suchas weight gain, length of stay and infections.There are no definite advantages of combinationsof feeding although studies are too small andunderpowered to make firm conclusions.However, working from first principles, the GDGfelt that the use of combination feeding makessense. The arrival of nutrients in the GI tract islikely to stimulate GI function and immunity andwill probably provide useful metabolic signallingto help with liver processing of nutrients. The GI
tract should therefore be used to supply as muchof the patient’s nutrient needs tolerance andfunction allows, with PN used if necessary toprovide the remainder.
The cost-effectiveness evidence varied withmethods and reporting but also support thewidely recognized notion that ETF is a cheaperoption. However, the use of PN in the costeffectiveness trails was not in line with the use inmost current UK practice.
1100..55.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
1100..55..11 PPaarreenntteerraall nnuuttrriittiioonn ffoorr ssuurrggiiccaall oorr ccrriittiiccaall ccaarree ppaattiieennttss
If intestinal tolerance persistently limits enteraltube feeding in surgical or critical care patients,parenteral nutrition should be used tosupplement or replace enteral tube feeding. [[BB]]
1100..66.. VVeennoouuss aacccceessss ffoorr PPNN
1100..66..11.. IInnttrroodduuccttiioonn
All PN admixtures should be administered viadedicated intravenous catheters, throughelectronic volumetric pumps/controllers withocclusion and air in line alarms. Someauthorities strongly endorse and recommend 1.2
NUTRITION SUPPORT IN ADULTS132
Study Year Country Patient group Reduction in cost p-value
McClave 1997 USA Pancreatitis 76.9% 0.001
Sand 1997 Finland GI surgery (cancer) 76.5% N/R
Bower 1986 USA GI surgery 73.6% 0.001
Braga 2001 Italy GI surgery (cancer) 72.5% N/R
Adams 1986 USA Laparotomy (trauma) 63.9% N/R
Trice 1997 USA Surgery (trauma) 62.9% N/R
Hamaoui 1990 USA Abdominal surgery 56.9% 0.001
Bauer 2000 France ICU (not surgery) 48.0% 0.0001
Barzotti 1994 USA Head injury 46.4% N/R
Abou-Assi 2002 USA Pancreatitis 23.4% 0.0004
Zhu 2003 China GI surgery (cancer) 11.8% <0.05
N/R=not reported
TTaabbllee 2233:: CCoosstt ssaavviinnggss aattttrriibbuuttaabbllee ttoo eenntteerraall ttuubbee ffeeeeddiinngg ccoommppaarreedd wwiitthh ppaarreenntteerraall nnuuttrriittiioonn ((RRCCTT eevviiddeennccee))

micron filtration of PN admixtures containing afat emulsion, and 0.2 micron filtration of otherPN admixtures for long term patients and thosewith complex PN formulations. This issue wasreviewed by the GDG but no papers wherefound which met the necessary criteria forreview. Venous catheters for PN can be eitherperipherally or centrally inserted and GDG didinvestigate whether there are advantages of oneroute over the other. The decision tocommence PN is never an emergency. Catheterinsertion should be planned and performedusing optimum aseptic precautions. Whenconsidering the need for intravenous access, themost appropriate site should be obtained byassessing the risk of infection against the risk of
mechanical complications80.
1100..66..22 PPeerriipphheerraall aacccceessss
Full intravenous feeding using low osmolality fatemulsion based feeds can be given via aperipherally placed small catheter (22 – 23 Fr)with 48 hourly change of catheter site. However,fine bore, mid length catheters insertedperipherally but running up into larger veins, orperipherally inserted central catheters are morecommonly used. All are alternatives to subclavian
and jugular venous catheter placement80.Catheters can be put in on the ward but onlywhen using a strict aseptic technique withadequate skin preparation e.g. 0.5%chlorhexidine in 70% methylated spirits), sterilefield, and sterile gloves.
1100..66..33 IInnddiiccaattiioonnss ffoorr iinnsseerrttiioonn ooff cceennttrraall vveennoouuss ((CCVV)) lliinneess
Central venous access The insertion of CV lines for PN is associated withgreater risks than peripheral feeding lines andshould therefore be undertaken by experiencedpersonnel, where other access is not available orfeasible, or where multiple lumen CV lines areneeded as part of the patient’s clinicalmanagement. Where multiple lumen CV lines areused a lumen should be dedicated for the use ofPN only. CV lines need to be considered inpatients with no peripheral access and in thoserequiring some specialised feeds. Indications for
CV lines include:• Patients identified as likely to require PN for a
period of more than 2 weeks
• Patients already having suitable central venousaccess with a lumen which can be used solelyfor feeding (e.g. post-op from theatre)
• Patients with no suitable veins for peripheralfeeding
• Patients requiring specialised PN feeds thatcannot be given into smaller peripheral veins(e.g. hypertonic feeds (>1300-1500 mosmol/lsuch as fat free or restricted volume solutions).
All central venous access devices should beinserted in optimum sterile conditions, using fullaseptic conditions including sterile drapes, gown
and gloves80.
1100..66..44.. MMeetthhooddoollooggyy
We conducted three reviews that looked at theeffect of delivering PN via different venous lines:
• peripherally-inserted central catheters versusstandard central venous catheters
• central versus peripheral venous catheterstunnelled versus non-tunnelled venous catheters
1100..66..55 PPeerriipphheerraallllyy-- iinnsseerrtteedd cceennttrraall ccaatthheetteerrss ((PPIICCCC))vveerrssuuss ssttaannddaarrdd cceennttrraall vveennoouuss ccaatthheetteerrss ((CCVVCC))
10.6.5.1 Introduction
PN solutions can be very hypertonic and somespecialised formulations can only be infused intoveins with high blood flow such as the superiorvena cava. Central venous catheters (CVC) insertedinto subclavian veins are commonly used for PNdelivery but traumatic insertion problems arecommon and, as with all central lines, there are risks
of sepsis and thrombosis135. Peripherally insertedcentral venous catheters (PICCs) can be used as analternative to central venous catheterisation. PICCsare inserted into the basilic or cephalic veins andthe tip is advanced into the superior vena cava. Ithas been suggested that the potential benefits ofPICCs might include the reduction of complications(it has been suggested that PICCs are associatedwith a lower rate of infection compared with other
non-tunnelled CVCs80) and perhaps cost savings, asPICCs can be inserted by non-physicians.
PARENTERAL NUTRITION IN HOSPITAL AND THE COMMUNIT Y 133
A review was therefore conducted to identifystudies which compared the efficacy of PNdelivered through PICCs compared to CVCs. We
identified only one RCT71 (Table 70).
10.6.5.2 Study considered for this review
The RCT included 102 hospitalised adult patientswho required PN. The patients were all GI sufferingfrom pancreatitis, post-operative ileus and primaryabdominal malignancy among other diseases. Fifty-one patients were randomised to receive PN througha PICC (catheters were inserted into the basilic veinin most cases, other vessels used were the cephalicand median antecubital veins), while fifty-one hadPN via a CVC (subclavian vein).
10.6.5.3 Clinical evidence
The use of both access techniques was oftensuccessful. The main outcome reported was thecompletion of therapy without complication. TheCVC group had significantly higher percentage ofpatients that completed the therapy withoutcomplication than the PICC group (p<0.05). PICClines were associated with greater number ofdifficult insertion attempts (required more thantwo but less than five needle sticks) (p<0.05),clinically-evident thrombophlebitis (p<0.01) andmal-position on insertion (p<0.05). There weresignificantly higher incidence of falsely suspectedline infection in the CVC group (p<0.05). Nosignificant difference was noted between the twogroups in aborted insertion attempts, insertiontime, pneumothorax, line occlusion, catheterinfection, dislodgement or mortality.
10.6.5.4 Cost-effectiveness evidence
A US study71 compared the cost of CVC with thecost of PICC. It included hospital costs forinserting catheters and costs of diagnosing andtreating complications arising from catheterinsertion. It was expected that PICCs would havelower hospital costs, because nurses can insertthem. However, the results of the analysisshowed that PICCs were more costly by £39 perpatient because PICC insertion and maintenancewas more difficult and associated with higherrates of thrombophlebitis.
10.6.5.5 Conclusion
Findings from this study suggest that PICCs areassociated with higher incidence of placementand mechanical complications than CVCs butnevertheless, their use is often successful. Therelative costs of PICCs versus CVCs depends uponinsertion success rates and rates of linecomplications. Studies were limited becausechanges in health status or quality of life werenot measured or reported and results may not betransferable to specific patient subgroups.
1100..77.. RReeccoommmmeennddaattiioonn ffoorr cclliinniiccaall pprraaccttiiccee
1100..77..11 RRoouuttee ooff aacccceessss
In hospital, parenteral nutrition can be given via adedicated peripherally inserted central catheter as analternative to a dedicated centrally placed centralvenous catheter. A free dedicated lumen in a multi-lumen centrally placed catheter may also be used. [[BB]]
1100..88.. PPeerriipphheerraall PPNN vveerrssuuss cceennttrraall PPNN
1100..88..11.. IInnttrroodduuccttiioonn
Many PN admixtures are very hypertonic and canonly be administered into veins with high bloodflow (central veins) since peripheral vein infusion islikely to result in thrombophlebitis, characterised byredness, a severe burning sensation and rapid
thrombosis135. However, there are alsocomplications associated with central venous PNparticularly catheter insertion trauma, sepsis andthrombosis. An alternative to central PN is theinfusion of peripheral parenteral nutrition using afine-bore silicone catheter delivery system. Fatemulsion containing admixtures are often used inperipheral parenteral nutrition as these generallyare not as hypertonic as admixtures using glucosealone as an energy source. Similarly fat emulsionbased admixtures may have a pH better toleratedby small vessels. Additions of concentratedelectrolytes can increase the tonicity and affect thepH of PN admixtures, careful attention toformulation is required for successful peripheralparenteral nutrition. Peripheral delivery systemsmay avoid some of the complications associated
NUTRITION SUPPORT IN ADULTS134

with central venous catheterisation and the factthat they are easier to place may provide overall
cost savings189.
A review was conducted to assess the potentialbenefits of peripheral PN compared with central
PN. The review identified three RCTs70,189,221
(Table 71).
1100..88..22 SSttuuddiieess ccoonnssiiddeerreedd ffoorr tthhiiss rreevviieeww
One study189 included adult surgical inpatientsrequiring PN. These were GI patients whounderwent pancreatic, oesophageal and gastricsurgery among other procedures. Patients whoreceived PN in the intensive care unit and thosewho required multiple-lumen venous access wereexcluded. This exclusion affects a considerablenumber of potential PN patients.
Patients were randomised to receive peripheral PN(n= 23) or central PN (n=23). Patients allocatedto receive peripheral PN were given a fatemulsion containing PN admixture through apaediatric fine-bore silicone catheter inserted intothe deep median basilic vein. The catheters werenot tunnelled subcutaneously or sutured to theskin for fixation. Patients allocated to receivecentral PN were given a glucose-based PNadmixture through a single-lumen siliconecatheter inserted into the subclavian vein.
The other two studies70,221 includedgastroenterological patients requiring PN. The totalnumber of patients included in these studies was91: 42 received peripheral PN and 49 receivedcentral PN infused into the superior vena cava.
1100..88..33 CClliinniiccaall eevviiddeennccee
In one study189, the patients allocated to receiveperipheral PN had higher total patient treatmentdays (426 d compared to 322), spontaneouscatheter retraction (3 cases vs. no cases in thecentral group) and cases of non-infectivethrombophlebitis (4 vs. no cases). Patientsallocated to receive central PN had higherinsertion-site infection (2 vs. 1), problems withvenous access (1 vs. 0) and catheter-relatedbacteraemia (3 vs. 0); however only one of thethree cases of bacteraemia was thought to be dueto a primary catheter infection. The main outcome
reported was probability of a complication-freesystem function with time. There was nosignificant difference in the risk of overallcomplication. The incidence density ofcomplication ratio was 0.66 (95% confidenceinterval 0.24-1.82).
Another study70 reported no significantdifferences between the groups regarding medianduration of feeding. However, morbidity occurredmore frequently in the group of patients allocatedto receive PN (one catheter related sepsis and twopneumothoraces) than in the group allocated toreceive peripheral PN (severe phlebitis was notencountered).
In the other study221 21 out of the 26 patients(80%) allocated to receive central PN completedtheir course of PN compared with 13 out of the23 of the patients (56%) who received peripheralPN. Four patients who received peripheral PNwere immediate failures because inadequateforearm veins and six were converted to centralfeeding as peripheral access became difficult.There were six line fevers (23%) and twopneumothoraces (7%) in the group of patientsallocated to receive central PN (n=26) comparedwith 3 line fevers (13%) in the group of patientswho received peripheral PN (n=23).
1100..88..44 CCoosstt eeffffeeccttiivveenneessss eevviiddeennccee
A UK study221 compared the cost of central PNwith the cost of peripheral PN. Their analysis wasbased on a prospective trial. The study group wasall hospitalised patients who required PN. PNdelivered peripherally was found to be cost-savingby £125 per patient compared with using thecentral route. This was because peripheral PNhad a lower cost associated with insertion andfewer complications.
1100..88..55 CCoonncclluussiioonn
The studies reviewed were limited by their smallsample size and because changes in health statusor quality of life were not measured or reported.The overall results from this analysis suggest thatthere is little significant difference in the risk ofcomplication between peripheral and central PNand only marginal savings in cost, with theanalysis dependent on assumptions regarding
PARENTERAL NUTRITION IN HOSPITAL AND THE COMMUNIT Y 135

successful insertion and rates of linecomplications. The formulation of the PN, inparticular its volume, the use of fat emulsions andhypertonic concentrated electrolytes, will make amajor difference to the complication rates andlength of feeding achieved via the peripheralroute, but it has not been possible to ascertainthese factors from these studies. Similarly the useof drug therapy might ameliorate thethrombophlebitic complications and thombosis,but their inclusion may detrimentally affect thestability of the PN admixtures used and wouldadd to cost. The results may not be generalisableto specific patient subgroups.
1100..88..66.. RReeccoommmmeennddaattiioonn ffoorr cclliinniiccaall pprraaccttiiccee
10.8.6.1 Route of access
Administration of parenteral nutrition via aperipheral venous catheter should be consideredfor patients who are likely to need short-termparenteral nutrition (less than 14 days) who haveno need for central access for other reasons. Careshould be taken in catheter choice, and inattention to pH, tonicity and long-termcompatibility of the parenteral nutritionformulations in order to avoid administration orstability problems. [[BB]]
1100..99.. PPNN vviiaa aa ttuunnnneelllleedd ccaatthheetteerr vveerrssuuss PPNN vviiaa aa nnoonn--ttuunnnneelllleedd ccaatthheetteerr
1100..99..11.. IInnttrroodduuccttiioonn
A practice used widely in the 1980s to potentiallyreduce the risk of central catheter relatedinfection was the use of tunnelled catheters.These catheters are inserted through the skin andadvanced subcutaneously before the tip isinserted into the vein. It has been suggested thatthis technique reduces the risk of infection byincreasing the distance between the potentiallycontaminated skin entry site and the venous entry
site284. A tunnelled catheter also grants practicaladvantage to ambulant patients in that theyallow easier dressing of the catheter entry siteand provide more stability, reducing the risk of
dislodgement120.
1100..99..22.. SSttuuddiieess ccoonnssiiddeerreedd ffoorr tthhiiss rreevviieeww
A review was conducted to assess the benefits ofPN through tunnelled catheters compared to non-tunnelled catheters (Table 72). One systematicreview was identified that looked at the efficacyof tunnelling short-term central venous cathetersto prevent catheter-related infections. While theinclusion criteria for this review were RCTs onadult or paediatric patients with catheters inplace for an average of <30 days, only studiesinvestigating adults were found. Catheters wereplaced using a subcutaneous tunnel. The review
identified seven RCTs on adult patients74,78,120,
138,183,230,351 but two 74,351 were excluded from ouranalysis since the catheters were not placed forPN. Five studies were therefore included in tourassessment. The population of these studies
were: surgical (n=150230 and n=38120), medical
and surgical (n=83183) and cancer patients
(n=74138 and n=10978). In all the studiescatheters were inserted into the subclavian vein.
The systematic review extracted data from eachstudy for three outcomes: catheter colonisation,clinical sepsis and catheter-related bacteraemia.These data were used in the review (excludingdata from the two studies mentioned above) toconduct a meta-analysis for these three outcomes.
1100..99..33.. CClliinniiccaall eevviiddeennccee
Catheter colonisationFour studies reported catheter
colonisation78,138,183,230. The pooled effectshowed that tunnelling decreases the risk ofinfection (relative risk 0.46; 95% confidenceinterval 0.26- 0.80).
Four studies reported catheter related
sepsis78,120,138,230. The overall result showed nosignificant difference between the groups (relativerisk 0.63; 95% confidence interval 0.29-1.38).
Clinical sepsis
Two studies reported clinical sepsis120,230. Theoverall result showed no significant differencebetween the groups (relative risk 1.25; 95%confidence interval 0.63-2.48).
NUTRITION SUPPORT IN ADULTS136

1100..99..44.. CCoonncclluussiioonn
Results from this analysis indicate that tunnelledcatheters reduce the risk of catheter colonisationcompared with non-tunnelled catheters. However,there are no significant differences in the risk ofcatheter related septicaemia and catheter sepsis.In long-term catheter use the tunnelling of ashort segment of line with a cuff that allowsfibrosis to occur avoids external fixation andimproves comfort.
1100..99..55 RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
10.9.5.1 Route of access
Tunnelling subclavian lines is recommended forlong-term use (more than 30 days). [[DD((GGPPPP))]]
Catheters do not have to be tunnelled for short-term use (less than 30 days). [[BB]]
1100..1100.. TTaaiilloorreedd PPNN pprreeppaarraattiioonnss vveerrssuuss ssttaannddaarrdd PPNN pprreeppaarraattiioonnss
1100..1100..11.. IInnttrroodduuccttiioonn
Patients requiring PN can either receive astandardised fixed feeding regimen, or a PN regimencompounded to meet individual nutritional,electrolyte and fluid requirements. Both methodsshould always have the addition of vitamins andtrace elements and standardised PN may also needthe addition of electrolytes and other nutrients toensure it is complete and appropriate. Additionsmust be made under controlled pharmaceuticalconditions and not at ward level. The stability ofeither means of providing PN needs to be known toavoid serious complications resulting from unstablePN formulations. One of the disadvantages of fixedregimens is that in order to achieve an adequateamino acid intake, patients may receive calories inexcess of their requirements or metabolic capacity(excess energy intake may worsen respiratorydifficulties and may lead to hyperglycaemia).Furthermore, standardised PN may not always beappropriate for patients with special prescriptionneeds such as the critically ill, those with organfailure, or those who have high electrolyte losses.
1100..1100..22.. SSttuuddiieess iinncclluuddeedd iinn tthhiiss rreevviieeww
A review was performed to assess the efficacy oftailored (individualised) PN preparations
compared with standard preparations (Table 73).
Only one real RCT was identified293. The studyincluded twenty hospital inpatients requiring PNafter abdominal surgery. The mean age ofpatients was 46 (3 patients where under 18: two17 and one 15 years old). Patients wererandomised to receive either a constant regimencontaining 2600 calories per day and 15.55gNitrogen per day (n=10) or a varied regimen withfixed calorie: Nitrogen ratio of 167:1 but with thecalorie intake adjusted according to the previousdays metabolic expenditure (n=10).
1100..1100..33 CClliinniiccaall eevviiddeennccee
The study reported calorie and nitrogen intake,respiratory quotient, production of CO2, body fat
and body mass change. There were no significantdifferences in any of the outcomes.
1100..1100..44 CCoosstt--eeffffeeccttiivveenneessss eevviiddeennccee
No studies were found that estimated theincremental cost or cost-effectiveness of standardvs. tailored PN.
1100..1100..55.. CCoonncclluussiioonn
Findings from the included study suggest that thereare no differences in outcome from either form ofPN. However, the study is nowhere near largeenough to identify possible clinical advantages ofone or other approach, or to assist in identifyingwhich patient groups are suitable for standardisedas opposed to individualised PN regimens.
1100..1111.. RReeccoommmmeennddaattiioonn ffoorr cclliinniiccaall pprraaccttiiccee
PPrreessccrriippttiioonn
Patients prescribed standardised PN should havetheir nutritional requirements determined byhealthcare professionals with the relevant skillsand training in the prescription of nutritionsupport before selection of a particular parenteralnutrition product. The addition of vitamins andtrace elements is always required and occasionallythe addition of electrolytes or other nutrientsupplements is also needed. Additions must bemade under appropriate pharmaceuticallycontrolled environmental conditions beforeadministration. [[DD ((GGPPPP))]]
PARENTERAL NUTRITION IN HOSPITAL AND THE COMMUNIT Y 137

1100..1122.. DDeelliivveerryy ooff PPNN ccyycclliiccaallllyy vveerrssuuss ccoonnttiinnuuoouussllyy
1100..1122..11.. IInnttrroodduuccttiioonn
PN can be administered as continuous infusion(24 h) or cyclically (intermittently over shorterperiods e.g.10-18 hours). For patients on longterm PN cyclical administration allows patientsperiods of free movement, periods when the lineis available for other therapeutic purposes, andpotential metabolic benefits (a period of ‘rest’ forprocessing and assimilating nutrients). However,controversy persists as to the optimal method ofPN administration and a review was thereforeconducted to compare PN given cyclically with PNgiven continuously.
1100..1122..22.. SSttuuddiieess ccoonnssiiddeerreedd ffoorr tthhiiss rreevviieeww
The review conducted identified six RCTs7,115,184,220,264,305 (Table 74).
1100..1122..33.. CClliinniiccaall eevviiddeennccee
In three studies patients received peripheral PN
only184,220,264. The main outcome reported wasincidence of infusion phlebitis. The populationincluded in these studies were patients requiringPN excluding those in whom central venouscatheterisation was necessary. Continuous PNwas delivered as a constant 24 h infusion and cyclic PN as a 12 h infusion with a 12 h break (Table 74).
In one study184, patients on cyclical PN hadsignificantly lower Daily Madox Score (Criteriaused for assessing phlebitis. There are 6 scorelevels from 0 mild phlebitis to 5 severe phlebitis)(p< 0.001-0.05) and incidence of severe phlebitis(p<0.05) compared to patients on continuous PNwith or without elective cannula change. In
another study220, patients on cyclical PN withelective cannula change had significant lowerphlebitis score compared to patients on cyclicalPN with cannulas left in situ (p<0.05) andpatients on continuous PN with fine-bore catheterleft in situ (p<0.01). The same study showedsignificantly lower phlebitis score with 18 GTeflon cannulas (4-5 cm) comparing with 18-GSilastic (15 cm) cannulas in patients on cyclicalPN when cannulas were left in situ (p<0.05).
Another RCT264 reported significantly lowerincidence of PN failures in patients on cyclical PNgroup with elective change of 18G Tefloncannulas compared with patients on continuousPN group with 23G Teflon cannulas (15 cm) leftin situ (p<0.05). The same study recordedpatients’ signs of anxiety and depression. Therewere no significant differences between thegroups for these two outcomes.
The other three studies included patientsreceiving central venous PN (one study did notreport the infusion site) in post bone marrow
transplant patients7, traumatised or infected
patients on mechanical ventilation115 and post
major surgery patients305. Continuous PN wasadministered as a constant 24 hour infusion in allthree studies but there were variations in the
cyclic PN regimens. In one study7 the patients
received 12 hour cyclical infusions, in another115
patients were infused PN for 12 hours and lowenergy glucose for the following 12 hours, and in
the third study 305 patients received bolus PNinfusions for 1 hour followed by 2 hours withoutinfusion for 12 hours.
The outcomes reported were also varied andincluded both clinical and metabolic parameters.
The study in bone marrow transplant patients7
showed no significant differences in duration ofPN, energy provided, plasma level of glucose andproteins, neutropenia time, change of weight ,hepatic parameters, use of haematopoietic growthfactors, incidence of hepatic veno-occlusivedisease, incidence of catheter infection, or post-transplantation length of stay. The study ontrauma or infected patients on mechanical
ventilation115 showed no differences in clinicalparameters including length of artificialventilation, length of stay in ICU and in hospitalmortality , but patients in the cyclic group hadstatistically significant higher: energy expenditure(p< 0.05), O2 uptake (p< 0.05), CO2 elimination
(p< 0.05), and nutrient induced thermogenesis(p< 0.05). They also had lower positive energybalance (p< 0.05) and hence the authorsconcluded that continuous PN resulted in a moreefficient utilisation of nutrients.
NUTRITION SUPPORT IN ADULTS138

The study on major surgery patients 305 also showedslight metabolic advantages from continuous PNadministration in terms of less negative “minimum”nitrogen balance (p< 0.01) and higher “maximum”nitrogen balance (p< 0.05).
1100..1122..44.. CCoonncclluussiioonnss
The three studies comparing patients receivingperipheral PN continuously with those receivingperipheral PN cyclically showed that patients in thecyclical PN group with elective cannula change hadlower rates of phlebitis compared with thecontinuous PN group but this may well reflectcatheter management rather than PNadministration times. The three studies ofcontinuous versus cyclical centrally administered PNshow that continuous PN leads to better nutrientbalance than cyclical administration. None of thestudies apply to longer term PN when cyclicaladministration becomes very important to helpmaintain patients’ free movement and quality oflife. There may also be metabolic advantages forlonger term patients to have nutrient free ‘breaks’.
1100..1133.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
MMooddee ooff ddeelliivveerryy
Continuous administration of parenteral nutritionshould be offered as the preferred method ofinfusion in severely ill people who requireparenteral nutrition. [[BB]]
Cyclical delivery of parenteral nutrition should beconsidered when using peripheral venous cannulaewith planned routine catheter change. [[BB]]
A gradual change from continuous to cyclicaldelivery should be considered in patients requiringparenteral nutrition for more than 2 weeks. [[DD((GGPPPP))]]
1100..1144.. CCoommpplliiccaattiioonnss ffrroomm PPNN
1100..1144..11.. IInnttrroodduuccttiioonn
The use of PN in inexperienced hands isassociated with a number of potential risks. Noformal literature reviews on these problems wereundertaken but nevertheless, the GDG felt thatbrief recommendations based on expert opinionand previous published recommendations e.g.
NICE Guidelines on Infection243 and The
Department of Health80 could be made.
1100..1144..22 CCoommpplliiccaattiioonnss rreellaatteedd ttoo iinnttrraavveennoouuss aacccceessss
Establishing and maintaining the intravenouscatheters needed for PN support can lead to:
Trauma on central line placement e.g. carotidpuncture, pneomothorax
Thrombophlebitis (particularly with peripheralvenous access)
Catheter occlusion and thromboembolism(including serious pulmonary embolism)
Air embolism
Catheter related sepsis
All the above can be reduced if lines for PN usageare inserted by suitably trained and experiencedpersonnel using full aseptic technique. Allcatheters used for PN should then be monitored(see Chapter 6) and cared for by suitably trainedand experienced individuals (see Chapter 10). AllPN admixtures should be administered viadedicated intravenous catheters, throughelectronic volumetric pumps/controllers withocclusion and air in line alarms. Risks fromcatheter related sepsis can be reduced if allcatheter and changes of PN bags are made usingstrict aseptic techniques (see NICE Guidelines on
Infection control243). Hospitals should audit theirrates of PN catheter related complications,especially catheter related sepsis.
1100..1144..33.. MMeettaabboolliicc aanndd fflluuiidd rreellaatteedd ccoommpplliiccaattiioonnss
PN overrides many homeostatic mechanisms andpresents a large osmolar load to the circulation.Rapid and serious derangement of biochemistrycan therefore occur including the re-feedingsyndrome (see Section 6.6). Hyperglycaemia,especially if a patient is diabetic or has stressinduced insulin resistance is common and shouldgenerally be treated with insulin using a slidingscale. PN can also cause liver dysfunctionalthough this is relatively uncommon andabnormalities seen in PN fed patients are morefrequently due to other factors such as the
PARENTERAL NUTRITION IN HOSPITAL AND THE COMMUNIT Y 139

presence of sepsis or side effects from otherdrugs. In view of the above, all PN fed patientsshould be monitored closely (see Chapter 7)
PN usage inevitably contributes a significant fluidload and it is essential that fluid balance ismonitored careful in all patients receiving PN (seeChapter 7) with careful allowance for fluid fromall other sources e.g. oral, ETF, and otherintravenous fluids and/or intravenous drugs.
1100..1155.. RReeccoommmmeennddaattiioonn ffoorr cclliinniiccaall pprraaccttiiccee
MMaannaaggeemmeenntt ooff ccaatthheetteerrss
Only healthcare professionals competent incatheter placement should be responsible for theplacement of catheters and they should be awareof the importance of monitoring and managing
these safely48. [[DD((GGPPPP))]]
1100..1166.. RReesseeaarrcchh rreeccoommmmeennddaattiioonnss
WWhhaatt aarree tthhee bbeenneeffiittss ttoo ppaattiieennttss wwhhoo nneeeedd sshhoorrtt--tteerrmm PPNN ssuuppppoorrtt bbeeiinngg ooffffeerreedd ssttaannddaarrdd PPNNccoommppaarreedd ttoo eeiitthheerr PPNN aanndd mmiinniimmaall EETTFF ((<<2255mmll//hhrr))oorr PPNN wwiitthh GGlluuttaammiinnee aanndd mmiinniimmaall EETTFF ((<<2255mmll//hhrr))iinn tteerrmmss ooff ssuurrvviivvaall,, ccoommpplliiccaattiioonnss aanndd hhoossppiittaall ccoossttss??
This is an area of untested yet advocated practiceand requires a number or a large randomisedcontrol trial.
WWhhaatt aarree tthhee bbeenneeffiittss ttoo ppaattiieennttss wwhhoo pprreesseennttwwiitthh tthhee iinnddiiccaattiioonnss ffoorr PPNN bbeeiinngg ffeedd oonnllyy 5500%% ooffeessttiimmaatteedd pprrootteeiinn aanndd eenneerrggyy nneeeeddss bbuutt wwiitthh ffuullllmmiiccrroonnuuttrriieenntt aanndd eelleeccttrroollyyttee pprroovviissiioonn ffoorr ffiirrsstt 55ddaayyss,, ffoolllloowweedd bbyy ffeeeeddiinngg aatt ffuullll nneeeeddss ccoommppaarreeddttoo bbeeiinngg ffeedd 110000%% ooff eessttiimmaatteedd nneeeeddss ffrroomm tthheeffiirrsstt ddaayy ooff ffeeeeddiinngg iinn tteerrmmss ooff;; mmeettaabboolliiccccoommpplliiccaattiioonnss,, iinnffeeccttiioonn rraatteess,, lleennggtthh ooff PPNNffeeeeddiinngg,, mmoorrttaalliittyy,, lleennggtthh ooff hhoossppiittaall ssttaayy,, aannddttiimmee ttoo ‘‘mmeeddiiccaallllyy ffiitt ffoorr ddiisscchhaarrggee..
In the absence of evidence on the managementof feeding very sick people with marked metabolicdisturbance research in this area is essential tosupport/refute concerns about early feeding insick people.
WWhhaatt aarree tthhee bbeenneeffiittss ttoo ppaattiieennttss wwhhoo hhaavveeiinnddiiccaattiioonnss ffoorr PPNN dduuee ttoo aaccuuttee bbuutt rreevveerrssiibblleeiinntteessttiinnaall ffaaiilluurree ((ee..gg.. pprroolloonnggeedd iilleeuuss)) bbeeiinnggccoommmmeenncceedd oonn PPNN wwiitthhiinn 66 ddaayyss ooff ddeevveellooppiinnggtthhaatt ffaaiilluurree ccoommppaarreedd ttoo nnoott ccoommmmeenncciinngg uunnttiill1122 ddaayyss aafftteerr tthhee ddeevveellooppmmeenntt ooff tthhaatt ffaaiilluurree iifftthhee ffeeeeddiinngg pprroobblleemm hhaass nnoott rreessoollvveedd iinn tteerrmmss ooff;;mmeettaabboolliicc ccoommpplliiccaattiioonnss,, iinnffeeccttiioonn rraatteess,, dduurraattiioonnooff PPNN ffeeeeddiinngg,, mmoorrttaalliittyy,, dduurraattiioonn ooff hhoossppiittaall ssttaayy,,ttiimmee ttoo ‘‘mmeeddiiccaallllyy ffiitt ffoorr ddiisscchhaarrggee..
A randomised control trial is required to furthersupport the rationale for the timings proposed inthe PN nutrition support recommendations.
WWhhaatt aarree tthhee bbeenneeffiittss ttoo IInntteennssiivvee ccaarree ppaattiieennttsslliikkeellyy ttoo ssttaayy ffoorr >>55 ddaayyss wwhhoo hhaavveeccoonnttrraaiinnddiiccaattiioonnss ttoo EETTFF bbeeiinngg ooffffeerreedd ssttaannddaarrddPPNN ccoommppaarreedd ttoo eeiitthheerr PPNN wwiitthh aaddddiittiioonnaallgglluuttaammiinnee,, PPNN wwiitthh aaddddiittiioonnaall sseelleenniiuumm,, oorr PPNNwwiitthh aaddddiittiioonnaall gglluuttaammiinnee aanndd sseelleenniiuumm iinn tteerrmmssooff ssuurrvviivvaall,, ccoommpplliiccaattiioonnss iinncclluuddiinngg ccaatthheetteerrrreellaatteedd iinnffeeccttiioonnss aanndd hhoossppiittaall ccoossttss??
Although the use of novel substrates such asglutamine were not included in the scope of thisguideline the GDG believed that over the last 10years, two important nutritional observations fromclinical trials are the improved survival andreduced infection rates of ICU patientsadministered these novel substrates via parenteralnutrition. However further RCT’s are required toconfirm this and furthermore the benefits of novelsubstrates should perhaps be addressed when thisguideline is updated.
NUTRITION SUPPORT IN ADULTS140
48 Infection control: prevention of healthcare – associated infection in primary and community care. NICE clinical guideline No.2 (2003).Available from www.nice.org.uk/CG002

1111..11 HHoommee eenntteerraall ttuubbee ffeeeeddiinngg
1111..11..11.. IInnttrroodduuccttiioonn aanndd pprreevvaalleennccee
Long term home enteral tube feeding (HETF) isusually required in patients who are unlikely to beable to eat and drink adequately for an indefiniteperiod. The commonest reasons for prolongedfailure of oral intake are dysphagia caused byneurological problems (e.g. CVA, MND, MS) orpartial intestinal failure that either prevents enoughfrom being eaten or limits its absorption. Anorexiawhich can also cause prolonged failure of oralintake is a very uncommon indication for HETF.
In 2003 there were 16,890 adult HETF patientsregistered via the British Artificial Nutrition Surveywith point prevalence of 359/million adult
population in England and 386/million in Wales172.This may be an underestimate since significantnumbers of patients may not be registered. Theindication for HETF was swallowing disorder in 70%of cases, more than two-thirds of which related toneurological problems especially CVA.
1111..11..22.. OOrrggaanniissaattiioonn ooff hhoommee eenntteerraall ttuubbee ffeeeeddiinngg
Patients requiring HETF will normally have enteralaccess and their ETF regimen established inhospital from where they will be dischargedhome. In most cases, gastrostomy or jejunostomytube feeding is used for convenience althoughsome prefer to self-intubate with an NG tube eachtime they need to feed or have long term NGtubes. The organisation required to successfullydischarge and establish a patient on HETF needsa multidisciplinary team approach usuallyinvolving a doctor, ward nurse, dietitian, nutritionnurse specialist, community nurse, speech andlanguage therapist, GP, . home care company
nurses and other allied healthcare professionalsare also involved in many cases according to localpolicy and patient choice.
All patients should receive pre-discharge educationon the management of their feeding regimen whichwould include self monitoring of their enteralfeeding tube and how to deal with problems thatmight occur. Any community staff who are involvedin the care of the patient after discharge should alsoreceive appropriate training. Patients will also requirethe organisation of supplies of feeds and ancillariesand regular support and monitoring.
1111..11..33.. MMeetthhooddss
No specific reviews were undertaken for HETFalthough we did identify information on patient’sperspectives about this aspect of care (section 11.5).Nevertheless, the GDG recognised that severalimportant recommendations could be made relatingto patients needing long term nutrition support andthat some recommendations made elsewhere in thereport had particular relevance in this context.
1111..22 RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
1111..22..11 HHoommee eenntteerraall ttuubbee ffeeeeddiinngg
All people in the community having enteral tubefeeding should be supported by a coordinatedmultidisciplinary team, which includes dietitians,district, care home or homecare company nurses,GPs, community pharmacists and other alliedhealthcare professionals (for example, speech andlanguage therapists) as appropriate. Close liaisonbetween the multidisciplinary team and patientsand carers regarding diagnoses, prescription,arrangements and potential problems is essential.[[DD((GGPPPP))]]
SUPPORTING PATIENTS IN THE COMMUNIT Y 141
11 Supporting patients in the community

Patients in the community having enteral tubefeeding and their carers should receive anindividualised care plan which includes overallaims and a monitoring plan. [[DD((GGPPPP))]]
Patients in the community having enteral tubefeeding and their carers, should receive trainingand information from members of themultidisciplinary team on:
• the management of the tubes, deliverysystems and the regimen, outlining allprocedures related to setting up feeds, usingfeed pumps, the likely risks and methods fortroubleshooting common problems and beprovided with an instruction manual (andvisual aids if appropriate)
• both routine and emergency telephone numbersto contact a healthcare professional whounderstands the needs and potential problemsof people on home enteral tube feeding
• the delivery of equipment, ancillaries and feedwith appropriate contact details for anyhomecare company involved. [[DD((GGPPPP))]]
1111..33.. HHoommee ppaarreenntteerraall nnuuttrriittiioonn
1111..33..11.. IInnttrroodduuccttiioonn aanndd pprreevvaalleennccee
Prolonged PN is needed for patients with chronicintestinal failure; where oral or enteral feeding iseither ineffective or unsafe. If the intestinal failureis considered to be irreversible within theforeseeable future the feasibility of homeparenteral nutrition (HPN) should be considered.
In 2003 there were 517 adult HPN patientsregistered via the British Artificial Nutrition Surveywith point prevalence of 9.5/million adultpopulation for England and 4.5/million for
Wales172. However point prevalence varied between0 and 21/million in different Strategic HealthAuthorities suggesting the application of widelyvarying selection criteria or standards of care.
Short bowel syndrome is the most commonindication (54%) for HPN, followed bymalabsorption 17%, fistula 8% and GI obstruction6%. Crohn’s disease is the commonest underlyingdiagnosis in new registrations.
1111..33..22 OOrrggaanniissaattiioonn ooff hhoommee ppaarreenntteerraall nnuuttrriittiioonn
Patients requiring HPN will have their intravenousaccess (usually tunnelled catheter (seerecommendation 9.6.3.5.1) and PN regimenestablished in hospital from where they will bedischarged home. The organisation required tosuccessfully discharge and establish a patient onHPN requires a multidisciplinary team approachwith a minimum of; a gastroenterologist/GIsurgeon, pharmacist, nutrition nurse specialist,dietitian, GP and community nurses. All patientsshould receive pre-discharge training in themanagement of their HPN and this educationshould extend to any community based staff whoare to be involved in the care of the patient oncedischarged. It is essential that close support andmonitoring by a hospital based team, experiencedin looking after these complex patients, iscontinued after discharge for as long as thepatient requires HPN.
Patients also need the organisation of allequipment, feed supplies and ancillaries on aregular basis. In many cases, home carecompanies (pharmaceutical) are contracted toprovide for these needs and for some patientsthey also provide on-going specialist nursing carein the home or community setting.
1111..33..33.. MMeetthhooddss
No specific reviews were performed for HPNalthough we did identify information on thepatient’s perspectives about this aspect of care.Nevertheless, the GDG felt that importantrecommendations could be made for patientsreceiving this form of long term nutrition support.
1111..44.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
HHoommee ppaarreenntteerraall nnuuttrriittiioonn
All people in the community having parenteralnutrition should be supported by a co-ordinatedmultidisciplinary team, which includes input fromspecialist nutrition nurses, dietitians, GPs,pharmacists and district and/or homecarecompany nurses. Close liaison between themultidisciplinary team and patients and carersregarding diagnoses, prescription, arrangementsand potential problems is essential. [[DD((GGPPPP))]]
NUTRITION SUPPORT IN ADULTS142

People in the community having parenteralnutrition and their carers should receive anindividualised care plan which includes overallaims and a monitoring plan. [[DD((GGPPPP))]]
People in the community having parenteralnutrition and their carers should receive trainingand information from members of themultidisciplinary team on:
• the management of the delivery systems andthe regimen, outlining all procedures related tosetting up feeds, using feed pumps, the likelyrisks and methods for troubleshooting commonproblems and be provided with an instructionmanual (and visual aids if appropriate)
• routine and emergency telephone numbers tocontact a healthcare professional with therelevant competencies (specialist nutritionnurse, pharmacist)
• the arrangements for the delivery ofequipment, ancillaries and feed withappropriate contact details for any homecarecompany involved. [[DD((GGPPPP))]]
1111..55.. WWoorrkkiinngg iinn ppaarrttnneerrsshhiipp wwiitthh ppaattiieennttss,, ffaammiilliieess aanndd ccaarreerrss
Patients may use nutrition support in the long orshort term and be based in hospital or communitysettings. This section addresses general issues tofacilitate working in partnership with patients(and their carers) who are using short and longterm nutrition support.
1111..55..11.. PPaattiieennttss oonn sshhoorrtt aanndd lloonngg--tteerrmm nnuuttrriittiioonn ssuuppppoorrtt
Suffering from malnutrition can be a distressingexperience for both the patient and their family orcarers. It is important that appropriateinformation and support for the patient andcarer(s) is provided so that informed choices canbe made. Information should include diagnosis,treatment options according to clinical condition,side effects and sources of physical, psychologicaland social (such as disability benefits) supportwhere appropriate. The format and language ofthe information provided should be tailored tothe individual’s situation.
When delivering information, considerationshould be given as to whether short or long-termnutrition support is required, and the method tobe used (enteral and/or parenteral), as this hasvery different implications for both patients andcarers. Consideration should also be given to thepatient’s cognitive abilities, gender, physicalneeds, culture and stage of life of the individual.The patient should be given the recognition fortheir ability to self-care or in their ability as acarer when receiving nutrition support at home.Many patients who have received nutritionsupport for a long time and their carers will haveinvested a lot of time into the management oftheir nutrition support and will consequently havebecome very knowledgeable in the administrationof nutrition support in addition to being able torecognise and respond to any changes in order toremain healthy and free from complications.
Checklists can be used to remind both healthcareprofessionals and patients about information thatshould be discussed during consultations.
Patients and/or carers should be involved in thedecision-making process regarding the method(s)of feeding and any cultural and/or ethnic needsand/or preferences should be taken into account.Whenever possible patients and carers should beaware of why nutrition support is necessary, howit will be delivered and the effect it will have onthe patient.
Once the patient has been diagnosed and is usingnutrition support, it is likely that care from arange of different healthcare professionals will beneeded depending on the different setting:hospital (emergency/inpatient) or the communityi.e. patients own home or care home setting. It isvery important that everyone providing care ortreatment for patients using nutrition support isfamiliar with the management of the differentforms of such support and is able to provideessential information. Patients should understandthat ongoing monitoring may establish a need forchanges in their nutrition support and clinicaldevelopments may lengthen or shorten the needfor artificial nutrition.
SUPPORTING PATIENTS IN THE COMMUNIT Y 143

1111..55..22.. MMeetthhooddss
We conducted a literature search to identifypatients’ and carers’ views on nutrition support.The majority of the studies in the review focussedon patients using long-term ETF or HPN. Thesewere qualitative studies (surveys, questionnairesand personal accounts). Below is a summary ofthe review.
1111..55..33.. FFiinnddiinnggss ffrroomm ssttuuddiieess ooff ppaattiieennttss uussiinngg lloonngg--tteerrmmnnuuttrriittiioonn ssuuppppoorrtt
A predominant feature in the literature was theneed for counselling:
• Living with the reality of what it means not to
eat was reported in five studies37,97,211,319,384.Not being able to eat was a major adjustmentfor the patients. A survey conducted in the
United States on patients receiving HPN 319
reported that patients felt hungry whilereceiving PN and those in whom eating wascontra-indicated found it difficult to cope withthe temptation not to do so. Patients alsoexplained how this affected their social livesas they were reluctant to join social
events37,211,294,319,384. In one survey 207 somecarers of patients on HETF reported theyfound it uncomfortable to eat in the presenceof the patient.
• Feelings of guilt and low self-esteem: this was
reported in three studies37,211,319. Patientsfound it difficult to accept the physical
limitations of their body and body image37,294.Patients also experienced guilt and personalresponsibility in relation to their illness.
• How to cope with the reaction of friends orthe community at large
“Probably the most difficult aspect of enteralfeeding is the emotional side. Once againthere was never any discussion with eithermedics or family as to how one coped withthe reaction of friends or the community atlarge and this for patients is equally as
important as the practical aspect.”211
“[….]When patients come home they will meetwith differing reactions from others. Theymay be surprised to find that some formerfriends or acquaintances do not come to visitthem, some will come with almostoverwhelming sympathy, some will perform avery hurried visit, and there are the mostwonderfully sensitive people who put a handon one’s arm and ask if there is anything theycan do to help. Patients need to be aware ofthese varying reactions as soon as possible so they can be mentally prepared to deal
with them.” 211
[….] “there was no discussion at all about thevarying emotions that may be experienced andhow to cope with perhaps anger and a feeling
of isolation or being ostracized by society”211
• A need to talk to someone who is on ETF or
PN: In two studies211,319 patients expressed theimportance of sharing their experiences withsomeone who is also receiving nutritionsupport.
“My friends have been very helpful [..] butthey really don’t get what it is like to live TPN-dependent. I need to talk to other adultswho have been through what I am going
through.”319
• Fear of death/fear of liver damage fromprolonged PN: this was reported in one survey
conducted in the United States319. Patientsexpressed their fear of death from theirunderlying disease or the use of PN.
• Disturbed sleeping patterns were reported in
two studies294,319.
From the above accounts, it is clearly veryimportant that healthcare professionals are fullyfamiliar with all these issues when dealing withpatients on long-term nutrition support. This issummarised in the following conclusion from astudy on patients on HPN :
“Health professionals involved in the home care ofthis group of patients (or indeed considering theuse of this therapy even on a short-term in-patient
NUTRITION SUPPORT IN ADULTS144

basis) need to recognise the impact that thistherapy can have on the individual. Anunderstanding of the life of the chronically illpatient in the community can assist healthcarepractitioners to ‘…gauge the intended as well asunintended effects of clinical measures
(GERHARDT1990)” 227
It is also important to involve patients in thedecision-making process about methods offeeding. A study conducted in a single NHS trustarea offering a community-based support advice
service to patients choosing HETF 207, looked atdecision-making around this process. Patientsand carers reported that decisions were varieddepending on whether or not it had taken placeat a time of medical emergency. For example, ina sudden deterioration in swallowing, patientsand carers stated that the advice of professionalswas taken without hesitation but, in general,patients appreciated having time to consideroptions and being able to decide for themselves.
“Patients and carers generally perceivedprofessional advice as a recommendationrather than an option for them to consider.One person reported that his consent hadbeen influenced by discussion with thedietitian who had left the decision more open.
[…] Another patient reported that it wouldhave helped to have some opportunity to seethe tube before surgery.
[…] A number of patients revealed theirreluctance to commence tube feeding, andthat the opinion and influence of their familywere important factors in their weighing up ofthe decision, as well as professional
advice.”207
A US study 311 evaluated patient preference forETF compared to PN. A written questionnaire wasdistributed to 101 hospitalised oncology patientsand 98 outpatients without gastrointestinalillness who acted as controls. Responses wereobtained from 197 patients. Results from thestudy revealed that most patients preferred PN toETF. This preference was related to patient’sperception of the comfort of these interventions.
Another important area is the information needsfor patient and carers particularly at discharge.Two surveys in the UK including patients on HETF
and HPN 59,277 revealed some areas of concern:
“21% of patients were not provided with aninstruction manual to undertake procedures(e.g. connecting up) when first discharged.14% were not issued with emergencytelephone numbers. In the event of anemergency, patients were advised to contacttheir hospital (75%), the local hospital (16%),or the general practitioner (14%). Fourpatients were advised to contact acombination of these.
“[..] Overall impression of home nutritionservices was assessed [..]. Just over half therespondents had no comment to make (51%).22% had positive comments to make (e.g.‘fine’, ‘always satisfied’, ‘homecare companyexcellent’, ‘service very good’, ‘excellent localhospital service’. 18% had negativecomments: ‘total lack of support’, ‘a pain toget dry goods’, ‘communication poor at times’,‘tied by delivery service’, ‘would preferadditives already mixed’, ‘homecare service
omits items’.”59
An audit of adult patients on HETF in a region of
Northern Ireland 97 looked at whether patientsand carers were satisfied with the trainingreceived to prepare for HETF.
“Patients and carers felt that more emphasisshould have been placed on the causes ofpump alarming, preventing leaks, how to runfeed properly through the giving set,preventing and treating tube blockages, andon stoma care. Further training was receivedby five of the patients and carers at home(26%); 12 (35%) of those who had notreceived further training felt it would have
been useful”.97
SUPPORTING PATIENTS IN THE COMMUNIT Y 145

In three qualitative studies in the UK97,207,277
patients expressed their concerns about the lackof experience of health professionals with homenutrition support:
“Whilst 12 (63%) of the patients and carers athome expressed satisfaction with the level ofsupport received since coming home, seven(36%) were not satisfied. The issues ofconcern included: not being weighedregularly, lack of district nurse experience withhome enteral tube feeding, stoma care andlack of emotional support for not being
able to eat”97
“This rapid building of expertise enabledpatients and carers to recognise theinexperience of some of the healthprofessionals whom they encountered. [..]One patient commented that the communitynurse was ‘very nice but didn’t seem to knowas much as me’. Conversely, recognition ofinexpert practice by a health professional wasa matter of concern. Some distress wasreported when health professionals did not
meet carers’ or patients’ standards.”207
“We had a vast array of comments in relationto emergency visits with the common factorbeing that parenteral nutrition was notcommonly known about and the methods fordealing with such patients and related issueswas commonly only known by the patient
themselves or their carers.”277
One of the surveys mentioned above277, alsolooked at patients’ and carers’ opinion aboutaccessibility to nutrition support services. Themajority of respondents preferred to have accesscloser to home in preference to a remote centre.
1111..66.. RReeccoommmmeennddaattiioonnss ffoorr cclliinniiccaall pprraaccttiiccee
Healthcare professionals should ensure thatpatients having enteral or parenteral nutrition inthe community and their carers:
• are kept fully informed and have access toappropriate sources of information in formats,languages and ways that are suited to anindividual’s requirements. Consideration shouldbe given to cognition, gender, physical needs,culture and stage of life of the individual
• have the opportunity to discuss diagnosis,treatment options and relevant physical,psychological and social issues
• are given contact details for relevant supportgroups, charities and voluntary organisations.[[DD((GGPPPP))]]
1111..77.. RReesseeaarrcchh RReeccoommmmeennddaattiioonnss
DDoo ppaattiieennttss mmaannaaggeedd bbyy ssppeecciiaalliisseedd cceennttrreess hhaavveeaa bbeetttteerr oouuttccoommee ((mmoorrttaalliittyy,, mmoorrbbiiddiittyy,,ccoommpplliiccaattiioonnss,, QQOOLL)) tthhaann tthhoossee mmaannaaggeedd bbyy aallooccaall hhoossppiittaall??
WWhhaatt ffaaccttoorrss ccoonnttrriibbuuttee ttoo tthhee ddiiffffeerreenntt nnuummbbeerrssaanndd iinnddiiccaattiioonnss ffoorr lloonngg tteerrmm HHEETTFF aanndd lloonngg tteerrmmHHPPNN iinn ddiiffffeerreenntt rreeggiioonnss iinn tthhee UUKK ((aanndd iinnddiiffffeerreenntt ccoouunnttrriieess))??
WWhhaatt aarree tthhee hheeaalltthh eeccoonnoommiicc iimmpplliiccaattiioonnss ((ccoosstt eeffffeeccttiivveenneessss)) ooff lloonngg tteerrmm HHEETTFF aanndd lloonnggtteerrmm HHPPNN??
HHooww aarree ssppeecciiffiicc ccoommpplliiccaattiioonnss bbeesstt ttrreeaatteedd ((aanndd aavvooiiddeedd)) iinn tthhee ccoommmmuunniittyy ((ee..gg.. ttuubbee //ccaatthheetteerr bblloocckkaaggee))??
NUTRITION SUPPORT IN ADULTS146

AUDIT CRITERIA 147
12. Audit criteria
To determine the risk of malnutrition:
∑• hospital inpatients are screened onadmission and this is repeated weekly
∑• hospital outpatients are screenedat their first clinic appointment andat subsequent appointments wherethere is clinical concern
∑• people in care homes should bescreened on admission and whenthere is clinical concern
A clear process should be establishedfor documenting the outcomes ofscreening (that is, ‘nutritional riskscore’) and the subsequent actions(that is, ‘nutritional care plan’) taken ifthe patient is recognised asmalnourished or at risk of malnutrition.
Documentation in patient records thatconsideration has been given as towhether the patient presents with anyindications for malnutrition or risk ofmalnutrition and a record of whetheroptions of nutrition support have beenconsidered for people who present with:
∑• a BMI less than 18.5 kg/m2 ,
∑• unintentional loss of greater than10% body weight within theprevious 3–6 months,
∑• a BMI less than 20 kg/m2 andmore than 5% unintentional bodyweight loss within the previous3–6 months,
Hospital departments considered tohave people at low risk ofmalnutrition. They will havespecifically opted out of screeninghaving followed an explicit process todo so via the local clinical governancestructure and involving experts innutrition support.
Subsequent screening of people incare homes if there is no clinicalconcern about risk of under nutrition.
A simple screening tool should be usedthat includes BMI (or other estimate,for example mid-arm circumferencewhen weight cannot be measured),percentage weight loss, and considersthe time over which nutrient intake hasbeen reduced (for example themalnutrition universal screeningtool,(‘MUST’). Examples for clinical concern; peoplewith fragile skin, poor wound healing,apathy, wasted muscles, poor appetite,altered taste sensation, impairedswallowing, altered bowel habit, loosefitting clothes or prolongedintercurrent illness).
Criterion Exception Definition of terms
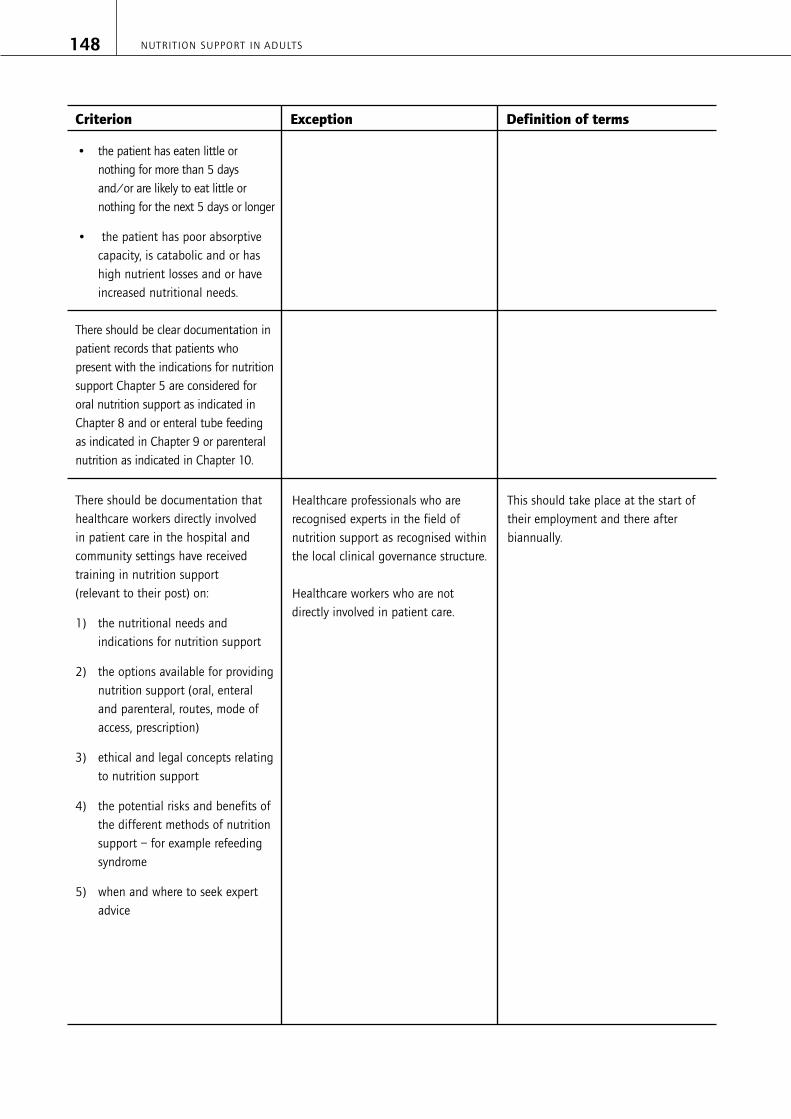
NUTRITION SUPPORT IN ADULTS148
∑• the patient has eaten little ornothing for more than 5 daysand/or are likely to eat little ornothing for the next 5 days or longer
∑• the patient has poor absorptivecapacity, is catabolic and or hashigh nutrient losses and or haveincreased nutritional needs.
There should be clear documentation inpatient records that patients whopresent with the indications for nutritionsupport Chapter 5 are considered fororal nutrition support as indicated inChapter 8 and or enteral tube feedingas indicated in Chapter 9 or parenteralnutrition as indicated in Chapter 10.
There should be documentation thathealthcare workers directly involved in patient care in the hospital andcommunity settings have receivedtraining in nutrition support (relevant to their post) on:
1) the nutritional needs andindications for nutrition support
2) the options available for providingnutrition support (oral, enteraland parenteral, routes, mode ofaccess, prescription)
3) ethical and legal concepts relatingto nutrition support
4) the potential risks and benefits ofthe different methods of nutritionsupport – for example refeedingsyndrome
5) when and where to seek expertadvice
Healthcare professionals who arerecognised experts in the field ofnutrition support as recognised withinthe local clinical governance structure.
Healthcare workers who are notdirectly involved in patient care.
This should take place at the start oftheir employment and there afterbiannually.
Criterion Exception Definition of terms

AUDIT CRITERIA 149
In patients who receive nutritionsupport there should be cleardocumentation of which health careprofessionals have been involved inthe prescription, administration andmonitoring. Records should be kept ofimportant outcome measures such asfrequency of GP visits, hospitalduration, complications e.g. infections.
In acute hospitals trusts the nutritionsteering committee should support atleast one hospital specialist nutritionsupport nurse who should workalongside nursing staff, dietitians andother experts in nutrition support tofacilitate ongoing training of wardstaff who care for people on nutritionsupport. A system of documentinghospital staff adherence to nutritionsupport protocols should beestablished for each patient prescribednutrition support, along with datacollection on complications related tothe use of nutrition support – forexample, poor tolerance of feeds ortubes, infections rate, site of infection.
Senior managers of hospitals shouldmaintain clear documentation of theoutcomes of nutrition steeringcommittees meetings. They shouldattempt to record the benefits of theirwork such as clinicians adherence tonutrition support protocols that havebeen developed and agreed by thenutrition steering committee.
People not prescribed nutritionsupport
GP practice Nutrition Steering Committee workingwithin the clinical Governanceframework may include representativesfrom medical staff, dietetics, nursing,pharmacy, catering and management.
Criterion Exception Definition of terms

NUTRITION SUPPORT IN ADULTS150
To determine the risk of malnutrition:
∑• hospital inpatients are screenedon admission and this is repeatedweekly
∑• hospital outpatients are screenedat their first clinic appointmentand at subsequent appointmentswhere there is clinical concern
∑• people in care homes should bescreened on admission and whenthere is clinical concern
A clear process should be establishedfor documenting the outcomes ofscreening (that is, ‘nutritional riskscore’) and the subsequent actions(that is, ‘nutritional care plan’) taken ifthe patient is recognised asmalnourished or at risk of malnutrition.
Documentation in patient records thatconsideration has been given as towhether the patient presents with anyindications for malnutrition or risk ofmalnutrition and a record of whetheroptions of nutrition support have beenconsidered for people who present with:
∑• a BMI less than 18.5 kg/m2 ,
∑• unintentional loss of greater than10% body weight within theprevious 3–6 months,
∑• a BMI less than 20 kg/m2 andmore than 5% unintentional bodyweight loss within the previous3–6 months,
∑• the patient has eaten little ornothing for more than 5 daysand/or are likely to eat little ornothing for the next 5 days or longer
∑• the patient has poor absorptivecapacity, is catabolic and or hashigh nutrient losses and or haveincreased nutritional needs.
Hospital departments considered tohave people at low risk ofmalnutrition. They will havespecifically opted out of screeninghaving followed an explicit process todo so via the local clinical governancestructure and involving experts innutrition support.
Subsequent screening of people incare homes if there is no clinicalconcern about risk of under nutrition.
A simple screening tool should be usedthat includes BMI (or other estimate,for example mid-arm circumferencewhen weight cannot be measured),percentage weight loss, and considersthe time over which nutrient intake hasbeen reduced (for example themalnutrition universal screeningtool,(‘MUST’).
Examples for clinical concern; peoplewith fragile skin, poor wound healing,apathy, wasted muscles, poor appetite,altered taste sensation, impairedswallowing, altered bowel habit, loosefitting clothes or prolongedintercurrent illness).
Criterion Exception Definition of terms

AUDIT CRITERIA 151
There should be clear documentationin patient records that patients whopresent with the indications fornutrition support, Chapter 5, areconsidered for oral nutrition support asindicated in Chapter 8 and or enteraltube feeding as indicated in Chapter 9or parenteral nutrition as indicated inChapter 10.
There should be documentation thathealthcare workers directly involved inpatient care in the hospital andcommunity settings have receivedtraining in nutrition support (relevantto their post) on:
1) the nutritional needs andindications for nutrition support
2) the options available for providingnutrition support (oral, enteraland parenteral, routes, mode ofaccess, prescription)
3) ethical and legal concepts relatingto nutrition support
4) the potential risks and benefits ofthe different methods of nutritionsupport – for example refeedingsyndrome
5) when and where to seek expertadvice
In patients who receive nutritionsupport there should be cleardocumentation of which health careprofessionals have been involved inthe prescription, administration andmonitoring. Records should be kept ofimportant outcome measures such asfrequency of GP visits, hospitalduration, complications e.g. infections.
Healthcare professionals who arerecognised experts in the field ofnutrition support as recognised withinthe local clinical governance structure.
Healthcare workers who are notdirectly involved in patient care.
People not prescribed nutritionsupport
This should take place at the start oftheir employment and thereafterbiannually.
Criterion Exception Definition of terms

NUTRITION SUPPORT IN ADULTS152
In acute hospitals trusts the nutritionsteering committee should support atleast one hospital specialist nutritionsupport nurse who should workalongside nursing staff, dietitians andother experts in nutrition support tofacilitate ongoing training of wardstaff who care for people on nutritionsupport. A system of documentinghospital staff adherence to nutritionsupport protocols should beestablished for each patient prescribednutrition support, along with datacollection on complications related tothe use of nutrition support – forexample, poor tolerance of feeds ortubes, infections rate, site of infection.
Senior managers of hospitals shouldmaintain clear documentation of theoutcomes of nutrition steeringcommittees meetings. They shouldattempt to record the benefits of theirwork such as clinicians adherence tonutrition support protocols that havebeen developed and agreed by thenutrition steering committee.
GP practice Nutrition Steering Committee workingwithin the clinical Governanceframework may include representativesfrom medical staff, dietetics, nursing,pharmacy, catering and management.
Criterion Exception Definition of terms

1. (1992) A positive approach to nutrition astreatment. Report of a working party chaired byProfessor JE Lennard-Jones on the role of enteraland parenteral feeding in hospital and at home.London: Kings Fund.
2. Dorland’s Illustrated Medical Dictionaryhttp://www.mercksource.com/pp/us/cns/cns_hl_dorlands.jspzQzpgzEzzSzppdocszSzuszSzcommonzSzdorlandszSzdorlandzSzdmd_a-b_00zPzhtm[accessed 25-4-0005].
3. (2005) Hospital episode statistics: England:financial year 2003 to 2004. London:Department of Health.
4. Abou-Assi S, Craig K, O’Keefe SJD. Hypocaloricjejunal feeding is better than total parenteralnutrition in acute pancreatitis: Results of arandomized comparative study. American Journalof Gastroenterology 2002, 97(9):2255-62.
5. Adams S, Dellinger EP, Wertz MJ, Oreskovich MR,Simonowitz D, Johansen K. Enteral versusparenteral nutritional support followinglaparotomy for trauma: a randomized prospectivetrial. Journal of Trauma-Injury Infection & CriticalCare 1986, 26(10):882-91.
6. Aihara H, Kawamura YJ, Konishi F. Reducedmedical costs achieved after elective oncologicalcolorectal surgery by early feeding and fewerscheduled examinations. Journal ofGastroenterology 2003, 38(8):747-50.
7. Aldamiz-Echevarria L, Bachiller MP, Ariz MC,Gimenez A, Barcia MJ, Marin M. Continuousversus cyclic parenteral nutrition during bonemarrow transplantation: assessment and follow-up. Clinical Nutrition 1996, 15(6):333-6.
8. Allsup SJ, Shenkin A, Gosney MA, Taylor S, TaylorW, Hammond M et al. Can a short period ofmicronutrient supplementation in olderinstitutionalized people improve response toinfluenza vaccine? A randomized, controlled trial.Journal of the American Geriatrics Society 2004,52(1):20-4.
9. Arnaud-Battandier F, Malvy D, Jeandel C, SchmittC, Aussage P, Beaufrère B et al. Use of oralsupplements in malnourished elderly patientsliving in the community: a pharmaco-economicstudy. Clinical Nutrition 2004, 23(5):1096-103.
10. Arnold C, Richter MP. The effect of oral nutritionalsupplements on head and neck cancer.International Journal of Radiation Oncology,Biology, Physics 1989, 16(6):1595-9.
11. Arrowsmith H. A critical evaluation of the use ofnutrition screening tools by nurses. British Journalof Nursing 1999, 8(22):1483-90.
12. Askanazi J, Rosenbaum SH, Hyman AI, SilverbergPA, Milic-Emili J, Kinney JM. Respiratory changesinduced by the large glucose loads of totalparenteral nutrition. JAMA : the Journal of theAmerican Medical Association 1980,243(14):1444-7.
13. Askanazi J, Weissman C, Rosenbaum SH, HymanAI, Milic-Emili J, Kinney JM. Nutrition and therespiratory system. Critical Care Medicine 1982,10(3):163-72.
14. Avenell A, Handoll HHG. A systematic review ofprotein and energy supplementation for hipfracture aftercare in older people. EuropeanJournal of Clinical Nutrition 2003, 57(8):895-903.
BIBLIOGRAPHY 153
Bibliography
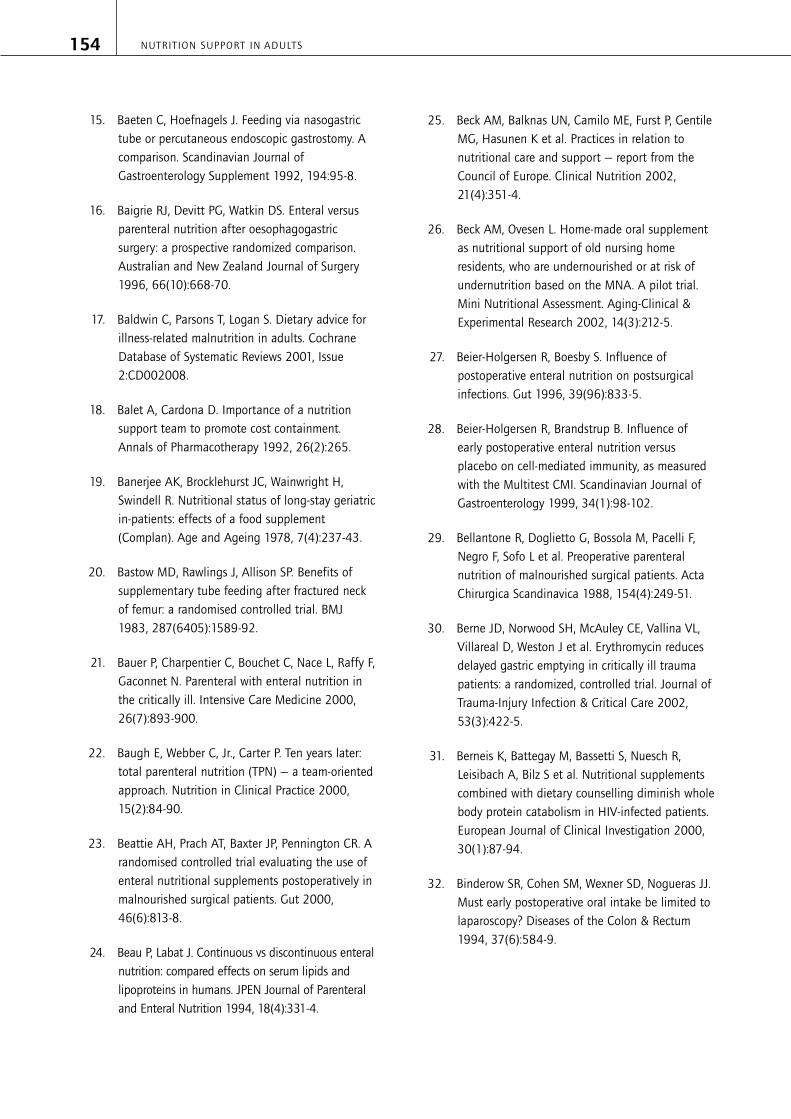
15. Baeten C, Hoefnagels J. Feeding via nasogastrictube or percutaneous endoscopic gastrostomy. Acomparison. Scandinavian Journal ofGastroenterology Supplement 1992, 194:95-8.
16. Baigrie RJ, Devitt PG, Watkin DS. Enteral versusparenteral nutrition after oesophagogastricsurgery: a prospective randomized comparison.Australian and New Zealand Journal of Surgery1996, 66(10):668-70.
17. Baldwin C, Parsons T, Logan S. Dietary advice forillness-related malnutrition in adults. CochraneDatabase of Systematic Reviews 2001, Issue2:CD002008.
18. Balet A, Cardona D. Importance of a nutritionsupport team to promote cost containment.Annals of Pharmacotherapy 1992, 26(2):265.
19. Banerjee AK, Brocklehurst JC, Wainwright H,Swindell R. Nutritional status of long-stay geriatricin-patients: effects of a food supplement(Complan). Age and Ageing 1978, 7(4):237-43.
20. Bastow MD, Rawlings J, Allison SP. Benefits ofsupplementary tube feeding after fractured neckof femur: a randomised controlled trial. BMJ1983, 287(6405):1589-92.
21. Bauer P, Charpentier C, Bouchet C, Nace L, Raffy F,Gaconnet N. Parenteral with enteral nutrition inthe critically ill. Intensive Care Medicine 2000,26(7):893-900.
22. Baugh E, Webber C, Jr., Carter P. Ten years later:total parenteral nutrition (TPN) — a team-orientedapproach. Nutrition in Clinical Practice 2000,15(2):84-90.
23. Beattie AH, Prach AT, Baxter JP, Pennington CR. Arandomised controlled trial evaluating the use ofenteral nutritional supplements postoperatively inmalnourished surgical patients. Gut 2000,46(6):813-8.
24. Beau P, Labat J. Continuous vs discontinuous enteralnutrition: compared effects on serum lipids andlipoproteins in humans. JPEN Journal of Parenteraland Enteral Nutrition 1994, 18(4):331-4.
25. Beck AM, Balknas UN, Camilo ME, Furst P, GentileMG, Hasunen K et al. Practices in relation tonutritional care and support — report from theCouncil of Europe. Clinical Nutrition 2002,21(4):351-4.
26. Beck AM, Ovesen L. Home-made oral supplementas nutritional support of old nursing homeresidents, who are undernourished or at risk ofundernutrition based on the MNA. A pilot trial.Mini Nutritional Assessment. Aging-Clinical &Experimental Research 2002, 14(3):212-5.
27. Beier-Holgersen R, Boesby S. Influence ofpostoperative enteral nutrition on postsurgicalinfections. Gut 1996, 39(96):833-5.
28. Beier-Holgersen R, Brandstrup B. Influence ofearly postoperative enteral nutrition versusplacebo on cell-mediated immunity, as measuredwith the Multitest CMI. Scandinavian Journal ofGastroenterology 1999, 34(1):98-102.
29. Bellantone R, Doglietto G, Bossola M, Pacelli F,Negro F, Sofo L et al. Preoperative parenteralnutrition of malnourished surgical patients. ActaChirurgica Scandinavica 1988, 154(4):249-51.
30. Berne JD, Norwood SH, McAuley CE, Vallina VL,Villareal D, Weston J et al. Erythromycin reducesdelayed gastric emptying in critically ill traumapatients: a randomized, controlled trial. Journal ofTrauma-Injury Infection & Critical Care 2002,53(3):422-5.
31. Berneis K, Battegay M, Bassetti S, Nuesch R,Leisibach A, Bilz S et al. Nutritional supplementscombined with dietary counselling diminish wholebody protein catabolism in HIV-infected patients.European Journal of Clinical Investigation 2000,30(1):87-94.
32. Binderow SR, Cohen SM, Wexner SD, Nogueras JJ.Must early postoperative oral intake be limited tolaparoscopy? Diseases of the Colon & Rectum1994, 37(6):584-9.
NUTRITION SUPPORT IN ADULTS154

33. Black NA, Murphy M, Lamping D, McKee M.Consensus development methods: a review of bestpractice in creating clinical guidelines. Journal ofHealth Services Research and Policy 1999, 4:236-48.
34. Boivin MA, Levy H. Gastric feeding witherythromycin is equivalent to transpyloric feedingin the critically ill. Critical Care Medicine 2001,29(10):1916-9.
35. Bonten MJ, Gaillard CA, van der HR, de LeeuwPW, van der GS, Stobberingh EE et al. Intermittententeral feeding: the influence on respiratory anddigestive tract colonization in mechanicallyventilated intensive-care-unit patients. AmericanJournal of Respiratory and Critical Care Medicine1996, 154(2 Pt 1):394-9.
36. Bourdel-Marchasson I, Barateau M, Rondeau V,Dequae-Merchadou L, Salles-Montaudon N,Emeriau J-P et al. A multi-center trial of theeffects of oral nutritional supplementation incritically ill older inpatients. Nutrition 2000,16(1):1-5.
37. Boutin L. Bringing TPN home: a patient’sperspective. Journal of Home Health Care Practice1995, 8(1):9-17.
38. Bower RH, Talamini MA, Sax HC, Hamilton F,Fischer JE. Postoperative enteral vs parenteralnutrition. A randomized controlled trial. Archivesof Surgery 1986, 121(9):1040-5.
39. Bowling T. Nutritional support for adults andchildren - a handbook for hospital practice.Oxford: Radcliffe Medical Press, 2003.
40. Bozzetti F. Is enteral nutrition a primary therapy incancer patients? Gut 1994, 35(1 Suppl):S65-S68.
41. Bozzetti F, Braga M, Gianotti L, Gavazzi C, MarianiL. Postoperative enteral versus parenteral nutritionin malnourished patients with gastrointestinalcancer: a randomised multicentre trial. Lancet2001, 358(9292):1487-92.
42. Bozzetti F, Gavazzi C, Miceli R, Rossi N, Mariani L,Cozzaglio L et al. Perioperative total parenteralnutrition in malnourished, gastrointestinal cancerpatients: a randomized, clinical trial. JPEN Journal ofParenteral and Enteral Nutrition 2000, 24(1):7-14.
43. Braga M, Gianotti L, Gentilini O, Parisi V, Salis C,Di C, V. Early postoperative enteral nutritionimproves gut oxygenation and reduces costscompared with total parenteral nutrition. CriticalCare Medicine 2001, 29(2):242-8.
44. British Dietetic Association, Royal College ofSpeech and Language Therapists. (2002) Nationaldescriptors for texture modification in adults.Birmingham: British Dietetic Association.
45. Brooks AD, Hochwald SN, Heslin MJ, Harrison LE,Burt M, Brennan MF. Intestinal permeability afterearly postoperative enteral nutrition in patientswith upper gastrointestinal malignancy. JPENJournal of Parenteral and Enteral Nutrition 1999,23(2):75-9.
46. Brown DN, Miedema BW, King PD, Marshall JB.Safety of early feeding after percutaneousendoscopic gastrostomy. Journal of ClinicalGastroenterology 1995, 21(4):330-1.
47. Brown KM, Seabrook NA. (1992) Nutritionalinfluences on recovery and length of hospital stayin elderly women following femoral fractureProceedings of the Nutrition Society 132A-Abstract
48. Brown RO, Carlson SD, Cowan GS, Jr., Powers DA,Luther RW. Enteral nutritional supportmanagement in a university teaching hospital:team vs nonteam. JPEN Journal of Parenteral andEnteral Nutrition 1987, 11(1):52-6.
49. Bruce D, Laurance I, Mcguiness M, Ridley M,Goldswain P. Nutritional supplements after hipfracture: poor compliance limits effectiveness.Clinical Nutrition 2003, 22(5):497-500.
50. Brunelle D. Impact of a dedicated infusion therapyteam on the reduction of catheter-relatednosocomial infections. J Infus Nurs 2003,26(6):362-6.
BIBLIOGRAPHY 155

51. Burrows WR, Gingo AJJ, Rose SM, Zwick SI, KostyDL, Dierker LJJ et al. Safety and efficacy of earlypostoperative solid food consumption aftercesarean section. Journal of ReproductiveMedicine 1995, 40(6):463-7.
52. Cabre E, Gonzalez-Huix F, Abad-Lacruz A, EsteveM, Acero D, Fernandez-Banares F et al. Effect oftotal enteral nutrition on the short-term outcomeof severely malnourished cirrhotics. A randomizedcontrolled trial. Gastroenterology 1990,98(3):715-20.
53. Calvo M, V. Intensive monitoring program for oralfood intake in patients undergoing allogenichematopoietic cell transplantation: a cost benefitanalysis. Nutrition 2002, 18(9):769-71.
54. Campbell IT, Morton RP, Cole JA, Raine CH,Shapiro LM, Stell PM. A comparison of the effectsof intermittent and continuous nasogastricfeeding on the oxygen consumption and nitrogenbalance of patients after major head and necksurgery. American Journal of Clinical Nutrition1983, 38(6):870-8.
55. Campbell IT, Morton RP, Macdonald IA, Judd S,Shapiro L, Stell PM. Comparison of the metaboliceffects of continuous postoperative enteralfeeding and feeding at night only. AmericanJournal of Clinical Nutrition 1990, 52(6):1107-12.
56. Campbell SE, Avenell A, Walker AE. Assessment ofnutritional status in hospital in-patients. QuarterlyJournal of Medicine 2002, 95(2):83-7.
57. Cardona D, Del M, V, Salvador R. Earlypostoperative total parenteral nutrition in gastriccancer: A cost-effectiveness study. Journal ofClinical Nutrition & Gastroenterology 1986,1(6):267-70.
58. Carr CS, Ling KD, Boulos P, Singer M. Randomisedtrial of safety and efficacy of immediatepostoperative enteral feeding in patientsundergoing gastrointestinal resection. BMJ 1996,312(7035):869-71.
59. Carter DM, Wheatley C, Payne-James JJ, Pick A.Home nutrition survey in the UK: the patient’sperspective. Clinical Nutrition 1993, 12(4):208-12.
60. Chaix C, Durand-Zaleski I, Alberti C, Brun-BuissonC. A model to compute the medical cost ofpatients in intensive care. Pharmacoeconomics1999, 16(6):573-82.
61. Chapman MJ, Fraser RJ, Kluger MT, Buist MD, DeNichilo DJ. Erythromycin improves gastricemptying in critically ill patients intolerant ofnasogastric feeding. Critical Care Medicine 2000,28(7):2334-7.
62. Charlin V, Carrasco F, Sepulvedo C, Torres M, KehrJ. Nutritional supplementation according toenergy and protein requirements in malnourishedHIV-infected patients. Archivos Latinoamericanosde Nutricion 2002, 52(3):267-73.
63. Choudhry U, Barde CJ, Markert R, Gopalswamy N.Percutaneous endoscopic gastrostomy: arandomized prospective comparison of early anddelayed feeding. Gastrointestinal Endoscopy1996, 44(2):164-7.
64. ChrisAnderson D, Heimburger DC, Morgan SL, GeelsWJ, Henry KL, Conner W et al. Metaboliccomplications of total parenteral nutrition: effects of anutrition support service. JPEN Journal of Parenteraland Enteral Nutrition 1996, 20(3):206-10.
65. Chuntrasakul C, Siltharm S, ChinswangwatanakulV, Pongprasobchai T, Chockvivatanavanit S,Bunnak A. Early nutritional support in severetraumatic patients. Journal of the MedicalAssociation of Thailand 1996, 79(1):21-6.
66. Ciocon JO, Galindo-Ciocon DJ, Tiessen C, GalindoD. Continuous compared with intermittent tubefeeding in the elderly. JPEN Journal of Parenteraland Enteral Nutrition 1992, 16(6):525-8.
67. Clarke PJ, Ball MJ, Tunbridge A, Kettlewell MG.The total parenteral nutrition service: an update.Annals of the Royal College of Surgeons ofEngland 1988, 70(5):296-9.
NUTRITION SUPPORT IN ADULTS156

68. Collins S, Myatt M, Golden B. Dietary treatment ofsevere malnutrition in adults. Am J Clin Nutr1998, 68(1):193-9.
69. Cook IJ, Kahrilas PJ. AGA technical review onmanagement of oropharyngeal dysphagia.Gastroenterology 1999, 116(2):455-78.
70. Couse N, Pickford LR, Mitchell CJ, MacFie J. Totalparenteral nutrition by peripheral vein - substituteor supplement to the central venous route? Aprospective trial. Clinical Nutrition 1993,12(4):213-6.
71. Cowl CT, Weinstock JV, Al Jurf A, Ephgrave K,Murray JA, Dillon K. Complications and costassociated with parenteral nutrition delivered tohospitalized patients through either subclavian orperipherally-inserted central catheters. ClinicalNutrition 2000, 19(4):237-43.
72. Curtis L, Netten A. Unit costs of health and socialcare. Canterbury: Personal Social ServicesResearch Unit, University of Kent, 2004.
73. Cutillo G, Maneschi F, Franchi M, Giannice R,Scambia G, Benedetti-Panici P. Early feedingcompared with nasogastric decompression aftermajor oncologic gynecologic surgery: arandomized study. Obstetrics & Gynecology 1999,93(1):41-5.
74. Dahlberg PJ, Yutuc WR, Newcomer KL. Subclavianhemodialysis catheter infections. AmericanJournal of Kidney Diseases 1986, 7(5):421-7.
75. Dalton MJ, Schepers G, Gee JP. Consultative totalparenteral nutrition teams: The effect on theincidence of total parenteral nutrition-relatedcomplications. JPEN Journal of Parenteral andEnteral Nutrition 1984, 8(2):146-52.
76. Davies AR, Froomes PR, French CJ, Bellomo R,Gutteridge GA, Nyulasi I et al. Randomizedcomparison of nasojejunal and nasogastricfeeding in critically ill patients. Critical CareMedicine 2002, 30(3):586-90.
77. Day L, Stotts NA, Frankfurt A, Stralovich-RomaniA, Volz M, Muwaswes M et al. Gastric versusduodenal feeding in patients with neurologicaldisease: a pilot study. Journal of NeuroscienceNursing 2001, 33(3):148-9.
78. De Cicco M, Panarello G, Chiaradia V, Fracasso A,Veronesi A, Testa V et al. Source and route ofmicrobial colonisation of parenteral nutritioncatheters. Lancet 1989, 2(8674):1258-61.
79. Delmi M, Rapin CH, Bengoa JM, Delmas PD,Vasey H, Bonjour J-P. Dietary supplementation inelderly patients with fractured neck of the femur.Lancet 1990, 335(8696):1013-6.
80. Department of Health. Guidelines for preventinginfections associated with the insertion andmaintenance of central venous catheters. Journalof Hospital Infection 2001, 47 Suppl1(Supplement 1):S47-S67.
81. Department of Health. Reference guide to consentfor examination or treatmenthttp://www.dh.gov.uk/assetRoot/04/01/90/79/04019079.pdf [accessed 1-4-2005].
82. Department of Health. (2001) The essence ofcare. patient-focussed benchmarking for healthcare practitioners. London: Department of Health.
83. Detsky AS, Baker JP, O’Rourke K, Goel V.Perioperative parenteral nutrition: a meta-analysis.Annals of Internal Medicine 1987, 107(2):195-203.
84. Detsky AS, Jeejeebhoy KN. Cost-effectiveness ofpreoperative parenteral nutrition in patientsundergoing major gastrointestinal surgery. JPENJournal of Parenteral and Enteral Nutrition 1984,8(6):632-7.
85. Diamond L, Soon E. Sensory evaluation of oralnutritional supplements: a comparison of patientand dietitian preferences. Journal of the CanadianDietetic Association 1994, 55(2):85-90.
BIBLIOGRAPHY 157

86. Douglass HO, Jr., Milliron S, Nava H, Eriksson B,Thomas P, Novick A et al. Elemental diet as anadjuvant for patients with locally advancedgastrointestinal cancer receiving radiationtherapy: a prospectively randomized study. JPENJournal of Parenteral and Enteral Nutrition 1978,2(5):682-6.
87. Edington J, Barnes R, Bryan F, Dupree E, Frost G,Hickson M et al. A prospective randomisedcontrolled trial of nutritional supplementation inmalnourished elderly in the community: Clinicaland health economic outcomes. Clinical Nutrition2004, 23(2):195-204.
88. Efthimiou J, Fleming J, Gomes C, Spiro SG. Theeffect of supplementary oral nutrition in poorlynourished patients with chronic obstructivepulmonary disease. American Review ofRespiratory Disease 1988, 137(5):1075-82.
89. Eisenberg JM, Glick HA, Buzby GP, Kinosian B,Williford WO. Does perioperative total parenteralnutrition reduce medical care costs? JPEN Journalof Parenteral and Enteral Nutrition 1993,17(3):201-9.
90. Ekberg O, Hamdy S, Woisard V, Wuttge-Hannig A,Ortega P. Social and psychological burden ofdysphagia: its impact on diagnosis and treatment.Dysphagia 2002, 17(2):139-46.
91. Elia M, Stratton R, Russell C, Green C, Pang F. Thecost of malnutrition in the UK and the economiccase for the use of oral nutritional supplements(ONS) in adults. [unpublished data] 2005.
92. Elia M, Stratton RJ. How much undernutrition isthere in hospitals? British Journal of Nutrition2000, 84(3):257-9.
93. Elia, M. and Stratton, R. J. Geographicalinequalities in nutrient status and risk ofmalnutrition among English people aged 65 yearsand over [in press]. Nutrition 2005.
94. Elia MCaE. (2003) The ‘MUST’ report: nutritionalscreening of adults: a multidisciplinaryresponsibility. Development and use of the‘Malnutrition Universal Screening Tool’ (‘MUST’)for adults. A report by the Malnutrition AdvisoryGroup of the British Association for Patenteraland Enteral Nutrition. Redditch: BritishAssociation for Parenteral and Enteral Nutrition(BAPEN).
95. Elmstahl S, Bulow M, Ekberg O, Petersson M,Tegner H. Treatment of dysphagia improvesnutritional conditions in stroke patients.Dysphagia 1999, 14(2):61-6.
96. Esparza J, Boivin MA, Hartshorne MF, Levy H.Equal aspiration rates in gastrically andtranspylorically fed critically ill patients. IntensiveCare Medicine 2001, 27(4):660-4.
97. Estrange F. An audit of adult patients on homeenteral tube feeding in a region of NorthernIreland. Journal of Human Nutrition and Dietetics1997, 10(5):277-87.
98. Eyer SD, Micon LT, Konstantinides FN, Edlund DA,Rooney KA, Luxenberg MG et al. Early enteralfeeding does not attenuate metabolic responseafter blunt trauma. Journal of Trauma-InjuryInfection & Critical Care 1993, 34(5):639-43.
99. Fan ST, Lau WY, Wong KK, Chan YPM. Pre-operative parenteral nutrition in patients withoesophageal cancer: a prospective, randomisedclinical trial. Clinical Nutrition 1989, 8(1):23-7.
100. Fan ST, Lo CM, Lai EC, Chu KM, Liu CL, Wong J.Perioperative nutritional support in patientsundergoing hepatectomy for hepatocellularcarcinoma. New England Journal of Medicine1994, 331(23):1547-52.
101. Faubion WC, Wesley JR, Khalidi N, Silva J. Totalparenteral nutrition catheter sepsis: Impact of theteam approach. JPEN Journal of Parenteral andEnteral Nutrition 1986, 10(6):642-5.
NUTRITION SUPPORT IN ADULTS158

102. Faubion WC, Wesley JR, Khalidi N, Silva J. Totalparenteral nutrition catheter sepsis: impact of theteam approach. JPEN Journal of Parenteral andEnteral Nutrition 1986, 10(6):642-5.
103. Faubion WC, Wesley JR, Khalidi N, Silva J. Totalparenteral nutrition catheter sepsis: impact of theteam approach. JPEN Journal of Parenteral andEnteral Nutrition 1986, 10(6):642-5.
104. Feo CV, Romanini B, Sortini D, Ragazzi R, ZamboniP, Pansini GC et al. Early oral feeding aftercolorectal resection: a randomized controlled study.ANZ Journal of Surgery 2004, 74(5):298-301.
105. Ferguson M, Capra S, Bauer J, Banks M.Development of a valid and reliable malnutritionscreening tool for adult acute hospital patients.Nutrition 1999, 15(6):458-64.
106. Ferguson M, Capra S, Bauer J, Banks M.Development of a patient satisfaction survey withinpatient clinical nutrition services. AustralianJournal of Nutrition and Dietetics 2001,58(3):157-63.
107. Fernandez R, Griffiths R, Naylor CJ. Effectivenessof a multidisciplinary total parenteral nutritionteam in the hospital setting. JBI Reports 2003,1(2):17-48.
108. Fettes SB, Lough M. An audit of the provision ofparenteral nutrition in two acute hospitals: teamversus non-team. Scottish Medical Journal 2000,45(4):121-5.
109. Finch S, Doyle W, Lowe C, Bates CJ, Prentice A,Smithers G et al. (1998) National diet andnutrition survey: people aged 65 years and over.Volume 1: report of the diet and nutrition survey.London: The Stationary Office.
110. Finestone HM, Foley NC, Woodbury MG, Greene-Finestone L. Quantifying fluid intake in dysphagicstroke patients: a preliminary comparison of oraland nonoral strategies. Archives of PhysicalMedicine and Rehabilitation 2001, 82(12):1744-6.
111. Fisher GG, Opper FH. An interdisciplinary nutritionsupport team improves quality of care in ateaching hospital. Journal of the AmericanDietetic Association 1996, 96(2):176-8.
112. Flynn MB, Leightty FF. Preoperative outpatientnutritional support of patients with squamouscancer of the upper aerodigestive tract. AmericanJournal of Surgery 1987, 154(4):359-62.
113. Forli L. Dietary support to underweight patientswith end-stage pulmonary disease assessed forlung transplantation. Respiration 2001, 68(1):51-7.
114. Forli L, Bjortuft O, Vatn M, Kofstad J, Boe J. Astudy of intensified dietary support inunderweight candidates for lung transplantation.Annals of Nutrition & Metabolism 2001,45(4):159-68.
115. Forsberg E, Soop M, Lepape A, Thorne A.Metabolic and thermogenic response tocontinuous and cyclic total parenteral nutrition intraumatised and infected patients. ClinicalNutrition 1994, 13(5):291-301.
116. Foschi D, Cavagna G, Callioni F, Morandi E, RovatiV. Hyperalimentation of jaundiced patients onpercutaneous transhepatic biliary drainage. BritishJournal of Surgery 1986, 73(9):716-9.
117. Frankel AM, Horowitz GD. Nasoduodenal tubes inshort-stay cholecystectomy. Surgery, Gynecology &Obstetrics 1989, 168(5):433-6.
118. Fuenzalida CE, Petty TL, Jones ML, Jarrett S,Harbeck RJ, Terry RW et al. The immune responseto short-term nutritional intervention in advancedchronic obstructive pulmonary disease. AmericanReview of Respiratory Disease 1990, 142(1):49-56.
119. Gales BJ, Riley DG. Improved total parenteralnutrition therapy management by a nutritionalsupport team. Hospital Pharmacy 1994,29(5):469-70, 473-5.
120. Garden OJ, Sim AJW. A comparison of tunnelled andnontunnelled subclavian vein catheters: Aprospective study of complications during parenteralfeeding. Clinical Nutrition 1983, 2(1):51-4.
BIBLIOGRAPHY 159

121. Gariballa SE, Parker SG, Taub N, Castleden CM. Arandomized, controlled, a single-blind trial ofnutritional supplementation after acute stroke.JPEN Journal of Parenteral and Enteral Nutrition1998, 22(5):315-9.
122. General Medical Council. (2002) Withholding andwithdrawing life-prolonging treatments: goodpractice in decision-making. London: GeneralMedical Council.
123. Gianino MS, Brunt LM, Eisenberg PG. The impactof a nutritional support team on the cost andmanagement of multilumen central venouscatheters. Journal of Intravenous Nursing 1992,15(6):327-32.
124. Girodon F, Blache D, Monget A-L, Lombart M,Brunet-Lecompte P, Arnaud J et al. Effect of a two-year supplementation with low doses ofantioxidant vitamins and/or minerals in elderlysubjects on levels of nutrients and antioxidantdefense parameters. Journal of the AmericanCollege of Nutrition 1997, 16(4):357-65.
125. Girodon F, Galan P, Monget AL, Boutron-RuaultMC, Brunet-Lecomte P, Preziosi P et al. Impact oftrace elements and vitamin supplementation onimmunity and infections in institutionalizedelderly patients: a randomized controlled trial.MIN. VIT. AOX. geriatric network. Archives ofInternal Medicine 1999, 159(7):748-54.
126. Girodon F, Lombard M, Galan P, Brunet-Lecomte P,Monget AL, Arnaud J et al. Effect of micronutrientsupplementation on infection in institutionalizedelderly subjects: a controlled trial. Annals ofNutrition & Metabolism 1997, 41(2):98-107.
127. Gist RS, Swing KT, Connell NC, Robinson DC.Randomized prospective trial of early feeding inobese, high-risk cesarean-section patients. Journalof Gynecologic Surgery 2002, 18(3):95-9.
128. Gocmen A. Early post-operative feeding aftercaesarean delivery. Journal of InternationalMedical Research 2002, 30(5):506-11.
129. Goel V, Detsky AS. A cost-utility analysis ofpreoperative total parenteral nutrition.International Journal of Technology Assessment inHealth Care 1989, 5(2):183-94.
130. Goldstein M, Braitman LE, Levine GM. The medicaland financial costs associated with termination of anutrition support nurse. JPEN Journal of Parenteraland Enteral Nutrition 2000, 24(6):323-7.
131. Gonzalez-Huix F, Fernandez-Banares F, Esteve-Comas M, Abad-Lacruz A, Cabre E, Acero D et al.Enteral versus parenteral nutrition as adjuncttherapy in acute ulcerative colitis. AmericanJournal of Gastroenterology 1993, 88(2):227-32.
132. Gosney M. Are we wasting our money on foodsupplements in elder care wards? Journal ofAdvanced Nursing 2003, 43(3):275-80.
133. Government Actury’s Department. Interim lifetableshttp://www.gad.gov.uk/Life_Tables/Interim_life_tables.htm [accessed 17-3-2005].
134. Gowardman J, Sleigh J, Barnes N, Smith A, HavillJ. Intermittent enteral nutrition — a comparativestudy examining the effect on gastric pH andmicrobial colonization rates. Anaesthesia &Intensive Care 2003, 31(1):28-33.
135. Grant JP. Parenteral access. In: Rombeau JL,Rolandelli RH, eds. Clinical nutrition: parenteralnutrition, 6, 2001. pp 109-17. Philadelphia: W.B.Saunders Company.
136. Greenberg GR, Fleming CR, Jeejeebhoy KN,Rosenberg IH, Sales D, Tremaine WJ. Controlledtrial of bowel rest and nutritional support in themanagement of Crohn’s disease. Gut 1988,29(10):1309-15.
137. Guedj P, Eldor J, Stark M. Immediate postoperativeoral hydration after caesarean section. Asia-Oceania Journal of Obstetrics & Gynaecology1991, 17(2):125-9.
NUTRITION SUPPORT IN ADULTS160

138. Guichard I, Nitenberg G, Abitbol JL, et al.Tunneled versus non tunneled catheters forparenteral nutrition (PN) in an intensive care unit.A controlled study of catheter related sepsis(CRS). Clinical Nutrition 2004,(5S):A169.
139. Hamaoui E, Lefkowitz R, Olender L, Krasnopolsky-Levine E, Favale M, Webb H et al. Enteral nutritionin the early postoperative period: a new semi-elemental formula versus total parenteralnutrition. JPEN Journal of Parenteral and EnteralNutrition 1990, 14(5):501-7.
140. Han-Geurts IJ, Jeekel J, Tilanus HW, Brouwer KJ.Randomized clinical trial of patient-controlledversus fixed regimen feeding after electiveabdominal surgery. British Journal of Surgery2001, 88(12):1578-82.
141. Hankins C. Dietary supplementation withsustagen in elderly patients with fractured neck offemur [dissertation]. University of Sydney . 1996.
142. Harper JR, McAlpine S, Hetherington MM, Bolton-Smith C, McMurdo ME. Preferences for differenthigh-energy foods in elderly medical in-patients.Scottish Medical Journal 2001, 46(6):171-2.
143. Hartgrink HH, Wille J, Konig P, Hermans J, BreslauPJ. Pressure sores and tube feeding in patientswith a fracture of the hip: a randomized clinicaltrial. Clinical Nutrition 1998, 17(6):287-92.
144. Hartsell PA, Frazee RC, Harrison JB, Smith RW.Early postoperative feeding after electivecolorectal surgery. Archives of Surgery 1997,132(5):518-20.
145. Hasse JM, Blue LS, Liepa GU, Goldstein RM,Jennings LW, Mor E et al. Early enteral nutritionsupport in patients undergoing livertransplantation. JPEN Journal of Parenteral andEnteral Nutrition 1995, 19(6):437-43.
146. Hassell JT, Games AD, Shaffer B, Harkins LE.Nutrition support team management of enterallyfed patients in a community hospital is cost-beneficial. Journal of the American DieteticAssociation 1994, 94(9):993-8.
147. Hedberg AM, Lairson DR, Aday LA, Chow J, SukiR, Houston S et al. Economic implications of anearly postoperative enteral feeding protocol.Journal of the American Dietetic Association1999, 99(7):802-7.
148. Heslin MJ, Latkany L, Leung D, Brooks AD,Hochwald SN, Pisters PW et al. A prospective,randomized trial of early enteral feeding afterresection of upper gastrointestinal malignancy.Annals of Surgery 1997, 226(4):567-77.
149. Heyland D, Bradley C, Mandell LA. Effect ofacidified enteral feedings on gastric colonizationin the critically ill patient. Critical Care Medicine1992, 20(10):1388-94.
150. Heyland DK. Parenteral nutrition in the critically-ill patient: more harm than good? Proceedings ofthe Nutrition Society 2000, 59(3):457-66.
151. Heyland DK, Dhaliwal R, Drover JW. Nutritionsupport in mechanically ventilated, critically illadult patients: are we ready for evidence-basedclinical practice guidelines? Nutrition in ClinicalPractice 2004, 19(3):193-200.
152. Heyland DK, Dhaliwal R, Drover JW, Gramlich L,Dodek P, Canadian Critical Care Clinical PracticeGuidelines Committee. Canadian clinical practiceguidelines for nutrition support in mechanicallyventilated, critically ill adult patients. JPENJournal of Parenteral and Enteral Nutrition 2003,27(5):355-73.
153. Heyland DK, Drover JW, MacDonald S, Novak F,Lam M. Effect of postpyloric feeding ongastroesophageal regurgitation and pulmonarymicroaspiration: results of a randomizedcontrolled trial. Critical Care Medicine 2001,29(8):1495-501.
154. Heymsfield SB, Casper K, Grossman GD.Bioenergetic and metabolic response tocontinuous v intermittent nasoenteric feeding.Metabolism: Clinical & Experimental 1987,36(6):570-5.
BIBLIOGRAPHY 161
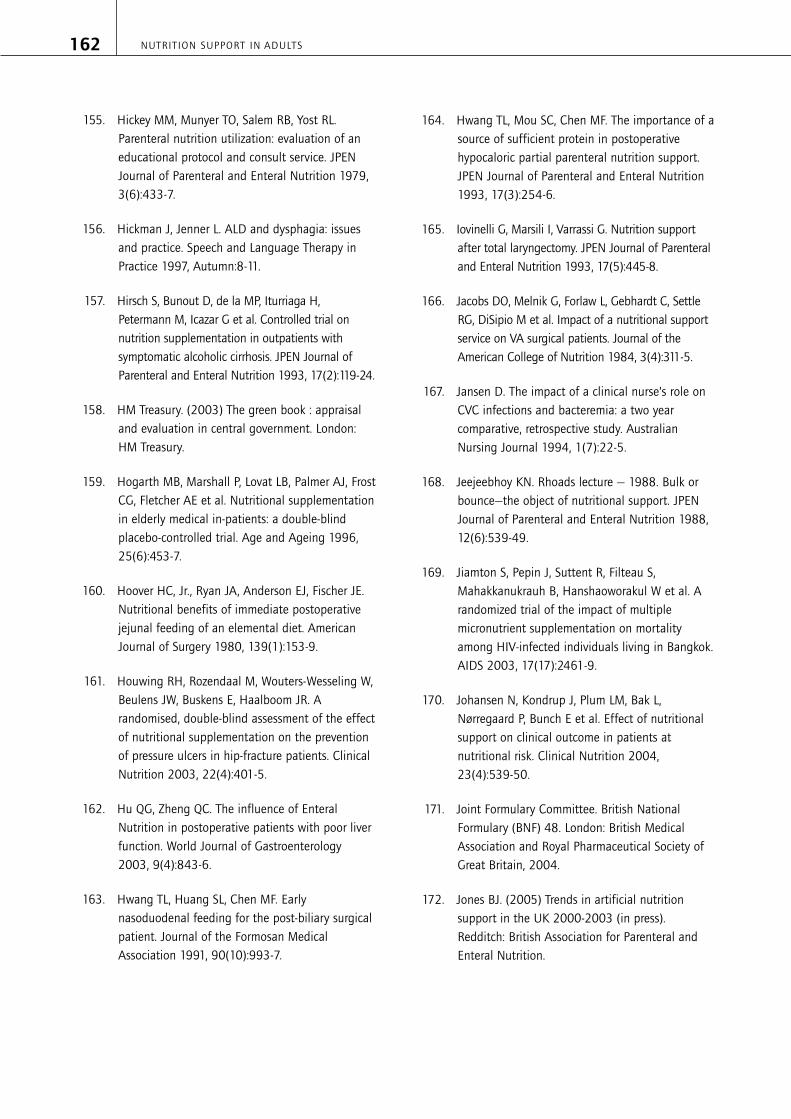
155. Hickey MM, Munyer TO, Salem RB, Yost RL.Parenteral nutrition utilization: evaluation of aneducational protocol and consult service. JPENJournal of Parenteral and Enteral Nutrition 1979,3(6):433-7.
156. Hickman J, Jenner L. ALD and dysphagia: issuesand practice. Speech and Language Therapy inPractice 1997, Autumn:8-11.
157. Hirsch S, Bunout D, de la MP, Iturriaga H,Petermann M, Icazar G et al. Controlled trial onnutrition supplementation in outpatients withsymptomatic alcoholic cirrhosis. JPEN Journal ofParenteral and Enteral Nutrition 1993, 17(2):119-24.
158. HM Treasury. (2003) The green book : appraisaland evaluation in central government. London:HM Treasury.
159. Hogarth MB, Marshall P, Lovat LB, Palmer AJ, FrostCG, Fletcher AE et al. Nutritional supplementationin elderly medical in-patients: a double-blindplacebo-controlled trial. Age and Ageing 1996,25(6):453-7.
160. Hoover HC, Jr., Ryan JA, Anderson EJ, Fischer JE.Nutritional benefits of immediate postoperativejejunal feeding of an elemental diet. AmericanJournal of Surgery 1980, 139(1):153-9.
161. Houwing RH, Rozendaal M, Wouters-Wesseling W,Beulens JW, Buskens E, Haalboom JR. Arandomised, double-blind assessment of the effectof nutritional supplementation on the preventionof pressure ulcers in hip-fracture patients. ClinicalNutrition 2003, 22(4):401-5.
162. Hu QG, Zheng QC. The influence of EnteralNutrition in postoperative patients with poor liverfunction. World Journal of Gastroenterology2003, 9(4):843-6.
163. Hwang TL, Huang SL, Chen MF. Earlynasoduodenal feeding for the post-biliary surgicalpatient. Journal of the Formosan MedicalAssociation 1991, 90(10):993-7.
164. Hwang TL, Mou SC, Chen MF. The importance of asource of sufficient protein in postoperativehypocaloric partial parenteral nutrition support.JPEN Journal of Parenteral and Enteral Nutrition1993, 17(3):254-6.
165. Iovinelli G, Marsili I, Varrassi G. Nutrition supportafter total laryngectomy. JPEN Journal of Parenteraland Enteral Nutrition 1993, 17(5):445-8.
166. Jacobs DO, Melnik G, Forlaw L, Gebhardt C, SettleRG, DiSipio M et al. Impact of a nutritional supportservice on VA surgical patients. Journal of theAmerican College of Nutrition 1984, 3(4):311-5.
167. Jansen D. The impact of a clinical nurse’s role onCVC infections and bacteremia: a two yearcomparative, retrospective study. AustralianNursing Journal 1994, 1(7):22-5.
168. Jeejeebhoy KN. Rhoads lecture — 1988. Bulk orbounce—the object of nutritional support. JPENJournal of Parenteral and Enteral Nutrition 1988,12(6):539-49.
169. Jiamton S, Pepin J, Suttent R, Filteau S,Mahakkanukrauh B, Hanshaoworakul W et al. Arandomized trial of the impact of multiplemicronutrient supplementation on mortalityamong HIV-infected individuals living in Bangkok.AIDS 2003, 17(17):2461-9.
170. Johansen N, Kondrup J, Plum LM, Bak L,Nørregaard P, Bunch E et al. Effect of nutritionalsupport on clinical outcome in patients atnutritional risk. Clinical Nutrition 2004,23(4):539-50.
171. Joint Formulary Committee. British NationalFormulary (BNF) 48. London: British MedicalAssociation and Royal Pharmaceutical Society ofGreat Britain, 2004.
172. Jones BJ. (2005) Trends in artificial nutritionsupport in the UK 2000-2003 (in press).Redditch: British Association for Parenteral andEnteral Nutrition.
NUTRITION SUPPORT IN ADULTS162
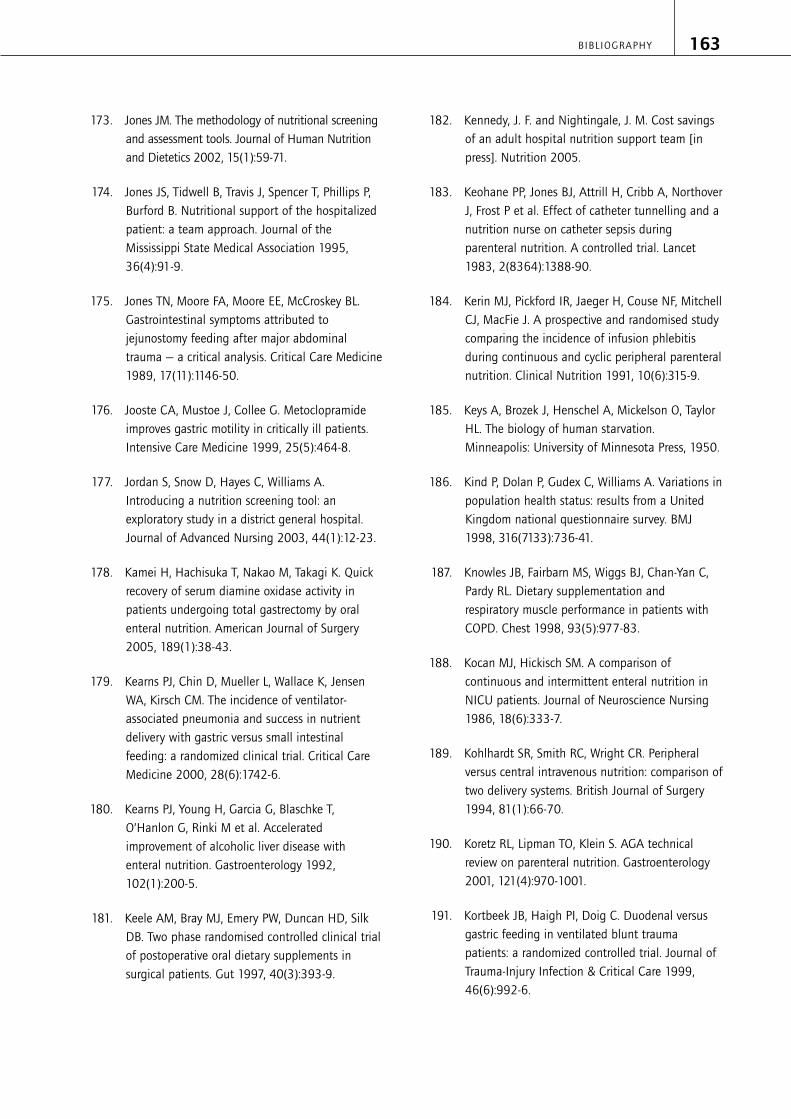
173. Jones JM. The methodology of nutritional screeningand assessment tools. Journal of Human Nutritionand Dietetics 2002, 15(1):59-71.
174. Jones JS, Tidwell B, Travis J, Spencer T, Phillips P,Burford B. Nutritional support of the hospitalizedpatient: a team approach. Journal of theMississippi State Medical Association 1995,36(4):91-9.
175. Jones TN, Moore FA, Moore EE, McCroskey BL.Gastrointestinal symptoms attributed tojejunostomy feeding after major abdominaltrauma — a critical analysis. Critical Care Medicine1989, 17(11):1146-50.
176. Jooste CA, Mustoe J, Collee G. Metoclopramideimproves gastric motility in critically ill patients.Intensive Care Medicine 1999, 25(5):464-8.
177. Jordan S, Snow D, Hayes C, Williams A.Introducing a nutrition screening tool: anexploratory study in a district general hospital.Journal of Advanced Nursing 2003, 44(1):12-23.
178. Kamei H, Hachisuka T, Nakao M, Takagi K. Quickrecovery of serum diamine oxidase activity inpatients undergoing total gastrectomy by oralenteral nutrition. American Journal of Surgery2005, 189(1):38-43.
179. Kearns PJ, Chin D, Mueller L, Wallace K, JensenWA, Kirsch CM. The incidence of ventilator-associated pneumonia and success in nutrientdelivery with gastric versus small intestinalfeeding: a randomized clinical trial. Critical CareMedicine 2000, 28(6):1742-6.
180. Kearns PJ, Young H, Garcia G, Blaschke T,O’Hanlon G, Rinki M et al. Acceleratedimprovement of alcoholic liver disease withenteral nutrition. Gastroenterology 1992,102(1):200-5.
181. Keele AM, Bray MJ, Emery PW, Duncan HD, SilkDB. Two phase randomised controlled clinical trialof postoperative oral dietary supplements insurgical patients. Gut 1997, 40(3):393-9.
182. Kennedy, J. F. and Nightingale, J. M. Cost savingsof an adult hospital nutrition support team [inpress]. Nutrition 2005.
183. Keohane PP, Jones BJ, Attrill H, Cribb A, NorthoverJ, Frost P et al. Effect of catheter tunnelling and anutrition nurse on catheter sepsis duringparenteral nutrition. A controlled trial. Lancet1983, 2(8364):1388-90.
184. Kerin MJ, Pickford IR, Jaeger H, Couse NF, MitchellCJ, MacFie J. A prospective and randomised studycomparing the incidence of infusion phlebitisduring continuous and cyclic peripheral parenteralnutrition. Clinical Nutrition 1991, 10(6):315-9.
185. Keys A, Brozek J, Henschel A, Mickelson O, TaylorHL. The biology of human starvation.Minneapolis: University of Minnesota Press, 1950.
186. Kind P, Dolan P, Gudex C, Williams A. Variations inpopulation health status: results from a UnitedKingdom national questionnaire survey. BMJ1998, 316(7133):736-41.
187. Knowles JB, Fairbarn MS, Wiggs BJ, Chan-Yan C,Pardy RL. Dietary supplementation andrespiratory muscle performance in patients withCOPD. Chest 1998, 93(5):977-83.
188. Kocan MJ, Hickisch SM. A comparison ofcontinuous and intermittent enteral nutrition inNICU patients. Journal of Neuroscience Nursing1986, 18(6):333-7.
189. Kohlhardt SR, Smith RC, Wright CR. Peripheralversus central intravenous nutrition: comparison oftwo delivery systems. British Journal of Surgery1994, 81(1):66-70.
190. Koretz RL, Lipman TO, Klein S. AGA technicalreview on parenteral nutrition. Gastroenterology2001, 121(4):970-1001.
191. Kortbeek JB, Haigh PI, Doig C. Duodenal versusgastric feeding in ventilated blunt traumapatients: a randomized controlled trial. Journal ofTrauma-Injury Infection & Critical Care 1999,46(6):992-6.
BIBLIOGRAPHY 163

192. Kramer RL, Van Someren JK, Qualls CR, Curet LB.Postoperative management of cesarean patients:the effect of immediate feeding on the incidenceof ileus. Obstetrics & Gynecology 1996, 88(1):29-32.
193. Kudsk KA, Croce MA, Fabian TC, Minard G, TolleyEA, Poret HA et al. Enteral versus parenteralfeeding. Effects on septic morbidity after bluntand penetrating abdominal trauma. Annals ofSurgery 1992, 215(5):503-11.
194. Kuhlemeier KV. Epidemiology and dysphagia.Dysphagia 1994, 9(4):209-17.
195. Kwok T, Woo J, Kwan M. Does low lactose milkpowder improve the nutritional intake andnutritional status of frail older Chinese peopleliving in nursing homes? Journal of Nutrition,Health & Aging 2001, 5(1):17-21.
196. Lange P, Pedersen T. Initial treatment of acutepancreatitis. Surgery, Gynecology & Obstetrics1983, 157(4):332-4.
197. Larsson J, Unosson M, Ek A, Nilsson L, ThorslundS, Bjurulf P. Effect of dietary supplement onnutritional status and clinical outcome in 501geriatric patients — a randomised study. ClinicalNutrition 1990, 9(4):179-84.
198. Lawson RM, Doshi MK, Barton JR, Cobden I. Theeffect of unselected post-operative nutritionalsupplementation on nutritional status and clinicaloutcome of orthopaedic patients. ClinicalNutrition 2003, 22(1):39-46.
199. Le Cornu KA, McKiernan FJ, Kapadia SA,Neuberger JM. A prospective randomized study ofpreoperative nutritional supplementation inpatients awaiting elective orthotopic livertransplantation. Transplantation 2000,69(7):1364-9.
200. Ledeboer M, Masclee AA, Biemond I, Lamers CB.Effect of intragastric or intraduodenaladministration of a polymeric diet on gallbladdermotility, small-bowel transit time, and hormonerelease. American Journal of Gastroenterology1998, 93(11):2089-96.
201. Lee JSW, Auyeung TW. A comparison of twofeeding methods in the alleviation of diarrhoea inolder tube-fed patients: a randomised controlledtrial. Age and Ageing 2003, 32(4):388-93.
202. Lennard-Jones JE. (1992) Positive approach tonutrition as treatment. London: Kingsfund.
203. Lennmarken C, Sandstedt S, Von Schenck H,Larsson J. The effect of starvation on skeletalmuscle function in man. Clinical Nutrition 1986,5:99-103.
204. Leslie P, Carding PN, Wilson JA. Investigation andmanagement of chronic dysphagia. BMJ 2003,326(7386):433-6.
205. Lewis MI, Belman MJ, Dorr-Uyemura L. Nutritionalsupplementation in ambulatory patients withchronic obstructive pulmonary disease. AmericanReview of Respiratory Disease 1987, 135(5):1062-8.
206. Lewis SJ, Egger M, Sylvester PA, Thomas S. Earlyenteral feeding versus “nil by mouth” aftergastrointestinal surgery: systematic review andmeta-analysis of controlled trials. BMJ 2001,323(7316):773-6.
207. Liley A, Manthorpe J. The impact of home enteraltube feeding in everyday life: a qualitative study.Health & Social Care in the Community 2003,11(5):415-22.
208. Lim ST, Choa RG, Lam KH, Wong J, Ong GB. Totalparenteral nutrition versus gastrostomy in thepreoperative preparation of patients withcarcinoma of the oesophagus. British Journal ofSurgery 1981, 68(2):69-72.
209. MacFie J, Woodcock NP, Palmer MD, Walker A,Townsend S, Mitchell CJ. Oral dietary supplementsin pre- and postoperative surgical patients: aprospective and randomized clinical trial.Nutrition 2000, 16(9):723-8.
NUTRITION SUPPORT IN ADULTS164

210. Mack LA, Kaklamanos IG, Livingstone AS, Levi JU,Robinson C, Sleeman D et al. Gastricdecompression and enteral feeding through adouble-lumen gastrojejunostomy tube improvesoutcomes after pancreaticoduodenectomy. Annalsof Surgery 2004, 240(5):845-51.
211. Mackie E. Home enteral feeding: III. A patient’sperspective. Clinical Nutrition 2001, 20 (Suppl 1):77-9.
212. MacLaren R, Kuhl DA, Gervasio JM, Brown RO,Dickerson RN, Livingston TN et al. Sequentialsingle doses of cisapride, erythromycin, andmetoclopramide in critically ill patients intolerantto enteral nutrition: a randomized, placebo-controlled, crossover study. Critical Care Medicine2000, 28(2):438-44.
213. MacLaren R, Patrick WD, Hall RI, Rocker GM,Whelan GJ, Lima JJ. Comparison of cisapride andmetoclopramide for facilitating gastric emptyingand improving tolerance to intragastric enteralnutrition in critically III, mechanically ventilatedadults. Clinical Therapeutics 2001, 23(11):1855-66.
214. MacMillan SL, Kammerer-Doak D, Rogers RG,Parker KM. Early feeding and the incidence ofgastrointestinal symptoms after major gynecologicsurgery. Obstetrics and Gynecology 2000,96(4):604-8.
215. Magnusson J, Tranberg KG, Jeppsson B,Lunderquist A. Enteral versus parenteral glucoseas the sole nutritional support after colorectalresection. A prospective, randomized comparison.Scandinavian Journal of Gastroenterology 1989,24(5):539-49.
216. Malhotra A, Mathur AK, Gupta S. Early enteralnutrition after surgical treatment of gutperforations: A prospective randomised study.Journal of Postgraduate Medicine 2004,50(2):102-6.
217. Malnutrition Advisory Group. (2000) MAGguidelines for detection and management ofmalnutrition. Maidenhead: British Association forParenteral and Enteral Nutrition (BAPEN).
218. Marchini JS, Vannucchi H, Dutra de Oliveira JE.Effect of two carbohydrate:lipid ratios of dietsenterally fed to chronic alcoholics. HumanNutrition - Clinical Nutrition 1983, 37(5):329-37.
219. Marik PE, Zaloga GP. Meta-analysis of parenteralnutrition versus enteral nutrition in patients withacute pancreatitis. BMJ 2004, 328(7453):1407-10.
220. May J, Murchan P, MacFie J, Sedman P, Donat R,Palmer D et al. Prospective study of the aetiologyof infusion phlebitis and line failure duringperipheral parenteral nutrition. British Journal ofSurgery 1996, 83(8):1091-4.
221. May J, Sedman P, Mitchell C, MacFie J. Peripheraland central parenteral nutrition: a cost-comparison analysis. Health Trends 1993,25(4):129-32.
222. McAlpine SJ, Harper J, McMurdo ME, Bolton-SmithC, Hetherington MM. Nutritional supplementationin older adults: pleasantness, preference andselection of sip-feeds. British Journal of HealthPsychology 2003, 8(Pt 1):57-66.
223. McCarter TL, Condon SC, Aguilar RC, Gibson DJ,Chen YK. Randomized prospective trial of earlyversus delayed feeding after percutaneousendoscopic gastrostomy placement. AmericanJournal of Gastroenterology 1998, 93(3):419-21.
224. McClave SA, Greene LM, Snider HL, Makk LJ,Cheadle WG, Owens NA et al. Comparison of thesafety of early enteral vs parenteral nutrition inmild acute pancreatitis. JPEN Journal of Parenteraland Enteral Nutrition 1997, 21(1):14-20.
225. McClave SA, Lukan JK, Stefater JA, Lowen CC,Looney SW, Matheson PJ et al. Poor validity ofresidual volumes as a marker for risk of aspirationin critically ill patients. Critical Care Medicine2005, 33(2):324-30.
226. McEvoy AWJ, James OFW. The effect of a dietarysupplement (Build-Up) on nutritional status inhospitalized elderly patients. Human Nutrition -Applied Nutrition 1982, 36(5):374-6.
BIBLIOGRAPHY 165

227. McManus S. Living with parenteral nutrition: apatient’s perspective. In: Total parenteral nutrition: apractical guide for nurses (Hamilton H), 2000. pp219-6. Churchill Livingstone Inc., (New York, NY).
228. McWhirter JP, Pennington CR. A comparisonbetween oral and nasogastric nutritionalsupplements in malnourished patients. Nutrition1996, 12(7-8):502-6.
229. Mercer CD, Mungara A. Enteral feeding inesophageal surgery. Nutrition 1996, 12(3):200-1.
230. Meyenfeldt MM, Stapert J, de Jong PCM, SoetersPB, Wesdorp RIC, Greep JM. TPN catheter sepsis:lack of effect of subcutaneous tunnelling of PVCcatheters on sepsis rate. JPEN Journal ofParenteral and Enteral Nutrition 1980, 4(5):514-7.
231. Milne AC, Potter J, Avenell A. Protein and energysupplementation in elderly people at risk frommalnutrition. Cochrane Database of SystematicReviews 2005, Issue 1:CD003288.
232. Mirtallo JM. (1987) Cost-effective nutrition supportNutrition in Clinical Practice 2 142-151 Abstract
233. Mirtallo JM, Lisitano RC. Designing cost-effectivenutritional support. Hospital Therapy 1986,11:69-78.
234. Mitchell SL, Buchanan JL, Littlehale S, Hamel MB.Tube-feeding versus hand-feeding nursing homeresidents with advanced dementia: a costcomparison. Journal of the American MedicalDirectors Association 2003, 4(1):27-33.
235. Montecalvo MA, Steger KA, Farber HW, Smith BF,Dennis RC, Fitzpatrick GF et al. Nutritionaloutcome and pneumonia in critical care patientsrandomized to gastric versus jejunal tubefeedings. The Critical Care Research Team. CriticalCare Medicine 1992, 20(10):1377-87.
236. Montejo JC, Grau T, Acosta J, Ruiz-Santana S,Planas M, Garcia-De-Lorenzo A et al. Multicenter,prospective, randomized, single-blind studycomparing the efficacy and gastrointestinalcomplications of early jejunal feeding with earlygastric feeding in critically ill patients. CriticalCare Medicine 2002, 30(4):796-800.
237. Moore AA, Siu A, Partridge JM, Hays RD, Adams J.A randomized trial of office-based screening forcommon problems in older persons. AmericanJournal of Medicine 1997, 102(4):371-8.
238. Moore EE, Jones TN. Benefits of immediatejejunostomy feeding after major abdominaltrauma — a prospective, randomized study.Journal of Trauma-Injury Infection & Critical Care1986, 26(10):874-81.
239. Mulder PO, Bouman JG, Gietema JA, VanRijsbergen H, Mulder NH, van der GS et al.Hyperalimentation in autologous bone marrowtransplantation for solid tumors. Comparison oftotal parenteral versus partial parenteral plusenteral nutrition. Cancer 1989, 64(10):2045-52.
240. Muller JM, Brenner U, Dienst C, Pichlmaier H.Preoperative parenteral feeding in patients withgastrointestinal carcinoma. Lancet 1982,1(8263):68-71.
241. Munro J. Value-added benefits. Nursing Times1998, 94(48):59-60.
242. Murphy MK, Black NA, Lamping DL, McKee CM,Sanderson CF, Askham J et al. Consensusdevelopment methods, and their use in clinicalguideline development. Health Technol Assess1998, 2(3):i-88.
243. National Institute for Clinical Excellence. (2003)Infection control, prevention of healthcare-associated infection in primary and communitycare - NICE Guideline. London: National Institutefor Clinical Excellence.
244. National Institute for Clinical Excellence. Eatingdisorders: core interventions in the treatment andmanagement of anorexia nervosa, bulimia nervosaand related eating disordershttp://www.nice.org.uk/pdf/cg009niceguidance.pdf
245. National Institute for Health and ClinicalExcellence. (2005) Guideline developmentmethods: information for national collaboratingcentres and guideline developers. London:National Institute for Clinical Excellence.
NUTRITION SUPPORT IN ADULTS166
246. National Patient Safety Agency. Advice to theNHS on reducing harm caused by themisplacement of nasogastric feeding tubeshttp://www.npsa.nhs.uk/health/display?contentId=3525 [accessed 1-7-2005].
247. Neumann DA, DeLegge MH. Gastric versus small-bowel tube feeding in the intensive care unit: aprospective comparison of efficacy. Critical CareMedicine 2002, 30(7):1436-8.
248. NHS Estates. Better Hospital Foodwww.betterhospitalfood.com [accessed 1-7-0005].
249. NHS Estates. Better hospital food: protectedmealtimeshttp://195.92.246.148/nhsestates/better_hospital_food/bhf_content/protected_mealtimes/overview.asp [accessed 1-7-0005].
250. NHS Executive. (2005) NHS Reference costs2004. London: NHS Executive.
251. Norton B, Homer-Ward M, Donnelly MT, Long RG,Holmes GK. A randomised prospective comparisonof percutaneous endoscopic gastrostomy andnasogastric tube feeding after acute dysphagicstroke. BMJ 1996, 312(7022):13-6.
252. Nursing and Midwifery Practice DevelopmentUnit. (2002) Nutrition assessment and referral inthe care of adults in hospital: best practicestatement. Edinburgh: NHS Scotland.
253. O’Brien DD, Hodges RE, Day AT, Waxman KS,Rebello T. Recommendations of nutrition supportteam promote cost containment. JPEN Journal ofParenteral and Enteral Nutrition 1986, 10(3):300-2.
254. Ochoa JB, Magnuson B, Swintowsky M, Loan T,Boulanger B, McClain C et al. Long-term reductionin the cost of nutritional intervention achieved bya nutrition support service. Nutrition in ClinicalPractice 2000, 15(4):174-80.
255. Odderson IR, Keaton JC, McKenna BS. Swallowmanagement in patients on an acute strokepathway: quality is cost effective. Archives of PhysicalMedicine and Rehabilitation 1995, 76(12):1130-3.
256. Ofman J, Koretz RL. Clinical economics review:nutritional support. Alimentary Pharmacology &Therapeutics 1997, 11(3):453-71.
257. Olveira FG, Mancha DI, Gonzalez-Romero S,Goiburu ME, Munoz Aguilar A, Garcia AlmeidaJM. [The quality of the care in parenteralnutrition: the benefits after the incorporation of anutritional support team]. Nutricion Hospitalaria2000, 15(3):118-22.
258. Ortiz H, Armendariz P, Yarnoz C. Is earlypostoperative feeding feasible in elective colonand rectal surgery? International Journal ofColorectal Disease 1996, 11(3):119-21.
259. Ott L, Annis K, Hatton J, McClain M, Young B.Postpyloric enteral feeding costs for patients withsevere head injury: blind placement, endoscopy,and PEG/J versus TPN. Journal of Neurotrauma1999, 16(3):233-42.
260. Otte KE, Ahlburg P, D’Amore F, Stellfeld M.Nutritional repletion in malnourished patientswith emphysema. JPEN Journal of Parenteral andEnteral Nutrition 1989, 13(2):152-6.
261. Pacelli F, Bossola M, Papa V, Malerba M, ModestiC, Sgadari A et al. Enteral vs parenteral nutritionafter major abdominal surgery: an even match.Archives of Surgery 2001, 136(8):933-6.
262. Page CP, Carlton PK, Andrassy RJ, Feldtman RW,Shield CF, III. Safe, cost-effective postoperativenutrition. Defined formula diet via needle-catheterjejunostomy. American Journal of Surgery 1979,138(6):939-45.
263. Page RD, Oo AY, Russell GN, Pennefather SH.Intravenous hydration versus naso-jejunal enteralfeeding after esophagectomy: a randomised study.European Journal of Cardio-Thoracic Surgery2002, 22(5):666-72.
264. Palmer D, MacFie J, Bradford IM, Murchan PM,Harrison J, Mitchell CJ. Administration ofperipheral parenteral nutrition: a prospectivestudy comparing rotation of venous access siteswith ultrafine cannulas. Clinical Nutrition 1996,15(6):311-5.
BIBLIOGRAPHY 167

265. Pang F, Dewilde S, Ossa D, Hutton J, Edington J.Modelling the economic impact of nutritionalsupplements in the UK in pre-operative patients.[unpublished data] 2004.
266. Pang F, Saleh A, Girod I, Edington J. Determiningthe prevalence and economics of enteral tubefeeding in patients at nutritional risk in the UKusing retrospective database methodology.[unpublished data] 2004.
267. Park RH, Allison MC, Lang J, Spence E, Morris AJ,Danesh BJ et al. Randomised comparison ofpercutaneous endoscopic gastrostomy andnasogastric tube feeding in patients withpersisting neurological dysphagia. BMJ 1992,304(6839):1406-9.
268. Patolia DS, Hilliard RLM, Toy EC, Baker B. Earlyfeeding after cesarean: randomized trial.Obstetrics & Gynecology 2001, 98(1):113-6.
269. Paton NI, Chua Y-K, Earnest A, Chee CBE.Randomized controlled trial of nutritionalsupplementation in patients with newlydiagnosed tuberculosis and wasting. AmericanJournal of Clinical Nutrition 2004, 80(2):460-5.
270. Payette H, Boutier V, Coulombe C, Gray-Donald K.Benefits of nutritional supplementation in free-living, frail, undernourished elderly people: aprospective randomized community trial. Journalof the American Dietetic Association 2002,102(8):1088-95.
271. Peake HJ, Evans S, Chambers A, Riches C, FrostCG. Nutritional supplementation: how much dopeople drink [abstract]. Proceedings of theNutrition Society 1998, 57:94a.
272. Pearl ML, Frandina M, Mahler L, Valea FA,DiSilvestro PA, Chalas E. A randomized controlledtrial of a regular diet as the first meal ingynecologic oncology patients undergoingintraabdominal surgery. Obstetrics & Gynecology2002, 100(2):230-4.
273. Pearl ML, Valea FA, Fischer M, Mahler L, Chalas E.A randomized controlled trial of earlypostoperative feeding in gynecologic oncologypatients undergoing intra-abdominal surgery.Obstetrics & Gynecology 1998, 92(1):94-7.
274. Peck MD, Alexander JW, Gonce SJ, Miskell PW.Low protein diets improve survival from peritonitisin guinea pigs. Annals of Surgery 1989,209(4):448-54.
275. Penn ND, Purkins L, Kelleher J, Heatley RV,Mascie-Taylor BH, Belfield PW. The effect ofdietary supplementation with vitamins A, C and Eon cell-mediated immune function in elderly long-stay patients: a randomized controlled trial. Ageand Ageing 1991, 20(3):169-74.
276. Pichard C, Roulet M. Constant rate enteralnutrition in bucco-pharyngeal cancer care. Ahighly efficient nutritional support system.Clinical Otolaryngology & Allied Sciences 1984,9(4):209-14.
277. PINNT (Patients on Intravenous and NasogastricNutrition Therapy). Ensuring equity of access andquality of care patients’ perspectives and resultsof our national survey. PINNT QuarterlyNewsletter 2002,(March):10-1.
278. Png D-JC, Ong CL, Chan S. Surgical nutritionalteam and its impact on total parenteral nutritionin the National University Hospital, Singapore.International Journal of Clinical Practice 1997,51(6):350-2.
279. Potter JM, Roberts MA, McColl JH, Reilly JJ.Protein energy supplements in unwell elderlypatients — a randomized controlled trial. JPENJournal of Parenteral and Enteral Nutrition 2001,25(6):323-9.
280. Powers DA, Brown RO, Cowan GS, Jr., Luther RW,Sutherland DA, Drexler PG. Nutritional supportteam vs nonteam management of enteralnutritional support in a Veterans AdministrationMedical Center teaching hospital. JPEN Journal ofParenteral and Enteral Nutrition 1986, 10(6):635-8.
NUTRITION SUPPORT IN ADULTS168

281. Pupelis G, Selga G, Austrums E, Kaminski A.Jejunal feeding, even when instituted late,improves outcomes in patients with severepancreatitis and peritonitis. Nutrition 2001,17(2):91-4.
282. Rabeneck L, Palmer A, Knowles JB, Seidehamel RJ,Harris CL, Merkel KL et al. A randomizedcontrolled trial evaluating nutrition counselingwith or without oral supplementation inmalnourished HIV-infected patients. Journal ofthe American Dietetic Association 1998,98(4):434-8.
283. Rana SK, Bray J, Menzies-Gow N, Jameson J,James JJP, Frost P et al. Short term benefits ofpost-operative oral dietary supplements insurgical patients. Clinical Nutrition 1992, 11:337-44.
284. Randolph AG, Cook DJ, Gonzales CA, Brun-Buisson C. Tunneling short-term central venouscatheters to prevent catheter-related infection: ameta-analysis of randomized, controlled trials.Critical Care Medicine 1998, 26(8):1452-7.
285. Ravasco P, Monteiro-Grillo I, Vidal PM, Camilo ME.Dietary Counseling Improves Patient Outcomes: AProspective, Randomized, Controlled Trial inColorectal Cancer Patients UndergoingRadiotherapy. Journal of Clinical Oncology 2005,23(7):1431-8.
286. Ray SA, Rainsbury RM. Patient tolerance of theearly introduction of oral fluids after laparotomy.Annals of the Royal College of Surgeons ofEngland 1993, 75(3):157-60.
287. Reddy P, Malone M. Cost and outcome analysis ofhome parenteral and enteral nutrition. JPENJournal of Parenteral and Enteral Nutrition 1998,22(5):302-10.
288. Reeds PJ, Fjeld CR, Jahoor F. Do the differencesbetween the amino acid compositions of acute-phase and muscle proteins have a bearing onnitrogen loss in traumatic states? J Nutr 1994,124(6):906-10.
289. Reignier J, Bensaid S, Perrin-Gachadoat D, BurdinM, Boiteau R, Tenaillon A. Erythromycin and earlyenteral nutrition in mechanically ventilatedpatients. Critical Care Medicine 2002,30(6):1237-41.
290. Reilly C. Nutritional trace elements. Oxford:Blackwell Publishing, 2004.
291. Reissman P, Teoh TA, Cohen SM, Weiss EG,Nogueras JJ, Wexner SD. Is early oral feeding safeafter elective colorectal surgery? A prospectiverandomized trial. Annals of Surgery 1995,222(1):73-7.
292. Reynolds JV, Kanwar S, Welsh FK, Windsor AC,Murchan P, Barclay GR et al. 1997 Harry M. VarsResearch Award. Does the route of feeding modifygut barrier function and clinical outcome inpatients after major upper gastrointestinalsurgery? JPEN Journal of Parenteral and EnteralNutrition 1997, 21(4):196-201.
293. Rhodes JM, Carroll A, Dawson J. A controlled trialof fixed versus tailored calorie intake in patientsreceiving intravenous feeding after abdominalsurgery. Clinical Nutrition 1985, 4(3):169-74.
294. Roberge C, Tran M, Massoud C, Poirée B, Duval N,Damecour E et al. Quality of life and homeenteral tube feeding: a French prospective studyin patients with head and neck or oesophagealcancer. British Journal of Cancer 2000,82(2):263-9.
295. Roberts MF, Levine GM. Nutrition support teamrecommendations can reduce hospital costs.Nutrition in Clinical Practice 1992, 7(5):227-30.
296. Roberts S, Miller J, Pineiro L, Jennings L. Totalparenteral nutrition vs oral diet in autologoushematopoietic cell transplant recipients. BoneMarrow Transplantation 2003, 32(7):715-21.
297. Royal College of Physicians. (2002) Nutrition andpatients: a doctor’s responsibility. London: RoyalCollege of Physicians of London.
BIBLIOGRAPHY 169

298. Ryan JA, Jr., Page CP, Babcock L. Earlypostoperative jejunal feeding of elemental diet ingastrointestinal surgery. American Surgeon 1981,47(9):393-403.
299. Rypkema G, Adang E, Dicke H, Naber T, De SwartB, Disselhorst L et al. Cost-effectiveness of aninterdisciplinary intervention in geriatricinpatients to prevent malnutrition. Journal ofNutrition, Health & Aging 2004, 8(2):122-7.
300. Sackett DL, Straus SE, Richardson WS, RosenbergW, Haynes RB. Evidence based medicine: how topractice and teach EBM. Edinburgh: ChurchillLivingstone, 2000.
301. Sagar S, Harland P, Shields R. Early postoperativefeeding with elemental diet. BMJ 1979,1(6159):293-5.
302. Saluja SS, Kaur N, Shrivastava UK. Enteralnutrition in surgical patients. Surgery Today 2002,32(8):672-8.
303. Sand J, Luostarinen M, Matikainen M. Enteral orparenteral feeding after total gastrectomy:prospective randomised pilot study. EuropeanJournal of Surgery 1997, 163(10):761-6.
304. Sandstrom R, Drott C, Hyltander A, Arfvidsson B,Schersten T, Wickstrom I et al. The effect ofpostoperative intravenous feeding (TPN) onoutcome following major surgery evaluated in arandomized study. Annals of Surgery 1993,217(2):185-95.
305. Sandstrom R, Hyltander A, Korner U, Lundholm K.The effect on energy and nitrogen metabolism bycontinuous, bolus, or sequential infusion of adefined total parenteral nutrition formulation inpatients after major surgical procedures. JPENJournal of Parenteral and Enteral Nutrition 1995,19(5):333-40.
306. Saudny-Unterberger H, Martin JG, Gray-Donald K.Impact of nutritional support on functional statusduring an acute exacerbation of chronicobstructive pulmonary disease. American Journalof Respiratory and Critical Care Medicine 1997,156(3 Pt 1):794-9.
307. Scherbaum V, Furst P. New concepts on nutritionalmanagement of severe malnutrition: the role ofprotein. Current Opinion in Clinical Nutrition andMetabolic Care 2000, 3(1):31-8.
308. Schilder JM, Hurteau JA, Look KY, Moore DH, RaffG, Stehman FB et al. A prospective controlled trialof early postoperative oral intake following majorabdominal gynecologic surgery. GynecologicOncology 1997, 67(3):235-40.
309. Schofield WN. Predicting basal metabolic rate,new standards and review of previous work.Human nutrition Clinical nutrition 1985,39(Suppl 1):5-41.
310. Schroeder D, Gillanders L, Mahr K, Hill GL. Effectsof immediate postoperative enteral nutrition onbody composition, muscle function, and woundhealing. JPEN Journal of Parenteral and EnteralNutrition 1991, 15(4):376-83.
311. Scolapio JS, Picco MF, Tarrosa VB. Enteral versusparenteral nutrition: the patient’s preference.JPEN Journal of Parenteral and Enteral Nutrition2002, 26(4):248-50.
312. Scott F, Beech R, Smedley F, Timmis L, Stokes E,Jones P et al. A prospective randomised controlledsingle-blind trial of the costs and consequences ofsystematic nutrition team follow-up over 12months after percutaneous endoscopicgastrostomy. [unpublished data] 2003.
313. Seri S, Aquilio E. Effects of early nutritionalsupport in patients with abdominal trauma.Italian Journal of Surgical Sciences 1984,14(3):223-7.
314. Serpa LF, Kimura M, Faintuch J, Ceconello I.Effects of continuous versus bolus infusion ofenteral nutrition in critical patients. Revista doHospital das Clinicas; Faculdade de Medicina DaUniversidade de Sao Paulo 2003, 58(1):9-14.
315. Seven H, Calis AB, Turgut S. A randomizedcontrolled trial of early oral feeding inlaryngectomized patients. Laryngoscope 2003,113(6):1076-9.
NUTRITION SUPPORT IN ADULTS170

316. Shildt RA, Rose M, Stollman L, Bell B.Organization of the nutritional support service ata medical center: one year’s experience. MilitaryMedicine 1982, 147(1):55-8.
317. Shirabe K, Matsumata T, Shimada M, Takenaka K,Kawahara N, Yamamoto K et al. A comparison ofparenteral hyperalimentation and early enteralfeeding regarding systemic immunity after majorhepatic resection — the results of a randomizedprospective study. Hepato-Gastroenterology 1997,44(13):205-9.
318. Shukla HS, Rao RR, Banu N, Gupta RM, Yadav RC.Enteral hyperalimentation in malnourishedsurgical patients. Indian Journal of MedicalResearch 1984, 80:339-46.
319. Silver HJ. The lived experience of home totalparenteral nutrition: an online qualitative inquirywith adults, children, and mothers. Nutrition inClinical Practice 2004, 19(3):297-304.
320. Simpson F, Doig GS. Parenteral vs. enteral nutritionin the critically ill patient: a meta-analysis of trialsusing the intention to treat principle. Intensive CareMedicine 2005, 31(1):12-23.
321. Singh G, Ram RP, Khanna SK. Early postoperativeenteral feeding in patients with nontraumaticintestinal perforation and peritonitis. Journal ofthe American College of Surgeons 1998,187(2):142-6.
322. Sizer T. (1996) Standards and guidelines fornutritional support of patients in hospitals.Maidenhead: British Association for Parenteraland Enteral Nutrition.
323. Skiest DJ, Khan N, Feld R, Metersky ML. The roleof enteral feeding in gastric colonisation: Arandomised controlled trial comparing continuousto intermittent enteral feeding in mechanicallyventilated patients. Clinical Intensive Care 1996,7(3):138-43.
324. Skipper A, Gregoire MB. Liquid nutritionalsupplements: who should be involved inselection? Topics in Clinical Nutrition 2001,16(3):44-50.
325. Smedley F, Bowling T, James M, Stokes E, GoodgerC, O’Connor O et al. A prospective randomisedcontrolled trial of the effects of pre- and post-operative oral nutritional supplements on clinical course and cost of care. [unpublisheddata] 2003.
326. Smedley F, Bowling T, James M, Stokes E, GoodgerC, O’Connor O et al. Randomized clinical trial ofthe effects of preoperative and postoperative oralnutritional supplements on clinical course andcost of care. British Journal of Surgery 2004,91(8):983-90.
327. Smith RC, Hartemink R. Improvement ofnutritional measures during preoperativeparenteral nutrition in patients selected by theprognostic nutritional index: a randomizedcontrolled trial. JPEN Journal of Parenteral andEnteral Nutrition 1988, 12(6):587-91.
328. Smith RC, Hartemink RJ, Hollinshead JW, GillettDJ. Fine bore jejunostomy feeding following majorabdominal surgery: a controlled randomizedclinical trial. British Journal of Surgery 1985,72(6):458-61.
329. Smithard DG, O’Neill PA, England RE, Park CL,Wyatt R, Martin DF et al. The natural history ofdysphagia following a stroke. Dysphagia 1997,12(4):188-93.
330. Stableforth PG. Supplement feeds and nitrogenand calorie balance following femoral neckfracture. British Journal of Surgery 1986,73(8):651-5.
331. Steed HL, Capstick V, Flood C, Schepansky A,Schulz J, Mayes DC. A randomized controlled trialof early versus “traditional” postoperative oralintake after major abdominal gynecologic surgery.American Journal of Obstetrics & Gynecology2002, 186(5):861-5.
332. Steevens EC, Lipscomb AF, Poole G, V, Sacks GS.Comparison of continuous vs intermittentnasogastric enteral feeding in trauma patients:perceptions and practice. Nutrition in ClinicalPractice 2002, 17(2):118-22.
BIBLIOGRAPHY 171

333. Stein J, Schulte-Bockholt A, Sabin M, Keymling M.A randomized prospective trial of immediate vs.next-day feeding after percutaneous endoscopicgastrostomy in intensive care patients. IntensiveCare Medicine 2002, 28(11):1656-60.
334. Stewart BT, Woods RJ, Collopy BT, Fink RJ, MackayJR, Keck JO. Early feeding after elective opencolorectal resections: a prospective randomizedtrial. Australian and New Zealand Journal ofSurgery 1998, 68(2):125-8.
335. Stratton RJ, Green CJ, Elia M. Disease-relatedmalnutrition: an evidence-based approach. Oxford:CABI Publishing, 2003.
336. Stratton RJ, Hackston A, Longmore D, Dixon R,Price S, Stroud M et al. Malnutrition in hospitaloutpatients and inpatients: prevalence, concurrentvalidity and ease of use of the ‘malnutritionuniversal screening tool’ (‘MUST’) for adults.British Journal of Nutrition 2004, 92(5):799-808.
337. Stratton RJ, Hackston AJ, Price S, Joseph K, Elia M.Concurrent validity of the newly developedMalnutrition Universal Screening Tool (‘MUST’)with the Mini Nutritional Assessment andSubjective Global Assessment tools. [unpublisheddata] 2004.
338. Strong RM, Condon SC, Solinger MR, Namihas BN,Ito-Wong LA, Leuty JE. Equal aspiration rates frompostpylorus and intragastric-placed small-borenasoenteric feeding tubes: a randomized,prospective study. JPEN Journal of Parenteral andEnteral Nutrition 1992, 16(1):59-63.
339. Sullivan DH, Nelson CL, Bopp MM, Puskarich-MayCL, Walls RC. Nightly enteral nutrition support ofelderly hip fracture patients: a phase I trial.Journal of the American College of Nutrition1998, 17(2):155-61.
340. Sullivan DH, Nelson CL, Klimberg VS, Bopp MM.Nightly enteral nutrition support of elderly hipfracture patients: a pilot study. Journal of theAmerican College of Nutrition 2004, 23(6):683-91.
341. Swails WS, Babineau TJ, Ellis FH, Kenler AS, ForseRA. The role of enteral jejunostomy feeding afteresophagogastrectomy: a prospective, randomizedstudy. Diseases of the Esophagus 1995, 8(3):193-9.
342. Szeluga DJ, Stuart RK, Brookmeyer R, UtermohlenV, Santos GW. Nutritional support of bone marrowtransplant recipients: a prospective, randomizedclinical trial comparing total parenteral nutritionto an enteral feeding program. Cancer Research1987, 47(12):3309-16.
343. The FOOD Trial Collaboration. Effect of timing andmethod of enteral tube feeding for dysphagicstroke patients (FOOD): a multicentre randomisedcontrolled trial. Lancet 2005, 365(9461):764-72.
344. The FOOD Trial Collaboration. Routine oralnutritional supplementation for stroke patients inhospital (FOOD): a multicentre randomisedcontrolled trial. Lancet 2005, 365(9461):755-63.
345. The Parenteral and Enteral Nutrition Group of theBritish Dietetic Association (PEN Group). A pocketguide to clinical nutrition. London: PEN GroupPublications, 2004.
346. The Veterans Affairs Total Parenteral NutritionCooperative Study Group. Perioperative totalparenteral nutrition in surgical patients. NewEngland Journal of Medicine 1991, 325(8):525-32.
347. Thomas B. Manual of dietetic practice. Oxford:Blackwell, 2001.
348. Thompson BR, Julian TB, Stremple JF. Perioperativetotal parenteral nutrition in patients withgastrointestinal cancer. Journal of SurgicalResearch 1981, 30(5):497-500.
349. Tidermark J, Ponzer S, Carlsson P, Söderqvist A,Brismar K, Tengstrand B et al. Effects of protein-rich supplementation and nandrolone in leanelderly women with femoral neck fractures.Clinical Nutrition 2004, 23(4):587-96.
NUTRITION SUPPORT IN ADULTS172

350. Timsit JF, Bruneel F, Cheval C, Mamzer M-F,Garrouste-Orgeas M, Wolff M et al. Use of tunneledfemoral catheters to prevent catheter-relatedinfection. A randomized, controlled trial. Annals ofInternal Medicine 1999, 130(9):729-35.
351. Timsit JF, Sebille V, Farkas JC, Misset B, Martin JB,Chevret S et al. Effect of subcutaneous tunnelingon internal jugular catheter-related sepsis incritically ill patients: a prospective randomizedmulticenter study. JAMA : the Journal of theAmerican Medical Association 1996,276(17):1416-20.
352. Tkatch L, Rapin CH, Rizzoli R, Slosman D,Nydegger V, Vasey H et al. Benefits of oral proteinsupplementation in elderly patients with fractureof the proximal femur. Journal of the AmericanCollege of Nutrition 1992, 11(5):519-25.
353. Todorovic V, Russell C, Stratton R, Ward J, Elia M.(2003) The ‘MUST’ explanatory booklet: a guideto the ‘Malnutrition Universal Screening Tool’(‘MUST’) for adults. Redditch: British Associationfor Parenteral and Enteral Nutrition (BAPEN).
354. Traeger SM, Williams GB, Milliren G, Young DS,Fisher M, Haug MT, III. Total parenteral nutritionby a nutrition support team: improved quality ofcare. JPEN Journal of Parenteral and EnteralNutrition 1986, 10(4):408-12.
355. Trice S, Melnik G, Page CP. Complications andcosts of early postoperative parenteral versusennteral nutrition in trauma patients. Nutrition inClinical Practice 1997, 12(3):114-9.
356. Trudeau E, Dubé L. Moderators and determinantsof satisfaction with diet counseling for patientsconsuming a therapeutic diet. Journal of theAmerican Dietetic Association 1995, 95(1):34-9.
357. Trujillo EB, Young LS, Chertow GM, Randall S,Clemons T, Jacobs DO et al. Metabolic andmonetary costs of avoidable parenteral nutritionuse. JPEN Journal of Parenteral and EnteralNutrition 1999, 23(2):109-13.
358. Twomey PL, Patching SC. Cost-effectiveness ofnutritional support. JPEN Journal of Parenteraland Enteral Nutrition 1985, 9(1):3-10.
359. Unosson M, Larsson J, Ek AC, Bjurulf P. Effects ofdietary supplement on functional condition andclinical outcome measured with a modifiedNorton scale. Clinical Nutrition 1992, 11(3):134-9.
360. van Berge Henegouwen MI, Akkermans LM, vanGulik TM, Masclee AA, Moojen TM, Obertop H etal. Prospective, randomized trial on the effect ofcyclic versus continuous enteral nutrition onpostoperative gastric function after pylorus-preserving pancreatoduodenectomy. Annals ofSurgery 1997, 226(6):677-85.
361. van Bokhorst-De Van Der Schueren MA, Quak JJ,von Blomberg-van der Flier BM, Kuik DJ,Langendoen SI, Snow GB et al. Effect ofperioperative nutrition, with and without argininesupplementation, on nutritional status, immunefunction, postoperative morbidity, and survival inseverely malnourished head and neck cancerpatients. American Journal of Clinical Nutrition2001, 73(2):323-32.
362. van den Berghe G, Wouters P, Weekers F, VerwaestC, Bruyninckx F, Schetz M et al. Intensive insulintherapy in the critically ill patients. New EnglandJournal of Medicine 2001, 345(19):1359-67.
363. Vermeeren MAP, Wouters EFM, Geraerts-KeerisAJW, Schols AMWJ. Nutritional support inpatients with chronic obstructive pulmonarydisease during hospitalization for an acuteexacerbation; a randomized controlled feasibilitytrial. Clinical Nutrition 2004, 23(5):1184-92.
364. Vlaming S, Biehler A, Hennessey EM, Jamieson CP,Chattophadhyay S, Obeid OA et al. Should thefood intake of patients admitted to acute hospitalservices be routinely supplemented? Arandomized placebo controlled trial. ClinicalNutrition 2001, 20(6):517-26.
BIBLIOGRAPHY 173

365. Volkert D, Hubsch S, Oster P, Schlierf G. Nutritionalsupport and functional status in undernourishedgeriatric patients during hospitalization and 6-month follow-up. Aging-Clinical & ExperimentalResearch 1996, 8(6):386-95.
366. von Meyenfeldt MF, Meijerink WJHJ, RouflartMMJ, Buil-Maassen MTHJ, Soeters PB.Perioperative nutritional support: a randomisedclinical trial. Clinical Nutrition 1992, 11(4):180-6.
367. Watters JM, Kirkpatrick SM, Norris SB, Shamji FM,Wells GA. Immediate postoperative enteralfeeding results in impaired respiratory mechanicsand decreased mobility. Annals of Surgery 1997,226(3):369-77.
368. Weinsier RL, Heimburger DC, Samples CM, DimickAR, Birch R. Cost containment: a contribution ofaggressive nutritional support in burn patients.Journal of Burn Care & Rehabilitation 1985,6(5):436-41.
369. Weinstein L, Dyne PL, Duerbeck NB. The PROEFdiet — a new postoperative regimen for oral earlyfeeding. American Journal of Obstetrics &Gynecology 1993, 168(1 Pt 1):128-31.
370. Welsh Assembly Government. (2003)Fundamentals of care: guidance for health andsocial care staff. Cardiff: Welsh AssemblyGovernment.
371. Whelan K. Inadequate fluid intakes in dysphagicacute stroke. Clinical Nutrition 2001, 20(5):423-8.
372. Wicks C, Somasundaram S, Bjarnason I, MenziesIS, Routley D, Potter D et al. Comparison ofenteral feeding and total parenteral nutritionafter liver transplantation. Lancet 1994,344(8926):837-40.
373. Wilson B, Fernandez-Madrid A, Hayes A, HermannK, Smith J, Wassell A. Comparison of the effectsof two early intervention strategies on the healthoutcomes of malnourished hemodialysis patients.Journal of Renal Nutrition 2001, 11(3):166-71.
374. Windsor JA, Knight GS, Hill GL. Wound healingresponse in surgical patients: recent food intake ismore important than nutritional status. BritishJournal of Surgery 1988, 75(2):135-7.
375. Woo J, Ho SC, Mak YT, Law LK, Cheung A.Nutritional status of elderly patients duringrecovery from chest infection and the role ofnutritional supplementation assessed by aprospective randomized single-blind trial. Age andAgeing 1994, 23(1):40-8.
376. Woodcock NP, Zeigler D, Palmer MD, Buckley P,Mitchell CJ, MacFie J. Enteral versus parenteralnutrition: a pragmatic study. Nutrition 2001,17(1):1-12.
377. Woolfson AMJ, Smith JAR. Elective nutritionalsupport after major surgery: a prospectiverandomised trial. Clinical Nutrition 1989, 8(1):15-21.
378. World Health Organization. (2002) Nationalcancer control programmes: policies andguidelines. Geneva: WHO.
379. Wouters-Wesseling W, Wouters AEJ, Kleijer CN,Bindels JG, de Groot CPMG, van Staveren WA.Study of the effect of a liquid nutritionsupplement on the nutritional status of psycho-geriatric nursing home patients. European Journalof Clinical Nutrition 2002, 56(3):245-51.
380. Yavagal DR, Karnad DR, Oak JL. Metoclopramidefor preventing pneumonia in critically ill patientsreceiving enteral tube feeding: a randomizedcontrolled trial. Critical Care Medicine 2000,28(5):1408-11.
381. Yeo CJ, Barry MK, Sauter PK, Sostre S, LillemoeKD, Pitt HA et al. Erythromycin accelerates gastricemptying after pancreaticoduodenectomy. Aprospective, randomized, placebo-controlled trial.Annals of Surgery 1993, 218(3):229-37.
382. Zhao G, Wang CY, Wang F, Xiong JX. Clinical studyon nutrition support in patients with severe acutepancreatitis. World Journal of Gastroenterology2003, 9(9):2105-8.
NUTRITION SUPPORT IN ADULTS174

383. Zhu W, Zhang W, Zhao Z, Feng P, Huang Q, Cen Qet al. The effect of early enteral nutritive supporton patients after esophageal and gastricoperation. Chinese Journal of ClinicalRehabilitation 2003, 7(1):146-7.
384. Ziegler SW. Living on nutritional support. Onepatients’ perspective. Nutrition in Clinical Practice1989, 4(2):57-61.
BIBLIOGRAPHY 175