nutrition and breast cancer prognosis: the heal cohort · nutrition and breast cancer prognosis:...
TRANSCRIPT
Nutrition and Breast Cancer Prognosis: the HEAL Cohort
Marian L. Neuhouser, PhD, RD
Anne McTiernan, MD, PhD
Fred Hutchinson Cancer Research Center October 21, 2010

Why Study Nutrition in Breast Cancer Survivor Cohorts?
• Survival numbers and duration increasing• Long-term treatment effects increasing• Excess or deficit of body mass are associated
with poorer prognosis• Survivors want to know what they can do• Nutritional effects on biology of
cure/stabilization/progression not established• Few adequately powered randomized trials
have been funded

5 year relative survival rates – 1999-2005
CA; Cancer J Clin2010

Prognostic Effect of Body Size in Early Stage Breast Cancer
BMI (kg/m2)
Estim
ated
Rel
ativ
e R
isk
of A
dver
se E
vent
20 30 40 50
05
1015
25 35 45 55
Distant Recurrence, p=0.0005
Death, p=0.0007
Goodwin JCO 2002

Contralateral Breast Cancer & Overweight/Obesity (n=15,000)
Majed et al. Br Ca Res Treat 2010 [epub Sept]

BMI and Recurrences: ATAC Trial BMI and Recurrences: ATAC Trial
.
Eligibility Criteria:
Postmenopausal women
Early breast cancer
ER+ or PR+
R A N D O M I Z E
R A N D O M I Z E
Anastrazole 1 mgAnastrazole 1 mg
Anastrazole 1 mg +Tamoxifen 20 mgAnastrazole 1 mg +Tamoxifen 20 mg
(n = 4,939 with baseline BMI data)
Tamoxifen 20 mgTamoxifen 20 mg
100
MONTHS
100
MONTHS
Sestak et al. JCO 2010; 28(21):3411-5.

All Breast Cancer Recurrences According to BMI (ATAC Trial Participants, N~5000)
Sestak I et al. JCO 2010;28:3411-3415
©2010 by American Society of Clinical Oncology

Hazard Plots for Anastrozole vs Tamoxifen by BMI: All & Distant Recurrences
Sestak I et al. JCO 2010;28:3411-3415
©2010 by American Society of Clinical Oncology
HEAL: Health, Eating, Activity and Lifestyle StudyCollaboration between National Cancer
Institute and three SEER Registries
Western WashingtonNew MexicoLos Angeles

HEAL: Health, Eating, Activity and Lifestyle StudyExamine associations between health
behaviors, clinical characteristics and a variety of potential mechanisms
sex hormones, C-peptide, IGFs, vitamin D, inflammatory markers
Examine longitudinal relationships of weight, diet and physical activity with breast cancer survivorship

HEAL Design and Data CollectionBaseline 6-8 months post diagnosis
Survey and ExamN = 1,183, Stg 0-IIIa, 1997-99- 615 New Mexico, Hispanic & non-Hispanic White- 202 Washington, primarily White- 366 Los Angeles, African-American
30 months post diagnosis Survey, Exam, & Follow-Up
Diet, dietary supplements, blood drawN = 944
Five Year Survey & Follow-upN = 817
Ten Year Survey & Follow-upN = 647
QOL Assessment~3 years post diagnosis
N = 858
Regular SEER updates: survival, recurrence, 2nd
breast primaries

HEAL – Dietary Exposures and Mechanisms
Set of exposures Set of mechanisms
Fiber Hormones
Diet Quality Inflammatory Factors
Dietary Supplements IGFs
Alcohol Insulin Resistance
BMI
Survival, recurrence, 2nd primaries

Dietary fiber and serum sex hormones in postmenopausal breast cancer survivors
Wayne et al. Br Cancer Res Treat 2008
Ptrend < 0.05

Dietary fiber and serum sex hormones in postmenopausal breast cancer survivors
Wayne et al. Br Cancer Res Treat 2008
Ptrend < 0.05
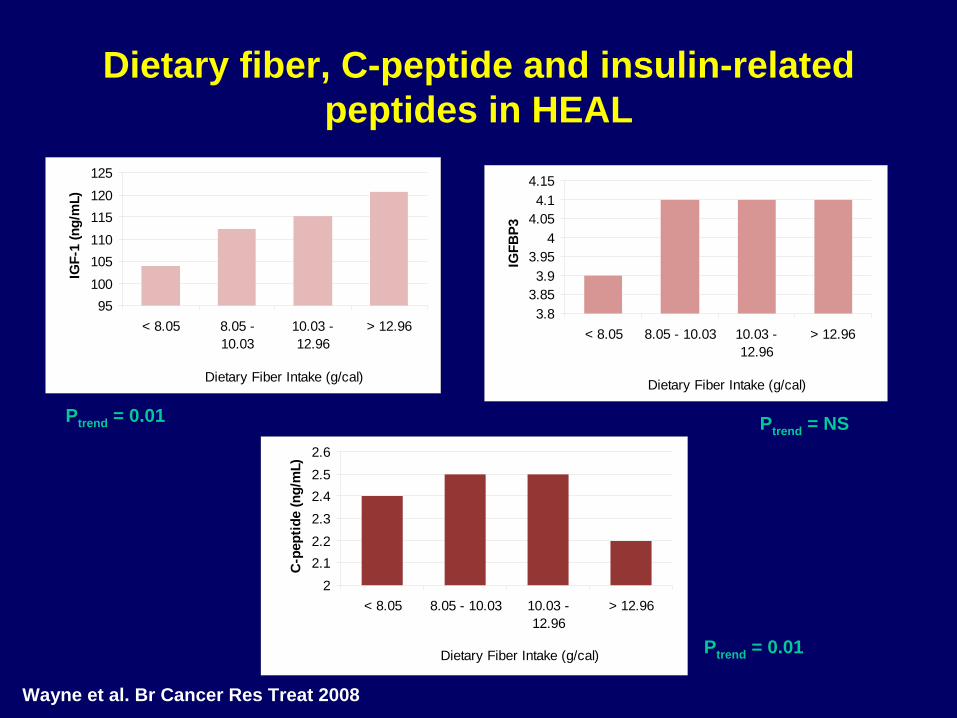
Dietary fiber, C-peptide and insulin-related peptides in HEAL
Wayne et al. Br Cancer Res Treat 2008
95100105110115120125
< 8.05 8.05 -10.03
10.03 -12.96
> 12.96
Dietary Fiber Intake (g/cal)
IGF-
1 (n
g/m
L)
3.83.853.9
3.954
4.054.1
4.15
< 8.05 8.05 - 10.03 10.03 -12.96
> 12.96
Dietary Fiber Intake (g/cal)
IGFB
P3
22.12.22.32.42.52.6
< 8.05 8.05 - 10.03 10.03 -12.96
> 12.96
Dietary Fiber Intake (g/cal)
C-p
eptid
e (n
g/m
L)
Ptrend = 0.01 Ptrend = NS
Ptrend = 0.01
Alcohol and Sex Hormones• < ½ were alcohol users • In drinkers vs. nondrinkers:
– androgens were higher (p=0.01)– leptin was lower (p=0.06)
• No association with estrogens• Some evidence for effect modification by
tamoxifen use
S Wayne et al CEBP 2008

Estrogen Levels by BMI in 505 Postmenopausal Patients (HEAL)
0
5
10
15
20
25
30
< 22 22-25 25-27.5 27.5-30 > 30
kg/m2
pg/m
l
EstroneEstradiol
P trend < 0.005
McTiernan et al. JCO 2003;21:1961-66

Testosterone Levels by BMI in 505 Postmenopausal Patients (HEAL)
020406080
100120140160180200
< 22 22-25 25-27.5 27.5-30 > 30
kg/m2
pg/m
l
Testosterone
P trend = 0.0001
McTiernan et al. JCO 2003;21:1961-66

Healthy Eating Index Scores in HEAL
S George et al CEBP 2009

SM George et al CEBP 2009
Dietary fiber, C-peptide, and insulin-related peptides and CRP in HEAL
• High vs. low dietary fiber intake was significantly associated with low serum levels of C-peptide (p = 0.01) and low estradiol (p< 0.05)
• Women in highest quartile of dietary fiber had C-peptide levels that were lower by 28% compared to women in lowest three quartiles
• Better quality diet was associated with lower C- reactive protein

Dietary fiber, C-peptide, and insulin-related peptides and CRP in HEAL
• High vs. low dietary fiber is associated with lower circulating C-reactive protein (p<0.01)
• The odds of having elevated CRP was halved among those with high fiber intake
Are these fiber-biomarker relationships associated with outcomes/survivorship?
Insulin Resistance & Prognosis
• Calculated HOMA score – (Insulin mU/mLxGlucose mmol/L)/22.5
• Explored association with survival• Followed median 76.9 months after 30-
month blood draw• Hazard ratio for breast cancer mortality
with each unit HOMA increase:– 1.12 (95% CI 1.05-1.20, p trend=0.001)
• Similar results for all-cause mortality
Duggan et al. JCO 2010 (in press)
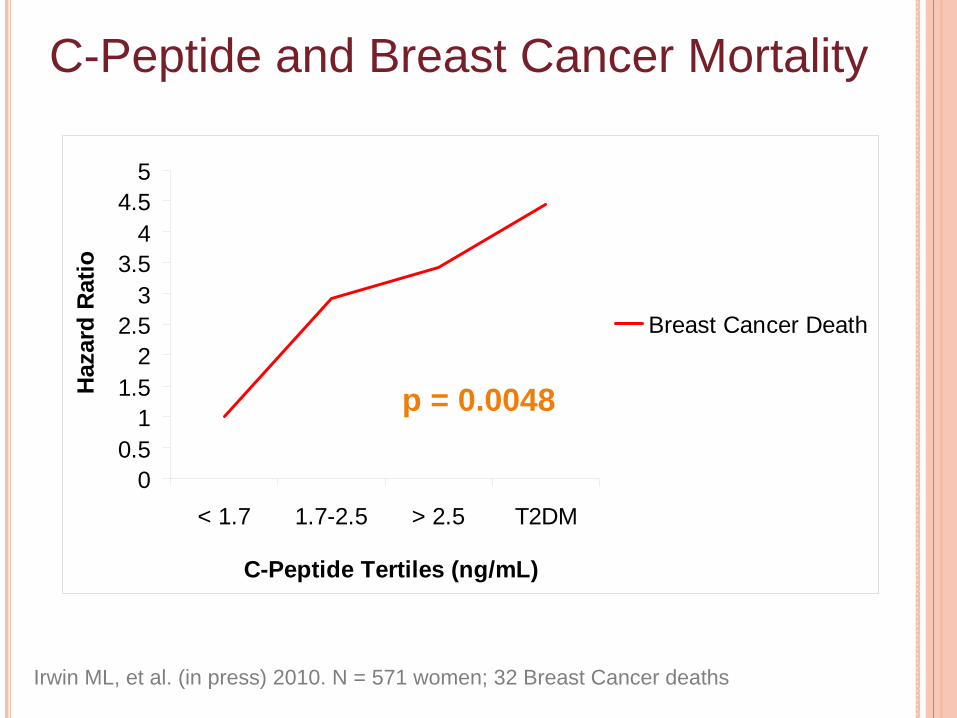
C-Peptide and Breast Cancer Mortality
00.5
11.5
22.5
33.5
44.5
5
< 1.7 1.7-2.5 > 2.5 T2DM
C-Peptide Tertiles (ng/mL)
Haz
ard
Rat
io
Breast Cancer Death
p = 0.0048
Irwin ML, et al. (in press) 2010. N = 571 women; 32 Breast Cancer deaths
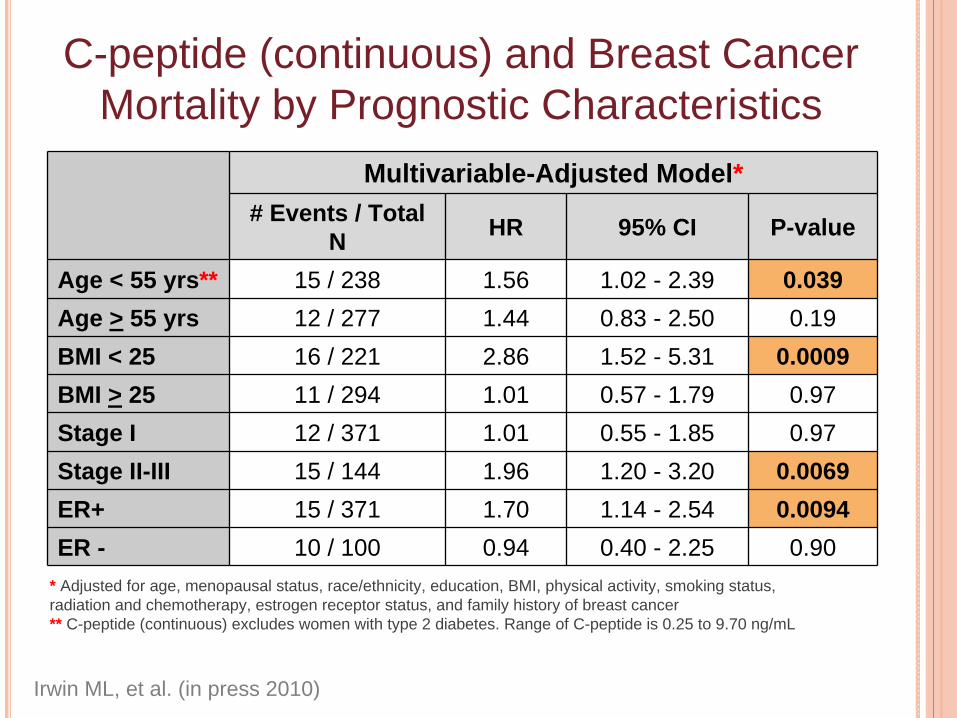
C-peptide (continuous) and Breast Cancer Mortality by Prognostic Characteristics
Multivariable-Adjusted Model*# Events / Total
N HR 95% CI P-value
Age < 55 yrs** 15 / 238 1.56 1.02 - 2.39 0.039Age > 55 yrs 12 / 277 1.44 0.83 - 2.50 0.19 BMI < 25 16 / 221 2.86 1.52 - 5.31 0.0009BMI > 25 11 / 294 1.01 0.57 - 1.79 0.97Stage I 12 / 371 1.01 0.55 - 1.85 0.97Stage II-III 15 / 144 1.96 1.20 - 3.20 0.0069 ER+ 15 / 371 1.70 1.14 - 2.54 0.0094 ER - 10 / 100 0.94 0.40 - 2.25 0.90
Irwin ML, et al. (in press 2010)
* Adjusted for age, menopausal status, race/ethnicity, education, BMI, physical activity, smoking status, radiation and chemotherapy, estrogen receptor status, and family history of breast cancer** C-peptide (continuous) excludes women with type 2 diabetes. Range of C-peptide is 0.25 to 9.70 ng/mL
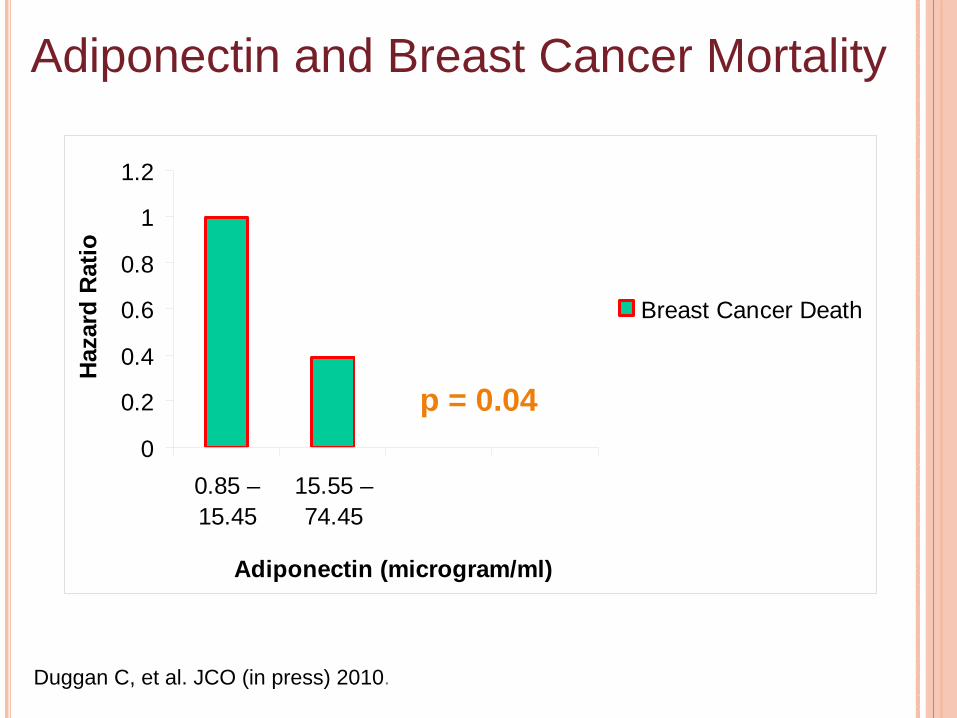
Adiponectin and Breast Cancer Mortality
0
0.2
0.4
0.6
0.8
1
1.2
0.85 –15.45
15.55 –74.45
Adiponectin (microgram/ml)
Haz
ard
Rat
io
Breast Cancer Death
p = 0.04
Duggan C, et al. JCO (in press) 2010.

C-Reactive Protein (CRP) and Breast Cancer Mortality
(HEAL, 734 Stage I-IIIa patients, follow up mean of 6 years)
0
0.5
1
1.5
2
2.5
Haz
ard
Rat
io
<1.2 mg/L1.3-3.8 mg/L> 3.8 mg/L
Pierce, et al. JCO, 2009
Ptrend = 0.01
CRP tertiles
Inflammation Biomarkers and Survival Among Breast Cancer Patients
Elevated CRP and SAA were associated with reduced survival regardless of adjustment for age, tumor stage, race, and BMI (SAA Ptrend < 0.0001; CRP Ptrend = 0.002)
Hazard ratios for SAA and CRP (highest vs. lowest tertiles) suggested a threshold rather than a dose- response relationship:• SAA HR = 3.15 (95% CI 1.73–5.65)• CRP HR = 2.27 (95% CI 1.27–4.08)
Associations were similar and still significant after adjusting for self-reported history of cardiovascular events and censoring cardiovascular disease deaths.
Pierce et al., JCO 2009
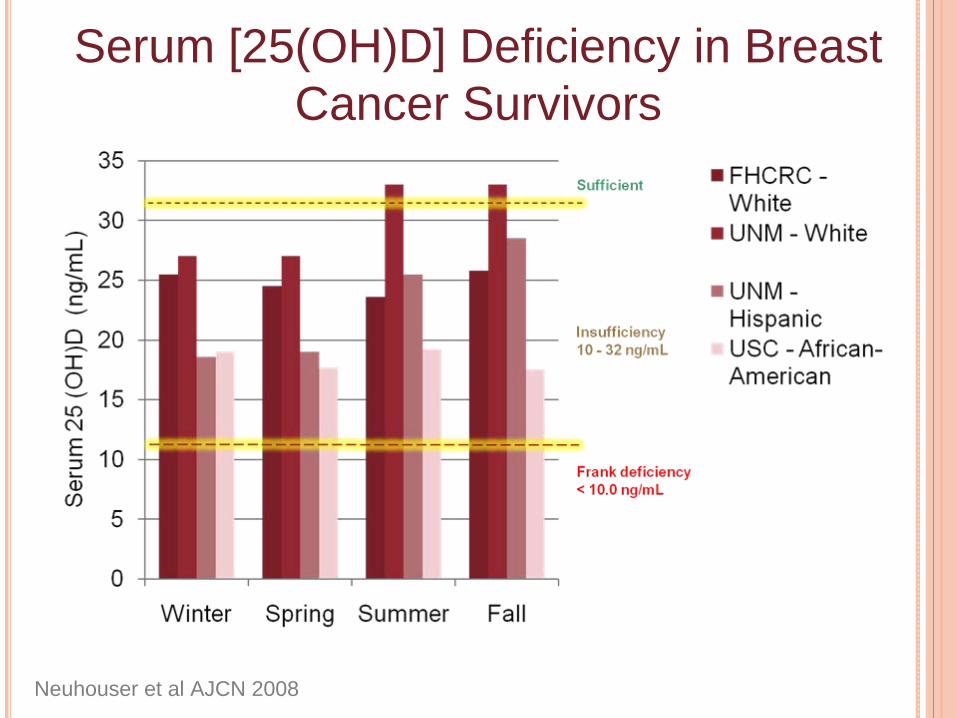
Serum [25(OH)D] Deficiency in Breast Cancer Survivors
Neuhouser et al AJCN 2008

Serum [25(OH)D] by Stage of Disease in Breast Cancer Survivors
Neuhouser, et al AJCN 2008

Serum [25(OH)D] by Tamoxifen Use and Estrogen Receptor Status in Breast
Cancer Survivors
* p = 0.008 vs. no tamoxifen currently ** p = 0.005 vs. no tamoxifen ever^ NS vs. negative estrogen receptor status
Dietary Supplements Use by Cancer Survivors
Review: 64-81% of cancer survivors used dietary supplements vs. 50% of general US population
Velicer et al. J Clin Oncol 2008

HEAL Supplement Inventory: “Since the breast cancer diagnosis have you taken any herbal or alternative remedies?”
• Alfalfa• Bee Pollen• Black Cohosh• Blue Cohosh• Cat’s Claw• Chaste Berries• Dong Quai• Echinacea• Evening Primrose
Oil• False unicorn• Flax seed oil• Fo ti tieng
• Garlic• Ginko biloba• Ginseng• Green tea• Gotukola• Licorice Root• Motherwort• Nux vomica• Pulsatilla• Red clover • Red raspberry• Royal jelly• Sage tea
• Sarsaparilla• Saw palmetto• Sephia• Shark cartilage• Soy supplement• St John’s wort• Valerian• Wild yam/
Mexican yam • Yerba buena• Other – over 200
write-ins
Determining Estrogenicity128 supplements were reviewed (34
listed & 94 write-ins)Sources
– PDR for Herbal Medicines – Herb-Drug Interactions in Oncology– Natural Medicines Comprehensive
DatabaseDefined as estrogenic if any indication
that supplement had estrogenic properties (in vitro, animals, humans)

0 10 20 30 40 50 60 70 80
Yam
Turmeric
Soy
Saw Palmetto
Red Clover
Nettles
Licorice
Ginseng
Fo ti tieng
Flax
Dong Quai
DHEA
Combination supp
Cat's Claw
Burdock Root
Boron
Black Cohosh
Astragalus
Alfalfa
Number of people reporting use
Use of estrogenic-type supplements in HEAL at 24 month interview

Estrogenic Supplements & Mean Hormone Concentrations in Breast Cancer Survivors (postmenopausal)Hormones£ Users Non-Users
(n=174) (n=328)
Estrone (pg/ml) 20.8 23.6*Estradiol (pg/ml) 12.8 14.7*Free Estradiol (pg/ml) 0.29 0.35**Testosterone (ng/ml) 167.9 183.3DHEAS (ng/dl) 47.7 56.2*SHBG (nmol/L) 52.2 49.1*p<0.05, ** p<0.01£Adjusted for age, race, physical activity, BMI, stage of disease at
diagnosis, dietary genestein, tamoxifen use, educationS Wayne et al Br Can Res Treat, 2008

Soy Supplements & Mean Hormone Concentrations in Breast Cancer SurvivorsHormones£ Soy Users Non-Users
(n=26) (n=328)
Estrone (pg/ml) 20.5 23.4Estradiol (pg/ml) 11.8 14.9Free Estradiol (pg/ml) 0.27 0.36Testosterone (ng/ml) 180.3 180.6DHEAS (ng/dl) 48.6 53.9SHBG (nmol/L) 60.1 48.8No statistically significant differences£Adjusted for age, race, physical activity, BMI, stage of disease
at diagnosis, dietary genestein, tamoxifen use, education
S Wayne et al Br Can Res Treat, 2008

Estrogenic Supplements & Mean Hormone Concentrations in Breast Cancer SurvivorsHormones£ Non-users 1 supp > 2 supp p, trend
(n=328) (n=85) (n=89)Estrone (pg/ml) 23.7 21.6 19.7 0.01Estradiol (pg/ml) 14.7 12.2 13.2 0.08Free Estradiol (pg/ml) 0.35 0.27 0.30 0.02Testosterone (ng/ml) 184.0 177.4 157.1 0.09DHEAS (ng/dl) 56.1 47.5 48.2 0.04SHBG (nmol/L) 48.8 58.3 47.4 0.79£Adjusted for age, race, physical activity, BMI, stage of disease
at diagnosis, dietary genestein, tamoxifen use, education
S Wayne et al BR Can Res Treat 2008
Dietary Supplements and Cancer Survivors in HEALUse of botanical supplements by breast
cancer survivors is commonMany of these supplements have estrogenic
propertiesIn the HEAL study, use of estrogenic
botanical supplements was associated with lower estrone, estradiol, free estradiol and DHEAS – analyses to examine survival and quality of life are in progress

Dietary Supplements and Cancer Survivors in HEALCAVEATS Variety of botanical supplements were used
by HEAL participants
We cannot guarantee content or purity
Difficulties in “estrogenic” classification
Observational study – possible that breast cancer patients who had more estrogen withdrawal symptoms/lower estrogen used the supplements
Nutrition and Breast Cancer Prognosis: HEAL
• A cancer diagnosis can be a “teachable moment” for making diet/activity changes, but accurate data are needed on effects of changes
• Evidence from HEAL that these lifestyle changes can influence hormones, insulin-like growth factors, inflammatory factors and subsequently, mortality
• New opportunities for interventions

HEAL INVESTIGATOR TEAM
FHCRC
Anne McTiernan
Marian Neuhouser
Catherine Duggan
CY Wang
City of Hope/USC
Leslie Bernstein
Roberta McKean-Cowdin
Kathy Meeske
UNM/ U Louisville
Charles Wiggins
Rick Baumgartner
Kathy Baumgartner
NCI
Rachel Ballard-Barbash
Lynne Harlan
Ashley Wilder-Smith
Catherine Alfano
Yale
Melinda Irwin
** Plus numerous outstanding students, fellows, staff, and former investigators