nursing management: respiratory failure and acute respiratory distress syndrome chapter 68 overview...
TRANSCRIPT

Nursing Management: Respiratory Failure
and Acute Respiratory Distress Syndrome
Chapter 68 Overview
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

2
Acute Respiratory Failure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 68-1. Normal gas exchange unit in the lung.

3
Acute Respiratory Failure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 68-2. Classification of respiratory failure.

4
Acute Respiratory Failure
Etiology and Pathophysiology Hypoxemic respiratory
failure Ventilation-perfusion mismatch
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
5
Acute Respiratory Failure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
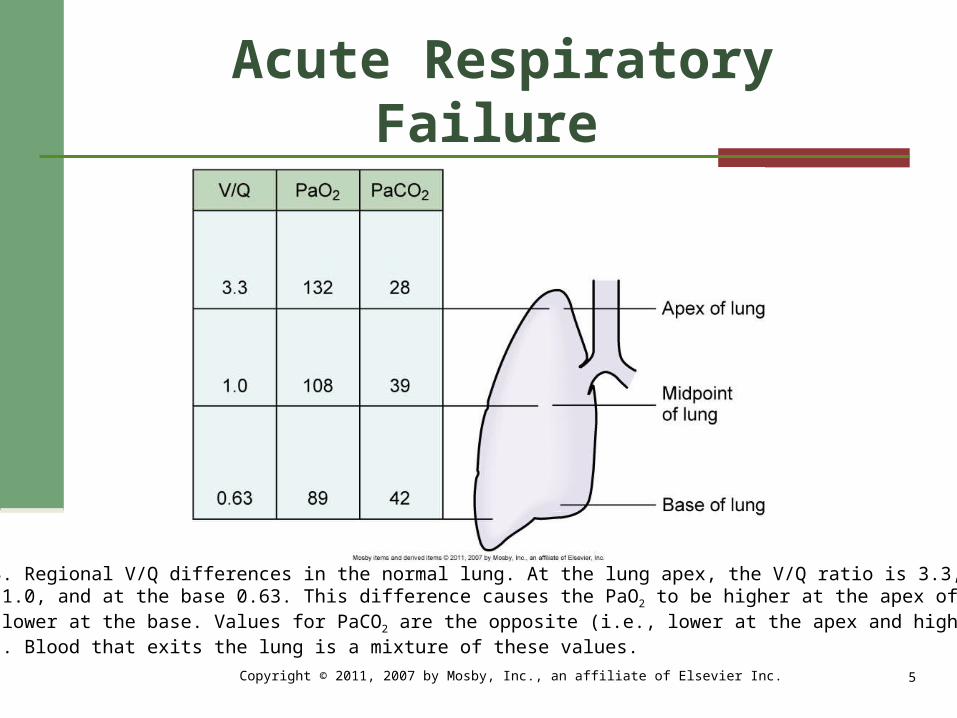
Fig. 68-3. Regional V/Q differences in the normal lung. At the lung apex, the V/Q ratio is 3.3, at themidpoint 1.0, and at the base 0.63. This difference causes the PaO2 to be higher at the apex of thelung and lower at the base. Values for PaCO2 are the opposite (i.e., lower at the apex and higher atthe base). Blood that exits the lung is a mixture of these values.

6
Acute Respiratory Failure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 68-4. Range of ventilation to perfusion (V/Q) relationships. A, Absolute shunt, no ventilation dueto fluid filling the alveoli. B, V/Q mismatch, ventilation partially compromised by secretions in theairway. C, Normal lung unit. D, V/Q mismatch, perfusion partially compromised by emboli obstructingblood flow. E, Dead space, no perfusion due to obstruction of the pulmonary capillary.

7
Acute Respiratory Failure
Etiology and Pathophysiology Hypoxemic respiratory
failure, continued Shunt Diffusion limitation
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

8
Acute Respiratory Failure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 68-5. Diffusion limitation. Exchange of CO2 and O2 cannot occur becauseof the thickened alveolar-capillary membrane.

9
Acute Respiratory Failure
Etiology and Pathophysiology Hypoxemic respiratory
failure, continued Alveolar hypoventilation Interrelationship of mechanisms
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

10
Acute Respiratory Failure
Etiology and Pathophysiology, continued Hypercapnic respiratory
failure Airways and alveoli Central nervous system Chest wall Neuromuscular conditions
Tissue oxygen needs
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

11
Acute Respiratory Failure
Clinical Manifestations Consequences of hypoxemia
and hypoxia Specific clinical
manifestations Diagnostic Studies
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

12
Nursing and Collaborative Management:
Acute Respiratory Failure Nursing Assessment Nursing Diagnoses Planning Prevention
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

13
Nursing and Collaborative Management:
Acute Respiratory Failure Respiratory Therapy
Oxygen therapy Mobilization of secretions
Effective coughing and positioning
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

14
Nursing and Collaborative Management:
Acute Respiratory Failure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 68-6. Augmented coughing is performed by placing the palm of the hand on the abdominalmusculature below the xiphoid process. As the patient ends a deep inspiration and begins theexpiration, the hand should be moved forcefully downward, increasing abdominal pressure,resulting in a forceful cough.

15
Nursing and Collaborative Management:
Acute Respiratory Failure Respiratory Therapy
Mobilization of secretions, continued
Hydration and humidification Chest physical therapy Airway suctioning
Positive pressure ventilation
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

16
Nursing and Collaborative Management:
Acute Respiratory Failure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 68-7. Noninvasive bilevel positive pressure ventilation. A mask is placed over the nose or noseand mouth. Positive pressure from a mechanical ventilator assists the patient’s breathing efforts,decreasing the work of breathing.

17
Nursing and Collaborative Management:
Acute Respiratory Failure Drug Therapy
Relief of bronchospasm Reduction of airway
inflammation Reduction of pulmonary
congestion Treatment of pulmonary
infections Reduction of severe anxiety,
pain, and agitationCopyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

18
Nursing and Collaborative Management:
Acute Respiratory Failure Medical Supportive Therapy
Treating the underlying cause
Maintaining adequate cardiac output
Maintaining adequate hemoglobin concentration
Nutritional Therapy Evaluation
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

19
Gerontologic Considerations:Respiratory Failure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

20
Acute Respiratory Distress Syndrome
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 68-8. Stages of edema formation in acute respiratory distress syndrome. A, Normal alveolusand pulmonary capillary. B, Interstitial edema occurs with increased flow of fluid into the interstitialspace. C, Alveolar edema occurs when the fluid crosses the blood-gas barrier.

21
Acute Respiratory Distress Syndrome
Etiology and Pathophysiology
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

22
Acute Respiratory Distress Syndrome
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 68-9. Pathophysiology of acute lung injury (ALI)/acute respiratory distress syndrome (ARDS).

23
Acute Respiratory Distress Syndrome
Etiology and Pathophysiology, continued Injury or exudative phase Reparative or proliferative
phase Fibrotic phase
Clinical Progression
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

24
Acute Respiratory Distress Syndrome
Clinical Manifestations and Diagnostic Studies
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

25
Acute Respiratory Distress Syndrome
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 68-10. Chest x-ray of a patient with acute respiratory distress syndrome (ARDS). The x-rayshows new, bilateral, diffuse, homogeneous pulmonary infiltrates without cardiac failure, fluidoverload, chest infection, or chronic lung disease.

26
Acute Respiratory Distress Syndrome
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Table 68-7. Diagnostic Findings in Acute Lung Injury/Acute Respiratory Distress

27
Acute Respiratory Distress Syndrome
Complications Ventilator-associated
pneumonia
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

28
Acute Respiratory Distress Syndrome
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Table 68-8. Key Components of Ventilator Bundle

29
Acute Respiratory Distress Syndrome
Complications, continued Barotrauma Volutrauma Stress ulcers Renal failure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

30
Nursing and Collaborative Management:
Acute Respiratory Distress Syndrome Nursing Assessment
Nursing Diagnoses Planning
Oxygen administration Positive pressure ventilation
Positioning strategies
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

31
Nursing and Collaborative Management:
Acute Respiratory Distress Syndrome
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 68-11. A, Turning patient prone on Vollman Prone Positioner. B, Patient lying prone on Vollman Prone Positioner.

32
Nursing and Collaborative Management:
Acute Respiratory Distress Syndrome
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 68-12. TotalCare SpO2RT® Bed System offers continuous lateral rotation therapy andpercussion and vibration therapies. Patients can easily and quickly be repositioned.

33
Nursing and Collaborative Management:
Acute Respiratory Distress Syndrome Medical Supportive Therapy
Maintenance of cardiac output and tissue perfusion
Maintenance of nutrition and fluid balance
Evaluation
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.