nurse sensitive quality indicators (nsqi) definitions and reports october 2, 2008 12:00 – 1:00 p.m
TRANSCRIPT

Nurse SensitiveQuality Indicators
(NSQI)
Definitions and Reports
October 2, 200812:00 – 1:00 p.m.

Presenters
Jim Cannon, Executive Director, Health Information Program, Washington State Hospital Association
Carol Wagner, Vice President, Patient Safety,
Washington State Hospital Association
Anne Wagg, National Database of Nursing Quality Indicators (NDNQI) Program Coordinator,
Central Washington Hospital, Wenatchee, Washington Photo Not Available

Web Cast Overview
Why are we making this effort? Jim Cannon
What are you going to be asked to do? Carol Wagner
• What is the tool? • What are the definitions?
Stories from the field Anne Wagg
What will you get out of the system? Jim Cannon

Nurse Staffing Agreement
NWONE, WSHA, and the three nursing unions agreed to work together to address nurse staffing and quality of care issues, including data collection.
One outcome was a Memorandum of Agreement.
NWONE and WSHA boards endorsed the legislation and Memorandum of Agreement.

Memorandum of AgreementData Collection
Surveyed on nurse sensitive quality indicators.
Based on the results, five indicators were selected for collection.
Steering committee agreed to give due consideration for the need not to create unreasonable data collection burdens.
Overview of the NSQI Project
Monthly, five NSQIs will be collected at the unit level.
Hospitals report data to WSHA via web-based tool – Quality Benchmarking System (QBS).
Reports will be generated for hospitals and nurse staffing committees.
Nurse Sensitive Quality Indicators
Consistent definitions between:• National Quality Forum (NQF)• National Database on Nursing
Quality Indicators (NDNQI)• Coalition for Nursing Outcome
Indicators (CalNOC)• The Washington NSQI Project

Data and Quality Care
Unit level data will inform administrators, managers, and clinicians
• Use by hospitals’ nurse staffing committees
• Illustrates effect of staffing decisions on patient care
• Support quality performance improvement

NSQI: The Indicators
Patient falls
Falls with injury
Pressure ulcer rate/prevalence
Nursing care hours per patient day – direct variable hours
Skill mix

Collection Tool: QBS
Data collection is through WSHA’s Quality Benchmarking System (QBS).
Six hospitals are piloting the system: Grays Harbor Community Hospital, Central Washington Hospital, Harrison Medical Center, Kadlec Medical Center, United General Hospital, and Swedish Health Services.
Secure, easy to use, web-based application.
Help is available for data display, analysis, and timely dissemination.
Quality Benchmarking System
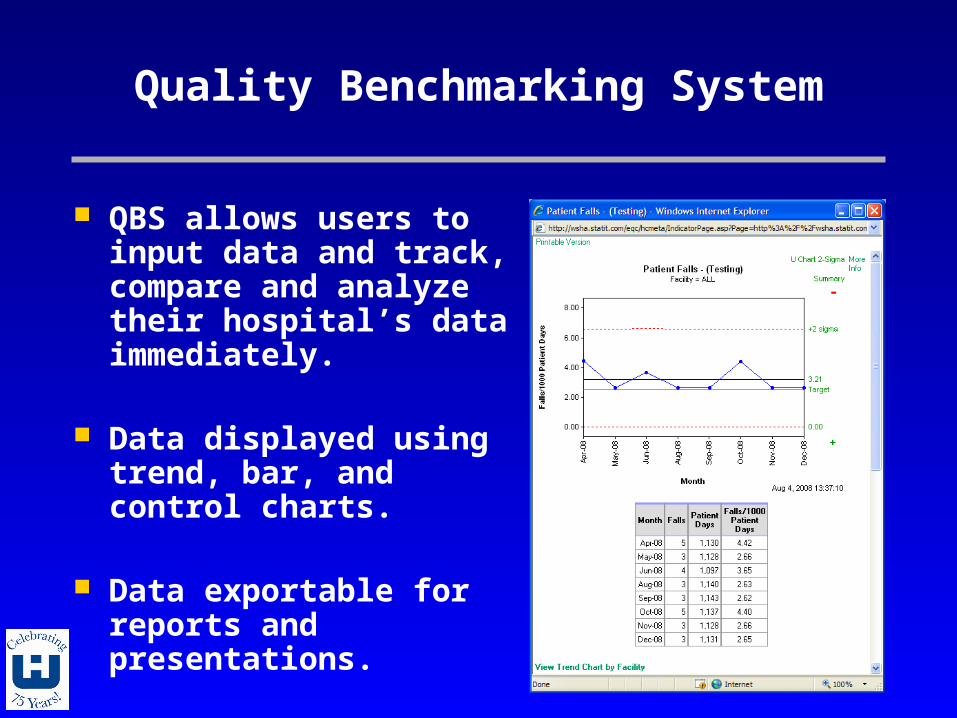
QBS allows users to input data and track, compare and analyze their hospital’s data immediately.
Data displayed using trend, bar, and control charts.
Data exportable for reports and presentations.

Score Card

Unit Level Drilldown

Drilldown Trend

Indicator Trend Matrix

Definitions
Indicator Data - Units
The indicator data are collected for each of the following units:
1. Medical2. Surgical3. Medical / Surgical4. ICU5. Step-down units
Patient Falls
Description: All documented falls with or without injury, experienced by patients on an
eligible unit in a calendar month.
Patient Falls
Data Elements: 1. Month / Year2. Type of unit3. Number of Patient Falls4. Patient Days
Patient Falls
Numerator: Number of patient falls, with or without injury
to the patient, by type of unit during the calendar month x 1,000.

Patient Falls - Numerator
Included Populations: Inpatients, short stay patients, observation
patients, and same day surgery patients who receive care on eligible inpatient units for all or part of a day.
Excluded Populations: Patients in units other than medical, surgical,
medical/surgical, ICU and step-down.

Patient Falls
Denominator Statement: Patient days by type of unit during the
calendar month.
Patient Falls - Denominator
Included Populations: Inpatients, short stay patients, observation
patients and same day surgery patients who receive care on eligible inpatient units for all or part of a day.
Excluded Populations: Patients in units other than medical, surgical,
medical/surgical, ICU and step-down.

Falls with Injury
Description: All documented patient falls with an injury level
of minor or greater.

Falls with Injury
Data Elements:1. Month / Year2. Type of unit3. Number of injury falls4. Patient days

Falls with Injury
Numerator Statement:Number of patient falls with an injury level of minor or greater by type of unit during the calendar month X 1000.

Falls with Injury - Numerator
Included Populations: Patient falls occurring while on an eligible
reporting unit An injury level of minor or greater defined as:
1. None – patient had no injuries resulting from the fall.2. Minor – results in application of a dressing, ice,
cleaning of a wound, limb elevation, or topical medication.
3. Moderate – results in suturing, application of steri-strips/skin glue, or splinting.
4. Major – results in surgery, casting, traction, or required consultation for neurological or internal injury.
5. Death – results in death as a result of the fall.
Falls with Injury - Numerator
Excluded Populations: Visitors Students Staff Members Falls by patients from eligible reporting unit,
however patient was not on unit at time of fall (e.g., patients falls in radiology department)
Falls with an injury level of “none” Falls by persons who are not patients, e.g., hospital
staff, visitors. Falls on other unit types (e.g., pediatric, obstetrical,
rehab, etc)

Falls with Injury
Denominator Statement: Patient days by type of unit during the
calendar month.

Falls with Injury - Denominator
Included Populations: Inpatients, short stay patients, observation
patients and same day surgery patients who receive care on eligible inpatient units for all or part of a day.
Excluded Populations: Patients in units other than medical, surgical,
medical/surgical, ICU and step-down.

Pressure Ulcer Rate/Prevalence
Description: The total number of patients that have
nosocomial (hospital-acquired) stage II or greater pressure ulcers on the day of the prevalence study.

Pressure Ulcer Rate
Data Elements:1. Day of First Staff Discovery/Documentation of
Pressure Ulcer2. Day of Hospitalization for Patient on Prevalence Study
Day3. Observed Pressure Ulcer4. Observed Pressure Ulcer – Hospital Acquired5. Observed Pressure Ulcer – Stage6. Admission Date7. Birthdate8. Month9. Year10.Type of Unit
Pressure Ulcer Rate
Numerator Statement: Patients surveyed on an eligible reporting unit
that have at least one stage II or greater [National Ulcer Advisory Panel (NPUAP)] nosocomial pressure ulcer on the day of the prevalence study.

Pressure Ulcer Rate - Numerator
Included Populations:Hospital Acquired Pressure Ulcers – Pressure Ulcers of Stage II or greater AND the Day of First Staff Discovery/Documentation of Pressure Ulcer is greater than or equal to 0003.
Pressure Ulcer Rate - Numerator
Excluded Populations: Patients with skin breakdown due to arterial occlusion, venous insufficiency, diabetes related neuropathy, or incontinence dermatitis. Patients with NO ulcers greater than stage I on the day of the prevalence study. Patients with an ulcer (any stage) present on the patient’s first day in the hospital. Patients with ulcers greater than Stage I on the day of the prevalence study where ALL the ulcers were documented to be present on day 2 of the patient’s hospitalization.
Pressure Ulcer Rate
Denominator Statement:All patients on the selected unit at the time of the study who are surveyed for the study by type of unit.

Pressure Ulcer Rate - Denominator
Included Populations:Patients 18 years or older who are admitted to medical, surgical, medical-surgical combined, critical care and step-down units that are surveyed for the study.
Excluded Populations:Patients less than 18 years of age.

Pressure Ulcer Stage
Stage I – non blanching erythema of intact skin.
Stage II – partial thickness involving epidermis and/or dermis; superficial and presents clinically as an abrasion, blister, or shallow crater.

Pressure Ulcer Stage
Stage III – Full thickness skin loss involving damage or necrosis of subcutaneous tissue that may extend down to but not through underlying fascia; presents clinically as a deep crater with or without undermining of adjacent tissue.
Stage IV – Full thickness skin loss with extensive destruction, tissue necrosis or damage to muscle, bone or supporting tissues.
Eschar – Unable to stage

Nursing Care Hours per Patient Day
Description of Indicators: 1. The number of productive hours worked by
RN nursing staff per patient day.2. The number of productive hours worked by
nursing staff (RN, LPN and UAP) per patient day.
Nursing Care Hours
Data Elements:1. Month / Year2. Type of unit3. Hours by RN, LPN, and UAP [Contract:
Agency]4. Hours by RN, LPN, and UAP [Employee]5. Patient days
Nursing Care Hours
Numerator Statement:Total number of productive hours worked by RN staff with direct patient care responsibilities by type of unit during the calendar month.
Total number of productive hours worked by RN, LVN, UAP with direct care responsibilities by type of unit during the calendar month.

Nursing Care Hours
Included Populations:Productive hours worked by RN staff with direct patient care responsibilities for greater than 50% of their shift. Includes:
1. Staff who are counted in the staffing matrix, and
2. Who are replaced if they call in sick, and3. Work hours are charged to the unit’s cost
center4. Contract staff

Nursing Care Hours
Excluded Populations: Persons whose primary responsibility is
administrative in nature. Specialty teams, patient educators or case
managers who are not assigned to a specific unit.

Skill Mix Indicators
Percentage of hours worked…Registered Nurse Licensed Vocational/Practical NurseUnlicensed Assistive PersonnelContract Staff
Skill Mix
Data Elements:1. Month / Year2. Type of unit3. RN hours [Contract: Agency]4. RN hours [Employee]5. LPN hours [Contract: Agency]6. LPN hours [Employee]7. UAP hours [Contract: Agency]8. UAP hours [Employee]

Skill Mix - Numerator
Included:Productive hours worked by [RN, LPN, UAP] staff with direct patient care responsibilities for greater than 50% of their shift. Includes:Staff who are counted in the staffing matrix, andWho are replaced if they call in sick, andWork hours are charged to the unit’s cost centerContract staff

Skill Mix - Numerator
Included Populations:Productive hours worked by contract staff [RN, LPN, UAP] with direct patient care responsibilities for greater than 50 percent of their shift. Includes:Staff not employed by your facility.Staff hired on a contractual basis to fill staffing needs
for a designated shift or on another short-term basis.Registry staff from outside the facility (e.g., not floating
staff from within the facility).Traveling nurse staff contracted to the facility for a
designated period of time.

Skill Mix - Numerator
Excluded Populations:Persons whose primary responsibility is
administrative in nature.Specialty teams, patient educators or case
managers who are not assigned to a specific unit.
Unit secretary, monitor techs.

Skill Mix - Denominator
Included Populations:Units:1. Medical2. Surgical3. Medical/Surgical4. ICU5. Step-down
Excluded Populations:Other unit types:(e.g., pediatric, obstetric)
Stories from the Field
What are your suggestions for collecting the data?
Have you been able to use the information to improve care or staffing?
Central Washington Hospital

NSQI: The Project
WSHA’s Health Information Program (HIP) coordinating the NSQI Project and the interface with QBS.
HIP will analyze the data based on WSHA and steering committee guidance.
HIP will provide technical assistance and guidance for project reporting.

Future WSHA Web Casts
Tomorrow, October 3, from 12:00-1:00 p.m.
Topic: Technical Components
Connection information is the same as for today.

Contact Information
Contact for help or more information:
With the NSQI Project:
Jane Feldman: [email protected]
About House Bill 3123 or the Memorandum of Agreement:
Kristin Petersen: [email protected]

Any Questions?