nuevas recomendaciones para la estadificación y … · nuevas recomendaciones para la...
TRANSCRIPT

Nuevas recomendaciones para la estadificación y evaluación de la respuesta al tratamiento
de los linfomas: la clasificación de Lugano
Armando López-Guillermo Servicio de Hematología
Hospital Clínic Barcelona
VIII Curso GOTEL de formación en linfomas Málaga, 17-18 de abril de 2015

Diagnosis (histology, sometimes cytology) Staging Treatment (or not!) Re-assessment (“response to therapy”) Follow-up
Management of lymphomas
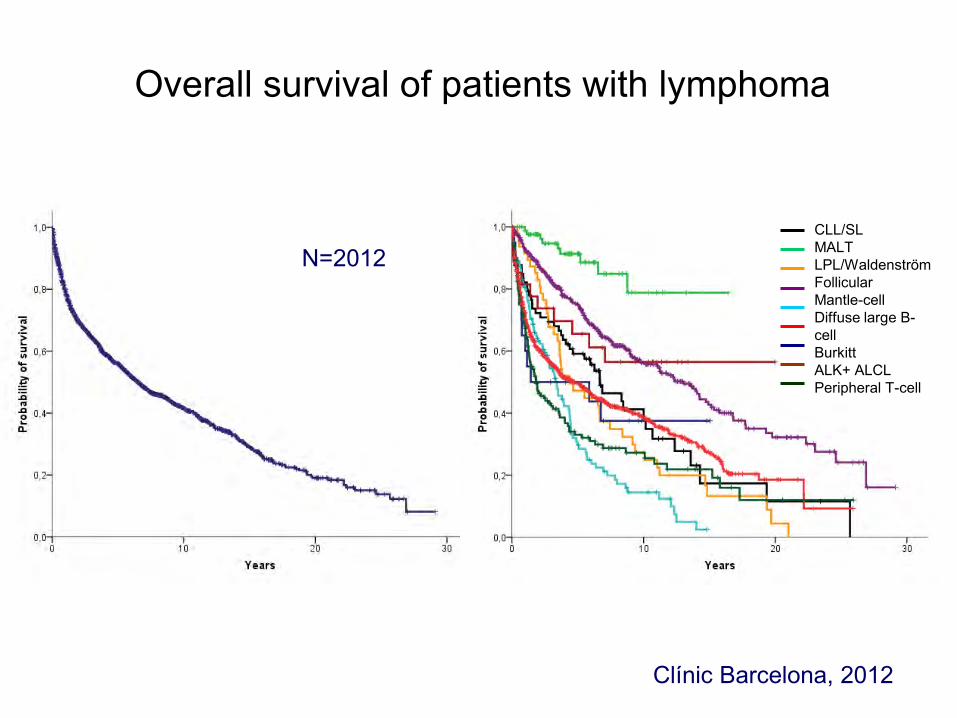
CLL/SL MALT LPL/Waldenström Follicular Mantle-cell Diffuse large B-cell Burkitt ALK+ ALCL Peripheral T-cell
Overall survival of patients with lymphoma
Clínic Barcelona, 2012
N=2012
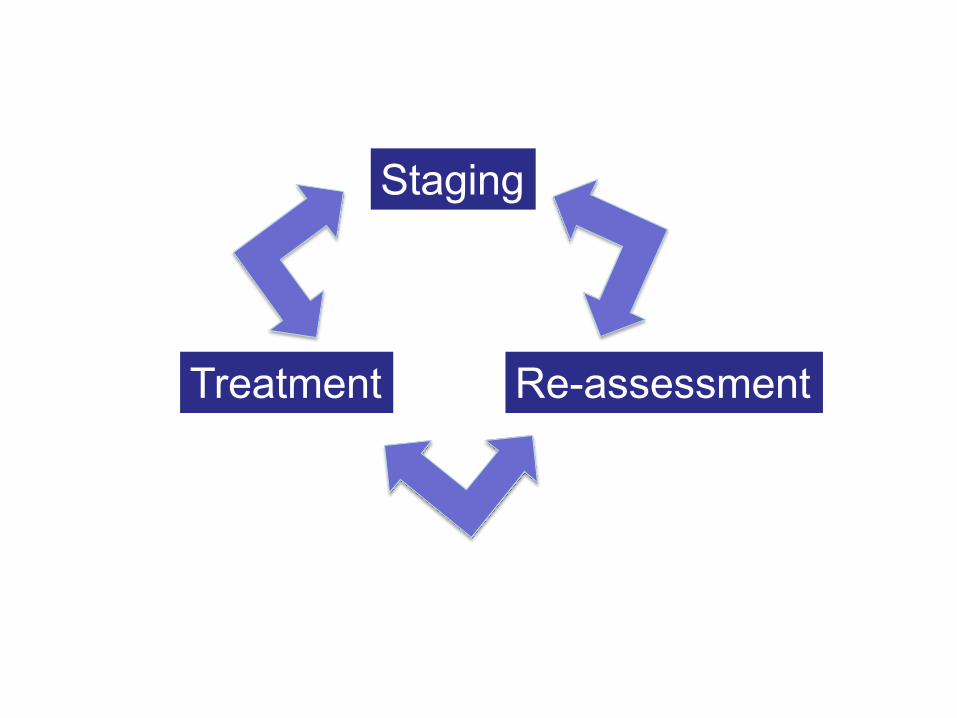
Staging
Treatment Re-assessment


Anamnesis y exploración física Hemograma y estudio bioquímico del
suero (LDH y beta2-m) Biopsia medular Rx tórax TAC torácico, abdominal y pélvico PET/CT?
Linfomas
Estudio inicial

Response definitions
CR Disappearance of all evidence of disease
PR Regression of measurable disease and no new sites
SD Failure to attain CR/PR or PD
Relapsed disease or PD
Any new lesion or increase by >50% of previously involved sites from
nadir
Cheson et al, JCO 2007

Ann Arbor (1971) Cotswolds (1989) NCI criteria (1999) NCI criteria (PET/CT) (2007) Lugano classification (2014)
Staging in lymphomas

Purpose: “to modernize recommendations for evaluation, staging and response assessment of patients with lymphoma”
Authors: − Leading hematologists, oncologists, radiation oncologists,
pathologists, radiologists, and nuclear medicine physicians − Representing major international lymphoma clinical trials
groups and cancer centers
Development steps: − 11-ICML (2011) started the process − Clinical and imaging sub-committees worked during 2 years − Workshop at 12-ICML (2013) to present conclusions and
discuss main recommendations − Steering committee (lead by B. Cheson) wrote two
manuscripts (J Clin Oncol 2014;32:3048-67)
The Lugano classification: why, when and who?
Staging criteria − Imaging − Tumor bulk − Spleen and liver involvement − Bone marrow
Prognostic groups and treatment allocation Assessment of response Follow-up and outcome
Outline

Morphology, immunohistochemistry, flow cytometry, (and molecular studies when appropriate) reviewed by an experienced pathologist
Fine-needle aspirate inadequate for initial diagnosis
Incisional or excisional biopsy preferred; core-needle biopsy acceptable when not possible the others
Material for future research (with consent)
Diagnosis of lymphomas
Staging criteria − Imaging − Tumor bulk − Spleen and liver involvement − Bone marrow
Prognostic groups and treatment allocation Assessment of response Follow-up and outcome
Outline

Recommendations are for nodal lymphomas and all DLBCL (primary extranodal –CNS, skin- have specific guidelines)
Ann Arbor stage only as component of factors in prognostic indices
PET-CT for staging of routinely FDG-avid histologies (particularly in clinical trials) strongly recommended
CT preferred in FDG nonavid lymphomas All lymphomas are considered FDG-avid, except:
─ CLL/SLL ─ Lymphoplasmocytoid/Waldenström ─ Mycosis fungoides ─ Marginal zone lymphomas
Anatomic staging
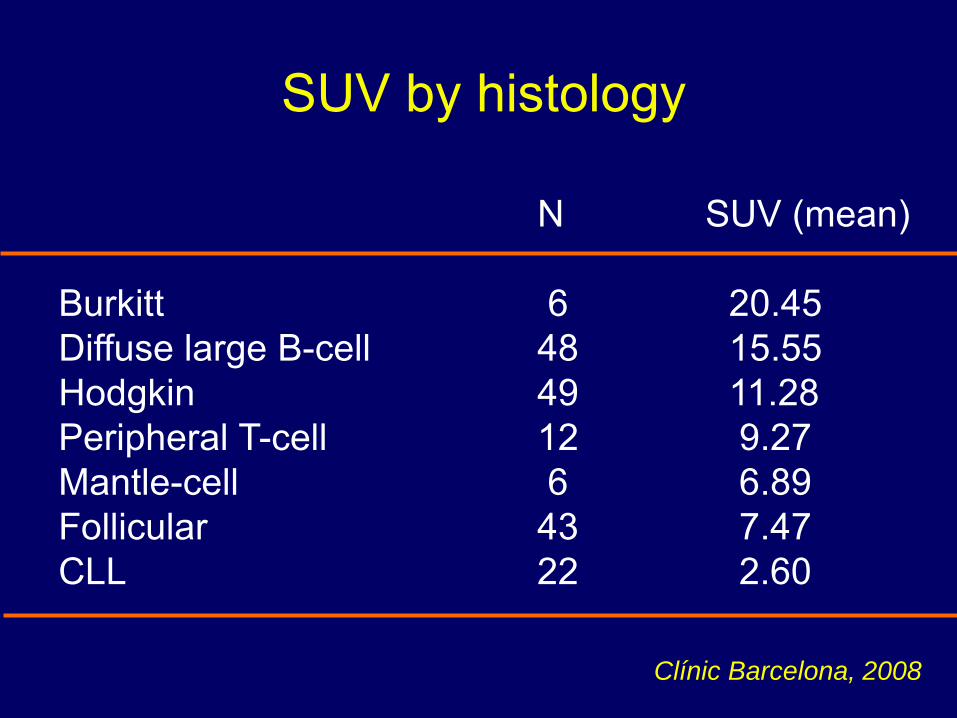
SUV by histology
N SUV (mean) Burkitt 6 20.45 Diffuse large B-cell 48 15.55 Hodgkin 49 11.28 Peripheral T-cell 12 9.27 Mantle-cell 6 6.89 Follicular 43 7.47 CLL 22 2.60
Clínic Barcelona, 2008
Staging criteria − Imaging − Tumor bulk − Spleen and liver involvement − Bone marrow
Prognostic groups and treatment allocation Assessment of response Follow-up and outcome
Outline
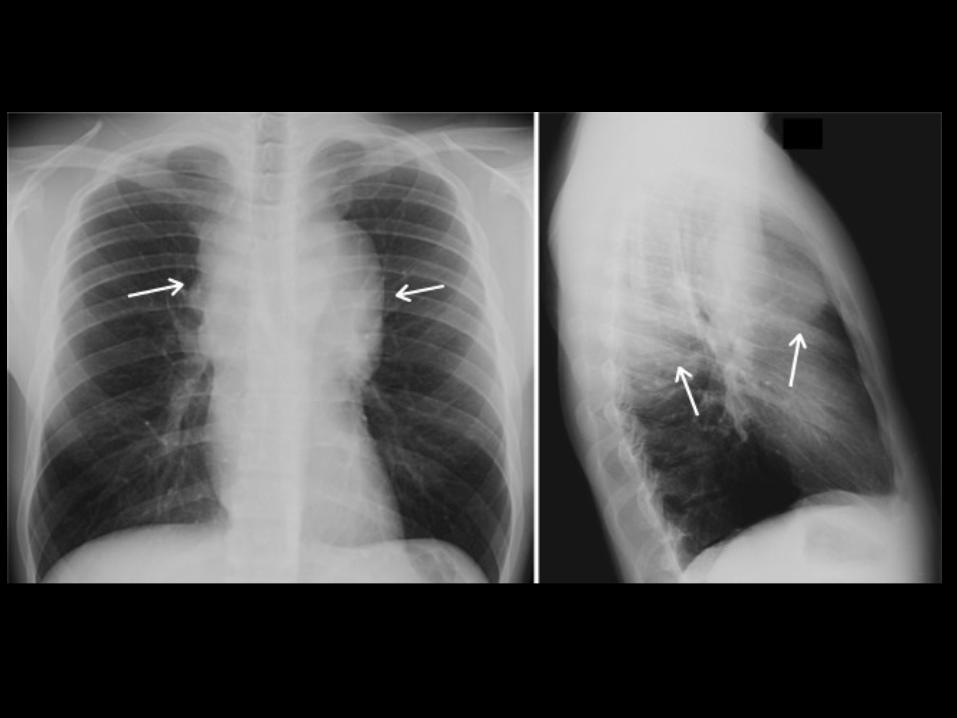

A single nodal mass ≥10 cm or >1/3 of transthoracic diameter as determined by TAC is retained as definition of bulky disease for Hodgkin’s lymphoma
Chest x-ray not required
Variety of sizes have been suggested for non-Hodgkin’s lymphomas to define “bulky”
Recommendation: to record the longest measurement by CT
The term “X” no longer necessary
Tumor bulk

Staging criteria − Imaging − Tumor bulk − Spleen and liver involvement − Bone marrow
Prognostic groups and treatment allocation Assessment of response Follow-up and outcome
Outline
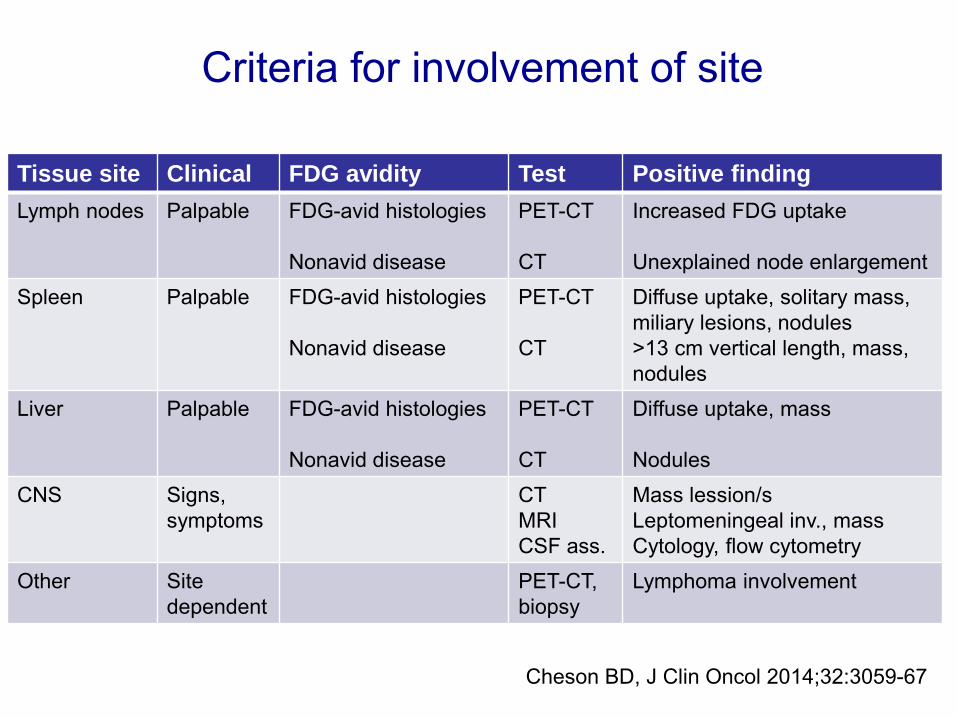
Criteria for involvement of site
Cheson BD, J Clin Oncol 2014;32:3059-67
Tissue site Clinical FDG avidity Test Positive finding Lymph nodes Palpable FDG-avid histologies
Nonavid disease
PET-CT CT
Increased FDG uptake Unexplained node enlargement
Spleen Palpable FDG-avid histologies Nonavid disease
PET-CT CT
Diffuse uptake, solitary mass, miliary lesions, nodules >13 cm vertical length, mass, nodules
Liver Palpable FDG-avid histologies Nonavid disease
PET-CT CT
Diffuse uptake, mass Nodules
CNS Signs, symptoms
CT MRI CSF ass.
Mass lession/s Leptomeningeal inv., mass Cytology, flow cytometry
Other Site dependent
PET-CT, biopsy
Lymphoma involvement
Staging criteria − Imaging − Tumor bulk − Spleen and liver involvement − Bone marrow
Prognostic groups and treatment allocation Assessment of response Follow-up and outcome
Outline

BM biopsy has been the gold-standard for decades
High sensitivity of PET/CT for BM involvement
Hodgkin’s lymphoma: 18% focal skeletal lesions by PET/CT with only 6% BM infiltration by BM biopsy, in all cases with disseminated disease by PET/CT
DLBCL: ─ PET/CT more sensitive than biopsy ─ 27% of BM+, including 94% by PET/CT and 40% by biopsy ─ Discordant histologies issue?
Insufficient data in other histologies
Bone marrow (BM)

BM biopsy has been the gold-standard for decades
High sensitivity of PET/CT for BM involvement
Hodgkin’s lymphoma: 18% focal skeletal lesions by PET/CT with only 6% BM infiltration by BM biopsy, in all cases with disseminated disease by PET/CT
DLBCL: ─ PET/CT more sensitive than biopsy ─ 27% of BM+, including 94% by PET/CT and 40% by biopsy ─ Discordant histologies issue?
Insufficient data in other histologies
Bone marrow (BM)
Recommendation: If a PET/CT is performed, a BM biopsy in no longer indicated for HL; A BM biopsy is only needed for DLBCL if the PET is negative and identifying a discordant histology is important for patient management
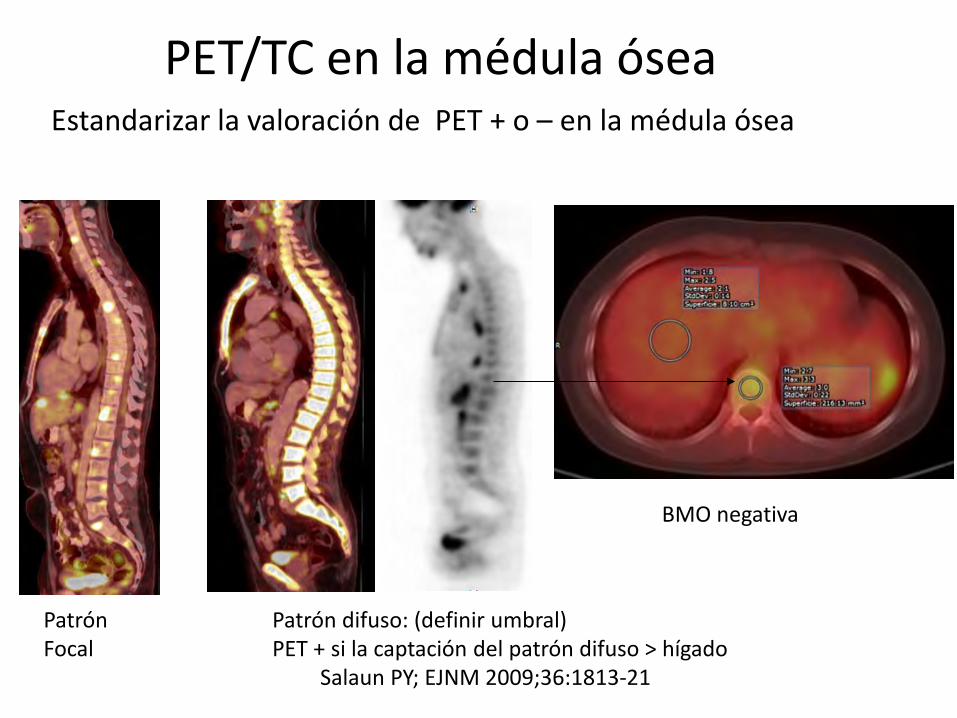
BMO negativa
Patrón difuso: (definir umbral) PET + si la captación del patrón difuso > hígado
Salaun PY; EJNM 2009;36:1813-21
Estandarizar la valoración de PET + o – en la médula ósea
Patrón Focal
PET/TC en la médula ósea
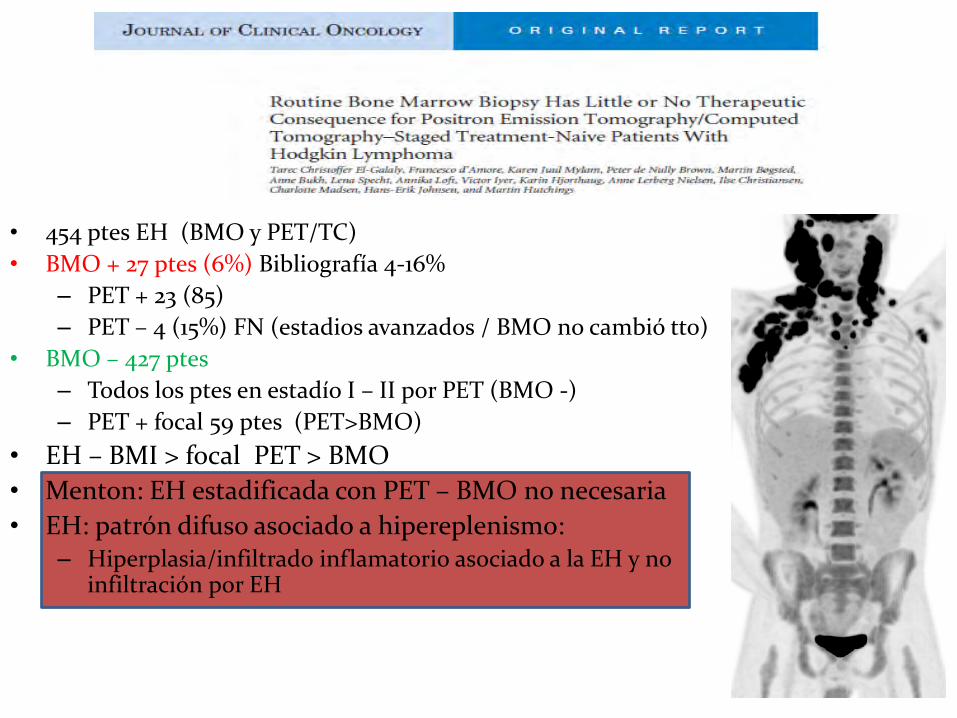
• 454 ptes EH (BMO y PET/TC) • BMO + 27 ptes (6%) Bibliografía 4-16%
– PET + 23 (85) – PET – 4 (15%) FN (estadios avanzados / BMO no cambió tto)
• BMO – 427 ptes – Todos los ptes en estadío I – II por PET (BMO -) – PET + focal 59 ptes (PET>BMO)
• EH – BMI > focal PET > BMO • Menton: EH estadificada con PET – BMO no necesaria • EH: patrón difuso asociado a hipereplenismo:
– Hiperplasia/infiltrado inflamatorio asociado a la EH y no infiltración por EH
2012

PET vs BMO en LDCG ?? Meta-análisis y revisión sistemática del EJNM
Estudios Nº Ptes Sensibilidad (%) Especificidad (%)
Kahn (2013) 130 94 100
Cortés (2013) 84 95 100
Berthet (2013) 133 94 99
Hong (2012) 89 70 100
Pelosi (2011) 120 84 100
Ribrag (2008) 43 89 100
GLOBAL 654 88 99
PET – BMO + = 3.1 % FN PET + BMO - = 12.5 %
PET - descarta infiltración de MO BMO podría evitarse Eur J Nucl Med 2013
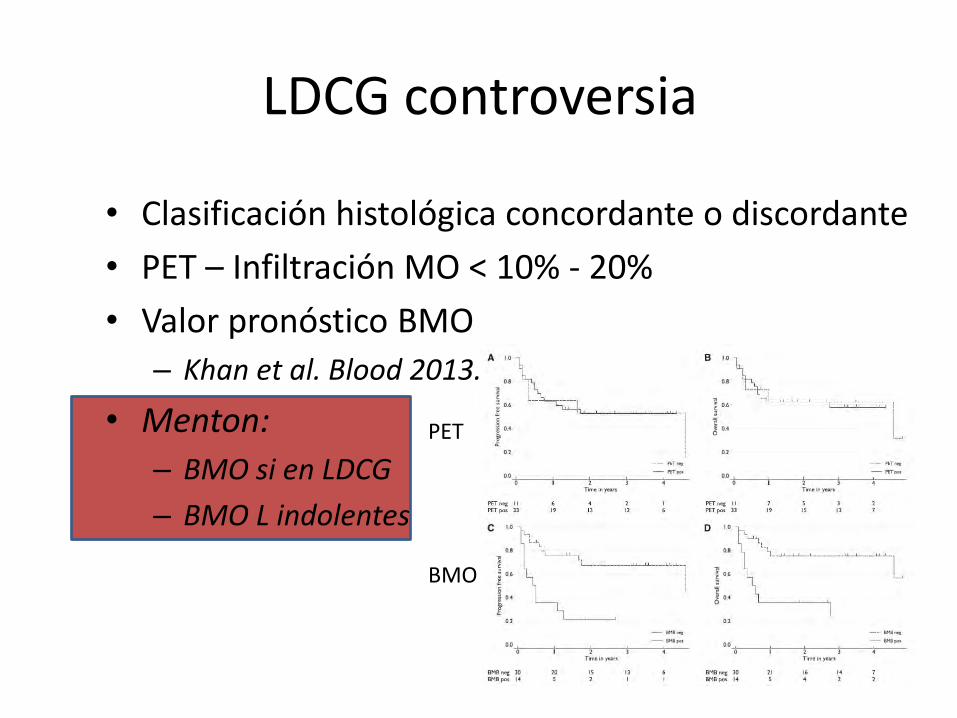
LDCG controversia
• Clasificación histológica concordante o discordante • PET – Infiltración MO < 10% - 20% • Valor pronóstico BMO
– Khan et al. Blood 2013.
• Menton: – BMO si en LDCG – BMO L indolentes
PET BMO

BM biopsy has been the gold-standard for decades
High sensitivity of PET/CT for BM involvement
Hodgkin’s lymphoma: 18% focal skeletal lesions by PET/CT with only 6% BM infiltration by BM biopsy, in all cases with disseminated disease by PET/CT
DLBCL: ─ PET/CT more sensitive than biopsy ─ 27% of BM+, including 94% by PET/CT and 40% by biopsy ─ Discordant histologies issue?
Insufficient data in other histologies
Bone marrow (BM)
Recommendation: If a PET/CT is performed, a BM biopsy in no longer indicated for HL; A BM biopsy is only needed for DLBCL if the PET is negative and identifying a discordant histology is important for patient management

Staging criteria − Imaging − Tumor bulk − Spleen and liver involvement − Bone marrow
Prognostic groups and treatment allocation Assessment of response Follow-up and outcome
Outline

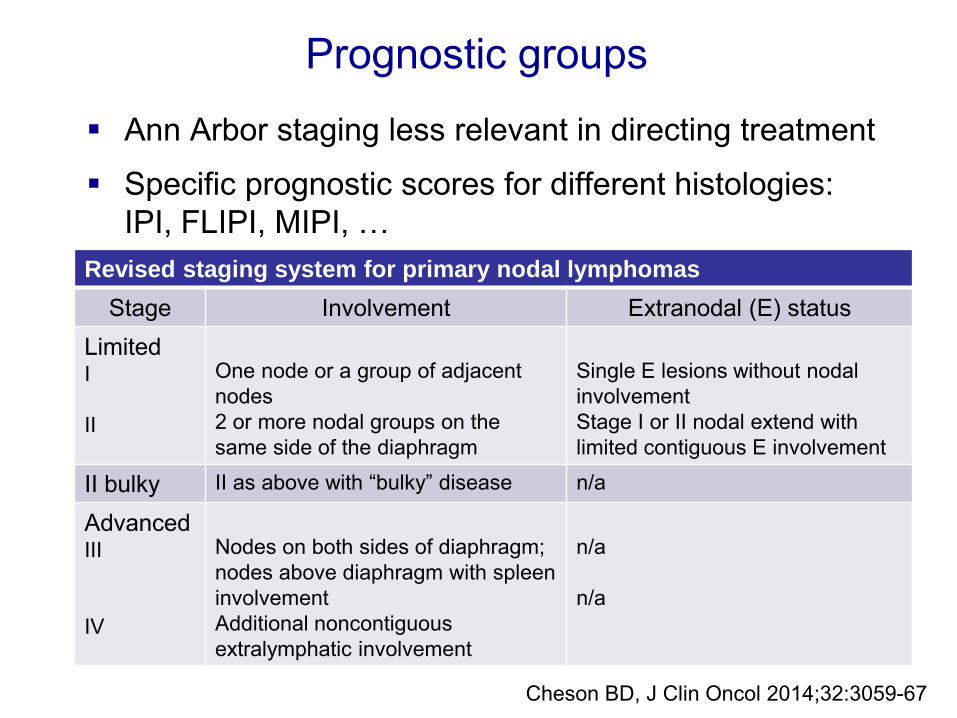
Ann Arbor staging less relevant in directing treatment
Specific prognostic scores for different histologies: IPI, FLIPI, MIPI, …
Prognostic groups
Ann Arbor staging less relevant in directing treatment
Specific prognostic scores for different histologies: IPI, FLIPI, MIPI, …
Prognostic groups
Revised staging system for primary nodal lymphomas Stage Involvement Extranodal (E) status
Limited I II
One node or a group of adjacent nodes 2 or more nodal groups on the same side of the diaphragm
Single E lesions without nodal involvement Stage I or II nodal extend with limited contiguous E involvement
II bulky II as above with “bulky” disease n/a
Advanced III IV
Nodes on both sides of diaphragm; nodes above diaphragm with spleen involvement Additional noncontiguous extralymphatic involvement
n/a n/a
Cheson BD, J Clin Oncol 2014;32:3059-67

Staging criteria − Imaging − Tumor bulk − Spleen and liver involvement − Bone marrow
Prognostic groups and treatment allocation Assessment of response Follow-up and outcome
Outline
Non Hodgkin’s lymphoma
CR[u]
“A large abdominal or mediastinal mass that undergoes greater than 50% reduction in size and remains stable for 2 to 4 months should not prevent classification as a CR given the absence of all other measurable disease.”
Coiffier, JCO 1989
End-of-treatment assessment is more accurate with PET/CT, especially in CRu or PR patients in HL, DLBCL and FL
PET/CT criteria eliminate CRu
PET/CT in HL: ─ Negative predictive value: 95-100%
─ Positive predictive value: >90%
PET/CT in DLBSL: ─ Negative predictive value: 80-100%
─ Positive predictive value: 50-100%
Assessment of response (end-of-treatment)
Cheson BD, J Clin Oncol 2014;32:3059-67

Five-point scale is recommended for reporting PET/CT; results should be interpreted in context of anticipated prognosis, clinical findings and other markers of response
Scores 1 and 2 represent complete metabolic response (CMR)
Score 3 also probably represents CMR in patients receiving standard treatment
Scores 4 or 5 with reduced uptake from baseline likely represents partial metabolic response, but at the end of treatment represents residual metabolic disease
Increase in FDG uptake to score 5, score 5 with no decrease in uptake, and new FDG-avid foci consistent with lymphoma represent treatment failure and/or progression
Interpretation of PET/CT scans
Barrington SF, J Clin Oncol 2014;32:3048-58
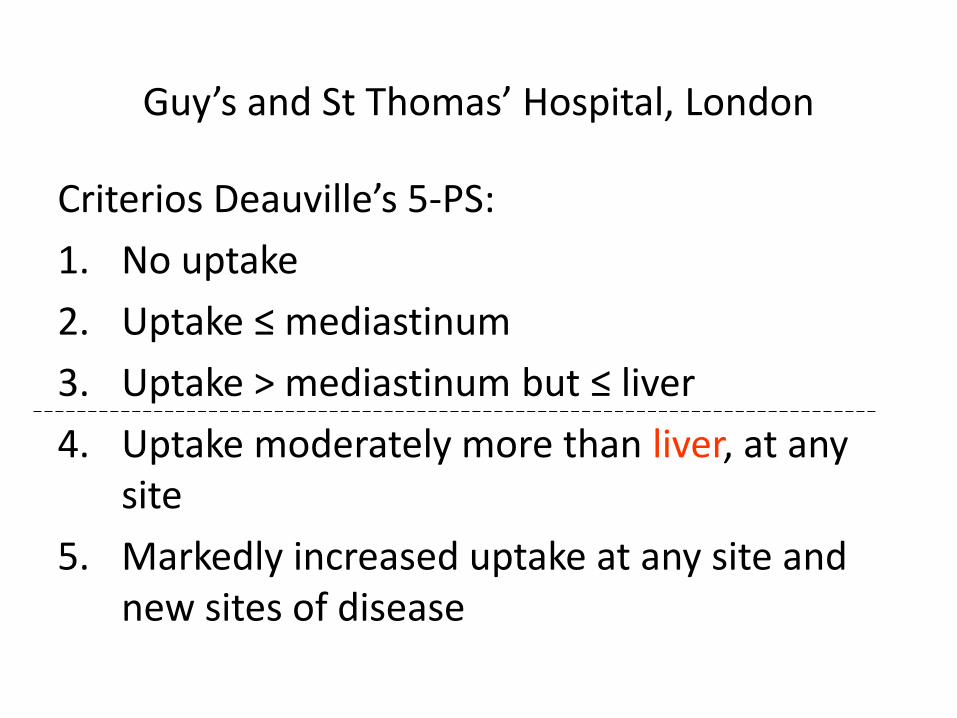
Guy’s and St Thomas’ Hospital, London
Criterios Deauville’s 5-PS: 1. No uptake 2. Uptake ≤ mediastinum 3. Uptake > mediastinum but ≤ liver 4. Uptake moderately more than liver, at any
site 5. Markedly increased uptake at any site and
new sites of disease

Five-point scale is recommended for reporting PET/CT; results should be interpreted in context of anticipated prognosis, clinical findings and other markers of response
Scores 1 and 2 represent complete metabolic response (CMR)
Score 3 also probably represents CMR in patients receiving standard treatment
Scores 4 or 5 with reduced uptake from baseline likely represents partial metabolic response, but at the end of treatment represents residual metabolic disease
Increase in FDG uptake to score 5, score 5 with no decrease in uptake, and new FDG-avid foci consistent with lymphoma represent treatment failure and/or progression
Interpretation of PET/CT scans
Barrington SF, J Clin Oncol 2014;32:3048-58

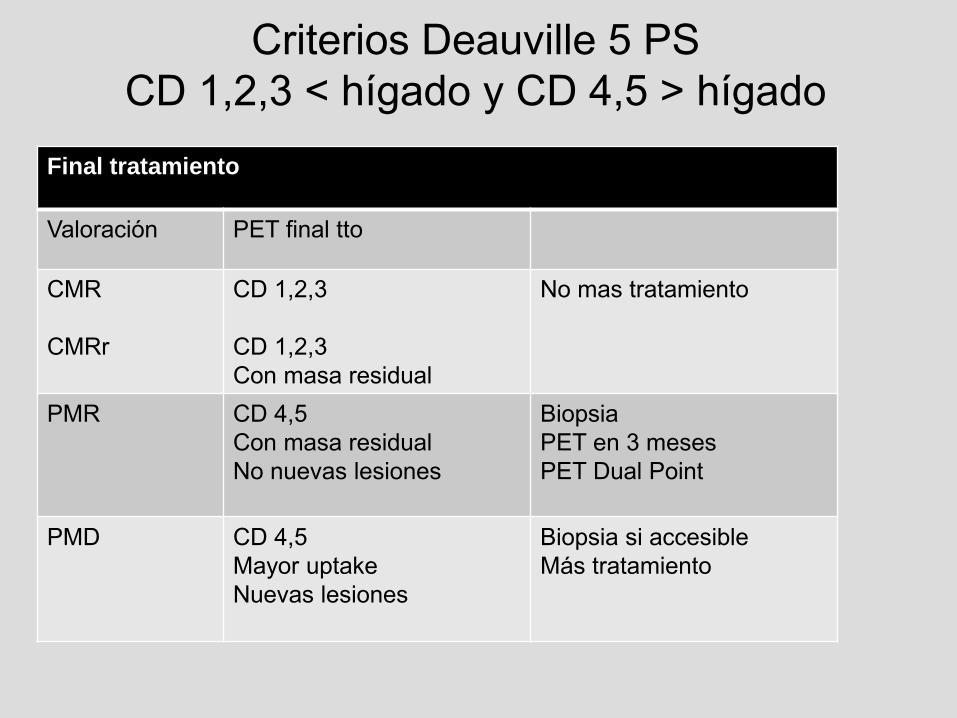
Criterios Deauville 5 PS CD 1,2,3 < hígado y CD 4,5 > hígado
Final tratamiento
Valoración PET final tto
CMR CMRr
CD 1,2,3 CD 1,2,3 Con masa residual
No mas tratamiento
PMR CD 4,5 Con masa residual No nuevas lesiones
Biopsia PET en 3 meses PET Dual Point
PMD CD 4,5 Mayor uptake Nuevas lesiones
Biopsia si accesible Más tratamiento

CMR
Cortesía del Dr. X. Setaín

Criterios Deauville 5 PS CD 1,2,3 < hígado y CD 4,5 > hígado
Final tratamiento
Valoración PET final tto
CMR CMRr
CD 1,2,3 CD 1,2,3 Con masa residual
No mas tratamiento
PMR CD 4,5 Con masa residual No nuevas lesiones
Biopsia PET en 3 meses PET Dual Point
PMD CD 4,5 Mayor uptake Nuevas lesiones
Biopsia si accesible Más tratamiento

FDG uptake < liver CMRr (retroperitoneal)
Cortesía del Dr. X. Setaín

Criterios Deauville 5 PS CD 1,2,3 < hígado y CD 4,5 > hígado
Final tratamiento
Valoración PET final tto
CMR CMRr
CD 1,2,3 CD 1,2,3 Con masa residual
No mas tratamiento
PMR CD 4,5 Con masa residual No nuevas lesiones
Biopsia PET en 3 meses PET Dual Point
PMD CD 4,5 Mayor uptake Nuevas lesiones
Biopsia si accesible Más tratamiento
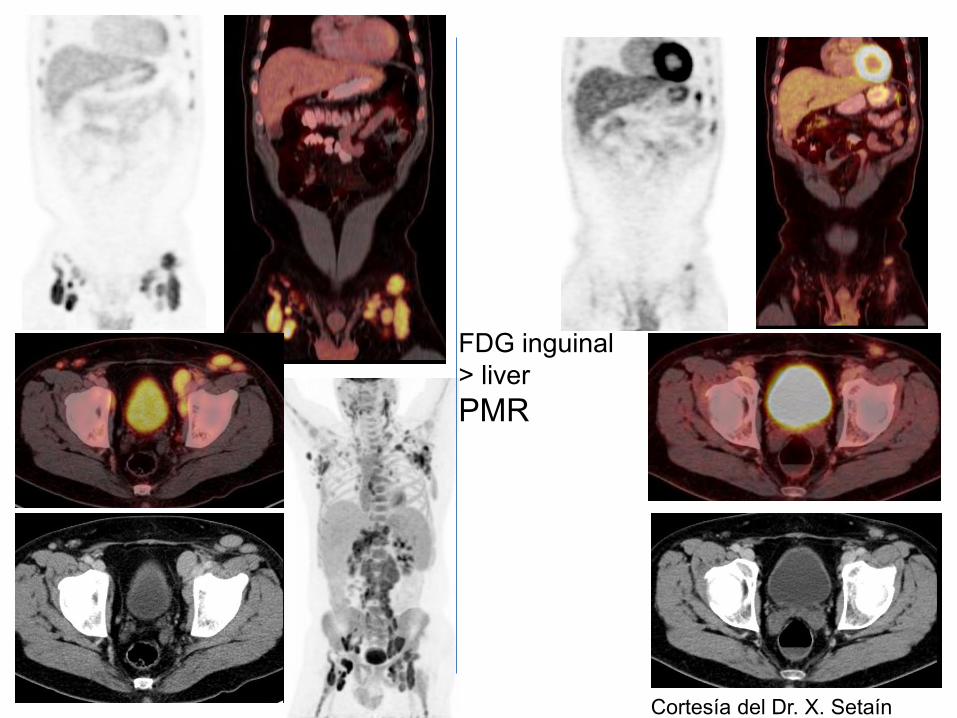
FDG inguinal > liver PMR
Cortesía del Dr. X. Setaín
Criterios Deauville 5 PS CD 1,2,3 < hígado y CD 4,5 > hígado
Final tratamiento
Valoración PET final tto
CMR CMRr
CD 1,2,3 CD 1,2,3 Con masa residual
No mas tratamiento
PMR CD 4,5 Con masa residual No nuevas lesiones
Biopsia PET en 3 meses PET Dual Point
PMD CD 4,5 Mayor uptake Nuevas lesiones
Biopsia si accesible Más tratamiento

Menton 2012 Interim PET Validado para uso clínico
Enfermedad de Hodgkin 400 ptes (IVS) – 260 Criterios Deauville 5-PS Negativo Positivo 1,2,3 4,5 Lesión < hígado Lesión > hígado
∆SUV > 66% ∆SUV < 66%
LDCG - B Criterios Deauville 5-PS Negativo Positivo 1,2,3 4,5 Lesión < hígado Lesión > hígado
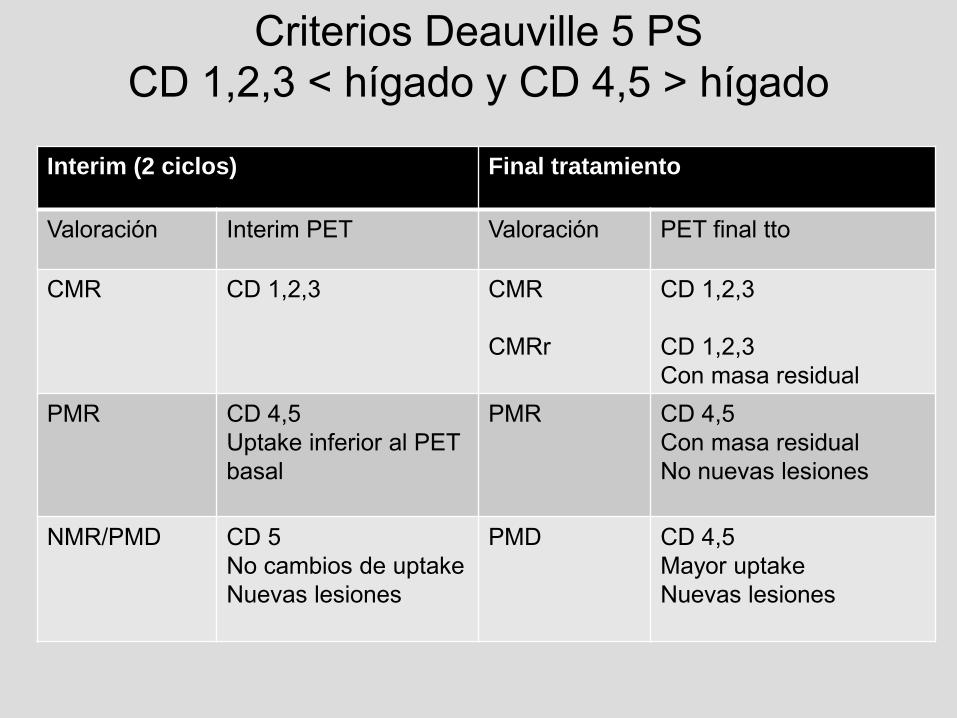
Criterios Deauville 5 PS CD 1,2,3 < hígado y CD 4,5 > hígado
Interim (2 ciclos) Final tratamiento
Valoración Interim PET Valoración PET final tto
CMR CD 1,2,3 CMR CMRr
CD 1,2,3 CD 1,2,3 Con masa residual
PMR CD 4,5 Uptake inferior al PET basal
PMR CD 4,5 Con masa residual No nuevas lesiones
NMR/PMD CD 5 No cambios de uptake Nuevas lesiones
PMD CD 4,5 Mayor uptake Nuevas lesiones

SUV PET inicial 12.5 SUV interim PET 2.6
PET inicial PET interim
Varón de 68 a. LDCG-B estadio III-A masa voluminosa abdominal Tratamiento con R-CHOP x 6
Cortesía del Dr. X. Setaín
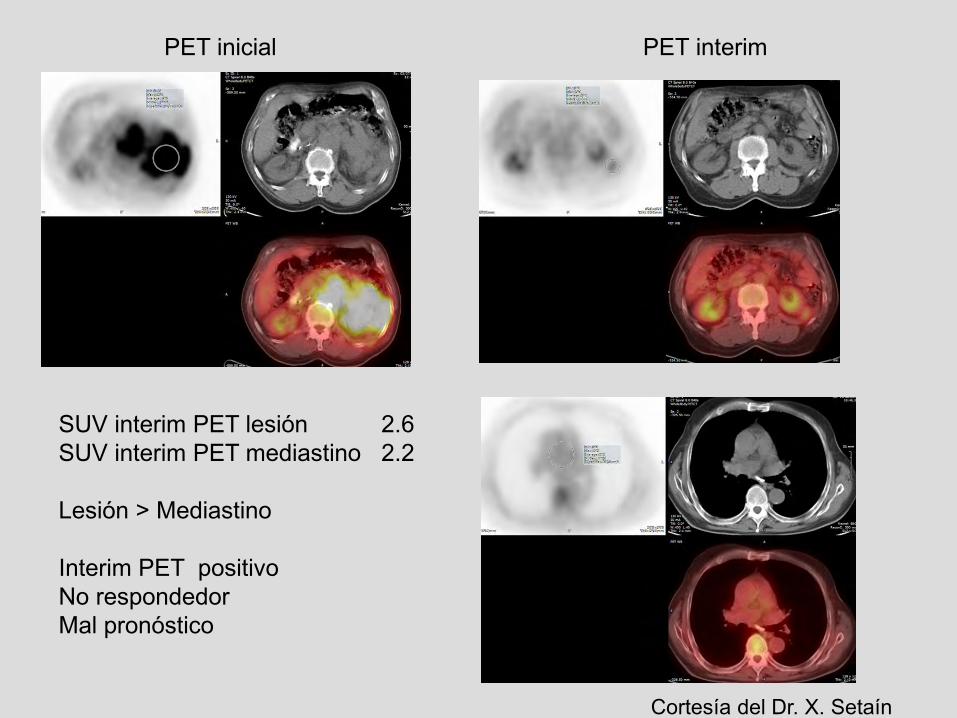
SUV interim PET lesión 2.6 SUV interim PET mediastino 2.2 Lesión > Mediastino Interim PET positivo No respondedor Mal pronóstico
PET inicial PET interim
Cortesía del Dr. X. Setaín
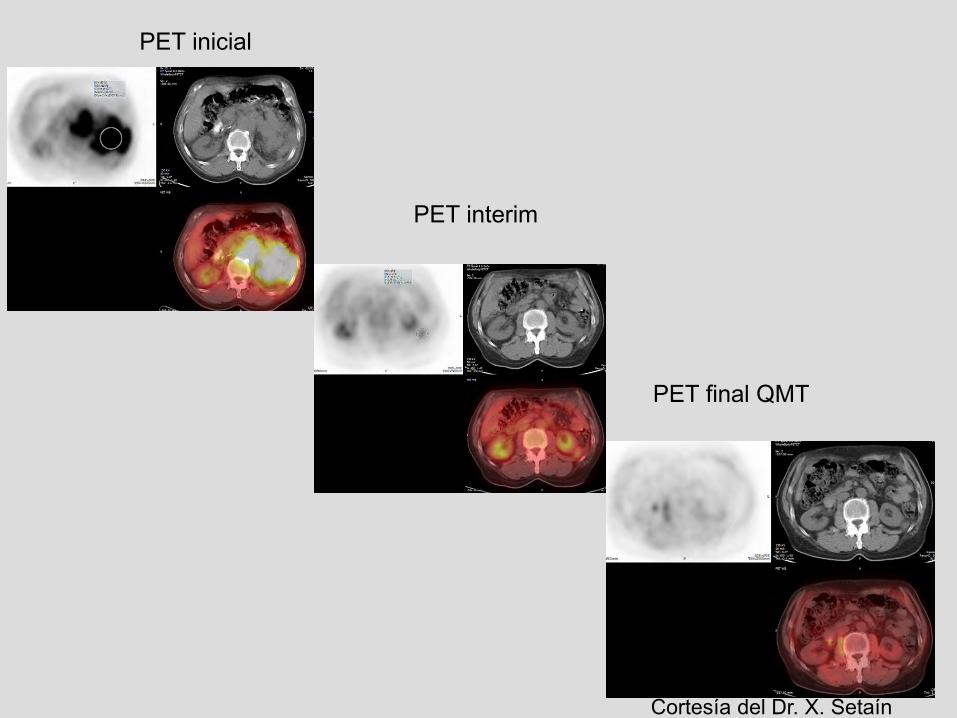
PET inicial
PET final QMT
PET interim
Cortesía del Dr. X. Setaín

SUV interim PET lesión 2.6 SUV interim PET hígado 2.8 Lesión < Hígado Interim PET negativo Respondedor Buen pronóstico
Cortesía del Dr. X. Setaín

SUV PET inicial 12.5 SUV interim PET 2.6
∆ SUV 79% > 66% Interim PET negativo Respondedor Buen pronóstico
Cortesía del Dr. X. Setaín
Staging criteria − Imaging − Tumor bulk − Spleen and liver involvement − Bone marrow
Prognostic groups and treatment allocation Assessment of response Follow-up and outcome
Outline

Good clinical judgment, a careful history, and physical examination are the cornerstone of patient follow-up
Specific guidelines available for the follow-up of the different lymphoma subtypes
Published studies fail to support routine surveillance scans (false-positive rate with PET is >20%)
RECOMMENDATIONS
─ Surveillance scans after remission are discouraged, especially for DLBCL and HL, although a repeat study may be considered after equivocal findings after treatment
─ Judicious use of follow-up scans may be considered in indolent lymphomas with residual intra-abdominal or retroperitoneal disease
Follow-up and outcome
Cheson BD, J Clin Oncol 2014;32:3059-67

“Simplificación “ de Ann Arbor
La biopsia medular deja de ser imprescindible en el estudio de extensión del linfoma de Hodgkin y el linfoma difuso de células grandes
PET/CT como prueba estándar para la mayoría de linfomas (excepto LLC, Waldenström, micosis fungoides y linfomas marginales)
El sistema de 5 puntos de Deauville como criterio estándar de valoración de respuesta
Clasificación de Lugano: modificaciones más significativas
