novita’ dall’ash leucemia acuta mieloide · novita’ dall’ash leucemia acuta mieloide...
TRANSCRIPT
NOVITA’ DALL’ASH
LEUCEMIA ACUTA MIELOIDE
Moderatori: Prof Attilio Olivieri
Dr Massimo Catarini
Relatore Drssa Debora Capelli
Facilitatore Dr Francesco Saraceni
Discussant
Drssa Denise Maravalle
Drssa Kimberley Garvey
Drssa Monica Poiani

Can we revert MDR?Origin of RelapseTARGET THERAPY
Mutazione coesina in cloni
preleucemici
Correla con ridotta attivazione dei
fattori trascrizionali coinvolti nella
differenziazione della cellula staminale
e aumenta l’espressione di fattori
coinvolti nel mantenimento della
staminalità:
ERG
GATA2
RUNX1
La coesina favorisce lo svolgimento della
cromatina, la riparazione del DNA e
l’attivazione di fattori trascrizionali
coinvolti nella differenziazione della
cellula staminale
Possibili target di terapia
Leukemia-Associated Cohesin Mutants Dominantly Enforce Stem Cell Programs and Impair Human Hematopoietic Progenitor Differentiation. Mazumdar C. et al., Blood 2015.

In vivo NGS model CD34+/CD38- di pazienti refrattari vengono inoculate al topo CD34+/CD38+CD34-/CD38+CD34-/CD38-
Conferma della refrattarietà ai chemioterapici ex vivo…GEP analysis delle cellule dei refrattari vs quelle dei responder:Homebox transcription factor, Wnt, Hedgehog pathways coinvolte nel mantenimento della staminalità.Metabolismo degli aminoacidi, disregolazione del segnale di IL-1.Mendler J et al., Blood 2015.
RELAPSED REFRACTORY AML:BIOLOGICAL STUDIES
Le mutazioni di SETBP1 e ASXL1 sono frequenti nelle LAM refrattarie
Correlano con la fosforilazione di MEF2C da parte di una MARK kinasi
Transattivazione di MEF2C promuve la sopravvivenza delle cellule leucemiche nella LAM MLL-AF9 tramite l’inibizione dell’apoptosi
Inhibition of MARK Kinase (MRT199665) potrebbe bypassare la chemioresistenza delle LAM con t(9;11).Brown F et al., Blood 2015.

Mechanisms of AZA/DEC resistance in MDS/AML: pre-clinical study
*Standard dose; †Dose rationalised for non-cytotoxic DNMT1 depletion (0.1–0.2mg/kg 1–3x/week)
DCK = deoxycytidine kinase; DEC = decitabine; DNMT1 = DNA methyltransferaseHMA = hypomethylatingagent; QRT-PCR = quantitative reverse transcriptase PCR; UCK = uridine-cytidine kinase
Ebrahem Q et al. Oral presentation at ASH 2015. Abstract 678
failure to deplete DNMT1 RESISTANCE TO HMA
• Expression levels of UCK2 increased, and DCK decreased at relapse in BM cells from MDS patients treated with DEC, and vice versa with AZA
• Differences in pyrimidine metabolism enable cells to avoid DNMT1 depletion and cause resistance of cells to AZA/DEC
UCK1, UCK2, DCK are pyrimidine metabolism enzymes that phosphorylate and trap AZA/DEC in cells, enabling DNMT1 depletion.
Expression levels of these enzymes (QRT-PCR) were measured pre-treatment and at relapse in BM cells from MDS patients treated with AZA or DEC.
0.0000128
625
1
25
125
5
0.2
0.04
0.008
0.0016
0.00032
0.000064
0.04
625
25
125
5
1
0.2
Rel
ativ
e ex
pre
ssio
n
Rel
ativ
e ex
pre
ssio
n
Pre-tx Relapse Pre-tx Relapse
AZA* (n=6) DEC† (n=12)UCK2
DCK
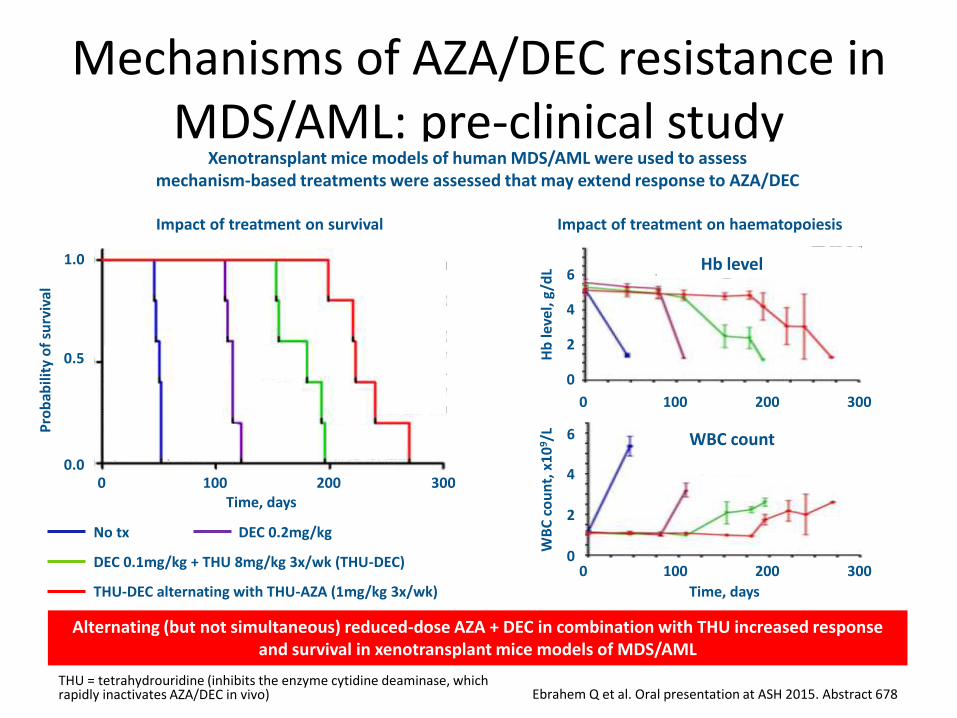
Mechanisms of AZA/DEC resistance in MDS/AML: pre-clinical study
THU = tetrahydrouridine (inhibits the enzyme cytidine deaminase, which rapidly inactivates AZA/DEC in vivo) Ebrahem Q et al. Oral presentation at ASH 2015. Abstract 678
Alternating (but not simultaneous) reduced-dose AZA + DEC in combination with THU increased response and survival in xenotransplant mice models of MDS/AML
Xenotransplant mice models of human MDS/AML were used to assess mechanism-based treatments were assessed that may extend response to AZA/DEC
Impact of treatment on survival Impact of treatment on haematopoiesis
6
4
2
0
Hb
leve
l, g
/dL
0 300100 200
Time, days
6
4
2
0W
BC
co
un
t, x
10
9/L
0 300100 200
Hb level
WBC count
1.0
0.0
0.5
Pro
bab
ility
of
surv
ival
0 100 200 300Time, days
No tx DEC 0.2mg/kg
DEC 0.1mg/kg + THU 8mg/kg 3x/wk (THU-DEC)
THU-DEC alternating with THU-AZA (1mg/kg 3x/wk)
Prognostic FactorsAre there new?

Landscape of Secondary Genetic Lesions in Acute Myeloid Leukemia with Inv(16)/CBFB-MYH11. Fasan A. et al., Blood 2015
NGS of 22-gene panel in 127 AML pts with CBFB-MYH11 AML
Additional cytogenetic aberrations in 38% of patients91% of patients had a secondary genetic lesions42% had 2-4 additional mutations (NRAS 35%, KIT 32%, FLT3 20%, KRAS 17%)
ASXL1 mutation 1% in CBFB-MYH11 pos AML vs 12% in RUNX1-RUNX1T1 pos AML
KRAS mut had worse prognosis OS 23% in mut vs 43% in wt KRAS pts (p<.001)Trisomy 22 and KIT mutations did not have any impact on survival.

DNMT3A Mutations Associate with Shorter Survival and Modulate the Prognostic Impact of Mutated NPM1: an Analysis Based on Comprehensive Mutational Screening of 660 AML Patients Treated on German AML Cooperative Group (AMLCG) Trials. Metzeler et al.
Mutazioni DNMT3A 30-40% CN-AML660 LAM Arruolate in studi del gruppo cooperatore tedescoEtà mediana 57 anni (18-86 anni)Sequenziamento Multiplexed amplicon delle varianti negli Esoni 7-23
207/660 (31%) AML RI ha mutazioni DNMT3A
Maggiore incidenza negli anziani e nelle donneIperleucocitosi e elevata conta di blasti midollari
Analisi Multivariata:
Mutazioni DNMT3A si associano aridotte RFS (HR: 1.44; P= 0.01) e OS (HR 1.26, P=0.04) nelle LAM NPM mutate, indipendentemente dalla presenza o meno dell’FLT3.

Characteristics and Prognosis of AML Patients with or without a History of Clonal Hematopoiesis. Thol F. et al., Blood 2015.
40 DNMT3A mutation in MNC, T cells CHIP (TET2, RUNX1, SF3B1, U2AF1 mutation) No change of allelic frequencies at relapse benefit from HSCT (HR .082, p=.027)
131 DNMT3A mutation only in MNC No CHIP
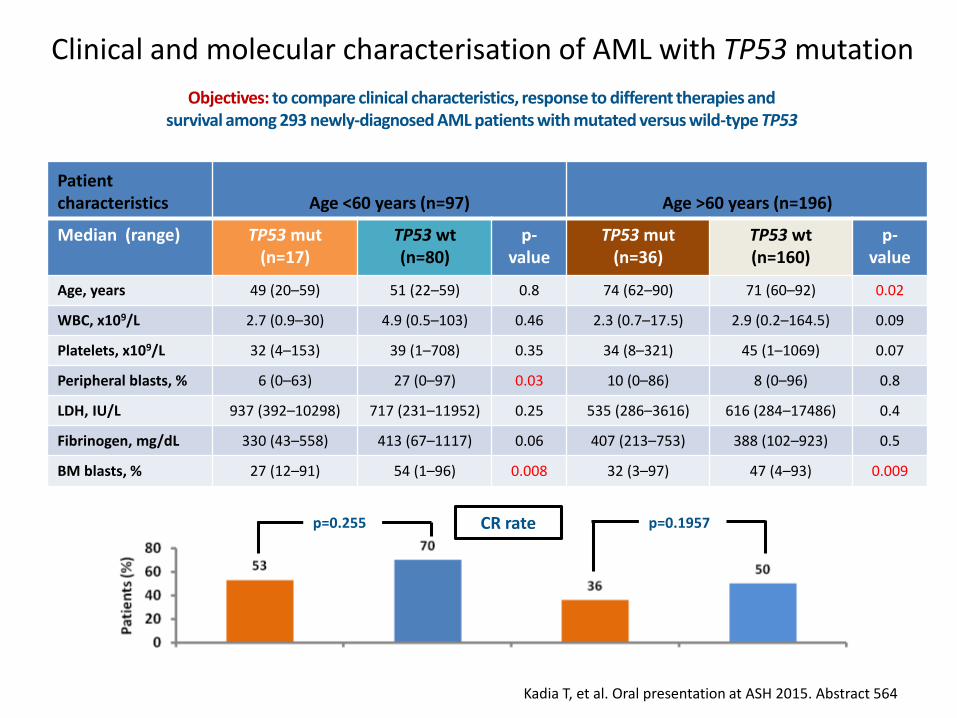
Clinical and molecular characterisation of AML with TP53 mutation
Kadia T, et al. Oral presentation at ASH 2015. Abstract 564
Patientcharacteristics Age <60 years (n=97) Age >60 years (n=196)
Median (range) TP53 mut(n=17)
TP53 wt(n=80)
p-value
TP53 mut(n=36)
TP53 wt(n=160)
p-value
Age, years 49 (20–59) 51 (22–59) 0.8 74 (62–90) 71 (60–92) 0.02
WBC, x109/L 2.7 (0.9–30) 4.9 (0.5–103) 0.46 2.3 (0.7–17.5) 2.9 (0.2–164.5) 0.09
Platelets, x109/L 32 (4–153) 39 (1–708) 0.35 34 (8–321) 45 (1–1069) 0.07
Peripheral blasts, % 6 (0–63) 27 (0–97) 0.03 10 (0–86) 8 (0–96) 0.8
LDH, IU/L 937 (392–10298) 717 (231–11952) 0.25 535 (286–3616) 616 (284–17486) 0.4
Fibrinogen, mg/dL 330 (43–558) 413 (67–1117) 0.06 407 (213–753) 388 (102–923) 0.5
BM blasts, % 27 (12–91) 54 (1–96) 0.008 32 (3–97) 47 (4–93) 0.009
Objectives: to compare clinical characteristics, response to different therapies and survival among 293 newly-diagnosed AML patients with mutated versus wild-type TP53
CR ratep=0.255 p=0.1957

Clinical and molecular characterisation of AML with TP53 mutation (18%)
Kadia T, et al. Oral presentation at ASH 2015. Abstract 564
Gene mutation screen
Disease characteristics
• Mutations less frequent in pts with TP53 mut versus TP53 wt:
– FLT3 (p=0.02)
– RAS (p=0.04)
– NPM1 (p=0.03)
– MPL (p=0.03)
– RUNX1 (p=0.09)
Characteristic, %TP53 mut
(n=53)TP53 wt(n=240) p-value
Complex karyotype 81 15 <0.0001
Diploid 9 49 <0.0001
–5/5q– and/or –7/7q– 72 16 <0.0001
Chrom 17 abn 53 5 <0.0001
tAML 30 13 0.0035
Prior haematological disorder 17 20 0.847
Response according to treatment regimen
p=0.3 p=0.6
p=0.8

Clinical and molecular characterisation of AML with TP53 mutation
NR = not reached Kadia T, et al. Oral presentation at ASH 2015. Abstract 564
Overall survival
1.0
Time, months
0.6
0
0.2
0.8
0.4
12 186 24 300
Surv
ival
pro
bab
ility
1.0
Time, months
0.6
0
0.2
0.8
0.4
12 186 24 300
Surv
ival
pro
bab
ility
Median OS: NR
10.7 months
12.6 months
6.6 months
p=0.005 p=0.004
TP53 wt (n=80)TP53 mut (n=17)
TP53 wt (n=160)TP53 mut (n=36)
Age <60 years Age ≥60 years
NEW DRUGSWHERE ARE WE?

Clinical Response to Idasanutlin (RG7388) in Acute Myeloid Leukemia Patients IsAssociated with Pre-Treatment MDM2 Protein Expression in Leukemic Blasts andLeukemic Stem Cells Reis B. et al., Blood 2015 Abs 2580
IDASANUTLIN
P53
MDM2Risposta a Idasanutlin correla con l’espressione di MDM2
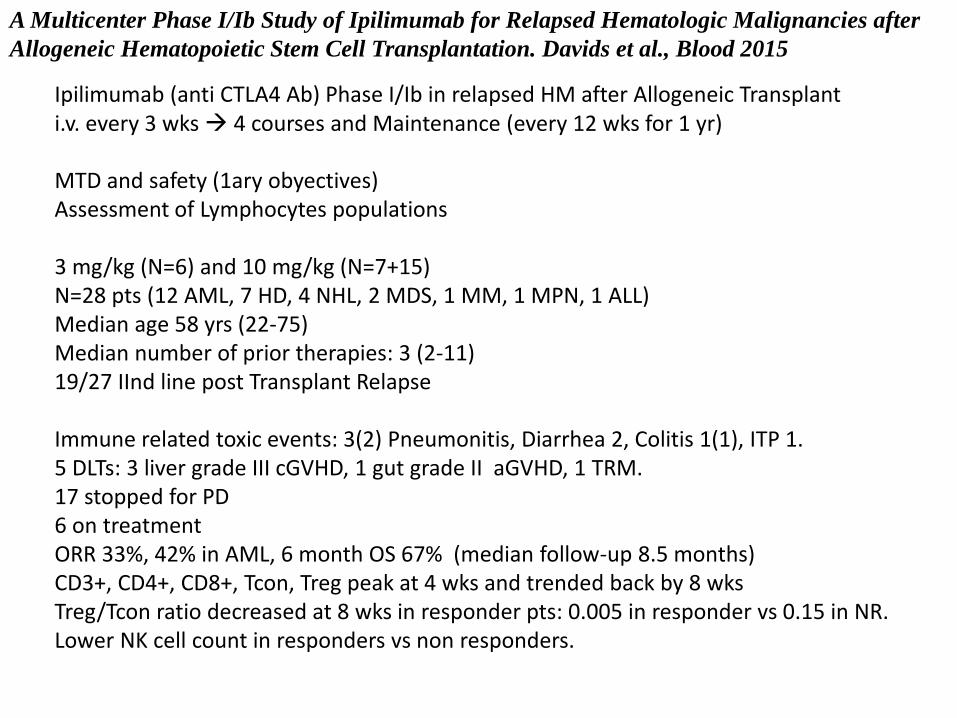
A Multicenter Phase I/Ib Study of Ipilimumab for Relapsed Hematologic Malignancies after
Allogeneic Hematopoietic Stem Cell Transplantation. Davids et al., Blood 2015
Ipilimumab (anti CTLA4 Ab) Phase I/Ib in relapsed HM after Allogeneic Transplanti.v. every 3 wks 4 courses and Maintenance (every 12 wks for 1 yr)
MTD and safety (1ary obyectives)Assessment of Lymphocytes populations
3 mg/kg (N=6) and 10 mg/kg (N=7+15)N=28 pts (12 AML, 7 HD, 4 NHL, 2 MDS, 1 MM, 1 MPN, 1 ALL)Median age 58 yrs (22-75)Median number of prior therapies: 3 (2-11)19/27 IInd line post Transplant Relapse
Immune related toxic events: 3(2) Pneumonitis, Diarrhea 2, Colitis 1(1), ITP 1.5 DLTs: 3 liver grade III cGVHD, 1 gut grade II aGVHD, 1 TRM.17 stopped for PD6 on treatmentORR 33%, 42% in AML, 6 month OS 67% (median follow-up 8.5 months)CD3+, CD4+, CD8+, Tcon, Treg peak at 4 wks and trended back by 8 wksTreg/Tcon ratio decreased at 8 wks in responder pts: 0.005 in responder vs 0.15 in NR.Lower NK cell count in responders vs non responders.

FLT3 INHIBITORS
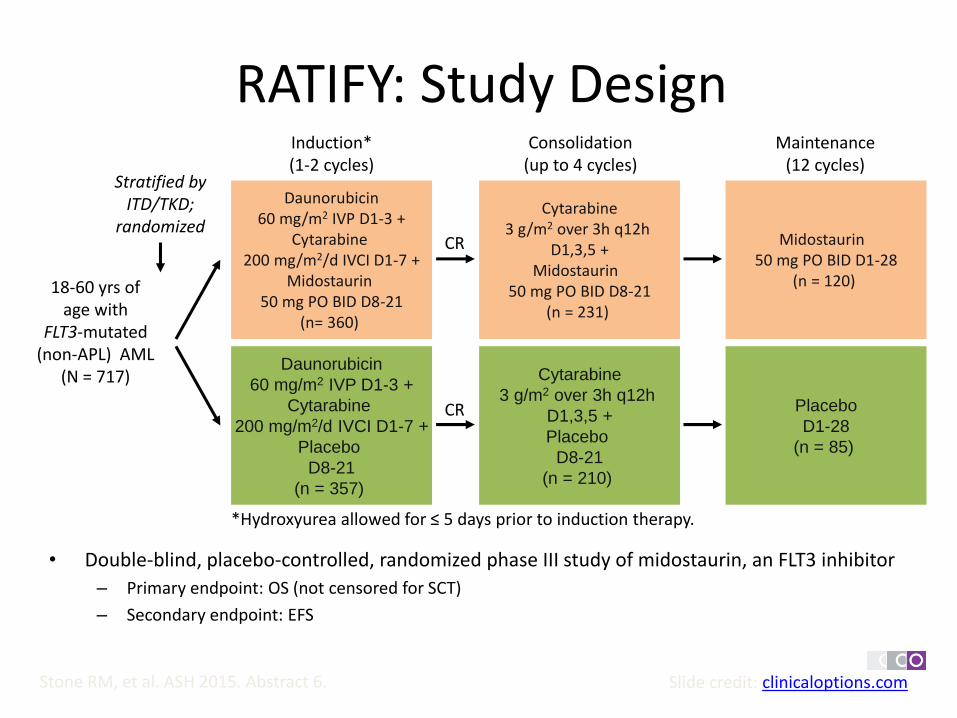
Slide credit: clinicaloptions.comStone RM, et al. ASH 2015. Abstract 6.
RATIFY: Study Design
• Double-blind, placebo-controlled, randomized phase III study of midostaurin, an FLT3 inhibitor
– Primary endpoint: OS (not censored for SCT)
– Secondary endpoint: EFS
18-60 yrs of age with
FLT3-mutated(non-APL) AML
(N = 717)
Daunorubicin60 mg/m2 IVP D1-3 +
Cytarabine200 mg/m2/d IVCI D1-7 +
Midostaurin50 mg PO BID D8-21
(n= 360)
Daunorubicin
60 mg/m2 IVP D1-3 +
Cytarabine
200 mg/m2/d IVCI D1-7 +
Placebo
D8-21
(n = 357)
Cytarabine3 g/m2 over 3h q12h
D1,3,5 +Midostaurin
50 mg PO BID D8-21(n = 231)
Cytarabine
3 g/m2 over 3h q12h
D1,3,5 +
Placebo
D8-21
(n = 210)
Midostaurin 50 mg PO BID D1-28
(n = 120)
Placebo
D1-28
(n = 85)
Stratified by ITD/TKD;
randomized
Induction* (1-2 cycles)
Consolidation (up to 4 cycles)
Maintenance (12 cycles)
CR
CR
*Hydroxyurea allowed for ≤ 5 days prior to induction therapy.

RATIFY: Efficacy
• Longer OS shown in midostaurin arm in all FLT3 cohorts.• 4-yr EFS rate was 28% with midostaurin vs 20% in placebo, regardless of FLT3
Slide credit: clinicaloptions.comStone RM, et al. ASH 2015. Abstract 6.
CharacteristicMidostaurin + Chemo
(n = 360)Placebo + Chemo
(n = 357)P Value
Median OS, mos (range) 74.7 (31.7-NE) 25.6 (18.6-42.9)
4-yr OS, % (95% CI) Uncensored* Censored for SCT†
51.4 (46.0-57.0)63.8 (56.0-71.0)
44.2 (39.0-50.0)55.7 (47.0-63.0)
.0074.04
SCT, n (%) Any time CR1 only
212 (59)100 (28)
196 (55)79 (22)
.28
.08
CR, n (%) By Day 60 In induction/consolidation
212 (59)239 (66)
191 (53)211 (59)
.15.045
Median EFS, mos (range) Uncensored Censored for SCT
8.0 (5.1-10.6)11.3 (8.4-15.1)
3.0 (1.9-5.9)6.1 (4.7-7.5)
.0025
.0002
DFS, mos (range) 25.9 (19.4-NE) 14.4 (11.0-22.2) .002
*HR: 0.77. †HR: 0.75.
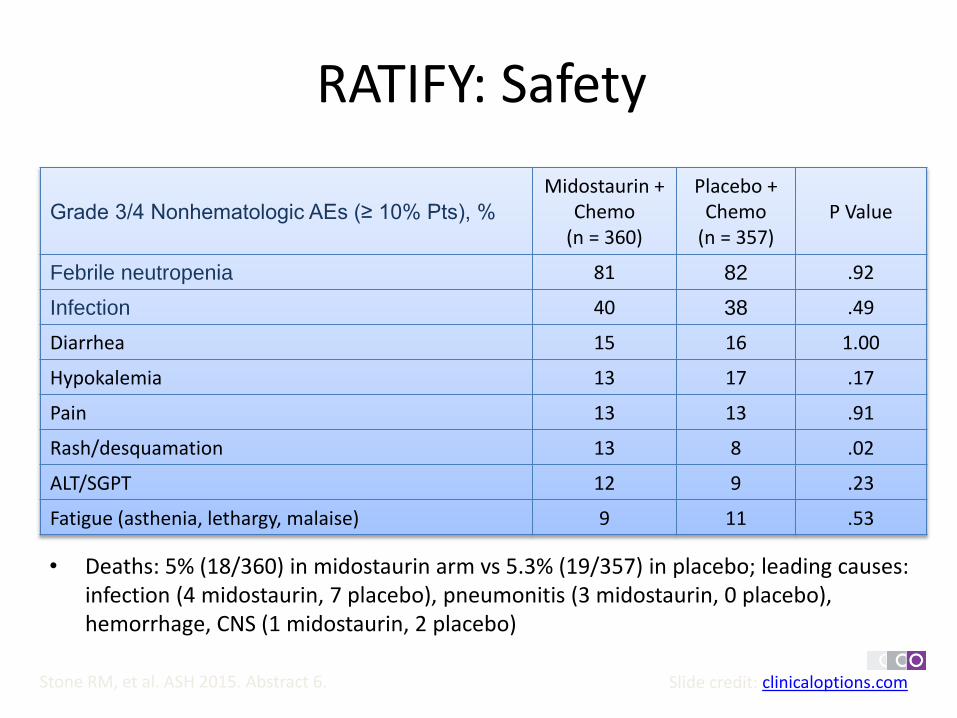
RATIFY: Safety
Slide credit: clinicaloptions.com
Grade 3/4 Nonhematologic AEs (≥ 10% Pts), %
Midostaurin + Chemo
(n = 360)
Placebo + Chemo
(n = 357)P Value
Febrile neutropenia 81 82 .92
Infection 40 38 .49
Diarrhea 15 16 1.00
Hypokalemia 13 17 .17
Pain 13 13 .91
Rash/desquamation 13 8 .02
ALT/SGPT 12 9 .23
Fatigue (asthenia, lethargy, malaise) 9 11 .53
• Deaths: 5% (18/360) in midostaurin arm vs 5.3% (19/357) in placebo; leading causes: infection (4 midostaurin, 7 placebo), pneumonitis (3 midostaurin, 0 placebo), hemorrhage, CNS (1 midostaurin, 2 placebo)
Stone RM, et al. ASH 2015. Abstract 6.
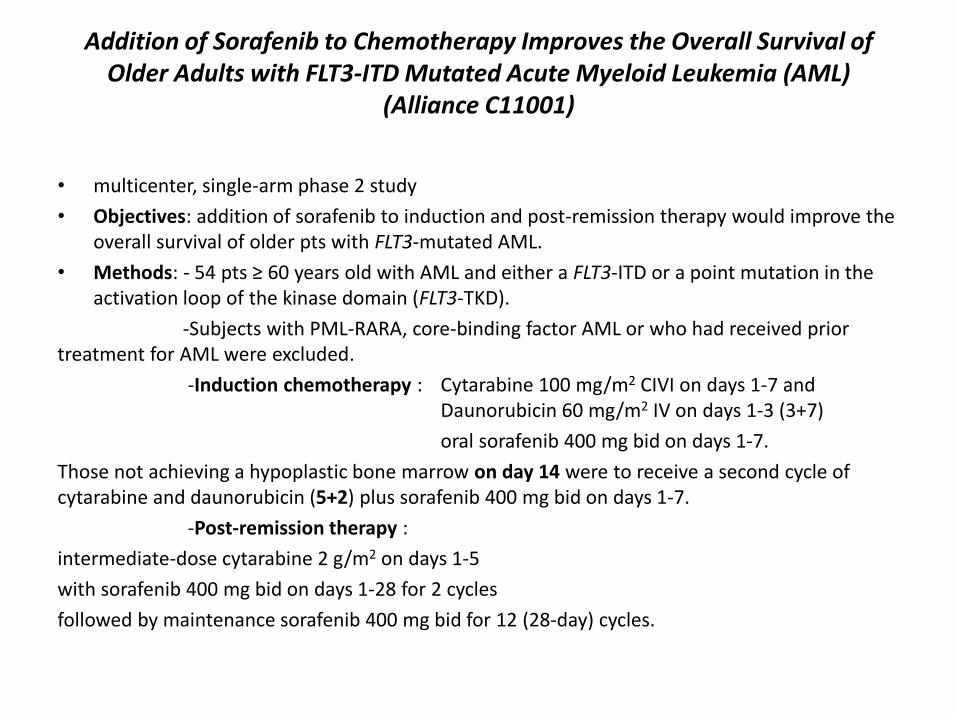
Addition of Sorafenib to Chemotherapy Improves the Overall Survival of Older Adults with FLT3-ITD Mutated Acute Myeloid Leukemia (AML)
(Alliance C11001)
• multicenter, single-arm phase 2 study
• Objectives: addition of sorafenib to induction and post-remission therapy would improve the overall survival of older pts with FLT3-mutated AML.
• Methods: - 54 pts ≥ 60 years old with AML and either a FLT3-ITD or a point mutation in the activation loop of the kinase domain (FLT3-TKD).
-Subjects with PML-RARA, core-binding factor AML or who had received prior treatment for AML were excluded.
-Induction chemotherapy : Cytarabine 100 mg/m2 CIVI on days 1-7 and Daunorubicin 60 mg/m2 IV on days 1-3 (3+7)
oral sorafenib 400 mg bid on days 1-7.
Those not achieving a hypoplastic bone marrow on day 14 were to receive a second cycle of cytarabine and daunorubicin (5+2) plus sorafenib 400 mg bid on days 1-7.
-Post-remission therapy :
intermediate-dose cytarabine 2 g/m2 on days 1-5
with sorafenib 400 mg bid on days 1-28 for 2 cycles
followed by maintenance sorafenib 400 mg bid for 12 (28-day) cycles.
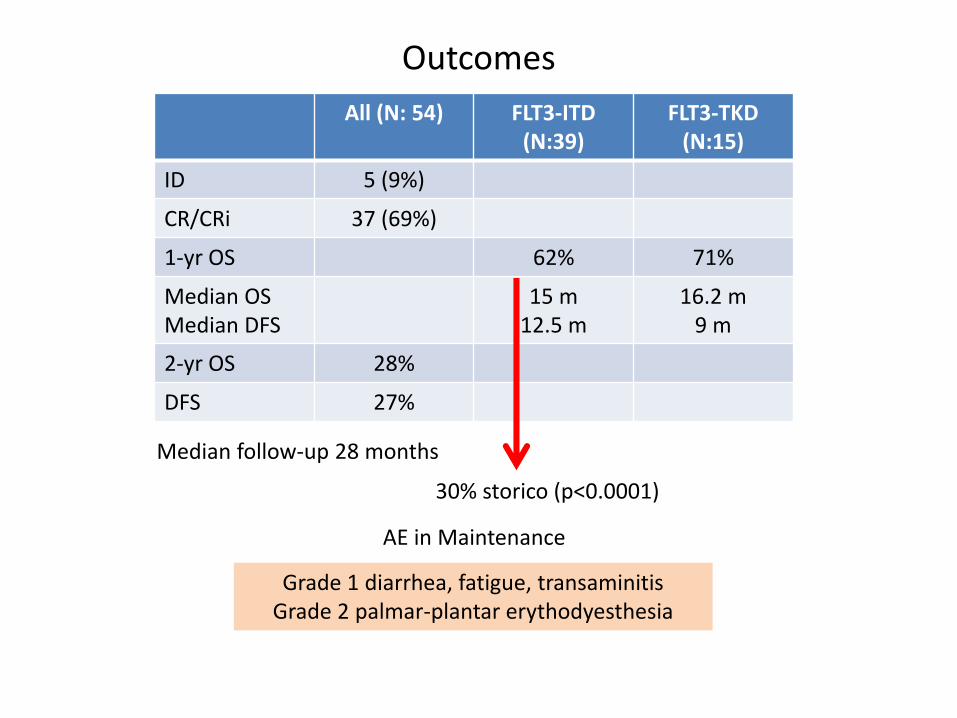
Outcomes
All (N: 54) FLT3-ITD (N:39)
FLT3-TKD (N:15)
ID 5 (9%)
CR/CRi 37 (69%)
1-yr OS 62% 71%
Median OSMedian DFS
15 m12.5 m
16.2 m9 m
2-yr OS 28%
DFS 27%
Median follow-up 28 months
Grade 1 diarrhea, fatigue, transaminitisGrade 2 palmar-plantar erythodyesthesia
AE in Maintenance
30% storico (p<0.0001)
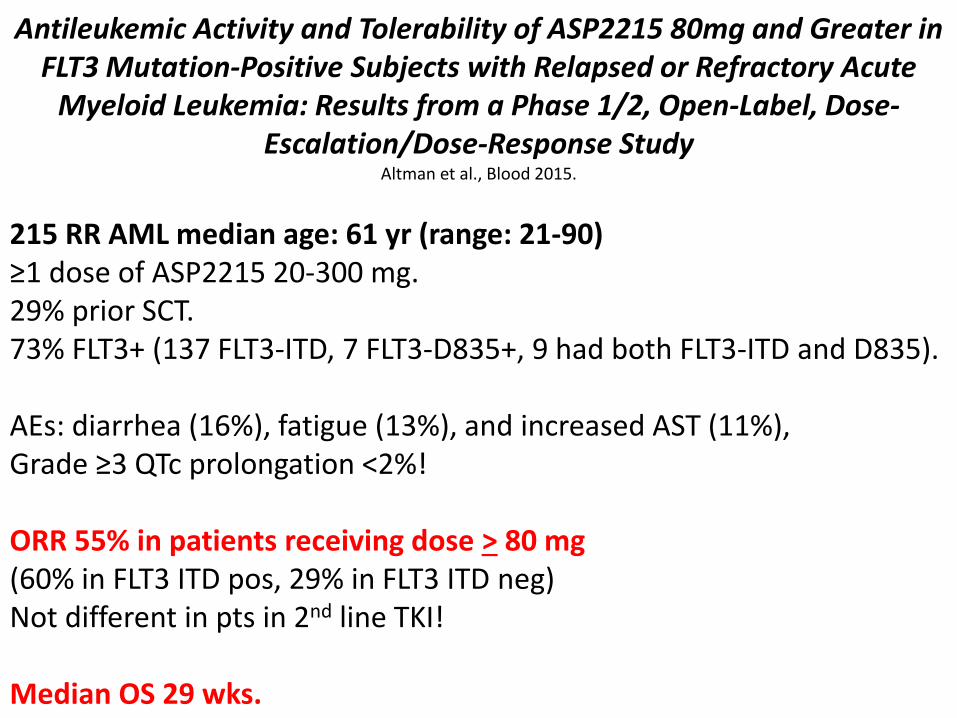
Antileukemic Activity and Tolerability of ASP2215 80mg and Greater in FLT3 Mutation-Positive Subjects with Relapsed or Refractory Acute
Myeloid Leukemia: Results from a Phase 1/2, Open-Label, Dose-Escalation/Dose-Response Study
Altman et al., Blood 2015.
215 RR AML median age: 61 yr (range: 21-90)≥1 dose of ASP2215 20-300 mg.29% prior SCT.73% FLT3+ (137 FLT3-ITD, 7 FLT3-D835+, 9 had both FLT3-ITD and D835).
AEs: diarrhea (16%), fatigue (13%), and increased AST (11%),Grade ≥3 QTc prolongation <2%!
ORR 55% in patients receiving dose > 80 mg(60% in FLT3 ITD pos, 29% in FLT3 ITD neg)Not different in pts in 2nd line TKI!
Median OS 29 wks.

INIBITORI IDH2

Safety and Efficacy of AG-221 ( NCT01915498), a Potent Inhibitor of Mutant IDH2 That Promotes Differentiation of Myeloid Cells in Patients with Advanced Hematologic Malignancies: Results of a Phase 1/2 Trial
• Phase 1\2 Trial (N=181 Ist and following lines)
• OBJECTIVES: -AG-221 safety, efficacy in pts with advanced myeloid malignancies; responding in RR-AML pts, evaluate response by mIDH2 mutation type, associations between ANC improvement and AEs, and mIDH2 VAF over time.
• METHODS: -Pts ≥18 years with mIDH2-positive myeloid malignancies
-AG-221 administered QD or BID in continuous 28-day cycles.
Dosing began at 50 mg QD or 30 mg BID and increased in subsequent cohorts.
-Response measured from peripheral blood (PB) and bone marrow (BM) samples on days 15, 29, 57, and every 56 days thereafter, and by objective investigator report.
- ANC ≥1.0x109/L increase from baseline (BL).
-assessment of mIDH2 VAF longitudinally using the FoundationOne Hemetest on purified mononuclear cells from BM or PB ( Next-generation sequencing)
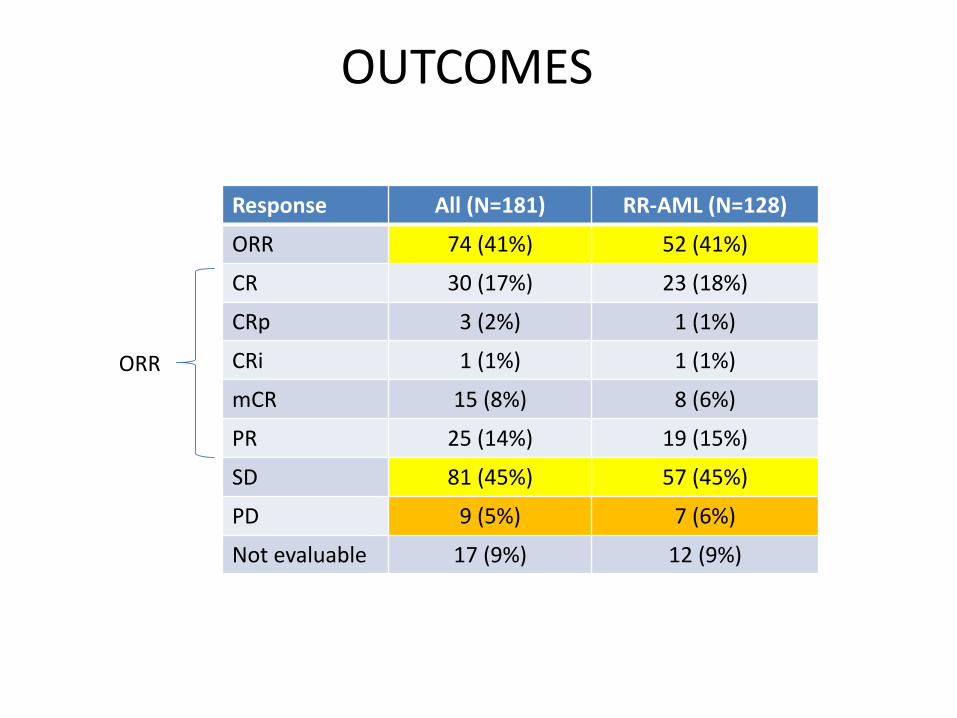
OUTCOMES
Response All (N=181) RR-AML (N=128)
ORR 74 (41%) 52 (41%)
CR 30 (17%) 23 (18%)
CRp 3 (2%) 1 (1%)
CRi 1 (1%) 1 (1%)
mCR 15 (8%) 8 (6%)
PR 25 (14%) 19 (15%)
SD 81 (45%) 57 (45%)
PD 9 (5%) 7 (6%)
Not evaluable 17 (9%) 12 (9%)
ORR
Conclusions
• AG-221 : well-tolerated and induce responses in pts with advanced myeloid malignancies, including heavily pretreated RR-AML.
• Response rates in RR-AML were consistent regardless of number of prior Tx regimens or mIDH2 type.
• mIDH2 VAF did not change from BL in responding pts;
• rapid ANC improvements suggest that despite the persisting mutant clone, differentiation into mature myeloid cells (eg, neutrophils) occurred.
ASSOCIAZIONI HMA
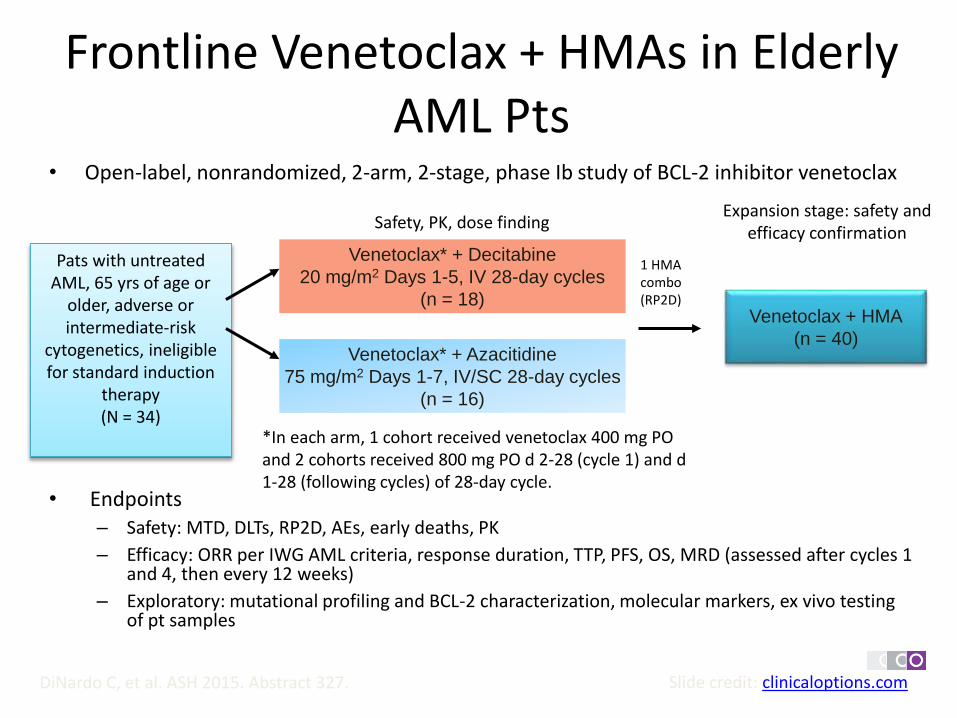
Frontline Venetoclax + HMAs in Elderly AML Pts
• Open-label, nonrandomized, 2-arm, 2-stage, phase Ib study of BCL-2 inhibitor venetoclax
• Endpoints– Safety: MTD, DLTs, RP2D, AEs, early deaths, PK
– Efficacy: ORR per IWG AML criteria, response duration, TTP, PFS, OS, MRD (assessed after cycles 1 and 4, then every 12 weeks)
– Exploratory: mutational profiling and BCL-2 characterization, molecular markers, ex vivo testing of pt samples
Slide credit: clinicaloptions.comDiNardo C, et al. ASH 2015. Abstract 327.
Pats with untreated AML, 65 yrs of age or
older, adverse or intermediate-risk
cytogenetics, ineligible for standard induction
therapy(N = 34)
Venetoclax* + Decitabine
20 mg/m2 Days 1-5, IV 28-day cycles
(n = 18)
Venetoclax* + Azacitidine
75 mg/m2 Days 1-7, IV/SC 28-day cycles
(n = 16)
Safety, PK, dose finding
Venetoclax + HMA
(n = 40)
Expansion stage: safety and efficacy confirmation
1 HMA combo (RP2D)
*In each arm, 1 cohort received venetoclax 400 mg PO and 2 cohorts received 800 mg PO d 2-28 (cycle 1) and d 1-28 (following cycles) of 28-day cycle.
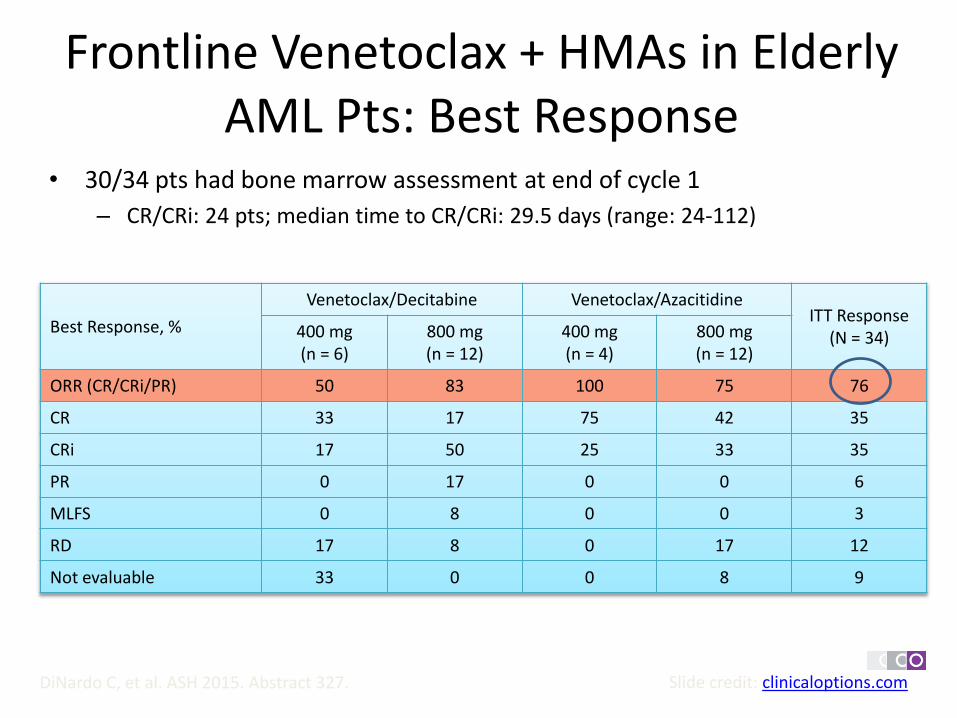
Frontline Venetoclax + HMAs in Elderly AML Pts: Best Response
• 30/34 pts had bone marrow assessment at end of cycle 1
– CR/CRi: 24 pts; median time to CR/CRi: 29.5 days (range: 24-112)
• Median days on study: 106.5 (range: 6-305)
Slide credit: clinicaloptions.comDiNardo C, et al. ASH 2015. Abstract 327.
Best Response, %
Venetoclax/Decitabine Venetoclax/AzacitidineITT Response
(N = 34)400 mg(n = 6)
800 mg(n = 12)
400 mg(n = 4)
800 mg(n = 12)
ORR (CR/CRi/PR) 50 83 100 75 76
CR 33 17 75 42 35
CRi 17 50 25 33 35
PR 0 17 0 0 6
MLFS 0 8 0 0 3
RD 17 8 0 17 12
Not evaluable 33 0 0 8 9
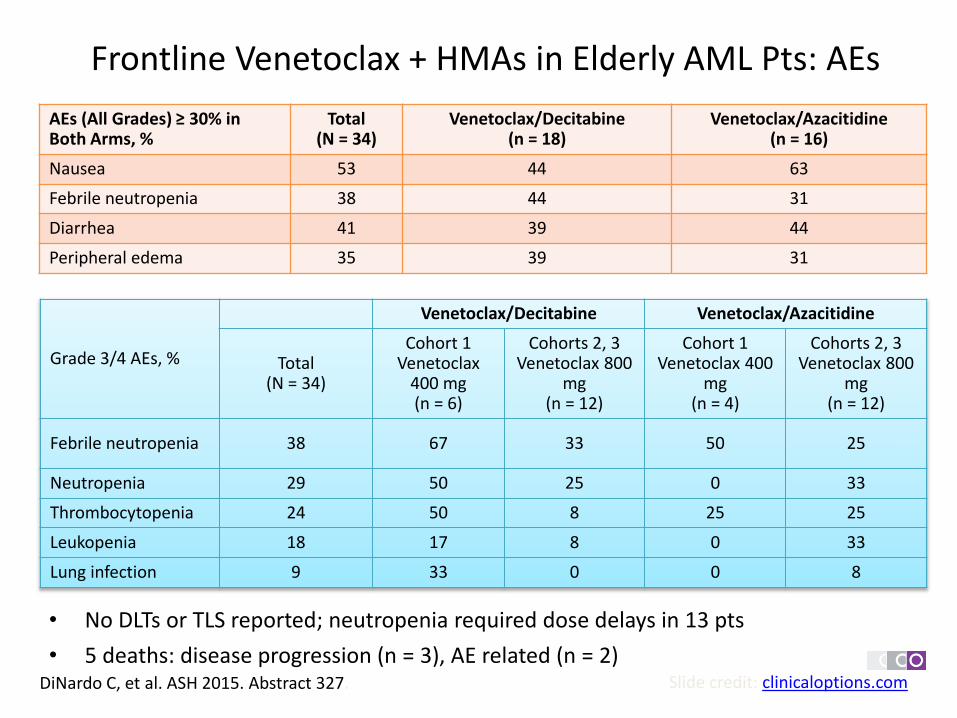
Frontline Venetoclax + HMAs in Elderly AML Pts: AEs
• No DLTs or TLS reported; neutropenia required dose delays in 13 pts
• 5 deaths: disease progression (n = 3), AE related (n = 2)DiNardo C, et al. ASH 2015. Abstract 327. Slide credit: clinicaloptions.com
AEs (All Grades) ≥ 30% in Both Arms, %
Total(N = 34)
Venetoclax/Decitabine(n = 18)
Venetoclax/Azacitidine(n = 16)
Nausea 53 44 63
Febrile neutropenia 38 44 31
Diarrhea 41 39 44
Peripheral edema 35 39 31
Grade 3/4 AEs, %
Venetoclax/Decitabine Venetoclax/Azacitidine
Total(N = 34)
Cohort 1Venetoclax
400 mg(n = 6)
Cohorts 2, 3Venetoclax 800
mg(n = 12)
Cohort 1Venetoclax 400
mg(n = 4)
Cohorts 2, 3Venetoclax 800
mg(n = 12)
Febrile neutropenia 38 67 33 50 25
Neutropenia 29 50 25 0 33
Thrombocytopenia 24 50 8 25 25
Leukopenia 18 17 8 0 33
Lung infection 9 33 0 0 8

Frontline Venetoclax + HMAs in Elderly AML Pts: Conclusions
• Combination venetoclax with decitabine or azacitidine tolerable, similar safety profile in both treatment arms
– No TLS or DLTs
• No effect of decitabine or azacitidine on venetoclax exposure in early pharmacokinetic data
• Early CR/CRi observed across all treatment cohorts and arms as compared with HMA alone
• MTD not reached in either arm; dose escalation ongoing
• Study will progress to expansion stage
• Alternative venetoclax schedule to address dose delays due to neutropenia
Slide credit: clinicaloptions.comDiNardo C, et al. ASH 2015. Abstract 327.

Mechanisms of Acquired Resistance to Venetoclax in Preclinical AML Models. Zhang et al., Blood 2015
Venetoclax Anti-apoptotic BCL-2 induction of apoptotic BAX3 and BH3 proteins
5 VEN-resistant cell lines immunoblotting showed increase of MCL-1 or BCL-Xl(anti apoptotic proteins)
Inhibitor of MCL-1 and BCL-XL inhibits growth in all parental cell lines
Venetoclax increases the response to MCL-1 inhibitor in 4/5 VEN-resistant cell lines
mTOR, MEK and Flt3 pathways are implicated
mTOR inhibitor AZD2014 achieved synergistic effects in 5 resistant cell linesRapamicina synergistic in 3 cell lines
FLT3 inhibitor Quizartinib and Sorafenib are not synergistic with VEN, BUT are sensitive in the 2 FLT3pos resistant cell lines
In vivo Model of Venetoclax resistant AML showed that BCL-XL and BCL-2 were decreased in Blasts resistant to Venetoclax 4 wks infusion indicating that BCL proteins antiapoptotic and proapoptotic balance is at the basis of the mechanism of Resistance to Venetoclax.

Pracinostat + Azacitidine in Elderly AML: Study Design
• Multicenter, open-label, single-arm phase II study of HDAC inhibitor pracinostat combined with azacitidine
• Response assessments at end of cycle 1 or 2 then every other cycle until CR achieved or when clinically indicated
• Primary endpoint: CR + CRi + MLFS (IWG criteria)
• Secondary endpoints: ORR, DoR, EFS, OS, complete cytogenetic response + molecular complete remission, safety Slide credit: clinicaloptions.com
Garcia-Manero G, et al. ASH 2015. Abstract 453.
Pts 65 yrs of age or older,
previously untreated AML (≥ 20% bone marrow blasts),
unsuitable for intensive chemotherapy,
intermediate- or high-risk cytogenetics
(N = 50)
Pracinostat 60 mg PO
Days 1, 3, 5 for 21 days
Azacitidine 75 mg/m2 SC or IV
Days 1-7 or Days 1-5, 8, 9
28-day cycle
Intolerance, lack of response, or PD

Pracinostat + Azacitidine in Elderly AML: Efficacy
• CR + CRi + morphologic leukemia-free state: 56%
– CR: 42% (N:21)
• 19/21 pts who achieved CR still living
• 1-yr survival among pts achieving CR: 100%
• At median observation time of 14.3 mos, median OS not yet reached in overall study population
– Estimated 1-yr overall OS: 56%
– Median OS with high-risk cytogenetics: 13.3 mos(n = 21)
Slide credit: clinicaloptions.comGarcia-Manero G, et al. ASH 2015. Abstract 453.

Pracinostat + Azacitidine: Safety
Slide credit: clinicaloptions.comGarcia-Manero G, et al. ASH 2015. Abstract 453.
AE % All Grades(N = 50)
Grades 3/4(N = 50)
Hematologic
Febrile neutropenia 40 32
Thrombocytopenia 32 32
Anemia 26 14
Neutropenia 24 22
Nonhematologic
Nausea 66 4
Constipation 58 0
Fatigue 48 16
Diarrhea 30 2
Vomiting 28 2
Decreased appetite 28 4
Hypokalemia 26 0
Pyrexia 24 0
Dizziness 24 0
Dyspnea 24 0
Rash 20 0

Pracinostat + Azacitidine in Elderly AML: AEs Leading to Discontinuation
Slide credit: clinicaloptions.comGarcia-Manero G, et al. ASH 2015. Abstract 453.
Treatment-Emergent AEs Leading to Drug Discontinuation (n = 8)
Cycle/Day Outcome
Sepsis, grade 5 1/6 Fatal
Sepsis, grade 5 1/17 Fatal
Prolonged QTc/AF, grade 3 2/4 Resolved
Failure to thrive, grade 2 2/39 Not recovered
Parainfluenza, grade 3 3/9 Resolved with sequelae
Peripheral motor neuropathy, grade 3 3/35 Resolved
Mucositis, grade 3 3/9 Not recovered
Fatigue, grade 2 4/28 Not recovered

Pracinostat + Azacitidine in Elderly AML: Conclusions
• Pracinostat combined with azacitidine shows clinical activity in elderly pts with newly diagnosed AML– 56% achieved primary endpoint of CR + CRi + MLFS
– CR rate: 42%
• Most clinical responses occur within first 2 cycles and continue to improve with ongoing therapy
• Investigators concluded that pracinostat and azacitidinegenerally well tolerated in this population – At least 5 pts have received study drug beyond 1 yr
• Phase III study planned for 2016
Slide credit: clinicaloptions.comGarcia-Manero G, et al. ASH 2015. Abstract 453.
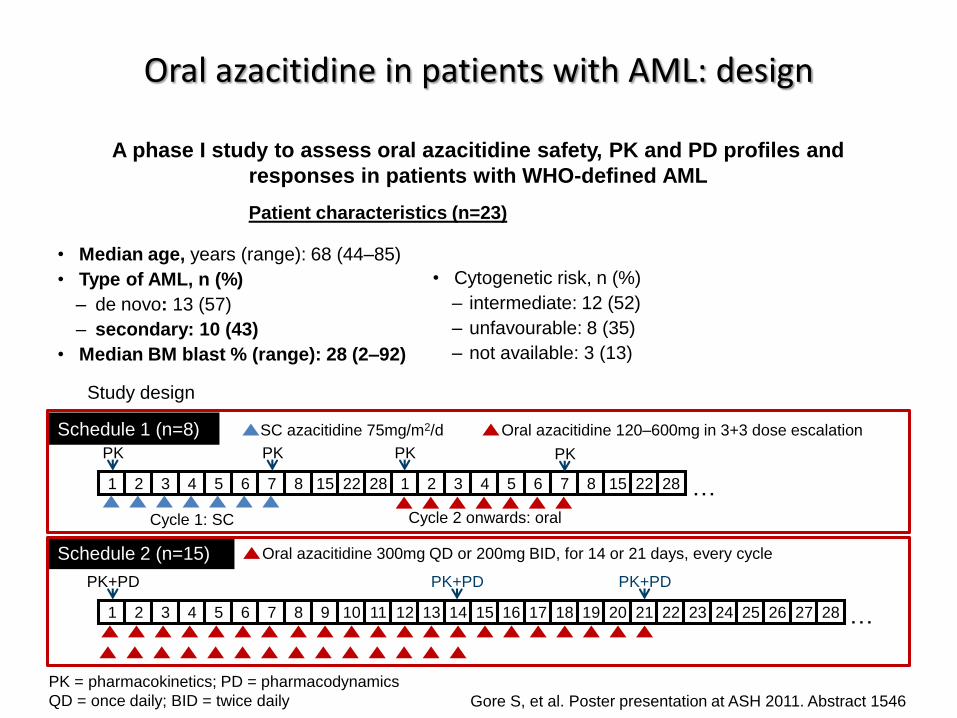
Oral azacitidine in patients with AML: design
Gore S, et al. Poster presentation at ASH 2011. Abstract 1546
A phase I study to assess oral azacitidine safety, PK and PD profiles and
responses in patients with WHO-defined AML
Patient characteristics (n=23)
• Median age, years (range): 68 (44–85)
• Type of AML, n (%)
– de novo: 13 (57)
– secondary: 10 (43)
• Median BM blast % (range): 28 (2–92)
Study design
Schedule 1 (n=8)
Schedule 2 (n=15)
1 2 3 4 5 6 7 8 15 22 28 1 2 3 4 5 6 7 8 15 22 28
• Cytogenetic risk, n (%)
– intermediate: 12 (52)
– unfavourable: 8 (35)
– not available: 3 (13)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28
PK PK PK PK
PK+PD PK+PD PK+PD
SC azacitidine 75mg/m2/d Oral azacitidine 120–600mg in 3+3 dose escalation
Cycle 1: SC Cycle 2 onwards: oral
Oral azacitidine 300mg QD or 200mg BID, for 14 or 21 days, every cycle
…
…
PK = pharmacokinetics; PD = pharmacodynamics
QD = once daily; BID = twice daily

Oral azacitidine in patients with AML: outcomes
Gore S, et al. Poster presentation at ASH 2011. Abstract 1546
Oral azacitidine was well tolerated and showed bioactivity in patients with AML
Response
mCR mPR HI RBC TI Platelet TI
0
10
20
30
40
Pa
tie
nts
, %
Median no. cycles received, n (range): 4 (1–14)
Toxicities
AE Grade 3/4, % AE Grade 3/4, %
Febrile neutropenia 35 Diarrhoea 9
Pneumonia 17 Fatigue 9
Syncope 17 Dehydration 9
Nausea 13 Headache 9
Thrombocytopenia 9 Mental status changes 9
PK
• No accumulation following multiple oral doses
• Single 300mg oral azacitidine dose:
– AUC0–∞ = 230±210 ng*hr/mL
– Cmax = 150±114 ng/mL
– t½ = 0.54±0.21 hr
– median Tmax = 0.8 hr
• Compared with SC azacitidine, cumulative exposure on schedule 2: 55–104% (300mg QD, 200mg BID, respectively)
Schedule 1 Schedule 2
25
0
13
33
13
2725
40
0
17
mPR = marrow partial response
Hematological Response

Phase I/II Study of Vosaroxin and Decitabine in Newly Diagnosed Older Patients (pts) with Acute Myeloid Leukemia (AML) and High Risk
Myelodysplastic Syndrome (MDS) Abs 461 Daver et al.
Induction dose N
Median
OS
8-wk
mortality ORR CR
Response after 1°
cycle
90 mg/m2 22 5.5 mos 25% 73% 41% 23%
70 mg/m2 34 11.5 mos 6% 79% 62% 23%
Topoisomerase inhibitor P-gp and p-53 indipendent
50 AML 6 HR MDS
Median age 69 yrs (range 60-78)
Median follow-up 4.7 months (1.3-20.8)
Parameter Category N
Overall response
(CR, CRp, CRi) CR
Cytogenetics
Diploid 19 86% 57%
-5/-7/adverse 21 68% 42%
Miscellaneous 16 75% 63%
Mutation
Status
IDH2 11 91% 73%
IDH1 14 57% 43%
TP53 11 73% 55%
RAS 11 64% 28%
Vosaroxin 90 mg/m2 days 1 and 4 early mortality 25%.
Vosaroxin 70 mg/m2 days 1 and 4 early mortality 6%.
Decitabine 20 mg/m2 for 5 days.
Up to 7 cycles.
Vosaroxin 90
Vosaroxin 70
Main toxicity grade III-IV Mucositis

SGN-CD33A = anticorpo diretto contro il CD33 coniugato a 2 molecole dipirrolobenzodiazepina (PBD)
meccanismo d’azione: SGN-CD33A si lega al marcatore CD33,viene internalizzato e trasportato ai lisosomi dove il dimero PBDviene rilasciato e si lega al DNA della cellula portando ad apoptosi
Anticorpi Monoclonali
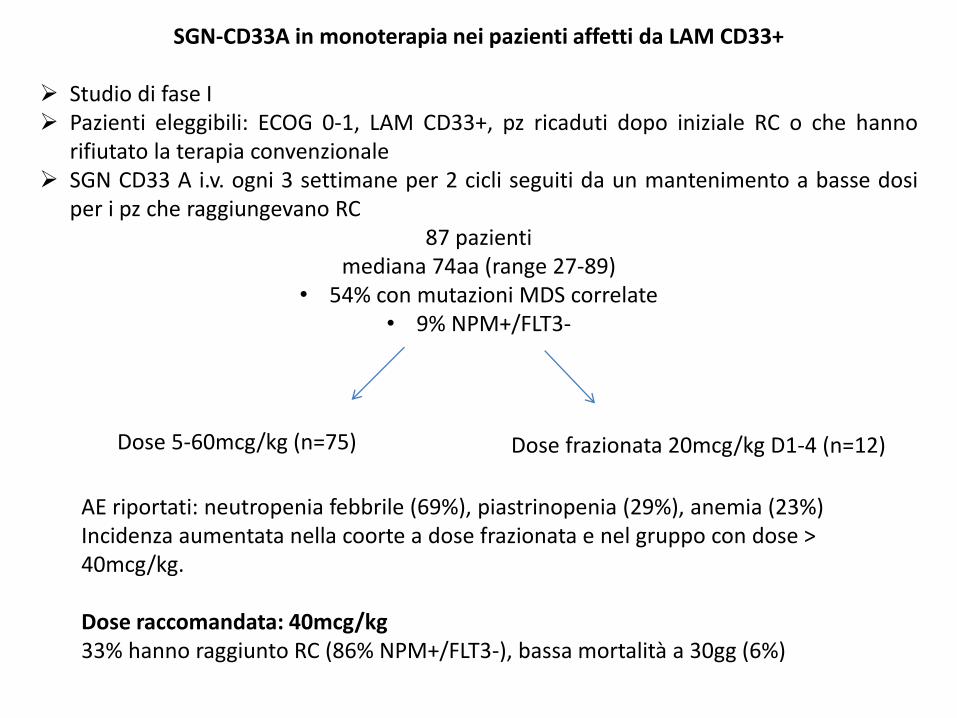
SGN-CD33A in monoterapia nei pazienti affetti da LAM CD33+
Studio di fase I Pazienti eleggibili: ECOG 0-1, LAM CD33+, pz ricaduti dopo iniziale RC o che hanno
rifiutato la terapia convenzionale SGN CD33 A i.v. ogni 3 settimane per 2 cicli seguiti da un mantenimento a basse dosi
per i pz che raggiungevano RC87 pazienti
mediana 74aa (range 27-89)• 54% con mutazioni MDS correlate
• 9% NPM+/FLT3-
Dose 5-60mcg/kg (n=75) Dose frazionata 20mcg/kg D1-4 (n=12)
AE riportati: neutropenia febbrile (69%), piastrinopenia (29%), anemia (23%)Incidenza aumentata nella coorte a dose frazionata e nel gruppo con dose > 40mcg/kg.
Dose raccomandata: 40mcg/kg 33% hanno raggiunto RC (86% NPM+/FLT3-), bassa mortalità a 30gg (6%)
SGN-CD33A in combinazione con agenti ipometilanti (AZA o Decitabina)
l’associazione si basa sul riscontro su modelli preclinici di aumentati livelli di CD33 espressi dalle cellule tumorali in seguito al trattamento con agenti ipometilanti (dal 2° al 4° giorno di trattamento con Decitabina e dal 4° giorno con AZA)
Più dimeri di PBD vengono internalizzati e legati al DNA con aumento dei livelli di PARP (marker apoptotico)
L’associazione determinerebbe una riduzione della crescita delle cellule tumoralicon maggiore attività antitumorale

SGN-CD33A in combinazione con agenti ipometilanti (AZA o Decitabina)
Studio di fase I Pazienti eleggibili: ECOG0-1, LAM CD33+ mai trattata o che ha rifiutato la
chemioterapia standard SGN-CD33 A 10 mcg/kg i.v ogni 4 settimane l’ultimo giorno di trattamento con
agenti ipometilanti (7°gg per AZA e 5°gg per Decitabina)
24 pazientiMediana 77 aa (range 66-83)
AE riscontrati: neutropenia febbrile (46%), anemia (25%), neutropenia (25%),piastrinopenia (21%)
- 65% hanno raggiunto RC dopo 2 cicli di trattamento(75% evoluti da MDS, 89% con cariotipo sfavorevole)
- 4% mortalità a 60 giorni

A Phase II of Combination D aunorubicin and Cytarabine (A ra-c) and Nilotinib (TA signa) (DATA) in Patients Newly Diagnosed with Acute Myeloid
Leukemia and KIT Expression: Interim Results
• A single arm, Phase II study,
• Goals: To study the efficacy and safety of combination 7+3 and nilotinib in patients (pts) with AML and KIT expression. Primary goal is to determine the complete response (CR) rate; secondary goals include 2-year overall survival (OS) and disease free survival (DFS) in addition to safety of DATA regimen.
• Methods: -Pts newly diagnosed with AML with KIT (CD117) expression of 20% or higher on myeloblasts by flow cytometry.
induction (3+7)and consolidation (4 ARAC HD)
+ Nilotinib 300 mg twice daily on days 4-14
continuous daily maintenance therapy for up to 2 years.
Conclusions
• Combination daunorubicin and cytarabine with nilotinib (DATA) appears to be safe and effective.
• Interim results show an acceptable safety profile in the first 12 evaluable pts with most common AE being infection as expected.
• Thirty day mortality is acceptable (7%).
• DATA regimen has encouraging CR rates of 80% (intent to treat) and 86% in assessed pts, with half of the pts who achieved remission requiring 2 cycles of induction.
• Relapse rate seems to be low at 17%.

Selinexor, ARA-C and Idarubicin: An Effective and Tolerable Combination in Patients with Relapsed/Refractory AML: A Multicenter Phase II Study
• Multicenter Phase II Study
• Aims: -efficacy & tolerability of Ara-C and Idarubicin in combination with selinexor in patients with relapsed or refractory AML;
-percentage of patients achieving a complete remission or complete remission without normalization of peripheral blood counts (CRi).
-partial remission rate, percentage of patients undergoing subsequent allogeneic stem cell transplantion, early death rate, overall survival (OS), event-free survival and toxicity.
• Methods:- Patients with RR AML were treated with Ara-C (100 mg/m2, continuous infusion, day 1-7), idarubicin (10 mg/m2, day 1, 3, 5) every 4 weeks.
• Selinexor was administered twice weekly orally starting on day 2 (40 mg/m2).• A small cohort of patients received selinexor after registration and before first
induction cycle for correlative studies.

Outcome
Response All (N=21)*
ORR 60%
CR 25%
CRi 25%
PR 10%
SCT/DLI 60%
*Median age: 60 yr (range 34-78).Karyotype: 7 complex, 6 normal, 7 unknown.Median prior courses: 3.5 (range 1-6).
2 primary refractory, 11 early relapse, 7 late relapse, 7 prior allogeneic transplantation.
1 death for subarachnoid haemorrhage during thrombocytopenia grade 4.
Extrahematological AE:vomiting, diarrhoea, nausea,fatigue, anorexia,neutropenic fever.


TRAPIANTO ALLOGENICO
Results of a Two-Arm Phase II Clinical Trial Using Post-Transplantation Cyclophosphamide for Prevention of Graft-Versus-Host Disease in Haploidentical and Mismatched Unrelated Donors Hematopoietic
Stem-Cell Transplantation. Gaballa S. et al., Blood 2015
HAPLO (n=60) and 9/10 MUD (n=46) Advanced hematologic malignancies or aplastic anemia.
Conditioning:(FM140)MEL 140 mg/m2 (day -7),Thiotepa 5 mg/kg (day -6)/TBI 2Gy -1,and four daily IV doses of fludarabine 40 mg/m2 (day -5 to day -2)
>55 years or with significant comorbidities received FM100 with MEL100 mg/m2
CD20+ Lymphoma received Rituximab (375 mg/m2) on days -13, -6, +1 and +8.
GVHD prophylaxis:PTCy 50 mg/kg on day +3 and +4, tacrolimus 6 m and mycophenolate for 3 m.
Stem cell source: BM except 2 PB in the HAPLO arm and 8 in the 9/10 MUD arm.

Aplo 9/10 MUD Aplo 9/10 MUD
Median Age, (Range) 45 (20-63) 51 (20-64) Diagnosis
Sex (M/F) 29/31 23/23 AML/MDS 33 (55%) 18 (39%)
KPS>90 53 (88%) 40 (87%) Lymphoma 10 (17%) 13 (28%)
KPS<90 7 (12%) 6 (13%) Others 10 (17%) 10 (22%)
Disease Risk Index* Disease Stage
Very high 5 (8%) 3 (7%) AL CR1/CR2 24 (66%) 9 (56%)
High 18 (30%) 15 (33%) AL CR3 or higher/ CRpx 6 (17%) 5 (31%)
Intermediate 29 (48%) 12 (26%) AL Active disease 6 (17%) 2 (13%)
Low 8 (13%) 12 (26%) Lymphoma CR 3 (30%) 8 (62%)
NA 0 4 (9%)** Lymphoma PR 5 (50%) 3 (23%)
Conditioning Regimen Lymphoma Chemoresistant 2 (20%) 2 (15%)
FM100 20 (33) 18 (39%) Follow up
FM140 40 (67%) 28 (61%) Median 24 m 29 m
Patients’ Characteristics

Haplo 9/10 MUD
Median time to ANC recovery (days) 18 18
Median time to platelet recovery (days) 25 28
Primary graft failure 2/60 (3%) 1/46 (2%)
mixed donor chimerism at day 100 1/60 (1.7%) 1/46 (2.2%)
1-yr OS 70% 60%
1-yr PFS 60% 47%
II-IV aGVHD d100 28% 3%
2 yr cGVHD 13% 14%
1 yr NRM 21% 31%
1 yr RR 19% 25%
Results
NS
NS
NS
NS

COSA FARE QUANDO FALLISCE

Efficacy, Safety and Long Term Results of Prophylactic and Preemptive Donor Lymphocyte Infusion after Allogeneic Stem Cell Transplantation for Acute Leukemia: A Registry-Based
Evaluation on 343 Patients By the Acute Leukemia Working Party of EBMT. Schmid, et al., Blood 2015.
Survey of 343 patients with AML (n=266) or ALL (n=77), who received DLI in CHR after alloSCT.
Median age: 48y.CR1/CR2/advanced disease in 68%/14%/17%.Standard/reduced intensity conditioning in 53%/47%.
Pre emptive DLI persisting mixed or decreasing donor cells chimerism (n=167, 49%) and persisting or recurrent minimal residual disease (MRD; n=32, 9%).ProDLI 144 patients (42%) with high risk disease without any sign of relapse.
Median follow up from DLI1 was 6.5 years (range, 1.1-14.5).Median interval from alloSCT to first DLI (DLI1) was 180 days (range, 15-1178).Median No.: 2 infusions.Median CD3+ cell dose at DLI1: 1x106/kg (range, 0.1-163). STOP DLI: end of treatment (56%), GvHD (17%), PD (13%), and documented improvement of donor chimerism (6%).
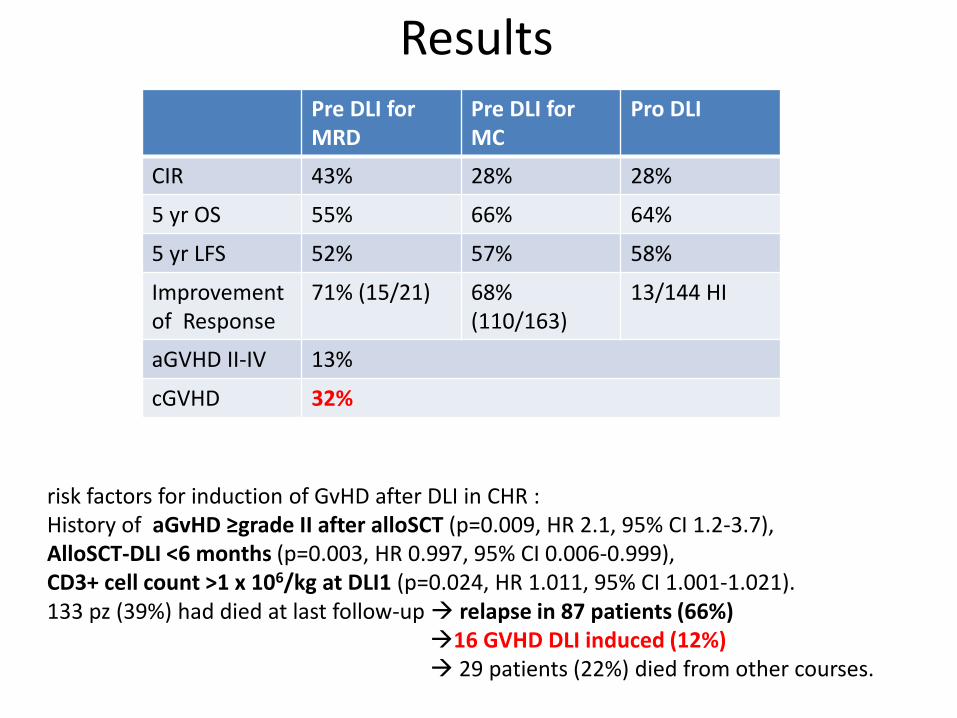
risk factors for induction of GvHD after DLI in CHR :History of aGvHD ≥grade II after alloSCT (p=0.009, HR 2.1, 95% CI 1.2-3.7),AlloSCT-DLI <6 months (p=0.003, HR 0.997, 95% CI 0.006-0.999),CD3+ cell count >1 x 106/kg at DLI1 (p=0.024, HR 1.011, 95% CI 1.001-1.021).133 pz (39%) had died at last follow-up relapse in 87 patients (66%)
16 GVHD DLI induced (12%) 29 patients (22%) died from other courses.
Pre DLI forMRD
Pre DLI forMC
Pro DLI
CIR 43% 28% 28%
5 yr OS 55% 66% 64%
5 yr LFS 52% 57% 58%
Improvementof Response
71% (15/21) 68% (110/163)
13/144 HI
aGVHD II-IV 13%
cGVHD 32%
Results

Hematopoietic Cell Transplantation with or without Sorafenib Maintenance for Patients with FLT3-ITD Acute
Myeloid Leukemia in CR1.Brunner et al., Blood 2015.
Landmark Analysis (median date of Sorafenib starting: d +68) of AML patients receiving or not Sorafenib.
Sorafenib Maintenance (26) Control (41) p
Median Follow-up 22.1 m (6.3-49.8) 37.5 m (12.4-88.9) 0.02
2 yr OS 83% (HR for death 0.146) 58% 0.019
2 yr DFS 85% 52% 0.0047
2 yr CIR 9.5% 41% 0.0065
aGVHD 2/26 (7.7%) 4/41 (9.75%) NS
2 yr NRM 5.7% 7.6% 0.61
1 yr cGVHD 50% 37% 0.31
80 consecutive AML FLT3-ITDpos (2008-2014) HCT in CR1.

Phase I Trial of IL-21 Ex Vivo Expanded NK Cells Administration to Prevent Disease Relapse after Haploidentical Stem-Cell Transplantation for Myeloid Leukemias.
O Ciurea et al., Blood 2015.
PB MNC from donor obtained prior to marrow harvest expanded ex vivo for 14 days with K562 APC expressing membrane-bound (mb) IL21.
Infused on days -2 (fresh), +7 and on/after +28 (cryopreserved).
Dose escalation 1x104/kg (N=1), 1x105/kg (N=2), 1x106/kg (N=3) and 1x107/kg (N=2)
Evaluation of NK alloreactivity and/or donor KIR B genotyping.
Mel Fluda TBI

Results
8/10 pts (5 AML and 3 CML).
Median age was 39 years (range 18-59)
Median time to PMN engraftment 18 daysMedian time to platelet engraftment 26 days
Grade II aGVHD 2/8 (25%), Grade III-IV aGVHD and cGVHD 0%.
Low rate of viral reactivation 43% (3/7) CMV reactivation vs 71% in retrospective data.
1 secondary graft failure 2nd Transplant from different donor Death.1 relapse after 1x105/kg NK cell dose salvage treatment, alive at last follow-up6 alive and disease free after a median follow-up of 6 months (range 1-12.5).

Can we measure MRD?How? When? And Then?
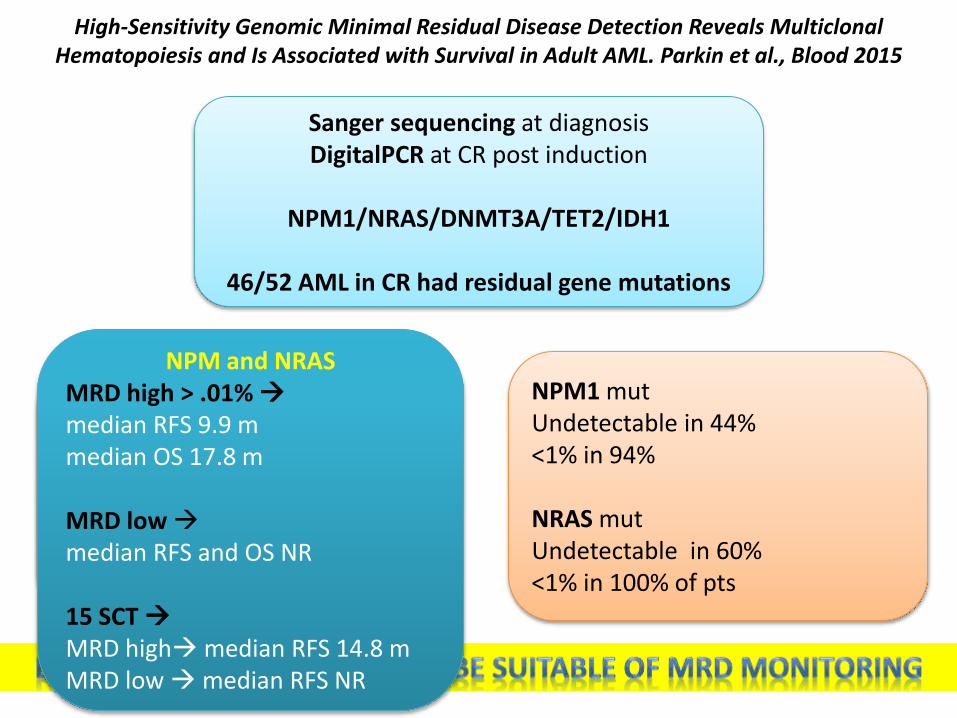
High-Sensitivity Genomic Minimal Residual Disease Detection Reveals Multiclonal Hematopoiesis and Is Associated with Survival in Adult AML. Parkin et al., Blood 2015
Sanger sequencing at diagnosisDigitalPCR at CR post induction
NPM1/NRAS/DNMT3A/TET2/IDH1
46/52 AML in CR had residual gene mutations
DNMT3A >1% VAF in 85%
TET2 >1% VAF in 50%
No correlation with RFS
NPM1 mutUndetectable in 44%<1% in 94%
NRAS mutUndetectable in 60%<1% in 100% of pts
NPM and NRASMRD high > .01% median RFS 9.9 mmedian OS 17.8 m
MRD low median RFS and OS NR
15 SCT MRD highmedian RFS 14.8 mMRD low median RFS NR
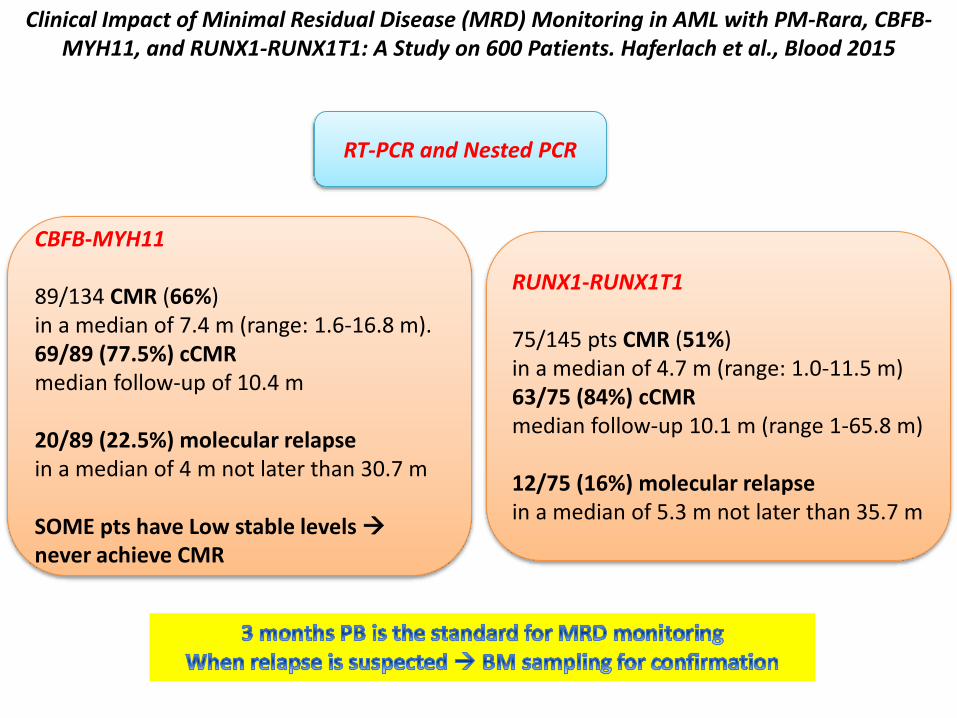
Clinical Impact of Minimal Residual Disease (MRD) Monitoring in AML with PM-Rara, CBFB-MYH11, and RUNX1-RUNX1T1: A Study on 600 Patients. Haferlach et al., Blood 2015
RT-PCR and Nested PCR
CBFB-MYH11
89/134 CMR (66%)in a median of 7.4 m (range: 1.6-16.8 m).69/89 (77.5%) cCMRmedian follow-up of 10.4 m
20/89 (22.5%) molecular relapsein a median of 4 m not later than 30.7 m
SOME pts have Low stable levels never achieve CMR
RUNX1-RUNX1T1
75/145 pts CMR (51%)in a median of 4.7 m (range: 1.0-11.5 m)63/75 (84%) cCMRmedian follow-up 10.1 m (range 1-65.8 m)
12/75 (16%) molecular relapsein a median of 5.3 m not later than 35.7 m
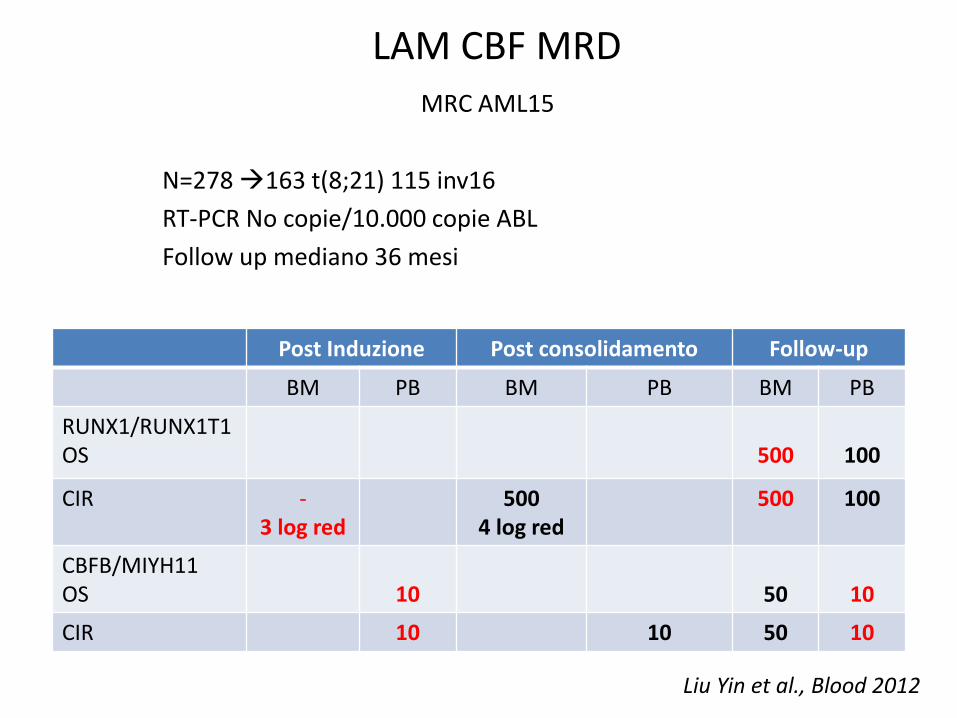
LAM CBF MRDMRC AML15
N=278163 t(8;21) 115 inv16
RT-PCR No copie/10.000 copie ABL
Follow up mediano 36 mesi
Post Induzione Post consolidamento Follow-up
BM PB BM PB BM PB
RUNX1/RUNX1T1OS 500 100
CIR -3 log red
5004 log red
500 100
CBFB/MIYH11OS 10 50 10
CIR 10 10 50 10
Liu Yin et al., Blood 2012
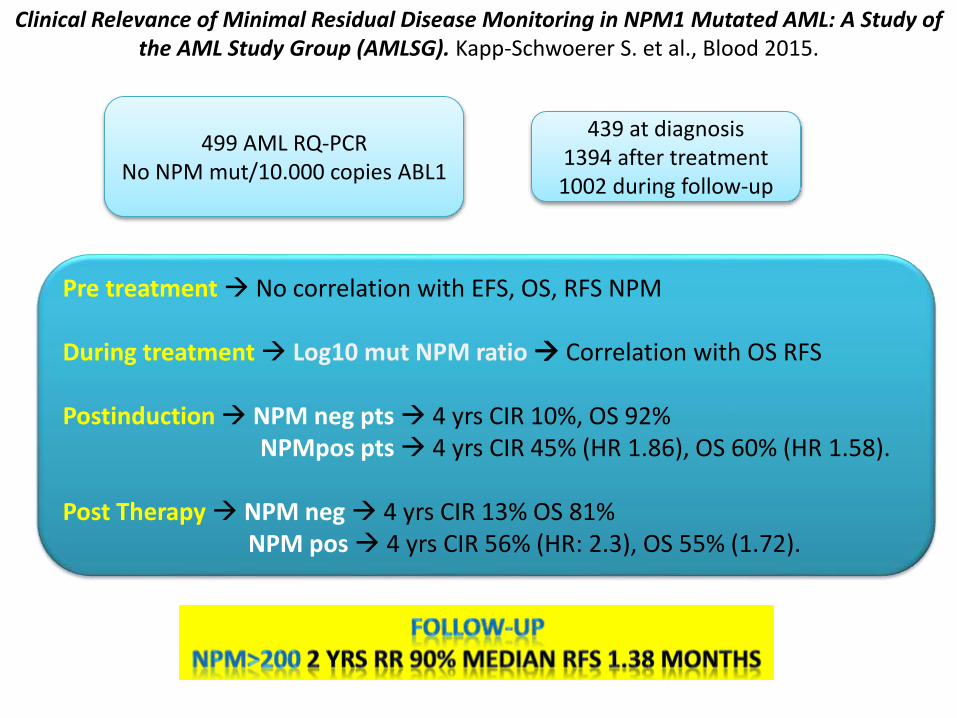
Clinical Relevance of Minimal Residual Disease Monitoring in NPM1 Mutated AML: A Study of the AML Study Group (AMLSG). Kapp-Schwoerer S. et al., Blood 2015.
499 AML RQ-PCRNo NPM mut/10.000 copies ABL1
439 at diagnosis1394 after treatment1002 during follow-up
Pre treatment No correlation with EFS, OS, RFS NPM
During treatment Log10 mut NPM ratio Correlation with OS RFS
Postinduction NPM neg pts 4 yrs CIR 10%, OS 92% NPMpos pts 4 yrs CIR 45% (HR 1.86), OS 60% (HR 1.58).
Post Therapy NPM neg 4 yrs CIR 13% OS 81%NPM pos 4 yrs CIR 56% (HR: 2.3), OS 55% (1.72).

GRAZIE DELL’ATTENZIONE
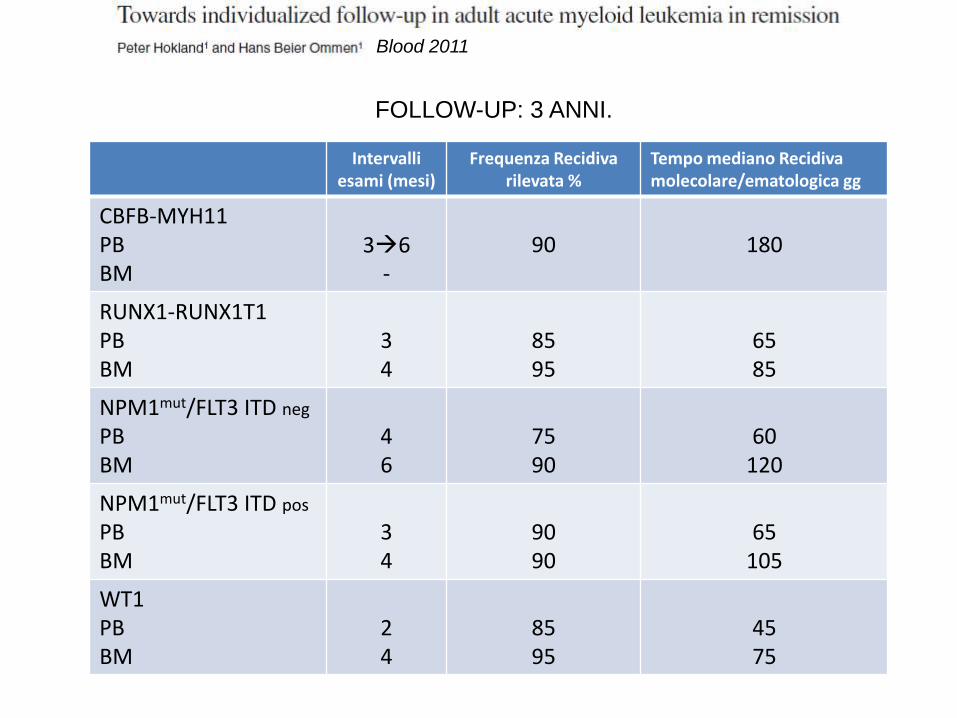
Intervalli esami (mesi)
Frequenza Recidiva rilevata %
Tempo mediano Recidiva molecolare/ematologica gg
CBFB-MYH11PBBM
36-
90 180
RUNX1-RUNX1T1PBBM
34
8595
6585
NPM1mut/FLT3 ITD neg
PBBM
46
7590
60120
NPM1mut/FLT3 ITD pos
PBBM
34
9090
65105
WT1PBBM
24
8595
4575
Blood 2011
FOLLOW-UP: 3 ANNI.