norwood operation for univentricular heart with subaortic stenosis in the neonate
TRANSCRIPT

Norwood Operation for Univentricular Heart With Subaortic Stenosis in the Neonate Christ0 I. Tchervenkov, MD, Marie J. Bkland, MD, David A. Latter, MD, and Anthony R. C. Dobell, MD Division of Cardiovascular and Thoracic Surgery, The Montreal Children‘s Hospital, McGill University, Montreal, Quebec, Canada
In the setting of a single ventricle, subaortic stenosis may be enhanced by pulmonary artery banding and may later contraindicate a Fontan operation. The Norwood opera- tion may prove a preferable alternative in some infants as a preparatory procedure. We have successfully used this
procedure as the initial operation to palliate a newborn with tricuspid atresia, transposition of the great arteries, coarctation, and severe arch hypoplasia secondary to a restrictive bulboventricular foramen.
(Ann Thorac Surg 1990;50:822-5)
pectacular advances have been made in the surgical S treatment of hypoplastic left heart syndrome. What used to be a virtually uniformly fatal condition can now be successfully palliated in the newborn period [l]. We report on the successful application of the Norwood operation in a patient with tricuspid atresia, transposition of the great arteries, coarctation, and severe arch hypopla- sia resulting from a restrictive bulboventricular foramen.
A 2.2-kg baby boy was transferred to The Montreal Children’s Hospital on the seventh day of life for respira- tory distress and congestive heart failure. Echocardiog- raphy revealed the diagnosis of (S,D,D) tricuspid atresia, transposition of the great arteries, coarctation, and marked hypoplasia of the aortic arch (Fig 1). Decreasing systemic perfusion was reversed by the administration of prostaglandins to maintain ductal patency. Balloon atrial septostomy performed at cardiac catheterization con- firmed the diagnosis and demonstrated a restrictive bul- boventricular foramen leading into the subaortic chamber (Fig 2).
Operation was performed at 10 days of age. The follow- ing observations were made: the ascending aorta was 6 mm in diameter; the aortic arch between the innominate artery and the left common carotid artery was 3 mm in diameter, tapering to 2 mm distal to it. The main pulmo- nary artery was 14 mm in diameter and the right and left pulmonary arteries were well developed (Fig 3). The baby underwent the Norwood operation (Fig 4). Under deep hypothermic circulatory arrest, the main pulmonary ar- tery was transected at its bifurcation and the distal end closed with a patch of aortic homograft. The patent ductus was ligated and divided. The concave surface of the aortic arch was incised and the incision was carried distally 10 mm past the area of coarctation. Proximally the incision was carried into the ascending aorta up to the level of the
Accepted for publication May 2, 1990.
Address reprint requests to Dr Tchervenkov, The Montreal Children’s Hospital, 2300 Tupper St-Room C-827, Montreal, Que, Canada H3H 1M.
stump of the main pulmonary artery. The aortic arch was augmented with an appropriately fashioned aortic ho- mograft patch well beyond the area of coarctation. Prox- imally the reconstruction involved the main pulmonary artery stump, which was sutured to the side of the ascending aorta. Pulmonary artery flow was provided by a 4-mm Gore-Tex shunt from the undersurface of the newly reconstructed aortic arch and the confluence of the right and left pulmonary arteries. The sternum was not closed at the end of the operation because of cardiopul- monary compromise, but was successfully closed 2 days later.
The baby was extubated 8 days postoperatively. He was kept in the hospital 5 weeks after the operation because of prematurity. At 9 months of age, increasing cyanosis was noted and a cardiac catheterization was carried out (Fig 5 ) . The baby underwent a right modified Blalock-Taussig shunt with a 6-mm Gore-Tex graft and take-down of the previous central shunt. Now, at the age of 2 years, a Fontan operation is anticipated.
Comment There is a group of patients who have the physiological equivalent of hypoplastic left heart syndrome and require complex palliative aortic reconstruction in the newborn period to achieve survival. We are reporting on the case of a patient with tricuspid atresia and transposed great arteries with coarctation and severe aortic arch hypoplasia secondary to a restrictive bulboventricular foramen, which resulted in decreased forward flow to the ascend- ing aorta. In such a patient, a substantial part of the systemic perfusion, especially to the lower body, is pro- vided by the patent ductus arteriosus. It is doubtful that a more classic approach such as coarctation repair and pulmonary artery banding would result in survival. It is possible to carry out a complex reconstruction of the aortic arch via a left thoracotomy as reported by Elliott [2]. However, the restrictive bulboventricular foramen would remain and the application of the pulmonary artery band would further accelerate its reduction in size by stimulat-
0 1990 by The Society of Thoracic Surgeons 0003-4975/90/$3.50

Ann Thorac Surg 1990;50: 822-5
CASE REPORT TCHERVENKOV ET AL 823 UNIVENTRICULAR HEART, SUBAORTIC STENOSIS
Fig 1. Two-dimensional echocardiog- raphy demonstrating the hypoplastic aortic arch. ( A 0 = aorta; lsa = left subclavian ar tey; MPA = main pul- mona y arte y ; PDA = patent duc- tus arteriosus.)
ing ventricular hypertrophy. The resultant subaortic ste- nosis, we have learned, is very difficult to treat and adversely affects survival of these patients [3, 41.
Jonas and colleagues [5] have recently reported 3 pa-
tients in whom subaortic stenosis developed rapidly after the application of a pulmonary artery band. All 3 patients were converted to a Nonvood circulation between 4 and 10 weeks of age because of the presence of severe subaor- tic stenosis. It is becoming clear that patients with single ventricle and clinically significant subaortic stenosis have a higher mortality after the Fontan operation [6, 71 or ventricular septation [8]. Furthermore, Freedom and col- leagues [9] have clearly identified pulmonary artery band-
Fig 2. Cardiac catheterization showing the subaortic stenosis (*). The ascending aorta (AO) is much smaller than the main pulmonary ar- t e y (PA). meters.
Fig 3. Operative findings of subaortic stenosis (*) and the relative sizes of the great vessels. All numbers indicate diameter in milli-
824 CASE REPORT TCHERVENKOV ET AL UNIVENTRICULAR HEART, SUBAORTIC STENOSIS
Ann Thorac Surg 1990;50:822-5
n Central shunt
Aortic homograft
A
B Fig 4. The Nomood operation: (A) An aortic homograft is used to reconstruct the ascending aorta and hypoplastic aortic arch as well as to close the distal main pulmona ry artery. f B ) The completed recon- struction.
ing as a significant etiological factor in the development of subaortic stenosis in patients with univentricular heart. The pulmonary artery band will stimulate marked myo- cardial hypertrophy, which will undoubtedly alter ven- tricular compliance and impair atrial emptying. Kirklin and colleagues [lo], in a review of their experience with
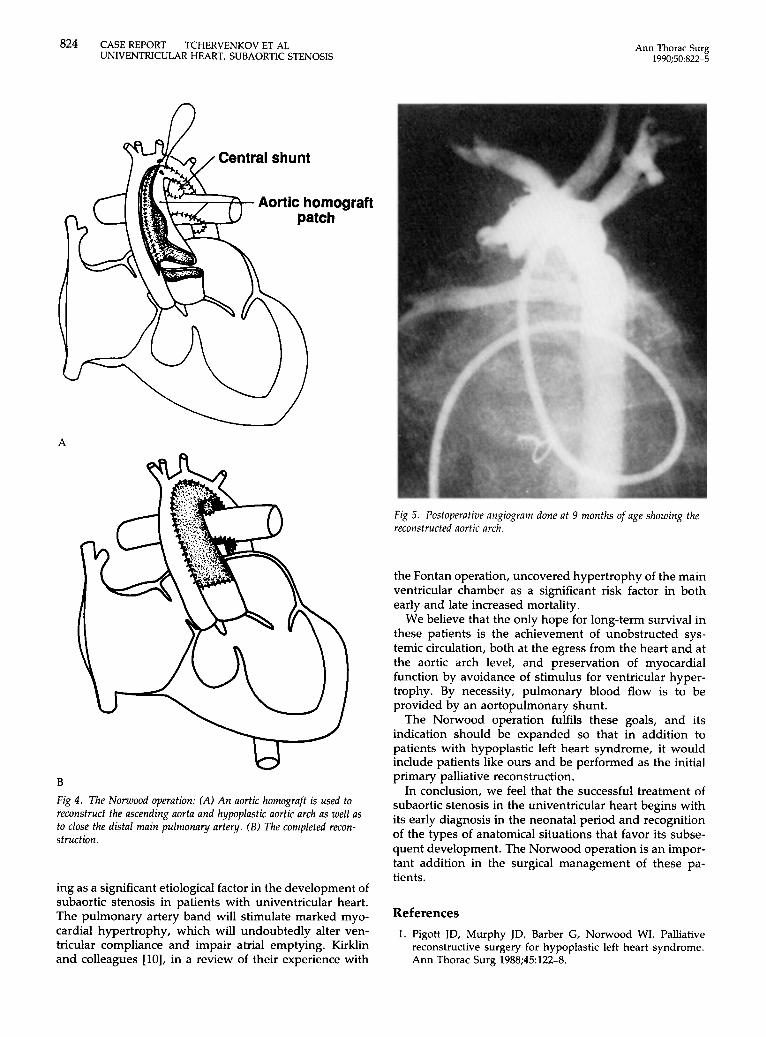
Fig 5. Postoperative angiogram done at 9 months of age showing the reconstructed aortic arch.
the Fontan operation, uncovered hypertrophy of the main ventricular chamber as a significant risk factor in both early and late increased mortality.
We believe that the only hope for long-term survival in these patients is the achievement of unobstructed sys- temic circulation, both at the egress from the heart and at the aortic arch level, and preservation of myocardial function by avoidance of stimulus for ventricular hyper- trophy. By necessity, pulmonary blood flow is to be provided by an aortopulmonary shunt.
The Norwood operation fulfils these goals, and its indication should be expanded so that in addition to patients with hypoplastic left heart syndrome, it would include patients like ours and be performed as the initial primary palliative reconstruction.
In conclusion, we feel that the successful treatment of subaortic stenosis in the univentricular heart begins with its early diagnosis in the neonatal period and recognition of the types of anatomical situations that favor its subse- quent development. The Nonvood operation is an impor- tant addition in the surgical management of these pa- tients.
References 1. Pigott JD, Murphy JD, Barber G, Norwood WI. Palliative
reconstructive surgery for hypoplastic left heart syndrome. Ann Thorac Surg 1988;45:122-8.

Ann Thorac Surg 1990;50:822-5
CASE REPORT TCHERVENKOV ET AL 825 UNIVENTRICULAR HEART, SUBAORTIC STENOSIS
2. Elliott MJ. Coarctation of the aorta with arch hypoplasia: improvements on a new technique. Ann Thorac Surg 1987;
3. Rothman A, Lang P, Lock JE, Jonas RA, Mayer JE, Castaneda AR. Surgical management of subaortic obstruction on single left ventricle and tricuspid atresia. J Am Coll Cardiol 1987;lO: 421-6.
4. Penkoske PA, Freedom RM, Williams WG, Trusler GA, Rowe RD. Surgical palliation of subaortic stenosis in the univentricular heart. J Thorac Cardiovasc Surg 1984;87: 767-81.
5. Jonas RA, Castaneda AR, Lang P. Single ventricle (single or double-inlet) complicated by subaortic stenosis: surgical op- tions in infancy. Ann Thorac Surg 1985;39:361-6.
6. DeLeon SY, Ilbawi MN, Idriss FS, et al. Fontan type opera- tion for complex lesions, surgical considerations to improve survival. J Thorac Cardiovasc Surg 1986;92:1029-37.
44~321-3.
7. Coles JG, Kielmanowicz S, Freedom RM, et al. Surgical experience with the modified Fontan procedure. Circulation 1987;76(Suppl3):61-6.
8. McKay R, Pacifico AD, Blackstone EH, Kirklin JW, Bargeron LM Jr. Septation of the univentricular heart with left anterior subaortic outlet chamber. J Thorac Cardiovasc Surg 1982;84: 77-87.
9. Freedom RM, Benson LN, Smallhorn JF, Williams WG, Trusler GA, Rowe RD. Subaortic stenosis, the univentricular heart and banding of the pulmonary artery: an analysis of the courses of 43 patients with univentricular heart palliated by pulmonary artery banding. Circulation 1986;73:758-64.
10. Kirklin JK, Blackstone EH, Kirklin JW, Pacifico AD, Bargeron LM Jr. The Fontan operation, ventricular hypertrophy, age and date of operation as risk factors. J Thorac Cardiovasc Surg 1986;92:1049-64.
REVIEW OF RECENT BOOKS
Surgery of the Chest, 5th Edition, Volume I1 Edited by David C . Sabiston, Jr, M D , and Frank C . Spencer, M D Philadelphia: W.B. Saunders 2,084 p p , illustrated, $250.00
Reviewed by Anthony R. C . Dobell, M D
Volume I1 of Sabiston and Spencer’s fifth edition of Surgery of the Chest is primarily devoted to acquired and congenital cardiac surgery. Each chapter has been prepared by recognized author- ities, many of whom have made the original contributions in the area under discussion.
Chapters are written according to a uniform framework. His- torical aspects are usually briefly described; pathophysiology and clinical features are succinctly recorded. Surgical management
and postoperative care are extensively described and updated. The quality and quantity of figures vary considerably. Postoper- ative results and long-term management are generally thor- oughly described and supported by the most recent literature.
A strong point of this textbook is the selected bibliography that accompanies each chapter; the authors have chosen key articles that are very well summarized. The bibliography itself is always extensive, and this is a major reason for the book‘s extreme usefulness to cardiothoracic trainees. This textbook offers a complete review of almost every aspect of cardiothoracic surgery, and the authors and editors have done a remarkable service in compressing an extraordinary amount of data into a manageable form.
Montreal, Quebec, Canada