normal sinus rhythm (nsr): “rrr”, coordinated, regular
TRANSCRIPT
4/1/2015
1
Steven Heifetz, MD FACC UMP-Heart
(don’t be afraid of the big bad “WOLF”)
Normal Sinus Rhythm (NSR): “RRR”, coordinated, regular rhythm
The “definitive” way to diagnose Afib – EP Lab
4/1/2015
2
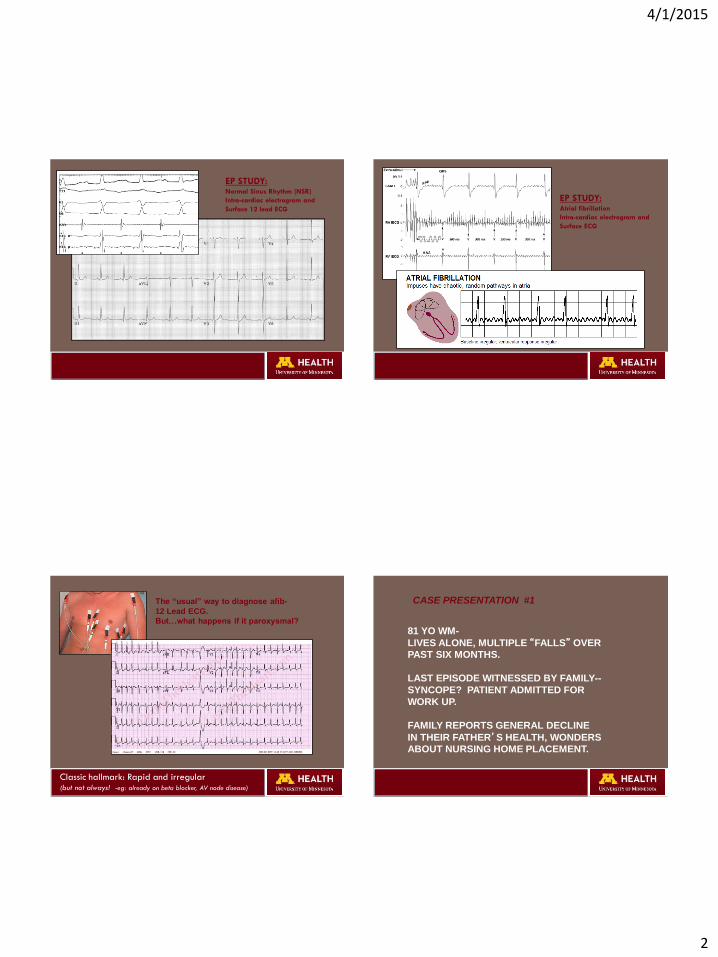
EP STUDY: Normal Sinus Rhythm (NSR)
Intra-cardiac electrogram and
Surface 12 lead ECG
EP STUDY: Atrial fibrillation
Intra-cardiac electrogram and
Surface ECG
The “usual” way to diagnose afib-
12 Lead ECG.
But…what happens if it paroxysmal?
Classic hallmark: Rapid and irregular (but not always! -eg: already on beta blocker, AV node disease)
81 YO WM-
LIVES ALONE, MULTIPLE “FALLS” OVER
PAST SIX MONTHS.
LAST EPISODE WITNESSED BY FAMILY--
SYNCOPE? PATIENT ADMITTED FOR
WORK UP.
FAMILY REPORTS GENERAL DECLINE
IN THEIR FATHER’S HEALTH, WONDERS
ABOUT NURSING HOME PLACEMENT.
CASE PRESENTATION #1

4/1/2015
3
EXAM:
AFEBRILE, 162/68 (NO ORTHOSTASIS), 66
LUNGS-CLEAR
COR- RRR, Gr II/VI SEM
CAROTIDS- NORMAL UPSTROKE, SOFT BRUIT (L)
CNS- NON FOCAL, EARLY DEMENTIA?
LABS: ELECTROLYTE-UNREMARKABLE CBC-UNREMARKABLE CXR-MILD HYPERINFLATION, Ca++ AORTIC BULB HEAD CT- ATROPHY EKG-NSR, LAD ECHO-MILD LVH, NORMAL EF, AORTIC SCLEROSIS TELEMETRY (ON CSC)- UNREMARKABLE
PATIENT DISCHARGED AFTER 48 HOURS
OUT PATIENT HOLTER ORDERED
WHAT DID THE HOLTER SHOW?
WHAT WOULD YOU DO?
Holter monitor: • Continuous 24 hour recording
• Patient “diary”-trigger
• “Post” analysis
4/1/2015
4
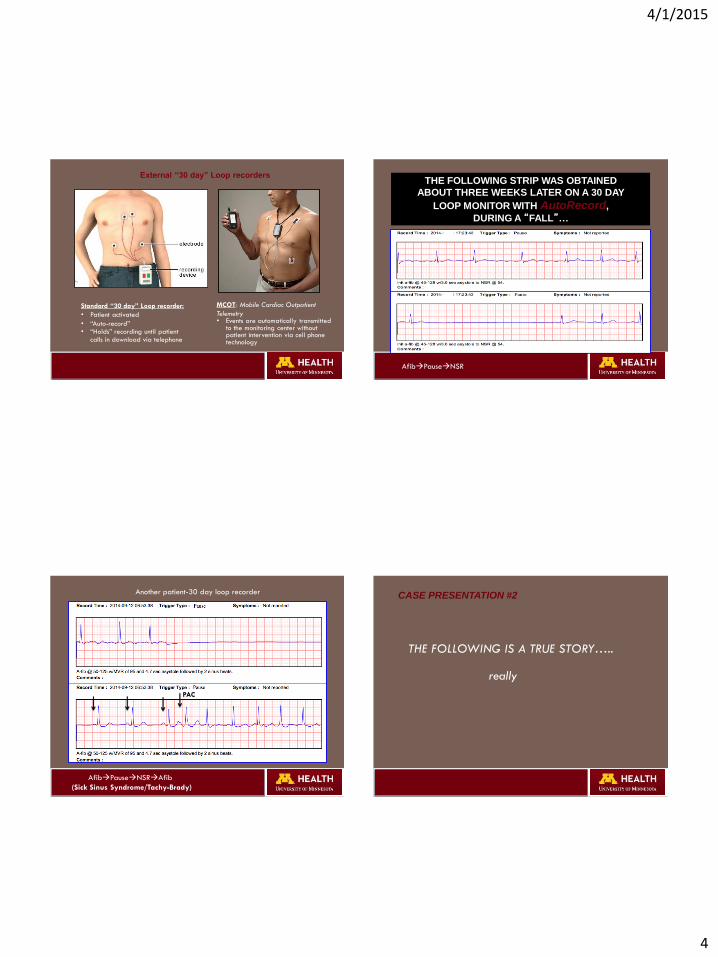
Standard “30 day” Loop recorder:
• Patient activated
• “Auto-record” • “Holds” recording until patient
calls in download via telephone
MCOT: Mobile Cardiac Outpatient
Telemetry • Events are automatically transmitted
to the monitoring center without patient intervention via cell phone technology
External “30 day” Loop recorders
AfibPauseNSR
THE FOLLOWING STRIP WAS OBTAINED
ABOUT THREE WEEKS LATER ON A 30 DAY
LOOP MONITOR WITH AutoRecord,
DURING A “FALL”…
AfibPauseNSRAfib
(Sick Sinus Syndrome/Tachy-Brady)
PAC
Another patient-30 day loop recorder CASE PRESENTATION #2
THE FOLLOWING IS A TRUE STORY…..
really
4/1/2015
5
A 72 YO WIDOWER GOES INTO A BAR
HE SITS DOWN AT THE BAR AND IMMEDIATELY
BECOMES ASHEN
THE BARTENDER ASKS HIM IF HE IS OK
THE MAN REPLIES “NO” AND ASKS THE BARTENDER--
HAVE YOU HEARD THE ONE ABOUT A GUY WITH
“SPELLS”
THE BARTENDER REPLIES, “YES, I HAD SPELLS
BUT DR. HEIFETZ FIXED THEM”
HE WAS “SELF REFERRED” ON THE RECOMMENDATION OF HIS BARTENDER
HE HAS SEEN NUMEROUS PHYSICIANS IN THE PAST AND HAD NUMEROUS
TESTS INCLUDING-HEAD CT, EEG, ECG, ECHO, HOLTER etc
THE SPELLS OCCUR 1-2/YEAR. THEY COME ON
SUDDENLY AND LAST UP TO 30 MINUTES
HE FEELS WEAK IN HIS LEGS, AND SHAKY. HE HAS NEVER PASSED OUT,
BUT HE FEELS LIKE HE MIGHT. OCCASIONALLY HE IS SOB BUT NEVER
HAS CHEST PAIN. THERE ARE NO TRIGGERS, AND THE EPISODES SUBSIDE
SPONTANEOUSLY. THE EPISODES HAVE BECOME LESS WELL TOLERATED
AS HE HAS GOTTEN OLDER.
HIS EXAM, PMH, AND ROUTINE LABS ARE UNREMARKABLE
THE PATIENT WAS OFFERED A 30 DAY LOOP MONITOR--BUT HE WISELY
POINTED OUT THAT HE WAS UNLIKELY TO HAVE A SPELL IN THE NEXT
30 DAYS. HE REQUESTS A “DEFINITIVE” TEST
THIS 72 YO HAS BEEN HAVING “SPELLS”
FOR ALMOST 22 YEARS
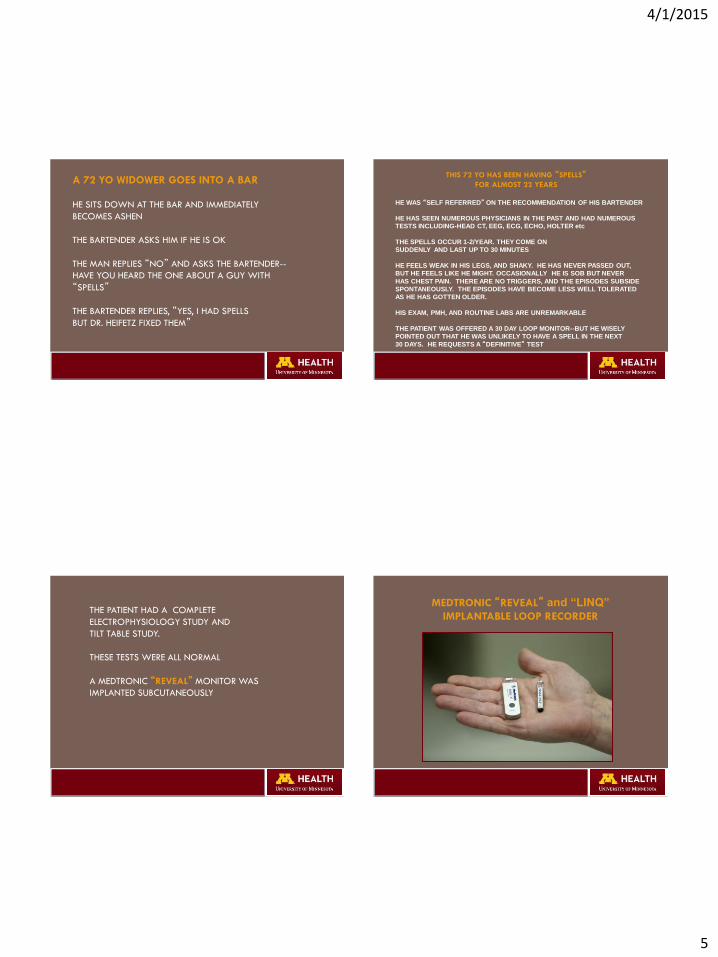
THE PATIENT HAD A COMPLETE
ELECTROPHYSIOLOGY STUDY AND
TILT TABLE STUDY.
THESE TESTS WERE ALL NORMAL
A MEDTRONIC “REVEAL” MONITOR WAS
IMPLANTED SUBCUTANEOUSLY
MEDTRONIC “REVEAL” and “LINQ”
IMPLANTABLE LOOP RECORDER

4/1/2015
6
SEVEN WEEKS LATER HE REPORTED TO
OUR OFFICE, TO TRANSMIT A CAPTURED “EVENT”
TELEMETRY REVEALED THE FOLLOWING STRIP...
UPON NEWS OF THE DIAGNOSIS, THE PATIENT BEGAN TO CRY.
WHEN ASKED WHY HE WAS CRYING, HE STATED HE WISHED HIS
WIFE WAS STILL ALIVE TO SEE THIS, HE WAS STARTING TO THINK
HE WAS CRAZY AND THERE REALLY WAS NOTHING WRONG WITH HIM,
AS HE HAD BEEN TOLD IN THE PAST
This patient was at a bar and referred in by his
bartender.
This patient was at a bar and referred in by his
bartender.
Perhaps this is an untapped marketing
opportunity.
This patient was at a bar and referred in by his
bartender.
Perhaps this is an untapped marketing
opportunity.
Medical professional groups may want to
consider this in their future direct to consumer
advertising campaigns.

4/1/2015
7
Reduce morbidity, mortality, and disability from CV & pulmonary diseases through education, prevention, rehabilitation, research, and aggressive disease management
Patient Eligibility
Enrolled after new dual-chamber pacemaker or ICD
Age ≥ 65 years
History of hypertension
Excluded if any history of AF
Excluded if on Vitamin K antagonist
Pre-specified primary analysis:
Monitor from enrolment to 3 month visit for atrial tachyarrhythmia
defined as >6 minutes and an atrial rate of >190 bpm
Prospective follow up for ischemic stroke or systemic embolism from 3
month visit onwards
Statistical power to detect ≥ 1% per year increase in primary outcome
ASSERT Healy S, NEJM 2012; 366:120-9
ASSERT: Study Design

4/1/2015
8
Panel A shows the risk of
electrocardiographically documented
clinical atrial tachyarrhythmias after the
3-month visit, according to whether
subclinical atrial tachyarrhythmias were
or were not detected between enrolment and the 3-month visit.
Panel B shows the risk of ischemic stroke or
systemic embolism after the 3-month visit,
according to whether subclinical atrial
tachyarrhythmias were or were not detected
between enrollment and the 3-month visit.
The insets show the same data on an
enlarged y axis.
A: Risk of Clinical Atrial Tachyarrhythmias
B: Ischemic Stroke or Systemic Embolism
ASSERT-trial
Over 2.8 years mean follow up, device-detected atrial
tachyarrhythmias (>6 min, >190 bpm) are present in 36% of
pacemaker patients with hypertension; but no prior history of AF
In patients with CHADS2 score > 2, device-detected atrial
tachyarrhythmias increase the absolute risk of stroke or systemic
embolism to 4% per year
Among pacemaker patients without prior AF, 35% of all strokes
or systemic emboli are preceded by device-detected atrial
tachyarrhythmias.
ASSERT Conclusions
Gladstone DJ. N Engl J Med 2014; 370:2467-2477
EMBRACE Investigators: AF in patient with cryptogenic stroke
To determine the diagnostic yield of a 30-day cardiac event monitor compared to a repeat 24-hour Holter monitor for detecting occult paroxysmal atrial fibrillation in patients with a recent ischemic stroke or TIA of undetermined etiology.
• 55 years or older • Experienced ischemic stroke or TIA within previous 6
months • No cause identified by post-stroke/TIA diagnostic workup,
including ECG, 24-hr Holter, brain imaging, and echo. • No history of atrial fibrillation or flutter.
EMBRACE: Primary objective
Study Population
30 day event monitor vs 24 hr Holter
Incremental Yield of Prolonged ECG Monitoring for the Detection of Atrial Fibrillation in
Patients with Cryptogenic Stroke or TIA
EMBRACE Gladstone DJ. N Engl J Med 2014; 370:2467-2477
4/1/2015
9
• Among patients 55 years or older with a recent cryptogenic stroke or TIA, paroxysmal atrial fibrillation was common.
• Noninvasive ambulatory ECG monitoring for a target of 30 days significantly improved the detection of atrial fibrillation by a factor of more than five and nearly doubled the rate of anticoagulant treatment, as compared with the standard practice of short-duration ECG monitoring.
Conclusions
EMBRACE Gladstone DJ. N Engl J Med 2014; 370:2467-2477 CRYSTAL-AF: Sanna T. N Engl J Med 2014; 370:2478-2486
Cryptogenic Stroke and Underlying AF
• 441 Pts >40 yo, no h/o Afib with cryptogenic stroke.
(“controls”)
• At 12 months detection of AF >30 sec: REVEAL vs ECG: 12.4% vs 2.0% (p <0.001)
Calculate a patient’s stroke risk to determine
who benefits from anticoagulants

4/1/2015
10
S>R Vitamin K epoxide reductase (VKOR)
VKORC1
GrpA-(Asia, more sens to W so rapid INR inc), Lower W dose
GrpB-(Black, res to inhib by W so need higher W dose)
CYP2C9
S-warf metabolized by 2C9
Among patients with non-valvular
atrial fibrillation, anticoagulation
that results in an INR of 2.0 or
greater reduces not only the
frequency of ischemic stroke but
also its severity and the risk of
death from stroke.
Hylek EM, Go AS, Chang Y, et al N Engl J Med. 2003;349:1019-1026
Effect of intensity of oral anticoagulation on stroke severity and mortality
in atrial fibrillation
As HbA1c is to FBG, TTR is to INR
Figure 4. TTR versus adverse events (weighted by sample size) for retrospective studies.
Wan Y et al. Circ Cardiovasc Qual Outcomes. 2008;1:84-91
Copyright © American Heart Association, Inc. All rights reserved.
4/1/2015
11
1
1.5
2
2.5
3
3.5
4
4.5
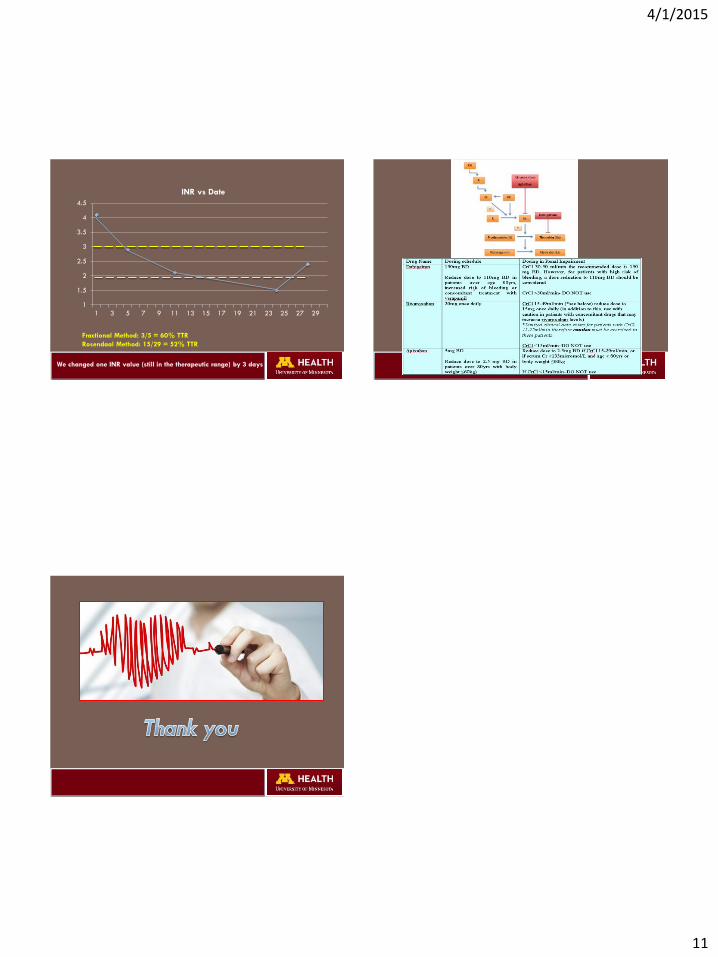
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29
INR vs Date
Fractional Method: 3/5 = 60% TTR
Rosendaal Method: 15/29 = 52% TTR
We changed one INR value (still in the therapeutic range) by 3 days