normal hypocretin-1 (orexin-a) levels in the cerebrospinal fluid of patients with huntington's...
TRANSCRIPT
www.elsevier.com/locate/brainres
Brain Research 1063
Short Communication
Normal hypocretin-1 (orexin-A) levels in the cerebrospinal fluid of
patients with Huntington’s disease
Andreas Meier a,*, Brit Mollenhauer b, Stefan Cohrs a, Andrea Rodenbecka, Wolfgang Jordana,
Johannes Meller c, Markus Otto a,b
aSleep Disorders Center, Department of Psychiatry and Psychotherapy, Georg-August-University, von-Siebold-Strasse 5, 37075 Goettingen, GermanybDepartment of Neurology, Georg-August-University, Goettingen, Germany
cDepartment of Nuclear Medicine, Georg-August-University, Goettingen, Germany
Accepted 25 September 2005
Available online 2 November 2005
Abstract
A significant atrophy and loss of hypocretin neurons in the brains of human patients with Huntington’s disease (HD) and in R6/2 mice
have been reported. We included 10 patients with HD and 12 patients with chorea-like hyperkinetic movement disorders (non-HD). All
patients of the HD group and eleven patients of the non-HD group showed normal hypocretin-1 levels. Thus, hypocretin-1 may not serve as
an additional diagnostic marker for HD.
D 2005 Elsevier B.V. All rights reserved.
Theme: Disorders of the nervous system
Topic: Degenerative disease: other
Keywords: Hypocretin; Huntington; Orexin
A significant atrophy and loss of hypocretin neurons in the
brains of human patients with Huntington’s disease (HD) and
in R6/2 mice have been reported [6]. It has been hypothesized
that cerebrospinal fluid level of hypocretin-1 could constitute
a novel marker for assessing the progression and the
effectiveness of therapeutic interventions in human HD
patients [6]. Therefore,we tested this hypothesis in 22 patients
who where under the differential diagnosis of having HD.
Huntington’s disease (HD) is an autosomal dominantly
inherited progressive neurodegenerative condition. It is
characterized by movement disorders, personality changes
and dementia [3]. Furthermore, psychotic symptoms and a
disrupted sleep pattern with prolonged sleep latency, frequent
nocturnal awakenings, reduced slow-wave sleep and a higher
density of sleep spindles have been reported [7]. Usually, the
clinical manifestation is in the mid-age but symptoms may
0006-8993/$ - see front matter D 2005 Elsevier B.V. All rights reserved.
doi:10.1016/j.brainres.2005.09.028
* Corresponding author. Fax: +49 551 39 3887.
E-mail address: [email protected] (A. Meier).
also appear in younger or older patients. The progression of
the disease leads inescapably to death within 10–15 years.
The characteristic neuropathological findings in HD are
neuronal loss and astrocytosis in the striatum and massive
atrophy of caudate nucleus. There is also a loss of neurones in
the substantia nigra pars reticulate, the subthalamic nucleus
and the thalamus [3]. It is caused by a mutation in the gene
encoding huntingtin leading to expansion of a trinucleotide
repeat (CAG) [11]. Even if the function of the protein is still
unknown, mutant huntingtin may alter the function of
transcriptional factors, reduce the level of acetylated histones
and is supposed to induce a decreased expression of genes
which may play important roles in neuronal survival [3].
The hypocretin system is likely to have a role in
modulating the stability of sleep–wake cycles and in the
promotion of vigilance but also physiological functions in
addition to food intake such as regulation of blood pressure,
the neuroendocrine system and body temperature [10].
Hypocretin neurons are located in the lateral and medial
hypothalamic region exclusively but project to all relevant
(2005) 201 – 203
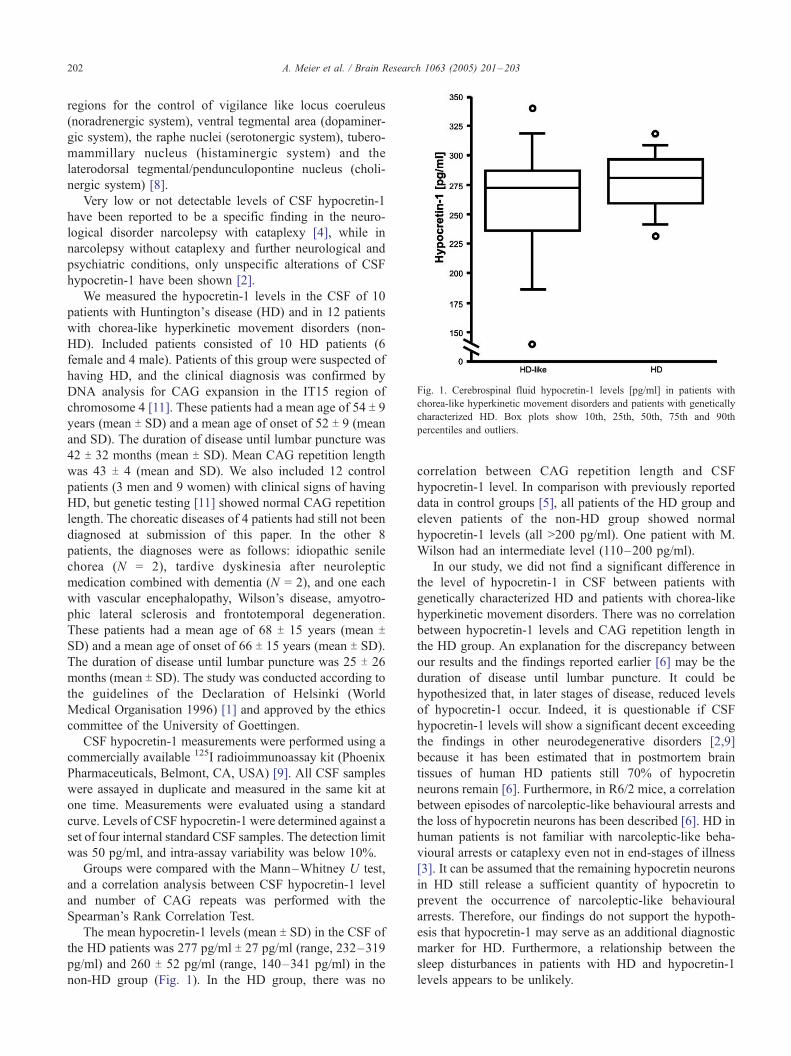
Fig. 1. Cerebrospinal fluid hypocretin-1 levels [pg/ml] in patients with
chorea-like hyperkinetic movement disorders and patients with genetically
characterized HD. Box plots show 10th, 25th, 50th, 75th and 90th
percentiles and outliers.
A. Meier et al. / Brain Research 1063 (2005) 201–203202
regions for the control of vigilance like locus coeruleus
(noradrenergic system), ventral tegmental area (dopaminer-
gic system), the raphe nuclei (serotonergic system), tubero-
mammillary nucleus (histaminergic system) and the
laterodorsal tegmental/pendunculopontine nucleus (choli-
nergic system) [8].
Very low or not detectable levels of CSF hypocretin-1
have been reported to be a specific finding in the neuro-
logical disorder narcolepsy with cataplexy [4], while in
narcolepsy without cataplexy and further neurological and
psychiatric conditions, only unspecific alterations of CSF
hypocretin-1 have been shown [2].
We measured the hypocretin-1 levels in the CSF of 10
patients with Huntington_s disease (HD) and in 12 patients
with chorea-like hyperkinetic movement disorders (non-
HD). Included patients consisted of 10 HD patients (6
female and 4 male). Patients of this group were suspected of
having HD, and the clinical diagnosis was confirmed by
DNA analysis for CAG expansion in the IT15 region of
chromosome 4 [11]. These patients had a mean age of 54 T 9years (mean T SD) and a mean age of onset of 52 T 9 (mean
and SD). The duration of disease until lumbar puncture was
42 T 32 months (mean T SD). Mean CAG repetition length
was 43 T 4 (mean and SD). We also included 12 control
patients (3 men and 9 women) with clinical signs of having
HD, but genetic testing [11] showed normal CAG repetition
length. The choreatic diseases of 4 patients had still not been
diagnosed at submission of this paper. In the other 8
patients, the diagnoses were as follows: idiopathic senile
chorea (N = 2), tardive dyskinesia after neuroleptic
medication combined with dementia (N = 2), and one each
with vascular encephalopathy, Wilson’s disease, amyotro-
phic lateral sclerosis and frontotemporal degeneration.
These patients had a mean age of 68 T 15 years (mean TSD) and a mean age of onset of 66 T 15 years (mean T SD).
The duration of disease until lumbar puncture was 25 T 26
months (mean T SD). The study was conducted according to
the guidelines of the Declaration of Helsinki (World
Medical Organisation 1996) [1] and approved by the ethics
committee of the University of Goettingen.
CSF hypocretin-1 measurements were performed using a
commercially available 125I radioimmunoassay kit (Phoenix
Pharmaceuticals, Belmont, CA, USA) [9]. All CSF samples
were assayed in duplicate and measured in the same kit at
one time. Measurements were evaluated using a standard
curve. Levels of CSF hypocretin-1 were determined against a
set of four internal standard CSF samples. The detection limit
was 50 pg/ml, and intra-assay variability was below 10%.
Groups were compared with the Mann–Whitney U test,
and a correlation analysis between CSF hypocretin-1 level
and number of CAG repeats was performed with the
Spearman’s Rank Correlation Test.
The mean hypocretin-1 levels (mean T SD) in the CSF of
the HD patients was 277 pg/ml T 27 pg/ml (range, 232–319
pg/ml) and 260 T 52 pg/ml (range, 140–341 pg/ml) in the
non-HD group (Fig. 1). In the HD group, there was no
correlation between CAG repetition length and CSF
hypocretin-1 level. In comparison with previously reported
data in control groups [5], all patients of the HD group and
eleven patients of the non-HD group showed normal
hypocretin-1 levels (all >200 pg/ml). One patient with M.
Wilson had an intermediate level (110–200 pg/ml).
In our study, we did not find a significant difference in
the level of hypocretin-1 in CSF between patients with
genetically characterized HD and patients with chorea-like
hyperkinetic movement disorders. There was no correlation
between hypocretin-1 levels and CAG repetition length in
the HD group. An explanation for the discrepancy between
our results and the findings reported earlier [6] may be the
duration of disease until lumbar puncture. It could be
hypothesized that, in later stages of disease, reduced levels
of hypocretin-1 occur. Indeed, it is questionable if CSF
hypocretin-1 levels will show a significant decent exceeding
the findings in other neurodegenerative disorders [2,9]
because it has been estimated that in postmortem brain
tissues of human HD patients still 70% of hypocretin
neurons remain [6]. Furthermore, in R6/2 mice, a correlation
between episodes of narcoleptic-like behavioural arrests and
the loss of hypocretin neurons has been described [6]. HD in
human patients is not familiar with narcoleptic-like beha-
vioural arrests or cataplexy even not in end-stages of illness
[3]. It can be assumed that the remaining hypocretin neurons
in HD still release a sufficient quantity of hypocretin to
prevent the occurrence of narcoleptic-like behavioural
arrests. Therefore, our findings do not support the hypoth-
esis that hypocretin-1 may serve as an additional diagnostic
marker for HD. Furthermore, a relationship between the
sleep disturbances in patients with HD and hypocretin-1
levels appears to be unlikely.

A. Meier et al. / Brain Research 1063 (2005) 201–203 203
Acknowledgments
This study was in part supported by a grant from the
ministry of health and social security and the ministry for
science and technology. For technical assistance we thank
Ms. Schreivogel (Department of Nuclear Medicine, Goet-
tingen) and Ms. Reich-Erkelenz (Department of Psychiatry
and Psychotherapy, Goettingen).
References
[1] Declaration of Helsinki (1964), BMJ 313 (1996) 1448a–1449a.
[2] I.O. Ebrahim, Y.K. Semra, S. De Lacy, R.S. Howard, M.D. Kopelman,
A. Williams, M.K. Sharief, CSF hypocretin (orexin) in neurological
and psychiatric conditions, J. Sleep Res. 12 (2003) 83–84.
[3] G. Gardian, L. Vecsei, Huntington’s disease: pathomechanism and
therapeutic perspectives, J. Neural Transm. 111 (2004) 1485–1494.
[4] T. Kanbayashi, Y. Inoue, S. Chiba, R. Aizawa, Y. Saito, H. Tsukamoto,
Y. Fujii, S. Nishino, T. Shimizu, CSF hypocretin-1 (orexin-A)
concentrations in narcolepsy with and without cataplexy and idio-
pathic hypersomnia, J. Sleep Res. 11 (2002) 91–93.
[5] E. Mignot, G.J. Lammers, B. Ripley, M. Okun, S. Nevsimalova, S.
Overeem, J. Vankova, J. Black, J. Harsh, C. Bassetti, H. Schrader, S.
Nishino, The role of cerebrospinal fluid hypocretin measurement in
the diagnosis of narcolepsy and other hypersomnias, Arch. Neurol. 59
(2002) 1553–1562.
[6] A. Petersen, J. Gil, M.L. Maat-Schieman, M. Bjorkqvist, H. Tanila,
I.M. Araujo, R. Smith, N. Popovic, N. Wierup, P. Norlen, J.Y. Li, R.A.
Roos, F. Sundler, H. Mulder, P. Brundin, Orexin loss in Huntington’s
disease, Hum. Mol. Genet. 14 (2005) 39–47.
[7] D. Petit, J.F. Gagnon, M.L. Fantini, L. Ferini-Strambi, J. Montplaisir,
Sleep and quantitative EEG in neurodegenerative disorders,
J. Psychosom. Res. 56 (2004) 487–496.
[8] C. Peyron, D.K. Tighe, A.N. van den Pol, L. de Lecea, H.C. Heller,
J.G. Sutcliffe, Neurons containing hypocretin (orexin) project to
multiple neuronal systems, J. Neurosci. 18 (1998) 9996–10015.
[9] B. Ripley, S. Overeem, N. Fujiki, S. Nevsimalova, M. Uchino, J.
Yesavage, D. Di Monte, K. Dohi, A. Melberg, G.J. Lammers, Y.
Nishida, F.W. Roelandse, M. Hungs, E. Mignot, S. Nishino, CSF
hypocretin/orexin levels in narcolepsy and other neurological con-
ditions, Neurology 57 (2001) 2253–2258.
[10] J.G. Sutcliffe, L. de Lecea, The hypocretins: excitatory neuromodu-
latory peptides for multiple homeostatic systems, including sleep and
feeding, J. Neurosci. Res. 62 (2000) 161–168.
[11] The Huntington’s Disease Collaborative Research Group, A novel
gene containing a trinucleotide repeat that is expanded and unstable on
Huntington’s disease chromosomes, Cell 72 (1993) 971–983.