no.of pages9 article in press rev bras anestesiol. … sentinel node biopsy, ... and remifentanyl...
TRANSCRIPT

ARTICLE IN PRESS+ModelBJANE-7385; No. of Pages 9
Rev Bras Anestesiol. 2016;xxx(xx):xxx---xxx
REVISTABRASILEIRA DEANESTESIOLOGIA Publicação Oficial da Sociedade Brasileira de Anestesiologia
www.sba.com.br
SCIENTIFIC ARTICLE
Axillary local anesthetic spread after the thoracicinterfacial ultrasound block --- a cadaveric andradiological evaluation
Patricia Alfaro de la Torrea, Jerry Wayne Jones Jr.b, Servando López Álvarezc,Paula Diéguez Garciac, Francisco Javier Garcia de Migueld,Eva Maria Monzon Rubioe, Federico Carol Boeris f, Monir Kabiri Sacramentog,Osmany Duanyh, Mario Fajardo Pérez i,∗, Borja de la Quintana Gordonj
a Tajo University Hospital, Madrid, Spainb Department of Anesthesiology, College of Medicine, University of Tennessee Health Science Center/Regional One Health,Memphis, TN, USAc Hospital Complexo Hospitalario de A Coruna, Coruna, Spaind Department of Anesthesia, Segovia General Hospital, Segovia, Spaine Deparment of Anesthesia, Tajo University Hospital, Madrid, Spainf Hospital Universitario Parc Tauli Sabadell, Sabadell, Spaing Hospital Universitario de Guadalajara, Guadalajara, Spainh Primary Care and Chronic Pain Management Attending, Dept of Veterans Affairs, Muskogee, OK, USAi Hospital Universitario de Móstoles, Madrid, Spainj Deparment of Anesthesia, Móstoles University Hospital, Madrid, Spain
Received 23 February 2015; accepted 14 April 2015
KEYWORDSAxillary anesthesia;Serratus anteriorblock;Intercostal block;Axillary dissection;Inter costo brachialnerve block;
AbstractBackground: Oral opioid analgesics have been used for management of peri and postoperativeanalgesia in patients undergoing axillary dissection. The axillary region is a difficult zone to blockand does not have a specific regional anesthesia technique published that offers its adequateblockade.Methods: After institutional review board approval, anatomic and radiological studies wereconducted to determine the deposition and spread of methylene blue and local anestheticinjected respectively into the axilla via the thoracic inter-fascial plane. Magnetic Resonance
Inter fascial thoracic Imaging studies were then conducted in 15 of 34 patients scheduled for unilateral breast surgeryowing: axillary clearance, sentinel node biopsy, axillary node biopsy,to ascertain the deposition and time course of spread of solutioncial plane in vivo.
block that entailed any of the follor supernumerary breasts,
within the thoracic interfas
Please cite this article in press as: de la Torre PA, et al. Axillary local anesthetic spread after thethoracic interfacial ultrasound block --- a cadaveric and radiological evaluation. Rev Bras Anestesiol. 2016.http://dx.doi.org/10.1016/j.bjane.2015.04.007
∗ Corresponding author.E-mail: [email protected] (M.F. Pérez).
http://dx.doi.org/10.1016/j.bjane.2015.04.0070104-0014/© 2016 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. This is an open access article under the CCBY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).

ARTICLE IN PRESS+ModelBJANE-7385; No. of Pages 9
2 P.A. de la Torre et al.
Results: Radiological and Cadaveric studies showed that the injection of local anesthetic andmethylene blue via the thoracic inter-fascial plane, using ultrasound guide technique, resultsin reliable deposition into the axilla. In patients, the injection of the local anesthetic produceda reliable axillary sensory block. This finding was supported by Magnetic Resonance Imagingstudies that showed hyper-intense signals in the axillary region.Conclusions: These findings define the anatomic characteristics of the axillary region block,and underline the clinical potential of these novel blocks.© 2016 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. This is anopen access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVEAnestesia axilar;Bloqueio serrátilanterior;Bloqueio intercostal;Esvaziamento axilar;Bloqueio do nervointercostobraquial;Bloqueio torácicointerfascial
Dispersão axilar de anestésico local após bloqueio interfascial torácico guiado porultrassom - estudo radiológico e em cadáver
ResumoJustificativa: Os analgésicos orais à base de opioides têm sido usados para o manejo da analgesianos períodos peri e pós-operatório de pacientes submetidos à linfadenectomia axilar. A regiãoaxilar é uma zona difícil de bloquear e não há registro de uma técnica de anestesia regionalespecífica que ofereca o seu bloqueio adequado.Métodos: Após a aprovacão do Conselho de Ética institucional, estudos anatômicos e radi-ológicos foram realizados para determinar a deposicão e disseminacão de azul de metileno eanestésico local, respectivamente injetados na axila via plano interfascial torácico. Exames deressonância magnética foram então realizados em 15 de 34 pacientes programados para cirurgiade mama unilateral envolvendo qualquer um dos seguintes procedimentos: esvaziamento axi-lar, biópsia de linfonodo sentinela, biópsia de linfonodo axilar, ou mamas supranumerárias, paraverificar a deposicão e tempo de propagacão da solucão dentro do plano interfascial torácicoin vivo.Resultados: Estudos radiológicos e em cadáveres mostraram que a injecão de anestésico locale azul de metileno via plano interfascial torácico usando a técnica guiada por ultrassom resultaem deposicão confiável na axila. Em pacientes, a injecão de anestésico local produzido umbloqueio sensorial axilar confiável. Esse achado foi corroborado por estudos de ressonânciamagnética que mostraram sinais hiperintensos na região axilar.Conclusões: Esses achados definem as características anatômicas do bloqueio da região axilare destacam o potencial clínico desses novos bloqueios.© 2016 Sociedade Brasileira de Anestesiologia. Publicado por Elsevier Editora Ltda. Este e um
a lic
I
PouvTanwe[(tp
3vn
r
tiwtibtpiliagbe
pt
artigo Open Access sob umnc-nd/4.0/).
ntroduction
atients who undergo axillary surgery suffer variable post-perative discomfort and pain.1 Until today, there is noltrasound-guided regional anesthesia technique that pro-ides adequate blockade of the axillary compartment.horacic paravertebral block (TPVB) is the main regionalnesthetic technique used in breast surgery,2,3 but it doesot provide analgesia from the anterior and lateral chestall, such as the supraclavicular nerves (C4---C5), the lat-ral pectoral nerve [LPn] (C5---C6), medial pectoral nerveMPn] (C8---T1) and medial brachio-cutaneous nerve [MBCn]C8---T1).4 The chronic pain that occurs after axillary dissec-ion (AD), often results from inadequate treatment of acuteostoperative pain.5---7
As described by Moore and Dalley,8 the axilla has 4 walls, of which are muscular Fig. 1. The cutaneous sensory inner-ation of the axilla is supplied by the intercostobrachial
Please cite this article in press as: de la Torre PA,thoracic interfacial ultrasound block --- a cadaveric andhttp://dx.doi.org/10.1016/j.bjane.2015.04.007
erves (ICBn) and medial brachio-cutaneous nerve (MBCn).In the present report, we will discuss three tho-
acic interfascial ultrasound-guided approaches.9---13 Theseic
enca CC BY-NC-ND (http://creativecommons.org/licenses/by-
echniques have been recently described, with encourag-ng effects on blockade of the neural afferents of the chestall, in spite of the few samples reported.8---11 However,
he detailed anatomic characteristics and the spread of LAn these interfascial ultrasound-guided blocks have not yeteen determined. We hypothesize that LA injection intohe interfascial plane of the antero-lateral chest wall; willroduce enough spread into the axillary fascia, due thenter-fascial connection of the muscles that form the axil-ary wall. This may help in reducing acute postoperative painn patients undergoing axillary dissection and may becomen alternative to other techniques used to provide anal-esia after breast surgery. We consider these inter-fasciallocks easy techniques: they are superficial blocks and thecho-anatomy is simple to understand.9---11,13---17
The Pec’s block,14 appears to be particularly useful foratients who have breast expanders placed during recons-ructive breast cancer surgery or subpectoral prostheses.13
et al. Axillary local anesthetic spread after the radiological evaluation. Rev Bras Anestesiol. 2016.
The Serratus-Intercostal Fascial Block (SIFB) anterior,15
nvolve injecting the LA between the Serratus Anterior mus-le and the External Intercostal muscle. The efficacy of

ARTICLE IN+ModelBJANE-7385; No. of Pages 9
Local anesthetic spread after the thoracic interfacial
30
25
20
15
10
5
0
0 1 2 3
Recovery 12 hours 24 hours Discharge
Figure 1 The boundaries of the axilla. Visual analog scalescores in patient with Serratus --- intercostal fascial block ante-rior approach after axillary surgery. Visual analog scale (VAS;
astt
mbeb
acta
tvoatv5bb4P
focbMtK1pmtr
avitaaPopioPfmpppA
0 = no pain, 10 = worst pain imaginable) was zero are VAS atrecovery, 12; 24 discharge.
SIFB techniques have been reported by findings described intwo observational studies in patient under no reconstructivebreast surgery.11,15
We conducted a cadaveric dissections and radiologicalstudy, with the goal of characterizing the SIFB injection,as well as evaluating the spread of local anesthetic agentsinjected via this interfascial plane.
Methods
Thirty five consecutive patients, scheduled for axillarysurgery, were recruited to take part in the radiological study,34 females and 1 male. The age range was 18---80 years. Insti-tutional review board approval and written consents wereobtained before conducting the ultrasound thoracic inter-fascial blocks and MRI studies in 5 of 35 patients. The timeperiod was September 2013 through May 2014.
The inclusion criteria were: patients scheduled for axil-lary clearance, sentinel node biopsy, axillary node biopsy,axillary supernumerary breasts or melanoma excisions.
Exclusion criteria included patients unable or unwilling tocooperate in this study, known allergy to LA and/or to opi-oids, bleeding disorders, on anticoagulants, significant liveror renal disease, diabetes, history of drug or alcohol abuse,pain patients receiving chronic analgesics or corticosteroids.
Patients were randomly allocated by a computer-generated list of numbers, which were placed inside sealedenvelopes to three groups. Intravenous (IV) access wasestablished, routine monitoring (EKG, non-invasive bloodpressure, oxygen saturation) was used. All patients weregiven midazolam 1---2 mg IV before the block. The patientsreceived a preoperative, ipsilateral SIPB, anterior approach
Please cite this article in press as: de la Torre PA,thoracic interfacial ultrasound block --- a cadaveric andhttp://dx.doi.org/10.1016/j.bjane.2015.04.007
single-injection (Fig. 2).The ultrasound blocks were performed in the Radiol-
ogy Department, before surgery using a Locoplex (Vygon;Ecouen, France) block needle (17 degree, 25 gauge, 100 mm)
T
ao
PRESS3
nd a Mindray M7 (Mindray Medical; Madrid, Spain) ultra-ound machine with a high-frequency probe (6---13 MHz). Theotal amount of local anesthetic was injected under real-ime ultrasound visualization.
Decreased temperature sensation in the T1---T3 der-atomes was determined as an indication of successfullock of the axilla. An unbiased observer evaluated thextent of blockade. The fine and gross touch were evaluatedy using a cotton wool and pin prick, respectively.
The patients were then transferred to the operating roomnd general anesthesia was induced with target injectionontrol (TCI) of Propofol and Remifentanyl (depending onhe patient’s age and physical condition). Laryngeal maskirways appropriate for weight were inserted.
Controlled ventilation was maintained aiming at an end-idal CO2 pressure between 35---40 mm/Hg. The patient’sital signs remained within 20% of baseline values through-ut the operation. Anesthesia was maintained with Propofolnd Remifentanyl TCI and an oxygen/air mix with a frac-ion of inspired oxygen (FiO2) of 40%. Bispectral Indexalues were maintained between 40 and 60. Remifentanyl---10 mcg/kg bolus doses were given whenever mean arteriallood pressure or heart rate exceeded 20% of preoperativeaseline values. All patients were treated with Ondansetron
mg IV, 30 min before the end of the procedure, to preventONV.
After emerging from anesthesia, the patients were trans-erred to the post anesthesia care unit (PACU) for a 24 hbservation period. Analgesia was provided with patient-ontrolled analgesia (PCA) with Morphine 1 mg/mL, set atoluses of 1 mg with a lockout period of 10 min. Maximumorphine consumption at 4 h was set at 24 mg. In addi-
ion, the patients were given IV Acetaminophen 1 g andetoprophen 25 mg every 8 h. Nausea lasting more than0 min or vomiting was treated with 4 mg Ondansetron. Mor-hine consumption, as well as administration of antiemeticedication and incidence of adverse effects (nausea, vomi-
ing, pruritus, sedation, headache, and hypotension) wasecorded.
Postoperative analgesia data was collected using a visualnalog scale (VAS). Initial pain assessment in the PACU byisual analog scale (VAS; 0 = no pain, 10 = worst pain imag-nable) was zero, as well as painful restricted movement ofhe shoulder, classified into three grades (restricted, fair,nd free) every 4 h starting from the arrival of the patientt PACU, and lasting throughout the 24 h study period.ainful restricted movements were assessed as abductionf the arm and scores were as follows: all 3 modalitiesresent = free, 2 modalities present = fair, 1 or 0 modal-ty present = restricted. Data was collected by an unbiasedbserver who was not otherwise involved in the study.atients were monitored throughout their hospital stayor complications related to SIFB (pneumothorax, externalammary artery lesion), and for signs of LA toxicity as wellain in the site of injection. After 24 h of post-operativeeriod and free of surgical or anesthetic complications, theatients were discharged home. Patients were given oralcetaminophen 1 g plus Ketoprophen 25 mg every 8 h, and
et al. Axillary local anesthetic spread after the radiological evaluation. Rev Bras Anestesiol. 2016.
ramadol 50 mg every 4 h to use at home.After receiving approval from the local ethics committee
nd written consent from the cadavers’ families, as partf a donation program from the ‘‘Universidad Autonoma de
ARTICLE IN PRESS+ModelBJANE-7385; No. of Pages 9
4 P.A. de la Torre et al.
pmmsam r 2
r 3
PMM
A
B
PF
CPF
Clavicle
D
C
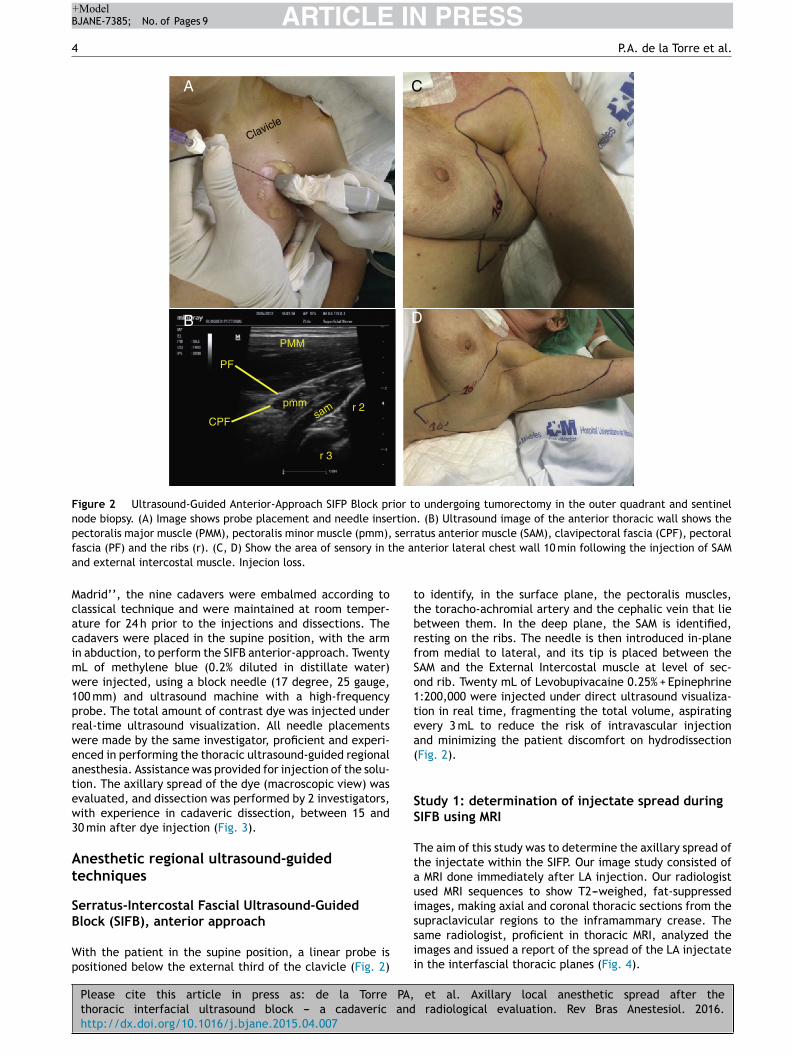
Figure 2 Ultrasound-Guided Anterior-Approach SIFP Block prior to undergoing tumorectomy in the outer quadrant and sentinelnode biopsy. (A) Image shows probe placement and needle insertion. (B) Ultrasound image of the anterior thoracic wall shows thepectoralis major muscle (PMM), pectoralis minor muscle (pmm), serratus anterior muscle (SAM), clavipectoral fascia (CPF), pectoralf he aa
Mcacimw1prweatew3
At
SB
Wp
ttbrfSo1tea(
SS
Ttaui
ascia (PF) and the ribs (r). (C, D) Show the area of sensory in tnd external intercostal muscle. Injecion loss.
adrid’’, the nine cadavers were embalmed according tolassical technique and were maintained at room temper-ture for 24 h prior to the injections and dissections. Theadavers were placed in the supine position, with the armn abduction, to perform the SIFB anterior-approach. TwentyL of methylene blue (0.2% diluted in distillate water)ere injected, using a block needle (17 degree, 25 gauge,00 mm) and ultrasound machine with a high-frequencyrobe. The total amount of contrast dye was injected undereal-time ultrasound visualization. All needle placementsere made by the same investigator, proficient and experi-nced in performing the thoracic ultrasound-guided regionalnesthesia. Assistance was provided for injection of the solu-ion. The axillary spread of the dye (macroscopic view) wasvaluated, and dissection was performed by 2 investigators,ith experience in cadaveric dissection, between 15 and0 min after dye injection (Fig. 3).
nesthetic regional ultrasound-guidedechniques
erratus-Intercostal Fascial Ultrasound-Guided
Please cite this article in press as: de la Torre PA,thoracic interfacial ultrasound block --- a cadaveric andhttp://dx.doi.org/10.1016/j.bjane.2015.04.007
lock (SIFB), anterior approach
ith the patient in the supine position, a linear probe isositioned below the external third of the clavicle (Fig. 2)
ssii
nterior lateral chest wall 10 min following the injection of SAM
o identify, in the surface plane, the pectoralis muscles,he toracho-achromial artery and the cephalic vein that lieetween them. In the deep plane, the SAM is identified,esting on the ribs. The needle is then introduced in-planerom medial to lateral, and its tip is placed between theAM and the External Intercostal muscle at level of sec-nd rib. Twenty mL of Levobupivacaine 0.25% + Epinephrine:200,000 were injected under direct ultrasound visualiza-ion in real time, fragmenting the total volume, aspiratingvery 3 mL to reduce the risk of intravascular injectionnd minimizing the patient discomfort on hydrodissectionFig. 2).
tudy 1: determination of injectate spread duringIFB using MRI
he aim of this study was to determine the axillary spread ofhe injectate within the SIFP. Our image study consisted of
MRI done immediately after LA injection. Our radiologistsed MRI sequences to show T2---weighed, fat-suppressedmages, making axial and coronal thoracic sections from the
et al. Axillary local anesthetic spread after the radiological evaluation. Rev Bras Anestesiol. 2016.
upraclavicular regions to the inframammary crease. Theame radiologist, proficient in thoracic MRI, analyzed themages and issued a report of the spread of the LA injectaten the interfascial thoracic planes (Fig. 4).
ARTICLE IN PRESS+ModelBJANE-7385; No. of Pages 9
Local anesthetic spread after the thoracic interfacial 5
Apex
Lateral wall
Base
BasePMMpmmSAM
LDBB
Posterior wall
Medial wall
Anterior wall
2nd
H
3rd
4th
5th
Sternum
Clavicle
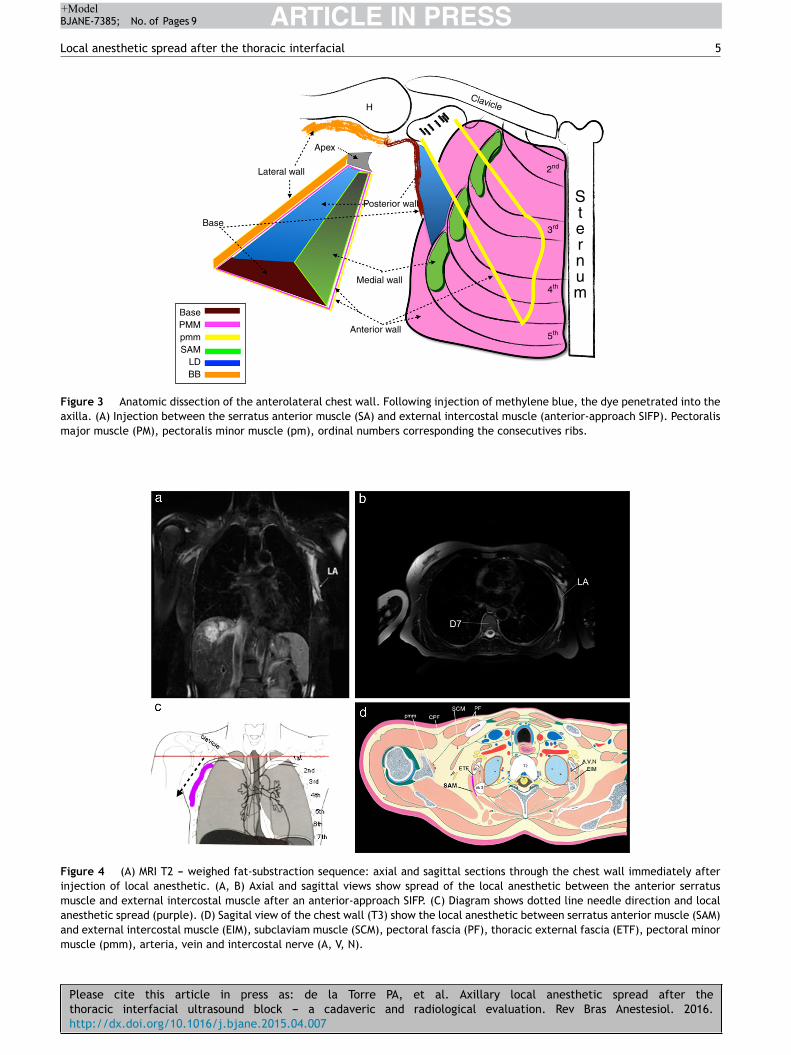
Figure 3 Anatomic dissection of the anterolateral chest wall. Following injection of methylene blue, the dye penetrated into theaxilla. (A) Injection between the serratus anterior muscle (SA) and external intercostal muscle (anterior-approach SIFP). Pectoralismajor muscle (PM), pectoralis minor muscle (pm), ordinal numbers corresponding the consecutives ribs.
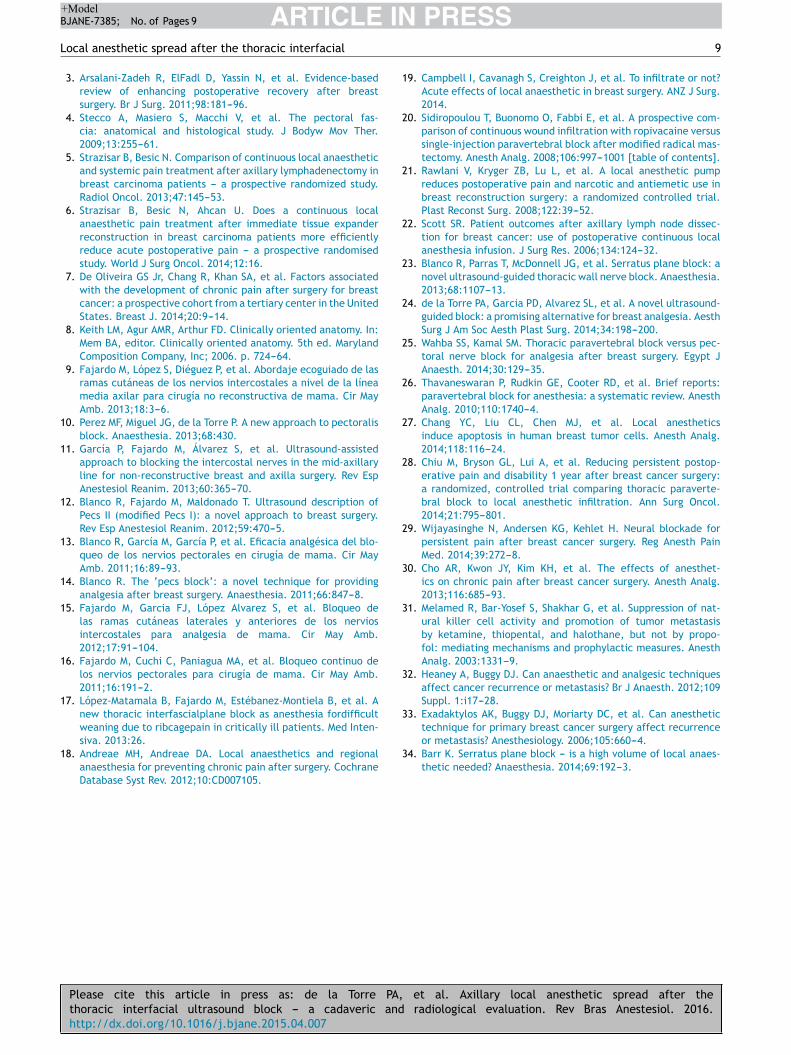
Figure 4 (A) MRI T2 --- weighed fat-substraction sequence: axial and sagittal sections through the chest wall immediately afterinjection of local anesthetic. (A, B) Axial and sagittal views show spread of the local anesthetic between the anterior serratusmuscle and external intercostal muscle after an anterior-approach SIFP. (C) Diagram shows dotted line needle direction and localanesthetic spread (purple). (D) Sagital view of the chest wall (T3) show the local anesthetic between serratus anterior muscle (SAM)
Please cite this article in press as: de la Torre PA,thoracic interfacial ultrasound block --- a cadaveric andhttp://dx.doi.org/10.1016/j.bjane.2015.04.007
and external intercostal muscle (EIM), subclaviam muscle (SCM), pecmuscle (pmm), arteria, vein and intercostal nerve (A, V, N).
et al. Axillary local anesthetic spread after the radiological evaluation. Rev Bras Anestesiol. 2016.
toral fascia (PF), thoracic external fascia (ETF), pectoral minor

ARTICLE IN+ModelBJANE-7385; No. of Pages 9
6
Table 1 Patients characteristic (n35). Dates are presentedas absolutely number or median with 25th to 75th interquar-tile range.
Parient characteristics (n = 34)
Female/male 33/1Age 46 (22---68)BMI 24 (18---35)ASA I/II/III 2/30/2
Surgical procedureAxillary biposy 4Reintervention of axillary lymph none
cleareance2
Melanoma 1Lumpectomy with centinele node 23Mastectomy with axillary cleareance 4
Data are present as absolute number or medians with 25th to
Sc
Tuteuo
R
PsritMtgea
St
IfpLecMp
Lwm2
Etcrmtppw
St
Adi
ftal
D
Tstbiiopumli
DtbbaLbatsccatuawglc
75th interquartile range ASA indicates American Society of Anes-thesiologist. BMI, body mass index.
tudy 2: Validation of Ultrasound-Guided SIFB in aadaver model
he aim of this study was to validate the describedltrasound-guided regional technique, by demonstratinghat they resulted in the deposition of dye within the lat-ral thoracic interfascial planes reaching the axilla. Anltrasound-guided SIFB anterior approach) was performedn nine embalmed cadavers (Fig. 3).
esults
atient data, the type of surgery and dermatomic loss sen-ory are showed in Table 1 and Fig. 1 respectively. Weealized that the LA reached the axilla if injected into thenterfascial planes of the medial axillary wall. In our opinion,he radiological findings support the correlation betweenRI images and territories blocked. Thirty two patients of
he SIFB groups reported a VAS = 0. No patient from thisroups needed a rescue Remifentanyl bolus in the intraop-rative or Morphine in PACU. 32/35 patients classified thenesthesia technique used as excellent and 2/35 as good.
tudy 1: Validation of Ultrasound-Guided SIFBechniques using MRI
n five patients our study, the imaging studies (T2 weighed,at-subtraction, axial and coronal views) clearly showed theresence of a hyperintense signal (corresponding with theA) between the interfascial planes in the anterior and lat-ral chest wall. The LA was noted to spread into the axilla,overing the intercostobrachial nerve territories, and theedial Brachio-Cutaneous nerve (MBCn) (Fig. 3) in the 35/35atients (Fig. 1).
In patients who received the SIFB-anterior approach, the
Please cite this article in press as: de la Torre PA,thoracic interfacial ultrasound block --- a cadaveric andhttp://dx.doi.org/10.1016/j.bjane.2015.04.007
A spread into the interfascial plane of the lateral chestall reaching the axilla (Figs. 2 and 4). The patients wereonitored during the performance of these bocks and for
4 h after for signs of local anesthetic toxicity. We used
io
p
PRESSP.A. de la Torre et al.
co-Doppler images in real time to avoid intravascular injec-ion. There were not recognized symptoms and signs of thisomplication on any patient. We did not point out Long Tho-acic nerve (LTn) palsy in both approaches. Brachial plexusotor deficit was not seen in any patient. The MBCn and
he Intercostobrachial nerve territories were blocked in allatients, reaching the upper third of the medial arm. Allatients referred discomfort after needle bone contact andhen the LA hydrodissection started.
tudy 2: Validation of Ultrasound-Guided SIFBechniques in a cadaver
natomic dissection of the 9 embalmed cadavers (asescribed above) showed the spread of dye into the serratusntercostal fascial plane, reaching the axilla (Fig. 3).
In the SIFB anterior approach, the methylene blue wasound into the axilla in all cadavers. The ICBn, MCBn andhe intercostal territories from T1 to T3 were stained. Welso observed the contrast reaching the posterior axillaryine.
iscussion
his radiological and cadaveric study evaluated and demon-trated the feasibility of using ultrasound-guided approacheso block the axillary region, through the interfascial planesetween the muscles of the medial axillary wall. Our find-ngs show that the SIFP injections provide a potential spacento which LA can be deposited to achieve sensory blockadef the IBCn and MBCn. These studies also indicate that it isossible the injection of the LA into the SIFP in vivo usingltrasound-guided techniques. These findings show that theedial chest wall offer an easy mean to reach the axil-
ary due the communication or permeability of the thoracicnterfascial planes.
The axillary compartment is a difficult region to block.espite the thoracic para-vertebral block (TPVB) beinghe gold standard technique for breast surgery, we haveeen using these new interfascial thoracic ultrasound-guidelocks. We described here to achieve analgesia after breastnd axillary surgery with good results.9,11,15---17 Pre-incisionalA infiltration reduces pain during the initial hours afterreast and axilla operations, and therefore this has become
standard procedure in our unit.5,6 Campbell et al. inheir study concluded the LA infiltration during breasturgery has a marked opioid sparing effect, with signifi-ant patient benefits, reducing nursing workload and drugosts.19 Sidiropoulou et al.20 in their study, evaluated thenalgesic efficacy and morphine consumption of the twoechniques after mastectomy, concluding that the contin-ous wound infiltration of local anesthetics is an effectivelternative to paravertebral analgesia after mastectomyith axillary dissection. These new thoracic ultrasounduide interfascial blocks may have some similar aspects toocal wound infiltration, but they use less amount of LA, aatheter can also be placed before the surgery to cause no
et al. Axillary local anesthetic spread after the radiological evaluation. Rev Bras Anestesiol. 2016.
nterference with the surgical field and thus reduce the postperatory pain.16
Oral opioid analgesics have traditionally been used torovide peri and postoperative analgesia in patients who

IN+Model
tar
ttdtatbwstwo
dcb
mt
fBsStetwEac‘na
(cm
niTrdsfIabs
mbt
ARTICLEBJANE-7385; No. of Pages 9
Local anesthetic spread after the thoracic interfacial
undergo axillary dissection. Previous studies evaluated theeffects of peri and postoperative administration of LA.The results obtained by Rawlani21 in his double-blind, ran-domized, prospective study, supports the efficacy of apostoperative local anesthetic pain pump in reducing pain,narcotic use, and postoperative nausea and vomiting inwomen undergoing breast reduction. Scott22 compared theefficacy of continuous axillary administration of bupiva-caine versus standard surgical treatment or placebo inpatients undergoing axillary lymph node dissection. Thepatients treated with a continuous infusion of bupivacaineexperienced significantly lower pain scores. The postopera-tive opioid analgesic requirements also were significantlydecreased in the bupivacaine group. The use of continu-ous administration of bupivicaine after axillary lymph nodedissection significantly decreases pain and opioid analgesicrequirements, with concomitant decreases in nausea andsedation. This study provides encouraging evidence of thetherapeutic benefits of continuous infusion of local anes-thesia and may represent a valuable adjunct for surgicalpatients who require ALND, including those with breast can-cer and melanoma. Strazisar5 observed that wound infusionin the LA group (vs. the standard opioid-based analgesiagroup) resulted in a greater reduction of acute pain andenabled reduced opioid consumption; they also noted atrend toward reduction of chronic pain in the LA group.Fajardo et al.16 published the interpectoral fascia infusionof Levobupivacaine 0.125% (5 mL/h) in patients undergoingmastectomy and axillary clearance and found good analge-sia and less opioid consumption. Diéguez et al.11 in January2013, published (article in Spanish) the LA infiltration on themid-axillary line in a patient for breast surgery. Diéguez11 inher study demonstrated the effectiveness of the ultrasound-guided injection of LA between serratus anterior muscle(SAM) and external intercostal muscle (EIM) named BRILMA(in Spanish: intercostal branch nerves in the midaxillaryline block) in an observational study in 30 patients sched-uled for non-reconstructive breast and axilla dissection.Diéguez11 found that injecting 15 mL Levobupivacaine 0.25%(3 mL in each intercostal space) provides adequate intra-operative and post operatory analgesia. Blanco et al., in201323 performed the Serratus block at 2 different levelsin four healthy volunteers’. The first was superficial to theSAM, similar to Pec’s block II,11 technique published in 2012.This approach aims to block at least the pectoral nerves, theintercostobrachial and the intercostals branches.
On September 2012, Fajardo published a descriptive,observational study in 44 women scheduled for breastsurgery,15 on which he combined the block of the lateraland anterior cutaneous branches of the intercostal nerves.The objective of this study was to evaluate extension ofLA through MRI, after the ultrasound-guided injection ofLA between SAM and EIM. It was observed that, in mostpatients, the LA spread to the axila and under the lateral andposterior chest wall, between T2 and T7 dermatomes, resultcomparable with Blanco et al.23 We believe that LA injectionbetween the SAM and EIM is more advantageous than injec-tions superficial to the SAM because it may avoid transitory
Please cite this article in press as: de la Torre PA,thoracic interfacial ultrasound block --- a cadaveric andhttp://dx.doi.org/10.1016/j.bjane.2015.04.007
palsy of the LTN and likely achieve more distal dermatomalspread. The LA injection between the Pectoral Minor Muscle(pmm) and SAM (Pec’s block II) has a good spread to, butthe spread beyond T3 is erratic because the axillary fatty
SttT
PRESS7
issue may limit the LA spread. In our clinical practice, webandoned this block in breast surgery because the patientseferred pain al level of the nipple-aereola complex.
The Pec’s II block12 achieves suitable axillary dissemina-ion. Nevertheless, we did not evaluate this technique dueo being a more complex technique to perform than SIFBespite of greater axillary spread. The fascial space betweenhe pectoralis minor and serratus anterior muscles is notlways easy to find, especially in the elderly patients. Con-rary to the Pec’s block II, we intentionally injected the LAelow the SAM for two reasons: to achieve greater spreadithin the serratus-intercostal plane and thus blocking the
econd and third intercostal nerves (ICBn), while avoidinghe possibility of transitory palsy of the LTN, leading to ainged scapula than can be mistaken with a surgical lesionf this nerve.
The serratus interfascial plane (SIFP) is a small, poorlyistensible neurovascular space between the SAM and EIMontaining the perforating lateral intercostal cutaneousranches of the intercostal nerves.
The SIFP’s poor distensibility, along with the respiratoryovements, allows the LA to be extensively dispersed within
his plane.We would like to unify concepts in order to avoid con-
using our readers. We use the term SIFB9,15,17,24 insteadRILMA11 because for anglo readers it is easier to under-tand, but the interfascial plane injection is the same. TheAM has several anatomical relationship in the chest wall,he same way the transversus abdominis muscle in the lat-ral abdominal wall, keeps an anatomical relationship withhe internal oblique muscle. The SAM, in the lateral chestall, attaches to the ribs and gets in contact with theIM, being covered by the PMM, pmm and latissimus dorsi,nd later gets enmeshed with the external oblique mus-le in the antero-inferior thoracic wall. Therefore the name‘serratus anterior plane’’ would be incorrect, since it doesot describe the specific interfascial plane where the localnesthetic gets deposited.
Wahba25 evaluated the thoracic paravertebral blockTPVB) versus pectoral nerve block in regard to morphineonsumption and analgesic efficacy after modified radicalastectomy.It was concluded that 24 h morphine consumption was sig-
ificantly lower in Pec’s block group, and lower pain scoresn the first 12 h in comparison with TPVB after mastectomy.his result are contradictory, no corresponding with theesults published.2,18,26 Based on the current evidence nowa-ays, the TPVB is the gold standard technique for breasturgery, despite the encouraging results of these new inter-ascial thoracic block.2,18 Based on our experience, the Pec’sI block does not provide adequate analgesia for mastectomynd the LA hardly reaches beyond the level of T3---T4. Weelieve that Pec’s II block is a good technique for axillaryurgery, not for mastectomy.
The SIPB lateral approach was recently evaluated as aethod to achieve analgesia after breast surgery, breastrachitherapy, chest drain tube.9,11,15,17,24 To improve thisechnique we use a long needle to advance it through the
et al. Axillary local anesthetic spread after the radiological evaluation. Rev Bras Anestesiol. 2016.
IFP lateral approach and when practiced hydrodissection,hus placing the LA as distal as possible. The ribs are impor-ant ultrasound landmarks to avoid pleural or lung puncture.he use of sedation analgesia relieves patient discomfort

IN+ModelB
8
dsabsaps
nt
tshptpwf
ccpgsmeisbbrpcn
lIorcautsiewsbrou
ustoots
bi
C
TdrS
gotoipstg
prutocrwrtiicoa
C
T
A
Tw‘tdsCWS
R
ARTICLEJANE-7385; No. of Pages 9
ue the SAM puncture, ribs periosteum contact and hydrodis-ection of the interfascial plane. To perform SIFB-lateralpproach, we prefer placing the patient in the lateral decu-itus position or place a pillow under the chest because theoft tissue will drop down and the distance between the skinnd the ribs is shortened. Also, resting the hand holding therobe on the lateral chest wall will make the technique moretable.
To improve these blocks, now we use fine and sharpeedles for ‘‘single shots’’ and Tuohy needles to place con-inuous catheters.
This thoracic interfascial ultrasound block are simpleechnique and relatively quick to perform, since they areuperficial and sonographically easy to understand, and theyave a reproducible sonoanatomy in the vast majority ofatients, and may be perform in patient under general anes-hesia. For that reason these novels block are techniqueerformed usually by anesthesiologists, but nurse anestheticith training in regional block and surgeons would feel com-
ortable to perform such blocks.They may also provide additional options when cir-
umstances are unfavorable to perform a TPVB (such asoagulopathy, intolerance of sympathectomy or inability toosition a patient properly). In addition, these can be tar-eted to unilateral or segmental surgery and can covereveral dermatomes and the axilla with one injection. Theyay also very easily be performed as continuous periph-
ral nerve blocks with catheters, when extended analgesias required. In our experience and from discussions with oururgeons, these blocks do not interfere with the surgical fieldecause the LA is placed between interfascial planes. Theselocks may open new doors to investigation regarding theecurrence of breast cancer and the incidence of chronicain after breast surgery.27 Today, we do not have enoughlinical data to compare these techniques with other tech-iques used in patients undergoing breast surgery.
We consider that these new blocks may have the fol-owing indications, according to our experience: the Pec’s
block may be used in subpectoral prosthesis surgery withr without axillary approach, as well as for axillary surgery,emembering that it is also necessary to block the inter-ostal nerves, hence this block should not be used as the onlynesthetic technique. The SIFB anterior approach can besed for non-reconstructive breast surgery and in combina-ion with Pec’s I block in patients undergoing reconstructiveurgery, and for subpectoral prosthesis to block the lateralntercostal branches and the pectoral nerves. The SIFB lat-ral approach can be used for mastectomy, lumpectomy asell axillary clearance, and may be an alternative for latis-
imus dorsi flaps. The LA placed in the under ribs will diffuseetween the intercostal muscles, thus blocking the ante-ior and lateral intercostal branches, producing sensory lossf the whole breast and diffusing anteriorly and posteriorlynder the ribcage, reaching the posterior axillary line.
Even though our results are encouraging, we deemed itnnecessary to submit a large number of patients to an inva-ive investigation, for a small sample could bear out ourheory. This study might open a new door to the analgesia
Please cite this article in press as: de la Torre PA,thoracic interfacial ultrasound block --- a cadaveric andhttp://dx.doi.org/10.1016/j.bjane.2015.04.007
f the axilla. We also did not explore the minimum amountf LA required to block the intercostal nerves that supplyhe breast and axilla. Despite using embalmed cadavers, theame level of adequate spread was demonstrated ‘‘in vivo’’
PRESSP.A. de la Torre et al.
y using MRI. This is a descriptive study, further investigations warranted.
onclusions
his study represents, in our opinion, the first detailedepiction of the anatomic characteristics of interfascial tho-acic blocks to achieve sensory block of the axilla (IPFP andIFB blocks).
These novel techniques may become widely used anal-esic alternatives in axilla surgery given their low ratef complications and the characteristic single-punctureechnique that allows simultaneous blockade of numer-us dermatomes. Additional benefits of these techniquesnclude applicability to the outpatient setting and toatients who have undergone a neuraxial block, may beafely practiced in a patient under general anesthesia, andhe time consumed to block, 5---10 min, does not affect sur-ical time.
These blocks also might reduce the incidence of chronicain after axillary dissection,5,6,28,29 the likelihood of tumorecurrence, decreasing noxious stimuli, as well as to atten-ate the surgical stress response.29,30 Studies have shownhat breast cancer patients who received the combinationf a nerve block plus general anesthesia for their breastancer surgery, had less cancer recurrence than those whoeceived only general anesthesia.31---33 Moreover, patientsho received a nerve block, needed less post-operative pain
elief from opioid drugs. We are waiting for a result ofhe observational studies and randomized controlled clin-cal trials, that are needed to confirm whether the thoracicnterfascial block techniques are appropriate for routinelinical practice, and to determine the minimum amountf LA34 required for blockade as well as the serum localnesthetic concentrations.
onflicts of interest
he authors declare no conflicts of interest.
cknowledgments
he authors want to express their gratitude to the familiesho participated in the cadaver donation program of the
‘Universidad Autonoma de Madrid’’. We would like to thankhe Department of Anatomy of the ‘‘Universidad Autonomae Madrid’’, especially Dr. Francisco Clascá Cabré, Profe-or of Anatomy and Human Embriology, and Andrés Olayaéspedes, Anatomy Technician, for their continued support.e also thank Dr. Tomislav Stanic, Dr. Luis Valdes, Dr. Carlos
alazar for his help in the review of this manuscript.
eferences
1. Corten E, Schellekens P, Hage J, et al. Clinical outcome afterpedicled segmental pectoralis major island flaps for head and
et al. Axillary local anesthetic spread after the radiological evaluation. Rev Bras Anestesiol. 2016.
neck reconstruction. Ann Plast Surg. 2009;63:292---6.2. Schnabel A, Reichl SU, Kranke P, et al. Efficacy and safety of
paravertebral blocks in breast surgery: a meta-analysis of ran-domized controlled trials. Br J Anaesth. 2010;105:842---52.
IN+Model
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3technique for primary breast cancer surgery affect recurrence
ARTICLEBJANE-7385; No. of Pages 9
Local anesthetic spread after the thoracic interfacial
3. Arsalani-Zadeh R, ElFadl D, Yassin N, et al. Evidence-basedreview of enhancing postoperative recovery after breastsurgery. Br J Surg. 2011;98:181---96.
4. Stecco A, Masiero S, Macchi V, et al. The pectoral fas-cia: anatomical and histological study. J Bodyw Mov Ther.2009;13:255---61.
5. Strazisar B, Besic N. Comparison of continuous local anaestheticand systemic pain treatment after axillary lymphadenectomy inbreast carcinoma patients --- a prospective randomized study.Radiol Oncol. 2013;47:145---53.
6. Strazisar B, Besic N, Ahcan U. Does a continuous localanaesthetic pain treatment after immediate tissue expanderreconstruction in breast carcinoma patients more efficientlyreduce acute postoperative pain --- a prospective randomisedstudy. World J Surg Oncol. 2014;12:16.
7. De Oliveira GS Jr, Chang R, Khan SA, et al. Factors associatedwith the development of chronic pain after surgery for breastcancer: a prospective cohort from a tertiary center in the UnitedStates. Breast J. 2014;20:9---14.
8. Keith LM, Agur AMR, Arthur FD. Clinically oriented anatomy. In:Mem BA, editor. Clinically oriented anatomy. 5th ed. MarylandComposition Company, Inc; 2006. p. 724---64.
9. Fajardo M, López S, Diéguez P, et al. Abordaje ecoguiado de lasramas cutáneas de los nervios intercostales a nivel de la líneamedia axilar para cirugía no reconstructiva de mama. Cir MayAmb. 2013;18:3---6.
10. Perez MF, Miguel JG, de la Torre P. A new approach to pectoralisblock. Anaesthesia. 2013;68:430.
11. García P, Fajardo M, Álvarez S, et al. Ultrasound-assistedapproach to blocking the intercostal nerves in the mid-axillaryline for non-reconstructive breast and axilla surgery. Rev EspAnestesiol Reanim. 2013;60:365---70.
12. Blanco R, Fajardo M, Maldonado T. Ultrasound description ofPecs II (modified Pecs I): a novel approach to breast surgery.Rev Esp Anestesiol Reanim. 2012;59:470---5.
13. Blanco R, García M, García P, et al. Eficacia analgésica del blo-queo de los nervios pectorales en cirugía de mama. Cir MayAmb. 2011;16:89---93.
14. Blanco R. The ‘pecs block’: a novel technique for providinganalgesia after breast surgery. Anaesthesia. 2011;66:847---8.
15. Fajardo M, Garcia FJ, López Alvarez S, et al. Bloqueo delas ramas cutáneas laterales y anteriores de los nerviosintercostales para analgesia de mama. Cir May Amb.2012;17:91---104.
16. Fajardo M, Cuchi C, Paniagua MA, et al. Bloqueo continuo delos nervios pectorales para cirugía de mama. Cir May Amb.2011;16:191---2.
17. López-Matamala B, Fajardo M, Estébanez-Montiela B, et al. Anew thoracic interfascialplane block as anesthesia fordifficultweaning due to ribcagepain in critically ill patients. Med Inten-
Please cite this article in press as: de la Torre PA,thoracic interfacial ultrasound block --- a cadaveric andhttp://dx.doi.org/10.1016/j.bjane.2015.04.007
siva. 2013:26.18. Andreae MH, Andreae DA. Local anaesthetics and regional
anaesthesia for preventing chronic pain after surgery. CochraneDatabase Syst Rev. 2012;10:CD007105.
3
PRESS9
9. Campbell I, Cavanagh S, Creighton J, et al. To infiltrate or not?Acute effects of local anaesthetic in breast surgery. ANZ J Surg.2014.
0. Sidiropoulou T, Buonomo O, Fabbi E, et al. A prospective com-parison of continuous wound infiltration with ropivacaine versussingle-injection paravertebral block after modified radical mas-tectomy. Anesth Analg. 2008;106:997---1001 [table of contents].
1. Rawlani V, Kryger ZB, Lu L, et al. A local anesthetic pumpreduces postoperative pain and narcotic and antiemetic use inbreast reconstruction surgery: a randomized controlled trial.Plast Reconst Surg. 2008;122:39---52.
2. Scott SR. Patient outcomes after axillary lymph node dissec-tion for breast cancer: use of postoperative continuous localanesthesia infusion. J Surg Res. 2006;134:124---32.
3. Blanco R, Parras T, McDonnell JG, et al. Serratus plane block: anovel ultrasound-guided thoracic wall nerve block. Anaesthesia.2013;68:1107---13.
4. de la Torre PA, Garcia PD, Alvarez SL, et al. A novel ultrasound-guided block: a promising alternative for breast analgesia. AesthSurg J Am Soc Aesth Plast Surg. 2014;34:198---200.
5. Wahba SS, Kamal SM. Thoracic paravertebral block versus pec-toral nerve block for analgesia after breast surgery. Egypt JAnaesth. 2014;30:129---35.
6. Thavaneswaran P, Rudkin GE, Cooter RD, et al. Brief reports:paravertebral block for anesthesia: a systematic review. AnesthAnalg. 2010;110:1740---4.
7. Chang YC, Liu CL, Chen MJ, et al. Local anestheticsinduce apoptosis in human breast tumor cells. Anesth Analg.2014;118:116---24.
8. Chiu M, Bryson GL, Lui A, et al. Reducing persistent postop-erative pain and disability 1 year after breast cancer surgery:a randomized, controlled trial comparing thoracic paraverte-bral block to local anesthetic infiltration. Ann Surg Oncol.2014;21:795---801.
9. Wijayasinghe N, Andersen KG, Kehlet H. Neural blockade forpersistent pain after breast cancer surgery. Reg Anesth PainMed. 2014;39:272---8.
0. Cho AR, Kwon JY, Kim KH, et al. The effects of anesthet-ics on chronic pain after breast cancer surgery. Anesth Analg.2013;116:685---93.
1. Melamed R, Bar-Yosef S, Shakhar G, et al. Suppression of nat-ural killer cell activity and promotion of tumor metastasisby ketamine, thiopental, and halothane, but not by propo-fol: mediating mechanisms and prophylactic measures. AnesthAnalg. 2003:1331---9.
2. Heaney A, Buggy DJ. Can anaesthetic and analgesic techniquesaffect cancer recurrence or metastasis? Br J Anaesth. 2012;109Suppl. 1:i17---28.
3. Exadaktylos AK, Buggy DJ, Moriarty DC, et al. Can anesthetic
et al. Axillary local anesthetic spread after the radiological evaluation. Rev Bras Anestesiol. 2016.
or metastasis? Anesthesiology. 2006;105:660---4.4. Barr K. Serratus plane block --- is a high volume of local anaes-
thetic needed? Anaesthesia. 2014;69:192---3.