nihr clahrc east midlands annual meeting 2015 presentations - day 2
TRANSCRIPT

WelcomeNIHR CLAHRC East Midlands Annual Meeting
Partners in Progress – Sharing and Learning
A partnership between
Nottinghamshire Healthcare NHS Foundation Trust
and the Universities of Nottingham and Leicester
25 March 2015, Eastwood Hall Hotel, Nottingham
NIHR CLAHRC for EM Annual Meeting –
Welcome and Introduction
Kamlesh Khunti, Director, CLAHRC East Midlands
A partnership between
Nottinghamshire Healthcare NHS Foundation Trust
and the Universities of Nottingham and Leicester
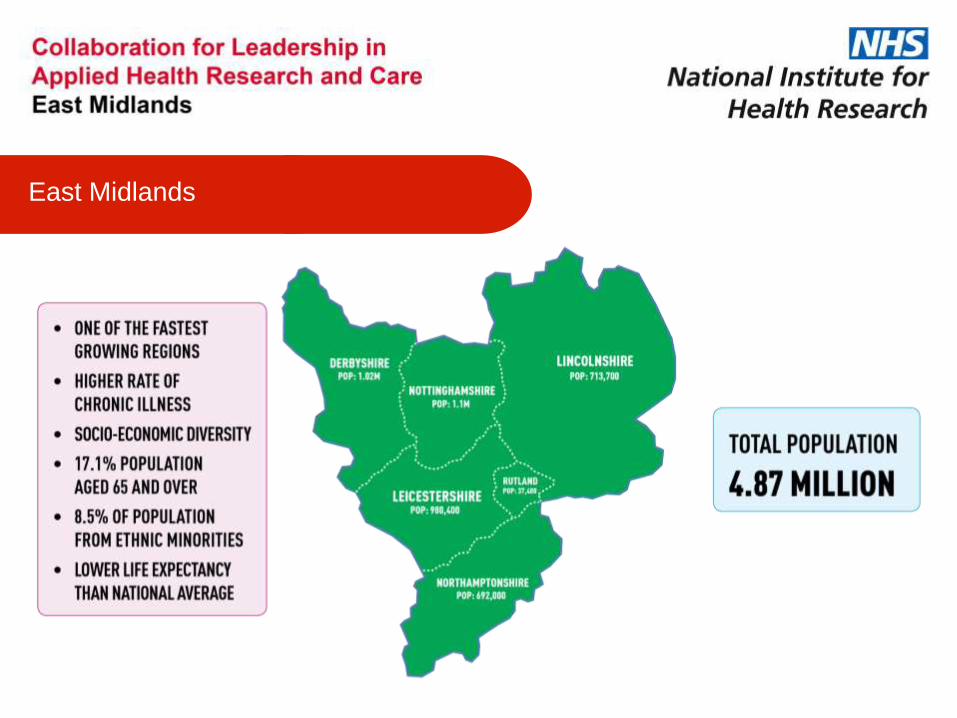
East Midlands

NHS Outcomes Framework 5 Domains
Public Health England Priorities
Department of Health Priorities for the East Midlands (Set out in the East Midlands Health Strategy 2009)
“The priorities for the East Midlands are to address health inequalities, levels of tobacco use, harmful alcohol use, obesity, physical activity, avoidable injury and death, affordable warmth and the health of children and young people.”
Key National and Local Priorities
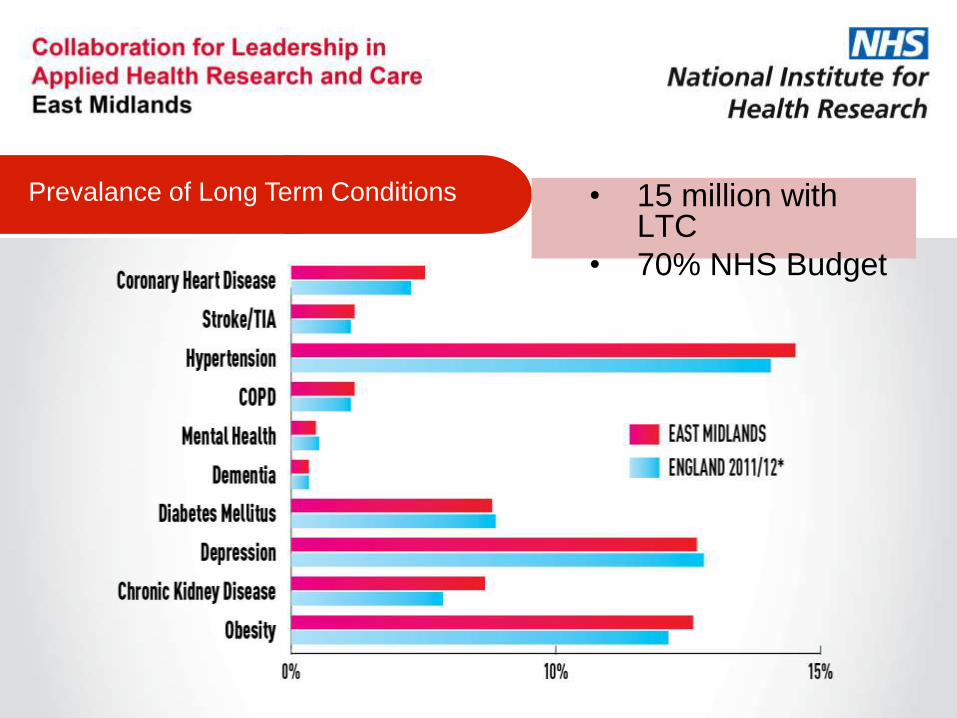
Prevalance of Long Term Conditions • 15 million with LTC
• 70% NHS Budget
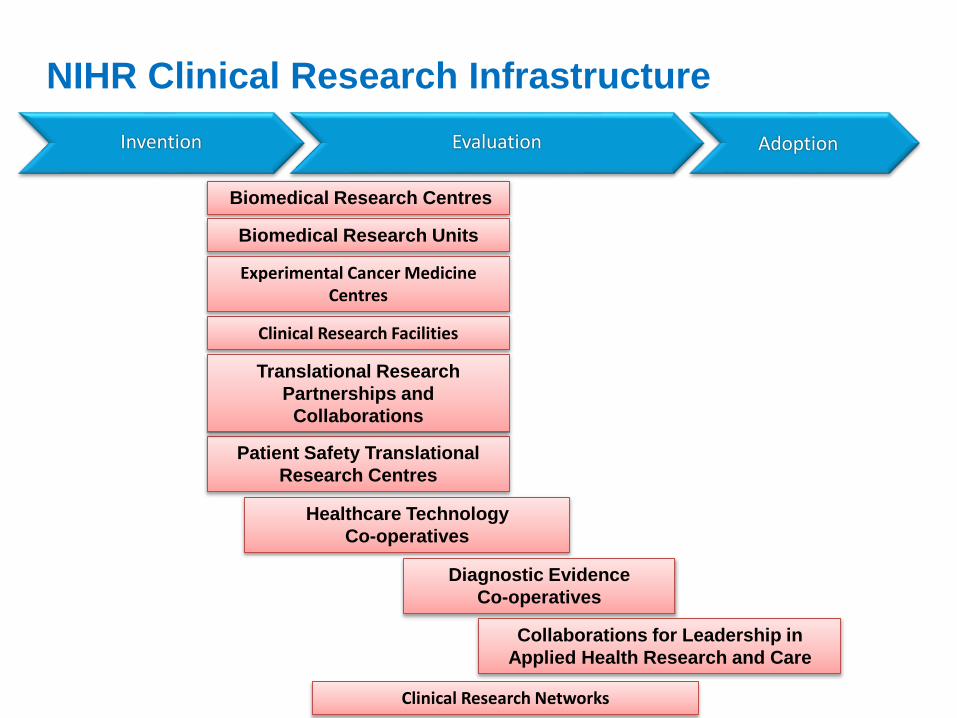
NIHR Clinical Research Infrastructure
Biomedical Research Centres
Biomedical Research Units
Clinical Research Facilities
Experimental Cancer Medicine Centres
Clinical Research Networks
Invention Evaluation Adoption
Healthcare Technology
Co-operatives
Diagnostic Evidence
Co-operatives
Patient Safety Translational
Research Centres
Collaborations for Leadership in
Applied Health Research and Care
Translational Research
Partnerships and
Collaborations

NIHR Collaborations for Leadership in Applied Health Research and Care
• 9 Pilot CLAHRCs created in 2008 for 5 years
• £50m funding awarded (rising to £88m over course of award)
• Second competition: 13 CLAHRCs funded for 5 years from January 2014
• Funding increased to £124 million
• Address the “second translational gap”

North West London
Greater
Manchester
West Midlands
South WestPeninsula
Yorkshire & Humber
13 NEW Collaborations from January 2014
East of England
NIHR Centres for Leadership in Applied Health Research and Care (CLAHRCs)
East Midlands
South London
North West Coast
North Thames
Oxford
West Country
Wessex
Pilot scheme to 2014

Contributions from Matched Funding

NIHR CLAHRC East Midlands
Structure

NIHR CLAHRC EM
Vision and Mission
Create an International
Centre for Excellence
Deliver a Large Volume of High Quality Applied Health Research
Build Strength and Capacity to
Implement World Class Research

NIHR CLAHRC EM
Partnership Vision
Partnerships are at the Centre of Everything we do!

NIHR CLAHRC EM
Partner Commitments
• Improve patient outcomes through the conduct and application of research evidence of local relevance and international quality
• Bring together health providers, commissioners, patient groups, health and research networks, life science industries and academic institutions to support the NHS Increase capacity in the EM to conduct high quality health research

Partnership Wheel
“Improve patient outcomes through the conduct and
application of research evidence of local relevance and international quality”
Applied Health Research
Year One
• 18 Phase One and Two projects are up and running across the East Midlands.
• 10 Projects provisionally selected for Phase Three from an rigorous approach involving Partners and Public

Bringing People Together
Year One
• Received £591k in matched cash funding
• On track to receive £18m in overall matched funding
• Set up the East Midlands CLAHRC faculty. We currently have 90 members.
• PARADES Event in December 2014 with the EM AHSN #StephenFryLiked
“Build on the achievements of the LNR and NDL CLAHRCs in
bringing together stake holders to support the NHS to meet locally identified priorities”

“Bring about a further step change in the quality and
quantity of activity taking place to bridge the second gap in
translation”
Implementing Evidence
Year One
• EM AHSN have pledged funding of £525,000 to support the implementation of CLAHRC EM projects.
• We have appointed 34
knowledge brokers who are
playing a key role in developing
research interest and capability
We said we’d: “Increase capacity in the EM to conduct
high quality health research and to apply research evidence”
Capacity Development
Year One
• We have appointed seven PhD students and three more planned in September
• Commenced our training programme presenting short courses for NHS staff in 2015. Courses were put forward after consultation with NHS partners.

Year One
• PPI strategy completed and being implemented.
• Partners Council set up and meeting regularly.
• Set up the Centre for BME Health. The Centre has already delivered 11 community health information events to raise awareness of diabetes and safer fasting during Ramadan to more than 250 individuals from 13 different ethnic groups.
Public Involvement
“Provide opportunities for stakeholder engagement and across
all of its structures, themes and projects so that intended end-users
of research can help to shape its selection, design, delivery,
dissemination and implementation”

• Overview of our progress including
achievements
• Give a wider perspective on the
relationship between our partners
• Outline our chanllenges
• Encourage networking
• To thank you for all that you have
done in the last year. We could
not have achieved this without
your support!
Aims and Objectives of Today

Mission Statement

Thank you for listening and
Enjoy the Day
www.clahrc-em.nihr.ac.uk
@kamleshkhunti
@CLAHRC_EM
This research was funded by the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care East Midlands (NIHR CLAHRC EM). The views expressed in this presentation are those of
the speaker(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
NIHR CLAHRC East Midlands Annual Meeting
Partners in Progress – Sharing and Learning
A partnership between
Nottinghamshire Healthcare NHS Foundation Trust
and the Universities of Nottingham and Leicester

CLAHRC EM Annual Meeting 25th
March 2015
Partners in Progress:
Sharing & Learning
Professor Rachel Munton
Managing Director, EMAHSN

“There is a clear relationship between the
EM CLAHRC and EM AHSN, with the
CLAHRC resources supporting the
generation of high quality and locally
relevant evidence and developing the
science of implementation and the AHSN
supporting the practicalities of “putting
evidence into practice” at a suitable
stage of development.”

Creation
• new things
• new ideas
• new techniques
• new approaches
Assessment
• new things
• new ideas
• new techniques
• new approaches
Uptake
• new things
• new ideas
• new techniques
• new approaches
Spread
• new things
• new ideas
• new techniques
• new approaches
Basic ResearchApplied
ResearchCommissioning Patient Care
• Better Quality
• Better Value
•Health and Wealth
NIHRNHS
CommissionersMRC & others incl Charities
Providers of NHS services
Working across the Innovation Pathway
INVENTION EVALUATION ADOPTION DIFFUSION

7.9% employment rate for people with serious mental health
conditions
Work leads to better mental health, physical health and
economic well-being
IPS consistently more effective than other approaches at getting
people into work: 61% IPS vs 23% Traditional
IPS reduces health service use: fewer days in hospital, reduced
rates of readmission (Hoffman, 2014)
Economic studies estimate £1.59 saving for every £1 spent
(Van Stolk, 2014)
Individual Placement & Support
“We felt that it was very important to get back into full time work, where I was before I had my depression.” - IPS Service User

EMAHSN IPS Project Impacts
More people with severe mental illness will be offered evidenced best
practice employment support as part of their recovery plan
NHS providers will be afforded expert support and facilitation leading to
increased fidelity of IPS services available to patients
NHS providers will be given the means to ensure that these
improvements are sustained far beyond the life of this project
IPS practitioners will have a regional network of peers in order to share
best practice and access support
“Even though I live with a diagnosis of schizophrenia, with support I have achieved a sense of satisfaction in my job. Over time I have developed insight into my illness, which has helped my recovery and reduced the symptoms.” - IPS Service User


A £2m NIHR Research Programme constituting 5 research studies:
The event and dissemination activities look to spread best practice as
outputs from the programme and how they have influenced new NICE
guidelines on bipolar disorder (released 24th September
http://www.nice.org.uk/Guidance/CG185)
Better Care for People
with Bipolar Disorder:
.

PARADES Event & Booklet
Event jointly hosted by CLAHRC EM and EMAHSN to:
• Launch the Advance Planning guide
• Communicate PARADES research findings to participants, service
users and healthcare professionals
• Showcase new NICE Guideline on Bipolar Disorder
Advance Planning guide received support from Stephen Fry, Nick
Clegg MP and Nicky Morgan MP – nearly 20,000 downloads from
EMAHSN website to date + 4000 distributed
EMAHSN now supporting Nottingham Recovery College in the delivery
of specialist educational provision on Advance Planning directly to
service users with a view to expanding to other Recovery Colleges in
the region in 2015/16

EMAHSN:
Transforming the health of
4.5m East Midlands
residents and stimulating
wealth creation
Name: Rachel Munton
Phone: 0115 8231300
Email: [email protected]
www.emahsn.org.uk
@EM_AHSN
@RachelMunton

NIHR CLAHRC East Midlands Annual Meeting
Partners in Progress – Sharing and Learning
A partnership between
Nottinghamshire Healthcare NHS Foundation Trust
and the Universities of Nottingham and Leicester
NIHR CLAHRC East Midlands Annual Meeting –
Building Partnerships
Chair: Professor Richard Morriss, Director of Research
A partnership between
Nottinghamshire Healthcare NHS Foundation Trust
and the Universities of Nottingham and Leicester

‘Building Partnerships’
Karen Glover
Director of Partner Relations and Operations,
NIHR CLAHRC EM
Head of Clinical Programmes EM AHSN
A partnership between
Nottinghamshire Healthcare and the
Universities of Nottingham and Leicester

• NHS, Industry, Academia
• Voluntary Sector and Local Authorities
• Patients/Public
• Region-wide: BRU, CRN, SCN, Clinical Senate,
HEEM, EMLA, AHSN
• National NIHR CLAHRC
Who are our Partners?
• Improve Population Health
• Increase Capacity and Capability for Research
and Innovation
• Shared Understanding and Ownership
• Translation of Research into Practice
Why Collaborate?
• Communications
• Networks
• Events
• Organisational Presentations - NHS, Academia
• Industry
How Do We Engage?

• Governance Arrangements
• Project Selection
• CLAHRC Faculty
• Networks of Practice
• Knowledge Brokers
How Do We Engage?

Thank you for listening
www.clahrc-em.nihr.ac.uk
@CLAHRC_EM
This research was funded by the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care East Midlands (NIHR CLAHRC EM). The views expressed in this presentation are those of
the speaker(s) and not necessarily those of the NHS, the NIHR or the Department of Health.

NIHR CLAHRC East Midlands Annual Meeting
Partners in Progress – Sharing and Learning
A partnership between
Nottinghamshire Healthcare NHS Foundation Trust
and the Universities of Nottingham and Leicester

BUILDING PARTNERSHIPS
PROFESSOR AZHAR FAROOQIChair – Leicester City CCG

44
Leicester – one of the UK’s most richly diverse cities.
The resting place of Cardinals and Kings
Where all ethnic groups are a minority.


On average city residents live 4 years less than those in the county
• In some areas of the city the life expectancy gap rises to 10 years
• While life expectancy is improving, the gap with the rest of England is
widening
Understanding the reasons for the gap…

Deprivation and Ethnicity- ‘A Culturally Rich but Economically Deprived City’
Directorate of Public Health and Health Improvement
NHS Leicester City 4
WHAT IS KNOWN:• 75% of Leicester’s population live in the 40% most
deprived areas nationally, with nearly half living in the 20% most deprived areas.• An estimated 25,625 children in the city live in poverty• Leicester has a high proportion of black and minority
ethnic (BME) population (36%), primarily in the east of the city; the west of the city has a predominantly white
population• The majority of BME population is of Indian descent (26%)
IMPLICATIONS:
• Ethnicity and deprivation are strong independent factors causing health inequality in population, both point to high CVD
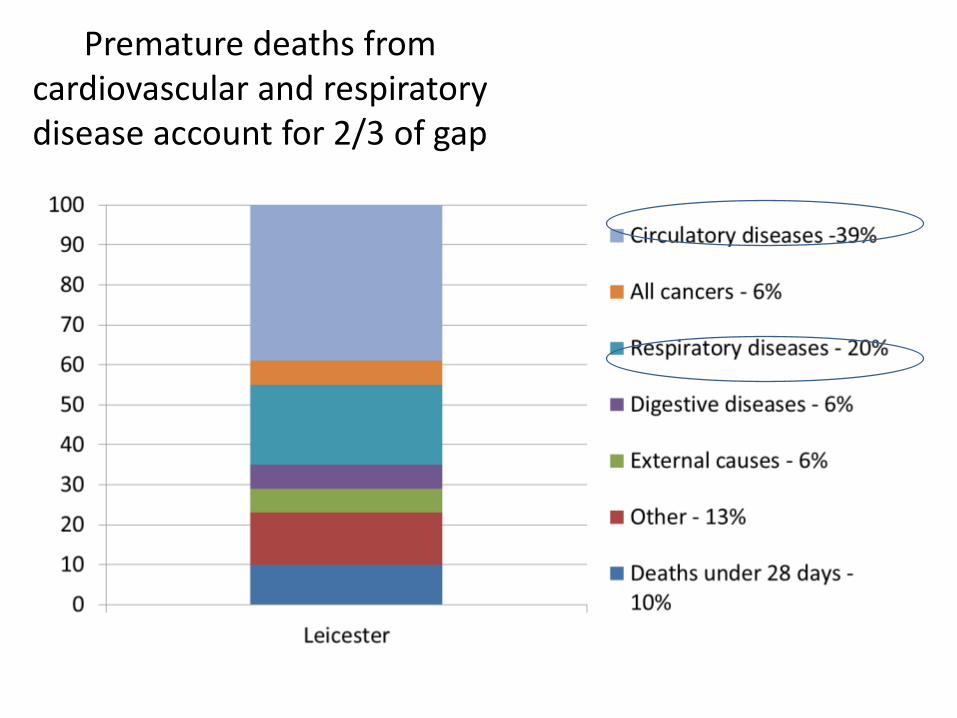
Premature deaths from cardiovascular and respiratory disease account for 2/3 of gap
Priorities
49
Our five year plan, focusing on things that…
• would do most to improve health and wellbeing;
• have biggest impact on closing the life expectancy gap;
• affect the largest numbers of patients;
• place heaviest demand on services;
• fit with what patients and partners told us should be a
priority.

Smoking prevalence is high, particularly in the west of the city

High levels of adult obesity, again concentrated in west of
the city
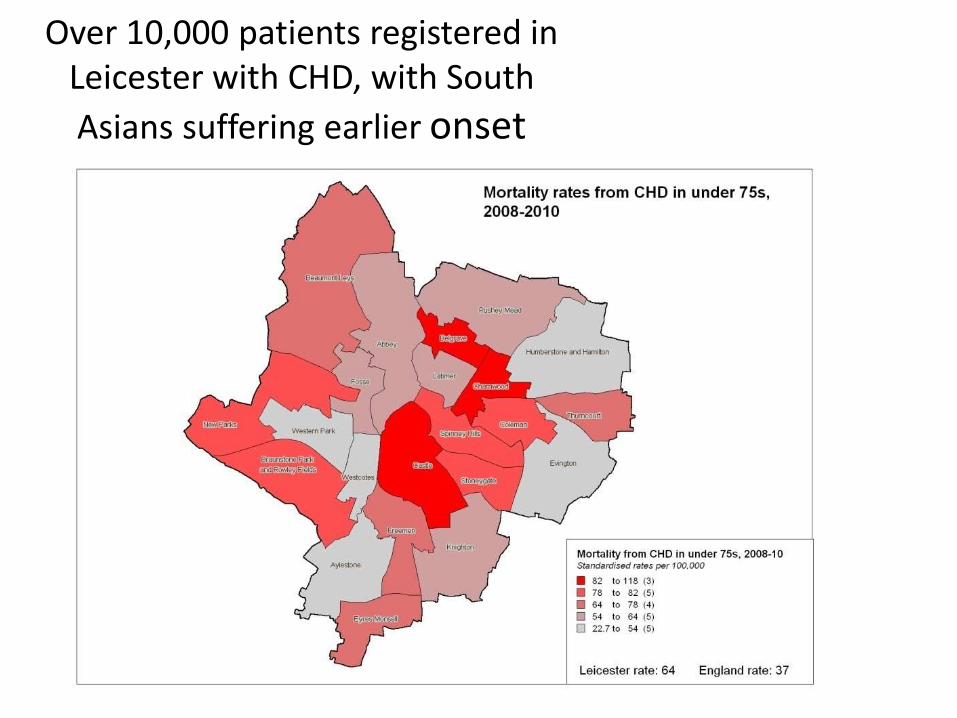
Over 10,000 patients registered in Leicester with CHD, with South
Asians suffering earlier onset

Diabetes prevalence higher than national average, particularly in areas where BME
population is high
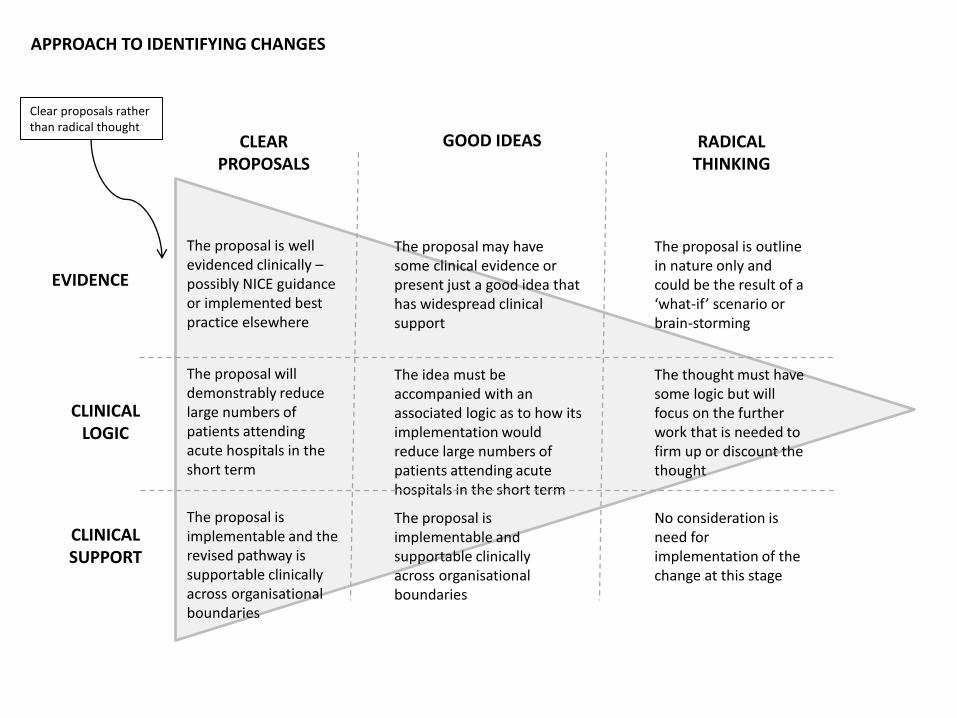
APPROACH TO IDENTIFYING CHANGES
CLEAR PROPOSALS
GOOD IDEAS RADICAL THINKING
The proposal is well evidenced clinically –possibly NICE guidance or implemented best practice elsewhere
The proposal will demonstrably reduce large numbers of patients attending acute hospitals in the short term
The proposal is implementable and the revised pathway is supportable clinically across organisational boundaries
The proposal may have some clinical evidence or present just a good idea that has widespread clinical support
The idea must be accompanied with an associated logic as to how its implementation would reduce large numbers of patients attending acute hospitals in the short term
The proposal is implementable and supportable clinically across organisational boundaries
The proposal is outline in nature only and could be the result of a ‘what-if’ scenario or brain-storming
The thought must have some logic but will focus on the further work that is needed to firm up or discount the thought
No consideration is need for implementation of the change at this stage
EVIDENCE
CLINICAL LOGIC
CLINICAL SUPPORT
Clear proposals rather than radical thought

Priorities: CVD
1. Identify the unidentified and those at risk of CVD
– Systematic, high quality health check programme which is accessible, quality assured, and leads on to management and prevention
2. Transformation of pathways – appropriate left shift
– Services should be where they are most accessible, good quality, where they deliver services effectively and cost effectively
– Concentrate on 3 or 4 big areas – already working on transforming diabetes, atrial fibrillation and anti coagulation, heart failure, CHD pathways
– They will reduce admissions and dependency on hospital based care and improve overall quality
– Challenge– resources have to follow services
3. Invest to save – up skilling, particularly in primary care
– IT that works across whole pathway
– Need sufficient workforce, in the right areas. Could be partly about moving staff (i.e. from hospital to community) but also identifying gaps and workforce planning so the programme can be delivered properly
55
Three work programmes have been identified for PID development:
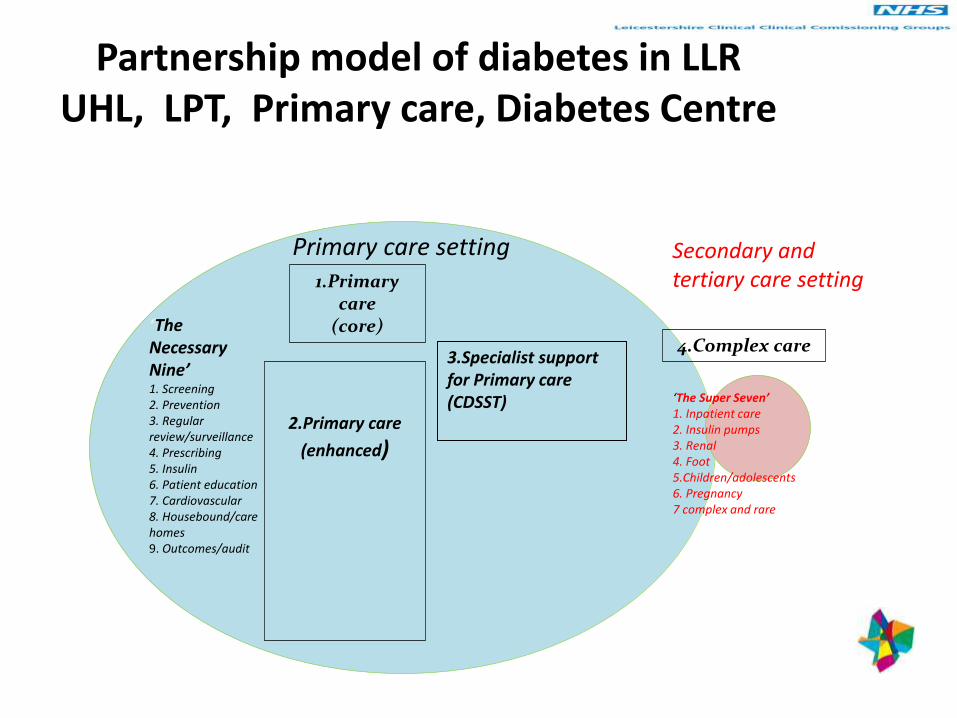
Partnership model of diabetes in LLRUHL, LPT, Primary care, Diabetes Centre
1.Primary care
(core)
2.Primary care
(enhanced)
Primary care setting Secondary and tertiary care setting
‘The Super Seven’1. Inpatient care2. Insulin pumps3. Renal4. Foot5.Children/adolescents6. Pregnancy7 complex and rare
3.Specialist support for Primary care (CDSST)
‘The Necessary Nine’1. Screening2. Prevention3. Regular review/surveillance4. Prescribing5. Insulin6. Patient education7. Cardiovascular8. Housebound/care homes9. Outcomes/audit
4.Complex care

Ensuring practices have the skills required for providing diabetes care – in city £300,000 x 3 years investment. Each practice has a PDP for diabetes
• Post graduate certificate• Regular updates• Case reviews
• Msc Diabetes• Case reviews & management• Journal club• Regular updates• Behaviour change training
• Mini modules
• Mentorship
• Healthcare Assistant training
• Patient education
• Mini modules
• CPD accredited training
• Insulin training
• Nursing home Community
Nurse support
• Mentorship

Cardiovascular disease
59
• 40,000+ residents have
received a health check;
• 4,000+ people are now
receiving care and
support.
• CLAHRC involved in
evaluation
• patients admitted to
hospital with suspected
strokes and irregular
heartbeats fell in
2013/14;
• emergency stroke
admissions reduced by
5.1% and atrial fibrillation
emergency admissions
by 16.7%.
Diabetes Atrial fibrillation40-74 health checks
• self-management
education programmes;
• Enhanced primary care
• Professional development
• better hospital care
• Better community
engagement-
collaboration with EM
Centre for BME health.
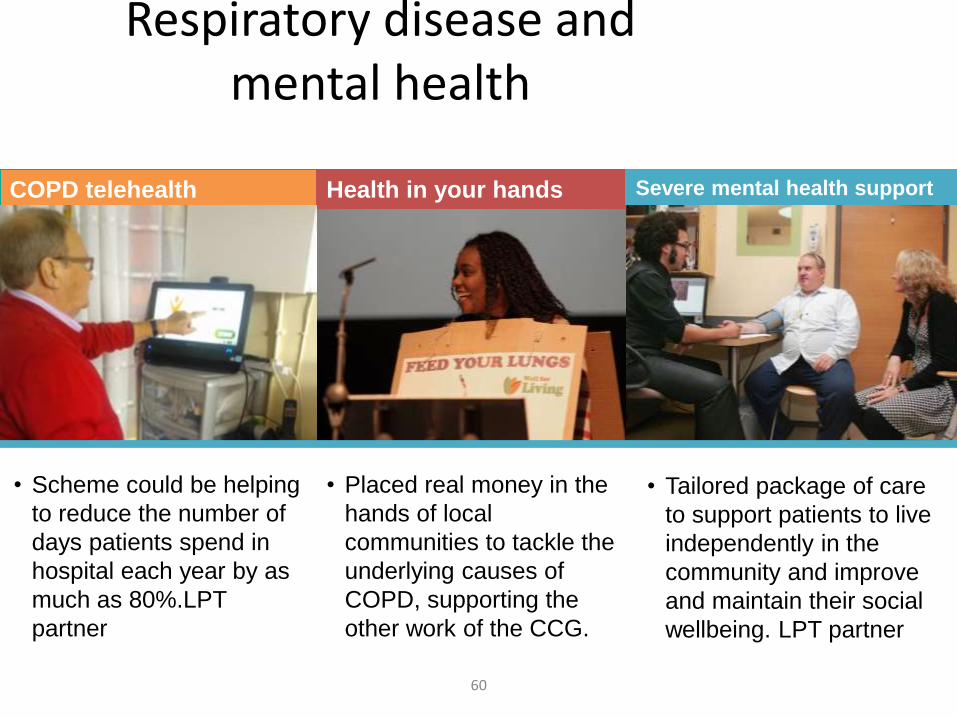
Respiratory disease and mental health
60
COPD telehealth Health in your hands
• Scheme could be helping
to reduce the number of
days patients spend in
hospital each year by as
much as 80%.LPT
partner
• Placed real money in the
hands of local
communities to tackle the
underlying causes of
COPD, supporting the
other work of the CCG.
Severe mental health support
• Tailored package of care
to support patients to live
independently in the
community and improve
and maintain their social
wellbeing. LPT partner
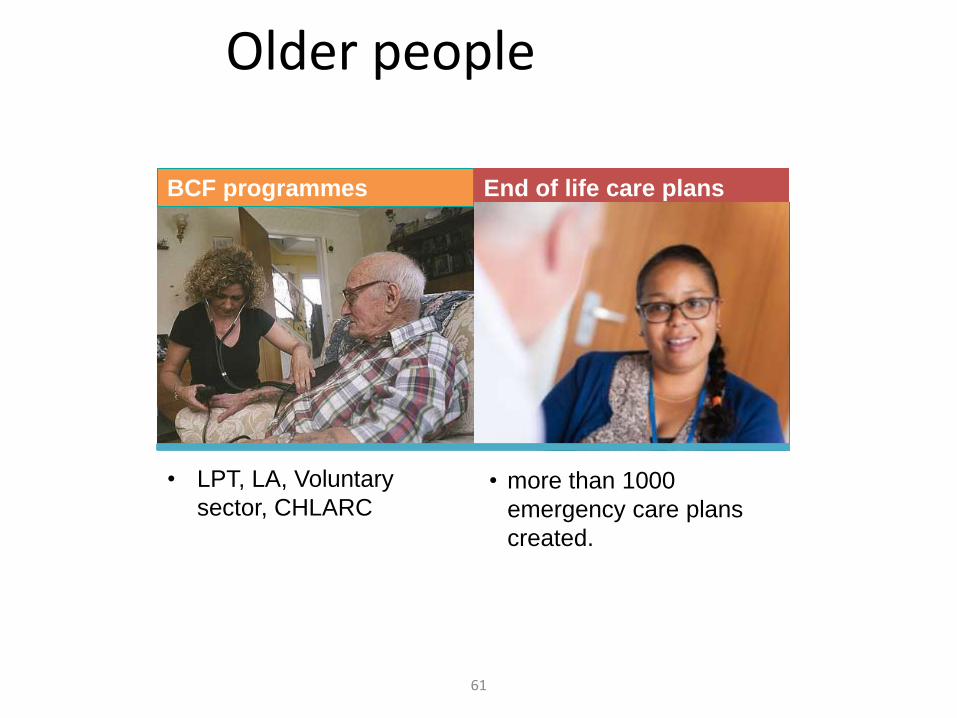
Older people
61
BCF programmes End of life care plans
• LPT, LA, Voluntary
sector, CHLARC• more than 1000
emergency care plans
created.

The Leicester City Integrated Care model- part of BTC
62
10 Joint Planned Intervention Teams
offering:
Community nursing services
LA planned services
Community Geriatrics
Care navigator per locality
Current LA offer across 12 teams
Integrated Crisis Response Service
Assistive technologies/Community equipment
Health and social care coordinators
Single Point of Contact
Emergency Duty Team
Adult mental health practitioners
Unscheduled Care Team offering:
RIT
ICRS
Night nursing
ICS
Community Geriatrics
H@H
EDT
Current community health offer across teams:
Rapid Intervention Team
Community nursing
24 virtual ICS capacity
Hospital at home
Therapy
Night nursing
Single point of Access/EDT
Up to 3 GP/ANP led ambulatory care teams offering:
Interventions targeted to high risk population
Range of diagnostics (except x-ray) to assess
and stabilise patient
Co-located with Non-elective Team above
Current ambulatory care offer across 4 localities:
GP service (24/7)
GP in a Car
Emergency Response Service
Various next day clinics
Live warm transfer capability between SPA & SPOC Access to a further 6 specialist step up/down virtual ICS beds
Inflow referral
points from
EMAS/111/
GP/SPA/SPOC
Outflow referral
points from
inpatient
beds/ED/GP/
SPA/SPOC

We cannot succeed without partnerships
• Engage- identify common problems and devise solutions
• Learning from other’s success
• Evaluate- role of universities, CLARHC
• improve
• Disseminate
• Thank You for Listening
NIHR CLAHRC East Midlands Annual Meeting
Partners in Progress – Sharing and Learning
A partnership between
Nottinghamshire Healthcare NHS Foundation Trust
and the Universities of Nottingham and Leicester
Dr Peter Miller
Chief Executive
Leicestershire Partnership Trust
Building Partnerships

We have a problem
Su
rplu
s / D
efi
cit
(£
m)
Long Term Conditions
‘Without unprecedented, sustained increases in health service productivity, including more effective management of chronic conditions, funding for the NHS in England will need to increase in real terms between 2015/16 and 2021/22 to avoid cuts to the service or a fall in quality’
Innovation and Translation

The Heineken Challenge
NHS Trust Feedback
CLAHRC EM research and implementation activities aligned to the priorities of the Trust – Long term Conditions/Mental health
Rigorous assessment of projects ensures quality
Diffusion fellows/knowledge Brokers – embedded in clinical services
Important new opportunities for clinical staff and non-clinical staff to obtain funding for translational activities to get their research findings quickly into practice – again focused on Trust priorities
World class research – recruitment and retention
New training opportunities for non-medical staff to undergo PhD training and build new cadre of research active/aware staff
Good structures in place for learning and sharing experiences across East Midlands and beyond – CLAHRC EM ‘Show and Tell Events’ for example
Allows researchers to influence nationally
Encourages researchers in to ‘think bigger’ by facilitating collaborations across the East Midlands and beyond

But more challenge
• Alignment of research to big change programmes
• Emergency admissions in LLR up 8% in 14/15
• Adopt innovation at Pace and Scale

NIHR CLAHRC East Midlands Annual Meeting –
Building Partnerships
Chair: Professor Richard Morriss, Director of Research
A partnership between
Nottinghamshire Healthcare NHS Foundation Trust
and the Universities of Nottingham and Leicester

Public Involvement in CLAHRC
East MidlandsDr Paula Wray, Public Involvement Programme Lead
A partnership between
Nottinghamshire Healthcare NHS Foundation Trust
and the Universities of Nottingham and Leicester

Why involve stakeholders?

A Whole System Approach
CLAHRC
Partners’ Council
Projects
Scientific Committee
Executive & Governance
Board
Partners
East Midlands Centre for
BME Health

Involvement, Engagement and Participation
“Being part of the Partners' Council has opened up a whole new world for
me. It's been a steep learning curve but with the support and
encouragement from colleagues I have grown in confidence. This has enabled me to gain new skills for
example as a Lay Assessor and I have already helped develop and refine a number of research proposals. It's
been so satisfying to utilise the extensive network of voluntary
groups I am involved in to help shape and inform research.”

Stakeholder views
"It is often not possible to meet our clinicians or patients face-to-face. However,our feedback from our PPI group (a family support group for ADHD) has providedthe research team with a valuable education in the need to have a flexibleapproach to communication, using the media (phone, email, text, postal letter)that is preferred for each given family. Additionally, it has been important to adaptthe implementation of our protocol to the needs and clinical practice of eachsite. By working closely with our clinicians, … we have developed a strongcommunity which is reflected in our participant and site recruitment andretention figures “ Researcher
“I am delighted to be a part of the Aqua Research Study, this is a very excitingproject to be involved in and could be revolutionary in ADHD Care, in particularthe assessment process. As a clinician, I have been an integral part of the study,the University of Nottingham and the team have ensured the engagement ofclinicians, on all levels. The help and support provided by the team has beenoverwhelming in my role as a knowledge broker.” Clinician
East Midlands Centre for Black and
Minority Ethnic Health
Health Literacy -The ability to understand, access and use health information.• Social and cognitive skills to do these tasks• Motivation and engagement in health‐promoting and disease‐management activitiesWorld Health Organization: Health Promotion Glossary. Health Promotion International 1998, 13(4):349‐364

East Midlands Centre for Black and
Minority Ethnic Health
• Capacity building programmes. • Workshop and seminar programmes
• PPI Panel to review and support funding applications
• Centralised repository of resources • Website with resources• Community facilitators, interpreters
and support • Celebration events • Community engagement
• Run health information events and workshops to share knowledge
• Training and support for individuals
Source: Out Front Minnesota

Thank you for listening
[email protected], [email protected]
www.clahrc-em.nihr.ac.uk
@CLAHRC_EM
@EMCBMEH
This research was funded by the National Institute for Health Research Collaboration for Leadership in Applied Health
Research and Care East Midlands (NIHR CLAHRC EM). The views expressed in this presentation are those of the
speaker(s) and not necessarily those of the NHS, the NIHR or the Department of Health.

NIHR CLAHRC East Midlands Annual Meeting
Partners in Progress – Sharing and Learning
A partnership between
Nottinghamshire Healthcare NHS Foundation Trust
and the Universities of Nottingham and Leicester
NIHR CLAHRC East Midlands Annual Meeting –
Getting Research Into Practice
Chair: Professor Richard Morriss, Director of Research
A partnership between
Nottinghamshire Healthcare NHS Foundation Trust
and the Universities of Nottingham and Leicester

Dr Darren ClarkChief Executive
Medilink East Midlands
Building Partnerships
with Industry
Medilink UK Network
MedilinkY&H
MedilinkNW
MedilinkWM
MediWales
MedilinkEM
BioBusinessIreland
SEHTAMedilink SW
• Federation of regional organisations
• UK’s largest healthcare representative body
(1,500 members)
• Providing sector support for two decades

Common Goal

NPDTraditional Markets
Customer need Solution
Everybody’s Happy Sell to customer
Translate into product
NPDHealthcare
Clinician
Patient
Commissioner
Who is the
customer?
Allied HC
Professional

Optima Life
Aspiration:
• To introduce Firstbeat HEALTH heart rate monitoring device into the NHS
Medilink support helped:
• Identify a cardiology unit partner
• Support initial validation study - evaluation of exercise capacity in patients with chronic heart failure
Results:
• Better understanding of NHS needs / constraints
• Medilink award for collaboration

iQudosAspiration:
• To gain regulatory approval for clinical decision support software developed in the NHS
Medilink support helped:
• Engagement with regulatory experts
• Reduce project risk
• Take software to full regulatory approval (one of the first in the country)
Results:
• New product ready for commercial role out
• Further investment secured
• Future job creation
• Digital Innovation award winners
www.iqudos.com
Biomarkers for prostate cancer
Aspiration:
• To define a panel of proteomic biomarkers to improve clinical management
Medilink support helped:
• Introduce an additional pre-clinical trial
• Maximise the use of clinical data & samples
• Interaction with local SME
Results:
• New tools for biomarker discovery
• Conference presentations
• Additional funding applications
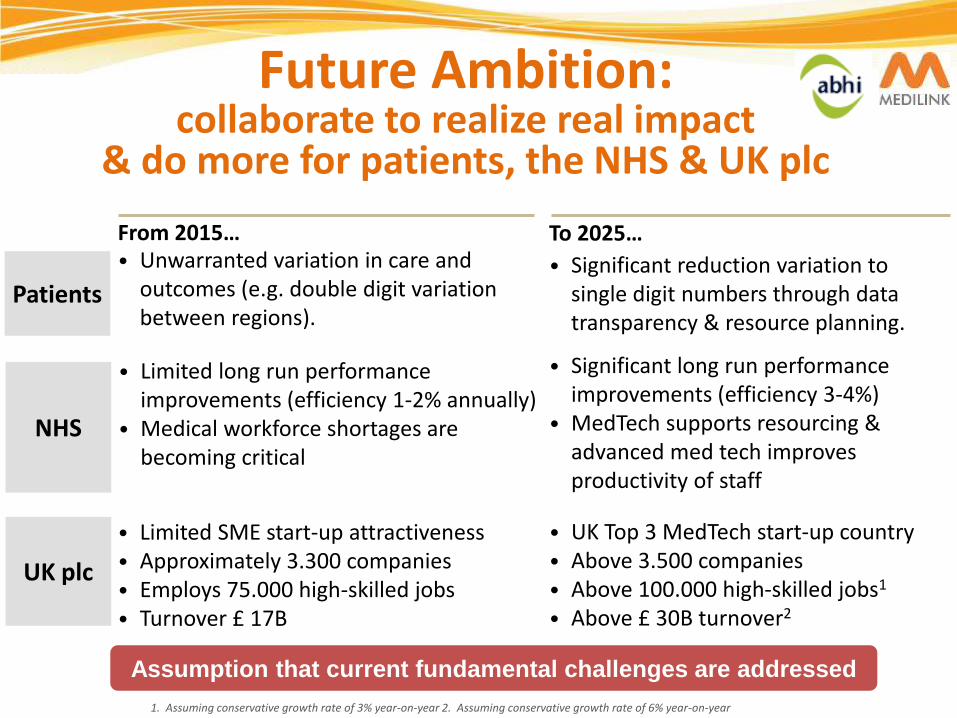
Future Ambition: collaborate to realize real impact
& do more for patients, the NHS & UK plc
To 2025…
• Significant reduction variation to single digit numbers through data transparency & resource planning.
From 2015…• Unwarranted variation in care and
outcomes (e.g. double digit variation between regions).
Patients
NHS
UK plc
• Limited long run performance improvements (efficiency 1-2% annually)
• Medical workforce shortages are becoming critical
• Significant long run performance improvements (efficiency 3-4%)
• MedTech supports resourcing & advanced med tech improves productivity of staff
• Limited SME start-up attractiveness• Approximately 3.300 companies• Employs 75.000 high-skilled jobs • Turnover £ 17B
• UK Top 3 MedTech start-up country• Above 3.500 companies• Above 100.000 high-skilled jobs1
• Above £ 30B turnover2
1. Assuming conservative growth rate of 3% year-on-year 2. Assuming conservative growth rate of 6% year-on-year
Assumption that current fundamental challenges are addressed

Further Information
Dr Darren ClarkChief Executive
Medilink East MidlandsBioCity Nottingham
Pennyfoot StreetNottingham
NG1 1GFTel: 0115 912 4330Fax: 0115 912 4331
e-mail: [email protected]: www.medilinkuk.com
www.medilinkem.com

NIHR CLAHRC East Midlands Annual Meeting
Partners in Progress – Sharing and Learning
A partnership between
Nottinghamshire Healthcare NHS Foundation Trust
and the Universities of Nottingham and Leicester

Qbtech and East Midlands CLAHRC
Illustrated benefits of partnership
Tony Doyle
Managing Director Qbtech Ltd

Touch points
• Some context
• Better design
• Better delivery
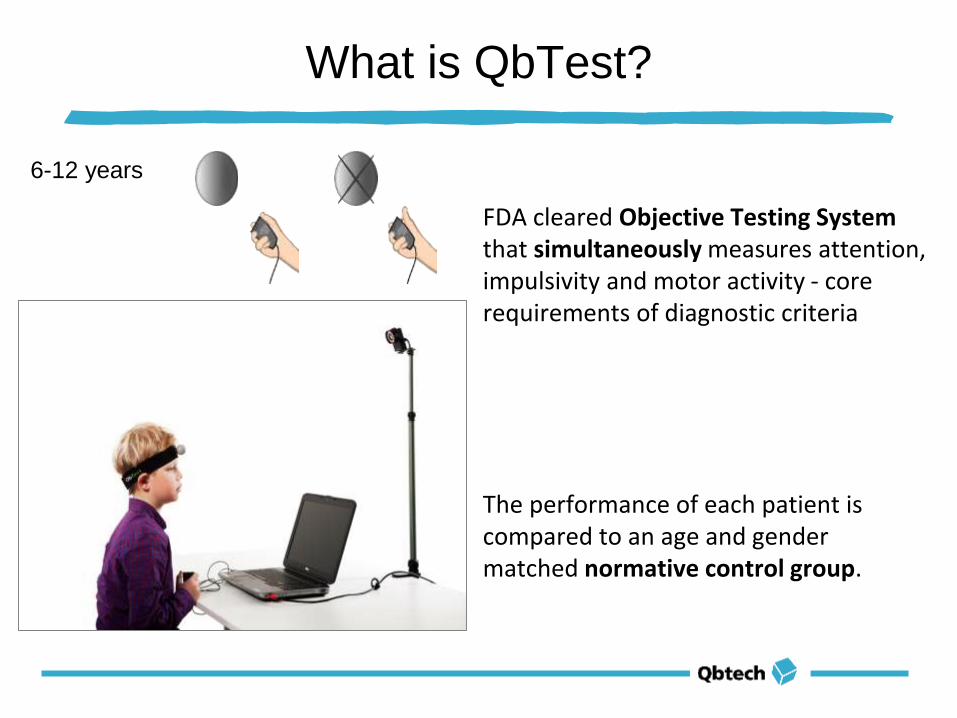
What is QbTest?
FDA cleared Objective Testing Systemthat simultaneously measures attention, impulsivity and motor activity - core requirements of diagnostic criteria
The performance of each patient is compared to an age and gender matched normative control group.
6-12 years

12 countries
8 languages
More than 180 000 patients tested
Over 5 000 tests performed in the UK across >50 clinics in 2014
Cleared by FDA and registered by EMA
But..... we have a long way to go
QbTest - A Better View of ADHD
Qbtech and QbTest
QbTest
Touch points
• Some context
• Better design
• Better delivery

Better design
• Clinical audit data to inform the study from Qbtech
• Iteration of primary and secondary end points and design with experts from Nottingham
- Does providing feedback from QbTest lead to:
• earlier correct diagnosis?
• earlier optimisation of treatment?
• improved patient outcomes?
• A more relevant and potentially impactful study

Touch points
• Some context
• Better design
• Better delivery

Expertise from the Nottingham University Study team led by Professor Chris Hollis, Lead researcher Dr Charlotte Hall
Joint site recruitment effort
Real time data and weekly monitoring from Qbtech
Weekly contact with Site PIs by the Nottingham team
Monthly joint teleconferences and quarterly forums
Touch points
• Some context
• Better design
• Better delivery
• Stronger team
NIHR CLAHRC East Midlands Annual Meeting
Partners in Progress – Sharing and Learning
A partnership between
Nottinghamshire Healthcare NHS Foundation Trust
and the Universities of Nottingham and Leicester

What are the benefits of Higher Education Institutions working with CLAHRC-EM?
Dr Lauren Sherar
Senior Lecturer Physical Activity and Public Health Research Group
Academic lead for the BHF National Centre for Physical Activity and Health
School of Sport, Exercise & Health Sciences, Loughborough University, UK
The aim of my research
Create evidence that can be used to leverage
changes to policies and practices to improve
physical activity opportunities for children and
youth
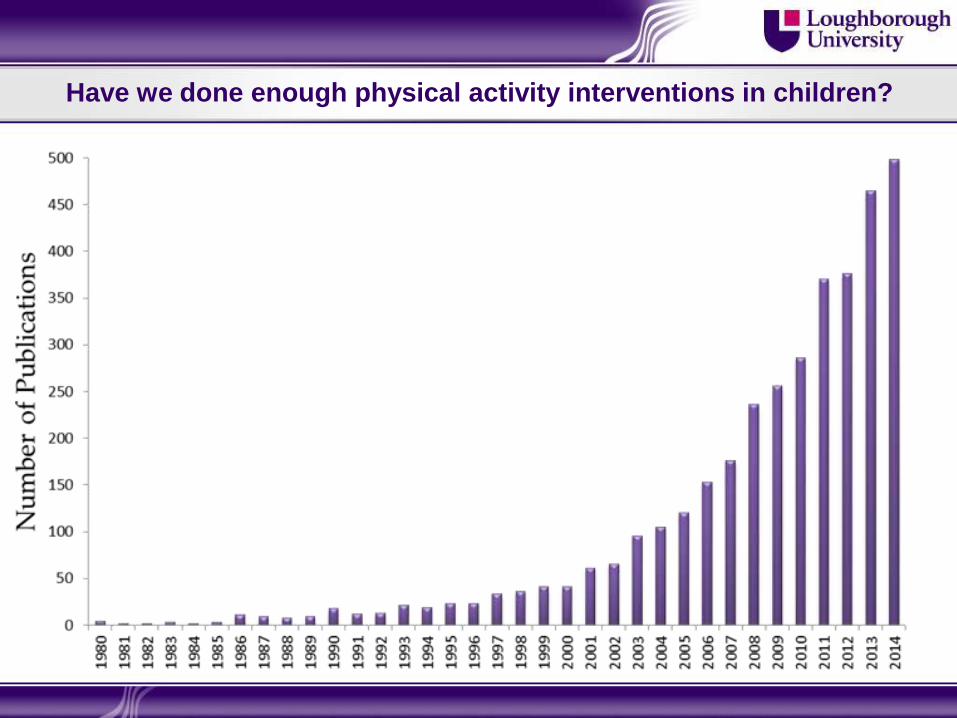
Have we done enough physical activity interventions in children?

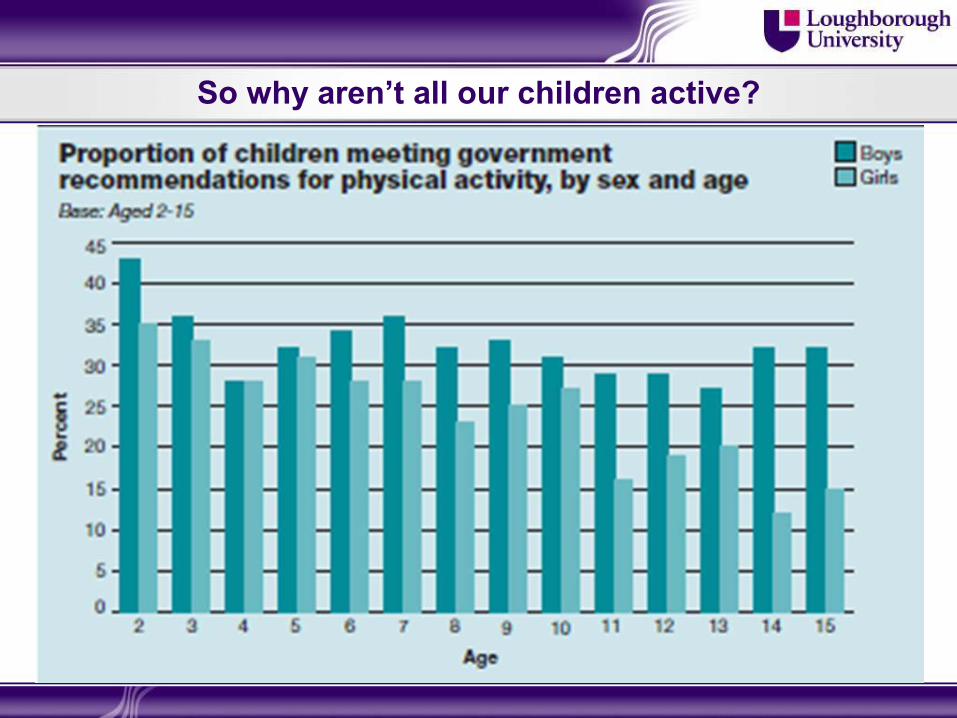
So why aren’t all our children active?
Academics likely don’t know best!

Move to Teach Project

Benefits of HEI working with CLAHRC
Getting research into practice (GRIP)
1. Co-production of research
2. Knowledge mobilisation
3. Training and support
4. Flexibility and academic concession
5. Actively encouraging industry partnership
1. Co-production of research
Forces meaningful engagement, not just simple
consultation
Wider understanding of the problem
Insights that improve the intervention
More realistic, relevant and sustainable service
Update and innovate practice
Empower users by influencing change
Provides the ‘user’ with a voice
1. Co-production of research: Move to Teach project
Teacher/parent on advisory committee
Knowledge brokers
Teacher, pupil and parent involvement in
intervention development
Pilot of intervention in schools with teacher
and pupil feedback sessions
Wide interaction with a range of stakeholders
2. Knowledge mobilisation
Tacit knowledge co-created and shared in real
time between academia and practice
Knowledge brokers (diffusion fellows), CLAHRC
associates and stakeholder network facilitate this
continual knowledge mobilisation
Not just passive transfer of knowledge through
guidelines, policy, and professional bodies
standards
3. Training and Support
Engage with and support
research team in appointment
of knowledge brokers,
formation of stakeholder
research network etc.
Quarterly progress report to
monitor and advise on
implementation activities
Provide implementing change
guide and knowledge
translation strategy
Provide training events (e.g.
Implementing Change
seminar)
4. Flexibility and academic concession
Unlike some funders CLAHRC recognises the
shift in hierarchy of evidence when conducting
implementation research
Thus, academic concession is made
Not always a need for a RCT
Not all outcomes need to be measured
CLAHRC recognise implementation is not
linear, thus allow for iterative approach to
implementation

5. Actively encourage industry partnership
Partnership with industry is essential:
To translate research into practice
Drive innovation
Speed up transfer of the best ideas into new
interventions
Encourage sustainability

5. Actively encourage industry partnership: Move to Teach project
Benefits of industry partner to the project:
In kind contribution of marketing time to help with
the development of intervention resources
Disseminate the finalised teacher resource (e.g.
web platform, training materials) through existing
social media and websites
Promote the service and/or facilitate discussions
with their wider network of stakeholders and
policy makers

Funding for implementation research: The dangling carrot for HEI
The aim of my research
Create evidence that can be used to leverage
changes to policies and practices to improve
physical activity opportunities for children and
youth
Rather than informing, I want to be part of the solution

Thank you for listening!
8 year old boy, PPI event, Nov 11 2014

NIHR CLAHRC East Midlands Annual Meeting
Partners in Progress – Sharing and Learning
A partnership between
Nottinghamshire Healthcare NHS Foundation Trust
and the Universities of Nottingham and Leicester

Cognitive Stimulation Therapy (CST)
for dementia
=> getting evidence into practice
Professor Martin Orrell
Director, Institute of Mental Health, Nottingham
Bob Woods, Aimee Spector, Elisa Aguirre, Amy Streater, Juanita Hoe, Zoe Hoare, Ian
Russell, Charlotte Gardner, Vasiliki Orgeta, Fara Hamidi, Phoung Leung, Lauren Yates

Cognitive Stimulation
• Distinguish from cognitive training and cognitive
rehabilitation (Clare & Woods, 2004)
• Cognitive stimulation:
– Targets cognitive and social function
– Has a social element – usually in a group or with a
family care-giver
– Cognitive activities do not primarily consist of practice
on specific cognitive modalities
NICE-SCIE guidance (2006) www.nice.org.uk
• People with mild/moderate
dementia of all types should be
given the opportunity to
participate in a structured
group cognitive stimulation
programme … provided by
workers with training and
supervision … irrespective of
any anti-dementia drug
received …’

CST & maintenance CST
programme

The programme
1) 14, 45 minute sessions (2 x week, 7 weeks)
2) Participants asked to give a group name
3) RO board
4) Sessions begin with warm up exercise
5) Bridging between sessions, consistency in time,
place, participants and facilitators
6) Presenting sessions in a fun and stimulating way
CST trial (Spector et al., 2003)
CST Key Principles
• Orientating people sensitively / when appropriate
• Information processing and opinion rather than factual
knowledge -> implicit learning
• Multi-sensory stimulation
• Flexible activities to cater for group’s needs and abilities
• Using reminiscence (as an aid to here-and-now)
• Building / strengthening relationships

Attrition Rate: n= 201, n=168 at follow up
Significant improvement in the primary outcome measures
cognition and quality of life
Improvement in QoL mediated by improvement in cognitive
function
Numbers needed to treat for cognition = 6similar to AChEIs
CST trial (Spector et al., 2003)
•23 centres (18 care homes and 5 day care)
•A multicentre Randomised Controlled Trial (RCT)
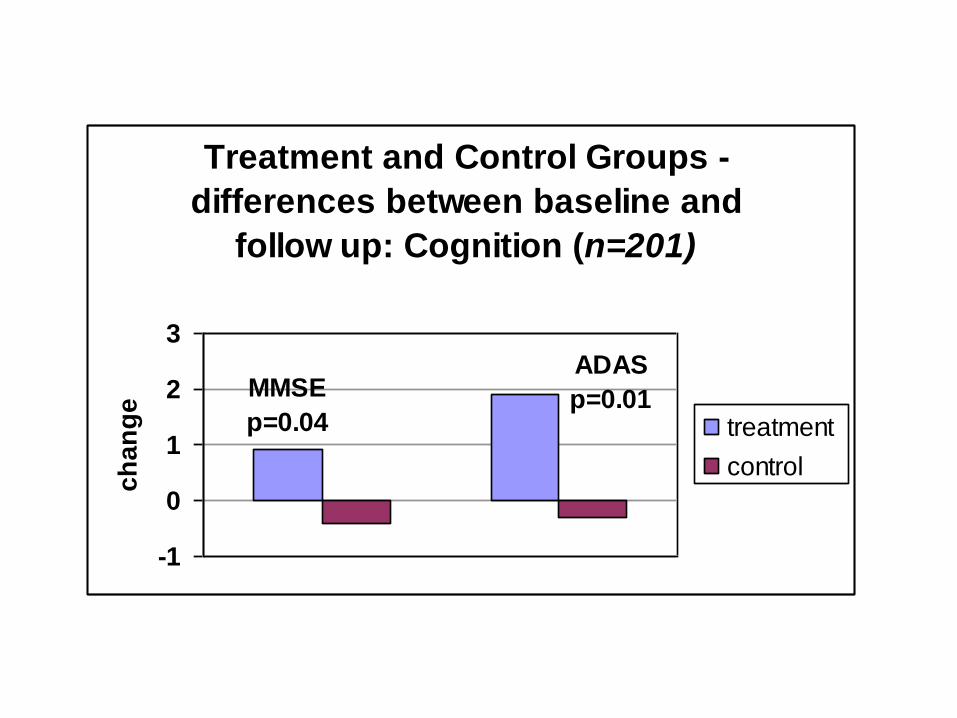
Treatment and Control Groups -
differences between baseline and
follow up: Cognition (n=201)
MMSE
p=0.04
ADAS
p=0.01
-1
0
1
2
3
ch
an
ge
treatment
control

p=0.03
-1
-0.5
0
0.5
1
1.5
1ch
an
ge
QOL
Treatment and Control Groups -differences between baseline and
follow up: Quality of Life (n=201)
treatment
control

Cost-effectiveness (Knapp et al., 2006)
CST is more cost-effective than usual activities using both
outcome measures:
• Incremental cost-effectiveness ratio: £75.32 per
additional point on MMSE (111 euros), £22.82 per point
on QoL-AD (33.2 euros)
• Donepezil had larger cost per incremental outcome gain
(AD2000, 2004)
Conclusions: Small costs outweighed by larger gains likely
that decision makers will see CST as cost-effective.
Limitations – short time span, mainly focused on people in
residential care

Cochrane Review 2012Woods, Aguirre, Orrell, Spector
• 15 trials, 407 treatment and 311 controls participants
• Length of intervention varied: 1 to 24 months
• MMSE difference at follow up = 1.74 points (Z = 5.57, p < 0.00001)
• Holden Communication Scale SMD = 0.47 (Z = 3.22, p = 0.001)
• Wellbeing/QoL SMD = 0.38 (Z = 2.76, p = 0.006)
• Depression (GDS) SMD = 0.34 (Z = 1.88, p = 0.06)
• No benefits to ADL, behaviour, or carers measures

Development of the MCST trial
programme
Maintenance CST development
• Extract features of research trials which had demonstrated
effectiveness
• New themes : Useful tips (caring from oneself, memory
tips, use of calendars, alarms) and Visual Clips from
Requena (2007) and Olazaran (2004)
• 24 sessions based on the CST and MCST pilot plus new
identified studies
• Presentation of the draft version 1 in a consensus
conference to develop draft version 2 of the manual.

Modelling the programme
9 Focus Groups
(Aguirre et al., 2010)
• 17 people with dementia, 13 staff and 18 family carers
• Inductive thematic analysis to examine user perceptions
of the Maintenance CST programme
• Mental stimulation highly valued by PWD, vital to keep
healthy and active.
• Most family carers and staff very positive towards
cognitive stimulation programmes BUT some concerns:
- When use it or lose it doesn’t apply
- Concerns about loss of confidence, anxiety, sense of inferiority.
• Positive agreement was found among 14 themes and
suggestions were made for the 5 remaining themes.
• Carers and staff rated using money and current affairs
very low - felt using money could be a sensitive topic
and current affairs was a theme people with dementia
wouldn't relate to
• In contrast people with dementia expressed a great
interest in the using money theme and in the news
Focus Groups results
(Aguirre et al., 2010)
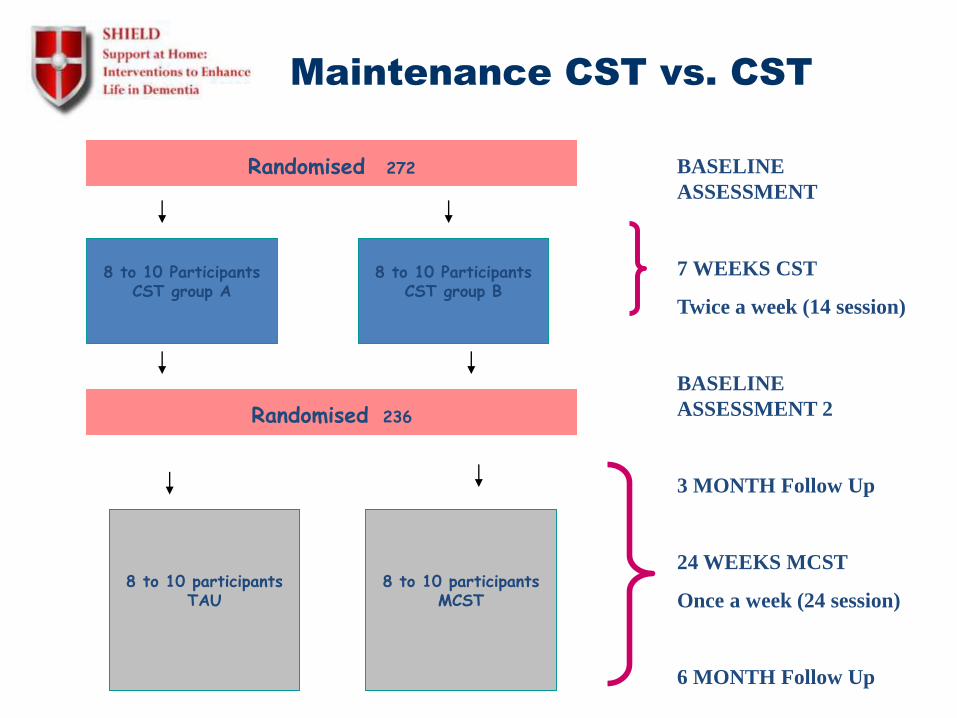
Maintenance CST vs. CST
8 to 10 ParticipantsCST group A
8 to 10 participantsTAU
Randomised 236
BASELINE
ASSESSMENT
7 WEEKS CST
Twice a week (14 session)
BASELINE
ASSESSMENT 2
3 MONTH Follow Up
24 WEEKS MCST
Once a week (24 session)
6 MONTH Follow Up
8 to 10 ParticipantsCST group B
8 to 10 participantsMCST
Randomised 272
CST Predictors of change
• 272 recruited to CST groups as first stage of
Maintenance CST Trial and 236 completed 7
weeks
• Improvement 1.09 MMSE points (p < 0.001),
ADAS-Cog 2.34 points (p< 0.001)
• Improvement 1.85 DEMQOL points (p < 0.003)
• Female gender was associated with higher
improvement
• use of ACHEIs did not alter improvement
Maintenance CST Trial –results
• 236 participants (123 MCST/123 CST only)
• After 6 months MCST
– Quality of life better QoL-AD p = 0.03
• After 3 months MCST
– Quality of life better (proxy)
DEMQOL p = 0.03, QoL-AD = 0.01
– ADCS-ADL better p = 0.04
• People on ACHEIs did significantly better on
cognition if MCST rather than on CST only

• Qualitative study of experiences of the people attending CST groups, carers & group facilitators (N=34)
• Data analysed using Framework Analysis
• Two main themes:' Positive experiences of being in the group’ & ‘Changes experienced in everyday life’
• Experience of CST seen as being emotionally positive
• Most reported some cognitive changes.
• Findings support the mechanisms of change suggested by the previous RCT of CST.
• Spector, Gardner, Orrell 2011
CST mechanisms of change

Maintenance CST implementation in practice
Amy Streater – study overview
Title STANDOUT trial MONOU trial Observational study
Aim To assess the
effectiveness of staff
training & outreach
support
To assess the
implementation in
practice of CST&
outreach support
To assess the effectiveness of
CST in practice
Participants Qualified & non qualified
dementia care staff
Qualified & non
qualified dementia
care staff
People with dementia
Expected
number
120 120 100
Actual
number
175 66 89
Resources CST manual,
maintenance CST
manual & DVD
CST manual,
maintenance CST
manual & DVD
CST manual, maintenance
CST manual & DVD
Training Yes Variable Variable
Outreach 50% 50% Variable
Assessment
schedule
Baseline, 6 & 12 months Baseline, 6 & 12
months
Before & after CST and after
maintenance CST
Outreach support queries
15 uses of outreach supporting across 35 centres raising 21 queries relating to:
group participation, inclusion criteria, practicalities, delivery of the programme, group facilitation. After CST, activity theme and general queries.
3 centres signed up to the online forum

Staff CST results
No statistically significant difference in the proportion of CST groups run in
the intervention group compared to the TAU group (p=.458).
Intervention Number of centres No CST CST programmesrun
Outreach support n (%)
35 17 (49) 18 (51)
No outreach support n (%)
28 16 (57) 12 (43)

Staff maintenance CST results
There is a statistically significant difference with more
maintenance CST groups run in the outreach support group
compared to TAU group (p=.011)
Secondary outcome measures
Approach to dementia, job satisfaction, controllability of challenging behaviour, sense of competence, learning transfer, barriers to change and dementia knowledge
No difference

Observational study
Cognition and quality of life remained unchanged over the duration of the study.
When excluded participants scoring 25 or above on the MMSE.
Significant improvement in cognition after CST (p=.04)
No difference between BL and after maintenance CST.
Quality of life remained unchanged.

Comparison with a control group
Measure Spector (2003) contolmean change (SD) [N]
Current study meanchange (SD) [N]
Values
MMSE -0.4(3.5) [70] 1(4.6) [47] t = 2.04; p = 0.04
QoL-AD -0.8(5.6) [70] -1.4(9.3) [46] t = 0.08; p = 0.94
Conducted as no control group for this study.
Meta analysis comparison of mean change in CST groups
compared to control group (Spector et al., 2003).
1.4 point increase on MMSE for CST programme.
Quality of life unchanged.

Development of Individual Cognitive Stimulation Therapy
• 75 individual cognitive stimulation
sessions
– Delivered by the family carer
– for 30 minutes, 3 times a week, over 25 weeks
Sessions aim to:
• Provide mental stimulation
• Each individual CST session consists of a themedactivity, i.e. being creative
• iCST is guided by therapeutic principles, avoidingdirect memory questions, focusing on opinions ratherthan facts
______________________________________________________________
iCST Revision of Materials
Useful comments by experts, people with dementia, and carers
Key comments and revisions
Emphasise on positive aspects of iCST
This will empower carers involved in the programme
iCST needs an emphasis on both the family carer and
the person with dementia and should be person centred
Describe the purpose and content of activities as an
opportunity for discussion
Focus on images in the iCST sessions, as ‘images are
less threatening than words”
______________________________________________________________

iCST Carer Support
Key areas of support for family carers in main RCT
Carers receive the following types of support
A Set-up visit
Home based training with an opportunity to ask questions about iCST
Telephone support (preference for weekly support)
Two home visits after completion of 50% of the iCST sessions and at the end of iCST
Training protocol in place to ensure consistency in training
Treatment protocol in order to guide researchers
Treatment Adherence Reporting following previous models emphasizing the need to specify treatment implementation
______________________________________________________________


Referred/screened (n = 1340)
Baseline Assessment & Randomisation (n = 356)
Follow-up 1 - 13 weeks assessment (n = 288) 68 losses52 withdrawals (including 4 deaths) 16 agreed to follow up 2
Follow-up 2 - 26 weeks assessment (n = 273) Further 31 dyads withdrew (4 deaths)83 withdrawals overall retention rate 77%, attrition rate was 21% excluding deaths (predicted rate in updated sample size calculations
No difference between centres at FUP2 p = 0.33

Perception of allocation at 26 weeks
Treatment allocation
Researcher rating iCST (%) TAU (%) Total (%)
‘Definite’ judgment: Correct 22 (19) 4 (3) 26 (10)
‘More likely’ judgment: Correct 17 (15) 17 (12) 34 (13)
Equally likely to be in iCST or TAU 65 (57) 80 (57) 145 (57)
‘More likely’ judgment: Incorrect 10 (9) 31 (22) 41 (16)
‘Definite’ judgment: Incorrect 0 9 (6) 9 (4)
Total 114 141 255
Main Results356 participants across 8 UK centres seen at baseline, 3 & 6 months
At six months no differences in primary outcomes
ADAS-Cog cognition: difference -0.55 (SE) 0.74; p = 0.45
quality of life: difference -0.14, (SE) 0.50; p = 0.78
People with dementia (iCST) improved carer relationship
difference 1.77 (SE) 0.77; p = 0.02
Improved quality of life for the carer at 6 months Carers (iCST) higher quality of life difference 0.06 (SE) 0.02; p = 0.01
Adherence analyses:
Dyads completing more iCST sessions also showed lower carer
depressive symptoms p = 0.018

Positive outcomes for people with dementia
My dad’s mood is
lifted during
sessions
My mum seems
more confident
and like her old
self
Mum is more alert
after sessions
Mum’s
conversational
skills seem to
have improved
Mum is enjoying
the activities
Cognitive Stimulation Therapy for dementia
• Cognitive and social activities in group or with family carer
• Easy to deliver using standard manuals & DVD
• CST principles also useful in practice
• Benefits to cognition and quality of life (Spector 2003; NICE, 2006, Woods 2012; World Alzheimer Report ADI, 2011; Orrell et al., 2014).
• Cost effective (Knapp et al 2006) and savings to NHS of potentially £54 million/year (Institute for Innovation 2011).
• Works in synergy with cholinesterase inhibitors
• Used in 65% of UK memory services
• CST website: www.cstdementia.com
• Making a difference 1/2/3 and DVDs from http://www.careinfo.org/books/
• 25 countries using CST
• Join the CST Network - email [email protected]

NIHR CLAHRC East Midlands Annual Meeting
Partners in Progress – Sharing and Learning
A partnership between
Nottinghamshire Healthcare NHS Foundation Trust
and the Universities of Nottingham and Leicester
NIHR CLAHRC East Midlands Annual Meeting –
Creating New Solutions to Healthcare Challenges
A partnership between
Nottinghamshire Healthcare NHS Foundation Trust
and the Universities of Nottingham and Leicester
From Research to the
Real World
Facilitator – Sally Boyce,
Implementation Manager
Ambergate Room
Building a Research
Active Workforce
Facilitator – Dr Emma
Rowley, Capacity
Development Lead
Alfreton Room
Engaging Diverse
Communities: Why its
Crucial & How to Do it
Facilitator – Dr Paula Wray,
Public Involvement
Programme Lead
Barber Room

Thank you for attending
www.clahrc-em.nihr.ac.uk
@CLAHRC_EM