nhs greater glasgow and clyde pathway for the ...library.nhsggc.org.uk/mediaassets/back pain...
TRANSCRIPT
© GGBPS June 2006 (Review date 2009)
NHS Greater Glasgow
and Clyde Pathway for
the Physiotherapy
Management of Low
Back Pain
1st Edition
June 2006

© GGBPS June 2006
ii
Table of Contents
Forewords Gordon Waddell v Helen Frost vii Mick McMenemy
xi
Acknowledgements
xii
1 Purpose and Aims of Pathway Document 1 2 Executive Summary 3 3 Introduction 5 3.1
Introductory Statement 5
3.2 Make up of the Pathway Group 5
3.3 Main Aims of the Pathway Group 5
4 The need for the Pathway Group for Low Back Pain
6
4.1 Reasons Behind the Pathway Group 6 4.2 Frost Report 6 4.3 A Scoping Exercise to Gather
Thoughts and Opinions of all Physiotherapy Staff
7
5 Overview of Low Back Pain 8 5.1 Definition of Low Back Pain 8 5.2 UK Perspective of Low Back Pain
8
6 Greater Glasgow Back Pain Service (GGBPS) 9 6.1 GGBPS Overview 9 6.2 GGBPS Initiatives
9

© GGBPS June 2006
iii
7 Description of Population Area Represented by GGBPS
10
7.1 Population of Greater Glasgow 10
7.2 Overview of GGBPS patients 10 7.3 Community Health Partnerships
12
8 Clinical Guidelines 13 8.1 Overview of Clinical Guidelines 13 8.2 Clinical Guidelines for Low Back Pain 13 8.3 Red and Yellow Flags 13 8.4 Royal College of General Practitioner
(RCGP) Guidelines 14
8.5 European and Cochrane Guidelines
16
9 Physiotherapy management of low back pain 20 9.1 Low Back Pain Studies Relating to
Physiotherapy Opinion
20
9.2 UK Studies 20
9.3 Glasgow Study 21
24 10 Entry routes for Patients with Low Back Pain 24
10.1 GP/Consultant Referrals 24 10.2 Patient Self Referral 24 10.3 Re-directed Referrals from
Orthopaedics
26
11 Exit routes for Patients with Low Back Pain 27 11.1 Psychology 27 11.2 Surgery 28 11.3 Imaging 28 11.4 DEXA 29 11.5 Physiotherapy-led Back Class 29 11.6 Community-led Class 29 11.7 Self Care 30

© GGBPS June 2006
iv
11.8 Pain Association Scotland (PAS) 30 11.9 Pain Clinic 31 11.10 Back to GP 32 11.11 Vertebroplasty 32 11.12 Paediatric cases
33
12 Audit 34 12.1 Baseline Audit 34 12.2 Ongoing Audit
34
13 Summary
35
14 References
37
15 Appendices 42 1 Pathway Group Members 42 2 Delphi Study 44 3 GGBPS Referral Pad 47 4 Acute Low Back Pain Information
Sheet 49
5 Modified Linton Questionnaire 51 6 Enhanced Back Class referral forms
(1) East 57
(2) South 60 7 DEXA Referral Form 63 8 Back to Basics 65 9 Cauda Equina Triage chart 66 10 GGBPS Direct access audit 67 11 (1) Acute Management Treatment
Audit
69
(2) Non Acute Management Audit 70

© GGBPS June 2006
v
Forewords
Gordon Waddell (June 2006)
Low back pain is still one of the most common causes of chronic
pain and disability, sickness absence, and long-term incapacity.
Yet most low back pain should be manageable, recovery is
normally to be expected (albeit often with some persistent or
recurrent symptoms) and long-term incapacity is not inevitable.
Clearly, much still needs to be done to provide all patients with
low back pain with the best management they deserve.
There is now a solid evidence-base on which treatments are
effective for low back pain and, equally important, which are
ineffective. There is a growing demand for evidence-based
practice and it is no longer acceptable to provide ineffective
treatments simply because ‘I’ve always done it that way’. Yet
busy health professionals do not have time to keep up with the
latest research, which is why there is a need for evidence
reviews and clinical guidelines like this.
There is also now overwhelming evidence and increasing
agreement that low back pain can only be understood and
managed by a ‘biopsychosocial model’. This is a clumsy,
technical term but unfortunately no one has offered a better
alternative. Put simply, this is an individual-centred model that
takes account of the person, his or her health condition, and the
social context. Biological, psychological and social factors can
aggravate and perpetuate chronic pain and disability; they can
also act as obstacles to recovery: clinical management and
rehabilitation must then address the bio – psycho – social

© GGBPS June 2006
vi
obstacles to recovery. All health professionals who treat patients
with low back pain should be interested in and accept
responsibility for rehabilitation and for social/occupational
outcomes.
The Greater Glasgow Back Pain Service is a UK leader in this
approach and this Pathway Document is an important further
step to meeting these challenges. The authors are to be
congratulated and I am delighted to support and recommend it.

© GGBPS June 2006
vii
Helen Frost MSc MCSP (June 2006)
Research Fellow, Department of Public Health, Warwick
Medical School, University of Warwick
Low back pain is a common problem that results in 7% of the
adult population seeking consultation each year incurring high
costs to patients and the NHS. The prognosis of acute low back
pain is favourable with an estimated 90% of back pain sufferers
recovering within 6 weeks, however, low levels of pain and
disability often persist and most people will have at least one
recurrence within 12 months. 1 The challenge for all those
dealing with back pain is not how to cure it but how to manage it
effectively. A clinical model was pioneered by Gordon Waddell
in 1987 2 that rejected the traditional medical approach to back
pain and called for active management based on psychosocial
factors that challenges beliefs about pain, focuses on coping
rather than curing pain and encourages return to normal activity.
This model has been adopted by many health care providers but
there are still numerous different types of treatments available
for back pain sufferers many of which have not been subjected to
scientific scrutiny. Over the last 2 decades there has been a vast
number of randomised controlled trials and reviews of back pain
interventions aiming to evaluate some of these interventions.
The quality of the trials is variable but the recent larger trials
show either no differences between groups or only small
treatment effects for pain, disability and general health.3-6 This
is disappointing but these small treatment effects may well be
important to patients and can be cost effective.7 The trial of
physiotherapy intervention that compared a one off session of
© GGBPS June 2006
viii
advice encouraging return to normal activity with additional
physiotherapy treatment caused considerable controversy when
published in 2004.4 It reported no evidence of a significant short
term or lasting effect of additional physiotherapy treatment in
back pain or health related quality of life measures. The most
novel aspect of the trial was the introduction of a single
physiotherapy session of advice, based on The Back Book8, as the
“control” treatment. The data suggests that this model of
treatment was, in general, well received and the trial was
designed and did reflect everyday physiotherapy provision in the
NHS. 9 The trial cannot tell us which treatments work best for
low back pain, but for patients with similar symptom profiles of
low levels of back pain disability, it suggests that
physiotherapists should consider one session of assessment and
advice rather than prolonged treatment. In a feasibility study
that evaluated prompt access to physiotherapy treatment in
primary care more than 70% of patients were satisfied and
successfully treated with a single visit indicating that this type of
treatment can be a useful approach for selected patients.10
Back pain resources are over stretched in the NHS and it is
essential to look at all the evidence to make the best use of
services available. The European guidelines were compiled by a
group of experts in the back pain field and are based on
systematic evidence and consensus.11 12 The guidelines provide a
sound evidence based platform to work from and build upon. The
simple advice to remain active is universally accepted but some
patients need help to motivate them and overcome fear of

© GGBPS June 2006
ix
activity and exercise. Exercise is recommended for patients with
sub-acute and chronic low back pain and, unlike other passive
forms of treatment, has additional health benefits. Unfortunately
exercise is not always a popular option and it can only be
effective if compliance is high. Physiotherapists are well trained
to address this problem but it is a hurdle that needs to be
overcome in order to optimize any potential benefits.
The publication of guidelines does not automatically result in
clinicians following recommendations because barriers to change
remain across the NHS 13-15 This document presents care pathways
for the management of all back pain that could assist
implementation in other Health Authorities. It has been
developed by researchers and clinicians with an aim to help
physiotherapists adopt an evidence-based approach to the
management of back pain and it provides a consistent clear
message that should help to prevent confusion, frustration and
raised expectations experienced by many patients. It presents a
careful approach to the assessment and identification of those
with serious back problems and offers sensible alternatives for
others taking into account severity, disability and psychosocial
factors. It has the potential to be enormously helpful as a guide
to those managing back pain patients in the NHS and will no
doubt evolve with the publication of ongoing research and
further clinical input.
References
1. Pengel HM, Maher CG, Refshauge KM. Systematic review of conservative interventions for
subacute low back pain. Clin Rehabil 2002; 16(8):811-20.
2. Waddell G. 1987 Volvo award in clinical sciences. A new clinical model for the treatment
of low-back pain. Spine 1987; 12(7):632-44.

© GGBPS June 2006
x
3. BEAM. United Kingdom back pain exercise and manipulation (UK BEAM) randomised trial:
effectiveness of physical treatments for back pain in primary care. BMJ 2004;
329(7479):1377.
4. Frost H, Lamb SE, Doll HA, Carver PT, Stewart-Brown S. Randomised controlled trial of
physiotherapy compared with advice for low back pain. BMJ 2004; 329(7468):708.
5. Hay EM, Mullis R, Lewis M, Vohora K, Main CJ, Watson P, et al. Comparison of physical
treatments versus a brief pain-management programme for back pain in primary
care: a randomised clinical trial in physiotherapy practice. Lancet 2005;
365(9476):2024-30.
6. Wyatt M, Underwood MR, Scheel IB, Cassidy JD, Nagel P. Back pain and health policy
research: the what, why, how, who, and when. Spine 2004; 29(20):E468-75.
7. BEAM. United Kingdom back pain exercise and manipulation (UK BEAM) randomised trial:
cost effectiveness of physical treatments for back pain in primary care. BMJ 2004;
329(7479):1381.
8. Roland MWG, Klaber Moffett J, Burton K, main C, and Cantrell T. The Back Book. 1996.
9. Foster NE, Thompson KA, Baxter GD, Allen JM. Management of non-specific low back pain
by physiotherapists in Britain and Ireland. A descriptive questionnaire of current
clinical practice. Spine 1999; 24(13):1332-42.
10. Pinnington MA, Miller J, Stanley I. An evaluation of prompt access to physiotherapy in
the management of low back pain in primary care. Fam Pract 2004; 21(4):372-80.
11. Airaksinen O, Bronx JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, et al.
Chapter 4 European guidelines for the management of chronic non-specific low
back pain. Eur Spine J 2006; 15(Supplement 2):s192-s300.
12. Van Tulder M, Becker A, Bekkering T, al. E. European guidelines for the management of
acute non-specific low back pain in primary care. European Commission, Research
Directorate General. 2004.
13. Dey P, Simpson CW, Collins SI, Hodgson G, Dowrick CF, Simison AJ, et al.
Implementation of RCGP guidelines for acute low back pain: a cluster randomised
controlled trial. Br J Gen Pract 2004; 54(498):33-7.
14. Bishop A, Foster NE. Do physical therapists in the United Kingdom recognize
psychosocial factors in patients with acute low back pain? Spine 2005; 30(11):1316-
22.
15. Bishop PB, Wing PC. Compliance with clinical practice guidelines in family physicians
managing worker's compensation board patients with acute lower back pain. Spine
J 2003;3(6):442-50.

© GGBPS June 2006
xi
Mick McMenemy (June 2006)
Lead Clinician, Greater Glasgow Back Pain Service
The Greater Glasgow Back Pain Service was launched in
September 2002. Its stated aim was to ‘develop into a city-wide
centre of excellence’.
This document now provides a resource describing ‘best practice’
and will be available in all physiotherapy departments. It
describes current entry and exit routes for patients in the
Greater Glasgow area and should help clinicians make the best
decisions with their patients.
A strength of the document is that it is a consensus statement
from a representative cross-section of physiotherapy clinicians
from Greater Glasgow, enhanced by the input from recognised
external experts, Professor Gordon Waddell and Helen Frost. A
huge thanks goes to the group members who contributed to this
piece of work, especially Fraser Ferguson who both convened the
group and compiled the document.
In Glasgow we now have a guide for best practice to help
individual clinicians in every physiotherapy department and a
model which can be audited to ensure patients are receiving the
best care. Publication of this document is an important step in
developing the highest standards of care for all patients with low
back pain.

© GGBPS June 2006
xii
Acknowledgements
Thanks is given to the feedback was obtained from all Clinical
Specialist Physiotherapists working within the GGBPS and from all
other physiotherapy staff working within Greater Glasgow.

© GGBPS June 2006
1
1 Purpose and Aims of Pathway
Document
The Pathway document contains:
o Reasons for its development;
o Evidence based background of management of LBP;
o Areas of confusion and concern raised by physiotherapy
staff;
o UK and Glasgow perspective of physiotherapy management
of LBP;
o Diagram of entry routes for LBP;
o Clear instructions on exit routes from physiotherapy;
o Clear indication of who should refer patients on to other
services;
o Clear timescale for these referrals;
o Plan for baseline and future audits.
• The information in this document is evidence based,
referencing the most recent clinical guidelines for low back
pain.
• More in depth information in the appendices section
supports the basic information contained in the main body
of the text.

© GGBPS June 2006
2
• The aim of the document is designed to optimise the
physiotherapy management of low back pain (LBP) within
NHS Greater Glasgow and Clyde (NHSGGC), and promote an
up to date, clinically effective pathway in this
management.
• The intended audience is for physiotherapists who manage
LBP within NHSGGC. It is hoped this document is relevant to
all professionals.
• The document will be updated regularly and any impact of
the document will be audited on a regular basis.

© GGBPS June 2006
3
2 Executive Summary
1. The Chartered Society of Physiotherapy (CSP) demands that
there is a system to ensure that all physiotherapists provide
care that is based on the best available evidence of
effectiveness.’ (CSP, Service Standards 4.1) There should be
links established ‘to identify good practice…through sharing
of information…with national sources of critically appraised
reviews of evidence’ (CSP, Service Standards 4.3). This has
been supported by the Scottish Executive, which has recently
reaffirmed its aim to root out ineffective clinical treatment
and promote equity of care (Scottish Executive, 2005).
2. The Greater Glasgow Back Pain Service (GGBPS) includes ALL
PHYSIOTHERAPY STAFF responsible for the management of
low back pain within NHSGGC.
3. Every physiotherapist, working within NHSGGC, should have a
working knowledge of the contents of this document. This
will help ensure the best use of the available resources of
the GGBPS.
4. Review of clinical evidence and clinical guidelines of the best
available evidence of effectiveness conclude that modalities
such as TENS, ultrasound, interferential, pulsed or non-
pulsed shortwave, laser, traction or acupuncture lack
credible evidence based on rigorous scientific trails.

© GGBPS June 2006
4
Therefore their use in the physiotherapy management of low
back pain is not routinely recommended (van Tulder et al
2005; Burton et al 2005; Airaksinen; NHS 2005).
5. If the physiotherapy management of LBP within NHSGGC is to
be seen as a credible, evidence based service then we must
critically review our selection of modalities for the
management of low back pain.
6. A good understanding of the available exit routes for patients
with LBP should result in best practice for more patients.
7. However, production of the Pathway Document alone will
not in itself change clinical practice Ongoing education,
service development, staff training and awareness of the
most up to date literature around LBP is equally vital. These
factors will be driven by the 13 clinical physiotherapy
specialists attached to the GGBPS.
8. Work on this Pathway Document for the physiotherapy
management of low back pain (LBP) was started prior to the
recent reorganisation of health services within Greater
Glasgow, which resulted in the newly merged NHS Greater
Glasgow and Clyde Health Board. This pathway document
therefore refers to the management of LBP only within NHS
Greater Glasgow (NHSGG).

© GGBPS June 2006
5
3 Introduction
3.1 Introductory Statement
The Greater Glasgow Back Pain Service aims to provide the
highest standards of care to the healthcare users of Greater
Glasgow. The service is evidence based, and systematically
evaluated and developed to ensure this. Patient centered, we
will respect the individuality of all patients and their carers.
Using a bio psychosocial model of back pain, self-management
and the principles of rehabilitation are central to the service
approach; the aim is to develop the GGBPS as a centre of
excellence for the management of patients with low back pain.
3.2 Make up of the Pathway Group
This document has been a consensus of opinion amongst
representatives of NHSGGC physiotherapy staff, covering both
primary care and acute sites. This was supplemented with the
input of recognised world experts in the management of LBP See
appendix 1.
3.3 Main Aims of the Pathway Group
The main aim of this group was to review and redefine the
pathways for the physiotherapy management of LBP within the
NHSGGC.

© GGBPS June 2006
6
4 The Need for the Pathway
Group for Low Back Pain
4.1 Reasons Behind the Pathway Group
The Greater Glasgow Back Pain Service Health Board Steering
Group initiated the concept of reviewing the patient pathway for
LBP across NHSGGC.
This is an opportunity to review the pathway for patients, and
the pathway group has representatives of all key areas of
physiotherapy across Glasgow.
Although there is strong anecdotal evidence that many
physiotherapists working within NHSGGC are following evidence
based practice, there is at present no formal verification of this.
4.2 Frost Report
The need for this review was highlighted further following an
influential articles published by Frost (et al, 2004). The main
findings of this article were:
• A full assessment followed by evidence-based advice is as
effective as traditional physiotherapy treatment.
• There was no evidence of effectiveness of additional
physiotherapy sessions.

© GGBPS June 2006
7
4.3 A Scoping Exercise to Gather Thoughts and Opinions
of all Physiotherapy Staff
Widespread consultation amongst outpatient physiotherapy staff
took place. At every stage staff had the opportunity to comment
on, or raise points on the aims of the Pathway Document. The
following points were raised as problematic by the Greater
Glasgow NHS Health Board:
i. Confusion over entry routes to GGBPS and for
physiotherapy in general for patients with LBP
ii. Exit routes from treatment for patients with LBP
iii. Awareness of clinical guidelines and present pathway
(see table 5 below)
iv. Ongoing support for changes in clinical practice as a
result of Pathway recommendations
v. How will changes be monitored?
© GGBPS June 2006
8
5 Overview of Low Back Pain
5.1 Definition of Low Back Pain
LBP is defined as pain, muscle tension, or stiffness localized
between the areas covered by the 12th rib and the gluteal folds,
with or without leg pain (Frank et al, 1996; Thomas et al, 1999;
Harkness et al, 2003; Manek and MacGregor, 2005).
5.2 A UK Perspective of Low Back Pain
More than three quarters of the UK population can expect to
experience LBP at some point in their lifetime, but 90% of these
presentations are self-limiting within 6 weeks (Nachemson al,
2000; Pengel et al 2003; Pinnington et al 2004). Rates of
recurrence can be as high as 50% (McKenzie, 2005).
The remaining 10% of patients who do not improve within the 6
weeks require a disproportionate use of health services,
estimated at as much as 80% of the total cost of treating LBP
(Nachemson, 1992; Indahl et al, 1995).

© GGBPS June 2006
9
6 Greater Glasgow Back Pain
Service (GGBPS)
6.1 GGBPS Overview
The GGBPS was launched in September 2002. The Service consists
of a team of 13 clinical physiotherapy specialists in low back pain
who lead the management of low back pain in Greater Glasgow.
The team also liaises with 2 dedicated Clinical Psychologists. The
GGBPS though includes all physiotherapy staff within NHSGGC
who manage LBP. The overall aim of the GGBPS is to develop into
a citywide centre of excellence for the management of patients
with low back pain. This management aims to be evidence based.
6.2 GGBPS Initiatives
Since its launch in 2003, the GGBPS has begun to establish itself
as a centre of excellence in the management of low back pain.
(CSP, 2003; NHS Scotland 2004, QIS 2005).
© GGBPS June 2006
10
7 Description of Population Area
Represented by GGBPS
7.1 Population of Greater Glasgow
The GGBPS covers the entire population of Greater Glasgow, a
population of 900,000.
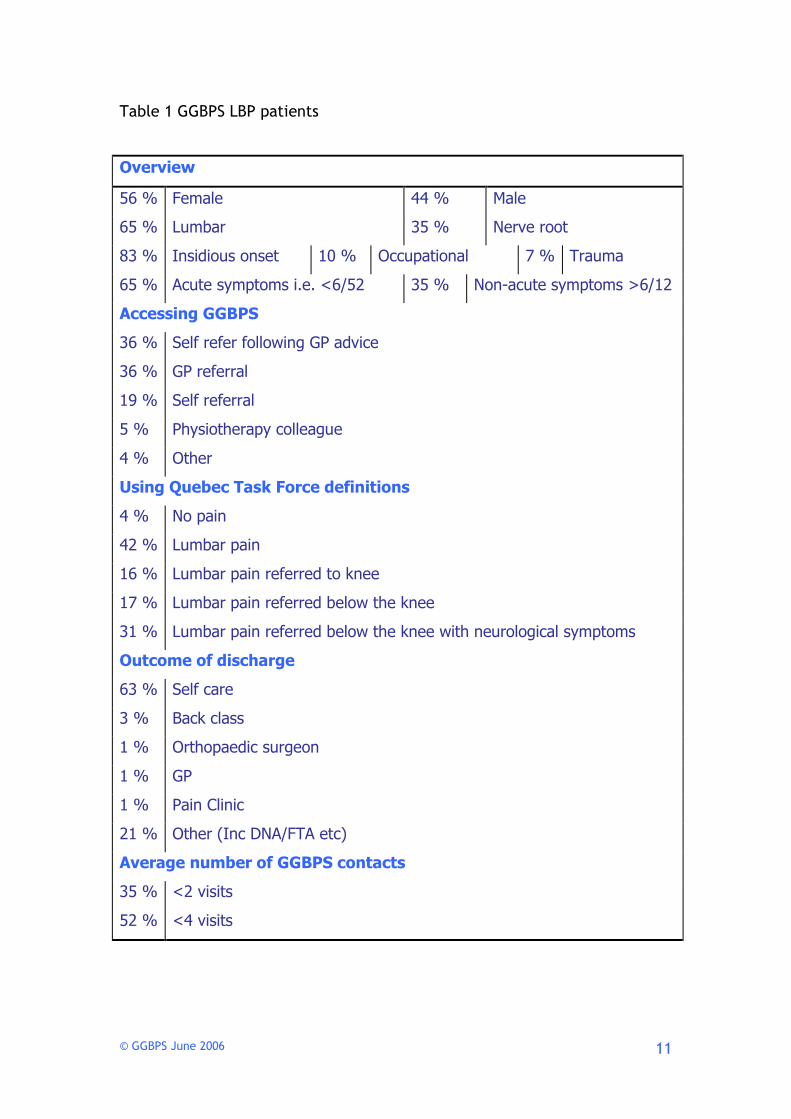
7.2 Overview of GGBPS Patients
Table 1 below contains a breakdown of all patients with LBP who
have been assessed by GGBPS specialists from January 2004 to
January 2006. Recent changes have seen parts of Argyll and Clyde
absorbed by Greater Glasgow. It is not clear yet how this will
affect GGBPS.
© GGBPS June 2006
11
Table 1 GGBPS LBP patients
Overview
56 % Female 44 % Male
65 % Lumbar 35 % Nerve root
83 % Insidious onset 10 % Occupational 7 % Trauma
65 % Acute symptoms i.e. <6/52 35 % Non-acute symptoms >6/12
Accessing GGBPS
36 % Self refer following GP advice
36 % GP referral
19 % Self referral
5 % Physiotherapy colleague
4 % Other
Using Quebec Task Force definitions
4 % No pain
42 % Lumbar pain
16 % Lumbar pain referred to knee
17 % Lumbar pain referred below the knee
31 % Lumbar pain referred below the knee with neurological symptoms
Outcome of discharge
63 % Self care
3 % Back class
1 % Orthopaedic surgeon
1 % GP
1 % Pain Clinic
21 % Other (Inc DNA/FTA etc)
Average number of GGBPS contacts
35 % <2 visits
52 % <4 visits

© GGBPS June 2006
12
7.3 Community Health Partnerships
All Community Health Partnerships (CHPs) have input from the
Clinical Specialists working within the GGBPS. All acute sites
where outpatient physiotherapy is provided also have input from
these Clinical Specialists These sites are the Western Infirmary,
Glasgow Royal Infirmary, Gartnavel General, Stobhill, Southern
General and the Victoria Infirmary. The management of LBP by
the GGBPS is based on the recommendations of the RCGP
guidelines for LBP (Hutchison et al, 1996).

© GGBPS June 2006
13
8 Clinical Guidelines
8.1 Overview of Clinical Guidelines
Clinical guidelines for the management and treatment of LBP are
plentiful (see table 2). These clinical guidelines have been
produced following the strictest criteria and all the evidence
reported in them was graded in relation to the strength of the
evidence reviewed. Further information on this grading is clearly
contained in each guideline.
8.2 Clinical Guidelines for Low Back Pain
These clinical guidelines have common themes throughout such
as encouraging patients to avoid bed rest, to stay active and
continue ordinary activities as normally as possible, to receive
active treatments and avoid passive therapies where possible
(Koes et al, 2001; Grimmer et al, 2003; Frost et al, 2004).
8.3 Red and Yellow Flags
The recognition of red flags as a means of raising suspicion of
serious spinal pathology (AHCPR, 1994) and the assessment of
yellow flags, which are psychosocial factors which can increase
the risk of a patient with acute LBP developing prolonged pain
and disability, affecting work and social circumstances (Accident
Compensation Corporation, 2003) were also encouraged.

© GGBPS June 2006
14
8.4 Royal College of General Practitioners (RCGP)
Guidelines
The RCGP guidelines have become the agreed guidelines of all
the health professionals who treat patients with LBP in UK
(Waddell, 1998; Pinnington, 2004). Recently the Prodigy
Guidelines have superseded the RCGP guidelines for the
management of LBP in England; however the GGBPS is
underpinned by the RCGP guidelines.

© GGBPS June 2006
15
Table 2 Overview of International guidelines for the management of LBP
* For the purpose of this table the European Guidelines are a combination of Airaksinen et al (2004); Burton et al (2004) van
Tulder et al (2004), which made up these guidelines.
** Prodigy guidelines have now supersede RCGP guidelines in the UK
*** Prodigy guidelines have been submitted to Quality Improvement Scotland for ratification for NHS Scotland
Name Country Patient
Group
Target
Group
Treatment recommendations
Agency for Health Care
Policy and Research
(AHCPR)
United
States
(1994)
Acute <12 weeks
from onset
Primary
care
Low impact aerobics. Manipulation <1/12
Dutch College of General
Practice (NHG),
Netherlands
(1996)
Acute and
chronic
GPs Exercise >6/52 Manipulation < 6/52 no use
National Advisory
Committee on Health
and Disability
New Zealand
(1997, 2003)
<12 weeks from
onset
Primary
care
No specific exercise. Manipulation <6/52 useful
Finnish Medical
Association
Finland
(1999)
Acute, sub acute
and chronic > 12
weeks from
onset
Primary and
secondary
care
Graded exercise>2/52Manipulation useful <6/52
National Health and
Medical Research
Council
Australia
(1999)
<12 weeks from
onset
Primary
care GPs
General exercise useful
Royal College of General
Practitioners (RCGP)
United
Kingdom
(1999)
<12 weeks from
onset
Primary
care GPs
Exercise useful >6/52 Manipulation useful to help non
responders
Danish Institute for
Health Technology
Assessment,
Denmark
(2000)
Acute < 12,
chronic > 12
weeks
Primary
care
Manipulation <1/52. McKenzie diagnosis and treatment
The Swedish Council on
Technology Assessment
in Health Care
Sweden
(2000)
> 12 weeks from
onset
Primary
care
Manual therapy and physical exercise
European Guidelines for
LBP *
Europe
(2004)
Acute <12
weeks, chronic >
12 weeks
Anybody
developing
/updating
guidelines
for LBP,
including
professional
bodies
A bio psychosocial approach by musculoskeletal
physiotherapists or osteopaths, or chiropractors. Exercise
therapy and manipulation for a short course
Traction, Electrotherapy Ultrasound Interferential therapy,
Laser treatments and TENS are specifically and clearly
listed as NOT recommended due to their ineffectiveness
PRODIGY Guidance -
Back pain – lower**
England
***(2005)
Acute < 12
weeks, chronic >
12 weeks.
Health care
professional
s
This guidance takes account of the 2004 European
Guidelines listed above

© GGBPS June 2006
16
8.5 European and Cochrane Guidelines
The European Guidelines (Airaksinen et al 2004; Burton et al
2004; Van Tulder et al 2004) have produced wide ranging,
evidence-based recommendation on treatments and interventions
for the management of LBP (See table 3). This again reiterates
the lack of evidence amongst many of the passive interventions
often attributed to physiotherapy management of LBP. Table 3
below gives a brief summary of these guidelines in relation to
acute LBP. Further information is available via the reference list.
Intervention Cochrane
Review
European
Guidelines For
Acute LBP
(Reviewed To Oct
2003)
Comments
Advice to stay
active
Review to July
2001
Small beneficial
effect for
simple acute
LBP
Little or no
effect for
sciatica
Less harmful
than bed rest
Evidence to
recommend staying
active including
work if possible;
avoid bed rest
Note difference between
simple low back pain and
sciatica
Bed rest Review to May
2004
Increased pain
levels and
poorer function
with bed rest
compared to
staying active.
No difference
Evidence suggests
avoiding bed rest
Note difference between
simple low back pain and
sciatica

© GGBPS June 2006
17
for sciatica
patients
between bed
rest and staying
active
Information and
re-assurance
Currently being
reviewed
Give information
about good
prognosis for
recovery, no need
for imaging when
full history and
examination suggest
no serious problem
Mentions back book
improves beliefs and
function but not pain
compared to other
information booklet.
Small number of studies
Psychosocial
risk factors
Assess psychosocial
risk factors early
and review if there
is no improvement
in overall condition
Urgent need for validated
instruments to assess
psychosocial risk factors
and to identify sub-groups
of patients with a high
risk of chronicity
Pain medication
and NSAIDs
Use paracetamol
first then NSAIDs as
second choice
Muscle
relaxants
Reviewed to Oct
2002
Strong evidence
effective for
acute LBP
Recommend if no
change with
paracetamol/NSAIDs
Caution due to drowsiness
Surgery for disc
prolapse
Reviewed to
May2000
Strong evidence
that sciatica
patients have
faster relief of
pain than with
conservative
27 randomised and quasi-
randomised studies with
methodological
weaknesses

© GGBPS June 2006
18
management
Long term
effect unknown
Multidisciplinary
treatment in
occupational
setting
(sub-acute)
Reviewed to
May 2001
Workplace visit,
occupational
health
intervention
with
multidisciplinary
treatment may
lead to
increased return
to work,
reduced sick
leave and
disability
Consider if sick
leave is greater
than 4-6 weeks
2 low quality RCTs
Manipulation Reviewed to
Sept 2003
Manipulation
superior to
sham treatment
for short term
benefit but no
difference
compared to GP
care, analgesia,
exercises,
education, PT
Consider
manipulation if
patients not
returning to normal
activities.
Need to identify
sub-groups of acute
LBP that this
benefits in future
studies
Contraindicated in
patients with severe or
progressive neurological
deficit
Exercise
therapy
Review to Feb
2000
No difference
between
exercise
therapy,
inactive or
other active
treatments
Current evidence
does not support
exercise therapy in
acute LBP
Only one out of twelve
RCTs found better
outcomes for exercise
therapy compared to
conservative treatment or
information.

© GGBPS June 2006
19
Massage Reviewed to Feb 2002
Massage inferior to
manipulation and TENS;
equal to corsets and
exercises; superior to
relaxation therapy,
acupuncture, self care
education and inert
treatments, Acupuncture
massage superior to
Swedish massage
Not
recommended
for acute LBP
Limited evidence for or
against use in LBP
Acupuncture Reviewed to Feb 2003
No conclusions possible in
acute low back pain
3 RCTs with low
participant numbers and
poor methodology
Traction Current
evidence does
not support the
use of traction
in acute low
back pain
Only 2 RCTs one showing
significant improvement
the other showing no
difference
TENS Not
recommended
for acute LBP
Insufficient evidence as
only 2 RCTs one showing
no significant difference
the other showing TENS
more effective than
paracetamol
Lumbar supports Reviewed to May 2000
No conclusions possible
5 poor quality RCTs
2 non randomized trials
Table 3 Review of evidence based European Guidelines for acute low back pain treatment

© GGBPS June 2006
20
9 Physiotherapy Management of
Low Back Pain
9.1 Low Back Pain Studies Relating to Physiotherapy
Opinion
Five studies have investigated the physiotherapy management of
LBP by directly questioning the physiotherapists’ involved over
their thoughts on the management of LBP (Battie et al 1994;
Foster et al 1999; Li and Bombardier 2001; Gracey et al 2002;
Mikhail et al, 2005).
Although they reported what they thought was a gradual
reduction in the use of interventions with poor evidence base,
many of these treatments were still seen as suitable modalities
to offer patients with LBP.
9.2 UK Studies
With direct reference to the UK, the findings by Foster et al
(1998) and Gracey et al (2001) are the most applicable to the
physiotherapy practice explored in this study (Table 4). Foster et
al (1999) found a preference for manual therapy for the
treatment of LBP. However, 48% of the respondents answered
the question on most commonly used electrotherapy treatment.
Gracey et al (2002) highlight the use of advice as being given in
almost 90% of referrals. This is in line with the most such as
current evidence (Hay et al, 2005), which has reported on the
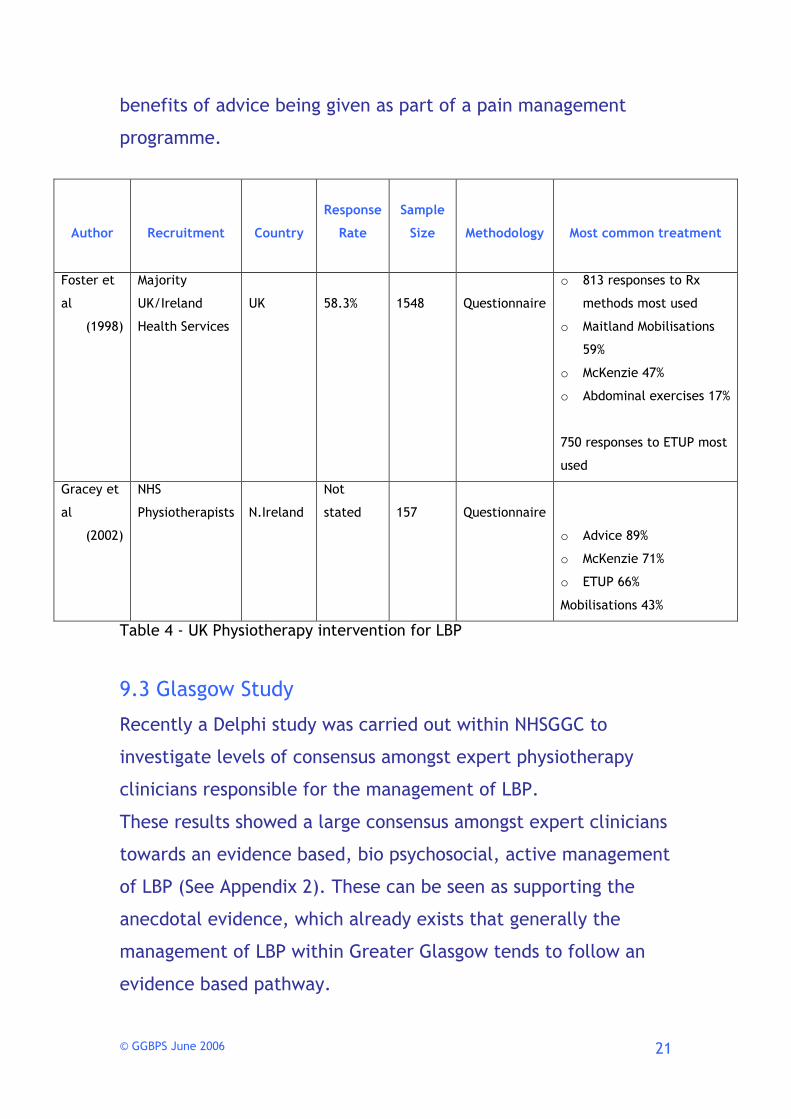
© GGBPS June 2006
21
benefits of advice being given as part of a pain management
programme.
Table 4 - UK Physiotherapy intervention for LBP
9.3 Glasgow Study
Recently a Delphi study was carried out within NHSGGC to
investigate levels of consensus amongst expert physiotherapy
clinicians responsible for the management of LBP.
These results showed a large consensus amongst expert clinicians
towards an evidence based, bio psychosocial, active management
of LBP (See Appendix 2). These can be seen as supporting the
anecdotal evidence, which already exists that generally the
management of LBP within Greater Glasgow tends to follow an
evidence based pathway.
Author
Recruitment
Country
Response
Rate
Sample
Size
Methodology
Most common treatment
Foster et
al
(1998)
Majority
UK/Ireland
Health Services
UK
58.3%
1548
Questionnaire
o 813 responses to Rx
methods most used
o Maitland Mobilisations
59%
o McKenzie 47%
o Abdominal exercises 17%
750 responses to ETUP most
used
Gracey et
al
(2002)
NHS
Physiotherapists
N.Ireland
Not
stated
157
Questionnaire
o Advice 89%
o McKenzie 71%
o ETUP 66%
Mobilisations 43%

© GGBPS June 2006
22
A recent audit (See Appendices 11(1) and 11(2) show in some
detail the actual physiotherapy management for LBP within
NHSGG. This data will form a baseline that will be re audited to
evaluate any impact of the Pathway Document.
© GGBPS June 2006
23

© GGBPS June 2006
24
10 Entry Routes for Patients
with Low Back Pain
10.1 GP/Consultant Referrals
In some cases a written referral is appropriate e.g. complex
medical history. (See appendix 3 for GP referral form) These
patients should be prioritised on an individual basis.
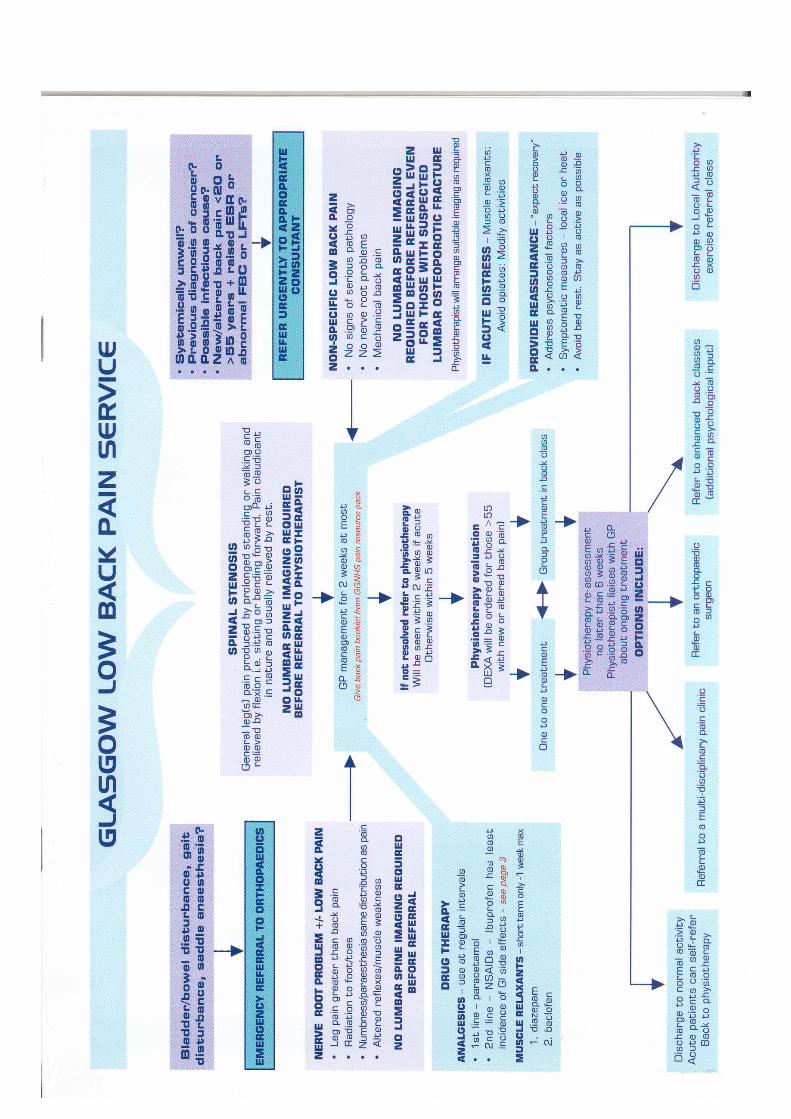
10.2 Patient Self Referral
This is the most common way of accessing physiotherapy. The
flow chart below has been designed to assist physiotherapy
clinicians in the initial management of LBP after they have
accessed treatment via self referral clinics. The acute LBP
information sheet is in appendix 4.
© GGBPS June 2006
25
If improving
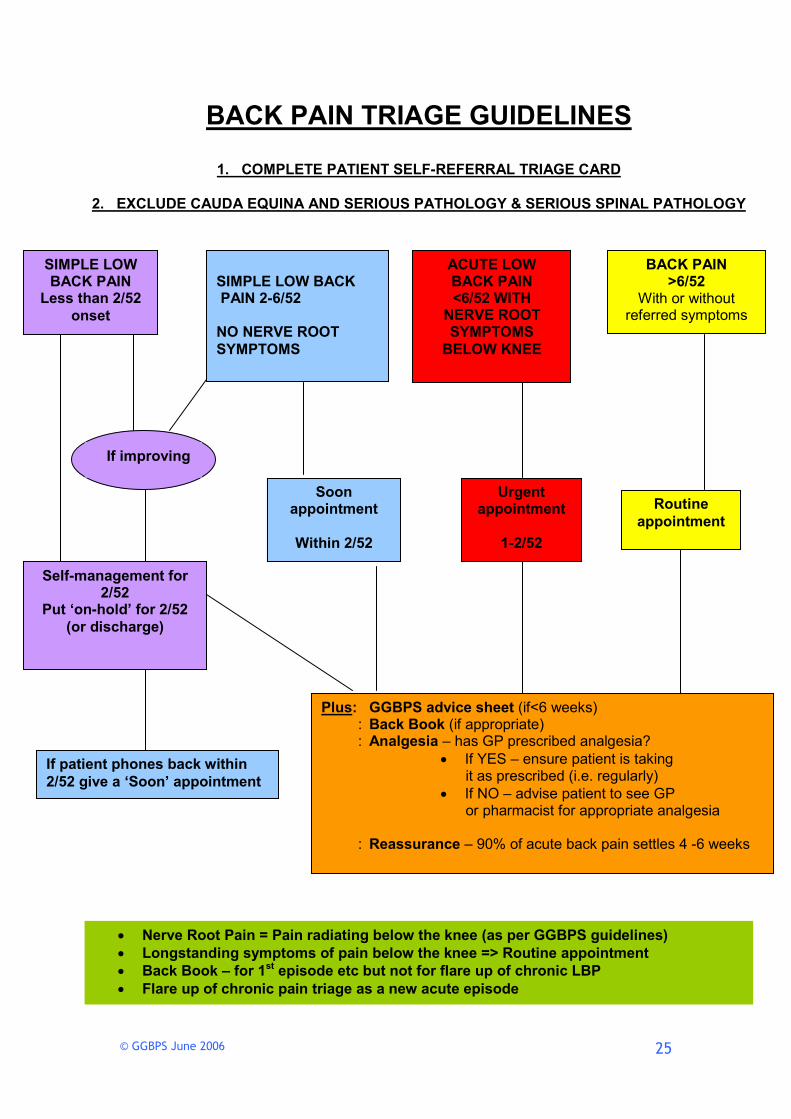
BACK PAIN TRIAGE GUIDELINES
1. COMPLETE PATIENT SELF-REFERRAL TRIAGE CARD
2. EXCLUDE CAUDA EQUINA AND SERIOUS PATHOLOGY & SERIOUS SPINAL PATHOLOGY
SIMPLE LOW BACK PAIN
Less than 2/52
onset
SIMPLE LOW BACK PAIN 2-6/52 NO NERVE ROOT
SYMPTOMS
ACUTE LOW BACK PAIN <6/52 WITH
NERVE ROOT SYMPTOMS
BELOW KNEE
BACK PAIN >6/52
With or without referred symptoms
Self-management for 2/52
Put ‘on-hold’ for 2/52
(or discharge)
Soon appointment
Within 2/52
Urgent appointment
1-2/52
Routine
appointment
Plus: GGBPS advice sheet (if<6 weeks) : Back Book (if appropriate) : Analgesia – has GP prescribed analgesia?
• If YES – ensure patient is taking it as prescribed (i.e. regularly)
• If NO – advise patient to see GP or pharmacist for appropriate analgesia
: Reassurance – 90% of acute back pain settles 4 -6 weeks
If patient phones back within
2/52 give a ‘Soon’ appointment
• Nerve Root Pain = Pain radiating below the knee (as per GGBPS guidelines)
• Longstanding symptoms of pain below the knee => Routine appointment
• Back Book – for 1st episode etc but not for flare up of chronic LBP
• Flare up of chronic pain triage as a new acute episode

© GGBPS June 2006
26
10.3 Re-directed Referrals from Orthopaedics
The preferred route for surgical opinion should be through the
back pain specialists. Occasionally however a GP will refer
directly to an orthopaedic surgeon. In such cases these referrals
are usually redirected to local physiotherapy departments for
GGBPS to assess initially.
These patients could be seen by any member of the
physiotherapy staff. On discharge a copy of the discharge letter
should be sent to the GP and orthopaedic consultant.

© GGBPS June 2006
27
11 Exit Routes for Patients with
Low Back Pain
11.1 Psychology (Enhanced Back Class)
Acute (6/52) and sub acute (12/52) patients at risk of developing chronic pain symptoms; especially those with significant Yellow Flags and not responding to physiotherapy management.
The Enhanced Back Class (EBC) was devised by psychology and is run jointly with physiotherapy. The class is designed to help those with back pain who have a presentation that includes psychosocial Yellow Flags. The class helps people to limit the influence of these flags on
their pain, through the development of practical skills.
Patients with symptoms > 6/12 are ineligible for EBC.
These patients can be referred for EARLY intervention by psychologists. If appropriate, these patients will be referred onto the EBC.
Modified Linton questionnaire and EBC referral form. (See Appendices 5 and 6)
Referrals should be discussed first with the
Back Pain Specialist.

© GGBPS June 2006
28
11.2 Surgery
11.3 Imaging
Routine plain film x-rays are not to be routinely
carried out.
Should a GP feel the need for plain film x-ray of the lumbar spine, they should discuss the
case with the radiologist.
MRI requests for acute symptoms should be made in tandem with an orthopaedic referral.
There is a fast tracking system in place for these
patients.
Chronic LBP of ANY duration (including stenotic patients) can be referred onto orthopaedics for opinion.
At present there is existing agreement on imaging for these patients.
Acute and sub acute LBP for which there may be a surgical indication and is not improving with 3/12 conservative treatment can be referred for imaging and an orthopaedic
opinion.
Surgery is usually indicated for nerve root pain, below the knee, which is not resolving with conservative physiotherapy and correct drug management.
ALL referrals should be made by the Back Pain Specialist
ALL referrals should be made by the Back Pain Specialist after review.

© GGBPS June 2006
29
11.4 DEXA
11.5 Physiotherapy-led back class
11.6 Community-led classes
All physiotherapy staff can refer a patient for a DEXA scan if concerned about osteoporosis. (See appendix 7)
Osteoporosis may affect the type of exercises prescribed or if the patients should be referred to an osteoporosis
class.
These exercise classes are designed to help people manage their back pain and return to normal activities. They also aim to prevent recurrence of back problems by helping the person to stay active.
A modified Linton questionnaire should be filled out before referral to these classes; patients scoring >105 (if working) and >80 (if not working) should not generally be
referred.
Back to Basics classes are an easy introduction to exercise and exercise techniques, with non-
medical supervision.
Suitable for those experiencing back pain or those who want to become more active and combine a range of activities at a lower intensity level.

© GGBPS June 2006
30
11.7 Self care
11.8 Pain Association Scotland (PAS)
Patients who are discharged to self care should be told that they can contact their physiotherapist within two months if their pain returns. After the two months, the patient should access physiotherapy through
their local self referral clinic.
This standard should be applied to all LBP patients no matter who is treating them.
Pain Association Scotland (PAS) utilises groups which are participant led, and helps to educate them about the causes of pain, the management and coping with chronic pain. Patients may attend regularly or only when they need support. An information leaflet is available for patient
information and PAS contact details.
© GGBPS June 2006
31
11.9 Pain Clinic
The Pain Clinic involves individual assessment and the intervention by the appropriate clinician (physiotherapist, psychologist or anaesthetist), or group of clinicians to help the patient cope with their pain.
Patients with poor pain management (particularly with chronic pain) may benefit from a multidisciplinary team approach.
Some patients with <6/12 duration of nerve root symptoms may benefit from an early assessment at the Pain Clinic for nerve root
blocks or caudal epidurals.
GGBPS may refer directly to the Pain Clinic. GP are also able to initiate referral.
ALL referrals should be made by the Back Pain Specialist after review.

© GGBPS June 2006
32
11.10 Back to GP
11.11 Vertebroplasty
Patients with suspected serious spinal pathology should be referred immediately back to their GP for review, including screening bloods. Serious spinal pathology would include the presence of significant Red Flags such as weight loss and history of
cancer.
Cauda Equina Syndrome (CES) is a potential surgical emergency. These patients should not be referred back to their GP. They that should be managed in line with the GGBPS CES triage chart (appendix 9).
Patients with suspected LBP from osteoporotic collapse may benefit from
vertebroplasty.
Symptoms should be
present >3/12 - < years.
These referrals should be made via Back Pain Specialist.

© GGBPS June 2006
33
11.12 Paediatric cases
<13 year olds with LBP should be referred to Yorkhill physiotherapy.
Discuss with Back Pain Specialist
>13 year olds should be managed by adult service.

© GGBPS June 2006
34
12 Audit
12.1 Baseline Audit
Two baselines audits are being carried out.
The first was to examine the appropriateness of physiotherapy
referrals of patients with LBP (see appendix 10).
The second is assessing treatment preferences amongst all out
patient staff. This builds on the Delphi study mentioned earlier
(see appendix 11).
12.2 Ongoing Audit
These audits will be reviewed regularly.

© GGBPS June 2006
35
13 Summary
This document is the work of the pathway group (see appendix
1), and all staff have had the opportunity to influence and
comment on the document. The GGBPS includes ALL
PHYSIOTHERAPY STAFF responsible for the management of low
back pain within NHSGGC.
Issues around lack of clarity on how to enter and exit LBP
services have been cleary defined, and awareness of these should
improve patient care.
Whilst not prescribing physiotherapy treatment for LBP, the
document clearly lays out professional requirements from the
CSP (CSP, Service Standards 4.1) and the most recent evidence to
manage LBP. This has been supported by the Scottish Executive,
which has recently reaffirmed its aim to root out ineffective
clinical treatment and promote equity of care (Scottish
Executive, 2005).
If the physiotherapy management of low back pain (LBP) within
NHSGGC is to be seen as a credible, evidence based service, then
we must critically review our selection of modalities for the
management of low back pain.
Ongoing education, audit, service development, staff training
and awareness of the most up to date literature around LBP is

© GGBPS June 2006
36
equally vital. These factors will be driven by the 13 clinical
physiotherapy specialists attached to the GGBPS.

© GGBPS June 2006
37
14 References
Accident Compensation Corporation (2003) New Zealand Acute
Low Back Pain Guide, incorporating the guide to assessing
psychological yellow flags in acute low back pain.
www.nzgg.og.nz/guidelines/0072/albp_guide_col.pdf (last
accessed 29/08/05)
Agency for Health Care Policy and Research (1994) Acute Low
Back Problems in Adults, Clinical Practice Guideline Number 14,
AHCPR publ no 94-0642, Public Health Service, US Department of
Health and Human Services Rockville, MD.
Airaksinen, O., Bronx, J.I., Cedraschi, C. et al. (2004) European
guidelines for the management of chronic non-specific low back
pain. European Commission, Research Directorate
General.http://www.backpaineurope.org (last accessed 29/08/05)
Bogduk N. Draft evidence based clinical guidelines for the
management of acute low back pain. National Health and Medical
Research Council, Australia, 2000 (URL: http://www.health.gov.au
:80/nhmrc/media/2000rel/pain.htm) (last accessed 29/08/05)
Burton, A.K., Balagué, F., Cardon, G. et al. (2004) European
guidelines for prevention in low back pain. European Commission,
© GGBPS June 2006
38
Research Directorate General. www.backpaineurope.org (last
accessed 29/08/05)
Chartered Society of Physiotherapy Standards of physiotherapy
practice
http://www.csp.org.uk/uploads/documents/SOPPservice.pdf Last
accessed 25/10/05
Clinical Standards Advisory Back Pain (1994) Report of a clinical
standards advisory group on back pain. HMSO, London.
Danish Health Technology Assessment (1999) Low Back Pain –
frequency, management and prevention from an HTA perspective.
Danish Health Technology Assessment 199 Vol.1 (1).
http://www.sst.dk/Applikationer/cemtv/publikationer/docs/Low-
back%20pain/LowBackPain.pdf (last accessed 29/08/05)
Ferguson. F. (2006) An investigation of referrals for low back pain
to outpatient physiotherapy. Consensus of expert physiotherapy
clinicians using a three round Delphi questionnaire. MPhil project
(unpublished as yet)
Foster, N., Thompson, K., Baxter, J.M., (1999) Management of
non-specific low back pain by therapists in Britain and Ireland
Spine Vol. 24 (13) pp.1332-1342.
Frost, H., Lamb, S., Doll, H., Carver, P., Stewart-Brown, S. (2004)
Randomised controlled trial of physiotherapy compared with advice
for low back pain. BMJ Vol.329 pp.708-714.

© GGBPS June 2006
39
Gracey, J.H., McDonough, S.M., Baxter, G.D (2002) Physiotherapy
management of low back pain: a survey of current practice in
Northern Ireland Spine Vol. 27(4) pp. 406-411
Greater Glasgow NHS Board (2005) Audit of patient satisfaction of
the Greater Glasgow Back Pain Service
Grimmer, K., Milanese, S., Bialocerkowski, A. (2003) Clinical
guidelines for low back pain: a physiotherapy perspective.
Physiotherapy Canada Vol. (55) pp.185-194.
Hutchinson, A., Waddell, G., Feder, G. Clinical Guidelines for the
Management of Acute Low Back Pain. London: Royal College of
General Practitioners; 1996 www.rcgp.org.uk (last accessed
29/08/05)
Johsson E. (2000) The Swedish Council on Technology Assessment
in Health Care. Back Pain Neck Pain, an evidence based review
Report number I-45
http://www.sbu.se/Filer/Content0/publikationer/1/back_neckpain_
2000/backpainslut.pdf (last accessed 29/08/05)
Keeney, S., Hasson, F., McKenna, H.P. (2001) A critical review of
the Delphi technique as a research methodology for nursing.
International Journal of Nursing studies Vol. 38 pp.195-200.
Koes, B.W., van Tulder, M.W., Ostelo, R., Burton, K., Waddell, G
(2001) Clinical guidelines for the management of low back pain in

© GGBPS June 2006
40
primary care: an international comparison. Spine Vol. 26 pp 2504-
2513.
McKenzie R.A. (2005) The myth of acute low back pain The New
Zealand Family Physician Vol.32 (2) pp.125-126
Malmivaara, A., Kotilainen, E., Laasonen, E., Poussa, M.,
Rasmussen, M. (1999) Clinical Practice Guidelines of the Finnish
Medical Association Diseases of the low back. Finnish Medical
Association Diseases of the low back.
Mikhail, C., Korner-Bitensky, N., Rossignol, M., Jean-Pierre Dumas,
J.P. (2005) Physical therapists’ use of interventions with high
evidence of effectiveness in the management of a hypothetical
typical patient with acute low back pain Physical Therapy . Vol. 85
(11) pp.1151-1167
NHS (2005) Prodigy guidelines for low back pain
www.prodigy.nhs.uk/guidance.asp?gt=Back pain - lower (last
accessed 29/08/05)
Pinnington, M. A, Miller, J., Stanley, I. (2004). An evaluation of
prompt access to physiotherapy in the management of low back
pain in primary care. Famil. Pracicet. Vol. 21 pp.372-380
Pope, G., Mockett, S., Wright J. (1995) A survey of electrotherapy
modalities. Physiotherapy Vol.81 pp. 82-91

© GGBPS June 2006
41
Turner, G.H., Weiner, D.K. (2002) Essential components of a
medical student curriculum on chronic pain management in older
adults: results of a modified Delphi process. Pain Medicine Vol. 3
(3) pp. 249-252.
Van der Valk, R.W.A., Dekker, J., Van Baar, M.E. (1995) Physical
therapy for patients with back pain. Physiotherapy; Vol. 81
pp.345–51
van Tulder, M., Becker, A., Bekkering, T. et al. (2004) European
guidelines for the management of acute non-specific low back pain
in primary care. European Commission, Research Directorate
General. www.backpaineurope.org (last accessed 29/08/05)
Waddell, G. (1998) The Back Pain Revolution. 1st edition Churchill
Livingstone. Edinburgh
Whitley Council (1992) Whitley Councils for health services (Great
Britain). Conditions of service. HMSO (Scottish Executive, 2005)
Department of Health (2005) Delivering for Health- A response to
the Kerr Report
www.scotland.gov.uk/Topics/Health/care/communitynursing/delive
ringforhealth

© GGBPS June 2006
42
15 Appendices
Appendix 1 Pathway Group Members
Chair: Mick McMenemy (Lead Clinician, GGBPS)
Helen Frost (Research Fellow and published author)
Professor Gordon Waddell
Janice Miller (Physiotherapy Manager West Glasgow CHCP)
Nicholas Evans (Clinical Specialist Physiotherapist, GGBPS)
Fraser Ferguson (Clinical Specialist Physiotherapist, GGBPS)
Convener/Minute taker
Julie Cuff (Senior Physiotherapist, Milngavie Health Centre)
(Alternate; Marion McLaren Senior Physiotherapist, Drumchapel
Health Centre)
Judith Corcoran (Physiotherapy Team Lead for OP in South
Glasgow)
Judith Reid (Orthopaedic Specialist Physiotherapist, Western
Infirmary, Glasgow) (Alternate; Caroline Hoskins. Orthopaedic
Specialist Physiotherapist, Western Infirmary, Glasgow)

© GGBPS June 2006
43
Fiona Wright (Outpatients Superintendent Physiotherapist,
Western Infirmary, Glasgow)
Dr Mary Newton
Isobel Baxter Clinical Effectiveness Facilitator NHSGGC
Jane Forbes GGBPS team secretary

© GGBPS June 2006
44
Appendix 2 Delphi Study
Breakdown of expert physiotherapy panel
34 physiotherapists – Percentage who replied to round one 84% (N=33)
27 female 6 male
23 senior 1 physiotherapists 10 clinical specialist physiotherapists
Mean of 9.4 years working as an out patient physiotherapist,
Range from 6 to 18 years
Response rates of physiotherapists
Round Number Response Rate
1 97.1% (N=33)
2 76.5% (N=26)
3 73.5% (N=25)
To reach a consensus, a three round sequential questionnaire
called a Delphi Technique took place. The first round asked the
panel to list as many answers to the five questions below (Table
7). Subsequent rounds then asked the panel to rate these options
until the predetermined level of consensus had been reached.
Questions answered by the expert panel
1. CONDITIONS OF LBP YOU CONSIDER SUITABLE FOR
REFERRAL TO PHYSIOTHERAPY
2. FACTORS WHICH YOU FEEL SHOULD INFLUENCE THE
DECISION TO REFER PATIENTS WITH LBP TO
PHYSIOTHERAPY
3. PATIENTS WITH LBP ARE REFERRED TO
PHYSIOTHERAPY TO ACHIEVE WHAT?

© GGBPS June 2006
45
4. APPROACHES THAT YOU FEEL SHOULD BE EMPLOYED
IN THE MANAGEMENT OF LBP ARE?
5. CONDITIONS OF LBP YOU CONSIDER NOT SUITABLE
FOR REFERRAL TO PHYSIOTHERAPY ARE?
Preliminary results of this research are contained above
(Ferguson, Webster et al 2005). Expert physiotherapy clinicians
were asked, via a series of questionnaires, their opinions on
factors associated with the overall management of LBP. Initially
the expert panel were asked to list as many points as they
wished, which they felt were important. Subsequent rounds
asked the panel to rank these options to obtain consensus. The
main findings of this study suggest that in fact expert
physiotherapy clinicians can reach consensus on many aspects
associated with the management of LBP. These points of
consensus do in fact hints at a following of evidence-based care.
And may be seen as differing from the studies previously
published, which have directly asked physiotherapists, which
modalities they employ to manage LBP (Foster et al, 1999;
Gracey et al, 2002). Results suggest an awareness of current best
practice. For example these areas of consensus tended to support
a biopsychosocial approach to physiotherapy management in the
study area reviewed. Active rather than passive treatment
approaches were points of consensus. There were no points of
consensus reached, or even raised as options around many of the
electrotherapy modalities often used by physiotherapists (Pope
et al, 1995; Foster et al, 1999).

© GGBPS June 2006
46
Appendix 3 GGBPS referral pad
How long has the patient had THIS episode of low back pain? ................... weeks .............. days
Is the patient OFF work because of this episode of low back pain? Yes No
Does this patient have low back pain only? Yes No
OR
Does this patient have pain radiating below the knee in addition to
low back pain? Yes No
Imaging not recommended at this stage (see back pain guideline)
Other relevant information .....................................................................................................................
................................................................................................................................................................
................................................................................................................................................................
................................................................................................................................................................
................................................................................................................................................................
................................................................................................................................................................
GREATER GLASGOW BACK PAIN SERVICE REFERRAL FORM
Cord signs? - TREAT AS EMERGENCY
Systemically unwell? · Previous diagnosis of cancer? · Possible infectious cause? · New/altered back pain <20 or >55 years + raised ESR or abnormal FBC or LFTs?
Do not use this form – refer urgently to relevant OP clinic
Patient details Sex M F Name ………………………………………….. Address………………………………………… ………………………………………………….……………………Post Code……………….. DoB………………….Tel. No. ………………. CHI number……………………………………
Practice stamp Practice code......................... Tel No. ......................Fax No.....................

© GGBPS June 2006
47
Referrer’s signature ...........................................Please print name.......................................................
Date ...............................................
Physiotherapy use only below this line.
Outcome Symptoms resolved Spontaneous resolution Referred to orthopaedic surgeon
Referred to DEXA Referred to psychology Referred to community exercise class
Referred for imaging Referred to enhanced back pain class
Discharge comments ………………………………………………………………………………………………..
………………………………………………………………………………………………………………………….
PLEASE POST OR FAX THIS FORM TO YOUR LOCAL PHYSIOTHERAPY SERVICE

© GGBPS June 2006
48
Appendix 4 Acute LBP info sheet
Greater Glasgow Back Pain Service
ACUTE BACK PAIN ADVICE
Back Pain…
• Many people get back pain at some point in their lives. It can be very distressing and you
may feel it limits your daily activities. It is reassuring to know that back pain is very
rarely due to something serious.
• The first few days, or sometimes weeks, tend to be the most difficult to cope with. This
period of time, however, is the most important time to try to follow the advice given.
Things will then be a lot easier longer term.
• Back Pain is normally due to the muscles, ligaments and joints in this area. They have just
been over stressed for some reason and need to be given a chance to work properly again.
The best thing you can do for them is to try to gradually return to normal activity.
How Active Should I Be…
• The most up to date information on Back Pain tells us that we need to keep as active as
we are able to be. It may be that your pain is so much that you feel you need to stay in
bed for a few days. It is very important that this is only one to two days then really try
hard to gradually build up your activity level again. Staying in bed weakens your body
and makes you feel down - avoid this if you can.
Pain Control…
• Sometimes over the counter medication can help greatly. It is very important that you
take your medication as it says on the side of the packet, and regularly. You will be able
to keep much more active if your pain is kept at a constant lower level, rather that letting
it get out of control. If in doubt, talk to your pharmacist or make an appointment with
your Doctor for a review of your medication.
© GGBPS June 2006
49
Scans…
• Up to date medical information tells us that x-rays or other scans are rarely required for
back pain. If an x-ray were to be carried out it would probably show changes in the
surfaces of the joints of the spine. This, thankfully, means nothing other than the fact that
we are continuing to grow a little older.
In General…
• The best person to help your back pain recover quickly is you. Try to balance gradually
returning to your normal activity, including work, with continuing to be aware of not
over stressing your back. General Exercise is also important, if, for example walking
does not aggravate your back pain then gradually try to increase your walking distance
everyday. Your Physiotherapist will be able to give you further advice on this if
required.
GGBPS Jan 2006

© GGBPS June 2006 (Adapted with permission from Linton and Halldén, 1998)
(GGBPS, Updated June 2004)
50
Appendix 5 Modified Linton Questionnaire
THE GLASGOW ACUTE BACK PAIN SCREENING QUESTIONNAIRE
Name____________________________________________________________________________
Address__________________________________________________________________________
________________________________________________________________________________
Date_____________________________________________________________________________
Are you (please tick),
in full-time work in part-time work unemployed retired
a student a full-time carer a home-maker
These questions and statements apply if you have aches or pains, such as back, shoulder or neck
pain. Please read and answer each question carefully. Do not take too long to answer the questions.
However, it is important that you answer every question. There is always a response for your
particularly situation.
1. Where do you have pain? Place a � for all the appropriate sites.
Neck Shoulders Upper back Lower back Leg
2. How long have you had your current pain problem? Tick (�) one.
0-1 weeks [1] 1-2 weeks [2] 3-4 weeks [3] 4-5 weeks [4]
6-8 weeks [5]
9-11 weeks [6] 3-6 months [7] 6-9 months [8] 9-12 months [9]
over 1 year [10]
3. How would you rate the pain that you have had during the past week? Circle one.
0 1 2 3 4 5 6 7 8 9 10
No pain Pain as bad
as it could be
© GGBPS June 2006 (Adapted with permission from Linton and Halldén, 1998)
(GGBPS, Updated June 2004)
51
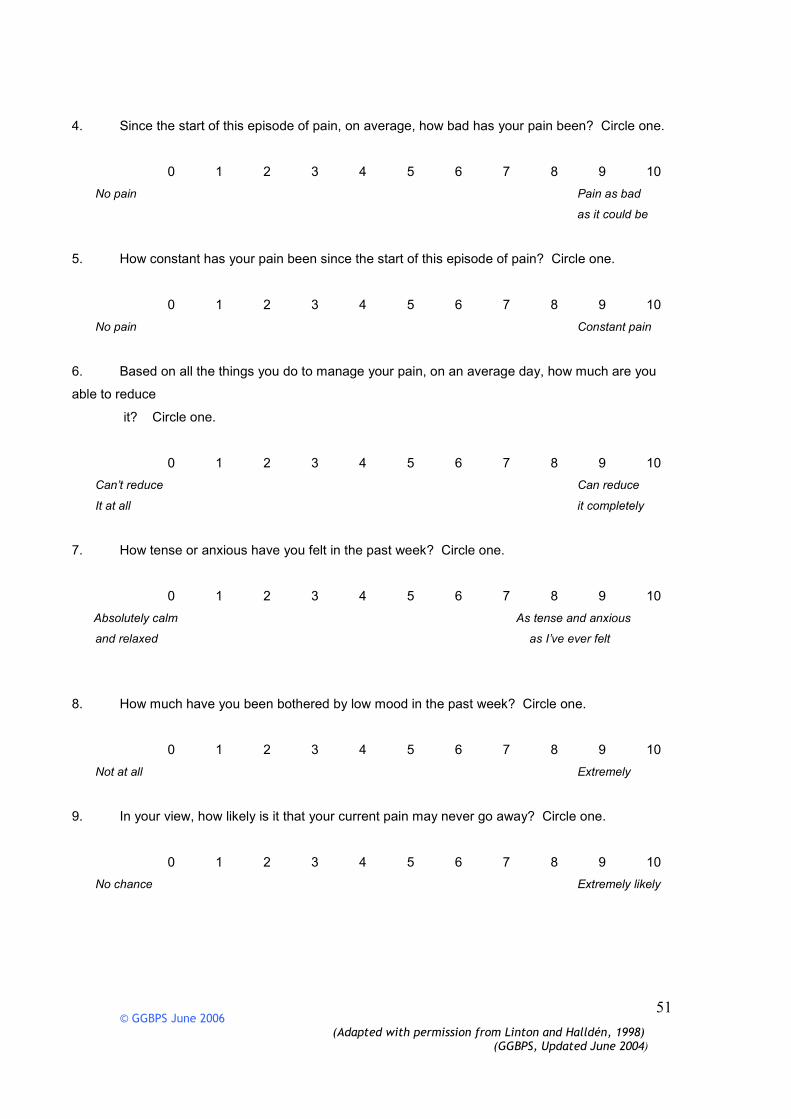
4. Since the start of this episode of pain, on average, how bad has your pain been? Circle one.
0 1 2 3 4 5 6 7 8 9 10
No pain Pain as bad
as it could be
5. How constant has your pain been since the start of this episode of pain? Circle one.
0 1 2 3 4 5 6 7 8 9 10
No pain Constant pain
6. Based on all the things you do to manage your pain, on an average day, how much are you
able to reduce
it? Circle one.
0 1 2 3 4 5 6 7 8 9 10
Can’t reduce Can reduce
It at all it completely
7. How tense or anxious have you felt in the past week? Circle one.
0 1 2 3 4 5 6 7 8 9 10
Absolutely calm As tense and anxious
and relaxed as I’ve ever felt
8. How much have you been bothered by low mood in the past week? Circle one.
0 1 2 3 4 5 6 7 8 9 10
Not at all Extremely
9. In your view, how likely is it that your current pain may never go away? Circle one.
0 1 2 3 4 5 6 7 8 9 10
No chance Extremely likely
© GGBPS June 2006 (Adapted with permission from Linton and Halldén, 1998)
(GGBPS, Updated June 2004)
52
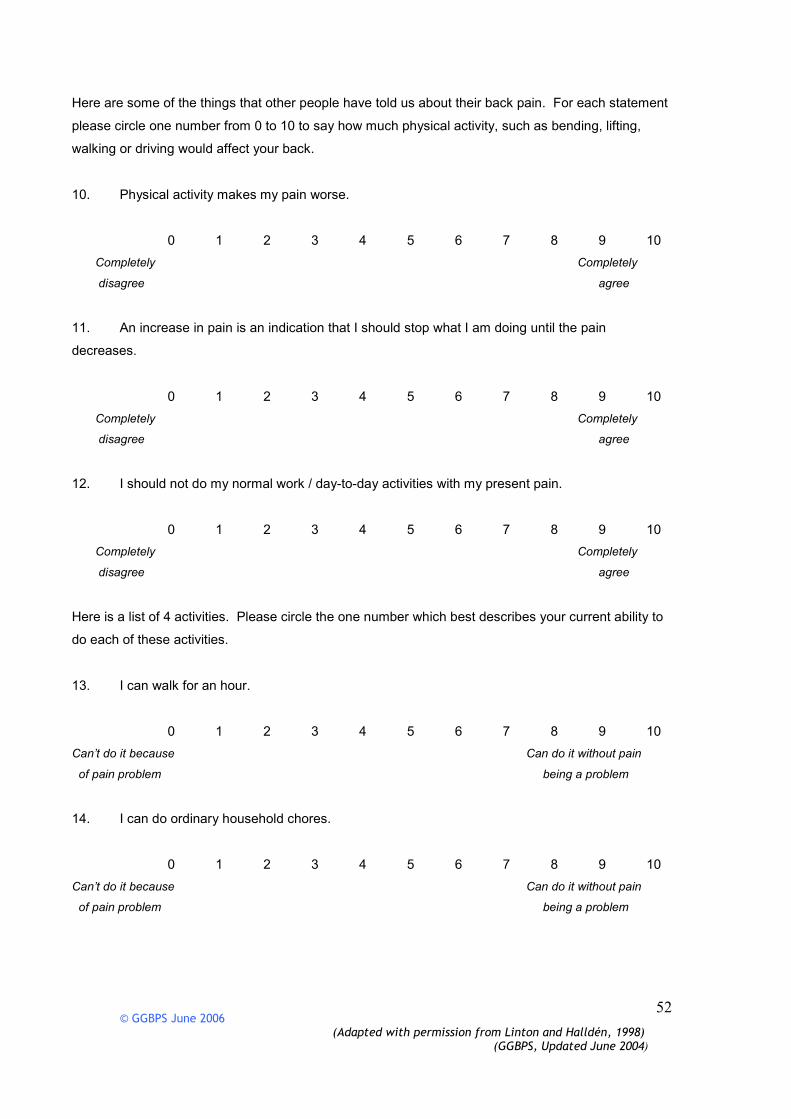
Here are some of the things that other people have told us about their back pain. For each statement
please circle one number from 0 to 10 to say how much physical activity, such as bending, lifting,
walking or driving would affect your back.
10. Physical activity makes my pain worse.
0 1 2 3 4 5 6 7 8 9 10
Completely Completely
disagree agree
11. An increase in pain is an indication that I should stop what I am doing until the pain
decreases.
0 1 2 3 4 5 6 7 8 9 10
Completely Completely
disagree agree
12. I should not do my normal work / day-to-day activities with my present pain.
0 1 2 3 4 5 6 7 8 9 10
Completely Completely
disagree agree
Here is a list of 4 activities. Please circle the one number which best describes your current ability to
do each of these activities.
13. I can walk for an hour.
0 1 2 3 4 5 6 7 8 9 10
Can’t do it because Can do it without pain
of pain problem being a problem
14. I can do ordinary household chores.
0 1 2 3 4 5 6 7 8 9 10
Can’t do it because Can do it without pain
of pain problem being a problem
© GGBPS June 2006 (Adapted with permission from Linton and Halldén, 1998)
(GGBPS, Updated June 2004)
53
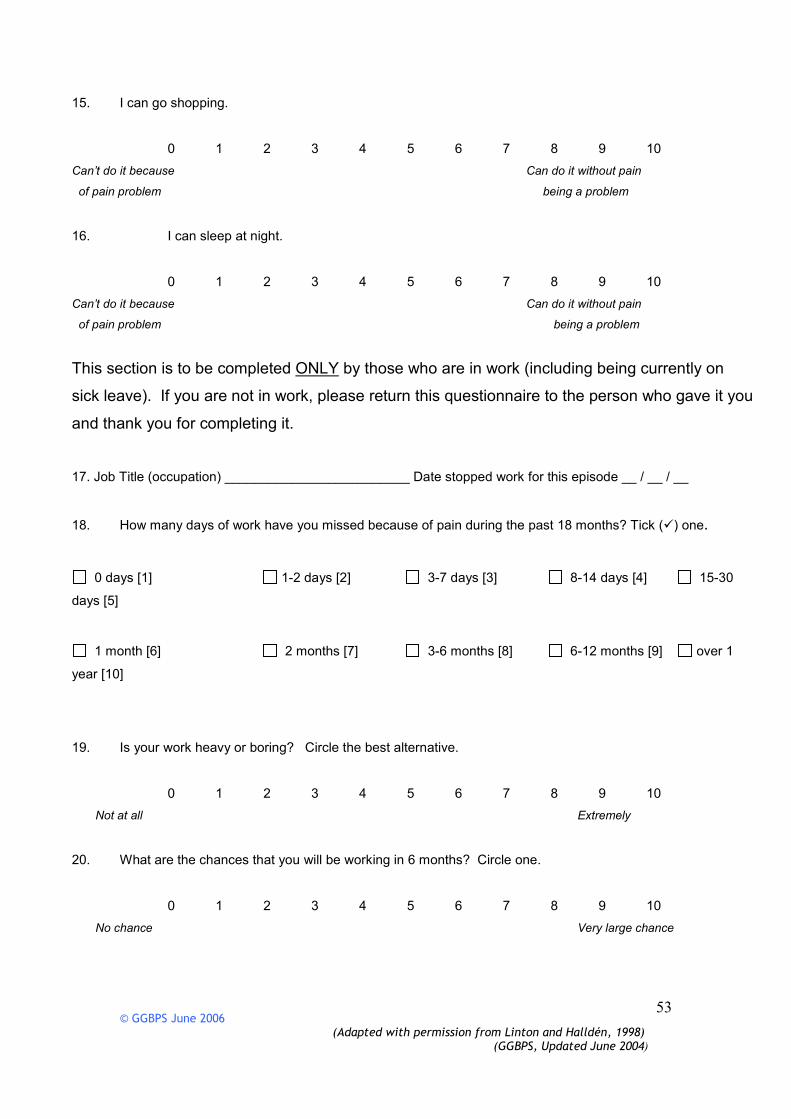
15. I can go shopping.
0 1 2 3 4 5 6 7 8 9 10
Can’t do it because Can do it without pain
of pain problem being a problem
16. I can sleep at night.
0 1 2 3 4 5 6 7 8 9 10
Can’t do it because Can do it without pain
of pain problem being a problem
This section is to be completed ONLY by those who are in work (including being currently on
sick leave). If you are not in work, please return this questionnaire to the person who gave it you
and thank you for completing it.
17. Job Title (occupation) _________________________ Date stopped work for this episode __ / __ / __
18. How many days of work have you missed because of pain during the past 18 months? Tick (�) one.
0 days [1] 1-2 days [2] 3-7 days [3] 8-14 days [4] 15-30
days [5]
1 month [6] 2 months [7] 3-6 months [8] 6-12 months [9] over 1
year [10]
19. Is your work heavy or boring? Circle the best alternative.
0 1 2 3 4 5 6 7 8 9 10
Not at all Extremely
20. What are the chances that you will be working in 6 months? Circle one.
0 1 2 3 4 5 6 7 8 9 10
No chance Very large chance
© GGBPS June 2006 (Adapted with permission from Linton and Halldén, 1998)
(GGBPS, Updated June 2004)
54
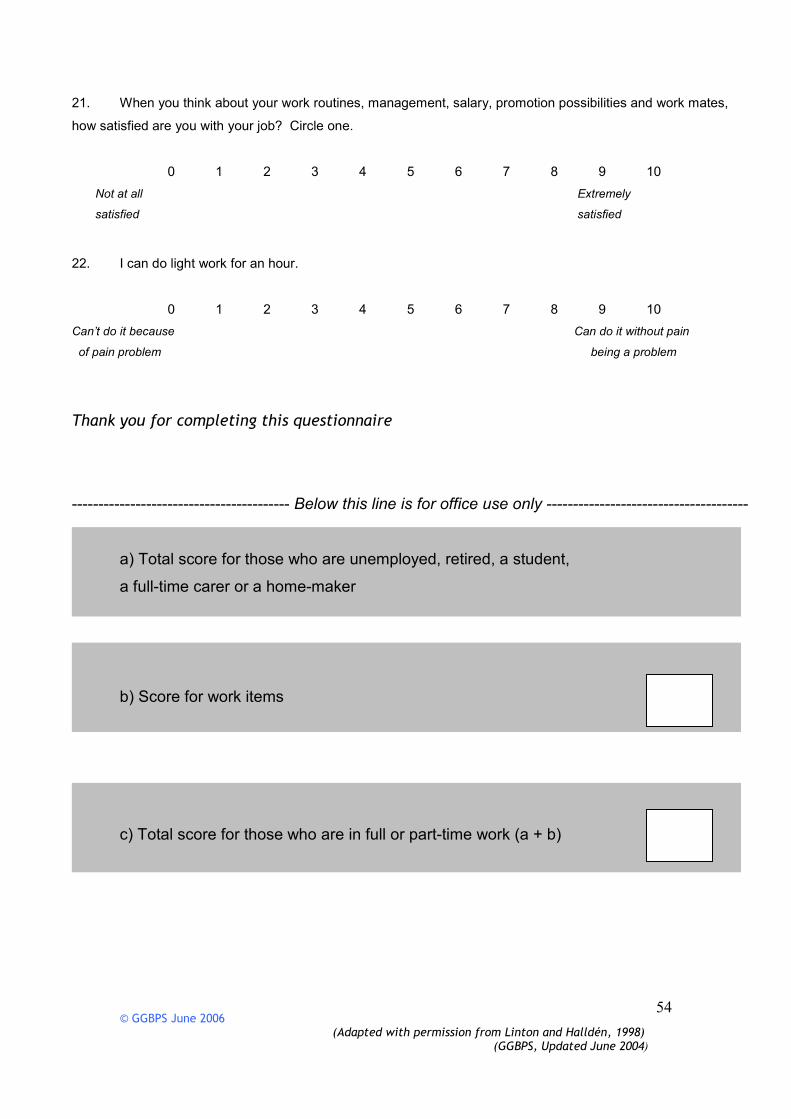
21. When you think about your work routines, management, salary, promotion possibilities and work mates,
how satisfied are you with your job? Circle one.
0 1 2 3 4 5 6 7 8 9 10
Not at all Extremely
satisfied satisfied
22. I can do light work for an hour.
0 1 2 3 4 5 6 7 8 9 10
Can’t do it because Can do it without pain
of pain problem being a problem
Thank you for completing this questionnaire
----------------------------------------- Below this line is for office use only --------------------------------------
a) Total score for those who are unemployed, retired, a student,
a full-time carer or a home-maker
b) Score for work items
c) Total score for those who are in full or part-time work (a + b)

© GGBPS June 2006
55
Appendix 6 Enhanced Back Class referral forms
(1) East
GREATER GLASGOW BACK PAIN SERVICE
REFERRAL FOR ENHANCED BACK CLASS
Refer if patient not making expected progress at 3-6 weeks (or longer up to 3 months)
(still limited in activities, failure to return to work or normal activities, unsatisfactory
response to treatment)
Patient details Sex: F ٱ M ٱ
Name
…………………………………………………………………………………………..
Address
…………………………………………………………………………………………
Post Code …………………………………………………..
DoB ………………………… Tel No: ……………………………………..
CHI number ………………………………………………………………….
GP Name
…………………………………………………………………………………………..
Address
…………………………………………………………………………………………
Post Code …………………………………………………..
Tel No ……………………………………………………
How long has patient had this episode of back pain? …………..weeks ……….months
Yellow flags noted at initial presentation? ٱ NO ٱYES
If yes describe…………………………………………………………………………

© GGBPS June 2006
56
………………………………………………………………………………………..
What management has the patient had so far (physiotherapy, analgesia, relaxation,
acupuncture, etc)? ………………………………………………………………………
…………………………………………………………………………………………
Attitudes and beliefs……………………………………………………………………
…………………………………………………………………………………………
………………………………………………………………………………………….
…………………………………………………………………………………………
Behaviours………………………….…………………………………………………
…………………………………………………………………………………………
…………………………………………………………………………………………
Compensation………………………………………………………………………….
…………………………………………………………………………………………
Diagnosis and Treatment Issues..…………………………………………………….
…………………………………………………………………………………………
Emotions…………………………………………………………………………….
…………………………………………………………………………………………
© GGBPS June 2006
57
Family………………………………………………………………………………….
…………………………………………………………………………………………
Work…………………………………………………………………………………….
…………………………………………………………………………………………
………………………………………………………………………………………….
Other relevant
information…………………………………………………………………………….
…………………………………………………………………………………………
Clinical Specialist Name …………………………………………………………….
Date……………………………………………………………………………………
Contact details…………………………
PLEASE ATTACH GLASGOW ACUTE BACK PAIN SCREENING QUESTIONNAIRE
There are unlikely to be negative consequences of over identification of Psychosocial Yellow Flags so
if in doubt, please discuss with the clinical psychologist or refer anyway. Do not delay referral.
Please post this form to: Dr Martin Dunbar, Clinical Psychologist, Anaesthetic
Department, Stobhill Hospital, 133 Balornock Road, Glasgow G21 3UW. Tel :
0141 201 3005. Email: [email protected]

© GGBPS June 2006
58
(2) South
GREATER GLASGOW BACK PAIN SERVICE
REFERRAL FOR ENHANCED BACK CLASS
Refer if patient not making expected progress at 3-6 weeks (or longer up to 3 months)
(still limited in activities, failure to return to work or normal activities, unsatisfactory
response to treatment)
Patient details Sex: F ٱ M ٱ
Name
…………………………………………………………………………………………..
Address
…………………………………………………………………………………………
Post Code …………………………………………………..
DoB ………………………… Tel No: ……………………………………..
CHI number ………………………………………………………………….
GP Name
…………………………………………………………………………………………..
Address
…………………………………………………………………………………………
Post Code …………………………………………………..
Tel No ……………………………………………………
How long has patient had this episode of back pain? …………..weeks……….months
Yellow flags noted at initial presentation? ٱ NO ٱYES
If yes describe…………………………………………………………………………
…………………………………………………………………………………………

© GGBPS June 2006
59
What management has the patient had so far (physiotherapy, analgesia, relaxation,
acupuncture, etc)? ……………………………………………………………………
…………………………………………………………………………………………
Attitudes and beliefs……………………………………………………………………
…………………………………………………………………………………………
…………………………………………………………………………………………
…………………………………………………………………………………………
Behaviours…………………………………………………………………………….
…………………………………………………………………………………………
…………………………………………………………………………………………
Compensation..……………………………………………………………………….
…………………………………………………………………………………………
Diagnosis and Treatment Issues …………………………………………………….
…………………………………………………………………………………………
Emotions..…………………………………………………………………………….
…………………………………………………………………………………………
Family………………………………………………………………………………….

© GGBPS June 2006
60
…………………………………………………………………………………………
Work…………………………………………………………………………………….
…………………………………………………………………………………………
…………………………………………………………………………………………
Other relevant information…………………………………………………………….
…………………………………………………………………………………………
Clinical Specialist Name …………………………………………………………….
Date……………………………………………………………………………………
Contact details…………………………
PLEASE ATTACH GLASGOW ACUTE BACK PAIN SCREENING QUESTIONNAIRE
There are unlikely to be negative consequences of over identification of Psychosocial Yellow Flags so
if in doubt, please discuss with the clinical psychologist or refer anyway. Do not delay referral.
Please post or fax this form to: Dr David Craig, Chartered Clinical Psychologist,
Dept of Anaesthetics, Southern General Hospital, 1345 Govan Road, G51 4TF
Tel: 0141-201-1658/2385

© GGBPS June 2006
61
Appendix 7 DEXA referral form
Please return to Local Dexa Service
DIRECT ACCESS DEXA SERVICE (DADS) REFERRAL FORM
Name………………………………………… Name…………………………………………………. Address……………………………………… Address………………………………………………. ………………………………………………. Post Code…………………………….. Hospital No….……… Post Code………… Tel No………………………Fax No………………… D.O.B…………………….Tel No……….. CHI No…………………………………….
PATIENT DETAILS GP DETAILS (or stamp)
Steroids >5mg of prednisolone or equivalent per day for more than 3 months Indication…………………………………………………………………..
Age >60 years + menopause aged less than 45 years
Age >60 years + acquired kyphosis
Age >60 years + significant self-reported height loss
Age patient >60 years + family history of a first-degree relative with fracture (>60 at time of fracture)
Age >60 years + family history of a first-degree relative with acquired kyphosis
Age >60 years + family history of a first-degree relative with DEXA confirmed osteoporosis
Depo Provera for > 5 years if DEXA result will influence use of the drug.........................................
Monitoring as recommend by DADS or Bone Mineral Metabolism Clinic or Fracture Liaison Nurse Service (usually 5 years from previous scan). Date of most recent scan ...................................................................................
Men and women over 50 with a fracture at any site (not attributable to RTA nor a fall from above head height) Site of fracture ...................................Date of fracture........................
INDICATE REASON FOR REFERRAL

© GGBPS June 2006
62
Signature of referring person .....................................Designation …...............................................
Address if not GP .......................................................Date …….......................................................
Other current health problems: Current medication:

© GGBPS June 2006
63
Appendix 8 Back to Basics
These sessions employ a range of low impact exercise techniques suitable for those experiencing back pain or those who want to become more active as an easy introduction to exercise.
Available at:
Bellahouston Leisure Centre Friday 5:15 – 6:00pm Gorbals Leisure Centre Wednesday 10:30 – 11:30am Pollok Leisure Centre Thursday 10:30 –11:30am Scotstoun Leisure Centre Tuesday 2:30 – 3:30pm Springburn Leisure Centre Thursday 1:00 – 2:00pm Tollcross Park Leisure Centre Tuesday 11:30 –12:30pm
For more information Please Phone: 0141 287 5913
www.activeglasgow.com

© GGBPS June 2006
64
Appendix 9 Cauda Equina Triage chart
Complete urinary retentionComplete urinary retention
Lack of awareness of bladder fillingLack of awareness of bladder filling
Saddle anaesthesiaSaddle anaesthesiaOverflow incontinenceOverflow incontinence
Saddle anaesthesia can be tested in a less invasive manner by Saddle anaesthesia can be tested in a less invasive manner by
light touch over sacral/medial gluteal area. Testing sphincter light touch over sacral/medial gluteal area. Testing sphincter
tone is not necessary.tone is not necessary.
Usually bilateral sciatica with neurological signsUsually bilateral sciatica with neurological signs
Increased frequency
Incontinence withoutwithoutwithoutwithout saddle anaesthesia
Whole clinical picture to be considered
Table 2: PATIENTS NEEDING TO BE MONITOREDTable 2: PATIENTS NEEDING TO BE MONITOREDTable 2: PATIENTS NEEDING TO BE MONITOREDTable 2: PATIENTS NEEDING TO BE MONITORED
Table 1 : PATIENTS NEEDING URGENT REFERRALTable 1 : PATIENTS NEEDING URGENT REFERRALTable 1 : PATIENTS NEEDING URGENT REFERRALTable 1 : PATIENTS NEEDING URGENT REFERRAL
A&E/Neurosurgery
GGBPS CAUDA EQUINA TRIAGEGGBPS CAUDA EQUINA TRIAGEGGBPS CAUDA EQUINA TRIAGEGGBPS CAUDA EQUINA TRIAGE30/09/04
Pre-existing urological problemse.g. history of incontinence, history of prostate problems, uterine prolapse, previous urology treatment etc. Incontinence due to lack of mobilityIn general these patients are aware of bladder filling but due to severe pain and fear associated with low back pain can find it difficult to reach the toilet in time.Medication causing altered bladder/bowel function
Discuss case with your local GGBPS member if available.If not available contact another GGBPS member.
If patient is to be sent onto A&E or Neurosurgical unit, please make sure you have a letter prepared explaining the clinical presentation
If final outcome is known, complete CES register form and give to your local GGBPS member
Table 3. PATIENTS UNLIKELY TO BE CESTable 3. PATIENTS UNLIKELY TO BE CESTable 3. PATIENTS UNLIKELY TO BE CESTable 3. PATIENTS UNLIKELY TO BE CES
Table 4. GGBPS PREFERRED PATHWAY FOR SUSPECTED CESTable 4. GGBPS PREFERRED PATHWAY FOR SUSPECTED CESTable 4. GGBPS PREFERRED PATHWAY FOR SUSPECTED CESTable 4. GGBPS PREFERRED PATHWAY FOR SUSPECTED CES

© GGBPS June 2006
65
Appendix 10 GGBPS Direct access audit
Greater Glasgow Back Pain Service
Direct Access Referrals Audit
Instructions
Starting on 1st March, 2006, (or your next working day after 1
st March) please complete a form for the next 10 Direct Access
patients you see. Once all 10 forms have been completed please return in envelope provided. If you do not receive 10
referrals by the 31st March, 2006, please return the forms you have completed along with the remaining blank ones.
Many thanks for you help. Isobel Baxter,
Department Public Health, Greater Glasgow NHS Board, Dalian House.
1. About the patient
a. Was the patient:
Do not
write in
this area
Self referred Other – please detail:
Came at GPs suggestion
b. Was the patient triaged:
At drop in clinic Other – please detail:
By telephone
2. Key dates d d m m y y
a. Date of triage 06
b. Date of onset of
symptoms
06
OR
Duration of symptoms:
c. Date of first
appointment
06
3. Your Opinion
In your judgement, was the length of time the patient waited for their appointment:
Any comments:
Too short
About right
Too long
4. Regarding Page 2 of the triage form
a. Was the section on BACK PAIN filled in?
Yes
Most questions completed If the section was NOT fully completed,
About half completed were all the BACK PAIN RED FLAG

© GGBPS June 2006
66
Less than half completed questions completed?
No Yes
No
b. Was the section on PAST MEDICAL HISTORY filled in?
Yes If the section was NOT fully completed,
Most questions completed were all the RED FLAG HISTORY
About half completed questions for BACK PAIN completed?
Less than half completed Yes
No No
5. Which geographical sector are you based in?
North East South East South West

© GGBPS June 2006
67
Appendix 11 GGBPS Management of low back pain audit
Table 1 Non-acute - All cases N=114 NON Acute Always Sometimes Rarely Never Missing
Count % Count % Count % Count % Count %
Manual Therapy 8 7.0% 60 52.6% 37 32.5% 6 5.3% 3 2.6%
Mobilisation 4 3.5% 70 61.4% 32 28.1% 5 4.4% 3 2.6%
Pain management 60 52.6% 46 40.4% 4 3.5% 4 3.5%
McKenzie 18 15.8% 63 55.3% 25 21.9% 5 4.4% 3 2.6%
Active rehabilitation 96 84.2% 16 14.0% 2 1.8%
Graded return to normal activity
89 78.1% 23 20.2% 2 1.8%
Minimal hands on 47 41.2% 54 47.4% 8 7.0% 2 1.8% 3 2.6%
Hands on 5 4.4% 65 57.0% 36 31.6% 3 2.6% 5 4.4%
Postural education 99 86.8% 14 12.3% 1 .9%
Heat 11 9.6% 33 28.9% 40 35.1% 29 25.4% 1 .9%
Ice 2 1.8% 22 19.3% 39 34.2% 50 43.9% 1 .9%
Biofeedback 2 1.8% 13 11.4% 30 26.3% 68 59.6% 1 .9%
Interferential 2 1.8% 17 14.9% 93 81.6% 2 1.8%
Back classes 7 6.1% 96 84.2% 9 7.9% 1 .9% 1 .9%
TENS 1 .9% 48 42.1% 50 43.9% 13 11.4% 2 1.8%
Acupuncture 36 31.6% 42 36.8% 34 29.8% 2 1.8%
Cognitive behavioural therapy
8 7.0% 42 36.8% 18 15.8% 42 36.8% 4 3.5%
Liaise with employers 24 21.1% 48 42.1% 40 35.1% 2 1.8%
Promotion of self-management
106 93.0% 7 6.1% 1 .9%
Bio-psychosocial model 55 48.2% 38 33.3% 12 10.5% 6 5.3% 3 2.6%
Explanation of correct treatment/prognosis
94 82.5% 15 13.2% 1 .9% 1 .9% 3 2.6%
Negotiated approach 74 64.9% 30 26.3% 4 3.5% 1 .9% 5 4.4%
Listening 108 94.7% 5 4.4% 1 .9%
Integrated approach 60 52.6% 44 38.6% 1 .9% 4 3.5% 5 4.4%
Evidence based 61 53.5% 45 39.5% 5 4.4% 3 2.6%
Ortho referral 11 9.6% 82 71.9% 20 17.5% 1 .9%
Psychology referral 1 .9% 35 30.7% 55 48.2% 22 19.3% 1 .9%
Strapping 10 8.8% 43 37.7% 60 52.6% 1 .9%
Manipulation 14 12.3% 39 34.2% 60 52.6% 1 .9%
Exercise 104 91.2% 10 8.8%
Education 112 98.2% 2 1.8%
Advice 112 98.2% 2 1.8%

© GGBPS June 2006
68
Table 2 Acute - All cases N=114 Table 2 Acute
All cases N=114 Table 2 Acute All cases N=114
Table 2 Acute All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
% Count % Count %
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
27.2 5 4.4% 5 4.4%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
27.2 2 1.8% 6 5.3%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
7.0 1 .9% 4 3.5%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
9.6 4 3.5% 5 4.4%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
.9 1 .9% 5 4.4%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
.9 1 .9% 5 4.4%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
12.3 2 1.8% 5 4.4%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
26.3 2 1.8% 7 6.1%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
.9 5 4.4%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
20.2 23 20.2% 5 4.4%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
26.3 39 34.2% 5 4.4%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
23.7 68 59.6% 6 5.3%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
16.7 81 71.1% 5 4.4%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
21.9 12 10.5% 6 5.3%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
35.1 21 18.4% 5 4.4%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
26.3 33 28.9% 6 5.3%

© GGBPS June 2006
69
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
26.3 40 35.1% 8 7.0%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
33.3 39 34.2% 5 4.4%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
.9 4 3.5%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
17.5 9 7.9% 9 7.9%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
7 6.1%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
2.6 1 .9% 9 7.9%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
4 3.5%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
4.4 5 4.4% 10 8.8%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
1.8 5 4.4%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
55.3 22 19.3% 5 4.4%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
42.1 45 39.5% 5 4.4%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
33.3 56 49.1% 5 4.4%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
28.9 59 51.8% 5 4.4%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
4 3.5%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
4 3.5%
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
Table 2 Acute
All cases N=114
4 3.5%