nhs east and north hertfordshire annual report and accounts 2008/09
DESCRIPTION
The third Annual Report from NHS East and North Hertfordshire.TRANSCRIPT

Annual Report and Accounts
2008/09

During the production of this annual report, Pam Handley, Chair of NHS East and North Hertfordshire sadly died following a short illness. The staff and Board of NHS East and North Hertfordshire would like to dedicate this report to Pam Handley in memory of her outstanding contribution to health services in Hertfordshire.

www.enherts-pct.nhs.uk | 3
Contents
Welcome 5About us 9Our history and background How we are managedLocation and type of facilities provided
Keeping Herts healthy 21Planned carePatient experienceMental health and learning disabilitiesMaternity and newbornOur peopleVision and valuesChildren’s healthEnd of lifeStaying healthyChanging services
Quality report 43Operating and financial review 47Our performance 51Strategic objectives and progress Key performance indicatorsAnnual health check
Financial review 61Financial duties and targetsAnalysis of 2008/09 Net ExpenditureFinancial outlookImplementation of International Financial Reporting Standards (IFRS) in 2009/10
Looking to the future 67Governance controls and audit 71The accounts 85Notes to the accounts 96Alternative formats and additional copies 128Contact usAnother language

4 | Annual Report and Accounts 2008/09
Welcome
www.enherts-pct.nhs.uk | 5
WelcomeWe are very pleased to welcome you to our third annual report. We have come a long way since we were established in October 2006. Back then we were struggling to get to grips with a massive inherited debt; working with our residents and stakeholders to agree on the future of health services in Hertfordshire and to improve staff morale following yet another reorganisation.

6 | Annual Report and Accounts 2008/09
How things have changed since those days! Our financial position is now back on track; we are beginning to see real progress with the implementation phase of Delivering quality health care for Hertfordshire and we have developed a vision and set of values for our organisation that we are all working hard to achieve.
As ever things have not stood still in the NHS. Since the two Hertfordshire PCTs were established we have been moving steadily towards separating our “provider arm” from the commissioning part of the organisations. By provider arm we mean those health services delivered directly to patients in their own homes, in community hospitals and health clinics by clinical staff such as community nurses, health visitors and therapists.
Similar changes are taking place across the country and reflect the fact that community services are now seen as central to the modernisation of the NHS with the transfer of services traditionally provided in hospital settings out into the community close to where patients live and work.
As from 1 April 2009 the provider arm of NHS West Hertfordshire and NHS East and North Hertfordshire formally became an “arms length” organisation that is now known as Hertfordshire Community Health Services.
This separation will enable NHS East and North Hertfordshire to concentrate on becoming a world class commissioning organisation, purchasing health care from a range of providers including the private and third (voluntary) sector.
Throughout this report we refer to ourselves as NHS East and North Hertfordshire. This name was adopted in 2009 to better reflect our position as local leaders of the NHS. The change of name is in line with national recommendations and follows
what is happening elsewhere around the country. It does not change our legal status as primary care trusts.
During the year our staff and local people participated in the national consultation which led up to the first ever NHS Constitution. The Constitution establishes the principles and values of the NHS in England. It sets out rights to which patients, public and staff are entitled, and pledges which the NHS is committed to achieve, together with responsibilities which the public, patients and staff owe to one another to ensure that the NHS operates fairly and effectively.
2008 also saw the NHS reach its 60th birthday. As part of the celebrations we held well attended events that took a look at the way key NHS services had changed over the six decades; held a poster competition for local school children and some of our staff attended a service at Westminster Abbey.
Other achievements this year include the expansion of our minor injuries unit at Herts and Essex Hospital, working with local patient and community representatives to choose the preferred site for the new local general hospital in Welwyn Hatfield, increased investment to improve the availability of NHS dental appointments and extended opening hours at a large number of GP practices to make it easier for you to see a GP or nurse at a time that suits you. More detail about these and a range of other developments and new health services can be found within this report.
Finally we would like to pay tribute to the outstanding contribution and dedication of our staff. Whether on the front line delivering services directly to patients or working behind the scenes to ensure that quality services are in place when our residents need them, everyone has a played their part in helping people in Hertfordshire to remain healthy and stay active.
Achievements this year include the expansion of our minor injuries unit at Herts and Essex Hospital, extended opening hours at many GP surgeries, working with local patient and community representatives to choose the preferred site for the new local general hospital in Welwyn Hatfield
Anne Walker Richard Henry Dr Tony Kostick Chief Executive Chair Chair Professional Executive

Everyone has a played their part in helping people in Hertfordshire to remain healthy and stay active.
8 | Annual Report and Accounts 2008/09
About us

www.enherts-pct.nhs.uk | 9
About usNHS East and North Hertfordshire was established on 1 October 2006. We are made up of the former South East Hertfordshire; Welwyn Hatfield; North Hertfordshire and Stevenage; and Royston, Buntingford and Bishop’s Stortford primary care trusts.

10 | Annual Report and Accounts 2008/09
Structure of business, its main services and users
With NHS West Hertfordshire, we hold the vast majority of the NHS budget locally and are the lead health commissioning organisation in the county. Commissioning means that we assess the health needs of our population then use our resources to buy services from hospitals and other providers such as mental health trusts, GPs and dentists to meet those needs. By doing this we can have a positive impact on the health and well-being of the local population. We also fund the cost of medicines and drugs prescribed by GPs and nurse prescribers.
We commission services in a number of different ways:
Directly with providers such as hospitals• Practice based commissioning (PBC) – where GPs, •nurses and therapists can design services that meet the needs of their patients in a particular area. Primary care commissioning – this involves services •provided by GPs, community pharmacists, dentists and optometrists Sharing the commissioning of services - this means •that we join together with Hertfordshire County Council and we both contribute some of our budgets to a partnership who then arrange mental health and learning disability services in the county. We use the majority of this money to commission services from Hertfordshire Partnership NHS Foundation Trust and from Adult Care Services.
Providing careAs we explained in our introduction, on 1 April 2009 our clinical staff together with their support teams became an arms length organisation from NHS East and North Hertfordshire. This organisation is now known as
Our history and backgroundAlthough primary care trusts have been in existence since 2000, our organisation came into being on 1 October 2006 with the merger of four predecessor organisations. There are now 152 PCTs in England, the majority of which are linked to county/unitary council boundaries to ensure better joint working with social care.

12 | Annual Report and Accounts 2008/09
Hertfordshire Community Health Services (HCHS). From October 2009 all HCHS staff will be formally employed by NHS East and North Hertfordshire until their separation into a new organisation is complete.
These moves are in response to national guidance which requires that all PCT direct provider organisations move into a contractual relationship with their PCT commissioning function by April 2009. In addition we will be applying for HCHS to become a Community Foundation Trust (CFT). A CFT is a ‘Public Benefit Organisation’ authorised to provide goods and services to the NHS. It is an independent legal entity, accountable to local people who can become members and governors.
Initially NHS East and North Hertfordshire has to ensure that HCHS can operate effectively as an arms length organisation, and this is the first priority. A detailed action plan is in place to ensure robust internal organisational arrangements are put in place to deliver this organisational change.
Before becoming a CFT, directly provided services would have to operate successfully as an arms length organisation for at least one year.
This separation will mean that the PCT can concentrate on becoming world class commissioners.
Effective commissioning means that we can help people to stay healthy whilst ensuring that we have the right services in place to help people if they fall ill and to assist them with their recovery.
We are managed by a board of non executive and executive directors and share a single management team with NHS West Hertfordshire.
The executive directors on the board are employed by the PCTs. The non executive directors are independent people who work on a part time basis, to make sure that we act in the best interests of the public. (The names of the board directors can be found on the following page).
The board is responsible for ensuring we meet our performance targets and also oversees the work of the Professional Executive Committee (PEC) that covers the whole of Hertfordshire. In 2008/09 the PEC was made up of GPs and other clinical staff who advised us on clinical matters.

www.enherts-pct.nhs.uk | 13

Non
-exe
cuti
ve
Dir
ecto
rs
Ch
airs
Linda Farrant
Non-executive Director
Chris Learmonth
Non-executive Director
Elaine Fox
Non-executive Director
Phil Picton
Non-executive Director
Richard Henry
Non-executive Director
Julia Witting
Non-executive Director
Pam Handley
Chair
Dr Tony Kostick
Joint Chair, Professional Executive Committee
We are run by a Board of non-executive and executive directors and share a single management team with NHS West Hertfordshire.
How we are managed

Exe
cuti
ve
Dir
ecto
rs
The executive directors of the Board are employed by the PCT. The non-executive directors are independent people appointed to make sure that the PCT acts in the best interest of local people. The Board is responsible for the performance of the PCT and also oversees the work of the Professional Executive Committee (PEC).
The joint PEC, which covers the whole of Hertfordshire, is made up of local clinicians who advise on clinical matters.
Anne Walker
Chief Executive
Gareth Jones
Director of Strategic Planning
Pauline Pearce
Director of Public Involvement and Corporate Services
Gloria Barber
Director of Human Resources (HR)
Andrew Parker
Director of Primary Care and Service Redesign
Beverley Flowers
Director of Commissioning
Heather Moulder
Director of Nursing/Interim Chief Operating Officer, HCHS
Jane Halpin
Director of Public Health
Alan Pond
Director of Finance
Clare Hawkins
Interim Director of Nursing

16 | Annual Report and Accounts 2008/09
Location and type of facilities provided
The main facilities and community hospitals from which we provide services and at which our clinical staff are based are:
Bedford Road Health Centre, Hitchin•Bull Plain Clinic, Hertford•Bishop’s Stortford Health Centre•Bowling Road Clinic, Ware•Buntingford Health Centre•Cheshunt Community Hospital•Cuffley Health Centre•Danesbury Hospital, Welwyn•Danestrete Clinic, Stevenage•Hertford County Hospital•Herts and Essex Hospital, Bishop’s Stortford•Hitchin Hospital•Hoddesdon Health Centre•Lister Hospital, Stevenage•Nevells Road Health Centre, Letchworth Garden City•Park Drive Clinic, Baldock•Parkway Health Centre, Welwyn Garden City•QEII Hospital, Welwyn Garden City•Queensway Health Centre, Hatfield•Queen Victoria Memorial Hospital, Welwyn•Royston Health Centre•Royston Hospital•Sawbridgeworth Clinic•South Street Clinic/Church Street Clinic, Bishop’s Stortford•Southgate Health Clinic, Stevenage•St. Nicholas Health Centre, Stevenage•Standon Health Centre•Stanmore Road Health Centre, Stevenage•Waltham Cross Clinic.•

www.enherts-pct.nhs.uk | 17
In addition, services are also provided in other locations such as GP practices and in people’s own homes.
This year saw the adoption of the PCT’s Estate Strategy. The strategy included a summary of the results of the most comprehensive survey of the PCT buildings ever undertaken and clearly set out the short and medium-term objectives for the development of the estate.
The results of the surveys highlighted that the PCT had many elderly buildings that were poorly maintained and no longer suitable for delivering health services in the 21st century.
Well-designed and well-maintained buildings can improve a patient’s experience of healthcare, promote wellbeing and assist recovery. They can also help in recruiting and retaining high quality staff. This is recognised in the East of England Commissioning Framework that requires PCTs to secure year-on-year improvements in the patient experience.
Therefore, this year it has been a priority to improve the quality of the therapeutic environment for both staff and patients and to bring some older buildings in line with the requirements of the Disability Discrimination Act (2005). In the past year, NHS East and North Hertfordshire spent over £1m of capital monies to improve buildings and facilities.
These projects have included:
refurbishment at Bull Plain, Queensway, Bowling Road, •Danestrete and Southgate Clinics internal and external improvements to Danesbury, •Queen Victoria Memorial and Royston Community Hospital upgrade at Tewin Road Wheelchair centre • redevelopment of the Minor Injuries Unit at Herts •and Essex Hospital
In addition, we have spent an additional £500,000 of revenue monies on small works improvements, such as redecoration, concentrating on improving the patient environment which we expect to be reflected in improved Patient Environmental Action Team assessment scores.
Improving the health and safety of staff and patients has been another priority for the PCT during the financial year.
To this end, we have completed:
a £200,000 programme of health and safety •upgrades across the PCT a comprehensive gas boiler servicing and safety •testing programme new Type 2 asbestos surveys for all building• new water safety risk assessments for all buildings •and a programme of works to remove piping dead legs and redundant sanitary ware to reduce the risk of legionella.
In addition, we have:
put in place a new comprehensive solution for the •management of medical devices, including an audit of all current medical equipment. implemented a comprehensive programme of •planned preventative maintenance of all critical plant and machinery. implemented a programme of fixed wire testing for •all buildings created a new web-based database of all relevant risk •assessments with access for staff and external building contractors working onsite
.The estate contributes significantly to the local NHS’ carbon footprint and this year we began the process of reducing carbon emissions.
This has included:
producing energy certificates for all buildings over •1000 m2 ensuring that 25% of our energy is procured from •suppliers who use Combined Heat and Power (a fuel-efficient energy technology) or renewables a commitment to achieving a BREEAM (Building •Research Establishment Environmental Assessment Method) Healthcare score rating of ‘excellent’ and energy efficiency levels of at least 35-55 GJ/ m3 for new builds and ‘very good’ for major refurbishments.
External environmentThe external environment within which the PCT operates is characterised by partnership working. Key to developing appropriate health and social care services are partnerships with the public, carers, other health service organisations, county council, district councils, housing providers, colleges and employment services. This year we have strengthened these partnerships, especially those with users and carers and have developed ways to enable more people to have their say and so influence our work.
We work with a large number of partners including:
Hertfordshire County Council •All Hertfordshire District/Borough Councils •Hertfordshire Constabulary and Police Authority •University of Hertfordshire •A number of Hertfordshire voluntary organisations •Hertfordshire Fire Service •Utility organisations relating to Hertfordshire•
The ways in which we work with these partners are described overleaf.

18 | Annual Report and Accounts 2008/09
Hertfordshire Forward – The countywide LSPHertfordshire Forward is the countywide Local Strategic Partnership (LSP) which brings together key agencies which have an interest in improving the quality of life and well-being of local people.
As a full partner the PCT has played a large part in assisting in the development of the sustainable Community Strategy.
‘Hertfordshire 2021: a brighter future’ is the county’s Community Strategy. It identifies an ageing population, and health and wellbeing as key areas of concern for improvement and describes both long-term objectives (2008–2021) and short-term actions (2008–2011).
The ‘ageing population’ long-term objectives are:
A focus on prevention of illnesses•Helping older people to maintain their independence• Ensuring older people have the opportunities to be •active members of their communities.
The short-term actions include:
Strengthening intermediate care provision•Supporting independent living•Increasing physical activity. •
The ‘health and wellbeing’ long-term objectives include:
Improving health and wellbeing, life chances, •and access to health care.
The short-term actions include:
Increasing levels of physical activity across all age groups•Reducing smoking and obesity in areas of deprivation•Providing greater support to carers.•
The Local Area Agreement (LAA) Hertfordshire Forward is responsible for coordinating the Local Area Agreement (LAA). The LAA is a contract between central and local government designed to improve services to the public by bringing organisations together locally to focus on the issues that matter most to local people.
Hertfordshire’s LAAs are a major part of the PCT’s partnership working. LAA1 finished on 31 March 2009. Delivery of ‘stretch’ targets will generate a significant financial reward to be shared by LAA partners. The Performance Reward Grant is expected to be in the region of £18m and available at the end of 2010.
In LAA1, three of the four ‘Healthier Communities and Older People’s’ (HCOP) sub-group stretch targets are on track to generate the expected Performance Reward Grant.
Hertfordshire’s LAA2 was signed off by the Government Office East of England (GO-East) in June 2008. Five of the National Indicators chosen by Hertfordshire are being delivered under the HCOP theme, which is aligned with the ‘Health and Wellbeing’ and ‘An Ageing Population’ themes of Hertfordshire’s Sustainable Community Strategy, Hertfordshire 2021: ‘A Brighter Future’ and with the PCTs’ Health Inequalities Plans.
The five HCOP indicators are:
NI 8 Physical activity •NI123 Stopping smoking •NI125 Achieving independent living for older people •NI135 Carers receiving needs assessment • NI141 Percentage of vulnerable people achieving •independent living
Working with the voluntary sectorThe voluntary sector plays an important role in promoting healthy lifestyles, disease prevention, supporting the elderly and disabled to live healthy lives in their own homes and in a variety of ways. The PCT commissions a number of
services from the voluntary sector such as Carers in Herts, Age Concern Herts, Herts Health Action for the Homeless, The Crescent and Herts Hearing Advisory Service. Funding is also available through the Joint Commissioning team for initiatives such as Viewpoint and other mental health and learning disability groups.
Community safety partnershipsCommunity safety partnerships are linked to the LAA ‘Safer and Stronger’ strand and set additional local targets based upon the findings of their strategic assessments. In addition to targeting crime and anti-social behaviour, community safety partnerships seek to address the underlying societal problems caused by alcohol and drugs, and the various elements that cause fear of crime in communities. Reducing both crime and fear of crime has an impact on physical and mental health, which helps to promote independent living for vulnerable groups of people and helps to build social cohesion. Children and young people’s partnershipHertfordshire Children’s Trust Partnership, supported by District Children’s Trust Partnerships (DCTPs) supports delivery of the five Every Child Matters outcomes. They are set to become key vehicles to support the delivery of children’s services countywide and in local districts.
Working with vulnerable groupsThe PCT recognises the importance of providing appropriate services for vulnerable people, minority ethnic communities, travellers, homeless people, migrants (including asylum seekers), and people with learning disabilities or mental health problems. The PCT works closely with partnership groups on their specific issues and links closely with relevant communities. NHS East and North Hertfordshire was a partner in events organised for the Polish community, aimed at informing them about services available and listening to their needs. These events were held in Royston and Hatfield. NHS East and North Hertfordshire is a key member of the Hertfordshire Asylum Seekers Multi Agency Forum which is

www.enherts-pct.nhs.uk | 19
a partnership that seeks to improve services for groups of migrant workers and asylum seekers.
Partnership working on planning for emergenciesThe PCT is an active member of Hertfordshire Resilience, the county’s local resilience forum, and many of its sub-committees, including the Health Services group which it chairs. The PCT takes part in local risk assessment work and emergency planning exercises, covering emergencies such as flooding, train crashes, London evacuation and radiation.
The PCT also plays a lead role in county-wide pandemic flu planning and preparedness, supporting partners in the development of multi-agency arrangements and ensuring that rigorous plans are in place including not only the health sector, but also local authorities, police, fire, utilities and voluntary organisations.Partnership working with utility companiesThe PCT works closely with suppliers of gas, electricity and water as well as the Highways agencies in its emergency planning roles. In recognition of the particular effect water supply has on public health, we have developed a strong relationship with Three Valleys Water.
Sustaining a healthy futureHerts NHS Environment Group, which includes all major NHS organisations in Hertfordshire and representatives from the county council and district councils has helped individual NHS organisations undertake environmental improvements in their own workplaces including recycling, waste control and green transport.
The group is a member of Hertfordshire Environment Forum (HEF) and we have developed good links with county and district council officers on various environmental projects. The group also produces the annual Hertfordshire ‘Quality of Life’ report, which has won plaudits worldwide.

20 | Annual Report and Accounts 2008/09

www.enherts-pct.nhs.uk | 21
KeepingHertsHealthy

22 | Annual Report and Accounts 2008/09
Planned careNHS East and North Hertfordshire, together with NHS West Hertfordshire, are the lead health commissioning organisation in the county. This means that, alongside NHS West Hertfordshire, we are responsible for planning and improving local NHS services for the residents of Hertfordshire and ensuring that we help people to keep fit and healthy. To do this we work closely with GPs, dentists, optometrists, community pharmacists, the county and district councils, hospitals and the mental health trust to secure the best possible healthcare and health services for over one million residents in the county. Here are some of our key achievements over the past year.
Longer GP surgery opening hours and more choice in your healthcarePatients tell us they want more convenience and choice from the service they receive from GPs - for instance, being able to see a doctor in the evening, at weekends or when you’re away from home.
Extended hoursWe understand that ill-health doesn’t just strike during office hours. That is why we have been working with local GP surgeries to ensure that many stay open for longer, giving you the opportunity to see a doctor early in the morning, during the evening, or at the weekend.
This means that now 39 GP practices (around 62%) in East and North Hertfordshire now offer appointments outside normal working hours, including more than 20 which open on a Saturday morning.
Fast, easy access to your doctorWhen you need to see a doctor quickly, you should be offered an appointment within two working days. All GP surgeries should also allow you to book an appointment more than two days in advance, if you prefer.
New health centre provides extra GP services A new kind of GP surgery – Spring House Medical Centre is now open in Welwyn Garden City, close to the QEII Hospital.
Open from 8am to 8pm, 7 days a week, every day of the year, Spring House is open to anyone who wants to use it – and you don’t need to be registered with the centre to use its services.
Open to everyone living, working or visiting east and north Hertfordshire (not just Welwyn Garden City), Spring House Medical Centre offers:
Pre-booked appointments to people registered with •the centre Pre-booked appointments to people not registered •with the centre, and A walk-in service (no appointment needed) •
You can contact the centre on 01707 294354 or find out more online go to: www.springhouse.nhs.uk
Shortest waits ever get thumbs-up from patientsVirtually all patients in Hertfordshire are now seen, diagnosed and start their hospital treatment within 18 weeks – the shortest waits since NHS records began. *
Anne Walker, Chief Executive of NHS East and North Hertfordshire, said: “This is excellent news for Hertfordshire patients, who are now having their treatment faster than ever before. This challenging target has been met and exceeded thanks to the close partnership between the PCTs and the hospital trust.”
Results from a recent Department of Health survey also show that the majority of Hertfordshire patients reported having good experiences when being referred for hospital treatment:
68% of patients were happy with how long they had •to wait for treatment Two-thirds of patients found it easy to make their •first hospital appointment (either by phone, online or within their GP practice) and 91% who were offered a choice of where to be treated, were able to go to their preferred hospital 96% of patients felt that they were treated with •respect and dignity during their treatment.

www.enherts-pct.nhs.uk | 23
Anne Walker said: “The feedback from this survey shows that in general, local people are having a positive patient experience in hospital. Our focus for the coming year will be on those areas we know can be improved, including reducing the number of cancelled outpatient appointments, reducing waits in clinics and helping more patients to choose the hospital they want to be treated at”.
* The 18 Week target levels are 90% for admitted patients and 95% for non-admitted patients to allow for patients who do not want to start their treatment within 18 weeks and patients for who need further tests before treatment begins.
Choose your hospital!Patient choice was introduced in April 2008, which means that if your GP refers you to a hospital you can choose which hospital you go to. You can choose to go anywhere in England where your treatment is being offered, funded by the NHS. This includes all NHS hospitals as well as some private hospitals. Patient choice allows you to make decisions about your care based on your personal circumstances and what is most convenient for you. Making your choice is simple. Your GP has access to information on all the different hospitals which offer the care you need. You can discuss your options with your GP and make a decision together. Once you have made a
decision, your appointment can be booked then and there on a day and time that’s convenient for you. Alternatively, if you would like some time to think your options through, your GP can give you a unique password and booking reference which you can use to make your own appointment online or via an appointment line.
As a patient you may want to consider a number of factors when deciding which hospital to choose, including:
Your own personal experience of a particular hospital • The location – whether it is easy for you to get to, •close to work, or near family and friends Reputation of the hospital •The hygiene standards and MRSA infection rates •Waiting times for your care • Good facilities at the hospital e.g. parking and •disabled facilities.
More information is available at www.nhs.uk/choices Hotline to NHS dental appointmentsGetting an NHS dental appointment has been made easier this year with the launch of a new dental appointments helpline.
Hertfordshire residents can telephone 01707 369645 or email [email protected] to find out the practice nearest to where they live or work that is offering NHS dental appointments.
Since its launch in January 2009, the dental appointments helpline has received more than 600 calls from people in East and North Hertfordshire (to April 2009).
“It’s a popular misconception that NHS dental appointments are rare - but that is simply not the case”, says Jane Robinson, Dental Lead at NHS East and North Hertfordshire.
“We really want to make sure that good quality and accessible NHS dental treatment is available locally for all who need it. Across the county, there are 204 dental practices offering approximately 47,000 appointments every month. So there really are plenty of appointments out there.”

24 | Annual Report and Accounts 2008/09
NHS Constitution launchedLocal patient groups in Hertfordshire got a preview of the first ever NHS constitution last summer, when we sought their views on the contents of this historic document.
We passed on people’s comments to the Department of Health and were pleased to be given the opportunity to witness first hand the official launch of the constitution at a Downing Street reception in January 2009.
Heather Aylward from the PCTs’ public engagement team attended the launch. She said: “This landmark document will put in one place what patients, staff and the public can expect of the health service. It is designed to safeguard the future of the NHS, making sure it continues to be relevant to the needs of patients, the public and staff for many years to come. We were delighted that the NHS in Hertfordshire was able to be present at this historic event.”
The constitution sets out patients’ rights as well as their responsibilities to look after their own health, and also contains a range of pledges to patients, public and staff, which the NHS is committed to achieving.
The NHS Constitution can be found at: www.dh.gov.uk/nhsconstitution
Birthday celebrations for the NHSYoungsters from a Hitchin primary school had a rare encounter with a 1950s Daimler ambulance when it parked up on their playground during a special day to mark the 60th anniversary of the NHS.
Pam Handley, Chair of NHS East and North Hertfordshire, visited Wilshere-Dacre Junior School in July 2008 to explain to Year 3 and 4 pupils about how the health service has changed since 1948.
During the event, children met a modern day paramedic, designed posters which will be displayed in health centres and clinics across the county, and released 60 balloons, one for every year of the NHS. Talking to the publicThroughout the past year patients and other members of the public have been giving us their views on existing services and helping us develop new ones.
A Stakeholder Forum – independently chaired, with senior representation from councils, voluntary sector and patient groups is supporting the local NHS through its major service changes. Since its inception the forum has given its views on several key projects including hospital transport, how intermediate care services will develop and the PCTs’ commissioning priorities for the next five years. You can find our more about service changes on page 40.
The independent Hertfordshire Local Involvement Network (LINk) was also launched in 2008 as a way for everyone in the community – from individuals to voluntary groups to:
Say what they think about local health and social care •services – what is working and what is notInfluence how services are planned and run•See how their feedback helps services to improve•
The LINK has focused its work on issues such as access to dentists, the location of family planning clinics and cancer screening. More information on the LINk can be found at: www.communityvoicesonline.org/
Local patient groupsA number of local patients are also now supporting the practice based commissioning group in Welwyn Hatfield. This group of eight GP surgeries in the area are responsible for buying and designing health services that best meet the needs of local residents. During the past year the group has begun working with GPs and consultants to introduce some gynaecology services in local surgeries. This means that many women won’t have to go to hospital for their outpatient appointments.
Over the next year we aim to establish a patient group to support each practice based commissioning area – 13 in total across the county.
Patient experienceWe believe in putting people at the centre of everything we do and believe that understanding and improving the health care experiences of patients, families and carers is fundamental to providing safe and effective care. Over the past 12 months, a number of initiatives have been put in place locally and nationally to improve patient experience.

www.enherts-pct.nhs.uk | 25
Mental health and learning disabilitiesWe work alongside Hertfordshire County Council to make sure mental health and learning disability services are in place for all who need them. Here are some of our achievements from the past 12 months.
BrainBox – unlocking the secrets of mental health
We are proud of our innovative and committed approach to caring for people with mental health and learning disabilities. Last year, adults and children with anxiety, anger and addiction issues all benefited from using the BrainBox – the unique creation of our Emotional and Mental Health Advisor Deborah Bone. Deborah explains more:
What inspired you to develop the BrainBox?I wanted a tool that I could use with young people to help deal with anger and anxiety and help remove the stigma surrounding accessing mental health services.
How does it work?The BrainBox uses recycled computer parts to show how our bodies react in stressful situations. It demonstrates to children, young people and adults how the response is triggered, how neuro connections are re-routed and why children are not always to blame for their actions but can do something about them.
How effective is it?It has proved to be very popular, especially with boys, and has been found to make a real difference to their emotional and mental health and wellbeing.
Who uses it?The BrainBox can be used for anger management and to treat anxiety and addiction issues in both children and adults. Best of all, it can be used in the classroom by educational professionals who do not have advanced mental health training.
It comes complete with a manual and DVD, which includes a demonstration of the BrainBox in action. Around 25 organisations across East and North Hertfordshire are now using the BrainBox as part of a new wellbeing project in schools.
PCT is award winning!Deborah Bone and her colleague Julie Nash picked up a prize in the 2009 Innovation Competition organised by Health Enterprise East. Their Sticking Plasters for Children’s Souls story book won in the ‘Publications and Training Aids’ category. Aimed at five to 11 year olds, this contains poems and stories written to help with healing, learning and
personal transformation. The stories deal with a number of mental health issues and can be used by parents, teachers or children themselves.
Talking therapies expanded across county People with mental health problems in Hertfordshire are getting faster access to more treatment choices, thanks to an expansion in our ‘Improving Access to Psychological Therapies’ (IAPT) programme.
‘Talking therapies’ have already been offered to more than 1,000 people with mild to moderate mental health issues in Letchworth and Stevenage. Each patient is given a fast-track service which involves an assessment within 10 days of the initial referral, and a choice of therapy sessions in their GP surgery, over the phone or even online. This allows patients to fit therapy around their busy lives and helps some patients to remain in work while undergoing treatment.
Initial project findings show that more than 90% of patients are satisfied with their psychological treatment; many preferring ‘talking therapy’ to being dependent on anti-depressant medication. In addition, waiting times for psychological treatment of anxiety and depression have fallen to just 25 days where the IAPT service is available. Thanks to the success of the initial pilot, talking therapies will now be available across the county.
One patient, a retired senior manager suffering from agoraphobia, received psychological therapy on the IAPT programme following unsuccessful drug treatment. After 10 sessions with a psychologist, and attending an anxiety management group, the patient was discharged. In a letter, he wrote:
“Our sessions have encouraged me to build on the lessons from the anxiety management course and the ‘targets’ you have set me have given me something to aim for. All of this has helped me to improve and gradually increase my quality of life. I aim to make the most out of it – thank you.”
26 | Annual Report and Accounts 2008/09
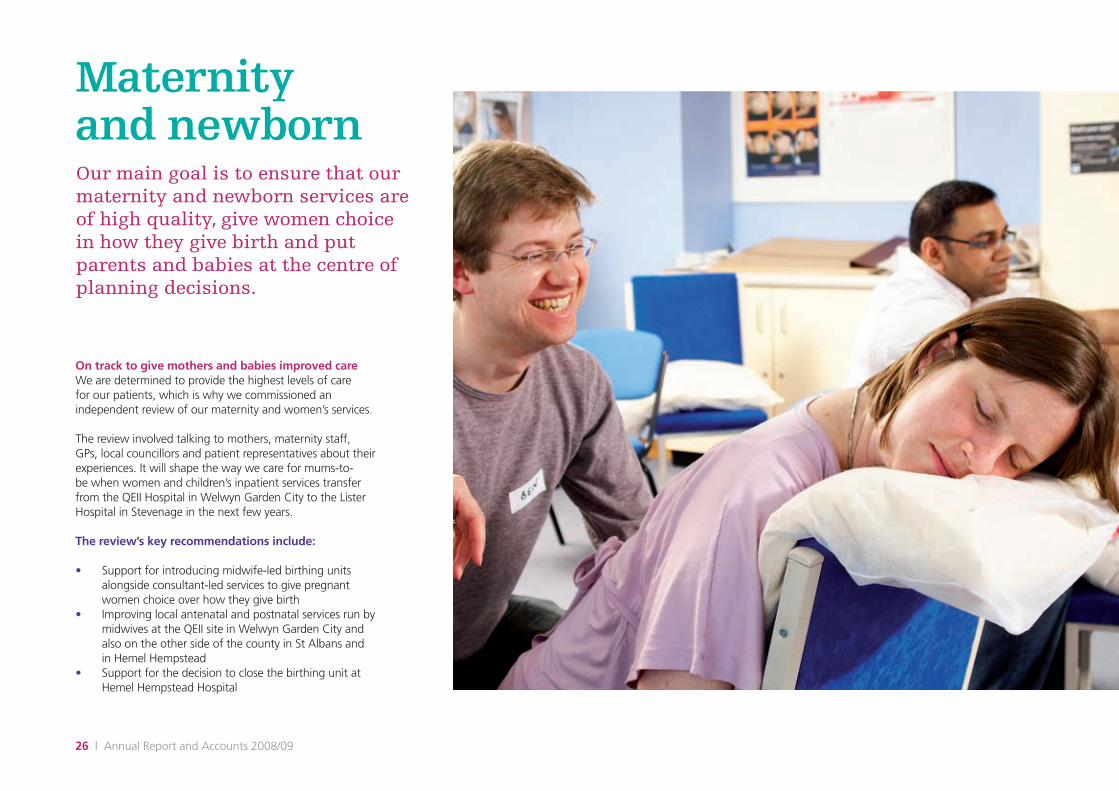
Maternity and newbornOur main goal is to ensure that our maternity and newborn services are of high quality, give women choice in how they give birth and put parents and babies at the centre of planning decisions.
On track to give mothers and babies improved care We are determined to provide the highest levels of care for our patients, which is why we commissioned an independent review of our maternity and women’s services.
The review involved talking to mothers, maternity staff, GPs, local councillors and patient representatives about their experiences. It will shape the way we care for mums-to-be when women and children’s inpatient services transfer from the QEII Hospital in Welwyn Garden City to the Lister Hospital in Stevenage in the next few years.
The review’s key recommendations include:
Support for introducing midwife-led birthing units •alongside consultant-led services to give pregnant women choice over how they give birth Improving local antenatal and postnatal services run by •midwives at the QEII site in Welwyn Garden City and also on the other side of the county in St Albans and in Hemel Hempstead Support for the decision to close the birthing unit at •Hemel Hempstead Hospital

www.enherts-pct.nhs.uk | 27
Anne Walker, Chief Executive of NHS East and North Hertfordshire, said: “Our aim is to provide women with access to safe, high quality maternity care for themselves and their babies. It is now our responsibility to make sure that services are developed that meet these needs and which provide the right balance of quality, choice, safety and accessibility for mums-to-be.”
Listening to local mothersMaternity services are some of the most widely used and important services delivered by the local NHS. Ensuring that the views and experiences of mothers help shape these services is the idea behind our Maternity Service Liaison Committee (MSLC). In Hertfordshire there are two local MSLCs – one in East and North Hertfordshire and one in West Hertfordshire.
Members of the group include people who are currently or have recently used maternity services, as well as NHS staff such as doctors, midwives, GPs and paediatricians.
The committee performs an important role, ensuring that families from all parts of the community have an opportunity to comment on services, suggesting which areas could benefit from improvement, and providing advice to the community on childbirth.
Melanie Peeke is a parent and a member of the East and North Hertfordshire MSLC. She says: “I have been involved with the local MSLC for about four years. I must admit that at first, the thought of attending meetings with consultants, midwives and NHS managers was a little daunting but they couldn’t have been more welcoming. My thoughts and opinions are taken as seriously as anybody else’s and I believe
that ‘lay’ members make a valuable contribution to the development of local maternity services. Women talk about their birth experiences to their friends so why not share them with the people who can make a real difference?”
If you are interested in joining the MSLC please contact NHS East and North Hertfordshire on [email protected]

Our peopleOur staff are our greatest asset and we are proud of the first class services they deliver for patients. We have in place an organisational development programme to make sure that our organisation is somewhere people want to come and work and where they feel their contribution is recognised. During the past year we have held our first long service awards ceremony for staff where we celebrated those staff who have committed their careers to the NHS. We also hosted our first staff awards to say thank you to those staff who have gone the extra mile.
Applauding our people
From nurses and therapists to office administrators, our staff are working hard to provide excellent health services. Last year we launched the ‘Applauding Our People’ awards as a way of recognising the individuals and teams who go the extra mile to help patients.
Nominations for awards came from patients, staff and managers. Here are the deserving winners:
Patient Excellence
Winner: Jane Scanlon, Community MatronNominated by a colleague, Jane was recognised for being a true patient advocate. She said: “I feel really overwhelmed to win as there were so many outstanding applicants and I hope this award will bring greater recognition for the matron service.

Achievement in Learning
Winner: Karen Kelly, Senior Occupational Health NurseKaren was rewarded for studying for a degree in Occupational Health Nursing - a qualification which was above and beyond what her role required. She is now regularly putting forward innovative ideas to improve the quality of services. Karen said: “It was lovely to have my achievements recognised in such a positive way. All too often no news is good news, with regards to performance and development, so it was great that the opposite was the case this time.”
Unsung Hero
Winner: Dot Lutkin, Communications OfficerDot was recognised for being enthusiastic, dedicated to her role and for her personal commitment to improving communication within the organisation. She said: “I have always enjoyed my job and working with staff. The fact that I’ve received an award has inspired me to encourage people in everything they do.”
Team of the Year
Winner: Intermediate Care Team East (based in Welwyn) This team was nominated for its tireless efforts to provide outstanding care to patients. Staff were praised for their ability to alleviate both the clinical and social problems that can prevent older people living in their own homes.
Innovation
Winner: Patient Advice and Liaison (PALS) Team and Heather Aylward, Patient Engagement Manager The team was recognised for its work with prisoners at the Mount Prison in Bovingdon. A team member said: “The PALS team were happy and surprised to be nominated – it was morale boosting and was great to feel appreciated.”
Individual of the Year
Winner: Pam Gledstone, Professional Lead – Health Visiting Pam received support from many different colleagues for this award. She has been described by her staff as “vigilant, reliable, sensible, approachable and knowledgeable”, and described by her managers as someone who always gives her best and puts patient care at the forefront of all her endeavours.
Pam said: “I started as a student nurse in 1964 and have worked continuously within the NHS, mainly as a community health visitor. I have seen many changes and reorganisations but I can honestly say I still look forward to coming to work and have enjoyed all my 44 years in the NHS, and especially within Hertfordshire.“

30 | Annual Report and Accounts 2008/09
Vision and values
In 2006 the merger of eight PCTs in Hertfordshire into two, severely disrupted traditional lines of communication and ways of operating. This led to low staff morale and uncertainty about the future. In order to help establish a new identity for our organisation and to make it somewhere people wanted to come and work, we introduced and developed our first vision and values.
Our Vision
Our ambition is to be a high performing PCT, recognised by our people, patients and partners as commissioning outstanding care and improving the wellbeing of all.
Our Values
Caring• I care about everything I do for colleagues, patients and partners. Confident• I am trusted to make informed and timely decisions and have the confidence to see them through. Creative• I have the freedom to bring forward new ideas and solutions Learning• I take responsibility for my personal development as part of our learning culture Fun• I play my part in making this an enjoyable and rewarding place to work Proud• I am proud to work for NHS East and North Hertfordshire
More than 2,000 of our staff have taken part in events we have hosted to introduce our vision and values during 2008/09. These events have given staff the opportunity to meet the executive team and get to know colleagues from across the organisation.

www.enherts-pct.nhs.uk | 31

32 | Annual Report and Accounts 2008/09
Children’s healthWe are committed to improving the health and wellbeing of children in Hertfordshire and responding to their particular needs. We want to make sure that services are child-friendly and we want to take their own views into account when planning services
Where children take centre-stage
In 2008, Hertfordshire reached its ambitious aim of having 50 Children’s Centres across the county with the opening of a centre in Sawbridgeworth.
Children’s Centres are facilities for local communities, where under-fives and their families can receive a range of services under one roof.
Offering day care for babies and children, a variety of parenting programmes and clinics, centres give help to parents and children alike. All of our centres reflect the needs and concerns of local people. Reflecting the large number of parents who work, centres in our towns have well established day care programmes, whereas centres in more rural parts of Hertfordshire may have more of an emphasis on signposting parents to local services.
Children’s Centres are managed by a variety of statutory and voluntary agencies. Ensuring that families receive care that is seamless and joined-up, staff work alongside many other agencies including Children’s Schools and Families, schools and community groups.
By 2010 there will be a Sure Start Children’s Centre in every community in Hertfordshire – a total of 82 centres serving children and families from birth, right through to when children start school.
Healthy eating starts young
If national trends continue, 90% of today’s children could be overweight or obese by 2050. That shocking statistic is the motivation behind the Department of Health-led campaign Change4Life
These days, ‘modern life’ can mean that we’re a lot less active. With so many opportunities to watch TV or play computer games, and with so much convenience and fast food available, we don’t move about as much, or eat as well as we used to. Which means that 9 out of 10 kids today could grow up with dangerous amounts of fat in their
bodies. This can cause life-threatening diseases like cancer, diabetes and heart disease - so it’s really important that we do something about it.
It can be hard these days to live a happy, healthy life but Change4Life can help. After all, none of us are perfect. The way we live in modern society means a lot of us, especially our kids, have fallen into unhealthy habits. But we can make small changes that make a big difference.
If you join Change4Life you will receive lots of helpful information, games, tools, tips and a free welcome pack designed to help you to give your family a happier, healthier future.
You can join Change4Life by visiting www.nhs.uk/changeforlife or by phoning 0300 123 4567* for a chat. Offices are open 9am – 6.30pm, Monday to Friday.

www.enherts-pct.nhs.uk | 33
End of lifeBeing diagnosed with cancer or a life-limiting illness is challenging for the patient but also for the people who love and care for them. Our team give people living with cancer and their families and carers, the support and help they need to improve their quality of life.
Dignity until the end
Our palliative care team comprises Macmillan nurses, consultants and nurse specialists who work with patients and their families mainly in their own home but also in care homes and community hospitals. They work alongside our local hospices.
They provide complex specialist care and advice regarding symptom control, act as advocates and help patients discuss the choices they have and the extremely sensitive subject of where they want to die. They help families prepare for the death of their loved one and encourage patients and their families to talk about their feelings as well as more practical issues such as the type of funeral the patient would prefer. They can offer a calm and practical presence at what is a very emotional time.
Making sure that patients who need palliative care receive an effective and supportive service is a key priority for NHS East and North Hertfordshire.
That is why we have carried out a review of our end-of-life care and identified specific goals which will help us improve the provision of these important services and the way in
which people access them. These goals include giving patients greater choice about where they receive care, ensuring that patients can be admitted to a hospice seven days a week, and delivering a 24-hour community nursing service across the county. We will also implement a scheme that will improve the care given to patients in their final few days.
We are also working closely with other agencies including cancer and other clinical networks, patients and carers associations, social care services and the private sector to help ensure that the care of terminally-ill patients is as seamless and coordinated as possible.

34 | Annual Report and Accounts 2008/09
Staying healthy
NHS East and North Hertfordshire offers a wide range of primary care services that can help you lead a healthier life, including help to quit smoking
Be a quitter!
Did you know that stopping smoking is the one single thing you can do to dramatically increase your chances of living longer?
If you want to quit the habit and you live or work in Hertfordshire, you’re in the right place! We have a broad range of local support services in locations and at times to suit you. From one-to-one clinics to drop ins at your nearest pharmacy, we’ve got the help that’s right for you.
In 2008/2009 the Hertfordshire Stop Smoking Service (SSS) helped 1,768 people in East and North Hertfordshire to give up smoking.
Once you stop smoking, your body’s self-healing mechanism kicks in very quickly – and marks the beginning of a remarkable journey:
After 8 hours…Your blood oxygen levels return to normal and your chance of having a heart attack falls
After 24 hours…Carbon monoxide leaves your body. Your lungs start to clear out mucus and debris
After 48 hours…Your body is now nicotine free and your sense of taste and smell should have improved
After 2-12 weeks…Circulation is improved throughout your body. It’s easier for you to walk and exercise now
After 3-9 months…Your lung capacity has increased by 5-10%. Coughing, shortness of breath and wheezing are all steadily diminishing
After 5 years…You now have only half the chance of getting a heart attack compared to a smoker
After 10 years…The chance of you getting lung cancer is now half that of a smoker. Your chances of having a heart attack are now the same as someone who’s never smoked
John Greaves successfully quit using the Hertfordshire Stop Smoking Service “Until I met Liz from the Hertfordshire Stop Smoking Service I had no intention of giving up. I met her by chance at an event where I was working and arranged to meet her again for a chat about quitting. I remember thinking on my way to our first meeting that there was no way I would be giving up but actually during that journey I smoked my last cigarette. Liz and the service supported me to kick a 32 year smoking habit and I have now been a non smoker for 20 weeks. If I can do it then anyone can.”
To find out more visit: www.hpherts.nhs.uk or call 0800 389 3998.

www.enherts-pct.nhs.uk | 35
Immunisation
Immunisation is a way of protecting yourself against serious disease. Once you have been immunised, your body is equipped to fight that disease if you come into contact with it. NHS East and North Hertfordshire is responsible for making sure that local vaccination programmes are in place.
MMR The MMR vaccination provides protection against measles, mumps and rubella (German measles). MMR is given to children aged 12 to 15 months and again before starting school at three to five years of age.
Measles, mumps and rubella are viruses that are easily passed on by close contact, coughing and sneezing. All three are often mild illnesses but can be potentially more serious. If contracted during pregnancy they can both cause miscarriage, and rubella can cause babies to be born with heart problems, deafness, blindness or other major problems.
The uptake of the MMR vaccination in Hertfordshire is slightly lower than the national average. There were 37 confirmed cases of measles in Hertfordshire during 2008. It is important that parents immunise their children against measles, mumps and rubella to help prevent measles becoming more widespread.
Dr Jane Halpin, Director of Public Health at NHS East and North Hertfordshire, says: “Some parents are worried that MMR is linked to autism or bowel problems. Researchers in many countries have not found evidence of any link between MMR and these conditions. I understand the anxieties that
this issue generates but parents need to be aware of how important it is for their children to receive this vaccination.
For further information on the MMR jab, speak to your health visitor or GP, or call NHS Direct on 0845 4647 or go to: www.immunisation.nhs.uk/vaccines/mmr
FluFlu, or influenza, can be a serious illness, contributing to the deaths of between 3,000 and 4,000 people each year in the UK.
People aged 65 and over are particularly at risk, even if they are otherwise healthy. Flu jabs are also strongly recommended for anyone with a chronic illness, such as diabetes and asthma, and for people living close together in residential care homes.
You are eligible for a free flu jab on the NHS if you:
are aged 65 or older•live in a long-stay residential home•care for people who are elderly or infirm• have a history of chronic illness including heart •conditions, kidney disease, chronic asthma or diabetes that requires medication have lowered immunity to infection due to HIV, •steroid medication or cancer treatment.
Last winter, almost 77% of people aged 65 and over had a free flu jab in East and North Hertfordshire, as did a further 46% of people identified as ‘at risk’ of contracting flu.
Immunisation is a way of protecting yourself against serious disease. Once you have been immunised, your body is equipped to fight that disease if you come into contact with it

36 | Annual Report and Accounts 2008/09
For more information visit www.immunisation.nhs.uk/vaccines/flu or www.nhchoices.nhs.uk
Swine fluSince the emergence of a new kind of flu virus (swine flu) in Mexico this year, NHS East and North Hertfordshire has been implementing its plans to make sure we are well placed to manage pandemic flu in Hertfordshire.
We have worked closely with colleagues at the Health Protection Agency, the Strategic Health Authority, neighbouring NHS organisations, local councils and the emergency services so that our approach is co-ordinated, robust and involves all relevant bodies.
Pandemic flu is different from ordinary flu because it is a new flu virus that appears in humans and spreads very quickly from person to person worldwide.
Because it’s a new virus, no one will have immunity to it and everyone could be at risk of catching it. This includes healthy adults as well as older people, young children and those with existing medical conditions.
The best way to protect yourself and stop the spread of flu viruses is to:
cover your nose and mouth when coughing or •sneezing, using a tissue when possibledispose of dirty tissues promptly and carefully • wash your hands with soap and water to reduce the •spread of the virus from your hands to face, or to other people.
An easy way to remember this is: Catch it, Bin it, Kill it.
HPVNearly three-quarters of cervical cancers could soon be eliminated thanks to a new vaccination programme.
The HPV, or ‘human papilloma virus’ vaccine is now being offered to all 12 and 13-year-old girls in school year 8 across Hertfordshire.
The vaccine protects against the two types of HPV which cause more than 70% of cervical cancers.
“New cases of cervical cancer have been falling for years thanks to the national cervical cancer screening programme,” said Dr Hilary Angwin, Public Health Consultant for Women and Children’s Services at NHS East and North Hertfordshire.
“The HPV vaccination should ensure the number of women who get cervical cancer in Hertfordshire will fall significantly in the years to come.”
While the vaccine protects against the most dangerous types of HPV, it will still be necessary for girls, like their mothers, to take part in the NHS cervical cancer screening programme once they are old enough.
Girls who are currently aged 17 or 18 will also be offered a vaccination. From August 2009 there will be a catch-up vaccination programme for girls aged 15 to 18 (school years 10 and 11), so that by summer 2011, all girls in Hertfordshire up to the age of 18 will be protected.
Latest figures show that uptake of the HPV vaccine by 12-13 year olds living in East and North Hertfordshire is broadly in line with the national average at around 80%. Uptake by 17-18 year olds is slightly higher than the national average at around 55% although this is still lower compared to the younger age group. This difference is because the vaccination programme for the school aged children is carried out in schools. The older age group receive their vaccination in health clinics. We plan to increase uptake by the older age group next year by offering the vaccination in school and in clinics.

www.enherts-pct.nhs.uk | 37
Further information is available at www.immunisation.nhs.uk/Vaccines/HPV or by calling the national HPV helpline on 0845 602 3303.
cleanyourhands campaign
Determined to reduce the number of healthcare-related infections, NHS East and North Hertfordshire has joined the National Patient Safety Agency’s ‘Cleanyourhands’ campaign.
‘Cleanyourhands’ staff champions have been identified at each of our sites, and are responsible for encouraging all staff, patients and visitors, to clean their hands regularly. So far, informal feedback has been very positive and we believe the campaign will play an important role in reducing infection amongst patients.
Healthy weight, healthy lives
Few parents like to admit that their child is overweight, many simply don’t realise what a healthy weight should be. We want to raise awareness amongst parents about what a healthy weight is and how they can help their family to achieve it.
We have distributed 55,000 leaflets to parents of primary school children, explaining the link between a healthy weight and its importance for the future health of children.
We have also made sure that more than 10,000 children in reception class (aged 4 to 5 years) and year 6 (aged 10 to 11years) have been weighed and measured in 2007/08, as part of the National Child Measurement Programme. We have told parents the results and given them information to make the first small changes in lifestyle.
We also understand that information must be clear. That’s why we have developed an easy-to-use toolkit, which every GP, health visitor and school nurse in the east and north
Hertfordshire area will use to talk to parents about healthy eating and fitness for their family.
By working closely with all our partners, and coordinating the support available to children and their families, we are determined to meet our target of halting the year-on-year rise in obesity among local children, helping families make healthier choices along the way.
Bowel Cancer Screening
People across east and north Hertfordshire are benefiting from bowel cancer screening. The bowel cancer screening home kits have so far helped to save the lives of 30 people in its first year.
Under the NHS-funded scheme, nearly 37,000 screening packs were sent to people, aged between 60 and 69, across east and north Hertfordshire.
Faye Beard, one of East and North Hertfordshire NHS Trust’s specialist bowel cancer screening sisters, said: “We’ve been really busy over the last year and there’s been a lot of support for the screening programme.
“We’ve been working really hard to get the message out there about the programme but unfortunately there are still a lot of people who don’t know what it is and how beneficial it could potentially be for them.
“We also hear lots of people saying they haven’t got any symptoms, are fit and well and don’t see why they have to do anything. But the fact is that there are often no symptoms of bowel cancer when it’s at such an early stage, which is why the screening test kits are designed to detect early traces of bleeding from a cancer that are invisible to the naked eye.

38 | Annual Report and Accounts 2008/09
“Basically, the earlier bowel cancer is caught, before it has chance to spread to other parts of the body, the easier it is to cure.”
Susan Marsden, screening manager at NHS East and North Hertfordshire, says: “The NHS offers a range of cancer screening programmes including bowel, cervical and breast cancer screening. Routine screening aims to detect disease whilst it is in its early stages. The earlier we can start treating patients, the more likely they are to make a good recovery. We strongly recommend that people take advantage of invitations to attend for screening.”
Bowel cancer is the third most common cancer in the UK and claims the lives of more than 16,000 people every year. But research has shown that regular screening reduces the risk of dying from bowel cancer by 16%.
The programme is part of a nationwide initiative led by the Department of Health. From March 2008, the local NHS has offered every resident aged between 60-69 free screening once every two years to catch the disease before it has a chance to take hold. Although not part of the national programme, anyone over the age of 70 can request a home screening kit by contacting 0800 707 60 60.
Could you spot a stroke? You could save a life
Every five minutes someone in the UK suffers a potentially deadly stroke. That’s more than 100,000 people every year, 1,000 of whom are under 30 years old.
It’s an undeniably gloomy picture but it doesn’t have to be this way. The quicker a stroke is spotted and treated by specialists, the better the chance of survival and recovery.
Learning the FAST test could save your life, or the life of a loved one.
FAST stands for:
Facial weakness - can the person smile? •Has their mouth or eye drooped?Arm weakness - can the person raise both arms?• Speech problems - can the person speak clearly and •understand what you say?Time to call 999•
Stroke is definitely an emergency and if you suspect one, you should dial 999 immediately.
Dr Declan O’Kane from the QEII Hospital in Welwyn Garden City agrees. He says: “If someone fails the FAST test, you must call 999. Swift action can prevent further damage to the brain and help someone make a full recovery. On the other hand, delay can result in death or major long-term disabilities, such as paralysis, severe memory loss and communication problems. Everyone should remember to think FAST!”
You can find out more about how to spot the symptoms of a stroke and read about how other people have coped with a stroke by visiting www.nhs.uk/stroke
Helping patients to help themselves
We have also put in place a number of projects for patients to help them gain the confidence and the skills to manage their long term conditions themselves.
Over the past year we have run self management courses for patients with Diabetes and Multiple Sclerosis.
People with sight difficulties have also been taking part in the ‘Eye Can Help’ programme run by local charity Hertfordshire Society for the Blind in partnership with NHS East and North Hertfordshire.
The courses, held in Hertford and Letchworth give patients the knowledge, skills and confidence to live with their long term eye conditions. Further courses are planned across the county including some for patients with dual sight and hearing difficulties.

www.enherts-pct.nhs.uk | 39

40 | Annual Report and Accounts 2008/09
Decision on site of new local general hospital
In July 2008, NHS East and North Hertfordshire approved the QEII Hospital site in Welwyn Garden City as the location for a new local general hospital.
This decision was supported by local patient and community representatives and follows a rigorous financial appraisal to select the most suitable and sustainable site for the new development.
Work on redeveloping the QEII site is expected to start at the end of 2011 with the new hospital ready to open by the end of 2013.
Full steam ahead for Lister Surgicentre
In April 2009, plans were approved for the creation of a state-of-the-art, multi-million pound Surgicentre at the Lister hospital site in Stevenage.
The Surgicentre will serve patients from across east and north Hertfordshire and south Bedfordshire who require routine surgery, along with some short stay operations.
The three-storey, high-tech building will have six operating theatres including two with highly specialised ventilation systems needed for orthopaedic joint replacements, a dedicated eye theatre; and around 26 short-stay inpatient beds. The Surgicentre will also house day surgery, outpatient and ophthalmology services, including urgent eye clinic facilities.
It is estimated that the Surgicentre will treat around 15,000 NHS patients a year for common procedures such as hip and knee replacements, hernia repairs and cataracts.
Changing services
NHS East and North Hertfordshire and NHS West Hertfordshire have an ambitious strategy to improve and modernise acute care services across the county. Over the past year, significant progress has been made towards our goal of providing better levels of primary and community care closer to where people live and also investing in services such as mental health. Some of the milestones include:

www.enherts-pct.nhs.uk | 41
Nick Carver, Chief Executive of East and North Hertfordshire NHS Trust said: “Patients are always the driving force behind any decisions we make and the development of the new Surgicentre is excellent news for them. By helping us to separate planned and emergency surgery, this exciting new facility should mean that our patients experience much shorter waiting times and fewer cancelled operations.’
Clinicenta will finance the building of the Surgicentre, with NHS East and North Hertfordshire purchasing clinical services on behalf of local people.
Construction work will begin shortly with the centre expected to open in March 2011.
Major boost to maternity services
In 2008, further steps were taken towards a major £15.4m expansion of the maternity unit at the Lister hospital in Stevenage, which will create state-of-the-art midwife and consultant-led units.
The project will expand the Lister’s current maternity unit and will be designed with new delivery rooms – some of which will have water birth facilities – and neonatal cots. The new facility, is expected to assist more than 5,500 births every year.
The unit will enable the hospital trust to bring together all of its specialist maternity staff on to a single site, providing women with more choice in how they give birth. These choices may include home birth, a midwife-led birth, or specialist care in a consultant-led unit. Whichever option is chosen, women will continue to receive their ante and post natal care close to where they live, just as they do now.
Urgent Care Centres
The county’s first 24-hour, 7 days a week Urgent Care Centre (UCC) opened at Hemel Hempstead Hospital in October 2008. It is designed to treat the majority of people who have an illness or minor injury that is not life threatening.
Latest figures show that the average waiting time is just 20 minutes and the majority of people are seen, treated and discharged within two hours.
Brand new Urgent Care Centres for Hertford and Cheshunt will open in autumn 2009, St Albans in March 2010 with more to follow across the county over the next 3 years.
Elsewhere in Hertfordshire
Changes are also afoot in neighbouring West Hertfordshire. In 2008/09, progress has included the successful transfer of AandE services from Hemel Hempstead to Watford General Hospital and agreement has been reached on plans for a new local hospital for Hemel Hempstead.

42 | Annual Report and Accounts 2008/09
Quality Report

www.enherts-pct.nhs.uk | 43
Quality ReportThis year is the first year the PCTs have had to write a quality report as part of the annual report. The introduction of a quality report was proposed as a first step towards the introduction of quality accounts which are to be a statutory requirement from 2009/10. The PCTs quality report focuses on the clinical services provided by our provider services.

44 | Annual Report and Accounts 2008/09
The drive for improvements in quality are firmly embedded in the strategic plans of the PCT and the 3 components of quality: safety, clinical effectiveness and patient experience all come together to inform the board, clinicians, patients and the public about the services we provide.
In 2008/09 we continued to develop our competencies as World Class Commissioners and with that saw the separation of our provider services into Hertfordshire Community Health Services (HCHS). It is vital in taking forward the development of HCHS we do not lose focus on the need to ensure a high quality service is delivered to our population.
As commissioners of services we continue to implement the Delivering quality health care for Hertfordshire (DQHH) programme with increasing emphasis on the need to ensure where it is clinical effective and safe to do so we bring care closer to home.
Quality improvement priorities for 2009/10
In determining our priorities we are building on the work already in place to improve quality and considered areas which fit with our agreed strategic plans. The quality priorities relate to the services provided by HCHS.
We consider our quality priorities to be:
Delivery of same sex accommodation•healthcare associated infections•safeguarding children•developing a systematic approach to patient experience. •
Quality overview 2008/09
Patient experienceThe patient experience has remained at the core of the clinical governance activity undertaken in year. Work undertaken in the first six months of the year supported the transfer of the complaints process from the Hertfordshire PCTs central team to the HCHS team.
For the year April 2008 to March 2009 a total of 159 complaints were received over the whole year. In addition 142 compliments were received from October 2008 to March 2009. Follow up with services by a named patient experience lead and implementation of the complaints training programme has assisted improved engagement by service leads in the management of complaints and this programme will be continued as part of the annual training programme.
Some changes in practice following investigation of complaints include:
Introduction of revised patient group directions for •Genito Urinary Medicine, reaffirming safe clinical practice. Introduction of specialist speech and language •therapists in children’s services, improving access for children with specific needs. A review of access to the complaints process to improve •access for patients wishing to respond via email. Implementation of specific training and managerial •support for identified bed based intermediate care services to raise awareness of privacy and dignity and communication needs of patients in this care pathway.
To read the full quality report please visit our website: www.enherts-pct.nhs.uk
www.enherts-pct.nhs.uk | 45
GP access In response to the commitment to offer patients choice in their healthcare and longer GP surgery opening hours the PCTs have worked closely with GP practices to commission extended hours services across the county. As a result 39 GP practices (around 62%) in East and North Hertfordshire now offer appointments outside normal working hours, including more than 20 which open on a Saturday morning.
Dental servicesThe PCTs are committed to ensuring that good quality and accessible NHS dental treatment is available locally for all who need it. Opinion Research Services (ORS) was commissioned by the two PCTs to undertake a telephone survey of residents’ attitudes and opinions about dental care in Hertfordshire. In particular, the PCTs were interested to know whether the perception that patients were unable to obtain an NHS dental appointment was true.
The survey results reveal that for most people visits to the dentist are part of their regular routine with most making dental visits at least yearly. However, there is some evidence to suggest that younger people and those in full time work are less inclined to make regular check-up visits with a tendency to visit only when seeking treatment. On the other hand, part time workers and retired people find the time to make regular visits to the dentist.
Views about how easy or difficult it is to access NHS appointments were split between respondents with about two fifths saying it is easy to get appointments and the same proportion saying it is difficult. This is in spite of the fact that awareness of NHS dentists within 12 miles of home is relatively high at 68%.
Overview of performance against the key national priorities from the operating framework and the DH core standards
National targets and regulatory requirements 2008-2009
The Trust has fully met the CQC core standards and national targets
23/24
18-week maximum wait from point of referral to treatment (non-admitted patients)
West Herts PCT 98.1%East and North Herts PCT 98.8%

46 | Annual Report and Accounts 2008/09

www.enherts-pct.nhs.uk | 47
Operating & financial review
The year ending 31 March 2009 has seen NHS East and North Hertfordshire build on its financial recovery of the preceding year, and marks an important shift in our direction of travel.
48 | Annual Report and Accounts 2008/09
Overview
NHS East and North Hertfordshire is in financial balance and stable. While we are never complacent, we are no longer restricted by debt or deficit, and can look forward to a year of continued financial security which is good news for our patients, staff and the wider health and wellbeing agenda.
From April 2009 our clinical services became an ‘arms-length’ organisation –Hertfordshire Community Health Services. We are now aiming for excellence in local services by developing our role as strong and ambitious commissioners.
We are making good progress on the world-class commissioning programme – a government-backed scheme aimed at transforming the way health and care services are commissioned. In undertaking this challenging reform of the way we work, NHS East and North Hertfordshire is seeking to deliver a more strategic and long-term approach to commissioning services, with a clear focus on improving the health of our population and delivering improved health outcomes. This is guided by our ambitious commissioning strategy which will frame our vision for more patient-centred care, delivered in a variety of community settings.
Responsibility for the healthcare budget lies with us, and we are determined to carry out our commissioning role with precision, creativity and the needs of patients at the fore.
Agreement has been reached to consolidate emergency and acute care on the Lister Hospital site in Stevenage, and on the same site, moves are afoot to create an elective care centre, known as a Surgicentre. This new centre will mean less disruption for patients because planned operations will be separate from emergency treatment, reducing the likelihood of operations being cancelled due to unexpected emergencies.
Our out-of-hours GP service has been launched, offering access to GP services between 6.30pm-8am, and all day at weekends. The service is fulfilling a vital role in bringing healthcare provision closer to the community.
A fresh approach to the treatment of people with mental health problems has been agreed which seeks to consolidate inpatient provision while strengthening our community-based services. Specialist care will be provided at sites in Hemel Hempstead, Welwyn/Hatfield and Stevenage; all designed to complement a more proactive and community-based approach to treating people with mental health needs.
As ever, our staff have proved instrumental in our achievements. Over the past 12 months, their dedication to the health and wellbeing of the people of East and North Hertfordshire has helped the PCT consolidate its financial recovery and embed new ways of working.
To help support them during these changing times, we developed a staff organisational development programme
called ‘Making the Difference’. Many of our staff from across departments have taken part in workshops, appraisals and other learning opportunities to equip them with the skills and knowledge needed to deliver our ambitious vision.
The past year has also seen the implementation of our ‘Reward and Recognition’ scheme which aims to acknowledge formally the hard work and commitment of our staff. During four awards ceremonies in November and December, the achievements of staff members were recognised with many also receiving awards for long service.
While we have much to be proud of and certainly more challenges ahead, ensuring that local people play a greater role in shaping health services is one of our key strategic objectives. Going forward into 2009/2010, as we develop better and more innovative ways of delivering healthcare, we will seek to further strengthen our patient and public involvement processes enabling the people of East and North Hertfordshire to have their say in the way services are provided.


50 | Annual Report and Accounts 2008/09
www.enherts-pct.nhs.uk | 51
Our Performance
Operating and financial review

52 | Annual Report and Accounts 2008/09
Strategic objectives and progressThe PCT’s objectives for 2008/09 are shown below.
Objective Progress
The PCT, together with Practice Based Commissioning Groups (PBC) lead the local NHS
Clinical leadership roles agreed- PBC commissioning plans agreed-
Implement ‘Delivering quality health care for Hertfordshire’ 38 practices open for extended hours- New ‘out of hours’ GP and dental contract in place covering all of Hertfordshire- Contract awarded for new Spring House Medical Centre in Welwyn Garden City. - County workforce group in place-
Building and sustaining the reputation of the PCT and local NHS Communications strategy agreed-
Develop an effective and engaged workforce ‘Making the Difference’ programme rolled out to all staff- Reward and Recognition scheme in place- Long service awards and staff awards scheme now in place- Significant increase in staff appraisals and personal development plans-
Continue to develop the Boards and Committees, to ensure that robust arrangements are in place for all aspects of integrated governance
Performance Management Framework agreed- Integrated Governance Strategy updated and agreed- Board 360- o Review undertaken
Deliver on local and national targets and standards See section on Key Performance Indicators on page 54-
Become increasingly effective commissioners Commissioning Strategy agreed- Joint Strategic Needs Assessment completed alongside social care colleagues- Primary Care Balanced Scorecard developed and published to help patients understand how their practice - is performingQuality metrics built into contracts and monitored- Key indicators agreed for GPs, dentists and pharmacists- First assessment under new World Class Commissioning programme completed- Organisation Development Programme to support World Class Commissioning developed.-
Ensure patients and the public can contribute effectively to improving health and shaping health services
Patient and Public Involvement Strategy agreed- Action plan developed and on track-
Ensure further development of Practice Based Commissioning PBC group-based needs assessments complete- Better information given to PBC groups- Increased financial support and advice to PBC groups- Template for review of business cases agreed- Fast track process for business cases in place-

www.enherts-pct.nhs.uk | 53
Objective Progress
Sustain financial recovery Financial targets met- Priorities for investment agreed in Commissioning Strategy - See Financial Review section for further details
Ensure our Provider arm delivers services to patients that are personalised, effective and of high quality
Patient Experience Group established- Revised privacy and dignity toolkit being rolled out to staff- Complaints and incident reporting processes in place- Plan in place to reduce waiting times- Staff vacancy rates reduced-
Build capacity and capability within PCT Provider Services to enable their progression towards arms- length status
Organisation Development Programme in place- Contract agreed between Provider Services and PCT-

54 | Annual Report and Accounts 2008/09
Key performance indicatorsIn addition to finance, performance in the NHS is judged by measuring a large number of non-financial targets. In the 2008/09 operating framework, the Department of Health described five key priority areas which had been developed through listening to what patients and the public believe are the most important issues. Performance or progress on measures which contribute to delivery of the key priority areas is shown below.
The national key priority areas for 2008/09 were:
1 Improving access, eg:
maximum 18 weeks waiting time for referral •to treatment improving access (including at evenings and •weekends) to GP servicesbetter access to genito-urinary medicine (GUM) clinics• maintaining 98% operational standard for accident •and emergency departments
2 Keeping adults and children well, improving their health and reducing health inequalities, eg:
helping people to stop smoking •tackling childhood obesity•increased screening for chlamydia •reducing waiting times for cancer treatment•
3 Improving cleanliness and reducing healthcare-associated infections, eg:
Methicillin Resistant Staphylococcus Aureus (MRSA)•Clostridium Difficile (CDiff) •
4 Improving patient experience, staff satisfaction, and engagement
5 Preparing to respond in a state of emergency, such as an outbreak of pandemic flu
Performance in these priority areas
1 Improving access Maximum 18 weeks waiting time for referral to treatmentThroughout 2008/09 the PCT has been working with service providers to reduce the length of time patients wait for treatment in consultant-led services.
From December 2008, the targets are:
for patients needing admission, 90% to wait no more •than 18 weeks from referral by their GP to treatment for patients treated without admission, 95% to wait •no more than 18 weeks from referral by their GP to treatment.
In December 2008, NHS East and North Hertfordshire achieved these targets, with 91% of patients requiring admission being seen and treated within 18 weeks; and 96% of non-admitted patients being seen and treated within 18 weeks. Performance against these targets was maintained during the remaining months of 2008/09.
Improving access (including at evenings and weekends) to GP services38 GP practices (62.3%) now operate extended hours, exceeding the target of 50% of practices which was set for 31 March 2009.

www.enherts-pct.nhs.uk | 55
Better access to genito-urinary medicine (GUM) clinicsThe national target is to ensure 100% of patients are offered an appointment to be seen within 48 hours by GUM services. By the end of March 2009 performance was 99.37% - this is close to target and improving further. This figure incorporates performance across a high number of GUM clinics, some of which are local, others further afield. The changes implemented within local services, where we obviously have the greatest influence, are now regularly delivering 100%.
Maintaining 98% operational standard for accident and emergency departmentsThe standard for A&E performance is that 98% of people should not have to wait for more than four hours before being admitted or discharged. East and North Hertfordshire NHS Trust achieved this operational standard across the year. There were times from late December to early February where performance was less than 98%. However, the PCT supported its partners to find solutions to ease the pressures and improve performance during this period. Performance has subsequently improved.
2 Keeping adults and children well, improving their health and reducing health inequalitiesHelping people to stop smoking Achievement of the smoking cessation target remains a significant challenge. Our target for 2008/09 was to achieve 3,489 4-week quitters. By the end of March 2009 we had reached 1,768. A number of measures have been undertaken over the year to increase the numbers of patients making use of these services. These include recruiting more staff, advertising the service more actively, training up a large number of smoking cessation advisers in local pharmacies and general practices, offering an incentive scheme for service providers seeing more patients, and working directly with large pharmacy groups.
Whilst our performance against the quitting target is not where we would like it to be, this is only one element of more widespread work to reduce smoking across the whole
population, e.g. discouraging teenagers from becoming smokers in the first place. A recent ‘health and lifestyle’ survey has shown the success of the overall approach, and smoking levels are continuing to fall across NHS East and North Hertfordshire.
Tackling childhood obesityThe national objective for the NHS and its partners is to halt the year-on-year rise in obesity among children under 11 by 2010. At a local level, the PCT is expected to deliver the National Child Height and Weight programme to 85% of children in reception and year 6. Under this programme, every child is measured, with the data used to help the PCT forward plan health provision and provide more tailored health services for local children.
This year NHS East and North Hertfordshire weighed and measured more children than its original plan, however the overall participation rate for the year just missed the target (84.986%) because there were more children than expected in each year.
Increased screening for chlamydiaThe target is to screen 17% of 15-24 year olds. During 2008/09 we screened 11.3%. Performance in the final quarter of 2008/09 shows improvement with 3,421 screens undertaken in the final quarter. Had this rate been undertaken across the whole year 12.8% of the target population would have been screened. The target for 2009/10 has increased from 17% of the “at risk” population to 25% of the “at risk” population. The PCT will need to assure it begins its screening programme early enough in the year to achieve this even more challenging target. Further mailshots continue, and together with other initiatives, are leading to an ongoing increase in screening levels.
Reducing cancer waiting timesPerformance for quarter 3 showed that each of the four cancer waiting times targets were met. This means that 100% of patients waited less than 2 weeks from urgent GP referral to first outpatient appointment. The overall
wait from referral to treatment was 62 days or less for all patients and there was a wait of 31 days or less from diagnosis to treatment for all patients.
Quarter 4 performance was measured against a new set of definitions to bring them in line with the 18 week measurement definitions. This meant fewer opportunities to ‘stop the clock’, for example if a patient wanted to consider their treatment options then the clock could not be paused whilst they were deciding what they wanted to do.
Performance against two of the four indicators was affected by this change. Our performance is shown below:
Q1 – Q3% receiving first definitive treatment in one month
99.734%
Q4% receiving first definitive treatment in one month
97.590%
Q4% subsequent treatment in one month
98.305%
Q1 – Q3Percent treated in 2 months - GP
98.380%
Q4Percent treated in 2 months - GP
84.375%
Q4Percent treated in 2 months - screening
100%
Q4Percent treated in 2 months – consultant upgrade
100%
3 Improving cleanliness and reducing healthcare-associated infectionsThe further reduction of methicillin resistant staphylococcus aureus (MRSA) and clostridium difficile (CDiff) rates remained key targets for 2008/09.
East and North Hertfordshire NHS Trust met both these targets with just 18 MRSA infections reported to the end of the year against a limit of 21, and 114 CDiff cases against a

56 | Annual Report and Accounts 2008/09
limit of 183. Primary care organisations also worked towards targets on cleanliness and reducing healthcare-associated infections during 2008/09. This was constructed on the basis of incidence rates for the population. The target for 2008/09 was to have fewer than 386 incidents of clostridium difficile. NHS East and North Hertfordshire has made excellent progress with 239 reported cases by the end of March 2009.
4 Improving patient experience, staff satisfaction, and engagementNHS East and North Hertfordshire is committed to developing a strategic approach to patient and public engagement, to ensure that involvement is linked to both national and local NHS priorities; and to provide an opportunity for patients to have a say in their health services.
The PCT is a partner in a public engagement partnership with the county and district councils, and Hertfordshire Police.
A countywide stakeholder forum of local authority and voluntary sector partners has been established to advise on the implementation of health service changes from a stakeholder perspective.
The PCT regularly engages with carers, black and minority ethnic (BME) communities, people who are homeless, Travellers, Gypsy and Roma communities; and young people, through the Health Care Ambassador programme.
Members of the Hertfordshire Local Involvement Network (LINK) serve on many of the PCT’s committees, and play an active part in PCT activities. The PCT has an observer on the LINK Board.
Staff engagement is considered to be a high priority within the PCT and communication with staff continues to improve.
The NHS National Staff Survey which takes place every October revealed that staff are generally more satisfied that the PCT has improved in many areas.
Twice as many staff as last year responded positively when asked if management has set out a clear vision for the organisation and if they had a clear understanding of the values of the organisation.
Further indicators include the number of staff who have considered leaving the organisation. This has dropped by 10%, with 90% of staff saying they felt trusted to do their job, 84% believing their role makes a difference, and 80% saying they found their jobs interesting.
Further actions from the results of the staff survey are being identified and followed up to reinforce our position as an employer of choice.
5 Preparing to respond in a state of emergency, such as an outbreak of pandemic flu NHS East and North Hertfordshire is the lead PCT for emergency planning in Hertfordshire. Our emergency planning team works across both of the Hertfordshire PCTs. The role of our team is to prepare the two Hertfordshire PCTs to respond to a range of incidents as defined in NHS and central government guidance and to support our local hospitals and mental health trust to do the same.
In 2008/09 we created a dedicated control and command centre from which we can manage incidents. We participated in a number of local and regional emergency
planning exercises that included scenarios involving train and aircraft accidents and pandemic flu.
During this year we spent much of our time developing arrangements to prepare for and respond to an influenza pandemic. This included examining workforce issues, preparing for massive increases in demand for care, as well as developing recovery management arrangements. We also worked with GP surgeries to implement business continuity software that would enable them to plan for a pandemic flu outbreak.
We worked on supporting all Hertfordshire trusts in developing business continuity arrangements and the continuing development of hospital evacuation plans, aiming to ensure that the local health economy has flexible arrangements in place to maintain services during challenging circumstances.
During the year we also dealt with live incidents including the delivery of a suspicious package to the PCT offices and the effects of severe weather and snow.
Reporting to the PCTs’ Emergency Planning and Resilience Sub-Committee ensures that the work of our emergency planning team reflects local needs, while our active engagement with partners across Hertfordshire and the East of England region is building robust working arrangements essential in responding to major incidents and emergencies.

www.enherts-pct.nhs.uk | 57
Annual health checkThe Annual Health Check, published by the Healthcare Commission (now the Care Quality Commission) in October each year, is the system for assessing and rating the performance of NHS organisations in England.
The results published in October 2008 (covering the period April 2007 to March 2008) gave the PCT a ‘fair’ rating in both ‘Use of Resources’ and ‘Quality of Services’. These ratings were a marked improvement from the previous year when the PCT was assessed as ‘weak’ for both.
For 2008/09, the PCT will for the first time do separate self assessments on core standards for better health for the provider and commissioning functions. This will form part of the assessment of the quality of services that we provide to our residents and commission on behalf of the population that we serve.
The PCT continues to make good progress on meeting the core standards and the national targets. The following tables show our performance for this year’s (2008/09) existing commitments and national priorities.

National Priorities
Indicators Target 2008/09; Performance
18 week referral to treatment times 3
18-week Referral to Treatment (RTT) target for Admitted pathways 90% 3
18-week Referral to Treatment (RTT) Data Completeness for Admitted pathways 90-110% 3
18-week Referral to Treatment (RTT) target for Non-Admitted pathways 95% 3
18-week Referral to Treatment (RTT) Data Completeness for Non-Admitted pathways 90-110% 3
Access to primary careThis indicator is now wholly based on the GP survey results across 5 areas. We underachieved on this in 07/08 and thresholds for 08/09 have not yet been published so the estimate is that we will underachieve
85% –
Access to primary care dental services – the proportion of population visiting an NHS dentist in past 24 months 338,269 3
Existing Commitments
Indicators Target 2008/09; Performance
Access to GUM clinics within 48 hours 100% 3
Category A calls meeting 19 minute standard (Ambulance Trust Performance) 95% 3
Category A calls meeting 8 minute standard (Ambulance Trust Performance)We are measured on the performance of the ambulance trust as a whole across the East of England region. The performance of the ambulance trust for Hertfordshire residents met the targets.
75% –
Category A calls meeting 8 minute standard (Ambulance Trust Performance)We are measured on the performance of the ambulance trust as a whole across the East of England region. The performance of the ambulance trust for Hertfordshire residents met the targets.
95% –
Commissioning of crisis resolution/home treatment servicesHertfordshire Partnership Foundation Trust (HPfT) has identified a data quality issue in the counting of people receiving Crisis Home Treatment. The data issue which has now been corrected resulted in the performance against target which was thought to be good, being below target. An action plan is being prepared by HPfT and the Joint Commissioning Team to rectify the situation in 2009/10.
829 7
Commissioning of early intervention in psychosis services 3
Data quality on ethnic groupDespite significant improvement over recent years NHS East and North Hertfordshire did not meet this target. This target predominately relates to data collected at the East and North Herts NHS Trust. Plans are in place to improve, with performance being monitored at the commissioning and information group
85% –
Delayed transfers of care (6 per 100,000 pop)We have identified that these delays were the result of poor communication between the various agencies involved and a lack of awareness of the correct process in some cases. We have developed a project to integrate all those involved in the discharge planning process with the objective of reducing the number of delays.
–
Diabetic retinopathy screening 100% 3
Inpatients waiting longer than the 26 week standard 0% 3
Outpatients waiting longer than the 13 week standard 0% 3
Patients waiting longer than three months (13 weeks) for revascularisationThis target was missed under achieved by 0.059% (the equivalent of one patient).
0% –
Time to reperfusion for patients who have had a heart attack 68% –
Total time in AandE (maximum 4 hour wait) 98% 3

National Priorities
Indicators Target 2008/09; Performance
All age all cause mortality 640 males - 463 females 3
Reduction in CVD mortality rate in people age under 75 (40% by 2010) 65.441 3
Reduction in cancer mortality rate in people age under 75 (20% by 2010) 105 3
All cancers: one month diagnosis to treatment (including new cancer strategy commitment) 96% 3
All cancers: two month GP urgent referral to treatment (including new cancer strategy commitment) 85%3 Subject to
benchmarking
All cancers: two week wait 93% 3
Breast cancer screening for women aged 53 to 70 years>70% (aged 53-64)>65% (aged 65-70)
3
Childhood obesity rateParticipation rate fell below target of 85% due to increase in number of pupils in each year above expected levels
85% participation rateMaintain / reduce rate 9% for YR 15% for yr 6
7
Chlamydia screening (as a proxy for chlamydia prevalence)This is a challenging target for Hertfordshire and further promotional work will continue to bring about an ongoing increase in screening levels
17% of population 7
Commissioning a comprehensive child and adolescent mental health service (CAMHS) Achieve level 3 3
Experience of patients 60 3
Four week smoking quitters See information on page 34
3,528 7
Incidence of Clostridium difficile 386 3
NHS staff satisfaction 3% 3
Number of drug users recorded as being in effective treatment 1,6523 Subject to
benchmarking
Prevalence of breastfeeding at 6-8 weeks from birth (data completeness)Our data was rejected as the CQC did not record that the PCT had submitted Q3 data. The PCT have queried this.
Recorded coverage 85%Prevalence 46%
7
Proportion of individuals who complete immunisation by recommended ages(Dtap/IPV/Hib: aged 1) = 95% (PCV: aged 2) 86%
(Hib/ MenC: aged 2) 85% (MMR: aged 2) 86% (DTaP/IV:aged 5) 95% (MMR:aged 5) 85%
3
Stroke careThis target refers to the percentage of patients spending time on a dedicated stoke ward after being admitted with a stoke. The Stroke Network manage this on behalf of the PCT and a plan is in place to improve this.
25% 7
Teenage conception rates per 1,000 females aged 15-17This target was missed by 7% more than planned figure (Herts-wide figure)
24.6– Subject to
benchmarking
Women who have seen a midwife or maternity healthcare professional by 12 completed weeks of pregnancyThis target relates to women who have seen a midwife or maternity healthcare professional by 12 completed weeks of pregnancy. The indicator this year relates to the data quality of the information submission. We reported that data was collected from some trusts but not comprehensive across all locations.
Level 2 –
Key: 3 = achieved – = close to achieving 7 = not achieved
60 | Annual Report and Accounts 2008/09

www.enherts-pct.nhs.uk | 61
FinancialReview
The year ended 31 March 2009 was successful on many fronts. The PCT returned to a strong financial position, recording an underspend of £1.7m, whilst at the same time improving performance on key service targets.
62 | Annual Report and Accounts 2008/09
Whilst the PCT can look forward with some confidence, the economic situation and the fact that the PCT receives more than its target share of funding, is likely to result in lower growth in resources beyond 2010/11. Therefore the PCT must continue to strive to achieve value for money across all of its spending.
The key features in setting budgets for 2008/09 were:
headline growth in revenue resources of £36m (5.46%)• additional funding of £25m available because the •historic accumulated debt has now been paid off a deposit of £7.5m into a strategic reserve held at the •Strategic Health Authority (SHA) to ensure that growth is smoothed over the next three years to ensure a more sustainable approach to new investment contingency reserves set aside at the beginning of the •year of 1% of funding planned increase in expenditure compared to 2007/08 •recurrent expenditure of 7.8% inflation of generally 2.3%, except for primary care •where the uplift was 1.5% additional net investment above inflation, on acute •services of 2.8%, to meet the targets for reducing waiting times growth in prescribing budgets of 7% over 2007/08 •expenditure growth in other primary care budgets, including •dentistry, of 6% above inflation reinvestment of all the underspends on provider •services in 2007/08investment in continuing care of 3.7% above inflation• investment in mental health and learning disabilities of •4% above inflation.
Whilst achieving financial balance in 2008/09, there were some significant variances on individual budget lines.
Expenditure on acute services exceeded the budget set, with the main contributory factors being the higher than expected levels of activity required to achieve the 18-week waiting time target, increased referrals and higher than planned costs for some specific treatments including renal activity, critical care, cancer services and high cost drugs.
The overspend on acute services was offset by underspends on corporate services, mental health, primary care services and drugs prescribed. The underspend on mental health arose because not all of the 4% additional funding included in the budget was spent by year end.

www.enherts-pct.nhs.uk | 63
1) Costs not to exceed revenue resource limit The PCT’s revenue resource limit was £693m and expenditure was £691m. The PCT had always planned to underspend by £1m and this target was exceeded with expenditure being within the agreed resource limit by £1,683,000. This underspend will be returned to the PCT by the Department of Health, who will increase the PCT’s resource limit by £1,683,000 in 2009/10.(Accounts – Note 2.1)
2) To remain within cash limitAll PCTs are set a cash limit. This is the amount of cash that can be drawn from the Department of Health. PCTs are not allowed to be overdrawn and are expected to end the year with minimal cash balances.
The PCT drew down its full cash limit and retained no cash at 31 March 2009.
The target was therefore achieved. (Accounts – Balance Sheet)
3) Capital costs not to exceed capital resource limit The PCT’s capital resource limit was set at £2.7m and capital expenditure incurred was £2.6m. The PCT achieved this duty, underspending by £66,000. (Accounts – Note 2.2)
4) To recover the full cost of provider servicesNHS East and North Hertfordshire both commissions services and also provides them directly. The PCT has to demonstrate that it has received income to cover the full costs of the services it directly provides. In 2008/09, the net cost of services provided was £48m and the funding provided from the PCT’s own allocation was £48m. The PCT therefore achieved an underspend on provider services of £31,000, consequently meeting the target. (Accounts – Note 2.3)
Management costsAlthough no formal national targets are set for PCTs, a concerted effort was made to keep costs to the minimum while still ensuring the smooth running of the PCT and achievement of its objectives. Management costs recorded in the accounts are only a small part of ‘headquarters’ costs and are defined nationally. In 2008/09 management costs made up less than 1.6% of total spending. The total for the year was £10.8m or £22.08 per head of weighted population, a reduction on 2007/08.
The pay rise for staff and managers in 2008/09 was 2.75% and was the first year of a three-year agreement on pay. This was in line with the guidance from the Department of Health. Lower paid staff received slightly higher awards, with the removal of the lowest pay point which increased the NHS minimum wage by 5.8%.
The pay rise for Very Senior Managers in 2008/09 was 2.2%. (Accounts – Note 5.5)
Public Sector Payment PolicyThe PCT has an obligation to pay non-NHS creditors within 30 days of receipt of goods or a valid invoice (whichever is later), unless other payment terms have been agreed. This is monitored during the year. The PCT paid 88% of invoices from non-NHS organisations within this target. This is an improvement on performance in 2007/08 (71%), but is still short of good practice. By value, 90% of invoices were paid within target, an improvement on 2007/08, but also short of good practice.
On invoices from other NHS organisations, the PCT paid 72% of invoices (97% by value) within 30 days. In both cases this is an improvement on 2007/08. Performance on all measures steadily improved during the year and the PCT expects performance in 2009/10 to be better still.(Accounts – Note 6.1)
Related party transactionsIn the year to 31 March 2009, a number of local GPs sat on the Board and Executive Committee of the PCT. Payments amounting to £5.5m were made to these GPs’ practices, in their capacity as providers of primary care services.
Payments for similar services were made to other GP practices within the PCT. The GPs on the Board and Executive Committee had no direct control over how these funds were allocated.
All Board members and senior managers are required to complete a declaration setting out any outside interests. In the year to 31 March 2009, there were no payments made by the PCT to organisations included in the register of interests.
The Department of Health is regarded as a related party. During the year, the PCT had a significant number of material transactions with the Department, and with other entities for which the Department is regarded as the parent Department. Further details of the amounts and the parties involved are included in the accounts. (Accounts – Note 20)
Where the money was spentAs mentioned above, the PCT is both a commissioner of services and a provider. The majority of the PCT’s funding was spent on commissioning services from other NHS and non-NHS organisations. The largest single element was spent on general and acute services (43.6%). Next came prescribing (10.9%), and primary care general medical services (10.4%). Around 7% of total spending went on services provided directly by the PCT. A more detailed analysis of where the money was spent is shown in the pie chart on the following page.
Financial duties and targetsThere are four main financial targets. Performance on these in 2008/09 is detailed below.

64 | Annual Report and Accounts 2008/09
Analysis of 2008/09 Net Expenditure
PCT Provided Services 7.0%
Prescribing 10.9%
General Medical Services 10.4%
Other Family Health Services 6.5%
Maternity 2.0%
General and Acute 43.6%
AandE 2.1%
Learning Disabilities 6.6%
Mental Healthcare 6.8%
Other Healthcare 4%

www.enherts-pct.nhs.uk | 65
Financial outlook
Implementation of International Financial Reporting Standards (IFRS) in 2009/10Achieving financial balance in
the last two years has been a major success
In the 2008 budget it was announced that public sector bodies would produce financial statements based on IFRS from 2009/10.
Growth funding for next year and the year after is 5.5% and 5.8% respectively. However, it is clear that growth funding in the following years will be considerably less. The PCT has therefore developed a five-year financial plan, alongside the Commissioning Strategy. The plan will see increased investment in services, but with £2.6m additional funds held back in reserve for investment after 2009/10 when growth in funding is expected to be smaller. The plan also sees a reduction in the proportion of the PCT’s funding spent on acute services. There will be increased funding in particular for mental health services, prescribing, community and primary care. The strategy also includes the development of a new local general hospital in the Welwyn Hatfield area, with a likely capital cost of around £30m.
In 2009/10, with the additional deposit with the SHA of £2.6m (making £10.1m in total), and the return of the underspend in 2008/09, the PCT is planning for an underspend of £1m. This will act as a safety net in-year and be carried forward to future years if not utilised.
The reasons for introducing IFRS were set in the context of the government’s need for “high value performance data in combination with appropriate financial data”. IFRS, as adapted for use in the public sector, will be used to provide benefits in consistency and comparability between financial reports in the global economy and to follow private sector best practice.
In April 2008, the PCT created a project team to oversee implementation. Members of the team attended specialised
external training courses to ensure appropriate accounting treatment. An internal course was developed and delivered for the development of the wider finance community and other relevant PCT staff.
The PCT successfully restated its 2007/8 closing balances on 19 December 2008. The PCT has reviewed and amended its internal procedures to ensure that IFRS was fully operational from 1 April 2009.

66 | Annual Report and Accounts 2008/09

www.enherts-pct.nhs.uk | 67
Looking to the Future
The business plan for 2009/10 is important as it is the first plan produced by the PCT to reflect its aspiration to become a World Class Commissioner.

68 | Annual Report and Accounts 2008/09
Our strategic objectives
1) Delivering our strategy and national targets
The vision of the PCT is as follows:
“Our ambition is to be a high performing PCT recognised by our people, patients and partners as commissioning outstanding care and improving the wellbeing of all.”
The strategy has three strategic priorities. These are:
Keeping Hertfordshire healthy•Enhancing the patient experience• Commissioning high quality healthcare for the •population of Hertfordshire
The World Class Commissioning assurance framework requires us to select a number of outcomes to measure our success. These clearly need to relate to the delivery of our strategic priorities. With this in mind, we have chosen the following 15 outcomes:
1. Increase life expectancy2. Reduce the difference in life expectancy between the
most and least deprived communities3. Increase the number of people who give up smoking4. Reduce the prevalence of obesity in year 6 school children5. Increase uptake of the MMR vaccination6. Reduce the mortality rate from cardiovascular disease7. Improve patient satisfaction with access to GP services8. Increase the proportion of people visiting an NHS dentist.9. Reduce the number of babies born by caesarean section10. Increase the number of people who can control
their diabetes11. Reduce the prevalence of chronic obstructive
pulmonary disease12. Increase the number of people with long-term
conditions who have personal health plans13. Increase the number of people who are able to die in
their own homes14. Improve patient experience scores15. Reduce then eliminate Clostridium Difficile within
healthcare settings.
In order to deliver our strategy we have identified the following nine strategic workstreams:
Staying Healthy•Acute Care, Planned Care•Mental Health•Learning Disabilities•Maternity and New Born•Children’s Health•Long Term Conditions•End of Life•Patient Experience•
2) Developing capacity and capability
The World Class Commissioning Assurance Framework recognises 10 competencies. In order to become World Class Commissioners, PCTs need to demonstrate that they are at level 4 for each of these competencies. At the end of 2008, NHS East and North Hertfordshire was assessed against these competencies. This identified that we were operating at either level 2 or 1 for all of the competencies. In order to improve and become World Class Commissioners, we have developed a World Class Commissioning Organisational Development Plan. This aims to transform the PCT so that it will operate at level 3 or 4 for all of the competencies within a two-year period and at level 4 for all of the competencies in a three-year period. The development plan includes the following 10 strategic priorities:
1.Develop a commissioning mindset2. Improve contracting and commercial capabilities3. Develop and utilise a prioritisation framework for all
investment and service redesign4. Development of a data repository and analytical skills5. Assessment of provider market6. Drive clinically led evidence based change 7. Proactively engage public and patients8. Focus on working with all our partners to improve care
and reduce health inequalities9. Develop real and structured processes and an appropriate
workforce to deliver World Class Commissioning10. To be more responsive to patient experience within
commissioning.
In order to deliver the strategic priorities we have identified eight projects. Detailed plans have been drafted for these projects.
Key to our success will be the further development of Practice Based Commissioning.

www.enherts-pct.nhs.uk | 69
3) Making best use of resources
In order to achieve our strategic priorities, the PCT needs to ensure that it makes the most efficient and effective use of its resources including:
Finance•Human Resources•Estates•Information Communication and Technology•Governance•
The business plan outlines objectives for these areas, clearly relating them to the delivery of our strategic priorities.
The PCT has two strategies in place setting out the configuration of community and hospital services – ‘Delivering Quality Healthcare for Hertfordshire’ (DQHH) and ‘Investing in Your Mental Health’ (IiYMH).
These have both been widely consulted on and DQHH is the subject of a full business case. Implementation has commenced, with IiYMH currently being the subject of a stock take. This aim is for both strategies to align with the recommendations of Professor Lord Ara Darzi’s Next Stage Review and the East of England SHA’s ‘Towards the Best, Together’, as well as the requirements of the World Class Commissioning assurance programme.

70 | Annual Report and Accounts 2008/09

www.enherts-pct.nhs.uk | 71
GovernanceControls and Audit

72 | Annual Report and Accounts 2008/09
Policy on managing principal risksThe Assurance Framework provides a comprehensive method for the effective management of the principal risks that arise in meeting the key strategic objectives agreed by the PCT Board.
It identifies objectives which are at risk, gaps in control and insufficient assurances. It also provides a structure for evidence to support the ‘Statement on Internal Control’ and facilitates reporting key information regularly to the PCT Board.
Directors are responsible for the continual updating of the Assurance Framework including evaluation of the risk score, updates on progress and identification of actions against gaps in control and assurance. The Assurance Framework is monitored by the Joint Integrated Governance Committee and PCT Board.
Role of the Joint Integrated Governance CommitteeThe committee is responsible for the management of risk including organisational and that related to the delivery of healthcare. It also provides assurance to the Board on the systems and processes by which the PCT achieves organisational objectives, and the safety and quality of clinical services.
The core membership of the committee includes representatives from the Audit Committee. This provides a mechanism for the Audit Committees together with management reporting to oversee the detailed monitoring of progress against the Assurance Framework.
Information GovernanceIn line with the Information Governance Strategy the PCT has assigned responsibility for information governance. Risks are managed, monitored and reviewed by the Information Governance Sub-Committee, which reports through the Joint Integrated Governance Committee, to the Board.
Any personal data-related incidents and breaches are published within the PCT’s annual report in line with Department of Health directives.
In total there were 36 personal data-related incidents reported to the PCT in 2008/09. This includes seven incidents classified as serious untoward incidents and reported to the SHA.
The table below shows serious untoward incidents that were reported to NHS East and North Hertfordshire from commissioned and Provider Services.
Category Nature of Incident Total
I Loss of inadequately protected electronic equipment, devices or paper documents from secured NHS premises
5
II Loss of inadequately protected electronic equipment, devices or paper documents from outside secured NHS premises
14
III Insecure disposal of inadequately protected electronic equipment, devices or paper documents
0
IV Unauthorised disclosure 4
V Other 13
In view of the high level of national interest in potential data loss, all hardware and portal devices have now been encrypted. Policies and procedures incorporating information governance have been reviewed, ratified and approved by the board. Stringent reporting procedures have been implemented with associated risk assurance measures being assigned.
Our staff induction has been revised to incorporate a stronger emphasis on information governance.
Freedom of Information requestsThere has been one Freedom of Information request. The enquirer request the PCT provide the number of patient records that have potentially been reported as ‘compromised’.
Role of the Audit CommitteeThe committee’s principle function is to advise the Board on the adequacy and effectiveness of the PCT’s systems of internal control and its arrangements for risk management, control and governance processes.
In order to fulfil this function, the Audit Committee prepares an annual report for the Board and Accountable Officer. This report includes information provided by Internal Audit, External Audit and other assurance providers.
The opinion of the Audit Committee was that adequate assurance can be given to the Board on the effectiveness of the risk management and control processes in place during 2008/09.
Environmental matters, including policies NHS East and North Hertfordshire is committed to playing an active role in reducing carbon emissions.
We have signed up and been accepted on a programme run by the Carbon Trust. This will assist us in our work to implement the NHS Carbon Management Initiative - which provides healthcare organisations with support and guidance to identify realistic carbon reduction opportunities that deliver significant cost savings. All of the PCT’s operations will be assessed in terms of their energy consumption and related carbon emissions. Technical and change management support is provided to enable organisations to work through a step-by-step process to identify and quantify carbon reduction opportunities. The final element of the
www.enherts-pct.nhs.uk | 73
programme; a Carbon Management Plan (CMP) will provide a business case to support each of the most appropriate measures of reducing carbon emissions.
In addition, the PCT is represented on the multi agency Climate Change LAA Group; and the Herts NHS Environment Group which feeds into the Hertfordshire Environmental Forum (HEF) has been active for almost five years.
With the support of this group the PCT has undertaken a range of environmental improvements in the workplace which include recycling schemes for waste paper and cardboard, installation of compactors for waste control and green transport initiatives.
Furthermore, Hertfordshire County Council and Herts NHS Environment Group recently commissioned a review of the effects of climate change on the delivery of health and adult care services in Hertfordshire.
PCT employees, including policies The PCT is fully committed to supporting all staff to develop and enhance their skills ensuring they can provide the best patient care and support services possible.
Our staff undertake training to ensure they can deliver safe care, for example infection control and hand hygiene, health and safety, and fire training. This year we have provided our biggest health and safety training programme ever, with more than 1,400 course places taken up.
We have also sought to ensure that clinical skills are up-to-date by providing a range of in-house training sessions covering issues such as continence and intravenous therapy. Other courses have been provided by the University of Hertfordshire.
Several of our community matrons and other nursing staff have attended a ‘Non Medical Prescribing’ course at the University of Hertfordshire. This means that an increasing number of our nurses can prescribe some medicines
without the need for patients to ask their GP, helping to ensure that patients receive care closer to home.
Where training cannot be provided locally, we have funded individuals to train at specialist centres. For example, our paediatric speech and language therapists have been continually updating their skills, helping to enhance their work with children who have speech and language difficulties.
During 2008/09 the PCT developed and implemented a number of HR policies including a bullying and harassment policy, recruitment and selection policy and Working time regulations policy and guidance. All approved policies can be viewed on our website at www.enherts-pct.nhs.uk and clicking on ‘Publications’.
The PCT offers staff the opportunity to join the NHS pension scheme, details of which are set out in note 1(o) of the Accounts on page 77.
Provision of information to and consultation with employees
We have a range of mechanisms that encourage two-way dialogue within the PCT. These include:
A monthly team briefing, comprising key messages •from the executive team, an update on our organisational development programme, a list of newly approved policies and guidance documents; and opportunities for managers to add items of interest for their individual service. The team briefing is cascaded throughout the organisation and its purpose is to encourage managers to discuss PCT matters with their staff face to face and includes a mechanism to convey staff views, thoughts and comments back up to the executive team A very successful intranet that receives many hits per •day containing a wide range of corporate information
such as policies, training courses and information on forthcoming events. It also contains a social area Regular chief executive meetings with staff that take •place in a range of locations around the county. These meetings give community and other staff the opportunity to meet the chief executive, learn about progress with our priorities and to raise issues or ask questions A programme of visits to staff at their bases or to their •team meetings by the chair and the executive team All staff have been invited to an event to understand •and engage in our new vision and values.
Absence due to staff sickness The overall sickness absence rate for the PCT from April 1st 2008 to March 31st 2009 was 3.91%. 1
The average regional PCT rate for 2008 was 5.58% (placing the organisation 2nd out of 14 PCTs regionally). 2
The average national PCT rate for 2008 was 4.48% (placing the organisation 37th out of 147 PCTs nationally). 2
1 Source: ESR Absence Timeline Analysis2 Source NHS Information Centre iView database


www.enherts-pct.nhs.uk | 75
Policy in relation to disabled employeesThe PCT retains the positive (or two ticks) symbol from Jobcentre Plus and actively supports the employment of staff with disabilities.
A Disability Staff Network Group was launched in March 2009 and a participant of this group is also a member of the Equality and Diversity Steering Group. Our latest records show that 10 members of staff from NHS East and North Hertfordshire declare themselves to have a disability.
Policy on equal opportunities The PCT has an equal opportunities policy which aims to ensure that all employees, irrespective of their background, are supported to develop their full potential. An equal opportunity statement is also included in all contracts of employment to ensure that all staff are aware of their responsibilities.
NHS East and North Hertfordshire is determined to ensure that we practise a culture of equality, diversity and human rights in the heart of the organisation and improve relations with the diverse population and identify health inequalities among our patients.
The PCT recruited an Equality and Diversity Manager in December 2008.
The PCT also has the following staff network groups:
Black and minority ethnic staff (BME)•Lesbian, Gay, Bisexual and Transgender staff (LGBT)•Staff with a disability•
We have confirmed our commitment to improving access of services to all through publication of a ‘Single Equality Scheme’ and the ongoing implementation of the action plan.
NHS East and North Hertfordshire works with many partners on the advancement of equal opportunities. Over the past year we have:
Held discussions with Hertfordshire County Council •to support the development of Hertfordshire Race Equality Council. This will assist the development of direct partnership work with local BME communities and help to improve relations within the county Produced information in 16 different languages as well •as large print, Braille and audio Continued to develop close links with local disability •organisations and BME communities through a series of ‘Fresh Start’ workshops which have helped us identify key issues such as funding for specialist services, production of accessible communications, interpretation services and promoted links with the traveller communities.
A three-year action plan has been developed to address health inequalities among certain groups in Hertfordshire, including people with learning difficulties, people in contact with the criminal justice system, and travellers.
The public health team has also been working with localised communities on specific health issues such smoking and adult obesity.
The PCTs jointly commissioned chartered surveyors to carry out Disability Discrimination Act (DDA) compliance surveys of the majority of our leasehold and freehold premises. As a result we have prioritised the issues identified by the audit and allocated £60,000 for adaptations to premises.
The PCTs have commissioned services from DisabledGo to provide information on all our estate facilities and make information on disabled access available to the public.
Members of the Remuneration Committee are non-executive directors only, and membership during the year was:
Phil Picton, Non executive Director, East and North, •(Chair and member of the Committee for part year)Pam Handley, Chair, East and North PCT•Linda Farrant, Non Executive Director, East and North•Stuart Bloom, Chair, West• Diane Bailey, Non executive director, West Herts, •(Chair of the Committee for part year) Elaine Fox, Non executive director, East and North, •(part year to replace Phil Picton).
The remuneration of senior managers is determined by national terms and conditions – Very Senior Manager Pay Framework. The framework includes the ability to pay performance related pay and in 2008/09 this has been applied.
The senior managers are employed under the nationally agreed contractual arrangements, all having been employed on permanent contracts which include a six month notice period. There is no provision in the contracts for termination payments save any contractual entitlements to redundancy compensation which would be calculated using the agreed NHS formula.
The majority of senior manager contracts commenced on 1st October 2007, are not fixed term so do not have any unexpired term, and include a six month notice period.
Remuneration report

76 | Annual Report and Accounts 2008/09
Remuneration Report
Salaries and AllowancesRelating to the period 1st April 2008 to 31st March 2009
2008 - 09 2007 - 08
Name Title
Salary/Fees (bands of
£5,000)
Other Remuneration
(bands of £5,000)
Benefits in kind
(rounded to the nearest
£000)
Salary (bands of
£5,000)
Other Remuneration
(bands of £5,000)
Benefits in kind
(rounded to the nearest
£000)
£000 £000 £000 £000
Pam Handley Chair 35-40 0 0 35-40 0 0
Richard Henry Non Executive Member 5-10 0 0 5-10 0 0
Phil PictonNon Executive Member and Chair of the Joint Remuneration Committee
5-10 0 0 5-10 0 0
Linda FarrantNon Executive Member and Chair of E and N Herts Audit Committee
10-15 0 0 10-15 0 0
Julia WittingNon Executive Member and Chair of Joint Integrated Governance Committee
5-10 0 0 5-10 0 0
Chris Learmonth Non Executive Member 5-10 0 0 5-10 0 0
Elaine Fox Non Executive Member [from 01/09/2008] 0-5 0 0
Anne Walker Chief Executive (50%) 70-75 0 0 65-70 0 0
Alan Pond Director of Finance and Commercial Development (50%) 55-60 0 0 45-50 0 0
Jane Halpin Director of Public Health (50%) 60-65 0 0 55-60 0 0
Gareth Jones Director of Strategic Planning (50%) 50-55 0 0 45-50 0 0
Beverley Flowers Director of Commissioning [from 21/11/2007] (50%) 45-50 0 0 15-20 0 0
Pauline PearceDirector of Public Involvement and Corporate Services (50%)
35-40 0 0 30-35 0 0
Heather MoulderInterim Chief Operating Officer Provider Services [from 01/12/2008] and Director of Nursing [up to 30/11/2008] (50%)
55-60 0 0 40-45 0 0
Clare Hawkins Interim Director of Nursing from [01/12/2008] (50%) 5-10 0 0
Andrew Parker Director of Primary Care and Service Redesign (50%) 45-50 0 0 40-45 0 0
Gloria Barber Director of Human Resources (50%) 40-45 0 0 35-40 0 0
Dr Tony Kostick Chair of the Professional Executive Committee 65-70 0 0 30-35 0 0

www.enherts-pct.nhs.uk | 77
Pension Benefits: Relating to the period 1 April 2008 to 31st March 2009
Name and title
Real increase In pension at age 60 (bands
of £2,500)
£000
Lump sum at aged 60
related to real
increasein pension
(bands of £2,500)
£000
Total accruedpension at
age 60 at 31 March 2008
(bands of£5,000)
£000
Lump sum at age 60
relatedto accrued
pension at 31 March 2008
(bands of £5,000)
£000
Cash Equivalent
Transfer Valueat 31 March
2009
£000
Cash Equivalent
Transfer Valueat 31 March
2008
£000
Real increase in Cash
EquivalentTransfer Value
funded by PCT
£000
Employer’s contribution
to stakeholder
pension
£000
Anne Walker - Chief Executive 0-2.5 5-7.5 25-30 75-80 474 333 93 0
Alan Pond - Director of Finance and Commercial Development
0-2.5 2.5-5 15-20 45-50 247 173 49 0
Jane Halpin - Director of Public Health 2.5-5 7.5-10 15-20 45-50 245 162 56 0
Gareth Jones - Director of Strategic Planning
0-2.5 0-2.5 15-20 55-60 367 266 66 0
Beverley Flowers - Director of Commissioning (from 21/11/2007)
0-2.5 2.5-5 5-10 20-25 113 78 23 0
Pauline Pearce - Director of Public Involvement and Corporate Services
0-2.5 2.5-5 10-15 30-35 204 143 40 0
Heather Moulder - Interim Chief Operating Officer Provider Services
2.5-5 12.5-15 20-25 60-65 342 214 86 0
Clare Hawkins - Director of Nursing from [01/12/2008]
0-2.5 0-2.5 10-15 30-35 167 123 10 0
Gloria Barber - Director of Human Resources
0-2.5 2.5-5 15-20 5.-55 392 273 79 0
Andrew Parker - Director of Primary Care and Service Redesign
0-2.5 2.5-5 10-15 40-45 249 173 50 0

78 | Annual Report and Accounts 2008/09
NHS East and North Hertfordshire Board Expenses 2008/2009
PositionPeriod Parking
at Office £
Official Mileage
£
Lump Sum
£
Excess Travel
£Subsistence
£Parking
£
Public Transport
£
Course Expenses
£
Telephone Costs
£
Total Expenses
£From To
Chair
Pam Handley 01/04/08 31/03/09 0 3,561 0 3 0 0 1,095 0 0 4,656
Non-Executive Directors
Richard Henry 01/04/08 31/03/09 No Claim
Philip Picton 01/04/08 31/03/09 0 760 0 0 0 65 0 0 0 825
Linda Farrant 01/04/08 31/03/09 0 1,053 0 0 0 131 0 0 0 1,183
Julia Witting 01/04/08 31/03/09 0 675 0 0 0 250 0 0 0 925
Christopher Learmonth 01/04/08 31/03/09 0 225 0 0 0 33 0 0 0 258
Notes:
1. As Non Executive Members do not receive pensionable remuneration, there will be no entries in respect of pensions for Non Executive Members.
2. Cash Equivalent Transfer Values
A Cash Equivalent Transfer Value (CETV) is the •actuarially assessed capital value of the pension scheme benefits accrued by a member at a particularly point in time. The benefits valued are the member’s accrued benefits •and any contingent spouse’s pension payable from the scheme.
A CETV is a payment made by a pension scheme or •arrangement to secure pension benefits in another pension scheme or arrangement when the member leaves a scheme and chooses to transfer the benefits accrued in their former scheme. The pension figures shown relate to the benefits that •the individual has accrued as a consequence of their total membership of the pension scheme, not just their service in a senior capacity to which disclosure applies. The CETV figures and the other pension details include •the value of any pension benefits in another scheme or arrangement which the individual has transferred to the NHS pension scheme. They also include any additional pension benefit •accrued to the member as a result of their purchasing additional years of pension service in the scheme at their own cost.
CETVs are calculated within the guidelines and •framework prescribed by the Institute and Faculty of Actuaries.
3. Real Increase in CETVThis reflects the increase in CETV effectively funded by the employer. It takes account of the increase in accrued pension due to inflation, contributions paid by the employee (including the value of any benefits transferred from another scheme or arrangement) and uses common market valuation factors for the start and end of the period.
4. Pension BenefitsRepresents 50% of the total amount claimed, the balance being paid by NHS West Hertfordshire.
ExpensesThe table below details the expenses claimed by Board members during 2008/09. This information is also available on the NHS East and North Hertfordshire website: www.enherts-pct.nhs.uk along with more details of the specific policies governing expense arrangements.

www.enherts-pct.nhs.uk | 79
NHS East and North Hertfordshire Board Expenses 2008/2009
PositionPeriod Parking
at Office £
Official Mileage
£
Lump Sum
£
Excess Travel
£Subsistence
£Parking
£
Public Transport
£
Course Expenses
£
Telephone Costs
£
Total Expenses
£From To
Elaine Fox 01/09/08 31/03/09 0 608 0 0 0 139 0 0 0 747
Voting Directors
Anne Walker*Chief Executive
01/04/08 31/03/09 (509) 1,315 700 544 0 145 363 0 (10) 2,548
Alan Pond*Director of Finance
01/04/08 31/03/09 (509) 1,690 917 0 0 114 88 0 0 2,299
Dr Jane Halpin*Director of Public Health
01/04/08 31/03/09 (509) 371 833 0 0 56 39 0 0 789
Non-Voting Directors
Gloria Barber* Director of Human Resources
01/04/08 31/03/09 (509) 0 0 0 0 0 0 0 0 (509)
Gareth Jones* Director of Strategic Planning
01/04/08 31/03/09 (509) 1,643 844 0 0 455 0 0 0 2,433
Pauline Pearce* Director of Public Involvement and Corporate Services
01/04/08 31/03/09 (509) 43 0 0 0 3 7 0 0 (456)
Heather Moulder*Director of Nursing / Interim Chief Operating Officer
01/04/08 31/03/09 0 0 253 0 0 0 0 0 0 253
Clare Hawkins*Interim Director of Nursing
01/12/08 31/03/09 0 0 253 0 0 0 0 0 0 253
Beverley Flowers*Director of Commissioning
01/04/08 31/03/09 No Claim
Andrew Parker*Director of Primary Care and Service Redesign
01/04/08 30/11/08 (509) 683 844 0 0 23 0 0 0 1,041
*Represents 50% of the total amount claimed, the balance being paid by NHS East and North HertfordshireFigures in brackets represent payments made to the organisation by the director for on-site parking.”
80 | Annual Report and Accounts 2008/09
Adherence to principles for remedyThe PCT follows the six principles set down by the Parliamentary and Health Service Ombudsman in ‘Principles for Remedy’ (October 2007). The aim of these principles is to ensure that instances of injustice or hardship as a result of poor service or maladministration are redressed.
The principles are:
Getting it right•Being customer focused•Being open and accountable•Acting fairly and proportionately•Putting things right•Seeking continuous improvement.•
How have we met these principles?
We have incorporated the NHS complaints procedures •into our own policy The Chief Executive takes a personal interest in all •complaints and the quality of investigation and response We have a responsive Patient Advice and Liaison •Service (PALS) which can resolve many problems or concerns without the need for a formal complaint We have in place a ‘losses and compensations’ procedure• Regular reporting to the Board of complaints •received and PALS issues as part of the PCT’s performance monitoring Applying Department of Health published best practice •guidance on NHS Continuing Healthcare Redress, in response to the Parliamentary and Health Service Ombudsman’s report ‘Retrospective Continuing Care Funding and Redress’.
Directors’ statement on audit information All Executive and Non-Executive Directors have stated that as far as they are aware, there is no relevant audit information of which the NHS body’s auditors are unaware and that they have taken all the steps that they ought to have taken as a Director in order to make themselves aware of any relevant audit information and to establish that the NHS body’s auditors are aware of that information.
External auditors and costs of audit workAudit Commission2nd FloorSheffield HouseLytton Way (Off Gates Way)StevenageSG1 3HG
The external audit fees for 2008/09 were £240,300 plus VAT.
The external auditors have been commissioned to undertake statutory audit work only and have not provided any services of an audit or non-audit nature that would compromise their independence as auditors.
Audit Committee members East and North:Linda Farrant (Chair)Julia WittingChris Learmonth

Directors’ disclosure of interests
Board Member Declarations of Pecuniary and other Interests for NHS East and North Herts Board Date Declared
Pam Handley, Chair Chair Watford CVS (unpaid) 18/10/2006
Trustee/Director (unpaid), Nine Lives Furniture (a charity receiving occasional grants from JCPB) 20/6/2007
Director, Choice Shapers (service brokerage for disabled people, with work possibly commissioned by HCC) 24/6/2008
Daughter works for HPFT 24/6/2008
Chair and Director Watford Charity Centre Ltd (unpaid) - a social enterprise 10/2/2009
Hypnotherapist in West Hertfordshire in private practice
Consultancy work for Housing and Support Partnership
Phil Picton, NED PhD research in investment reform and transition in the NHS (Carrying out research throughout the NHS within the University Business School which develops contracts with a range of NHS organisations and their partners) in receipt of a research bursary
3/11/2006
Independent management consultant – Phil Picton Consulting (sole trader) carrying out assignments in police and local government organisations
Richard Henry, NED Councillor for Stevenage Borough Council (Executive member) 18/10/2006
Lecturer North Herts College
Works 1 day/week for HPT specialist mental health team for older people
Chair and Trustee member Group 117 (organises holidays for people with disabilities) 9/1/2008
Wife works for HPT as a manager
Prospective Parliamentary Candidate, NE Hertfordshire Constituency
Linda Farrant, NED Husband is Chief Executive of Leisure Connection, a company which manages leisure facilities and works in partnership with PCTs to deliver health improvement programmes (outside of Hertfordshire) Board member of Metropolitan Housing Partnership
18/10/2006 1/10/2007
Chris Learmonth, NED Parent Governor of Mandeville Primary School in Sawbridgeworth 31/10/2006
Non-executive Director of Adroit-e (a Market Research Company). The company does not have any interaction with the PCT but it does pitch for contracts in the public sector (including health care)
14/7/2008
Finance Director, The Bridal Path (est. 2006) Limited
Director, Learmonth and Company (accountancy and financial advice – no health links)
Julia Witting, NED Parish Councillor and Chair, Stanstead Abbotts 16/10/2006
Eastern Region Development Officer (part time), National Association of Local Councils 24/6/2008
Independent Member of the Circle Anglia Group Audit Committee (Term of three years beginning 1 Sept 2008) 21/8/2008
One-off payment of £100 received for participation in a telephone interview for market research on behalf of pharmaceutical companies (March 2009)
17/3/2009
Husband is a training consultant, providing training in interpersonal communication, management skills, appraisal training and presentation skills. This occasionally includes provision of training to NHS trusts in other regions.

82 | Annual Report and Accounts 2008/09
Directors’ disclosure of interests
Board Member Declarations of Pecuniary and other Interests for NHS East and North Herts Board Date Declared
Elaine Fox Committee member, Fairfield Park Residents association (looks after the interests of the new community being built in the grounds of (what was) Fairfield Park Hospital.
3/9/2008
Anne Walker,Chief Executive
None16/10/2006
Alan Pond, Director of Finance
None4/10/2006
Heather Moulder, Interim Chief Operating Officer, Provider Services
Member of Vitiligo Society (a voluntary organisation that supports people, including a member of her family, with this condition)25/6/2008
Andrew ParkerDirector of Primary Care and Service Redesign
Wife is Bone Marrow Transplant Quality Manager at Royal Free Hospital NHS Trust, (PCT has an Service Level Agreement with RFH)7/2/2007
Beverley Flowers Director of Commissioning
None6/7/2007
Gareth Jones, Director of Strategic Planning
None4/10/2006
Clare HawkinsInterim Director of Nursing
None18/4/2007
Pauline Pearce, Director of Public Involvement and Corporate Services
Son undertakes occasional temporary clerical work in other directorates20/7/2007
Dr Jane HalpinDeputy Chief Executive and Director of Public Health
None16/10/2006
Gloria Barber Director of Human Resources
None25/1/2007
Tony KostickChair, Professional Executive Committee
Principal, Dr Baxani and Partners, Stevenage, Clinical Lead, Stevenage PBC Group 13/12/2006
Club Doctor, Stevenage Borough Football Club, Navigant Consulting Clinical consultancy 10/1/2007
Expert 24 Ltd Health assessment software (clinical consultancy) 26/6/2008

www.enherts-pct.nhs.uk | 83

84 | Annual Report and Accounts 2008/09
Alan Pond, Director of Finance
The Accounts

www.enherts-pct.nhs.uk | 85
The AccountsThese accounts for the year ended 31 March 2009 have been prepared by the East and North Hertfordshire Primary Care Trust (PCT) under section 232 Sch 15(3) of the National Health Service Act 2006 in the form which the Secretary of State has, with the approval of Treasury, directed.

86 | Annual Report and Accounts 2008/09
Statement of Chief Executive’s responsibilities as the Accountable Officer of the PCT The Secretary of State has directed that the Chief Executive should be the Accountable Officer to the Primary Care Trust. The relevant responsibilities of Accountable Officers are set out in the Accountable Officers Memorandum issued by the Department of Health.
These include ensuring that:
there are effective management systems in place to •safeguard public funds and assets and assist in the implementation of corporate governance; value for money is achieved from the resources •available to the primary care trust; the expenditure and income of the primary care •trust has been applied to the purposes intended by Parliament and conform to the authorities which govern them; effective and sound financial management systems •are in place; and annual statutory accounts are prepared in a format •directed by the Secretary of State with the approval of the Treasury to give a true and fair view of the state of affairs as at the end of the financial year and the net operating cost, recognised gains and losses and cash flows for the year.
To the best of my knowledge and belief, I have properly discharged the responsibilities set out in my letter of appointment as an Accountable Officer.
Statement of the Directors’ responsibilities in respect of the accounts The directors are required under the National Health Service Act 2006 to prepare accounts for each financial year. The Secretary of State, with the approval of the Treasury, directs that these accounts give a true and fair view of the state of affairs of the organisation and the net operating cost, recognised gains and losses and cash flows for the year. In preparing these accounts, Directors are required to:
I. apply on a consistent basis accounting policies laid down by the Secretary of State with the approval of the Treasury;II. make judgements and estimates which are reasonable and prudent;III. state whether applicable accounting standards have been followed, subject to any material departures disclosed and explained in the accounts.
The directors are responsible for keeping proper accounting records which disclose with reasonable accuracy at any time the financial position of the organisation and to enable them to ensure that the accounts comply with requirements outlined in the above mentioned direction of the Secretary of State. They are also responsible for safeguarding the assets of the health authority and hence for taking reasonable steps for the prevention of fraud and other irregularities.
The directors confirm to the best of their knowledge and belief they have complied with the above requirements in preparing the financial statements.
By order of the board.
Statement on internal control 2008/09
1. Scope of responsibilityThe Board is accountable for internal control. As Accountable Officer, and Chief Executive of this Board, I have responsibility for maintaining a sound system of internal control that supports the achievement of the organisation’s policies, aims and objectives. I also have responsibility for safeguarding the public funds and the organisation’s assets for which I am personally responsible as set out in the Accountable Officer Memorandum.
I am also the Chief Executive of West Hertfordshire PCT. Although the two PCTs are separate statutory bodies, they have a single management and executive team and share some common strategic and operational goals and control system objectives.
My responsibilities as Accountable Officer in respect of internal controls are supported by the (Joint) Integrated Governance Committee and the Audit Committee. Both of these committees report to the Board.
The (Joint) Integrated Governance Committee is chaired by a Non-Executive Director. The chair is rotated between the two PCTs on an annual basis. In addition the chairs of the two Hertfordshire PCTs’ Audit Committees are also members of the (Joint) Integrated Governance Committee. The membership of the Audit Committee is entirely made up of Non-Executive Directors.
When appropriate, internal control issues also feature at weekly meetings of the Executive Director Team. Controls are also reviewed by the PCT’s internal and external auditors.
The PCT is held to account for its performance by the East of England Strategic Health Authority. It also works closely with local authorities (Hertfordshire County Council, North Herts District Council, Stevenage Borough Council,
Anne Walker Chief Executive
Anne Walker Chief Executive
Alan Pond Financial Director

www.enherts-pct.nhs.uk | 87
Welwyn Hatfield Borough Council, Broxbourne Borough Council, East Herts Council) and is subject to scrutiny by the Hertfordshire County Council Health Scrutiny Committee consisting of County and District Councillors.
The PCT in turn, its primary role as being a commissioning organisation, has responsibilities for monitoring levels of standards, compliance and quality achieved by healthcare organisations and independent health practitioners from which it commissions services. This is evidenced through the Annual Health Check and monitoring of the contracts entered into for services.
2. The purpose of the system of internal controlThe system of internal control is designed to manage risk to a reasonable level rather than to eliminate all risk of failure to achieve policies, aims and objectives; it can therefore only provide reasonable and not absolute assurance of effectiveness.
The system of internal control is based on an ongoing process designed to:
identify and prioritise the risks to the achievement of •the organisation’s policies, aims and objectives, evaluate the likelihood of those risks being realised •and the impact should they be realised, and to manage them efficiently, effectively and economically.
The system of internal control has been in place in East and North Hertfordshire Primary Care Trust for the year ended 31 March 2009 and up to the date of approval of the annual report and accounts.
3. Capacity to handle riskThe Chief Executive is the Accountable Officer for risk management within the PCT. Day to day executive responsibility for governance and control is delegated to the Director of Public Involvement and Corporate Services, who is supported by an Assistant Director of Integrated
Governance and a Compliance Team that provides organisational capacity to effectively monitor and facilitate risk control within the PCT.
A core programme of risk management training based on Training Needs Analysis for all staff groups is in place. Staff are made aware of the key risk-related policies, procedures and protocols at corporate induction and through team briefings, newsletters and the PCT’s intranet. Learning from the reporting and investigation of adverse incidents, serious untoward incidents, complaints, claims, PALS enquiries and internal and external audit reviews is a key part of the internal controls on mitigating risks.
The Board Assurance Framework that identifies principal risks to achieving strategic objectives, assurances and controls to mitigate these risks along with the high level risk register are a standing agenda item on the (Joint) Integrated Governance Committee and reported to the board as per the board business cycle. The Audit Committee receives regular reports from the (Joint) Integrated Governance Committee for the purpose of assuring the board that risks are identified and managed appropriately.
The Secretary of State’s Directions 2004 on work to counter fraud and corruption require NHS bodies to appoint a Local Counter Fraud Specialist (LCFS). The overarching body is the NHS Counter Fraud and Security Management Service (CFSMS). The PCT employs a LCFS who reports directly to the Director of Finance and Commercial Development.
East and North Hertfordshire PCT participated in the Audit Commission’s National Fraud Initiative. The work plan for 2008/2009 has been completed. A local proactive exercise was conducted looking at time sheets and expenses for all PCT staff, as a result new policy and claim forms have been drafted.
4. The risk and control framework
The PCT’s Integrated Governance Strategy along with the Risk Management Policy provide details of the Risk Management systems and process in place.
The Integrated Governance Strategy and the Risk Management Policy are supported by the policy on Reporting and Investigating Adverse Incidents, Serious Untoward Incidents, Information Security, Information Governance and the Risk Assessment Procedure.
An overview of the PCT’s strategic objectives, associated risks and controls is provided by the “Board Assurance Framework”. The Board Assurance Framework was approved by the Board in July 2008 following consideration by the (Joint) Integrated Governance Committee and the Audit Committee. The Framework is a working document and is regularly reviewed by the (Joint) Integrated Governance Committee, the Audit Committee and the Board and updated as objectives, risks, controls or required actions change.
The version of the Board Assurance Framework in place as at 31 March 2009 has identified 14 principal risks relating to the PCT’s 12 strategic objectives. The Board Assurance Framework along with regular performance reports provide a mechanism for the board to monitor the controls in place and manage the gaps or weaknesses in controls where the PCT is failing to achieve its strategic objectives. This includes regular reporting and discussions regarding management actions for mitigating the risks associated with under achieving choose and book, Chlamydia screening, smoking cessation, 18 weeks and AandE targets.
The full Assurance Framework can be seen on the PCT’s website by following the link below: http://www.enherts-pct.nhs.uk/Documents/publications/AssuranceframeworkFeb09.pdf
In addition as part of the risk and control framework the PCT maintains both “High Level” and operational risks

88 | Annual Report and Accounts 2008/09
registers, with risks rated as “high” being reported to the (Joint) Integrated Governance Committee and being subject to review by the Board. The PCT’s Information Governance (IG) Strategy is based on the Department of Health’s guidance and the requirements of the Information Governance toolkit. Data security risks are managed in line with the Information Governance Strategy and the PCT’s risk management policy. The Director of Public Involvement and Corporate Services is the Senior Information Risk Owner (SIRO) at board level. The SIRO is also a member of the PCT’s Information Governance Sub-Committee (IGSC) which is chaired by the PCT’s Caldicott Guardian and is responsible for the monitoring and management of the Information Governance arrangements. The committee monitors trends in data security incidents with a view to improving security measures to protect personal identifiable data. This is achieved via a regular review of the identified gaps or risks in meeting the Information Governance agenda. Work on meeting the requirements of the IG toolkit has been ongoing through out the year with the PCT achieving good levels of compliance by March 2009.
The PCT has completed encryption of all PCT owned portable devices that connect to the network and is currently implementing encryption control for external memory devices.
Information Governance training is part of the corporate induction. In addition a training needs analysis for all staff groups for IG training has been completed with tailored training available to meet the needs of the different staff groups.
In 2008 the PCT verified the Information Governance Statement of Compliance (SoC) for all GPs in East and North Hertfordshire with action plans where required. Work is in progress to help support pharmacies to comply with the IG toolkit ahead of the requirement for these services to submit statement of compliance to the Department of Health.
The PCT works in collaboration with public stakeholders including the Overview and Scrutiny Committee, Local Involvement Networks (LINks), Partnership Boards, Carers Forums and the local community networks. The collaborative work ensures that the public are involved with decision making and management of risks that impact on service provision.
Complementary to, and consistent with, the Assurance Framework, is the PCT’s Declaration on Compliance with the “Standards for Better Health”, which forms part of the Government’s “Annual Health Check” overseen by the Care Quality Commission.
Declaration on compliance covering 2008/09 was submitted in April 2009. A copy of the PCTs full Declaration can be seen on the PCT’s website by the following link.http://www.enherts-pct.nhs.uk/Content.asp?id=SXC74F-A77F7D62
The Commissioning Arm of the PCT is ‘fully met’ with the Standards for Better Health with one standard which was declared as ‘met at year end’ rather than for the full year. The Provider arm of the PCT is ‘almost met’ with the Standards for Better Health with 4 standards declared as ‘met at year end’ and one standard where significant lapse in compliance has led to the standard being declared as ‘not met’ for the year.
As an employer with staff entitled to membership of the NHS Pension scheme, control measures are in place to ensure all employer obligations contained within the Scheme regulations are complied with. This includes ensuring that deductions from salary, employer’s contributions and payments in to the Scheme are in accordance with the Scheme rules, and that member Pension Scheme records are accurately updated in accordance with the timescales detailed in the Regulations.
Control measures are in place to ensure that all the organisation’s obligations under equality, diversity and human rights legislation are complied with.
5. Review of effectivenessAs Accountable Officer, I have responsibility for reviewing the effectiveness of the system of internal control. My review is informed in a number of ways. The head of internal audit provides me with an opinion on the overall arrangements for gaining assurance through the Assurance Framework and on the controls reviewed as part of the internal audit work. Executive managers within the organisation who have responsibility for the development and maintenance of the system of internal control provide me with assurance. The Assurance Framework itself provides me with evidence that the effectiveness of controls that manage the risks to the organisation achieving its principal objectives have been reviewed.
My review is also informed by
Audit Commission Use of Resources review•A risk-based programme of internal audits• The PCT’s self-declaration of compliance with the •Healthcare Commission’s “Standards for Better Health” and a review of evidence to support the declarationHealthcare Commission monitoring visits•
I have been advised on the implications of the result of my review of the effectiveness of the system of internal control by the following:-
The PCT Board - The Board places reliance upon the •Audit Committee and (Joint) Integrated Governance Committee for assurances on the extent to which the system of internal control is sound. The Audit committee – The Audit Committee’s primary •role is to independently oversee the governance and assurance process on behalf of the PCT and to report to the Board on the soundness and effectiveness of the systems in place for risk management and internal

www.enherts-pct.nhs.uk | 89
control. In order to provide this assurance to the Board, both Internal and External Audit undertake systems based reviews providing an opinion to the committee on the processes and controls in place. The (Joint) Integrated Governance Committee – •the (Joint) Integrated Governance Committee is responsible for overseeing the identification and management of risks facing the PCT, including the development and monitoring of the PCT’s Assurance Framework and the self declaration on compliance with core standards as part of the Healthcare Commission’s “Annual Health Check”. Executive Directors – the Executive Directors meet •weekly. Risk-related items feature as agenda items for these meetings. All directors have signed and returned Stewardship Statements to me confirming that as far as they are aware, there is no relevant audit information of which the PCT’s auditors are unaware. They have taken all steps that they ought to have taken as directors in order to make themselves aware of any relevant audit information and to establish that the PCT’s auditors are aware of that information. Internal Audit – Internal Audit reviews the system of •internal control and report their findings to the Audit Committee. This includes specific reports on areas relevant to controls, risk and governance and also a Head of Internal Audit Opinion, which informs this Statement on Internal Control.External Audit – Use of Resources review•
A plan to address weaknesses and ensure continuous improvement of the system is in place.
Significant Control IssuesThe Head of Internal Audit Opinion for the period 1 April 2008 – 31 March 2009, states that significant assurance can be given that there is a generally sound system of internal control, designed to meet the organisation’s objectives, and that controls are generally being applied consistently.
The Head of Internal Audit Opinion for 1 April 2008 – 31 March 2009 has not identified any significant issues which require disclosure within the Statement on Internal Control.
There have been no personal data related serious untoward incidents (as classified by the Department of Health) reported by East and North Hertfordshire PCT.
For Standards for Better Health the Commissioning Arm is ‘fully’ compliant with all standards with the exception of C1b (safety alerts) which was ‘met at year end’ rather than for the full year:
Standard C1b (Safety alerts)
Met at year end – this position is based on a lapse identified during the year whereby safety alerts from the predecessor PCTs and also those received and circulated during 2007/08 and early part of 2008/09 were not actioned within the required timescales.
Action taken: Robust actions were put in place with regular reporting to the Clinical Governance Committee. All outstanding alerts were dealt with and appropriately managed with no recorded lapses since December 2008.
The provider arm declared ‘met at year end’ rather than met for the full year on the following 4 standards:
Standard C1b (Safety alerts)
Met at year end – this position is based on a lapse identified during the year whereby safety alerts from the predecessor PCTs and also those received and circulated during 2007/08 and early part of 2008/09 were not actioned within the required timescales.
Action taken: Robust actions were put in place with regular reporting to the Clinical Governance Committee. All outstanding alerts were dealt with and appropriately managed with no recorded lapses since December 2008.
Standard C4b (Medical devices)
Met at year end – this position is based on a lapse identified during the year regarding lack of inventory for medical devices across all services from predecessor PCTs.
Action taken: Action plan has been progressed in year to meet this lapse with a Medical Devices Policy, detailed inventory in place and an annual report to the Board in March 2009.
Standard C5b (Clinical supervision)
Met at year end –A formal supervision framework that was consistently used across the PCT could not be established.
Action taken: A clinical supervision policy and framework has been developed and was implemented by 31 March 2009.
Standard C13c (Confidential Information)
Met at year end – this is based on a lapse identified through incidents of mislaid records during transfer
Action taken: Actions implemented to ensure all records are transferred using secure courier bags and using a tracking system.

90 | Annual Report and Accounts 2008/09
The provider arm declared ‘not met’ for standard C9 details for which are as follows:
Standard C9 – Records Management
Not met - The position is based on lapse identified through the reporting and investigation of serious untoward incidents regarding misplacement of confidential information and lack of universal archiving and retrieval process for medical notes.
Action planned or taken: An action plan has been commenced in year to address this gap with projected completion by June 2009. Actions implemented by March 2009 include all records are transferred using secure courier bags and using a tracking system.
SignedAnne Walker, Chief Executive OfficerEast and North Hertfordshire Primary Care Trust
Date: 10th June 2009 (on behalf of the Board)
Independent Auditors Report of the Board of Directors of East and North Hertfordshire Primary Care Trust
Opinion on the financial statementsI have audited the financial statements of East and North Hertfordshire Primary Care Trust for the year ended 31 March 2009 under the Audit Commission Act 1998. The financial statements comprise the Operating Cost Statement, the Balance Sheet, the Cashflow Statement, the Statement of Total Recognised Gains and Losses and the related notes. These financial statements have been prepared in accordance with the accounting policies directed by the Secretary of State with the consent of the Treasury as relevant to the National Health Service set out within them. I have also audited the information in the Remuneration Report that is described as having been audited.
This report is made solely to the Board of Directors of East and North Hertfordshire Primary Care Trust in accordance with Part II of the Audit Commission Act 1998 and for no other purpose, as set out in paragraph 49 of the Statement of Responsibilities of Auditors and of Audited Bodies prepared by the Audit Commission.
Respective responsibilities of Directors and auditorThe Directors’ responsibilities for preparing the financial statements in accordance with directions made by the Secretary of State are set out in the Statement of Directors’ Responsibilities. The Chief Executive’s responsibility, as Accountable Officer, for ensuring the regularity of financial transactions is set out in the Statement of the Chief Executive’s Responsibilities.
My responsibility is to audit the financial statements in accordance with relevant legal and regulatory requirements and International Standards on Auditing (UK and Ireland).
I report to you my opinion as to whether the financial statements give a true and fair view in accordance with the accounting policies directed by the Secretary of State as
being relevant to the National Health Service in England. I report whether the financial statements and the part of the Remuneration Report to be audited have been properly prepared in accordance with the accounting policies directed by the Secretary of State as being relevant to the National Health Service in England. I report to you whether, in my opinion, the information which comprises the commentary on the financial performance included within the Financial Review, included in the Annual Report, is consistent with the financial statements. I also report whether in all material respects the expenditure and income have been applied to the purposes intended by Parliament and the financial transactions conform to the authorities which govern them.
I review whether the Directors’ Statement on Internal Control reflects compliance with the Department of Health’s requirements, set out in ‘Guidance on Completing the Statement on Internal Control 2008/09’, issued on 25 February 2009. I report if it does not meet the requirements specified by the Department of Health or if the statement is misleading or inconsistent with other information I am aware of from my audit of the financial statements. I am not required to consider, nor have I considered, whether the Directors’ Statement on Internal Control covers all risks and controls. Neither am I required to form an opinion on the effectiveness of the PCT’s corporate governance procedures or its risk and control procedures.
I read the other information contained in the Annual Report and consider whether it is consistent with the audited financial statements. This other information comprises the welcome, about us, facts and figures, the remaining elements of our performance and the unaudited part of the Remuneration Report. I consider the implications for my report if I become aware of any apparent misstatements or material inconsistencies with the financial statements. My responsibilities do not extend to any other information.

www.enherts-pct.nhs.uk | 91
Basis of audit opinionI conducted my audit in accordance with the Audit Commission Act 1998, the Code of Audit Practice issued by the Audit Commission and International Standards on Auditing (UK and Ireland) issued by the Auditing Practices Board. An audit includes examination, on a test basis, of evidence relevant to the amounts and disclosures in the financial statements and the part of the Remuneration Report to be audited. It also includes an assessment of the significant estimates and judgments made by the Directors in the preparation of the financial statements, and of whether the accounting policies are appropriate to the PCT’s circumstances, consistently applied and adequately disclosed.
I planned and performed my audit so as to obtain all the information and explanations which I considered necessary in order to provide me with sufficient evidence to give reasonable assurance that:
the financial statements are free from material •misstatement, whether caused by fraud or other irregularity or error; the financial statements and the part of the •Remuneration Report to be audited have been properly prepared; and in all material respects the expenditure and income •have been applied to the purposes intended by Parliament and the financial transactions conform to the authorities which govern them.
In forming my opinion I also evaluated the overall adequacy of the presentation of information in the financial statements and the part of the Remuneration Report to be audited.
OpinionIn my opinion:
the financial statements give a true and fair view, in •accordance with the accounting policies directed by the Secretary of State as being relevant to the National Health Service in England, of the state of the PCT’s affairs as at 31 March 2009 and of its net operating costs for the year then ended; the part of the Remuneration Report to be audited •has been properly prepared in accordance with the accounting policies directed by the Secretary of State as being relevant to the National Health Service in England; in all material respects the expenditure and income •have been applied to the purposes intended by Parliament and the financial transactions conform to the authorities which govern them; and information which comprises the commentary on the •financial performance included within the Financial Review, included within the Annual Report, is consistent with the financial statements.
Conclusion on arrangements for securing economy, efficiency and effectiveness in the use of resources
Directors’ ResponsibilitiesThe Directors are responsible for putting in place proper arrangements to secure economy, efficiency and effectiveness in the PCT’s use of resources, to ensure proper stewardship and governance and regularly to review the adequacy and effectiveness of these arrangements.
Auditor’s ResponsibilitiesI am required by the Audit Commission Act 1998 to be satisfied that proper arrangements have been made by the PCT for securing economy, efficiency and effectiveness
in its use of resources. The Code of Audit Practice issued by the Audit Commission requires me to report to you my conclusion in relation to proper arrangements, having regard to the Use of Resources Guidance issued by the Audit Commission. I report if significant matters have come to my attention which prevent me from concluding that the PCT has made such proper arrangements. I am not required to consider, nor have I considered, whether all aspects of the PCT’s arrangements for securing economy, efficiency and effectiveness in its use of resources are operating effectively.
Conclusion I have undertaken my audit in accordance with the Code of Audit Practice and having regard to the Use of Resources Guidance published by the Audit Commission in May 2008 and updated in February 2009, I am satisfied that, in all significant respects, East and North Hertfordshire Primary Care Trust made proper arrangements to secure economy, efficiency and effectiveness in its use of resources for the year ending 31 March 2009.
CertificateI certify that I have completed the audit of the accounts in accordance with the requirements of the Audit Commission Act 1998 and the Code of Audit Practice issued by the Audit Commission.
Mark HodgsonDate: 12 June 2009Officer of the Audit CommissionRegus House, 1010 Cambourne Business Park, Cambourne, Cambridge, CB23 6DP

92 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
Op
erat
ing
cost
sta
tem
ent
fo
r th
e ye
ar e
nd
ed 3
1 M
arch
200
9
2008
/09
2007
/08
Not
e£0
00£0
00
Com
mis
sion
ing
Gro
ss o
pera
ting
cost
s4
661,
963
615,
579
Less
: Mis
cella
neou
s in
com
e3
(14,
430)
(10,
517)
Com
mis
sion
ing
net
oper
atin
g co
sts
647,
533
605,
062
Prov
ider
Gro
ss o
pera
ting
cost
s4
56,3
8951
,102
Less
: Mis
cella
neou
s in
com
e3
(8,3
77)
(9,1
41)
Prov
ider
Net
ope
ratin
g co
sts
48,0
1241
,961
Net
ope
rati
ng c
osts
bef
ore
inte
rest
695,
545
647,
023
Inte
rest
rec
eiva
ble
00
Inte
rest
pay
able
818
22
Net
ope
rati
ng c
ost
for
the
finan
cial
yea
r69
5,56
364
7,04
5
The
note
s on
pag
es 9
6 to
127
for
m p
art
of t
his
acco
unt.
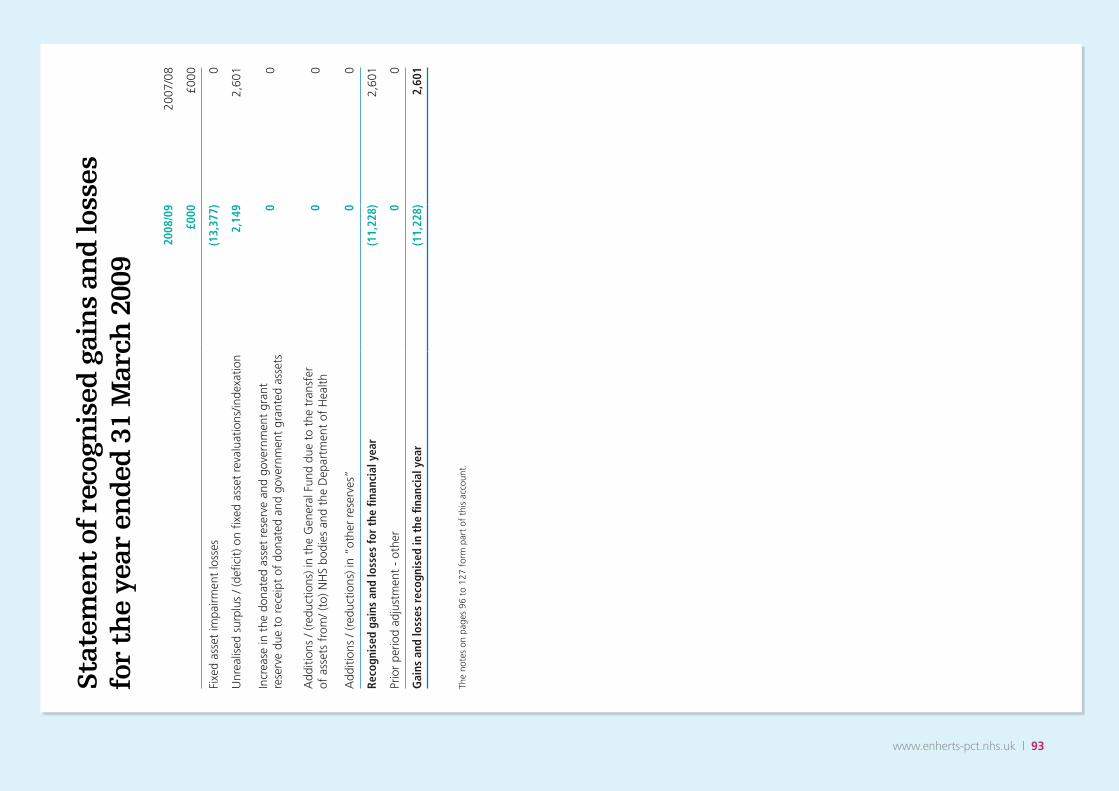
www.enherts-pct.nhs.uk | 93
Sta
tem
ent
of r
ecog
nis
ed g
ain
s an
d lo
sses
fo
r th
e ye
ar e
nd
ed 3
1 M
arch
200
9
2008
/09
2007
/08
£000
£000
Fixe
d as
set
impa
irmen
t lo
sses
(13,
377)
0
Unr
ealis
ed s
urpl
us /
(defi
cit)
on
fixed
ass
et r
eval
uatio
ns/in
dexa
tion
2,14
92,
601
Incr
ease
in t
he d
onat
ed a
sset
res
erve
and
gov
ernm
ent
gran
t re
serv
e du
e to
rec
eipt
of
dona
ted
and
gove
rnm
ent
gran
ted
asse
ts0
0
Add
ition
s / (
redu
ctio
ns) i
n th
e G
ener
al F
und
due
to t
he t
rans
fer
of
ass
ets
from
/ (to
) NH
S bo
dies
and
the
Dep
artm
ent
of H
ealth
00
Add
ition
s / (
redu
ctio
ns) i
n “o
ther
res
erve
s”0
0
Reco
gnis
ed g
ains
and
loss
es fo
r th
e fin
anci
al y
ear
(11,
228)
2,60
1
Prio
r pe
riod
adju
stm
ent
- ot
her
00
Gai
ns a
nd lo
sses
rec
ogni
sed
in t
he fi
nanc
ial y
ear
(11,
228)
2,60
1
The
note
s on
pag
es 9
6 to
127
for
m p
art
of t
his
acco
unt.

94 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
31 M
arch
200
931
Mar
ch 2
008
NO
TE£0
00£0
00£0
00
Fixe
d as
sets
Inta
ngib
le a
sset
s9
00
Tang
ible
ass
ets
10.1
34,8
7245
,098
Inve
stm
ents
10.4
290
Fina
ncia
l ass
ets
10.5
0
34,9
0145
,098
Curr
ent
asse
ts
Stoc
ks a
nd w
ork
in p
rogr
ess
1111
911
9
Deb
tors
1213
,823
11,5
73
Oth
er fi
nanc
ial a
sset
s10
.50
Cas
h at
ban
k an
d in
han
d16
.30
0
Tota
l cur
rent
ass
ets
13,9
4211
,692
CRE
DIT
ORS
: A
mou
nts
falli
ng d
ue w
ithin
one
yea
r13
.1(4
7,25
1)(4
0,12
2)
Oth
er fi
nanc
ial l
iabi
litie
s fa
lling
due
with
in o
ne y
ear
13.1
/10
Net
cur
rent
ass
ets
/ (lia
bilit
ies)
(3
3,30
9)(2
8,43
0)
Tota
l ass
ets
less
cur
rent
liab
iliti
es1,
592
16,6
68
Cre
dito
rs: A
mou
nts
falli
ng d
ue a
fter
mor
e th
an o
ne y
ear
13.1
(32)
(97)
Oth
er fi
nanc
ial l
iabi
litie
s fa
lling
due
aft
er m
ore
than
one
yea
r13
.1/1
0
Prov
isio
ns f
or li
abili
ties
and
char
ges
14(3
,484
)(2
,802
)
Tota
l ass
ets
empl
oyed
(1,9
24)
13,7
69
Fina
nced
by:
Taxp
ayer
s eq
uity
Gen
eral
fun
d15
(12,
460)
(8,0
53)
Reva
luat
ion
rese
rve
158,
917
20,0
43
Don
ated
ass
et r
eser
ve15
1,61
91,
779
Gov
ernm
ent
gran
t re
serv
e15
00
Oth
er r
eser
ves
150
0
Tota
l Tax
paye
rs E
quit
y(1
,924
)13
,769
The
note
s on
pag
es 9
6 to
127
for
m p
art
of t
his
acco
unt.
The
finan
cial
sta
tem
ents
on
page
s 1
to 4
wer
e ap
prov
ed b
y th
e Bo
ard
on 1
0th
June
200
9 an
d si
gned
on
its b
ehal
f by
Chi
ef E
xecu
tive:
D
ate:
10t
h Ju
ne 2
009
Bal
ance
sh
eet
as a
t 31
Mar
ch 2
009
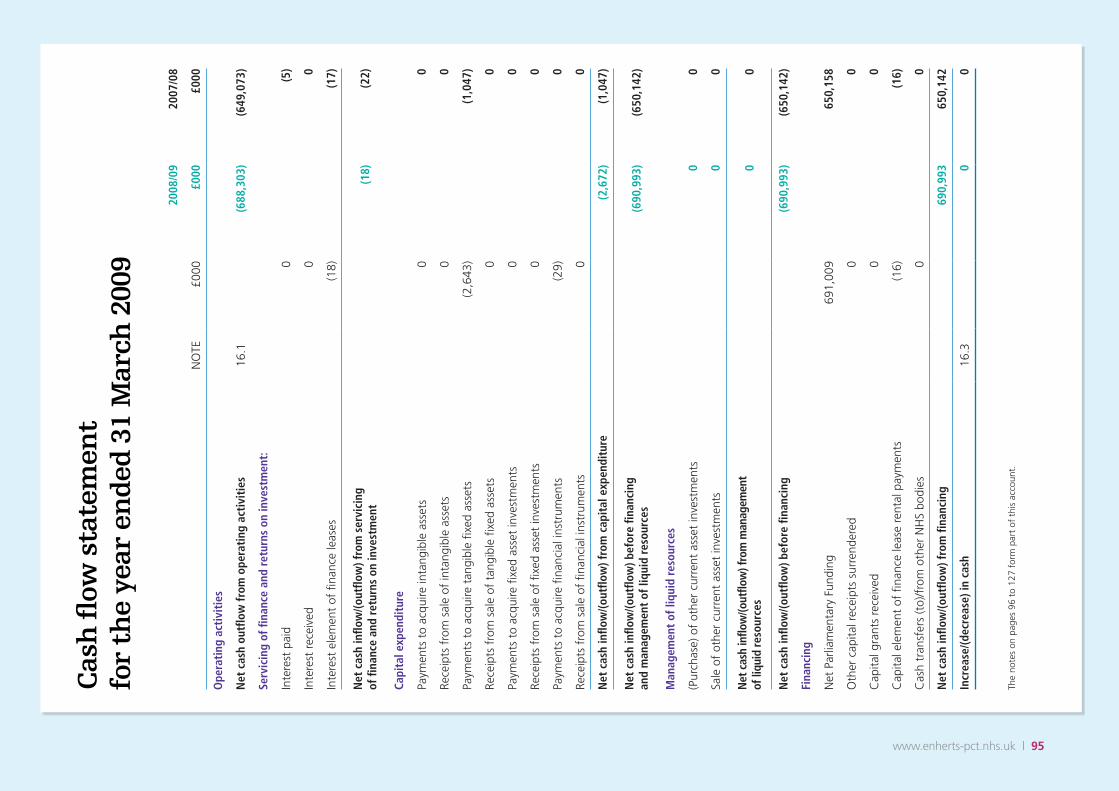
www.enherts-pct.nhs.uk | 95
Cas
h fl
ow s
tate
men
t
for
the
year
en
ded
31
Mar
ch 2
009
2008
/09
2007
/08
NO
TE£0
00£0
00£0
00
Ope
rati
ng a
ctiv
itie
s
Net
cas
h ou
tflow
from
ope
rati
ng a
ctiv
itie
s16
.1(6
88,3
03)
(649
,073
)
Serv
icin
g of
fina
nce
and
retu
rns
on in
vest
men
t:
Inte
rest
pai
d0
(5)
Inte
rest
rec
eive
d0
0
Inte
rest
ele
men
t of
fina
nce
leas
es(1
8)(1
7)
Net
cas
h in
flow
/(out
flow
) fro
m s
ervi
cing
of
fina
nce
and
retu
rns
on in
vest
men
t(1
8)(2
2)
Capi
tal e
xpen
ditu
re
Paym
ents
to
acqu
ire in
tang
ible
ass
ets
00
Rece
ipts
fro
m s
ale
of in
tang
ible
ass
ets
00
Paym
ents
to
acqu
ire t
angi
ble
fixed
ass
ets
(2,6
43)
(1,0
47)
Rece
ipts
fro
m s
ale
of t
angi
ble
fixed
ass
ets
00
Paym
ents
to
acqu
ire fi
xed
asse
t in
vest
men
ts0
0
Rece
ipts
fro
m s
ale
of fi
xed
asse
t in
vest
men
ts0
0
Paym
ents
to
acqu
ire fi
nanc
ial i
nstr
umen
ts(2
9)0
Rece
ipts
fro
m s
ale
of fi
nanc
ial i
nstr
umen
ts0
0
Net
cas
h in
flow
/(out
flow
) fro
m c
apit
al e
xpen
ditu
re(2
,672
)(1
,047
)
Net
cas
h in
flow
/(out
flow
) bef
ore
finan
cing
an
d m
anag
emen
t of
liqu
id r
esou
rces
(690
,993
)(6
50,1
42)
Man
agem
ent
of li
quid
res
ourc
es
(Pur
chas
e) o
f ot
her
curr
ent
asse
t in
vest
men
ts0
0
Sale
of
othe
r cu
rren
t as
set
inve
stm
ents
00
Net
cas
h in
flow
/(out
flow
) fro
m m
anag
emen
t of
liqu
id re
sour
ces
00
Net
cas
h in
flow
/(out
flow
) bef
ore
finan
cing
(690
,993
)(6
50,1
42)
Fina
ncin
g
Net
Par
liam
enta
ry F
undi
ng69
1,00
965
0,15
8
Oth
er c
apita
l rec
eipt
s su
rren
dere
d0
0
Cap
ital g
rant
s re
ceiv
ed0
0
Cap
ital e
lem
ent
of fi
nanc
e le
ase
rent
al p
aym
ents
(16)
(16)
Cas
h tr
ansf
ers
(to)
/fro
m o
ther
NH
S bo
dies
00
Net
cas
h in
flow
/(out
flow
) fro
m fi
nanc
ing
690,
993
650,
142
Incr
ease
/(dec
reas
e) in
cas
h16
.30
0
The
note
s on
pag
es 9
6 to
127
for
m p
art
of t
his
acco
unt.

96 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
The
finan
cial
sta
tem
ents
hav
e be
en p
repa
red
in a
ccor
danc
e w
ith t
he 2
008/
09 F
inan
cial
Rep
ortin
g M
anua
l (FR
eM) i
ssue
d by
HM
Tre
asur
y. T
he p
artic
ular
acc
ount
ing
polic
ies
adop
ted
by t
he P
rimar
y C
are
Trus
t (P
CT)
are
des
crib
ed b
elow
. The
y ha
ve b
een
appl
ied
in d
ealin
g w
ith it
ems
cons
ider
ed m
ater
ial
in r
elat
ion
to t
he a
ccou
nts.
Thes
e ac
coun
ts h
ave
been
pre
pare
d un
der
the
hist
oric
al
cost
con
vent
ion,
mod
ified
to
acco
unt
for
the
reva
luat
ion
of
fixed
ass
ets,
and
sto
ck w
here
mat
eria
l, at
the
ir va
lue
to t
he
busi
ness
by
refe
renc
e to
cur
rent
cos
ts. T
his
is in
acc
orda
nce
with
dire
ctio
ns is
sued
by
the
Secr
etar
y of
Sta
te a
nd a
ppro
ved
by H
M T
reas
ury.
a) In
com
e an
d F
un
din
gTh
e m
ain
sour
ce o
f fu
ndin
g fo
r th
e PC
T is
allo
catio
ns
(Par
liam
enta
ry f
undi
ng) f
rom
the
Dep
artm
ent
of H
ealth
with
in
an a
ppro
ved
cash
lim
it, w
hich
is c
redi
ted
to t
he G
ener
al F
und
of t
he P
CT.
Par
liam
enta
ry f
undi
ng is
reco
gnis
ed in
the
fina
ncia
l pe
riod
in w
hich
the
cas
h is
rece
ived
.
Mis
cella
neou
s in
com
e is
inco
me
whi
ch r
elat
es d
irect
ly t
o th
e op
erat
ing
activ
ities
of
the
PCT.
It p
rinci
pally
com
pris
es
fees
and
cha
rges
for
ser
vice
s pr
ovid
ed o
n a
full
cost
bas
is
to e
xter
nal c
usto
mer
s, a
s w
ell a
s pu
blic
rep
aym
ent
wor
k. It
in
clud
es b
oth
inco
me
appr
opria
ted-
in-a
id o
f th
e Vo
te a
nd
inco
me
to t
he C
onso
lidat
ed F
und
whi
ch H
M T
reas
ury
has
agre
ed s
houl
d be
tre
ated
as
oper
atin
g in
com
e.
Inco
me
is a
ccou
nted
for
app
lyin
g th
e ac
crua
ls c
onve
ntio
n.
Inco
me
is r
ecog
nise
d in
the
per
iod
in w
hich
ser
vice
s ar
e pr
ovid
ed. W
here
inco
me
has
been
rec
eive
d fo
r a
spec
ific
activ
ity t
o be
del
iver
ed in
the
fol
low
ing
finan
cial
ye
ar, t
hat
inco
me
will
be
defe
rred
.
b)
Taxa
tio
nTh
e PC
T is
not
liab
le t
o pa
y co
rpor
atio
n ta
x. M
ost
of t
he
activ
ities
of
the
PCT
are
outs
ide
the
scop
e of
VA
T an
d,
in g
ener
al, o
utpu
t ta
x do
es n
ot a
pply
and
inpu
t ta
x on
pu
rcha
ses
is n
ot r
ecov
erab
le. I
rrec
over
able
VA
T is
cha
rged
to
the
rel
evan
t ex
pend
iture
cat
egor
y or
incl
uded
in t
he
capi
talis
ed p
urch
ase
cost
of
fixed
ass
ets.
Whe
re o
utpu
t ta
x is
ch
arge
d or
inpu
t VA
T is
rec
over
able
, the
am
ount
s st
ated
are
ne
t of
VA
T.
c) F
ixed
Ass
ets
Cap
ital
isat
ion
i.
All
asse
ts f
allin
g in
to t
he f
ollo
win
g ca
tego
ries
are
capi
talis
ed:
Inta
ng
ible
ass
ets
whi
ch c
an b
e va
lued
, are
cap
able
of
bein
g us
ed in
the
PCT’
s ac
tiviti
es fo
r mor
e th
an o
ne y
ear
and
have
a c
ost e
qual
to o
r gre
ater
than
£5,
000;
In
tang
ible
fixe
d as
sets
hel
d fo
r ope
ratio
nal u
se a
re v
alue
d at
hist
oric
al c
ost a
nd a
re d
epre
ciat
ed o
ver t
he e
stim
ated
lif
e of
the
asse
t on
a st
raig
ht li
ne b
asis.
The
car
ryin
g va
lue
of in
tang
ible
ass
ets
is re
view
ed fo
r im
pairm
ent a
t the
end
of
the
first
full
year
follo
win
g ac
quisi
tion
and
in o
ther
pe
riods
if e
vent
s or
cha
nges
in c
ircum
stan
ces
indi
cate
the
carr
ying
val
ue m
ay n
ot b
e re
cove
rabl
e.
Purc
hase
d co
mpu
ter s
oftw
are
licen
ces
are
capi
talis
ed
as in
tang
ible
fixe
d as
sets
whe
re e
xpen
ditu
re o
f at l
east
£5
,000
is in
curr
ed.T
hey
are
amor
tised
ove
r the
sho
rter
of
the
term
of t
he li
cenc
e an
d th
eir u
sefu
l eco
nom
ic li
ves
Tan
gib
le a
sset
s w
hich
are
cap
able
of
bein
g us
ed f
or a
pe
riod
whi
ch e
xcee
ds o
ne y
ear
and
whi
ch:
- in
divi
dual
ly h
ave
a co
st e
qual
to
or g
reat
er t
han
£5,0
00; o
r -
colle
ctiv
ely
have
a c
ost
equa
l to
or g
reat
er t
han
£5,0
00 a
nd in
divi
dual
ly c
ost
mor
e th
an £
250,
whe
re
the
asse
ts a
re f
unct
iona
lly in
terd
epen
dent
, the
y ha
d br
oadl
y si
mul
tane
ous
purc
hase
dat
es a
nd a
re
antic
ipat
ed t
o ha
ve s
imul
tane
ous
disp
osal
dat
es; a
nd
are
unde
r si
ngle
man
ager
ial c
ontr
ol; o
r
- fo
rm p
art
of t
he in
itial
equ
ippi
ng a
nd s
ettin
g-up
cos
t of
a n
ew b
uild
ing,
war
d or
uni
t irr
espe
ctiv
e of
the
ir in
divi
dual
or
colle
ctiv
e co
sts;
or
- fo
rm p
art
of a
n I.T
. net
wor
k w
hich
col
lect
ivel
y ha
s a
cost
of
mor
e th
an £
5,00
0 an
d in
divi
dual
ly h
ave
a co
st
of m
ore
than
£25
0. V
alu
atio
nii.
Inta
ngib
le fi
xed
asse
ts h
eld
for
oper
atio
nal u
se
are
valu
ed a
t hi
stor
ical
cos
t, e
xcep
t Re
sear
ch a
nd
Dev
elop
men
t w
hich
is v
alue
d us
ing
appr
opria
te in
dex
figur
es. S
urpl
us in
tang
ible
ass
ets
are
valu
ed a
t th
e ne
t re
cove
rabl
e am
ount
. Ta
ngib
le fi
xed
asse
ts a
re s
tate
d at
the
low
er o
f re
plac
emen
t co
st a
nd r
ecov
erab
le a
mou
nt. O
n in
itial
rec
ogni
tion
they
are
mea
sure
d at
cos
t (f
or
leas
ed a
sset
s, f
air
valu
e) in
clud
ing
any
cost
s su
ch a
s in
stal
latio
n di
rect
ly a
ttrib
utab
le t
o br
ingi
ng t
hem
into
w
orki
ng c
ondi
tion.
The
car
ryin
g va
lues
of
tang
ible
fixe
d as
sets
are
rev
iew
ed f
or im
pairm
ent
in p
erio
ds if
eve
nts
or c
hang
es in
circ
umst
ance
s in
dica
te t
he c
arry
ing
valu
e m
ay n
ot b
e re
cove
rabl
e.
Lan
d a
nd
Bu
ildin
gs
and
Dw
ellin
gs
Land
and
bui
ldin
gs a
re r
esta
ted
at c
urre
nt c
ost
usin
g pr
ofes
sion
al v
alua
tions
at
five-
year
ly in
terv
als
in a
ccor
danc
e w
ith F
RS 1
5. B
etw
een
valu
atio
ns p
rice
indi
ces
appr
opria
te
to t
he c
ateg
ory
of a
sset
are
app
lied
to a
rriv
e at
the
cur
rent
va
lue.
The
bui
ldin
gs in
dexa
tion
is b
ased
on
the
All
in T
ende
r Pr
ice
Inde
x pu
blis
hed
by t
he B
uild
ing
Cos
t In
form
atio
n Se
rvic
e (B
CIS
). Th
e la
nd in
dex
is b
ased
on
the
resi
dent
ial
build
ing
and
land
val
ues
repo
rted
in t
he P
rope
rty
Mar
ket
Repo
rt p
ublis
hed
by t
he V
alua
tion
Offi
ce. P
rofe
ssio
nal
valu
atio
ns a
re c
arrie
d ou
t by
Val
uers
on
a fiv
e-ye
arly
bas
is.
The
prev
ious
val
uatio
n w
as c
arrie
d ou
t as
at
1 A
pril
2006
.
In v
iew
of
the
sign
ifica
nt f
alls
in t
he U
K p
rope
rty
mar
ket,
Ea
st a
nd N
orth
Her
tfor
dshi
re P
CT
inst
ruct
ed B
oshi
er a
nd
Com
pany
an
inde
pend
ent
firm
of
char
tere
d su
rvey
ors
(RIC
S),
to p
rovi
de a
dvic
e in
acc
orda
nce
with
FRS
11
in r
espe
ct
of v
ario
us f
reeh
old
prop
ertie
s fo
rmin
g pa
rt o
f th
e PC
T’s
esta
te a
s at
31
Mar
ch 2
009.
The
rev
alua
tion
resu
lted
in a
ne
t re
duct
ion
of £
10,9
95,0
00 o
n La
nd a
nd £
266,
000
on
Build
ings
tot
allin
g £1
1,26
1,00
0.
The
valu
atio
ns w
ere
carr
ied
out
in a
ccor
danc
e w
ith t
he
Roya
l Ins
titut
e of
Cha
rter
ed S
urve
yors
(RIC
S) A
ppra
isal
and
Va
luat
ion
Man
ual i
nsof
ar a
s th
ese
term
s ar
e co
nsis
tent
with
th
e ag
reed
req
uire
men
ts o
f th
e D
epar
tmen
t of
Hea
lth a
nd
Not
es t
o th
e ac
cou
nts
www.enherts-pct.nhs.uk | 97
HM
Tre
asur
y. T
here
are
dep
artu
res
from
the
RIC
S A
ppra
isal
an
d Va
luat
ions
Sta
ndar
ds a
gree
d be
twee
n H
M T
reas
ury
and
the
NH
S Ex
ecut
ive
whi
ch a
re n
oted
in t
he v
alua
tion
repo
rt.
The
valu
atio
ns h
ave
been
car
ried
out
prim
arily
on
the
basi
s of
Dep
reci
ated
Rep
lace
men
t C
ost
for
spec
ialis
ed o
pera
tiona
l pr
oper
ty a
nd E
xist
ing
Use
Val
ue f
or n
on-s
peci
alis
ed
oper
atio
nal p
rope
rty.
In r
espe
ct o
f no
n-op
erat
iona
l pro
pert
ies,
incl
udin
g su
rplu
s la
nd, t
he v
alua
tions
hav
e be
en c
arrie
d ou
t at
Ope
n M
arke
t Va
lue.
The
val
ue o
f la
nd f
or e
xist
ing
use
purp
oses
is a
sses
sed
to E
xist
ing
Use
Val
ue.
Add
ition
al a
ltern
ativ
e O
pen
Mar
ket
Valu
e fig
ures
hav
e on
ly
been
sup
plie
d fo
r op
erat
iona
l ass
ets
sche
dule
d fo
r im
min
ent
clos
ure
and
subs
eque
nt d
ispo
sal.
Gai
ns m
ade
from
inde
xatio
n an
d re
valu
atio
ns a
re t
aken
to
the
rev
alua
tion
rese
rve.
Los
ses
aris
ing
from
rev
alua
tions
ar
e re
cogn
ised
as
impa
irmen
ts a
nd a
re c
harg
ed t
o th
e re
valu
atio
n re
serv
e to
the
ext
ent
that
a b
alan
ce e
xist
s in
re
latio
n to
the
rev
alue
d as
set.
Los
ses
in e
xces
s of
tha
t am
ount
are
cha
rged
to
the
curr
ent
year
’s O
pera
ting
Cos
t St
atem
ent
(OC
S), u
nles
s it
can
be d
emon
stra
ted
that
the
re
cove
rabl
e am
ount
is g
reat
er t
han
the
reva
lued
am
ount
in
whi
ch c
ase
the
impa
irmen
t is
tak
en t
o th
e re
valu
atio
n re
serv
e. Im
pairm
ents
res
ultin
g fr
om p
rice
chan
ges
are
char
ged
to t
he S
tate
men
t of
Rec
ogni
sed
Gai
ns a
nd L
osse
s.
As
a re
sult
of t
his
reva
luat
ion,
a t
otal
of
£33,
000
was
ch
arge
d to
the
OC
S in
200
8/9
finan
cial
yea
r. Fa
lls in
val
ue
whe
n ne
wly
con
stru
cted
ass
ets
are
brou
ght
into
use
are
ch
arge
d in
ful
l to
the
OC
S. T
hese
fal
ls in
val
ue r
esul
t fr
om
the
adop
tion
of id
eal c
ondi
tions
as
the
basi
s fo
r de
prec
iate
d re
plac
emen
t co
st v
alua
tions
.
Land
and
bui
ldin
gs h
eld
unde
r fin
ance
leas
es a
re c
apita
lised
at
ince
ptio
n at
the
fai
r va
lue
of t
he a
sset
but
may
be
subs
eque
ntly
rev
alue
d by
the
Dis
tric
t Va
luer
. The
val
uatio
ns
do n
ot in
clud
e no
tiona
l dire
ctly
att
ribut
able
acq
uisi
tion
cost
s no
r ha
ve s
ellin
g co
sts
been
ded
ucte
d, s
ince
the
y ar
e re
gard
ed a
s no
t m
ater
ial.
Fixe
d a
sset
inve
stm
ents
On
1st
July
200
8 Ea
st a
nd N
orth
Her
tfor
dshi
re P
CT
acqu
ired
both
loan
not
es a
nd 4
00 s
hare
s to
the
val
ue o
f £2
7,57
0 an
d £4
00 r
espe
ctiv
ely
in “
Ass
embl
e C
omm
unity
Par
tner
ship
” th
e na
me
of t
he n
ewly
for
med
par
tner
ship
com
pany
. Thi
s 25
ye
ar p
artn
erin
g ag
reem
ent
arra
ngem
ent
is w
ith B
edfo
rdsh
ire
PCT,
Milt
on K
eyne
s PC
T, G
uild
hous
e (a
priv
ate
deve
lopm
ent
com
pany
) and
loca
l pub
lic s
ecto
r au
thor
ities
cov
ered
by
the
thre
e pa
rtic
ipan
t PC
T ar
eas.
This
typ
e of
arr
ange
men
t is
for
mal
ly k
now
as
LIFT
(Loc
al
Impr
ovem
ent
Fina
nce
Trus
t) a
nd t
he v
alue
is s
how
n at
the
hi
stor
ical
cos
t to
acq
uire
the
loan
not
es a
nd s
hare
s as
at
1st
July
200
8. F
ixed
ass
et in
vest
men
ts a
re r
ecor
ded
at M
arke
t Va
lue
and
will
be
valu
ed a
nnua
lly. A
ny in
crea
se in
val
ue is
ta
ken
in f
ull t
o th
e re
valu
atio
n re
serv
e. A
ny im
pairm
ent
in
valu
e is
cha
rged
to
oper
atin
g ex
pend
iture
.
Equ
ipm
ent
Ope
ratio
nal e
quip
men
t is
car
ried
at c
urre
nt v
alue
. Whe
re
asse
ts a
re a
t lo
w v
alue
, and
/or
have
sho
rt u
sefu
l eco
nom
ic
lives
, the
se a
re c
arrie
d at
dep
reci
ated
his
toric
cos
t as
a p
roxy
fo
r cu
rren
t va
lue.
Equ
ipm
ent
surp
lus
to r
equi
rem
ents
is
valu
ed a
t ne
t re
cove
rabl
e am
ount
and
ass
ets
held
und
er
finan
ce le
ases
are
cap
italis
ed a
t th
e fa
ir va
lue
of t
he a
sset
s.
Ass
ets
in t
he
cou
rse
of
con
stru
ctio
nA
sset
s in
the
cou
rse
of c
onst
ruct
ion
are
valu
ed a
t cu
rren
t co
st u
sing
the
inde
x as
for
land
and
bui
ldin
gs (s
eeab
ove)
. The
se a
sset
s in
clud
e an
y ex
istin
g la
nd o
r bu
ildin
gs
unde
r th
e co
ntro
l of
a co
ntra
ctor
.
Res
idu
al in
tere
sts
in o
ff-b
alan
ce
shee
t Pr
ivat
e Fi
nan
ce In
itia
tive
pro
per
ties
Resi
dual
inte
rest
s in
off
-bal
ance
she
et P
rivat
e Fi
nanc
e In
itiat
ive
prop
ertie
s ar
e in
clud
ed in
tan
gibl
e fix
ed a
sset
s un
der
‘’ass
ets
unde
r co
nstr
uctio
n an
d pa
ymen
ts o
n ac
coun
t’ w
here
th
e PF
I con
trac
t sp
ecifi
es t
he a
mou
nt a
t w
hich
the
ass
ets
will
be
tran
sfer
red
to t
he P
CT
at t
he e
nd o
f th
e co
ntra
ct.
The
resi
dual
inte
rest
is b
uilt
up d
urin
g th
e lif
e of
the
con
trac
t by
cap
italis
ing
the
unita
ry c
harg
e so
tha
t at
the
end
of
the
cont
ract
the
bal
ance
she
et v
alue
of
the
resi
dual
val
ue p
lus
the
spec
ified
am
ount
equ
al t
he e
xpec
ted
valu
e of
the
resi
dual
as
set
at t
he e
nd o
f th
e co
ntra
ct. T
he e
stim
ated
fai
r va
lue
of
the
asse
t on
reve
rsio
n is
det
erm
ined
by
the
Dis
tric
t Va
luer
ba
sed
on D
epar
tmen
t of
Hea
lth g
uida
nce.
iii
. Dep
reci
atio
n, a
mo
rtis
atio
n a
nd
imp
airm
ents
Ta
ngib
le fi
xed
asse
ts a
re d
epre
ciat
ed a
t ra
tes
calc
ulat
ed
to w
rite
them
dow
n to
est
imat
ed r
esid
ual v
alue
on
a st
raig
ht li
ne b
asis
ove
r th
eir
estim
ated
use
ful l
ives
. Fr
eeho
ld la
nd a
nd la
nd a
nd b
uild
ings
sur
plus
to
requ
irem
ents
are
not
dep
reci
ated
. Ass
ets
in t
he c
ours
e of
con
stru
ctio
n an
d re
sidu
al in
tere
sts
in o
ff-b
alan
ce
shee
t Pr
ivat
e Fi
nanc
e In
itiat
ive
cont
ract
ass
ets
are
not
depr
ecia
ted
until
the
ass
et is
bro
ught
into
use
or
reve
rts
to t
he P
CT,
res
pect
ivel
y.
Build
ings
, ins
talla
tions
and
fitt
ings
are
dep
reci
ated
on
thei
r cu
rren
t va
lue
over
the
est
imat
ed r
emai
ning
life
of
the
asse
t as
adv
ised
by
the
Dis
tric
t Va
luer
. Le
aseh
olds
are
dep
reci
ated
ove
r the
prim
ary
leas
e te
rm.
Equi
pmen
t is
dep
reci
ated
on
curr
ent
cost
eve
nly
over
th
e es
timat
ed li
fe o
f th
e as
set.
In
tang
ible
ass
ets
are
amor
tised
ove
r th
e es
timat
ed li
ves
of t
he a
sset
s.
Whe
re t
he u
sefu
l eco
nom
ic li
fe o
f an
ass
et is
red
uced
fr
om t
hat
initi
ally
est
imat
ed d
ue t
o th
e re
valu
atio
n of
an
ass
et f
or s
ale,
dep
reci
atio
n is
cha
rged
to
brin
g th
e va
lue
of t
he a
sset
to
its v
alue
at
the
poin
t of
sal
e.
Purc
hase
d co
mpu
ter s
oftw
are
licen
ces
are
amor
tised
ove
r th
e sh
orte
r of t
he te
rm o
f the
lice
nse
and
thei
r use
ful
econ
omic
live
s. T
hey
are
amor
tised
ove
r the
sho
rter
of
the
term
of t
he li
cenc
e an
d th
eir u
sefu
l eco
nom
ic li
ves.
In
form
atio
n Te
chno
logy
equ
ipm
ent i
s de
prec
iate
d ov
er 4
ye
ars
in li
ne w
ith it
s re
plac
emen
t pol
icy.
iv
. Do
nat
ed A
sset
s D
onat
ed t
angi
ble
fixed
ass
ets
are
capi
talis
ed a
t th
eir
valu
atio
n on
rec
eipt
and
thi
s va
lue
is c
redi
ted
to t
he
dona
ted
asse
t re
serv
e. D
onat
ed a
sset
s ar
e re
valu
ed
and
depr
ecia
ted
as d
escr
ibed
abo
ve f
or p
urch
ased
as
sets
. Gai
ns a
nd lo
sses
on
reva
luat
ions
are
tak
en
98 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
Not
es t
o th
e ac
cou
nts
to t
he D
onat
ed A
sset
Res
erve
and
, eac
h ye
ar, a
n am
ount
equ
al t
o th
e de
prec
iatio
n ch
arge
on
the
asse
t is
rel
ease
d fr
om t
he D
onat
ed A
sset
Res
erve
to
the
Ope
ratin
g C
ost
Stat
emen
t. S
imila
rly, a
ny im
pairm
ent
on d
onat
ed a
sset
s ch
arge
d to
the
Ope
ratin
g C
ost
Stat
emen
t is
mat
ched
by
a tr
ansf
er f
rom
the
don
ated
as
set
rese
rve.
On
sale
of
dona
ted
asse
ts, t
he v
alue
of
the
sale
pro
ceed
s is
tra
nsfe
rred
fro
m t
he d
onat
ed
asse
t re
serv
e to
the
gen
eral
fun
d.
Go
vern
men
t G
ran
tsv.
Gov
ernm
ent
gran
ts a
re g
rant
s fr
om G
over
nmen
t bo
dies
oth
er t
han
fund
s fr
om N
HS
bodi
es o
r fu
nds
awar
ded
by P
arlia
men
tary
Vot
e. G
over
nmen
t gr
ants
in
res
pect
of
capi
tal e
xpen
ditu
re a
re c
redi
ted
to a
go
vern
men
t gr
ant
rese
rve
and
are
rele
ased
to
the
OC
S ov
er t
he e
xpec
ted
usef
ul li
ves
of t
he r
elev
ant
asse
ts
by e
qual
ann
ual i
nsta
lmen
ts. G
rant
s of
a r
even
ue
natu
re a
re c
redi
ted
to m
isce
llane
ous
inco
me
in t
he
Ope
ratin
g C
ost
Stat
emen
t so
as
to m
atch
the
m w
ith
the
expe
nditu
re t
o w
hich
the
y re
late
.
d)
Cas
h, B
ank
and
Ove
rdra
ft:
Cas
h, b
ank
and
over
draf
t ba
lanc
es a
re r
ecor
ded
at c
urre
nt
valu
es. I
nter
est
earn
ed o
n ba
nk a
ccou
nts
and
inte
rest
ch
arge
d on
ove
rdra
fts
are
reco
rded
as,
res
pect
ivel
y, ‘I
nter
est
rece
ivab
le’ a
nd ‘
Inte
rest
pay
able
’ in
the
perio
ds t
o w
hich
th
ey r
elat
e. B
ank
char
ges
are
reco
rded
as
oper
atin
g ex
pend
iture
in t
he p
erio
ds t
o w
hich
the
y re
late
.
e) P
oo
led
bu
dg
ets
The
PCT
has
ente
red
into
a p
oole
d bu
dget
with
Her
tfor
dshi
re
Cou
nty
Cou
ncil.
Und
er t
he a
rran
gem
ent
fund
s ar
e po
oled
un
der
S75
of t
he N
HS
Act
200
6 fo
r M
enta
l Hea
lth, L
earn
ing
Dis
abili
ties
and
cert
ain
othe
r se
rvic
es.
The
pool
is h
oste
d by
Her
tfor
dshi
re C
ount
y C
ounc
il. T
he P
CT
mak
es c
ontr
ibut
ions
to
the
pool
for
ser
vice
s to
be
prov
ided
as
par
t of
its
com
mis
sion
ing
role
.
In a
ccor
danc
e w
ith F
RS9,
the
PC
T’s
shar
e of
the
ass
ets
and
liabi
litie
s of
the
poo
l will
be
acco
unte
d fo
r in
the
boo
ks o
f ac
coun
ts a
s de
term
ined
in t
he p
oole
d bu
dget
agr
eem
ent.
f) L
ease
sW
here
sub
stan
tially
all
risks
and
rew
ards
of
owne
rshi
p of
a
leas
ed a
sset
are
bor
ne b
y th
e PC
T, t
he a
sset
is r
ecor
ded
as a
ta
ngib
le fi
xed
asse
t an
d a
debt
is r
ecor
ded
to t
he le
ssor
of
the
min
imum
leas
e pa
ymen
t di
scou
nted
by
the
inte
rest
rat
e im
plic
it in
the
leas
e. T
he in
tere
st e
lem
ent
of fi
nanc
e le
ase
paym
ents
is c
harg
ed t
o th
e O
pera
ting
Cos
t St
atem
ent
over
th
e pe
riod
of t
he le
ase
at a
con
stan
t ra
te in
rel
atio
n to
the
ba
lanc
e ou
tsta
ndin
g.
Oth
er le
ases
are
reg
arde
d as
ope
ratin
g le
ases
and
the
ren
tals
ar
e ch
arge
d to
the
Ope
ratin
g C
ost
Stat
emen
t on
a s
trai
ght
line
basi
s ov
er t
he t
erm
of
the
leas
e.
g)
Priv
ate
Fin
ance
Init
iati
veTh
e N
HS
follo
ws
HM
Tre
asur
y’s
‘Tec
hnic
al N
ote
1 (r
evis
ed)
How
to
Acc
ount
for
PFI
tra
nsac
tions
‘ w
hich
pro
vide
s pr
actic
al g
uida
nce
for
the
appl
icat
ion
of t
he A
pplic
atio
n
Not
e F
FRS5
am
endm
ent
and
the
guid
ance
‘Lan
d an
d Bu
ildin
gs in
PFI
sch
emes
Ver
sion
2’.
Whe
re t
he b
alan
ce o
f th
e ris
ks a
nd re
war
ds o
f ow
ners
hip
of t
he P
FI p
rope
rty
are
born
e by
the
PFI
ope
rato
r, th
e PF
I pa
ymen
ts a
re re
cord
ed a
s an
ope
ratin
g ex
pens
e. W
here
the
PC
T ha
s co
ntrib
uted
ass
ets,
a p
repa
ymen
t fo
r th
eir
fair
valu
e is
reco
gnis
ed a
nd a
mor
tised
ove
r th
e lif
e of
the
PFI
con
trac
t by
a c
harg
e to
the
OC
S. W
here
, at
the
end
of a
PFI
con
trac
t,
a pr
oper
ty re
vert
s to
the
PC
T, t
he d
iffer
ence
bet
wee
n th
e ex
pect
ed f
air
valu
e of
the
resi
dual
ass
et o
n re
vers
ion
and
any
agre
ed p
aym
ent
on re
vers
ion
is b
uilt
up o
ver
the
life
of t
he
cont
ract
by
capi
talis
ing
part
of
the
unita
ry c
harg
e ea
ch y
ear,
as a
tan
gibl
e fix
ed a
sset
.Und
er U
K G
AA
P, t
he c
urre
nt H
erts
an
d Es
sex
hosp
ital i
s an
off
bal
ance
she
et s
chem
e. T
he P
CT
is
capi
talis
ing
part
of
the
annu
al u
nita
ry p
aym
ent
to re
ach
the
resi
dual
inte
rest
of
appr
ox £
7m in
the
yea
r 20
33. T
his
resi
dual
in
tere
st is
sho
wn
as a
n as
set
unde
r co
nstr
uctio
n w
ithin
fixe
d as
sets
and
the
val
ue a
s at
31s
t M
arch
200
9 is
£95
6,00
0.
h)
Sto
cks
and
wo
rk-i
n-p
rog
ress
Stoc
ks c
ompr
ise
raw
mat
eria
ls a
nd c
onsu
mab
les
and
are
valu
ed a
t th
e lo
wer
of
cost
and
net
rea
lisab
le v
alue
.
i) R
esea
rch
an
d d
evel
op
men
tEx
pend
iture
on
rese
arch
is n
ot c
apita
lised
. Exp
endi
ture
on
deve
lopm
ent
is c
apita
lised
if it
mee
ts t
he f
ollo
win
g cr
iteria
;-
ther
e is
a c
lear
ly d
efine
d pr
ojec
t-
the
rela
ted
expe
nditu
re is
sep
arat
ely
iden
tifiab
le-
the
outc
ome
of t
he p
roje
ct h
as b
een
asse
ssed
with
re
ason
able
cer
tain
ty a
s to
;-
its t
echn
ical
fea
sibi
lity
- its
res
ultin
g in
a p
rodu
ct o
r se
rvic
e w
hich
will
ev
entu
ally
be
brou
ght
into
use
- ad
equa
te r
esou
rces
exi
st, o
r ar
e re
ason
ably
exp
ecte
d to
be
ava
ilabl
e, t
o en
able
the
pro
ject
to
be c
ompl
eted
and
to
prov
ide
any
cons
eque
ntia
l inc
reas
e in
wor
king
cap
ital.
Expe
nditu
re s
o de
ferr
ed is
lim
ited
to t
he v
alue
of
futu
re
bene
fits
expe
cted
and
is a
mor
tised
thr
ough
the
Ope
ratin
g C
ost
Stat
emen
t on
a s
yste
mat
ic b
asis
ove
r th
e pe
riod
expe
cted
to
bene
fit f
rom
the
pro
ject
. It
is r
eval
ued
on t
he
basi
s of
cur
rent
cos
t. T
he a
mor
tisat
ion
char
ge is
cal
cula
ted
on t
he s
ame
basi
s as
for
dep
reci
atio
n i.e
. on
a qu
arte
rly
basi
s. E
xpen
ditu
re w
hich
doe
s no
t m
eet
the
crite
ria f
or
capi
talis
atio
n is
tre
ated
as
an o
pera
ting
cost
in t
he y
ear
in
whi
ch it
is in
curr
ed.
PCTs
are
una
ble
to d
iscl
ose
the
tota
l am
ount
of
rese
arch
and
de
velo
pmen
t ex
pend
iture
cha
rged
to
the
Ope
ratin
g C
ost
Stat
emen
t be
caus
e so
me
rese
arch
and
dev
elop
men
t ac
tivity
ca
nnot
be
sepa
rate
d fr
om p
atie
nt c
are
activ
ity.
Fixe
d as
sets
acq
uire
d fo
r us
e in
res
earc
h an
d de
velo
pmen
t ar
e am
ortis
ed o
ver
the
life
of t
he a
ssoc
iate
d pr
ojec
t.
j) P
rovi
sio
ns
The
PCT
prov
ides
for
lega
l or
cons
truc
tive
oblig
atio
ns t
hat
are
of u
ncer
tain
tim
ing
or a
mou
nt a
t th
e ba
lanc
e sh
eet
date
on
the
bas
is o
f th
e be
st e
stim
ate
of t
he e
xpen
ditu
re r
equi
red
to s
ettle
the
obl
igat
ion.
Whe
re t
he e
ffec
t of
the
tim
e va
lue
of m
oney
is s
igni
fican
t, t
he e
stim
ated
ris
k-ad
just
ed c
ash

www.enherts-pct.nhs.uk | 99
Not
es t
o th
e ac
cou
nts
flow
s ar
e di
scou
nted
usi
ng t
he T
reas
ury’
s di
scou
nt r
ate
of
2.2%
in r
eal t
erm
s.
k) C
linic
al N
eglig
ence
Co
sts
The
NH
S Li
tigat
ion
Aut
horit
y (N
HSL
A) o
pera
tes
a ris
k po
olin
g sc
hem
e un
der
whi
ch t
he P
CT
pays
an
annu
al c
ontr
ibut
ion
to t
he N
HSL
A w
hich
in re
turn
set
tles
all c
linic
al n
eglig
ence
cl
aim
s. A
lthou
gh t
he N
HSL
A is
adm
inis
trat
ivel
y re
spon
sibl
e fo
r al
l clin
ical
neg
ligen
ce c
ases
the
lega
l lia
bilit
y re
mai
ns w
ith t
he
PCT.
The
tot
al v
alue
of
clin
ical
neg
ligen
ce p
rovi
sion
s ca
rrie
d by
th
e N
HSL
A o
n be
half
of t
he P
CT
is d
iscl
osed
at
Not
e 14
.
l) N
on
-clin
ical
ris
k p
oo
ling
The
PCT
part
icip
ates
in t
he P
rope
rty
Expe
nses
Sch
eme
and
the
Liab
ilitie
s to
Thi
rd P
artie
s Sc
hem
e. B
oth
are
risk
pool
ing
sche
mes
und
er w
hich
the
PC
T pa
ys a
n an
nual
con
trib
utio
n to
the
NH
S Li
tigat
ion
Aut
horit
y an
d, in
ret
urn,
rec
eive
s as
sist
ance
with
the
cos
ts o
f cl
aim
s ar
isin
g. T
he a
nnua
l m
embe
rshi
p co
ntrib
utio
ns, a
nd a
ny ‘e
xces
ses’
pay
able
in
res
pect
of
part
icul
ar c
laim
s ar
e ch
arge
d to
ope
ratin
g ex
pens
es a
s an
d w
hen
they
bec
ome
due.
m)
Loss
es a
nd
Sp
ecia
l Pay
men
tsLo
sses
and
spe
cial
pay
men
ts a
re it
ems
that
Par
liam
ent
wou
ld
not
have
con
tem
plat
ed w
hen
it ag
reed
fun
ds f
or t
he h
ealth
se
rvic
e or
pas
sed
legi
slat
ion.
By
thei
r na
ture
the
y ar
e ite
ms
that
idea
lly s
houl
d no
t ar
ise.
The
y ar
e th
eref
ore
subj
ect
to
spec
ial c
ontr
ol p
roce
dure
s co
mpa
red
with
the
gen
eral
ity o
f pa
ymen
ts. T
hey
are
divi
ded
into
diff
eren
t ca
tego
ries,
whi
ch
gove
rn t
he w
ay e
ach
indi
vidu
al c
ase
is h
andl
ed.
Loss
es a
nd s
peci
al p
aym
ents
are
cha
rged
to
the
rele
vant
fu
nctio
nal h
eadi
ngs,
incl
udin
g lo
sses
whi
ch w
ould
hav
e be
en m
ade
good
thr
ough
insu
ranc
e co
ver
had
PCTs
not
be
en b
earin
g th
eir
own
risks
(with
insu
ranc
e pr
emiu
ms
then
be
ing
incl
uded
as
norm
al r
even
ue e
xpen
ditu
re).
How
ever
, th
e lo
sses
not
e is
com
pile
d di
rect
ly f
rom
the
loss
es a
nd
com
pens
atio
ns r
egis
ter
whi
ch is
pre
pare
d on
a c
ash
basi
s.
n)
Pen
sio
n C
ost
sPa
st a
nd p
rese
nt e
mpl
oyee
s ar
e co
vere
d by
the
pro
visi
ons
of
the
NH
S Pe
nsio
ns S
chem
e. D
etai
ls o
f th
e be
nefit
s pa
yabl
e un
der
thes
e pr
ovis
ions
can
be
foun
d on
the
NH
S Pe
nsio
ns
web
site
at
ww
w.n
hspa
.nhs
.uk/
pens
ions
. The
Sch
eme
is
an u
nfun
ded,
defi
ned
bene
fit s
chem
e th
at c
over
s N
HS
empl
oyer
s, G
ener
al P
ract
ices
and
oth
er b
odie
s, a
llow
ed
unde
r th
e di
rect
ion
of t
he S
ecre
tary
of
Stat
e, in
Eng
land
an
d W
ales
. The
sch
eme
is n
ot d
esig
ned
to b
e ru
n in
a w
ay
that
wou
ld e
nabl
e N
HS
bodi
es t
o id
entif
y th
eir
shar
e of
th
e un
derly
ing
Sche
me
asse
ts a
nd li
abili
ties.
The
refo
re, t
he
Sche
me
is a
ccou
nted
for
as
if it
wer
e a
defin
ed c
ontr
ibut
ion
sche
me:
the
cos
t to
the
NH
S bo
dy o
f pa
rtic
ipat
ing
in t
he
Sche
me
is t
aken
as
equa
l to
the
cont
ribut
ions
pay
able
to
the
Sche
me
for
the
acco
untin
g pe
riod.
The
sche
me
is s
ubje
ct t
o a
full
actu
aria
l val
uatio
n ev
ery
four
ye
ars
(unt
il 20
04, b
ased
on
a fiv
e ye
ar v
alua
tion
cycl
e), a
nd
a FR
S17
acco
untin
g va
luat
ion
ever
y ye
ar. A
n ou
tline
of
thes
e fo
llow
: a.
Fu
ll ac
tuar
ial (
fun
din
g)
valu
atio
n
The
purp
ose
of t
his
valu
atio
n is
to
asse
ss t
he le
vel
of li
abili
ty in
res
pect
of
the
bene
fits
due
unde
r th
e
sche
me
(tak
ing
into
acc
ount
its
rece
nt d
emog
raph
ic
expe
rienc
e), a
nd t
o re
com
men
d th
e co
ntrib
utio
n ra
tes
to b
e pa
id b
y em
ploy
ers
and
sche
me
mem
bers
. The
last
su
ch v
alua
tion,
whi
ch d
eter
min
ed c
urre
nt c
ontr
ibut
ion
rate
s w
as u
nder
take
n as
at
31 M
arch
200
4 an
d co
vere
d th
e pe
riod
from
1 A
pril
1999
to
that
dat
e.
The
conc
lusi
on f
rom
the
200
4 va
luat
ion
was
tha
t th
e Sc
hem
e ha
d ac
cum
ulat
ed a
not
iona
l defi
cit
of £
3.3
billi
on a
gain
st t
he n
otio
nal a
sset
s as
at
31 M
arch
200
4.
How
ever
, aft
er t
akin
g in
to a
ccou
nt t
he c
hang
es in
the
be
nefit
and
con
trib
utio
n st
ruct
ure
effe
ctiv
e fr
om 1
A
pril
2008
, the
Sch
eme
actu
ary
repo
rted
tha
t em
ploy
er
cont
ribut
ions
cou
ld c
ontin
ue a
t th
e ex
istin
g ra
te o
f 14
% o
f pe
nsio
nabl
e pa
y. O
n ad
vice
fro
m t
he S
chem
e ac
tuar
y, s
chem
e co
ntrib
utio
ns m
ay b
e va
ried
from
tim
e to
tim
e to
refl
ect
chan
ges
in t
he s
chem
e’s
liabi
litie
s. U
p to
31
Mar
ch 2
008,
the
vas
t m
ajor
ity o
f em
ploy
ees
paid
co
ntrib
utio
ns a
t th
e ra
te o
f 6%
of
pens
iona
ble
pay.
Fr
om 1
Apr
il 20
08, e
mpl
oyee
s co
ntrib
utio
ns a
re o
n a
tiere
d sc
ale
from
5%
up
to 8
.5%
of
thei
r pe
nsio
nabl
e pa
y de
pend
ing
on t
otal
ear
ning
s.
b
. FR
S17
Acc
ou
nti
ng
val
uat
ion
In
acc
orda
nce
with
FRS
17, a
val
uatio
n of
the
Sch
eme
liabi
lity
is c
arrie
d ou
t an
nual
ly b
y th
e Sc
hem
e A
ctua
ry
as a
t th
e ba
lanc
e sh
eet
date
by
upda
ting
the
resu
lts o
f th
e fu
ll ac
tuar
ial v
alua
tion.
Be
twee
n th
e fu
ll ac
tuar
ial v
alua
tions
at a
two-
year
m
idpo
int,
a fu
ll an
d de
taile
d m
embe
r dat
a-se
t is
prov
ided
to
the
Sche
me
Act
uary
. At t
his
poin
t the
ass
umpt
ions
re
gard
ing
the
com
posit
ion
of th
e Sc
hem
e m
embe
rshi
p ar
e up
date
d to
allo
w th
e Sc
hem
e lia
bilit
y to
be
valu
ed.
The
valu
atio
n of
the
Sch
eme
liabi
lity
as a
t 31
Mar
ch
2009
, is
base
d on
det
aile
d m
embe
rshi
p da
ta a
s at
31
Mar
ch 2
006
(the
late
st m
idpo
int)
upd
ated
to
31 M
arch
20
09 w
ith s
umm
ary
glob
al m
embe
r an
d ac
coun
ting
data
. The
late
st a
sses
smen
t of
the
liab
ilitie
s of
the
Sc
hem
e is
con
tain
ed in
the
Sch
eme
Act
uary
rep
ort,
w
hich
for
ms
part
of
the
annu
al N
HS
Pens
ion
Sche
me
(Eng
land
and
Wal
es) R
esou
rce
Acc
ount
, pub
lishe
d an
nual
ly. T
hese
acc
ount
s ca
n be
vie
wed
on
the
NH
S Pe
nsio
ns w
ebsi
te. C
opie
s ca
n al
so b
e ob
tain
ed f
rom
Th
e St
atio
nery
Offi
ce.
Sch
eme
Pro
visi
on
s as
at
31 M
arch
200
9.Th
e sc
hem
e is
a ‘fi
nal s
alar
y’ s
chem
e.
For e
arly
retir
emen
ts o
ther
than
thos
e du
e to
ill h
ealth
the
addi
tiona
l pen
sion
liabi
litie
s ar
e no
t fun
ded
by th
e sc
hem
e. T
he
full
amou
nt o
f the
liab
ility
for t
he a
dditi
onal
cos
ts is
cha
rged
to
the
Ope
ratin
g C
ost S
tate
men
t at t
he ti
me
the
PCT
com
mits
its
elf t
o th
e re
tirem
ent,
rega
rdle
ss o
f the
met
hod
of p
aym
ent.
The
Sche
me
prov
ides
the
opp
ortu
nity
to
mem
bers
to
incr
ease
the
ir be
nefit
s th
roug
h m
oney
pur
chas
e A
dditi
onal
Vo
lunt
ary
Con
trib
utio
ns (A
VC
s) p
rovi
ded
by a
n ap
prov
ed
pane
l of
life
com
pani
es. U
nder
the
arr
ange
men
t th
e em
ploy
ee/m
embe
r ca
n m
ake
cont
ribut
ions
to
enha
nce
an
empl
oyee
’s pe
nsio
n be
nefit
s. T
he b
enefi
ts p
ayab
le r
elat
e di
rect
ly t
o th
e va
lue
of t
he in
vest
men
ts m
ade.
Fro
m 1

100 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
Not
es t
o th
e ac
cou
nts
Apr
il 20
08 a
vol
unta
ry a
dditi
onal
pen
sion
fac
ility
bec
omes
av
aila
ble,
und
er w
hich
mem
bers
may
pur
chas
e up
to
£5,0
00
per
annu
m o
f ad
ditio
nal p
ensi
on a
t a
cost
det
erm
ined
by
the
actu
ary
from
tim
e-to
-tim
e.
Early
pay
men
t of
a p
ensi
on is
ava
ilabl
e to
mem
bers
of
the
Sche
me
who
are
per
man
ently
inca
pabl
e of
ful
fillin
gth
eir
dutie
s ef
fect
ivel
y th
roug
h ill
ness
or
infir
mity
. A d
eath
gr
atui
ty o
f tw
ice
final
yea
r’s p
ensi
onab
le p
ay f
or d
eath
in s
ervi
ce, a
nd fi
ve t
imes
the
ir an
nual
pen
sion
for
dea
th a
fter
re
tirem
ent,
less
pen
sion
alre
ady
paid
, sub
ject
to
am
axim
um a
mou
nt e
qual
to
twic
e th
e m
embe
r’s fi
nal y
ear’s
pe
nsio
nabl
e pa
y le
ss t
heir
retir
emen
t lu
mp
sum
for
thos
e w
ho d
ie a
fter
ret
irem
ent,
is p
ayab
le.
Exis
tin
g m
emb
ers
at 1
Ap
ril 2
008
Ann
ual p
ensi
ons
are
norm
ally
bas
ed o
n 1/
80th
of
the
best
of
the
last
3 y
ears
pen
sion
able
pay
for
eac
h ye
ar o
f se
rvic
e. A
lu
mp
sum
nor
mal
ly e
quiv
alen
t to
3 y
ears
pen
sion
is p
ayab
le
on r
etire
men
t. F
rom
1 A
pril
2008
the
re is
the
opp
ortu
nity
of
giv
ing
up s
ome
of t
he p
ensi
on t
o in
crea
se t
he r
etire
men
t lu
mp
sum
. Ann
ual i
ncre
ases
are
app
lied
to p
ensi
on
paym
ents
at
rate
s de
fined
by
the
Pens
ions
(Inc
reas
e) A
ct
1971
, and
are
bas
ed o
n ch
ange
s in
ret
ail p
rices
in t
he t
wel
ve
mon
ths
endi
ng 3
0 Se
ptem
ber
in t
he p
revi
ous
cale
ndar
ye
ar. O
n de
ath,
a p
ensi
on o
f 50
% o
f th
e m
embe
r’s p
ensi
on
is n
orm
ally
pay
able
to
the
surv
ivin
g sp
ouse
or
elig
ible
un
mar
ried
part
ner.
New
en
tran
ts f
rom
1 A
pri
l 200
8A
nnua
l pen
sion
s fo
r ne
w e
ntra
nts
from
1 A
pril
2008
w
ere
base
d on
1/6
0th
of t
he b
est
thre
e-ye
ar a
vera
ge o
f pe
nsio
nabl
e ea
rnin
gs in
the
ten
yea
rs b
efor
e re
tirem
ent.
M
embe
rs w
ishi
ng t
o ob
tain
a re
tirem
ent
lu p
sum
may
giv
e up
som
e of
thi
s pe
nsio
n to
obt
ain
a re
tirem
ent
lum
p of
up
to
25%
of
the
tota
l val
ue o
f th
eir
retir
emen
t be
nefit
s. S
urvi
vor
pens
ions
will
be
avai
labl
e to
mar
ried
and
unm
arrie
d pa
rtne
rs
and
will
be
equa
l to
37.5
% o
f th
e m
embe
r’s p
ensi
on.
o)
Fore
ign
Cu
rren
cyTr
ansa
ctio
ns in
for
eign
cur
renc
ies
are
tran
slat
ed in
to
ster
ling
at t
he r
ates
of
exch
ange
cur
rent
at
the
date
s of
the
tr
ansa
ctio
ns.R
esul
ting
exch
ange
gai
ns a
nd lo
sses
are
tak
en
into
the
Ope
ratin
g C
ost
Stat
emen
t.
p)
Thir
d P
arty
Ass
ets
Ass
ets
belo
ngin
g to
thi
rd p
artie
s (s
uch
as m
oney
hel
d on
be
half
of P
atie
nts)
are
not
rec
ogni
sed
in t
he a
ccou
nts
sinc
e th
e Pr
imar
y C
are
Trus
t ha
s no
ben
efici
al in
tere
st in
the
m.
Det
ails
of
third
par
ty a
sset
s ar
e gi
ven
in N
ote
23 t
o th
e ac
coun
ts a
nd N
ote
16.3
for
Pat
ient
s m
onie
s.
q)
Co
st o
f C
apit
al C
har
ge
The
trea
tmen
t of
fixe
d as
sets
in t
he a
ccou
nts
is in
ac
cord
ance
with
the
prin
cipa
l cap
ital c
harg
es o
bjec
tive
to
ensu
re t
hat
such
cha
rges
are
ful
ly r
eflec
ted
in t
he c
ost
of
capi
tal.
The
inte
rest
rat
e ap
plie
d to
the
cos
t of
cap
ital c
harg
e in
the
fina
ncia
l yea
r 20
08/2
009
was
3.5
% (2
007/
2008
: 3.
5%) o
n al
l ass
ets
less
liab
ilitie
s, e
xcep
t fo
r ca
shba
lanc
es
with
the
Offi
ce o
f th
e Pa
ymas
ter
Gen
eral
(OPG
) and
for
D
onat
ed a
sset
s w
here
the
cha
rge
is n
il.
r) F
inan
cial
Inst
rum
ents
Fin
anci
al a
sset
sFi
nanc
ial a
sset
s ar
e re
cogn
ised
on th
e ba
lanc
e sh
eet w
hen
the
PCT
beco
mes
par
ty to
the
finan
cial
inst
rum
ent c
ontr
act o
r, in
th
e ca
se o
f tra
de d
ebto
rs, w
hen
the
good
s or
ser
vice
s ha
ve b
een
deliv
ered
. Fin
anci
al a
sset
s ar
e de
reco
gnise
d w
hen
the
cont
ract
ual
right
s ha
ve e
xpire
d or
the
asse
t has
bee
n tr
ansf
erre
d.
Fina
ncia
l ass
ets
are
initi
ally
rec
ogni
sed
at f
air
valu
e.
Fina
ncia
l ass
ets
are
clas
sifie
d in
to t
he f
ollo
win
g ca
tego
ries:
fin
anci
al a
sset
s ‘a
t fa
ir va
lue
thro
ugh
profi
t an
d lo
ss’;
‘hel
d to
mat
urity
inve
stm
ents
’; ‘a
vaila
ble
for
sale
’ fina
ncia
l ass
ets,
an
d ‘lo
ans
and
rece
ivab
les’
. The
cla
ssifi
catio
n de
pend
s on
the
nat
ure
and
purp
ose
of t
he fi
nanc
ial a
sset
s an
d is
de
term
ined
at
the
time
of in
itial
rec
ogni
tion.
Fin
anci
al a
sset
s at
fai
r va
lue
thro
ug
h p
rofi
t an
d lo
ss
Embe
dded
der
ivat
ives
tha
t ha
ve d
iffer
ent
risks
and
ch
arac
teris
tics
to t
heir
host
con
trac
ts, a
nd c
ontr
acts
with
em
bedd
ed d
eriv
ativ
es w
hose
sep
arat
e va
lue
cann
ot b
e as
cert
aine
d, a
re t
reat
ed a
s fin
anci
al a
sset
s at
fai
r va
lue
thro
ugh
profi
t an
d lo
ss. T
hey
are
held
at
fair
valu
e, w
ith a
ny
resu
ltant
gai
n or
loss
rec
ogni
sed
in t
he O
CS.
The
net
gai
n or
lo
ss in
corp
orat
es a
ny in
tere
st e
arne
d on
the
fina
ncia
l ass
et.
Hel
d t
o m
atu
rity
inve
stm
ents
H
eld
to m
atur
ity in
vest
men
ts a
re n
on-d
eriv
ativ
e fin
anci
al
asse
ts w
ith fi
xed
or d
eter
min
able
pay
men
ts a
nd fi
xed
mat
urity
, and
the
re is
a p
ositi
ve in
tent
ion
and
abili
ty t
o ho
ld t
o m
atur
ity. A
fter
initi
al re
cogn
ition
, the
y ar
e he
ld a
t am
ortis
ed
cost
usi
ng t
he e
ffec
tive
inte
rest
met
hod,
less
any
impa
irmen
t.
Inte
rest
is re
cogn
ised
usi
ng t
he e
ffec
tive
inte
rest
met
hod.
Ava
ilab
le f
or
sale
fin
anci
al a
sset
sA
vaila
ble
for
sale
fina
ncia
l ass
ets
are
non-
deriv
ativ
e fin
anci
al
asse
ts t
hat
are
desi
gnat
ed a
s av
aila
ble
for
sale
or
that
do
not
fal
l with
in a
ny o
f th
e ot
her
thre
e fin
anci
al a
sset
cl
assi
ficat
ions
. The
y ar
e m
easu
red
at f
air
valu
e w
ith c
hang
es
in v
alue
tak
en t
o th
e re
valu
atio
n re
serv
e, w
ith t
he e
xcep
tion
of im
pairm
ent
loss
es. A
ccum
ulat
ed g
ains
or
loss
es a
re
recy
cled
to
the
inco
me
stat
emen
t on
de-
reco
gniti
on.
Loan
s an
d r
ecei
vab
les
Loan
s an
d re
ceiv
able
s ar
e no
n-de
rivat
ive
finan
cial
ass
ets
with
fix
ed o
r de
term
inab
le p
aym
ents
whi
ch a
re n
ot q
uote
d in
an
activ
e m
arke
t. A
fter
initi
al r
ecog
nitio
n, t
hey
are
mea
sure
d at
am
ortis
ed c
ost
usin
g th
e ef
fect
ive
inte
rest
met
hod,
less
any
im
pairm
ent.
Inte
rest
is r
ecog
nise
d us
ing
the
effe
ctiv
e in
tere
st
met
hod.
Fai
r va
lue
is d
eter
min
ed b
y re
fere
nce
to q
uote
d m
arke
t pr
ices
whe
re p
ossi
ble,
oth
erw
ise
by v
alua
tion
tech
niqu
es.
The
effe
ctiv
e in
tere
st r
ate
is t
he r
ate
that
exa
ctly
dis
coun
ts
estim
ated
fut
ure
cash
rec
eipt
s th
roug
h th
e ex
pect
ed li
fe
of t
he fi
nanc
ial a
sset
, to
the
net
carr
ying
am
ount
of
the
finan
cial
ass
et.
At
the
bala
nce
shee
t da
te, t
he P
CT
asse
sses
whe
ther
any
fin
anci
al a
sset
s, o
ther
tha
n th
ose
held
at
‘fai
r va
lue
thro
ugh
profi
t an
d lo
ss’ a
re im
paire
d. F
inan
cial
ass
ets
are
impa
ired
and
impa
irmen
t lo
sses
rec
ogni
sed
if th
ere
is o
bjec
tive
evid
ence
of
impa
irmen
t as
a r
esul
t of
one
or
mor
e ev
ents

www.enherts-pct.nhs.uk | 101
Not
es t
o th
e ac
cou
nts
whi
ch o
ccur
red
afte
r th
e in
itial
rec
ogni
tion
of t
he a
sset
and
w
hich
has
an
impa
ct o
n th
e es
timat
ed f
utur
e ca
sh fl
ows
of
the
asse
t.
For
finan
cial
ass
ets
carr
ied
at a
mor
tised
cos
t, t
he a
mou
nt o
f th
e im
pairm
ent
loss
is m
easu
red
as t
he d
iffer
ence
bet
wee
n th
e as
set’s
car
ryin
g am
ount
and
the
pre
sent
val
ue o
f th
e re
vise
d fu
ture
cas
h flo
ws
disc
ount
ed a
t th
e as
set’s
orig
inal
ef
fect
ive
inte
rest
rat
e. T
he lo
ss is
rec
ogni
sed
in t
he in
com
e st
atem
ent
and
the
carr
ying
am
ount
of
the
asse
t is
red
uced
di
rect
ly, o
r th
roug
h a
prov
isio
n fo
r im
pairm
ent
of r
ecei
vabl
es.
If, in
a s
ubse
quen
t pe
riod,
the
am
ount
of
the
impa
irmen
t lo
ss d
ecre
ases
and
the
dec
reas
e ca
n be
rel
ated
obj
ectiv
ely
to
an e
vent
occ
urrin
g af
ter
the
impa
irmen
t w
as r
ecog
nise
d, t
he
prev
ious
ly r
ecog
nise
d im
pairm
ent
loss
is r
ever
sed
thro
ugh
the
inco
me
stat
emen
t to
the
ext
ent
that
the
car
ryin
g am
ount
of
the
rece
ivab
le a
t th
e da
te o
f th
e im
pairm
ent
is
reve
rsed
doe
s no
t ex
ceed
wha
t th
e am
ortis
ed c
ost
wou
ld
have
bee
n ha
d th
e im
pairm
ent
not
been
rec
ogni
sed.
Fin
anci
al li
abili
ties
Fina
ncia
l lia
bilit
ies
are
reco
gnis
ed o
n th
e ba
lanc
e sh
eet
whe
n th
e Tr
ust
beco
mes
par
ty t
o th
e co
ntra
ctua
l pro
visi
ons
of t
he
finan
cial
inst
rum
ent
or, i
n th
e ca
se o
f tr
ade
cred
itors
, whe
n th
e go
ods
or s
ervi
ces
have
bee
n re
ceiv
ed. F
inan
cial
liab
ilitie
s ar
e de
-rec
ogni
sed
whe
n th
e lia
bilit
y ha
s be
en d
isch
arge
d,
that
is, t
he li
abili
ty h
as b
een
paid
or
has
expi
red.
Fina
ncia
l lia
bilit
ies
are
initi
ally
rec
ogni
sed
at f
air
valu
e.Fi
nanc
ial l
iabi
litie
s ar
e cl
assifi
ed a
s ei
ther
fina
ncia
l lia
bilit
ies
‘at
fair
valu
e th
roug
h pr
ofit a
nd lo
ss’ o
r oth
er fi
nanc
ial l
iabi
litie
s.
Fin
anci
al li
abili
ties
at
fair
val
ue
thro
ug
h p
rofi
t an
d lo
ssEm
bedd
ed d
eriv
ativ
es t
hat
have
diff
eren
t ris
ks a
nd
char
acte
ristic
s to
the
ir ho
st c
ontr
acts
, and
con
trac
ts w
ith
embe
dded
der
ivat
ives
who
se s
epar
ate
valu
e ca
nnot
be
asce
rtai
ned,
are
tre
ated
as
finan
cial
liab
ilitie
s at
fai
r va
lue
thro
ugh
profi
t an
d lo
ss. T
hey
are
held
at
fair
valu
e, w
ith a
ny
resu
ltant
gai
n or
loss
rec
ogni
sed
in t
he in
com
e st
atem
ent.
Th
e ne
t ga
in o
r lo
ss in
corp
orat
es a
ny in
tere
st e
arne
d on
the
fin
anci
al a
sset
.
Oth
er fi
nan
cial
liab
iliti
esA
fter
initi
al re
cogn
ition
, all
othe
r fina
ncia
l lia
bilit
ies
are
mea
sure
d at
am
ortis
ed c
ost u
sing
the
effe
ctiv
e in
tere
st m
etho
d.
The
effe
ctiv
e in
tere
st ra
te is
the
rate
that
exa
ctly
disc
ount
s es
timat
ed fu
ture
cas
h pa
ymen
ts th
roug
h th
e lif
e of
the
asse
t,
to th
e ne
t car
ryin
g am
ount
of t
he fi
nanc
ial l
iabi
lity.
Inte
rest
is
reco
gnise
d us
ing
the
effe
ctiv
e in
tere
st m
etho
d.
s) G
oin
g c
on
cern
The
PCT
is f
unde
d by
the
Dep
artm
ent
of H
ealth
and
th
eref
ore
rem
ains
a g
oing
con
cern
.
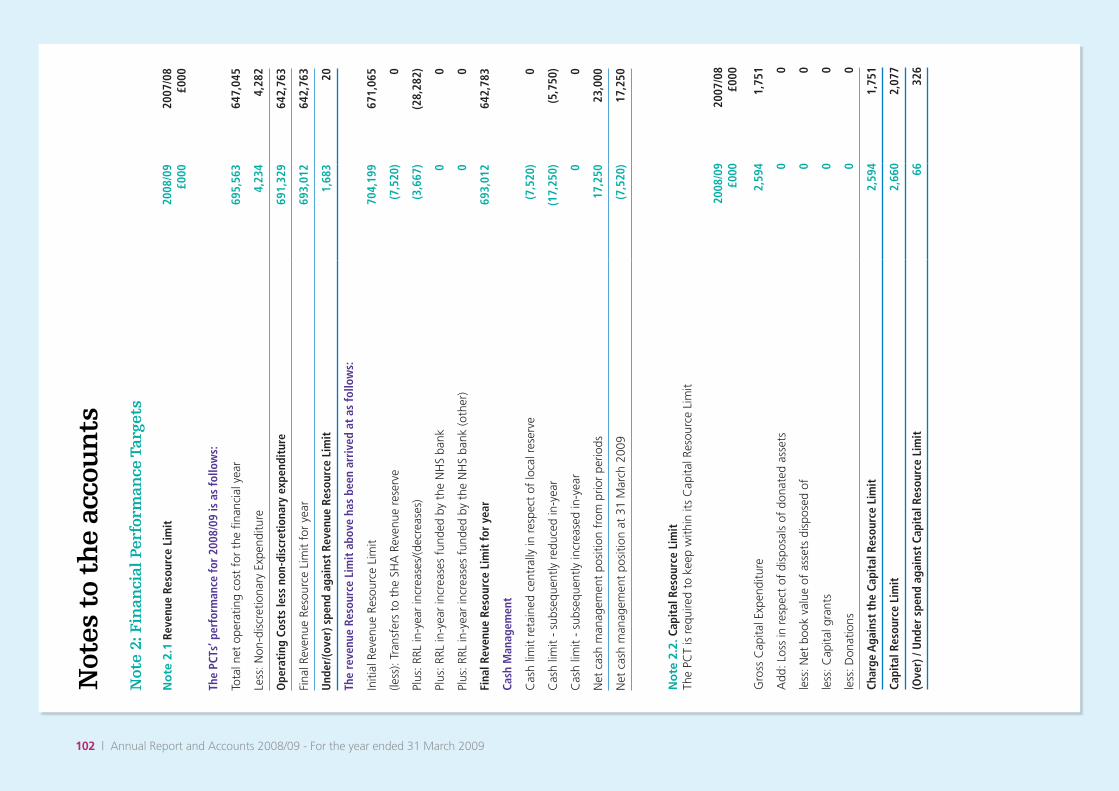
102 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
Not
es t
o th
e ac
cou
nts
No
te 2
.2. C
apit
al R
esou
rce
Lim
itTh
e PC
T is
req
uire
d to
kee
p w
ithin
its
Cap
ital R
esou
rce
Lim
it
2008
/09
£000
2007
/08
£000
Gro
ss C
apita
l Exp
endi
ture
2,59
41,
751
Add
: Los
s in
res
pect
of
disp
osal
s of
don
ated
ass
ets
00
less
: Net
boo
k va
lue
of a
sset
s di
spos
ed o
f0
0
less
: Cap
ital g
rant
s0
0
less
: Don
atio
ns0
0
Char
ge A
gain
st t
he C
apit
al R
esou
rce
Lim
it2,
594
1,75
1
Capi
tal R
esou
rce
Lim
it2,
660
2,07
7
(Ove
r) /
Und
er s
pend
aga
inst
Cap
ital
Res
ourc
e Li
mit
6632
6
Not
e 2:
Fin
anci
al P
erfo
rman
ce T
arge
ts
No
te 2
.1 R
even
ue R
esou
rce
Lim
it20
08/0
9 £0
0020
07/0
8 £0
00
The
PCTs
’ per
form
ance
for
2008
/09
is a
s fo
llow
s:
Tota
l net
ope
ratin
g co
st f
or t
he fi
nanc
ial y
ear
695,
563
647,
045
Less
: Non
-dis
cret
iona
ry E
xpen
ditu
re4,
234
4,28
2
Ope
rati
ng C
osts
less
non
-dis
cret
iona
ry e
xpen
ditu
re69
1,32
964
2,76
3
Fina
l Rev
enue
Res
ourc
e Li
mit
for
year
693,
012
642,
763
Und
er/(o
ver)
spe
nd a
gain
st R
even
ue R
esou
rce
Lim
it1,
683
20
The
reve
nue
Reso
urce
Lim
it a
bove
has
bee
n ar
rive
d at
as
follo
ws:
Initi
al R
even
ue R
esou
rce
Lim
it70
4,19
967
1,06
5
(less
): Tr
ansf
ers
to t
he S
HA
Rev
enue
res
erve
(7,5
20)
0
Plus
: RRL
in-y
ear
incr
ease
s/(d
ecre
ases
)(3
,667
)(2
8,28
2)
Plus
: RRL
in-y
ear
incr
ease
s fu
nded
by
the
NH
S ba
nk0
0
Plus
: RRL
in-y
ear
incr
ease
s fu
nded
by
the
NH
S ba
nk (o
ther
)0
0
Fina
l Rev
enue
Res
ourc
e Li
mit
for
year
693,
012
642,
783
Cash
Man
agem
ent
Cas
h lim
it re
tain
ed c
entr
ally
in r
espe
ct o
f lo
cal r
eser
ve(7
,520
)0
Cas
h lim
it -
subs
eque
ntly
red
uced
in-y
ear
(17,
250)
(5,7
50)
Cas
h lim
it -
subs
eque
ntly
incr
ease
d in
-yea
r0
0
Net
cas
h m
anag
emen
t po
sitio
n fr
om p
rior
perio
ds17
,250
23,0
00
Net
cas
h m
anag
emen
t po
sitio
n at
31
Mar
ch 2
009
(7,5
20)
17,2
50

www.enherts-pct.nhs.uk | 103
Not
es t
o th
e ac
cou
nts
No
te 2
.3. P
rovi
der
full
cost
rec
over
y du
tyTh
e PC
T is
req
uire
d to
rec
over
ful
l cos
ts in
rel
atio
n to
its
prov
ider
fun
ctio
ns. T
he p
erfo
rman
ce f
or 2
008/
09 is
as
follo
ws:
2008
/09
£000
2007
/08
£000
Prov
ider
gro
ss o
pera
ting
cost
56,3
8951
,102
less
: Mis
cella
neou
s in
com
e re
latin
g to
pro
vide
r fu
nctio
ns(8
,377
)(9
,141
)
Net
Ope
ratin
g C
ost
48,0
1241
,961
less
: Cos
ts m
et f
rom
PC
T’s
own
allo
catio
n(4
8,04
3)(4
3,22
2)
Und
er /
(ove
r) r
ecov
ery
of c
osts
(31)
(1,2
61)
No
te 3
. Mis
cella
neou
s In
com
e
£0
00
App
ropr
iate
d in
Aid
£000
N
ot A
ppro
pria
ted
in A
id
2008
/09
£000
2007
/08
£000
Fees
and
Cha
rges
9191
88
Den
tal C
harg
e in
com
e fr
om c
ontr
acto
r le
d G
DS
and
PDS
6,83
36,
833
6,77
4
Den
tal C
harg
e in
com
e fr
om t
rust
led
G
DS
and
PDS
00
0
Pres
crip
tion
Cha
rge
Inco
me
256
256
229
Stra
tegi
c H
ealth
Aut
horit
ies
4,84
44,
844
352
NH
S Tr
usts
4,82
64,
826
5,05
6
Foun
datio
n Tr
usts
882
882
1,14
0
Prim
ary
Car
e Tr
usts
for
Dru
g A
ctio
n Te
ams
00
0
Prim
ary
Car
e Tr
usts
- o
ther
1,95
61,
956
2,73
2
Prim
ary
Car
e Tr
usts
- L
ead
Com
mis
sion
ing
Inco
me
00
20
Engl
ish
RAB
Spec
ial H
ealth
Aut
horit
ies
9898
0
Oth
er E
nglis
h Sp
ecia
l Hea
lth
Aut
horit
ies/
CG
A B
odie
s0
00
Dep
artm
ent
of H
ealth
- S
MPT
B0
00
Dep
artm
ent
of H
ealth
- o
ther
240
240
1
Inco
me
for
Trus
t Im
pairm
ent
00
00
Loca
l Aut
horit
ies
1,23
21,
232
513
Patie
nt T
rans
port
Ser
vice
s0
00
0
Educ
atio
n, T
rain
ing
and
Rese
arch
232
023
247
9
Non
NH
S: P
rivat
e Pa
tient
s0
01
Non
-NH
S: O
vers
eas
Patie
nts
(non
-rec
ipro
cal)
00
0
NH
S In
jury
Cos
ts R
ecov
ery
00
0
Oth
er N
on-N
HS
patie
nt c
are
serv
ices
218
218
753
Cha
ritab
le a
nd o
ther
con
trib
utio
ns
to e
xpen
ditu
re0
00
15
Tran
sfer
fro
m t
he d
onat
ed a
sset
res
erve
058
5858
Tran
sfer
fro
m t
he g
over
nmen
t gr
ant
rese
rve
00
00
Rent
al in
com
e fr
om fi
nanc
e le
ases
00
00
Rent
al in
com
e fr
om o
pera
ting
leas
es0
00
0
Oth
er in
com
e10
293
91,
041
1,44
7
Tota
l mis
cella
neou
s in
com
e8,
964
13,8
4322
,807
19,6
58

104 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
Not
es t
o th
e ac
cou
nts
Not
e 4.
Op
erat
ing
Cos
ts
No
te 4
.1. A
naly
sis
of g
ross
ope
rati
ng c
osts
:
2008
/09
£000
2007
/08
£000
Goo
ds a
nd s
ervi
ces
from
oth
er P
rim
ary
Care
Tru
sts
Hea
lthca
re61
,842
35,4
32
Non
Hea
lthca
re59
042
8
Tota
l62
,432
35,8
60
Goo
ds a
nd s
ervi
ces
from
oth
er N
HS
bodi
es e
xclu
ding
Fou
ndat
ion
Trus
ts
Hea
lthca
re26
2,55
825
8,79
8
Non
Hea
lthca
re71
523
4
Tota
l26
3,27
325
9,03
2
Goo
ds a
nd S
ervi
ces
from
Fou
ndat
ion
Trus
ts32
,186
36,2
67
Purc
hase
of
heal
thca
re f
rom
non
-NH
S pr
ovid
ers
96,3
7791
,294
Soci
al C
are
from
inde
pend
ent
prov
ider
s0
0
Expe
nditu
re o
n D
rugs
Act
ion
Team
s0
0
Non
-GM
S se
rvic
es f
rom
GPs
1,50
71,
185
Con
trac
tor
led
GD
S an
d PD
S30
,663
28,9
37
Trus
t le
d G
DS
and
PDS
179
0
PCT
Boar
d m
embe
rs’ c
osts
422
385
PCT
Exec
utiv
e C
omm
ittee
non
-offi
cer
mem
bers
’ cos
ts13
967
Staf
f co
sts
47,4
0143
,622
Con
sulta
ncy
serv
ices
886
569
GM
S/PM
S/A
PMS/
PCTM
S70
,413
65,6
05
Pres
crib
ing
cost
s75
,535
73,5
65
Phar
mac
eutic
al S
ervi
ces
2,61
92,
179
Loca
l Pha
rmac
eutic
al S
ervi
ce P
ilots
00
New
Pha
rmac
y C
ontr
act
6,96
53,
233
Gen
eral
Oph
thal
mic
Ser
vice
s4,
234
4,28
2
Supp
lies
and
serv
ices
- c
linic
al2,
901
2,61
9
Supp
lies
and
serv
ices
- g
ener
al2,
058
1,45
8
Esta
blis
hmen
t2,
965
3,10
0
Tran
spor
t3
1
Prem
ises
8,27
66,
341
Impa
irmen
t of
deb
tors
491
Dep
reci
atio
n1,
559
2,11
5
Am
ortis
atio
n0
0
Tang
ible
fixe
d as
set
impa
irmen
ts a
nd r
ever
sals
330
Inta
ngib
le fi
xed
asse
t im
pairm
ents
and
rev
ersa
ls0
0
Impa
irmen
ts a
nd r
ever
sals
of
finac
ial a
sset
s (b
y cl
ass)
00

www.enherts-pct.nhs.uk | 105
Not
es t
o th
e ac
cou
nts
Not
e 4.
Op
erat
ing
Cos
ts
No
te 4
.1. A
naly
sis
of g
ross
ope
rati
ng c
osts
:
2008
/09
£000
2007
/08
£000
Cha
nge
in t
he f
air
valu
e of
fina
ncia
l ins
trum
ents
00
NH
S Tr
ust
Impa
irmen
ts0
0
(Pro
fit)/l
oss
on d
ispo
sal o
f fix
ed a
sset
s0
0
Cos
t of
cap
ital c
harg
e14
831
7
Aud
it fe
es27
822
7
Oth
er a
udito
r’s r
emun
erat
ion
00
Clin
ical
neg
ligen
ce c
osts
00
Oth
er fi
nanc
e co
sts
- un
win
ding
of
disc
ount
5285
Redu
ndan
cies
273
216
Educ
atio
n an
d tr
aini
ng68
370
8
Oth
er3,
843
3,41
1
Tota
l71
8,35
266
6,68
1
PCT
Boar
d m
embe
rs’ c
osts
abo
ve in
clud
e £0
for
ear
ly r
etire
men
ts p
rior
to 6
/3/9
5 (2
007/
08 £
0).
Staf
f co
sts
abov
e in
clud
e £0
for
ear
ly r
etire
men
ts p
rior
to 6
/3/9
5 (2
007/
08 £
0).

106 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
Not
es t
o th
e ac
cou
nts
No
te 4
.2. A
naly
sis
of o
pera
ting
exp
endi
ture
by
expe
ndit
ure
clas
sific
atio
nN
ote
4.2
. Pur
chas
e of
Hea
lth
Care
by
PCT
2008
/09
£000
2007
/08
£000
Purc
hase
of P
rim
ary
Hea
lth
Care
GM
S / P
MS/
APM
S / P
CTM
S70
,413
65,6
05
Pres
crib
ing
cost
s75
,535
73,5
65
Phar
mac
eutic
al s
ervi
ces
2,61
92,
179
Con
trac
tor
led
GD
S an
d PD
S30
,663
27,8
83
Trus
t le
d G
DS
and
PDS
677
0
Gen
eral
Oph
thal
mic
Ser
vice
s4,
234
4,28
2
Dep
artm
ent
of H
ealth
Initi
ativ
e Fu
ndin
g0
0
Loca
l Pha
rmac
eutic
al S
ervi
ces
Pilo
ts0
0
New
Pha
rmac
y C
ontr
act
6,96
53,
233
Non
-GM
S Se
rvic
es f
rom
GPs
1,50
71,
185
Oth
er0
0
Tota
l Pri
mar
y H
ealt
hcar
e pu
rcha
sed
192,
613
177,
932
Purc
hase
of S
econ
dary
Hea
lthc
are
Lear
ning
Diffi
culti
es45
,774
42,7
22
Men
tal I
llnes
s47
,098
45,8
67
Mat
erni
ty13
,602
11,9
26
Gen
eral
and
Acu
te30
1,13
428
1,30
3
Acc
iden
t A
nd E
mer
genc
y14
,321
13,4
49
Com
mun
ity H
ealth
Ser
vice
s41
,767
36,3
73
Oth
er C
ontr
actu
al33
,203
29,4
73
Tota
l Sec
onda
ry H
ealt
hcar
e Pu
rcha
sed
496,
899
461,
113
Impa
irmen
ts in
Tru
sts
00
Gra
nts
(rev
enue
) to
fund
Cap
ital P
roje
cts
- G
MS
00
Gra
nts
(rev
enue
) to
LAs
to f
und
Cap
ital P
roje
cts
013
6
Gra
nts
(rev
enue
) to
priv
ate
sect
or t
o fu
nd C
apita
l Pro
ject
s40
31,
272
Gra
nts
(rev
enue
) to
fund
Cap
ital P
roje
cts
- D
enta
l0
0
Gra
nts
(rev
enue
) to
fund
Cap
ital P
roje
cts
- ot
her
00
Tota
l hea
lthc
are
purc
hase
d by
PCT
689,
915
640,
453
Am
ount
of
self-
com
mis
sion
ed s
econ
dary
hea
lthca
re in
clud
ed a
bove
*48
,043
43,2
22
Hea
lthca
re p
urch
ased
fro
m F
ound
atio
n Tr
usts
incl
uded
abo
ve32
,186
35,8
47
Soci
al C
are
from
Inde
pend
ent
Prov
ider
s
* Th
is is
the
tot
al o
f se
cond
ary
heal
thca
re t
hat
the
PCT
com
mis
sion
ed f
rom
itse
lf
Expe
nditu
re o
n m
enta
l hea
lth a
nd le
arni
ng d
isab
ilitie
s in
clud
e th
e co
ntrib
utio
ns m
ade
by t
he P
CT
to t
heco
unty
-wid
e po
oled
bud
get
with
Her
tfor
dshi
re C
ount
y C
ounc
il.
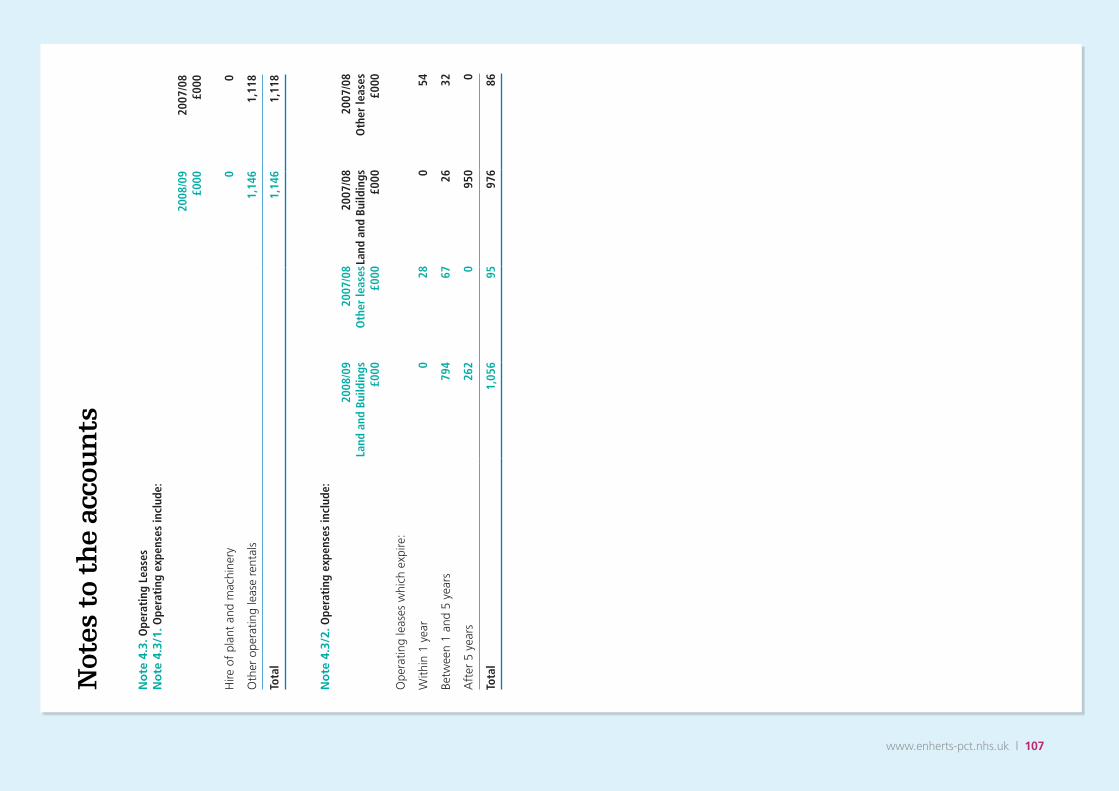
www.enherts-pct.nhs.uk | 107
Not
es t
o th
e ac
cou
nts
No
te 4
.3. O
pera
ting
Lea
ses
No
te 4
.3/1
. Ope
rati
ng e
xpen
ses
incl
ude:
2008
/09
£000
2007
/08
£000
Hire
of
plan
t an
d m
achi
nery
00
Oth
er o
pera
ting
leas
e re
ntal
s1,
146
1,11
8
Tota
l1,
146
1,11
8
No
te 4
.3/2
. Ope
rati
ng e
xpen
ses
incl
ude:
2008
/09
Land
and
Bui
ldin
gs
£000
2007
/08
Oth
er le
ases
£0
00
2007
/08
Land
and
Bui
ldin
gs
£000
2007
/08
Oth
er le
ases
£0
00
Ope
ratin
g le
ases
whi
ch e
xpire
:
With
in 1
yea
r0
280
54
Betw
een
1 an
d 5
year
s79
467
2632
Aft
er 5
yea
rs26
20
950
0
Tota
l1,
056
9597
686

108 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
Not
es t
o th
e ac
cou
nts
Not
e 5.
Sta
ff n
um
ber
s an
d r
elat
ed c
osts
No
te 5
.1. S
taff
cos
ts
Tota
l £0
00
2008
/09
Perm
anen
tly
Empl
oyed
£0
00O
ther
£0
00To
tal
£000
2007
/08
Perm
anen
tly
Empl
oyed
£0
00O
ther
£0
00
Sala
ries
and
wag
es39
,847
37,6
202,
227
36,6
6935
,650
1,01
9
Soci
al s
ecur
ity c
osts
2,87
52,
875
02,
638
2,63
80
Empl
oyer
con
trib
utio
ns t
o N
HSB
SA5,
101
5,10
10
4,70
04,
700
0
Oth
er p
ensi
on c
osts
00
00
00
Tota
l47
,823
45,5
962,
227
44,0
0742
,988
1,01
9
No
te 5
.2. S
taff
Num
bers
Tota
l N
umbe
r
2008
/09
Perm
anen
tly
Empl
oyed
N
umbe
rO
ther
N
umbe
rTo
tal
Num
ber
2007
/08
Perm
anen
tly
Empl
oyed
N
umbe
rO
ther
N
umbe
r
Med
ical
and
den
tal
1615
111
83
Am
bula
nce
staf
f0
00
00
0
Adm
inis
trat
ion
and
esta
tes
488
444
4441
840
018
Hea
lthca
re a
ssis
tant
s an
d ot
her
supp
ort
staf
f22
622
33
209
209
0
Nur
sing
, mid
wife
ry a
nd h
ealth
vi
sitin
g st
aff
425
419
641
541
05
Nur
sing
, mid
wife
ry a
nd h
ealth
vi
sitin
g le
arne
rs8
80
99
0
Scie
ntifi
c, t
hera
peut
ic a
nd
tech
nica
l sta
ff26
526
14
269
261
8
Soci
al C
are
staf
f0
00
00
0
Oth
er20
200
1313
0
Tota
l14
4813
9058
1344
1310
34

www.enherts-pct.nhs.uk | 109
Not
es t
o th
e ac
cou
nts
No
te 5
.3. E
mpl
oyee
ben
efits
Ther
e w
ere
no e
mpl
oyee
ben
efits
in 2
008/
9 or
200
7/8
No
te 5
.4. R
etire
men
ts d
ue to
ill-h
ealth
D
urin
g 20
08/0
9 th
ere
wer
e 6
early
ret
irem
ents
fro
m t
he P
rimar
y C
are
Trus
t ag
reed
on
the
grou
nds
of il
l-hea
lth (2
007/
08:
2). T
he e
stim
ated
add
ition
al p
ensi
on li
abili
ties
of t
hese
ill-h
ealth
ret
irem
ents
(cal
cula
ted
on a
n av
erag
e ba
sis
and
born
e by
th
e N
HS
Pens
ion
Sche
me)
will
be
£220
,527
(200
7/08
: £87
,111
).
No
te 5
.5. M
anag
emen
t co
sts
2008
/09
2007
/08
Man
agem
ent
cost
s (£
000s
)10
,829
10,9
90
Wei
ghte
d po
pula
tion
(Num
ber)
490,
489
490,
489
Man
agem
ent
cost
per
hea
d of
wei
ghte
d po
pula
tion
(£)
22.0
822
.41
The
PCT
mea
sure
s it
s m
anag
emen
t co
sts
acco
rdin
g to
the
defi
niti
ons
prov
ided
by
the
Dep
artm
ent
of H
ealt
h
Not
e 6.
Bet
ter
Pay
men
t P
ract
ice
Cod
e
No
te 6
.1. B
ette
r Pa
ymen
t Pr
acti
ce C
ode
- mea
sure
of c
ompl
ianc
e
2008
/09
Num
ber
2008
/09
£000
2007
/08
Num
ber
2007
/08
£000
Non
-NH
S Cr
edit
ors
Tota
l bill
s pa
id in
the
yea
r19
,935
126,
210
15,1
6812
3,53
7
Tota
l bill
s pa
id w
ithin
tar
get
17,5
0411
4,01
310
,720
108,
334
Perc
enta
ge o
f bi
lls p
aid
with
in t
arge
t87
.81%
90.3
4%70
.68%
87.6
9%
NH
S Cr
edit
ors
Tota
l bill
s pa
id in
the
yea
r2,
007
333,
943
1,89
332
3,09
9
Tota
l bill
s pa
id w
ithin
tar
get
1,44
832
4,51
41,
136
308,
396
Perc
enta
ge o
f bi
lls p
aid
with
in t
arge
t72
.15%
97.1
8%60
.01%
95.4
5%
The
Bett
er P
aym
ent
Prac
tice
Cod
e re
quire
s th
e PC
T to
aim
to
pay
all v
alid
invo
ices
by
the
due
date
or
with
in 3
0 da
ys o
f re
ceip
t of
a v
alid
invo
ice,
whi
chev
er is
late
r.
No
te 6
.2. T
he L
ate
Paym
ent o
f Com
mer
cial
Deb
ts (I
nter
est)
Act
199
8N
o pa
ymen
ts w
ere
mad
e in
res
pect
of
clai
ms
unde
r th
is le
gisl
atio
n in
200
8/9
or 2
007/
8.

110 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
Not
es t
o th
e ac
cou
nts
No
te 7
.2. A
naly
sis
of Im
pair
men
ts c
harg
ed t
o op
erat
ing
cost
s
Inta
ngib
le
Ass
ets
£000
Tang
ible
A
sset
s £0
00
Fixe
d Fi
nanc
ial
Inst
rum
ents
£0
00
Curr
ent
Fina
ncia
l In
stru
men
ts
£000
Tota
l Im
pair
men
ts
£000
Loss
or
dam
age
from
nor
mal
ope
ratio
ns0
00
00
Loss
as
a re
sult
of c
atas
trop
he0
00
00
Aba
ndon
men
t of
ass
ets
in c
ours
e of
co
nstr
uctio
n0
00
00
Unf
orse
en o
bsol
esce
nce
00
00
0
Ove
r sp
ecifi
catio
n of
ass
ets
00
00
0
Oth
er (d
etai
l bel
ow)
00
00
0
Cha
nges
in M
arke
t Pr
ice
033
00
33
Tota
l0
330
033
Not
e 8.
Fin
ance
Cos
ts
2008
/09
£000
2007
/08
£000
Paya
ble:
Fina
nce
leas
es18
17
Late
pay
men
t of
com
mer
cial
deb
t pe
nalti
es0
0
Loan
s0
0
Bank
loan
s an
d ov
erdr
afts
00
Oth
er in
tere
st a
nd fi
nanc
e co
sts
05
Tota
l18
22
Not
e 7.
1. O
ther
Gai
ns
and
Los
ses
Ther
e w
as n
o pr
ofit
or lo
ss o
n th
e di
spos
al o
f ta
ngib
le, i
ntan
gibl
e an
d in
vest
men
t as
sets
, in
2008
/9 a
nd 2
007/
8.
Not
e 9
Inta
ngi
ble
Fix
ed A
sset
s
The
PCT
did
not
hold
any
inta
ngib
le fi
xed
asse
ts in
200
8/9
or 2
007/
8.

www.enherts-pct.nhs.uk | 111
Not
es t
o th
e ac
cou
nts
Not
e 10
. Tan
gib
le F
ixed
Ass
ets
No
te 1
0.1.
Tan
gibl
e fix
ed a
sset
s at
the
bal
ance
she
et d
ate
com
pris
e th
e fo
llow
ing
elem
ents
:
Land£000
Buildings excluding dwellings
£000
Dwellings£000
Assets under construc-tion and payments on
account £000
Plant and machinery£000
Transport equipment
£000
Information technology
£000
Furniture and fittings
£000
Total £000
Cost
or
valu
atio
n
at 1
Apr
il 20
0827
,328
14,7
770
803
729
05,
431
619
49,6
87
Add
ition
s -
purc
hase
d0
1,14
40
277
241
060
732
52,
594
Add
ition
s -
dona
ted
00
00
00
00
0
Add
ition
s -
gove
rnm
ent
gran
ted
00
00
00
00
0
Impa
irmen
ts(1
2,02
6)(1
,351
)0
00
00
0(1
3,37
7)
Inde
xatio
n0
00
00
00
00
Recl
assi
ficat
ions
41(1
74)
00
00
013
30
In y
ear
tran
sfer
s to
/fro
m N
HS
bodi
es0
00
00
00
00
Oth
er in
yea
r re
valu
atio
n1,
031
1,11
80
00
00
02,
149
Dis
posa
ls0
00
00
00
00
At
31 M
arch
200
916
,374
15,5
140
1,08
097
00
6,03
81,
077
41,0
53
Acc
umul
ated
dep
reci
atio
n
at 1
Apr
il 20
0849
60
3,69
340
04,
589
Prov
ided
dur
ing
the
year
852
060
060
443
1,55
9
Impa
irmen
ts0
330
00
00
33
Reve
rsal
of
Impa
irmen
ts0
00
00
00
Recl
assi
ficat
ions
(8)
00
80
Inde
xatio
n0
00
0
Oth
er in
yea
r re
valu
atio
n0
00
00
00
In y
ear
tran
sfer
s to
/fro
m N
HS
bodi
es0
00
00
00
Dis
posa
ls0
00
00
00
Acc
umul
ated
dep
reci
atio
n at
31
Mar
ch 2
009
087
70
055
60
4,29
745
16,
181
Net
boo
k va
lue
- Pu
rcha
sed
at 1
Apr
il 20
0827
,328
13,0
220
803
219
01,
738
209
43,3
19
- D
onat
ed a
t 1
Apr
il 20
080
1,75
50
014
00
101,
779
- G
over
nmen
t G
rant
ed a
t 1
Apr
il 20
080
00
00
00
00
Tota
l at
1 A
pril
2008
27,3
2814
,777
080
323
30
1,73
821
945
,098
Net
boo
k va
lue
- Pu
rcha
sed
at 3
1 M
arch
200
916
,374
13,0
400
1,08
040
10
1,74
161
733
,253
- D
onat
ed a
t 31
Mar
ch 2
009
01,
597
00
130
09
1,61
9
- G
over
nmen
t G
rant
ed
at 3
1 M
arch
200
90
00
00
00
00
Tota
l at
31 M
arch
200
916
,374
14,6
370
1,08
041
40
1,74
162
634
,872
Of
the
tota
ls a
t 31
Mar
ch 2
009,
£50
0,00
0 re
late
d to
land
val
ued
at o
pen
mar
ket
valu
e.

112 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
Not
es t
o th
e ac
cou
nts
No
te 1
0.2/
1 A
sset
Fin
anci
ng Land
£000
Build
ings
ex
clud
ing
dwel
lings
£000
Dw
ellin
gs£0
00
Ass
ets
unde
r co
nstr
ucti
on
and
paym
ents
on
acc
ount
£000
Plan
t an
d m
achi
nery
£000
Tran
spor
t eq
uipm
ent
£000
Info
rmat
ion
tech
nolo
gy
£000
Furn
itur
e an
d fit
ting
s £0
00To
tal
£000
Net
boo
k va
lue
31
Mar
ch 2
009
Ow
ned
16,0
7514
,470
012
441
40
1,74
162
633
,450
Fina
nce
Leas
ed29
916
70
00
00
046
6
On
bala
nce
shee
t PF
I co
ntra
cts
00
00
00
00
0
PFI r
esid
ual i
nter
ests
00
095
60
00
095
6
Tota
l 31
Mar
ch 2
009
16,3
7414
,637
01,
080
414
01,
741
626
34,8
72
Net
boo
k va
lue
1
Apr
il 20
08
Ow
ned
27,2
2914
,546
00
233
01,
738
219
43,9
65
Fina
nce
Leas
ed99
231
00
00
00
330
On
bala
nce
shee
t PF
I co
ntra
cts
00
00
00
00
0
PFI r
esid
ual i
nter
ests
00
080
30
00
080
3
Tota
l 1 A
pril
2008
27,3
2814
,777
080
323
30
1,73
821
945
,098
No
te 1
0.2/
2 Th
e to
tal a
mou
nt o
f dep
reci
atio
n ch
arge
d to
the
inco
me
and
expe
ndit
ure
in r
espe
ct o
f ass
ets
held
und
er
finan
ce le
ases
and
hir
e pu
rcha
se c
ontr
acts
:
Land
£000
Build
ings
ex
clud
ing
dwel
lings
£000
Dw
ellin
gs£0
00
Ass
ets
unde
r co
nstr
ucti
on
and
paym
ents
on
acc
ount
£000
Plan
t an
d m
achi
nery
£000
Tran
spor
t eq
uipm
ent
£000
Info
rmat
ion
tech
nolo
gy
£000
Furn
itur
e an
d fit
ting
s £0
00To
tal
£000
Dep
reci
atio
n
31 M
arch
200
964
00
00
064
Dep
reci
atio
n
31 M
arch
200
813
00
00
013
No
te 1
0.3
The
net
book
val
ue o
f lan
d, b
uild
ings
and
dw
ellin
gs a
t 31
Mar
ch 2
009
com
pris
es:
2008
/09
Purc
hase
d£0
00
2008
/09
Don
ated
£000
2008
/09
Gov
ernm
ent
Gra
nted
£000
2008
/09
Tota
l£0
00
2007
/08
Tota
l£0
00
Free
hold
28,9
481,
597
030
,545
41,7
75
Long
Lea
seho
ld46
60
046
633
0
Shor
t Le
aseh
old
00
00
0
Tota
l29
,414
1,59
70
31,0
1142
,105

www.enherts-pct.nhs.uk | 113
Not
es t
o th
e ac
cou
nts
Not
e 11
. Sto
ck a
nd
wor
k i
n p
rogr
ess
31 M
arch
200
9£0
0031
Mar
ch 2
008
£000
Raw
mat
eria
ls a
nd c
onsu
mab
les
119
119
Wor
k-in
-pro
gres
s0
0
Fini
shed
goo
ds0
0
Tota
l11
911
9
Not
e 12
. Deb
tors
31 M
arch
200
9£0
0031
Mar
ch 2
008
£000
Am
ount
s fa
lling
due
wit
hin
one
year
:
NH
S de
btor
s4,
883
4,48
5
Non
NH
S tr
ade
debt
ors
1,25
395
6
Prov
isio
n fo
r im
pairm
ent
of d
ebto
rs(4
9)0
Prep
aym
ents
and
acc
rued
inco
me
4,29
92,
442
Cap
ital d
ebto
rs -
NH
S0
0
Cap
ital d
ebto
rs -
Non
NH
S0
0
Cur
rent
par
t of
PFI
pre
paym
ents
00
Oth
er d
ebto
rs1,
801
1,97
6
12,1
879,
859
No
te 1
0.4
Fixe
d a
sset
s in
vest
men
tsO
n 1s
t Ju
ly 2
008,
the
PC
T ac
quire
d lo
an n
otes
and
sha
res
to t
he v
alue
of
£27,
570
and
£400
res
pect
ivel
y.Th
is is
in r
espe
ct o
f th
e A
ssem
ble
Com
mun
ity P
artn
ersh
ip, t
he n
ame
of t
he n
ewly
for
med
par
tner
ship
com
pany
bet
wee
n Be
dfor
dshi
re P
CT,
Milt
on K
eyne
s PC
T, G
uild
hous
e (a
priv
ate
deve
lopi
ng c
ompa
ny) a
nd lo
cal p
ublic
sec
tor
auth
oriti
es
cove
red
by t
he t
hree
par
ticip
ant
PCT
area
s.
No
te 1
0.5
Oth
er F
inan
cial
Ass
ets
Apa
rt f
rom
Not
e 10
.4 a
bove
, the
PC
T di
d no
t ho
ld a
ny fi
xed
or c
urre
nt fi
nanc
ial a
sset
whi
ch is
not
sep
arat
ely
disc
lose
d el
sew
here
on
the
finan
cial
sta
tem
ents
in 2
008/
9 or
200
7/8.
No
te 1
0.6.
Eco
nom
ic L
ives
of F
ixed
Ass
ets
Min
imum
Life
(yea
rs)
Max
imum
Life
(yea
rs)
Soft
war
e Li
cenc
es0
0
Lice
nces
and
Tra
dem
arks
00
Pate
nts
00
Dev
elop
men
t Ex
pend
iture
00
Build
ings
exc
l. D
wel
lings
540
Dw
ellin
gs0
0
Plan
t an
d M
achi
nery
515
Tran
spor
t Eq
uipm
ent
00
Info
rmat
ion
Tech
nolo
gy3
4
Furn
iture
and
Fitt
ings
528

114 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
Not
es t
o th
e ac
cou
nts
Not
e 12
. Deb
tors
31 M
arch
200
9£0
0031
Mar
ch 2
008
£000
Am
ount
s fa
lling
due
aft
er m
ore
than
one
yea
r:
NH
S de
btor
s0
0
Non
NH
S tr
ade
debt
ors
00
Prov
isio
n fo
r im
pairm
ent
of d
ebto
rs0
0
Prep
aym
ents
and
acc
rued
inco
me
1,63
61,
714
Cap
ital d
ebto
rs -
Non
NH
S0
0
Oth
er d
ebto
rs0
0
1,63
61,
714
Tota
l13
,823
11,5
73
NH
S D
ebto
rs in
clud
e;-
£0 p
repa
id p
ensi
on c
ontr
ibut
ions
at
31 M
arch
200
9 (3
1 M
arch
200
8 £0
); an
d-
£0 p
repa
ymen
ts f
rom
the
buy
out
of e
arly
ret
irem
ents
(31
Mar
ch 2
008
£0).
No
te 1
2.1
Prov
isio
n fo
r im
pair
men
t of
deb
tors
31 M
arch
200
9£0
00
Bala
nce
at 1
Apr
il0
Am
ount
writ
ten
off
durin
g th
e ye
ar0
Am
ount
rec
over
ed d
urin
g th
e ye
ar0
(Incr
ease
)/dec
reas
e in
deb
tors
impa
ired
(49)
Bala
nce
at 3
1 M
arch
(49)
No
te 1
2.2
Deb
tors
pas
t du
e da
te b
ut n
ot im
pair
ed:
31 M
arch
200
9£0
00
By u
p to
3 m
onth
s4,
821
By 3
to
6 m
onth
s61
0
By m
ore
than
6 m
onth
s40
5
Tota
l5,
836

www.enherts-pct.nhs.uk | 115
Not
es t
o th
e ac
cou
nts
Oth
er c
redi
tors
incl
ude;
- £4
9,12
7 fo
r pa
ymen
ts d
ue in
fut
ure
year
s un
der
arra
ngem
ents
to
buy
out
the
liabi
lity
for
one
early
ret
irem
ents
ove
r 5
year
s (2
007/
08 £
98,2
54);
and
- £6
59,0
00 o
utst
andi
ng p
ensi
ons
cont
ribut
ions
at
31 M
arch
200
9 (£
582,
900
at 3
1 M
arch
200
8)
No
te 1
3.1/
1 O
ther
Fin
anci
al L
iabi
litie
sTh
ere
are
no fi
nanc
ial l
iabi
litie
s ca
rrie
d at
fai
r va
lue
thro
ugh
profi
t an
d lo
ss f
or 2
008/
9.
Not
e 13
Cre
dit
ors
No
te 1
3.1.
Cre
dito
rs a
t th
e ba
lanc
e sh
eet
date
are
mad
e up
of:
31 M
arch
200
9£0
0031
Mar
ch 2
008
£000
Am
ount
s fa
lling
due
wit
hin
one
year
:
Bank
ove
rdra
fts
00
Inte
rest
pay
able
00
Paym
ents
rec
eive
d on
acc
ount
00
NH
S cr
edito
rs -
rev
enue
10,7
288,
088
NH
S cr
edito
rs -
cap
ital
00
Fam
ily H
ealth
Ser
vice
s (F
HS)
cre
dito
rs25
,152
20,9
34
Non
- N
HS
trad
e cr
edito
rs -
rev
enue
7,95
67,
615
Non
- N
HS
trad
e cr
edito
rs -
cap
ital
656
704
Tax
517
229
VAT
10
Soci
al S
ecur
ity c
osts
472
440
Obl
igat
ions
und
er fi
nanc
e le
ases
and
hire
pur
chas
e co
ntra
cts
1616
Oth
er c
redi
tors
1,60
12,
007
Acc
rual
s an
d de
ferr
ed in
com
e15
289
Cur
rent
par
t of
fina
nce
leas
e el
emen
t of
on
bala
nce
shee
t PF
I con
trac
ts0
0
Am
ount
s fa
lling
due
aft
er m
ore
than
one
yea
r:
Obl
igat
ions
und
er fi
nanc
e le
ases
and
hire
pur
chas
e co
ntra
cts
3248
NH
S cr
edito
rs0
0
Impu
ted
finan
ce le
ases
ele
men
t of
on
bala
nce
shee
t PF
I con
trac
ts0
0
Oth
er0
49
3297
Tota
l47
,283
40,2
19

116 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
Not
es t
o th
e ac
cou
nts
No
te 1
3.2.
Fin
ance
leas
e ob
ligat
ions
31 M
arch
200
9£0
0031
Mar
ch 2
008
£000
Paya
ble:
In n
ot m
ore
than
1 y
ear
or in
dem
and
3333
In m
ore
than
1 y
ear
but
no lo
nger
tha
n 2
year
s5
33
In m
ore
than
2 y
ears
but
no
long
er t
han
5 ye
ars
1414
Aft
er fi
ve y
ears
268
273
Subt
otal
320
353
Less
fina
nce
char
ges
allo
cate
d to
fut
ure
perio
ds(2
72)
(289
)
Tota
l48
64
No
te 1
3.3
Fina
nce
Leas
e Co
mm
itmen
tsTh
e PC
T ha
s no
fina
nce
leas
e co
mm
itmen
ts, o
ther
tha
n th
ose
in n
ote
13.2
.
* Pr
ovis
ions
rel
atin
g to
the
PC
T’s
own
prov
ider
fun
ctio
ns a
re s
how
n gr
oss
with
the
exp
ecte
d re
imbu
rsem
ents
fro
m t
he N
HSL
A in
clud
ed in
deb
tors
.Pe
nsio
ns re
latin
g to
oth
er s
taff
is th
e es
timat
ed fu
ll am
ount
of t
he P
CT’
s lia
bilit
y fo
r the
add
ition
al c
ost t
o th
e N
HS
Pens
ions
sch
eme
of e
mpl
oyee
s re
tirin
g ea
rly. T
he
liabi
lity
has
been
cal
cula
ted
follo
win
g ac
tuar
ial a
dvic
e, b
ut is
by
its n
atur
e on
ly a
n es
timat
e.
Rest
ruct
urin
g pr
ovis
ions
rel
ate
to t
he P
rovi
der
Serv
ices
arm
of
the
PCT
and
the
man
agem
ent
stru
ctur
e ch
ange
s re
quire
d, a
s it
mov
es t
o be
com
e a
sepa
rate
org
anis
atio
n.
The
Oth
er P
rovi
sion
s re
late
to
the
PCT’
s fu
ture
liab
ility
for
Con
tinui
ng C
are
unde
r th
e C
ough
lan
agre
emen
t an
d in
jury
ben
efit.
£2
80,2
18 is
incl
uded
in t
he p
rovi
sion
s of
the
NH
SLA
at
31.3
.200
9 in
res
pect
of
clin
ical
neg
ligen
ce p
rovi
sion
s of
the
PC
T (3
1.3.
2008
£15
,609
)
Not
e 14
. Pro
visi
ons
for
liab
ilit
ies
and
ch
arge
s
Pens
ions
re
lati
ng t
o fo
rmer
di
rect
ors/
mem
bers
£0
00
Pens
ions
re
lati
ng t
o ot
her
staf
f £0
00Le
gal c
laim
s £0
00Re
stru
ctur
ings
£0
00O
ther
£0
00To
tal
£000
At
1 A
pril
2008
01,
915
80
879
2,80
2
Aris
ing
durin
g th
e ye
ar*
054
048
137
290
7
Util
ised
dur
ing
the
year
0(2
37)
00
(40)
(277
)
Reve
rsed
unu
sed
00
00
00
Unw
indi
ng o
f di
scou
nt0
350
017
52
Tran
sfer
in-y
ear
00
00
00
At
31 M
arch
200
90
1,76
78
481
1,22
83,
484
Futu
re P
aym
ents
to
NH
S tr
usts
051
20
070
01,
212
Futu
re P
aym
ents
to
NH
S
Foun
datio
n Tr
usts
01,
173
00
01,
173
Futu
re P
aym
ents
to
Prim
ary
C
are
Trus
ts0
00
00
0
Expe
cted
tim
ing
of c
ash
flow
s:
With
in 1
yea
r0
263
048
156
21,
306
1 -
5 ye
ars
039
58
012
853
1
Ove
r 5
year
s0
1,10
90
053
81,
647

www.enherts-pct.nhs.uk | 117
Not
es t
o th
e ac
cou
nts
Not
e 15
Mov
emen
ts o
n R
eser
ves
Mov
emen
ts o
n re
serv
es in
the
yea
r co
mpr
ised
the
fol
low
ing:
Reva
luat
ion
rese
rve
Don
ated
as
set
rese
rve
Gov
ernm
ent
gr
ant
rese
rve
Oth
er r
eser
ves
Gen
eral
Fun
d
2008
/09
£000
2007
/08
£000
2008
/09
£000
2007
/08
£000
2008
/09
£000
2007
/08
£000
2008
/09
£000
2007
/08
£000
2008
/09
£000
2007
/08
£000
At
1 A
pril
20,0
4317
,582
1,77
91,
697
00
00
(8,0
53)
(11,
483)
PPA
: elim
inat
ion
of
nega
tive
reva
luat
ion
rese
rves
in r
espe
ct o
f ch
ange
in p
olic
y
on im
pairm
ents
00
00
Net
Par
liam
enta
ry
Fund
ing
691,
009
650,
158
Cos
t of
Cap
ital C
harg
e14
831
7
Tran
sfer
fro
m t
he O
CS
(695
,563
)(64
7,04
5)
Fixe
d as
set
impa
irmen
ts(1
3,26
0)0
(117
)0
00
Surp
lus/
(defi
cit)
on
othe
r re
valu
atio
ns/in
dexa
tion
of
fixe
d as
sets
2,13
42,
461
1514
00
0
Tran
sfer
of
real
ised
pro
fits
(loss
es)
00
00
00
00
Rece
ipt
of d
onat
ed/
Gov
ernm
ent
gran
ted
asse
ts0
00
0
Dep
reci
atio
n an
d di
spos
al
of d
onat
ed/G
over
nmen
t gr
ante
d as
sets
(58)
(58)
00
Tran
sfer
s to
/(fro
m) o
ther
N
HS
Bodi
es0
00
00
0
Oth
er m
ovem
ents
on
rese
rves
00
00
00
00
(1)
0
At
31 M
arch
8,91
720
,043
1,61
91,
779
00
00
(12,
460)
(8,0
53)

118 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
Not
es t
o th
e ac
cou
nts
No
te 1
6.1.
Rec
onci
liati
on o
f ope
rati
ng c
osts
to
net
cash
flow
from
ope
rati
ng a
ctiv
itie
s:
2008
/09
£000
2007
/08
£000
Net
ope
ratin
g C
ost
(695
,545
)(6
47,0
23)
Dep
reci
atio
n ch
arge
1,55
92,
115
Cos
t of
cap
ital c
harg
e14
831
7
Fixe
d as
set
impa
irmen
ts33
0
(Pro
fit)/l
oss
on d
ispo
sal o
f fix
ed a
sset
s0
0
Non
-cas
h m
ovem
ent
in p
rovi
sion
s95
915
1
Tran
sfer
fro
m d
onat
ed a
sset
res
erve
(58)
(58)
Tran
sfer
fro
m t
he G
over
nmen
t gr
ant
rese
rve
00
(Incr
ease
)/dec
reas
e in
sto
cks
057
(Incr
ease
)/dec
reas
e in
deb
tors
(2,2
50)
15,0
58
Incr
ease
/(dec
reas
e) in
cre
dito
rs7,
128
(16,
523)
Incr
ease
/(dec
reas
e) in
pro
visi
ons
(277
)(3
,167
)
Net
cas
h in
flow
/(out
flow
) fro
m o
pera
ting
act
ivit
ies
(688
,303
)(6
49,0
73)
Not
e 16
Not
es t
o th
e ca
sh fl
ow s
tate
men
t

www.enherts-pct.nhs.uk | 119
Not
es t
o th
e ac
cou
nts
No
te 1
6.2.
Rec
onci
liati
on o
f net
cas
h flo
w t
o m
ovem
ent
in n
et d
ebt
2008
/09
£000
2007
/08
£000
Incr
ease
/(dec
reas
e) in
cas
h in
the
per
iod
00
Cas
h ou
tflow
fro
m fi
nanc
e le
ase
paym
ents
1616
Cas
h (in
flow
)/out
flow
fro
m (d
ecre
ase)
/incr
ease
in li
quid
res
ourc
es0
Chan
ge in
net
deb
t re
sult
ing
from
cas
h flo
ws
1616
Non
- c
ash
chan
ges
in d
ebt
00
Net
deb
t at
1 A
pril
2008
(64)
(80)
Net
deb
t at
31
Mar
ch 2
009
(48)
(64)
No
te 1
6.3
Ana
lysi
s of
cha
nges
in n
et d
ebt
At
31 M
arch
20
09£0
00
Cash
flow
s in
ye
ar£0
00
Non
-cas
h ch
ange
s in
ye
ar£0
00
Tran
sfer
s to
/ fr
om N
HS
bodi
es£0
00A
t 1
Apr
il 20
08£0
00
OPG
cas
h at
ban
k0
00
0
Cas
h at
ban
k an
d in
han
d0
00
0
Bank
ove
rdra
fts
00
00
Fina
nce
leas
es d
ue w
ithin
one
yea
r(1
6)0
00
(16)
Fina
nce
leas
es d
ue a
fter
one
yea
r(3
2)16
00
(48)
Cur
rent
ass
et in
vest
men
ts
Tota
l(4
8)16
00
(64)
Excl
uded
abo
ve: £
1,90
6 he
ld in
PC
T ac
coun
ts r
elat
ing
to P
atie
nts’
mon
ey (£
1,90
2 at
31
Mar
ch 2
008)
Patie
nts’
mon
ies
are
excl
uded
fro
m c
redi
tors
.

120 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
Not
es t
o th
e ac
cou
nts
Not
e 17
. Cap
ital
Com
mit
men
ts
Com
mitm
ents
und
er c
apita
l exp
endi
ture
con
trac
ts a
t th
e ba
lanc
e sh
eet
date
wer
e £2
77,0
00 (2
007/
08: £
0).
Not
e 18
. Pos
t B
alan
ce S
hee
t E
ven
ts
Ther
e ar
e no
pos
t ba
lanc
e sh
eet
even
ts h
avin
g a
mat
eria
l eff
ect
on t
he fi
nanc
ial s
tate
men
ts.
The
maj
ority
of
cont
inge
nt li
abili
ty r
elat
es t
o cl
aim
s fo
r th
e re
imbu
rsem
ent
of c
ontin
uing
car
e ex
pend
iture
, fol
low
ing
the
deci
sion
of
the
Hea
lth S
ervi
ce O
mbu
dsm
an. W
here
a r
easo
nabl
e es
timat
e of
the
PC
T’s
liabi
lity
can
be m
ade,
base
d on
exp
erie
nce
to d
ate,
it h
as b
een
incl
uded
as
a pr
ovis
ion
(Not
e 14
). H
owev
er, g
iven
the
unc
erta
inty
reg
ardi
ngth
e fin
al o
utco
me
of in
divi
dual
cas
es, a
con
tinge
nt li
abili
ty h
as b
een
incl
uded
to
refle
ct t
he p
oten
tial c
ost
of t
hose
clai
ms
to t
he P
CT.
Not
e 19
. Con
tin
gen
cies
The
Prim
ary
Car
e Tr
ust
has
the
follo
win
g co
ntin
gent
(los
ses)
/gai
ns w
hich
hav
e no
t be
en in
clud
ed in
the
acc
ount
s:
2008
/09
£000
2007
/08
£000
Gro
ss v
alue
(479
)(2
44)
Am
ount
s re
cove
rabl
e (if
any
)0
0
Net
Con
tinge
nt L
iabi
lity
(479
)(2
44)

www.enherts-pct.nhs.uk | 121
Not
es t
o th
e ac
cou
nts
The
Dep
artm
ent
of H
ealth
is r
egar
ded
as a
rel
ated
par
ty. D
urin
g th
e ye
ar t
he P
CT
has
had
a si
gnifi
cant
num
ber
of m
ater
ial t
rans
actio
ns w
ith t
he D
epar
tmen
t, a
nd w
ith o
ther
ent
ities
for
whi
ch t
he D
epar
tmen
t is
reg
arde
d as
the
pare
nt D
epar
tmen
t. T
he P
CT
has
adop
ted
a di
sclo
sure
leve
l of
£5m
illio
n in
200
8/09
. The
se e
ntiti
es a
re li
sted
bel
ow;
In a
dditi
on, t
he P
CT
has
had
a si
gnifi
cant
num
ber
of m
ater
ial t
rans
actio
ns w
ith o
ther
Gov
ernm
ent
Dep
artm
ents
and
oth
er
cent
ral a
nd lo
cal G
over
nmen
t bo
dies
. Whe
re a
ppro
pria
te, t
hese
tra
nsac
tions
hav
e be
en r
eflec
ted
in t
he a
bove
tab
le.
The
PCT
has
also
rec
eive
d re
venu
e an
d ca
pita
l pay
men
ts f
rom
a n
umbe
r of
cha
ritab
le f
unds
, cer
tain
of
the
Trus
tees
for
w
hich
are
als
o m
embe
rs o
f th
e PC
T Bo
ard.
East
and
Nor
th H
ertf
ords
hire
PC
T is
a b
ody
corp
orat
e es
tabl
ishe
d by
ord
er o
f th
e Se
cret
ary
of S
tate
for
Hea
lth.
Dur
ing
the
year
non
e of
the
Boa
rd M
embe
rs o
r m
embe
rs o
f th
e ke
y m
anag
emen
t st
aff
or p
artie
s re
late
d to
the
m h
as
unde
rtak
en a
ny m
ater
ial t
rans
actio
ns w
ith t
he P
CT.
Dur
ing
the
year
loca
l GPs
sat
on
the
Boar
d an
d Ex
ecut
ive
Com
mitt
ee o
f th
e PC
T. P
aym
ents
are
mad
e to
all
prac
tices
in t
he
PCT
unde
r th
e ne
w G
P co
ntra
ct f
or t
he p
rovi
sion
of
GP
serv
ices
and
rei
mbu
rsem
ent
expe
nses
for
sta
ffing
and
com
putin
g.Th
e G
Ps o
n th
e Bo
ard
and
Prof
essi
onal
Exe
cutiv
e C
omm
ittee
had
no
dire
ct c
ontr
ol o
ver
how
the
se f
unds
wer
e al
loca
ted.
Det
ails
of
paym
ents
dur
ing
the
year
to
GP’
s on
the
Boa
rds
and
Prof
essi
onal
Exe
cutiv
e C
omm
ittee
wer
e as
fol
low
s.
£000
’s
Dr
M A
ndre
ws:
Par
tner
at
Dr
Hen
ders
on a
nd P
artn
ers
1,10
2
Dr
T K
ostic
k: P
artn
er a
t D
r Ba
xani
and
Par
tner
s1,
333
Dr
M H
offm
an:P
artn
er a
t D
r H
offm
an a
nd P
artn
ers
1,91
0
Dr
P Sh
illid
ay: P
artn
er a
t G
arde
n C
ity P
ract
ice
1,17
7
Paym
ents
to
Rela
ted
Part
y£0
00
Rece
ipts
from
Rela
ted
Part
y£0
00
Am
ount
s ow
ed t
o Re
late
d Pa
rty
£000
Am
ount
s du
e fr
om
Rela
ted
Part
y £0
00
Barn
et a
nd C
hase
Far
m H
ospi
tals
NH
S Tr
ust
20,3
820
320
0
Cam
brid
ge U
nive
rsity
Hos
pita
ls N
HS
Foun
datio
n Tr
ust
17,6
580
762
0
East
and
Nor
th H
erts
NH
S Tr
ust
177,
700
4,02
82,
862
1,15
7
East
of
Engl
and
Stra
tegi
c H
ealth
Aut
horit
y47
95,
128
3299
7
East
of
Engl
and
Am
bula
nce
Serv
ices
NH
S Tr
ust
14,4
3932
709
0
Her
tfor
dshi
re C
ount
y C
ounc
il87
,574
1,62
20
0
HM
Rev
enue
and
Cus
tom
s6,
092
051
837
8
NH
S Pe
nsio
n Sc
hem
e5,
101
065
90
Sout
h Ea
st E
ssex
PC
T41
,779
088
10
The
Prin
cess
Ale
xand
ra H
ospi
tal N
HS
Trus
t35
,794
837
486
837
Uni
vers
ity C
olle
ge L
ondo
n N
HS
Foun
datio
n Tr
ust
8,76
40
133
0
Wes
t H
ertf
ords
hire
PC
T18
,245
861
3,83
50
Not
e 20
. Rel
ated
Par
ty T
ran
sact
ion
s
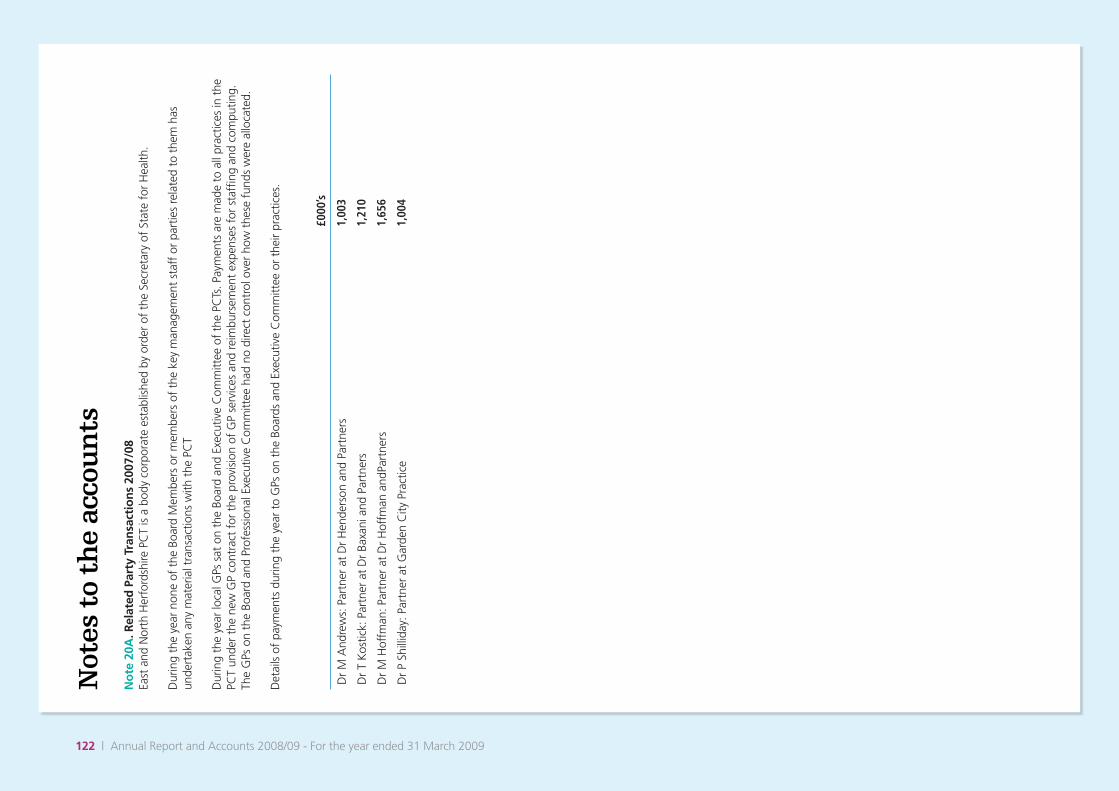
122 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
Not
es t
o th
e ac
cou
nts
No
te 2
0A. R
elat
ed P
arty
Tra
nsa
ctio
ns
2007
/08
East
and
Nor
th H
erfo
rdsh
ire P
CT
is a
bod
y co
rpor
ate
esta
blis
hed
by o
rder
of
the
Secr
etar
y of
Sta
te f
or H
ealth
.
Dur
ing
the
year
non
e of
the
Boa
rd M
embe
rs o
r m
embe
rs o
f th
e ke
y m
anag
emen
t st
aff
or p
artie
s re
late
d to
the
m h
asun
dert
aken
any
mat
eria
l tra
nsac
tions
with
the
PC
T
Dur
ing
the
year
loca
l GPs
sat
on
the
Boar
d an
d Ex
ecut
ive
Com
mitt
ee o
f th
e PC
Ts. P
aym
ents
are
mad
e to
all
prac
tices
in t
he
PCT
unde
r th
e ne
w G
P co
ntra
ct f
or t
he p
rovi
sion
of
GP
serv
ices
and
rei
mbu
rsem
ent
expe
nses
for
sta
ffing
and
com
putin
g.Th
e G
Ps o
n th
e Bo
ard
and
Prof
essi
onal
Exe
cutiv
e C
omm
ittee
had
no
dire
ct c
ontr
ol o
ver
how
the
se f
unds
wer
e al
loca
ted.
Det
ails
of
paym
ents
dur
ing
the
year
to
GPs
on
the
Boar
ds a
nd E
xecu
tive
Com
mitt
ee o
r th
eir
prac
tices
.
£000
’s
Dr
M A
ndre
ws:
Par
tner
at
Dr
Hen
ders
on a
nd P
artn
ers
1,00
3
Dr
T K
ostic
k: P
artn
er a
t D
r Ba
xani
and
Par
tner
s1,
210
Dr
M H
offm
an: P
artn
er a
t D
r H
offm
an a
ndPa
rtne
rs1,
656
Dr
P Sh
illid
ay: P
artn
er a
t G
arde
n C
ity P
ract
ice
1,00
4

www.enherts-pct.nhs.uk | 123
Not
es t
o th
e ac
cou
nts Pa
ymen
ts t
o Re
late
d Pa
rty
£000
Rece
ipts
from
Rela
ted
Part
y£0
00
Am
ount
s ow
ed t
o Re
late
d Pa
rty
£000
Am
ount
s du
e fr
om
Rela
ted
Part
y £0
00
Barn
et a
nd C
hase
Far
m H
osp
NH
ST19
,949
439
Bart
s an
d Th
e Lo
ndon
NH
S Tr
ust
3,23
916
6
Basi
ldon
and
Thu
rroc
k U
nive
rsity
Hos
pita
ls
NH
S Fo
unda
tion
Trus
t63
136
9
Bedf
ords
hire
PC
T17
155
028
25
Cam
brid
ge U
nive
rsity
Hos
pita
ls N
HS
Foun
datio
n Tr
ust
19,0
0015
85
Cam
brid
gesh
ire P
CT
768
49
East
and
Nor
th H
erts
NH
S Tr
ust
168,
733
4,18
43,
351
628
East
of
Engl
and
Stra
tegi
c H
ealth
Aut
horit
y16
974
7433
0
East
of
Engl
and
Am
bula
nce
Serv
ices
NH
S Tr
ust
12,8
3351
751
9
Guy
’s an
d St
Tho
mas
’ NH
S Fo
unda
tion
Trus
t1,
083
79
Her
tfor
dshi
re P
artn
ersh
ip N
HS
Foun
datio
n Tr
ust
243
994
1,15
21,
043
Her
tfor
dshi
re C
ount
y C
ounc
il80
,227
513
119
270
HM
Rev
enue
and
Cus
tom
s6,
106
1,36
222
953
6
Impe
rial C
olle
ge H
ealth
care
NH
S Tr
ust
2,27
295
Luto
n an
d D
unst
able
Hos
pita
l NH
S Fo
unda
tion
Trus
t2,
238
184
Mid
Ess
ex H
ospi
tal S
ervi
ces
NH
S Tr
ust
701
101
Moo
rfiel
ds E
ye H
ospi
tal N
HS
Foun
datio
n Tr
ust
628
Nor
th E
ssex
Par
tner
ship
NH
S Fo
unda
tion
Trus
t35
235
120
620
0
Nor
th M
iddl
esex
Uni
vers
ity H
ospi
tal N
HS
Trus
t2,
581
52
Nor
th W
est
Lond
on H
ospi
tals
NH
S Tr
ust
458
29
Nat
iona
l Ins
uran
ce F
und
2,63
842
3
NH
S Bu
sine
ss S
ervi
ces
Aut
horit
y48
346
NH
S Pe
nsio
n Sc
hem
e4,
700
583
Papw
orth
Hos
pita
l NH
S Fo
unda
tion
Trus
t3,
168
157
Roya
l Bro
mpt
on a
nd H
arefi
eld
NH
S Tr
ust
6,24
118
4
Roya
l Fre
e H
amps
tead
NH
S Tr
ust
6,09
023
0
Roya
l Nat
. Ort
hopa
edic
Hos
pita
l NH
S Tr
ust
2,17
645
9
Sout
h Ea
st E
ssex
PC
T14
,527
2320
23
The
Prin
cess
Ale
xand
ra H
ospi
tal N
HS
Trus
t32
,537
814
115
611
Uni
vers
ity C
olle
ge L
ondo
n N
HS
Foun
datio
n Tr
ust
7,59
01,
065
Wel
wyn
Hat
field
Dis
tric
t C
ounc
il63
638
Wes
t Es
sex
PCT
3,84
11,
820
5035
3
Wes
t H
ertf
ords
hire
PC
T16
,443
651
65
Wes
t H
ertf
ords
hire
NH
S Tr
ust
575
168
172
154
The
Dep
artm
ent
of H
ealth
is r
egar
ded
as a
rel
ated
par
ty. D
urin
g th
e ye
ar t
he P
CT
has
had
a si
gnifi
cant
num
ber
of m
ater
ial
tran
sact
ions
with
the
Dep
artm
ent,
and
with
oth
er e
ntiti
es f
or w
hich
the
Dep
artm
ent
is r
egar
ded
as t
he p
aren
t D
epar
tmen
t.
Thes
e en
titie
s ar
e lis
ted
belo
w;

124 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
Not
es t
o th
e ac
cou
nts
In a
dditi
on, t
he P
CT
has
had
a si
gnifi
cant
num
ber
of m
ater
ial t
rans
actio
ns w
ith o
ther
Gov
ernm
ent
Dep
artm
ents
and
oth
er
cent
ral a
nd lo
cal G
over
nmen
t bo
dies
. Whe
re a
ppro
pria
te, t
hese
tra
nsac
tions
hav
e be
en re
flect
ed in
thi
s ta
ble.
The
PCT
has
also
rec
eive
d re
venu
e an
d ca
pita
l pay
men
ts f
rom
a n
umbe
r of
cha
ritab
le f
unds
, cer
tain
of
the
Trus
tees
for
w
hich
are
als
o m
embe
rs o
f th
e PC
T Bo
ard.
Not
e 21
. Pri
vate
Fin
ance
Tra
nsa
ctio
ns
No
te 2
1.1.
PFI
sch
emes
dee
med
to
be
off
-bal
ance
sh
eet
2008
/09
£000
2007
/08
£000
Am
ount
s in
clud
ed w
ithin
ope
ratin
g ex
pens
es in
res
pect
of
PFI t
rans
actio
ns d
eem
ed t
o be
off
-bal
ance
she
et -
gros
s.2,
415
2,32
1
Am
ortis
atio
n of
PFI
def
erre
d as
set
(153
)(1
50)
Net
ch
arg
e to
op
erat
ing
co
sts
2,26
22,
171
The
PCT
is c
omm
itted
to
mak
e th
e fo
llow
ing
paym
ents
dur
ing
the
next
yea
r, in
whi
ch t
he P
FI s
chem
e ex
pire
s
2008
/09
£000
2007
/08
£000
With
in o
ne y
ear
00
2 to
5 y
ears
(inc
lusi
ve)
00
6 to
10
year
s (in
clus
ive)
00
11 t
o 15
yea
rs (i
nclu
sive
)0
0
16 t
o 20
yea
rs (i
nclu
sive
)0
0
21 t
o 25
yea
rs (i
nclu
sive
)2,
415
2,32
1
The
PFI s
chem
e is
a r
edev
elop
men
t on
the
Her
ts a
nd E
ssex
Hos
pita
l site
to
prov
ide
mod
ern
upda
ted
Hea
lth S
ervi
ces
to
incl
ude
Elde
rly M
edic
ine
and
Men
tal H
ealth
.Out
patie
nt f
acili
ties
for
a ra
nge
of s
peci
aliti
es a
re a
lso
bein
g pr
ovid
ed. T
he d
e-ve
lopm
ent
also
incl
udes
a M
inor
inju
ries
unit
and
acco
mm
odat
ion
for
com
mun
ity s
ervi
ces.
The
sch
eme
has
been
dev
elop
ed
in c
onju
nctio
n w
ith a
nur
sing
hom
e de
velo
pmen
t si
tuat
ed a
t H
arlo
w.
£000
The
estim
ated
cap
ital v
alue
of
the
PFI s
chem
e14
,200
Con
trac
t st
art
date
28/0
4/20
03
Con
trac
t en
d da
te28
/04/
2033

www.enherts-pct.nhs.uk | 125
Not
es t
o th
e ac
cou
nts
Not
e 22
. Fin
anci
al I
nst
rum
ents
FRS
29, F
inan
cial
Inst
rum
ents
: Dis
clos
ures
, req
uire
s di
sclo
sure
of
the
role
tha
t fin
anci
al in
stru
men
ts h
ave
had
durin
g th
e pe
riod
in c
reat
ing
or c
hang
ing
the
risks
an
entit
y fa
ces
in u
nder
taki
ng it
s ac
tiviti
es. B
ecau
se o
f th
e w
ay P
CTs
are
fina
nced
, th
ey a
re n
ot e
xpos
ed t
o th
e de
gree
of
finan
cial
ris
k fa
ced
by b
usin
ess
entit
ies.
Als
o fin
anci
al in
stru
men
ts p
lay
a m
uch
mor
e lim
ited
role
in c
reat
ing
or c
hang
ing
risk
than
wou
ld b
e ty
pica
l of
the
liste
d co
mpa
nies
to
whi
ch F
RS 2
9 m
ainl
y ap
plie
s. T
he
PCT
has
limite
d po
wer
s to
bor
row
or
inve
st s
urpl
us f
unds
and
fina
ncia
l ass
ets
and
liabi
litie
s ar
e ge
nera
ted
by d
ay-t
o-da
y op
erat
iona
l act
iviti
es r
athe
r th
an b
eing
hel
d to
cha
nge
the
risks
fac
ing
the
PCT
in u
nder
taki
ng it
s ac
tiviti
es.
As
allo
wed
by
FRS
29, d
ebto
rs a
nd c
redi
tors
tha
t ar
e du
e to
mat
ure
or b
ecom
e pa
yabl
e w
ithin
12
mon
ths
from
the
bal
ance
sh
eet
date
hav
e be
en o
mitt
ed f
rom
all
disc
losu
res
othe
r th
an t
he c
urre
ncy
profi
le.
Liqu
idity
risk
Mos
t of
the
PC
T’s
net
oper
atin
g co
sts
are
incu
rred
und
er a
nnua
l ser
vice
agr
eem
ents
with
loca
l PC
Ts, N
HS
Trus
ts a
nd N
HS
Foun
datio
n Tr
usts
and
are
fina
nced
fro
m r
esou
rces
vot
ed a
nnua
lly b
y Pa
rliam
ent
or d
irect
ly fi
nanc
ed f
rom
res
ourc
es v
oted
an
nual
ly b
y Pa
rliam
ent.
The
PC
T al
so la
rgel
y fin
ance
s its
cap
ital e
xpen
ditu
re f
rom
fun
ds m
ade
avai
labl
e fr
om G
over
nmen
t.
East
and
Nor
th H
ertf
ords
hire
PC
T is
not
, the
refo
re, e
xpos
ed t
o si
gnifi
cant
liqu
idity
ris
ks.
Inte
rest
-Rat
e Ri
sk10
0% o
f th
e PC
T’s
finan
cial
ass
ets
and
100%
of
its fi
nanc
ial l
iabi
litie
s ca
rry
nil o
r fix
ed r
ates
of
inte
rest
. Eas
t an
d N
orth
H
ertf
ords
hire
PC
T is
not
, the
refo
re, e
xpos
ed t
o si
gnifi
cant
inte
rest
-rat
e ris
k. T
he f
ollo
win
g tw
o ta
bles
sho
w t
he in
tere
st r
ate
profi
les
of t
he P
CT’
s fin
anci
al a
sset
s an
d lia
bilit
ies:
No
te 2
2.1
Fina
ncia
l Ass
ets
Fixe
d Ra
teN
on-in
tere
st
bear
ing
Curr
ency
Tota
l £0
00
Floa
ting
rate
£0
00Fi
xed
rate
£0
00
Non
-inte
rest
be
arin
g£0
00
Wei
ghte
d av
e in
tere
st
rate
%
Wei
ghte
d av
e pe
riod
for
whi
ch fi
xed
Year
s
Wei
ghte
d av
erag
e te
rm
Year
s
At
31 M
arch
200
9
Ster
ling
1,63
60
01,
636
00
22
Oth
er0
00
00
00
Gro
ss fi
nanc
ial a
sset
s1,
636
00
1,63
6
At
31 M
arch
200
8
Ster
ling
1,79
20
01,
792
00
23
Oth
er0
00
00
00
Gro
ss fi
nanc
ial a
sset
s1,
792
00
1,79
2

126 | Annual Report and Accounts 2008/09 - For the year ended 31 March 2009
Not
es t
o th
e ac
cou
nts
No
te 2
2.2
Fina
ncia
l Lia
bilit
ies
Fixe
d Ra
teN
on-in
tere
st
bear
ing
Curr
ency
Tota
l £0
00
Floa
ting
rate
£0
00Fi
xed
rate
£0
00
Non
-inte
rest
be
arin
g£0
00
Wei
ghte
d av
e in
tere
st
rate
%
Wei
ghte
d av
e pe
riod
for
whi
ch fi
xed
Year
s
Wei
ghte
d av
erag
e te
rm
until
mat
urity
Ye
ars
At
31 M
arch
200
9
Ster
ling
810
810
062
0
Oth
er0
00
00
00
Gro
ss fi
nanc
ial a
sset
s81
081
0
At
31 M
arch
200
8
Ster
ling
162
016
20
067
0
Oth
er0
00
00
00
Gro
ss fi
nanc
ial a
sset
s16
20
162
0
Fore
ign
Curr
ency
Ris
kTh
e PC
T ha
s ne
glig
ible
for
eign
cur
renc
y in
com
e or
exp
endi
ture
.
No
te 2
2.3
Fair
Valu
esTh
e fa
ir va
lues
of
finan
cial
ass
ets
and
liabi
litie
s in
Not
es 2
2.4
and
22.5
opp
osite
do
not
defe
r m
ater
ially
fro
m t
heir
carr
ying
am
ount
s.
No
te 2
2.4
Fina
ncia
l Ass
ets
At f
air v
alue
th
roug
h pr
ofit
and
loss
£000
Loan
s an
d
rece
ivab
les
£000
Avai
labl
e
for s
ale
£000
Tota
l£0
00
Embe
dded
der
ivat
ives
00
00
NH
S de
btor
s0
00
0
Non
NH
S de
btor
s0
00
0
Cas
h at
ban
k an
d in
han
d0
00
0
Oth
er fi
nanc
ial a
sset
s0
1,63
60
1,63
6
Tota
l at 3
1 M
arch
200
90
1,63
60
1,63
6
No
te 2
2.5
Fina
ncia
l Lia
bilit
ies
At f
air v
alue
th
roug
h pr
ofit
and
loss
£000
Avai
labl
e f
or s
ale
£000
Tota
l£0
00
Embe
dded
der
ivat
ives
00
0
NH
S cr
edito
rs0
00
Non
NH
S cr
edito
rs0
00
Borr
owin
gs0
00
Priv
ate
Fina
nce
Initi
ativ
e an
d fin
ance
leas
e ob
ligat
ions
032
32
Oth
er fi
nanc
ial l
iabi
litie
s0
4949
Tota
l at 3
1 M
arch
200
90
8181

www.enherts-pct.nhs.uk | 127
Not
es t
o th
e ac
cou
nts
No
te 2
3. T
hir
d p
arty
ass
ets
The
PCT
held
£1,
906
cash
at
bank
and
in h
and
at 3
1/3/
2009
whi
ch r
elat
es t
o m
onie
s he
ld o
n be
half
of p
atie
nts
(£1,
902
at
31/3
/08)
. Thi
s ha
s be
en e
xclu
ded
from
cas
h at
ban
k an
d in
han
d fig
ure
repo
rted
in t
he a
ccou
nts.
No
te 2
4. L
oss
es a
nd
Sp
ecia
l Pay
men
tsTh
ere
wer
e 26
cas
es o
f lo
sses
and
spe
cial
pay
men
ts (2
007/
08: 2
5 ca
ses)
tot
allin
g £7
0,69
5 (2
007/
08: £
34,8
30)
appr
oved
dur
ing
2008
/09.
Ther
e w
ere
no c
linic
al n
eglig
ence
cas
es w
here
the
net
pay
men
t ex
ceed
ed £
100,
000
in 2
008/
9 or
200
7/8.
Ther
e w
ere
no f
raud
cas
es w
here
the
net
pay
men
t ex
ceed
ed £
100,
000
in 2
008/
9 or
200
7/8.
Ther
e w
ere
no p
erso
nal i
njur
y ca
ses
whe
re t
he n
et p
aym
ent
exce
eded
£10
0,00
0 in
200
8/9
or 2
007/
8.
Ther
e w
ere
no c
ompe
nsat
ion
unde
r le
gal o
blig
atio
n ca
ses
whe
re t
he n
et p
aym
ent
exce
eded
£10
0,00
0 in
200
8/9
or 2
007/
8.
Ther
e w
ere
no f
ruitl
ess
paym
ent
case
s w
here
the
net
pay
men
t ex
ceed
ed £
100,
000
in 2
008/
9 or
200
7/8.
Not
e: T
he t
otal
cos
ts in
clud
ed in
thi
s no
te a
re o
n an
acc
rual
s ba
sis.
Not
e 25
. In
tra-
gove
rnm
ent
bal
ance
s
Deb
tors
Am
ount
s fa
lling
due
with
in
one
year
£000
Deb
tors
Am
ount
s fa
lling
due
aft
er
mor
e th
an o
ne
year
£000
Cred
itors
A
mou
nts
fa
lling
due
w
ithin
on
e ye
ar£0
00
Cred
itors
Am
ount
s fa
lling
due
aft
er
mor
e th
an o
ne y
ear
£000
Bala
nces
with
oth
er c
entr
al
gove
rnm
ent
bodi
es2,
237
07,
004
0
Bala
nces
with
loca
l aut
horit
ies
851
018
30
Bala
nces
with
NH
S Tr
usts
/FTs
3,02
40
5,37
30
Bala
nces
with
pub
lic c
orpo
ratio
ns
and
trad
ing
fund
s0
00
0
Bala
nces
with
bod
ies
exte
rnal
to
Gov
ernm
ent
6,07
51,
636
34,6
9132
At 3
1 M
arch
200
912
,187
1,63
647
,251
32
Bala
nces
with
oth
er c
entr
al
gove
rnm
ent
bodi
es1,
574
01,
731
0
Bala
nces
with
loca
l aut
horit
ies
288
044
60
Bala
nces
with
NH
S Tr
usts
/FTs
3,44
70
10,0
270
Bala
nces
with
pub
lic c
orpo
ratio
ns
and
trad
ing
fund
s0
00
0
Bala
nces
with
bod
ies
exte
rnal
to
Gov
ernm
ent
4,55
01,
714
27,9
1897
At 3
1 M
arch
200
89,
859
1,71
440
,122
97

128 | Annual Report and Accounts 2008/09
Alternative formats and additional copies
For people who may have difficulty reading the print in this report, a large print version can be made available by contacting our communications team:
Communications TeamHertfordshire Primary Care TrustsCharter HouseParkwayWelwyn Garden CityHertfordshireAL8 6JL
Telephone: 01707 390855Email: [email protected]
The communications team can also arrange to provide the following on request:
Additional copies of this document •(hard copy or electronic version) An audio-cassette or CD version •(arranged on request only) Help in understanding the document in languages other than English•
Please note that this Report is also available to download from the NHS East and North Hertfordshire website as follows:
www.enherts-pct.nhs.uk
Contact us
You can write to us at:
NHS East and North HertfordshireCharter HouseParkwayWelwyn Garden CityHertfordshireAL8 6JL
You can telephone us on: 01707 390855 (Switchboard open 8am – 6pm)
You can email us at: [email protected] visit our website: www.enherts-pct.nhs.uk

www.enherts-pct.nhs.uk | 129
Another language
If you would like information in another language or format, please ask us
01707 369705 - Urdu
01707 369705 - Bengali
01707 369705 - Italian
01707 369705 - Polish
01707 369705 - Portuguese
01707 369705 - Turkish
01707 369705 - Mandarin


We would like to pay tribute to the outstanding contribution and dedication of our staff. Everyone has a played their part in helping people in Hertfordshire to remain healthy and stay active.

Published September 2009