nhs city & hackney
TRANSCRIPT
NHS CITY & HACKNEY PATHFINDER CLINICAL COMMISSIONING GROUP
City & Hackney pathfinder Clinical Commissioning Group
Clinical Commissioning Group (CCG) Board Friday 25 May 2012, 1400-1600
CCG Meeting Room, 2nd Floor, Lawson Practice, Nuttall Street, London N1 5HZ
AGENDA Chair: Haren Patel Agenda Items
Led by & Appendix number
Timing
1. Declaration of Interests
Haren Patel 1400-1405 (5 mins)
2. CCG Committee business • Minutes of the last meeting; • Minutes of the May 2012 Finance, Performance and
Activity Subcommittee; • Actions log; • Forward Plan; • Register of Interests; • Matters arising.
Haren Patel Papers 2a, 2b, 2c, 2d & 2e
1405-1415 (10 mins)
FOR DISCUSSION
3. Finance, performance and activity
Philippa Lowe Verbal update
1415-1430 (15 mins)
4. CCG budgets post budget setting Philippa Lowe Verbal update
1430-1440 (10 mins)
5. Primary Care Quality Improvement Priorities Mark Rickets Paper 5
1440-1450 (10 mins)
6. Quality Accounts • East London Foundation Trust • Barts and the London Trust
Haren Patel Papers 6a & 6b
1450-1500 (10 mins)
7. Working with London Borough of Hackney
Haren Patel Paper 7
1500-1510 (10 mins)
FOR DECISION
8. Commissioning Primary Care Mental Health Liaison Service and SMI Depot LES
Rhiannon England Papers 8a, 8b, 8c, 8d & 8e
1510-1525 (15 mins)
9. Walk In Centre’s Business Case consultation response Alice Benton Paper 9
1525-1540 (15 mins)
10. 2011/12 CCLES final payment recommendations Teresa McInerney Papers 10a, 10b & 10c
1540-1555 (15 mins)
11. Any Other Business
Haren Patel 1555-1600 (5 mins)

CITY & HACKNEY PATHFINDER CLINICAL COMMISSIONING GROUP
City & Hackney pathfinder Clinical Commissioning Group Agenda Item 1
MINUTES OF THE NHS CITY AND HACKNEY PATHFINDER CLINICAL COMMISSIONING GROUP BOARD HELD ON FRIDAY 27 APRIL 2012
AT THE LAWSON PRACTICE, NUTTALL STREET, LONDON, N1 5HZ PRESENT: Dr Clare Highton (CCG Clinical Chair)
Dr Haren Patel, (GP Board member) Dr Gary Marlowe, (GP Board member) Jaime Bishop (Public Representative) Honor Rhodes (Associate Non Executive Director, NHS NELC) Paul Haigh (CCG Chief Operating Officer)
IN ATTENDANCE: Matthew Knell (CCG Business Co-ordinator) Chris Westcott (CSS Associate Director) Alison Leyshon (CSS Director of Resources) for item 5 Enrico Panizzo (CSS Quality and Clinical Governance Facilitator) for items 5 and 6 Danny Chesterman (Ashridge Consulting facilitator)
The Chair, Clare Highton (CH) welcomed members to the first meeting of the newly formed NHS City and Hackney pathfinder Clinical Commissioning Group Board (CCGB) meeting and asked attendees to introduce themselves. Apologies had been received from Mariette Davis (Associate Non Executive Director (NED) from NHS North East London and the City (NELC)) and Philippa Lowe (interim CCG Chief Financial Officer). Agenda Item 1 – Ashridge Consulting Board Development session Danny Chesterman (DC) led the Board through an exercise in establishing what behaviours the Board wanted to embrace, also covering how the group chould assess itself and how it might want to consider conducting its business. The Board continued to discuss relationships between the Board and other bodies and organisations, internal to the CCG, across the NHS and externally. The Board concluded that they wanted to see short, ordered and prioritised agendas by discussion and decisions needed, that they would meet in public by default and that conversations with Local Authorities (LAs) were needed to establish relationships with Health and Wellbeing Boards (HWBs) and identify their needs. Joint Boards with LAs and NHS Trusts would be useful to highlight shared work and build working relationships across organisations. Agenda Item 2 – CCG Board Establishment CCG Board Membership Paul Haigh (PH) outlined the CCGB membership and asked the Board to discuss

City & Hackney pathfinder Clinical Commissioning Group Agenda Item 1
whether Local Involvement Networks (LINks) representatives should be invited to attend as observers. The Board agreed to invite Hackney and City of London LINks to the next meeting and future meetings in a non voting capacity. DECISION: Hackney and City of London LINks representatives to be invited to monthly CCG Board meetings as observers. The Board noted that:
The CCG was awaiting details from NHS London on the recruitment process and timescale for a registered nurse and secondary care consultant to join the Board;
The CCG would probably seek to recruit its 2 lay members in the summer through NHS NELC following National Commissioning Board (NCB) guidance. In the meantime the CCG would have Jamie Bishop, the public member from the CCG pathfinder Committee and East London Integrated Care (ELIC) lay member, Honor Rhodes and Mariette Davis, associate NEDs from NHS NELC to support its work
PH continued to explain how the structure of the CCG functions, with the Programme Boards as the ‘engine rooms’ of the CCG, presenting options for consultation and discussion to the Clinical Executive Committee. The CCGB would retain responsibility for final signoff of any proposals incurring financial cost or presenting a clear risk to the delivery of the CCGs responsibilities in addition to its governance, finance, performance, quality and activity role. The simple rule to follow in assessing what should be addressed by the CCGC is the question “will the patient notice the proposal / change in service?”. Declarations of Interest The central guidance on conflicts of interest has now been published and will be detailed in the CCG Constitution. It will be communicated widely and steps taken to ensure all involved in the CCG are aware of, and abide by the document. Matthew Knell (MK) will be pursuing the outstanding Declarations of Interest before the May 2012 Committee meeting. ACTION: MK to ensure remaining Declarations of Interest are submitted for the 25 May 2012 Board meeting. Establishment Agreement The Board accepted the Delegation and Establishment agreements from NHS North East London and the City (NELC). DECISION: PCCGB accepted the Delegation and Establishment agreements from NHS NELC. Delegated Budgets The Board noted the 2011/12 Budgets delegated to the CCG by NHS NELC and that the CCG is operating at 100% delegation following the transfer of remaining budgets from NHS NELC at the March Board meeting. PH and Philippa Lowe (PI) are leading a budget setting exercise to assess all delegated budgets and agree draft 2012/13

City & Hackney pathfinder Clinical Commissioning Group Agenda Item 1
budgets and a scheme of delegation. The budget proposals will involve clinical review and the final proposals will return for agreement to the May or June 2012 Board meeting. The Board discussed and agreed that they would be transparent in all financial discussions and budgets would be open. It was noted that NHS NELC held the reserves for 2012/13 and that the methodology for CCG allocations for 2013/14 was still under development. Establishment of Sub Committees: The Board discussed and accepted the draft Terms of Reference for the Finance and Performance Subcommittee and the Clinical Executive Subcommittee as bodies of the CCG Board, with the proviso that the documents are kept up to date as the CCG and its Constitution develops. DECISION: Terms of Reference for the Finance and Performance Subcommittee and the Clinical Executive Subcommittee accepted with recognition that they will evolve with the CCG. It was noted that the CCG would operate under the NHS NELC Audit and Remuneration Subcommittees for the moment although shadow CCG Subcommittees will be established later in the year. Agenda Item 3 – CCG Pledge CH introduced the pledge, drafted by Louise Irvine and also tabled a similar document produced by a General Medical Council (GMC) working group. The Board discussed how to include the pledge, or the principles outlined in it within the CCG Constitution and ways of working. Discussions centred around the challenges of being as open, transparent and accountable as possible within the constraints of contractual law. The CCG Constitution, which followed the national template, would be consulted on in May to June 2012 with CCG Practices and other partner organisations widely across the area and will be subject to final agreement by the June CCG Board in preparation for authorisation. The Board requested that the principles of transparency, mutuality, learning, efficiency and effectiveness be included in the proposed text and that it should reflect the uniqueness of Hackney and the City of London. Agenda Item 4 – CCG Board business Actions bought forward from other bodies The Board accepted the actions log included with the Board papers, noting that actions will be delegated to the Programme Boards as start to conduct business as appropriate. Forward Plan

City & Hackney pathfinder Clinical Commissioning Group Agenda Item 1
The Forward Plan was accepted by the Board with CH asking that any requests for future items for discussion be submitted to MK. ACTION: Board members to communicate possible future items for discussion to MK. Matters arising No items were brought to the Board attention. Agenda Item 5 – Finance, performance, quality and activity CH welcomed Alison Leyshon (AL) to the Board, AL noted that this was likely her final appearance at the meeting due to the appointment of the CCG interim Chief Financial Officer, Philippa Lowe, who would in future provide the board with a report on financial performance for the CCG, based on the information produced by Commissioning Support Services (CSS). The reporting processes and detailed scrutiny of performance would be undertaken by the Finance and Performance Subcommittee. The information and projections of year end performance presented under this agenda item were based on month 11 (February 2012) out turn data. Contract negotiations were noted as concluded with Homerton University Hospital Trust (HUHT) with only final details left to be agreed. Barts Health and University College London Hospital (UCLH) negotiations led by CSS were continuing. Last period Budget performance The year end position for City and Hackney was indicating a £1.6m overspend, subject to month 12 returns. The headline approximate breakdown indicated a £2.2m overspend with HUHT, £2m overspend with Barts Health, £0.5m underspend with UCLH, £0.7m underspend with the Whittington and £70k overspend with Moorfields. Notable other budget lines included Continuing Care projecting a £1m underspend. The board noted that the report presented the budgets held by CSS rather than those delegated to the CCG and this would be rectified for future board reports. The overall position indicated that City and Hackney has achieved its targets and the NHS NELC Director of Finance had confirmed that he was comfortable with the financial performance and projected year end position of the CCG and Primary Care Trust (PCT), subject to final review. Last period Activity report Chris Westcott (CW) presented the activity report, explaining that an investigation of trends in the movement of activity across providers was needed in order to understand current performance and anticipate future changes. ACTION: Chris Westcott to undertake analysis of the movement of activity across providers during 2011/12 and report to the Board.

City & Hackney pathfinder Clinical Commissioning Group Agenda Item 1
Accident and Emergency (A&E) activity at HUHT had a higher than expected variance in month 11, even considering historical higher activity in the final quarter of the year, but generally financial positions were the result of cost pressures rather than activity increases across providers. HUHT had reported an increase in the number of GP referrals received, however these had not converted to attendances, in fact, attendances resulting from GP referrals decreased significantly between January and February 2012. It should be noted that the increase in referrals to HUHT have been matched with a decrease to Barts, the Whittington and UCLH and the sector wide referral position is down. The Board requested that the Planned Care Programme Board further investigate any issues around Homerton referrals and non attendances and would also address the contractual targets around outpatient department (OPD) follow ups agreed as part of the 2012/13 Homerton contract. ACTION: Planned Care Programme Board to investigate Homerton referrals and non attendances. Last period Quality report Enrico Panizzo (EP) presented the quarterly Quality and Clinical Governance report, produced by CSS to the Board and asked for feedback on the reports format. The Board noted that the quality report focusing on the services commissioned would be discussed by the Board although the Clinical Executive and Programme Boards would also receive a summary and be asked to address any areas of concern. Highlights from the report included that Health Care Acquired Infection (HCAI) rates had dropped dramatically across the area, including zero occurrences of MRSA at HUHT. The practice of screening patients on entry to hospital and treating accordingly was thought to be responsible for this performance. Mental Health bed occupancy is due to be discussed at a future Clinical Commissioning Committee (CCC) to establish a cluster wide approach. Staffing levels on any potential high occupancy wards risked incidents and would need to be carefully monitored and addressed. HUHT had not reached the Commissioning for Quality and Innovation (CQUIN) on Venous Thromboembolisms (VTE) risk assessments on initial assessment of data, although further investigation on coding and returns was needed to confirm. The Inpatient Survey CQUIN had also not been met. It was noted that the Homerton performance review meetings had been and would continue to be attended by the CCG Chair and Chief Operating Officer (COO) with CCG input to the monthly CQRM meetings with both East London Foundation Trust (ELFT) and Homerton. The Board remarked how useful the provision of benchmark data through the report was and asked for the practice to continue and be extended where possible. The group also questioned whether the mortality data was statistically relevant when looking at timescales of only around a year. EP confirmed that the Summary Hospital Mortality Index (SHMI) was the single recognised measurement of mortality now in use across NHS reports.

City & Hackney pathfinder Clinical Commissioning Group Agenda Item 1
The Board discussed the use of data to monitor ELFT in order to provide better performance and quality information on services. The upcoming Quarter 4 performance meetings could be used to address KPIs and data issues, although A&E performance remained the priority for discussion. Last period KPI report The Board accepted the month 11 Key Performance Indicator (KPI) report. The Homerton performance review meeting would focus on the variable performance on A&E waits, VTE and ambulance handovers. The CCG Maternity Programme Board was developing an action plan with Homerton in relation to 12+6 which would come to a future board meeting. Agenda Item 6 – Homerton Quality Account consultation response CH asked the Board to make any initial comments on the HUHT Quality Account that is being consulted on. EP informed the group that the PCT Cluster will need to make a formal statement endorsing or commenting on the report at publication at the end of May 2012. The Board endorsed the priorities laid out in the account and suggested that HUHT could include mention of the integrated care pathways and local audits worked on in partnership with the CCG. The group discussed how the document could be used more broadly, whether patients might need more narrative or the information displayed in a more accessible format or whether a version catering more to clinicians would be useful. The Board suggested that the use of benchmarks, against other local providers, London wide averages or national figures might be beneficial both in highlighting accomplishments and illustrating goals. The Board asked EP to investigate the Health Visiting metrics and figures, which seemed to vary from other sources with Pat Howley (PHo) in CSS and report back to HUHT and the Board. DECISION: The Board endorsed the priorities laid out in the HUHT Quality Account with several specific comments. ACTION: EP and Pat Howley to investigate the Health Visiting metrics and figures in the HUHT Quality Account and report findings to HUHT and the Board. Agenda Item 7 – CCG Authorisation update PH drew the Boards attention to the circulated summary guide to the CCG Authorisation process. City and Hackney CCG would be making an application in wave 3 of the authorisation process. Agenda Item 8 – IAPT Action Plan
City & Hackney pathfinder Clinical Commissioning Group Agenda Item 1
Haren Patel (HP) presented the Improved Access to Psychological Therapies (IAPT) action plan to the Board, updating the group that discussions with the Homerton had taken place and that self referrals remained a core part of the action plan. The Board expressed concern with the position, both due to the existence of a waiting list for access to the service currently, the proposed methods of ‘advertising’ self referral and the lack of long term planning for the future of the service. The Board asked that focus be given to a review of relative referral rates to the service by local practices, an investigation of any outliers be carried out and an investigation of methods of further varied, accessible engagement between the IAPT service, patients and GPs be instigated. The Board also noted that the CCG was still waiting on productivity data for the IAPT service. The Board approved the IAPT action plan, but requested that progress be closely monitored and noted that changes would likely be needed to the service. The Board asked for a progress review in 3 months time. DECISION: IAPT action plan approved, subject to close monitoring of performance, productivity and quality and potential changes in service provision in the future. ACTION: CCG to ask GPs to report outlier referrals to the CCG for discussion and review of relative referral rates to the service by local practices, an investigation of any outliers be carried out and an investigation of methods of further varied, accessible engagement between the IAPT service, patients and GPs be instigated. Agenda Item 9 – Any Other Business The next meeting of the CCG Board will take place 1330-1600 on Friday 25 May 2012 at the CCG meeting room. Agenda Item 10 – Feedback on Board meeting Danny Chesterman briefed the Board on his observation of the meeting, noting that he thought the session to be a good balance of challenge and support. The Board did request that future clinical items for discussion or decision at the meeting be presented by the relevant Clinical Lead and that a summary of action and decisions took place after each item.

CITY & HACKNEY PATHFINDER CLINICAL COMMISSIONING GROUP
City & Hackney pathfinder Clinical Commissioning Group Agenda Item 1
MINUTES OF THE NHS CITY AND HACKNEY PATHFINDER CLINICAL COMMISSIONING GROUP FINANCE AND PERFORMANCE SUB COMMITTEE
HELD ON FRIDAY 11 MAY 2012 AT THE HOMERTON IT SUITE, HOMERTON HOSPITAL
PRESENT: Dr Clare Highton (CCG Clinical Chair)
Paul Haigh (CCG Chief Operating Officer) Philippa Lowe (CCG interim Chief Financial Officer)
IN ATTENDANCE: Alison Leyshon (CSS Director of Resources) Chris Westcott (CSS Associate Director)
APOLOGIES: Mariette Davis (NHS NELC Non Executive Director) Operating arrangements:
We will move the date of the monthly Finance and Performance Sub Committee (FPSC) by 2-3 days to allow Philippa Lowe (PL) to review the first set of figures produced by Commissioning Support Services and iron out any discrepancies;
Matthew Knell (MK) will reschedule the dates of the meetings;
We will move to PL presenting the report to the FPSC and we will go through the finance and activity and agree actions.
Paul Haigh (PH) meeting with Alison Leyshon (AL), PL and Chris Westcott (CW) to review the format of the report which comes to the board but we felt on Friday:
We need something similar to what we get now to come to the FPSC - but focusing only on our delegated budgets;
This plus a summary/overview from Philippa would go to the Clinical Commissioning Group (CCG) Board, which gave us a sense on risks and issues.
The FPSC will have the key role in assigning responsibility for actions and for follow up - in many cases this will be either the Programme Boards and/or CSS and the Board will want to know who is taking what action, with FPSC reporting on progress. We agreed that the FPSC didn’t need to focus in detail on the key performance indicators (KPIs) - responsible for addressing any areas of concern would sit with the relevant Programme Board and we will probably have a system in place for the Boards to report on progress/actions direct to CCG Board (as we are doing with IAPT and 12+6):
We will use the weekly hot topics report which the CCG receives to track if any KPIs are going off track;
We need to find a way to incorporate KPI reporting into the Board report so they can be assured on a monthly basis and I suggest I pick this up via my forthcoming meeting on format of report.

City & Hackney pathfinder Clinical Commissioning Group Agenda Item 1
Actions: The specifics we agreed on Friday were as follows:
More detailed analysis needed by CSS on HRGs with increased spend under unplanned care (Nervous diseases; Musculoskeletal; Respiratory systems);
Chris to follow up and LTC Programme Board to agree what actions to take;
Planned Care Board to investigate increased cost of out patient department (OPD) procedures at Homerton;
Prescribing Board to review anticoagulation LES and potential to use as lever to reduce opd follow up (FU) and spend;
Planned Care Board will take lead on audits of OPD FU to explore opportunities to reduce and on action plan around direct access;
Prescribing Board to assess prescribing teams process for managing high cost drugs - assess by CSS and PL;
More detailed analysis of UCL spend to come to Planned Care Board to agree 12/13 action plan;
CSS to produce more detailed information on NCA spend - by POD and by specialty in first instance. to be sent to PH to agree actions;
Other acute contracts to be reviewed during 1st 6/12 of 12/13 to identify scope for reducing spend in 13/14.

Agenda Item 2a
Action Number (yymm.AN)
Action Action Owner Assigned Date
Due Date Update
1112.16 JB to submit formal terms of reference to the February 2012 PCCGC along with update on the work of the steering group.
Jaime Bishop 14/12/2011 25/05/2012 Terms of Reference to be produced in May 2012, presume will become CCG Board Sub Committee.
1204.01 MK to ensure remaining Declarations of Interest are submitted for the 25 May 2012 Committee meeting.
Matthew Knell 27/04/2012 25/05/2012
1204.02 Board members to communicate possible future items for discussion to MK.
Committee Members / Matthew Knell
27/04/2012 Ongoing
1204.03 Chris Westcott to undertake analysis of the movement of activity across providers during 2011/12 and report to the Board.
Chris Westcott / Commissioning Support Services
27/04/2012 27/07/2012
1204.04 Planned Care Programme Board to investigate Homerton referrals and non attendances.
Planned Care Programme Board
27/04/2012 27/07/2012 Action to be pursued via Planned Care Programme Board.
1204.05 EP and Pat Howley to investigate the Health Visiting metrics and figures in the HUHT Quality Account and report findings to HUHT and the Board.
Enrico Panizzo / Pat Howley
27/04/2012 27/07/2012 Action to be pursued via Children's Services Programme Board.
1204.06 CCG to ask GPs to report outlier referrals to the CCG for discussion and review of relative referral rates to the service by local practices, an investigation of any outliers be carried out and an investigation of methods of further varied, accessible engagement between the IAPT service, patients and GPs be instigated.
Paul Haigh 27/04/2012 27/07/2012 Action to be pursued via the Mental Health Programme Board.
NHS City and Hackney Pathfinder CCG Committee - OPEN ACTIONS

Agenda Item 12b
Pathfinder CCG Committee (PCCGC) Forward Plan
Subject Scheduled for
Led by Requested by
Request on / at Paper needed?
Revised 111 plan, specification and business case
sign off of specification and procurement process for decision
June 2012 Sarah McIlwaine
Paul Haigh 10/04/2012 email
Commissioning Primary Care Mental Health Liaison Service
Specification
Enhanced Service
May 2012 Rhiannon England
Paul Haigh 23/03/2012 email
Non Recurrent Funding Bids – April Tranche
Childrens IAPT Training
June 2012 Rhiannon England / David Maher
Paul Haigh 29/03/2012 email
Maternity 12+6 action plan June 2012 Kirsten Brown / Alison Glynn
Paul Haigh 06/02/2012 email CCG and/or Leads
Maternity Services Liaison Committee (MSLC) June 2012 Kirsten Brown / Alison Glynn
Alison Glynn 01/05/2012 email
IAPT action plan progress July 2012 Rhiannon England
Paul Haigh 30/04/2012 email

CITY & HACKNEY PATHFINDER CLINICAL COMMISSIONING GROUP
City & Hackney pathfinder Clinical Commissioning Group
City and Hackney pathfinder Clinical Commissioning Group Board
Name & CCG Role
Name of Individual / Company / Voluntary Body / Organisation
Nature of Business/ Organisation
Nature of Interest/Comments
Maureen Ford, Hackney LINk representative
Hackney LINk Health and Social Care watchdog
Co-Vice Chair
Maureen Ford, Hackney LINk representative
Hackney Centre for Independent Living
Centre for Independent Living Co-Chair
Maureen Ford, Hackney LINk representative
Commissioning for Personalisation Board, London Borough of Hackney
London Borough of Hackney Commissioning
Board member
Paul Haigh, CCG Chief Operating Officer
Helen Bullers, NHS ELC PCT NHS PCT Cluster Partner is Helen Bullers, NHS ELC Director of HR and OD
Dr Clare Highton, CCG Co-Chair
Lower Clapton Group Practice GP Principal Partner, our practice now provides a community ENT clinic run by my GP partner Dominic Roberts with our local ENT consultant. The practice also employs 3 Heart Failure nurses and their HCA and I am the clinical lead for this service.
Dr Clare Highton, CCG Co-Chair
Tavistock NHS Trust Mental Health Trust Rob Senior, the Medical Director is my husband.
Dr Haren Patel, Clinical Vice Chair
Latimer PMS Plus Practice Mental Health Service Provision
Senior Clinician and Management Lead for Project and Intermediate/Secondary Mental Health Service Provision
Dr Haren Patel, Clinical Vice Chair
NHS GMS Services at Acorn Lodge & Monarch Court Nursing Homes
Nursing Homes GMS and Enhanced Services under Nursing Home LES
Dr Haren Patel, Clinical Vice Chair
City and Hackney Local Medical Committee
Doctors organisation Member, may conflict with CCG role

CITY & HACKNEY PATHFINDER CLINICAL COMMISSIONING GROUP
City & Hackney pathfinder Clinical Commissioning Group
Name & CCG Role
Name of Individual / Company / Voluntary Body / Organisation
Nature of Business/ Organisation
Nature of Interest/Comments
Dr Haren Patel, Clinical Vice Chair
Specialised Commissioning Board
Commissioners for specialised tertiary activity
Board member, may conflict with CCG role
Dr Gary Marlowe, South West Consortium Co-Lead
Londonwide Medical Committee
Representative body for London’s GPs
City and Hackney Representative
Dr Gary Marlowe, South West Consortium Co-Lead
De Beauvoir Surgery
GP surgery
Partner at this provider of GMS services and a number of Locally Enhanced Services
Dr Gary Marlowe, South West Consortium Co-Lead
British Medical Association London Regional Council Representative
The major trades union for medical practitioners
Regional representative, representing doctors professional and working interests
Dr Paul Kelland, South West Consortium Co-Lead
Shoreditch Park Surgery GP Surgery GP at the Surgery
Philippa Lowe, interim Chief Financial Officer
Tower Hamlets CCG Newham CCG
NHS Commissioning Joint interim Chief Financial Officer
Philippa Lowe, interim Chief Financial Officer
PIQAS Ltd Consultancy Director of this Health care consultancy

CITY & HACKNEY PATHFINDER CLINICAL COMMISSIONING GROUP
City & Hackney pathfinder Clinical Commissioning Group
City and Hackney pathfinder Clinical Commissioning Group Clinical Executive Committee
Name & CCG Role
Name of Individual / Company / Voluntary Body / Organisation
Nature of Business/ Organisation
Nature of Interest/Comments
Heggy Wyatt, CCG Practice Nurse representative
City and Hackney Practice Nurse Forum
Representative and educational forum
Vice Chair of organisation, possible conflicts/confusion with CEC role to be discussed at next PNF
Heggy Wyatt, CCG Practice Nurse representative
Lower Clapton Group Practice GP Practice Employed by Lower Clapton Group Practice to work as a Practice Nurse at Lower Clapton Health Centre and Sorsby Health Centre
Jan Harley-Doyle, CCG Practice Manager co-representative
Somerford Grove Practice GP Practice General Manager - If the occasion arose that Somerford Grove Practice were the subject of discussion at an Executive Council Meeting, it may constitute a conflict of interests, although I am not present at those meetings in my capacity as their Manager, but as the representative of the views of all Practice Managers.
Dr Kirsten Brown, Urgent Care and Maternity Clinical Lead
The Lawson Practice GP practice Salaried GP
Dr Nikhil Katiyar Barton House Group Practice GMS GP Surgery GP Partner
Rhiannon England, Mental Health Clinical Lead
Central and North West Mental Health Foundation Trust
Provides mental health and primary care services to HMP Holloway
Working as a salaried GP for a neighbouring Mental Health Trust
Chloe David, Deputy for North West Hackney Consortium
Stamford Hill Group Practice
GP Surgery Office Development Manager, work at a practice which is part of the North East Hackney Consortium.
Mark Rickets North Middlesex Hospital
Acute Trust 3 month pilot post taken up in May 2012 as a GP Advisor to the Trust.

CITY & HACKNEY PATHFINDER CLINICAL COMMISSIONING GROUP
City & Hackney pathfinder Clinical Commissioning Group
Name & CCG Role
Name of Individual / Company / Voluntary Body / Organisation
Nature of Business/ Organisation
Nature of Interest/Comments
Dr Abdul Pathan, Rainbow Consortium Chair
Gadhvi Practice
GP Surgery GP practising at the organisation
Dr May Cahill, Well Consortium Lead
London Fields Medical Centre GP Surgery Lead Partner GP at the organisation
Dr May Cahill, Well Consortium Lead
Harmoni Out of Hours Provision for City and Hackney PCT
Sessional GP Provider to Harmoni-one session per month to teach, employed/contracted by HARMONI
Dr May Cahill, Well Consortium Lead
NHS ELC and NHS ONEL Cluster PCO Joint Medical Director in organisation
Dr Ajay Ojha, North Hackney Consortium Co-Chair
Nil return Nil return Nil return
Notes – Please declare all business with, or positions of authority in, a charity or voluntary body in the field of Health and Social Care and any connection with a voluntary or other body contracting for NHS Services. Nil returns to be completed if appropriate.
Include any relevant factors such as the extent of your involvement in the organisation and whether you gain any pecuniary benefit. Also, indicate the relationship the organisation may have with the NHS. Please include any relevant interests of your spouse/cohabiting partner.

Bid for NR funding for initiatives to develop care quality in primary care –
paper for discussion
Background
Formulating and agreeing the work and terms of reference for the Primary Care Quality Board
continues. To support some of the Board’s anticipated work it has been agreed that a bid be
submitted for non-recurrent funds held by NELC. This bid has been discussed in general terms with
Steve Gilvin at a meeting on 30.04.12 and seeks, in part, to address some of the KPIs outlined in the
NHS London’s GP Outcomes Standards (GPOS) dashboard.
The bid proposes ideas for general practice service development that don’t form part of the general
commissioning intentions for the coming year. The priorities are:
Determine what interventions would improve detection rates for various conditions
Improve practice performance in managing these conditions (both clinical and
organisational)
Improve indicators of that performance
For the bid, four clinical areas have been identified for attention:
Asthma/COPD
Dementia
Diabetes
Cardiovascular disease
Proposals for quality and productivity development have been garnered together through an
iterative process involving the CCG’s clinical leads for these areas, discussions with CCG
executives and Keith Prescott (manager of the Clinical Effectiveness Group - CEG) and were
discussed at the May CCG Executive meeting.
What is being asked of the CCG Board
At this stage, the CEG Board is only being asked to review these ideas and agree in principle the
areas for development. Following this, the bid will be worked up to include a clear strategy as to its
funding, delivery, monitoring and evaluation.
Proposals for consideration
The CCG executive meeting agreed 4 broad themes to inform the design of interventions:
Improved case finding to increase detection rates
Increased sharing of best practice
Develop patient education, empowerment, self-management and expertise
Increased education programmes for GPs, other clinicians, management and
administrative staff (either practice, consortia or patch based) using various models for
delivery.

Generic initiatives
Outline of proposal Delivery possibilities
CEG led work to increase disease prevalence. CEG run prevalence searches on EMIS web and
feedback to practices.
Support development of chronic disease
management clinics for patients with multiple
pathologies.
Similar model to the annual diabetic check but
for all chronic disease management especially
for patients with multiple pathologies (and
exploring possibilities for patient held record).
Model developed at the Nightingale Practice
involving both GP and nurse led clinics.
Share best practice. Develop improvement team approach (similar to
the diabetes improvement teams - DIT)
incorporating practitioners with high level
clinical, managerial and administrative skills
who are effective in developing similar skill sets
and behaviours in under-performing practices
and maintaining/supporting excellent practice
elsewhere. Such work to incorporate support
from both the Practice Managers’ and Practice
Nurses’ Forums and be aligned to CCG business
needs as commissioning intentions change.
Develop expert patient and self management
skills.
Education and training initatives, involve
practice-based patient participation groups and
CCG ley representation.
Develop educational activities. Educational activities need to be coordinated at
a patch, consortia and practice level and aligned
to business needs as commissioning intentions
change.
Asthma/COPD
Outline of proposal Delivery possibilities
Improving patients ability to recognise and self
manage the early signs of an exacerbation of
their symptoms. Practical advice and skills
development (eg get emergency inhaler from
pharmacist directly, alternatives to attending
A/E etc).
Education programme, especially involving
practice nurses extending the areas covered
during an As or COPD review to spend more
time on prevention and self-management of
exacerbations of symptoms.
Prevalence work, especially to address under
diagnosis of COPD.
Adapting the LES to include enhanced financial
incentive to undertake prevalence work.
Commission a service that would visit practices
to run searches to identify a population at risk of
developing COPD and offer these patients
diagnostic spirometry.

Dementia
Outline of proposal Delivery possibilities
Increase the diagnosis of dementia in a specific
at risk population (people recently admitted to
hospital with a history of delirium).
sessions to support pathway development and
cascade, and educational initiative.
Diabetes
Outline of proposal Delivery possibilities
Focusing on management of patients newly
diagnosed with diabetes with aim of achieving
very tight control (UKPDS Legacy effect).
Education programme, developing closer
working relationships with diabetic nurse
specialists (eg latter participating in practice
clinical meetings) and continued activity from
DIT (diabetic improvement teams).
CVD
Outline of proposal Delivery possibilities
Heart failure:
Increased detection rate (and accuracy of
diagnosis) and general management in primary
care
Develop methods to support improved case
finding to increase detection rates.
Consultant outreach education sessions.
AF:
Continue work to increase diagnosis and
improve management of patients with AF
Develop methods to support improved case
finding to increase detection rates.
Consultant outreach education programme, eg
an arrhythmia masterclass to consortia or
practices.
Hypertension:
Increased detection rate (and accuracy of
diagnosis) and general management in primary
care
Develop methods to support improved case
finding to increase detection rates.
Consultant outreach education sessions.
Mark Rickets – Primary Care Quality Board Clinical Lead 17.5.12

CITY & HACKNEY PATHFINDER CLINICAL COMMISSIONING GROUP
City & Hackney pathfinder Clinical Commissioning Group Agenda Item 1
NHS City and Hackney pathfinder Clinical Commissioning Group response to the East London Foundation Trust Quality Account
I've taken soundings from our mental health lead clinicians and the general views are:
Welcome the report and trusts openness;
Would find it useful to see more benchmarked information of how the Trust performs compared to other Trusts. User ratings are low so be useful to see this against benchmarks;
Similarly be helpful to get them to differentiate their data so can see the picture for each Borough they serve - a feeling that perhaps Trust wide data masks individual Borough issues;
Interesting research that women do better from day care than admission. The overriding comment was that the CQUIN performance reported was felt to bear little relationship to what GPs are seeing on the ground - eg discharge communications. So be good to get behind the audit results. Don't know how you are planning to engage GPs in CQUINs for 12/13?

CITY & HACKNEY PATHFINDER CLINICAL COMMISSIONING GROUP
City & Hackney pathfinder Clinical Commissioning Group Agenda Item 1
NHS City and Hackney pathfinder Clinical Commissioning Group response to the Barts and the London Trust Quality Account
Liked: 1. High rate of return post-discharge for heart failure, identified 3 factors (lack of
understanding of condition, poor recognition of symptoms, poor compliance meds) and set up system/ patient education to address this which has significantly reduced rate. Hope they plan to extend this to other areas.
2. Standardised and Summary Hospital Mortality Index below average (good). Concerns: 1. Number of measures still below target eg. prevention VTE, pressure ulcers,
non-elective admissions reviewed by consultant within 24hrs. 2. Especially concerning for the long-term quality of the hospital is that only 52%
of staff agreed organisational culture makes it easy to learn from mistakes of others and only 54% agreed leaders listen and respond to their patient safety concerns.

The CCG Board is asked to note and agree the proposed plans
WORKING WITH LONDON BOROUGH OF HACKNEY
NHS City & Hackney CCG 1
2 THEMES – 5 INITIATIVES
NHS City & Hackney CCG 2
COMMUNICATIONS Work with LBH Communications team to Recruit to and establish a Maternity Services Liaison
Committee to support our Programme Board and provide user input
Undertake a marketing campaign aimed at specific Hackney communities to promote early booking of pregnancy
Undertake a campaign to increase GP registration
We have agreed a non recurrent budget from NELC to support this work and test out the communications offer as an alternative to CSS offer for 13/14
WORKING WITH THE VOLUNTARY SECTOR
NHS City & Hackney CCG 3
Fund a scoping project to develop a business case for “social prescribing” This would explore how best to support GPs to refer suitable patients for
health and wellbeing/health promotion/support initiatives – primarily run by the voluntary sector
Commission LBH to run a small grants scheme We have secured 700k non recurrent funding for commissioning additional
voluntary sector services We would ask LBH to run a programme to invite bids which would focus on
Vulnerable Children & families Vulnerable elders People with MH Problems
We would establish a group to decide on where to award the money which would consist of a CCG GP, CCG lay member and public health
We would also ring fence £70k for a similar process with the City of London

SMI-DEPOT LES 12-13 Dr Rhiannon England (CCG GP MH lead) David Maher (CSS) and Eleanor Watson (CCG)

BACKGROUND: THE CASE FOR CHANGE:
System redesign in Mental Health Care is recommended “with a shift towards primary care provision” by: The Whole Systems Review 2011 London Health Programmes (2011)Mental Health Services Case for
Change RCGP / RCPsych (2012) Guidance for Commissioners of primary MH
care services Also financially, within the context of 12/13 being the PBR
shadow-year for MH and approaching cost pressures for C&H Commissioners for 13/14
Re: HONOS clustering and the need to develop cost- effective and clinically appropriate patient care packages
And concentrating on HONOS clusters 3 and 11 to realise a saving of £200k from the ELFT contract against a shift in activity from secondary care out-patients to primary care.

RATIONALE AND STRATEGY: To establish a Primary Care Mental Health Liaison service in
City & Hackney Consisting of enhanced secondary care support to primary
care Via Consultants attending practice MDT meetings And to recruit MH Liaison Workers (who although ELFT employed
will be “attached to practices”) In support of the Serious MH Illness / DEPOT LES for
improved integration of patients’ mental and physical health care and for better social outcomes
To facilitate the supported discharge of stable (and willing) patients into primary care
And thereby decrease future secondary care PBR costs for some patients who would be best treated within a primary care setting under the new supported MH Liaison Service (i.e. leading to a shift of activity)

WHERE THE MONEY IS COMING FROM:
As part of the 12/13 NHS C&H CCG Strategy Plan, £400k has been committed to the development of a Primary Care MH Liaison Service and an improved primary/secondary care interface
The £400k commitment is delivered from CSP Commissioning intentions to deliver £1m savings from the C&H MH Portfolio including improved productivity in psychological therapies
£100k is broadly allocated to the SMI-DEPOT LES 12/13 £300k is broadly allocated to fund the Primary Care MH
Liaison Workers (6 x band 5-6 Community MH Nurses)

PROGRESS TO DATE:
The SMI-DEPOT LES Specification has been presented to CCG CC Forum, emailed to all GPs for comment, and presented to and approved by the MHSIG (during 11/12)
The first meeting of the MH Programme Board will receive the final proposals on 28th May 2012
An earlier LES Specification was sent to the LMC in April and will be presented again within the next month: LMC objections raised: The need for MH training of GPs LMC requested to see the operational specification too

NEXT STEPS:
Eleanor, David and Dr Rhiannon England have met with Richard Evans, Caroline Methuen and Dr Valsraj (ELFT Deputy Clinical Director and Primary Care Liaison Service Lead) to plan the implementation of the service across all practices signing up to the LES
This will include letters and individual practice meetings with a presentation and questions and answers session (in July) to all practices to demonstrate the model and the process for discharge and “stepping up” of patients into the LES
The aim is to start discharges of patients under the LES / Liaison service by July 2012

PROPOSALS FOR THE CCG BOARD TO CONSIDER:
The CCG Board is asked to: Approve as per the CSP 2012 / 13 to reinvest £400k into the
LES (£100k) and the Primary Care MH Liaison Service (£300k)
And
To approve the use of £10k (one-off) funding from the London Health Programmes (allocated to the CCG) to work with secondary care to improve communication as preparation for the introduction of the Primary Care MH Liaison Service

1
Title of Report:
Development of primary care mental health service in City and Hackney
Author(s): Date finalised:
David Maher – Mental Health Commissioning, NHS East London and the City, Commissioning Support Services April 2012
Presented by: Sponsor (if different): For further information contact
Rhiannon England, CCG MH Lead [email protected] [email protected]
Executive Summary: This paper details proposals to establish a primary care mental health service in City and Hackney, consisting primarily of enhanced secondary care support to primary care (e.g. consultants attending regular practice based MDT meetings), a Serious Mental Illness Local Enhanced Service, and a primary care mental health liaison service. Key issues: The proposals to develop a primary care mental health service are in response to recommendations made in the East London & the City Whole Systems Review of mental health services, which found that there is a widely held view across east London that communication and the systems and processes that support clinical practice could be significantly improved across primary and secondary care mental health services. Evidence suggests that there are potentially a number of service users currently in receipt of secondary care mental health services who could be supported in a primary care setting, if there were appropriate support designed around them, including people with common mental health problems and with a serious, but stable, mental illness. The impending introduction of payment by results into mental health potentially places the City & Hackney Clinical Commissioning Group at financial risk. Service users are clear that they would like to be able to access non-stigmatising services as close to home as possible, but there is significant variability in their experience of primary care. Committee/Group (where has this been before being taken to the Board and what was the outcome) The proposals to develop a primary care mental health service are in response to recommendations made in the East London & the City Whole Systems Review of mental health services, implementation of which has been overseen by the CCG led East London & the City Mental Health Commissioning Board. Locally, the proposals have been to the Clinical Executive, the Clinical Commissioning executives and to the LMC, with plans for further engagement with service users and carers through the local Service Users Reference Group. The LES component has to be recirculated to LMC following some proposed
Meeting: City and Hackney CCG Board Date of meeting: May 2012
Enclosure

2
amendments. Risk implications (and action taken to mitigate any identified risk) Potential clinical risks are being controlled through the design of the LES and primary care mental health liaison service. With the imminent introduction of payment by results into mental health, there are significant potential financial risks to the NHS City and Hackney Clinical Commissioning Group should the infrastructure to support the discharge of patients from secondary to primary care not be put in place. Public and user involvement: The proposals have been considered at the Mental Health Commissioning Board where service users are represented. They have also been discussed at the Service User Reference Group Budget/Legal Issues: This paper proposes £10,000 one off funding from the London Health Programmes be allocated to networks to work with secondary care to improve communication as preparation for the introduction of the primary care mental health service. The paper proposes, as per the 2012/13 Commissioning Strategy Plan, to reinvest £400,000 into: the Local Enhanced Service (£100,000) and the primary care mental health liaison service (£300,000).

3
Development of primary care mental health service in City and Hackney
1. BACKGROUND: CASE FOR CHANGE
1.1 In Summer 2011, NHS East London & the City concluded a whole systems review of mental health services across inner north east London. The review process included a needs assessment, extensive stakeholder engagement including service users and carers, primary and secondary care clinicians, social care professionals and the third sector, an evidence and best practice review, and an initial health economic analysis. The review laid out a set of recommendations for developing and improving mental health services across inner north east London, including:
1.2 An inner north east London Mental Health Commissioning Board has been formed to oversee implementation of the recommendations. Led by the east London Clinical Commissioning Groups, the Board includes local authority and service user representatives. This oversight will migrate locally to the MH Programme Board where this work will be coordinated through a task and finish group. 1.3 The review found that a very strong emphasis was placed by clinician stakeholders on the importance of improving communication, and the systems and processes necessary to support effective clinical practice, across primary and secondary care, and that there was an outstanding need to properly integrate the mental and physical health care of people with long term mental health problems. It was also reported that current pathways into and out of secondary care mental health services are not always clear. Service users reported variability in their experience in primary care, with some noting that their GP’s knowledge of, and sensitivity to, their condition was excellent and others noting a more mixed experience. Local authorities were concerned about slow uptake of personal budgets and direct payments as a marker of a more personalised mental health service. 1.4 During the course of the review, East London NHS Foundation Trust reported that in their view there were a number of patients who were currently in receipt of secondary care mental health services who, if there were the right support available in primary care, would potentially be clinically appropriate for discharge back from secondary to primary care. 1.5 The London Health Programmes (2011) Mental Health Services Case for Change suggested that the east London experience is replicated in many parts of London, with current services that overlap with a lack of coherent pathways, a lack of integration of physical and mental health care, variability of primary and secondary care and their interface and a lack of routine outcome measurement (p. 29), and service users in receipt of secondary care services who could potentially be clinically appropriate for discharge to primary care with the right support available. The Case for Change proposes an outline model to deliver more effective primary/secondary care pathways for people with mental health problems, including clarity of pathways from primary to secondary care, better
System re-design is required with a shift towards primary care based provision
• We have high levels of mental ill health and resources are limited
• The current system of mental health and social care does not deliver the most effective care and treatment for those in need
• Options for the future configuration of services need agreement at a cluster, borough and practice level
A prevention strategy will reap short and long term benefits
• Social resilience and primary prevention improve individual and population mental well being
• Secondary prevention interventions, including employment, housing and social networking, improve the quality of life and recovery prospects for people with mental health problems
Pathways and access routes must be clear – a real single point of entry
• With information about the range of services readily available to users, carers and professionals
Quality improvement is vital
• We have on-going concerns about patient safety and experience
Outcome measurements need development
• To support a user centred recovery approach
• To systematically measure the effectiveness of services.

4
engagement of secondary care clinicians with primary care, the development of local enhanced services and qualified mental health and social care professionals working in a primary care setting. 1.6 The RCGP and RCPsych (2012) Guidance for Commissioners of primary mental health care services reaffirms the evidence base for developing primary care mental health services, and notes the QIPP opportunities of supporting more service users with a mental health problem in a primary care setting. 1.7 As context, Payment by Results is being introduced into mental health in shadow form in 2012/13 with full implementation in 2013/14. PbR in mental health is structured around 21 clusters, or descriptions of need, with associated timelines which will act as the episodes of activity for which providers will be paid (see Appendix One for details of the clusters). With the introduction of PbR in mental health, there is the potential for a significant cost pressure for the NHS City and Hackney Clinical Commissioning Group as from 2013/14 and beyond, should secondary care be providing support that could be potentially be provided more cost effectively in primary care. 1.8 A model1 of potential activity and costs to indicate the potential financial implications is detailed below. Included in the modelling for consideration for discharge to primary care are service users who have a condition in clusters 1, 2 and 18 (common mental health problems (low severity), common mental health problems, cognitive impairment (low need) and service users who have a condition in clusters 3 and 11 (non-psychotic (moderate severity) and on-going recurrent psychosis (low symptoms) and who have had 0 or 1 contacts in the last 6 months.
Cluster Newham C&H TH MHCOP Total patients
1 110 55 135 56 356
2 128 175 318 57 678
3 129 126 198 31 484
11 180 121 110 21 432
18 6 6 2 340 354
Total 553 483 763 505 2304
Cost model £587,811 £688,585 £1,256,885 £653,461 £3,186,742
1.9 It is primarily patients in cluster 3 & 11 who will be supported through the primary care LES. In this context, the 2012/13 NHS City and Hackney Clinical Commissioning Group Commissioning Strategy Plan includes a saving of £200,000 to be realised from the East London NHS Foundation Trust contract against a shift in activity from secondary care out-patients to primary care. ELFT have proposed that this saving is deferred to 2013/14.
2. DEVELOPMENT OF PRIMARY CARE MENTAL HEALTH SERVICE FOR PEOPLE WITH A SERIOUS MENTAL ILLNESS
2.1 As part of the 2012/13 NHS City and Hackney Clinical Commissioning Group Commissioning Strategy Plan, £400,000 has been committed2 to the development of a primary care mental health service and an improved primary/secondary care interface. The approach is intended to improve mental and physical health and social outcomes for people with mental health problems by
1 It should be noted that this is a broad model to outline potential scenarios based on November 2011 activity and estimated costs, and should not be taken as an exact current representation of currently clustered patients, and does not represent service users to be discharged. A revised list of 232 has been circulated by ELFT but further analysis is pending on this segmentation. 2 The £400,000 commitment is delivered from CSP commissioning intentions to deliver ~£1m savings from the City and Hackney mental health commissioning portfolio, including improved productivity in psychological therapies.

5
developing a primary care mental health service with an emphasis on healthy lifestyles and social inclusion:
• Embedding in practice a real single point of access to mental health services for people of working age, through Community Mental Health Teams
• Developing better joint working between secondary and primary care through each practice having an identified Community Psychiatric Nurse and a consultant psychiatrist link who attends regular practice multi-disciplinary meetings in the practice
• Developing streamlined systems and processes to improve communication between secondary and primary care, with agreed interface agreements between primary care the primary care liaison service
• Ensuring that people with a serious mental illness have access to regular physical health checks, have physical health problems identified and access to chronic disease management as appropriate, and are supported to access appropriate services to promote healthy living
• Developing a Local Enhanced Service to support practices to deliver an enhanced level of support for service users with a serious mental illness in primary care
• Developing a mental health liaison service, a team of mental health nurses, based in primary care, to provide support for service users receiving enhanced support via the LES
• Developing a clear pathway that details how service users receiving enhanced support via the LES will access healthy living advice and support
• Supporting the clinically appropriate discharge of service users from secondary to primary care, primarily service users in clusters 1, 2, 3, 11 and 18, in line with a good practice discharge protocol
• Promoting professional development in primary care through MDT meetings with link consultant psychiatrists and a programme of protected learning time on mental health issues.
2.2 East London NHS Foundation Trust have agreed that the four Community Mental Health Teams for adults of working age in the borough will act as the single point of access to referrers from the practices linked to them. In effect, the CMHT will channel referrals internally within ELFT to the appropriate team, should the CMHT itself in the first instance not be best suited to assess or provide treatment for the service user.
2.3 One approach to the development of better joint working across primary and secondary care will be closer defined working arrangements through Interface Agreements. These agreements will focus on the relationships between primary and secondary care and may include innovations such as regular telephone contact with secondary care clinicians, regular in practice development sessions etc. The agreed specification is attached.
2.4 A Local Enhanced Service is currently under development, and is being considered by the lead CCG clinicans with a view to a final draft being tabled for agreement at the LMC in June 2012. The purpose of the LES is to put in place the infrastructure to provide an enhanced level of support in primary care for people with mental health problems who would be eligible for inclusion on the QoF serious mental illness register, primarily service users in cluster 11, that is safe, recovery-focussed and which delivers positive outcomes for service users.

6
2.5 It is proposed that the LES will fund practices to continue to work with secondary care to develop and maintain robust systems of communication, following the end of any WSR development funding.
2.6 It is proposed that the LES will incentivise networks to support practices to deliver a package of care that includes:
• An annual GP-led mental and physical health review
• Access to the primary care mental health liaison worker service
• In partnership with the primary care mental health liaison worker, a recovery plan which will address how the service users mental and physical health and social care needs will be met
• Proactive sign-posting to healthy lifestyles advice where a service user has a high BMI or is a smoker
• Prescribing and administration of depot medication.
2.7 There is currently £100,000 (of the £400,000) broadly allocated to fund the LES. Full costings will be developed on receipt of further activity data from East London NHS Foundation Trust in the next two weeks.
2.8 To support the Local Enhanced Services, the CCG is currently working with public health to identify pathways into healthy lifestyles advice and support.
2.9 It is proposed that service users in receipt of support via the LES will have access to a primary care mental health liaison worker service. It is proposed that the primary care liaison worker service would:
• Liaise with practices and East London NHS Foundation Trust to identify service users potentially eligible for discharge into primary care
• Provide an assessment of service users stepping up from primary care into the LES
• In partnership with the practice, develop a recovery plan3 for service users receiving support via the LES, and ensure that the service user holds a copy of their recovery plan
• Provide a minimum of three monthly proactive contact with service users receiving support via the LES
• Where the service user is prescribed anti-psychotic medication, undertake side-effects screening as part of three monthly proactive contact
• Provide proactive contact with service users receiving support via the LES should they “Do Not Attend” a practice appointment
• Facilitate rapid access back into secondary care services where a patient previously discharged from ELFT into the LES appears to be at risk of relapse
• In partnership with the practice, identify service users for discharge from the LES
3 It is anticipated that the recovery plan will address how mental and physical health needs will be met with an emphasis on healthy lifestyles and social inclusion. It will explicitly include contingency planning.

7
• Provide advice to practices regarding service users who are not receiving support via the LES, but where the practice has concern about their mental health.
2.10 There is currently £300,000 (of the £400,000) broadly allocated to fund the primary care mental health liaison service. It is proposed that the service comprises circa 6 Band 5-6 Community Mental Health Nurses, to be distributed across borough in line with demand, and with cross-cover to ensure that service levels are maintained in the event of sickness or annual leave. It is proposed that the posts are based in practices. In view of the benefits for effective communication across primary/secondary care of the posts being employed via East London NHS Foundation Trust, and because the funding for the posts will be delivered through de-commissioning current East London NHS Foundation Trust services, it is proposed that a contract variation be agreed with East London NHS Foundation Trust for the delivery of the posts as part of contract negotiations for 2012/13, with posts being recruited to by June 2012.
3. SERVICE USERS WITH A COMMON MENTAL HEALTH PROBLEM OR COGNITIVE IMPAIRMENT WITH LOW NEEDS
3.1 There are currently a number of service users with a common mental health problem or a cognitive impairment with low needs in City and Hackney, who are generally seen in an out-patient setting. Whilst some of these patients are referred for assessment and then discharged back to primary care following a brief intervention as part of routine practice, it appears that the number of service users in clusters 1, 2 and 18 could be better served by services through IAPT services . IAPT services are not included in PBR for 2014 onwards and as part of the NHS City and Hackney Clinical Commissioning Group Commissioning Strategy Plan, it is proposed that £200,000 is generated as savings through discharging service users from secondary care out-patients back into primary care general medical services.
3.2 There are currently a range of services available for people with a common mental health problem or cognitive impairment and low to moderate needs outside of secondary care services, including general medical services, primary care psychology including IAPT services, and a range of voluntary sector services for people with a common mental health problem, and the Alzheimers Society Dementia Adviser Service for people with a cognitive impairment and low to moderate needs.
4. SOCIAL CARE
4.1 There may be some service users discharged from secondary to primary care who have on-going social care needs. Some social care needs may be met by universal third sector day opportunity and support services, for example social support and networking, or employment support. However some service users may be in receipt of formally commissioned social care services such as day care or home care. The number of service users in receipt of formally commissioned social care is likely to increase in the context of the London Borough of Hackney strategy to increase the number of service users purchasing services themselves via a personal budget increases, including service users accessing primary care mental health services.
4.2 The London Borough of Hackney are currently exploring options to ensure that their responsibilities for assessment and care management under the NHS & Community Care Act 1990 for service users who may access primary care mental health services are met. Interim options under consideration include access either via identified social work sessions within CMHT’s to take on a specific remit within the primary care mental health service, or via generic social work services. Longer term, the London Borough of Hackney is intending to realign social care pathways for people with mental health problems in the context of Transforming Adult Social Care.

8
5. DISCHARGE OF SERVICE USERS FROM EAST LONDON NHS FOUNDATION TRUST TO PRIMARY CARE
5.1 East London NHS Foundation Trust will populate a dataset which will detail service users that they believe may be clinically appropriate for discharge to primary care, which will form the basis of a pre-discharge clinical discussion between linked secondary and primary care clinicians to determine appropriateness from a primary care perspective.
5.2 Discharge will only take place where secondary and primary care clinicians are agreed it is appropriate, and subject to consultation with the service user. East London NHS Foundation Trust will discharge service users in line with a good practice discharge protocol, currently in development. All service users at the point of discharge will have a recovery plan in place4, which may include access to third sector services, primary care psychology services, the Local Enhanced Service and primary care mental health liaison service.
6. PROJECT MANAGEMENT
6.1 The development of the service is managed locally by Dr. Rhiannon England with project support provided by the Commissioning Support Organisation. Subject to CCG Board approval, it is anticipated that:
• Cluster mental health leads identified to work with secondary care leads by end July 2012 (ensuring the £10,000 one off funding is delivered)
• Arrangements for meeting the needs of service users with a commissioned social care service agreed by July 2012
• Primary care mental health liaison workers in post by June 2012
• Local Enhanced Service in place by June 2012
• Process of identifying patients for discharge from East London NHS Foundation Trust to primary care begins June 2012.
7. CONCLUSION
7.1 This paper has outlined proposals to develop a primary care mental health service in City and Hackney, including an approach to improving communication across primary and secondary care, the development of a local Enhanced Service for service users with a serious mental illness, and the development of a primary care mental health liaison service. It is anticipated that the development of the service will improve integrated mental and physical health care for service users with a serious mental illness, and will manage potential cost pressures on the NHS City and Hackney Clinical Commissioning Group in the context of the pending introduction of Payment by Results.
4 This may take the form of a discharge letter for service users with low levels of need, not discharged into the LES.

9

10
APPENDIX ONE
Mental Health Payment by Results Clusters
Cluster no.
Cluster label
0 Variance
1 Common mental health problems (low severity)
2 Common mental health problems
3 Non-psychotic (moderate severity)
4 Non-psychotic (severe)
5 Non-psychotic (very severe)
6 Non-psychotic disorders of overvalued Ideas
7 Enduring non-psychotic disorders (high disability)
8 Non-psychotic chaotic and challenging disorders
9 Blank cluster
10 First episode in psychosis
11 Ongoing recurrent psychosis (low symptoms)
12 Ongoing or recurrent psychosis (high disability)
13 Ongoing or recurrent psychosis (high symptom and disability)
14 Psychotic crisis
15 Severe psychotic depression
16 Dual diagnosis (substance abuse and mental illness)
17 Psychosis and affective disorder difficult to engage
18 Cognitive impairment (low need)
19 Cognitive impairment or dementia (moderate need)
20 Cognitive impairment or dementia (high need)
21 Cognitive impairment or dementia (high physical or engagement)

11
APPENDIX TWO
Local Enhanced Service

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
1
DRAFT: LOCAL ENHANCED SERVICE FOR MENTAL HEALTH (Version 2.3) 2012-2013 1 Introduction
1.1 This Local Enhanced Service recognises the importance of an effective evidence-based care pathway across primary and secondary care to support patients with a serious mental illness (SMI) to live healthy lives. 1.2 It recognises the high prevalence of mental illness across east London, and the consequent high demand placed on local health services, both in primary and secondary care. 1.3 Evidence suggests that across London (London Health Programmes, 2010) there are a number of patients currently treated within secondary care mental health services who, after a period of treatment, have become stable and therefore no longer meet the threshold for secondary care services but who need an enhanced level of support above that delivered through general medical services. East London Foundation Trust have identified a number of patients who they believe may be appropriate for discharge to an enhanced level of support in primary care. This Local Enhanced Service aims to provide the enhanced level of support in primary care that would support discharge where it is clinically appropriate. 1.3 There are also patients with a serious mental illness who do not receive secondary care mental health services, but who would benefit from an enhanced primary care mental health service, including patients currently receiving a regular depot administration in primary care. 1.4 This Local Enhanced Service aims to provide an enhanced primary care service for people with a serious mental illness, over and above the additional support patients with SMI currently receive through QoF. 1.5 Patients eligible for the Local Enhanced Service will also be eligible for a new Primary Care Liaison Service that will provide access to specialist mental health professionals in primary care. 2 General principles of the Local Enhanced Service: 2.1 All practices are expected to provide the essential and those additional services that they are contracted to provide to all their patients. This enhanced service specification outlines the more specialised services to be provided. The specification of this service is designed to cover the enhanced aspects of clinical care of the patient, all of which are currently beyond the scope of essential services.
2.2 No part of the specification by commission, omission or implication defines or redefines essential or additional services.

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
2
2.3 This LES will not replace the enhanced support that patients with SMI receive via the QoF SMI register, it is designed to work alongside the SMI register for patients who are clinically appropriate for the enhanced level of support that the LES will offer. 2.4 The specification has been developed on the basis of the substantial evidence concerning the benefits to patient outcomes and quality that both an enhanced primary care service can bring, alongside improved joint working with secondary care mental health services, including (as summarised from London Health Programmes (2011, p. 29):
• improved competence of primary care teams can reduce use of secondary are services and improves quality of care (e.g. Forrest et al., 2006; Katon et al., 2002; El-Adl et al., 2009; Meadows et al., 2007)1
• improved partnership working and communication between all relevant parties
can improve quality and outcomes of care (e.g. Foy et al., 2010; Fuller et al., 2011) • more active involvement of primary care teams can improve physical health
care for those with a long term mental health condition (e.g. Lawrence & Kisley, 2010; Phelan et al., 2001)
• addressing wider determinants of health can improve health outcomes and
reduce service usage (e.g. Burns et al., 2009; NMHDU, 2011)
• Implementation of evidence based interventions can improve clinical outcomes and increases service efficiencies (Benyon et al., 2008; Drake et al., 2009)
• Use of recovery oriented practice acknowledges the importance of enabling
individuals to move towards recovery using a range of community and self-help resources (NIMHE, 2006).
1 Summarised from London Health Programmes (2010) Mental Health Models of Care for London. London: LHP, available at: http://www.londonhp.nhs.uk/wp-content/uploads/2011/03/2.-Models-of-care-low-res.pdf . References: Forrest, C., Nutting, P. A., von Schrader, S., Roghe, C., & Starfield, B. (2006). Primary care physician speciality referral decision making: patient, physician, and healthcare system determinants. Medical Decision Making , 26, 76-85; Katon, W., Russo, J., Von Korff, M., Lin, E., Simon, G., Bush, T., et al. (2002). Long-Term Effects of a Collaborative Care Intervention in Persistently Depressed Primary Care Patients. Journal of General Internal Medicine , 17, 741-748; El-Adl, M., Burke, J., & Little, K. (2009). First-episode psychosis: primary care experience and implications for service development. Psychiatric Bulletin , 33, 165-168; Meadows, G. N., Harvey, C. A., Joubert, L., Barton, D., & Bedi, G. (2007). Best Practices: the consultation-liaison in primary care psychiatry proramme: a structured approach to long-term collaboration. Psychiatric Services , 58, 1036-1038; Shanman, R., et al. (2010). Meta-analysis: Effect of Interactive Communication Between Collaborating Primary Care Physicians and Specialists. Annals of Internal Medicine , 152, 247-258; Fuller, J. D., Perkins, D., Parker, S., Holdsworth, L., Kelly, B., Roberts, R., et al. (2011). Building effective service linkages in primary mental health care: a narrative review part 2. BMC Health Services Research , 11 (66); Lawrence, D., & Kisley, S. (2010). Inequalities in healthcare provision for people with severe mental illness. Journal of Psychopharmacology , 24 (11), 61–68; Phelan, M., Stradins, L., & Morrison, S. (2001). Physical health of people with severe mental illness: Can be improved if primary care and mental health professionals pay attention to it. British Medical Journal , 322 (443); Burns, T., Catty, J., White, S., Becker, T., Koletsi, M., Fioritti, A., et al. (2009). The Impact of Supported Employment and Working on Individual Placement and Support. Schizophrenia Bulletin , 35 (5), 949–958; National Mental Health Development Unit. (2011). Mental Health and Housing: Housing on the Pathway to Recovery. London: NMHDU; NIMHE (2006) Emerging best practices in mental health recovery. London:DH.

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
3
3 Service Outline 3.1 This LES will fund participating practices to provide an enhanced level of care to patients with Serious Mental Illness, including those discharged from East London Foundation Trust (ELFT) and those who are appropriate to step up from the Practice SMI Register. 3.2 Each practice will be supported by on-going quarterly clinical consultation sessions based in practices and led by the named consultant psychiatrist. 3.3 Each practice will attend a regular meeting with the lead consultant psychiatrist and liaison worker for the practice to discuss patients under CMHT or LES care, as part of a commitment to ongoing education and support. These sessions can form part of the quarterly consultations outlined in 3.2. 3.4 Where a patient is for sole management by primary care through the LES, practice responsibilities will include:
• annual mental health review by GP
• annual physical health check, in addition to the annual health check generated via requirements of QoF, i.e. patients will receive two physical health checks per year the second tailored to the needs of the patient concentrating on BMI/smoking/BP control/diabetes control/social inclusion/sexual health/drugs and alcohol
• an enhanced care plan with an emphasis on recovery via increase in daily
activities/employment and training advice/personal goal setting
• administration of depot medication. 3.5 Where a patient is receiving a service from East London NHS Foundation Trust (patients currently receiving depot in primary care and on CPA) , practice responsibilities will include:
• annual physical health check, in addition to the annual health check generated via requirements of QoF, i.e. patients will receive two physical health checks per year.
3.5 Practices will maintain a list of all patients receiving support via the LES. 3.6 Any patient eligible for the LES will have access to the Mental Health Liaison Service. Mental Health Liaison Service responsibilities will include:
• To agree with practices patients eligible for the LES where they are being discharged by East London NHS Foundation Trust
• To develop an enhanced care plan for patients on the LES including how their health
and social care needs will be met, with an emphasis on healthy living and accessing mainstream community services

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
4
• To provide a minimum of three monthly proactive contact with patients on the LES.
This can include case review activity with the primary care mental health liaison worker
• To provide proactive contact with patients on the LES should they DNA an
appointment, either within the practice, with the mental health liaison worker, or for depot injection
• To facilitate rapid access to secondary care assessment should a patient on the LES
relapse
• To participate in annual GP mental health review, should this be required
• To provide a mental health assessment of patients moving on to the LES from the primary care SMI register.
4 Patient Eligibility 4.1 Practices will be responsible for determining clinical eligibility for the LES, when the patient otherwise meets the following criteria:
• A resident of City and Hackney and permanently registered with a GP practice in City and Hackney
• Aged 18 years or older • Has an established diagnosis of a serious mental illness that would warrant their
inclusion on the practice SMI register (i.e. psychotic illness or bipolar affective disorder)
• Has needs above those that would ordinarily be provided for under normal GMS
care, either medical or social needs, that require additional support • Patients requiring lithium prescribing or depot injections in primary care will be
automatically included on the LES • The patient agrees to the support offered via the LES.
4.2 The Mental Health Liaison Function will use a case-finding tool outlined in 4.7 below. The decision as to a patient’s suitability for entry into the LES will not be made purely on a set of pre-determined criteria or SMI status as these factors are not the sole determinants of whether an individual can successfully self manage with ongoing support in primary care. Other factors that the practice may wish to take into account include:
• History of risk of self-harm or harm to others

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
5
• History of vulnerability • History of alcohol or substance misuse • On more than one drug • Co-morbid physical health problems • Complex social or family circumstances.
4.3 Patients considered for discharge from East London NHS Foundation Trust into the LES will generally include patients who:
• Are currently under the care of ELFT services • Have sustained their progress with less frequent support from the CMHT, and do not
need specialist interventions and treatments • Have settled accommodation • Are able to meet their own basic living needs • Are well-established on a medication regime and require minimal assistance with
concordance, but require regular monitoring and review • Are prepared to participate in the LES and attend additional appointments when
prompted to do so • Are discharged in accordance with the discharge protocol.
4.4 All patients eligible for entry on to the LES via discharge from ELFT services will generally have been assigned to a cluster under a new mental health Payment by Results framework being adopted NHS-wide over 2012/2013 for full adoption by 2014. Mental Health Care Clusters (Care Clusters) are groupings of service users based on their characteristics. They are a way of classifying individuals using Mental Health services that is intended to form the basis for payment when secondary care mental health services move to Payment by Results in 2014. 4.5 There are 21 possible Care Clusters, numbered from 01 (Common Mental Health Problems (Low Severity)) to 21 (Cognitive Impairment or Dementia (High Physical or Engagement)). There is also a variance cluster 0, used when none of the clusters are appropriate.
Cluster Number
Cluster Description
0 Variance 1 Common mental health problems (low severity)

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
6
2 Common mental health problems 3 Non-psychotic (moderate severity) 4 Non-psychotic (severe) 5 Non-psychotic (very severe) 6 Non-psychotic disorders of overvalued Ideas 7 Enduring non-psychotic disorders (high disability) 8 Non-psychotic chaotic and challenging disorders 9 Blank cluster 10 First episode in psychosis 11 Ongoing recurrent psychosis (low symptoms) 12 Ongoing or recurrent psychosis (high disability) 13 Ongoing or recurrent psychosis (high symptom and disability) 14 Psychotic crisis 15 Severe psychotic depression 16 Dual diagnosis (substance abuse and mental illness) 17 Psychosis and affective disorder difficult to engage 18 Cognitive impairment (low need) 19 Cognitive impairment or dementia (moderate need) 20 Cognitive impairment or dementia (high need) 21 Cognitive impairment or dementia (high physical or engagement)
4.6 For the purposes of this LES, only clusters 3 & 11 are included in the LES, but clusters 1, 2, and 18 are expected to be supported via QoF. All discharged patients will be supported by the new Primary Care Mental Health Liaison Function which augments the enhanced support provided by QoF and the LES. 4.7 The Primary Care Mental Health Liaison Function supporting this LES will initially use the case-finding tool outlined below for selecting potential patients for discharge onto either QoF or LES. The Locally Determined Exclusion Criteria elements will be subject to wider
review as part of the patient transfer process. Clinicians will need to collaborate to ensure appropriate patients are identified for discharge and additional support requirements are included in the care planning process for patients. 4.8 Additional clusters may be added in future iterations but this will be subject to local clinical judgement.
Pre-determined Inclusion Criteria Locally Determined Exclusion Criteria
Contacts in last 12 months
Cluster CPA Status
Medication Last admission Clinical Issues
Current medication/other therapy
Risk History
Social Care Issues
<2
1, 2, 3, 11, 18
Non CPA
Lithium, depot
<6 months

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
7
4.9 Patient choice is paramount in relation to referral into the LES. An eligible patient may decline a referral to the LES without prejudice to ongoing/future treatment. 5. Process for Entry on to the LES 5.1 Where a patient is being discharged from secondary care mental health services, East London NHS Foundation Trust will arrange for the discharge of the patient in line with the discharge protocol. Eligibility will be determined by the individuals own set of personal circumstances and will be made by a multi-disciplinary team consisting of the GP, consultant psychiatrist and the mental health liaison nurse. The mental health liaison nurse will prepare a care plan for the patient that outlines the enhanced support they will receive through the LES. 5.2 Where a patient has an established diagnosis of a serious mental illness which is being managed in primary care and they are not in receipt of any secondary care mental health services, the mental health liaison nurse will provide a collaborative assessment prior to entry on to the LES and prepare a care plan that outlines the enhanced support they will receive through the LES. 5.3 New patients registering with practices with a currently stable long-term mental health problem should be referred to the appropriate ELFT service via the agreed care pathway (currently the CMHT). Patients newly registering with Primary Care services will not be accepted directly onto the SMI LES as they will need a period of stability to be established with local CMHT services. This period of assessment will include the patient being allocated a PbR cluster. 5.4 Where there are differing clinical opinions not mediated by patient choice, or clinical collaboration, then the CCG medical director will support the resolution process. 6. Enhanced support for patients who are managed by primary care 6.1 All patients who are managed by primary care and are receiving support via the LES will have in place a care plan developed by the mental health liaison worker in partnership with the practice, which details the enhanced support the patient will receive through the LES. The care plan will focus on mental and physical health and well-being and healthy living. 6.2 The GP, alongside the mental health liaison worker as appropriate, will conduct a comprehensive annual mental health review for all patients under the LES. This is an extra review above the annual QoF requirement. The review will include:
• Mental state examination • Review of medication • Assessment of side-effects of medication e.g. Glasgow Anti-psychotic Side Effects
Scale • Assessment of physical health • Brief assessment of social circumstances • Develop an enhanced care plan to include consideration of what to do in a
crisis/relapse and promotion of healthy lifestyles. 6.3 The practice will conduct an annual physical health check for all patients under the LES. This physical health check will mirror the current QoF indicators, and will be an extra physical health check in addition to the annual QoF requirement, targeting areas of need for each particular patient as above.

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
8
6.4 The participating practice takes on responsibility for Lithium medication, administering depot medication, other antipsychotic, anti-depressant, and mood stabilising medication and associated relevant medication for specified patients agreed with secondary care on a case-by-case basis. Patients on Depot medication will receive their injections from the practice nurse at the GP surgery (or other primary care location where practices federate or have interpractice referrals to manage depot medication). 6.5 Practice staff will complete 6 monthly side effects monitoring using the Glasgow Anti-psychotic Side Effects Scale. There will be a formal practice policy around patients missing their depot. 6.6 Patients on the LES will receive additional support from the mental health liaison worker, including as specified above. The Liaison Worker will ensure feedback from practice staff is incorporated into the clinical review and will feedback any clinical updates/information from the review to practice staff. 6.7 The mental health liaison worker will help the practice develop and implement robust follow-up protocols for patients who DNA meetings. This will possibly necessitate domiciliary visits which should be conducted in accordance with Provider and Practice polices around Lone Working/Domiciliary Visits and will also include formal communication arrangements with the prescribing G.P. and relevant practice nurse/staff. 6.8 In any eventuality if the patient DNA’s two consecutive clinical reviews this will trigger a formal meeting involving the prescribing G.P., the mental health liaison worker and the practice nurse/staff, to be arranged/coordinated by the mental health liaison worker. 6.9 Relevant read codes are detailed in Appendix One (these codes are contained within the CEG SMI template). 7. Patients who are managed by secondary care mental health services 7.1 The practice will conduct an annual physical health check for all patients under the LES. This physical health check will mirror the current QoF indicators, and will be an extra physical health check in addition to the annual QoF requirement. There may be some patients receiving the LES who are in receipt of a depot within Primary Care, but remain on CPA in secondary care. These patients are included in this LES where clinically agreed. 8. Discharge from SMI LES Into Primary Care GMS 8.1 Patients are expected to move between levels of care and ultimately step down to GMS where appropriate. Patients suitability for movement to GMS will be considered at each yearly review. 8.2 Patients will be discharged from the SMI LES into primary care GMS following a formal multi-disciplinary review with the prescribing GP, practice staff and the mental health liaison worker. This will normally be at the Annual Review point, and when:
• The patient’s condition is stable
• The patient is compliant and has been on one drug for six months or more
• No significant clinical, social, or risk management issues
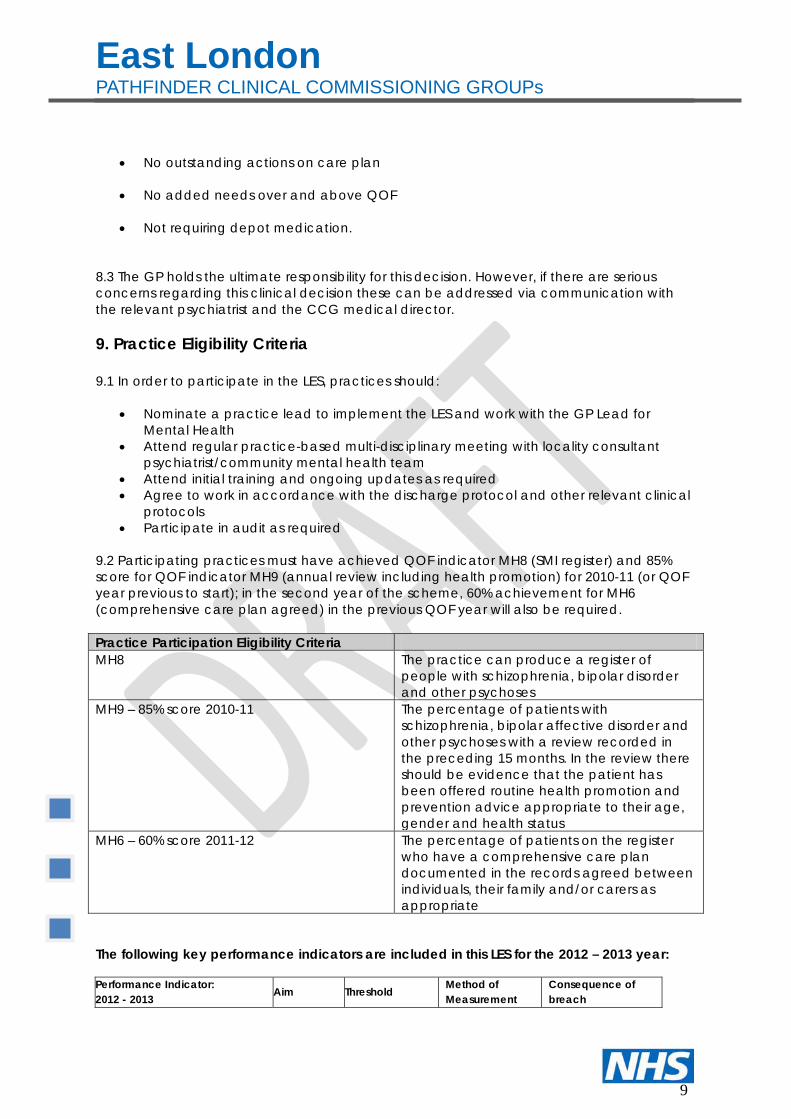
East London PATHFINDER CLINICAL COMMISSIONING GROUPs
9
• No outstanding actions on care plan
• No added needs over and above QOF
• Not requiring depot medication.
8.3 The GP holds the ultimate responsibility for this decision. However, if there are serious concerns regarding this clinical decision these can be addressed via communication with the relevant psychiatrist and the CCG medical director. 9. Practice Eligibility Criteria 9.1 In order to participate in the LES, practices should:
• Nominate a practice lead to implement the LES and work with the GP Lead for Mental Health
• Attend regular practice-based multi-disciplinary meeting with locality consultant psychiatrist/community mental health team
• Attend initial training and ongoing updates as required • Agree to work in accordance with the discharge protocol and other relevant clinical
protocols • Participate in audit as required
9.2 Participating practices must have achieved QOF indicator MH8 (SMI register) and 85% score for QOF indicator MH9 (annual review including health promotion) for 2010-11 (or QOF year previous to start); in the second year of the scheme, 60% achievement for MH6 (comprehensive care plan agreed) in the previous QOF year will also be required. Practice Participation Eligibility Criteria MH8 The practice can produce a register of
people with schizophrenia, bipolar disorder and other psychoses
MH9 – 85% score 2010-11 The percentage of patients with schizophrenia, bipolar affective disorder and other psychoses with a review recorded in the preceding 15 months. In the review there should be evidence that the patient has been offered routine health promotion and prevention advice appropriate to their age, gender and health status
MH6 – 60% score 2011-12 The percentage of patients on the register who have a comprehensive care plan documented in the records agreed between individuals, their family and/or carers as appropriate
The following key performance indicators are included in this LES for the 2012 – 2013 year: Performance Indicator: 2012 - 2013 Aim Threshold Method of
Measurement Consequence of breach

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
10
1> The GP practice has a named health professional responsible for mental health who provides leadership to practice participation in this LES
100% 100%
Practice self report – for inclusion on LES sign-up form
Non participation in the LES
2> GPs complete Mental Health template on EMIS to record data
NA NA
CEG conducts EMIS WEB audit of READ codes against activity
Failure to complete mandatory (*asterisked) information on EMIS template will result in non-payment for the activity in question or payment claw-back in the case of post payment verification checks
3> The GP practice has a minuted meeting with its attached mental health liaison worker at least every two months. These meetings can be virtual or face2face.
100% 80%
Practice self reports quarterly to CSS on dates of their monthly meetings with the liaison worker attaching the (patient anonymised) copies of the minutes
CSS to monitor / collate. Non –receipt of this information risks non-payment for activity conducted under this LES.
Complete and accurate data should allow clear benchmarking and effective monitoring of quality, safety and inequalities.

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
11
10 Payment schedule
LOCAL ENHANCED SERVICE
PAYMENT MONITORING
SMI patients discharged into primary care not on depot. This pays for the second of the bi-annual clinical reviews conducted by the practice for SMI patients (the first review is covered under QOF payments).
£75 per year per patient on enhanced list
Comprehensive care plan review including holistic health review – 2 per annum by Liaison Nurse, PN and GP. Practice attendance at training
SMI patients discharged into primary and on a depot. This payment includes the second bi-annual clinical reviews conducted by the practice for SMI patients (the first review is covered under QOF payments).
£70 per quarter (i.e. £280 per year)
Lithium – 3 monthly blood monitoring. Depot or other antipsychotic medication – 6 monthly GASS. Comprehensive care plan reviews
Initial year 1 payment for SMI register data matching with ELFT.
£250.00
SMI Register audit completed
SMI patients currently in primary care and currently on depottion. This payment replaces the previous payments for depot LES from April 2012.
£70 per quarter (i.e. £280 per year)
Lithium – 3 monthly blood monitoring. Depot oother antipsychotic medication – 6 monthly GASS. Practice attendance at training Comprehensive Care Plan Review (including 2 clinical reviews pa)

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
12
10.1 Practices will receive an Initial Service Payment on signing up to the Local Enhanced Service. This initial payment per practice is to facilitate the data matching and cleansing of SMI registers to ensure patients requiring further MH support are audited and documented. Thereafter payment will be 6 monthly in arrears. Payment Payable Amount Conditions
Initial Service Payment
SMI Register data matching with ELFT. 232 patients have been identified for discharge with varying degrees of support needs.
£250 Submission of: • signed Service Agreement • identified Practice Lead • list of all practice staff providing
the service. • Summary of SMI patients
currently: i) Receiving secondary care ii) Receiving primary care only
Q2 Service Payment
Quarter 2 £TBD Submission of: • Completion of Mental Health
template on EMIS to record data
• evidence of all patients receiving depot medication in the practice
• Evidence of all patients on enhanced care plan
• summary of liaison arrangements including evidence of three monthly liaison meetings and quarterly consultant-led sessions
• written policies and protocols • evidence of a list of patients
receiving the service • record of risk assessment
undertaken • participation in training of all
staff delivering service.

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
13
Q4 Service Payment
Quarter 4 £TBD
Submission of: • audit detailing depot date
injection administered and NHS No of patient
• audit detailing date of review and NHS No of patient
• evidence of bi monthly liaison meetings
9 Whom to contact:
• City and Hackney GP Clinical lead: Dr Rhiannon England • City and Hackney GP Clinical Lead: Dr Rhiannon England • LMC Clinical Lead PENDING • CCG/CSS Management Lead David Maher • CSS Performance Monitoring Patrick Schrijnen • CEG data collection Lead: Luis Rivas • For Clinical Governance CCG/ CSS TBC
10 Appendices: Appendix 1: CEG MH Template Appendix 2: Mental Health Liaison Function Service Specification

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
14
APPENDIX 1
GP Contract Mental Health Template Guide (N) The template includes coded data entry for all the quality indicators for severe long-term mental health problems required by the 2011 GMS GP contract. These are indicated in BOLD CAPITALS. We have included a number of other items which monitor good practice as outlined in the Fast-track Summary Guidelines for Severe Long-Term Mental Health Problems. The codes we recommend are (where the % sign refers to all daughter codes): Eu20% - for the concept of Schizophrenia Eu31% - for the concept of affective psychosis The register now includes all people with a diagnosis of schizophrenia, bipolar affective disorder and other psychoses. There is now a set of remission codes, which cancel the QOF requirements for that individual. Patients on Lithium will also be included in the register even if the diagnosis is not a major psychosis. However, these patients will only need to meet the two indicators related to Lithium control. Some patients will be stable on a lower than expected dose of Lithium, in this situation the code to use is 44W80. For 2011, the physical health check requires coding of a range of data items. Most of these have been in the SMI template since 2006. The new requirement is the Cholesterol/HDL ratio. In Tower Hamlets it is important to tick the TC/HDL box on the request. In other localities the ratio is automatically reported with a request for total cholesterol.
VERSION 8 – APR 2011

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
15
Prompt Code What does this prompt mean
When prompted for a date ensure the correct date is entered, as pressing “return” will default to today’s date SMI Checklist Protocol An explanation of what an ‘annual’ primary care
review for SMI should cover. SMI review done 6A6 This should be dated when you consider the items
listed in the SMI checklist above have been fulfilled. Mental Health Care Plan
8CR7 Enter ‘y’ when care plan is recorded. (If patient is treated under CPA it is acceptable to enter ‘y’)
SCHIZOPHRENIA IN REMISSION
E1005 Yes / No prompt
BIPOLAR DISORDER IN REMISSION
E1176 Yes / No prompt
MAJOR DEPRESSION WITH PSYCHOSIS IN REMISSION
Eu32A Yes / No prompt
Exception info Protocol An explanation of whole register exclusion criteria for “informed dissent” and “patient unsuitable”
EXCEPTION REASON 9h9 A picking list: Pt unsuitable (9h91) Informed dissent (9h92)
On lithium 6657 If ‘y’ then lithium sub-template is activated. (Patients on lithium will be identified through a drug search).
Sub template Start of lithium sub-template Monitored by 6657-1 A picking list:
Lithium monitoring by GP (EMISQLI1) Lithium monitoring by CMHT (EMISQLI2)
Lithium level 44W8 Value Serum Creatinine 44J3 Value Serum TSH level 442W Value Calcium level 44IC Value for corrected serum calcium level Stopped lithium 665B Enter date for when lithium stopped End of lithium sub-template On depot drug? 6656 On regular depot psychotropic injection. Text box
enables further detail Depot monitor by EMISQNE1 A picking list:
Depot monitoring by CMHT (665G) Depot monitoring by Outpatient clinic (EMISQOU1)
Depot monitored by GP
665H Yes / no prompt
Injectable neuroleptic given
665E Yes / no prompt Text line for batch no./exp/site
DNA Depot Appointment
9N4N Yes / no prompt Enter if does not attend for depot injection

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
16
Neuroleptic medication due
665D Diary entry Enter date next depot injection due
FULL MED. REVIEW
8B3V A picking list: Medication review (8B314) Medication review with patient (8B3x) Medication review done (8B3V) Consider all medications, the dose, compliance, side effects, interactions. There is a free text line for comments.
Drug user 13c Followed by a free text line to describe type of drug used
Health Ed. - drugs 679A Health education on drugs of addiction Alcohol intake 136 How many units of alcohol per week are consumed Alcohol advice 8CAM Health education on alcohol Audit C questions Protocol 3 Links to AUDIT C questions. Audit C Score 38D4 Enters a value. SMOKING STATUS Subtemplate This brings up a picking list of smoking options coded
under 137 Chews Tobacco 137W Yes / No prompt STOPPED SMOKING 137K Enter date patient stopped smoking, not today’s date CESSATION READINESS
137b Picking List:: Ready to stop smoking(137b) Thinking about stopping smoking (137c) Not interested in stopping smoking (137d)
SMOKINGADV (LVA) 6791 Brief stop smoking advice given CESSATIONADV (LVB) 8CAL Advice given by level two stop smoking advisor REFERCLINIC (LVC) 8HTK Referred to stop smoking clinic ON NRT 8B2B Has been prescribed NRT SYSTOLIC BP 2469 Value DIASTOLIC BP 246A Value O/E HEIGHT 229 Value for height: required to calculate BMI O/E WEIGHT 22A Value for weight: required to calculate BMI. (Weight
gain side effect of antipsychotics). BODY MASS INDEX 22K Calculated by EMIS automatically SERUM CHOLESTEROL/HDL RATIO
44lF Value
DIABETES SCREEN 6872 Yes / No prompt A picking list 44g Plasma glucose level 44f (Newham only) 44g1 Fasting glucose level 44f1 (Newham only)
QRISK 10yr CVD Risk 38DF Calculates the risk of developing CVD in the next 10 years.
CERVICAL SMEAR RESULT
4K2 A picking list of options
Suicide risk tool Protocol Links to information screen on suicide risk assessment Suicide risk Info Info It is important to indicate that an assessment of
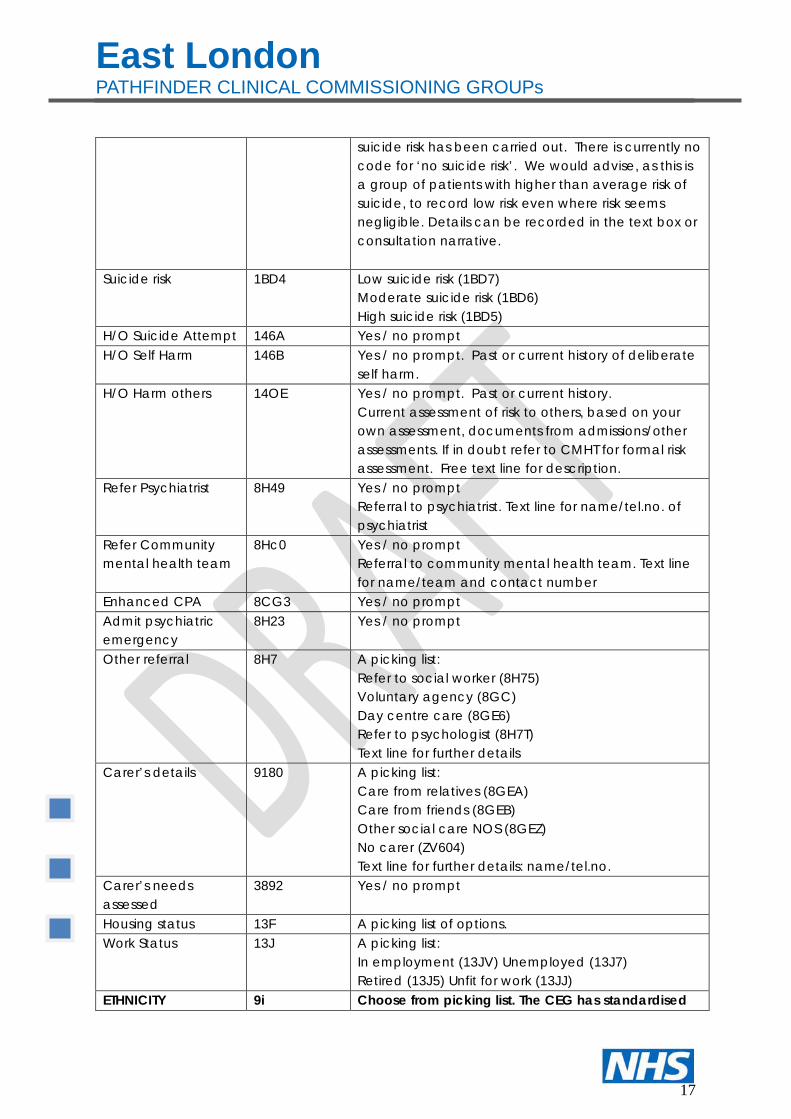
East London PATHFINDER CLINICAL COMMISSIONING GROUPs
17
suicide risk has been carried out. There is currently no code for ‘no suicide risk’. We would advise, as this is a group of patients with higher than average risk of suicide, to record low risk even where risk seems negligible. Details can be recorded in the text box or consultation narrative.
Suicide risk 1BD4 Low suicide risk (1BD7) Moderate suicide risk (1BD6) High suicide risk (1BD5)
H/O Suicide Attempt 146A Yes / no prompt H/O Self Harm 146B Yes / no prompt. Past or current history of deliberate
self harm. H/O Harm others 14OE Yes / no prompt. Past or current history.
Current assessment of risk to others, based on your own assessment, documents from admissions/other assessments. If in doubt refer to CMHT for formal risk assessment. Free text line for description.
Refer Psychiatrist 8H49 Yes / no prompt Referral to psychiatrist. Text line for name/tel.no. of psychiatrist
Refer Community mental health team
8Hc0 Yes / no prompt Referral to community mental health team. Text line for name/team and contact number
Enhanced CPA 8CG3 Yes / no prompt Admit psychiatric emergency
8H23 Yes / no prompt
Other referral 8H7 A picking list: Refer to social worker (8H75) Voluntary agency (8GC) Day centre care (8GE6) Refer to psychologist (8H7T) Text line for further details
Carer’s details 9180 A picking list: Care from relatives (8GEA) Care from friends (8GEB) Other social care NOS (8GEZ) No carer (ZV604) Text line for further details: name/tel.no.
Carer’s needs assessed
3892 Yes / no prompt
Housing status 13F A picking list of options. Work Status 13J A picking list:
In employment (13JV) Unemployed (13J7) Retired (13J5) Unfit for work (13JJ)
ETHNICITY 9i Choose from picking list. The CEG has standardised

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
18
the ethnicity codes on 9i 2001 census codes. Language 13l A picking list of main spoken language
Text box for entering in language if person speaks more than one language
Interpreter need? 9NU A picking list of interpreter needed for different languages. If language is not listed enter “interpreter needed “and free text the language required.
Interpreter present 9NQ A picking list: Interpreter present (9NQ0) Interpreter absent (9NQ1) Telephone interpreter (9NQ3) Family member interpreter (EMISNQFA8) Practice member interpreter (EMISNQPR13)
DNA MH review 9N4t Yes / no prompt Next review
6A6 Review date: this could be an annual review date, or a more frequent review linked to providing prescriptions.

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
19
Protocols Information on Protocol SMI Checklist
SMI checklist GP checklist covers the following:
• Assessment of current mental state • Review medication – consider dose, side effects, compliance • Review physical health • Review contact with mental health services
Check family and social situation including benefits Exception Reporting
Whole Register Exclusion Criteria 1. “Informed dissent” means that a patient does not agree to
investigation or treatment, and this is recorded in their medical records.
2. “Patient Unsuitable“ means it is not appropriate to review the chronic disease parameters due to particular circumstances, e.g. terminal illness or other supervening condition, or extreme frailty.
AUDIT C questions
The 3 AUDIT C questions are: Q1. How often did you have a drink containing alcohol in the past year? Never 0 pts Monthly or less 1 pts 2 or 4 times a month 2pts 2 to 3 times a week 3 pts 4 or more times a wk 4 pts Q2. How many did you have on a typical day when you were drinking in the past yr? 1 or 2 0 pts 3 or 4 1 pts 5 or 6 2 pts 7 to 9 3 pts 10 or more 4 pts Q3. How often did you have 6 or more drinks on one occasion in the past year? Never 0 pts Less than monthly 1 pts Monthly 2 pts Weekly 3 pts Daily or almost daily 4 pts Add up score

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
20
Drinking within limits: Men 0-4, women 0-3 Risky: men 5-7, women 4-7 Harmful: men and women 8+ A +ve score for males is 5 or more. A +ve score for females is 4 or more.
Suicide risk tool
Grade of risk: Is life not worth living? Have you thought how you might harm yourself/ *IF No: Currently low risk Active thoughts of self harm? Made plans to end your life? Might you act on these plans? *IF NO: Medium risk, assess, consider referral Made plans & proposed to act on them? Voices telling you to self harm? *IF YES: High risk, consider urgent referral

East London PATHFINDER CLINICAL COMMISSIONING GROUPs
21
Control page Clinical domain Mental Health v8 LV version File name Code they hang on What is this about? SMINT8.DAT CHRSPSE6 Main template EXREPPROT.DAT PROExcCHRSP157 Exception reporting ETHNIC.DAT 9i Ethnicity subtemplate AUDITCPROT.DAT PROCalCHRSP153 AUDIT C questions SMIPROT.DAT PROGP CHRSP95 SMI check list SUIPROT.DAT PRORisCHRSP143 Suicide risk questions LITHIUM.DAT PROlitCHRSP129 Lithiium subtemplate SMOKING.DAT 137 Smoking subtemplate PCS version Mental_Health_1st_page_CEG Audit_C_info_CEG Exception_info_CEG Smoking_status_CEG Suicide_risk_assessment_CEG Mental_Health_2nd_page_CEG Weight_BMI_CEG Lithium_CEG SMI_review_CEG Ethnicity_CEG Lifestyle_CEG Social_Details_CEG Cervical_Smear_CEG Changes since last review
• Deleted: o 6A60 = MH follow up o 8CG4 = standard CPA
• Added:
o 44lF = serum cholesterol/HDL ratio o E1005=Schizophrenia in remission o E1176=Unspecified Bipolar Disorder in full remission o Eu32A=Recurrent major depressive episodes, severe ,with psychosis, psychosis
in full remission
• Made unbold: MH review DNA

APPENDIX 2: Interface Protocols
FINAL: 29th March 2012
Agreement for the effective management of mental health patients across secondary and primary care interface in East London and the City
Purpose
This document contains the agreements for the effective management of mental health patients who will receive care and treatment that involves the transitioning of clinical responsibility across primary and secondary care interfaces and where there is shared care.
The document sets out roles, responsibilities and tasks of primary care, secondary care and the primary care mental health liaison function. It also sets out what to do when practice departs from this agreement, including dispute resolution.
The objectives of the protocols are to ensure patient safety and reduce risk and to ensure that the best care and treatment is provided in the most appropriate setting.
These are to be read in conjunction with the Primary Care Mental Health Liaison Function specification for services, where the composition, role and functions are described.
Description of services at the interface
Primary care
General medical services
LES / NIS - SMI
Secondary Care
CMHTsCrisis Teams
Early InterventionA&E Liaison
Hospital LiaisonInpatient services
Older peoples servicesAddiction services misuse
Personality disorder services
Primary Care Liaison
FunctionCPNs
employed by secondary
care, working in primary care

A full set of roles and functions exist which are not the preserve of this document. This protocol is concerned with the management of interfaces.
Description of interfaces
Key points to note:
There is a distinction between pathways and interfaces. These protocols describe interfaces between tiers of care (i.e. primary and secondary care) and not those between individual secondary care teams and primary care.
The community psychiatric nurses, with input from consultant psychiatrist, provide a liaison function and are not a discrete service. As such they do not create another interface but rather help to manage an interface.

Secondary care Primary care Liaison Function Patient as partners in care (known as co-production) Principle The entire process of assessment, care planning, reviewing plans and progress and transfer between levels of service must be done in partnership with the patient. The care programme approach (CPA) in secondary care provides the context for this. Develop all care plans based on assessments or reviews that have been developed through co-production with the patient. The content of plans, the pace of progress and the record of the extent to which plans have been delivered should be arrived at with patient. This co-production should be validated by signatures on care plans. Patient should be receive copies or have access to copies of plans, records of reviews of correspondence about their treatment and care
Develop all plans in partnership with patients and consider the possibility of patient held records, moving as close towards this as possible. Engage the primary care mental health liaison function to facilitate as much patient control and contribution as possible.
Enable patients to have as much control as possible over their care and treatment by: • Working as equal partners • Providing patients with information to enable
informed decision making • Supporting the knowledge and confidence of
GPs and facilitating communication • Facilitating the involvement of advocates,
carers or friends where patients desire this.
Discuss plan for discharge with patient and agree risk management and support Seek agreement to the planned discharge and document this in patient records
Offer initial welcome meeting to patients to explain what is on offer either: • Within the LES / NIS • Within GMS Assure patients of GP’s knowledge of their medication, side effects and risks Assure patients that the key information is known (e.g. histories that are significant in mental illness e.g. abuse, domestic violence, torture)
For patients who are content with being discharged: discuss with patient either face to face or by phone any concerns that they might have regarding receiving the treatment and care in primary care. Discuss any concerns that they may have in relation to loss of statutory benefits or social support. For patients who exercise choice to remain in secondary care: undertake face to face meetings to assess the concerns of the patient and provide assurances. As a minimum: • Establish a plan jointly with the patient to
meet with a view to resolving concerns and

anxiety • Provide advice to the patient based on
research evidence as to why there are health and social advantages (e.g. in relation to stigma) in receiving treatment and care in primary care
• Take practical steps, including by referring on, to solve obstacles experienced by the patient
Communication, information and developing competence and confidence in primary care Consultant psychiatrists to be aligned to specific practices Ensure that contact numbers and best means of contact are available to all linked practices Provide quarterly practice based- consultation sessions to advise on treatment and prescribing Participate in joint assessments in primary care as required to provide specialist mental health expertise in patients consultations, assessments and reviews Contribute to educational programmes for general practices
Consult with the primary care liaison function regarding the need to additional capacity or knowledge and skills in working with specific patients
A primary objective of the liaison function is to upskill GPs and other primary care staff in working with people with mental health problems. Provide advice to GPs on conditions, diagnoses, treatment, symptoms and presentation Provide advice on prescribing, patient responses to medicines (e.g. depots), side effects Contact consultant psychiatrists and determine the nature of their involvement in specific cases in primary care arising from concerns or questions about:- • symptoms • medication Work with CCGs to devise knowledge and skill development for GPs, engaging consultant psychiatrists for specialised input when required
Assessment and care planning Conduct initial assessment and allocate patients to clusters. For clusters 1,2 18 engage the liaison
GPs to undertake assessments and reviews in line with QOF and LES / NIS.
Undertake assessment to assert potential to divert cluster 1, 2 & 18 patients from secondary to

function to assess suitability for immediate discharge to primary care using the agreed discharge protocol, taking account of clinical and other needs.
GPs to set up diary call and recall systems for patients being discharged under the SMI-DEPOT LES and to ensure physical health checks for all patient are undertaken biannually Reviews of care plans of all patients on the SMI register must be undertaken on a quarterly basis, with input from the primary care mental health liaison function.
primary care utilising knowledge of primary care to manage risk. The following will be taken into account in assessments:- • Level of risk to patient or others (including
safeguarding children) • Complexity of social needs • Stability of symptoms • Frequency of contacts • History of admissions • Pattern of compliance with medication • Potential benefit of talking therapies either
through IAPT or voluntary sector provision Facilitate the diversion of patients who meet agreed criteria, from clusters 1,2,3,11 & 18 from secondary care to primary care provision utilising IAPT or voluntary or community sector provision.
Consultant psychiatrists to be available to be consulted about assessments where the GP or liaison nurses conclude this is desirable because of: • Concerns held by the patient about primary
care’s competence to take them on • Knowledge that in that patient’s case
transitions are key triggers in anxiety and psychiatric breakdowns
• Specific issues in relation to medicines that suggest a transitional period as opposed to a discharge at a point in time
• Any other clinical judgment by the primary care liaison function and / or the GP that suggests this would be required
Undertake care planning with primary care liaison function, including consultant psychiatrist where requested and interrogate care plan Ensure that knowledge and competence is sufficiently robust to offer each patient good treatment and care • Utilise established criteria for entry into
different tiers of primary care and register patients in the LES / NIS
• QOF According to agreed criteria
Undertake care planning: within 1 month of receiving discharge summary or a following a decision by for a transfer between tiers of primary care. Establish a care plan with the patient and GP. The plan is to include:- • Plans to improve social functioning and
meaningful day time activities • Improvement in physical health and well
being • Re-enablement in life roles and the
maintenance or development of social relationships
• Carer / family / advocate involvement

• Prescribing dosages & medication monitoring (e.g. side effects medication)
• Risk management • Relapse prevention plan • Referral on to additional psychological or
social input • Frequency of review
Discharge of patients from secondary care Discharge pool Maintain a list of patients who fit the broad criteria for discharge in the Case Finding Tool. Data provided routinely to CCGs will be:- • By practice • Patient identifiable • By PbR cluster at assessment or last review
Verify information about the patients on the list pertaining to: • Biographical data • Address • Current treatment episode
Create a phased timetable of patient discharge within the discharge pool and with secondary care create a discharge list taking into account: • Patients’ clinical need • Risk • Capacity across GP practices(to inform
sequencing not pace) • Competence of GPs to accept patients at that
point, being mindful of patient profiles Discharge summaries Produce a discharge summary including information on: • Diagnosis • Presentation • Risk • Medicines including risks and side effects • Pattern of compliance medication • Nursing concerns • Physical health • Social needs and current provision • Carer involvement
Ensure that secondary care is aware of receiving address and fax number at practices Confirm receipt of discharge summaries within 3 working days and accept clinical responsibility Request that the primary care liaison function undertakes an assessment GPs to participate in the assessment process for patients being discharged from secondary to
Review discharge summaries and advise GPs of: • Any significant gaps in information • Key risks in relation to the patient or
medication • Early indication of a care plan that will be
required Where queries are raised or additional information is required from secondary care discuss this with then and obtain supplementary information within 3 working days.

• Key information in patient histories that are pertinent and contributory to mental health problems
Discharge summaries to sent by: • Surface mail • Fax Patients are not to be considered as having been transferred until after primary care has confirmed receipt of the discharge summary and any queries are resolved, where these are critical to the ability of GPs to proceed to take clinical responsibility. Patients will be advised that they have been discharged only after their primary care has accepted clinical responsibility. The discharge checklist at containing this information and other steps is found at Appendix 1.
primary care Make decision about entry into either LES/ NIS or GMS Add patients to the relevant regular call and recall systems according to the outcomes of their physical and mental health assessment (and where any other LTCs or health conditions have been identified into QOF registers if not already included)
Liaison Staff to proactively follow up patients who DNA any of their regular reviews booked with the practice or who DNA depot injections due.
Crisis management Provide a single point of entry, which may be unique to each practice but which is reliable, which serves the standard mechanism for referring patients in a crisis Provide a same day response where patients who require re-escalation to secondary care
Ensure that each practice is clear about the single point of access to secondary care Use existing knowledge of systems or professional relationships with secondary care, to expedite rapid responses in a crisis. Where these are unavailable use the single point of access to refer patients
Ensure that the number for the single point of access is clear to all practices to which it relates Facilitate rapid referrals from primary to secondary care by producing drafts of information that will be critical and useful in secondary care determining the most appropriate response

Dispute resolution
Principles
The first step to resolving any disputes or conflicts which do not involve harm or the risk of serious harm is to speak directly with the professional involved.
Where this first step fails to resolve matters the clinical lead / supervisor should be advised of the problems and steps taken to resolve them. It is best practice to advise the professional involved that their clinical lead / supervisor is being contacted.
Where informal dialogue does not resolve matters the dispute should be escalated up managerial lines. The escalation route would be:
The manager of the individual or team involved
The manager one tier up until director level.
For practices, where GPs are subject to a dispute, once informal routes have been exhausted escalation should be to the CCG mental health lead.
Illustration 1
A GP has asked for a liaison nurse to follow up a patient who has not attended for depot injections. This request is not acted up. When challenged the nurse promises to follow up but again fails to do so. When challenged again, the nurse states that they have to make a judgement about use of their time and explained that they believe the GP’s request to be driven by anxiety.
Having tried to seek co-operation and reasonable engagement from the nurse the GP explained that they would contact the CMHT manager who has managerial responsibility for the nurse in question and raise an informal complaint. They did so by way of an initial telephone call to book a chance to speak through the incident and hear about the management action that would be taken.
Illustration 2
A GP sees a patient on oral medication who reports that she thinks she might be pregnant and has not been taking her medication for a few weeks. The doctor ends the consultation immediately and states that he would only have a consultation with a liaison nurse in the room. He advises the patient to wait until the nurse arrives. The liaison nurse is called saying there is an urgent situation

at the surgery that requires their attendance immediately. The nurse leaves a home visit (to follow u a depot DNA) and returns to the surgery. During the consultation the nurse was not asked to contribute and it became apparent that they were called back to provide support in case of an incident. This was the second time this had occurred and the last occasion resulted in a very difficult argument.
The nurse explained that she was going to contact the mental health lead in the GGG to raise concerns.
Near misses or serious incidents
Where serious incidents occur or where there are near misses reports must be filed, compliant with policies that govern risk and learning from incidents. Decisions about investigation and follow up will be taken under these policies. The agency with clinical responsibility at the time of the incident will be the lead in any investigation and reporting, were a joint approach is required due to the circumstances of the case.
Secondary Care Primary Care Liaison Function Invoke clinical governance policies in relation to near misses or incidents that meet the criteria
Practices to ensure that appropriate policies are in place for governing near misses and serious incidents Practices to invoke appropriate policies CCGs to receive notifications of all near missed and serious incidents.
Invoke clinical governance policy Co-ordinate an interagency review meeting, including senior representation to identify a plan for joint investigation and learning, in accordance with clinical governance policies
The CCG will maintain oversight of the investigation and reporting of findings from all serious incidents in accordance with their policies.
Transparency
Professionals should conform with the codes of practice of their registering bodies and ensure that communications are profession and open. Patients must be advised of all serious errors in relation to their care and treatment and of the steps taken to prevent a repeat of such incidents.

Secondary Care Discharge Checklist
Activity Date Notes 1. Plan for discharge developed and
discussed with patient
2. Plan for discharge discussed with primary care mental health liaison function
3. Liaison function confirmed that timing is appropriate given the clinical stability of patient, social and psychological needs, capacity in receiving services (e.g. IAPT) of general practice
4. Discharge summary produced, including information on: • Diagnosis • Cluster • Mental health presentation • Risk • Medicines including risks and side
effects • Date of last DEPOT given (where
relevant) • Pattern of compliance medication • Nursing concerns • Physical health • Social needs and current provision • Carer involvement • Key information in patient histories
that are pertinent and contributory to mental health problems
5. Discharge summary sent by: • Surface mail • Fax
6. Confirmation received from primary care that the summary is complete and that clinical responsibility is being accepted
7. Patient advised of discharge, including in writing


Annex to Community Mental Health Team Service Specification Primary Care Mental Health Liaison Function
Draft 1 23rd January 2012 Mental Health Commissioning Board 25th January 2012
Draft 2 29 January 2012 Revision following Mental Health Commissioning Board
Draft 3 10th February 2012 Issued for internal discussion & feedback
Draft 4 24th February 2012 Mental Health Commissioning Board 28thFebruary 2012
Clinical Forum membership
Draft 5 2nd March 2012 Clinical Forum.
Draft 6 16th March 2012 Clinical Forum
FINAL DRAFT 29th March 2012

Annex to Community Mental Health Team Service Specification Primary Care Mental Health Liaison Function
1. Population Needs
1.1 The national mental health strategy “No Health Without Mental Health” promotes
prevention and public health and whole system approaches. The provision of mental health care in primary care contributes to these aims.
1.2 The London Health Programme “Case for Change” and the “Models of Care” support a move towards more primary care provision for people with mental health who are not on the Care Programme Approach and who have mild to moderate symptoms including people with a serious mental illness but who are stable who do not need to receive the care and treatment in secondary care settings.
1.3 The Disability Rights Commission published research that shows that people with mental health problems die up to 20 years earlier than the rest of the population due to a range of physical conditions.
1.4 The East London and City Whole System Mental Health Review (May 2011) identified that there are some patients who meet the criteria for those who can be discharged from secondary care to primary care.
1.5 International and local evidence considered in the Whole System Review (WSR) indicates that these patients meet the criteria for transfer from secondary to primary care based on their right to receive the most appropriate care in the most appropriate context from the most appropriate professional, given their needs.
1.6 The criteria for transfer from secondary to primary care include patients who are: • Not on CPA (i.e. those on CPA have been excluded for consideration). • Identified in PBR clusters 1, 2 and 18 (mild to moderate common mental disorders and
low need cognitive impairment) can be discharged to primary care directly with the support of voluntary sector universal and other services as appropriate.
• In PBR clusters 3 and 11 (non-psychotic moderate, ongoing psychosis low symptoms) whose clinical and social circumstances justify this – most of these patients can be discharged into primary care with some support.
• A DNA (Did Not Attend) rate of 15% (ELFT wide average) is taken to account for the additional demand in contacts
1.7 The borough level data for those who meet the criteria for transfer are: • City and Hackney: • Newham: • Tower Hamlets:
2. Scope
2.1 Aims and objectives of service The primary care liaison function for adults of working age will facilitate and provide safety and high quality mental health treatment and care in primary care settings. The function will facilitate patient flows as follows:

• Step down from secondary to Service Mental Illness Local Enhanced Service (SMI LES)/ NIS
• Step down from secondary care to SMI Quality and Outcome Framework (QOF) • Step down from secondary care to General Medical Services • Step down from SMI LES to SMI QOF (or GMS where relevant) • Step up from SMI QOF to SMI LES
The primary care liaison function will create and maintain systems, structures and resource to enable effective management of mental health problems in primary care The objectives of the primary care liaison function are to:
• Enable the development of capacity, confidence and competence in relation to mental health treatment and care, in the primary care workforce through sharing knowledge and expertise
• Facilitate the engagement of partners in treatment and care from parties such as the service user, carers, social care, voluntary sector providers and universal services
• Facilitate the engagement of secondary care with the primary care workforce responsible for mental health, in particular ensuring the involvement of consultant psychiatrists in shared care
• Gather and provide information on the range of services that are available for people with mental health problems in the local community and facilitate referral to the appropriate services based on need
• Establish and maintain a model for each practice to have access to, as a minimum, a quarterly clinical consultation sessions for primary care staff led by a consultant psychiatrist from secondary care.
• Facilitate effective referral from primary care to secondary care consistent with operating interface agreements.
• Ensure the best clinical processes in the discharge of patients from secondary care to primary care
This service specification should be read in conjunction with the Interface Agreement [Annex 1] and the Operational Procedures for the primary care mental health liaison function, which set out clinical responsibilities of staff involved in the liaison function. 2.2 Service description/care pathway The staffing compliment of function will be decided by ELFT based on the following minimum requirements:
• Staff resources will be configured on a borough basis • Employment contracts and line management will enable the fulfilment of this
specification. Cover arrangement will be made to ensure that all practices have uninterrupted access to the primary care mental health liaison function during holidays and other absences
• The primary care mental health liaison function will operate during normal working hours. Arrangements will be in place in each borough to ensure access to services out of hours through the regular routes should this be required.
• The configuration and distribution of the borough liaison nurse resources across, though the managerial responsibility of ELFT will be decided through engagement and negotiation with CCGs.
• Sufficient Agenda for Change Band 6 Community Psychiatric Nurse resources will be provided as part of the staff compliment to ensure safety and skill levels to meet service needs
• Consultant psychiatrist time will be allocated to the primary care mental health liaison function, maintaining practice based relationships.

Accountability day-to-day for priority setting and direction will be to primary care. ELFT will ensure direct management of clinical governance or clarify the delegation of clinical governance responsibility to primary care through contractual frameworks that are operationally explicit and legally robust. These may include the provision of honorary contracts by practices to enable coverage by policies, such as information governance, thus allowing access to patient identifiable data. The primary care mental health liaison functions will be delivered according to patient flows. Using a stepped care approach. The flows are : Step down from secondary to Service Mental Illness Local Enhanced Service (SMI LES) Step down from secondary care to SMI Quality and Outcome Framework (QOF Step down from secondary care to General Medical Services Step down from SMI LES to SMI QOF Step down from SMI LES to GMS Step up from SMI QOF to SMI LES
The primary care liaison functions are:-
Consultative, Education and Advisory Role
• Develop capacity, confidence and competence of primary care by providing a
consultative function on specific cases and also in relation to specific topics as agreed in development programmes.
• Ensure that practise have access to, as a minimum, quarterly consultative sessions with practices to discuss both individual cases and clinically based questions of GPs
• Model best practice in working with patients with mental health problems within shared care to enable primary care to develop knowledge and skills in working with people with mental health problems
• Deliver components of a Development Curriculum to upskill primary care about managing mental health conditions, risk (including positive risk taking) and medications including side effects
• Provide training on the administration of depot medication • Share latest research, policy, guidelines and best practice models with GP practices • Facilitate the transfer of knowledge and help improve skills through co-working with
GPs • Provide information about social care provision such as the FACS criteria,
personalisation and individual budgets • Provide information on equalities and the interaction of identity and discrimination
with mental health problems
Secondary Care Diversion
Assess patients who have been referred to secondary with mild to moderate mental health problems, who will be mainly from cluster 1,2,3,11,and 18 and provide a

diversionary function back to primary care where clinical and social factors support such a decision Foster good relationships with IAPT services and other talking therapy services in the community or voluntary and community sector services such as befriending and support time and recovery workers. The liaison nurses will maintain up to date knowledge of issues and constraints to enable ease in referring so that patients’ needs may be met in the most appropriate and least stigmatising context. Involve GPs in the decision to divert and understanding the rationale for doing so, keeping good records of decisions. Offer sessions to GPs to speak though the rationale and pass on knowledge and confidence. Review patients diverted to the LES / NIS every three months and provide GPs with summaries of progress and any outstanding issues.
Transfer between different levels of primary care provision
• Produce summaries of care plans and risk assessments with GPs to support the entry or exit into functions such as the LES/NIS.
• The Consultant Psychiatrist contributing to the liaison function will provide advice to GPs on prescribing and management for patients leaving the LES / NIS into GMS.
• Provide detailed referrals and care plan summaries for patients being escalated within primary care to the LES/NIS.
Support functions for patients in primary care
• Proactively review patients quarterly for the first 3 quarters following discharge then review whether frequency may be decreased to six monthly reviews
• Factors taken into account when considering frequency will be:- • Clinical stability • Consistent and non-problematic medication • Confidence and competence of GP, to be agreed in discussion with the GP
• Increase monitoring at the request of GPs because of:- • Changes in symptoms or presentations • Medication lapses / DNAs • Absence of GP • Other factors that might have an impact of clinical outcomes
• Following up patients who DNA for depot • Ensure practise have access to, as a minimum, quarterly clinical consultation sessions
for primary care staff, based in practices led by the named consultant psychiatrist. • Deliver shared care with GP, with GPs retaining clinical responsibility and the liaison
function providing expertise Information Management • Review EMIS with GPs to ensure that all fields required are available and fit for
purpose • Ensure all consultations and patient contact is recorded on GP IT systems (EMIS LV/
PCS and INPS) for a consistent and continuous record of patient care and all interventions and with the assistance of the practice implementing call and recall systems according to each patient’s need
• Ensure the SMI-DEPOT LES template is used to record physical and mental health checks and interventions for all patients on the practice SMI register and for all patients discharged from ELFT
• Monitor case notes and ensure they are up to date across EMIS and INPS management systems in GP practices.
• Ensure with the assistance of the practice that each patient’s prescribing records are current and updated from any care plans provided on discharge from ELFT
• Maintain a patient registration and tracking system maintained for the liaison function

to ensure data is available to supports functions such as reviews • Support GPs in maintaining information about satisfaction and other quality assurance
metrics which will be reported quarterly to assess the impact of the transfer of patients from secondary to primary care.
•
Mental health, psychological and social provision including social care The primary care mental health liaison function will use its expertise in holistic mental health provision to ensure that services and potential partners in supporting recovery are engaged and able to contribute to treatment and care. The primary care mental health function will:-
• Review and advise upon care plans to ensure where required, that referrals are made for social care and housing provision
• Make referrals under the safeguarding adult procedures where criteria are met • Make referrals to voluntary and community provision pursuant of the recovery
approach, including advice about state benefits • Co-ordinate a minimum of annual reviews of mental health plans and provision which
include patients and where appropriate, carers The function will play a central role in ensuring that the provision of services to people with mental health problems in primary care are safe, clinically sound and part of a system, which includes specialist mental health services as well as universal community based services and support. To ensure knowledge transfer to primary care and to routinise support and interventions to support primary care, the function will:-
• Create a database of community, psychological, self help and social care provision that will aid recovery and ensure its availability to primary care
• Ensure that arrangements are in place out of hours for primary care to have access to specialist mental health advice.
• Ensure that all contact numbers for advice and out of hours provision are up to date and available to primary care
• Ensure that referral pathways out of hours are clear and effectively functioning, by reviewing these with partners including local authority emergency duty systems
• Ensure the availability and review of interface protocols between secondary and primary care
• Be responsible for reviewing breaches, escalation and arranging resolution of disputes consistent with existing interface protocols
• Organise quarterly face to face consultant psychiatrist led clinical review meetings for primary care staff
• Identify the most efficient systems for transfer of information such as discharge protocols as required for each practice to ensure safe and secure discharges and referrals
• Ensure the availability of positive practice information in the formats and mediums best meeting primary care practices needs
Discharge from secondary to primary care • Determine the appropriateness of referrals from secondary to primary care according
to local protocols. • Co-ordinate the transfer process. • Receive discharge summaries and ensure that information includes a brief overview of
the condition and more detailed information on the treatment being transferred for which each partner has managerial and clinical responsibility on prescribing, medical and nursing issues and social factors.
• Undertake assessments to ensure that patients meet the agreed criteria for discharge and acceptance in primary care
• Develop primary care mental health care plans that are recovery focused and promote

well-being and social inclusion • Include support for improved physical health as part of care plans in primary care • Collate risk assessments and work with GPs to agree medication management plan. • Where psychotropics are used it should identify the product's licensed indications,
therapeutic classification, dose, route of administration and duration of treatment, adverse effects (their identification, management, importance and incidence), monitoring requirements and responsibilities, clinically relevant drug interactions and their management, storage and reconstitution of product, peer-reviewed references for product use, and contacts for more detailed information.
• Monitor side effects of medication and report to GPs. • Ensure primary care’s access to patient records held by secondary care • Meet with patients who are concerned about being discharged to primary care and
reassure them about benefits of being treated in the most appropriate setting by the most appropriate professional given their needs. Establish a timetable for discharge with the consultant psychiatrist and the patient
• Co-ordinate transfer of patient to GP care including Information Governance authorisation from patient.
• Enable development of rapport between the patient, any carer, secondary care and the GP.
The detailed operational policy for delivery of the primary care mental health liaison function will be developed by ELFT, achieving negotiated agreement with the CCGs. 2.3 Population covered 2.4 Any acceptance and exclusion criteria The primary care mental health liaison function across ELC will accept: Patients in PbR clusters 1, 2 and 18 discharged from secondary care to general medical services Patients in PbR clusters 3 and 11 discharged into the Local enhanced services / network improvement service Patients on the practice SME register Adults of working age Older adults Exclusions Patients with severe mental health problems and complex needs Patient experiencing a crisis Patients admitted to psychiatric hospital in the last six months Children and adolescents 2.5 Interdependencies with other services The primary care mental health liaison function will operate at interfaces and therefore interdependencies arise. These need to be well managed if the system is to operate effectively. The primary care mental health liaison function will need community mental health teams (CMHTS) to comply with discharge protocols Consultant psychiatrist input into primary care within a shared care model is required, with clarity that clinical responsibility is retained by GPs Information sharing and collaboration will be required with services out of hours such as the A&E Liaison service, which will be the source of mental health expertise out of hours, along with the AMHP service provided by the local authority. The LES and GMS will need to manage capacity so that patients can be accepted following assessments supported by the primary care liaison function
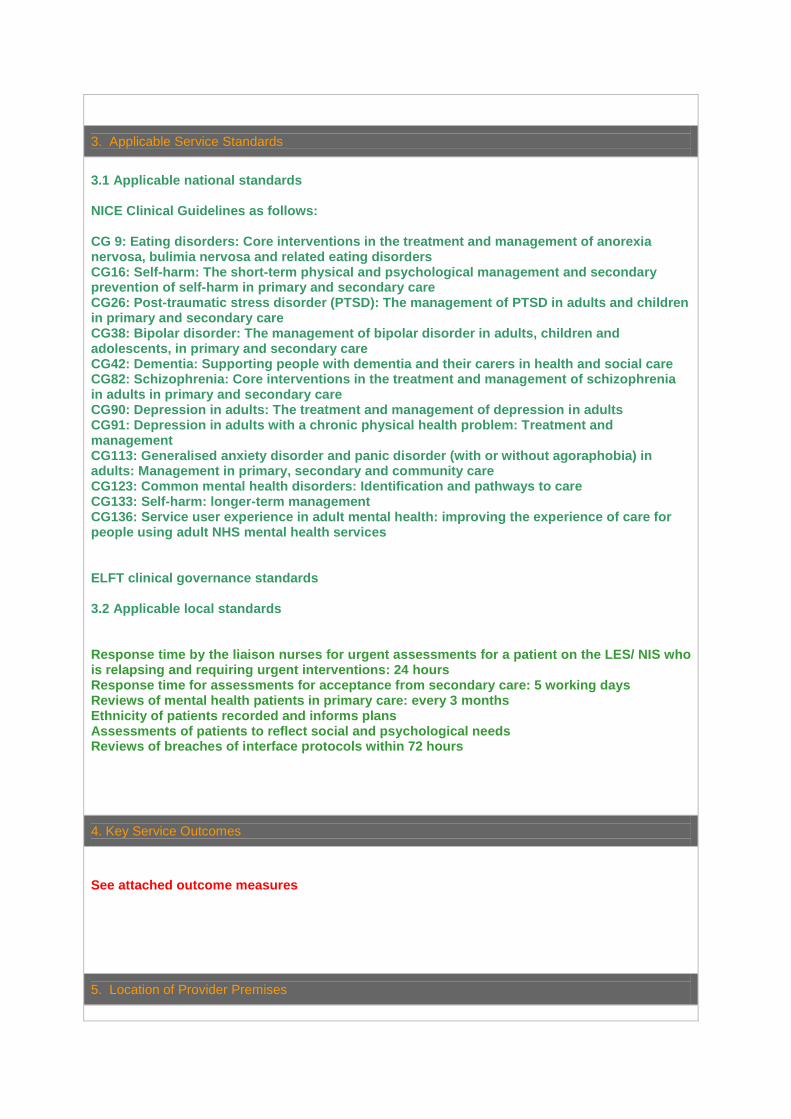
3. Applicable Service Standards
3.1 Applicable national standards NICE Clinical Guidelines as follows: CG 9: Eating disorders: Core interventions in the treatment and management of anorexia nervosa, bulimia nervosa and related eating disorders CG16: Self-harm: The short-term physical and psychological management and secondary prevention of self-harm in primary and secondary care CG26: Post-traumatic stress disorder (PTSD): The management of PTSD in adults and children in primary and secondary care CG38: Bipolar disorder: The management of bipolar disorder in adults, children and adolescents, in primary and secondary care CG42: Dementia: Supporting people with dementia and their carers in health and social care CG82: Schizophrenia: Core interventions in the treatment and management of schizophrenia in adults in primary and secondary care CG90: Depression in adults: The treatment and management of depression in adults CG91: Depression in adults with a chronic physical health problem: Treatment and management CG113: Generalised anxiety disorder and panic disorder (with or without agoraphobia) in adults: Management in primary, secondary and community care CG123: Common mental health disorders: Identification and pathways to care CG133: Self-harm: longer-term management CG136: Service user experience in adult mental health: improving the experience of care for people using adult NHS mental health services ELFT clinical governance standards 3.2 Applicable local standards Response time by the liaison nurses for urgent assessments for a patient on the LES/ NIS who is relapsing and requiring urgent interventions: 24 hours Response time for assessments for acceptance from secondary care: 5 working days Reviews of mental health patients in primary care: every 3 months Ethnicity of patients recorded and informs plans Assessments of patients to reflect social and psychological needs Reviews of breaches of interface protocols within 72 hours
4. Key Service Outcomes
See attached outcome measures
5. Location of Provider Premises

The Provider’s Premises are located at: ELFT will negotiate with CCGs / cluster to agree the location of the primary care liaison function to meet the needs of primary care. The assumption if that the nurse roles within the primary care mental health liaison function will be based in practices, with networks and clusters making the decision about the practices in which these roles are located. [Name and address of the Provider’s Premises OR details of the Provider’s Premises OR state “Not Applicable”] 6. Individual Service User Placement
[Insert details including price where appropriate of Individual Service User Placement]

SECTION B PART 2 - ESSENTIAL SERVICES
[For local agreement]
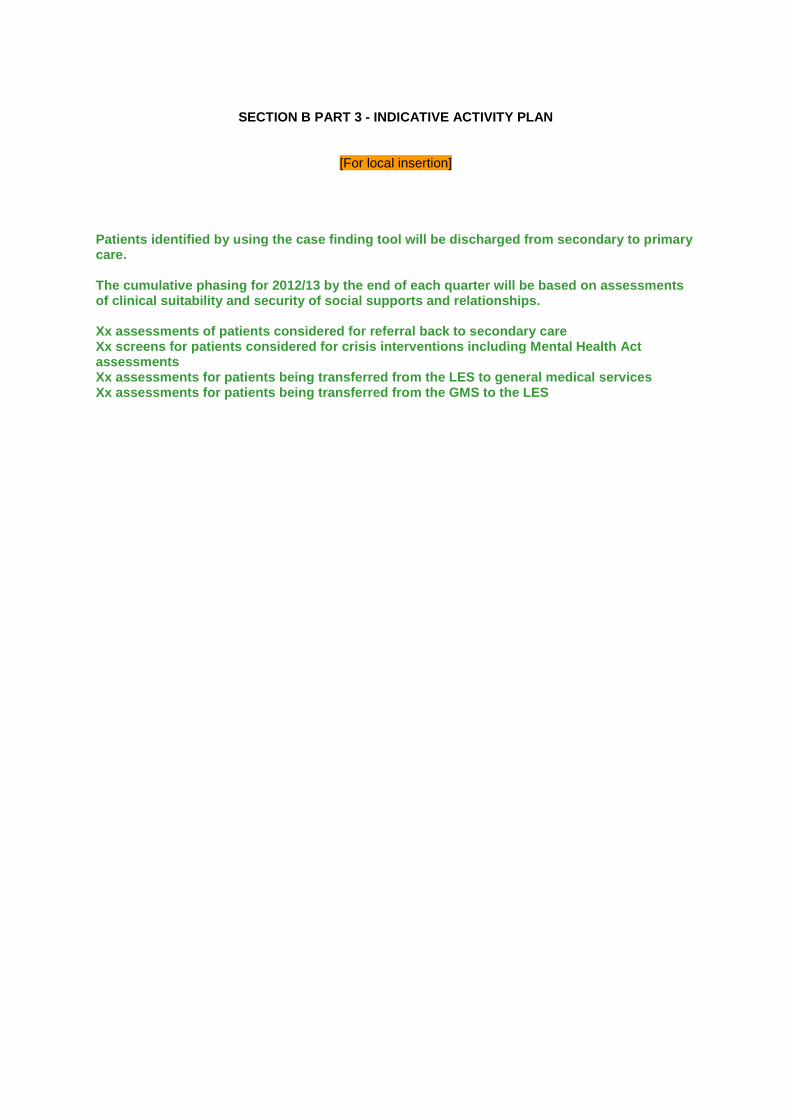
SECTION B PART 3 - INDICATIVE ACTIVITY PLAN
[For local insertion]
Patients identified by using the case finding tool will be discharged from secondary to primary care. The cumulative phasing for 2012/13 by the end of each quarter will be based on assessments of clinical suitability and security of social supports and relationships. Xx assessments of patients considered for referral back to secondary care Xx screens for patients considered for crisis interventions including Mental Health Act assessments Xx assessments for patients being transferred from the LES to general medical services Xx assessments for patients being transferred from the GMS to the LES

SECTION B PART 4 – ACTIVITY PLANNING ASSUMPTIONS
[Insert/append Activity Planning Assumptions]
The primary care liaison function will enable the development of confidence and competence in primary care so that patients can be discharged safely and with clinical stability. The development of confidence and competence will be an incremental process hence the phasing showing an accelerated rate of discharge / acceptance as the year progresses.

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 1 of 21 01 May 2012
Pre-consultation Business Case
North Hackney Primary Care: improving
access and walk in centre
decommissioning
Authors: Sarah Young & Nick Sodhi
Sponsor: Alice Benton
Version 2.3
1 May 2012
Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 2 of 21 01 May 2012
Contents
Page
A Introduction 1 Executive Summary 3
2 Introduction and Overview 4
3 Summary and recommendations from studies 6
4 Engagement feedback 9
5 Plans to consult 9
B The case for decommissioning the walk in centres
1 Market Analysis 10
2 Assessment of Benefits 12
3 Cost / Benefits Analysis 14
4 Options Appraisal 15
5 Key Assumptions and Dependencies 15
6 Risk and Sensitivity Analysis 16
C Conclusions and next steps
1 Timescales 18
2 Conclusions / Recommendations 18
Appendices
A Map 21
B Local strategic context 22
C Clinical Audit } Attached as
} separate
} documents
}
D Stakeholder feedback report
E Stakeholder consultation strategy and plan
F Equalities Impact Assessment (2 documents)
Version Date Author Reason
2.2 17 April Nick Sodhi Final amends
2.3 1 May Sarah Young NELC logo and formatting

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 3 of 21 01 May 2012
A. Introduction
1. Executive Summary
NHS ELC has been considering how to improve Hackney and the City‟s urgent care service including the role of in and out-of-hours GP services, walk-in centres, urgent care (specifically the Primary Urgent Care Centre at the Homerton), the London Ambulance Service and Accident and Emergency. By urgent care we mean: “The range of responses that health and social care services provide to people who require (or perceive the need for) urgent advice, care, treatment or diagnosis” - Direction of Travel for Urgent Care, Department of Health” Four workstreams form the City and Hackney draft Urgent Care Strategy would be integrated within the context of the 111 "phone before you go" pilot in 2012: 1) Review of walk in centres in the north of Hackney; 2) Primary Care improving access and demand management across Hackney; 3) Strengthening out of hours services and integrating with Urgent Care 4) Managing A&E and PUCC attendances, including admission avoidance at the Homerton Hospital. As part of the strategy, ELC is proposing to close walk-in services at Tollgate Lodge (Stamford Hill, N16) and Springfield Medical Centre (Oldhill Street, N16) in north east Hackney. ELC believes the current services are not properly meeting the health needs of local people and are proposing a number of alternative services to better meet the health requirements of the community.
The proposal, led by Direct Commissioning, for Primary Care access improvement aims to maximise the chances of all Hackney residents registering with a GP. This means up to 9,600 additional patients (projected maximum) could access primary urgent care services through their GP and have the associated benefits including "phone before you go" access, prevention and health check services and continuity of care. Patients who are unregistered or unsure would be able to access the new telephone number 111, going live in 2012. Combined, these proposals are expected to improve the health benefits of the population of Hackney and increase equity of access by releasing capacity and resources for improvements to primary care. We have undertaken four separate studies of walk activity to understand their use better: a. A clinical audit lead by clinicians to identify the clinical reasons for use and follow up b. A patient flow analysis to understand the patterns of use over a full year, over calendar
months and a typical week c. A patient survey to ascertain patients‟ reasons for using the walk in centres d. A series of stakeholder engagement meetings followed by an event in January to understand
patients‟ views on all proposals for improving urgent care services. The results of these, together with the financial and cost benefit analysis, are set out in this business case, which recommends a six-week period of public consultation, starting in May 2012 on the proposal to decommissioning both walk in centres.

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 4 of 21 01 May 2012
2. Introduction and Overview
This business case sets out the rationale for, and seeks approval of, the proposal to decommissioning walk in centre services at Tollgate Lodge Walk-in Centre and Springfield Medical Centre in north east Hackney. The business case sets out:
The financial case for closure of the walk in centre services which would require no or
minimal investment and would yield overall projected savings of £2,631,398 to March 2015
In line with the CSP, the realisation of £325,000 savings in 2012-13 by closing the walk in centres in Quarter 3
The case for Direct Commissioning identifying and reinvesting further savings into Primary Care capacity, which could create up to 9,600 (the projected maximum) additional registered patients at Springfield and Tollgate Lodge, or other services to be shaped by consultation and engagement.
The proposals deliver the vision and objectives of two key programmes for City and Hackney:
The Primary Care improving access and demand management programme - to enable both health centres to expand their GP registered lists and thereby create greater capacity for patient registration in the area
The Urgent Care Programme and 111 pilot - to enable greater emphasis on Primary Care First and „Phone before you go‟.
ELC Direct Commissioning are responsible for commissioning the walk centre contracts and the the proposals have been and will continue to be clinically lead. Accompanying the business case is a stakeholder communications strategy and equalities impact assessment. Note that consultation would be concluded in June 2012. The proposed approach is realistically scoped to ensure that the benefits and costs to deliver are in line with the expected benefits.
Context Walk in centres provide access to primary health care services for patients not registered with a GP or who are not in their local area. The two walk in centres in north east Hackney were set up as a result of two national programmes, as per the guidance of the previous administration:
Springfield Medical Centre was commissioned as part of the national programme for Equitable Access to Primary Medical Services and therefore meets the criteria of a GP Lead Health Centre. This was defined as opening hours of 8am to 8pm, 365 days per year; accessible for registered and unregistered patients; offering bookable and walk-in appointments; and operating as a GP-lead service.
Tollgate Lodge Walk-in Centre was commissioned ahead of this national programme under the previous government‟s administration, and operates 365 days a year, with daily open times from 8am-8pm, and from 10.00 on weekends and bank holidays. It also provides services to registered and unregistered patients through bookable and walk-in appointments. Tollgate is a nurse-lead service. Due to the circumstances in which they were commissioned, they are very close to each other –
two streets apart - as illustrated by the map on page at Appendix A.
City and Hackney
Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 5 of 21 01 May 2012
The proposals deliver the vision and objectives of four key strategies for Hackney and the City:
Urgent Care Improvement
Four workstreams form the draft Urgent Care Strategy for City and Hackney and would be integrated within the context of the 111 "phone before you go" pilot in 2012: 1) Review of walk in centres in the north of Hackney; 2) Primary Care improving access and demand management across Hackney; 3) Strengthening out of hours services and integrating with Urgent Care 4) Managing A&E and PUCC attendances at Homerton, including admission avoidance. The aims
and design principles of the Strategies are set out in Appendix B.
Primary Care improvement There are two strategies which are relevant to the delivery of Primary Care:
Care closer to home strategy
Bigger, Brighter, Better Strategy A „GP Choice‟ one year pilot will start in 2012 in The City and Hackney which will allow patients for the first time to choose whether to register with a practice close to their workplace or home.
Primary Care improving access and demand management programme Continuing to improve access to primary care is a key priority for quality improvement and a key workstream within the Urgent Care Strategy. This programme is to be delivered across Hackney in 2012-13, with a focus not only on increasing capacity in general practice, but also on Primary Care being the first and most appropriate point of access for patients with primary care needs.
Its objectives are set out in Appendix B.
Walk in usage Walk in centres show a consistent year on year increase in use - in 2010 approximately 23% of the population reported to have used a walk in centre (not specifically in Hackney) in the previous 12 months.
1
The two walk in centres in north Hackney had approximately 36,000 attendances last year (2011-12) and are forecast to increase in 2012-13. A patient attendance time analysis summarised all patient urgent care activity in 2010-11. From this, the WICs show similar weekday trends with both showing a slight peak in activity on the Monday and Wednesday followed by relatively steady performance until the weekend. Activity slows down on the weekend with both WICS showing a drop on the Saturday which continues through to Sunday for Tollgate. The analysis of weekday activity by hour shows that the WIC are particularly busy between 4pm and 8pm. The analysis of activity by hour on the weekend shows the service peak between 10am and 12pm.
The full results for the Walk in Centres are in the audit report at Appendix C.
1 City and Hackney Joint Strategic Needs Assessment, 2010 (Appendix B, Figure 8.2)
Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 6 of 21 01 May 2012
3. Summary and recommendations from studies Four separate studies of walk activity have been completed to understand their use better:
a. A clinical audit led by clinicians to identify the clinical reasons for use and follow up b. A patient flow analysis to understand the patterns of use over a full year, over calendar
months and a typical week c. A patient survey to ascertain patients‟ reasons for using the walk in centres d. A series of stakeholder engagement meetings, followed by an event in January led by
clinicians to understand patients‟ views on all proposals for improving urgent care services.
Clinical audit findings
A clinical audit, led by clinicians, was undertaken to understand why, when and by whom the walk in centres are used. Findings and recommendations are summarized below, the full report
is at Appendix C.
Clinical evidence: While perceived as urgent by patient, all but a minority of the walk in centre cases could have been appropriately managed by a competent nurse or nurse practitioner within a primary care setting and/or through community pharmacy. The majority of attendances were for minor injuries and ailments, with the most prevalent diagnoses being: 1) upper respiratory tract infections; 2) skin infections; 3) dressings and wounds; and 4) ear infections and wax – these 4 diagnoses made up 56% of the caseload in the audit. Of the remaining 44% of 422 cases, only 17 cases could be considered requiring urgent care: 7 cases referred to A&E and a further 7 cases related to abdominal pain, the only category which could warrant referral. Another factor considered was whether patients were seeking a second opinion – 13.5% of patients said they had received advice on a previous occasion for the presenting problem and, therefore, could require greater continuity of care than available at walk in.
Patient use: Around half of the patients in the audit were attending a walk in centre for the first time. 19% had attended once before and this declined consistently for those having visited 2-5 times previously. During the week there is a steady demand at both walk in centres with slight peaks on Mondays and Wednesdays. Both WICs are busy 4pm – 8pm, overlapping with the time when GP in hours ends. Activity slows down at the weekend with both WICs showing a drop on the Saturday which continues through to Sunday for Tollgate. Demand is high on Sundays at Springfield with a peak in demand from 10am-12noon. This peak is due to the Charedi Community recommencing use of services at centres after Sabbath.
Patient address: Very localised use of the WICs as well as use from out of area residents means inequality of use for all residents of Hackney and The City as a whole. The scatter maps
depicting use in Appendix C illustrate this point well. 27% of use was by out of area residents, the majority of unregistered attended Tollgate: 37% of Tollgate‟s patients. Some were also registered with GP practices outside of Hackney - also reduces the service offer for local people – and thus value for money for the population overall.

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 7 of 21 01 May 2012
Patient registration: Almost a quarter (24%) of both WIC patients was not registered with a GP. Of those that were registered:
3-4 Hackney practices‟ patients were the highest users of the WIC
Some were registered with practices in neighbouring Haringey
Demographic: The profile of patients using the Walk in Centres differs in terms of age and
ethnicity and this is considered in the equality impact assessment at Appendix F.
Key recommendations from the studies
a. Clinical audit report - recommendations
1. Clinical evidence
Consider decommissioning the WICs due to evidence of primary care rather than urgent care clinical activity.
Improve access to and communication about late-night pharmacies
2. Evidence of patient use
WIC activity to be managed back to in hours primary care
Weekend WIC activity to be managed through a transition period by extended hours at a practice in north Hackney or a satellite out of hours service on a Saturday and/or Sunday in the short/medium term or at least for a transition period
3. Evidence of patient address
Consider decommissioning the WICs at Tollgate Lodge and Springfield due to evidence of unequal in levels of access by Hackney and The City patients
Consider mechanisms for improving primary care access to encourage patient communication with their practices and with the primary care out of hours service
4. Evidenced of patient registration
Support primary care to improve and extend access and manage demand effectively:
Support patients to register with a GP
Work with local GPs to consider triage options to help prioritise patient access
Explore the reasons for second opinions in the Improving Primary Care Access programme
Explore the reasons why patients use walk in centres regularly
Share findings with NHS North Central London to review primary care access for patients in Haringey
5. Population demographic
Consider the implications of transition and new service arrangements for the most represented populations and how to mitigate effects
b. The patient flow analysis
There were no recommendations but observations about peaks in activity which would need to be managed outside of GP surgery hours after any change in service. From this, the WICs show similar weekday trends with both showing a slight peak in activity on the Monday and Wednesday followed by relatively steady performance until the weekend. Activity slows down on the weekend with both WICs showing a drop on the Saturday which continues through to Sunday for Tollgate. The analysis of weekday activity by hour shows that the WICs are

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 8 of 21 01 May 2012
particularly busy between 4pm and 8pm. The analysis of activity by hour on the weekend shows the service peak between 10am and 12pm.
c. LINks report - recommendations:
1. Primary care and community health care teams to promote and explain existing out of hours‟ provision as users are muddled by its complexity. What to do when their doctor‟s is closed and it is not an emergency?
2. Design a less complex out of hours‟ service so people know where to go when their GP is closed or they can‟t get an appointment or telephone consultation that day.
3. To explore further why some people use urgent care centres more than others using more traditional market research techniques and exploring the meaning of “urgent”.
4. To facilitate a more multi- professional approach to health information and advice provision to be given opportunistically regarding management of minor ailments such as cough/colds/rashes (community pharmacists, midwifes, health visitors, child care providers, family support workers, community nurses, home carers).
d. Stakeholder meetings – summary of recommendations
References to walk in centres in italics:
111 and phone before you go
111 to have access to patients‟ clinical notes, particularly for those with a long-term condition and/or a complex medical history.
111 call handlers to be trained in empathetic customer service, to include cultural awareness and interaction with older people, those with blocks to communication (such as Alzheimer‟s, dementia or mental health conditions) and those under stress / in crisis.
111 to have the facility to directly book GP appointments and make referrals to community services.
Interpreter service to be available.
111 marketing to include reassurance of validity of algorithms and clinicians in the room and to put in place clear transitional communications strategy.
Some urgent walk-in provision to remain, either at front of A&E or walk-in centres.
GP out-of-hours service
Improve out-of-hours GP services, including shorter wait times and better communications between the patients and the service and the service and in-hours GPs.
Better communication about when home visits are appropriate
Other urgent care provision
Improve access to and communication about mental health crisis services.
The Charedi community were in favour of an extension to walk-in centre hours.
A joined up service
Improve access to GP surgery appointments.
Improve access to and communication about late-night pharmacies.
Improve access to and communication about social care and respite care pathways.
Improve on-going training for patient-facing NHS staff, such as GP receptionists.

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 9 of 21 01 May 2012
6. Engagement feedback
To inform the redesign NHS ELC conducted or commissioned several pieces of research/ patient engagement from October 2011 to January 2012:
Five patient discussion forums
A patient questionnaire about walk-in centres
A clinical survey of patient activity and clinical outputs at Tollgate Lodge and Springfield walk-in centres
A stakeholder event in January 2012.
Summary of feedback
A summary report is attached at Appendix E, below are key points:
Confusion around the difference between “emergency” and “urgent” care
Problems with the out-of-hours service; including lack of knowledge about the service
A&E is a guaranteed way to receive rapid treatment so is used as the default
Lack of late-night pharmacies and patchy information about opening hours leads to A&E attendances
Many people are using walk-in centres (WICs) because they either find it difficult to access their GP or it is more convenient. Some people reported being told by their GP practice to use them GP out of hours service: waits are too long and needs better communications – particularly around when home visits are appropriate
Need better signposting and clear pathways for crisis services for mental health patients and those with Alzheimer‟s and dementia
Need a more joined-up process e.g. communication about social care and respite care pathways; and the need for improved training for staff such as GP receptionists
7. Plans to consult
Following extensive discussions with local community groups and clinicians the local NHS is proposing a six week period of public engagement and consultation, starting on 4 May 2012, including a variety of activities described in this document. This approach has been agreed with the Hackney Overview and Scrutiny Committee. After an assessment of the responses received, consideration of any amendments to the proposals and of any other information (e.g. the equalities impact assessment) it is expected that a decision on the future of the services would be taken in mid-July. The proposal is to close the services from September/October 2012.
The strategy and action plan at Appendix E describes the communications actions required to manage a successful engagement and consultation process regarding the closure of walk-in services at Tollgate and Springfield with:
1. Staff (e.g. at the walk-in centres and hospital trusts, GPs and commissioners)
2. Patients and carers
3. Health partners (e.g. local councils and charitable organisations)
4. The community (e.g. the public, health and community groups)
5. Influencers (e.g. MPs, the media)
6. Representatives (e.g. OSCs, LINks and unions).

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 10 of 21 01 May 2012
B. The case for decommissioning the walk in centres
1. Market analysis:
Other practices in the area The two practices closest to the WICs to the north, Cranwich Road and Stamford Hill, both have closed lists and are consequently not registering new patients, apart from new born babies that are born to patients already registered at the practice. In both instances the high birth rate in the area is accountable for the list sizes remaining constant despite being closed. Both practices are limited by their premises, which preclude the opportunity to expand and employ additional clinicians to enable list growth.
Cranwich Road: situated 1km from Tollgate Lodge. The expectation with a closed list is that the list size would decrease until such time as it drops to a level where it can reopen.This has not been the case, however, with Cranwich Road - despite the fact that its list has been closed for 4 years, the list size has remained stable at around 6,000 patients.
Stamford Hill: located 0.75km from Springfield. The list has been closed for almost a year but as in the case for Cranwich, the list has remained stable at around 14,000 patients. Patients unable to register at these practices have been diverted to Tollgate and Springfield as the nearest alternative options. This has led to rapid list growth and increasing demands for registered services at both practices.
Future population growth After decades of decline, Hackney‟s population started to grow in the early 1990s and considerable growth is expected to continue over the coming decades. Health care services will therefore, not only need to increase to provide additional capacity to existing populations, but also to keep pace with population growth. Forecasts indicate that Hackney‟s total population:
Will increase by 6.9% by 2017 and reach a quarter of a million
Will increase by 15% by 2031.2
In the four wards in north east Hackney closest to the walk in centres, it is forecast that:
Over a quarter of Hackney‟s growth will be in this area to 2017
The rate population growth is higher than Hackney‟s total – predicted as 8.8% compared to 6.9 to 2017
Growth means that health care services will need to be provided to 4,500 more people. This is illustrated by Table 1 below:
2 City and Hackney Health and Wellbeing Profile, 2011-12, Future population growth, p19-20.

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 11 of 21 01 May 2012
Table 1: Population growth in Hackney compared with
Casenove, Lordship, New River and Springfield wards
Year 2011 2012 2013 2014 2015 2016 2017 TOTAL
Total 4 wards
48,828
49,628
50,428
51,221
52,017
52,806
53,342
358,270
Growth
800
800
793
796
789
536
4,514
Growth as % 1.6% 1.6% 1.6% 1.6% 1.5% 1.0% 8.8%
Hackney total
234,209
237,165
240,113
243,050
245,978
248,896
250,726
1,700,137
Growth
2,956
2,948
2,937
2,928
2,918
1,830
16,517
Growth as % 1.3% 1.2% 1.2% 1.2% 1.2% 0.7% 6.9%
Springfield and Tollgate Registered GP Services Springfield and Tollgate WICs are located within north east Hackney, an area experiencing a growth surge in the numbers of patients seeking to register with a GP, which is putting practices in the area under increasing pressure to meet demand. This is illustrated by the fact that list growth for both is amongst the highest within City and Hackney. As with other practices in the area, both Tollgate and Springfield are limited to the extent to which they can grow their lists by their premises, which both preclude further significant expansion. Active searches have and are being undertaken to locate new premises in NE Hackney in which to relocate and expand existing GP services, but as yet suitable premises have not been found and are unlikely to be a viable short-term option. Similarly, both practices are reaching full capacity which presents a significant challenge in terms of meeting the demand for GP services in NE Hackney. To contextualise this growth, the average list growth rate for both practices during this period is listed below compared to the City and Hackney average:
Table 2: Comparative % list growth
Table 2 % average list growth
Match 2009 to December
2011
Springfield
3.42%
Tollgate
3.39%
City and Hackney
0.94%

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 12 of 21 01 May 2012
GP Walk in Centre Activity Based on the reviews undertaken, it is believed Walk in centre activity neither encourages patients to seek Primary Care services wherever possible and consequently nor does it represent value for money. Over time, such patient behaviour incurs additional and not insignificant cost to the local health economy, since it:
Is clinically inappropriate activity: All but a minority of the WICs‟ caseload could have been appropriately managed within a primary care setting and/or through community pharmacy
Duplicates existing service provision. As in the clinical findings above:
During the week there is a steady demand at both walk in centres when local GP practices are open
13.5% of patients indicated they were seeking a second opinion for the presenting problem.
In addition, 27% of use was by out of area residents, the majority of which were registered with a GP.
Encourages frequent use and inappropriate management of long term conditions: Around half of patients have used the WIC before and of those, 19% had attended once before and this declining gradually for 2-5 visits previously. One patient had attended on 26 occasions.
Encourages local use: Trends indicate that people living close to a WIC are more likely to use a walk in centre
Does not encourage registration: Almost a quarter of users were not registered with a GP. This is a loss of income for local GPs, Conversely, if these patients require urgent services, practices will provide them despite lack of registration.
2. Assessment of benefits: The main benefits of decommissioning the GP WIC services can be summarized into patient health and financial benefits as follows:
Patient Benefits Given the pressure on GP services in north east Hackney decommissioning WICs at Tollgate and Springfield would free up clinical space and capacity to enable more patients to be registered at both sites. In the calendar years 2010-2011 Tollgate saw an average of 447 WIC patients per week. Under the terms of the APMS contract, Springfield is able to see 245 WIC patients per week a figure which increases each year. PCT benchmarks for access to a registered GP states that practices should aim to provide 72 appointments per 1,000 registered patients per week.
3 Table 4 below utilizes this benchmark to
3 This is in line with the benchmark recommended by the Royal College of General Practitioners (RCGP).

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 13 of 21 01 May 2012
illustrate the potential additional capacity for registered patients if the slots currently being used for patients to see a GP as part of the WIC service were to be made available for registered patients.
Table 3 GP WiC Activity per
week
WiC activity divided by
72
Multiplied by 1000 =
additional capacity for
registered patients
Springfield 245 3.40 3,403
Tollgate 447 6.21 6,208
TOTAL 692 9.61 9,611
If, therefore, the 692 appointments per week currently used for WIC were to be switched to appointments for registered patients, it would potentially enable up to 9,611 additional patients
4
to register at these practices over time. These patients would be residing predominantly in the NE of Hackney and would have access to services above and beyond those currently offered to WIC attendees including:
A full range of enhanced services
A range of additional services
A pro-active system of health promotion and prevention through immunisations and screening programmes
Active and ongoing management of long term conditions
Continuity of care Switching activity from WIC to registered services would alleviate much of the pressure on GP services in NE Hackney and enable patients to register with a choice of practices
Health benefits
In summary, the proposed closure of walk-in services at Tollgate and Springfield would, through
the release of physical capacity and resources, achieve the following anticipated patient benefits:
Provide more GPs so that more patients are able to register. This would ensure a greater focus on the prevention of ill-health, and the management of long-term conditions and social care needs;
Enable patients who are currently registered with Tollgate and Springfield GPs to access urgent appointments more quickly;
Make it easier for patients to register with a GP;
Make it easier for people to access advice from healthcare professionals so that they could avoid having to travel if it is unnecessary;
Provide a less confusing service to patients and clinicians.
4 This figure is an indicative upper maximum for illustrative purposes only and is based on GP appointments only and
does not include other activity delivered in primary care such as by nursing and HCAs.

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 14 of 21 01 May 2012
Financial Benefits The financial case for closure of walk in centre services would require no or minimal investment
yet would yield overall projected savings of £2,631,398 to March 2015. As set out in Table 5 below:
£520,650 of savings would be realised in 2012-13 due to the half year effect
As agreed in the Corporate Strategic Plan, £325,000 would be retained as the
contribution to the urgent care savings and the remaining £195,650 reinvested in Primary
Care.
Table 4: Walk in centre
expenditure and CSP savings
Full year effect
2013+
Half year effect
2012-13
Total 1,041,300 520,650
CSP Urgent care savings 500,000 325,000
Reinvestment in Primary Care 541,300 195,650
The ELC Corporate Strategic Plan states the intention, subject to consultation, to realise £325,000 savings in 2012-13 by considering the closure of the walk in centres from 1 October 2012. Thus, the first cut on these savings will be to achieve this requirement. Details of further plans to reinvest the remaining recurrent savings into much needed Primary Care capacity would be developed and costed following the consultation and engagement period in June 2012. 9, 611 is the projected maximum, additional number of patients who could be registered at Springfield and Tollgate Lodge. Investment could be made, however, into other services, such as extended hours for identified GP practices.
3. Cost / Benefits Assessment
Savings The projected savings from de-commissioning WICs under the current contractual terms is
£2,631,398 to March 2015 when the Springfield contract is due to expire:
Table 5: Cost of retaining WICs
Year Amount
2012/13 £513,685
2013/14 £1,041,300
2014/15 £1,076,413
Total £2,631,398
Costs There are management costs associated with managing the decommissioning of GP WIC services but these would be met within existing resources. There are potential contractual costs associated with varying the Springfield APMS contract which are explored further in the Risk Analysis section below.

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 15 of 21 01 May 2012
There are costs associated with the expected rise in registered patients that would register with Tollgate and Springfield, once capacity is freed up. However, the PCT has a statutory responsibility to ensure that residents are able to register with a GP practice and there would be a costs associated wherever the residents were to register.
4. Option appraisal – Recommended option: Options are summarized below, with option 4 recommended:
Option 1 Retain Springfield and Tollgate WICs WICs services are expensive and do not necessarily provide clinically necessary treatments. Much of the activity is from patients that are registered elsewhere with a GP and therefore a double payment is in effect being made. Services are not necessarily targeted where they are needed and up to 37% of activity is from patients residing outside of City and Hackney, with an estimated 16-25% from Haringey residents
5.
Option 2 Retain Springfield WIC and do not renew Tollgate The same considerations apply as with Option 1 above. The advantage of this option is that a contract variation is not required with Springfield which may have financial repercussions. However, this option would most likely encourage activity to switch from Tollgate to Springfield as they are in close proximity of each other.
Option 3 Renew Tollgate WIC and decommission Springfield WIC The same considerations apply as with Option 1 above. This option would most likely encourage activity to switch from Springfield to Tollgate as they are in close proximity of each other.
Option 4 Recommended: Decommission Springfield WIC and do not renew Tollgate
This would shift activity from a walk in service that is neither clinically appropriate nor cost effective to a GP-registered service in the area of highest need for such services in City and Hackney. All working assumptions included in this report are based on this recommendation.
The Springfield APMS contract would need approval for variation in order to decommission the walk-in element.
5. Key assumptions and dependencies: The key dependency is the ability and willingness of Tollgate and Springfield to agree contractually and engage with the proposed reconfiguration of services. Both providers have indicated this willingness and discussions are progressing well.
5 Walk in Centres, Clinical audit, Appendix C, page 10

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 16 of 21 01 May 2012
6. Risk and Sensitivity analysis:
Risk Mitigation
Increase in A&E activity – patients might attend A&E as an alternative to the GP WIC
Patients currently using the WICs would have a number of alternative options available to manage their primary urgent care needs- all of which would be integrated with the new 111 phone before you go service that would enable patients to access urgent care at the right level of care for their need. The service is designed to help people who are not sure, or who are having difficulty in gaining access to care or who are not registered with a GP:
The new 111 phone before you go service would enable patients to access urgent care at the right level of care for their need. The service is designed to help people who are not sure, are having difficulty in accessing care or who are not registered with a GP
GP practices are, and will remain, the first port of call for most local residents with urgent care needs in working hours. Out of hours, 111 would provide a single, easy to remember telephone number for accessing urgent care, including GP out of hours care. The OOH service currently has a presence in the Primary Urgent Care Centre and future arrangements are to be confirmed
NHS Choices provides web advice for minor ailments as “the online front door to the NHS.” It is the country's biggest health website and gives all the information patients need to make choices about their health. It will remain a resource after 111 goes live.
Chemists and pharmacies currently enable patients to manage their own self care for wherever possible. The new 111 service would have an option to advise patients that the best management of their condition is through self care, as well as advice on the location of the nearest pharmacy. It is recommended that access to and communication about late night pharmacies be improved.
Olympics – the influx of visitors may result in increased pressure for GP & WIC services
The proposed closure of the WICs is timed to take place after the end of the Olympics, on 30 September 2012.
New 111 service – impact of changes in timescale for implementation
The WIC proposal and the 111 programme to go live in 2012-13 do not have short-term timetabling interdependencies, but do form part of a holistic, integrated service over the long- term.
Ensure that intended improvements in other services are in place as soon as contractually possible, such as: improved access to late night pharmacies, the Find a doc service, Out of hours service, and arrangements for extended hours.

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 17 of 21 01 May 2012
Risk Mitigation
Charedi Orthodox Jewish community challenge - the Charedi community is clustered in the North East of Hackney and are high users of WIC services
An Extended Hours Enhanced GP service is in operation across City and Hackney and the majority of practices have signed up to this. This has increased opening hours during the evenings and weekends and has had a positive improvement on patient satisfaction with opening times.
Any community concerns would need to be addressed by the engagement and consultation process which would aim to address the concerns of residents by:
communicating the aim to provide more GP places for residents to register – especially around Tollgate and Springfield
support the provision of phone advice from healthcare professionals at local GP surgeries to avoid wasted journeys for patients
develop an electronic directory of services for clinicians so that they can provide better advice to patients
establish a Find a Doc service to help patients to register with a GP
improve the Out of Hours service – ensuring there is better liaison between the service and local GPs
improve access to and communication about late-night pharmacies
continue to work with London Ambulance Service and others to improve urgent access to community services (e.g. mental health) so there are fewer patients attending A&E who could have got more appropriate care for their condition elsewhere
continue providing urgent care (or signposting to primary care if this is more appropriate) at Homerton Hospital urgent care centre, The Royal London urgent care centre and Barts
Springfield APMS variation – there may be costs ssociated through varying the APMS contract before its end date
Springfield requested opening negotiations regarding WIC closure and this is being actively managed through a process of negotiation with the provider
The case for no or minimal financial compensation to Springfield for early contract termination is on the basis that the proposals for closure are the mutual preference of both commissioner and provider
Any financial loss of earnings would be largely compensated through additional earnings achieved through list growth
In any event, any minimal additional cost associated with contract termination will be more than outweighed by savings in the long term
Managing patient behavior – some patients may have grown accustomed to WIC services
Provider WIC closure plans would be implemented communicating the changes and the rationale ahead of the cessation date.
Active sign posting to alternative services and the option of registered for GP service would be implemented
Political - sensitivity of removing services and perception of cost cutting
The reinvestment of savings into improved Primary Care services needs to be clearly communicated ahead of the closure date, as above, to local providers in the health economy, stakeholders and the public.

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 18 of 21 01 May 2012
C. Conclusions and next steps
1. Timescales:
Next Steps
The following milestones identify the key governance and decision-making for the proposal:
Table 6: Main milestones and dates: Proposed start: Proposed end:
Health in Hackney Scrutiny Committee 21 March 2 April
ELC SMT 13 April 18 April
CCG Clinical Executive Committee 11 April 18 April
Business case and equalities impact assessment circulated to OSC members
Mid April 3rd
week April
Pre-consultation meetings Mid April End April
NELC Board (or Chair‟s action) (deadline TBC) 30 May
Consultation 4 May 29 June
Health in Hackney Scrutiny Committee (TBC) 9 July
Walk in contracts proposed termination - 31 September
Health centres expanded GP lists 1 October -
111 go live in City and Hackney In line with the national deadline
-
Contract reviews TBC -
2. Conclusions and Recommendations
NELC Board will be asked:
To agree:
1. The variation of the Springfield APMS contract in order to decommission the walk-in element of the contract
2. To invoke the appropriate clause in the Tollgate APMS contract in order to extend the registered service element only for a period of three years, to March 2015
To note:
3. No or minimal investment is required for these service improvements
4. Savings of £325,000 would be realised in 2012-13 in line with the CSP plan for Urgent Care in City and Hackney and that a plan for investment of further savings will be developed and costed for Primary Care improvement to focus on increased ability to register with General Practice and better access for registered patients.
5. The discontinuation of the Tollgate walk-in element of the APMS contract.
6. The stakeholder communications strategy and plan for a public process of engagement and consultation
7. The equalities impact assessment (EqIA, see Appendices Fi and Fii) prepared to Stage 1, in line with legal and best practice guidelines and approved by the ELC Equalities Lead. It is advised that the action plan should be embedded in the service plans for future years and be monitored.

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 19 of 21 01 May 2012

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 20 of 21 01 May 2012
Appendix B
Local strategic context – City and Hackney
Urgent Care Improvement Programme: The aims and design principles of the Hackney and City Urgent Care Strategy are set:
Aims
A clear, understandable 24/7 system
Local people less confused and better informed to make appropriate choices
Simpler more consistent services with follow up as required
People helped to look after themselves when appropriate
Primary care needs addressed by own practice whenever possible
A&E and ambulance services concentrate their skills on the more serious and life threatening conditions
Design Principles
Patient safety comes first
Patients are seen by the skill group best able to meet their needs
Clinical and operational processes to look at all patients and pathways to support safe care
Capacity is matched to demand
A cost effective service, maximising benefit for patients. The key ethos is to develop a phone before you go mentality for accessing urgent care and to develop a system that supports patients in gaining the right level of care for their need. The 111 service is designed to help people who are not sure or who are having difficulty in gaining access to care. In working hours GP practices are and will remain the first port of call for most local residents with urgent care needs. 111 will, however, provide a safety net for people
who are unsure where to go or how to access the appropriate care, are not registered or who are finding it difficult to access care. Out of hours, 111 will provide a single, easy to remember telephone number for accessing urgent care, including GP out of hours care.
Primary Care strategy
Care closer to home strategy: City and Hackney set out its vision for its Care Closer to Home Strategy as: “a place where people have the opportunities to lead healthy lives. We will improve the health and wellbeing of all the people in Hackney and the City of London by ensuring that
everyone has access to high quality and responsive health services in the community, high streets and in hospitals. We want to support people to be able to make informed choices about

Pre-consultation business case: North Hackney Primary Care: Improving access and walk in centre decommissioning Page 21 of 21 01 May 2012
their health and we are committed to empowering the community to be active, eat well and avoid behaviours that are harmful to health. We want people to feel at their best and make a positive contribution.”
Bigger, Brighter, Better Strategy: Care closer to home delivers the agreed principles of City and Hackney‟s Bigger, Brighter, Better Strategy:
The PCT’s Service Principles In designing our services, we will keep to the following principles:
Improved local access – making it easier for you to get services
Equity of provision – the same level of service whoever and wherever you are
Continuity of care – you will have your primary care provided by a familiar and consistent team of professional and support staff
Consistent service quality delivered to agreed national and local standards, providing the best value for money.
All of this is designed to add up the “joined up” approach to health, social and other services that contribute to the well-being of the people who live and work in City and Hackney.
Primary Care improving access and demand management programme: Continuing to improve access to primary care is a key priority for quality improvement. This programme is to be delivered across Hackney in 2012-13 as part of the Urgent Care Strategy. NHS ELC has recently approved additional resources to deliver and incentivise a programme of improvement for access to Primary Care and GP services. Extensions of the GP lists at Tollgate and Springfield will form part of this programme. Its objectives are to:
Establish the case for service improvement
Collect baseline data to better understand GP access and the impact on urgent care
Invest resources to drive sustainable GP access improvement
Ensure high performing practices are not disadvantaged The GP contracts require practices to meet the undefined “reasonable needs” of their registered lists, yet current performance of City and Hackney practices against the national benchmark of appointments per 1,000 is unknown. To support continued improvement in terms of both patient satisfaction and capacity, a baseline assessment of patient demand and available capacity in all 45 GP practices in City and Hackney will be undertaken. Based on the analysis of the baseline assessment, triangulated with the results of the national GP patient satisfaction survey, and in recognition that practices have different improvement requirements, practices will develop an access improvement plan and will choose to participate in any of a number of initiatives to best support individual improvement. Initiatives will include: 1. Intensive input including peer support for practices providing poorest access 2. Introduction of GP triage through participation in the national Patient Access pilot 3. Improvements to telephone systems and introduction of alternative booking options and text
messaging 4. Introduction of Touchscreen Surveys for recording patient satisfaction in real-time 5. Supported review of practice appointment system and reception policies 6. Piloting of waiting room facilitators to provide support for registration, signposting and patient
advice.
CCLES SUB COMMITTEE RECOMMENDATIONS
At the 24 February CCG Committee, the Board delegated the sign off recommendations for the 2011/12 CCLES to a Sub Committee who consisted of: Dr May Cahill – Medical Director, NELC Jan Harley-Doyle – Practice Manager Rep on the CCG Jaime Bishop – Public Representative on the CCG (Chair) Mariette Davies – Non Executive Director, NELC The Sub Committee met on 2 May and went through all practices CCLES trackers and noted the recommendations made by the Consortia Leads in conjunction with their “linked” Clinical Executive. The Sub Committee were happy to recommend that all practices receive their second £1.66 per patient payment (see attached spreadsheet) with the exception of Barretts Grove Surgery.

CCLES SUB COMMITTEE RECOMMENDATIONS The NH Consortia Leads had advised the Sub Committee that they did not feel able to recommend the full second payment to Barretts Grove as they felt their tracker wasn’t robust enough to withstand external audit. Their concern had been taken to Paul Haigh, Chief Operating Officer and Clare Highton, Chair, for advice. Other views were requested from Clinical Executive and Consortia Leads responsible for assessing their practice trackers. The Sub Committee took all views into consideration and agreed that the practice should receive a percentage of their second payment with the final decision resting with the Consortia Leads. The NH Consortia Leads agreed that 75% of the final payment should be paid to the practice

CCLES SUB COMMITTEE RECOMMENDATIONS
The Sub Committee were happy to endorse the Consortia Leads/Clinical Executive recommendations for all other practices to receive their final CCLES payment. The budget forms part of the CCG operating budget for 2011/12 The Board are asked to endorse the Sub Committee recommendations and agree to the payments

KLEAR INCENTIVE SCHEME SUB COMMITTEE RECOMMENDATIONS At the 24 February CCG Committee, the Board delegated the sign off recommendations for the 2011/12 KLEAR Incentive Scheme to a Sub Committee who consisted of: Jaime Bishop – Public Representative on the CCG (Chair) Mariette Davies – Non Executive Director, NELC Rhiannon England – CCG Clinical Lead The Sub Committee met on 16 May and went through the KLEAR practice audits and noted the statement from Haren Patel as follows: • The practices had identified the areas where they were over-referring for
audit • Following the first round of audits, the Consortium had two education
sessions and peer reviews • The practices re-audited the same specialties after 6 months to evidence
the changes implemented after learning

KLEAR INCENTIVE SCHEME SUB COMMITTEE RECOMMENDATIONS Unfortunately due to a member of staff leaving no paper records were to hand to support attendance at the education sessions. The Sub Committee requested that Haren provides the dates of the sessions to support his statement. The Sub Committee felt that the majority of practices had achieved the objectives of the scheme but a couple needed to provide a summary or conclusion of the learning together with an action plan. The Sub Committee wished to place on record that the Consortium should be offered support with the CCLES for 2012/13
KLEAR INCENTIVE SCHEME SUB COMMITTEE RECOMMENDATIONS The Sub Committee were happy to recommend that all KLEAR practices receive their final £1.00 per patient in respect of the KLEAR Incentive Scheme. The Board are asked to endorse the Sub Committee recommendations and agree to the payments

CCLES SECOND PRACTICE PAYMENTS
PRACTICE LIST SIZES AS AT DECEMBER 2011Practice List Size 2nd CCLES payment @ £1.66
SW ConsortiumDeBeauvoir 4323 7176Hoxton 5917 9822Lawson 11008 18273Neaman 8751 14527Queensbridge 8100 13446Shoreditch Park 6750 11205
North HackneyBarton House 12524 20790Cedar 6619 10988Heron 9148 15186Statham Grove 8107 13458Elm 2858 4744Gangola 3547 4416 75% payment agreed by Consortia LeadsSpitzer 5868 9741Nightingale 8294 13768Stamford Hill 14475 24029Somerford Grove 10697 17757Springfield 4861 8069
R & SGadhvi 5050 8383Rosewood 2123 3524Athena 5536 9190Clapton 6755 11213Rizk 2181 3620Southgate Rd 6900 11454Sandringham 4522 7507Beechwood MC 3299 5476

WellWell Street 11744 19495Elsdale Street 5718 9492London Fields 8700 14442Lower Clapton 11693 19410Wick 5503 9135Sorsby 5375 8923Trowbridge 3736 6202
TOTAL 364861