nha pharmaceutical aseptic services group - civas · pasg guidance on implementing the 2013 sharps...
TRANSCRIPT

PASG Guidance on Implementing the 2013 Sharps Regulations Page 1 of 12
NHS Pharmaceutical Aseptic Services Group
Guidance on implementing the Health and Safety (Sharp Instruments in Healthcare) Regulations 2013
in NHS Pharmacy Aseptic Services
Introduction
The Health and Safety (Sharp Instruments in Healthcare) Regulations 20131 came into force on May 11th 2013. They apply to all “healthcare employers using sharp objects or
instruments for the exercise of specific healthcare activities, which are able to cut, prick or cause injury”. They therefore apply to Pharmacy Aseptic Services.
This guidance is intended to support NHS Pharmacy Aseptic Services to comply with this new legislation – wider application to other healthcare environments is not
addressed here. It should be used in conjunction with the legislation1 and general guidance on these Regulations produced by the Health and Safety Executive (HSE)2. It is assumed that all products handled in aseptic units are sterile, ie. contain no viable
organisms – where units do handle sharps contaminated with live organisms in separate facilities the full legislation should be referred to.
It should be noted that compliance with the Regulations is a legal requirement, and is
not negotiable.
Background The Sharps Regulations are the UK enactment of a European Directive passed in 20103
which includes the statement that:-
“ Where the results of … risk assessment reveal a risk of injuries with a sharp and/or infection, workers’ exposure must be eliminated by taking the following measures, without prejudice to their order:
Specifying and implementing safe procedures for using and disposing of sharp medical instruments and contaminated waste. These procedures shall be regularly reassessed and shall form an integral part of the measure for the information and training of workers referred in clause 8,
Eliminating the unnecessary use of sharps by implementing changes in practice and on the basis of the results of the risk assessment, providing medical devices incorporating safety-engineering protection mechanisms,
The practice of recapping shall be banned with immediate effect”
Since this was passed the HSE has consulted4 and worked with UK specialist groups, including NHS Pharmaceutical Aseptic Services Group (PASG) and the UK
Radiopharmacy Group to produce UK legislation which complies with the Directive but provides pragmatic solutions for aseptic services. Further background is given on the
HSE site5

PASG Guidance on Implementing the 2013 Sharps Regulations Page 2 of 12
Guidance
1. Where do the regulations apply? They certainly apply to all aseptic services based in hospitals, including CIVAS, chemotherapy, PN and Radiopharmacy services. They apply equally to hospital
employees, locums, and contractors (eg. an outsourced service provided by a private company on-site).
They also apply to off-site Trust-owned aseptic manufacturing units, since the employer is a healthcare provider.
Some clinical trials may not be considered healthcare, especially phase 1 or 2 trials.
However the HSE guidance2 includes any trial in a hospital setting in the scope, where the sharps are handled by Trust employees, whether on- or off-site.
2. Avoiding sharps
The regulations primarily seek to avoid the use of sharps where possible. Aseptic units should review the devices they use, to identify where non-sharp devices could be used in their place where reasonably practicable. Some examples are given in the Resources
section below, although this list is not exhaustive and the available range is growing. An assessment of their suitability for local use, training and change control will be
needed, and it should be noted that cost is likely to be higher than current simple devices.
3. Use of safer sharps Where use of sharps cannot be avoided, Aseptic units must then look at how ‘safer
sharps’ can be substituted, where reasonably practicable. These are devices where the needle is protected from causing injury, eg. shielded or automatically contained. Again
the implications above will need to be considered, and some examples are given in the Resources section below.
4. Use of existing sharps and re-sheathing needles Only if non-sharp or safer-sharp devices are not reasonably practical can existing
exposed sharps be used. Whilst in clinical areas re-sheathing (re-capping) has been considered unsafe practice for some while, in aseptic units it is often vital in order to maintain asepsis and drug containment, as well as safe practice when working in the
constraints in an isolator. The HSE recognises this and has specifically allowed for re-sheathing in the UK legislation provided that:-
Re-capping is only undertaken if the process requires it, A risk assessment6 for the process is undertaken,
The risk of injury to employees is effectively controlled by the use of a suitable appliance, tool or other equipment – ie. a re-sheathing device.
PASG consider it best practice in general to re-sheath needles between stages of dose preparation and prior to disposal of the needle in a sharps bin, although local
circumstances should be considered as part of the risk assessment. It should be noted that removing the needle sheath can present as much risk of injury as re-sheathing,
and risk assessment should take this into account. An example risk-assessment is given in appendix 1 to this document, which may be copied and adapted for use locally, following local risk assessment. Trusts will have processes for risk assessment
PASG Guidance on Implementing the 2013 Sharps Regulations Page 3 of 12
in place and these should be referred to, however further guidance on the process is
available from HSE7. It is important that this is kept as a simple process, and that managers note that they do not need to exceed the requirements of the legislation
unless they choose to.
There are a few re-sheathing devices available at the moment, and work is going on with potential suppliers to bring more to the market. Not all are suitable for use in an aseptic unit, and we have listed those available at the time of writing which we consider
suitable in the Resources section below – our criteria for determining suitability for use is based on robustness, effectiveness for one-handed unsheathing and re-sheathing,
stability on the work-surface, ability to be cleaned, and that they do not present any other hazard to the operator or the controlled environment. Re-sheathing devices should not be stuck to surfaces as this prevents cleaning, even though some devices
are supplied with adhesive pads. When first introducing into Grade A zones thorough cleaning and decontamination is required; once in place they should be left in the
Grade A zone between sessions, and cleaned as part of the normal cleaning schedule.
5. Disposal
The regulations require that clearly-marked, secure, lidded sharps disposal bins are placed close to the place where the sharps are used, and that written instructions on disposal are displayed in that area. PASG consider it would be best practice to use
small, overwrapped, pre-sterilised sharps bins and transfer these into isolators and laminar flow cabinets for use during a work session, and to seal them before removal at
the end of day. Written information on disposal may best be displayed as a brief work instruction,
summing up key warnings (see 6 below) and procedure points for handling and disposing of sharps. Lamination will allow surface cleaning; where units use fixed multi-
pocket display systems for clean-room documents they will need to be arranged so that the sharps information is visible at all times.
6. Information for employees The Regulations require that staff are informed of the risk of injury from the sharps in
use, and that managers work with safety reps to develop and promote the information. Information may be provided in many forms, including SOPs, safety guides, posters, information on internal staff websites. The information must include:-
The risks of injuries from the sharps used in your department
The legal responsibility each member of staff and management have to comply with agreed safe practices (particularly around handling, re-sheathing and disposal)
Good practice in preventing injury The process for reporting sharps injuries (see 8 below)
The Regulations also require staff to be informed of the risk/benefits of vaccination and support for those injured with biologically contaminated sharps – in the context of a
conventional aseptic service these will not be relevant to the risks faced by staff.
PASG Guidance on Implementing the 2013 Sharps Regulations Page 4 of 12
7. Training for employees
Training should support the information given in item 6 above and be in an appropriate form for the staff to be able to work safely with the specific sharps in use in the service.
It would be appropriate for this to be part of induction training for new staff, repeated when they start competencies for aseptic preparation. It could also be referred to at
any regular update training, where this is done. The initial training must cover:-
The correct use of safer sharp devices;
The correct use of re-sheathing devices; Safe use and disposal of sharps;
What to do in the event of a sharps injury (see 8 below); Your arrangements for health surveillance and other relevant procedures.
8. Reporting injuries from sharps Under the Regulations all sharps injuries must be reported to the employer. For NHS
aseptic units this will most appropriately done on a Trust adverse event / incident report form. This should include an investigation of the circumstances and actions agreed to prevent recurrence – the HSE gives further guidance2 on this. The
regulations have further requirements for injuries with sharps potentially contaminated with micro-organisms or blood-borne viruses, which should not be encountered in an
aseptic service. 9. Review
Aseptic service managers should review their processes and risk assessments under this legislation at appropriate intervals, eg. annually, particularly the maintaining of
training, safe practices, use of re-sheathing devices and displayed information. The first annual review will be due now (May 2014). The Regulation states that there will be a national review of compliance within 5 years.
Resources (other devices may also be available)
Non-sharp devices which could be used in aseptic units:-
Infusion bags with needle-free additive ports (Maco)
Blunt-ended needles, for drawing up from vials (BD)
Filter straws, for drawing up from ampoules (Braun, Fannin)
Compounding pins, for withdrawing from vials (Braun, Codan, Baxter, Fannin, Sartorius,
others)
Compounding spikes, for withdrawing from bags (Braun, Codan, Baxter, Fannin, others)
Vial adaptors (Adelphi, Helapet, Fannin)
Needle-free compounding systems (BD Phaseal, Teva Tevadaptor, Helapet Vial2Bag,
Fannin Chemo-Clave/Spiros/Genie)
Safer-sharp devices which could be used in aseptic units:-
Cyto-luer device for adding to or withdrawal from infusion bags (Baxter)
Self-sheathing needles (various brands, NHS Supplies catalogue)
Double-ended compounding needles with protective surround (Maco, Helapet, Braun)
Vial-to-bag docking devices (Baxter Vialmate, Fresenius, Maco, Braun)
Re-sheathing (Re-capping) devices for use in aseptic units:-
Needle Recapper - Bright Technologies http://www.britec.net/syringe-accessories.html
Needle-Safe 2 http://www.ingenious.com/NS/ns.htm
(EU supplier:www.bestcaremedical.nl E-mail: [email protected]). PASG have some concerns about the suitability of this device, however few alternatives exist at present.
NeRD – Cardinal Health http://www.cardinal.com/us/en/Safety/Othersafetytools
PASG Guidance on Implementing the 2013 Sharps Regulations Page 5 of 12
Forceps have been used in some units, however risk assessment will need to determine
whether their use is fully effective at controlling the risk of injury – PASG recommend a
specific re-sheathing device is used where a need has been identified.
Peter Rhodes, May 2014 On behalf of NHS Pharmaceutical Aseptic Services Group References
1. The Health and Safety (Sharp Instruments in Healthcare) Regulations 2013 http://www.legislation.gov.uk/uksi/2013/645/made#f00002 (accessed 24.04.13)
2. Health Services Information Sheet 7 - Health and Safety (Sharp Instruments in Healthcare) Regulations 2013 - Guidance for employers and employees, March 2013 http://www.hse.gov.uk/pubns/hsis7.pdf (accessed 24.04.13)
3. Council Directive 2010/32/EU of 10 May 2010 - Implementing the Framework Agreement on prevention from sharp injuries in the hospital and healthcare sector concluded by HOSPEEM and EPSU http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2010:134:0066:0072:EN:PDF (accessed 24.04.13)
4. A report on HSE’s consultation on proposals to implement European Directive 2010/32/EU on preventing sharps injuries in the hospital and healthcare sector, HSE, 21.12.12. http://www.hse.gov.uk/consult/condocs/cd244-analysis.pdf
5. Further guidance on the EU Directive, HSE http://www.hse.gov.uk/healthservices/needlesticks/eu-directive.htm
6. The Management of Health and Safety at Work Regulations 1999 http://www.legislation.gov.uk/uksi/1999/3242/regulation/3/made
7. Risk Management, HSE http://www.hse.gov.uk/risk/index.htm
8. National Patient Safety Agency Risk Matrix for Risk Managers http://www.npsa.nhs.uk/nrls/improvingpatientsafety/patient-safety-tools-and-guidance/risk-assessment-guides/risk-matrix-for-risk-managers/ Accessed 26/07/2012
9. Sharps Safety – RCN Guidance to support the implementation of the Health and Safety (Sharp Instruments in Healthcare Regulations) 2013, Royal College of Nursing 2013, http://www.rcn.org.uk/__data/assets/pdf_file/0008/418490/004135.pdf (accessed 29.04.14)
This guidance is published by the NHS Pharmaceutical Aseptic Services Group, and is available at http://civas.co.uk

Version: 1 Master template effective from: [Date] Supersedes: None Page 6 of 12
Written by: [Name]
Document reference:
[Hospital & Aseptic Unit Name] Quality Assurance & Control Support Document
Risk Assessment Form
Appendix 1 Example for adaptation following local risk assessment
Risk Assessment Form Section(s) this assessment relates to:
Document History
Document version Date
implemented
Changes from previous
version
Issue location
1 New document 1.
Chemotherapy Radiopharmacy Nuclear Medicine [other]
TPN CIVAS Quality Control [other]
Assessment Completed by: Date:
Written by: Date:
Reviewed and Accepted By: Date: (include signature) Date:
Date:
Title: Preventing of Sharps Injuries under The Health and Safety (Sharp Instruments in Healthcare) Regulations 2013
Version: 1 Master template effective from: [Date] Supersedes: None Page 7 of 12
Written by: [Name]
Document reference:
[Hospital & Aseptic Unit Name] Quality Assurance & Control Support Document
Risk Assessment Form
Description of Assessment:
What:
The Health and Safety (Sharp Instruments in Healthcare) Regulations 2013 , SI 2013 (645) 1 This assessment considers the implementation and impact of this regulation which enacts EU Directive
2010/32/EU, and came into force on 11th May 2013. The regulation requires that:-
“…(a) the use of medical sharps at work is avoided so far as is reasonably practicable;
(b) when medical sharps are used at work, safer sharps are used so far as is reasonably practicable;
(c) needles that are medical sharps are not capped after use unless that [is done] to control a risk
identified by a risk assessment … and the risk of injury to employees is effectively controlled by the use
of a suitable appliance, tool or other equipment.” 1
This change in law will impact on medicines preparation work in the Aseptic Service, for which re-sheathing
needles is an essential part of the aseptic production process. There are no satisfactory alternatives to the use
of the type of needles currently employed. This has been recognised by the HSE during the consultation period
for the new regulations 2.
This assessment will assess the current re-sheathing practice and associated risks.
Why: There is a statutory obligation on employers under the Health and Safety Act to abide with this new regulation,
which is in the best interests of staff. Use of unprotected sharps has therefore been eliminated from the
Aseptic Service where possible, and non-sharp alternatives or ‘safer sharps’ put in their place. However,
conventional needles are still required in many parts of the service’s work, and re-sheathing (re-capping) of
these is required in order to:-
Maintain asepsis
Minimise operator exposure to hazardous drugs
Minimise risk of harm to the operator and isolator gloves/sleeves from sharps
Suitable equipment is utilised that adequately controls the risk of injury.

Version: 1 Master template effective from: [Date] Supersedes: None Page 8 of 12
Written by: [Name]
Document reference:
[Hospital & Aseptic Unit Name] Quality Assurance & Control Support Document
Risk Assessment Form
Risk Assessment Process
Risk assessment consists of three phases:
1. Identify the Risk(s) To do this you need to look at the actual processes, with the staff involved
2. Analyse the Risk(s)
Why is the process done?
What is the risk of not doing the process?
What controls to reduce the risk are already in place? 3. Evaluate the Risk(s)
What hazards remain, given the controls already in place?
What is the Likelihood of the hazard occurring
What is the Consequence, if it were to happen The scoring tables below provide guidance on the
Guidelines for consequence/ probability analysis The ultimate consideration is the effect of the product, process, system being assessed on the quality, safety, efficacy of the final medicinal product (for other situations refer to the trusts risk assessment scoring system).
Likelihood score
Descriptor Frequency How often might it/does it happen
1 Rare This will probably never happen/recur
2 Unlikely Do not expect it to happen/recur but it is possible it may do so
3 Possible Might happen or recur occasionally
4 Likely Will probably happen/recur but it is not a persisting issue
5 Almost certain Will undoubtedly happen/recur, possibly frequently
Consequence score
Descriptor Frequency How often might it/does it happen
1 Negligible Minimal injury requiring no/ minimal intervention or treatment. No time off work
2 Minor Minor injury or illness, requiring minor intervention. Requiring time off work for < 3 days
3 Moderate Moderate injury requiring professional intervention. Requiring time off work for > 3 days
4 Major Major injury leading to long-term incapacity/ disability. Requiring time off work for > 14d
5 Catastrophic Incident leading to death. Multiple permanent injuries or irreversible health effects
Risk score = Likelihood score X Consequence score
[Source – NPSA3 ]
Version: 1 Master template effective from: [Date] Supersedes: None Page 9 of 12
Written by: [Name]
Document reference:
[Hospital & Aseptic Unit Name] Quality Assurance & Control Support Document
Risk Assessment Form
Risk Identification
Method: Once non-sharp and safer-sharp alternatives have been implemented where possible, undertake a
systematic walkthrough of the preparation processes with key staff, highlighting stages where use of exposed needles (or other sharps) remains.
1. Stages of preparation /QC where use of exposed sharps remains [add / remove according to local risk assessment]
a. Drawing-up of solvents for reconstituting powder vials & diluents to concentrate-vials b. Adding solvents to powder vials & diluents to concentrate-vials c. Drawing up solutions from vials d. Drawing up solutions from infusion bags, when the giving-set port must be kept intact e. Adding solutions to infusion bags f. Sampling of final product for QC testing, if applicable g. Replicating the above production processes with sterile microbiological growth medium as part of an
operator validation
2. Stages of preparation/QC where re-sheathing (re-capping) occurs, using a safe re-sheathing device. [add / remove according to local risk assessment]
a. After drawing up liquid into a syringe, to expel air from the syringe and confirm the volume drawn up b. After confirming the volume in a syringe, if it is to be set aside before independent checking and/or
adding to another vial or infusion bag c. After transferring the contents of a syringe to a vial or infusion bag d. After taking a QC sample from the finished product e. Prior to removing needle from syringe and discarding in sharps bin.
Version: 1 Master template effective from: [date] Supersedes: None Page 10 of 12
Written by: [name]
Template Review date:
[Hospital & Aseptic Unit Name] Quality Assurance & Control Support Document
Risk Assessment Form
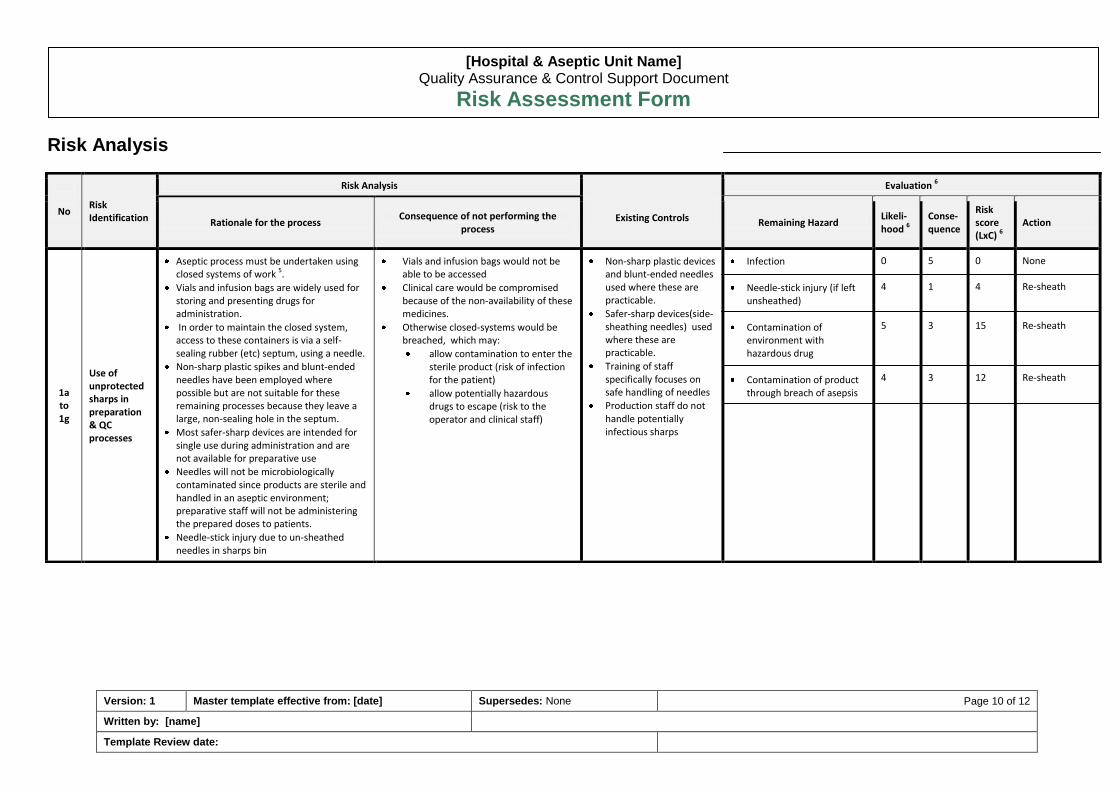
No Risk Identification
Risk Analysis
Existing Controls
Evaluation 6
Rationale for the process Consequence of not performing the
process Remaining Hazard
Likeli-hood 6
Conse-quence
Risk score (LxC) 6
Action
1a to 1g
Use of unprotected sharps in preparation & QC processes
Aseptic process must be undertaken using closed systems of work 5.
Vials and infusion bags are widely used for storing and presenting drugs for administration.
In order to maintain the closed system, access to these containers is via a self-sealing rubber (etc) septum, using a needle.
Non-sharp plastic spikes and blunt-ended needles have been employed where possible but are not suitable for these remaining processes because they leave a large, non-sealing hole in the septum.
Most safer-sharp devices are intended for single use during administration and are not available for preparative use
Needles will not be microbiologically contaminated since products are sterile and handled in an aseptic environment; preparative staff will not be administering the prepared doses to patients.
Needle-stick injury due to un-sheathed needles in sharps bin
Vials and infusion bags would not be able to be accessed
Clinical care would be compromised because of the non-availability of these medicines.
Otherwise closed-systems would be breached, which may:
allow contamination to enter the sterile product (risk of infection for the patient)
allow potentially hazardous drugs to escape (risk to the operator and clinical staff)
Non-sharp plastic devices and blunt-ended needles used where these are practicable.
Safer-sharp devices(side-sheathing needles) used where these are practicable.
Training of staff specifically focuses on safe handling of needles
Production staff do not handle potentially infectious sharps
Infection
Needle-stick injury (if left unsheathed)
Contamination of environment with hazardous drug
Contamination of product through breach of asepsis
0 4 5 4
5 1 3 3
0 4 15 12
None Re-sheath Re-sheath Re-sheath
Risk Analysis

Version: 1 Master template effective from: [date] Supersedes: None Page 11 of 12
Written by: [name]
Template Review date:
[Hospital & Aseptic Unit Name] Quality Assurance & Control Support Document
Risk Assessment Form
2a to 2e
Re-sheathing of needles referred to in 1a-1g above
Although medicine preparation is undertaken in an ultra-clean environment, there is still a risk of contamination from environmental microbes. Re-sheathing is considered to be essential to maintain asepsis
Some cytotoxic drugs and anti-virals handled in the unit are hazardous when operators are exposed repeatedly at low levels. Re- sheathing ensures any spillage from the needle is contained
Handling exposed needles in the confines of an isolator increases the risk of needle-stick compared to a more open environment. Re-sheathing (done following training and using a re-sheathing block) is consider to present less risk than handling unsheathed needles
The presence of unsheathed needles in sharps bins presents a risk to the operator, eg when putting further waste in the bin or if the bin is knocked over due to the constrained working environment of the isolator.
Microbial contamination would lead to growth in the product and potentially catastrophic infection in a patient receiving the dose
Continued low level exposure may lead to deficiencies in fertility, birth abnormality in pregnant female staff, and cancer
Needle-stick incidents cause direct harm to operators, and may carry small quantities of drug into the wound. In addition, the integrity of the aseptic environment is compromised, requiring time-consuming cleaning and replacement of gloves.
Needles only used where essential
Re-sheathing is done using a re-sheathing block to hold the sheath, using a one-handed technique
Production staff receive structured training for their role, including safe-handling of sharps.
Production staff do not handle potentially infectious sharps
Infection
Needle-stick injury (using re-sheathing device)
Contamination of environment with hazardous drug
Contamination of product through breach of asepsis
0 1 1 1
5 1 3 3
0 1 3 3
None Training & monitor incidents. None (consider surface residue testing). None (monitor via operator & process broth validations)
Version: 1 Master template effective from: Supersedes: None Page 12 of 12
Written by: [Name]
Template Review date:
[Hospital & Aseptic Unit Name] Quality Assurance & Control Support Document
Risk Assessment Form
Acknowledgements
Source of this example risk assessment – NHS Pharmaceutical Aseptic Services Group 5
Risk Assessment template design – Adam Hocking, Principal Pharmacist QA, University Hospital Southampton NHSFT
Risk evaluation scores - Máiréad O’Mahony, Anne Black & Alison Beaney 6
Recommendations / Conclusion
Use of exposed needles in the Aseptic Unit is required to performs tasks and maintain product sterility through use of closed systems
Re-sheathing of needles is required to maintain product sterility, prevent contamination of the environment, and protect the operator from exposure to hazardous drugs and injury.
Operator risk from needle stick injury is limited to low level exposure to the drugs being processed; the needles used are sterile and contain no biological or blood borne contamination.
Needle-stick risk will be reduced through re-sheathing, provided a re-sheathing block is used.
A programme of operator training and assessment incorporating safe practices with sharps is in-place.
The practice of using and re-sheathing needles will continue with the additional safeguard of a one handed re-sheathing device being made available for operators at each stage of production and QC where re-sheathing occurs.
List of references & documents appended:
1. The Health and Safety (Sharp Instruments in Healthcare) Regulations 2013 http://www.legislation.gov.uk/uksi/2013/645/made#f00002 (accessed 24.04.13)
2. Health Services Information Sheet 7 - Health and Safety (Sharp Instruments in Healthcare) Regulations 2013 - Guidance for employers and employees, March 2013 http://www.hse.gov.uk/pubns/hsis7.pdf (accessed 24.04.13)
3. National Patient Safety Agency risk matrix http://www.npsa.nhs.uk/nrls/improvingpatientsafety/patient-safety-tools-and-guidance/risk-assessment-guides/risk-matrix-for-risk-managers/ Accessed 26/07/2012
4. Quality Assurance of Aseptic Preparation Services, 4th Ed, Beaney, A on behalf of NHS QA Committee, Pharmaceutical Press 2007
5. Guidance on implementing the Health and Safety (Sharp Instruments in Healthcare) Regulations 2013 in NHS Pharmacy Aseptic Services, NHS Pharmaceutical Aseptic Services Group, May 2013
6. Risk scores Adapted from: Implications of the European Council Directive 2010/32/EU on aseptic practices in the UK, Máiréad O’Mahony MSc. GPhC, Alison Beaney D.Prof.,M.Sc.,M.R.Pharm.S., Newcastle upon Tyne Hospitals NHSFT, 2012
7. The Management of Health and Safety at Work Regulations 1999 http://www.legislation.gov.uk/uksi/1999/3242/regulation/3/made
8. Risk Management, HSE http://www.hse.gov.uk/risk/index.htm
Action Required
Action Required Action complete Completed by: Date: Reviewed by: Date: Comments:
1. One handed re-sheathing devices, which are compatible with aseptic pharmaceutical production are to be made available at the following locations within production and QC:
All manipulation isolators & LFCs
All QC sampling points if applicable
QC Laboratory if applicable