newsletter - anesthesia patient safety foundation
TRANSCRIPT

Inside: Report on Training Initiative ..............................................................................................Page 43
Dear SIRS: In-line Oxygen Monitor ....................................................................................Page 50
Cardiac Arrest After Popliteal Block..................................................................................Page 52
Donors ........................................................................................................................................Page 53
Q&A ............................................................................................................................................Page 54
Emergency Evacuation Drill ................................................................................................Page 56
NEWSLETTERVolume 21, No. 3, 41-60 Circulation 80,350 Fall 2006
www.apsf.org The Official Journal of the Anesthesia Patient Safety Foundation
by Wilson Somerville, PhD, and Robert C. Morell, MD
The 2006 Annual Meeting of the American Soci-ety of Anesthesiologists will be held at McCormickPlace in Chicago, Illinois, from Saturday, October14, 2006, through Wednesday, October 18, 2006.Patient safety will once again play a significant rolein the numerous lectures, presentations, and scien-tific topics integral to this annual conference. Theever popular Refresher Course Lectures will beginon Saturday, October 14, and continue dailythroughout the meeting, beginning with Dr. JanEhrenwerth reminding us of Fire in the OperatingRoom: It Could Happen to You (#108, 10:50-11:40 am,Room E271). Following this hot topic, in the sameroom, are Dr. William Rosenblatt presenting Deci-sion Making in Airway Management (#109, 1:40-2:30pm), and Dr. Jessica Alexander pointing out ThePotential Hazards of Perioperative Herb and DietarySupplement Use (#110, 2:50-3:40 pm). In Room E350,Dr. Evan Kharasch will break down Issues in Anes-thetic Degradation and Toxicity (#113, 9:40-10:30 am).Airway topics resurface in Room E351 as Dr.Andranik Ovassapian explores The Role of LMA,Combitube and Fiberoptics in the Difficult Airway(#120, 10:50-11:40 am). Dr. James Cottrell presentshis thinking on Perioperative Neuroprotection for theHigh Risk Surgical Patient in Room E352 (#129, 4:00-4:50 pm), while Dr. Mark Warner simultaneouslysheds light on Neuropathies, Blindness and PositioningProblems in Room E353b (#135). Dr. Arnold Berryawakens new perspectives with Our Health and theSafety of Our Patients in a 24/7 World: Are we Asleepon the Job? (#136, 8:30-9:20 am). Sunday afternoonbrings us the opportunity to hear Dr. RobertCaplan’s ever popular discussion of the ASA ClosedClaims Project: Lessons Learned (#217, 2:50-3:40 pm,
Grenda Fahy (#402, 9:40-10:30 am, Room E271).During this same time slot, in Room E351, Dr. SteveHall will review The Child With a Difficult Airway:Recognition and Management (#412). That afternoonseveral practical and important safety topics will bepresented including, Dr. Girish Joshi discussing ThePatient With Sleep Apnea Syndrome for AmbulatorySurgery (#414, 2:50-3:40 pm, Room E351), Dr. DanielCole delving into Depth of Anesthesia: Clinical Appli-cations, Awareness and Beyond (#418, 1:40-2:30 pm,Room E352), Dr. Michael Murray Managing MassCasualties (#423, 2:50-3:40 pm, Room E353b), and Dr.Alan Tait helping us by Minimizing and ManagingInfections in the Perioperative Period: The Role of theAnesthesiologist (#427, 1:40-2:30 pm, Room E353c).Room E450b is host to Dr. Frederic Berry remindingof us of What to do After an Adverse Outcome (#432,1:40-2:30 pm) and Dr. Jonathan Benumof explainingThe New ASA OSA Guidelines (#433, 2:50-3:40 pm).The ASA Refresher Courses conclude on Wednes-day, October 18, 2006, with Dr. Lucinda Everettreviewing Safety and Quality in Ambulatory Anesthesia(#501, 8:30-9:20 am, Room E353b), followed in thesame room by Dr. Jeanine Wiener-Kronish explor-ing the question Infection Control for the Anesthesiolo-gist: Is There More than Handwashing? (#502,9:40-10:30 am), and Dr. Barbara Leighton toppingthings off with Epidural Analgesia for Labor: Safety andSuccess (#503, 10:50-11:40 am).
®
See “Topics,” Page 48
Room E350), presented concurrently with Dr. CarinHagberg refreshing the important topic of CurrentConcepts in the Management of the Difficult Airway(#235, Room E353b). Dr. John Eichhorn shares hisexpertise regarding Risk Management in AnesthesiaPractice in Room E353c (#240, 1:40-2:30 pm). OnMonday, October 16, Dr. Jerrold Levy starts themorning off with Anaphylaxis and Adverse DrugReactions (#310, 8:30-9:20 am, Room E351), and Dr.Tempelhoff follows that afternoon with advicetoward Avoiding Complications in Neuroanesthesia(#311, beginning at 1:40 pm, Room E351). Theemerging topic of Inflammatory Response: CurrentConcepts will be presented by Dr. Edward Sher-wood (#316, 2:50-3:40 pm, Room E352). Tuesday,October 17 revives us with Raising the Dead: Manage-ment of the Post-Arrest Patient presented by Dr.
2006 ASA Preview—Safety Topics Abound
Your APSF Executive Committee at work reviewing and planning safety initiatives.

APSF NEWSLETTER Fall 2006 PAGE 42
The APSFcontinues toaccept andappreciate
contributions.
Please make checks payable to the APSF
and mail donations to
Anesthesia Patient Safety Foundation (APSF)520 N. Northwest HighwayPark Ridge, IL 60068-2573
Check out our new andimproved website at
www.apsf.org• Grant Guidelines
• Search Engine
• Back Issues of the Newsletter
• Safety Links
• Sponsor List
• Foundation Information
User-Friendly & Informative!
NEWSLETTERThe Official Journal of the Anesthesia Patient Safety Foundation
The Anesthesia Patient Safety FoundationNewsletter is the official publication of the nonprofitAnesthesia Patient Safety Foundation and ispublished quarterly at Wilmington, Delaware.Annual contributor status: Individual – $100.00, Cor-porate – $500.00. This and any additional contri-butions to the Foundation are tax deductible. © Copy-right, Anesthesia Patient Safety Foundation, 2006.
The opinions expressed in this Newsletter are notnecessarily those of the Anesthesia Patient SafetyFoundation or its members or board of directors.Validity of opinions presented, drug dosages,accuracy, and completeness of content are notguaranteed by the APSF.
APSF Executive Committee:Robert K. Stoelting, MD, President; Jeffrey B.
Cooper, PhD, Executive Vice President; George A.Schapiro, Executive Vice President; David M. Gaba,MD, Secretary; Casey D. Blitt, MD, Treasurer; Sorin J.Brull, MD; Robert A. Caplan, MD; Nassib G.Chamoun; Robert C. Morell, MD; Michael A.Olympio, MD; Richard C. Prielipp, MD.Newsletter Editorial Board:
Robert C. Morell, MD, Editor; Sorin J. Brull, MD;Joan Christie, MD; Jan Ehrenwerth, MD; John H.Eichhorn, MD; Lorri A. Lee, MD ; Rodney C. Lester,PhD, CRNA; Glenn S. Murphy, MD; Denise O’Brien,BSN, RN; Karen Posner, PhD; Keith Ruskin, MD;Wilson Somerville, PhD; Jeffery Vender, MD.
Address all general, contributor, and subscriptioncorrespondence to:Administrator, Deanna WalkerAnesthesia Patient Safety FoundationBuilding One, Suite Two8007 South Meridian StreetIndianapolis, IN 46217-2922e-mail address: [email protected]: (317) 888-1482
Address Newsletter editorial comments, questions, letters, and suggestions to:Robert C. Morell, MDEditor, APSF Newsletterc/o Addie Larimore, Editorial AssistantDepartment of AnesthesiologyWake Forest University School of Medicine9th Floor CSBMedical Center BoulevardWinston-Salem, NC 27157-1009e-mail: [email protected]
www.apsf.org
®
Be sure to check out the APSF Booth in the Exhibit Hall
at the 2006 ASA Meeting inChicago, IL, October 14-18, 2006.
There you can
☛ Meet APSF Leaders/Representatives
☛ Make a Donation
☛ See Current and Prior Issues
of the APSF Newsletter
☛ Explore Current Safety Initiatives

APSF NEWSLETTER Fall 2006 PAGE 43
in particular.8 One member of the Council expressedhis concerns as follows:
“Further on the topic of education, training,and safety, I would like to share with you thefrequent reality of clinicians refusing in-serviceon new anesthesia equipment because they are‘too busy’ or, ‘can figure things out for them-selves,’ or, if they show up at all, they stickaround for a few cursory minutes before theyrun out to do something else. We find ourselveschasing clinicians so we can fulfill our commit-ment to ensure that our equipment is operatedsafely. My colleague put it this way, ‘No oneshows, no one listens, and very few care.’ Theseare usually the guys who scream the loudest ifsomething goes wrong, or they misuse, or mis-understand some facet of the equipment’s opera-tion. This probably sounds harsh, butunfortunately it is true—an aspect of the busi-ness which all manufacturers face, and one notusually discussed. This situation appears to bemore a function of how a specific institution‘runs its business.’ The local ‘champion’ concept,which we discussed in our other emails, is anessential part of the solution to this problem, butI think that this may be another opportunity forthe APSF to make a difference by making thisissue more visible and recommending a meansof ensuring that users of anesthesia equipmentare adequately trained on their equipment. “
With these and other imperatives to take action,the Committee on Technology of the APSF soughtexamples of mandated technology training pro-grams and developed a pilot program for implemen-tation, analysis, and presentation to the anesthesiacommunity. That program is described below.
The Problem with CurrentPractice
Conventional “in-service” programs are oftenrecognized as superficial and inadequate becausethey do not require advanced preparation, are notmandated, do not allow individual practice, do nottest for learning nor application skills, and are fre-quently abandoned for lack of time (as the morningbreak or refreshments run out). They typically occuronly once, when new equipment is installed, do notaccount for personnel who are away from work, nordo they accommodate new hires or new classes oftrainees. Many clinicians lack the interest to learn, orthey verbalize a great reluctance to accept change,or they find it very difficult to learn complex newtechnologies. Not all institutions designate or recog-nize an equipment advocate-enthusiast, and only ahandful has sent a clinician to the factory for addi-tional training. Some anesthesia departments have
on-site biomedical technicians, but they may nothave obtained the specialized training prior toinstallation, or don’t have time for teaching. Finally,simplistic instructional aides may not exist.
Getting the clinicians and educators togetherseems to be the problem. Should the “carrot” or“stick” method be applied to mandate training, as itpromises to close the gap on deficiencies of knowl-edge and application skills, in order to improvepatient safety?
Experience With MandatedTechnology Training Initiatives
Clinical and corporate members of the Commit-tee on Technology of the APSF were asked to providedetailed examples of organized, comprehensive, andmandatory technology training programs withintheir clinical base. Only 3 were provided. Oneincluded a 6-hour training session for 50CRNA/student nurse anesthetists (SRNAs), and allMD attendings in a Michigan academic department9
prior to installation of 25 new machines. The timeand manpower expense for nursing was providedby the hospital, while the manufacturer provided aline-item training expense on the customer’s invoice.Components of the training included manuals, man-ufacturing experts, train-the-trainers, hands-onworkshops, 6 weeks of on-site company representa-tives, and super-user training, but no competencetesting. No information was provided on trainingfor the anesthesiologists at that same institution, northe effects of that training on subsequent use of theequipment.
Another program was described by a majormanufacturing company’s director of clinical edu-cation in the United Kingdom.10 This program uti-lized a new guided workbook with directedhands-on learning and response format, led by thecompany representative for a period of 3 hours, orby a train-the-trainer, who would have received afull day of training. The cost of the training pro-gram was line-itemized on the customer’s invoice.The program was not mandated, and thespokesman commented that cooperation for train-ing among physicians and consultants was the mostdifficult to obtain because of time restrictions, cul-ture, and venue for learning.
In a third description of training in a privatehospital in Michigan,11 the Anesthesiology Depart-ment Chair mandated completion of a formal train-ing program for 45 anesthesiologists and 20CRNAs, who could not use the new and modernmachine clinically, until they completed a 30-minute training session with a company representa-tive, during a 3-week period. Those who did notinitially participate were continuously assigned to
Michael A. Olympio, MD, Bonnie Reinke,and Abe Abramovich
IntroductionThe most effective method of introducing new
anesthesia equipment into the operating room hasnot been thoroughly investigated, despite recentand dramatic increases in complexity of these newmachines. New machines have unique and subtlevariations in breathing circuit design, automatedcheckout, volatile agent delivery, hidden pistonventilators, fresh gas delivery, and ventilationmodes.1 Despite conventional pre-use instructionwith, or without simulation, Dalley and colleaguesrecently concluded that anesthesiologists could notreliably assess their ability to safely use the equip-ment in clinical practice. However, those clinicianswho received additional training in simulationwere more likely to correctly apply the machine fea-tures during a simulated anesthesia emergency.2
Furthermore, Dalley learned that new designsmeant to enhance patient safety can actually haveunintended and detrimental consequences particu-larly when latent errors surface during abnormal(and particularly stressful) clinical situations.
Although the incidence of equipment-relatedcritical events is relatively low, morbidity associ-ated with such events can be quite high. Humanerror is the leading contributor to equipmentrelated problems, and is typically magnitudesgreater than pure equipment failure, which itself israre.3,4 The implication, of course, is that we needgreater training and facility with our equipment asrecognized by leading authorities.3,5,6
The APSF Committee on Technology was chal-lenged to consider the adequacy of pre-use instruc-tion when Dr. Michael Cox asked the Dear SIRScolumn to “suggest how I might propose to ourgroup changing our approach” to a more organizedand formal instructional program.7 Cox described hisperception of inadequate training and ability to trou-bleshoot newly installed anesthesia machines, evenafter an 18-month period. Although APSF represen-tatives argued that 1) a local champion for trainingwas essential to overall satisfaction, 2) institutionalsupport for training be provided, 3) the manufactur-ers develop educational programs that far exceedcurrent standards, and 4) manufacturers must play acrucial role with continuing after-the-sale support,APSF neglected to demonstrate how those elementscould actually succeed, and probably ignored thekey element: participation of the clinical staff.
Concurrently, the Corporate Advisory Councilof the APSF discussed and summarily expressedindustry’s frustration with the inability to enforcethe training of anesthesia clinicians, and physicians
Challenges Ahead in Technology Training:A Report on the Training Initiative of the Committee on Technology
See “Training,” Next Page
APSF NEWSLETTER Fall 2006 PAGE 44
“less desirable” off-site locations that did not have thenew machine, or they were left unassigned with nega-tive financial consequences. Such affected individualsquickly sought training once the negative conse-quences were realized. The Chair further described ahighly receptive CRNA staff, as well as cases of “purearrogance” and antipathy by several anesthesiologists,some of whom initially refused to be trained.
Design of a Mandated APSF Pilot Program
Developing consensus. The authors of the pilottraining program (MAO, BR, AA) from the APSFagreed that initial consensus would have to beachieved among the key advocates for change.Wake Forest University Health Sciences was chosenas the test site for the program. The authors metwith the Wake Forest University Health SciencesVice President for Operations, the Director for Sur-gical Services, the Director of the Surgical ServicesAcademy, Chief CRNAs, Chair of the Nurse Anes-thesia Training Program, Chief of Surgery, RiskManagement officers, Residency Training ProgramDirector, and the Chairman of the Department ofAnesthesiology. All were informed of backgroundinformation and the intended scope of developing amodel, mandated training program for the antici-pated introduction of new and advanced anesthesiamachines. Universally, these institutional leadersfelt that additional machine training would be valu-able. In trying to develop consensus, however, theissues which were difficult to resolve included
1. demands for proof that training was necessary
2. establishment of baseline practices
3. convincing the community that this special pro-gram was valuable
4. convincing, specifically, staff anesthesiologiststhat the program was necessary
5. concurrent development of refresher courses
6. ability to accomplish training of 195 individualsprior to machine use
7. supportive statements from regulatory bodies(JCAHO or the ASA)
8. ability to simplify training (e.g., online pro-grams?)
9. determining the consequences of a refusal orfailure to participate
10. provision of appropriate amounts of time andresources
11. measuring the outcome and value of the train-ing process
12. approaching the mandate through positive ornegative reinforcement
13. training significant numbers of random newhires.
Mandating the training. The most difficultobstacle was the method for mandating the pro-gram to so many different categories of clinicians.The student nurse anesthetists were easily directedinto the machine training modules as they wouldbe for other subject modules, and these were orga-nized into their classroom schedule. The residentswere informed by their Program Director that thetraining was a mandatory part of their curriculum,but with a less-than-structured environment, theywere expected to attend some of these modulesindependently. The Chief CRNAs instructed theiremployees to attend the sessions, the employeesreceived continuing education credits, and theywere typically provided relief from clinical duty byadditional CRNA clinical coverage. The facultywere initially informed of the planned training pro-gram, with an expectation from the training pro-gram director (MAO) that they would participate.
In a series of memos leading up to the training,the 4 groups were informed by the training pro-gram director that the program would be manda-tory, but the final detailed memo simply describedthe program and stated that the machines wouldnot be installed until all clinicians had completedtraining. The reason for the hesitation emanatedfrom discussions between the training programdirector and the Department Chair, and the resul-tant decision by the Chair to use a process ofencouragement, advertisement, individual judg-ment, and certificates of completion to achieve suc-cess, particularly in regard to faculty members. Theother 3 groups had their own respective leaderswho communicated a relative mandate. Thus, theChair remained silent on the issue and did not com-municate with any of the staff on this topic, norwere any punitive consequences for missing thetraining ever announced to any group.
Program content. The training program wasdesigned to extend over a 2-month period and con-tained 4 structured components: 1) a 60-minute lec-ture, repeated twice, with slides available on theDepartment intranet, 2) a 60-minute hands-onworkshop led by the manufacturer’s technician, aswaves of clinicians attended 9 machine stations, 3) apre-programmed, 30-minute clinical simulationapplication, which included functional trou-bleshooting, and 4) a formative assessment tool (or“test”) containing 40 questions derived from themanufacturer’s user manual. A fifth, unstructuredcomponent was the independent reading of theuser’s manual posted on the intranet.
Go live. After 2 months was allowed for partici-pants to complete the 4-stage program, themachines were installed for clinical use. Two manu-facturer’s clinical applications specialists were onhand for a total of 5 days to assist the clinicians, but
they were generally not called upon. Several fol-low-up announcements were made to encourage allto complete the 4 stages for awarding of a Certifi-cate of completion.
Results of Implementing theProgram
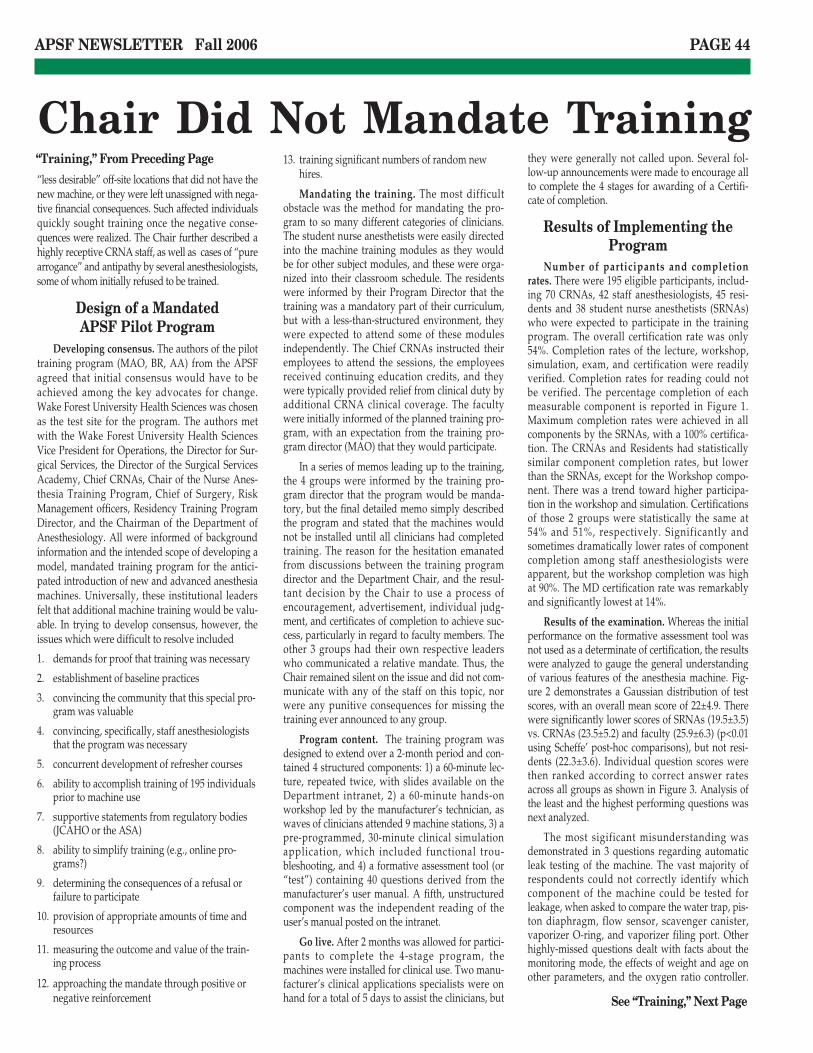
Number of participants and completionrates. There were 195 eligible participants, includ-ing 70 CRNAs, 42 staff anesthesiologists, 45 resi-dents and 38 student nurse anesthetists (SRNAs)who were expected to participate in the trainingprogram. The overall certification rate was only54%. Completion rates of the lecture, workshop,simulation, exam, and certification were readilyverified. Completion rates for reading could notbe verified. The percentage completion of eachmeasurable component is reported in Figure 1.Maximum completion rates were achieved in allcomponents by the SRNAs, with a 100% certifica-tion. The CRNAs and Residents had statisticallysimilar component completion rates, but lowerthan the SRNAs, except for the Workshop compo-nent. There was a trend toward higher participa-tion in the workshop and simulation. Certificationsof those 2 groups were statistically the same at54% and 51%, respectively. Significantly andsometimes dramatically lower rates of componentcompletion among staff anesthesiologists wereapparent, but the workshop completion was highat 90%. The MD certification rate was remarkablyand significantly lowest at 14%.
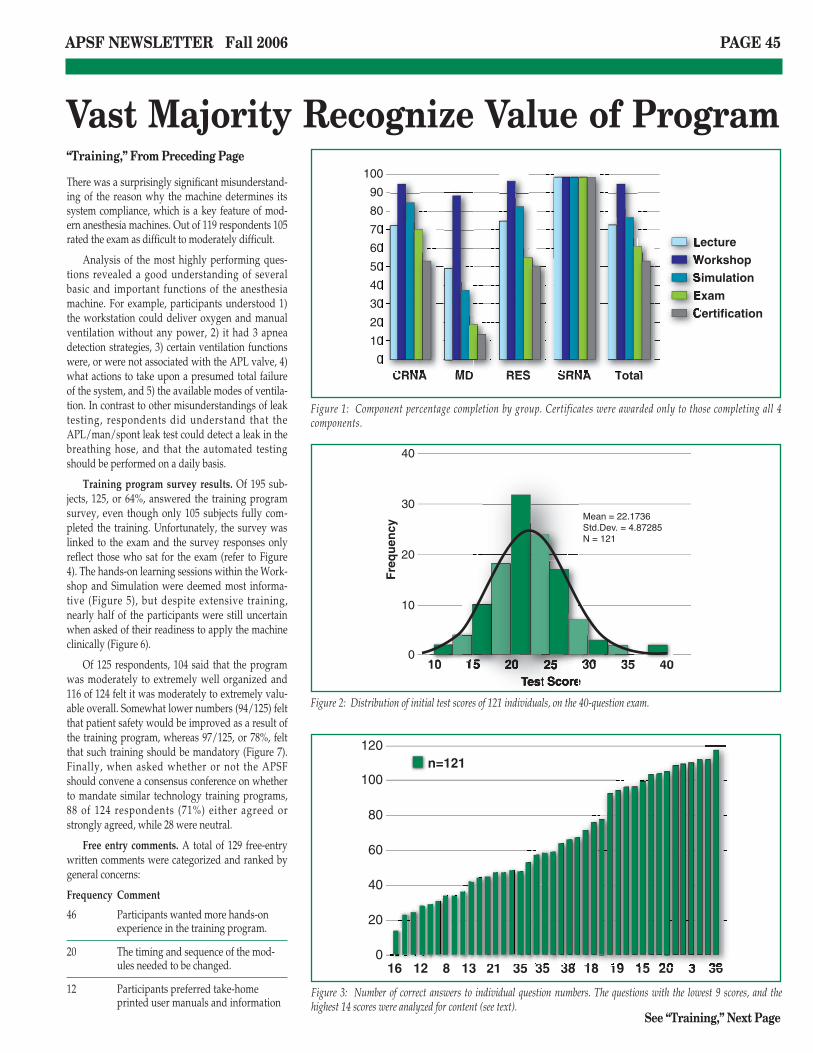
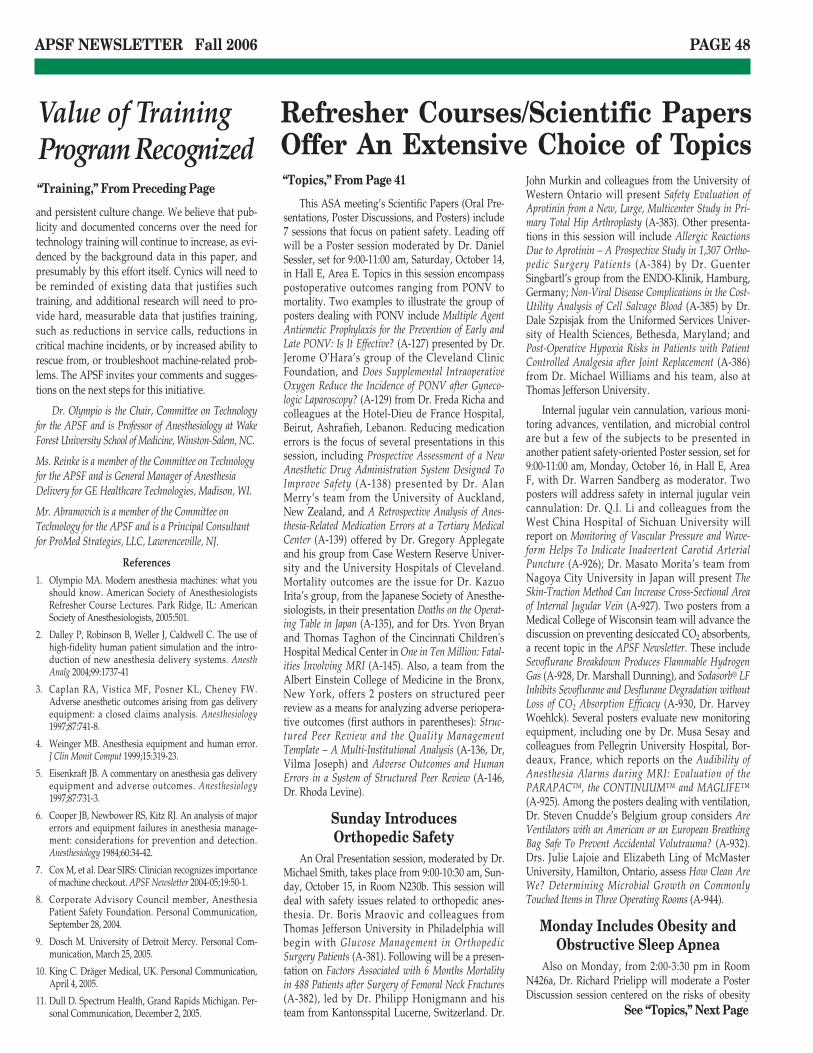
Results of the examination. Whereas the initialperformance on the formative assessment tool wasnot used as a determinate of certification, the resultswere analyzed to gauge the general understandingof various features of the anesthesia machine. Fig-ure 2 demonstrates a Gaussian distribution of testscores, with an overall mean score of 22±4.9. Therewere significantly lower scores of SRNAs (19.5±3.5)vs. CRNAs (23.5±5.2) and faculty (25.9±6.3) (p<0.01using Scheffe’ post-hoc comparisons), but not resi-dents (22.3±3.6). Individual question scores werethen ranked according to correct answer ratesacross all groups as shown in Figure 3. Analysis ofthe least and the highest performing questions wasnext analyzed.
The most sigificant misunderstanding wasdemonstrated in 3 questions regarding automaticleak testing of the machine. The vast majority ofrespondents could not correctly identify whichcomponent of the machine could be tested forleakage, when asked to compare the water trap, pis-ton diaphragm, flow sensor, scavenger canister,vaporizer O-ring, and vaporizer filing port. Otherhighly-missed questions dealt with facts about themonitoring mode, the effects of weight and age onother parameters, and the oxygen ratio controller.
Chair Did Not Mandate Training
See “Training,” Next Page
“Training,” From Preceding Page
APSF NEWSLETTER Fall 2006 PAGE 45
There was a surprisingly significant misunderstand-ing of the reason why the machine determines itssystem compliance, which is a key feature of mod-ern anesthesia machines. Out of 119 respondents 105rated the exam as difficult to moderately difficult.
Analysis of the most highly performing ques-tions revealed a good understanding of severalbasic and important functions of the anesthesiamachine. For example, participants understood 1)the workstation could deliver oxygen and manualventilation without any power, 2) it had 3 apneadetection strategies, 3) certain ventilation functionswere, or were not associated with the APL valve, 4)what actions to take upon a presumed total failureof the system, and 5) the available modes of ventila-tion. In contrast to other misunderstandings of leaktesting, respondents did understand that theAPL/man/spont leak test could detect a leak in thebreathing hose, and that the automated testingshould be performed on a daily basis.
Training program survey results. Of 195 sub-jects, 125, or 64%, answered the training programsurvey, even though only 105 subjects fully com-pleted the training. Unfortunately, the survey waslinked to the exam and the survey responses onlyreflect those who sat for the exam (refer to Figure4). The hands-on learning sessions within the Work-shop and Simulation were deemed most informa-tive (Figure 5), but despite extensive training,nearly half of the participants were still uncertainwhen asked of their readiness to apply the machineclinically (Figure 6).
Of 125 respondents, 104 said that the programwas moderately to extremely well organized and116 of 124 felt it was moderately to extremely valu-able overall. Somewhat lower numbers (94/125) feltthat patient safety would be improved as a result ofthe training program, whereas 97/125, or 78%, feltthat such training should be mandatory (Figure 7).Finally, when asked whether or not the APSFshould convene a consensus conference on whetherto mandate similar technology training programs,88 of 124 respondents (71%) either agreed orstrongly agreed, while 28 were neutral.
Free entry comments. A total of 129 free-entrywritten comments were categorized and ranked bygeneral concerns:
Frequency Comment
46 Participants wanted more hands-onexperience in the training program.
20 The timing and sequence of the mod-ules needed to be changed.
12 Participants preferred take-homeprinted user manuals and information
Vast Majority Recognize Value of Program
See “Training,” Next Page
“Training,” From Preceding Page 1009080706050403020100
CRNA MD RES SRNA Total
Lecture
Workshop
Simulation
Exam
Certification
10
20
30
40
010 15 20 25 30 35 40
Test Score
Fre
qu
ency
120100806040200
16 12 8 13 21 35 35 38 18 19 15 20 3 36
n=121
Figure 1: Component percentage completion by group. Certificates were awarded only to those completing all 4components.
Figure 2: Distribution of initial test scores of 121 individuals, on the 40-question exam.
Figure 3: Number of correct answers to individual question numbers. The questions with the lowest 9 scores, and thehighest 14 scores were analyzed for content (see text).

APSF NEWSLETTER Fall 2006 PAGE 46
as opposed to the on-line referencematerials.
11 Participants preferred on-site clinicaltraining with an experienced factoryrepresentative during actual clinicalcare.
11 Respondents advised that the programfocus on key points.
An overwhelming majority of the commentsindicated that participants wanted more hands-onexperience with the machine, and this is consistentwith their selected preference for the workshop andsimulation learning modules. Similarly, the detailsbehind timing and sequencing indicated that stu-dents wanted a much more concentrated effort ofhands-on learning, ideally located in the OR-envi-ronment for easy accessibility during breaks, oreven training in the clinical setting. They felt thatlectures and exam review should follow the hands-on sessions (and they did, after the survey wascompleted). Many stated that they could not under-stand nor remember the details within the early-phase lecture, having never seen the machine.
ConclusionsAn overwhelming effort to justify, to organize,
and to accomplish a comprehensive mandatorytechnology training program, prior to the installa-tion of a profoundly modern and unfamiliar anes-thesia machine, was a real challenge on manydifferent levels.
The biggest failure of intent was to NOT man-date the program for all categories of clinicians whowould be responsible for using the equipment uponinstallation. It was the authors’ impression (andlater confirmed) that this omission of the Chair-man’s mandate for staff anesthesiologists to com-plete the program was based upon a perceived lackof realistic and enforceable consequences for non-participation. Staff anesthesiologists in academicsettings, at least, are notoriously independent-minded and perhaps drawn to the academic envi-ronment by the promise of freedom of expression,and freedom of learning and specialization. Manywere simply not interested in learning the intrica-cies of the machine, and felt confident that theycould apply the machine with minimal training.Our institution does not routinely provide primarystaff-administered anesthesia, but rather staff-directed care, which could have made such trainingseem unnecessary. Similarly, mediocre (but muchhigher) certification rates of completion by residentsand CRNAs may have been secondary to the lack ofenforceable or threatened sanctions against thosewho did not complete the training.
Faculty Need Strong Motivation for Training Participation
See “Training,” Next Page
“Training,” From Preceding Page 100
80
60
40
20
0
CRNA
Number ofParticipants
in EachCategory
MD RES SRNA
Total
Survey
Exam
102030405060
0Lect Read Wkshp SimApp Exam
n=125
Number ofParticipants
102030405060
0Strongly
AgreeAgree Neutral Disagree Strongly
Disagree
n=125
Number ofParticipants
Figure 4: Survey and exam completion by group. Total refers to the number of individuals in each group. Note that thesurvey and exam participation are close in all groups, except that more faculty answered the survey (14) than answeredthe exam questions (8).
Figure 5: When asked which component they learned the most from, participants overwhelmingly chose the hands-onapplications in the workshop and simulation lab.
Figure 6: Participants demonstrated some reluctance when asked if they were ready to use the anesthesia machine, follow-ing all 4 components of training.

APSF NEWSLETTER Fall 2006 PAGE 47
the faculty in the workshop session speaks tohands-on training, but this preference is not sup-ported by their 38% participation in simulation.
It is not surprising, and rather gratifying that100% completion was obtained by the SRNAs, as thisparticular program is highly regarded for its quality,its rigor, its regimentation, and assertive leadership.Highly motivated students in a classroom-assign-ment system are unlikely to miss a mandated assign-ment by their Chair, presumably because ofperceived or actual severe negative consequences.
Is it possible, preferable, or incumbent uponother clinicians in anesthesiology to demonstratesimilar adherence to recommended training? Per-haps a cultural difference of more independent-minded practitioners, and even residents, needs to
be addressed. We don’t think that a lack of oppor-tunity to attend was the reason, but maybe the lackof “assignment structure” particularly among resi-dents and faculty, was a problem.
The next obvious failure of the training pro-gram was the low score on the formative assess-ment tool (which was reviewed and corrected afterthe initial grading). Despite what was considered tobe a heroic effort at training, a high percentage ofcorrect answers was not obtained. Although the testwas difficult and detailed, and designed to distin-guish variations in knowledge content, it was dis-appointing to see the low scores after such anintense amount of effort.
We also did not measure machine-applicationcapabilities in simulation, following the training,primarily because this project was NOT designed asan outcome study, but rather as a trial to test ourability to implement wide-scale training of a largegroup of clinicians, and to gather their perspectiveson that training. We already believed that simula-tion training would improve application of themachine, and ultimately patient safety, as it did inthe Dalley study.2
What did succeed in this pilot program was agreat deal of enthusiasm and broad participation inat least some of the components of training, and welearned that an overwhelming number of cliniciansfelt the training was valuable and would improvepatient safety. They made a number of consistentand constructive suggestions to improve the train-ing by making it more clinically focused, more suc-cinct, and with greater time spent on applicationstraining. We know that at least 50% of the entiregroup (97/195) felt such training should be manda-tory, whereas 91% of all respondents felt it shouldbe mandated (97/125).
The impediments to mandating this trainingstill remain, and will probably require a consistent
On the other hand, one would expect academicfaculty, at least, to understand and appreciate thesignificant literature on failures of human training,and the high rates of human error in the applicationof complex machines.4 Furthermore, the obligation offaculty to intervene in situations of sudden machinefailure is obvious, but apparently did not enhancethe faculty completion rate. Recent national empha-sis on patient safety, and documentation of capabil-ity and performance both within the ABA and theACGME, should be widely known by academic fac-ulty. Perhaps the negative motivational factors listedabove need to be overcome by negative consequen-tial mandates from the Chairman, if indeed suchtraining is deemed important for patient safety. Atleast one private hospital Chair (described above)had success in mandating training through the actu-alization of a threat to disallow preferred practiceassignments. It seems clear in this pilot program, andwith other evidence above, that the motivational“carrot” and certification was rejected for lack ofenforcement, and that a top-down mandate is essen-tial to accomplish such training.
The positive consequential mandates given tothe CRNAs and the residents (including a certificateand CE credits), were still an inadequate means ofaccomplishing a high certification rate. There wereno threats and no sanctions made by their supervi-sory personnel for a failure to certify. Regardless,there was a heroic effort and enthusiasm, particu-larly among the CRNAs and their leadership, tosecure all 70 individuals to participate. Further-more, there were high completion rates of theactive-learning modules that adult learners typi-cally find most interesting. The 90% participation of
Top-Down Mandate Effective For Student Nurse Anesthetists
102030405060
0Strongly
AgreeAgree Neutral Disagree Strongly
Disagree
n=125
Number ofParticipants
Figure 7: When asked if such training programs should be mandatory, 97 out of 125 (78%) either agreed or stronglyagreed.
“Training,” From Preceding Page
The following is a commentary andinsight from Dr. Raymond Roy pertainingto the decision not to mandate faculty par-ticipation in this study:
In the project development phase Dr. Olym-pio and I openly discussed the pros and cons ofvarious roles I could play as department chair.Despite Dr. Olympio’s prediction of poor compli-ance without strong top-down pressure, I chose totreat this proposal as a routine clinical study, i.e., Iendorsed it but did not mandate participation.Ironically, my decision enabled a clear demon-stration of what not to do. I am pleased with thestudy, but disappointed in the outcome.
Is it a faculty member’s fault for not doingwhat is right and for not being a good role modelfor residents and CRNAs? Is it the principal inves-tigator’s fault for not “selling the project” wellenough? Or is it the chair’s fault for not champi-oning the cause? Human nature being what it is, Iconsider it primarily a leadership issue. I hope tobe presented with a similar proposal in the future.
Armed now with real data I would view the pro-ject, not as a clinical study, but as a major depart-mental safety initiative. I would aggressively seekbuy-in prospectively from the faculty and shep-herd the project to completion. Faculty memberswho fail to receive their certificates by a certaintime would not be assigned clinically until theydid so. This penalty would create significant peerpressure. If that was not enough, it would havefinancial consequences related to a failure toacquire the requisite number of clinical serviceunits. And if that was not enough, it could ulti-mately affect recredentialing and the employmentcontract. What private or academic anesthesiagroup really wants to recruit an anesthesiologist,anesthesia resident, CRNA, SRNA, or AA whorefused to participate in a mutually agreed uponsafety initiative?
Raymond C. Roy, PhD, MDProfessor and Chair of AnesthesiologyWake Forest University School of [email protected] See “Training,” Next Page
APSF NEWSLETTER Fall 2006 PAGE 48
Refresher Courses/Scientific PapersOffer An Extensive Choice of Topics
This ASA meeting’s Scientific Papers (Oral Pre-sentations, Poster Discussions, and Posters) include7 sessions that focus on patient safety. Leading offwill be a Poster session moderated by Dr. DanielSessler, set for 9:00-11:00 am, Saturday, October 14,in Hall E, Area E. Topics in this session encompasspostoperative outcomes ranging from PONV tomortality. Two examples to illustrate the group ofposters dealing with PONV include Multiple AgentAntiemetic Prophylaxis for the Prevention of Early andLate PONV: Is It Effective? (A-127) presented by Dr.Jerome O'Hara’s group of the Cleveland ClinicFoundation, and Does Supplemental IntraoperativeOxygen Reduce the Incidence of PONV after Gyneco-logic Laparoscopy? (A-129) from Dr. Freda Richa andcolleagues at the Hotel-Dieu de France Hospital,Beirut, Ashrafieh, Lebanon. Reducing medicationerrors is the focus of several presentations in thissession, including Prospective Assessment of a NewAnesthetic Drug Administration System Designed ToImprove Safety (A-138) presented by Dr. AlanMerry’s team from the University of Auckland,New Zealand, and A Retrospective Analysis of Anes-thesia-Related Medication Errors at a Tertiary MedicalCenter (A-139) offered by Dr. Gregory Applegateand his group from Case Western Reserve Univer-sity and the University Hospitals of Cleveland.Mortality outcomes are the issue for Dr. KazuoIrita’s group, from the Japanese Society of Anesthe-siologists, in their presentation Deaths on the Operat-ing Table in Japan (A-135), and for Drs. Yvon Bryanand Thomas Taghon of the Cincinnati Children'sHospital Medical Center in One in Ten Million: Fatal-ities Involving MRI (A-145). Also, a team from theAlbert Einstein College of Medicine in the Bronx,New York, offers 2 posters on structured peerreview as a means for analyzing adverse periopera-tive outcomes (first authors in parentheses): Struc-tured Peer Review and the Quality ManagementTemplate – A Multi-Institutional Analysis (A-136, Dr,Vilma Joseph) and Adverse Outcomes and HumanErrors in a System of Structured Peer Review (A-146,Dr. Rhoda Levine).
Sunday Introduces Orthopedic Safety
An Oral Presentation session, moderated by Dr.Michael Smith, takes place from 9:00-10:30 am, Sun-day, October 15, in Room N230b. This session willdeal with safety issues related to orthopedic anes-thesia. Dr. Boris Mraovic and colleagues fromThomas Jefferson University in Philadelphia willbegin with Glucose Management in OrthopedicSurgery Patients (A-381). Following will be a presen-tation on Factors Associated with 6 Months Mortalityin 488 Patients after Surgery of Femoral Neck Fractures(A-382), led by Dr. Philipp Honigmann and histeam from Kantonsspital Lucerne, Switzerland. Dr.
John Murkin and colleagues from the University ofWestern Ontario will present Safety Evaluation ofAprotinin from a New, Large, Multicenter Study in Pri-mary Total Hip Arthroplasty (A-383). Other presenta-tions in this session will include Allergic ReactionsDue to Aprotinin – A Prospective Study in 1,307 Ortho-pedic Surgery Patients (A-384) by Dr. GuenterSingbartl’s group from the ENDO-Klinik, Hamburg,Germany; Non-Viral Disease Complications in the Cost-Utility Analysis of Cell Salvage Blood (A-385) by Dr.Dale Szpisjak from the Uniformed Services Univer-sity of Health Sciences, Bethesda, Maryland; andPost-Operative Hypoxia Risks in Patients with PatientControlled Analgesia after Joint Replacement (A-386)from Dr. Michael Williams and his team, also atThomas Jefferson University.
Internal jugular vein cannulation, various moni-toring advances, ventilation, and microbial controlare but a few of the subjects to be presented inanother patient safety-oriented Poster session, set for9:00-11:00 am, Monday, October 16, in Hall E, AreaF, with Dr. Warren Sandberg as moderator. Twoposters will address safety in internal jugular veincannulation: Dr. Q.I. Li and colleagues from theWest China Hospital of Sichuan University willreport on Monitoring of Vascular Pressure and Wave-form Helps To Indicate Inadvertent Carotid ArterialPuncture (A-926); Dr. Masato Morita’s team fromNagoya City University in Japan will present TheSkin-Traction Method Can Increase Cross-Sectional Areaof Internal Jugular Vein (A-927). Two posters from aMedical College of Wisconsin team will advance thediscussion on preventing desiccated CO2 absorbents,a recent topic in the APSF Newsletter. These includeSevoflurane Breakdown Produces Flammable HydrogenGas (A-928, Dr. Marshall Dunning), and Sodasorb® LFInhibits Sevoflurane and Desflurane Degradation withoutLoss of CO2 Absorption Efficacy (A-930, Dr. HarveyWoehlck). Several posters evaluate new monitoringequipment, including one by Dr. Musa Sesay andcolleagues from Pellegrin University Hospital, Bor-deaux, France, which reports on the Audibility ofAnesthesia Alarms during MRI: Evaluation of thePARAPAC™, the CONTINUUM™ and MAGLIFE™(A-925). Among the posters dealing with ventilation,Dr. Steven Cnudde’s Belgium group considers AreVentilators with an American or an European BreathingBag Safe To Prevent Accidental Volutrauma? (A-932).Drs. Julie Lajoie and Elizabeth Ling of McMasterUniversity, Hamilton, Ontario, assess How Clean AreWe? Determining Microbial Growth on CommonlyTouched Items in Three Operating Rooms (A-944).
Monday Includes Obesity andObstructive Sleep Apnea
Also on Monday, from 2:00-3:30 pm in RoomN426a, Dr. Richard Prielipp will moderate a PosterDiscussion session centered on the risks of obesity
See “Topics,” Next Page
“Topics,” From Page 41
and persistent culture change. We believe that pub-licity and documented concerns over the need fortechnology training will continue to increase, as evi-denced by the background data in this paper, andpresumably by this effort itself. Cynics will need tobe reminded of existing data that justifies suchtraining, and additional research will need to pro-vide hard, measurable data that justifies training,such as reductions in service calls, reductions incritical machine incidents, or by increased ability torescue from, or troubleshoot machine-related prob-lems. The APSF invites your comments and sugges-tions on the next steps for this initiative.
Dr. Olympio is the Chair, Committee on Technologyfor the APSF and is Professor of Anesthesiology at WakeForest University School of Medicine, Winston-Salem, NC.
Ms. Reinke is a member of the Committee on Technologyfor the APSF and is General Manager of AnesthesiaDelivery for GE Healthcare Technologies, Madison, WI.
Mr. Abramovich is a member of the Committee onTechnology for the APSF and is a Principal Consultantfor ProMed Strategies, LLC, Lawrenceville, NJ.
References1. Olympio MA. Modern anesthesia machines: what you
should know. American Society of AnesthesiologistsRefresher Course Lectures. Park Ridge, IL: AmericanSociety of Anesthesiologists, 2005:501.
2. Dalley P, Robinson B, Weller J, Caldwell C. The use ofhigh-fidelity human patient simulation and the intro-duction of new anesthesia delivery systems. AnesthAnalg 2004;99:1737-41
3. Caplan RA, Vistica MF, Posner KL, Cheney FW.Adverse anesthetic outcomes arising from gas deliveryequipment: a closed claims analysis. Anesthesiology1997;87:741-8.
4. Weinger MB. Anesthesia equipment and human error.J Clin Monit Comput 1999;15:319-23.
5. Eisenkraft JB. A commentary on anesthesia gas deliveryequipment and adverse outcomes. Anesthesiology1997;87:731-3.
6. Cooper JB, Newbower RS, Kitz RJ. An analysis of majorerrors and equipment failures in anesthesia manage-ment: considerations for prevention and detection.Anesthesiology 1984;60:34-42.
7. Cox M, et al. Dear SIRS: Clinician recognizes importanceof machine checkout. APSF Newsletter 2004-05;19:50-1.
8. Corporate Advisory Council member, AnesthesiaPatient Safety Foundation. Personal Communication,September 28, 2004.
9. Dosch M. University of Detroit Mercy. Personal Com-munication, March 25, 2005.
10. King C. Dräger Medical, UK. Personal Communication,April 4, 2005.
11. Dull D. Spectrum Health, Grand Rapids Michigan. Per-sonal Communication, December 2, 2005.
Value of TrainingProgram Recognized“Training,” From Preceding Page

APSF NEWSLETTER Fall 2006 PAGE 49
Study of Complications, Incidence and Predictive Fac-tors of Difficult Mask Ventilation (A-1687). Dr.Mohammad Maroof and his team from the Univer-sity of North Carolina at Chapel Hill will discusshow the Ambu Laryngeal Mask Is a Better Alternativeto Tracheal Extubation as Compared to LMA Classic (A-1688). Dr. Masami Yamazato and colleagues fromthe University of the Ryukyus in Okinawa, Japan,will present Bronchofiber-View Assist NasotrachealIntubation Technique Can Dramatically Reduce NasalTrauma (A-1696). Dr. Jong Seok Lee and his groupat Yonsei University College of Medicine in Seoul,Korea, report a case of Hypoglossal Nerve Injury Fol-lowing the Use of the CobraPLA™ (A-1698). Roundingout this session is a miscellany of posters on suchsubjects as acute intraoperative events and seda-tion. These include The Effect of IntramedullaryDecompression in Preventing Bone Marrow Embolismduring THA (A-1679) delivered by Dr. MasakiTakashina and colleagues from Osaka UniversityHospital, Japan, and a Retrospective Evaluation ofEfficacy and Safety of Emergency Room Sedation inPediatric Patients (A-1695) from Dr. Tricia Meyer’steam of the Scott and White Healthcare System,Temple, Texas.
This year’s annual ASA Meeting promises to bean exciting series of lectures, presentations, and dis-cussions replete with information, ideas, and foodfor thought. Patient safety again plays a major role.Please check out the ASA website and meeting pro-gram for a complete list of topics and schedules.
Dr. Somerville is a Research Administrative Coordinatorin the Department of Public Health Sciences at WakeForest University School of Medicine.
Dr. Morell is the Editor of this publication, ClinicalAssociate Professor of Anesthesiology, Wake ForestUniversity School of Medicine, Adjunct ClinicalAssociate Professor of Anesthesiology, University ofFlorida, and a private practice anesthesiologist living inNiceville, FL.
Electronic Medical RecordsSafety in electronic medical records will be the
theme of a Poster Discussion session set for 1:30-3:00 pm on Tuesday, October 17, in Room N426a,with Dr. Robert Johnstone moderating. Two reportsfrom Dr. Michael Vigoda and colleagues from theUniversity of Miami highlight beta blockade issues:Anesthesia Information System Shows Inadequate Intra-operative Beta Blockade in Patients with CAD (A-1376)and Intraoperative Beta Blocker Use Doesn't Changewith Electronic Reminder of Patients' Cardiac Status(A-1377). Dr. Fabian Kooij and his team from theOnze Lieve Vrouwe Gasthuis/Academical MedicalCenter, Amsterdam, Netherlands, will present Deci-sion Support System Increases Data Quality on Preoper-ative Record (A-1378). "Risky Business" in the OR: ASurvey of Anesthesia Information System Policy Deci-sions (A-1379) is the topic for Dr. Richard Epstein’sgroup from Jefferson Medical College. Dr. AlfredPinchak and his team from CWRU-MetrohealthMedical Center in Cleveland, Ohio, will report onAutomating the Analysis of Physiological Data fromComputerized Anesthesia Records (A-1380). Antibioticadministration is the issue in 2 presentations: aVanderbilt team lead by Dr. Paul St. Jacques willexamine the Effect of an Automated Antibiotic Promptas Part of an Integrated Perioperative Informatics Sys-tem (A-1381); Improved Compliance with AntibioticGuidelines with Implementation of an Electronic VisualReminder (A-1382) will be presented by Dr. DavidWax’s group from the Mount Sinai School of Medi-cine in New York. Dr. Warren Sandberg and col-leagues from Massachusetts General Hospital inBoston will offer recommendations for ImprovingDocumentation Quality with Automated AnesthesiaInformation Management (A-1383).
Airway management issues predominate in aPoster session scheduled for 9:00-11:00 am,Wednesday, October 18, in Hall E, Area E, andmoderated by Dr. Joan Christie. A sampling ofposters on that topic includes one by Dr. Anne-Marie Cros and her group from the Pellegrin Uni-versity Hospital, Bordeaux, France, titled Prospective
and obstructive sleep apnea. Four sessions will con-cern obesity: Dr. Ashish Sinha’s group from theUniversity of Pennsylvania will present Evaluating aRisk Assessment Tool in Morbidly Obese PatientsUndergoing Gastric Bypass Surgery (A-987); Dr. JamesBlum and his team from the University of Michiganwill consider both The Risk of Quality AssuranceEvents in 116,035 Patients Based on Body Mass Index(A-989) and The Risk of NSQIP Postoperative Compli-cations with Increasing BMI (A-990); Dr. Lois Con-nolly and colleagues from the Medical College ofWisconsin will address how Increases in Body MassIndex Correlate to Increasing Perioperative Event (A-992). Four other presentations investigate sleepapnea. Three of those come from a University ofToronto team: Should Surgical Patients with DifficultIntubation Be Referred to Sleep Clinic for Polysomnogra-phy? (A-986, Dr. Frances Chung); What Is the BestPreop Screening Tool for Surgical Patients withObstructive Sleep Apnea (OSA)?(A-991, Dr. Chung);and OSA Questionnaire: A New Short-Form ScreeningTool for Obstructive Sleep Apnea (OSA) Patients (A-993, Dr. Balaji Yegneswaran). Also, Dr. KevinFinkel’s group from Washington University in St.Louis will present Obstructive Sleep Apnea: The SilentPandemic (A-988).
Another Poster session, moderated by Dr. Dex-ter Franklin, is scheduled for 9:00-11:00 am, Tues-day, October 17, in Hall E, Area D. Here themajority of posters will analyze patient flowthrough the OR system. While patient safety isimplicitly central to this topic, a number of postersin this session stand out for specifically addressingsafety-related concerns in the OR and other clinicsettings. For example, Drs. Paul Barach andJonathan Wilverding of the University of Miamiexplore a standardized “hand-off” system for trans-ferring patients between hospital areas, such asfrom the ER to the ICU, in Assessing and ImprovingCommunication of Patient Care Information in CriticalCare Settings (A-1291). Drs. Jon Halling and Alexan-der Gutkin of the Ochsner Clinic Foundation inNew Orleans, in One Hospital's Response to a MassDisaster – Lessons and Thoughts (A-1304), summarizethe response of that institution, and particularlytheir Department of Anesthesiology to HurricaneKatrina, including preplanning, disaster manage-ment, a discussion of areas for improvement downthe road, and the status of the recovery of thehealthcare infrastructure in New Orleans. Also inthis session, Dr. Thierry Girard and colleagues fromthe University of Basel, Switzerland, address thepresent and future of testing for malignant hyper-thermia in Can We Improve on Phenotyping for Malig-nant Hyperthermia? (A-1309) and How Accurate IsTesting for Malignant Hyperthermia? (A-1310).
Poster Session Highlights Airway Management“Topics,” From Preceding Page
Be sure to check out the APSF Booth in the Exhibit Hall atthe 2006 ASA Meeting in Chicago, IL, October 14-18, 2006.
There you can
☛ Meet APSF Leaders/Representatives
☛ Make a Donation
☛ See Current and Prior Issues of the APSF Newsletter

APSF NEWSLETTER Fall 2006 PAGE 50
Dear SIRS:I am medical director of a free-standing surgery
center. One of our anesthesia machines has a non-functioning O2 sensor. We have an older OhmedaExcel 110. Our biomedical person claims the sensorbox would be impossible to replace. He said sincewe monitor O2 on our end-tidal/agent analyzer, thiswould satisfy O2 monitoring requirements. Is he cor-rect, or do we need the inline O2 sensor?
Thank you,Michael Nakata, MD
In Response:The anesthesia machine standard of 1979, as well
as the anesthesia workstation standards of 1988 and2000 (I chaired the committees that wrote the latter2) required an "in-line" O2 analyzer. It was our beliefthat the analyzer was the last line of defense againsta machine-generated hypoxic mixture, and further,would alarm sooner than an expired gas monitor. Ihope I have been of some help.
Sincerely,Stanley Weitzner, MD
Editors’ Note:
ASTM F-1161 was published in 1989, but hassince been withdrawn and replaced by ASTM F-1850. The relevant requirements from ASTM F-1850-00 are as follows:
Clause 51.11.1 The ANESTHESIA WORKSTA-TION shall be provided with an oxygen monitor incompliance with Specification F 1462 for measure-ment of the O2 concentration in the inspiratory limbor the Y-piece, or the manufacturer(s) of the ANES-THESIA GAS SUPPLY DEVICE and ANESTHESIABREATHING SYSTEM shall state in the accompany-ing documents that such a means is required.
51.8.2.1 Automatic Enabling - Means shall beprovided that the monitor and alarms mentioned inclauses 51.9.3 (breathing system pressure), and 51.11(oxygen concentration) shall be in the enabled con-dition and functioning automatically whenever theanesthesia gas supply device is in use. . . .
Dr. Olympio
In Response:The important aspect here is not where the O2 is
measured or by what, but rather that the O2 mea-surement is activated when the anesthesia machineis turned on. There are numerous reports from his-tory where stand-alone monitors for parameterswere available on the machine, but the incidentoccurred nonetheless because the user had forgot-ten to turn the device on or had not realized that thealarms were disabled.
In our view the O2 measurement should bechecked during the machine startup and should beautomatically activated on power-up of the machine.It should also have the same battery support time asthe gas machine.
Robert ClarkCareArea DirectorPerioperative CareDräger Medical, Inc.Telford, PA USA
In Response:The role of the O2 analyzer is to assess the
"machine"—not solely the patient. Both machine andpatient monitoring could be accomplished with aside-stream gas analyzer positioned at the Y-piece, ifit is always used. When a machine complies with theworkstation standard, there are other requirementsas well. For example, monitors must be activatedwhen the machine is turned on. Therefore, it istempting, but not necessarily possible, to create theequivalent of a workstation with a handful of eBaycomponents.
To the best of my knowledge, conformance to acurrent equipment standard is not necessarilyrequired for clinical use. In fact, it is almost impossi-ble for equipment to continue to comply with con-stantly updated standards. Naturally, newequipment should comply. In this case, the oldmachine no longer complies with an old standard.The ASA’s statement on machine obsolescence maybe relevant: http://www.asahq.org/publication-sAndServices/machineobsolescense.pdf
Michael Olympio, MD, Chair of the APSF Committee on Technologyand Co-Founder of the Dear SIRS Initiative.
Dear SIRS refers to the Safety InformationResponse System. The purpose of this column is
to allow expeditious communication of technol-
ogy-related safety concerns raised by our read-
ers, with input and responses from manufacturers
and industry representatives. This process was
developed by Drs. Michael Olympio, Chair of the
Committee on Technology, and Robert Morell,
Editor of this newsletter. Dr. Olympio is oversee-
ing the column and coordinating the readers’
inquiries and the responses from industry. DearSIRS made its debut in the Spring 2004 issue.
S AFETY
I NFORMATION
R ESPONSE
S YSTEM
Is an In-line Oxygen Monitor Still Necessary?Dear SIRS
The information in this column is provided for safety-related educational purposes only, and does not constitute medical or legal advice. Individual or groupresponses are only commentary, provided for purposes of education or discussion, and are neither statements of advice nor the opinions of APSF. It is not the intention ofAPSF to provide specific medical or legal advice or to endorse any specific views or recommendations in response to the inquiries posted. In no event shall APSF beresponsible or liable, directly or indirectly, for any damage or loss caused or alleged to be caused by or in connection with the reliance on any such information.
See “Dear SIRS,” Next Page

APSF NEWSLETTER Fall 2006 PAGE 51
Oxygen Monitor Must Be TurnedOn and Have Battery Backup SUPPORT
YOURAPSF
Your Donation:
• Funds ResearchGrants
• Supports YourAPSF Newsletter
• PromotesImportant SafetyInitiatives
• FacilitatesClinician-ManufacturerInteractions
• Supports theWebsite:www.apsf.org
Please make checks payable to the APSF
and mail donations to
Anesthesia Patient Safety Foundation (APSF)520 N. Northwest HighwayPark Ridge, IL 60068-2573
This issue probably resides within the scope ofpractice standards. Is the machine otherwise safeand fit for use? Will the O2/CO2 respiratory gasmonitor always be used when the machine is used?If so, it should be OK.
Julian Goldman, MDMassachusetts General HospitalDepartments of Anesthesia and Biomedical EngineeringPresident, Society for Technology in Anesthesiawww.jgoldman.info
In Response:Before fast oxygen measurements became avail-
able as part of anesthesia gas analyzers, it was asafety requirement to monitor the O2 content in theinspiratory limb of the breathing circuit. This was arelatively slow measurement (response time of sec-onds, not milliseconds) accomplished with polaro-graphic or fuel cells. They served to detect failuresin the oxygen supply.
In my opinion, a modern gas analyzer measur-ing as close as possible to the patient's lung, namelyat the Y-piece of the circuit, does an even better job.It not only monitors the O2 content delivered to thepatient but also captures the amount of oxygen com-ing out of the lungs. This gives more informationabout oxygen delivery and it even provides a sign ofeffective ventilation.
So, I think if the anesthesia machine is not com-promised elsewhere, it should be safe to use the O2
information from the gas monitor. But of course,one must take care that the defective O2 sensor doesnot generate distractive alerts on the anesthesiamachine, thus adding risk.
Kind regards,
Dr. Siegfried KästleProject Manager R&D Patient Monitoring DivisionPhilips Medizin Systeme Böblingen GmbHHewlett-Packard-Strasse 271034 Böblingen, Germany [email protected]://www.medical.philips.com
In Response:I’d say that, no, a facility doesn’t have to main-
tain an anesthesia unit to adhere to F1850, since thatstandard applies to manufacturers of new devices.Once a device is in a facility’s inventory, that facilityhas an obligation to maintain and operate it inaccordance with current standards of care, but that’s
outside the scope of ASTM. ASA and AANA stan-dards are better guidelines for the practitioner andclinical engineer.
In his original question, Dr. Nakata pointed outthat his medical-gas monitor can measure O2 con-centrations, and I’d say that’s sufficient to meetASA/AANA requirements. When healthcare facili-ties assemble anesthesia systems (the anesthesiaunit, gas monitoring, and physiologic monitoring)from separate components, there’s almost inevitablysome overlap of monitoring function. Paying greaterattention to a monitoring function on one compo-nent at the expense of the same feature on anothercomponent isn’t unreasonable.
What’s tricky is this: How does Dr. Nakata’sfacility ensure that a) everyone knows that the anes-thesia unit’s O2 monitor is unusable and b) the gasmonitor is always present and in use? Whatevermethod he chooses, Dr. Nakata needs to make surethat the gas monitor (or other O2 monitor) is auto-matically enabled during each case and that no oneever thinks to rely on the anesthesia unit’s (nowdefunct) integrated O2-monitor. If he can’t guaran-tee this, the safer route is to replace the anesthesiaunit entirely.
Additionally, I agree strongly with 2 pointsraised by other respondents. First, as more than oneresponse pointed out, Dr. Nakata will need toensure that the problem is truly limited to an inabil-ity to monitor and/or display oxygen concentra-tions and does not extend to other functions of theanesthesia machine. Second, as Rob Clark (DrägerMedical) pointed out, the new monitoring compo-nent should be supported by battery power at leastas long as the anesthesia machine is supported (asshould any important monitoring feature).
Best regards,
Dan AltSenior Project Engineer, Health Devices GroupManager, Problem Reporting SystemECRIP: +1-610-825-6000 ext. 5445F: [email protected]
In Response:An in-line O2 sensor tells you what is coming
out of the machine. In New Jersey, it is not replacedby any other peripheral sensor.
Erv Moss, MD
“Dear SIRS,” From Preceding Page
APSF NEWSLETTER Fall 2006 PAGE 52
To the Editor:
The APSF Newsletter has devoted 2 articles to asingle case report of local anesthetic-induced cardiactoxicity after a single-injection popliteal block.1,2
Miraculously, the patient survived without signifi-cant deficit after being placed on emergency car-diopulmonary bypass (CPB).3 Many readers of thenewsletter have concluded that the risks of periph-eral nerve block are unjustified now that generalanesthesia has become so safe.
Several safety-related aspects of this case meritdiscussion. First, why was high-dose bupivacainechosen for this block? Ropivacaine would probablyhave been a better choice. There are animal andhuman data suggesting that ropivacaine is a saferlocal anesthetic.4,5 Many reports of successful treat-ment of local anesthetic toxicity after high-dose ropi-vacaine have been promulgated;6-8 and theAPSF-reported case is just another in a litany ofreports of bupivacaine toxicity resistant to straight-forward resuscitation efforts.9
Epinephrine was not added to the local anestheticin the APSF-reported case. There has been a trend inregional anesthesia to avoid epinephrine due to a per-ceived increased risk of neural damage. These con-cerns are based on in vitro data and have not beenconfirmed in human or animal models of neuralblockade. With regard to systemic toxicity, epineph-rine probably does increase the margin of safety withsingle-injection nerve blocks. Epinephrine acts as anintravascular marker. When a significant amount oflocal is injected intravascularly, the increase in heartrate (pulse oximetry or ECG) can warn the physicianto halt further injection, and either avoid a toxic reac-tion or at least blunt its intensity.4
The use of a single, immobile injection techniquein the APSF-reported case should be discussed. Forseveral decades there was an ongoing debate amongaficionados of axillary block: students of Dr. Winniefavored single transarterial injection with an “immo-bile needle,” while followers of Dr. Thompson pre-ferred multiple injections around the artery. Thebulk of expert opinion now favors the identificationand injection of all 4 major nerves in the axilla.10
While the efficacy of the 2 techniques was debated,the relative safety of the techniques was not. Localanesthetic toxicity was fairly common with theimmobile needle, while there has never been a for-mal or informal report of toxicity with a multipleinjection axillary block.11 Critics maintain that multi-ple injections increase the possibility of nerve dam-age; however, no prospective randomized clinicaltrial has yet confirmed this assertion. Returning tothe APSF-reported case, some suggest that a 2-
injection approach to the sciatic nerve in thepopliteal fossa improves efficacy.12 By fractionatingthe total dose, a 2-injection technique could improvesafety. Would the APSF-reported case have beenprevented if the common peroneal and tibial compo-nents were identified and injected separately?
Our collective experience with epidural anesthe-sia also offers insight into this case. Thirty years agoepidural anesthesia was in its infancy. The usualmethod was to inject 20-30 ml of local anestheticthrough the Tuohy needle. Despite negative aspira-tion, the single injection technique often resulted inserious local anesthetic toxicity. The concept of thetest dose was introduced; however, serious compli-cations were still common with through-the-needledosing. The solution was to place an epiduralcatheter, test dose, and then dose incrementally.13
When incremental injections are separated by 3-5minutes, every dose is a test dose,14 and seriouscomplications became virtually non-existent.
Despite these caveats, serious local anesthetictoxicity will still occur rarely, just as severe disor-ders manifest during general anesthesia (e.g., malig-nant hyperthermia). Dantrolene has proven to be auseful antidote for the rare case of MH occurringduring general anesthesia. There is promise that asimilar antidote has been discovered for local anes-thetic toxicity. Studies have shown that administra-tion of lipid emulsion reliably rescues animals (ratand dog) from otherwise fatal doses of bupiva-caine.15,16 Rosenblatt et al.17 recently reported thesuccessful use of 20% Intralipid™ to rescue a patientwith bupivacaine-induced ventricular arrhythmiaswho had not responded to 20 minutes of ACLSefforts. Virtually all sites that provide general anes-thesia stock dantrolene for the rare case of MH. Sim-ilarly, 20% lipid emulsion should be stocked(together with dosage guidelines) in every operatingtheater and labor suite.18,19 Rather than avoidingperipheral nerve blocks, the APSF-reported caseshould prompt readers to evaluate their use of localanesthetics and their preparedness for rare, life-threatening complications.
Richard K. Baumgarten, MDDetroit, MI
References
1. Eichhorn JH. Patient perspectives personalize patientsafety. APSF Newsletter 2005;20:61-5.
2. van Pelt FA, Kenny L. Patient and doctor reconcile forgreater good. APSF Newsletter 2006;21:9-10.
3. Soltesz EG, van Pelt F, Byrne JG. Emergent cardiopul-monary bypass for bupivacaine cardiotoxicity. J Cardio-thorac Vasc Anesth 2003;17:357-8.
4. Finucane BT. Ropivacaine cardiac toxicity--not as trou-blesome as bupivacaine. Can J Anaesth 2005;52:449-53.
5. Borgeat A, Ekatodramis G, Blumenthal S. Interscalenebrachial plexus anesthesia with ropivacaine 5 mg/mLand bupivacaine 5 mg/mL: effects on electrocardiogram.Reg Anesth Pain Med 2004;29:557-63.
6. Gielen M, Slappendel R, Jack N. Successful defibrillationimmediately after the intravascular injection of ropiva-caine. Can J Anaesth 2005;52:490-2.
7. Huet O, Eyrolle LJ, Mazoit JX, Ozier YM. Cardiac arrestafter injection of ropivacaine for posterior lumbar plexusblockade. Anesthesiology 2003;99:1451-3.
8. Klein SM, Pierce T, Rubin Y, et al. Successful resuscita-tion after ropivacaine-induced ventricular fibrillation.Anesth Analg 2003;97:901-3.
9. Albright GA. Cardiac arrest following regional anesthe-sia with etidocaine or bupivacaine. Anesthesiology1979;51:285-7.
10. Koscielniak-Nielsen ZJ. Multiple injections in axillaryblock: where and how many? Reg Anesth Pain Med2006;31:192-5.
11. Baumgarten RK, Thompson GE. Is ultrasound necessaryfor routine axillary block? Reg Anesth Pain Med2006;31:88-9.
12. Paqueron X, Bouaziz H, Macalou D, et al. The lateralapproach to the sciatic nerve at the popliteal fossa: oneor two injections? Anesth Analg 1999;89:1221-5.
13. Cousins BG, Wildsmith JAW. Clinical pharmacology oflocal anesthetic agents. In: Cousins MJ, Bridenbaugh PO,eds. Neural Blockade in Clinical Anesthesia and Man-agement of Pain, 3rd ed. Philadelphia: Lippincott-Raven,1998:117.
14. Van Zundert A, Vaes L, Soetens M, et al. Every dosegiven in epidural analgesia for vaginal delivery can be atest dose. Anesthesiology 1987;67:436-40.
15. Weinberg GL, VadeBoncouer T, Ramaraju GA, et al. Pre-treatment or resuscitation with a lipid infusion shifts thedose-response to bupivacaine-induced asystole in rats.Anesthesiology 1998;88:1071-5.
16. Weinberg G, Ripper R, Feinstein DL, Hoffman W. Lipidemulsion infusion rescues dogs from bupivacaine-induced cardiac toxicity. Reg Anesth Pain Med2003;28:198-202.
17. Rosenblatt MA, Abel M, Fischer GW, et al. Successfuluse of a 20% lipid emulsion to resuscitate a patient aftera presumed bupivacaine-related cardiac arrest. Anesthe-siology 2006;105:217-218.
18. Picard J, Meek T. A response to 'lipid emulsion to treatbupivacaine toxicity.' Anaesthesia 2005;60:1158.
19. Weinberg G. Lipid infusion resuscitation for local anes-thetic toxicity: proof of clinical efficacy. Anesthesiology2006;105:7-8.
Letter to the Editor
Cardiac Arrest After Popliteal Block: AreThere Any Safety Lessons to Be Learned?

APSF NEWSLETTER Fall 2006 PAGE 53
Anesthesia Patient Safety FoundationCorporate DonorsFounding Patron ($500,000 and higher)American Society of Anesthesiologists (asahq.org)Grand Patron ($150,000 to $199,999)Cardinal Health Foundation (cardinal.com)Sustaining Patron ($100,000 to $149,999)Anesthesia Healthcare Partners, Inc. (AHP) (ahphealthcare.com)
Sponsoring Patron ($75,000 to $99,999)GE Healthcare (gemedical.com)
Foundation Patron ($50,000 to $74,999) Abbott Laboratories (abbott.com)
Benefactor Patron ($25,000 to $49,999)
Aspect Medical Systems (aspectms.com)
Hospira (hospira.com)
Organon (organon.com)
Philips Medical Systems (medical.philips.com)
Tyco Healthcare (tycohealthcare.com)
Supporting Patron ($15,000 to $24,999)Baxter Anesthesia and Critical Care (baxter.com)Dräger Medical (nad.com)Preferred Physicians Medical Risk Retention Group (ppmrrg.com)
Patron ($10,000 to $14,999)Cardinal Health, Alaris Products (alarismed.com)DocuSys (docusys.net)Endo Pharmaceuticals (endo.com)Ethicon Endo-Surgery (ethiconendo.com)iMDsoft (imd-soft.com) Oridion Capnography (oridion.com)Spacelabs Medical (spacelabs.com)
Sustaining Donor ($5,000 to $9,999)Anesthesiologists Professional Assurance Company
(apacinsurance.com)Arrow International (arrowintl.com)Becton Dickinson (bd.com)Datascope Corporation (datascope.com)GlaxoSmithKline (gsk.com)LMA of North America (lmana.com)Luminetx Corporation (luminetx.com)Masimo Corporation (masimo.com)ResMed (resmed.com)
Smiths Medical (smiths-medical.com)The Doctors Company (thedoctors.com)Vance Wall FoundationVital Signs (vital-signs.com)
Sponsoring Donor ($1,000 to $4,999)Anesthesia Business Consultants (anesthesiallc.com)Allied Healthcare (alliedhpi.com)Armstrong Medical (armstrongmedical.net)Cerner Corporation (cerner.com)Cook Critical Care (cookgroup.com)Intersurgical, Inc. (intersurgicalinc.com)Medical Education Technologies, Inc. (meti.com)TRIFID Medical Group LLC (trifidmedical.com)W.R. Grace (wrgrace.com)
Corporate Level Donor ($500 to $999)Belmont Instrument Corporation (belmontinstrument.com)Lippincott Williams and Wilkins
Participating AssociationsAmerican Association of Nurse Anesthetists (aana.com)
Subscribing SocietiesAmerican Society of Anesthesia Technologists and Technicians (asatt.org)
Community Donors (includes Anesthesia Groups, Individuals,
Specialty Organizations, and State Societies)Grand Sponsor ($5,000 and higher)American Association of Nurse AnesthetistsAsheville Anesthesia AssociatesFlorida Society of AnesthesiologistsDr. and Mrs. Thomas R. HillIndiana Society of AnesthesiologistsIowa Society of AnesthesiologistsKrishnarao V. R. Pinnamaneni, MDRobert K. Stoelting, MDSustaining Sponsor ($2,000 to $4,999)Alabama State Society of AnesthesiologistsAmerican Academy of Anesthesiologist
Assistants Anesthesia Associates of MassachusettsAnesthesia Consultants Medical GroupAnesthesia Resources ManagementArizona Society of AnesthesiologistsNassib G. ChamounGeorgia Society of AnesthesiologistsMadison Anesthesiology ConsultantsMassachusetts Society of AnesthesiologistsMichigan Society of AnesthesiologistsMinnesota Society of AnesthesiologistsFrank Moya Charitable FoundationOhio Society of AnesthesiologistsOld Pueblo Anesthesia GroupPennsylvania Society of AnesthesiologistsSociety of Cardiovascular AnesthesiologistsTennessee Society of AnesthesiologistsContributing Sponsor ($750 to $1,999)Academy of AnesthesiologyAffiliated Anesthesiologists, Inc.American Association of Oral and MaxillofacialSurgeonsAmerican Society of Critical Care AnesthesiologistsJ. Jeffrey Andrews, MDAnesthesia Associates of Northwest Dayton, Inc.Arkansas Society of AnesthesiologistsAssociation of Anesthesia Program DirectorsSorin J. Brull, MD
Capital Anesthesiology AssociationFrederick W. Cheney, MDConnecticut State Society of AnesthesiologistsJeffrey B. Cooper, PhDSteve F. Croy, MDDistrict of Columbia Society of AnesthesiologistsDavid M. Gaba, MDJohn H. Eichhorn, MDGreater Atlanta Society of AnesthesiologistsIllinois Society of AnesthesiologistsKentucky Society of AnesthesiologistsJohn W. Kinsinger, MDThomas J. Kunkel, MDRodney C. Lester, CRNAEdward R. Molina-Lamas, MDMadison Anesthesiology ConsultantsMaine Society of AnesthesiologistsMaryland Society of AnesthesiologistsMichiana Anesthesia CareMissouri Society of AnesthesiologistsRobert C. Morell, MDNebraska Society of AnesthesiologistsJohn B. Neeld, MDNorthwest Anesthesia PhysiciansNeshan Ohanian, MDNurse Anesthesia of MaineOklahoma Society of AnesthesiologistsOregon Society of AnesthesiologistsOregon Anesthesiology GroupPhysician Anesthesia ServicePittsburgh Anesthesia AssociatesSanta Fe Anesthesia Specialists Society of Academic Anesthesia ChairsSociety for Ambulatory Anesthesia Society of Neurosurgical Anesthesia and Critical CareSociety for Pediatric AnesthesiaStockham-Hill FoundationTexas Society of AnesthesiologistsDrs. Mary Ellen and Mark WarnerWashington State Society of AnesthesiologistsWisconsin Society of AnesthesiologistsSponsor ($100 to $749)Sean S. Adams, MD Robert Barth, MD
Manuel E. BonillaCalifornia Society of AnesthesiologistsRobert A. Caplan, MDCardiothoracic Anesthesia AssociatesCardiovascular Anesthesia, LLCMelvin A. Cohen, MDStuart M. Cohen, MDColorado Society of AnesthesiologistsDr. David ClementPaula A. Craigo, MDGlenn E. DeBoerJohn DesMarteau, MDNorig Ellison, MDJan Ehrenwerth, MDBasim I. Elhabashy, MDAnthony Frasca, MDB. L. Friedberg, MDThomas R. Farrell, MDGeorgia Anesthesia AssociatesIan Gilmour, MDBarry M. Glazer, MDGriffin Anesthesia AssociatesWilliam D. Heady, CRNAJames S. Hicks, MDDr. and Mrs. Glen E. HolleyVictor J. Hough, MDHoward E. Hudson, Jr., MDIndependence Anesthesia, Inc.Indianapolis Society of AnesthesiologistsRobert E. Johnstone, MDDaniel J. Klemmedson, DDS, MDKansas Society of AnesthesiologistsBettylou KoffelScott D. Kelley, MDAlan P. Marco, MDMaryland Association of Nurse AnesthetistsJohn P. McGee, MDMedical Anesthesiology Consultants CorporationMississippi Society of AnesthesiologistsA. J. Montes, MDRoger A. Moore, MDErvin Moss, MDNew Hampshire Society of AnesthesiologistsNew Jersey State Society of Anesthesiologists
New Mexico Society of AnesthesiologistsL. Charles Novak, MDMark S. Noguchi, CRNADenise O’Brien, RNMichael A. Olympio, MDPennsylvania Association of Nurse AnesthetistsPhysician’s Accounts ReceivableMukesh K. Patel, MDGaylon K. Peterson, MDPhysician Specialists in AnesthesiaRichard C. Prielipp, MDRhode Island Society of AnesthesiologistsHenry Safford, CRNADrs. Chris and David SantamoreMuthia Shanmugham, MDSociety for Obstetric Anesthesia and PerinatologySociety for Technology in AnesthesiaSouth County Anesthesia AssociationThe Woodlands Anesthesia AssociationUniversity of Maryland Anesthesiology
AssociatesUtah Society of AnesthesiologistsVermont Society of AnesthesiologistsVirginia Society of AnesthesiologistsMatthew B. Weinger, MDWest Virginia Association of Nurse AnesthetistsWest Virginia State Society of AnesthesiologistsDr. and Mrs. WetchlerLawrence Wobbrock, JDWest River Anesthesiology Consultants
In MemoriamIn memory of Leroy D. Vandam, MD (Dr. and
Mrs. George Carter Bell)In memory of Robert M. Chapman, MD (Texas
Society of Anesthesiologists)In memory of Dr. Anthony J. DiGiovanni (Texas
Society of Anesthesiologists)In memory of Laurie A. Noll, MD (The Coursin
family)
Note: Donations are always welcome. Send to APSF; c/o 520 N. Northwest Highway, Park Ridge, IL 60068-2573 (Donor list current through September 18, 2006)

APSF NEWSLETTER Fall 2006 PAGE 54
Numerous questions to the Committee on Technology are individually and quickly answered each quarter by knowledgeablecommittee members. Many of those responses would be of value to the general readership, but are not suitable for the DearSIRS column. Therefore, we have created this simple column to address the needs of our readership.
Dear Q&A,
One of my hospitals plans on purchasing newvaporizers for anesthetic delivery. Theirmachines already have anesthetic gas monitorsmounted and used on every case. The vendorstates that the "standard" vaporizercheck/recalibration occurs every 3 years. Heoffers an annual check/calibration of eachvaporizer for additional cost.
Does the APSF have any recommendation as toannual vs. every-3-year calibration of vaporizers?
And, if no recommendation, standard, orguideline exists for interval of calibration, doyou have any opinion about whether the pres-ence of anesthetic gas monitors in the circuitmight influence the interval between calibra-tions?
Thank you.
George Burgess MDVP, Innovation & TechnologyFranciscan Missionaries of Our Lady HealthSystemBaton Rouge, LA
Dear Dr. Burgess,
From a clinical use standpoint, I believe thatgas analyzers sampling at the endotrachealtube are far more useful to me than what thedial or output of the vaporizer actually is. Weknow that the actual vaporizer output is notwhat the patient inhales. Fresh gas flow,inspired flow, carrier gas composition, mixingcapacity of the circuit, circuit design, uptake,degradation, gas sampling extraction, etc., areall contributing factors. Thus, if the engineersand manufacturers believe the internal calibra-tion mechanisms are stable for up to 3 years,then I would say that more frequent calibra-tions are not clinically helpful. I would furtheradd that gross errors in output, secondary tointernal failure, might occur suddenly andshould be detectable by gas analysis. Vaporizeroutput must also be checked under highly reg-ulated conditions with controlled carrier gascomposition.
Dear Dr. Burgess,
The above response is absolutely right. Thevaporizer setting is only meaningful when anopen circuit is used. In all other configurations,the vaporizer setting is different from what themachine delivers at the Y-piece. So the onlyadequate number is what the gas analyzer mea-sures as “inspiratory Agent”/“expiratoryAgent” value. During low flow anesthesia thevaporizer setting may differ greatly from theinspired agent concentration. That's why a gasanalyzer is so helpful. The only reason for avaporizer check (as opposed to a calibration),may be to verify its functionality in general.
Dear Dr. Burgess,
I would defer to the vaporizer manufacturers,as they have the most definitive informationregarding field verification and factory calibra-tion process. Informally, I can tell you that verylittle is, or can be done, in the field, other thanidentifying an errant vaporizer and pulling itoff the machine.
Most vaporizers on the market today, regard-less of their manufacturer, cannot be cali-brated in the field. They can only be checked.Usually the first inkling that calibration maybe off comes from a disagreement with themulti-gas monitor. However, since the possi-bility exists that the gas analyzer could be mis-reading, then both devices need to be checked.Normally, vaporizer calibration should bechecked with a reference device such as theones made by Riken.
Different vaporizer manufacturers makegreatly varying claims about how often vapor-izers need to be checked or sent back for cali-bration. I remember that one manufacturerclaims a 10-year service-free life for its vapor-izer. There is also the school of thought thatmay suggest that “if it ain’t broke, don’t fix it,”meaning that if the multi-agent monitor agreeswith the vaporizer’s setting, then all is well.
Dear Dr. Burgess,
I suggest that one point deserves more empha-sis: I had this type of discussion with myvaporizer service people who insisted on a 6-
monthly check which seemed excessive apartfrom halothane and thymol accumulation.They made the point that most of the troublecame from foreign substances in the vaporiza-tion chamber, necessitating disassembly of theunit. In one case there was blood in a unit, andnot infrequently watery solutions that could becorrosive over a long period. The wrong agentcan confuse the issue. This type of problemmay not be detected by a check of concentra-tion output.
Dear Dr. Burgess,
While there is no formal standard thataddresses either a service, or calibration inter-val for inhalation anesthetic agent vaporizers,the vaporizer manufacturers normally haveboth device- or model-specific recommendedintervals for each. These intervals depend onthe age of the device and the degree to whichtechnology has advanced both the accuracyand reliability of the vaporizer. Since vaporiz-ers may be conventional pneumatic, pneumaticwith electronic monitoring, or entirely elec-tronic, the intervals will vary.
The original design for vaporizers included noelectronic means to verify vaporizer output,vaporizer fill status, or any number of otherpotentially important pieces of information theuser may wish to know. The advent of electron-ics in vaporizers has permitted a more carefulobservation of the current overall status of thevaporizer. Electronics also provide the oppor-tunity to notify the user when something unto-ward has occurred with the vaporizer that mayotherwise remain unnoticed by the user. Theinclusion of electronics affects both the serviceand calibration intervals. As a result of thesevariations many institutions select either onesingle vaporizer technology or a group of simi-lar technologies that require calibration andservicing at similar intervals.
NEW
The information provided in this column is for safety-related educational purposes only, and does not constitute medical or legal advice. Individual or groupresponses are only commentary, provided for purposes of education or discussion, and are neither statements of advice nor the opinions of APSF. It is not the intentionof APSF to provide specific medical or legal advice or to endorse any specific views or recommendations in response to the inquiries posted. In no event shall APSF beresponsible or liable, directly or indirectly, for any damage or loss caused or alleged to be caused by or in connection with the reliance on any such information.
APSF NEWSLETTER Fall 2006 PAGE 55
To the Editor:
I am an ABA Certified Anesthesiologist with 15years post-residency experience in community hos-pitals. I have become increasingly concerned withthe matter of “production pressure.” If ever therewas an unworthy appellation coined for a shamefuland inconsistent concept, this certainly qualifies. Myobservation of this phenomenon over a significantperiod of time leads me to conclude that it has nopositive connotations. It is shameful because it fre-quently results in a departure from patient advocacyin order to meet other competing goals, e.g., 1)deferring to a surgeon’s schedule in order to avoidcomplaints of delay, postponement, or cancellationdirected to an unsympathetic administration, 2)denying patients their legal right to informed con-sent and an adequate work-up due to a given facil-ity’s inefficiencies and imposed time constraints, 3)the perceived need to protect a business arrange-ment or exclusive contract in an environment where“production” is prized above quality or safety.
For example, when an 82-year-old, hypertensive,diabetic patient on multiple medications is treatedwith the same lack of laboratory work-up as a 30-year-old, ASA 1 patient on no medications, then Iam of the opinion that we have exceeded the limitfor rational laboratory parsimony. Similarly, con-sider the 59-year-old, obese patient with newly diag-nosed diabetes and poorly-controlled hypertensionwho was admitted 24 hours earlier with cellulitis ofthe foot who has still not received any work-upupon arrival in the operating room for “emergency”incision and drainage. A stat EKG also shows atrialflutter with a rapid ventricular response (120s in theabsence of fever or signs of sepsis), evidence of pre-vious infarction, age indeterminate, with currentischemic changes in the lateral leads. Which is thehigher priority emergency: toe pus or cardiovascularstabilization? In a profession that prides itself onskill—not just technical skills, but skills of clinicalacumen and judgment—I must conclude that insuch cases some “board certified” anesthesiologistshave included under “clinical judgment” a heavyreliance upon lady luck. The reality is that, fre-quently, the patients survive their procedures andanesthetics. What should I conclude from this? HaveI missed something? Has pre-anesthetic assessmentfor the purpose of patient preoperative stabilizationand the mitigation of chronic disease exacerbationbecome passé? Has the oft-touted improvement inanesthesia morbidity and mortality statistics(although the incidence of adverse events for MACanesthetics may be increasing again) renderedpatient work-up and preparation obsolete because itmay be inconvenient to a surgeon’s schedule?
My training and experience inform me that themost important determinant of a good outcome is arational, well thought-out anesthetic plan incorpo-
rating appropriate flexibility and based upon a thor-ough pre-anesthetic work-up. Vigilance does notbegin with the pushing of a medication or the onsetof an anesthetic. In the absence of knowledge, one isleft with ignorance. I refuse to accept that any of myanesthesia colleagues possess sufficient clairvoyanceto dispense either frequently or occasionally with anappropriate medical work-up, particularly whensuch obvious and powerful conflicts of interest asmentioned above are present.
It would seem that board certification no moreguarantees consistent and persistently high stan-dards of medical care than a license to drive impliesthe ability to handle a vehicle on a rain slick high-way or an increased propensity to obey the speedlimit. I contend that the historical insecurities ofanesthesiology are alive and strong and have cre-ated many environments in which certainapproaches to daily patient care would result in can-didate failure if advocated during an oral boardexamination. The only moderating influence to thisis the tort system, but the implementation of thisextreme process implies a bad outcome for a lot ofpeople. It is not really what one says during an oralboard exam that counts, it is how one performs forthe rest of his or her professional life. There areplainly many situations in which it is very difficultto “grasp the challenge” or to “educate” the vestedpower elite in order to induce positive change.Many times I have heard the saying: “It takes adeath to result in change.” Everyone correctly clucksthe tongue with an appropriate “tsk, tsk,” whenspeaking of “production pressure” and commiser-ates about this very real and dangerous antagonistto patient safety. However, the implementation ofactions to ameliorate and eliminate the palpablehazards of this disreputable and ultimately counter-productive phenomenon are frequently lacking.
Pressure should be exerted upon institutionsand medical staff to create environments in whicheach patient is provided a timely and appropriatework-up. Anesthesiologists should not be posi-tioned to succumb to the temptation to abandontheir responsibilities to patients in order to protecttheir jobs. Job insecurity seems to be where all thepressure focuses; this is unworthy of the disciplineas well as those practitioners who hold a high viewof anesthesiology and our responsibilities topatients. As long as hospital CEOs and variousphysicians pander to “customers” according to abusiness-oriented model of patient care, this situa-tion will not improve. However, there is anotherapproach that has been resurrected under the termi-nology of “systems thinking” that is first and fore-most patient-based. (See national editorial by CalThomas, “Hospitals: Heal Thyselves,” June 22, 2006,Tribune Media Services, 2225 Kenmore Ave. Suite114, Buffalo, N.Y. 14207). This approach is report-
edly enjoying a productive trial in numerous hospi-tals in St. Joseph, Missouri, and the Pittsburgh,Pennsylvania, areas.
I would suggest that the ASA provide leader-ship in proposing a practical and flexible model forinstitutional organization that could result inimproved efficiency and thoroughness in preopera-tive evaluation for use in all practice settings. Indi-vidual anesthesia groups clearly are no more up tothe challenge of suggesting and implementing sucha proposal than they were in developing a difficultairway algorithm. If hand-washing still remains anissue among some physicians over a century afterthe establishment of the germ theory of disease, thenwhy should anyone think that the more complexmatter of anesthetic pre-assessment should receiveits just consideration at some local levels. This is anational problem and deserves a high-profilenational emphasis. I have consistently found organi-zation to be preferable and more productive thanconfusion, and it decidedly contributes to betterperioperative control and predictability.
Ronald L. Hedderich, MDGray, TN
Letter to the Editor:
National Support Needed to Fight Production Pressures
AnesthesiaPatient Safety
Foundation
Working ForPatient Safetywww.apsf.org
®

APSF NEWSLETTER Fall 2006 PAGE 56
The emergency evacuation of an operatingroom may be required in the event of a fire or simi-lar emergency. Although the vast majority of prac-ticing anesthesiologists and nurse anesthetists willnever participate in an operating room evacuation,it is important to be prepared for such an eventual-ity. The pediatric anesthesia group at our institutionrecently participated in a mock operating roomevacuation drill. In this article we describe the plan-ning and execution of this drill and some of thelessons that were learned as a result of the exercise.
Planning and OrganizationThe Institutional fire safety officers, the operat-
ing room fire safety officer, and nursing administra-tion were responsible for the advance planning ofthe drill, which was designed to be consistent withour institutional health and safety policies. RileyHospital for Children has 2 operating room suites.The main 13-bed operating room suite is located onthe second floor of the main building in an area thatis adjacent to the PACU, PICU, and immediatelybelow the NICU. A second, 6-bed, operating room islocated in the basement of the Riley Outpatient Cen-ter and is dedicated primarily to same-day surgerycases. The Riley Outpatient Center is located in anewer building that is connected to the main hospi-tal by corridors, walkways, ramps, and steps. Theemergency scenario involved a fire within the samefire zone as the main operating room, but on a dif-ferent floor. The fire caused a loss of power to themain operating room and precluded evacuation tothe adjacent PICU or PACU. The plan involvedevacuation to the outpatient center operating rooms.The evacuation route was planned by the organizingcommittee prior to the drill and was approximately300 yards in length and included 2 elevator rides.These elevators were outside the fire zone of themock fire and were therefore thought to be safe foruse. Five patient scenarios were created with volun-teers or dolls representing patients undergoingsurgery. The drill was performed during weeklymorning conference time when the operating roomswere not occupied with elective cases. The organiz-ers recruited a staff anesthesiologist to participate ineach scenario. Each operating room had 4 nurses, 1of whom played the role of the surgeon. Severalanesthesia nurses, perfusionists, and respiratorytherapists also participated. There were also severalnurses acting as observers.
Conduct of the DrillThe 5 scenarios and their anesthesiologists`
response are briefly described below. The chargenurse distributed battery powered headlights to
each anesthesiologist shortly after the power wasinterrupted. In each case, the anesthetic was contin-ued using an intravenous technique during trans-port. Four of the five simulated patients arrived atthe intended destination in less than 15 minutes.
1. A 13-year-old undergoing a craniotomy in pins. Thesurgery was performed under a primarily intra-venous anesthetic. At the time the power wentout, the anesthesia machine and monitors wereunplugged to model the power failure. Therewere no backup lights in the room; however, theanesthesia machine monitoring screen continuedto have power from the anesthesia machine bat-tery. This screen proved to be an unanticipatedsource of light. The operating room control nursecame to the room to direct the operating roomteam to move the patient to the outpatient ORsuite. A transport monitor was sent for, whichwas set up as the patient’s monitor. In prepara-tion for moving the patient, the surgeon modeledstapling the scalp closed and a portable oxygensource was obtained. With that and a flashlight,the operating room table was unlocked and thepatient was moved on the OR table toward a setof elevators that was unaffected by the powerfailure. After navigation through the halls, anattempt was made to move the OR table into theelevator. In that process, it became apparent thatthe small wheels of the OR table along with theweight of the patient and table presented a signif-icant risk of getting stuck while entering or exit-ing the elevator. At that point the mock drill wasstopped for that patient.
2. A 15-year-old undergoing a posterior spinal fusion.Because the patient was undergoing evokedpotential monitoring, the anesthetic was primar-ily intravenous in nature; thus, it was relativelyeasy to prepare for transport. The wound wascovered in a transparent adhesive sterile drapewhile illuminated by flashlight. The spine wasunstable and it was thought that transport in theprone position on the operating room bed wasthe safest option. The patient was monitored withpulse oximetry during transport. Again, problemswere encountered while moving the operatingroom bed in and out of elevators. An unantici-pated issue was the difficulty encountered inmaneuvering the heavy OR bed safely up anddown the slopes connecting the 2 buildings.
3. A 3-month-old undergoing a hernia repair. Thewound was covered with a sterile dressing andthe patient was transferred to a transport isolette,making transport through the hospital relativelystraightforward. Ventilation was maintained with
a self-inflating resuscitation bag. A pulse oxime-ter was used for monitoring during transport.
4. A 6-month-old undergoing a VSD repair. Initiallythere was confusion about how to transport all ofthe supplies needed to maintain anesthesia, suchas drugs, intravenous fluids and tubing, extraendotracheal tubes, and other equipment. Mostitems were simply placed at the head of the oper-ating room table by the patient’s head or in alarge plastic bag found in the operating room.The biggest obstacle encountered involved themoving of the operating table in conjunction withthe cardiopulmonary bypass machine. The trans-port was slow and was frequently interrupted inorder to maintain appropriate CPB circuit lengthand tension. One unexpected challenge arosewhile transporting the cardiopulmonary bypassmachine through the basement tunnels. Thebypass machine had to be maneuvered throughnumerous, low-hanging maintenance pipes. Thisproved to be very time consuming and con-tributed to the 15-minute evacuation time.
5. An 8-year-old undergoing a laparotomy. When thelights went out a flashlight was used to aid thesurgeon. It was decided that the surgeon was farenough along to close the wound quickly andthen plan to come to finish later. The anestheticwas converted to a TIVA technique using keta-mine and propofol. Simultaneously, supplieswere prepared in zip lock bags, and an oxygentank and self-inflating resuscitation bag wereobtained for the move. A decision was made touse a cart to move the patient to another locationas the OR table would be difficult to move.
Findings1. The operating room lighting was designed to be
backed up by the hospital back-up generator. Asa result, there was no wall mounted emergencylighting designed to come on in the event ofpower failure coupled with a generator failure.We are evaluating the possible installation ofsuch emergency lighting. Flashlights and/orheadlights should be available at every anes-thetizing location.
2. The idea of moving a patient on the operatingroom table seemed like a good one. It probablyremains a good one if the patient is to be movedlaterally, perhaps to the adjacent ICU. However,moving the OR table into and out of an elevatorproved to be a significant problem. In addition,ramps can present significant obstacles to trans-porting OR beds.
Lessons Learned from an OperatingRoom Emergency Evacuation Drill
Simon C. Hillier, MD; William L. McNiece, MD; Tammy Brooks, RN; Marnie Sieber, RN; Jacqueline Allison, MD; George Sheplock, MD; Leigh Latham, MDSection of Pediatric Anesthesia and Operating Room Nursing Division, Riley Hospital for Children, 702 Barnhill Drive. Indianapolis, IN 46202
See “Evacuation,” Next Page

APSF NEWSLETTER Fall 2006 PAGE 57
3. We have sufficient portable monitors andportable oxygen sources to provide for close tohalf of the operating rooms. We would not havehad sufficient monitors and oxygen sources hadwe needed to evacuate the entire operating room.
4. Moving an intraoperative patient on an unex-pected basis presents major challenges. The deci-sion to move the patient needs to consider theurgency of the situation and the risk-benefit ratioof staying where you are vs. moving. In a real sit-uation, accurate information would be essentialto good decision making regarding patient man-agement. If our drill had only been a power fail-ure, it could have been better to have spent moretime preparing for the transport. However, weexpect accurate information might be difficult toobtain in a real situation.
5. Our drill had the premise of a fire and power fail-ure affecting adjoining units, but in fact thoseunits were not involved in the drill. Had theyalso been involved, there would have been amajor backup at the only set of functioning eleva-tors.
6. This drill has increased our awareness of theissues associated with emergency situations. Weadvocate the regular participation of the anesthe-sia department in such drills. The drills should bedesigned to simulate several different scenariosand evacuation routes. Anesthesiologists andnurse anesthetists should participate in the plan-ning and execution of emergency evacuationdrills.
7. When moving an anesthetized patient there is asignificant amount of ancillary equipment andsupplies that are required. In our experience, alaptop bag or briefcase with a shoulder strapproved to be extremely useful.
We hope that our description of this experiencewill stimulate other anesthesiologists and nurseanesthetists to participate in mock emergency drillsand become actively involved in their planning.
Corresponding author: Simon C. Hillier, MD,[email protected]
Letter to the Editor
Aims Should NotDistractTo the Editor:
With the increasing use of computerized anes-thesia records, I feel it is time for some standards.Specifically, I believe the computer screen andmouse should be within visual and hand reachwhile one is doing a chin lift. It does a disservice to apatient to instrument an airway for no reason otherthan to reach the computer. It also delays turnoverwhen one must later record the drugs and timestemporarily jotted down on scrubs, tongue blades,or whatever is available.
Glee Folsom, CRNAEdmonds, WA
Letter to the Editor
More Thoughtson PreventingCorneal AbrasionTo the Editor:
We also share concern regarding the potentialfor corneal injury in the perioperative period. Wewould like to add another possible mechanism ofinjury during minimally invasive surgery, afterwhich the patient, who suffers less postoperativepain, may be more acutely aware of other discom-forts. We have noticed that the edema of the depen-dent eye(s) may force the lid(s) slightly open, thusallowing dryness, irritation, and potential self-inflicted injury after emergence. We see this inrobotic-assisted radical prostatectomy, in which thepatient is in head-down position for hours, orlaparoscopic radical nephrectomy, in which 1 eye isdependent for hours. The solution, for which wegive credit to anesthesiologists at City of Hope Hos-pital in Los Angeles, is to lubricate the eyes, tapethem both vertically and horizontally, and, finally,to place a Sun-Med I Guard Eye Protector (Sun-MedDivision of Azimuth, Largo, FL) mask over the eyes.At the end of the case, tape is removed, eyes arerinsed, and mask is replaced over the eyes untilpatient is wide-awake in the recovery room. Patientsare warned they will be arriving in the recoveryroom wearing a blue super-hero mask. A small pin-hole can be made in the clear eye shield part of themask to prevent fogging.
Debra E. Morrison, MDAnne B. Wong, MDUniversity of California, IrvineOrange, CA
A N E S T H E S I A P A T I E N T
S A F E T Y F O U N D A T I O N
CORPORATE ADVISORY COUNCIL
George A. Schapiro, ChairAPSF Executive Vice President
Elizabeth Holland...................Abbott Laboratories
Sean Lynch...............................Anesthesia Healthcare Partners
Cliff Rapp.................................AnesthesiologistsProfessional InsuranceCompany
Nassib G. Chamoun ...............Aspect Medical Systems
William Floyd..........................Aspect Medical Systems
Raul A. Trillo, MD ..................Baxter Healthcare
Michael S. Ferrara ...................Becton Dickinson
Tim Vanderveen .....................Cardinal Healthcare
Thomas W. Barford ................Datascope Corporation
Robert Clark ............................Dräger Medical
Brian Mulnix............................Endo Pharmaceuticals
Paul Bruggeman .....................Ethicon Endo-Surgery
Paul A. Baumgart ...................GE Healthcare
Tim Hagerty ............................Hospira
Steven C. Mendell...................LMA of North America
Joe Kiana ..................................Masimo
Bert de Jong, MD.....................Organon
Dominic Corsale .....................Oridion
Walter Huehn..........................Philips Medical Systems
Edward C. Mills ......................Preferred PhysiciansMedical Risk RetentionGroup
Ron Richard.............................ResMed
Andrew Rose...........................Smiths Medical
Joseph Davin ...........................Spacelabs
Ann S. Lofsky, MD .................The Doctors Company
William T. Denman, MD .......Tyco Healthcare
Terry Wall ................................Vital Signs
Abe Abramovich
Casey D. Blitt, MD
Robert K. Stoelting, MD
“Evacuation,” From Preceding Page
Evacuation PlanningEncouraged
See Your APSF Website at
www.apsf.org
Lessons from“Can’t Intubate/Can’t Ventilate”Report
To the Editor:
Dr. C. Troop’s case summary of a “can’t intubate/can’t ventilate” outcome in a morbidly obesepatient reflects an event feared by all anesthesiolo-gists.1 Tracheal intubation, initially attempted witha standard technique, eventually proved ineffectiveduring a complex situation compounded by diffi-cult laryngoscopy. Two problems were present, asare possible in all patients requiring general anes-thesia. Initially, the anesthesiologist was unable toreliably predict a difficult airway in order to altermanagement preemptively. Subsequently, when adifficult laryngoscopy was encountered, furtherattempts at standard intubation proved both inef-fective and time-consuming, a recognized andrecurring outcome acknowledged in the anesthesi-ology literature. The continuing acceptance of whatis basically a flawed technique as the standard forroutine intubation stems from the unquestionedacceptance of a 60-year-old procedure originallyintended to secure the airway in MOST but NOTALL patients. The response to the inevitable “diffi-cult intubation” has led anesthesiologists todevelop personal “tricks” that are added as supple-ments to textbook intubation. Each additional step,however, requires extra time to implement anddoes not guarantee success at the time when dura-tion of hypoxia becomes critical to patient safety.The ideal solution is to routinely use a single tech-nique that is safe and effective for the normalpatient, and yet maximizes rapid tube placementwith difficult laryngoscopy. At the very least, suchan approach would, in the rare instance where intu-bation was impossible, considerably shorten thedelay between recognizing failure and entering thedifficult airway algorithm.
One system of routine intubation employing aMAC 4 laryngoscope blade and a standardizedendotracheal tube-stylet combination has been exe-cuted successfully in thousands of patients.2 Thissystem is based on 2 fundamental principles gov-erning use of a styletted endotracheal tube. First theoperator must purposefully control the endotra-cheal tube and deliberately place the tip at orbetween the vocal cords, and second, from thatposition slide the endotracheal tube forward intothe glottis while the stylet remains stationary.
Key steps incorporated into this system include
1. A correctly performed laryngoscopy tailored tothe patient. This creates a laryngoscopic channelthat allows access to the larynx and a path
Return toSpontaneousVentilation CanBe Life-SavingTo the Editor:
I read with considerable concern the articletitled, “Difficult Intubation in the Obese Patient,”(APSF Newletter, Winter 2005-2006 Issue, Page 83).While it is true that positioning is extremelyimportant in airway management in the obesepatient, I feel that the real lesson in this case isbeing overlooked. In an obese patient for an ELEC-TIVE procedure, when difficulty with visualiza-tion/mask ventilation is encountered, the goalshould be to return the patient to spontaneous ven-tilation with a clear airway as soon as possible, notinsertion of an ETT! I suspect that in this case quitea few attempts at intubation were tried with vari-ous devices before the airway was irretrievably lost.With succinylcholine, return to spontaneous venti-lation should occur fairly rapidly in most cases, andthe procedure should have been canceled and thepatient awakened. Better to come back another daywith such a patient, perhaps for an awake intuba-tion under appropriate sedation, than to lose him intrying to be heroic.
Marc A. Pressman, MD Surgicenter of Baltimore Owings Mills, MD
APSF NEWSLETTER Fall 2006 PAGE 58
Letters to the Editor:through which the endotracheal tube must passwithout contacting any part of the channel.
2. An endotracheal tube that is shaped to match aportion of the laryngoscopic channel.
3. The appropriate direction of travel within thechannel that permits intentional positioning ofthe endotracheal tube tip at the larynx.
4. A definable endpoint to confirm when the tra-cheal tube tip passes between the vocal cordsduring grade I-III 1/2 laryngoscopic views.
As learning and skill improve with daily prac-tice and experience, most difficult intubations grad-ually become routine and act as training for theanesthesiologist to respond quickly and effectivelyin critical situations.
Russell Stasiuk, MDVancouver, British Columbia.
References
1. Troop CS. Difficult intubation in the obese patient. APSFNewsletter Winter 2005-2006;20(4):83.
2. Stasiuk RBP. Improving styletted oral tracheal intuba-tion: rational use of the OTSU. Can J Anesth2001;48:911-8.
Overjet, NotOverbite isCorrect TermTo the Editor:
I enjoyed reading the well written article byCraig Troop entitled “Difficult Intubation in theObese Patient,” which appeared in the Winter2005-2006 APSF Newletter . In his article hedescribes 6 physical signs that can alert one to thepossibility of a difficult airway. One of the signs hehas listed is dental overbite, rather than dentaloverjet. I am writing to clarify the dental terminol-ogy used in his article.
Dental overbite describes the vertical relationshipof occlusion (bite) and dental overjet describes thehorizontal relationship of occlusion. A patient with alarge dental overjet (Andy Gump deformity) is ret-rognathic and would very likely have a difficult air-way. This description is consistent with such apatient having difficulty performing the upper lipbite test. A patient with reverse dental overjet is usu-ally prognathic (e.g., Jay Leno) and would not likelyhave a difficult airway. A patient can have a deepbiteor openbite (descriptions of dental overbite relation-ship) and may or may not have a difficult airway.
David W. Todd, DMD, MDLakewood, NY
Check out the Virtual Anesthesia Machine Website
and theAPSF Anesthesia
Machine Workbookat
www.anest.ufl.edu/vam

APSF NEWSLETTER Fall 2006 PAGE 59
User-FriendlyAlarms NeededTo the Editor:
While we all agree in principle that audiblealarms should be used, the problems incurred byexcessive false-positives cause many practitionersto shut them off. Especially for short cases, such asendoscopy, the anesthesiologist must spend exces-sive time and effort addressing alarms activated byan oximeter that falls off a finger, a patient whobreathes through his mouth instead of his nose, ablood pressure cuff blocking a pulse, and the like.Not a day goes by without my repeated disclaimerto procedurists, nurses, and even to awake patients,“Sorry, the patient is fine, it is just my alarms(falsely) acting up.”
My attempts to discuss the practitioners’ con-cerns to the equipment industry, as in the literature,have always yielded excuses and justifications forthe status quo. It is up to our profession's leaders, aswell as practitioners, to induce the industry todevelop user-friendly monitors and alarms that willbe a pleasure to use.
Howard Schranz, MDBrooklyn, NY
Fatigue StillA ProblemTo the Editor:
Bravo to Dr. Ellis for his remarks regardingfatigue and long work hours in the Fall 2004 issue ofthe newsletter. Now you even have to make surethat a resident is not too tired to drive. Are theydoing this in other critical occupations? How muchsleep does the President get before sending ourtroops into combat?
In my practice we are off the next day after tak-ing call; many practices that I am familiar with func-tion in this fashion.
It always bothered me that surgeons could startlong elective cases late at night or work during thenight, only to continue with their elective schedulethe next day.
Unfortunately, many of the important changesto healthcare cannot occur because of lack of fund-ing. When we do make a change, it is at the discre-tion of JCAHO, and it often lasts for the duration ofthe inspection.
Steven Ginsberg, MDBridgewater, NJ
Epidural Notthe OnlyOption ForLabor PainTo the Editor:
I write to you not as an anesthesia professional,but as the wife of an anesthesia professional and onewho has had 4 children. It has been of interest to meto follow the string of letters regarding Dr. Parker'scomments from the Summer 2005 Newsletter becauseI have often wondered, "What does the anesthesiolo-gist think about labor epidurals?" I was actually gladto hear Dr. Parker's comments. I was glad to hearthat a medical professional can see the abuse ofmedication so rampant with epidural labors.
Perhaps I should better explain my position. Ihave had 4 children in the past 10 years (1996, 1999,2001, 2004). My husband and I prepared to have lowrisk pregnancies and births with each. We utilizedthe 9 months of pregnancy as a time to preparephysically with exercise and excellent nutrition,emotionally with daily relaxation practices, andmentally with building confidence as we educatedourselves via books and classes. I understand thatmost pregnant couples do not utilize the 9 months ofpregnancy in this manner, but rather spend thattime decorating a nursery, buying a mini-van, andfinding the perfect 5-in-1 stroller. We, however,placed our focus on labor preparation. Therefore, atthe time of labor, we were prepared and managed"one of the most severe pains a woman will everexperience in her lifetime" (quoted from Drs. Cam-man, Hughes, and Birnbach from the Winter 2006Newsletter) without any medications. The followinglists our children's birth weights and lengths respec-tively: 11 lbs. 4 oz., 23; 9 lbs. 14 oz., 21; 9 lbs. 8 oz., 21oz.; and 9 lbs., 12 oz., 20 1/2. All 4 of our childrenwere born vaginally without Stadol, Nubain,Demerol, fentanyl, or an epidural. In my experience,viral meningitis was much more painful than allfour labors combined!
So, as a voice of the minority, I share our experi-ence with you to show that, while drugs and proce-dures have their place, an epidural is not the onlyway to manage labor. However, anesthesiologistsare at the beck and call of couples who do not pre-pare as we did, and for that, I am sorry.
Tami Maloney, BBA, AAHCCDecatur, AL
APSFWorking for Patient Safety
Letters to the Editor:
www.apsf.org

Anesthesia Patient Safety FoundationBuilding One, Suite Two8007 South Meridian StreetIndianapolis, IN 46217-2922
NONPROFIT ORG.U.S. POSTAGE
PAIDWILMINGTON, DEPERMIT NO. 1387
APSF NEWSLETTER Fall 2006 PAGE 60
Inside:• Training
Initiative forNew Machine
• Dear SIRS: In-line OxygenAnalyzer
• Mock EvacuationDrill
• Preview of SafetyPresentations at2006 ASA Meeting
Be sure to visit the APSF Booth in the Exhibit Hall atMcCormick Place at the 2006 ASA Meeting in Chicago, Illinois!