new title slide
TRANSCRIPT

July 20, 2021

Welcome & Introductions
Beth DelGiaccoVice President, Corporate Communications & Investor Relations

Forward Looking Statements
Safe Harbor: Certain statements contained in this presentation, other than present and historical facts and conditions independently verifiable at the date hereof, may constitute forward-looking statements. Examples of such forward-looking statements include those regarding the therapeutic and commercial potential of our product candidates; our clinical development and regulatory plans, including the timing, design and outcome of ongoing and planned clinical trials and preclinical activities; the timing, progress and benefits of commercialization activities; our plans to start registrational trials this year; our statements regarding new assets yearly from IIP; our statements regarding potential and effect of efgartigimod; our expectation to have IND filing this year; our plan to start Phase 2 trial in MMN this year; and the expected size of the markets for our product candidates. When used in this presentation, the words “anticipate,” “believe,” “can,” “could,” “estimate,” “expect,” “intend,” “is designed to,” “may,” “might,” “will,” “plan,” “potential,” “predict,” “objective,” “should,” or the negative of these and similar expressions identify forward-looking statements.Such statements, based as they are on the current analysis and expectations of management, inherently involve numerous risks and uncertainties, known and unknown, many of which are beyond the Company’s control. Such risks include, but are not limited to: the impact of COVID-19 pandemic on our business, the impact of general economic conditions, general conditions in the biopharmaceutical industries, changes in the global and regional regulatory environments in the jurisdictions in which the Company does or plans to do business, market volatility, fluctuations in costs and
changes to the competitive environment. Consequently, actual future results may differ materially from the anticipated results expressed in the forward-looking statements. In the case of forward-looking statements regarding investigational product candidates and continuing further development efforts, specific risks which could cause actual results to differ materially from the Company’s current analysis and expectations include: failure to demonstrate the safety, tolerability and efficacy of our product candidates; final and quality controlled verification of data and the related analyses; the expense and uncertainty of obtaining regulatory approval, including from the U.S. Food and Drug Administration and European Medicines Agency; the possibility of having to conduct additional clinical trials; our ability to obtain and maintain intellectual property protection for our product candidates; and our reliance on third parties such as our licensors and collaboration partners regarding our suite of technologies and product candidates. Further, even if regulatory approval is obtained, biopharmaceutical products are generally subject to stringent on-going governmental regulation, challenges in gaining market acceptance and competition. These statements are also subject to a number of material risks and uncertainties that are described in the Company’s filings with the U.S. Securities and Exchange Commission (“SEC”), including in argenx’s most recent annual report on Form 20-F filed with the SEC as well as subsequent filings and reports filed by argenx with the SEC. The reader should not place undue reliance on any forward-looking statements included in this presentation. These statements speak only as of the date made and the Company is under no obligation and disavows any obligation to update or revise such statements as a result of any event, circumstances or otherwise, unless required by applicable legislation.

Today’s Agenda
Advancing Towards argenx 2025 | Tim Van Hauwermeiren, Chief Executive Officer and Co-Founder
Efgartigimod: Differentiation of our Anti-FcRn Fc Fragment | Hans de Haard, Chief Scientific Officer and Co-Founder
Fifth Efgartigimod Indication: Myositis | Bas van der Woning, Research Fellow
Sixth Efgartigimod Indication: Bullous Pemphigoid | Peter Verheesen, Research Fellow
KOL Panel: Myositis and Bullous Pemphigoid | Moderated by Albert Kovera, Global Marketing• Rohit Aggarwal, MD, MS, University of Pittsburgh Medical Center• Russell Hall, MD, Duke University Medical Center
ARGX-117 Phase 1 Data | New Biology Insights for Multifocal Motor NeuropathyOlivier Van de Steen, Medical Director | Inge Van de Walle, Principal Scientist
Q + A
4

Visit the argenx R&D Day Microsite to View Additional Resources
Myositis and Bullous Pemphigoid
Disease Overview
Patient Stories
MG Experience in China
Discussion on FcRn and Albumin
Relevant Publications
5

Advancing Towards argenx 2025Tim Van HauwermeirenCo-Founder and CEO

Where critical patient need meets breakthrough science
That is where we redefine immunology

2021: Reaching Myasthenia Gravis Patients with EfgartigimodNew modality Only Fc fragment targeting FcRn
Designed ADAPT with patient input
Defined disease biology
Engaging MG community
Correlation of total IgG and MG ADL
8

Efgartigimod: A Precision Tool to Revolutionize Autoimmunity
ITP
Lupus Nephritis
MyastheniaGravis
Myositis
GBS
CIDP
NeuromyelitisOptica
PemphigusAMR
Sjogren’s Syndrome
MembranousNephropathy
ThyroidEye Disease
BullousPemphigoid
IgG
IgG IgG
IgG
9

Myositis: IgG-Mediated Biology
Neuromuscular Disease
Myasthenia Gravis
Chronic Inflammatory Demyelinating
Polyneuropathy
Myositis
AChR, MuSK, LRP4 autoantibodies comprise ~90% of MG patients
40% anti-myelinated peripheral nerve IgGs
Autoantibodies characterized in 70% of patients across IMNM, ASyS and DM
IND filing by end of 2021 pending interactions with FDA
ADHEREGO/NO-GO
+ ADAPT Data
NextOpportunity
+
+
Neuromuscular Disease
Neuromuscular Disease
IMNM: Immune-Mediated Necrotizing Myopathy ASyS: Anti-Synthetase Syndrome DM: Dermatomyositis
Gilhus et al., Nature Rev/Disease Primers. 2019; Gilhus et al., NEJM, 2016; Querol et al., Nat Rev Neurol. 2017; Schmidt, Journal Neuromusc Diseases. 2018; Aquilar-Vazquez et al., Frontiers in Immunology. 2021; McHugh, Managing Myositis. 2019 10

Bullous Pemphigoid: Expanding the Skin Franchise
Pemphigus Pemphigoid
Autoantibody Driven DSG1 and DSG3
Convincing Rationale IVIg, PLEX, Immunoadsorption demonstrate role of IgG
Unmet Patient Needs Fast-acting, tolerable therapies; ability to taper corticosteroids
Autoimmune Blistering Diseases
Primary Endpoint Complete or partial remission off corticosteroids
BP180 and BP230
Registrational trial to start by end of year in parallel to ongoing pemphigus trial
11

Our Pipeline Starts with our Immunology Innovation Program
ANTIBODY ENGINEERING
CLINICAL DEVELOPMENT
First in Class | Unique Design | Multiple Indications
Efgartigimod ARGX-119ARGX-117
Internal Value Creation
LEADING TRANSLATIONAL BIOLOGY LABS
External Value Creation
CusatuzumabLEO
(ARGX-112)Genor
(ARGX-109)AbbVie
(ARGX-115)
ARGX-118AgoMAb
(ARGX-114)Staten
(ARGX-116)Dualyx
12

Neuromuscular Franchise: A Company within a Company
2021 2022 2023 - 2026
MG MG-SC
Myositis
CIDP
MMN
Leveraging infrastructure across multiple indications and molecules
EfgartigimodFcRn antagonist
ARGX-117C2 inhibitor
ARGX-119SIMPLE Antibody™ aimed to boost
the neuromuscular junction in disease
IIP ProgramsMG
CIDP
ALS
MMN
Myositis
SMA
MuSK MG
Congenital MG
13

Efgartigimod in 15 indications (commercial or development)
Global autoimmune market has surpassed $150B
Vibrant neuromuscular, hematology and skin franchises
New asset each year from IIP
Efgartigimod available globally
ARGX-117 in multiple late-stage trials
Building a Leading Immunology Company
Committed to our Patients and their
Communities
Enviable Immunology
Pipeline
Proof-of-concept demonstrated with ARGX-119
Rooted in Science through our IIP
We believe the future belongs to those who collaborate best14

Efgartigimod in 15 indications (commercial or development)
Global autoimmune market has surpassed $150B
Vibrant neuromuscular, hematology and skin franchises
New asset each year from IIP
Efgartigimod available globally
ARGX-117 in multiple late-stage trials
Building a Leading Immunology Company
Committed to our Patients and their
Communities
Enviable Immunology
Pipeline
Proof-of-concept demonstrated with ARGX-119
Rooted in Science through our IIP
We believe the future belongs to those who collaborate best
argenx2025
15

Efgartigimod: Differentiation of our Anti-FcRn FragmentHans de HaardChief Scientific Officer and Co-Founder

FcRn Plays a Key Role in IgG and Albumin Homeostasis
Lysosome
Endothelial Cell
Circulating antibodies are taken up in the cell via pinocytosis. In the endosome, IgG antibodies bind to FcRn1,2
Unbound IgGs enter the lysosomal degradation pathway, while FcRn-bound IgGs are rescued from degradation1,2
The IgG antibodies bound by FcRn are then released back into circulation, thereby extending their half-life1,2
IgG Antibody
IgG Autoantibody
FcRn
Endosome
Studies have shown:
AlbuminAlbumin is recycled by FcRn, independently of IgG
FcRn, neonatal fragment crystallizable receptor; IgG, immunoglobulin G.(1) Sesarman et al., Cell Mol Life Sci. 2010; (2) Habib et al., Supp Neuro Review. 2020.
1
2
3
1
1
2
3
17

Efgartigimod Fc Fragment Binds to FcRn in Same Way as Endogenous IgGs
Efgartigimod binds to FcRn in the same formation as endogenous IgG
Our hypothesis is that different binding properties of FcRn antagonists lead to different subcellular trafficking pathways
Ulrichts et al, Clin Invest. 2018
1 2 3
EndogenousFcRn:IgG
Interaction
Anti-FcRn mAb
18

Efgartigimod Keeps FcRn in its Recycling Path
No treatment Efgartigimod Control anti-FcRn mAb
FcRn over time Normalized Sum Volume (FcRn)
No
rmal
ize
d V
olu
me
(%
)
Time (Min)
19

Albumin Serves a Crucial Role in Lipid Housekeeping
Serum albumin is proposed to enhance cholesterol transport, facilitating steady state levels as cholesterol is metabolized
Inflammatory process Underlying conditions
Low serum albumin levels
Vasodilatory ability ↓ Vascular permeability ↑ Anticoagulation ↓
Cholesterol transport and LDL catabolism
Adverse cardiovascular events
Small molecule binding(toxins & medicines)
Proposed Interactions Between Serum Albumin and CV Outcomes4
(1) Law S, et al. Int J Mol Sci. 2019; (2) Packard CJ, et al. J Lipid Res. 2000; Noto D. et al., Kidney International. 1999; (4) Chien SC, et al. Biomark Res. 2017; (5) Sankaranarayanan S, et al. J Lipid Res. 2013
↓
20

Efgartigimod Blocks IgG Binding to FcRn Without Reducing Albumin
• Potent reduction in IgG levels without decrease in albumin or increase in LDL levels• No albumin decreases observed with chronic dosing out to 34 weeks in Phase 2 pemphigus trial (25mg/kg dose)• Selective blockade of IgG recycling without affecting serum albumin levels is emerging as a key differentiator in the FcRn space• Maintaining levels of human serum albumin is important for lipid housekeeping as well as other key physiological functions
Phase 3 ADAPT Trial of Efgartigimod in Myasthenia Gravis Patients
IgG levels – 1st cycle Albumin and LDL Cholesterol levels – 1st & 2nd cycles
Alb
um
in (
g/L)
Howard et al., The Lancet Neurology. 2021
LDL
(mm
ol/
L)Week Week
21

Efgartigimod: Data Support Favorable Benefit to Risk Ratio
No evidence of dose-limiting toxicities in healthy volunteers or
patients across trials
Opportunity to dose efgartigimod to maximum PD effect
600+ subjects dosed
125+ patients on efgartigimod for
over 12 months
100patients on efgartigimod
for over 18 months
Clinical proof-of-concept in
four indications (MG, ITP, PV, CIDP)
22

Fifth Efgartigimod Indication: MyositisBas van der WoningResearch Fellow

Idiopathic Inflammatory Myopathy (IIM) or Myositis
Rare, severe autoimmune disorders characterized by chronic muscle inflammation, pain and impaired quality of life; no FDA-approved therapies for myositis
MYOSITIS IS MEDIATED BY AUTOANTIBODIES
14 per 100,000
Mid-adult onset
More commonin females
High impact on quality of life: muscle atrophy, pain, functional impairment, dysphagia, dyspnea
High mortality rate: malignancy, interstitial lung disease and infections
No consensus guidelines for management
Treated primarily by rheumatologists and neurologists
Proximal muscle weakness is unifying feature of myositis subsets
PREVALENCE BURDENTREATMENTHALLMARK
Significant market opportunity with ~33K eligible patients in the U.S.
Myositis subsets mediated by autoantibodies: immune-mediated necrotizing myopathy (IMNM), anti-synthetase syndrome (ASyS), and dermatomyositis (DM)
(1) Meyer et al., Rheumatology. 2015; (2) Pinal-Fernandez et al., Curr Rheumatol Rep. 2018; (3) Schmidt, Journal of Neuromuscular Diseases. 201824

Many Myositis-Specific Autoantibodies Have Been Identified
EULAR/ACR* classification criteria for adult myositis
Classification IMNM, ASyS and DMbased on clinical symptoms
*American College of Rheumatology European Alliance of Associations for Rheumatology
Aggarwal; Lundberg, Ann Rheum Dis. 2017
DMOverlapMyositis
SRP
U1RNP
PM-Scl
Ku
Mi-2
MJ
PL-12
Jo-1
PL-7
Polymyositis
EJ
TIF-1γ
HMGCR
MDA-5
KS
OJ
SAE
IMNM
ASyS Myositis classification is based on myositis-specific autoantibodies (IgG) and clinical symptoms
25

IMNM Autoantibodies Trigger Muscle Damage and Impair Muscle Regeneration
Anti-SRP/-HMGCR autoantibodies bind
muscle fiber
Classical complement activation →
Myolysis (muscle enzymes e.g., CK)
Macrophage recruitment and activationIL-1, IL-6, TNF → atrophy
5 Blocking myotube formation
Allenbach, Nature Reviews Rheumathology. 2020
Necrosis
Complement independent Autoantibodies
1
2
3 4
Complement dependent Complement independent
26

DM and ASyS Autoantibodies Activate Complement and Type 1 Interferon
Autoantibodies
Complement Activation
Interferon Production
Myolysis
Disruption of capillaries Hypoperfusion
Type 1 Interferon• Impaired myotube formation• Impaired angiogenesis: destruction of capillaries and hypoperfusion
Atrophy
21
21
Increased autoantibody production
Dendritic cells produce Type 1 interferon from immune complexes
Necrosis
complement
Complement Activation
1 2
27

Autoantibodies are Central Mediators of Myositis Pathophysiologies
Complement activation of muscle lysis
Complement activation of endothelial cell lysis
Interferon production alpha/beta induce atrophy
Inhibition of myotube formation
Summary of Mode of Action of Autoantibodies
complement
type 1 interferon
myotubeautoantibody
28

Efgartigimod Designed to Clear IgG Autoantibodies Regardless of Target Antigen
Myositis patients can have myositis-specific autoantibodies (MSA+), myositis-associated autoantibodies (MAA+) or autoantibodies against yet unknown targets
IMNM (70% MSA+) ASyS (100% MSA+) DM (75% MSA+)
Defining new myositis biology
anti-SRP
Anti-HMGCR
MAA or Abs against unidentified targets
anti-Jo-1
anti-PL-12
anti-PL-7
other anti-synthetases
anti-Mi-2
anti-NXP-2
anti-MDA5
anti-TIF-1y
anti-SAE
MAA or Abs againstunidentified targets
29

Biology Rationale is at the Core of our Indication Selection
Preclinical EvidencePassive transfer model of IMNM autoantibodies from patient serum induce muscle weakness and loss of grip strength in mice
Clinical EvidenceNo approved targeted therapies for myositis but common immune therapies* show correlation of autoantibodies to disease progression
• Correlation of identity of autoantibodies to muscle damage across myositis subtypes
• Direct link between titer of autoantibody and disease activity
• Rituximab and IVIg evidence demonstrate autoantibodies are foundational drivers of disease
*Plasmapheresis and immunoadsorption (commonly used as correlates for efgartigimod) are not used in the treatment of myositis
30

Autoantibody Levels Correlate to Indicators of Myositis: CK Levels and Muscle Strength
Benveniste et al., Arthritis Rheumatol. 2011; Stone et al., Arthritis and Rheumatism 2007; Allenbach et al, Medicine (Baltimore). 2014; Muro et al., Rheumatology 2012
Patients were treated with standard of care immunosuppressants
• Similarly, anti-HMGCR, -Jo-1 and -Mi-2 titers correlate with CK levels and muscle strength• Anti-MDA5, -Jo-1 and -Mi-2 titers correlate with extramuscular disease activities (e.g. interstitial lung disease, skin disease)
31

ASyS and DM: Anti-Jo-1 and Anti-Mi-2 Patients Respond to Rituximab
Shorter time to improvement in patients positive for anti-Jo-1 and anti-Mi-2 autoantibodies
Anti-Jo-1 and anti-Mi-2 levels decreased after B-cell depletion
Correlation of anti-Jo-1 and anti-Mi-2 titers with disease activity measures
Endpoint based on 6 measures: PhGA, PTGA, HAQ, MMT-8, muscle enzymes, extramuscular disease activity score
Anti-Jo-1 and anti-Mi-2 autoantibodies are predictive biomarkers for response
Aggarwal et al, Arthritis Rheumatol. 2015
32

DM Patients Respond to IVIg
ProDERM study:% of patients with increase of ≥20 points on Total Improvement Score (TIS) at week 16
IVIg Placebo
TIS≥20 78.7% 43.8%
TIS≥40 68.1% 22.9%
Aggarwal et al., Arthritis Rheumatol. 2020
2g/kg IVIg/Placebo
33

IMNM Autoantibodies from Patient Serum Induce Muscle Weakness and Loss of Grip Strength
IgG purified from plasma from anti-SRP and anti-HMGCR IMNM patients causes loss of grip strength and muscle weakness in recipient mice
Necrosis and complement deposition are observed similarly inrecipient mice as in IMNM patients
NECROSIS
COMPLEMENT DEPOSITION
Bergua et al., Ann Rheum Dis. 2018
34

1
2
3
Significant Market Opportunity Across Myositis Subsets
REA
CH
ING
PATIENTS
DEFINING NEW BIOLOGY
IMNM:
4K pts U.S.
ASyS:
8K pts U.S.
DM:
21K pts U.S.
33KEstimated eligible myositis patients in U.S.
Role of autoantibody is best-characterized in IMNM
IMNM anchors market opportunity
Building a Basket Trial Concept
Basket trial approach to include ASyS and DM as well
Reaching more patients with high unmet need
Efgartigimod may allow us to redefine all three myositis subsets as being truly IgG-mediated
35

Adaptive Phase 2/3 Enrichment Design
1000mg efgartigimod SC (+ SOC)
Placebo SC (+ SOC)
Total Duration: 26 weeks
Independent adjudication committee
Stratified for• IMNM• ASyS• DM• Severity of muscle
weakness (MMT)
Eligibility criteria• Minimal muscle
weakness• No malignancies Adaptive enrichment
Interim analysis
Independent DSMB
Subpopulation adjustment Sample size re-estimation
IMNM
ASyS
DM
PrimaryResponse based onTotal Improvement Score (TIS)ACR/EULAR endorsed
Key Secondary• Mean change and duration in TIS• Quality of Life• Individual Core Set Measures TIS
• MMT-8 score• Physician Global
Assessment• Patient Global Assessment• HAQ-Disability Index score• Extramuscular Global
Assessment• Muscle enzyme serum level
1000mg efgartigimod SC (+ SOC)
Placebo SC (+ SOC)
1000mg efgartigimod SC (+ SOC)
Placebo SC (+ SOC)
IND filing by end of 2021 pending interaction with DCOA and CID division of FDA
180 patients Proposed Endpoints
Adults
36

Efgartigimod is designed to reduce all IgGsregardless of target antigen and can further elucidate myositis biology
Clinical evidence links IgG levels to disease activity
Conclusions
First basket trial design based on unifying biology
>30,000 IMNM, ASyS and DM patients in the U.S. Diverse panel of IgG autoantibodies emerge as key driver of muscle inflammation
Adaptive enrichment trial enables enrollment of broader patient population
37

Sixth Efgartigimod Indication: Bullous PemphigoidPeter VerheesenResearch Fellow

Bullous Pemphigoid: Most Common Autoimmune Blistering DiseaseSevere, rare, chronic and recurrent autoimmune disorder characterized by fluid-filled blisters, itching and skin redness
BULLOUS PEMPHIGOID IS MEDIATED BY AUTOANTIBODIES
12 per 100,0001
Increasing with aging population
Median age of onset is 81 years
Time to remission
High relapse rate
Side effects from corticosteroids
No approved treatments
Topical/systemic corticosteroids, steroid-sparing agents, rituximab, IVIg
Severe blistering disease
Strong impact on quality of life
High mortality rate2.40 (U.S.)2
PREVALENCE UNMET NEEDTREATMENTBURDEN
Significant market opportunity with ~41K patients in the U.S.
(1) Wertenteil et al., J Am Acad Dermatol. 2019; (2) Tedbirt et al., JAMA Dermatol. 2021; argenx market research
39

Bullous Pemphigoid Autoantibodies are Origin of Blister Formation
Drawn after Schmidt E, Zillikens D. Lancet. 2013; Fang H, Li Q, Wang G. Autoimmun Rev. 2020
• BP180 and BP230: key pathogenic hemidesmosomal antigens driving blistering between epidermis and dermis
• Autoantibody actions:
• Mechanical disruption of keratinocyte adhesion
• IgG autoantibody deposition triggers complement activation
• Recruitment and activation of immune cells (inflammatory cell recruitment, release of proteolytic enzymes)
40

Passive Transfer Model Highlights Toxicity of Bullous Pemphigoid Autoantibodies
Pathogenic autoantibodies induce typical skin lesions in murine passive transfer model of bullous pemphigoid
FcRn-knockout mice show fast elimination of pathogenic autoantibodies and are resistant to disease
Mice injected with BP180 Ab HDIG lowers BP180 Ab levels and improves disease scores
Mice injected with BP180 Ab FcRn -/-: Degradation of BP180 Ab
HDIG: High-dose human IgGLi et al., J Clin Invest. 2005
41

Bullous Pemphigoid Disease Activity Improves with Increasingly Selective IgG Therapies
Selectivity for IgG ResponseTrial
• Clear therapeutic benefit• Stronger response in severe disease• Fast improvement
• 100% complete remission• 70% prednisone dose reduction
Clinical evidence for the role of pathogenic autoantibodies in bullous pemphigoid
• Phase 3 double-blind randomized trial• 56 patients • High dose IVIg (5 days) + oral
corticosteroids
• Case series• 5 patients• PLEX (7–14 cycles) in 4-8 weeks
• Two case series• 27 patients*• Immunoadsorption (most 1 cycle)
• Strong antibody reductions• 68% complete remission • 37% off oral corticosteroids • No need for second cycle in most
patients
IVIg
PLEX
Immunoadsorption(Protein A)
* 4 recalcitrant BP, 3 first line with high disease activity, 20 severe or refractory(1) Kasperkiewicz et al., J Am Acad Dermatol. 2014; (2) Hübner et al., J Dtsch Dermatol Ges. 2018(3) Mazzi, Transfusion and Apheresis Science. 2003; (4) Amagai et al., J. Dermatol. Sci. 2017
42
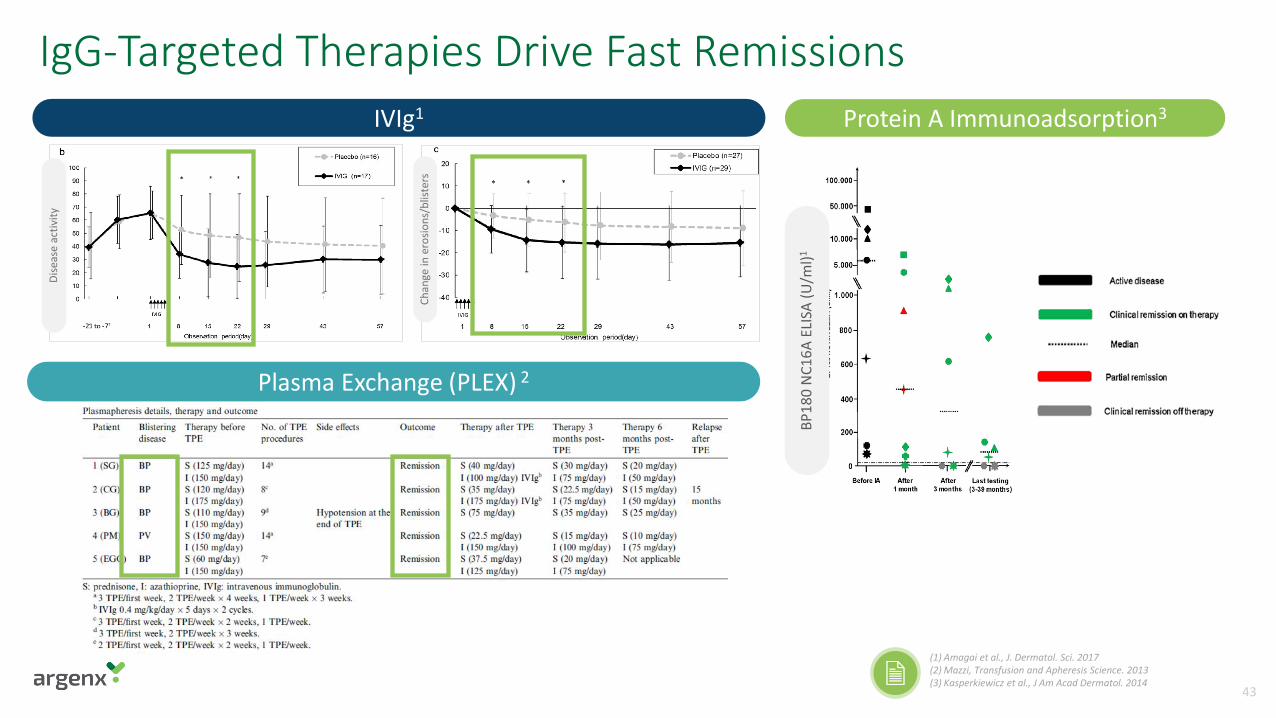
IgG-Targeted Therapies Drive Fast Remissions
Plasma Exchange (PLEX) 2
Dis
ease
act
ivit
y
Ch
ange
in e
rosi
on
s/b
liste
rs
IVIg1 Protein A Immunoadsorption3
BP
18
0 N
C1
6A
ELIS
A(U
/ml)
1
(1) Amagai et al., J. Dermatol. Sci. 2017(2) Mazzi, Transfusion and Apheresis Science. 2013(3) Kasperkiewicz et al., J Am Acad Dermatol. 2014
43

BULLOUS PEMPHIGOID
Pemphigus Serves as Proof of Concept for Autoimmune Blistering Diseases
PEMPHIGUS
Fast onset of action
Significant responses
Favorable tolerability seen in data to date
Autoantibodies initiate disease
Pathophysiology of blister formation more heterogeneous
Larger yet more elderly, fragile population
• 90% disease control after median time of 17 days
• 64% complete clinical remission after median 92 days• Corticosteroid sparing potential by using lower initial
doses of corticosteroids and rapid tapering
Proof of Concept in Initial Indication… …Before Expansion into Adjacent Indications
Important to confirm efgartigimod profile in pemphigus before expanding into other skin indications
S K I N B L I S T E R I N G D I S E A S E S – A U T O A N T I B O D Y D R I V E N
44

Registrational Study of Bullous Pemphigoid to Start in 2021
Total Duration: 36 weeks
Bullous Pemphigoid
Moderate-to-severe disease (BPDAI activity score ≥ 20)
Newly diagnosed and relapsing within 1 year of diagnosis
Proposed primary endpoint• proportion of participants in
complete or partial remission while off OCS
Secondary endpoints• cumulative dose of OCS• time to complete remission on
minimal OCS• proportion of participants with CDA
and remain free of relapse• quality of life
Followed by Open Label Extension study
Study Population Endpoints
Randomization (1:1)
Efgartigimod weekly SC
Placebo weekly SC
Concomitant Oral Corticosteroids (OCS)
OCS starting dose 0.5 mg/kg/day with ability to adjust
Active tapering to start from sustained control of disease activity (CDA)
45

IgG autoantibodies against BP180/BP230are hallmark of bullous pemphigoid
Conclusions
~41K bullous pemphigoid patients in U.S. Preclinical and clinical evidence links IgG autoantibody level to disease activity
Robust Phase 2 PoC data for efgartigimod in pemphiguslead to bullous pemphigoid Phase 3 trial design
Second registrational trial in skin franchise to start in parallel to ongoing pemphigus trial
46

KOL Panel: Myositis and Bullous Pemphigoid

Russell P. Hall III, MDJ. Lamar Callaway Professor, Department of Dermatology, Duke University Medical Center
Rohit Aggarwal, MD, MSRheumatology, Professor of Medicine, Medical Director, Arthritis and Autoimmunity Center, Co-Director UPMC Myositis Center, Division of Rheumatology and Clinical Immunology, Department of Medicine, University of Pittsburgh
48

ARGX-117 Phase 1 Data | New Biology Insights for Multifocal Motor NeuropathyOlivier Van de Steen, Medical Director
Inge Van de Walle, Principal Scientist

Inflammation
C5 convertase
C3 convertase
IgG IgM Mannose sugar Foreign surface
C3a-R
C5a-R
Sublytic MAC
ARGX-117 is First in Class Targeting C2(Auto)antibodies
Classical Lectin Alternative
Clearance by macrophages
Membrane damage
C3b C3 C3a
C5 C5a
C1qrs
C4
C2
C5b-C9MAC
C3
CFB CFD
MBL
MASPs
Microorganisms
50

C2 is Ideal Point of Intervention within Complement Cascade
C5 convertase
C3 convertase
Inflammation
IgG IgM Mannose sugar Foreign surface
C3a-R
C5a-R
Sublytic MAC
Target upstream of C5 to shut down all effector functions
Intact alternative pathway to reduce
infection risk
Crossroad of classical & lectin pathwaysManageable C2 levels in circulation
Benign C2-deficiency phenotype
(Auto)antibodies Microorganisms
Classical Lectin Alternative
Clearance by macrophages
Membrane damage
C3b C3 C3a
C5 C5a
C1qrs
C4
C2
C5b-C9MAC
C3
CFB CFD
MBL
MASPs
2
3
1
51

C5 convertase
C3 convertase
Inflammation
IgG IgM Mannose sugar Foreign surface
C3a-R
C5a-R
Sublytic MAC
Target upstream of C5 to shut down all effector functions
Intact alternative pathway to reduce
infection risk
Crossroad classical & lectin pathwayManageable C2 levels in circulation
Benign C2-deficiency phenotype
(Auto)antibodies Microorganisms
Classical Lectin Alternative
Clearance by macrophages
Membrane damage
C3b C3 C3a
C5 C5a
C1qrs
C4
C2
C5b-C9MAC
C3
CFB CFD
MBL
MASPs
2
3
1
IgG IgM Mannose sugar Foreign surface
C2 is Ideal Point of Intervention within Complement Cascade(Auto)antibodies Microorganisms
Classical Lectin Alternative
C1qrs
C4
C2
C3
CFB CFD
MBL
MASPs
Target upstream of C5 to shut down all effector functions
1
52

C5 convertase
C3 convertase
Inflammation
IgG IgM Mannose sugar Foreign surface
C3a-R
C5a-R
Sublytic MAC
Target upstream of C5 to shut down all effector functions
Intact alternative pathway to reduce
infection risk
Crossroad classical & lectin pathwayManageable C2 levels in circulation
Benign C2-deficiency phenotype
(Auto)antibodies Microorganisms
Classical Lectin Alternative
Clearance by macrophages
Membrane damage
C3b C3 C3a
C5 C5a
C1qrs
C4
C2
C5b-C9MAC
C3
CFB CFD
MBL
MASPs
2
3
1
IgG IgM Mannose sugar
C2 is Ideal Point of Intervention within Complement Cascade
Classical Lectin
C1qrs
C4
C2
MBL
MASPs
Intact alternative pathway to reduce
infection risk
2
53

C5 convertase
C3 convertase
Inflammation
IgG IgM Mannose sugar Foreign surface
C3a-R
C5a-R
Sublytic MAC
Target upstream of C5 to shut down all effector functions
Intact alternative pathway to reduce
infection risk
Crossroad classical & lectin pathwayManageable C2 levels in circulation
Benign C2-deficiency phenotype
(Auto)antibodies Microorganisms
Classical Lectin Alternative
Clearance by macrophages
Membrane damage
C3b C3 C3a
C5 C5a
C1qrs
C4
C2
C5b-C9MAC
C3
CFB CFD
MBL
MASPs
2
3
1
C2 is Ideal Point of Intervention within Complement Cascade
C4
C2
Crossroad of classical & lectin pathwaysManageable C2 levels in circulation
Benign C2-deficiency phenotype
3
54

Features of ARGX-117
Optimal recycling
pH and Ca2+
switch
No effector function
Sweeping Antibody
ARGX-117 Blocks and Actively Removes C2 from Circulation
Bind & block C2
Degradation of C2
1
3
Recycling of ARGX-1174
Uptake & drop off C22
55

Ongoing Robust Phase 1 First-in-Human Study
Single Ascending Dose (SAD): IV and SC
0.1 mg/kgIV
N=8
0.5 mg/kgIV
N=8
2.5 mg/kgIV
N=8
10 mg/kgIV
N=7
30 mg/kgIV
N=7
60 mg/kgIV
N=8
60 mg/kgSC
N=8
80 mg/kgIV
N=8
15 mg/kgSC
N=8
10-10-10-10*mg/kg
IVN=8
60-10-10# mg/kg
IVN=8
10-50-20# mg/kg
IVN=8
15-15-15-15* mg/kg SC
N=8
Multiple Ascending Dose (MAD): IV and SC
IMP = Investigational Medicinal Product*IMP administered on Days 1, 8, 15 & 22#IMP administered on Days 1, 8 & 22
• Broad dose range investigated with both IV and SC formulations (up to 80 mg/kg and 60 mg/kg respectively)• 102 subjects dosed (70 in SAD, 32 in MAD) yielding comprehensive clinical, PK/PD and biomarker dataset• 75 subjects exposed to ARGX-117
56

Phase 1 Safety Results Support Proof of Concept Studies in Patients
Treatment-Emergent Adverse Events (TEAE)
0.1mg/kg
0.5mg/kg
2.5mg/kg
10mg/kg
30mg/kg
60mg/kg
60mg/kg
SC
80mg/kg
15mg/kg
SC
10-10-10-10mg/kg
60-10-10mg/kg
10-50-20mg/kg
15-15-15-15mg/kg
SC
N (%)
Any 6 (75.0) 5 (62.5) 5 (62.5) 5 (71.4) 7 (100) 5 (62.5) 5 (62.5) 6 (75.0) 6 (75.0) 6 (75.0) 8 (100) 8 (100) 8 (100)
Grade 2 1 (12.5) 1 (12.5) 1 (12.5) - - 1 (12.5) 2 (25.0) - - - - - -
Grade 3 or higher
- - - - - - - - - - - - -
Serious - - 1 (12.5) - - - - - - - - - -
TEAE = treatment emergent adverse eventn = number of subjects that experienced at least one TEAE% = number of subjects (n) as percentageData Cut-off for Interim Analysis: May 20th 2021
• TEAEs primarily Grade 1 and not dose-related• Serious TEAE determined to be unrelated to drug• No increased risk of infection
Single and multiple administrations of ARGX-117 or placebo show favorable safety and tolerability profile to date*
*Safety data still blinded in Phase 1 study
57

Pharmacokinetics
• Estimated half-life ~ 65-70 days• Dose proportional increase of Cmax
• Sustained reduction in free C2 levels by 95% for > 100 days as of 30 mg/kg doseConclusions
Free C2 levels
Days
99% reduction
95% reduction
ARGX-117 SAD: Long Half-life and Sustained PD Profile
Days
58

• Induction dose followed by maintenance dosing concept established• Resulting robust PK/PD model informing dosing strategy for Phase 2 studies
DaysDays
99%reduction
95%reduction
ARGX-117 MAD: Consistent Activity
Pharmacokinetics Free C2 levels
Conclusions
59

Model assumes full complement blockage as of free C2 levels < 0.2 µg/mL or >99% reduction of free C2 levels
Model Predicts Potential for Infrequent Dosing
Free C2 levels
60

Phase 1 Data Support Path Forward and Potential for Individualized Dosing Schedule in Patients
Favorable safety & tolerability profile supports advancing to Phase 2 patient trials
Consistent PK/PD profile across IV and SC dosing that may enable infrequent dosing
Phase 2 trial in multifocal motor neuropathy (MMN) to start by end of year
61

Multifocal Motor Neuropathy:A Serious, Debilitating Autoimmune Disease
Need for new therapies that slow progression of disease and reduce reliance on IVIg
~13,000 patients in the U.S. –increasing
Often underdiagnosed
Predominantly men
Median age 40 years
Steroids ineffective
First line and only approved therapy is frequent, high doses of IVIg over 2-5 days
Often misdiagnosed as ALS
Takes ~1.5 years for correct diagnosis
Nerve conduction blocks
Anti-GM1 IgM antibody presence
Slowly progressive muscle weakness due to motor neuron degeneration
Mainly affects hands and forearms -patients become dependent
PREVALENCE UNMET NEEDDIAGNOSISHALLMARK
>$0.5B IVIg sales and growing
Persson et al., Br J Dermatol. 2021; Tedbirt et al., JAMA Dermatol. 2021; Wertenteil et al., J Am Acad Dermatol. 2019; argenx market research
62

Anti-GM1 Antibodies Activate Classical Complement Pathway
Muscle weakness
1 2
3 4
IgM autoantibodies bind to GM1 located on motor neurons and Schwann cells
IgM autoantibodies are potent activators of the complement cascade
IgM titer is correlated with classical pathway complement deposition
Complement activity correlates with disease severity
SoC IVIg reduces C3b deposition
Vlam et al, Neurol Neuroimmunol Neuroinflamm. 2015Yuki et al, J Peripheral Nervous System. 2011 IgM autoantibodies cannot be addressed by efgartigimod
63

ARGX-117 Inhibits Complement Deposition on Motor Neurons and Schwann Cells
C3
DEP
OSI
TIO
NC2 depleted serum + 100% C2
C3
DEP
OSI
TIO
NIsotype control IVIg C2 depleted serum ARGX-117
Complement active serum
Serum MMN Patient
Motor neurons
Schwann cells
64

Complement active serum
ARGX-117 Blocks C3 Deposition in Dose-Dependent Manner
Isotype control
C2 depleted serum
C3
DEP
OSI
TIO
NC
3 D
EPO
SITI
ON
ARGX-117 (200 µg/mL – 3,1 µg/mL)
Reconstitution with hC2 (1,97 µg/mL - 30 µg/mL)
Motor neurons
Schwann cells
Complement active serum
65

ARGX-117 Protects Axon Integrity While Blocking C3 Deposition in ex vivo ModelARGX-117 prevents loss of neurofilament staining at the nerve terminal and thereby preserves the integrity of the axon by blocking C3 deposition and downstream complement activation
Isotype control ARGX-117
C3
de
po
siti
on
Ne
uro
fila
men
t
GalNAcT-/- (neuronal mice) - Yao et al., Journal of Neuroscience. 2014; Mouse model - McGonigal et al., Acta Neuropathologica Communications. 2016
66

Phase 2 Multifocal Motor Neuropathy Trial Design
Total Duration: 16 weeks
Trial to enroll approximately 45 MMN patients• Probable or definite
MMN (per EFNS/PNS 2010)
• Independent adjudication committee
• Stable IVIg regimen• IVIg treatment
dependent
Safety and tolerability
Time to IVIg re-treatment
Measures of peripheral muscle strength: grip strength, mMRC sum score, 9-HPT, MMN-RODS
Patient-reported outcomes
PK, PD, biomarkers
Patient Population Key Outcome Measures
Trial on track to start by end of 2021
ARGX-117 Dose Regimen 1 (N=15)
ARGX-117 Dose Regimen 2 (N=15)
Placebo (N=15)
ARGX-117Open-label Extension
Ran
do
miz
atio
n(1
:1:1
)
IVIgMonitoring
Period
4-10 weeks
67

ARGX-117: Pipeline-in-a-Product Opportunityfitting our franchises
MMNNeuro
Heme
Skin
Kidney
Indications
TherapeuticFranchises
Classical Pathway
Lectin Pathway
GBS
IgAN
MN
CAD
IRI
MG
LN
ALS
ITP
C4GN
MGUS anti-MAG
BP
HS
68

Q&A
Tim Van HauwermeirenChief Executive Officer and Co-Founder, argenx
Hans de Haard, PhDChief Scientific Officer and Co-Founder, argenx
Wim Parys, MDChief Medical Officer, argenx
Keith WoodsChief Operating Officer, argenx
Karl GubitzChief Financial Officer, argenx
Bas van der Woning, PhDResearch Fellow, argenx
Peter Verheesen, PhDResearch Fellow, argenx
Rohit Aggarwal, MD, MSUniversity of Pittsburgh
Russell P. Hall III, MDDuke University
Olivier Van de Steen, MDMedical Director, argenx
Inge Van de Walle, PhDPrincipal Scientist, argenx