new thinking on fractionation in radiotherapy€¦ · vs standard fractionation. non-small-cell...
TRANSCRIPT

1
New Thinking on Fractionation in Radiotherapy
Alan E. NahumVisiting Professor, Physics dept., Liverpool university,

2
• An honorarium is provided by Accuray for this presentation
• The views expressed in this presentation arethose of the presenter and do not necessarilyreflect the views or policies of AccurayIncorporated or its subsidiaries. No officialendorsement by Accuray Incorporated, orany of its subsidiaries, of any vendor,products or services contained in thispresentation is intended or should beinferred.

3
• Aswin Hoffmann PhDOncoRay, Dresden
• Julien Uzan PhDRaySearch AB, Stockholm (formerly ClatterbridgeCancer Centre, Merseyside, UK)
Acknowledgements

4
• All tumours have α/β ~10 Gy
• All late normal-tissue complications have α/β ~3 Gy
• Fraction sizes of 2 Gy ensure optimal ’therapeutic ratio’
• Hypofractionation (~ 4 - 6 Gy) reserved for palliative cases
• New SBRT regimens with 15 – 20 Gy fraction sizes for small lung tumours considered by many to be ’dangerous’
• Advances in external-beam radiotherapy heavily focussed on intensity modulation, possibly also protons i.e. on evermore conformal dose distributions.
‘Old’ thinking on Fractionation up to ~15 years ago:

5
The LINEAR-QUADRATIC model:Surviving fraction SF = exp (-αD - βMAXD 2) -ln(SF)/D = α + βMAXD
Strong experimental support for the LQ model

The ’classic’ Withers LQ-basedIso-Effect Formula :
6
7
0 5 10 15 20 25 30 35 40 45 50 5510-5
10-4
10-3
10-2
10-1
100
20 × 2.75 Gy
3 × 8.9 Gy
Surv
ivin
g fra
ctio
n
Total (tumor) dose (Gy)
α/β = 3 Gy
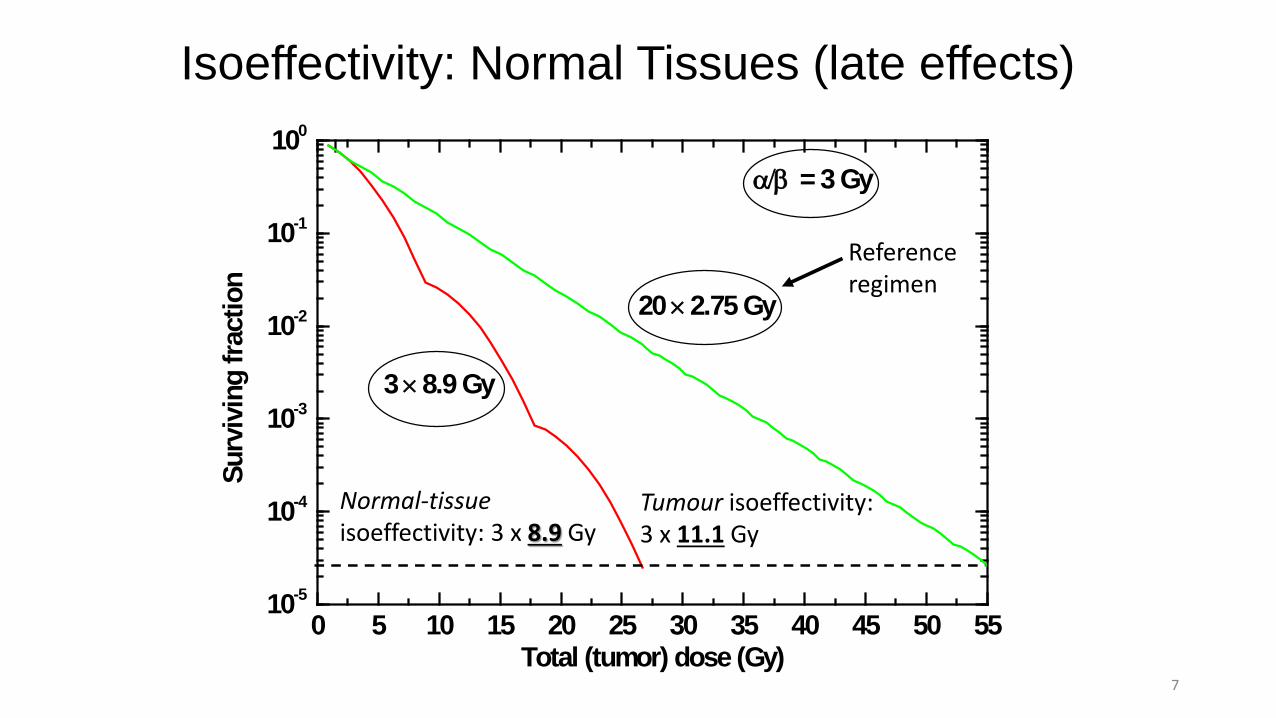
Isoeffectivity: Normal Tissues (late effects)
Normal-tissueisoeffectivity: 3 x 8.9 Gy
Tumour isoeffectivity: 3 x 11.1 Gy
Referenceregimen

8
Breast tumours (thanks to Dr. Navita Somaiah, Royal Marsden)
• Breast cancer clonogens as sensitive to fraction size as the dose-limiting normal tissues
• α/β ≈3 from trials done in the UK (J. Yarnold et al) and elsewhere.
• 40Gy/15F is ‘gentler’ than 50Gy/25F & non-inferior in terms of tumour control; 5-fraction schedule under test
Total hypo# α/β Ratio 95% CI
Mirabel 5969 3559 1.4 Gy 0.9-2.2
Proust-Lima 5093 1949 1.55 Gy 0.46-4.52Fowler IJROBP 2001;50:1024; Brenner IJROBP 2002;52:6; Mirabel IROBP 2011; Proust-Lima IJROBP 2011;79:195-201
Prostate tumours Clinical/biological modelling results:
(thanks to Dr. Isabel Syndikus, Clatterbridge)
9
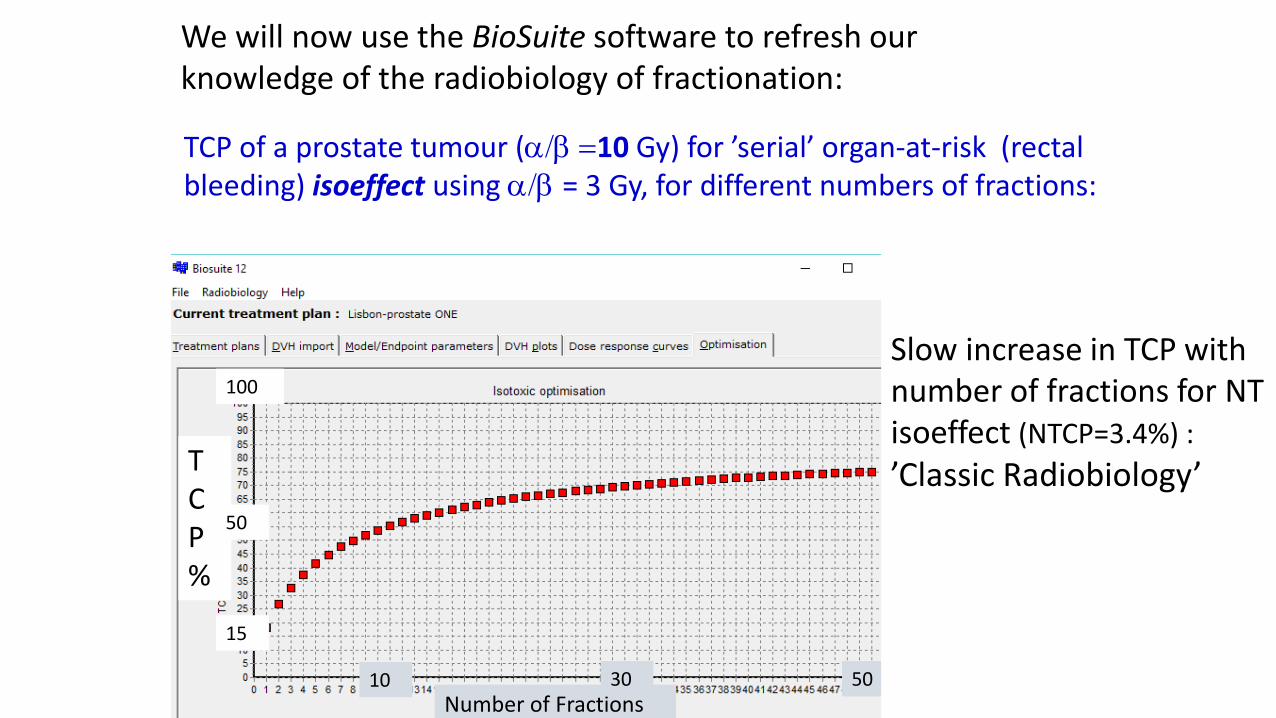
We will now use the BioSuite software to refresh ourknowledge of the radiobiology of fractionation:
TCP of a prostate tumour (α/β =10 Gy) for ’serial’ organ-at-risk (rectalbleeding) isoeffect using α/β = 3 Gy, for different numbers of fractions:
TCP%
100
50
15
Number of Fractions503010
Slow increase in TCP withnumber of fractions for NT isoeffect (NTCP=3.4%) :’Classic Radiobiology’

10
This time the α/β for the tumour is low :
Prostate tumour (α/β = 3 Gy) TCP for ’serial’ organ-at-risk (e.g. rectal bleeding) isoeffect using α/β = 3 Gy, for different numbers of fractions:
TCP constant as number offractions changes (for NT isoeffect - NTCP=3.4% )Also ’Classic Radiobiology’as α/β for normal tissue and tumour are equal.
TCP%
Number of Fractions 503010
100
50
15

Now we introduce tumour clonogen proliferation, starting 3 weeks into the treatment:Prostate tumour (α/β = 3 Gy) TCP for ’serial’ organ-at-risk (e.g. rectal bleeding) isoeffect using α/β = 3 Gy, for different numbers of fractions:
TCP constant out to fractionnumber 15 (3 weeks fromstart) then decreases due toclonogen proliferation; theeffect of the weekendbreaks can be seen.
TCP%
Number of Fractions15 5040
100
50
15

12
NTCPRP = 12% in each case
Computed using BioSuite
P20 PTV = 78.0 cm3
P01 PTV = 51.2 cm3
P16 PTV = 106.6 cm3
Significant Potential to individualize the number offractions i.e. not just SABR vs standard fractionation.
Non-small-cell Lung Tumours: 3 cases
Why such different behaviour from case to case?
Because the dose distributions in the paired lungs surrounding the tumour are so variable, and NTCP is a function of mean lung dose.
TCP%
Number of Fractions 5015

WIF is valid if:
– Early (animal) experiments which formed the basis for the low (α/β)NT and high (α/β)T hypothesis fulfilled the first of the above conditions
– For all other situations, WIF as presently applied to NTs is simply wrong
13
• EITHER NT receives the same uniform dose as the tumour.• OR the NT response is solely determined by its maximum
dose (100% serial organ) ≈ tumour dose
e.g. Lung NTCP follows ≈ mean dose
Back to the Withers Iso-Effect Formula (WIF) :

aasss
– Left-hand expression should use the dose distribution in the normal tissue instead of the tumour dose
Withers Isoeffect Formula (WIF)
14
– Practical Solution: replace (α/β)NT with an “effective” value which yields exact NT iso-effect whilst retaining the tumour dose in the WIF :
The Hoffmann-Nahum (α/β)eff concept
Normal tissue with ‘parallel’ architecture (n = 1):
WIF for Normal Tissue
(α/β)eff is frequently much higher than 3 Gyand can approach 10 Gy

15
RE-OXYGENATION – another reason to fractionate
Alite F. et al, Local control dependendence on consecutive vs.Nonconsecutive fractionation in lung stereotactic body radiation therapy,Radioth. Oncol. 121 9-14 2016.
”Five-fraction SBRT delivered over non-consecutive daysimparts superior Local Control and similar toxicity comparedto consecutive fractionation.”

• The ’old’ 2-Gy fraction size only applies to tumours with high α/βand with ’serial’ organ(s)-at-risk : i.e. head&neck.
• Small numbers of large fractions indicated for breast andprostate tumours due to their relatively low α/β
• ’Safe’ SBRT/SABR regimens with 15 – 20 Gy fraction sizes forearly-stage NSC lung tumours are ’proof’ of the influence of the’volume effect’ on fractionation sensitivity (N.B. lung tumour α/βnot low)
• The individualization of fraction size/number (TCP as f’n ofnumber of fractions under isoNTCP) e.g. with BioSuite ispotentially advantageous for any tumour where the principalorgan-at-risk is quasi-parallel – e.g. lung tumours surrounded bynormal lung
• Further advances in conformality - i,e. reduced normal-tissuecoverage per tumour dose - from RapidARC, proton therapy etc.will favour further hypofractionation: explore with BioSuite!
Take-home messages:

17
Fowler, J. F., Tome, W. A., Fenwick, J. D., and Mehta, M. P., A challenge totraditional radiation oncology, Int.J. Radiat. Oncol. Biol. Phys. 60 1241–12562004.
Uzan J and Nahum AE, Radiobiologically guided optimisation of the prescriptiondose and fractionation scheme in radiotherapy using BioSuite, British Journal ofRadiology 85 1279-86 2012.
Hoffmann A L and Nahum A E, Fractionation in normal tissues: the (α/β)effconcept can account for dose heterogeneity and volume effects, Physics inMedicine and Biology 58 6897-914 2013.
Chapman J.D. and Nahum A.E. Radiotherapy Treatment Planning Linear-Quadratic Radiobiology 2015 (CRC Press: Taylor & Francis Group). ISBN: 978-1-4398-6259-9.
Alan E Nahum. The Radiobiology of Hypofractionation. Clinical Oncology 27 260-269 2015.
BioSuite is available from [email protected]
References:

18
Thank you for your attention