new electronic submission for medicare secondary claims · issue for updates practitioner and ......
TRANSCRIPT

1
O C T O B E R 2 0 1 2 V O L . 1 4 , I S S U E 7
PHARMACY UPDATES
CLAIMS AND BILLING
WHAT ’S HAPPENING
HEALTH CARE POLICY
CPET CORNER
PROVIDER SEMINARS
QUALITY IMPROVEMENT
Office Injectable Medications and Vaccines . . . . . . 2
New Provider Portal Password Requirements . . 2
Get Your Payments Faster . . . . . . . . 2
Medical Policy Updates . . . . . . . 3
Check back next issue for updates
Practitioner and Staff Seminars and Training Sessions . . . . . . 7
Raising the Bar . . . . . . . . . . 9
Clinical Practice and Preventive Services Guidelines Online . . . . . . . 11
Prior Authorization . . 12
New Electronic Submission for Medicare Secondary Claims
Effective July 2012, professional providers can electronically submit Medicare secondary claims that did not automatically cross over from Medicare to CareFirst. Contact your electronic trading partner to find out if they have set up this capability with CareFirst.
How to Submit
These claims must contain specific information in the 837 claims transaction set. View the 5010 Companion Guide for details.
Claims received without the required information will be returned at the front-end with one of the following messages:
n 53815 or 53818 – Missing Primary Payer payment information
n 53816 – Adjustment cannot be sent electronically
n 53817 – Invalid Primary Payer Information
n 53819 – Provider must accept assignment to send Medicare Crossover electronically
View the chart with additional information on the front-end rejections. The rejection verbiage may differ depending on the trading partner.
Always allow 30 days from receipt of the Medicare Explanation of Benefits for claims to automatically cross over from Medicare and be processed by CareFirst. Before submitting a secondary claim to CareFirst, always check CareFirst Direct or the Voice Response Unit for claims status. The Medicare Explanation of Benefits indicates if the claim has been submitted to a secondary carrier for processing.
Questions?
For additional information, contact your trading partner or visit www.carefirst.com/providers/electronicclaims. Need an answer fast? Check out our online Medicare Secondary Claims FAQs.
Win a FREE gift . SEE HOW ON PAGE 12.

[ TABLE OF CONTE NTS] BLUEL INK > > OCTOBE R 2012
2WHAT ’S HAPPENING
CLAIMS AND BILLING
HEALTH CARE POLICY
CPET CORNER
PROVIDER SEMINARS
QUALITY IMPROVEMENT
PHARMACY UPDATES
W H A T ’ S H A P P E N I N G
New Provider Portal Password Requirements To improve the security of patient data, CareFirst requires users of CareFirst Direct and the Patient-Centered Medical Home (PCMH) Provider Portal to routinely update their passwords.
It is critical that you change your password to continue to have access to CareFirst Direct or the PCMH Provider Portal, if applicable.
n Users will be prompted to update their password five days prior to the password expiration date.
n If users do not reset their passwords within the five day timeline, another notification will be given two days prior to expiration and one final notification on the last day.
If your password expires and you are unable to reset, please contact your Office Manager for assistance initially. If your Office Manager is unable to reset your password, contact the CareFirst Service Desk at 1-877-526-8390.
Important: If you have more than one login due to multiple Tax IDs, we recommend that you change all of your passwords at the same time.
C L A I M S A N D B I L L I N G
Get Your Payments FasterAre you familiar with the Electronic Funds Transfer (EFT) process? EFT can make your claims payment process a quick and easy one by reducing paperwork, avoiding mail delays, and more. Visit www.carefirst.com/providers/electronicclaims for details.
How to Obtain Office Injectable Medications and Vaccines from Our Specialty Pharmacy Vendors Medications administered in the physician’s office are covered under the member’s medical benefit, not their prescription drug benefit. Prescription drug benefits cover injectable medications only when they are self-administered.
Providers should obtain office administered injectable medications and bill CareFirst directly. Providers should not write a prescription for the medication and have the member obtain the medication from the pharmacy with the intent of the member delivering the drug to the provider, as these medications are not covered by the member’s prescription drug benefit.*
For commercial members, providers may obtain injectable medications from a source of their choice. CareFirst and CareFirst BlueChoice have contracts with ICORE Healthcare** (ICORE Specialty Pharmacy), Walgreens Specialty Pharmacy** and OncoSourceRx** to ship single doses of most injectable medications and vaccines on an individual patient-prescription basis directly to the provider office for provider administration.
Please note that the Synagis vaccine can be ordered directly through ICORE and the Zostavax and the HPV vaccines can be ordered through ICORE and Walgreens. This option is available for most office injectables (drugs with limited distribution or special packaging requirements cannot go through this process), eliminating the need for upfront cost of stocking expensive specialty injectables as well as the need for patients to purchase the drug out-of-pocket and submit a claim. ICORE, Walgreens and OncoSourceRx obtain eligibility and benefits then bill CareFirst and CareFirst BlueChoice directly. Your practice should continue to bill CareFirst and CareFirst BlueChoice for the administration by following Current Procedural Terminology (CPT) guidelines and using the appropriate CPT code.
Orders for non-refrigerated, refrigerated and frozen medications and vaccines are packed in temperature controlled containers and shipped directly to your office-typically within 48 hours. Priority overnight delivery is also available. This is an optional service made available to our providers and not a guarantee of availability or supply by CareFirst. Not all drugs or individual prescriptions are available using this option. Please note that the arrangement with these specialty pharmacies does not apply to members whose primary coverage is Medicare.
If you are interested in using this service or verifying that a particular drug/prescription is eligible, please contact either ICORE Specialty Pharmacy at 866-554-2673, Walgreens Specialty Pharmacy at 888-347-3416 or OncoSourceRx at 888-662-6779.
FEP members only: Providers must obtain office injectables from Caremark.
* Exception: Depo-Provera® (when used for contraception) is the only non-self-administered injectable covered under the prescription drug benefit.
** Independent companies providing pharmaceutical services.
[ TABLE OF CONTE NTS] BLUEL INK > > OCTOBE R 2012
3WHAT ’S HAPPENING
CLAIMS AND BILLING
HEALTH CARE POLICY
CPET CORNER
PROVIDER SEMINARS
QUALITY IMPROVEMENT
PHARMACY UPDATES
H E A LT H C A R E P O L I C Y
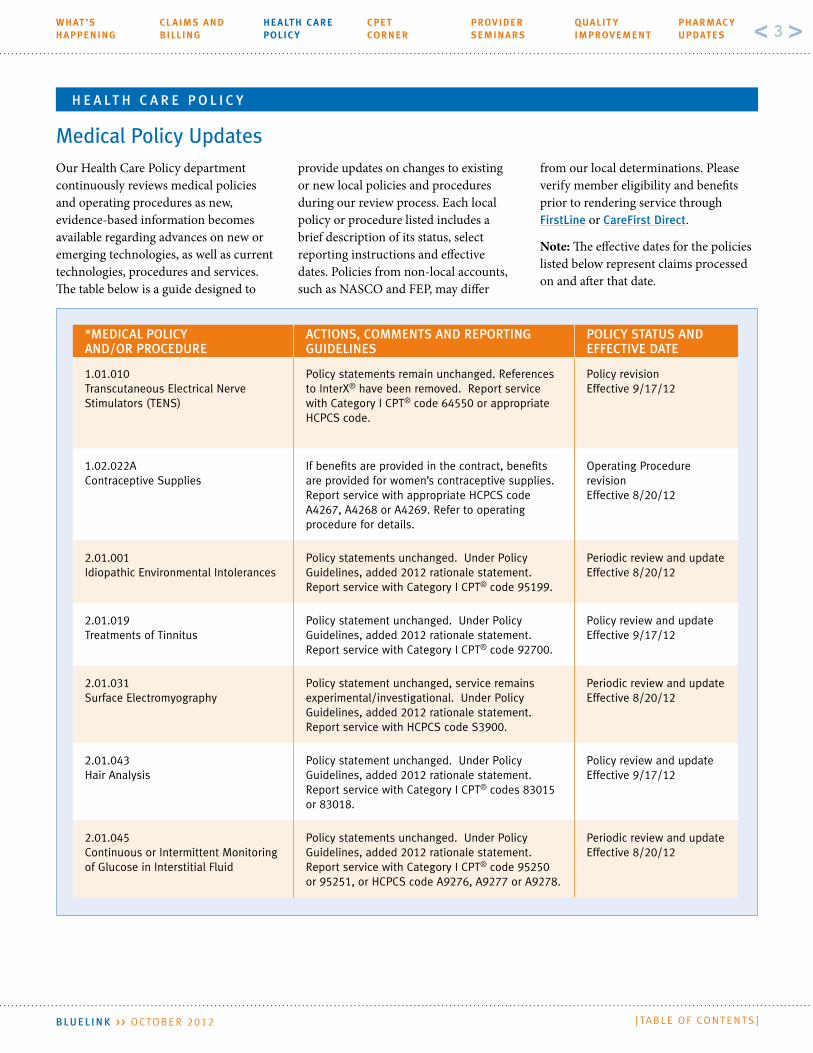
Medical Policy UpdatesOur Health Care Policy department continuously reviews medical policies and operating procedures as new, evidence-based information becomes available regarding advances on new or emerging technologies, as well as current technologies, procedures and services. The table below is a guide designed to
provide updates on changes to existing or new local policies and procedures during our review process. Each local policy or procedure listed includes a brief description of its status, select reporting instructions and effective dates. Policies from non-local accounts, such as NASCO and FEP, may differ
from our local determinations. Please verify member eligibility and benefits prior to rendering service through FirstLine or CareFirst Direct.
Note: The effective dates for the policies listed below represent claims processed on and after that date.
*MEDICAL POLICY AND/OR PROCEDURE
ACTIONS, COMMENTS AND REPORTING GUIDELINES
POLICY STATUS AND EFFECTIVE DATE
1 .01 .010Transcutaneous Electrical Nerve Stimulators (TENS)
Policy statements remain unchanged . References to InterX® have been removed . Report service with Category I CPT® code 64550 or appropriate HCPCS code .
Policy revisionEffective 9/17/12
1 .02 .022AContraceptive Supplies
If benefits are provided in the contract, benefits are provided for women’s contraceptive supplies . Report service with appropriate HCPCS code A4267, A4268 or A4269 . Refer to operating procedure for details .
Operating Procedure revisionEffective 8/20/12
2 .01 .001Idiopathic Environmental Intolerances
Policy statements unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with Category I CPT® code 95199 .
Periodic review and updateEffective 8/20/12
2 .01 .019Treatments of Tinnitus
Policy statement unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with Category I CPT® code 92700 .
Policy review and updateEffective 9/17/12
2 .01 .031Surface Electromyography
Policy statement unchanged, service remains experimental/investigational . Under Policy Guidelines, added 2012 rationale statement . Report service with HCPCS code S3900 .
Periodic review and updateEffective 8/20/12
2 .01 .043Hair Analysis
Policy statement unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with Category I CPT® codes 83015 or 83018 .
Policy review and updateEffective 9/17/12
2 .01 .045Continuous or Intermittent Monitoring of Glucose in Interstitial Fluid
Policy statements unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with Category I CPT® code 95250 or 95251, or HCPCS code A9276, A9277 or A9278 .
Periodic review and updateEffective 8/20/12

[ TABLE OF CONTE NTS] BLUEL INK > > OCTOBE R 2012
4WHAT ’S HAPPENING
CLAIMS AND BILLING
HEALTH CARE POLICY
CPET CORNER
PROVIDER SEMINARS
QUALITY IMPROVEMENT
PHARMACY UPDATES
H E A LT H C A R E P O L I C Y
*MEDICAL POLICY AND/OR PROCEDURE
ACTIONS, COMMENTS AND REPORTING GUIDELINES
POLICY STATUS AND EFFECTIVE DATE
3 .01 .011AAutism Spectrum Disorders (Virginia Mandate)
Updated Provider Guidelines regarding information on Applied Behavior Analysis . These services should be reported using HCPCS codes H0031, H0032, H2012, H2014 and H2019, and may only be reported by a Virginia Board of Medicine Licensed Behavior Analyst . Refer to Operating Procedure for details .
Operating procedure revisionEffective 8/20/12
4 .02 .008Recurrent Pregnancy Loss (Recurrent Spontaneous Abortion)
Policy statements unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with appropriate Category I CPT® code .
Review and updateEffective 8/20/12
5 .01 .019Palivizumab (Synagis®) for Immune Prophylaxis for Respiratory Syncytial Virus (RSV)
Palivizumab (Synagis®) is considered medically necessary for certain indications based on the current recommendations from The American Academy of Pediatrics (2012) . The prior authorization process for Palivizumab requests remains the same . Check the member’s contract to determine if prior authorization is required for Palivizumab services . When prior authorization is required, prior authorization approval for Palivizumab is obtained through ICORE Healthplan . Report service with Category I CPT® code 90378 . Refer to policy for details .
New policyEffective 9/17/12
6 .01 .014Ultrasound for the Evaluation of Paranasal Sinuses
Policy statement unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with HCPCS code S9024 .
Policy review and updateEffective 9/17/12
6 .01 .018Neutron Beam Radiotherapy
Policy statement unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with Category I CPT® codes 77422 or 77423 .
Policy review and updateEffective 9/17/12
7 .01 .003Bone-Anchored Hearing Aids
Policy statements unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with Category I CPT® codes 69714 or 69715 or HCPCS codes L8690, L8691, L8692 or L8693 .
Policy review and updateEffective 9/17/12
7 .01 .006Dynamic Cardiomyoplasty
Policy statement unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with Category I CPT® unlisted code 33999 .
Policy review and updateEffective 9/17/12

[ TABLE OF CONTE NTS] BLUEL INK > > OCTOBE R 2012
5WHAT ’S HAPPENING
CLAIMS AND BILLING
HEALTH CARE POLICY
CPET CORNER
PROVIDER SEMINARS
QUALITY IMPROVEMENT
PHARMACY UPDATES
H E A LT H C A R E P O L I C Y
*MEDICAL POLICY AND/OR PROCEDURE
ACTIONS, COMMENTS AND REPORTING GUIDELINES
POLICY STATUS AND EFFECTIVE DATE
7 .01 .074Extracorporeal Shock Wave Treatment for Plantar Fasciitis and Other Musculoskeletal Conditions
Policy statement unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with Category I CPT® code 28890 or Category III CPT® codes 0019T, 0101T, or 0102T .
Policy review and updateEffective 9/17/12
7 .01 .086Carotid Artery Angioplasty and Stenting
Policy statement unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with Category I CPT® codes 37215 or 37216 or Category III CPT® codes 0075T or 0076T .
Policy review and updateEffective 9/17/12
7 .01 .094Mechanical Embolus Retrieval for Acute Ischemic Stroke
Description updated . Policy statement unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with Category I CPT® unlisted code 37799 .
Policy review and updateEffective 9/17/12
7 .01 .096Dynamic Spinal Stabilization
Policy statement unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with Category I CPT® unlisted code 22899 .
Policy review and updateEffective 9/17/12
7 .01 .102Bronchial Thermoplasty for Control of Asthma
Policy statement unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with Category III CPT® codes 0276T or 0277T .
Policy review and updateEffective 9/17/12
7 .01 .117Minimally Invasive Lumbar Decompression
Minimally invasive lumbar decompression using the mild® Device Kit is experimental / investigational . Report service with Category III CPT® code .
New policyEffective 8/20/12
7 .01 .118Minimally Invasive Interventions for Fecal Incontinence
Sacral nerve stimulation is considered medically necessary for the treatment of fecal incontinence . Transanal radiofrequency therapy (Secca® procedure) is considered experimental / investigational . Report sacral nerve stimulation with Category I CPT® code 64561, 64581 or 64590 . Report transanal radiofrequency therapy (Secca® procedure) with Category III CPT® code 0288T . Refer to policy for details .
New policyEffective 8/20/12
7 .03 .001Human Organ Transplants
Policy statements unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with appropriate Category I CPT® code or HCPCS code .
Periodic review and updateEffective 8/20/12
7 .03 .002High Dose Chemotherapy with Autologous Stem Cell Support
Policy statements unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with appropriate Category I CPT® code .
Periodic review and updateEffective 8/20/12

[ TABLE OF CONTE NTS] BLUEL INK > > OCTOBE R 2012
6WHAT ’S HAPPENING
CLAIMS AND BILLING
HEALTH CARE POLICY
CPET CORNER
PROVIDER SEMINARS
QUALITY IMPROVEMENT
PHARMACY UPDATES
H E A LT H C A R E P O L I C Y
*MEDICAL POLICY AND/OR PROCEDURE
ACTIONS, COMMENTS AND REPORTING GUIDELINES
POLICY STATUS AND EFFECTIVE DATE
7 .03 .003High Dose Chemotherapy with Allogeneic Stem Cell Support
Policy revised . Considered to be experimental / investigational for multiple myeloma . Report service with appropriate Category I CPT® code or HCPCS code S2140 or S2142 .
Periodic review and updateEffective 12/17/12
7 .03 .006Nonmyeloablative Allogeneic Hemopoietic Stem Cell Transplantation for Hematologic Malignancies
Policy statements unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with Category I CPT® code 38240 or 38242 .
Periodic review and updateEffective 8/20/12
9 .01 .001AAnesthesia Services
Under Benefit Applications some references to “anesthesiologist” have been replaced by “qualified provider .” Refer to operating procedure for details .
Operating Procedure revision Effective 8/20/12
10 .01 .012ATelemedicine (Unified Communications)
Benefit Applications were clarified to read “Benefits are provided for telemedicine services in all CareFirst jurisdictions when meeting the definitions of Telemedicine in this Operating Procedure…” Report diagnostic, consultative and treatment Telemedicine services with the appropriate Category I CPT® code and the HCPCS modifier –GT . Refer to Operating Procedure for details .
Operating Procedure revisionEffective 9/17/12
11 .01 .039Genetic Testing for Cardiac Ion Channel Mutations
Policy statements unchanged . Under Policy Guidelines, added 2012 rationale statement . Report service with Category I CPT® molecular diagnostic stacking codes 83891, 83898, 83904, 83909 or 83912 and the modifier -8C .
Policy review and updateEffective 9/17/12

[ TABLE OF CONTE NTS] BLUEL INK > > OCTOBE R 2012
7WHAT ’S HAPPENING
CLAIMS AND BILLING
HEALTH CARE POLICY
CPET CORNER
PROVIDER SEMINARS
QUALITY IMPROVEMENT
PHARMACY UPDATES
P R O V I D E R S E M I N A R S
Professional SeminarsDATE AND TIME LOCATION ROOM
Wednesday, Oct . 17, 201210 a .m . to 1 p .m .Basics, Updates and More
Harbor Hospital3001 S . Hanover St . Baltimore, Md . 21225
Baum Auditorium
Wednesday, Oct . 24, 201210 a .m . to 1 p .m .Basics, Updates and More
Fair Oaks Hospital3700 Joseph Siewick Dr .Fairfax, Va . 22033
Conference Room B
Thursday, Nov . 8, 201210 a .m . to 1 p .m .Basics, Updates and More
Hilton Garden Inn4770 Owings Mills Blvd .Owing Mills, Md . 21117
Conference Room
Tuesday, Nov . 27, 20121 p .m . to 4 p .m . Basics, Updates and More
Shady Grove Adventist9901 Medical Center DriveRockville, Md . 20850
Sycamore Room
Hospital SeminarsDATE AND TIME LOCATION ROOM
Wednesday, Dec . 5, 201210 a .m . to 1 p .m .Hospital Quarterly
Johns Hopkins at Keswick, South Building3910 Keswick RoadBaltimore, Md . 21211
Second Floor Classroom
Wednesday, Dec . 12, 201210 a .m . to 1 p .m .Hospital Quarterly
Holy Cross Hospital1500 Forest Glen RoadSilver Spring, Md . 20910
Rooms A and C
Ancillary SeminarsDATE AND TIME LOCATION ROOM
Thursday, Oct . 25, 201210 a .m . to NoonHome Health
CareFirst Columbia Gateway6731 Columbia Gateway DriveColumbia, Md . 21046
Redwood
Tuesday, Nov . 13, 201210 a .m . to NoonHome Health
CareFirst Columbia Gateway6731 Columbia Gateway DriveColumbia, Md . 21046
Redwood
Practitioner and Staff Seminars and Training SessionsSee what the Center for Provider Education and Training has to offer. View upcoming sessions and find an opportunity that works for you and your staff.

[ TABLE OF CONTE NTS] BLUEL INK > > OCTOBE R 2012
8WHAT ’S HAPPENING
CLAIMS AND BILLING
HEALTH CARE POLICY
CPET CORNER
PROVIDER SEMINARS
QUALITY IMPROVEMENT
PHARMACY UPDATES
P R O V I D E R S E M I N A R S
WebinarsDATE TYPE TIME
11/6/2012 HealthyBlue 2 .0 & HealthyBlue Advantage 9 a .m .
11/6/2012 Corrected Claims 10:30 a .m .
11/6/2012 PCMH Portal Admin Training Noon
11/6/2012 New Guidelines for Independent Clinical Lab Claims 1 p .m .
11/6/2012 PT/OT/ST/Chiro 2:30 p .m .
11/6/2012 Programs & Products 4 p .m .
11/7/2012 New Guidelines for Specialty Pharmacy Claims 9 a .m .
11/7/2012 BlueChoice 11 a .m .
11/7/2012 Dialysis 12:30 p .m .
11/7/2012 CFD—Eligibility & Benefits 2 p .m .
11/7/2012 HealthyBlue Dual/Triple Option 3:30 p .m .
11/8/2012 New Guidelines for DME & Supplier Claims 9 a .m .
11/8/2012 CDH Noon
11/8/2012 Claims Submission & Requirements 2 p .m .
11/13/2012 PCMH Portal Admin Training 9 a .m .
11/13/2012 PCMH Member Health Record 10:30 a .m .
11/13/2012 MPOS 12:30 p .m .
11/13/2012 St . Mary’s Board Ed . Benefits 2 p .m .
11/13/2012 CFD – Claims Status & Inquiries 3 p .m .

[ TABLE OF CONTE NTS] BLUEL INK > > OCTOBE R 2012
9
Q U A L I T Y I M P R O V E M E N T
WHAT ’S HAPPENING
CLAIMS AND BILLING
HEALTH CARE POLICY
CPET CORNER
PROVIDER SEMINARS
QUALITY IMPROVEMENT
PHARMACY UPDATES
Quality Improvement (QI) Program:Raising the Bar for Improved Care and ServiceCareFirst Blue Cross and Blue Shield and CareFirst BlueChoice (collectively CareFirst) are committed to providing high quality care and service. The goal of the QI Program is to continuously improve the quality and safety of care (clinical and behavioral health) and services provided to Plan members, in all health care settings and at all levels. The Quality Improvement (QI) Council works with community physicians to develop and implement the QI program. As part of this effort, QI works to provide access to health care that meets The Institute of Medicine’s aims of being safe, timely, effective, efficient, equitable and patient-centered.
CareFirst annually implement a QI work plan that outlines specific clinical and service related improvement activities. Data is collected and analyzed for each clinical and service related improvement activity throughout the year, including the analysis for an increasingly diverse population. The QI Program is comprehensive and dynamic, and includes processes to identify, monitor, analyze, prioritize and implement interventions as necessary, to promote accessible, efficient, quality health care for every member.
The QI Program’s objectives are to:
n Support and promote all aspects of the CareFirst Patient-Centered Medical Home (PCMH) Program in order to improve quality of care, safety, access, efficiency, coordination and service.
n Establish partnerships with clinicians and organizations to put into action interventions that address the identified health and service needs of our membership and that are likely to improve desired health outcomes.
n Provide data that encourages clinicians to practice evidence-based medicine and make informed choices when making referrals.
n Maintain a systematic process to continuously identify, measure, assess, monitor and improve the quality, safety and efficiency of clinical care and quality of service.
n Assess the cultural, ethnic and language needs of our members and consider such diversity when analyzing data and implementing interventions to reduce health care disparities.
n Monitor and oversee the performance of delegated functions of certain vendors and large provider groups.
n Develop and maintain a high quality network of health care providers.
n Operate a QI Program that meets federal, state and local public health goals, and requirements of plan sponsors, regulators and accrediting bodies.
n Address health needs of the communities we serve.
n Support quality improvement principles throughout CareFirst, acting as a resource in process improvement.
As part of our QI effort, CareFirst participates in the annual Healthcare Effectiveness Data and Information Set (HEDIS®) project. HEDIS is a tool used by more than 90 percent of America’s health plans to measure performance on important dimensions of care and service. CareFirst’s HEDIS 2012 (measurement year 2011) results revealed the following strengths and opportunities:
continued on next page

[ TABLE OF CONTE NTS] BLUEL INK > > OCTOBE R 2012
10WHAT ’S HAPPENING
CLAIMS AND BILLING
HEALTH CARE POLICY
CPET CORNER
PROVIDER SEMINARS
QUALITY IMPROVEMENT
PHARMACY UPDATES
Q U A L I T Y I M P R O V E M E N T
Strengths
The following measure results were in the 90th percentile nationally:
n Flu shots for adults 50-64 (BluePreferred)
n Appropriate testing for children with pharyngitis (BluePreferred)
n Use of Spirometry testing in the assessment and diagnosis of COPD (BlueChoice)
n Use of appropriate medications for people with asthma (BluePreferred)
n Persistence of Beta-blocker treatment after a heart attack (BlueChoice)
n Antidepressant medication management – acute phase
n Antidepressant medication management – continuation phase
n Follow-up care for children prescribed ADHD medication – continuation and maintenance
n Timeliness of prenatal care
Opportunities for Improvement
A number of opportunities for improvement were identified, and the following have been determined to be those with the most impact on improving care for our members:
View a more detailed
description of our QI
Program and status
toward meeting our
goals here. You can also
call Clinical Innovations/
Quality Improvement at
410-605-2677 to request
a paper copy.
MEASUREGOAL
(NATIONAL 90TH PERCENTILE)
CAHPS 2011BLUECHOICE
RESULTS
CAHPS 2011BLUEPREFERRED
RESULTS
Breast Cancer Screening 77% 65 .14% 68 .14%
Cervical Cancer Screening 81% 77 .23% 68 .74%
Chlamydia Screening in Women (Total) 53% 35 .31% 38 .39%
Comprehensive Diabetes Care: Eye Exam 71% 48 .34% 52 .89%
Comprehensive Diabetes Care: HbA1c Testing 93% 86 .34% 86 .34%
Comprehensive Diabetes Care: LDL-C Screening 90% 84 .06% 84 .24%
Controlling High Blood Pressure 72% 54 .50% 51 .06%
Cholesterol Management for Patients with Cardiovascular Conditions: LDL-C Screening
93% 84 .22% 87 .21%
Postpartum Care 90% 87 .04% 82 .87%
Immunizations for Adolescents – Combination #1 71% 54 .21% 53 .85%
Adult BMI Assessment 73% 44 .47% 30 .02%
Outreach to our members is best provided through primary care physician offices, as numerous studies have indicated that members respond most readily to reminders from practitioners. PCMH staff is involved in the analysis of our HEDIS results, working with the Quality Improvement Council and the Quality Improvement Management Team. PCMH consultants and Care Coordinators will be the messengers of our quality priorities to the practices. We will work to identify and communicate organization-wide priorities and opportunities to our practitioners.

[ TABLE OF CONTE NTS] BLUEL INK > > OCTOBE R 2012
11WHAT ’S HAPPENING
CLAIMS AND BILLING
HEALTH CARE POLICY
CPET CORNER
PROVIDER SEMINARS
QUALITY IMPROVEMENT
PHARMACY UPDATES
Q U A L I T Y I M P R O V E M E N T
Clinical Practice and Preventive Services Guidelines Available OnlineThe CareFirst Quality Improvement Council annually reviews and adopts the latest clinical recommendations from nationally recognized sources. The following updated clinical practice and preventive services guidelines can be obtained here.
n 2012 Preventive Services Guidelines
n The Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma: 2007
n Global Strategy for the Diagnosis, Management and Prevention of COPD: 2011 Global Initiative for Chronic Obstructive Lung Disease (GOLD) Guidelines
n ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults: 2009 Focused Update
n ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult: 2005
n ACCF/AHA Performance Measures for Primary Prevention of Cardiovascular Disease in Adults: 2009
n AHA/ACCF Secondary Prevention and Risk Reduction Therapy for Patients With Coronary and Other Atherosclerotic Vascular Disease: 2011 Update
n AHA/ACC Guidelines for Secondary Prevention for Patients with Coronary and Other Atherosclerotic Vascular Disease: 2006 Update
n American Diabetes Association, Standards of Medical Care in Diabetes: 2011
n Clinical Practice Guidelines for Depression in Adults in the Primary Care Setting
n The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. August 2004
n Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society. October2007
n American College of Rheumatology 2012 Recommendations for the Use of Nonpharmacologic and Pharmacologic Therapies in Osteoarthritis of the Hand, Hip, and Knee April 2012
n Screening for Obesity in Children and Adolescents: US Preventive Services Task Force Recommendation Statement. January 2010
View a more detailed description of our
QI Program and status toward meeting
our goals here. You can also call Clinical
Innovations/Quality Improvement at
410-605-2677 to request a paper copy.

BLUELINK > > OCTOBE R 2012
CHIEF MEDICAL OFFICER AND SR . VICE PRESIDENT OF MEDICAL AFFAIRSJon P. Shematek M.D.
EDITORRobert Hilson
12
CareFirst BlueCross BlueShield is the shared business name of CareFirst of Maryland, Inc. and Group Hospitalization and Medical Services, Inc. CareFirst BlueCross BlueShield and CareFirst BlueChoice, Inc. are both independent licensees of the Blue Cross and Blue Shield Association.
WHAT ’S HAPPENING
CLAIMS AND BILLING
HEALTH CARE POLICY
CPET CORNER
PROVIDER SEMINARS
QUALITY IMPROVEMENT
PHARMACY UPDATES
Prior AuthorizationNew Generics
The following drugs will be available as generic. The generics will be covered on tier 1 and the brand-name drugs will be on tier 3 or non-preferred.
BRAND NAME GENERIC NAME
Actos® pioglitazone
Actoplus met® pioglitazone/metformin
Dovonex® cream calcipotriene
Singulair® montelukast
Xopenex® inhalation solution levalbuterol
Removed from Preferred Drug List
The following drugs have been moved to tier 3 or non-preferred drugs.
BRAND NAME GENERIC NAME
Actoplus met XR® pioglitazone/metformin
Duetact® pioglitazone/glimepiride
P H A R M A C Y U P D A T E S
How Are We Doing?How does BlueLink help you do your job? Let us know how BlueLink has made an impact on the way that you do business with CareFirst. Tell us what you think—what we’re doing right and what we could do better. Your feedback helps us deliver timely, engaging news that will help you have more time to care for our members.
Our goal is to provide you with the best articles possible and our feedback is vital. Email your comments to [email protected] and you will be entered to win a free gift.
For the most current drug list, prior authorization forms and pharmaceutical management procedures, visit www.carefirst.com/providers and click on Prescription Drugs. For a paper copy of the formulary and pharmaceutical management procedures, call 877-800-3086.