new ase guidelines: what you must know · new ase guidelines: what you must know federico m asch...
TRANSCRIPT

New ASE Guidelines:What you must know
Federico M Asch MD, FASE, FACCChair, ASE Guidelines and Standards Committee
Medstar Washington Hospital CenterMedstar Health Research Institute
Georgetown UniversityWashington, DC
Costa Rica, August 2015

DISCLOSURE
I, Federico Asch, have no relevant financialrelationships with pharmaceutical, devicescompanies or the Educational Committee relatedto this activity.

ASE Guidelines 2014• Expert Consensus for Multimodality Imaging Evaluation of
Adult Patients during and after Cancer Therapy: A Report from the ASE and EACVI, JASE, September 2014
• Guidelines for the Cardiac Sonographer in the Performance of Contrast Echocardiography: A Focused Update from the ASE, JASE, August 2014
• Radiation Safety for the Cardiac Sonographer: Recommendations of the Radiation Safety Writing Group for the Council on Cardiovascular Sonography of the ASE, JASE, August 2014
• Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot: A Report from the ASE, JASE, February 2014

ASE Guidelines 2015
• Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the ASE and the EACVI, JASE, January 2015
• Guidelines for the Use of Echocardiography as a Monitor for Therapeutic Intervention in Adults: A Report from the ASE, JASE, January 2015
• Multimodality Imaging of Diseases of the Thoracic Aorta in Adults: From the ASE and the EACVI. JASE, February 2015
• Use of Echo in Adult Hypertension: From EACVI and ASE. JASE July 2015
• Guidelines for the Evaluation of ASD and PFO: ASE and SCA. JASE August 2015
• Guidelines for the use echo in the management of patients with Left Ventricular Assist Device. JASE, August 2015


• Update from the 2005 ASE Chamber Quantification document (Lang et al)
• Most referenced article in JASE history (>5500)
• Need for update given
– newer technologies
– newer techniques
– wealth of normative data available
What is new in theUpdated CQ document
• Chamber dimension and function encompass many parameters, including strain and 3D echo.
• Describes all four chambers, and it is done in a way to avoid discrepancies with other guidelines. (2005 was only LV and LA)
• The writing group created the data from five databases representing > 3,000 patients. (2005 was expert opinion)
• The new document only indicates normal/abnormal. It will be left to the individual institutions to determine what they consider mild/moderate/severe.

Multiple modalities described
M-mode
2D linear
2D Volumes
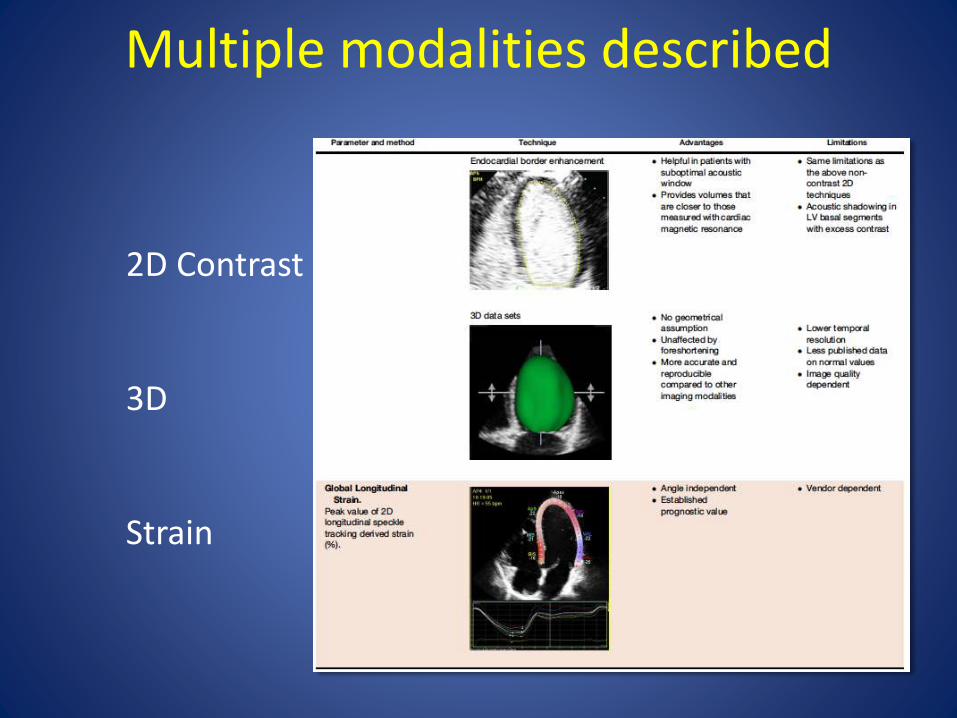
2D Contrast
3D
Strain
Multiple modalities described

LV Normal ranges
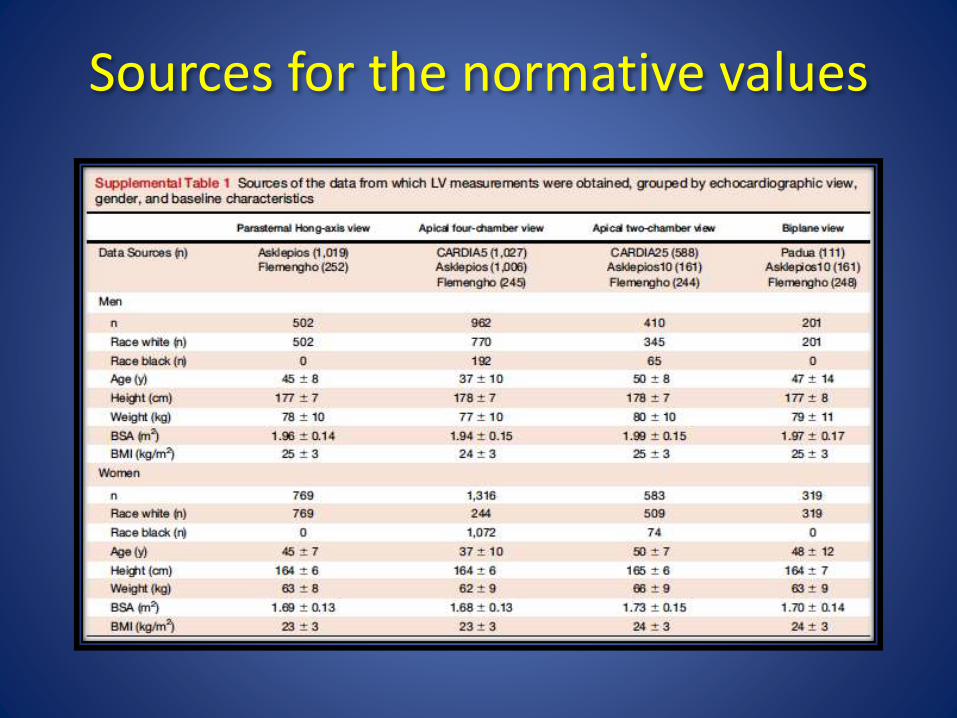
Sources for the normative values
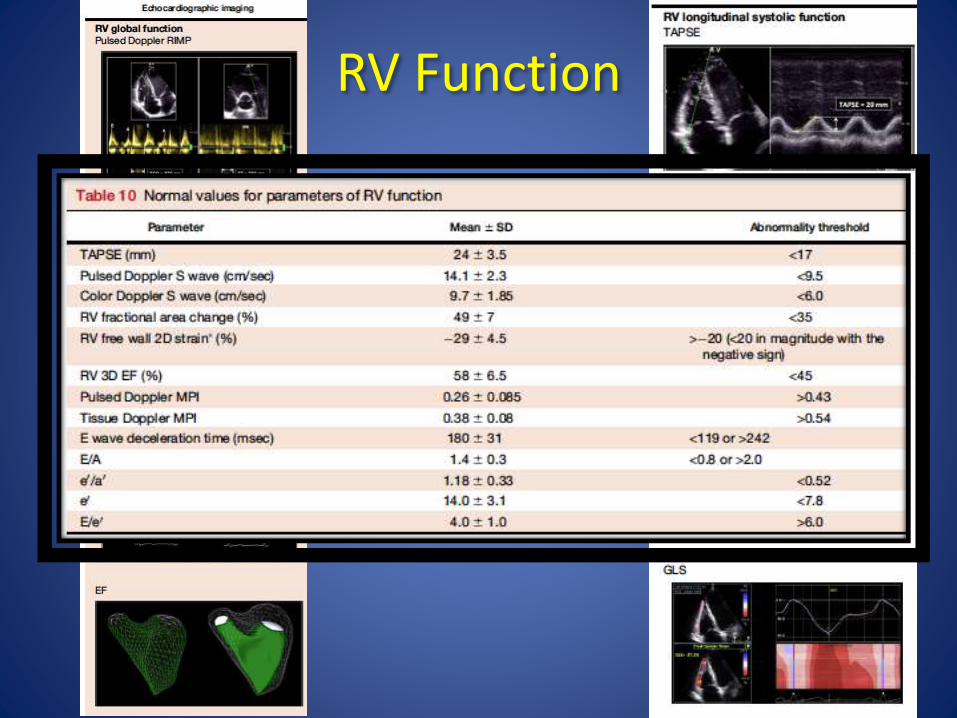
RV Function

• The document by R Lang et al has been published in the Jan 2015 issue of JASE.
J Am Soc Echocardiogr 2015;28:119-82
GUIDELINES AND STANDARDS
asecho.org Guidelineswww.

Imaging Techniques
• Chest X-ray
• Echo (TTE, TEE, 3D-echo, epiaortic)
• Intravascular echo (IVUS)
• Intracardiac echo (ICE)
• CT/MDCT
• Magnetic resonance imaging
• Aortography

Diseases of the Thoracic Aorta
• Acute aortic syndromes
• Thoracic aortic aneurysms
continued . . .
- Aortic dissection
- Intramural hematoma
- Penetrating aortic ulcer
- Ruptured aortic aneurysm
- Bicuspid aortic valve-related aortopathy
- Marfan syndrome
- Other genetic diseases(Ehlers-Danlos; Loeys-Dietz, Turner syndrome,etc)
Diseases of the Thoracic Aorta
• Traumatic injury of thoracic aorta
• Aortic coarctation
• Atherosclerosis
• Aortitis
- Noninfectious
- Infectious

Measuring
the Aorta


Measure perpendicular to the long-axis of the aorta

Measurement Options
• Inner edge-inner edge - CT
• Outer-outer
• Leading edge-leading edge- Echo
Recommended time to measure
the aortic root
A. End-systole
B. End-diastole
- Greater reproducibility
(Ao pressure more stable in late diastole)
- End-diastole easy to ID by QRS

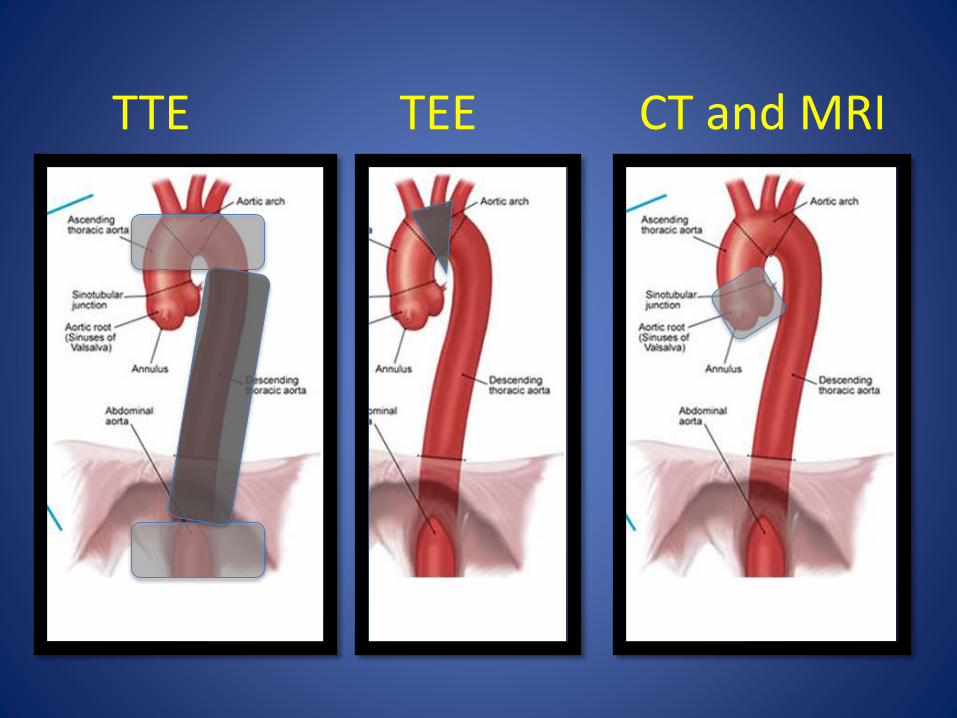
TTE TEE CT and MRI

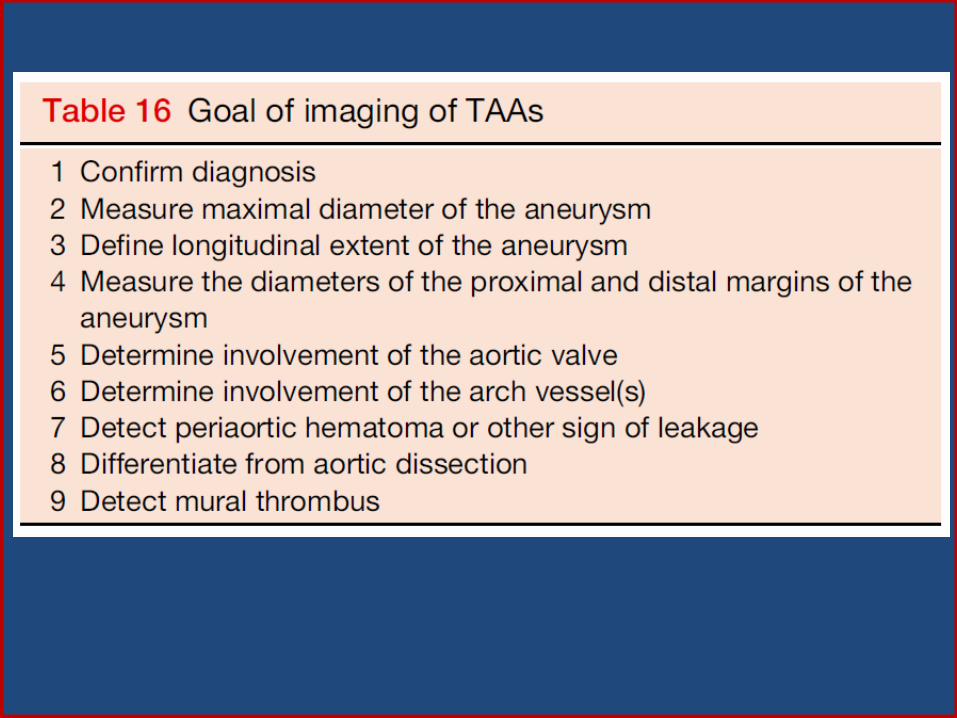
Thoracic Aortic
Aneurysms

What to look for?
• Normal Aortic size in the adult:
– Ao root < 40 mm
– Ascending Ao < 37 mm
– Descending Aorta < 28 mm
• These values are, however, very variable.

Aortic size to be adjusted by body size and age
< 20 yo 20-40 yo >40 yo
Roman M et al. Am J Cardiol 1989;64:507

Complications and Asc Ao sizeImportance of accurate measurements
Elefteriades, JACC 2010;55:841

Asc Aortic size at time of Type A Dissection
Pape et al for IRAD. Circulation 2007;116:1120
60% < 5.5
cm
40% <5 cm


You want to explore the ENTIRE Aorta, AT LEAST ONCE

Marfan - Ao Root aneurysm

Oct 2012
Marfan with prior graft in Asc Aorta
Need to look at
entire Aorta !!
Dec 2012
Dissections post graft !
Mostly in arch/Desc !
Asch FM, Weinsaft J et al. Manuscript Under Review

MarfanMVP
RPA aneurysm
Marfan Syndrome - Role of imagingMonitoring aortic enlargement
• Monitoring every 6/12 months
– (same method, side by side)
• Surgical Indication:
– Aortic diameter > 5cm
– Rapid progression (2-4 mm/year)
– Aortic dissection
– Family Hx of early dissection

BAV Aortopathy
RL fusion type – Most Common
• 33-60 % Normals
• Aortic root: 1-25 %
• Asc Aorta: 32-35%
• Arch: 10 %
Kang JW et al. J Am Coll Cardiol Img 2013; 6:150
Schaefer BM et al. Heart 2008;94:1634.

RN fusion type (or RL distribution)
RN fusion type
• 19-32 % Normals
• Aortic root: 1-15 %
• Asc Aorta: 26-54 %
• Arch: 41 %
Kang JW et al. J Am Coll Cardiol Img 2013; 6:150
Schaefer BM et al. Heart 2008;94:1634.

BAV Asc Ao/Arch aneurysm

Acute Aortic
Syndromes

Acute Aortic Syndromes
• Aortic dissection
• Intramural hematoma
• Penetrating aortic ulcer
• Ruptured aortic aneurysm

Aortic Dissection - Imaging
Primary Objectives
• Identify entry site
• Determine type A vs B
• Involvement of coronary arteries ?
• Identify complications:
• Presence, severity, mechanism of AR
• Pericardial or pleural effusion
• Rupture ?
• Branch ischemia

Suspected Aortic Dissection
Sensitivity of Imaging Modalities
Meta-Analysis of 1,139 Patients
Fig 23. Goldstein J Am Soc Echocardiogr 2015;28(2):119-82

Suspected Aortic Dissection
Specificity of Imaging Modalities
Meta-Analysis of 1,139 Patients
Fig 24. Goldstein J Am Soc Echocardiogr 2015;28(2):119-82


Aortic Dissection
2D-Echo Findings
• .
• Dilated aorta
• Widening of aortic walls
• Aortic insufficiency
• Pericardial and/or pleural effusion
Hallmark: dissection flap

TEE CT-scan
Descending Thoracic Aorta
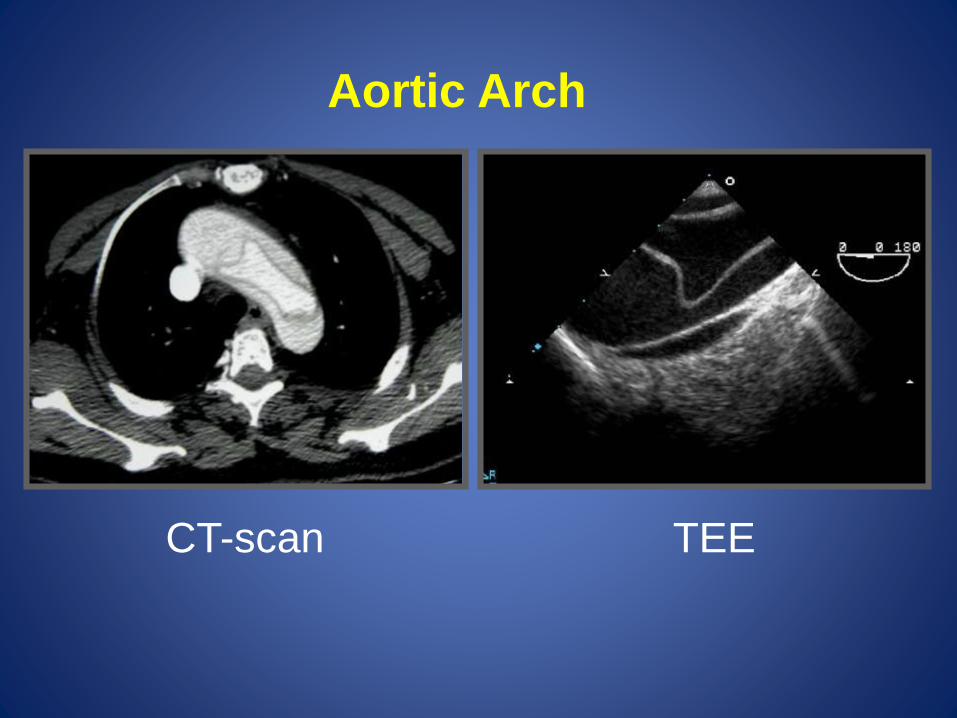
CT-scan TEE
Aortic Arch

Hemopericardium

Flow in right coronary artery

Left coronary artery

Left Subclavian Artery

Mechanisms of Aortic Regurgitation
B
C



“Atypical" Aortic Dissection
TL
FL
Typical
"Atypical"
= Dissection flap and false lumen
= No dissection flap; Medial hematoma
(Intramural Hematoma)

"Atypical" Aortic Dissection
(Intramural Hematoma)
• Prevalence 10-20% in CT/MRI/TEE studies
• Type III more common
• Normal size lumen
• False negative aortograms



Penetrating Aortic Ulcer
An ulceration of an atheromatous plaque
that disrupts the internal elastic lamina
and burrows deeply into the media
adventitia
media
intima

Ulcerated Aortic Plaque

Summary
• ASE takes Guidelines and Standards as a key component of its mission
• Newer roles of echocardiography trigger new guidelines:– LV Assist devices– Interventional Echocardiography– ASD/PFO
• Older problems still need to be addressed; Updates are needed– Valvular regurgitation and Stenosis– Stress testing beyond CAD– CSOE
• STAY TUNED FOR FURTHER GUIDELINES TO COME

Visite el sitio de ASE para America latina:
asecho.org/americas
Guias y Webinars en espanol