new approaches to disease management get connected knowledge forum larry g. anderson md mmc...
TRANSCRIPT

New Approaches to Disease Management
Get Connected Knowledge ForumLarry G. Anderson MD
MMC Physician-Hospital OrganizationJune, 2005
Maine Medical CenterPhysicians-Hospital Organization
• Recent transition from contracting to quality improvement focus
• 200 PCPs, 770 specialists, 4 hospitals in southern and central Maine
• Largely independent practices
• Low EHR penetration
Chronic Illnesses Are Costly
• Costly to employers productivity and absenteeism (8.3 days
compared to 1.7 days/year)
• Costly to society 44% with chronic illness drive 78% of
healthcare $
• Costly to patients and their families
Cost Burden of Diabetes
• 18.5 % of healthcare $ care of diabetes ($132 billion annually)
• Annual cost of healthcare: $13,243 for patient with diabetes $2,560 for patient without diabetes
• MMC: diabetes-related care $100 million annually!
The Burden of Diabetes Complications for Patients
• Retinopathy: leading cause of new blindness
• Amputations: half from diabetes
• Nephropathy: 40% of kidney failure requiring dialysis, from diabetes
• Death from heart attacks and stroke quadrupled
There Is Hope:“Best Practice” Care for Diabetes
Following evidence-based guidelines (“best practice”) lowers the risk of complications: heart attack and stroke by 53% retinopathy (eye) by 58% nephropathy (kidney) by 61%
New England Journal of Medicine, January, 2003
But Is “Best Practice”Care Delivered?
Only about half the time. Care delivered by evidence-based guidelines: Diabetes: only 46% of the time Chronic illness: 56% Preventative care: 55% Acute care: 54%
RAND
New England Journal of Medicine, June, 2003
Institute of Medicine (IOM):Crossing the Quality Chasm
• As medical science and technology have advanced at a rapid pace, the health care delivery system has floundered. Between the care we have and the care we could have lies not just a gap, but a chasm
• The “quality gap.”
IOM Conclusion
• The problem: bad systems, not bad doctors
• We have a healthcare delivery problem, solved by redesigning systems of care delivery
Medical Errors andQuality Improvement
IOM QUALITY GAP
Overuse
Misuse
Under use (the most common gap in
chronic illness care)
BEST PRACTICE
Do less
Do it right
Do more (by office system redesign)
PHO Clinical Improvement Plan(CLIP) Goals
• Promote best practice care
• Prevent or delay illness complications
• Develop reward system for best practice care
New Systems in CLIP
• The MaineHealth Chronic Illness Registry: a new system to make best practice easier for physicians and their office staffs
• The PHO Chronic Illness Care Management Program: a new system to engage the patients to take responsibility for caring for their diseases
The MaineHealthChronic Illness Registry (CIR)
• What the CIR is:– A secure web-based tool for physicians to
consolidate and track data (key clinical information) for patients with specific chronic illnesses
– Homegrown– Applicable to all patients, regardless of payer
source
The MaineHealthChronic Illness Registry
• What the CIR is:– Available at no cost to PHO physicians– Technically supported by the MMC
• What the CIR is NOT:– An electronic medical record (EMR)– Expensive like an EMR
What the Registry Provides
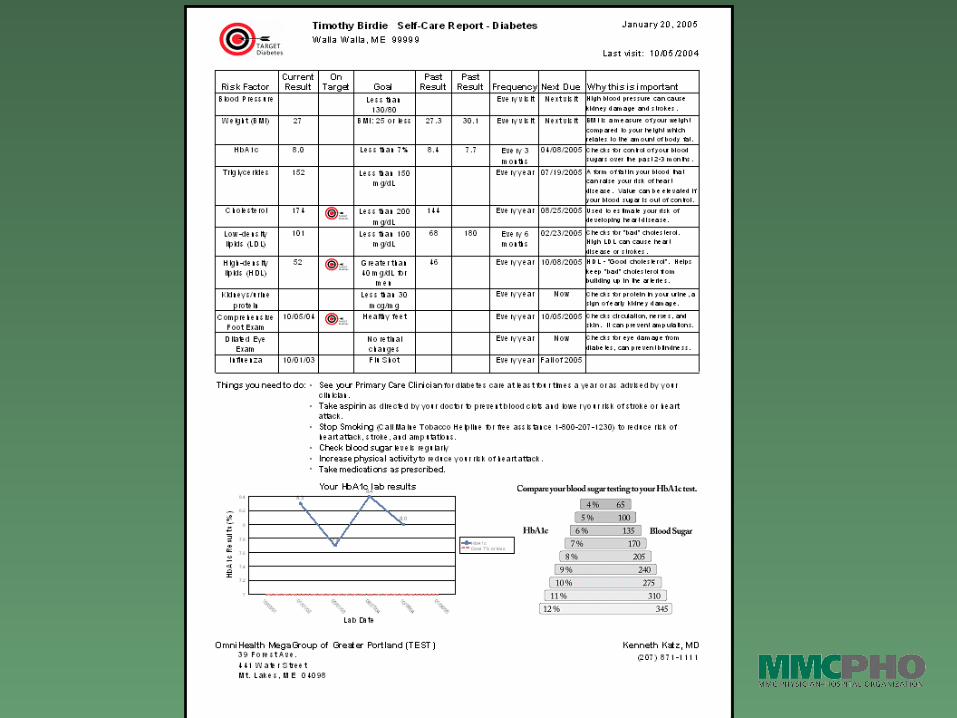
• Reminders based on best practice– A summary of updated patient information for
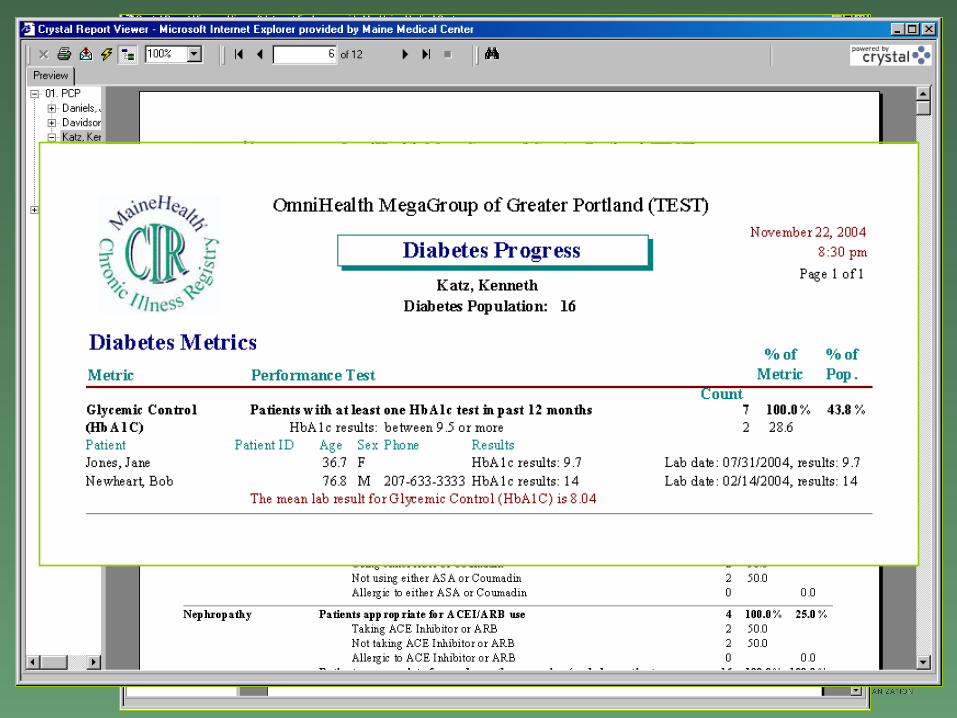
today’s visit - quality gaps for that patient– Population management reports: identify
opportunities to improve care for all the patients with a chronic illness - quality gaps for the practice
Population Based Care
Old Way
Reactive care, visits triggered by problems, focus on acute care
Missed appointments, lab Other health concerns distract doctor
from details of caring for diabetes Thick paper chart: when and what was
last LDL?
New Way
Systematic care, with proactive outreach for appointment and lab, focus on prevention
Important clinical data organized at time of visit
Prompts of need to treat blood pressure, blood sugar, LDL “to target”
Motivating the patient: self-management
New System to Engage Patients:Chronic Illness Care Management
Program
• An intensive, personalized approach to motivating and supporting the patient to embrace self-management skills
• RN Care Managers– Practice-based, at no cost to practice– All chronic illnesses, all patients
Pay for Performance (P4P)
New provider reimbursement model that promotes and rewards behavior changes and best practice system changes that produce better, more cost-effective outcomes
MMC PHO Internal P4P:Quality Care Rewards Program
• Cash awards for both physicians and staff teams for achieving good and superior levels of care delivery for childhood asthma and adult diabetes
• $270,000 distributed to primary care physicians and their practice teams for their work in achieving 2004 goals
• Rewards ranged up to $7240 for individual physician
2004 Quality Care Goals
• “Good Performance” measure examples– At least 80% of patients seen in 2004– 80% of patients with asthma classified– 80% of patients with persistent asthma on
controller med– 80% of patients with diabetes tested for
HbA1c and LDL
2004 Quality Care Goals
• “Superior Performance” measure examples– 90% visits, classification, lab testing– 90% flu shots in asthma– 90% aspirin in diabetes
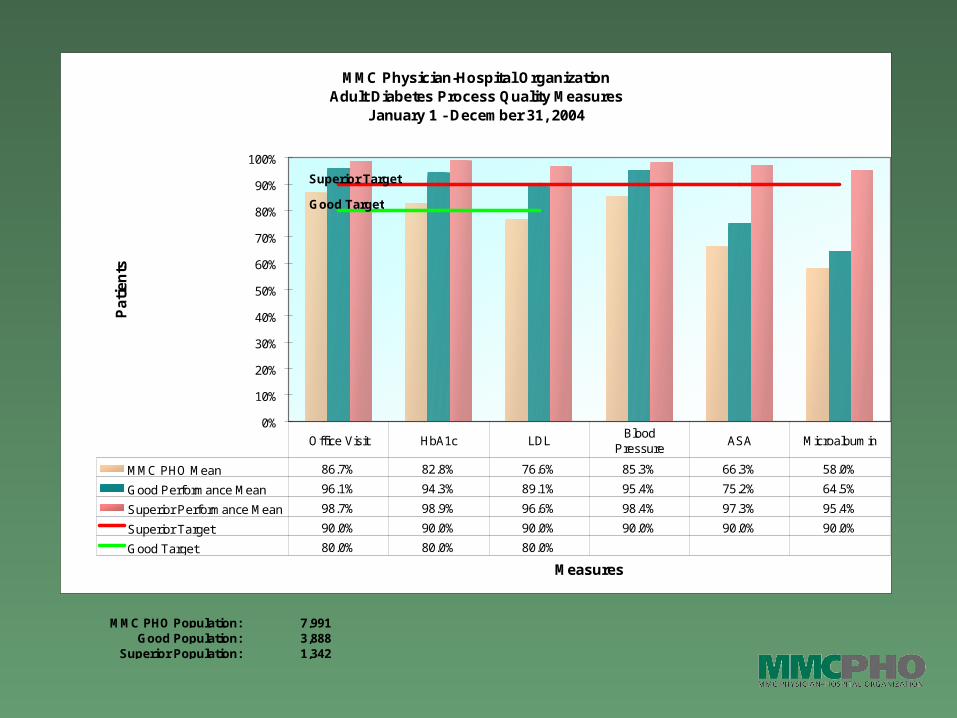
MMC PHO Population: 7,991 Good Population: 3,888
Superior Population: 1,342
MMC Physician-Hospital OrganizationAdult Diabetes Process Quality Measures
January 1 - December 31, 2004
Superior Target
Good Target
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Measures
Pa
tie
nts
MMC PHO Mean 86.7% 82.8% 76.6% 85.3% 66.3% 58.0%
Good Performance Mean 96.1% 94.3% 89.1% 95.4% 75.2% 64.5%
Superior Performance Mean 98.7% 98.9% 96.6% 98.4% 97.3% 95.4%
Superior Target 90.0% 90.0% 90.0% 90.0% 90.0% 90.0%
Good Target 80.0% 80.0% 80.0%
Office Visit HbA1c LDLBlood
PressureASA Microalbumin
What is Next?
• More chronic illnesses
• Focus on preventive health
• Specialist engagement
• New technology to improve patient safety (electronic prescribing)
Idealized IT-supported Illness Management
• Standardized evidence-based data sets
• Decision support with knowledge links and prompts
• Customizable documentation
• Workflow efficiency with one system, integrated with office management system and central data repository that push data and pre-populate data fields
MMC PHO AddressesChronic Illness Management
• New systems (CIR and care managers) to focus on areas of opportunity to strive for best practice care
• Well designed, significant financial incentives to accelerate the necessary system changes

If Innovative Approaches to Illness Management are Successful….
• Potential for tremendous payoffs– improved quality of life for our patients– cost savings from averted complications
• Win-win-win for patients-providers-community