neurological toxicity of tri-azole antifungals
DESCRIPTION
Neurological toxicity of Tri-azole Antifungals. DR CAROLINE BAXTER Clinical Research Fellow. www.aspergillus.org.uk. Tri-azole Antifungals. Voriconazole. Posaconazole. Itraconazole. Type 1 and 3 hypersensitivity. ABPA. ‘ASPERGILLUS BRONCHITIS’. SAFS. ASPERGILLOMA. CPA. - PowerPoint PPT PresentationTRANSCRIPT
Neurological toxicity ofTri-azole Antifungals
DR CAROLINE BAXTERClinical Research Fellow
www.aspergillus.org.uk
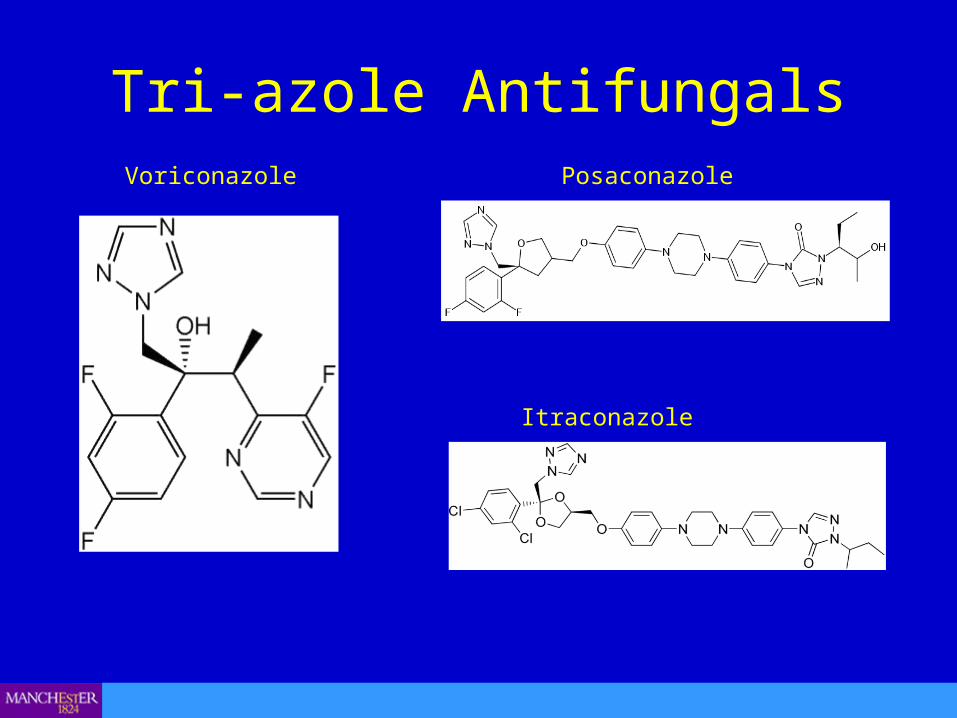
Tri-azole AntifungalsVoriconazole Posaconazole
Itraconazole
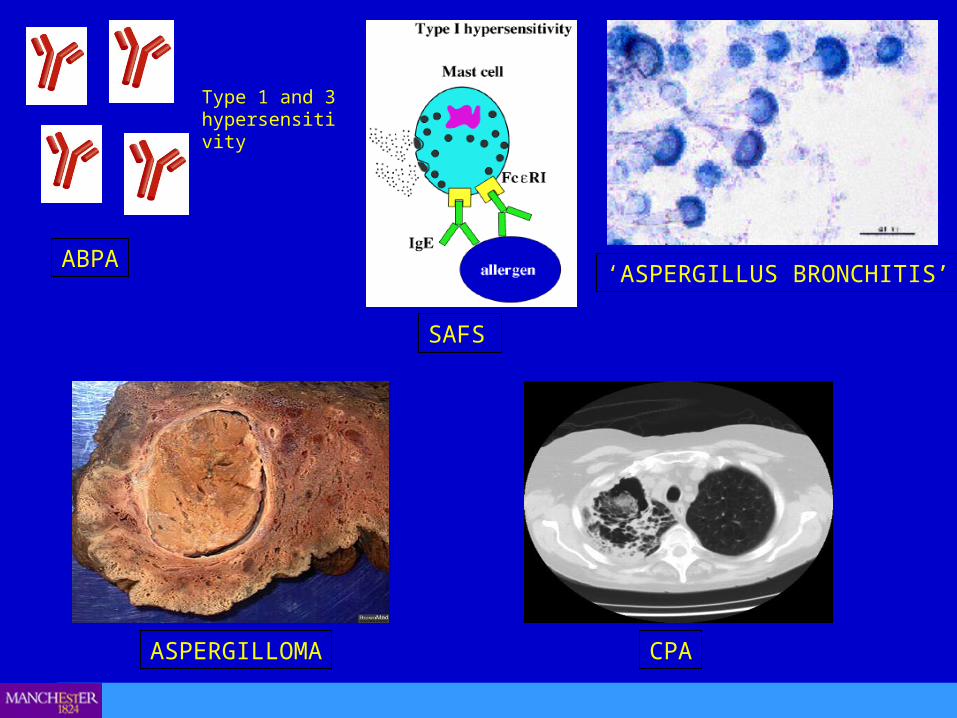
‘ASPERGILLUS BRONCHITIS’
SAFS
ABPA
Type 1 and 3 hypersensitivity
ASPERGILLOMA CPA
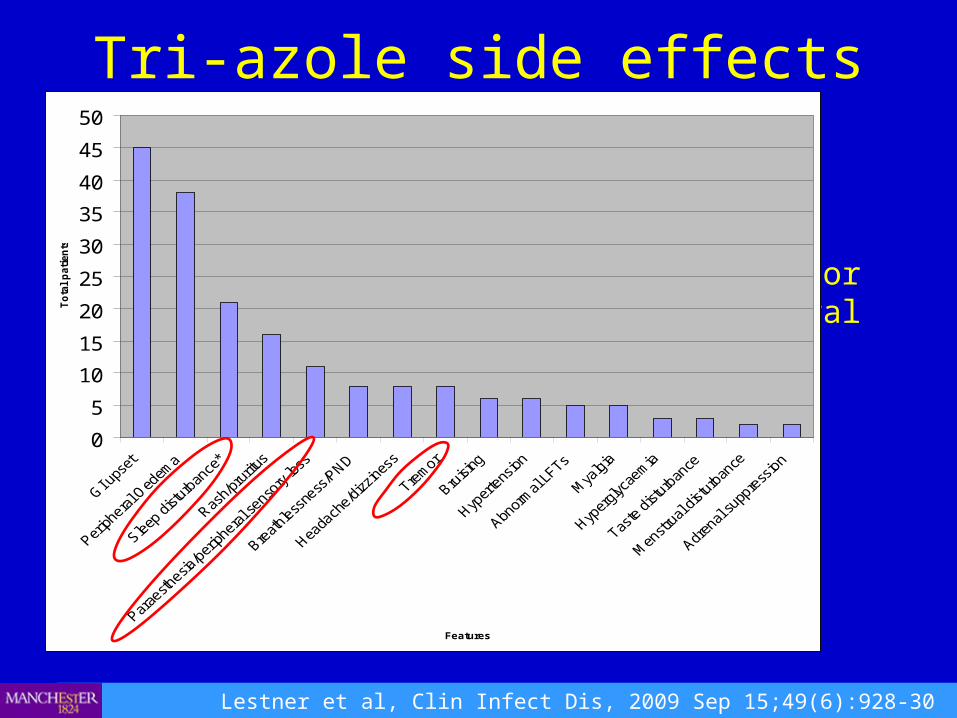
Tri-azole side effects
Lestner et al, Clin Infect Dis, 2009 Sep 15;49(6):928-30
• 216 patients taking itraconazole• 46% experienced adverse side effect• Neurological: 21% sleep disturbance/poor memory and
concentration, 11% peripheral neuropathy, 4% tremor.• Seizures described but rare.
0
5
10
15
20
25
30
35
40
45
50
Features
To
tal
pati
en
ts
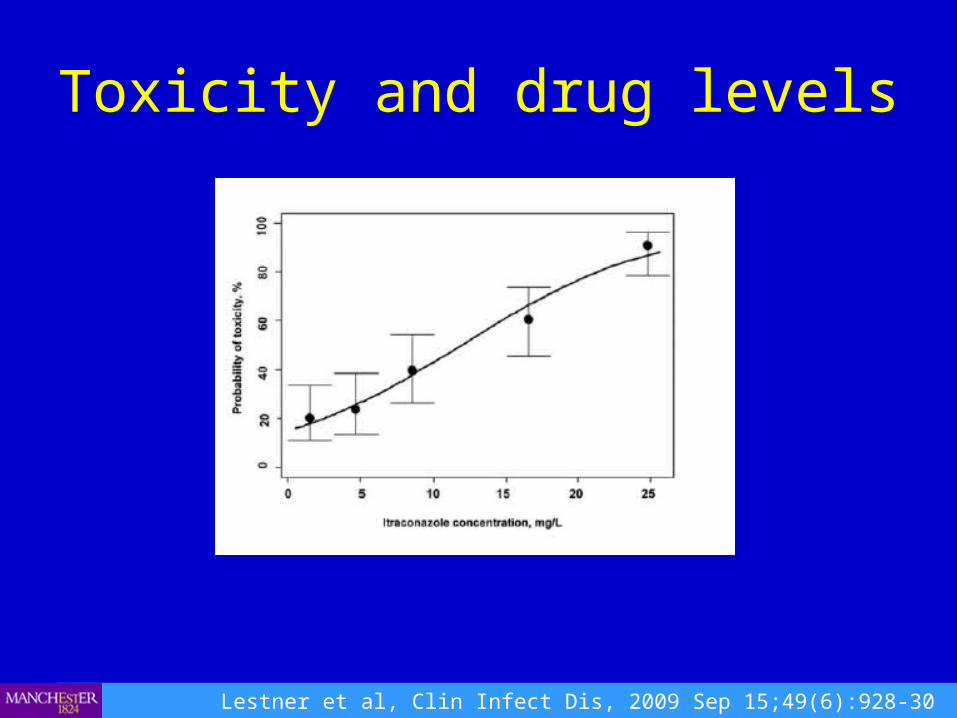
Toxicity and drug levels
Lestner et al, Clin Infect Dis, 2009 Sep 15;49(6):928-30
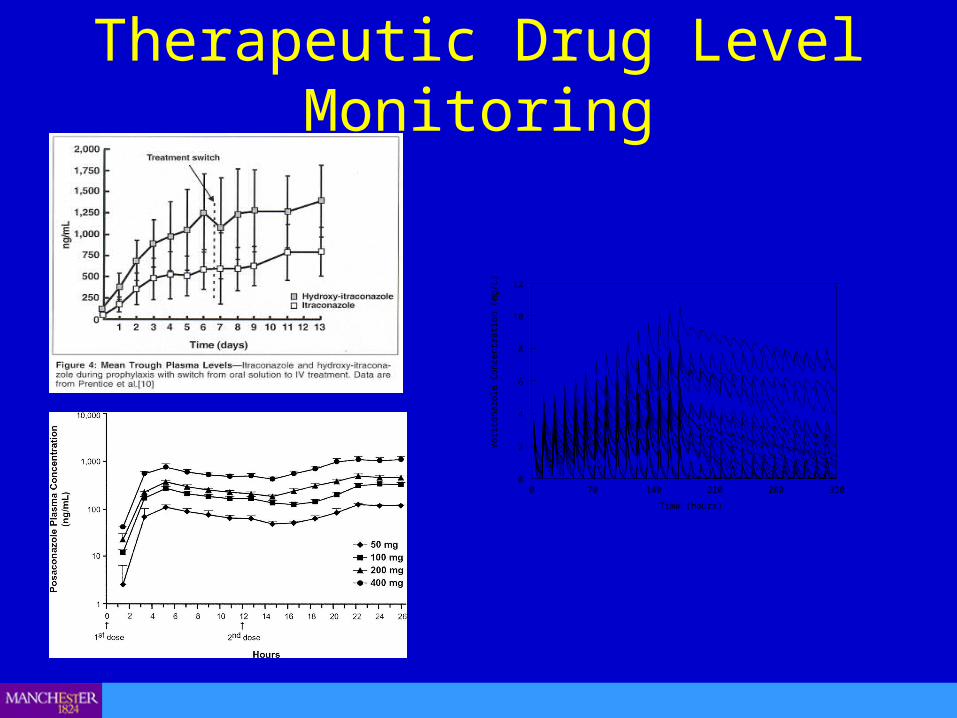
Therapeutic Drug Level Monitoring
0 70 140 210 280 350
Time (hours)
0
2
4
6
8
10
12
Vor
icon
azol
e C
once
ntra
tion
(mg/
L)

Tremor• 216 patients on itraconazole• 5 cases reported – confirmed by
accelerometry• Onset 3wk-12 months• 3 of 5 cases itraconazole
level>15mg/l• Dose reduction did not alter
symptoms• 1 case resolved off treatment and
recurred with recommencement of the drug
• Also described with voriconazole and posaconazole.
• Unlikely class effect
Lestner et al, J Neurol Neurosurg Psychiatry. 2010 Mar;81(3):327-9
Peripheral Neuropathy• Retrospective study• Patients with aspergillosis commenced on tri-azoles between
2007-2010.• 222 patients were commenced on tri-azole antifungals: 107
itraconazole, 75 voriconazole and 40 posaconazole.• 24 patients described symptoms of PN, 1 excluded as
diagnosed median nerve palsy.• 3 patients described symptoms with both itraconazole and
voriconazole.• Total of 26 ‘clinical episodes’ of PN.
Baxter et al. J Antimicrob Chemother. 2011 Sep;66(9):2136-9
Peripheral Neuropathy• 22 presented as a sensory disturbance of the
hands and/or feet developing over a median of 3 months.
• 4 presented with acute predominant lower limb weakness and difficulty walking over 1 to 4 weeks.
• 12 male, 11 female. Mean age 59.• 26 episodes: 18 itraconazole, 7 voriconazole, 1
posaconazole
Drug Levels
• 11 of the 26 had persistently elevated drug levels (despite dose reductions) in the 3 months prior to onset of symptoms.
• 10 of the 11 were high itraconazole levels and 1 elevated posaconazole level. All 7 patients experiencing symtoms with voriconazole had therapeutic drug levels.
NCS• 15 of the 26 episodes had formal nerve conduction
studies performed.• 12 of the 15 had confirmed PN:
- 6 sensory predominant axonal neuropathy- 2 small fibre sensory neuropathy- 3 motor predominant axonal neuropathy- 1 mixed axonal/demyelinating neuropathy
• Of the 3 negative studies – no baseline, no small fibre studies, all spent >1 month off therapy prior to NCS
Outcome
• 2 patients had persistent symptoms despite cessation of medication.
• 2 resolved with dose reduction• All others resolved with stopping medication• 3 patients had symptoms with both
itraconazole and voriconazole• 3 patients successfully changed to an
alternative triazole

Discussion
• Remarkably high rate of PN: itra 17%, vori 9%.• No direct relationship to drug levels but some on itraconazole
with high levels do respond to a reduction in dose.• First ever described case of posaconazole PN.• Most sensory predominant axonal neuropathy but must note
4 cases of rapid debilitating motor axonal neuropathy.• Must screen for other causes of PN.• Pathogenesis unknown – metronidazole (imidazole),
mitochondrial disorders, accumulation in phospholipids in neurons.
Discussion
• Risk, although low, of non recovery• Early detection vital• Neuropathy scales (chemotherapy, diabetes)• Baseline NCS and small nerve studies
Clinical Case
• HR• Female• 20 years old • Cystic fibrosis ∆F508/∆F508• Transferred to adult services (MACFU) in
March 2007
Clinical Case
CF past history:
• Hearing loss due to iv aminoglycosides.• Chronic transmissible strain Pseudomonas
auerginosa. Intermittent Staphylococcus aureus.
• 1998 RLL lobectomy - aspergilloma (histology). Post surgery treatment with itraconazole 200mg bd.

Clinical Case• Clinically stable since surgery.
Itraconazole 200mg bd continued.
DRUG LEVEL MONITORING
• 01.11.02 Random 0.5mg/L• 03.02.03 Random <0.4 no drug detected• 25.03.03 Post-dose 2.1• 03.07.03 Random 1.8• 27.08.03 Post-dose 1.6• 17.11.03 Post-dose 2.9• 16.01.04 Random 2.3• 14.06.04 Random 2.8
Clinical Case
• Compliance• Brand• Time taken/food• Other medication• CF – GI absorption
Clinical Case
• 2004 - Developed bilateral hand weakness and parasthesia.
• Seen by neurologist – peripheral neuropathy secondary to itraconazole. Itraconazole stopped. No recovery but no progression.
• Poor fine motor skills.
Clinical Case
• After transfer to MACFU, HR remained well with no complications
• Annual november 2008 – FEV1 1.8, FVC 2.15 (approx 65% predicted)
• Total IgE 880 KIU/l• Specific IgE Aspergillus 15.2 KUa/l• Eosinophils 0.13
Clinical Case• January 2009• Attended clinic feeling unwell• Increasing shortness of breath and cough• FEV1 1.7, FVC 2.0• CXR – no acute changes• Last sputum culture – Pseudomonas aeruginosa and Candida
glabrata.• Given 2 weeks oral ciprofloxacin and increased dose of
azithromycin.• Deterioration despite antibiotics (FEV1 1.0, CRP<5, culture
negative)• Admitted to hospital
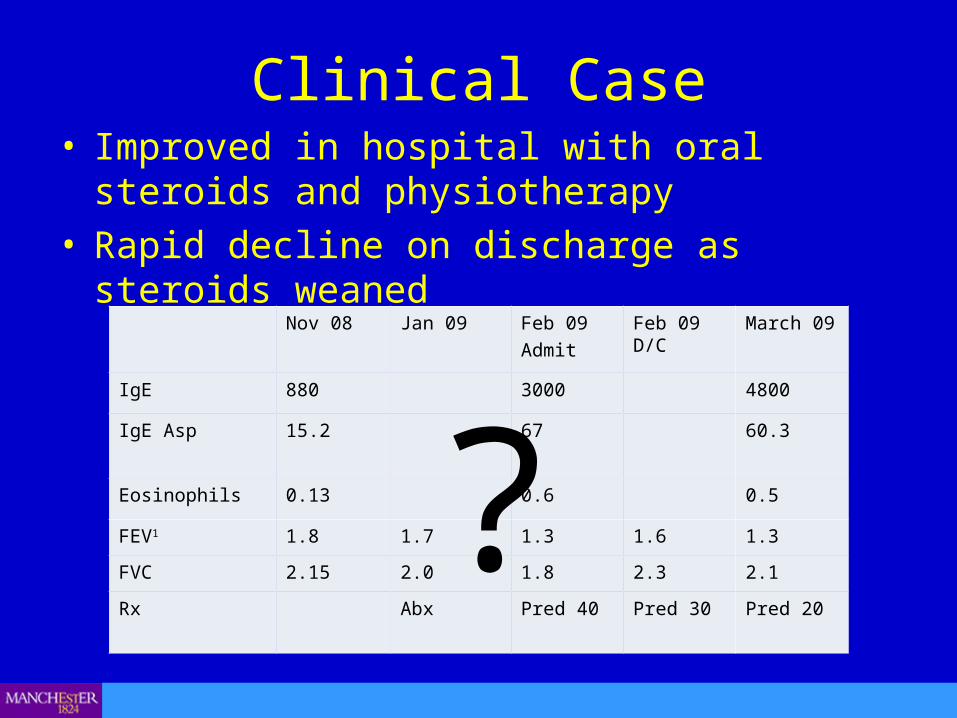
Clinical Case• Improved in hospital with oral steroids and
physiotherapy• Rapid decline on discharge as steroids weaned
Nov 08 Jan 09 Feb 09Admit
Feb 09 D/C March 09
IgE 880 3000 4800
IgE Asp 15.2 67 60.3
Eosinophils 0.13 0.6 0.5
FEV1 1.8 1.7 1.3 1.6 1.3
FVC 2.15 2.0 1.8 2.3 2.1
Rx Abx Pred 40 Pred 30 Pred 20
?
Altered mental function
• Wide description of different symptoms associated with all tri-azoles.
• Common – 20% patients• Sleep disturbance and nightmares• Poor concentration• Impaired memory - STM• Depression
Conclusions• Side effects with tri-azoles are common and often
limit their use.• The three most common neurological side effects of
tri-azoles are poor sleep/altered mental function, tremor and peripheral neuropathy.
• Drug level monitoring is important.• First ensure drug levels are in therapeutic range. If
symptoms not severe can first trial a dose reduction but maintain therapeutic levels.
• Risk balance of side effects and treatment benefit.

Questions?
www.aspergillus.org.uk