neuroimaging in bacterial and mycobacterial infections of ... · meningitis · tuberculosis ·...
TRANSCRIPT
Neuroimaging in Bacterialand Mycobacterial Infectionsof the Brain
Majda M. Thurnher
ContentsBacterial Meningitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Definition of Entity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Epidemiology/Demographics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Pathology and Pathogenesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Clinical Features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Imaging Features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Interpretation Checklist . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Clinical Case and Sample Report . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Brain Abscess . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Definition of Entity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Epidemiology/Demographics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Pathology and Pathogenesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Clinical Features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Imaging Features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Interpretation Checklist . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Clinical Case and Sample Report . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Tuberculosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
This publication is endorsed by: European Society ofNeuroradiology (www.esnr.org).
M. M. Thurnher (*)Section of Neuroradiology and MusculoskeletalRadiology, Department of Biomedical Imaging and Image-guided Therapy, University Hospital Vienna,Vienna, Austriae-mail: [email protected]
# Springer International Publishing AG, part of Springer Nature 2018F. Barkhof et al. (eds.), Clinical Neuroradiology,https://doi.org/10.1007/978-3-319-61423-6_46-1
1
Definition of Entity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Epidemiology/Demographics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Pathology and Pathogenesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Clinical Features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Imaging Features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Interpretation Checklist . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Clinical Case and Sample Report . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
AbstractBacterial infections of the central nervoussystem (CNS) continue to be an importantcause of morbidity and mortality. The spec-trum of bacterial infection of the CNS includescerebritis/brain abscesses, subdural or epidu-ral empyemas, pyogenic meningitis, andventriculitis. All carry high mortality and mor-bidity risks and, thus, require urgent and accu-rate diagnosis. Clinical neuroradiology is animportant part of patient management, as thecorrect diagnosis should be established beforefurther damage occurs. Computed tomography(CT) and magnetic resonance imaging (MRI)are radiological techniques used to detect bac-terial infections. This chapter discusses theimaging features of bacterial CNS infections.
KeywordsBrain · Infection · Bacterial brain abscess ·Meningitis · Tuberculosis · Magneticresonance imaging (MRI)
Bacterial Meningitis
Definition of Entity
Acute bacterial meningitis, or leptomeningitis,is one of the top ten infectious causes of deathworldwide and has a high potential for permanentneurological impairment, as well as high mortalityrates. It is a serious and life-threatening conditionthat requires prompt diagnosis and treatment.
Epidemiology/Demographics
The incidence of bacterial meningitis has declinedafter large-scale vaccination campaigns.
Group B Streptococcus and the E. coliand Listeria monocytogenes are the main causesof neonatal meningitis, and Streptococcuspneumoniae, Neisseria meningitides, andHaemophilus influenzae cause most cases ofmeningitis in adults. Pneumococcus causes45–72% of all bacterial meningitis cases inEurope, followed by meningococcus (11–33%).A less frequent cause of community-acquiredmeningitis is Listeria monocytogenes, whichpreferentially causes meningitis in neonates,immunosuppressed individuals, the elderly, andcancer patients.
Pathology and Pathogenesis
Most cases of bacterial meningitis develop asa result of hematogenous spread. Bacterial men-ingitis is characterized by diffuse inflammationof the pia mater and arachnoid. This leads to pusaccumulation over the surface of the brain,the cranial nerves, and the spinal cord. Due tothe dilatation and congestion of the meningealvessels, microhemorrhages and infarction willoccur. Inflammation of the ventricles results inventriculitis, with a concomitant loss of theependymal lining and gliosis of the subependymalcell layers.
2 M. M. Thurnher

Clinical Features
The classic symptoms, including high fever,neck stiffness, headache, and altered mental sta-tus, will be present in only a small percentage ofadult patients. Patients will usually present withtwo of these classic symptoms. Nausea andvomiting, signs of increased intracranial pressure,and nerve palsy are other symptoms. Even inthe absence of meningeal irritation, meningitiscannot be excluded. When a petechial rash ispresent, meningococcal infection is suspected.Waterhouse-Friderichsen syndrome is a seriouscomplication of acute fulminant meningococcalmeningitis, with bilateral adrenal insufficiencydue to hemorrhage into the adrenal glands, dis-seminated intravascular coagulation, coma, andrapid death.
Cerebrospinal fluid (CSF) analysis will showpleocytosis (100 to 10,000 white cells per cubicmillimeter), elevated protein levels (>50 mg perdeciliter), and decreased glucose levels (<40% ofsimultaneously measured serum glucose).
Imaging Features
Imaging findings in meningitis are often non-specific. Neuroimaging will be performed todetect/exclude brain shift as a precaution inselected patients before lumbar puncture.
Computed tomography (CT) may show nor-mal findings in an early stage of meningitis.Hydrocephalus, leptomeningeal enhancement, orinfarcts will be detected later with diseaseprogression.
MR imaging (MRI) is more sensitive forthe detection of meningeal pathology (Lummelet al. 2016). Fluid-attenuated inversion recovery(FLAIR) sequences have been reported to be themost sensitive MR technique for the detection ofmeningeal diseases. Congestion and hyperemia ofthe leptomeninges in meningitis produces exu-dates in the subarachnoid space. A high signalwill be present in the subarachnoid spaces,
which reflects the high protein content in thecerebral spinal fluid (CSF) (Fig. 1). High signalintensity within the CSF on FLAIR images mayalso be seen in metastatic disease, subarachnoidhemorrhage, oxygen administration, and somesedation agents. For the depiction ofleptomeningeal diseases, post-contrast 3DT2-FLAIR has been reported to be superior topost-contrast 3D T1-weighted MR imaging(Fukuoka et al. 2010) (Fig. 2).
Hyperintense diffusion-weighted (DW) MRimaging lesions are frequently found in the ven-tricles (especially the lateral ventricles) in patientswith bacterial meningitis, which represent puru-lent fluid in the ventricles (Fig. 3) (Fukui et al.2001). In addition, diffusion-weighted imaging(DWI) hyperintense lesions are seen in the corticalsulci (Fig. 3). Sulcal and ventricular DWI abnor-malities have been described to occur more oftenin Streptococcus pneumoniae, compared to men-ingitis caused by other organisms. In bacterialmeningitis, DWI hyperintense lesions may alsobe seen in the Virchow-Robin spaces (VRSs)(Fig. 4). Based on recent studies, VRSs arebelieved to be an important drainage pathway forparenchymal interstitial fluid returning to theblood (glymphatic system) (Plog and Nedeergard2018).
In pneumococcal meningoencephalitis, wide-spread FLAIR-hyperintense lesions may bepresent, which are indicative of extensive paren-chymal injury due to local areas of ischemia withcytotoxic edema and demyelination, secondary tothe immunologically mediated necrotizing vascu-litis and thrombosis (Fig. 4).
As a result of an inflammatory vasculitisand thrombosis of small vessels, ischemic infarc-tions will occur in 25% of meningitis cases.Commonly, they will be located in the genu ofthe internal capsule. Callosal infarction orinfection-associated cytotoxic lesions of the cor-pus callosum (CLOCC) have also been reported(Fig. 5).
Unilateral or bilateral subdural fluid collec-tions are more common in children with
Neuroimaging in Bacterial and Mycobacterial Infections of the Brain 3
bacterial meningitis, compared to adults. The ster-ile fluid collections will show CSF intensity on allsequences. Subdural empyema is defined asa purulent subdural collection. DWI is helpful indistinguishing sterile collections from empyema,
which show restricted diffusion and a high signalon DWI (Fig. 6). A predisposing condition forsubdural empyema is otitis or sinusitis withcontinuous spread to the subdural space.
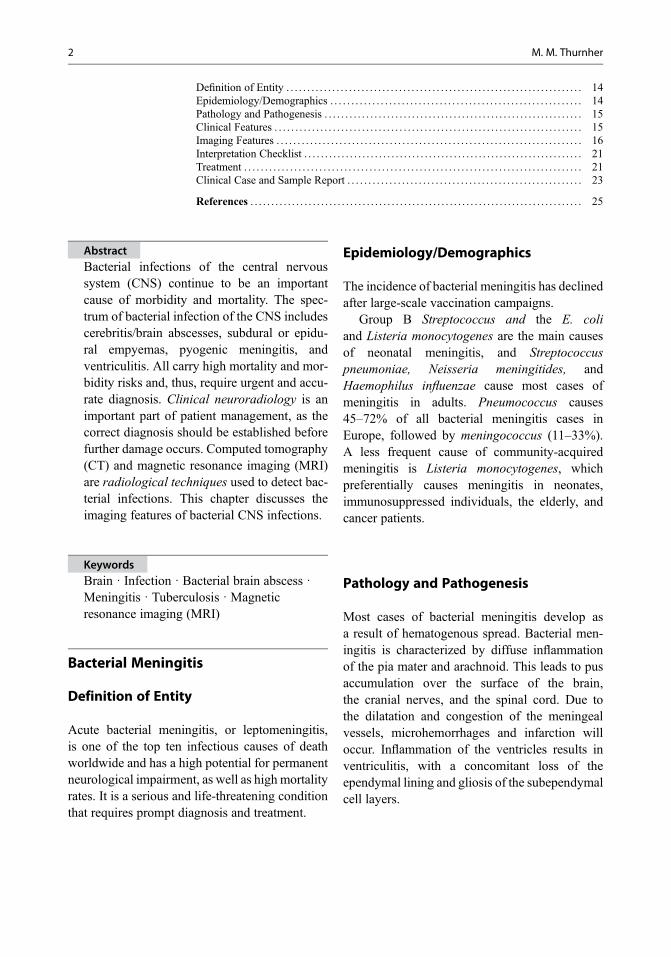
Fig. 1 Bacterial meningitis in a 4-year-old girl. On axialFLAIR images (a–c), the subarachnoid spaces and thebasal cistern appeared hyperintense, with dilatation of the
ventricular system. Post-contrast T1WI magnetization-transfer-contrast images showed leptomeningeal enhance-ment (d–f)
Fig. 2 Leptomeningealdisease is more prominenton contrast-enhancedFLAIR (b) compared topost-contrast 3DT1-weighted MRimaging (a)
4 M. M. Thurnher

Acute pneumococcal meningitis maybe accompanied by immunological para-infectious processes, such as acute demyelinatingencephalomyelitis (ADEM), cerebral vasculitis,or acute necrotizing hemorrhagic encephalomy-elitis. Intracranial hemorrhage is a rare but
devastating complication in patients withcommunity-associated bacterial meningitis, andthe risk is even higher in those treated with anti-coagulant therapy (Table 1).
Fig. 3 Pyogenic meningitis in a 64-year-old male patient.On DWI (a–c), hyperintensity was seen in the lateralventricle, which is consistent with pyogenic ventriculitis.
Post-contrast T1WI (d) demonstrated subependymalenhancement. DWI hyperintensities were present in thecortical sulci of both brain convexities (b, c)
Fig. 4 Pneumococcal meningitis in a 51-year-old femalepatient. On DWI, hyperintensities were detected in theoccipital horns of the lateral ventricles, representingrestricted diffusion of the pus (a). A high intraventricularsignal can also be seen on the FLAIR image (d). BilateralFLAIR and DWI hyperintensities were also detected in the
subcortical white matter of the frontal lobe (b, e), consis-tent with demyelinating lesions with cytotoxic edema.Multiple, small FLAIR and DWI hyperintensities weredetected in the watershed zones, representing infarctions(c, f)
Neuroimaging in Bacterial and Mycobacterial Infections of the Brain 5
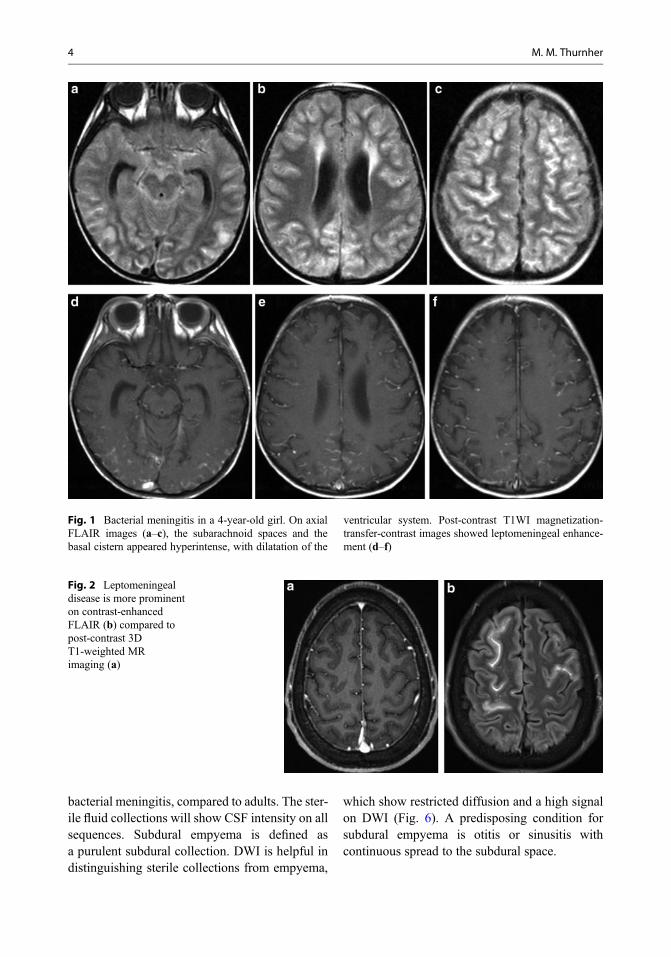
Fig. 5 Meningococcal meningitis in a 28-year-old patientwho presented with fever and meningeal signs. There were4400 μl white cells found at the CSF analysis. The FLAIRimage (a) showed a high signal intensity lesion in thecorpus callosum with restricted diffusion (c), consistent
with an infection-associated cytotoxic lesion of the corpuscallosum (CLOCC) (red arrow). Linear DWI hyper-intensity in the right frontal lobe represents purulent fluidin the VR spaces (arrow, c)
Fig. 6 Bacterial meningitis in a 42-year-old male patient.On FLAIR (a), a high signal was detected in the subarach-noid spaces and bilateral subdural fluid collections. OnDWI, a high signal was detected in the subdural
collections, indicating purulent fluid in the subdural empy-ema (b). Intense enhancement was observed on contrast-enhanced T1WI images (c, d)
Table 1 Summary of imaging findings in meningitis
FLAIR Post-contrast T1WI/FLAIR DWI
Subarachnoidspaces
Hyperintense Leptomeningealenhancement
High signal (purulent fluid)
Ventricles • High signal with debris inventriculitis• Enlarged in hydrocephalus
• Subependymalenhancement in ventriculitis• No enhancement inhydrocephalus
• High signal in ventriculitis(intraventricular pus)• Low signal in hydrocephalus
Subduralcollections
High signal (high proteincontent)
• No enhancement in sterilecollections• Peripheral enhancement inempyema
• Low signal in sterilecollections• High signal in empyema
Infarcts Hyperintense Enhancing in subacute stage High signal in acute stage(cytotoxic edema)
White matterlesions
Hyperintense No enhancement High signal (cytotoxic edema)
Virchow-Robinspaces
Linear hyperintensities No enhancement High signal (purulent fluid)
6 M. M. Thurnher
Interpretation Checklist
• FLAIR-hyperintense subarachnoid spaces.• Post-contrast 3D T2-FLAIR is superior to post-
contrast MPRAGE imaging in demonstratingmeningeal enhancement.
• Check the ventricles (hydrocephalus orventriculitis) when meningitis is suspected.
• Infarcts are common in bacterial meningitis.• Linear DWI hyperintensities in meningitis
reflect the spread of the infection through theperivascular spaces.
Treatment
Community-acquired meningitis caused byS. pneumoniae has high mortality rates(20–40%), with long-term neurologic sequelaedeveloping in 30% of cases (hearing loss andfocal neurologic deficits). The mortality andmorbidity for meningococcal meningitis arelower, with mortality rates up to 13% and morbid-ity rates of 3–7%. Predictors for unfavorable out-come in bacterial meningitis are advanced age,
low Glasgow Coma Scale (GCS), cranial nervepalsies, positive blood cultures, and <1000leucocytes/ul, as well as a high-protein concentra-tion in the CSF on admission.
Initial therapy is broad-spectrum cephalospo-rin combined with vancomycin, followed by clas-sic penicillin if no resistances are detected. Inaddition, the concomitant administration of dexa-methasone before or with antibiotics cansignificantly reduce mortality in pneumococcalmeningitis.
Neurosurgical intervention is the first-choicetherapy in patients with empyema that causesa midline shift and focal neurologic abnormalities,or a decreased level of consciousness.
Clinical Case and Sample Report
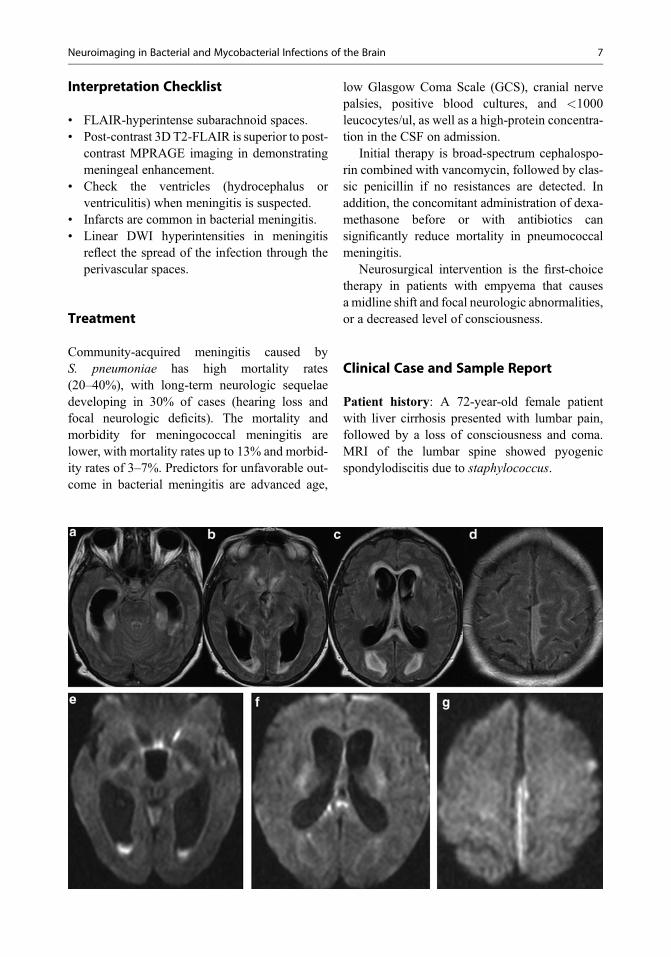
Patient history: A 72-year-old female patientwith liver cirrhosis presented with lumbar pain,followed by a loss of consciousness and coma.MRI of the lumbar spine showed pyogenicspondylodiscitis due to staphylococcus.
Neuroimaging in Bacterial and Mycobacterial Infections of the Brain 7
Clinical diagnosis: CT showed hydrocepha-lus, and CSF analysis revealed 72/cells, increasedproteins, and clinical suspicion of meningitis.
Purpose of MR study: Rule out meningitis,cause of hydrocephalus.
Imaging technique:Axial FLAIR, axial DWI,coronal T2WI, axial pre- and post-contrast T1WI.
Full findings: On axial FLAIR images, allsubarachnoid spaces appeared hyperintense(a–d). Ventricular system was enlarged, with peri-ventricular hyperintensities and a fluid levelin the occipital horns (b). In addition, subduraleffusion was noted on the parasagittal leftfrontoparietal image (d). On DWI, high signalwas observed in the ventricles (e), in the corpuscallosum (f), and also in the left subdural effusion(f).
Interpretation: The high signal of the sub-arachnoid spaces and enlargement of the ventri-cles suggested meningitis with hydrocephalus.Intraventricular fluid with restricted diffusionis consistent with purulent content in ventriculitis.The diffusion characteristics of subdural effusionclearly indicated the presence of pus in a subduralempyema.
Brain Abscess
Definition of Entity
A brain abscess is a focal infection of the brainthat begins as a localized area of softening ofthe brain parenchyma (cerebritis) and developsinto a collection of pus surrounded by a capsule.Brain abscess remains a serious medical issuedespite recent advances made in detection andtherapy.
Epidemiology/Demographics
The incidence of brain abscesses does not showgeographical differences and has been estimatedat 0.3–0.9 per 100,000 inhabitants per year witha male-to-female ratio of 2:1–3:1 and a medianage of 30–40 years. The risk of brain abscess ishigh in patients with hereditary hemorrhagic
telangiectasia, in patients with infective endocar-ditis, and in patients who have undergone cranialsurgery. The widespread use of antibiotics hascontributed to a decreased incidence of intracra-nial abscesses.
Approximately 80% of brain abscess arecaused by one pathogen, but polymicrobialabscesses will be seen in 20% of patients.Streptococci are the predominant bacteria,followed by staphylococci (S. aureus in morethan 80%) and gram-negative bacilli.
Pathology and Pathogenesis
Bacterial agents enter the brain either throughcontiguous spread (e.g., following otitis, mastoid-itis, sinusitis, neurosurgical procedures, or cranialtrauma) or through hematogenous dissemina-tion (endocarditis being the most common,followed by pulmonary and dental infections).Brain abscess has four well-defined stages: earlycerebritis (days 1–3), late cerebritis (days 4–9),early capsule formation (days 10–13), and latecapsule formation (14 days and later). Five dis-tinct histological zones are present: (a) a well-formed necrotic center; (b) a peripheral zoneof inflammatory cells, macrophages, and fibro-blasts; (c) a dense collagenous capsule; (d) alayer of neovascularization associated with con-tinuing cerebritis; and (e) astrogliosis and cerebraledema external to the capsule.
Clinical Features
Headache, fever, and focal neurologic deficitsare the most common symptoms; however, theclassic triad consisting of these three symptomsis only present in 20% of patients.
Imaging Features
Brain abscesses will be recognized as focal brainmasses with a T2 high-signal-intensity center,a three-layered T2 low-signal-intensity capsule,marked perifocal edema, and ring-like
8 M. M. Thurnher
enhancement on post-contrast T1WI. Enhance-ment can be smooth or irregular. The abscesscavity usually shows a homogeneous high signalon DWI with low apparent diffusion coefficient(ADC) values, reflecting restricted diffusion dueto the high viscosity content of the abscess cavity(Fig. 7).
On susceptibility-weighted MR imaging(SWI), pyogenic brain abscesses demonstrate the“dual-rim sign,” defined as two concentric rimssurrounding the central cavity at the lesion mar-gins, with the outer one hypointense and the innerone hyperintense relative to the cavity contents(Toh et al. 2012) (Fig. 8). The dual-rim sign hasnot been described in abscesses of other origins.
Hemorrhage is considered a rare finding inpyogenic brain abscesses. In some patients, moreprominent SWI hypointensities in the enhancingwalls of brain abscesses will be detected, indicat-ing some degree of hemorrhage. This has beenproven by a recent 3.0T study, with reported hem-orrhage in the wall of a brain abscess. One possi-ble explanation would be neoangiogenesis in
the wall of the abscess, with the rupture of newlyformed fragile blood vessels. Hemorrhagic brainabscesses may also be seen in patients with con-genital cyanotic heart diseases and in patients withinfective endocarditis.
Perfusion MRI has been shown to reliablydiscriminate pyogenic brain abscesses that displaylow regional cerebral blood volume (rCBV) fromnecrotic brain tumors, with elevated rCBV(Fig. 9). This can be explained by the histologicalfindings in mature brain abscesses, which arecharacterized by high amounts of mature collagenand decreased neovascularity. Rarely, in bacterialbrain abscesses, high rCBV in the enhancing partwill be detected (Fig. 10). The logical explanationis the stage of the abscess, where increased capil-lary density in an early capsular stage would pro-duce increased rCBV.
On MR spectroscopy (MRS) in bacterialabscesses, the following peaks will be observed:succinate, acetate, lactate, and amino acid peaks.Proteolytic enzymes released by neutrophils pro-duce cytosolic amino acids (valine, leucine,
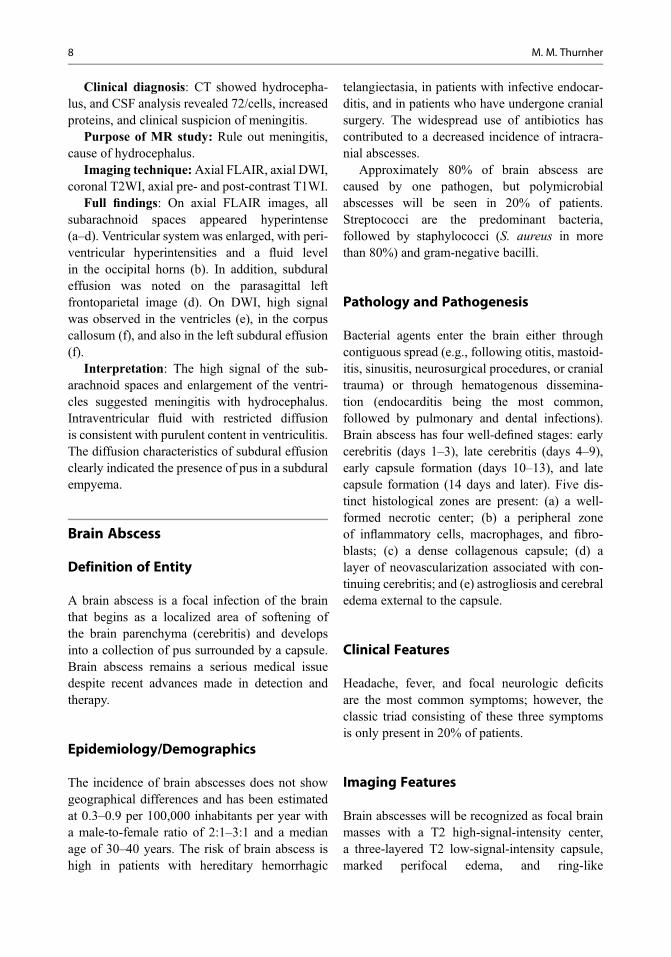
Fig. 7 A bacterial brain abscess in an immunocompetentpatient, with a ring-like, enhancing, intra-axial lesion in theright parietal lobe (a). On DWI, the center of the lesion
shows a high signal (b) with low ADC (c), reflectingrestricted diffusion due to the purulent content of theabscess cavity
Fig. 8 Axial T2WI (a) andSWI (b) in a pyogenic brainabscess demonstrating themultilayered appearance ofthe capsule with a “dual-rimsign” on SWI
Neuroimaging in Bacterial and Mycobacterial Infections of the Brain 9
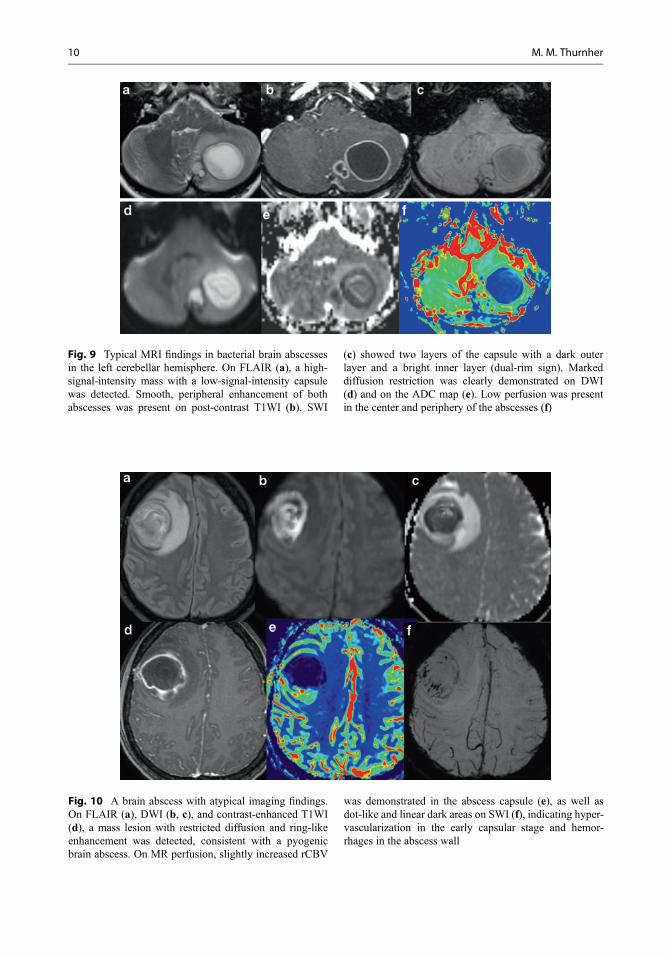
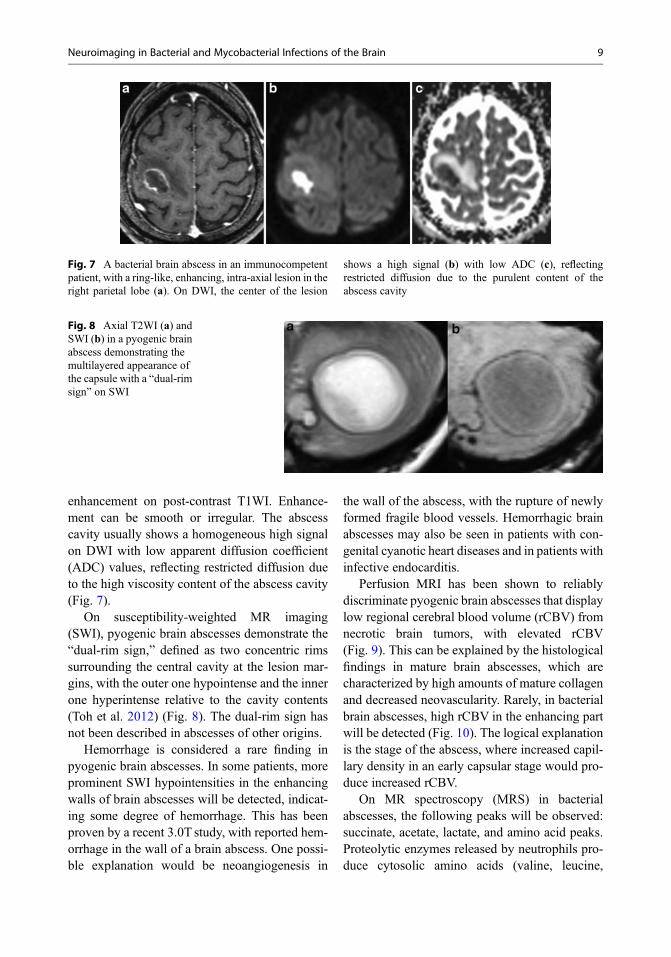
Fig. 10 A brain abscess with atypical imaging findings.On FLAIR (a), DWI (b, c), and contrast-enhanced T1WI(d), a mass lesion with restricted diffusion and ring-likeenhancement was detected, consistent with a pyogenicbrain abscess. On MR perfusion, slightly increased rCBV
was demonstrated in the abscess capsule (e), as well asdot-like and linear dark areas on SWI (f), indicating hyper-vascularization in the early capsular stage and hemor-rhages in the abscess wall
Fig. 9 Typical MRI findings in bacterial brain abscessesin the left cerebellar hemisphere. On FLAIR (a), a high-signal-intensity mass with a low-signal-intensity capsulewas detected. Smooth, peripheral enhancement of bothabscesses was present on post-contrast T1WI (b). SWI
(c) showed two layers of the capsule with a dark outerlayer and a bright inner layer (dual-rim sign). Markeddiffusion restriction was clearly demonstrated on DWI(d) and on the ADC map (e). Low perfusion was presentin the center and periphery of the abscesses (f)
10 M. M. Thurnher
isoleucine), while bacterial fermentation leads tothe occurrence of lactate, acetate, and succinate,and the necrosis of cerebral tissue results in theformation of lactate and lipids (Lai et al. 2005).Furthermore, MRS can differentiate betweenaerobic and anaerobic infections. Succinate andacetate signal resonances suggest an anaerobicagent.
Differential Diagnosis of Ring-LikeEnhancing Focal Brain LesionsNecrotic brain tumors (cystic glioblastoma,metastases) may present as ring-like, enhancing,focal brain masses. Differentiation from infec-tious lesions is an important diagnostic challenge.Conventional MRI sequences (FLAIR, T2WI,T1WI) cannot differentiate between those entities.
Bacterial brain abscesses will show restricteddiffusion with low ADC, whereas necrotic tumorswill demonstrate elevated diffusion with a lowsignal on trace DWI and high ADC values(Chiang et al. 2009). Pus in the cavity of a brainabscess consists of inflammatory cells, bacteria,necrotic tissue, and highly viscous proteinaceousexudates; in contrast, metastatic tumors usuallyconsist of necrotic tissue debris, fewer inflamma-tory cells, and serous fluid. Abscesses of otheraetiologies (fungal, parasitic, tuberculous) mayshow restricted and elevated diffusion (dependingon their content) and cannot be reliably differen-tiated from tumors based on DWI only. Hyper-cellular, highly viscous mucin content and
hemorrhagic metastases may present as ring-like,enhancing, focal brain masses with restricted dif-fusion (Fig. 11). A small percentage of untreatedbacterial brain abscesses will show a low diffusionsignal similar to that of brain tumors (5%–21%).
While the capsular portions of abscesses arehypovascular, causing a marked decrease in rCBVratios, the peripheral portions of malignant cystictumors have higher vascularization and higherrCBV ratios than those of abscesses. This is truefor all abscesses, independent of their causalagent. However, abscesses with increased rCBVin the enhancing part will be seen in the earlycapsular stage (Fig. 10).
SWI has proven useful in the differentiation ofbacterial brain abscesses and cystic neoplasticlesions. On SWI, the hypointense rims ofabscesses tend to be complete and smooth and tohave the same locations as the contrast-enhancingrims. In contrast, hypointense SWI rims innecrotic glioblastomas are incomplete, irregular,and frequently found at the inner aspect of thecontrast-enhancing rims (Toh et al. 2012). Whenusing SWI on 1.5 T, mild hypointensity or iso-intensity of the capsule will be detected, anda dual-rim sign will not be present (Lai et al.2012). The dual-rim sign will be present only inbacterial brain abscesses and will never be seenin metastatic lesions or glioblastomas. In necroticglioblastomas, conglomerates of dots or fine lin-ear susceptibility effects will be detected (Figs. 12and 13).
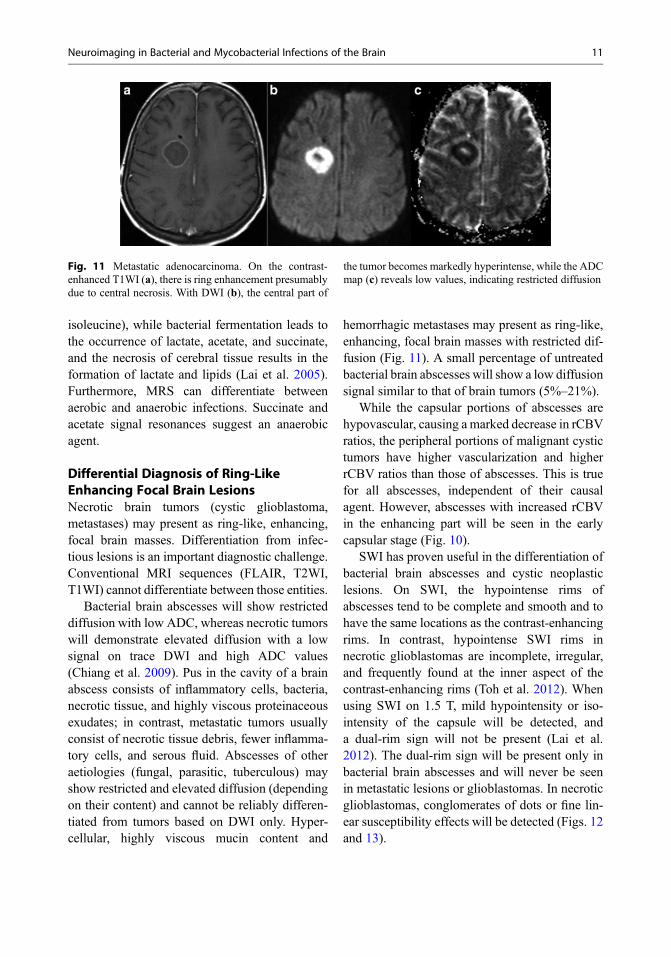
Fig. 11 Metastatic adenocarcinoma. On the contrast-enhanced T1WI (a), there is ring enhancement presumablydue to central necrosis. With DWI (b), the central part of
the tumor becomes markedly hyperintense, while the ADCmap (c) reveals low values, indicating restricted diffusion
Neuroimaging in Bacterial and Mycobacterial Infections of the Brain 11
Interpretation Checklist
• Bacterial brain abscesses have aT2-hyperintense center, a T2-hypointense cap-sule, and marked perifocal edema.
• Due to restricted diffusion, bacterial brainabscesses have a high signal on DWI and lowADC values.
• SWI can be used to distinguish between bacte-rial and fungal abscesses, as the “dual-rimsign” will be seen only in bacterial abscesseson 3T.
• Ring-enhancing lesions of infectious originhave low rCBV.
Treatment
The prognosis of patients with brain abscesseshas gradually improved due to improvements inimaging, neurosurgical technique, and antimicro-bial regimens. The mortality rate has decreasedfrom 40% to 10% in the last six decades, and therate of patients who achieve full recovery hasincreased from 33% to 70%.
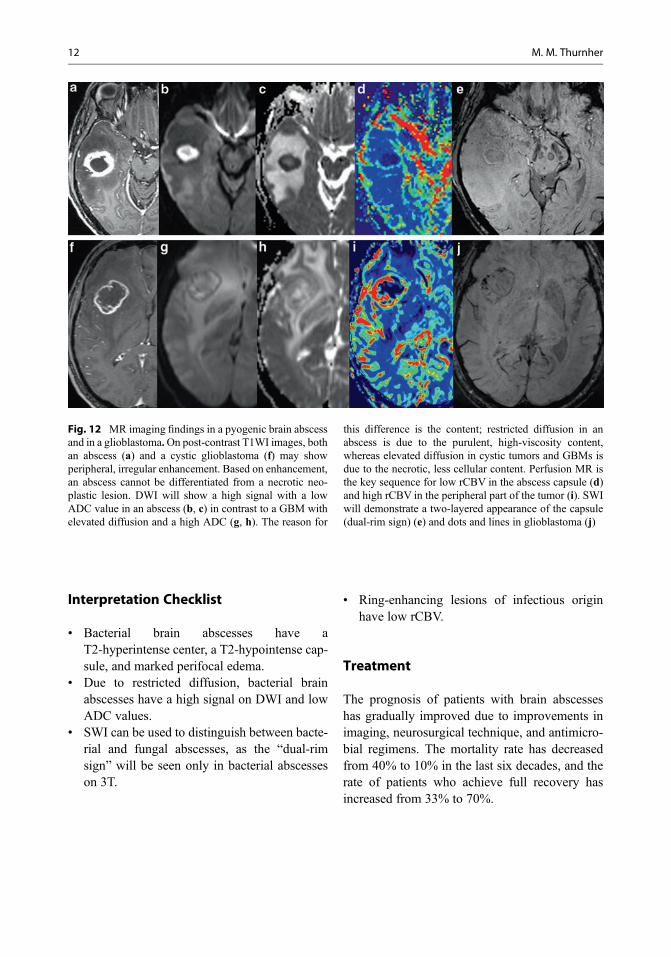
Fig. 12 MR imaging findings in a pyogenic brain abscessand in a glioblastoma.On post-contrast T1WI images, bothan abscess (a) and a cystic glioblastoma (f) may showperipheral, irregular enhancement. Based on enhancement,an abscess cannot be differentiated from a necrotic neo-plastic lesion. DWI will show a high signal with a lowADC value in an abscess (b, c) in contrast to a GBM withelevated diffusion and a high ADC (g, h). The reason for
this difference is the content; restricted diffusion in anabscess is due to the purulent, high-viscosity content,whereas elevated diffusion in cystic tumors and GBMs isdue to the necrotic, less cellular content. Perfusion MR isthe key sequence for low rCBV in the abscess capsule (d)and high rCBV in the peripheral part of the tumor (i). SWIwill demonstrate a two-layered appearance of the capsule(dual-rim sign) (e) and dots and lines in glioblastoma (j)
12 M. M. Thurnher
Clinical Case and Sample Report
Patient history: A 30-year-old male patient withcyanotic heart disease
Clinical diagnosis: Cerebral infectionPurpose ofMR study: Rule out focal brainmassImaging technique: Axial FLAIR, T1WI,
post-contrast T1WI, DWI, SWI
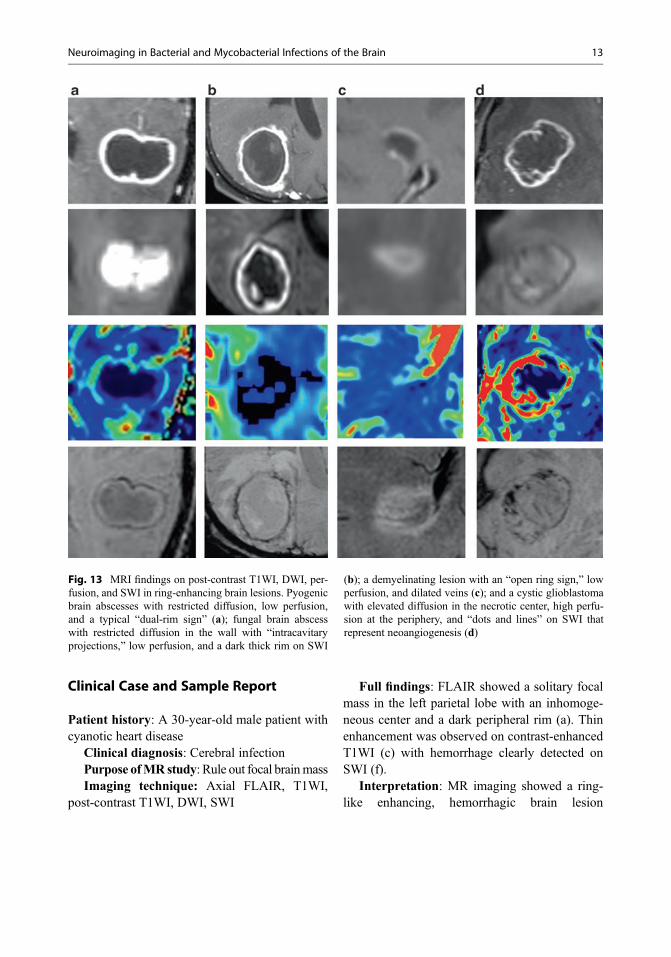
Full findings: FLAIR showed a solitary focalmass in the left parietal lobe with an inhomoge-neous center and a dark peripheral rim (a). Thinenhancement was observed on contrast-enhancedT1WI (c) with hemorrhage clearly detected onSWI (f).
Interpretation: MR imaging showed a ring-like enhancing, hemorrhagic brain lesion
Fig. 13 MRI findings on post-contrast T1WI, DWI, per-fusion, and SWI in ring-enhancing brain lesions. Pyogenicbrain abscesses with restricted diffusion, low perfusion,and a typical “dual-rim sign” (a); fungal brain abscesswith restricted diffusion in the wall with “intracavitaryprojections,” low perfusion, and a dark thick rim on SWI
(b); a demyelinating lesion with an “open ring sign,” lowperfusion, and dilated veins (c); and a cystic glioblastomawith elevated diffusion in the necrotic center, high perfu-sion at the periphery, and “dots and lines” on SWI thatrepresent neoangiogenesis (d)
Neuroimaging in Bacterial and Mycobacterial Infections of the Brain 13
consistent with a brain abscess or a necrotic neo-plastic lesion. Based on imaging findings, a neo-plastic or infectious origin could not be reliablydifferentiated. Perfusion MR imaging was addi-tionally performed, which demonstrated lowrCBV, suggesting an infectious origin of thelesion. Surgical drainage revealed a pyogenicbrain abscess (Fusobacterium necrophorum).Hemorrhagic pyogenic brain abscesses are fre-quently seen in patients with cyanotic heartdisease.
Tuberculosis
Definition of Entity
Tuberculosis (TB) is a granulomatous infection,caused by Mycobacterium tuberculosis. It mayinvolve the meninges, brain, spinal cord, calvar-ium, or bony spine. The incidence of tuberculosishas increased significantly in recent years in bothimmunocompetent and immunocompromisedindividuals. Among all forms of tuberculosis,
central nervous system (CNS) TB accounts forapproximately 10% of all cases and carries thehighest mortality.
Epidemiology/Demographics
Tuberculosis remains a global health problem,and the disease kills almost two million peopleeach year. The estimated number of tuberculosiscases was 10.4 million in 2015, with 1.8 milliondeaths resulting from the disease. Countries inthe eastern part of Europe are the most affectedby the TB epidemic (WHO 2017). In 2015, WHOreported 45% of new registered TB caseswere among people 25–44 years of age, and chil-dren under 15 years of age represent approxi-mately 4% of the total notified TB patients.Europe’s TB burden is among the lowest in theworld, but the number of new multidrug-resistantTB (MDR-TB) cases is the highest. The drug-resistant TB meningitis in people who areco-infected with human immunodeficiencyvirus-1 (HIV-1) has a particularly poor prognosis,approaching 100% mortality.
14 M. M. Thurnher

Pathology and Pathogenesis
Mycobacterium tuberculosis reaches the CNSthrough a hematogenous route secondary to dis-ease elsewhere in the body either during the stageof bacillemia of primary tuberculous infection orfollowing late reactivation of TB. An initial CNStuberculous lesion (Rich focus) may be inoculatedin the meninges, subpial or subependymal sur-faces of the brain, and the spinal cord and mayremain dormant for years. Later, rupture or growthof one or more of these tuberculous lesions pro-duces various types of CNS TB. In tuberculousmeningitis, gelatinous or fibrinous exudates arepresent in the subarachnoid spaces, often at thebase of the brain, obliterating the arteries andencasing the cranial nerves.
Tuberculous granuloma (tuberculoma) is com-posed of a central zone of caseation necrosis,surrounded by a capsule of collagenous tissue, epi-thelioid cells, multinucleated giant cells, and mono-nuclear inflammatory cells. Outside the capsule,there is parenchymal edema and astrocytic prolifer-ation. Tuberculomas do not contain TB organisms.
In contrast to the caseation seen in the granu-loma, the tuberculous abscess is formed by semi-liquid pus teeming with tubercle bacilli. A TBabscess has an inflammatory neovascular capsuleof granulation tissue and lacks the giant cell epi-thelioid granulomatous reaction of a TB granu-loma (Table 2).
Clinical Features
TB meningitis begins with nonspecific pro-dromes, followed by meningeal signs such as
headache, fever, vomiting, and neck stiffness.Meningeal signs and symptoms become progres-sively more prominent, with loss of conscious-ness, focal neurological deficits, cranial nervepalsies, and limb weakness. If treatment is notinitiated, death will occur. According to the Med-ical Research Council, tuberculous meningitis canbe classified as follows: Grade I (GCS score15, no focal neurological signs), Grade II (GCSscore 11–14 or 15 with focal neurological signs),and Grade III (GCS score � 10).
Cerebrospinal fluid (CSF) typically has150–1000 leukocytes per μl, with a mixed popu-lation of neutrophils and lymphocytes, elevatedprotein (0.8–2.0 g/dl), and CSF-plasma glucoseratios of <0.5 in 90% of individuals.
Sputum microscopy and culture in liquidmedium, with subsequent drug-susceptibility test-ing, are currently recommended as standardmethods for the diagnosis of active tuberculosis.The implementation of a new molecular diagnos-tic test, the Xpert MTB/RIF assay, can signifi-cantly improve the early detection of theMycobacterium tuberculosis complex (within2 h).
Imaging Features
Meningeal TuberculosisIn tuberculous meningitis (TBM), FLAIR willshow hyperintense subarachnoid spaces andcisterns at the base of the brain (interpeduncularfossa, suprasellar, perimesencephalic, and pon-tine cisterns), as well as intense leptomeningealenhancement on post-contrast T1WI or post-contrast FLAIR (Figs. 14 and 15). Basal enhance-ment is often less prominent in people who areco-infected with HIV-1, especially those with verylow CD4+ cell counts. The brain parenchyma willshow a high signal on T2WI and FLAIR dueto edema (Figs. 15 and 16). With disease prog-ression, communicating or non-communicatinghydrocephalus may occur. Communicatinghydrocephalus is the result of inflammatory exu-date in the basal cisterns, with obstruction.Non-communicating hydrocephalus will occurdue to ependymitis or compression of the
Table 2 shows the spectrum of CNS lesions in tubercu-losis (TB). (Adopted from Chaudhary et al. 2017)
Meningeal TB • Tuberculous meningitis (TBM)• Tuberculous pachymeningitis• Granulomatous basal meningitis
ParenchymalTB
• Tuberculous granuloma(tuberculoma)• En plaque tuberculoma• Miliary tuberculosis• Tuberculous abscess• Tuberculous encephalopathy
Neuroimaging in Bacterial and Mycobacterial Infections of the Brain 15
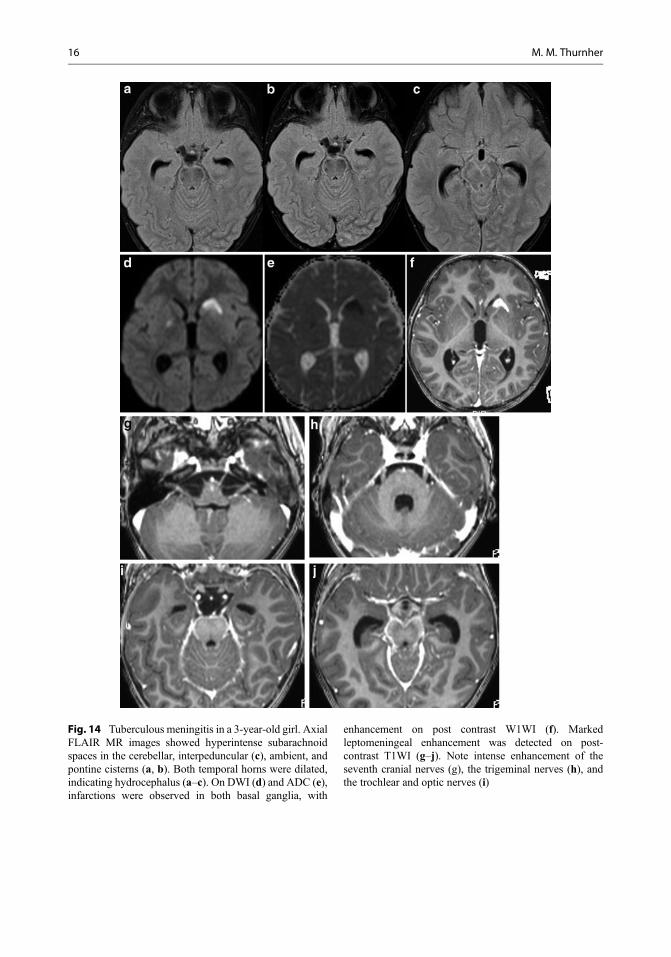
Fig. 14 Tuberculous meningitis in a 3-year-old girl. AxialFLAIR MR images showed hyperintense subarachnoidspaces in the cerebellar, interpeduncular (c), ambient, andpontine cisterns (a, b). Both temporal horns were dilated,indicating hydrocephalus (a–c). On DWI (d) and ADC (e),infarctions were observed in both basal ganglia, with
enhancement on post contrast W1WI (f). Markedleptomeningeal enhancement was detected on post-contrast T1WI (g–j). Note intense enhancement of theseventh cranial nerves (g), the trigeminal nerves (h), andthe trochlear and optic nerves (i)
16 M. M. Thurnher
ventricle by a tuberculous mass lesion. Childrenwith TBM are more likely to show hydrocephalusthan are adults with TBM. Spread of the infectionto small vessels will cause arteritis and subsequentthrombosis and infarctions. Infarctions are arterial
in origin, and the venous system is spared (Kalitaet al. 2018). Infarctions are located in the basalganglia region and in the internal capsule and willbe best depicted with DWI (Fig. 14). On MRangiography (MRA), narrowing or occlusion of
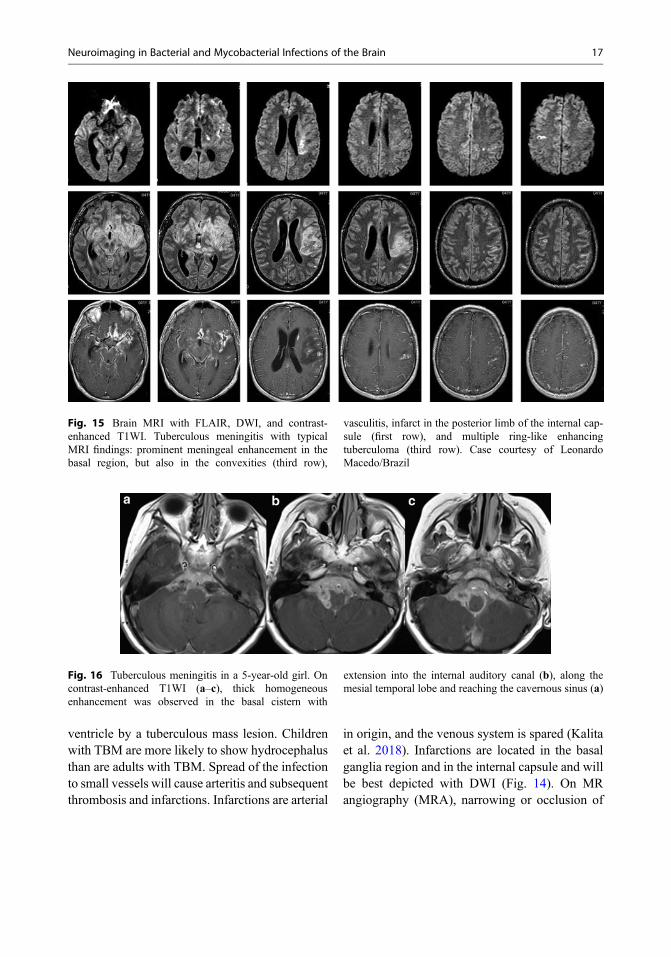
Fig. 15 Brain MRI with FLAIR, DWI, and contrast-enhanced T1WI. Tuberculous meningitis with typicalMRI findings: prominent meningeal enhancement in thebasal region, but also in the convexities (third row),
vasculitis, infarct in the posterior limb of the internal cap-sule (first row), and multiple ring-like enhancingtuberculoma (third row). Case courtesy of LeonardoMacedo/Brazil
Fig. 16 Tuberculous meningitis in a 5-year-old girl. Oncontrast-enhanced T1WI (a–c), thick homogeneousenhancement was observed in the basal cistern with
extension into the internal auditory canal (b), along themesial temporal lobe and reaching the cavernous sinus (a)
Neuroimaging in Bacterial and Mycobacterial Infections of the Brain 17
the arteries will be observed. Cranial nerveinvolvement will occur with a perineural infectionspread and thickened enhancing nerves (Fig. 14).The differential diagnosis of tuberculous menin-gitis includes nontuberculous bacterial meningi-tis, sarcoidosis, and neoplastic meningitis.
Chronic tuberculous infection may causepachymeningitis,with focal or diffuse dural thick-ening. Plaque-like focal thickening may appearhypointense on T1/T2 and show intense contrastenhancement.
Granulomatous tuberculous meningitis ischaracterized by dense basal enhancement withsuperimposed masses (Fig. 16).
Parenchymal TuberculosisTuberculous granuloma (tuberculoma) is the mostcommon parenchymal form of CNS TB.Tuberculomas are solitary or multiple focal brainlesions. They do not have to be associated withmeningitis, and the reported incidence of coexis-tent CNS tuberculoma and tuberculous meningitisis only 10–50%. Usually, tuberculomas arelocated in the corticomedullary junction, the
basal ganglia, and the cerebellum. Rare locationsinclude the pituitary stalk and ventricles. Intraven-tricular tuberculomas are mostly reported in chil-dren and are extremely rare in adults. Septumpellucidum traction, ependymal attachment, andasymmetric hydrocephalus have been observed incases of intraventricular tuberculoma of the thirdventricle, suggesting an adhesive process charac-teristic of intraventricular tuberculosis.
The imaging features of a tuberculoma dependon the stage of infection. Noncaseatingtuberculomas have low T1WI and high T2WIsignal and show nodular enhancement. Caseatingtuberculomas are T1- and T2WI hypointenseand demonstrate ring-like enhancement oncontrast-enhanced T1WI. DWI characteristicswill also depend on the stage and content;caseating tuberculomas with a T2 high-signal-intensity center show restricted diffusion and can-not be differentiated from bacterial abscesses(Fig. 17a–c), whereas caseating tuberculomaswith a T2-low-signal-intensity center have ele-vated diffusion (Fig. 17d–f) (Gupta et al. 2005).
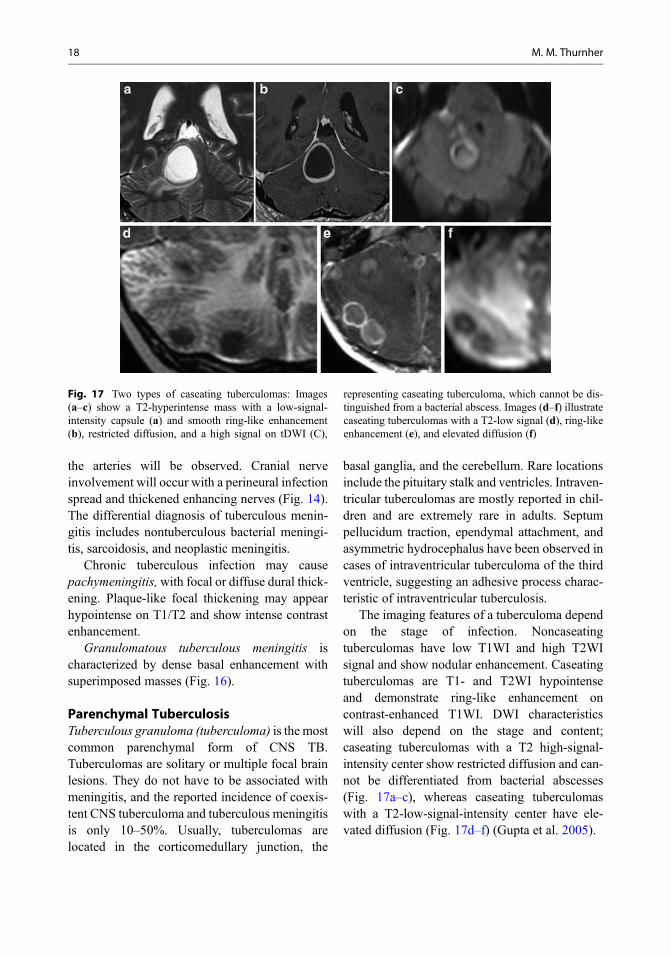
Fig. 17 Two types of caseating tuberculomas: Images(a–c) show a T2-hyperintense mass with a low-signal-intensity capsule (a) and smooth ring-like enhancement(b), restricted diffusion, and a high signal on tDWI (C),
representing caseating tuberculoma, which cannot be dis-tinguished from a bacterial abscess. Images (d–f) illustratecaseating tuberculomas with a T2-low signal (d), ring-likeenhancement (e), and elevated diffusion (f)
18 M. M. Thurnher
MR spectroscopy (MRS) is helpful in thedifferentiation of tuberculomas from ring-likeenhancing lesions of other origin (Fig. 18). Alarge lipid peak will be found in T2-hypointensecaseating tuberculomas, and large choline andlipid peaks will be detected in T2-hyperintensetuberculomas. Healed tuberculomas may calcifyin up to 23% of cases, and these are usually betterdetected on CT than on MRI.
Tuberculous AbscessTuberculous abscesses are common in elderlyand immunocompromised patients. On conven-tional MR imaging, TB abscesses are large, multi-loculated masses, with thick enhancement andperilesional edemawith mass effect. MR spectros-copy is helpful in these cases (Fig. 18). Theabsence of cytosolic amino acids in a tuberculosisabscess is regarded as very significant for
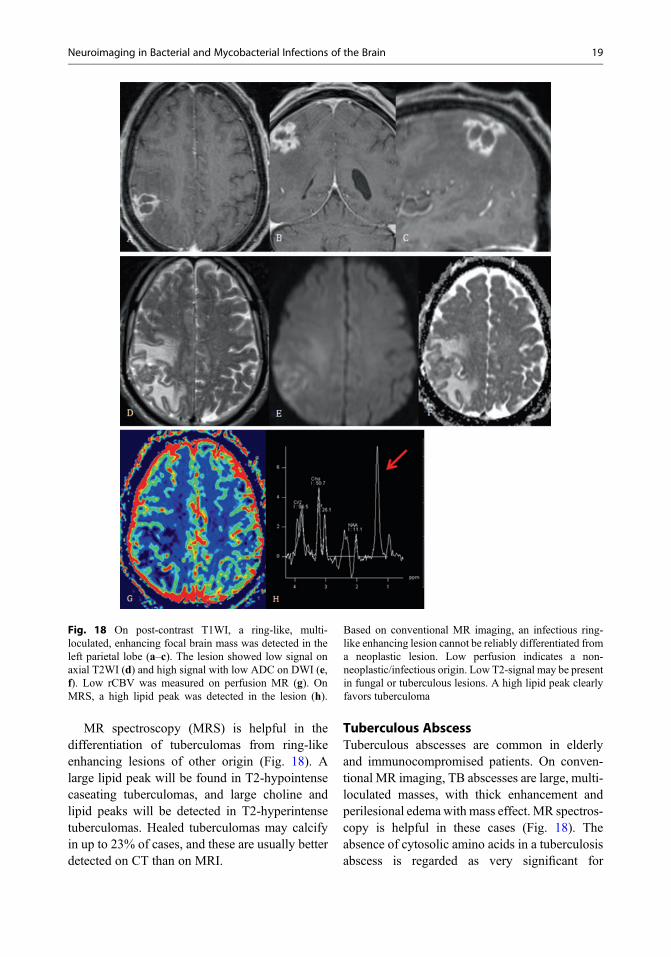
Fig. 18 On post-contrast T1WI, a ring-like, multi-loculated, enhancing focal brain mass was detected in theleft parietal lobe (a–c). The lesion showed low signal onaxial T2WI (d) and high signal with low ADC on DWI (e,f). Low rCBV was measured on perfusion MR (g). OnMRS, a high lipid peak was detected in the lesion (h).
Based on conventional MR imaging, an infectious ring-like enhancing lesion cannot be reliably differentiated froma neoplastic lesion. Low perfusion indicates a non-neoplastic/infectious origin. Low T2-signal may be presentin fungal or tuberculous lesions. A high lipid peak clearlyfavors tuberculoma
Neuroimaging in Bacterial and Mycobacterial Infections of the Brain 19
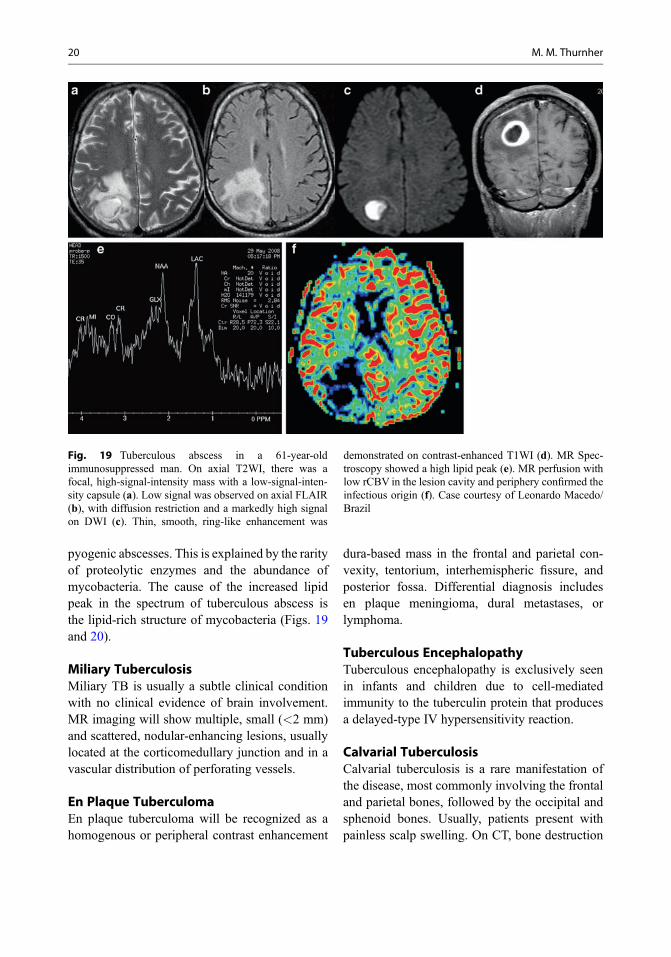
pyogenic abscesses. This is explained by the rarityof proteolytic enzymes and the abundance ofmycobacteria. The cause of the increased lipidpeak in the spectrum of tuberculous abscess isthe lipid-rich structure of mycobacteria (Figs. 19and 20).
Miliary TuberculosisMiliary TB is usually a subtle clinical conditionwith no clinical evidence of brain involvement.MR imaging will show multiple, small (<2 mm)and scattered, nodular-enhancing lesions, usuallylocated at the corticomedullary junction and in avascular distribution of perforating vessels.
En Plaque TuberculomaEn plaque tuberculoma will be recognized as ahomogenous or peripheral contrast enhancement
dura-based mass in the frontal and parietal con-vexity, tentorium, interhemispheric fissure, andposterior fossa. Differential diagnosis includesen plaque meningioma, dural metastases, orlymphoma.
Tuberculous EncephalopathyTuberculous encephalopathy is exclusively seenin infants and children due to cell-mediatedimmunity to the tuberculin protein that producesa delayed-type IV hypersensitivity reaction.
Calvarial TuberculosisCalvarial tuberculosis is a rare manifestation ofthe disease, most commonly involving the frontaland parietal bones, followed by the occipital andsphenoid bones. Usually, patients present withpainless scalp swelling. On CT, bone destruction
Fig. 19 Tuberculous abscess in a 61-year-oldimmunosuppressed man. On axial T2WI, there was afocal, high-signal-intensity mass with a low-signal-inten-sity capsule (a). Low signal was observed on axial FLAIR(b), with diffusion restriction and a markedly high signalon DWI (c). Thin, smooth, ring-like enhancement was
demonstrated on contrast-enhanced T1WI (d). MR Spec-troscopy showed a high lipid peak (e). MR perfusion withlow rCBV in the lesion cavity and periphery confirmed theinfectious origin (f). Case courtesy of Leonardo Macedo/Brazil
20 M. M. Thurnher
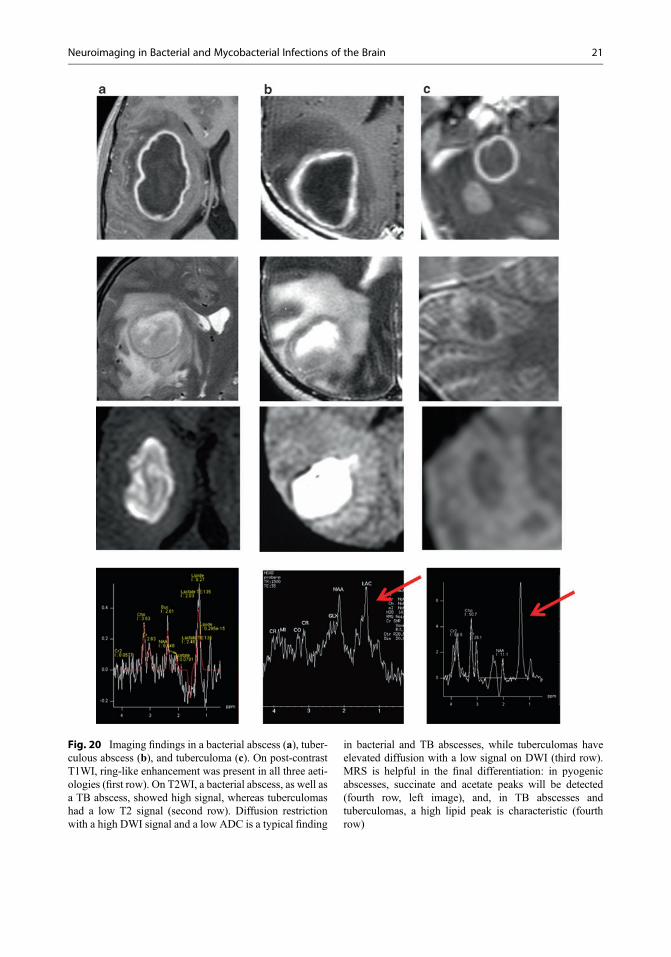
Fig. 20 Imaging findings in a bacterial abscess (a), tuber-culous abscess (b), and tuberculoma (c). On post-contrastT1WI, ring-like enhancement was present in all three aeti-ologies (first row). On T2WI, a bacterial abscess, as well asa TB abscess, showed high signal, whereas tuberculomashad a low T2 signal (second row). Diffusion restrictionwith a high DWI signal and a low ADC is a typical finding
in bacterial and TB abscesses, while tuberculomas haveelevated diffusion with a low signal on DWI (third row).MRS is helpful in the final differentiation: in pyogenicabscesses, succinate and acetate peaks will be detected(fourth row, left image), and, in TB abscesses andtuberculomas, a high lipid peak is characteristic (fourthrow)
Neuroimaging in Bacterial and Mycobacterial Infections of the Brain 21
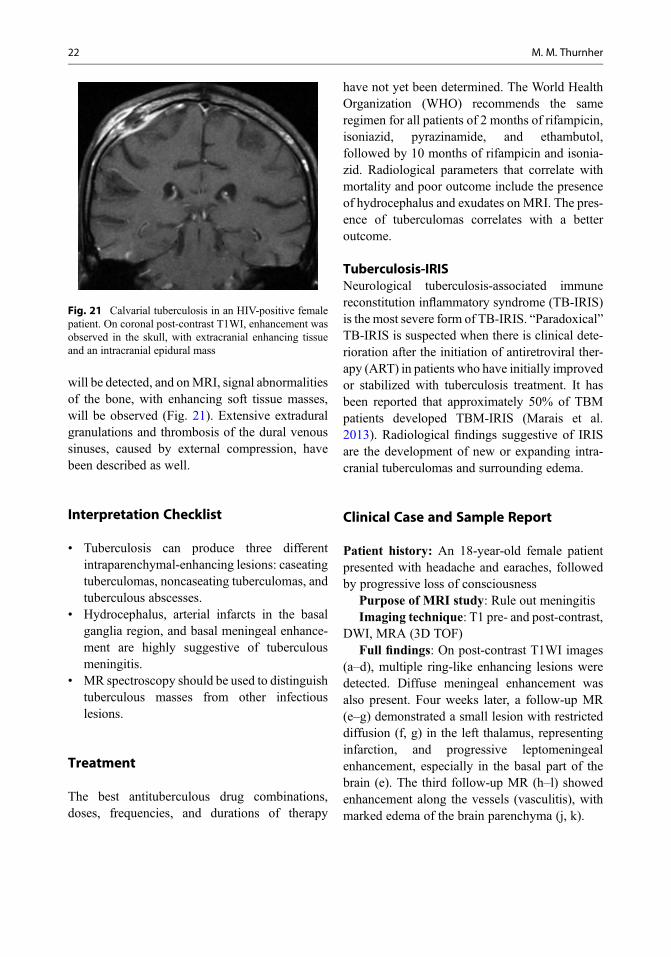
will be detected, and onMRI, signal abnormalitiesof the bone, with enhancing soft tissue masses,will be observed (Fig. 21). Extensive extraduralgranulations and thrombosis of the dural venoussinuses, caused by external compression, havebeen described as well.
Interpretation Checklist
• Tuberculosis can produce three differentintraparenchymal-enhancing lesions: caseatingtuberculomas, noncaseating tuberculomas, andtuberculous abscesses.
• Hydrocephalus, arterial infarcts in the basalganglia region, and basal meningeal enhance-ment are highly suggestive of tuberculousmeningitis.
• MR spectroscopy should be used to distinguishtuberculous masses from other infectiouslesions.
Treatment
The best antituberculous drug combinations,doses, frequencies, and durations of therapy
have not yet been determined. The World HealthOrganization (WHO) recommends the sameregimen for all patients of 2 months of rifampicin,isoniazid, pyrazinamide, and ethambutol,followed by 10 months of rifampicin and isonia-zid. Radiological parameters that correlate withmortality and poor outcome include the presenceof hydrocephalus and exudates on MRI. The pres-ence of tuberculomas correlates with a betteroutcome.
Tuberculosis-IRISNeurological tuberculosis-associated immunereconstitution inflammatory syndrome (TB-IRIS)is the most severe form of TB-IRIS. “Paradoxical”TB-IRIS is suspected when there is clinical dete-rioration after the initiation of antiretroviral ther-apy (ART) in patients who have initially improvedor stabilized with tuberculosis treatment. It hasbeen reported that approximately 50% of TBMpatients developed TBM-IRIS (Marais et al.2013). Radiological findings suggestive of IRISare the development of new or expanding intra-cranial tuberculomas and surrounding edema.
Clinical Case and Sample Report
Patient history: An 18-year-old female patientpresented with headache and earaches, followedby progressive loss of consciousness
Purpose of MRI study: Rule out meningitisImaging technique: T1 pre- and post-contrast,
DWI, MRA (3D TOF)Full findings: On post-contrast T1WI images
(a–d), multiple ring-like enhancing lesions weredetected. Diffuse meningeal enhancement wasalso present. Four weeks later, a follow-up MR(e–g) demonstrated a small lesion with restricteddiffusion (f, g) in the left thalamus, representinginfarction, and progressive leptomeningealenhancement, especially in the basal part of thebrain (e). The third follow-up MR (h–l) showedenhancement along the vessels (vasculitis), withmarked edema of the brain parenchyma (j, k).
Fig. 21 Calvarial tuberculosis in an HIV-positive femalepatient. On coronal post-contrast T1WI, enhancement wasobserved in the skull, with extracranial enhancing tissueand an intracranial epidural mass
22 M. M. Thurnher
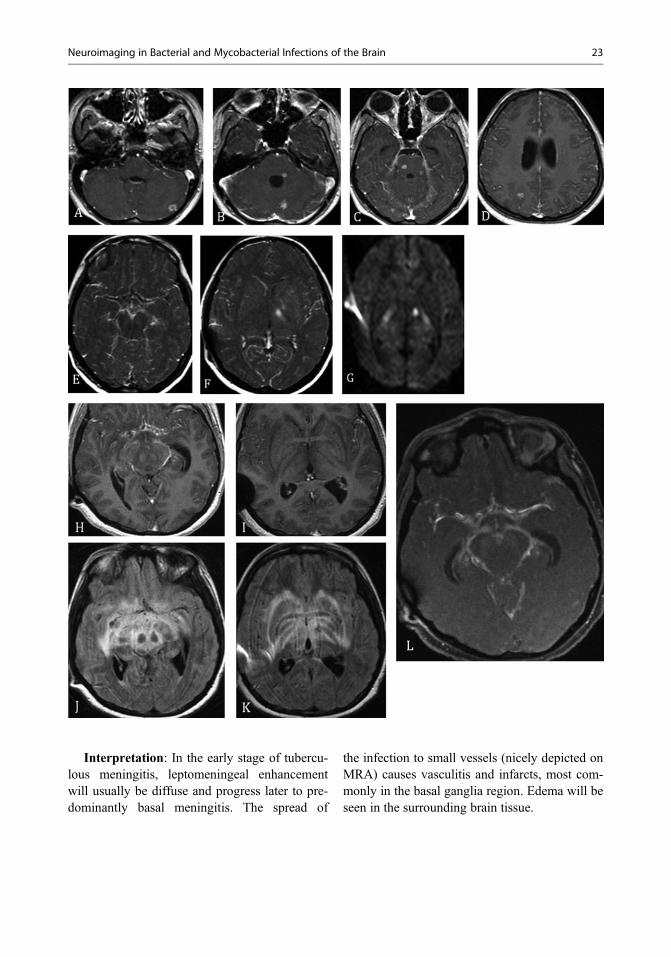
Interpretation: In the early stage of tubercu-lous meningitis, leptomeningeal enhancementwill usually be diffuse and progress later to pre-dominantly basal meningitis. The spread of
the infection to small vessels (nicely depicted onMRA) causes vasculitis and infarcts, most com-monly in the basal ganglia region. Edema will beseen in the surrounding brain tissue.
Neuroimaging in Bacterial and Mycobacterial Infections of the Brain 23

References
Chaudhary V, Bano S, Garga UC. Central nervous systemtuberculosis: an imaging perspective. Can AssocRadiol J. 2017;68(2):161–70.
Chiang IC, Hsieh TJ, Chiu M, et al. Distinction betweenpyogenic brain abscess and necrotic brain tumour using3-teslaMR spectroscopy, diffusion and perfusion imag-ing. Br J Radiol. 2009;82:813–20.
Fukui MB, Williams RL, Mudigonda S. CT and MRimaging features of pyogenic ventriculitis. AJNR AmJ Neuroradiol. 2001;22:1510–6.
Fukuoka H, Hirai T, Okuda T, et al. Comparison of theadded value of contrast-enhanced 3D fluid-attenuatedinversion recovery and magnetization-prepared rapidacquisition of gradient echo sequences in relation toconventional postcontrast T1-weighted images for theevaluation of leptomeningeal diseases at 3T. AJNR AmJ Neuroradiol. 2010;31:868–73.
Gupta RK, Prakash M, Mishra AM, et al. Role of diffusionweighted imaging in differentiation of intracranialtuberculoma and tuberculous abscess from cysticercusgranulomas-a report of more than 100 lesions. Eur JRadiol. 2005;55:384–92.
Kalita J, Singh RK, Misra UK, Kumar S. Evaluation ofcerebral arterial and venous system in tuberculousmeningitis. J Neuroradiol. 2018;45:130–135.
Lai PH, Li KT, Hsu SS, et al. Pyogenic brain abscess:findings from in vivo 1.5-T and 11.7-T in vitro protonMR spectroscopy. AJNR Am J Neuroradiol.2005;26:279–88.
Lai PH, Chang HC, Chuang TC, et al. Susceptibility-weighted imaging in patients with pyogenic brainabscesses at 1.5T: characteristics of the abscess cap-sule. AJNR Am J Neuroradiol. 2012;33(5):910–4.
Lummel N, Koch M, Klein M, et al. Spectrum and preva-lence of pathological intracranial magnetic resonance
imaging findings in acute bacterial meningitis. ClinNeuroradiol. 2016;26(2):159–67.
Marais S,Meintjes G, Pepper DJ, et al. Frequency, severity,and prediction of tuberculous meningitis immunereconstitution inflammatory syndrome. Clin InfectDis. 2013;56:450–60.
Plog BA, Nedergaard M. The glymphatic system in centralnervous system health and disease: past, present, andfuture. Annu Rev Pathol. 2018;13:379–94.
Toh CH, Wei KC, Chang CN, et al. Differentiation ofpyogenic brain abscesses from necrotic glioblastomaswith use of susceptibility-weighted imaging. Am JNeuroradiol AJNR. 2012;33:1534–8.
Further Reading
Batista RS, Gomes AP, Gazineo JLD, et al. Meningococcaldisease, a clinical and epidemiological review. AsianPac J Trop Med. 2017;10:1019–29.
Brouwer MC, Coutinho JM, van de Beek D. Clinical char-acteristics and outcome of brain abscess: systematicreview and meta-analysis. Neurology. 2014;82:806–13.
Jim KK, Brouwer MC, van der Ende A, van deBeek D. Subdural empyema in bacterial meningitis.Neurology. 2012;79(21):2133–9.
KimKS. Acute bacterial meningitis in infants and children.Lancet Infect Dis. 2010;10:32–42.
Lucas MJ, Brouwer MC, van de Beek D. Neurologicalsequelae of bacterial meningitis. J Inf Secur. 2016;73(1):18–27.
Tuberculosis. http://www.euro.who.intZumla A, Raviglione M, Hafner R, von Reyn
CF. Tuberculosis. N Engl J Med. 2013;368:745–55.Wilkinson RJ, Rohlwink U, Misra UK, et al. Tuberculous
meningitis. Nat Rev. Neurol. 2017;13(10):581–98.
24 M. M. Thurnher