neurocognitive issues among aging hiv positive adults
TRANSCRIPT
Neurocognitive Issues among Aging HIV Positive Adults
2nd APAAC Conference
June 1st-3rd, Hong Kong 2017
Edwina Wright
FRACP PhDThe Alfred Hospital, Burnet Institute, Monash University,
Peter Doherty Institute, Melbourne, Australia
Conflicts of Interest
• Gilead Sciences donated study drug for VicPrEP
• Receipt of unrestricted research funds– Gilead
– Abbott
– Janssen Cilag
– Boehringer Ingelheim
• Funding for consultancy work, lectures and developing educational resources that has been used for research purposes only – ViiV, Merck, Gilead, and Abbott

Overview
AIM
Review neurocognitive issues in ageing HIV+ adults
• Acute HIV infection
• START Neurology Substudy
• Factors that influence neurocognitive performance (NCP) in virologically suppressed populations, diagnosis and management
The effect of age highlighted where possible
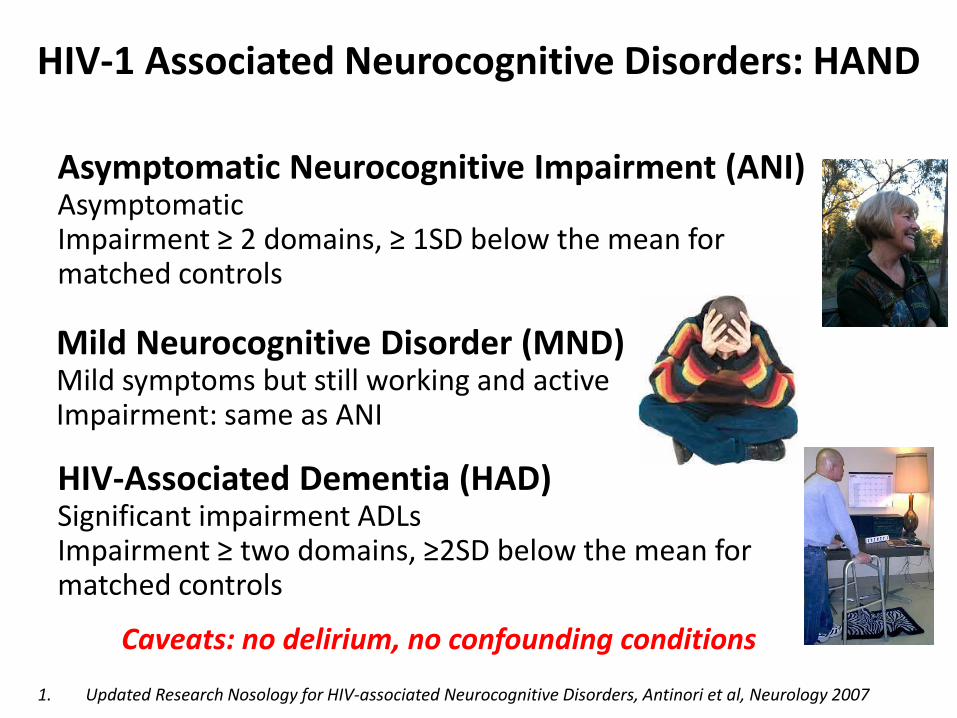
HIV-1 Associated Neurocognitive Disorders: HAND
1. Updated Research Nosology for HIV-associated Neurocognitive Disorders, Antinori et al, Neurology 2007
Mild Neurocognitive Disorder (MND)Mild symptoms but still working and activeImpairment: same as ANI
HIV-Associated Dementia (HAD)Significant impairment ADLsImpairment ≥ two domains, ≥2SD below the mean formatched controls
Asymptomatic Neurocognitive Impairment (ANI)Asymptomatic Impairment ≥ 2 domains, ≥ 1SD below the mean for matched controls
Caveats: no delirium, no confounding conditions

HAD: Synopsis
Pathogenesis
Navia et al, Ann Neurol 1986. www.goasiapacific.com. Gonzalez-Scarano et al, Nat Rev Immunol 2005. http://www.med.harvard.edu/AANLIB/ medcine,
plosjournals.org. Ferrando et al, AIDS 1998. Price et al, AIDS 1999. Cohen RA, AIDS 2001. Cysique et al, Arch Neurol 2004. Letendre et al, Annals Neurol 2004.
Letendre et al, Arch Neurol 2008. Cysique et al, Neurology 2009. Cysique, Waters, Brew. BMC Neurol 2011. Bell, Anthony, Simmons. Current HIV Research, 2006
www.emedicine.com/NEURO/topic447.htm ; www.pulitzer.org/.../ works/africa1.html Ellis et al. CID 2014
Treatment
Combination Antiretroviral
Therapy
Clinical
Diagnosis of
Exclusion
Caudate, Globus pallidus, Putamen
ScreeningIn practice, done for patients with cognitive complaints

Navia et al, Ann Neurol 1986. www.goasiapacific.com. Gonzalez-Scarano et al, Nat Rev Immunol 2005. http://www.med.harvard.edu/AANLIB/ medcine,
plosjournals.org. Ferrando et al, AIDS 1998. Price et al, AIDS 1999. Cohen RA, AIDS 2001. Cysique et al, Arch Neurol 2004. Letendre et al, Annals Neurol 2004.
Letendre et al, Arch Neurol 2008. Cysique et al, Neurology 2009. Cysique, Waters, Brew. BMC Neurol 2011. Bell, Anthony, Simmons. Current HIV Research, 2006www.emedicine.com/NEURO/topic447.htm ; www.pulitzer.org/.../ works/africa1.html
Caudate, Globus pallidus, Putamen
Treatment
CART vs no cART or mono/dual
therapy improves cognitive function
cART with 3 or more drugs with
effective CSF penetration appears
superior in patients with HAND
.
HAD: Synopsis
Clinical
Diagnosis of
Exclusion
Pathogenesis3
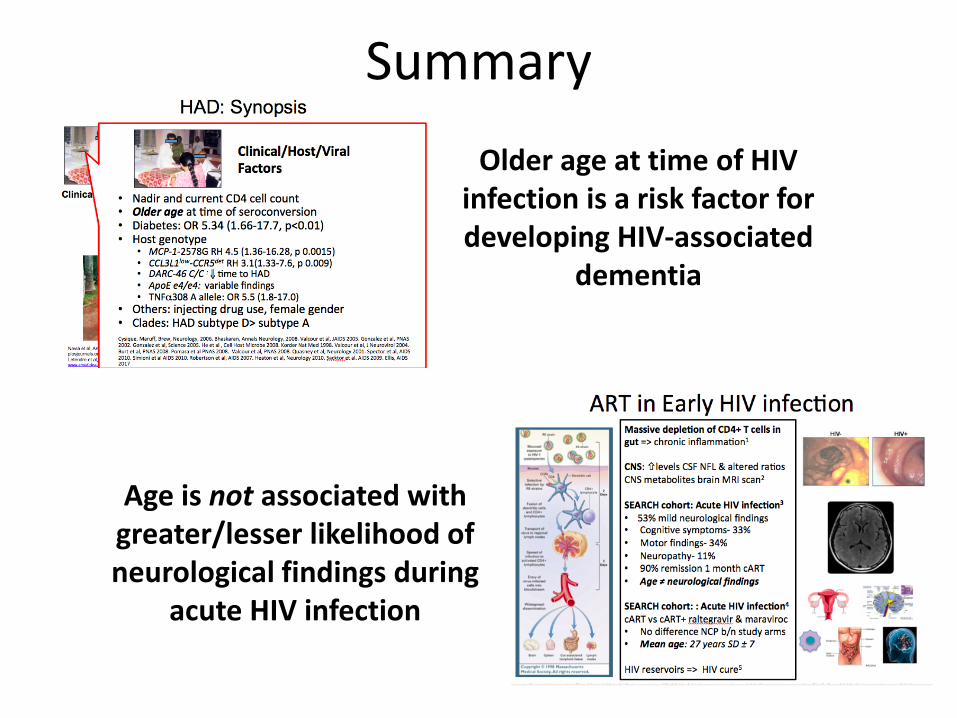
• Nadir and current CD4 cell count• Older age at time of seroconversion• Diabetes: OR 5.34 (1.66-17.7, p<0.01)• Host genotype
• MCP-1-2578G RH 4.5 (1.36-16.28, p 0.0015)• CCL3L1low-CCR5det RH 3.1(1.33-7.6, p 0.009) • DARC-46 C/C : time to HAD• ApoE e4/e4: variable findings• TNF308 A allele: OR 5.5 (1.8-17.0)
• Injecting drug use, female gender• HAD subtype D> subtype ACysique, Maruff, Brew, Neurology, 2006. Bhaskaran, Annals Neurology, 2008. Valcour et al, JAIDS 2005. Gonzalez et al, PNAS 2002. Gonzalez et al, Science 2005. He et al , Cell Host Microbe 2008. Korder Nat Med 1998. Valcour et al, J Neurovirol 2004. Burt et al, PNAS 2008. Pomara et al PNAS 2008. Valcour et al, PNAS 2008. Quasney et al, Neurology 2001. Spector et al, AIDS 2010. Simioni et al AIDS 2010. Robertson et al, AIDS 2007. Heaton et al, Neurology 2010. Sacktor et al. AIDS 2009. Ellis, AIDS 2017
Clinical/Host/Viral Factors
HAD: Synopsis
Navia et al, Ann Neurol 1986. www.goasiapacific.com. Gonzalez-Scarano et al, Nat Rev Immunol 2005. http://www.med.harvard.edu/AANLIB/ medcine,
plosjournals.org. Ferrando et al, AIDS 1998. Price et al, AIDS 1999. Cohen RA, AIDS 2001. Cysique et al, Arch Neurol 2004. Letendre et al, Annals Neurol 2004.
Letendre et al, Arch Neurol 2008. Cysique et al, Neurology 2009. Cysique, Waters, Brew. BMC Neurol 2011. Bell, Anthony, Simmons. Current HIV Research, 2006www.emedicine.com/NEURO/topic447.htm ; www.pulitzer.org/.../ works/africa1.html
HAD: Synopsis
Pathogenesis
Treatment
CART vs no cART or mono/dual
therapy improves cognitive function
cART with 3 or more drugs with
effective CSF penetration appears
superior in patients with HAND
.
Clinical
Diagnosis of
Exclusion
Caudate, Globus pallidus, Putamen
1. Cysique et al 2004. 2. Letendre et al, 2008. 3. Cysique et al, 2009.
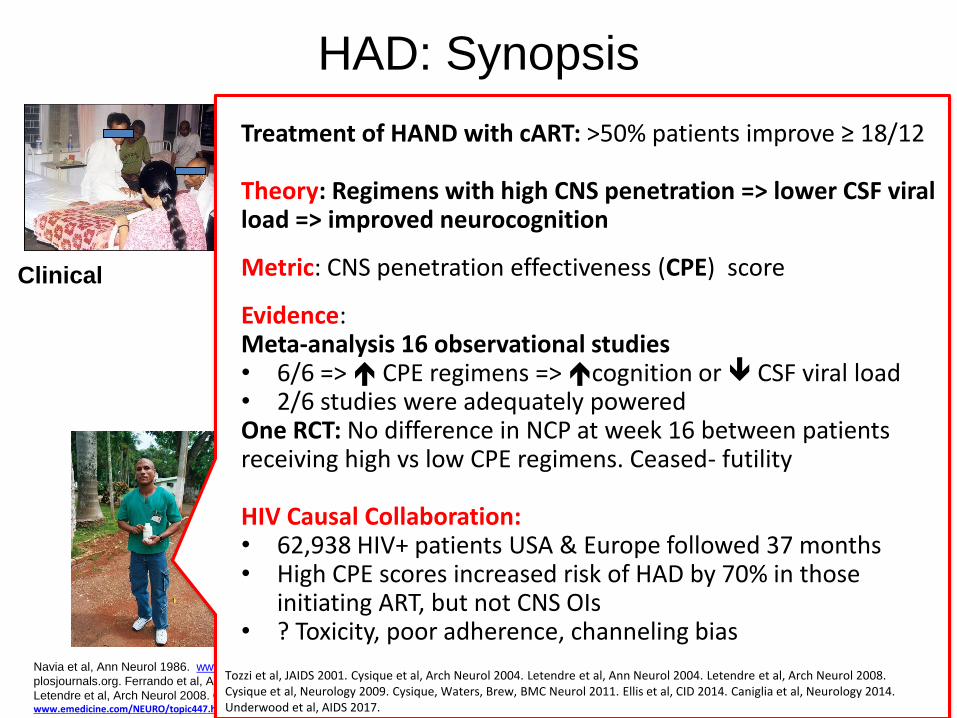
Treatment of HAND with cART: >50% patients improve ≥ 18/12
Theory: Regimens with high CNS penetration => lower CSF viral load => improved neurocognition
Metric: CNS penetration effectiveness (CPE) score
Evidence:Meta-analysis 16 observational studies• 6/6 => CPE regimens => cognition or CSF viral load • 2/6 studies were adequately poweredOne RCT: No difference in NCP at week 16 between patients receiving high vs low CPE regimens. Ceased- futility
HIV Causal Collaboration: • 62,938 HIV+ patients USA & Europe followed 37 months• High CPE scores increased risk of HAD by 70% in those
initiating ART, but not CNS OIs• ? Toxicity, poor adherence, channeling bias
Tozzi et al, JAIDS 2001. Cysique et al, Arch Neurol 2004. Letendre et al, Ann Neurol 2004. Letendre et al, Arch Neurol 2008. Cysique et al, Neurology 2009. Cysique, Waters, Brew, BMC Neurol 2011. Ellis et al, CID 2014. Caniglia et al, Neurology 2014. Underwood et al, AIDS 2017.
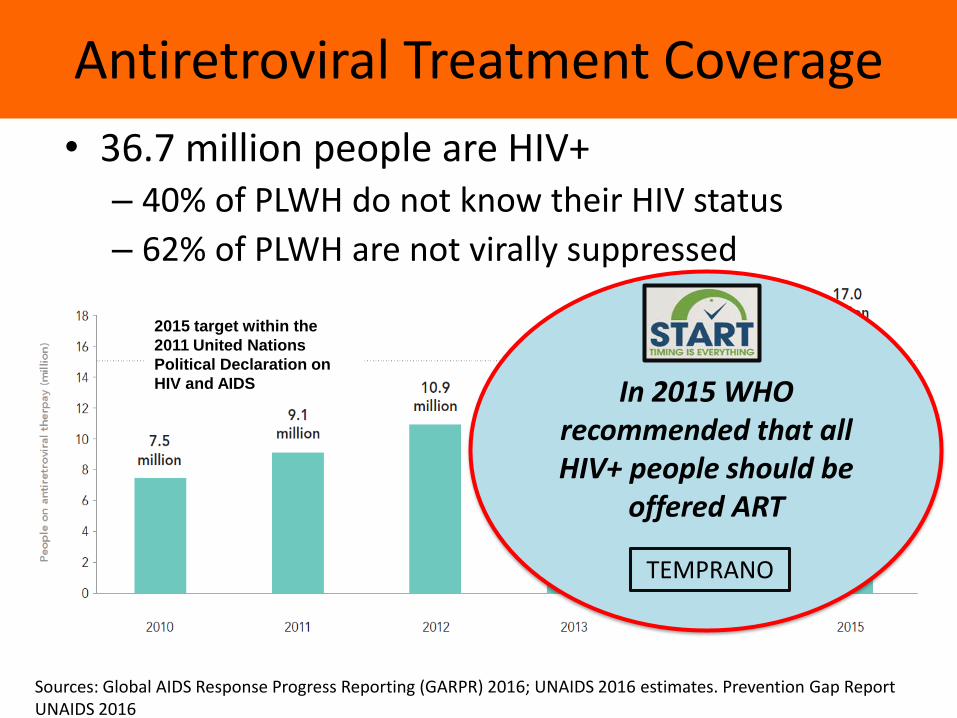
Sources: Global AIDS Response Progress Reporting (GARPR) 2016; UNAIDS 2016 estimates. Prevention Gap Report UNAIDS 2016
2015 target within the
2011 United Nations
Political Declaration on
HIV and AIDS
Antiretroviral Treatment Coverage
• 36.7 million people are HIV+– 40% of PLWH do not know their HIV status
– 62% of PLWH are not virally suppressed
In 2015 WHO recommended that all HIV+ people should be
offered ART
TEMPRANO
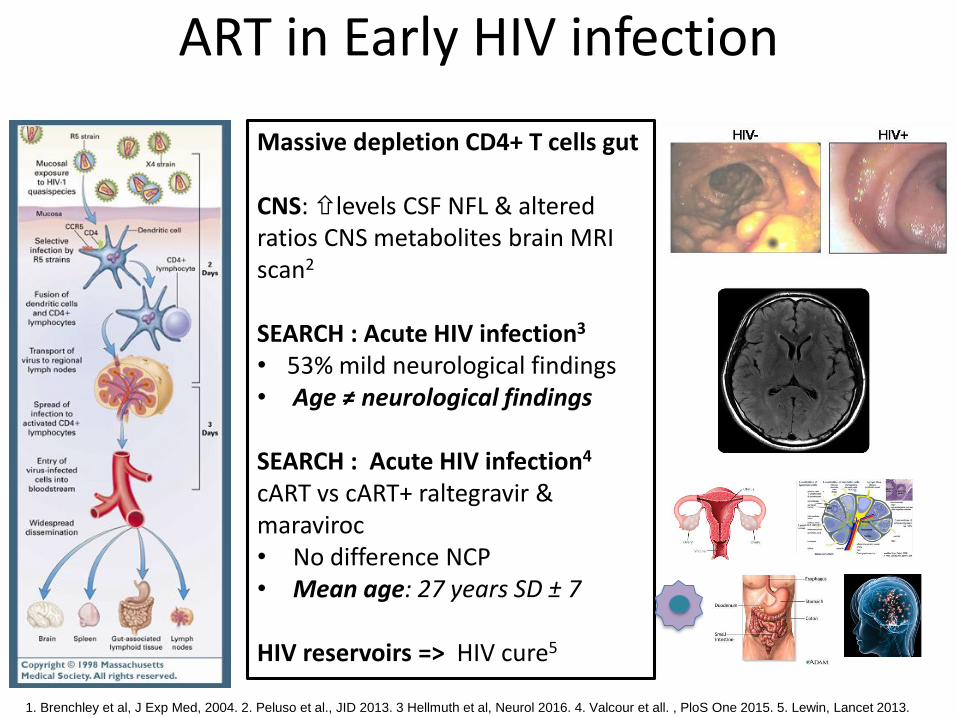
ART in Early HIV infection
Massive depletion CD4+ T cells gut
CNS: levels CSF NFL & altered ratios CNS metabolites brain MRI scan2
SEARCH : Acute HIV infection3
• 53% mild neurological findings• Age ≠ neurological findings
SEARCH : Acute HIV infection4
cART vs cART+ raltegravir & maraviroc• No difference NCP• Mean age: 27 years SD ± 7
HIV reservoirs => HIV cure5
1. Brenchley et al, J Exp Med, 2004. 2. Peluso et al., JID 2013. 3 Hellmuth et al, Neurol 2016. 4. Valcour et all. , PloS One 2015. 5. Lewin, Lancet 2013.

START Neurocognitive Substudy
HIV-infected, ARV naïve, CD4+ cell counts > 500 cells/mm3
Co-enrolled in START Study N=600
Early ART GroupN=300
Immediately initiate ART
Deferred ART GroupN=300
Defer ART until CD4+ <350 cells/mm3 or symptoms develop
START Funding: NIMH, NINDS and NHMRC

START
c(0, 1)
Change in QNPZ−8 score (Mean ± 2 SE)
●
●
●
●●
●
●
●
● Immediate ART
Deferred ART
0 4 8 12 24 36 48 60
Months from randomization
0.0
0.1
0.2
0.3
0.4
Ch
an
ge
in
QN
PZ
−8
fro
m b
aselin
e
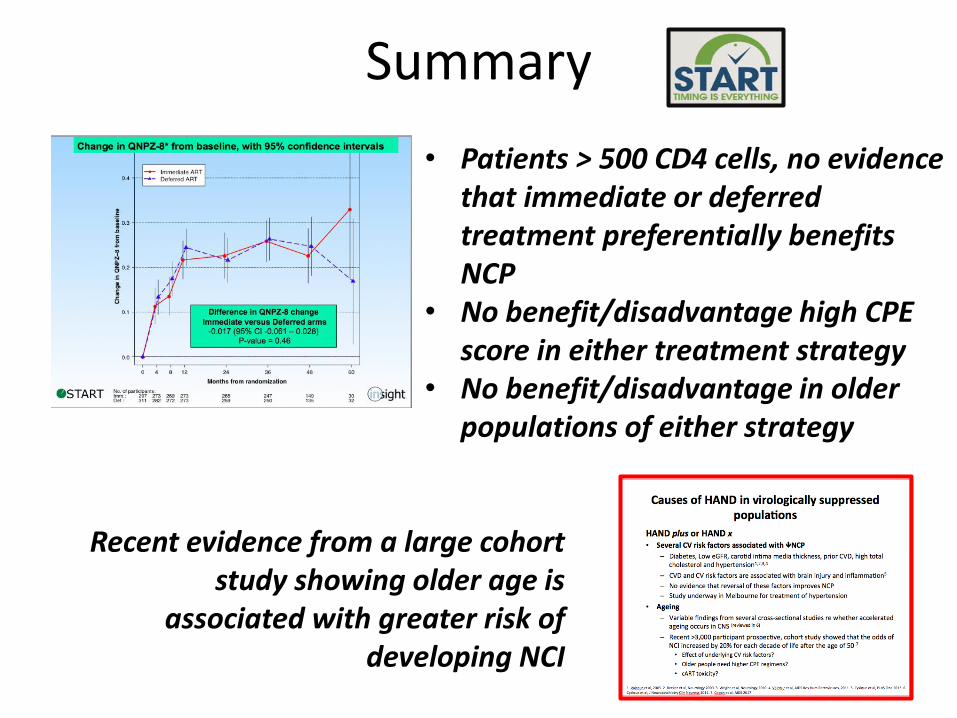
Figure. Change in QNPZ−8 from baseline, with 95% confidence intervals
No. of participants:Imm.:Def.:
297 273 269 273 265 247 149 30311 282 272 273 259 250 135 32
P−values, t−tests, unadj.:0.49 0.18 0.36 0.77 0.89 0.64 0.13
Longitudinal mixed model, adj. for baseline z−score and visit:Est. diff.: −0.01 95% CI: −0.05 − 0.04 P−value: 0.79
fig−qnpz8−chg.pdf File created= Data cutoff=
Difference in QNPZ-8 change
Immediate versus Deferred
arms
-0.017 (95% CI -0.061 – 0.028)
P-value = 0.46
Change in QNPZ-8 from baseline, 95% CIs

START
Findings START Neurology Substudy
1. ART deferral to <350 CD4+ cells is not associated with
poorer NCP over 3 years of follow-up in START
2. Immediate ART at > 500 CD4+ cells is not associated
with a cost in terms of poorer NCP (i.e. CNS toxicity)
3. No preferential benefit of either strategy for the NCP
of older people
1. Use of ART regimens with high CPE scores neither
benefitted, nor disadvantaged either treatment group
Wright et al. EACS 2015

HAND in HIV virologically suppressed populations
#Sydney 18%, n=116
*Prospective cohort study; #Cross-sectional study; ^ RCT
Cysique, Brew J Neurovirol, 2009;Sevignny et al, Neurol 2004; Heaton et al, Neurology 2010; Robertson et al, Neurology 2007; Simioni et al, AIDS 2010. Pumpradit et al, J Neurovirol 2010. http://www.bestbangkokdeals.com/ ; www.ville-geneve.ch/index.php?id=6675; 1001arabian.net/tourist/The%20Lights%20of%20S.
*NEAD Cohort: 21% n=203
#CHARTER Cohort: 30%, n=1,555
^ACTG longitudinal linked randomised trial (ALLRT) study, 26% baseline, n=1,160 patients
#Geneva 72%, n=200
#BK 37%, n=64
Age 48 Age 47
Age 42
Age 43
Age 44
Age 42
What proportion of your patients who are fully virologically suppressed may have HAND?
≈30%
AANI> MND>> HAD
HAND• Legacy effect?• Poor CNS HIV control?• Ongoing CNS parenchymal infection +/or
inflammation?HAND plus or HAND x• Cardiovascular risk factors?• Ageing?• cART toxicity?• Neurodegeneration?
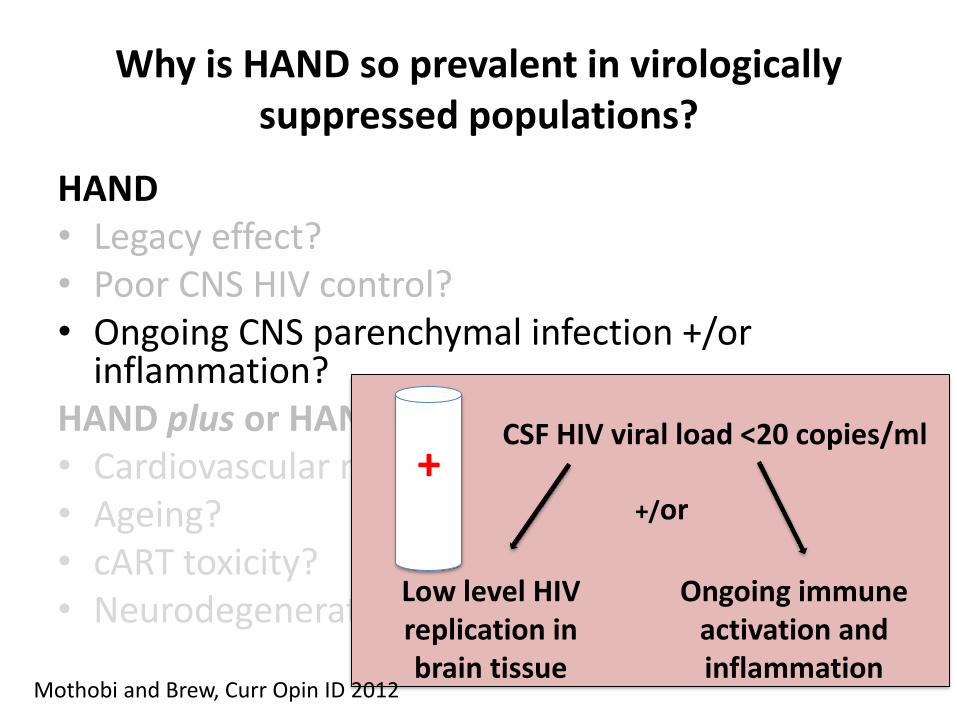
Why is HAND so prevalent in virologically suppressed populations?
Mothobi and Brew, Curr Opin ID 2012

HAND• Legacy effect?• Poor CNS HIV control?• Ongoing CNS parenchymal infection +/or
inflammation?HAND plus or HAND x• Cardiovascular risk factors?• Ageing?• cART toxicity?• Neurodegeneration?
Why is HAND so prevalent in virologically suppressed populations?
+ CSF HIV viral load >20 copies/ml
cART low CPE score HIV resistance
Mothobi and Brew, Curr Opin ID 2012
HAND• Legacy effect?• Poor CNS HIV control?• Ongoing CNS parenchymal infection +/or
inflammation?HAND plus or HAND x• Cardiovascular risk factors?• Ageing?• cART toxicity?• Neurodegeneration?
Why is HAND so prevalent in virologically suppressed populations?
+CSF HIV viral load <20 copies/ml
Low level HIV replication in brain tissue
+/or
Ongoing immune activation and inflammation
Mothobi and Brew, Curr Opin ID 2012
Causes of HAND in virologically suppressed populations: the evidence
• Legacy effect?– Can only determine by monitoring change over time
• Poor CNS HIV control?– Uncommon: ≈ 10% of patients on cART detectable CSF VL
• Ongoing CNS infection+/- inflammation?– Progression of HAND despite full CSF suppression
– Recent pilot studies ARV intensification with maraviroc or paroxetine and fluconazole showed improved NCP
Mothobi and Brew, Curr Opin ID, 2012. Robertson et al, AIDS 2007; Simioni et al, AIDS 2010; Canestri et al CID, 2010. Cysique et al, JAIDS 2005. Sevigny et al, Neurology 2004. Joseph et al, J Virus Erad 2016. Ndhlovu et al,. J Neurovirol 2014. Gates et al. AIDS 2016. Sacktor et al. CROI 2016

HAND• Legacy effect?• Poor CNS HIV control?• Ongoing CNS parenchymal infection +/or
inflammation?HAND plus or HAND x• Cardiovascular risk factors?• Ageing?• cART toxicity?• Neurodegeneration?
Why is HAND so prevalent in virologically suppressed populations?
Mothobi and Brew, Curr Opin ID 2012

Causes of HAND in virologically suppressed populations
1. Valcour et al, 2005. 2. Becker et al, Neurology 2009. 3. Wright et al, Neurology 2010. 4. Valcour et al, AIDS Res Hum Retroviruses, 2011. 5. Cysique et al, PLoS One 2013. 6. Cysique et al, J Neuropsychiatry Clin Neurosc 2011. 7. Coban et al, AIDS 2017
• Several CV risk factors associated with NCP
– Diabetes, low eGFR, carotid intima media thickness, prior CVD, BMI, high total cholesterol and hypertension1,2,3,4 => brain injury and inflammation5
– No evidence reversal of CV risk factor improves NCP, yet
• Ageing
– Variable findings re accelerated ageing in CNS6
– >3,000 participant cohort study: odds NCI 20% for each decade after age 50 years 7
• Effect of underlying CV risk factors?
• cART toxicity?

Causes of HAND in virologically suppressed populations
1. Underwood, Robertson & Winston, AIDS 20162. Vivithanaporn et al, AIDS 20173. Guinta et al, Mol Brain 20114. Marra et al, Neurology 20095. Ma et al, J Neurvirol 20166. Maddedu et al, AIDS 20127. Hoffman et al, HIV Medicine 20178. Gott et al, PLoS One, 20179. Coban et al, AIDS 2017
• cART toxicity
– Observed cell culture & animal models1, 2
– cART disrupts microglial phagocytosis of amyloid in brain and increase amyloid β generation by neurons3
– One RCT: CPE regimens may be CNS toxic4
– Efavirenz5, raltegravir6 and dolutegravir7 - CNS AEs/toxicity
– ARV duration: may play role1, but not seen in recent work8,9
1. Underwood, Robertson & Winston, AIDS 2016

Causes of HAND in virologically suppressed populations
• Neurodegeneration?
– Clinical, CSF, histopathological data suggesting that AD and PD may be more prevalent
– No evidence from neuropsychological testing that older HIV+ people perform more like HIV-people with Alzheimer’s disease
– Mostly cross-sectional studies
Tisch and Brew, Neurology 2009 . Brew, Crowe, Landay, Cysique , Guillemin, J Neuroimmune Pharmacol, 2008. Ciccarelli et al, Appl Neuropsychol Adult, 2016
Why is HAND so prevalent in virologically suppressed populations?
HAND• Legacy effect?• Poor CNS HIV control?• Ongoing CNS parenchymal infection+/or
inflammation?HAND plus or HAND x• Cardiovascular risk factors?• Ageing?• cART toxicity?• Neurodegeneration?
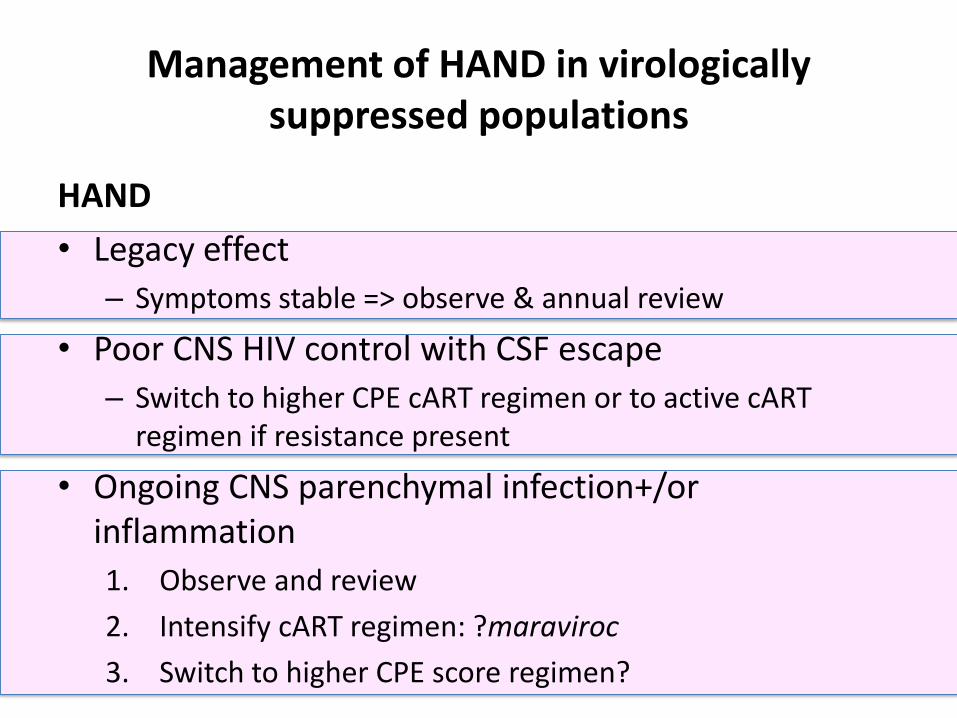
Management of HAND in virologically suppressed populations
HAND
• Legacy effect
– Symptoms stable => observe & annual review
• Poor CNS HIV control with CSF escape
– Switch to higher CPE cART regimen or to active cART regimen if resistance present
• Ongoing CNS parenchymal infection+/or inflammation
1. Observe and review
2. Intensify cART regimen: ?maraviroc
3. Switch to higher CPE score regimen?

Management of HAND in virologically suppressed populations
HAND plus or HAND x
• Cardiovascular risk factors?
– Optimise management of cardiovascular risk factors
• Ageing?
– Console your patients!
– Optimise exercise, diet, sleep, decrease alcohol use
• cART toxicity?– ? temporal relationship to new cART regimen? Chronic cART use?
• Neurodegeneration?– Believe your eyes despite patients’ youth and investigate accordingly
Monroe et al. HIV Med 2017
Summary
Age is not associated with greater/lesser likelihood of neurological findings during
acute HIV infection
Older age at time of HIV infection is a risk factor for developing HIV-associated
dementia
Summary
• Patients > 500 CD4 cells, no evidence that immediate or deferred treatment preferentially benefits NCP
• No benefit/disadvantage high CPE score in either treatment strategy
• No benefit/disadvantage in older populations of either strategy
Recent evidence from a large cohort study showing older age is
associated with greater risk of developing NCI

Summary
More studies• Impact of modifying CV risk factors• Intensifying cART regimens • ART toxicity • The impact of ageUpon neurocognitive performance of our ageing patients
ART CNS Toxicity• Suggested in US Causal Study, not
observed in START Neurology Substudy
• Some populations may be more vulnerable-? older/ those with CVD
• Duration and type of ART may be important

Acknowledgments
SMART and START Neurology substudy co-chairs and protocol teams
All Study Participants in SMART and START Neurology Substudies
Researchers whose work I have not included in this presentation
Thank you!!!
END