networks for hiv clinical care bhiva clinical audit sub-committee: j anderson, m backx, g brook, p...
TRANSCRIPT

Networks for HIV clinical care
BHIVA Clinical Audit Sub-Committee:J Anderson, M Backx, G Brook, P Bunting, C Carne, G Cairns, A De Ruiter, S Edwards, K Foster, A Freedman, P Gupta, M Johnson, M Lajeunesse, N Lomax, C O’Mahony, E Monteiro, E Ong, K Orton, A Rodger, C Sabin, E Street, I Vaughan, V Harindra,
R Weston, E Wilkins, D Wilson, M Yeomans.

• Background• Recap of in-patient snapshot audit• Networks survey
–Development of HIV clinical networks –Adherence to Standards for HIV Clinical Care –Clinically significant delays or failures–Conclusions and recommendations
Networks for HIV clinical care

Standards for HIV Clinical Care
Standards for HIV Clinical Care (March 2007) recommended:
1. Development of managed clinical networks comprising:– HIV units which provide outpatient care for the
majority of patients with uncomplicated infection– HIV centres - single-site or virtual/cluster - in each
network providing more specialised services including inpatient care, complex outpatient care, referral and advice services.

Standards for HIV Clinical Care, continued
2. Networks should develop referral protocols and patient pathways. – Patients who need inpatient care for OIs, HIV-related
tumours or other serious HIV disease should ordinarily be admitted to an HIV centre or tertiary service in liaison with the HIV centre
– Hepatitis B/C co-infection, lymphoma, KS, neurological or renal disease should usually be managed at HIV centre level.

Standards for HIV Clinical Care, continued
3. For national audit, HIV care providers should be able to:– Name the HIV clinical network of which they are a
member– Self-describe either as an outpatient HIV unit or as a
provider within an HIV centre– If an outpatient HIV unit, name one or more HIV
centre providers to which they would refer patients requiring complex care.

Description and aims of survey
• Networks survey conducted in November 2007-January 2008 to review implementation of Standards for HIV Clinical Care by:– Assessing current state of network development– Assessing adherence to recommended standards– Identifying issues and assessing satisfaction with care arrangements.
• Accompanied by “snapshot” audit of inpatients during week of 5-11 November 2007, for which results were presented at BHIVA Spring conference 2008.

Recap of inpatient “snapshot”
– 255 inpatients from 64 sites reviewed on one day during week of 5-11 November 2007.
– 190 (75%) diagnosed with HIV > 3 months before current admission.
– 120 (47%) on ART when admitted.– Of patients diagnosed > 3mths, but not on ART with
CD4<200, ART would probably have prevented the need for admission in at least 64% (27/42).

Distribution of patients by site
0
5
10
15
20
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Number of inpatients/day patients per site audited
Num
ber
of s
ites

Networks survey

Participation
– 106 sites responded.– 98 agreed to be un-blinded during analysis to
facilitate identification of network linkages.– Total reported caseload of participating sites
was at least 36,765 HIV patients, 71% of the UK SOPHID 2006 caseload.

Clinical network membership
– 60 (60%) sites were in 26 named or identifiable networks, including 2 in 2 networks
– 24 (23%) said they were in networks, but did not name the network or enough information to identify it
– 15 (14%) said they were not in networks, but other sites identified 2 of these as network members
– 6 (6%) were unsure– 1 (1%) did not answer.

Areas with named/identified networks

Self-described types of site
Sites classified themselves based on the types described in Standards for HIV Clinical Care:– 39 (37%) an HIV centre offering complex and inpatient
care– 49 (43%) outpatient HIV unit– 20 (19%) neither description fits– 2 (2%) did not answer.

Self-described types of site by region
0 2 4 6 8 10 12
East Midlands
East of England
London
North East
North West
Scotland
South Central
South East Coast
South West
Wales
West Midlands
Yorks & Humberside
Number of sites
HIV Centre

Self-described types of site by region
0 2 4 6 8 10 12
East Midlands
East of England
London
North East
North West
Scotland
South Central
South East Coast
South West
Wales
West Midlands
Yorks & Humberside
Number of sites
Outpatient HIV unitHIV Centre

Self-described types of site by region
0 2 4 6 8 10 12
East Midlands
East of England
London
North East
North West
Scotland
South Central
South East Coast
South West
Wales
West Midlands
Yorks & Humberside
Number of sites
NeitherOutpatient HIV unitHIV Centre

Caseload by self-described type of site
0
4
8
12
16
20
1-50 51-100 101-200 201-500 501-1000 >1000
HIV caseload
Num
ber
of s
ites
HIV CentreOutpatient HIV unitNeither
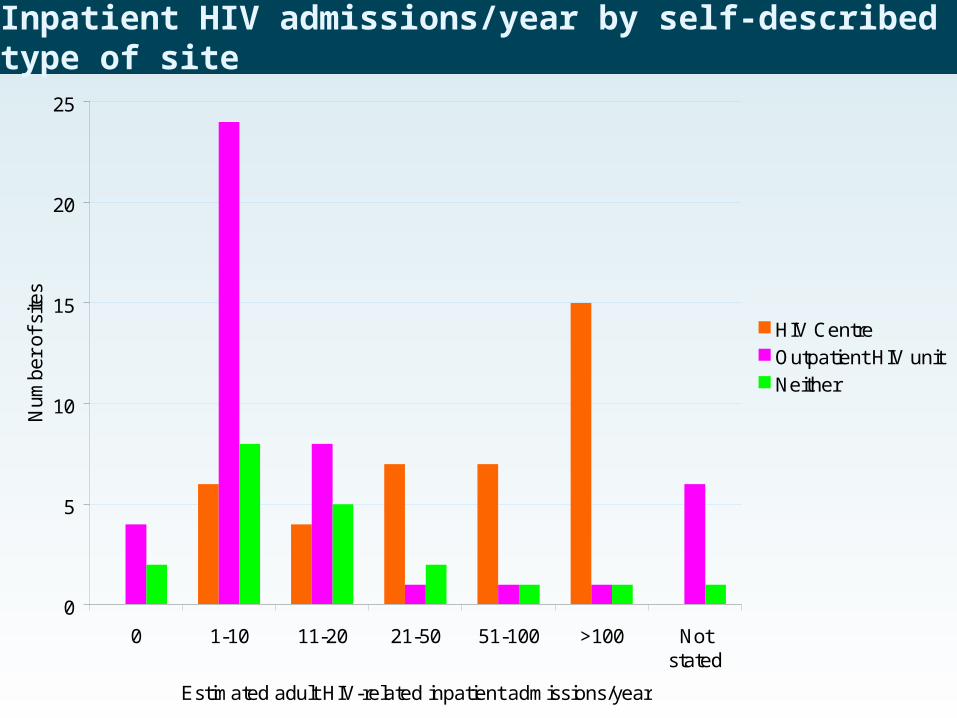
Inpatient HIV admissions/year by self-described type of site
0
5
10
15
20
25
0 1-10 11-20 21-50 51-100 >100 Notstated
Estimated adult HIV-related inpatient admissions/year
Num
ber
of s
ites
HIV CentreOutpatient HIV unitNeither

Whether provided specialist HIV advice to colleagues at other sites
HIV centre Outpatient HIV unit
Yes, 24/7 30 (76.9%) 8 (17.8%)
Yes, not 24/7 4 (10.3%) 12 (26.7%)
No 5 (12.8%) 25 (55.6%)
Total 39 (100%) 45 (100%)
Standards for HIV Clinical Care states: There must be network-wide arrangements for 24-hour on-call/referral advice, provided via the HIV centre.

Whether sites received referrals for more specialised aspects of HIV care
HIV centre Outpatient HIV unit
Inpatient referrals 22 (56.4%) 1 (2.2%)
Outpatient referrals 24 (61.5%) 6 (13.3%)
Neither 12 (30.8%) 38 (84.4%)
Total 39 (100%) 45 (100%)
Receiving referrals for more specialised aspects of care is one of the main roles of HIV centres under Standards for HIV Clinical Care.

Whether day case/ambulatory care facilities available
HIV centreOutpatient HIV unit
Yes, good 23 (59.0%) 8 (17.8%)
Yes, but unsatisfactory
9 (23.1%) 5 (11.1%)
No 7 (17.9%) 30 (66.7%)
Total 39 (100%) 45 (100%)
Standards for HIV Clinical Care states: Day case/ambulatory facilities should be available in HIV centres.
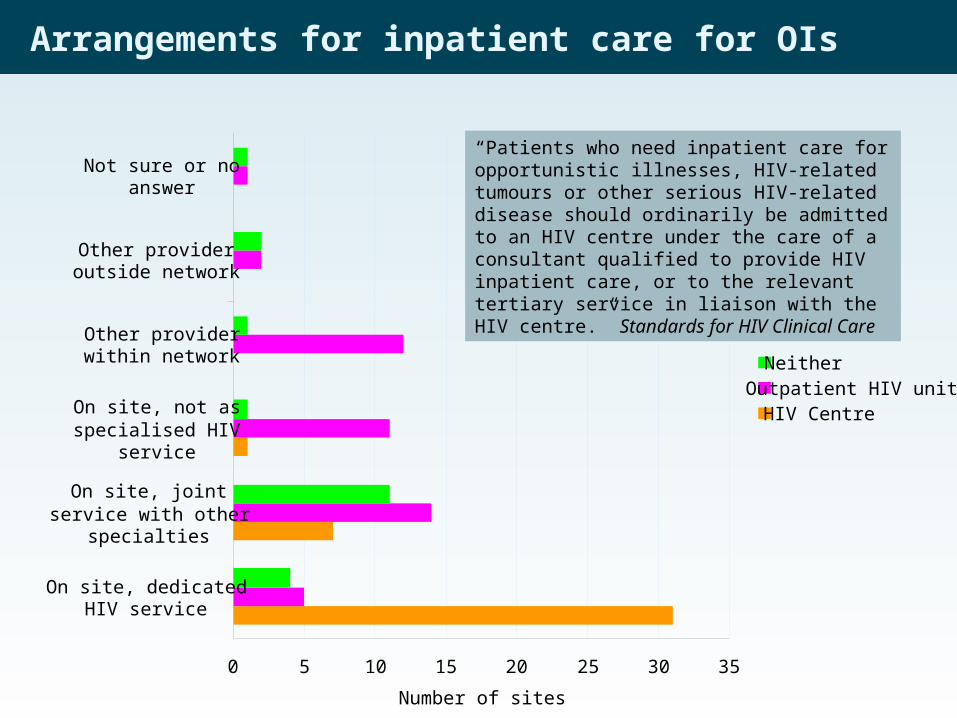
Arrangements for inpatient care for OIs
0 5 10 15 20 25 30 35
On site, dedicatedHIV service
On site, jointservice with other
specialties
On site, not asspecialised HIV
service
Other providerwithin network
Other provideroutside network
Not sure or noanswer
Number of sites
NeitherOutpatient HIV unitHIV Centre
“Patients who need inpatient care for opportunistic illnesses, HIV-related tumours or other serious HIV-related disease should ordinarily be admitted to an HIV centre under the care of a consultant qualified to provide HIV inpatient care, or to the relevant tertiary service in liaison with the HIV centre.” Standards for HIV Clinical Care

Hepatology Respiratory medicine Negative pressurefacilities
Oncology Neurology/neurosurgery
Hepatology Respiratory medicine Negative pressurefacilities
Oncology Neurology/neurosurgery
Arrangements for key specialist services
Outpatient HIV units
HIV centres
0%
20%
40%
60%
80%
100%
0%
20%
40%
60%
80%
100%
■ at this hospital; ■ referred within network; ■ referred outside network.

Out of network referrals
Referral (%) outside sites own network for specific services
15-25% 10-15% 5-10% 0-5% None
HIV resistance interpretation
Bone marrow transplantation
Oncology
Paediatric HIV care
Neurology/ neurosurgery
Liaison psychiatry/ mental health
Negative pressure facilities
Dentistry
Hepatology
Renal medicine
Clinical psychology
Neonatal care
Ophthalmology
Palliative care
Specialist HIV pharmacy
Haematology
Otorhinolaryngology
Social care
Respiratory Medicine
Gastroenterology
Dermatology
Lipid/cardiovascular medicine
Endocrinology
Full imaging/pathology
Dietetics
Physiotherapy
Occupational therapy
Obstetrics
GUM
Assessment of adherence to standards
• Only 15 of 39 sites self-describing as HIV centres broadly met the criteria in Standards for HIV Clinical Care, 6 had the potential to do so, 6 clearly did not.
• Many sites self-describing as outpatient HIV units undertook planned inpatient work and/or other complex aspects of care. Some of these appeared well-supported by network arrangements, but at least 13 did not.
• This is consistent with the inpatient snapshot audit in which 37 sites submitted only 1-2 inpatients each, and reflects planned management of inpatients at sites with small caseloads.

Clinically significant delays or failures
Reported delays or failures within 12 months
N (%)
Testing for and diagnosing HIV infection
79 (75%)
Informing clinician of patient's admission
30 (28%)
Transferring inpatients from local hospital to a specialised HIV centre
20 (19%)
Discharging back from a specialised HIV centre to the referring unit
10 (9%)
Discharging to supported care in the community.
22 (21%)

Examples of delays or failures
– Peripheral hospitals persevered with care for too long before transfer to HIV in-patient centre. Patients only referred when management of the patient becomes difficult or condition deteriorates requiring a more problematic transfer.
– Delays in transferring patients to network neurology/ neurosurgery centres
– Four cases of AIDS defining illnesses on ITU not diagnosed until the patients critically ill.

Satisfaction with care arrangements
Very satisfied
Broadly satisfied
Neutral Dissatisfied
Working of clinical networks
27 (26%) 47 (44%) 28 (26%) 4 (4%)
Patient pathways and referral arrangements
20 (19%) 52 (49%) 30 (28%) 4 (4%)
Overall care arrangements
28 (26%) 61 (58%) 16 (15%) 1 (1%)

Conclusions
• Most sites are in networks, but the development of these networks has not yet reached the level envisaged in Standards for HIV Clinical Care.
• Networks exist, but appear informal and likely succeed due to interest and commitment of individuals
• Need structures and a systematic approach to providing co-ordinated care.
• However, the survey took place only 6-9 months after publication of the Standards and these structures may now be evolving.

– Not all sites self-describing as HIV centres receive referrals, provide 24/7 advice, have day/ambulatory care facilities and/or offer a full range of key related specialties.
– Most sites self-describing as outpatient HIV units undertake inpatient HIV work or other complex aspects of care on site.
– While most inpatients are in larger HIV centres, many sites provide inpatient and complex aspects of care for small numbers of patients. This raises issues for governance, risk, training and cost-effectiveness.
Conclusions, continued

Conclusions, continued
• Clinically significant delays or failures remain widespread, especially relating to HIV diagnosis but also transfer of complicated patients to HIV centres.
• Problems associated with tertiary referral/transfer and step-down less common - may reflect the low level of such referrals.
• Respondents were mostly satisfied with existing arrangements.

• HIV clinicians should take the lead in developing networks in line with standards and appropriate to local circumstances
• Networks should provide a forum to influence commissioning of HIV services and set priorities for development and investment
Recommendations for Clinicians

• Commissioners should expect the services they commission to describe their network arrangements and patient pathways
• Commissioners should collaborate in planning HIV services across geographical boundaries and multiple providers/networks to make best use of resources and expertise
Recommendations for Commissioners