neck and shoulder
TRANSCRIPT
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 1/42
Neck and Shoulder
withAngie Dubis

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 2/42
What Is Fascia?
Connective tissue cells secrete a number of substances into the space around themselves. Theyalso secrete what is commonly called “ground substance”. Those connective tissue cellsecretions (primarily collagen, retinacular fibers, elastin fibers and the ground substance) cancombine with cellular components to form a variety of connective tissue structures, such ascartilage, bone, tendon, blood, adipose tissue, lymphatic tissue and fascia.
The combination of connective tissue secretions are often collectively referred to as TheExtracellular Matrix (ECM) - you may also hear it called ‘The Living Matrix’ or the ‘ConnectiveTissue Fabric’. Regardless of name, almost every cell in the human body is imbedded in thispervasive matrix that, among other things, provides a supportive framework for cells to anchorto and move around on, separates tissues from one another, nourishes cells by providing amechanism for the diffusion of nutrients and that regulates intercellular communication.
The Connective tissue properties are determined by the local components of the ExtracellularMatrix. In the case of Fascia, elastin and collagen fibers are secreted into the ECM along withground substance by the connective tissue’s cellular components (fibroblasts, mas t cells,adipose cells, macrophages, plasma cells, and leukocytes) to form this ever pervasive network.
This fascia network weaves its way through the body in every direction without interruption. Itsurrounds the cells of every nerve, blood vessel, organ, muscle and bone. An injury in one partof this dynamic web affects all other parts, which is why a client can have a resistanthyperextension in the upper cervical muscles as a result of a constricted planar fascia!
The Body Talks
Often when people think of communication systems of the body they think of nerve impulsesand chemical pathways not energy waves, oscillations and vibrations. Somehow, when used byphysicists the word “energy” is understood as science (as in E=MC²), but when used inreference to life force it can become something esoteric and mysterious. This has been partlydue to the lack of empirical evidence available on the subject. Until recently, cellular researchhas focused on the liquid portion of the cell. Scientists have used techniques to separate the
fluid matter from cells, throwing out the solid matter as unimportant.As it turns out, this solid matter is made up of some of the same insoluble structural proteins asfascia (elastin and collagen with some actin, myosin and keratin). Like the connective tissue, thesolid matter’s importance is just now beginning to be recognized. These insoluble structuralproteins form the internal structure and framework of every cell (cytoskeleton) and some of

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 3/42
these vital proteins extend across the cellular membrane to anchor the cell to the extracellularmatrix/connective tissues.
Isn’t it fascinating that the cell’s cytoskeleton, the extracellular matrix and the connectivetissues (collectively referred to by James Oschman as The Living Matrix) are all made of the
same substances, are all anchored together in one continuous fabric and have all beenconsistently ignored as unimportant by almost every discipline that studies the body?
As the importance and continuity of these structural components have come to light, researchhas begun to demonstrate that the nervous, hormonal and chemical systems only account for aportion of the communications occurring in the body. The Living Matrix is the ONLY systemthat connects to every cell in the body. It is an all pervasive communication network thatconducts energy and information at speeds so fast it makes nerve impulses look like they arerunning on dialup. Energy and information, including physical and emotional trauma, can also
be processed and stored within the matrix.
Healing occurs at a cellular level. If the flow of energy in the living matrix is disrupted it cancause breakdowns decreasing the ability of the system to communicate and coordinateimmune defenses and repair processes. Whether an injury is a gaping wound or a paper cut,the repair process is completed by the connective tissues and individual cells. The connectivetissue fabric summons the cells needed for healing by sending a variety of potential signalsthrough the matrix and the needed cells begin migrating to the injured tissues. Much of thiscell migration takes place as cells break existing connections and make new ones along theconnective tissue fabric – in essence the cells use the living matrix’s structural scaf folding tocrawl to the injury.
In my opinion, understanding how cells of the connective tissue fabric store energy, processtrauma and communicate with each other through vibrations, oscillations and waves (amongother things) can have a tremendous impact on the quality of care health practitioners offerclients.
What Does the Heart Have To Do with It?
In the book "The Little Prince," by Antoine de Saint-Exupéry, the Fox says to the little prince."And now here is my secret, a very simple secret: it is only with the heart that one can seerightly; what is essential is invisible to the eye." The meaning of this quote is very powerful -with the eyes one can see wealth, beauty and fame, but with the heart one can feel andperhaps even understand love, loyalty, friendship and truth.
If the heart is simply a pump, how can it help us feel or understand love? Researchers likethose at the Institute of HeartMath are working to answer this and other questions, such as,

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 4/42
how the heart communicates with the brain and how it influences information processing,perceptions, emotions and health. This research has established that the heart functions as aninformation processing center that is hardwired for bidirectional communication with the brain.Interestingly enough, the neural connections going from the heart to the brain outnumber the
connections coming from the brain to the heart. Additionally, many of the connections fromthe heart terminate in key brain centers that affect perception and autonomic response such asthe thalamus, hypothalamus, and amygdala.
Other than acting as an information processing center, the heart is also an endocrine gland,which has cells that produce and release the neurotransmitters norepinephrine and dopamine,as well as the hormone oxytocin. Oxytocin is sometimes referred to as the "love hormone"because recent research indicates that this hormone is involved in cognition, tolerance,adaptation, social recognition, pair bonding and maternal behaviors. Fascinatingly enough, theconcentrations of oxytocin found in the heart are greater than those found in the brain.
Besides neural and chemical communication, it has been found that each time the heart beats apulse of electricity flows from the heart through the circulatory system. As a result of thiselectric current, a magnetic field is created in the surrounding space that has been measured upto 15 feet away from the body. Have you had an experience where you walked into a room andimmediately sensed that something was wrong? Perhaps, it was your heart’s magnetic fieldthat turned your brain on to the disharmony in the environment. The rhythm of the heart beatitself varies based on emotional state – specifically negative emotions can result in heartrhythms that are erratic and disorganized, while positive emotions tend to increase harmony
and coherence in the heart rhythms.
The Liquid Body
Water molecules surround the genetic material in DNA in a way that directly influences itsstructure. The DNA double Helix is entirely covered by water molecules. These watermolecules in combination with ions actually hold the DNA together. Every molecule in the bodyis framed by water and ions. If you removed the water from this framework all of the moleculesin your body would be pushed apart rapidly. Water actually neutralizes the electrical charges ofthe atoms that make up the molecules.
Water doesn’t just hold your body’s atoms togethe r; it lubricates them and creates a cushion toprotect your tissues from shock - it allows force to be distributed across the system. Water actsas a transportation network that delivers vitamins, minerals and other essential elements to thebody’s tissues and organs. It also provides the pathway for the removal of waste products, suchas metabolites and toxins.

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 5/42
When collagen fibers become dehydrated they elicit an acute inflammatory response resultingin the release of histamine, dopamine and other chemical mediators which result in increasedfascial tension. If the dehydration is persistent this could lead to excessive bonding of collagenfibers, scar tissue formation and adhesions in the fascial net. As a result of this process the
tissue loses its ability to move freely, elasticity is lost and the ground substance begins todiminish.
Since the fascia is primarily collagen fibers and ground substance, dehydration can have aprofound effect on cellular activities within the fascia. Since fascia provides the communicationpathways for the nervous, circulatory and immune systems, dehydration can affect the body’sability to transfer and convey messages. Luckily, some of these negative consequences ofdehydration can be counteracted by rehydrating and performing active range of motionexercises – for individuals with chronic dehydration further steps may be needed. Conveyingthis information to clients may help them understand why water is so important. Everyone
knows that should stay hydrated, they just don’t always understand the profound effects of notdoing it.
Flow
Where there is congestion, FLOW cannot exist. Although not impossible, it is difficult to feel atease when things are stuck. Nasal congestion can make you feel like your head is going toexplode, traffic congestion can frustrate even the calmest of us, mental congestion can paralyzeour decision making processes to the point of complete self-destruction and bodily congestionscause pain, restricted movement (of both body and internal processes) and diseases such asatherosclerosis and cancer .
Flow or “being in the zone” on the other hand can result in feeling a sense of openness,freedom, peace, joy, elation and ZEN. Perhaps you have experienced periods of flow. When “inthe flow” the road opens up before you, obstacles magically disappear, concentr ation iseffortless, tasks seem to complete themselves, time stands still, and all other sensationsdisappear from perception as the material body seems to become one with the energy of theworld around it. Experiences of “flow” can be described as moment s of true inspiration,connectedness and complete ease.
I would say that the vast majority of people who end up on a massage therapist’s table arethere because they are experiencing some sort of congestion in their minds or bodies. Thecomplaints may be minor or more severe. Their congestion or dis-ease (lack of ease) maymanifest as chronic pain, edema, restricted range of motion, digestive problems orhypertension. It is our job as therapists to try to help clients move from a state of dis-ease toone of ease by using a variety of techniques to help release these congestions caused by

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 6/42
fibromyalgia, trauma, postural distortions, long hours of sitting and stress among other things,but how do we help clients “tune in” to the flow? Unfortunately, flow canno t be created; it canonly be experienced by letting go.
So the question becomes how can a therapist facilitate clients in letting go of the congestion
that is restricting their ability to flow? Of course, there isn’t one answer to this question. Eachclient has their own unique relationship with their body.
We are going to start by trying to bring awareness to what that relationship looks like. Forexample, I frequently find that clients, especially those with chronic pain, have unconsciouslygrown to re sent their bodies for “betraying” them. After all that “damn leg” (arm/shoulder/hip) has restricted their ability to do the things they want to do. As a result, the client has oftenunknowingly anchored in the congestion/pain/injury by putting the injured area on thedefensive.
Realizing that it matters how they speak to or about their body may seem like a foreign conceptto some clients so we can explain it like this:
“Each cell in your body is a living being. You can remove it from your body, plac e it in apetri dish and it can continue to grow and live. That being said you probably alreadyknow that your body talks to itself. It tells itself where to send blood and nutrients;when it is time to eat, sleep and excrete; and it communicates with itself to producehealing. So each cell has its own life and its life is dedicated to helping you not onlysurvive, but to thrive and adapt to all the challenges you face. When the cell needs help
it asks for it and if that need isn’t met it will scream fo r it – you may experience this asdiscomfort, pain or eventually disease.”
After the point has been made we will ask the client:
“Have you ever had a friend come to you hurting and in need of your advice orsupport?”
Typically they respond “yes”. If so, ask them:
“How would that person feel if you yelled at them or berated them?”
Often the response to this question is “I would never do that!” An appropriate reply would be:
“I wouldn’t think you would, but do you do it to your body? Isn’t your leg yo ur friend?Hasn’t it taken you places and supported you? Isn’t it asking for your help? How do youthink it feels when you yell at it? Do you think it helps it heal? ”
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 7/42
This very simple conversation can have profound effects on how a client perceives theirrelationship with their body. It can help them release frustrations they have been harboring andit opens the door to flow. Start listening to the language your clients use in regard to theirbodies to see if there are opportunities to foster flow by releasing pent up resentments and
frustrations that may be attributing to an inability to let go of congestion.
Posture
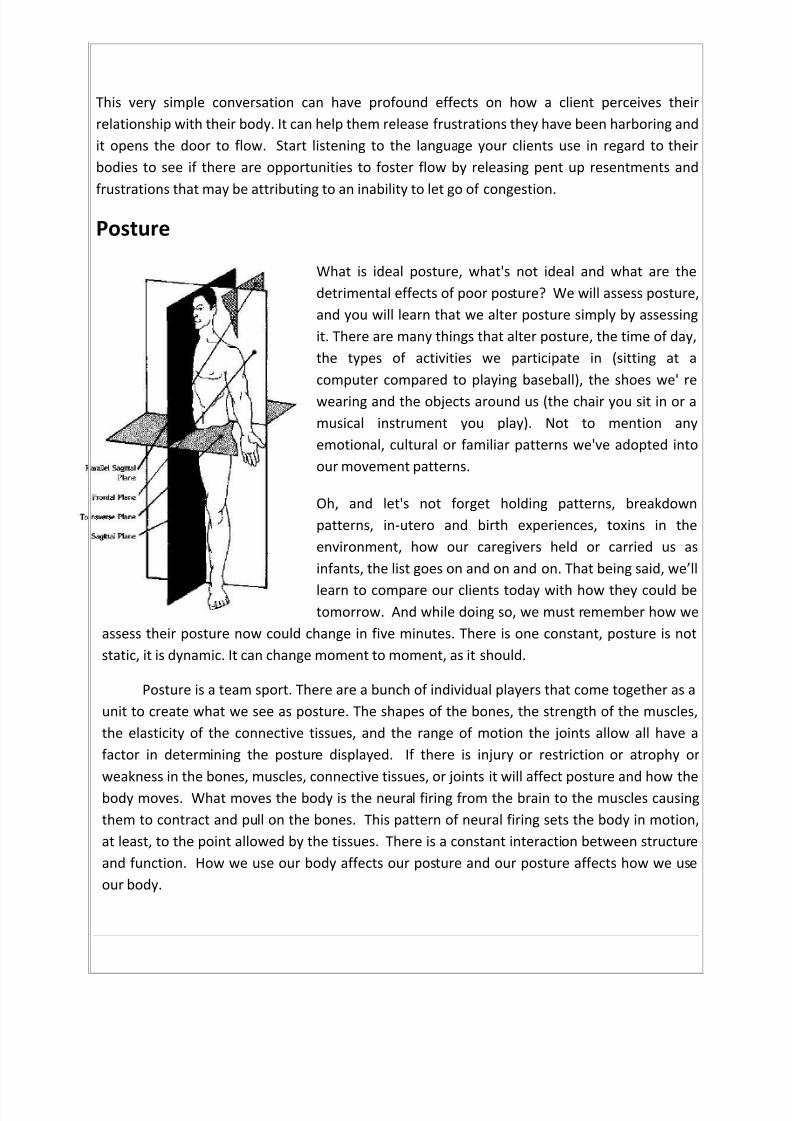
What is ideal posture, what's not ideal and what are thedetrimental effects of poor posture? We will assess posture,and you will learn that we alter posture simply by assessingit. There are many things that alter posture, the time of day,the types of activities we participate in (sitting at acomputer compared to playing baseball), the shoes we' rewearing and the objects around us (the chair you sit in or amusical instrument you play). Not to mention anyemotional, cultural or familiar patterns we've adopted intoour movement patterns.
Oh, and let's not forget holding patterns, breakdownpatterns, in-utero and birth experiences, toxins in theenvironment, how our caregivers held or carried us asinfants, the list goes on and on and on. That being said, we’ll
learn to compare our clients today with how they could betomorrow. And while doing so, we must remember how we
assess their posture now could change in five minutes. There is one constant, posture is notstatic, it is dynamic. It can change moment to moment, as it should.
Posture is a team sport. There are a bunch of individual players that come together as aunit to create what we see as posture. The shapes of the bones, the strength of the muscles,the elasticity of the connective tissues, and the range of motion the joints allow all have afactor in determining the posture displayed. If there is injury or restriction or atrophy orweakness in the bones, muscles, connective tissues, or joints it will affect posture and how thebody moves. What moves the body is the neural firing from the brain to the muscles causingthem to contract and pull on the bones. This pattern of neural firing sets the body in motion,at least, to the point allowed by the tissues. There is a constant interaction between structureand function. How we use our body affects our posture and our posture affects how we useour body.

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 8/42
As you work with clients it's important to remember that their body has created theirposture for a reason. It may not be the most efficient or the most effective posture, but it isstill theirs! They've created it based on their activities, their social life, their psychological lifeand their relationship with gravity. So before you go jumping in trying to change their posture,
be gentle, no one likes their balance point reset too quickly. It is not a good idea to try toimpose a new posture on someone. Posture is a habit, and fundamentally, understanding isrequired to change any habit. Start by assessing posture and acknowledging it for what it is.Then move into a plan that you and the client create together. As Tom Myers puts it, "the ideais to grow out of the tension-to literally grow up into something that is more functional-morethem-more authentically themselves. We don't do that by imposing more tension on top ofthe tension they already have. We do that by exposing the patterns and letting them grow outof t hem.” Hopefully together you can cultivate their posture into something more functionaland efficient for them.
As we try to figure out what ideal posture is, we have to remember that ideal posture is goingto be different from one person to another person. Some people are tall while others areshort. Some are top-heavy others bottom heavy. So the way that individuals carry their weightis different even though they may weigh the same amount numerically. Regardless, the key tobeing pain free is that gravity be our friend. If it is not, our muscles will spend an extraordinaryamount of energy trying to counteract its force, which is constant. One consistency regardlessof your theory of ideal posture is that the planes of motion should meet at 90° angles. PatrickMummy, of Symmetry for Health, calls this the right angle fundamental. Basically, the bodyshould maintain right angles around the planes of motion as it pertains to the load bearing
joints.
Planes of Motion Frontal – the frontal plane divides the body into front and backportions. Abduction and adduction are the movements that occuralong the frontal plane. Head forward postures cause deviations inthe frontal plane.
Sagittal – the sagittal plane divides the body into left and right
portions. Flexion and extension are the movements that occuralong the sagittal plane.
Transverse - the transverse plane divides the body into top andbottom portions. Rotation is the movement that occurs along thetransverse plane.

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 9/42
The body wants to be stable so it will sacrifices movement to ensure stability
o In head forward postures as the head moves forward the extensor muscle’sfascial bags adhere to one another to maintain balance resulting in limitedmobility. The extensor muscles must isometrically contract to resist the pull of
gravity on the head.
Regardless of where an individual holds their weight, ideal posture exists when their weight iscarried by the skeletal system. In order for the skeletal system to effectively weight-bear, thethree planes of motion should meet at 90° angles. Notice in the image above how thetransverse, sagittal and frontal planes all meet to form 90° angles. When the right anglefundamental is met the body’s eight load -bearing joints are vertically and horizontally alignedto the line of gravity and the horizon respectively. In this case minimal effort is needed from themuscles and ligaments to maintain balance.
So what happens if the right angle fundamental is not met? Let's start with thefundamental concept of planal deviation. Imagine in the image above that each of the linesrepresenting a plane of motion is a pane of glass. If one shoulder shifted higher than the other,the glass would break. This would be a transverse plane deviation . If the spine curved to theright from a scoliosis, the pane of glass would break. This would be a sagittal plane deviation .If the shoulders anteriorly rotated or the head jaunted forward from working too many hours atthe computer, again the glass would break. This would be a frontal plane deviation . Noticehow it each of these examples , the movement that breaks the glass is away from themovement of the plane. Flexion and extension occur in the sagittal plane (and strength of the
sagittal plane). While abduction/adduction break the sagittal plane (butstrengthen the frontal plane). Since our bodies are designed to move aproblem only occurs when our bodies don't go back to the right anglefundamental.
By assessing all three planes together we can assess alignment threedimensionally. A deviation in one plane affects all planes. As a result ofthese deviations, the skeletal system is no longer effectively weight-bearingand gravity is no longer our friend. The stretch sensors (muscle spindles and
the golgi tendon organs) deep in the muscles detect excessive or suddenchanges in muscle tension and the righting reflexes are invoked. There arefive righting reflexes designed to restore optimal position when the body hasdeviated from it. The reflexes attempt to correct the deviation through asignal relayed from a reflex mechanism that causes a muscular contraction.
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 10/42
In the case of an athlete, such as a gymnast, the righting reflexes are strong andenhance performance by allowing the athlete to overcome the effects of sudden headmovements. However, once the righting reflexes function improperly, the body enters into astate of compensated motion. The muscular system will adapt any way necessary to maintain
balance against the force of gravity and to keep the eyes parallel with the horizon. Forexample, if a client has an elevated right hip (transverse deviation) their body may compensateby elevating their left shoulder (transverse deviation), bowing their spine (sagittal deviation)and anteriorly rotating their hips and/or shoulders (frontal deviation) to keep their eyes parallelwith the horizon.
Ideally, we can move our body through its full range of motion. The agonistic andantagonistic muscle groups are balanced and hold the body in proper alignment. If this is thecase the body can typically move efficiently and effectively in all three planes of motion.However due to physical or emotional trauma, poor ergonomics or attitude, posture may
become compromised. In this case the body’s ability to move properly through all threeplanes of motion also becomes compromised, further affecting the balance and structure ofthe soft tissue system (muscular, fascial, etc).
MOVEMENT DETERMINES STRUCTURE! Children love to move! According to PatrickMummy movement is an instinctual priority for children. They run for fun, jump up and down,climb EVERYTHING and twist their little bodies every which way. Children move in all threeplanes (frontal, sagittal and transverse), and every joint gets used through its full range ofmotion EVERYDAY! As a result, children tend to have proper alignment. Their structure is ideal
because they move properly. However for many individuals, something happens that disruptstheir ability to move properly. Maybe it's a fall or a car accident or repetitive stress from typingtoo much or the restricted posture of depression. Often it's sitting. From the age of five whenchildren begin school, sitting (flexing) begins to dominate movement patterns. Erik Dalton callsour society "flexion addicts" because we spend so much time sitting curled around our desksor keyboards. As a result of this and other body patterns our ability to move becomes limited.Now movement is determined by our structure, instead of our structure being determined byour movement.
In order to meet the right angle fundamental, homeostasis must exist between tonic(postural/intrinsic) and phasic (dynamic) muscles. Tonic muscles are smaller muscles that donot change length with external force and cross only one joint, while dynamic muscles dochange length with external force and cross more than one joint. Tonic muscles, also known aspostural muscles are responsible for maintaining posture. They have more Slow Twitch (Type 1)muscle fibers . Phasic muscles on the other hand are responsible for moving our body throughtime and space. They have more Fast Twitch (Type II) muscle fibers . The slow twitch muscle

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 11/42
fibers are often referred to as red fibers. They have a higher number of capillaries, are slower toproduce maximal tension, and are more resistant to fatigue than type II fibers. The highconcentrations of slow twitch fibers in postural muscles enable long-term contractionsnecessary for stabilization and postural control. Fast twitch fibers are often referred to as white
fibers. They are quick to produce maximal tension and fatigue more quickly than type I fibers.The high concentrations of fast twitch fibers in dynamic muscles enable quick force and power.All muscles have a combination of slow and fast twitch fibers. Muscles are categorized intopostural or phasic groups based on their predominant activity. It is also been found that thenumber of slow and fast twitch fibers can change in any given muscle depending on activity.When under stress tonic muscles react by becoming short and tight and phasic muscles react bybecoming inhibited and weak. Stretching and releasing a tight hypertonic muscle leads to anautomatic regaining of strength of its antagonists.
Dynamic or phasic muscles - prone to develop inhibition and weakness Gluteus maximus, medius, and minimus Vastus medialis and lateralis Iliacus Thoracic extensors of the spine Abdominals Rhomboids Trapezius i, ii, and iii Triceps brachii
Anterior tibialis
Postural/tonic or antigravity muscles - prone to develop tightness Pectoralis major Levator scapula Trapezius Biceps brachii Scalenes Lumbar and cervical extensors of the spine
Quadratus lumborum (qlo) Psoas major Rectus femoris Vastus intermedius Gastocnemius and soleus Adductor magnus, brevis, and longus
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 12/42
Biceps femoris Semitendinosus Semimembranosus Gracilis
Piriformis Tensor fascia latae (tfl) Sternocleidomastoid Erector spinae muscles Hamstrings Iliopsoas Peroneal
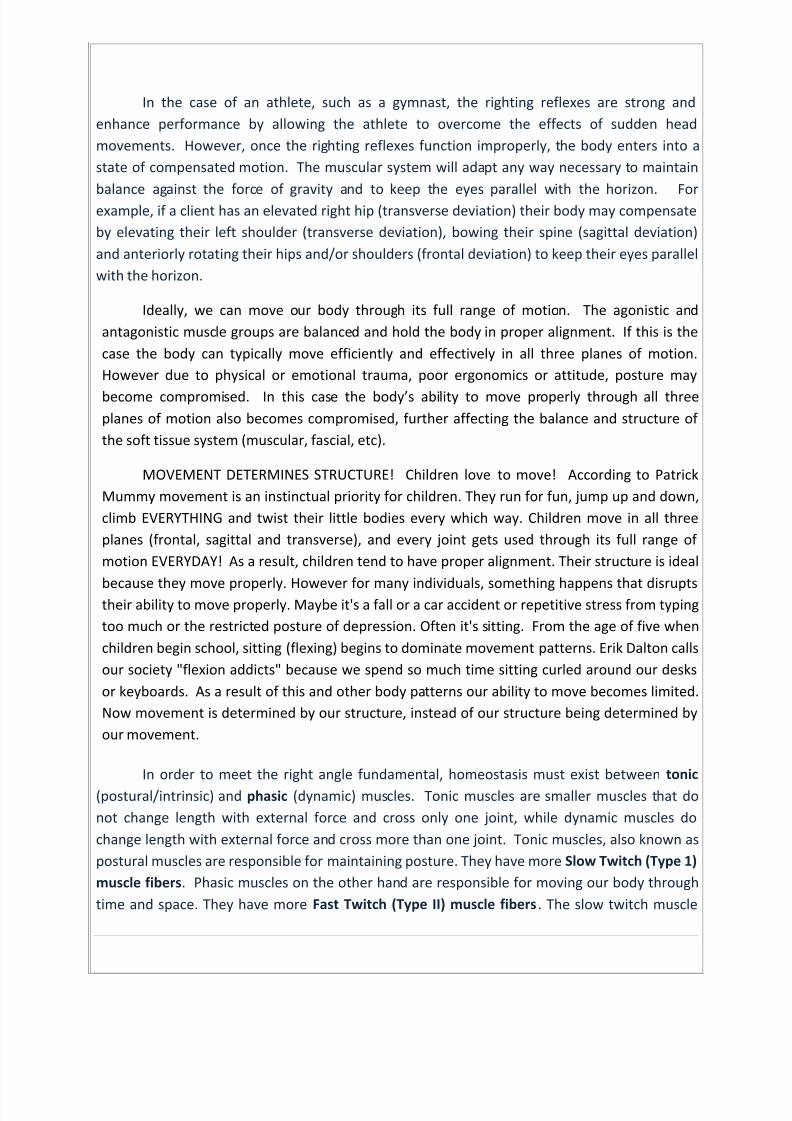
Let's think about this another way. Have you ever played tug-of-war? I often use this
example to help my clients understand the pulley system of the body. Imagine your bones arethe flag in a three-dimensional game of tug-of-war between the muscles on the front of yourbody and the muscles on the back of your body (and side to side/ up and down). Now in agame of regular tug-of-war, if one team pulls the flag to theirside, the rope is shorter between them and the flag incomparison to the other team, whose rope is now longerbetween them and the flag. In the image to the right who hasto work harder in order to get the flag on their side? The childdoes!
Not only is she smaller, but she also has more ground to make up. Can you imagine howtender, tired, over-worked and frustrated the child must feel? How much do you think givingher a backrub would help her win the game of tug-of-war? Probably not very much! She'salready under the gun, relaxing her might feel good, but it won't help her win.
Now, let's extend this example to our body. The adult represents pectoralis major and minorwhich are short, tight and facilitated while the child represents the rhomboids and trapeziuswhich are stretched, weakened and inhibited. Remember in this case, your shoulder is the flag.As the pectoralis muscles pulls the shoulder forward the brain initially fires to the rhomboids,
telling them to pull the shoulder backward. The rhomboids become tender, overworked andtired of fighting a battle they cannot win.
Now there's another factor we haven't talked about yet! Do you remember the termreciprocal inhibition ? Well, here we have altered reciprocal inhibition - muscle inhibitioncaused by a tight agonists, which decreases neural drive of its functional antagonist. To give

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 13/42
you a different example, a tight hip flexor (psoas) would decrease the neural drive of the hipextensor (gluteus maximus), resulting in muscle imbalances.
Okay, let's rewind a little. When we talk about the kinetic chain we are talking about themuscular, skeletal, and nervous systems working together. If any one segment is not working
properly we become misaligned and our bodies don't function properly, resulting in predictablepatterns of dysfunction. We call these predictable patterns of dysfunction postural distortionsor movement compensations. Once our body’s compensation becomes functional (the bodyhas integrated the compensation) there is a lack of structural integrity and decreasedfunctioning of one or more components of the kinetic chain (muscular, skeletal, and nervoussystems).
This lack of structural integrity comes in the form of altered length-tension relationships,
force-couple relationships, and arthrokinematrics . A length-tension relationship refers to the
length at which a muscle can produce the greatest force (Clark, et al). Each muscle has its ideallength that allows the potential for maximal force production of that muscle. If a muscle’slength is altered as a result of poor posture (or injury, etc) that muscle will not be able togenerate proper force to allow for efficient movement and its surrounding muscles will also beaffected and therefore they will also be unable to produce proper force , resulting in a lack ofstructural integrity. Remember our tug-of-war?
Now consider Davis’ law, which states that if a muscle is lax for an extended period of time itsmuscle spindles will take up the slack. This explains why when someone is casted in a flexposition when the cast is removed the muscle can't fully extend. Davis’ law can also occur inhip flexors from sitting for prolonged periods of time.
Our second consequence of lack of structural integrity occurs when force-couple relationshipsare altered . Force-couple relationships simply refer to muscle groups moving together toproduce movement around a joint. When muscles are working in a force-couple they areproviding divergent pulls on the bone or bones they connect with. Each muscle has a differentattachment point, pulls at a different angle, and creates a different force on a joint. When themuscles of the force-couple fire in proper order it ensures proper joint motion as well aseliminating any unwanted motion. Without proper length-tension relationships the force-
couple relationships cannot work properly, resulting in poor arthrokinematics (or joint motion).
One last term for you, synergistic dominance, this is the neuromuscular phenomenon thatoccurs when inappropriate muscles take over the function of a weak or inhibited prime mover.So you get sick at work, and someone else is brought in to do your job. It's not their job. Theydon't know how to do it. They don't do it as well as you do, they are just doing the best theycan. Our nervous system reacts much the same way; let's say that your psoas is tight, leading
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 14/42
to reciprocal inhibition of the gluteus maximus. Now the glute can't do its job, which is hipextension so it synergists (other muscles capable of hip extension) (hamstrings, adductormagnus, and erector spinae) takeover to compensate for the weakened gluteus maximus. Thiscan cause faulty patterns which lead to Arthrokinetic (joint) dysfunction and altered force-
couple relationships; all of which decrease neuromuscular efficiency and eventually lead topostural compensations and injury.
Head Forward Postures: Possible Head/Jaw Relationships-
Class I – NORMAL Head balanced – eyes level – Jaw and Cranial base aligned with transverse plane
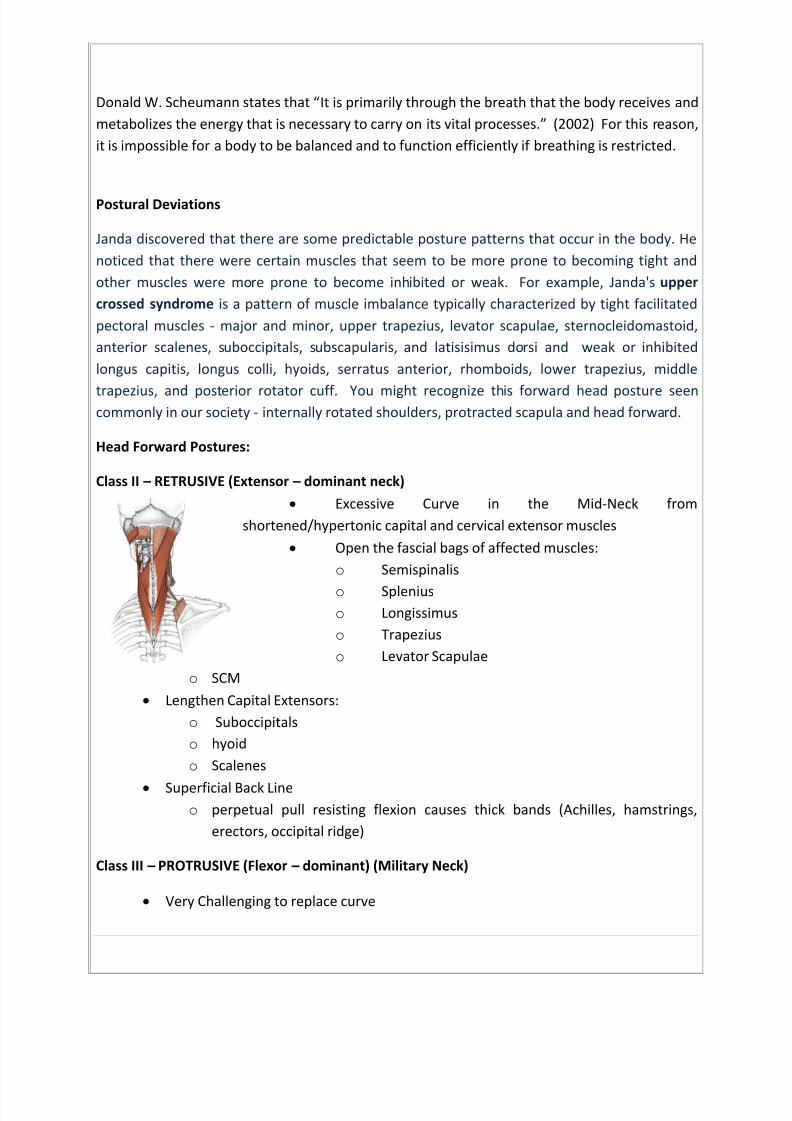
Class II – RETRUSIVE (Extensor – dominant neck) Excessive Curve in the Mid-Neck from shortened/hypertonic capital and cervical
extensor muscles
Open the fascial bags of affected muscles: Semispinalis – Splenius – Longissimus – trapezius – Levator Scapulae and SCM
Lengthen Capital Extensors such as Suboccipitals and hyoid and Scalenes Superficial Back Line – perpetual pull resisting flexion causes thick bands (Achilles,
hamstrings, erectors, occipital ridge)
Class III – PROTRUSIVE (Flexor – dominant) (Military Neck)
Very Challenging to replace curve Usually Begins in the pelvis
CED – Capital-extensor- dominant “straight neck”
Very common with computer use Cervical extensors are overstretched and tight (eccentric) – Semispinalis Cervicis Capital Extensors are short and hypercontracted (concentric): Semispinalis Capitis,
Splenius Capitis, Longissimus Capitis, Suboccipitals, Upper Trap
Techniques
Diaphragmatic breathingDiaphragmatic breathing is one of the best ways to center oneself. The process opens
energetic pathways throughout the body. As you rhythmically breathe in and out, musclesslowly unwind, releasing tension, stress, and locked up energy. This progressive melting of thebody leaves a feeling of peace behind. I have taught clients diaphragmatic breathing for years

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 15/42
and am still constantly amazed at how much pain can be eliminated from the body in minutes.All from just breathing correctly!
Diaphragmatic breathing is not just any form of breathing but a very specific one.Inhalation is initiated by the diaphragm - the muscular sheet that separates the chest cavity
from the abdominal cavity. Diaphragmatic breathing is a long, slow process which allows thebody to maximally absorb oxygen. As the diaphragm contracts it presses down on theabdominal viscera, the abdomen expands, and oxygen fills the lungs as it rushes into thevacuum created by the expanded chest cavity. (Majid, 2007) Exhalation releases the breathslowly, ridding the body of carbon dioxide. When we exhale our bodies relax, resumingessential body functions and activating the parasympathetic nervous system in the process.Sometimes we hold our breath when we are scared or in pain. Once we release the breath onexhale, ahh... the relief. Try it: Hold your breath for 10 seconds or so and then let it go. Nowfeel how your body reacts to the exhale.
Diaphragmatic breathing is the way we were meant to breathe - it is how baby’sbreathe. Unlike babies, adults tend to take shallow breaths much higher in their chests.Additionally, when adults feel nervous, anxious, fearful, or excited their breath may becomefaster and shallower, potentially increasing physical tension and stress. Diaphragmaticbreathing increases oxygen consumption while decreasing muscle hypertension which providesa more beneficial breath than one gained by a shallow chest breath. As a result of sedentarylife styles, high stress levels, and in some cases, paradoxically enough, over-developedabdominal muscles, some people’s diaphragms become dysfunctional. With such clients, it isespecially important to focus on slow inhalation and slow exhalation. Although the diaphragm
is intended to do the bulk of the work, many people are unaware of how to use this vitalmuscle. Diaphragmatic breathing may initially be difficult for clients, but with practice it canreinstate itself as the normal breathing pattern.
Diaphragmatic breathing can be used as a tool in moments of fear or stress. Asdiscussed earlier, when we have a fear based response to something in our environment, ourlimbic system takes control of the brain, releases a mix of strong hormones, and temporarilydisconnects the frontal lobes of the brain. At this point our Amygdala has hijacked our brain.We can use our breath to encourage parasympathetic activation - counteracting the fight or
flight response. This is done by taking several slow, long, deep, cleansing breaths. Another wayto reduce tension and stress is to become conscious ofhow our breath can be used as a tool tohelp us relax. In stressful situations, pause by taking a deep breath: inhale through your nosefrom your abdomen, then slowly exhale.
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 16/42
Diaphragmatic Breathing Exercises
Guided Breath
1. Have the client, clothed or unclothed, lie comfortably. If unclothed ensure that theclient is properly draped and warm enough.
2. Place one hand on the client’s chest and one on their stomach. Have the client do thesame.
3. Ask the client to inhale slowly either through the nose or through pursed lips (this slowsthe intake of air).
4. As the client inhales, feel the stomach expand. If the client’s chest expands instead, askher to focus on breathing with the diaphragm. You can tell her to push your handtoward the ceiling with her breath.
5. Instruct the client to pause for one or two seconds prior to exhaling.6. Ask the client to exhale slowly through pursed lips to regulate the release of air.
7. Allow the client to rest if necessary, and then repeat.
8. After several minutes of practice, ask the client if she notices any changes in her body.
9. Once the client is able to maintain the diaphragmatic breathing, remove your hands.Allowing the client to continue on her own without your guidance.
10. You may now proceed with massage or other therapies you decide to include in the
session.You may choose to add suggestions or visualizations to the guided-breath exercise. Dependingon the client’s situation suggestions can be added to the inhalation, exhalation or both. Themessage should be appropriate for the client’s individual circumstance. Fo r example, if theclient is in pain, or experiences pain, you might instruct her to carry a message via her breatheto all the cells of her body- “I know you are hurting. Is there anything I can do to help you letgo?” would be appropriate. The same client might follow with this message on the exhale “Letmy breathe carry the pain away.”
"The Complete Breath"
“The Complete Breath” is a technique taught in yoga classes. It adds thorax and chestexpansion to diaphragmatic breathing. “The Complete Breath” helps create the maximum flowof life force (Prana) through the body.
It must be noted that some breath therapists and breathing teachers feel diaphragmaticbreathing is better than “The Complete Breath” for maintaining balanced breathing. Their
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 17/42
reasoning goes as follows: We take some 20,000 breaths a day. If we expand the thorax andchest with each breath, the scalene, trapezius and sternocleidomastoid muscles overwork asthey contract to pull up the chest wall with each breath. This is wholly unnecessary – and istherefore a waste of energy since the lungs are more fully oxygenated with diaphragmatic
breathing. (Majid, 2007) For these reasons, I tend to agree that diaphragmatic breathing isbetter for a person’s normal breathing patterns; however, I feel “The Complete Breath” isbeneficial when the purpose is to open energy pathways during therapy.
8-4-8 Breathing8-4-8 breathing is a great exercise to give clients for homework. Practicing the breathingexercise for 5-10 minutes once or twice daily assists clients in becoming more relaxed. Clientscan use it to calm themselves by simply exhaling and their bodies will take over and supply therest of the response.
1. Sit in a relaxed position. Uncross your arms, fingers and legs. Put your feet flat onthe floor. Relax your hands.
2. Close your eyes and visualize a relaxing image: curtains blowing in the wind, asandy beach where you can hear the ocean, a color (white, blue, etc.)
3. Inhale from your abdomen, through your nose, to a count of 8.4. Hold your breath to a count of 4.5. Make your mouth open into a big “O”, and exhale through your mouth, to a
count of 8.6. Repeat steps 3, 4, and 5 for several minutes (5 minutes does an incredible job of
relaxing your body!)You can lower your blood pressure by 30 points and your pulse rate as much as 20-30 percentin 5 minutes, with practice. Use this technique before entering a potentially emotional situationor after you have participated in a highly charged situation, to maintain choice over yourbehavior.
Visualization
Visualization is a tool used to assist clients in becoming self-aware (physically,emotionally and mentally) by focusing their attention - resulting in a greater ability to manifesttheir desired outcomes. Using guided imagery a client can revisit, revise, and reintegrate pastexperiences allowing them to choose how the experience can best serve them in the future.Visualization exercises help clients “see” their options.
Research has shown that the use of visualization techniques can have powerful effects.Researchers, for instance, found that cancer patients who were offered a combination ofrelaxation and peaceful imagery rated their quality of life during chemotherapy higher andreported fewer side effects than patients who had received only the relaxation sessions. The

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 18/42
imagery group also had "enhanced lymphokine-activated killer cytotoxicity, higher numbers ofactivated T-cells and reduced blood levels of tumor necrosis factor" (Utay and Miller, 2006)
Guided imagery is a very diverse technique that can be used in many differentsituations. It can be used independent of, or as a complement to, other techniques. It may be
integrated throughout an entire session or, when appropriate, a short specific visualization maybe spontaneously added at any point in a session. For example, if my client is having difficultlyrelaxing while I am palpating a trigger point, I may have the client visualize a little knot tied upin the fibers of his muscle. I will ask the client to watch the knot struggle as it tries to free itself.I may ask the client to talk to it, tell it everything is okay and to relax as the client visualizesuntying it. It always amazes me how just connecting to how the body is feeling andacknowledging that feeling almost automatically creates change. When and how you use thistool will depend on the needs of your client, your setting, and your own comfort level using theapproach.
AWARENESS VISUALIZATION EXERCISE
"Take a slow deep breath in through your nose … good … feel your chest fill with oxygen …slowly exhale through your lips … notice how your body sinks into the massage table as yourelease tension with your breath… good … a few more times …. Inhale … feel your diaphragmexpand from under your ribs … good … Exhale … invite any stress (tension/pain/etc) you feel toleave with your breath … good … Inhale …. Feel for any discomfort or pain in the area of yourhead and face … Again invite any pain or discomfort to leave your body with your breath …Feel the warm, vibrant energy of your breath travel into your neck and shoulder area, note anyspot where there is pain or discomfort as your breath scans your body… As you breathe inacknowledge any area your breath has difficulty accessing … Good…Now fill any such areaswith the warm, vibrant energy of your breath.... feel those tissues sigh as you exhale, feelthem release any tension they are holding …. Bring your breath down your spine … good… feelyour breath expand your belly and pelvis…. Make a mental note of areas of pain anddiscomfort, and notice as your breath travels down that your relaxation increases with eachbreath…Nice deep breath as you fill your legs and arms releasing tension as you exhale… a fewmore times…slowly inhale … feel your body breathe…and exhale….feel your b odyrelax…Good…Your journey through your body is both productive and rewarding as areas ofdiscomfort are revealed to you. … let’s bring your mind’s eye to the area of your body thatsent you the strongest message of discomfort and focus on the message that awaits youthere… can you tell me what the message says?......(Wait for a response – this could takeseveral minutes)
(If the client has a message, fill in the next line. If not wait a few breaths and ask again. Ifstill no message, if appropriate, move on with an adaption.)

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 19/42
Breathe in a slow deep breath to this area of greatest restriction… good…and exhale…Asyou breath in have your breath carry a message… imagine the your breath quietly whisperingto the tissues surrounding the restriction….. (use wha tever is appropriate)
“I feel your ______________________” (pain, tightness, etc)
“I hear your message and I understand”
“Thank you for trying to protect me”
“I am listening and I accept you just as you are.”
“I know you are scared, but it is okay to let go (forgive, move on, cry, etc)
Wonderful… is there anything else this area needs or wants to tell you?....... (If so repeatabove) Are there other places in your body where you have noted strong pain or discomfortduring your body scan? If so, go to that area now … when you are there, acknowledge the
pain. (Repeat the process as many times as needed) Great job! See how you’re able toidentify the areas of blocked energy …take your time …feel your body … feel it’s vibrance… feel its energy flow through you… that’s right … nice…deep…breaths…….
Hands-On: Demonstrated in Class
Assessing PostureWe want to observe the body as a whole. How it moves as a unit. Is there an exaggeratedmovement in one segment to make up for a lack of movement in another? We are looking for
both what is symmetrical and what is not. We must consider the body’s experiences andincorporate them into our assessment. Often clients will enter our offices with a specific painor complaint they want to address, it is our duty to look deeper to find the underlying factors oftheir complaint. We will observe the body in static position and during dynamic movement.
Palpation:While you do a palpation assessment you want to work with relaxed hands. This will
allow you to get even the subtlest sensory information about your client’s soft tissues. Whenwe conduct a palpation assessment we are trying to get as much information as possible
without activating the body's protective response. Press your fingers into your massetermuscle. Just notice what that feels like. Now actively relax the muscle and check again. Doesthe tissue feel any different? Now actively contract the muscle and check again. What's thedifference this time? Can you feel the contraction of the muscle push your finger out? Thisprotective mechanism is activated subconsciously by the sympathetic nervous system insituations of potential and perceived danger. If you jab somebody with your finger they're
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 20/42
going to contract to push you out. If you instead slowly push your finger or your hands intotheir relaxed arm you can get much better information about their soft tissues. With ourpalpation assessment we’re evaluating temperatures, textures and movements of the softtissue.
Temperature – feel for localized areas of heat or coldTextures - hyper/hypotonic muscles, scar tissue, restricted fascia, trigger points, andedemaMovements – limited range of motion and stiffnessRhythms - breathing, pulse, craniosacral
o It is essential to determine which tissues are hypertonic and which arehypotonic. Then one must decide whether to increase or decrease tone.
o Place client in a supine position on massage table.o Using light pressure feel for differences in texture, tone and temperature as you
bilaterally palpate from head to toeo Chart difference
Assessment of Skin TemperatureIf circulation or energy is restricted the area may be cool to the touch. This could
indicate ischemia (reduced blood supply) which is sometimes caused by partial patients andhypotonic muscles. If energy is stuck in an area, that area may be warm to the touch. Heat canalso be a sign of inflammation or fever, either of which potentially could be a specific or ageneral contraindication for massage.
Textures and Movement of Soft TissuesThe better your palpation skills, the more able you will be able to distinguish the
difference between scar tissue and restricted fascia. These tissues feel as if they are bounddown and stuck together and sometimes they have a grainy, gristly feeling . Hypertonic musclesfeel resistant or tight, regardless of whether they're in a relaxed position or passivelycontracted. Trigger points feel like little knots within the muscle, and it hurts when you palpatethem and sometimes pain radiates to other parts of the body. Edema or swelling can feelspongy or like a water balloon full and squishy. Pay attention to what healthy muscle tissue tofeels like compared to unhealthy muscle tissue. Healthy tissue is soft and pliable compared toropey or sticky or gristly.
RhythmsMatch your clients breathing, what does it feel like?

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 21/42
Visual AssessmentFind the greatest disparity first then continue until you see the least. Remember, you arelooking for anything that is skewed from right angles around three-dimensional space first. It iswhat we refer to as “red flags”.
Here is the list:
a. Feet everted, pronated or supinated.
b. Hand forward or rounded more than the other.
c. Forward rotation of the pelvis.
d. Upper torso rotation (one arm in front more than the other).
e. Scapulae protracted, retracted, or elevated.
f. One hip higher than the other.
g. More space between one arm and the torso versus the other.
h. Knees medial or external or one knee medial and the other external.
i. Knees varus or valgus.
j. Offset of the torso.
k. Offset of the head.
l. Knee flexion or hyperextension.
m. Forward displacement of the pelvis or head from the frontal plane.
n. Also, take notice of muscular misdevelopements such as one calflarger than the other, etc.
IDENTIFY HOW EMOTION, STRESS AND TRAUMA ARE STORED IN THE BODY
Your mind and body are designed to process energy - designed to adapt to the situationat hand. It is only when mind and body do not successfully process and adapt to a givenexperience that stress or as Don Cohen and John E. Upledger (1996) put it “distress” is stored inthe body. This stress is often palpable in client’s soft tissues during massage.
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 22/42
In their book, Introduction to Craniosacral Therapy : Anatomy, Function, and Treatment ,Cohen and Upledger (1996) discuss stress storage in the membrane system of the body. Theystate that somatic tension can both be affected by and affect emotional and mental issues.When somatic tension patterns are released a client may experience emotion. The emotion is
not necessarily, but could be associated with past memories. It is possible that symptoms theclient experiences are related to painful memories that have been blocked from the consciousmind. Memories can come in many forms. They can be wanted or unwanted, conscious orunconscious, physical or emotional, traumatic or mundane, neurological or somatic. There aredifferent organs and organ systems responsible for specific types of memory. The amygdala,for example, remembers the emotional content of experiences while the hippocampus storesthe dry facts. (Goleman, 1997)
State-Dependant Memory is “the tendency for information learnt in a particular mentalor physical state to be most easily remembered in a similar state.” (Coleman, 2001) A state -
dependant memory can be any memory that is triggered by duplicating the original bodyposition, sensory input, location, body movements, emotions or nervous system activation thatwas experienced at the time of the original event. The memory can be of a pleasant orunpleasant nature. Mood dependant memory is a term used for emotional state-dependantmemories. Research has shown that positive experiences are more likely to be remembered bya person who is happy and negative experiences by someone who is unhappy.
Imagine you are driving down the highway. The interstate wall is on your left, a semitruck on the right. As you cross a bridge you hit black ice on the road, you loss control of yourcar and as your car is spinning out of control, you see the headlights of the semi truck 3 feet
from your drivers’ side door. You get lucky, your car is spinning fast enough that instead ofgetting run over by the semi it instead smashes into the interstate wall screeching as it slidesdown the wall 20 feet before it stops facing oncoming traffic. By now your amygdala hascertainly activated the sympathetic portion of your autonomic nervous system (ANS); a few ofyour body’s physiological reactions may be an increase in blood pressure, pupil dilation, andslowed respiration. This intense amygdala arousal has burned the characteristics of this eventinto memory to be stored in case a similar situation occurs again. The amygdala may potentiallysend a surge of anxiety through your system every time you are in an even slightly similarsituation - a reaction that may not always be appropriate and even dangerous depending on
the physiological reactions that accompany the anxiety!
I should know, this actually happened to me. I couldn’t figure out why my neck wouldfeel great after a massage and then an hour later would hurt again, that is until my therapistwalked me to my car one day. She pointed out to me that as soon as I closed my door andlatched my seatbelt my entire body tensed, my shoulders crawling up like earrings! My bodywas preparing for danger and I didn’t even notice! I used visualization and breathing

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 23/42
techniques to relax myself before and right after I got in my car. After a week my neck nolonger hurt and I noticed that I wasn’t as jumpy driving.
State-dependant memory interacts with the ANS. Massage affects the ANS and cantrigger state- dependant memory by placing the client’s body in certain positions, by using
certain movement patterns, or by replicating a particular pressure sensation. This can happenboth intentionally and unintentionally. When unintentional, the client may get confused orscared if the memory is overwhelming, especially if it is related to unresolved trauma. It isimportant for the therapist to make sure the client feels safe and understands that nothing iswrong with him/her - it is but energy being processed. The client may even be able to resolveon his/her own some of the energy associated with the memory, just as I did with my anxiety.Professional counseling may also be helpful in assisting the client in working through memorypatterns associated with deep trauma issues and to develop strategies for resolving,integrating, and transcending the trauma itself. (Salvo, 2003)
MEMBRANE PATTERNS
Holding patterns are the body’s tissues’ representation of emotional trauma. Holdingpatterns may manifest in obvious or inconspicuous ways. You may see it as the withdrawal reflexof an abuse survivor or the rigid posture of someone who isn’t going to be pushed around byanyone anymore! It is also important to remember that not all postural habits are holdingpatterns, so don’t go around making hasty generalizations about why people hold themselvesthe way they do. Everyone is unique and your ability to assess and differentiate will only
improve if you really tune in to all communication from clients, verbal and non-verbal.Sometimes neither you nor the client will be aware of emotionally traumatic holding patternsuntil they are released - and even then, you may have no idea where they came from unless amemory and/or emotion is also present at the time of release.
Where holding patterns are the body’s way of storing emotional energy, breakdownpatterns are the body’s way of adapting to physical trauma or micro-trauma. (Cohen &Upledger, 1996) When the body suffers an injury from an accident or fall, from a diseaseprocess, or from maladaptive use patterns (e.g. sitting at a desk 6 hours a day) it will adapt in anyway necessary to function. Our bodies will posturally compensate to take the weight off of a
sprained ankle to avoid pain and allow the best possible gait despite the injury. In the case ofpostural compensations and maladaptive use patterns, gravity is not your friend and onlyperpetuates the breakdown patterns. The body adapts to function; therefore, it does notrecognize that it’s functioning is dysfunctional – rather, it just accepts the new patterns asnormal. Because of this acceptance, the body keeps these patterns even after the injury has

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 24/42
healed or the disease has been cured. It can be tremendously burdening to the system. Massageis a wonderful tool to help clients release breakdown patterns and restore optimum health.
Holding and breakdown patterns can occur independently of each other, as reactions toeach other, or simultaneously. Let’s take as an example an auto accident. If a young girl breaks
her leg, she may develop breakdown patterns; if she walks away unharmed physically, but isberated by her father for being so stupid she may develop holding patterns; if she breaks her legand also endures her father’s wrath, she may develop both. The more powerful the experience,the more embedded the tension patterns. Imagine the same girl broke several bones, ended upin a coma for several days, and awoke to find out her boyfriend had died in the accident. Herbody/mind would have to process a level of both physical and emotional stress such that it is hardto imagine. She would be facing a long rehabilitation process on top of her grief, anger, denial,guilt, financial difficulties, etc. It is also possible for holding patterns and breakdown patterns toprevent the processing or healing of each other. In the last example, the girl’s body may
associate the physical and emotional trauma she experienced with one another. As a result someof the emotional trauma might be stored in the physical wound, preventing the girl’s brokenbones from healing as quickly or as well as they should. Simply put, it is essential to consider bothwhy a client has specific sym ptoms (cause) and why they aren’t going away (unsuccessfulprocessing). As regards to the latter, it is also important to realize that breakdown patterns canpile up on top of each other, such as with athletes who experience frequent injury. Regardless ofcause, both holding and breakdown patterns are taxing to the body, and require an enormousamount of energy form the autonomic nervous system, thus limiting available adaptive reserve.
Myofascial Tissue
The “myo” in myofascial refers to the muscles. The “fascia” in myofascial refers to aspecific type of deep fascia (connective tissue) that separates and defines muscle tissue. Theterm myofascial is sometimes used to reference the fascia that is bound to muscles, andsometimes to reference the muscle. Myofascial tissue surrounds each individual muscle fiber(endomysium), bundles of muscle fibers (perimysium) and the entire muscle (epimysium). Eachlayer of fascia has a function- the endomysium holds the individual muscle cells in place, theperimysium provides a pathway for nerve fibers and capillaries to reach the muscle fibers, andthe epimysium separates the individual muscles from one another and from other structures,and is continuous with the tendons of the muscles it surrounds.

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 25/42
The deep fascia of the muscles (myofascial tissue) is primarily avascular, yet highly innervatedwith sensory receptors that detect pain and proprioception. Trixotrophy is the term used todescribe how fascial tissue can chance consistency with temperature changes, manipulation,and pressure – it can be thicker and harder, or more pliable and softer. Deep fascia also has thecapacity to contract, relax, and change its composition in response to sensory input. This abilityfor deep fascia to add, reduce, or change its composition is called fascial remodeling.
It was believed that fascia was a passive tissue, but recent studies indicate that deepfascia can indeed actively contract and relax. These investigations have discovered that fasciacontains smooth muscle-like fibroblasts allowing it to autonomously stiffen. ( Schleip, Robert et
al, 2006) An example of rapid fascial contraction occurs during the fight-or- flight response to aperceived treat (real or imagined). The fascia will temporarily increase in stiffness whichincreases the tension in the fascia allowing the individual greater speed and strength in crisis.(Wikipedia) The mechanoreceptors in the deep fascia can initiate relaxation when indicated.The mechanoreceptors monitor for muscle tension, joint position, rate of movement, pressure,and vibration. In order to avoid injury, the myofascial tissue will be triggered to quickly releasetension in response to rapid movements or sudden muscular overload.
Rib Release
The thoracic cage is comprised or 12 pairs of ribs, the 12 thoracic vertebrae, costalcartilage, and the sternum. The 12 pairs of ribs attach to the vertebrae then wrap aroundtoward the anterior where they attach to the sternum via the costal cartilage. The thoraciccage is designed to provide protection for the heart and lungs, and to provide attachmentpoints for muscles.
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 26/42
Donald W. Scheumann states that “ It is primarily through the breath that the body receives andmetabolizes the energy that is necessary to carry on its vital proc esses.” (2002) For this reason,it is impossible for a body to be balanced and to function efficiently if breathing is restricted.
Postural Deviations
Janda discovered that there are some predictable posture patterns that occur in the body. Henoticed that there were certain muscles that seem to be more prone to becoming tight andother muscles were more prone to become inhibited or weak. For example, Janda's uppercrossed syndrome is a pattern of muscle imbalance typically characterized by tight facilitatedpectoral muscles - major and minor, upper trapezius, levator scapulae, sternocleidomastoid,anterior scalenes, suboccipitals, subscapularis, and latisisimus dorsi and weak or inhibitedlongus capitis, longus colli, hyoids, serratus anterior, rhomboids, lower trapezius, middle
trapezius, and posterior rotator cuff. You might recognize this forward head posture seencommonly in our society - internally rotated shoulders, protracted scapula and head forward.
Head Forward Postures:
Class II – RETRUSIVE (Extensor – dominant neck) Excessive Curve in the Mid-Neck from
shortened/hypertonic capital and cervical extensor muscles Open the fascial bags of affected muscles:
o Semispinaliso Spleniuso Longissimuso Trapeziuso Levator Scapulae
o SCM Lengthen Capital Extensors:
o Suboccipitalso hyoido Scalenes
Superficial Back Lineo perpetual pull resisting flexion causes thick bands (Achilles, hamstrings,
erectors, occipital ridge)
Class III – PROTRUSIVE (Flexor – dominant) (Military Neck)
Very Challenging to replace curve
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 27/42
Usually Begins in the pelvis
CED – Capital-extensor- dominant “straight neck”
Very common with computer use Cervical extensors are overstretched and tight (eccentric)
o Semispinalis Cervicis Capital Extensors are short and hypercontracted (concentric):
o Semispinalis Capitiso Splenius Capitiso Longissimus Capitiso Suboccipitalso Upper Trap

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 28/42
UPPER CROSSED SYNDROME
Muscles Typically Short, Tight and Facilitated:Upper TrapeziusPectoralis Major and MinorLevator ScapularSternocleidomastoidAnterior ScalenesSuboccipitalsSubscapularisLatisisimus Dorsi
Muscles Typically Weak and Inhibited:Longus Capitis (Deep Neck Flexor)
Longest Colli (Deep Neck Flexor)HyoidsSerratus AnteriorRhomboidsLower TrapeziusMiddle TrapeziusPosterior Rotator Cuff
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 29/42

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 30/42
Upper Trapezius
The trapezius muscle fibers can be divided intothree groups: upper (descending) fibers, middlefibers and lower (ascending) fibers. The upper and
lower fibers act as antagonists to each other inelevation and depression of the scapula.
Action o f Upper Fibers:Bilaterally
Extends the Head and NeckUnilaterally
Laterally Flex the Head and Neck to the Same SideRotate the Head and Neck to the Opposite SideElevate the ScapulaUpwardly Rotate the Scapula
Origin of Upper Fibers :Occipital Ridge, Ligamentum Nuchae,Spinous Process of C7 through T 12
Insertion of Upper Fibers :Lateral One Third of Clavicle, Acromiomand Spine of the Scapula
Dysfunction:The Upper Trap Can Combine Forces with the SCMto Elevate the Shoulder and Drag the Head and
Neck Forward on the Sagittal plane
Movement:
IAR neck bring client ’s right ear to right shoulder strip upper trapezius using knuckles from center to
attachments at the occipital Ridge and the spine ofthe scapula
Using the heel of a your hand strip the Upper Trapposterior
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 31/42
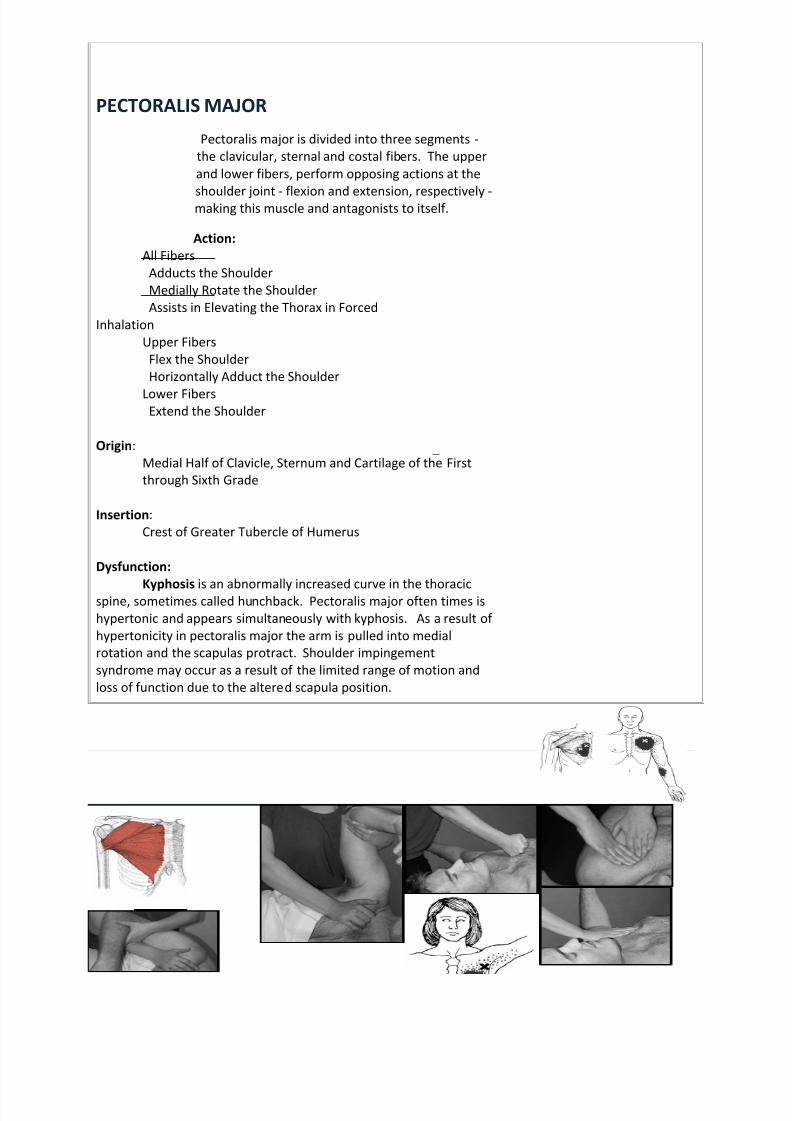
PECTORALIS MAJOR
Pectoralis major is divided into three segments -the clavicular, sternal and costal fibers. The upperand lower fibers, perform opposing actions at the
shoulder joint - flexion and extension, respectively -making this muscle and antagonists to itself.
Action:All Fibers
Adducts the ShoulderMedially Rotate the ShoulderAssists in Elevating the Thorax in Forced
InhalationUpper Fibers
Flex the ShoulderHorizontally Adduct the Shoulder
Lower FibersExtend the Shoulder
Origin :Medial Half of Clavicle, Sternum and Cartilage of the First
through Sixth Grade
Insertion :Crest of Greater Tubercle of Humerus
Dysfunction:
Kyphosis is an abnormally increased curve in the thoracicspine, sometimes called hunchback. Pectoralis major often times ishypertonic and appears simultaneously with kyphosis. As a result ofhypertonicity in pectoralis major the arm is pulled into medialrotation and the scapulas protract. Shoulder impingementsyndrome may occur as a result of the limited range of motion andloss of function due to the altered scapula position.
Movement:
IAR Shoulder
Therapist stretches pec major while maintaining a counterpressure to resists arm movement
Pec Scoop Attachment compressions
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 32/42
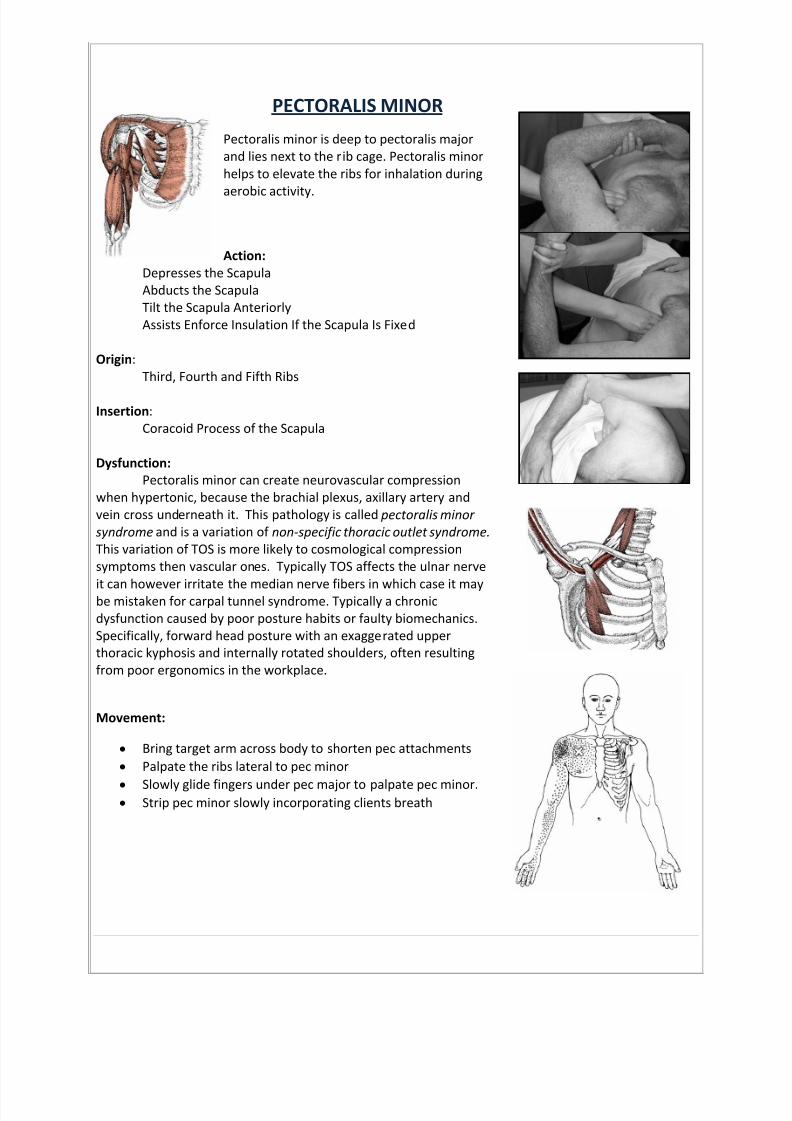
PECTORALIS MINOR
Pectoralis minor is deep to pectoralis majorand lies next to the rib cage. Pectoralis minorhelps to elevate the ribs for inhalation during
aerobic activity.
Action:Depresses the ScapulaAbducts the ScapulaTilt the Scapula AnteriorlyAssists Enforce Insulation If the Scapula Is Fixed
Origin :Third, Fourth and Fifth Ribs
Insertion :Coracoid Process of the Scapula
Dysfunction:Pectoralis minor can create neurovascular compression
when hypertonic, because the brachial plexus, axillary artery andvein cross underneath it. This pathology is called pectoralis minorsyndrome and is a variation of non-specific thoracic outlet syndrome.This variation of TOS is more likely to cosmological compressionsymptoms then vascular ones. Typically TOS affects the ulnar nerve
it can however irritate the median nerve fibers in which case it maybe mistaken for carpal tunnel syndrome. Typically a chronicdysfunction caused by poor posture habits or faulty biomechanics.Specifically, forward head posture with an exaggerated upperthoracic kyphosis and internally rotated shoulders, often resultingfrom poor ergonomics in the workplace.
Movement:
Bring target arm across body to shorten pec attachments Palpate the ribs lateral to pec minor
Slowly glide fingers under pec major to palpate pec minor. Strip pec minor slowly incorporating clients breath
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 33/42
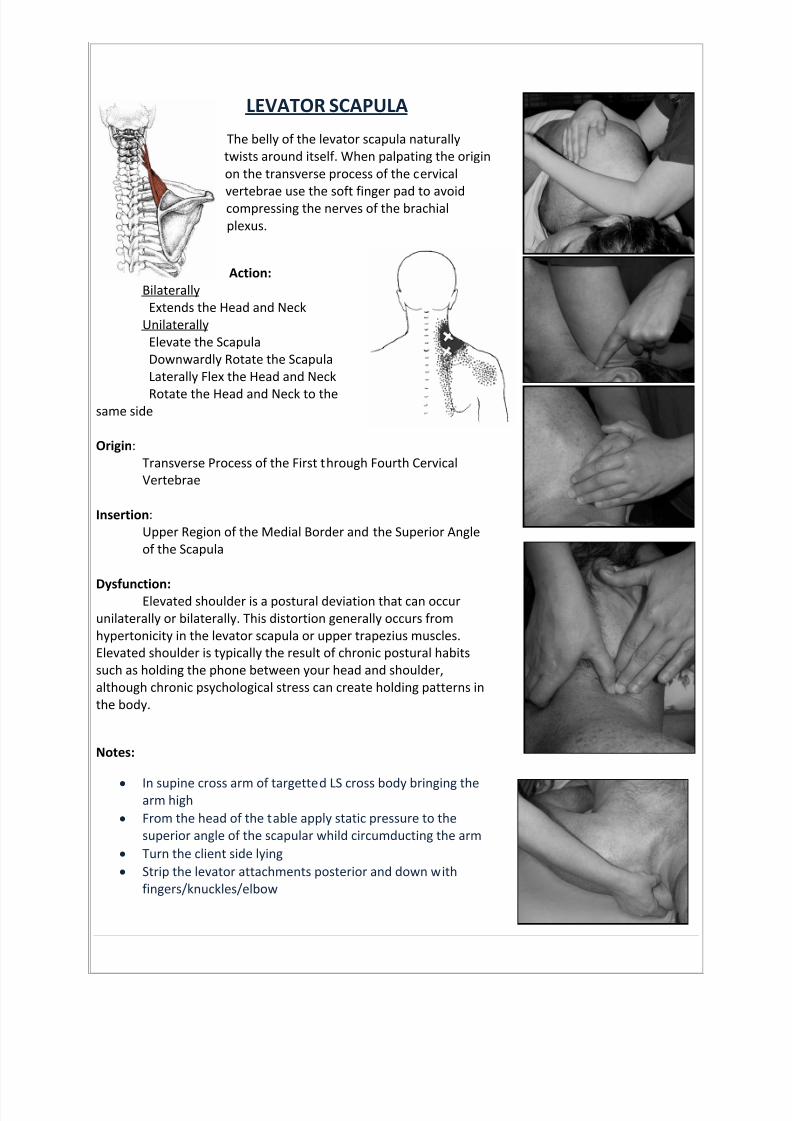
LEVATOR SCAPULA
The belly of the levator scapula naturallytwists around itself. When palpating the originon the transverse process of the cervical
vertebrae use the soft finger pad to avoidcompressing the nerves of the brachialplexus.
Action:Bilaterally
Extends the Head and NeckUnilaterally
Elevate the ScapulaDownwardly Rotate the ScapulaLaterally Flex the Head and Neck
Rotate the Head and Neck to thesame side
Origin :Transverse Process of the First through Fourth CervicalVertebrae
Insertion :Upper Region of the Medial Border and the Superior Angleof the Scapula
Dysfunction:Elevated shoulder is a postural deviation that can occurunilaterally or bilaterally. This distortion generally occurs fromhypertonicity in the levator scapula or upper trapezius muscles.Elevated shoulder is typically the result of chronic postural habitssuch as holding the phone between your head and shoulder,although chronic psychological stress can create holding patterns inthe body.
Notes:
In supine cross arm of targetted LS cross body bringing thearm high
From the head of the table apply static pressure to thesuperior angle of the scapular whild circumducting the arm
Turn the client side lying Strip the levator attachments posterior and down with
fingers/knuckles/elbow
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 34/42
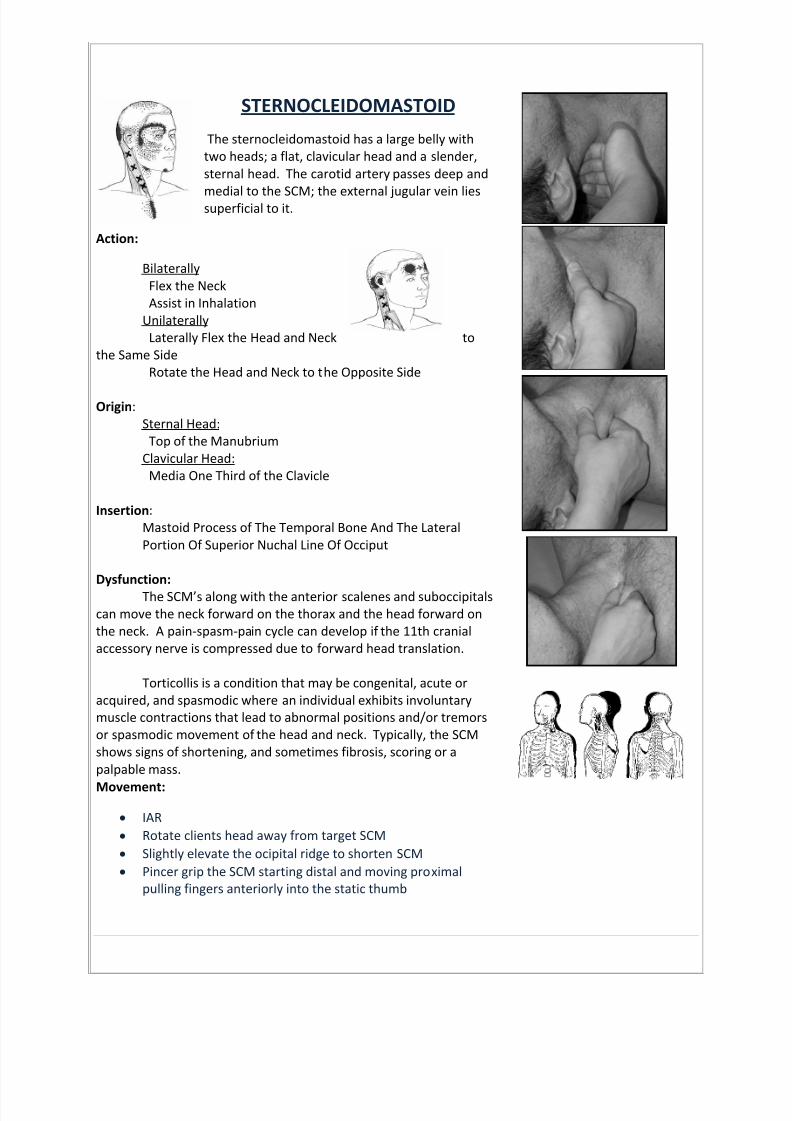
STERNOCLEIDOMASTOID
The sternocleidomastoid has a large belly withtwo heads; a flat, clavicular head and a slender,sternal head. The carotid artery passes deep and
medial to the SCM; the external jugular vein liessuperficial to it.
Action:
BilaterallyFlex the NeckAssist in Inhalation
UnilaterallyLaterally Flex the Head and Neck to
the Same SideRotate the Head and Neck to the Opposite Side
Origin :Sternal Head:
Top of the ManubriumClavicular Head:
Media One Third of the Clavicle
Insertion :Mastoid Process of The Temporal Bone And The LateralPortion Of Superior Nuchal Line Of Occiput
Dysfunction: The SCM’s along with the anterior scalenes and suboccipitals
can move the neck forward on the thorax and the head forward onthe neck. A pain-spasm-pain cycle can develop if the 11th cranialaccessory nerve is compressed due to forward head translation.
Torticollis is a condition that may be congenital, acute oracquired, and spasmodic where an individual exhibits involuntarymuscle contractions that lead to abnormal positions and/or tremorsor spasmodic movement of the head and neck. Typically, the SCMshows signs of shortening, and sometimes fibrosis, scoring or apalpable mass.
Movement:
IAR Rotate clients head away from target SCM Slightly elevate the ocipital ridge to shorten SCM Pincer grip the SCM starting distal and moving proximal
pulling fingers anteriorly into the static thumb

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 35/42
ANTERIOR SCALENES
There are three scalenes sandwichedbetween the SCM and the anterior flap ofthe trapezius. The anterior scalenes is
partially underneath SCM. The scaleneselevate the upper ribs during normalinhalation. The brachial plexus andsubclavian artery pass through a small gapbetween the anterior and middle scalenes
Action:Bilaterally
Elevate the Ribs during InhalationFlex the Head and Neck
UnilaterallyLaterally Flex the Head and Neck to the Same Side
Rotate the Head and Neck to the Opposite Side
Origin :Transverse Process of Third through Sixth Cervical Vertebrae
Insertion :First Rib
Dysfunction:When the brachial plexus and
subclavian artery are entrapped between the
anterior and middle scalene muscles a non-specific thoracic outlet syndrome called theanterior scalene syndrome occurs. As withpectoralis minor syndrome nerve compression is more common.
Movement:
Match clavicle angle with thumb or fingers Lift clients elbow anteriorly until clavicle “sucks” fingers
under accessing scalene attachments on ribs Gently oscillate on attachments while moving arm through
range of motion
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 36/42
SUBOCCIPITALS
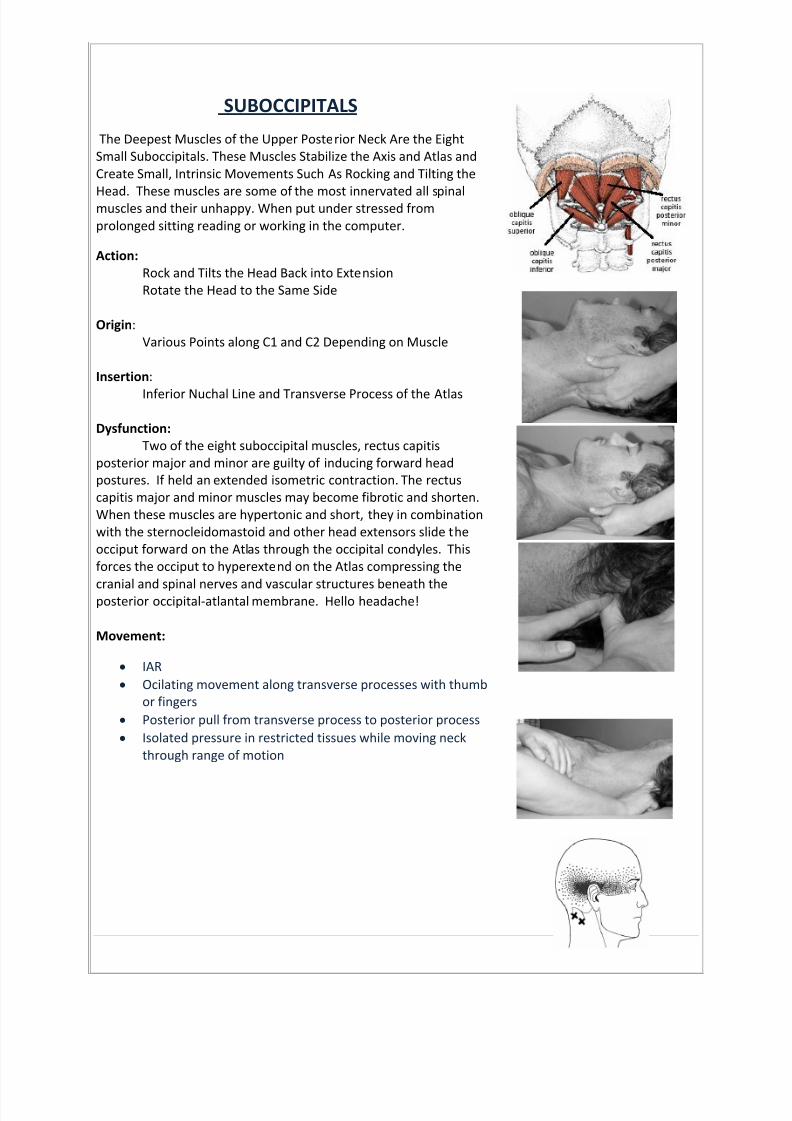
The Deepest Muscles of the Upper Posterior Neck Are the EightSmall Suboccipitals. These Muscles Stabilize the Axis and Atlas andCreate Small, Intrinsic Movements Such As Rocking and Tilting the
Head. These muscles are some of the most innervated all spinalmuscles and their unhappy. When put under stressed fromprolonged sitting reading or working in the computer.
Action:Rock and Tilts the Head Back into ExtensionRotate the Head to the Same Side
Origin :Various Points along C1 and C2 Depending on Muscle
Insertion :
Inferior Nuchal Line and Transverse Process of the Atlas
Dysfunction:Two of the eight suboccipital muscles, rectus capitis
posterior major and minor are guilty of inducing forward headpostures. If held an extended isometric contraction. The rectuscapitis major and minor muscles may become fibrotic and shorten.When these muscles are hypertonic and short, they in combinationwith the sternocleidomastoid and other head extensors slide theocciput forward on the Atlas through the occipital condyles. Thisforces the occiput to hyperextend on the Atlas compressing the
cranial and spinal nerves and vascular structures beneath theposterior occipital-atlantal membrane. Hello headache!
Movement:
IAR Ocilating movement along transverse processes with thumb
or fingers Posterior pull from transverse process to posterior process Isolated pressure in restricted tissues while moving neck
through range of motion

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 37/42
SUBSCAPULARIS
The subscapularis is one of four rotator cuffmuscles; it’s the only one that attaches to thehumerus’ lesser tubercle and acts as the
primary anterior support for theglenohumeral joint. It is located on thescapula' s anterior surface between the
subscapular fossa and the serratus anterior muscle.
Action:Medially Rotate the ShoulderStabilize the Head of the Humerus in the Glenoid Cavity
Origin :Subscapular Fossa of the Scapula
Insertion :Lesser Tubercle of the Humerus
Dysfunction:Together with pectoralis major latisisimusdorsi and teres major, subscapularismedially rotates the shoulder. When hypertonic, the increase inmedial rotation of the humerus causes increased protraction of thescapula rolling the shoulder forward and creating a classic slumpedposture. As subscapularis shortens the rhomboids lengthen andbecome weak and inhibited from reciprocal inhibition, therefore
increasing scapula protraction even more.
Movements:
Supineo Bring clients arm across body exposing lateral edge
of the scapulao Slide flat hand onto anterior scapula and holdo Take arm further across body anchoring scapula to
the table Sidelying
o Anchor elbow on anterior surface of the scapulao Bring arm anterior while resisting with anchored
elbow
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 38/42
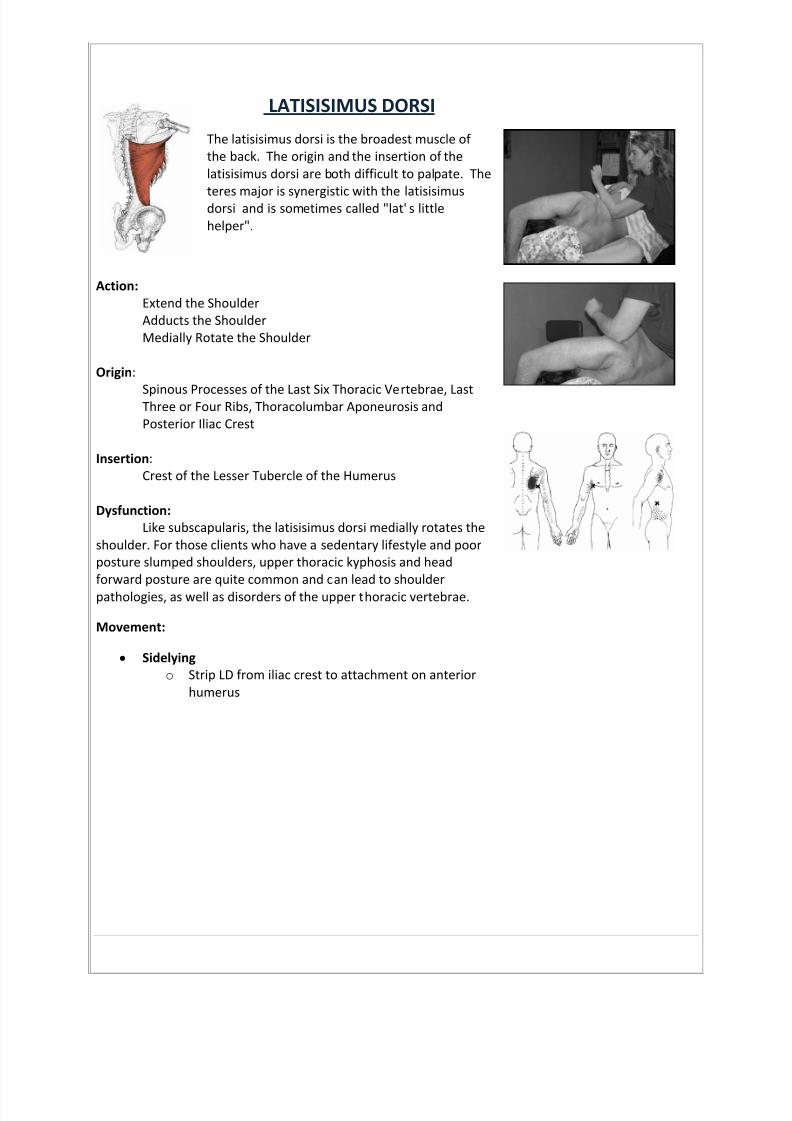
LATISISIMUS DORSI
The latisisimus dorsi is the broadest muscle ofthe back. The origin and the insertion of thelatisisimus dorsi are both difficult to palpate. The
teres major is synergistic with the latisisimusdorsi and is sometimes called "lat' s littlehelper".
Action:Extend the ShoulderAdducts the ShoulderMedially Rotate the Shoulder
Origin :
Spinous Processes of the Last Six Thoracic Vertebrae, Last Three or Four Ribs, Thoracolumbar Aponeurosis and Posterior Iliac Crest
Insertion :Crest of the Lesser Tubercle of the Humerus
Dysfunction:Like subscapularis, the latisisimus dorsi medially rotates the
shoulder. For those clients who have a sedentary lifestyle and poorposture slumped shoulders, upper thoracic kyphosis and headforward posture are quite common and can lead to shoulderpathologies, as well as disorders of the upper thoracic vertebrae.
Movement:
Sidelyingo Strip LD from iliac crest to attachment on anterior
humerus
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 39/42
Military neck
Sternocleidomastoid Unilaterally:
Laterally flex the head and neck to the same side Rotate the head and neck to the opposite side
Bilaterally: Flex the neck and assist in inhalation (elevation of the rib cage)
Longus capitis Unilaterally:
Laterally flex and rotate the head and neck to the same side Bilaterally:
Flex the head and neck Longus colli
Unilaterally: Laterally flex and rotate the head and neck to the same side
Bilaterally:
Flex the head and neck
Forward head
Scalenes Unilaterally:
With the ribs fixed, laterally flex the head and neck to the same side Rotate head and neck to the opposite side
Bilaterally: Elevate the ribs during inhalation Flex the head and neck
Splenius capitis Unilaterally:
Rotate the head and neck to the same side Laterally flex the head and neck
Bilaterally: Extend the head and neck
Upper trapezius – Bilaterally:
Extend the head and neck Unilaterally:
Laterally flex the head and neck to the same side Rotate the head and neck to the opposite side Elevate the scapula (scapulothoracic joint) Upwardly rotate the scapula
Semispinalis capitis- Extend the vertebral column and head
Hollow chest - the sternum is depressed, upper ribs are compressed, and shoulders are pulled forward

8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 40/42
2
Pectoralis major- All fibers:
Adduct and medially rotate the shoulder (glenohumeral joint) Assist in the elevating the thorax in forced inhalation
Upper fibers:
Flex the shoulder Horizontally adduct the shoulder Lower fibers:
Extend the shoulder Pectoralis Minor-
Depress and abduct the scapula (scapulothoracic joint) Tilt the scapula anteriorly
Subclavius- Draw clavicle inferiorly and anteriorly Elevate first rib (to assist in inhalation) Stabilize the sternoclavicular joint
Internal intercostals- Assist with exhalation by drawing the ribs inferiorly, decreasing the space of the thoracic cavity
Anterior deltoid – Flex, medially rotate, horizontally adduct Shoulder
Diaphragm - Draw down the central tendon of the diaphragm
Rectus abdominus - Flex the vertebral column
Rounded shoulders - shoulders are rotated medially
Upper trapezius – Bilaterally:
Extend the head and neck Unilaterally:
Laterally flex the head and neck to the same side Rotate the head and neck to the opposite side Elevate the scapula (scapulothoracic joint) Upwardly rotate the scapula
Lower trapezius- Depress the scapula (scapulothoracic joint) Upwardly rotate the scapula
Pectoralis major- All fibers:
Adduct and medially rotate the shoulder (glenohumeral joint) Assist in the elevating the thorax in forced inhalation
Upper fibers: Flex the shoulder Horizontally adduct the shoulder
Lower fibers: Extend the shoulder
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 41/42
3
Pectoralis Minor- Depress and abduct the scapula (scapulothoracic joint) Tilt the scapula anteriorly Anterior deltoid
Teres major- Extend, adduct and medially rotate the shoulder (glenohumeral joint)
Serratus anterior- Abduct and depress the scapula ( scapulothoracic joint)
Sagittal Plane Deviations
Lateral tilt of the head
Sternocleidomastoid- Unilaterally:
Laterally flex the head and neck to the same side Rotate the head and neck to the opposite side
Bilaterally: Flex the neck and assist in inhalation (elevation of the rib cage)
Scalenes Unilaterally:
With the ribs fixed, laterally flex the head and neck to the same side Rotate head and neck to the opposite side
Bilaterally: Elevate the ribs during inhalation Flex the head and neck
Upper trapezius – Bilaterally:
Extend the head and neck Unilaterally:
Laterally flex the head and neck to the same side Rotate the head and neck to the opposite side Elevate the scapula (scapulothoracic joint) Upwardly rotate the scapula
Levator scapula- Unilaterally:
Elevate and downwardly rotate the scapula Laterally flex the head and neck Rotate the head and neck to the at 830 same side
Bilaterally: Extend the head and neck
8/9/2019 Neck and Shoulder
http://slidepdf.com/reader/full/neck-and-shoulder 42/42
Notes: