ndis & learning from the uk experience of personalisation: a provider perspective peter...
TRANSCRIPT

NDIS & LEARNING FROM THE UK EXPERIENCE OF PERSONALISATION: A PROVIDER PERSPECTIVE
Peter [email protected]
© P. Gianfrancesco 2014

OVERVIEW
About meThe UK & ‘Personalisation’What we did well (and what we did wrong)
Insights arising from our experience
Lessons for NDIS providersMy emphasis is on the longer term view of market engagement
A provider emphasis and focus

GENERAL
NDIS concept exists elsewhere Implementation plans & progress are impressive
Not much written about ‘provider experience’
Most critical part of model is provider response
Observations about MH NFP sector in Oz Getting ‘fit’ for the NDIS will improve you
NDIS ‘fitness’ will result in a stronger NFP sector
England is a good place to learn from
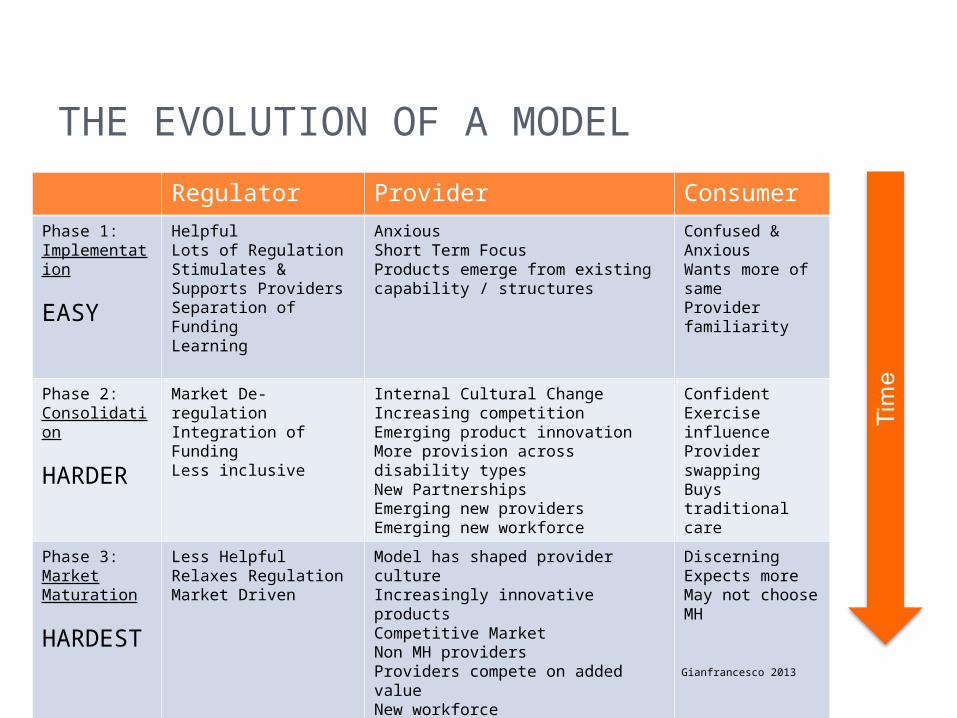
THE EVOLUTION OF A MODEL
Regulator Provider ConsumerPhase 1: Implementation
EASY
HelpfulLots of RegulationStimulates & Supports ProvidersSeparation of FundingLearning
AnxiousShort Term FocusProducts emerge from existing capability / structures
Confused & AnxiousWants more of sameProvider familiarity
Phase 2: Consolidation
HARDER
Market De-regulationIntegration of FundingLess inclusive
Internal Cultural ChangeIncreasing competitionEmerging product innovationMore provision across disability typesNew PartnershipsEmerging new providersEmerging new workforce
ConfidentExercise influenceProvider swappingBuys traditional care
Phase 3: Market Maturation
HARDEST
Less HelpfulRelaxes RegulationMarket Driven
Model has shaped provider cultureIncreasingly innovative productsCompetitive MarketNon MH providersProviders compete on added valueNew workforce
DiscerningExpects moreMay not choose MH
Gianfrancesco 2013

Over time………(if all goes well)
Regulators (the NDIA) relax control over market conditions (rules)
Consumers (customers) exercise more authority and discernment in relation to purchasing
Providers adapt, innovate and extend their markets

UK EXPERIENCE AS A PROVIDER

PERSONALISATION – THE ENGLISH EXPERIENCE
A national policy approach with strong political support Implementation devolved to 250+ Unitary Authorities Introduced on a national scale 5 years ago Tariffs and products (regulation) determined locally (with some exceptions) or by provider
Consumers ‘hold’ the budget (reality is different) or get a ‘notional’ budget
Brilliant when it is allowed to be used creatively (the Lathe example)
It has not worked that well in mental health because of the chaotic implementation and existing care planning biases
Being used to drive price down and eligibility up in some places
Implemented at a time of great financial austerity, loss of contracted care and regulatory capacity

Smaller providers demonstrated faster market entry, greater innovation and better quality but were often outlasted in the market (by larger providers) because of their more fragile infrastructure capacity, cash flow and (typically) higher supply costs
We should seek to counter this trend because quality, localism and innovation are critical to the success of the model

WHAT WOULD HAVE HELPED US
CLEAR NATIONAL TARRIFFS SUPPORT FOR PROVIDERS SUPPORT FOR CUSTOMERS INDEPENDENT CARE PLANNING BETTER TRANSITION FROM CONTRACTS BETTER PLANNING AND LESS MARKET CHAOS MORE STRATEGIC AND LESS REACTIVE SUPPLY TIME TO UNDERSTAND WHAT WE WERE DOING

WE SURVIVED AND THRIVED!
SO WHAT DID WE DO?
WHY US?

THE 5 C’SCultural confidence and readiness
Customer service and focus
Capability was understoodCapacity was identifiedCosts were known (eventually!)

CULTURAL CONFIDENCE & READINESSWho are we here for?Who could we be here for?What are the cultural barriers?
What values must we preserve?
What can we move on from?

CUSTOMER SERVICE & FOCUSWho are our customers?How do we reach them?How can we provide GREAT customer experience?
What do our customers tell us they want?
What more can we do to add value?

CAPABILITYWhat is it we ACTUALLY do?What is it that makes a difference?
What else are we good at?Who else might benefit?How willing are we to focus our development on the things that REALLY matter to customers?

CAPACITYHow much can we provide?How productive do we need to be?
How can we be more efficient?What new partnerships emerge?What are the markets we are seeking to appeal to?
What else do we need and how will we pay for it?

COSTS
How much does it cost us to supply?
Can we supply within the market tolerances?
Do we ‘loss lead’?Do we subsidise care?What assumptions do we make about our supply model?
What are our ‘lines in the sand’

KEY QUESTIONS WE CONTINUALLY ASKED….
Why are we considering entering this market?
What are our ambitions as a provider?Do we have a duty to supply?What happens if we choose not to?How does it fit with our organisational purpose?
Can we afford to do it?Do our values limit our market?What hidden capability is there?What would we do with the profit?How would we manage revenue loss?

OUR CONTEXT

IN NORFOLK, ENGLAND…
Population of 1 million people In any given year:*
120,000 people experience a mental health problem requiring help
45,000 see a GP ONLY15,000 use public or NGO mental health services
Less than 5,000 eligible for a personal budget
60,000 people may need help, get nothing or have no eligibility but many have a capacity and desire to purchase
The market opportunities here are pretty obvious?

WHAT WE DID….

WE….
Sought to engage with the larges market possible CONSISTENT with our values and purpose
For us this meant everyone? (Universality) We developed a broad product range We tested this with existing and potential customers
We packaged the offer differently for different markets? People with personal budget, employers, general public
We developed a safe but less qualified workforce? We went to market before we understood everything? We learnt about supply on the go and reviewed our offer continually

THE OFFER

Psychological Therapies Individual Recovery Support Complementary Therapies Learning & Personal Development Residential Care Wellness Retreats Befriending Personal Assistants Carer Support Condition Specific Packages (eg: Depression) Community Engagement Fitness & Nutrition Giving Back
Packaged and delivered through three distinct sub-brands

LIFEHELP Part of Norwich Mind (A$5M) New brand and product range developed
Psychosocial support, packages, psychological treatments, complementary therapies, training courses, nutrition, fitness, general wellbeing
Offered universally 600+ customers first two years 25% clients hold a personal budgets 40% have care purchased for them (notional budget) 25% self fund 10% free Profit is used to provide free care to 10% of the clients who would otherwise receive nothing

ADVANTAGES OF UNIVERSAL SUPPLY
Larger Market Less Stigma Less Regulation Greater Public Benefit & Impact & Reach Customer Expectations Higher Better Organisational Profile Fewer people excluded from available care Larger profit, greater potential to subsidise

The key things we learned

Staff are much more productive Staff are more flexible and multi-skilled Staff have become innovators and promoters The workforce is more diverse and more casualised
Volume matters as does a broad customer base Mixed economy of purchasers is critical MAXIMISING market size is key Financial planning and management is very complex
Client retention is good Clients say the service works and they welcome the choice
Staff are satisfied

11 insights

Mental Health NGOs often ‘punching below
their weight’

Our offer will always be 90% relational and
10% technical

There is very little product delineation amongst mental health providers - the key
difference, the real value is in the person you supply to assist the
customer


Market the ‘relational promise’

Celebrate and share success through story
telling…real people, real lives

Keep your values and history at the heart of your message and as the key driver for your
business model

Add ‘delight’ and value at every opportunity

Remember that customer experience is at least as important as efficacy for
most customers

Continually innovate and evolve your offer and expect others to
copy you

Listen carefully to what customers tell you before deciding what a ‘qualified
workforce’ is

Make part of your offer the opportunity for the customer to ‘pay it forward’, to give
back, to be involved

Supply Challenges – What we learned in the UK Our workforce had to increase productivity by 20% ‘Standing’ liability needs to be minimised Customers demand different qualities to those that organisations often hold dear….eg: Less qualified but experienced in life (not necessarily ‘lived experience)
Flexible and responsive Relationally competent
A new paradigm of staff deployment Move away from traditional structural model (teams) Multi-skilled staff covering full range of client needs are more efficient
Big increase in infrastructure demands Requires a different understanding of outcome Workforce has become more casual and/or self employed and generally operating at a lower level of qualification but with new sought after attributes
Organisational complexity increases Creativity needed to continually add value Greater reliance on technology to support distant delivery Very hard to supply remotely unless additional investment (by sponsor, provider, regulator or co-purchasing)
SUMMARY OF KEY POINTS It’s bloody hard! NDIS offers great opportunity BUT it should not be your only market
The implementation approach seems sound Providers need to think differently
In terms of who they supply to In terms of brand and marketing In terms of supply and productivity
Early to market is important Competition is inevitable and GOOD (particularly in urban settings)
Funding will be more complex and chaotic Customers will benefit if suppliers adapt Preparing for supply will improve your organisation

FURTHER INFORMATIONwww.norwichmind.org.uk
www.personalhealthbudgets.england.nhs.uk
www.mind.org.uk
www.scie.org.uk/topic/keyissues/personalisation
www.thinklocalactpersonal.org.uk
www.whitecoat.com.au
www.patientopinion.org.uk