ncpf: assessing early signals of efficacy to guide
TRANSCRIPT

NCPF: Assessing Early Signals of
Efficacy to Guide Clinical Development
Richard S. Finn, MD
Associate Professor of Medicine
Division of Hematology/Oncology
Co-director Signal Transduction and Therapeutics Program
Jonsson Comprehensive Cancer Center
Geffen School of Medicine at UCLA

Gefitinib: EGFR TKI
non-small cell lung cancer response

Nucleus
AngiogenesisMitogenesisInhibition of ApoptosisCytoskeleton changes
DNA
Transcription
Factors
COOH
ATP Activated RTK
Cell membrane
Differentiation
PI3-KPO-
AKT -OP
SHC
Grb2
SOS RAS
RAF
MEK
MAPK
PO-PLCγ
PKC
Epidermal Growth Factor Receptor (EGFR)

Human Protein Reference Database (www.hprd.org)450 genes
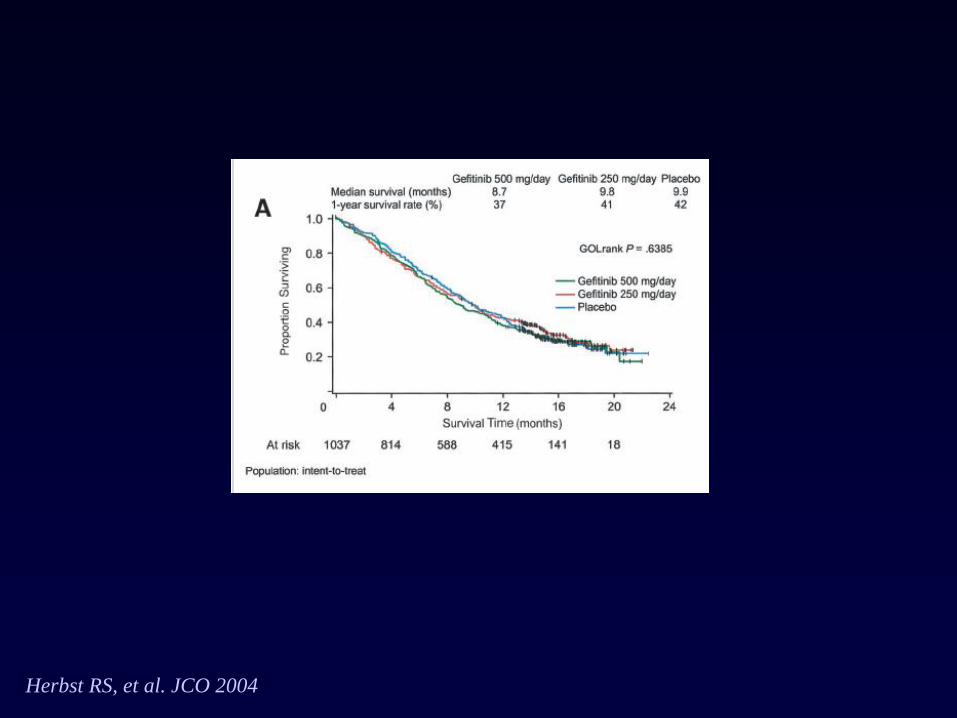
Herbst RS, et al. JCO 2004

Lynch etal NEJM 2004

Maemondo NEJM 2010

Molecularly Characterized Human Cancer Cell Lines
and Tissue Xenografts
Molecular CharacterizationDefine “target driven” disease
Target Expression
Target “activation”
Global expression profile
Biologic CharacterizationProliferation
Cell Cycle
Apoptosis
Novel Combinations
Correlate
Identify predictive markers for response/resistance
Downstream effects of agent
Identify non-empiric combinations for further
clinical development
Discovery
Early Clinical
Development
Phase II

Science 2014
10
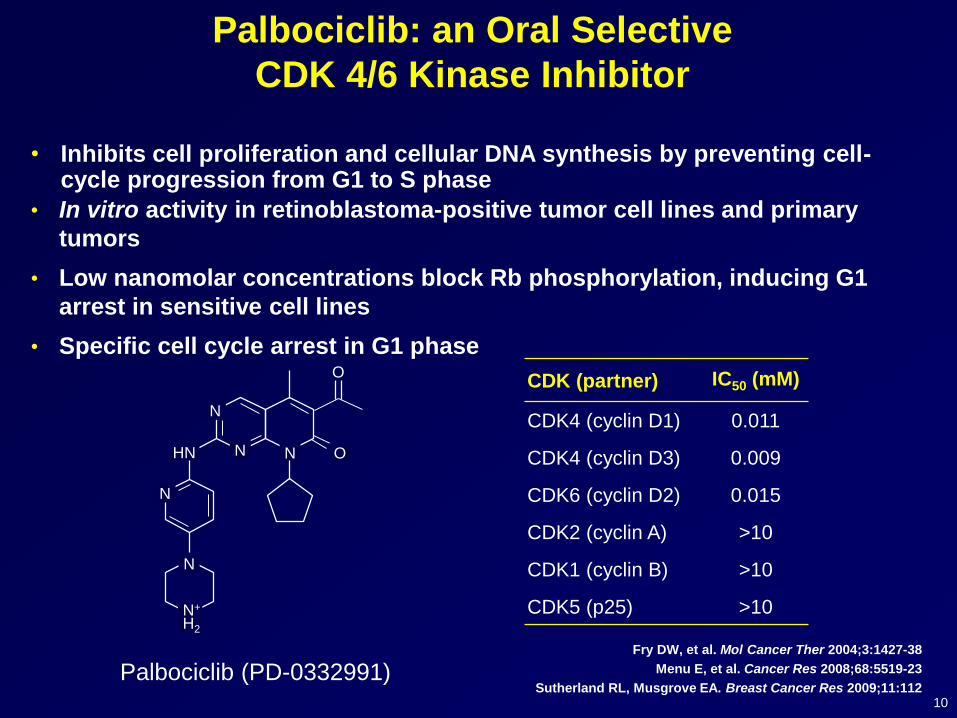
Palbociclib: an Oral Selective
CDK 4/6 Kinase Inhibitor
• Inhibits cell proliferation and cellular DNA synthesis by preventing cell-cycle progression from G1 to S phase
• In vitro activity in retinoblastoma-positive tumor cell lines and primary
tumors
• Low nanomolar concentrations block Rb phosphorylation, inducing G1
arrest in sensitive cell lines
• Specific cell cycle arrest in G1 phase
Fry DW, et al. Mol Cancer Ther 2004;3:1427-38
Menu E, et al. Cancer Res 2008;68:5519-23
Sutherland RL, Musgrove EA. Breast Cancer Res 2009;11:112Palbociclib (PD-0332991)
N
N
N
HN
N+
H2
O
ON
N
CDK (partner) IC50 (mM)
CDK4 (cyclin D1) 0.011
CDK4 (cyclin D3) 0.009
CDK6 (cyclin D2) 0.015
CDK2 (cyclin A) >10
CDK1 (cyclin B) >10
CDK5 (p25) >10


Trastuzumab
Chemotherapy
Anti-estrogens
15%
ER,PR,
HER2–
60%
ER+25%
HER2+
Sörlie T, et al. PNAS. 2001;98:10869-74

0
100
200
300
400
500
600
700
800
900
1000
MB-175
ZR75
-30
CAMA-1
MB13
4
HCC20
2
UACC-893
EFM
19
SUM19
0
EFM
192A
MB-361
HCC15
00
HCC14
19
HCC38
MB-415
MCF-
10A
UACC-812
HCC22
18
ZR75
-1
MDAMB45
3
184A
1
T47D
MCF7
BT-
20
MDAMB43
5
BT4
74
SKBR3
KPL-
1
HCC11
43
MDAMB23
1
HCC13
95
SUM-225
HS57
8T
184B
5
UACC73
2
CAL-51
BT5
49
COLO
824
DU44
75
HCC11
87
HCC15
69
HCC18
06
HCC19
37
HCC19
54
HCC70
MB-436
MB15
7
MDAMB46
8
Subtype
Luminal Non-luminal/post EMT
HER2 amplified Non-luminal
Immortalized
Palbociclib: CDK 4/6 Inhibitor – Breast Panel
Finn RS, et al. Breast Cancer Res. 2009;11(5):R77.

14
Palbociclib Acts Synergistically with
Tamoxifen in ER+ Breast Cancer Cell Lines
Tamoxifen 10000 5000 2500 1250 625 312
Palbociclib 100 50 25 12.5 6.25 3.125
100
80
60
40
20
0
Inh
ibitio
n (
%)
Concentration nM
Tamoxifen 5000 2500 1250 625 312
Palbociclib 50 25 12.5 6.25 3.125
100
80
60
40
20
0
Inh
ibitio
n (
%)
Concentration nM
Tamoxifen 5000 2500 1250 625 312
Palbociclib 50 25 12.5 6.25 3.125
100
80
60
40
20
0
Inh
ibitio
n (
%)
Concentration nM
MCF7CIm = 0.37±0.04
EFM19CIm = 0.45±0.09
T47D
CIm = 0.1±0.01
Palbociclib alone Tamoxifen alone Palbociclib/Tamoxifen combination
Finn RS, et al. Breast Cancer Res. 2009;11(5):R77
● Mean combination index (CIm) <1 indicates synergy for the combinations
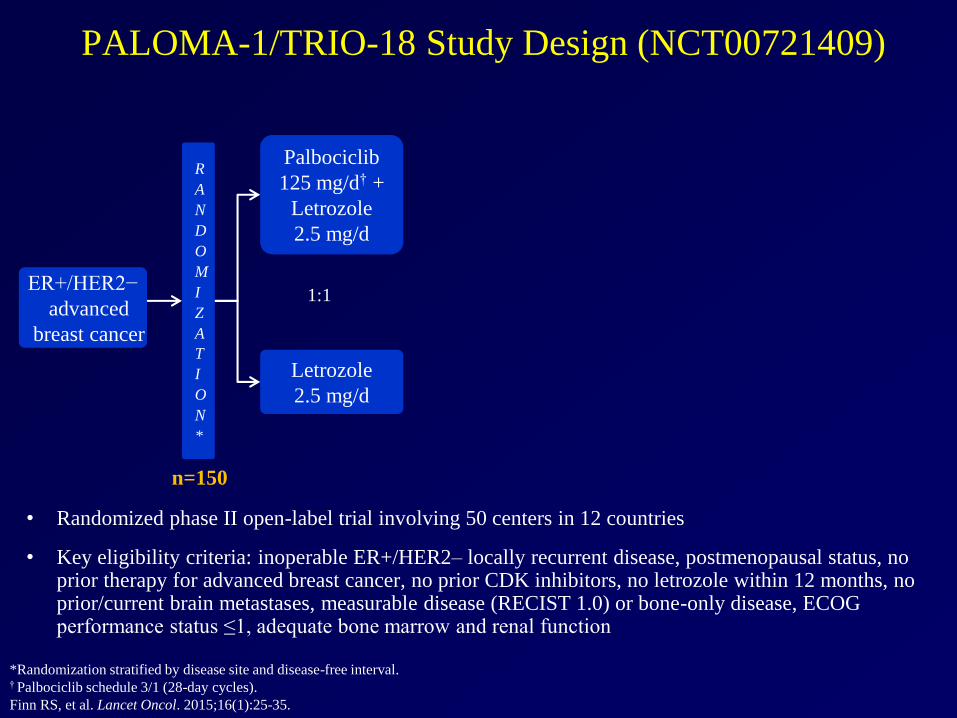
PALOMA-1/TRIO-18 Study Design (NCT00721409)
• Randomized phase II open-label trial involving 50 centers in 12 countries
• Key eligibility criteria: inoperable ER+/HER2– locally recurrent disease, postmenopausal status, no prior therapy for advanced breast cancer, no prior CDK inhibitors, no letrozole within 12 months, no prior/current brain metastases, measurable disease (RECIST 1.0) or bone-only disease, ECOG performance status ≤1, adequate bone marrow and renal function
Palbociclib
125 mg/d† +
Letrozole
2.5 mg/d
Letrozole
2.5 mg/d
ER+/HER2−
advanced
breast cancer
*Randomization stratified by disease site and disease-free interval.† Palbociclib schedule 3/1 (28-day cycles).
Finn RS, et al. Lancet Oncol. 2015;16(1):25-35.
1:1
R
A
N
D
O
M
I
Z
A
T
I
O
N
*
n=150

PALOMA-1/TRIO-18 Study Design (NCT00721409)
• Randomized phase II open-label trial involving 50 centers in 12 countries
• Key eligibility criteria: inoperable ER+/HER2– locally recurrent disease, postmenopausal status, no prior therapy for advanced breast cancer, no prior CDK inhibitors, no letrozole within 12 months, no prior/current brain metastases, measurable disease (RECIST 1.0) or bone-only disease, ECOG performance status ≤1, adequate bone marrow and renal function
Palbociclib
125 mg/d† +
Letrozole
2.5 mg/d
Letrozole
2.5 mg/d
ER+/HER2−
advanced
breast cancer
*Randomization stratified by disease site and disease-free interval.† Palbociclib schedule 3/1 (28-day cycles).
Finn RS, et al. Lancet Oncol. 2015;16(1):25-35.
1:1
R
A
N
D
O
M
I
Z
A
T
I
O
N
*
Palbociclib
125 mg/d† +
Letrozole
2.5 mg/d
Letrozole
2.5 mg/d
ER+/HER2−
advanced breast
cancer with
CCND1
amplification
and/or loss of
p16
1:1
n=66 n=99
R
A
N
D
O
M
I
Z
A
T
I
O
N
*
Cohort 1 Cohort 2

PFIZER CONFIDENTIAL
Progression-Free Survival
0 2 4 6 8 10 12 14 16 18 20 22 24 26Time, months
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pro
gre
ss
ion
-Fre
e S
urv
ival
Pro
bab
ilit
y
PD 0332991 + LET (N = 34),
Median PFS = 18.2 mo (CI, 12.6-)
LET (N = 32),
Median PFS = 5.7 mo (CI, 2.8-12.9)
Hazard ratio = 0.35
95% CI, 0.17-0.72
P = 0.006
34 30 27 25 24 21 17 13 10 6 2PD 0332991 + LET
32 22 15 11 9 8 8 7 5 3 3 1 1LET
Number of subjects at risk
Finn RS et al IMPAKT 2012

Progression-Free Survival
by Biomarker Status*
Population Comparison
Number
of
Patients
HR (95% CI) /
P value
Biomarker PositivePD 0332991 + Letrozole
vs. Letrozole
12
9
0.37 (0.10, 1.40) /
0.13
Biomarker NegativePD 0332991 + Letrozole
vs. Letrozole
10
15
0.19 (0.05, 0.67) /
<0.01
Biomarker Status
Unknown
PD 0332991 + Letrozole
vs. Letrozole
12
8
0.59 (0.11, 3.08) /
0.53
PD 0332991 + LetrozoleBiomarker Positive
vs. Biomarker Negative
12
10
1.42 (0.31, 6.43) /
0.65
LetrozoleBiomarker Positive
vs. Biomarker Negative
9
15
0.68 (0.24, 1.94) /
0.47
* CCND1 amplification and/or loss of p16.
18Finn RS et al IMPAKT 2012

PALOMA-1/TRIO-18: PFS (ITT Population)
0
10
20
30
40
50
60
70
80
90
100
Number at risk
Palbociclib plus letrozole
Letrozole
5
1
8
3
28
14
21
6
47
28
36
19
84
81
13
3
67
48
60
36
1
Palbociclib plus letrozole
Letrozole
HR 0.488 (95% CI 0.319–0.748; one-sided P = .0004)
Pro
gre
ssio
n-f
ree
surv
ival
, %
0 4 8 12 16 20 24 28 32 36 40
Time, months
Finn RS, et al. Lancet Oncol. 2015;16(1):25-35.
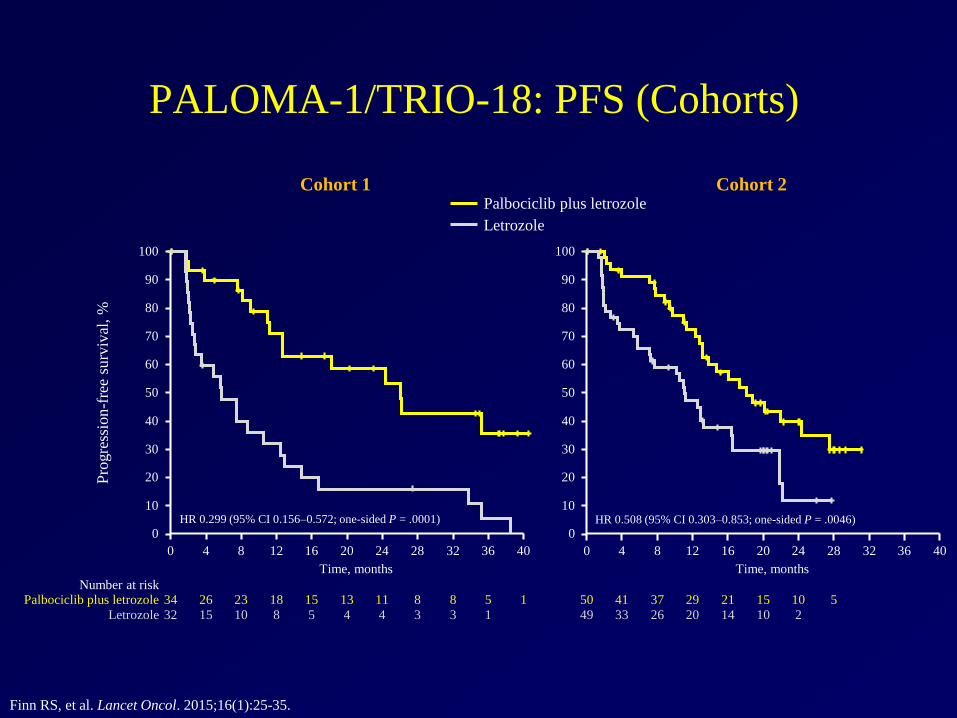
PALOMA-1/TRIO-18: PFS (Cohorts)
Cohort 1 Cohort 2
0
10
20
30
40
50
60
70
80
90
100
Pro
gre
ssio
n-f
ree
surv
ival
, %
Number at riskPalbociclib plus letrozole
Letrozole
5
1
8
3
13
4
11
4
18
8
15
5
34
32
8
3
26
15
23
10
1
HR 0.299 (95% CI 0.156–0.572; one-sided P = .0001)
Time, monthsTime, months
0
10
20
30
40
50
60
70
80
90
100
HR 0.508 (95% CI 0.303–0.853; one-sided P = .0046)
15
10
10
2
29
20
21
14
50
49
541
33
37
26
Palbociclib plus letrozole
Letrozole
0 4 8 12 16 20 24 28 32 36 40 0 4 8 12 16 20 24 28 32 36 40
Finn RS, et al. Lancet Oncol. 2015;16(1):25-35.
February 3rd 2015
• U.S. Food and Drug Administration (FDA) granted
accelerated approval of palbociclib (IBRANCE®)
• Indicated in combination with letrozole, for the treatment of
postmenopausal women with ER+/ HER2- advanced breast
cancer as initial endocrine-based therapy
• This indication is approved under accelerated approval based
on progression-free survival (PFS). Continued approval for
this indication may be contingent upon verification and
description of clinical benefit in a confirmatory trial
(PALOMA-2)


August 2007: in lab
Nov 2007: data shared
September 2008: Phase I open
November 2009: Phase II open
Development of Palbociclib:
First Approved CDK 4/6 Inhibitor
FDA Approved February 2015
Global Approval 2016
http://www.nejm.org/doi/pdf/10.1056/NEJMoa1609709
DOI: 10.1056/NEJMoa1609709

Kinase IC50 (nM)*
hCDK4 / cyclinD1 2.0
hCDK6 / cyclinD1 9.9
hCDK1 / cyclinB1 1627.0
hCDK9 / cyclinT1 57.0
hPIM1 50.0
*Abemaciclib mesylate
Abemaciclib (LY2835219)

Change in Tumor Size
(Part D, Abemaciclib)
NCT01394016
a3 non-evaluable patients are not shown. All patients in Part D were
required to have measurable disease. † Patient progressing on endocrine therapy before study entry and continued on that specific therapy
* Indicates HER2+ Tolaney et al. SABCS 2014

October 8th 2015
• U.S. Food and Drug Administration (FDA) granted
“Breakthrough Therapy Designation” as monotherapy for heavily
pre-treaetd patients with refractory hormone-receptor-positive
advanced breast cancer


Genomic Data by Breast Subtype
TCGA Nature 2012
Conclusions:
• The greatest advances in patient outcomes
have come from integrating biology into
clinical care
• Critical use of pre-clinical models can help
guide this process
• Generate hypothesis driven phase 1/2
studies

Canada
P Desjardins, H Lim
France
F Priou, P Soulie
Germany
W Abenhardt, M Clemens, J Ettl, C
Hanusch, A Kirsch, M Schmidt, V
Schulz, C Thomssen
Italy
D Amadori
Ukraine
I Bondarenko, S
Kulyk, Y Shparyk,
N Voytko
Russia
M Kopp, O Lipatov,
S Tjulandin, V
Vladimirov
Spain
M Ruiz Borrego, EM
Ciruelos Gil, JM Gil Gil, MJ
Vidal Losada, M Ramos
Vazquez
Hungary
K Boer, J Erfan, L
Landherr, I Lang, T
Pinter, A Weber, M
Wenczl
US
J Blum, D Chan, R
Dichmann, R Finn,
E Hu, W Lawler, A
Montero, R Patel, N
Robert, A Thummala
South Africa
M Coccia-Portugal
South Korea
SA Im, JS Ro
Ireland
J Crown, M Kennedy,
J McCaffrey, C
Murphy
This study is sponsored and funded by Pfizer Inc.
Acknowledgements

Acknowledgements
Canada
P Desjardins, H Lim
France
F Priou, P Soulie
Germany
W Abenhardt, M Clemens, J Ettl, C
Hanusch, A Kirsch, M Schmidt, V
Schulz, C Thomssen
Italy
D Amadori
Ukraine
I Bondarenko, S
Kulyk, Y Shparyk,
N Voytko
Russia
M Kopp, O Lipatov,
S Tjulandin, V
Vladimirov
Spain
M Ruiz Borrego, EM
Ciruelos Gil, JM Gil Gil, MJ
Vidal Losada, M Ramos
Vazquez
Hungary
K Boer, J Erfan, L
Landherr, I Lang, T
Pinter, A Weber, M
Wenczl
US
J Blum, D Chan, R
Dichmann, R Finn,
E Hu, W Lawler, A
Montero, R Patel, N
Robert, A Thummala
South Africa
M Coccia-Portugal
South Korea
SA Im, JS Ro
Ireland
J Crown, M Kennedy,
J McCaffrey, C
Murphy
The Patients and
Their Families
Network of
Investigators and
Study StaffRevlon-UCLA Women's
Cancer Research Program
Department of Defense
Innovator Award
This study is sponsored and funded by Pfizer Inc.

UCLA
Dylan Conklin
Andrew Kalous
Judy Dering
Sara Hurvitz
Meghan Brennan
Dennis Slamon
TRIO
Mary-Ann Lindsay
Matthieu Rupin
Valerie Bee
Pfizer
Sindy Kim
Sophia Randolph
Camilla Fowst
Eric Kowak
Eric Gauthier
Yuqiu (John) Jiang
Cynthia Huang
Maria Koehler
Mace Rothenberg
Gary Nichols
Acknowledgements