natural history of acute stroke from large vessel
TRANSCRIPT

Vallabh Janardhan, MD
Director, Texas Stroke Institute
Director, Comprehensive Stroke Program and Neuro-
Interventional Services, HCA North Texas Division
Natural history of acute stroke
from large vessel occlusion:
Results from the FIRST trial

Presenter Disclosure
FIRST Trial, Penumbra, Inc: Speakers Bureau
Principal Investigator
Data Safety Monitoring Board Member, Penumbra Pivotal Trial, Penumbra Inc.,
Consultant
Board Member, Insera Therapeutics Inc.,
Stocks/Stock Options
National Science Foundation Grant #0946099
Principal Investigator

FIRST Trial: Results 1
FIRST Cohort: Comparison with IMS 3
2
FIRST Cohort: Lessons learned about Infarct Core 3
Overview
FIRST Trial: Team 4
FIRST Trial: Results
FIRST Trial: Purpose
Termination of the IMS 3 trial due to futility has
led to further controversies surrounding the use
of IA endovascular therapy for stroke
intervention
Objective:
To assess the natural history of a stroke cohort
eligible for IA intervention and compare its
outcome with the IMS 3 results

Methods
Prospective, single arm, multi-center natural history study of a stroke cohort with the following inclusion criteria:
Large vessel occlusion
Present within 8 hours from symptom onset
Baseline NIHSS score ≥ 10
Ineligible or refractory to lytic therapy
Untreated with endovascular therapy
Interim analysis from 93 patients meeting study criteria
Primary endpoint is functional outcome at 90 days as defined by mRS 0-2
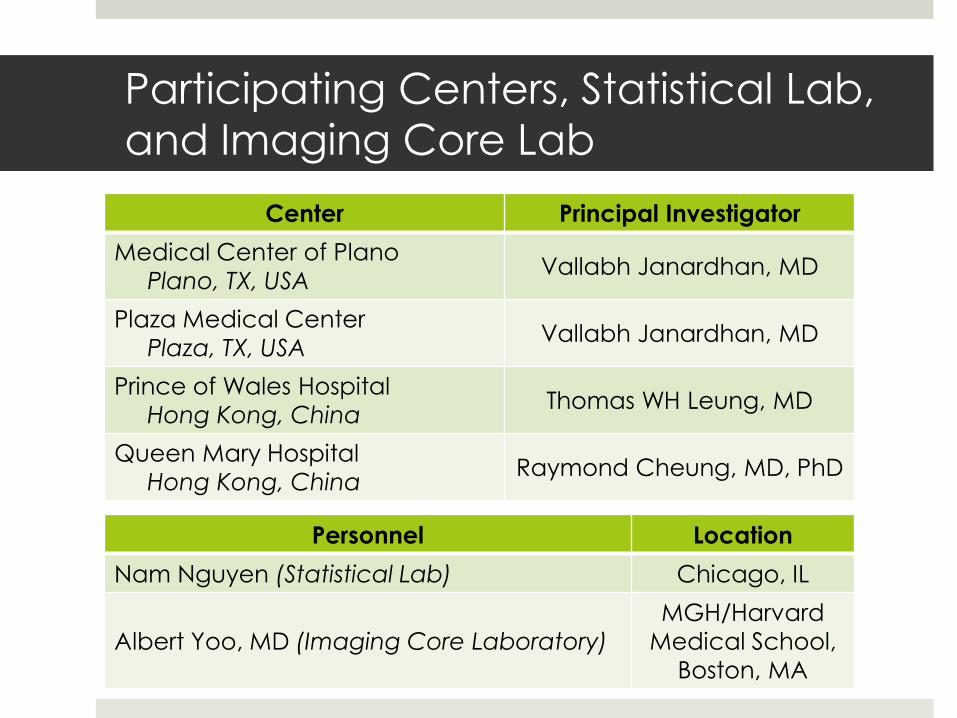
Participating Centers, Statistical Lab,
and Imaging Core Lab
Center Principal Investigator
Medical Center of Plano
Plano, TX, USA Vallabh Janardhan, MD
Plaza Medical Center
Plaza, TX, USA Vallabh Janardhan, MD
Prince of Wales Hospital
Hong Kong, China Thomas WH Leung, MD
Queen Mary Hospital
Hong Kong, China Raymond Cheung, MD, PhD
Personnel Location
Nam Nguyen (Statistical Lab) Chicago, IL
Albert Yoo, MD (Imaging Core Laboratory)
MGH/Harvard
Medical School,
Boston, MA

Target Vessel Location
MCA
ICA
ACA
Other
N=64/93
68.8%
N=1/93
1.1%
N=27/93
29.0%
N=1/93
1.1%

FIRST Baseline Characteristics
Patients (N) 93
Age (years) [mean/(SD)] 68.9 ± 14.9
Female 59.1% (55/93)
NIHSS [median/(IQR)] 18.0 (14.0-23.0)
TIMI 0-1 100% (93/93)
TICI 0-1 100% (93/93)
Refractory to IV rtPA 51.6% (48/93)
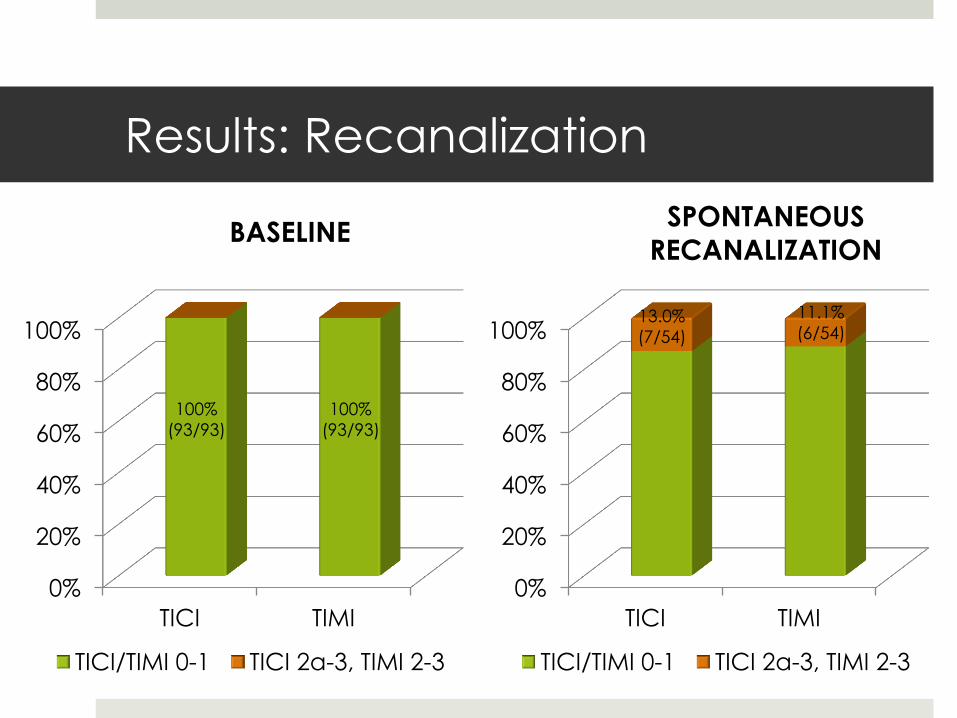
Results: Recanalization
0%
20%
40%
60%
80%
100%
TICI TIMI
TICI/TIMI 0-1 TICI 2a-3, TIMI 2-3
0%
20%
40%
60%
80%
100%
TICI TIMI
TICI/TIMI 0-1 TICI 2a-3, TIMI 2-3
BASELINE SPONTANEOUS
RECANALIZATION
100%
(93/93)
100%
(93/93)
11.1%
(6/54) 13.0%
(7/54)

Safety Results
Event Rate
All-Cause Mortality 39.8% (37/93)
All SAEs within 24 hrs of
stroke onset 26.9% (25/93)
Event Rate
Symptomatic ICH 5.4% (5/93)
Asymptomatic ICH 16.1% (15/93)
Total ICH 21.5% (20/93)
*29 events in 25 patients

Summary of SAEs within 24 hrs of Stroke Onset
Event % (n/N)
Cerebral Edema 7.5% (7/93)
Herniation Syndrome 1.1% (1/93)
Sequelae of CVA 4.3% (4/93)
Seizures 1.1% (1/93)
Respiratory Failure 6.5% (6/93)
Other Non-neurologic SAE 10.8% (10/93)
*29 events in 25 patients
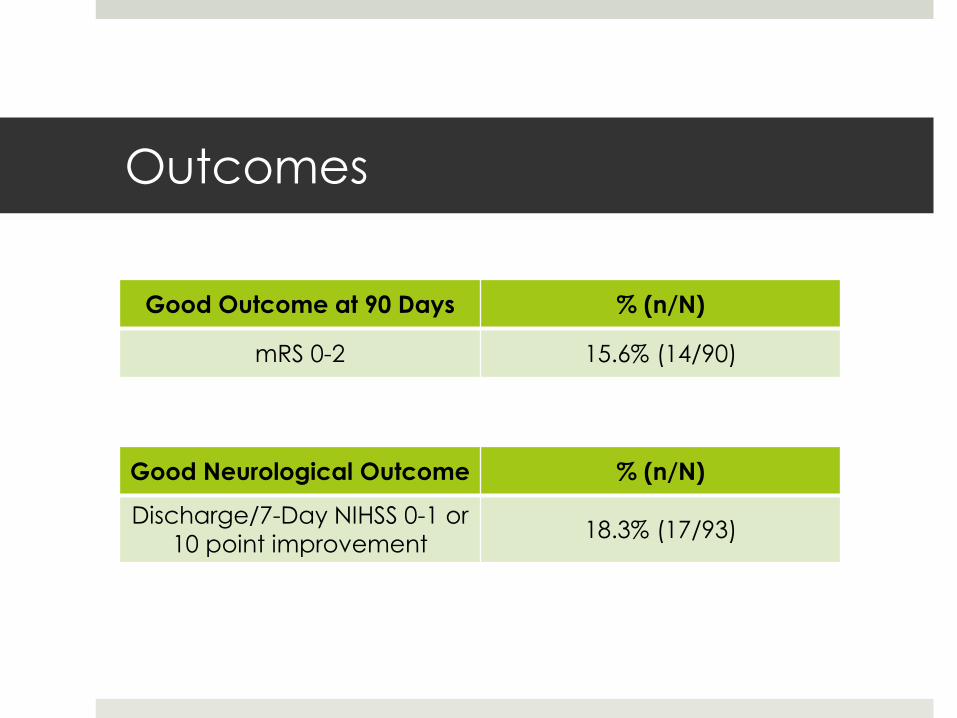
Outcomes
Good Neurological Outcome % (n/N)
Discharge/7-Day NIHSS 0-1 or
10 point improvement 18.3% (17/93)
Good Outcome at 90 Days % (n/N)
mRS 0-2 15.6% (14/90)

Outcome: Patients refractory to IV
tPA vs. Patients ineligible for IV tPA
Refractory to IV tPA
N=48
Ineligible for IV tPA
N=45
Recanalization 20.0% (6/30) 4.2% (1/24)
ICH (within 24 hrs) 16.7% (8/48) 15.6% (7/45)
Mortality 33.3% (16/48) 46.7% (21/45)
Discharge/7-Day NIHSS 0-1
or 10 point improvement 22.9% (11/48) 13.3% (6/45)
90-day mRS 0-2 21.7% (10/46) 9.1% (4/44)

FIRST Cohort: Comparison with IMS 3
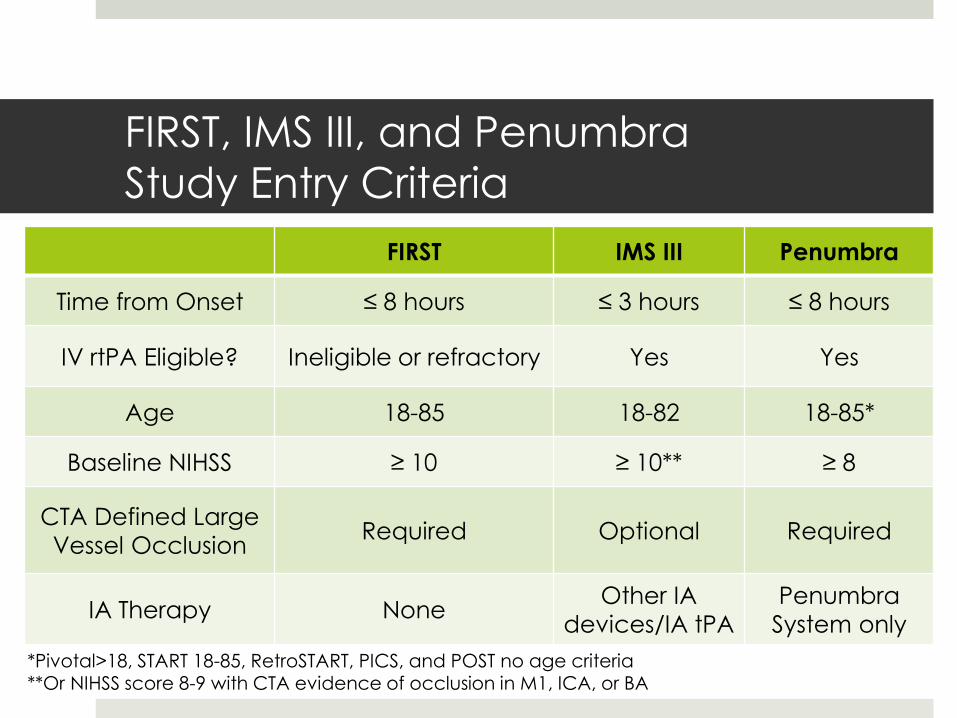
FIRST, IMS III, and Penumbra
Study Entry Criteria
FIRST IMS III Penumbra
Time from Onset ≤ 8 hours ≤ 3 hours ≤ 8 hours
IV rtPA Eligible? Ineligible or refractory Yes Yes
Age 18-85 18-82 18-85*
Baseline NIHSS ≥ 10 ≥ 10** ≥ 8
CTA Defined Large
Vessel Occlusion Required Optional Required
IA Therapy None Other IA
devices/IA tPA
Penumbra
System only
*Pivotal>18, START 18-85, RetroSTART, PICS, and POST no age criteria **Or NIHSS score 8-9 with CTA evidence of occlusion in M1, ICA, or BA
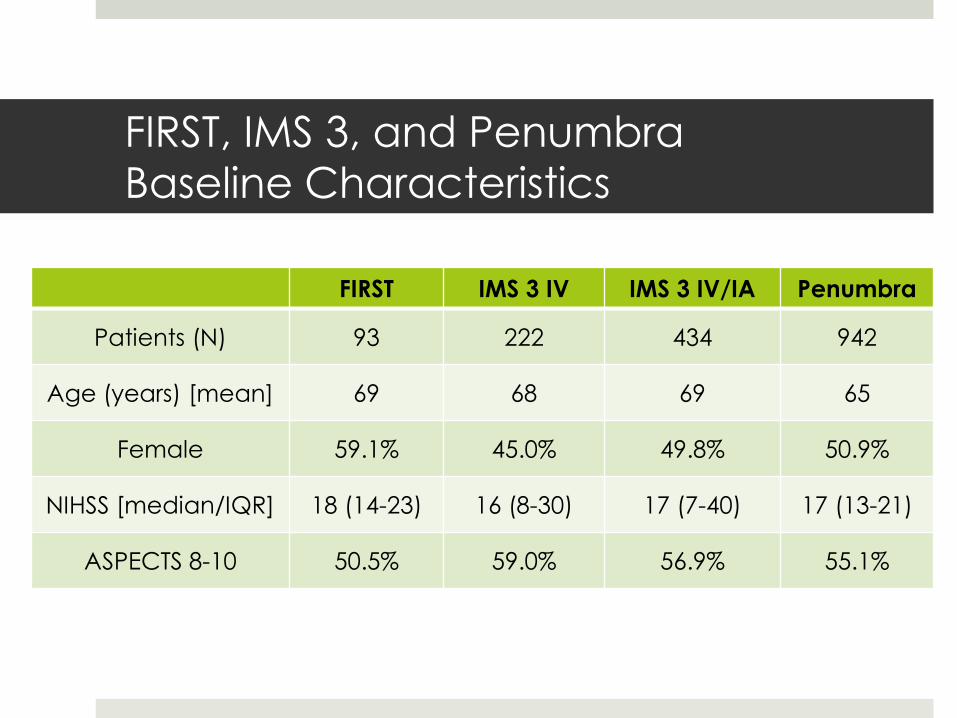
FIRST, IMS 3, and Penumbra
Baseline Characteristics
FIRST IMS 3 IV IMS 3 IV/IA Penumbra
Patients (N) 93 222 434 942
Age (years) [mean] 69 68 69 65
Female 59.1% 45.0% 49.8% 50.9%
NIHSS [median/IQR] 18 (14-23) 16 (8-30) 17 (7-40) 17 (13-21)
ASPECTS 8-10 50.5% 59.0% 56.9% 55.1%

FIRST, IMS 3, and Penumbra
Outcomes
FIRST
(N=93)
IMS 3 IV
(N=222)1
IMS 3 IV/IA
(N=434)1,2
Penumbra
(N=942)
TICI 2-3 13.0% 34.8%** 76.0%** 83.2%**
sICH 5.4% 5.9% 6.2% 12.6%*
Mortality 39.8% 21.6%** 19.1%** 21.7%**
90-Day mRS 0-2 15.6% 38.7%** 40.7%** 38.3%**
1Broderick JP, Palesch YY, Demchuk AM, et al. Endovascular Therapy after Intravenous t-PA versus t-
PA Alone for Stroke. N Engl J Med 2013;368:893-903. 2Tomsick TA, IMS III Investigators. IMS III: Comparison of Outcome by IA Approach and Interpretation
in Light of Comparative Trials. In: International Stroke Conference; Honolulu, Hawaii; 2013.
*P<0.05; **P<0.01 compared to FIRST, Fisher’s Exact two-sided test

Discussion
Large vessel acute ischemic stroke is a
malignant disease wherein 81.7% of patients will
either die or suffer long-term disabilities if
untreated (81.7% at 7 days; 84.4% at 90 days).
Endovascular therapy for large vessel occlusion
is safe and effective when compared to
medical therapy in an appropriate stroke
cohort ineligible or refractory to IV rtPA

FIRST Cohort: Lessons learned about
Infarct Core

Importance of Core Infarct Volume in
the Number Needed to Treat
Infarct core has been theorized to be an
important indicator for treatment success from
endovascular intervention in acute ischemic
stroke from large vessel proximal occlusion.
Objective:
To determine the extent to which it contributes to
the number of patients needed to treat (NNT) to
achieve long-term functional independence.
Zaidat O, Yoo A, Janardhan V, Frei D, Ammar L, Meyer D, To C, Kuo SS, Buell H, Barraza L, Bose A, Sit SP. The Importance of Core Infarct Volume in
the Number Needed to Treat in Endovascular Therapy for Acute Ischemic Stroke. Presented at SNIS, Colorado Springs, CO, July 2014.
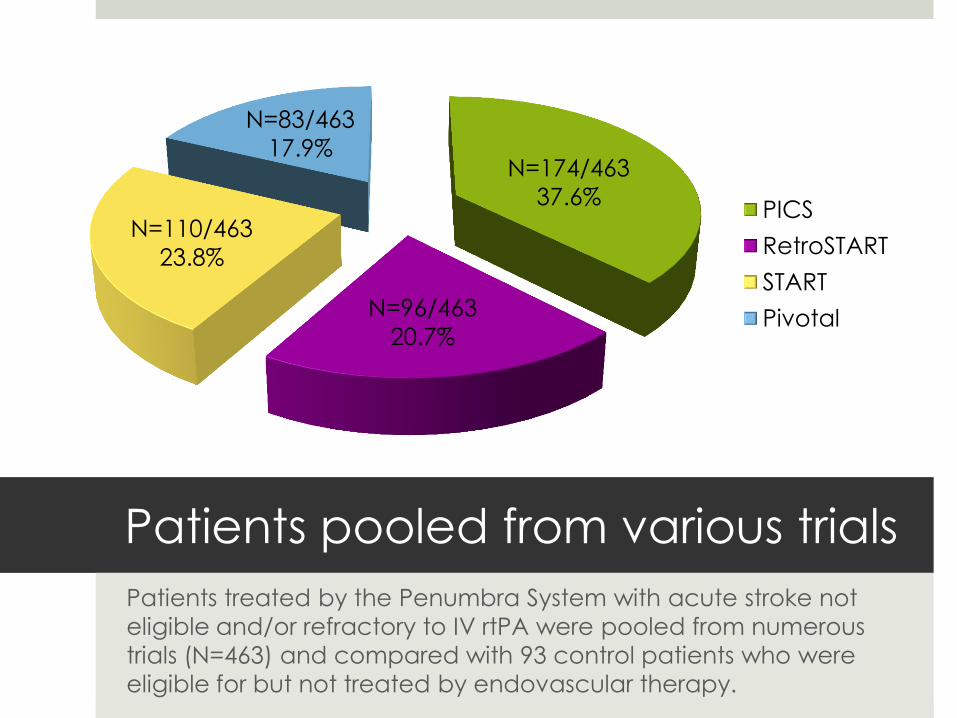
Patients pooled from various trials
Patients treated by the Penumbra System with acute stroke not
eligible and/or refractory to IV rtPA were pooled from numerous
trials (N=463) and compared with 93 control patients who were
eligible for but not treated by endovascular therapy.
PICS
RetroSTART
START
Pivotal
N=174/463
37.6%
N=96/463
20.7%
N=83/463
17.9%
N=110/463
23.8%

ASPECTS Distribution
Small
Medium
Large
N=257/463
55.5% N=155/463
33.5%
N=51/463
11.0%
N=29/84
34.5%
N=41/84
48.8%
N=14/84
16.7%
Note: 9 control patients did not have ASPECTS score.
CONTROL (N=93) PENUMBRA (N=463)

Outcomes Control (N=93) and Penumbra System (N=463)
TIMI 2-3 % (n/N)
sICH % (n/N)
Mortality % (n/N)
90-Day mRS 0-2 % (n/N)
Control Penumbra Control Penumbra Control Penumbra Control Penumbra
Overall 12.0% (6/50)
81.7%*** (376/460)
6.5% (6/93)
14.0% (65/463)
36.6% (34/93)
25.9%* (120/463)
12.9% (9/70)
38.4%*** (178/463)
ASP
8-10
8.3%
(2/24)
79.2%***
(202/255)
0.0%
(0/41)
11.7%*
(30/257)
41.5%
(17/41)
21.4%**
(55/257)
20.0%
(7/35)
42.8%**
(110/257)
ASP
5-7
11.1%
(2/18)
86.4%***
(133/154)
10.3%
(3/29)
16.1%
(25/155)
41.4%
(12/29)
24.5%
(38/155)
7.4%
(2/27)
41.3%***
(64/155)
ASP
0-4
12.5%
(1/8)
80.4%***
(41/51)
14.3%
(2/14)
19.6%
(10/51)
28.6%
(4/14)
52.9%
(27/51)
0.0%
(0/8)
7.8%
(4/51)
*P-value<0.05 **P-value<0.01 ***P-value<0.001 for Penumbra treatment as compared to control using Fishers Exact Test

Outcome: 90-Day mRS 0-2 Control (N=70) and Penumbra System (N=463)
0.0% (0/8)
7.4% (2/27)
20.0% (7/35)
12.9% (9/70)
7.8% (4/51)
41.3% (64/155)***
42.8% (110/257)**
38.4%(178/463)***
0.0 10.0 20.0 30.0 40.0 50.0
Large (0-4)
Medium (5-7)
Small (8-10)
Overall
Penumbra
Control
90-Day Good Outcome %
ASP
EC
TS G
rou
p
*P-value<0.05
**P-value<0.01
***P-value<0.001 for Penumbra treatment as compared to control using Fishers Exact Test
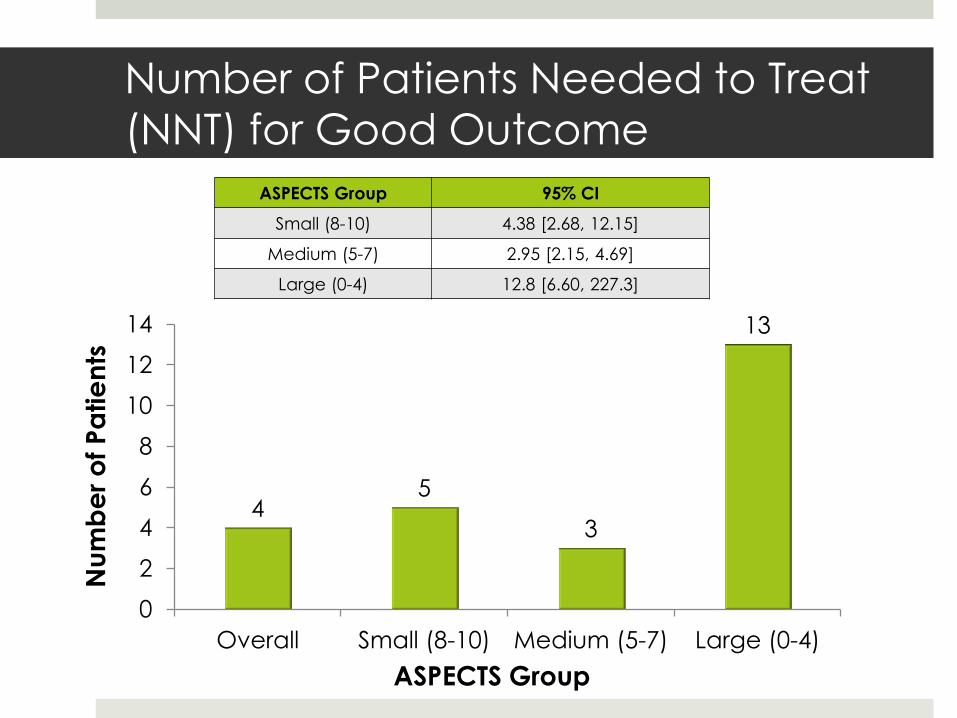
Number of Patients Needed to Treat
(NNT) for Good Outcome
4 5
3
13
0
2
4
6
8
10
12
14
Overall Small (8-10) Medium (5-7) Large (0-4)
ASPECTS Group
Nu
mb
er
of
Pa
tie
nts
ASPECTS Group 95% CI
Small (8-10) 4.38 [2.68, 12.15]
Medium (5-7) 2.95 [2.15, 4.69]
Large (0-4) 12.8 [6.60, 227.3]
Discussion
Data confirms that endovascular therapy may
not be as successful in patients with large
infarct core
Leads to high NNT
Excluding this group may lower overall NNT and
improve response rate of this therapy

FIRST Trial: The Team

FIRST Trial: Texas Stroke Institute Physician Team
Chandril Chugh, MD Alex Venizelos, MD Keyur Patel, MD Suman Nalluri, MD
TSI Stroke & Neuro-critical Care Physicians
Parita Bhuva, MD Ryan Gianatasio, MD Paul A. Hansen, MD Vallabh Janardhan, MD
Director, TSI
TSI Stroke Intervention Physicians
Tanzila Shams, MD
TSI Research Fellow
Texas Stroke Institute Administrative Team
Kathy Sheets
VP, HCAPS
Will Smitham
VP, HCAPS
Operations
Josh Canfield
TSI Practice Manager
Mark Whitley
Sr. VP Bus. Dev.
Dana Davis
TSI Clinical
Coordinator
Helen Hare
Program Coordinator
Anita Guthmann
Director,
Comprehensive Stroke
Rubina Muzina, MD MPH,
Supervisor, Research
Office, Plaza Medical
Center of Fort Worth
Prof. Raymond Cheung
Rosalind Ge
Queen Mary Hospital
Prince Wales Hospital Dr. Thomas Leung
Roxanna Liu
Synapse Therapeutics (CRO)
Clinton Wong Irene Hung Karen Chan
Core Lab
Dr. Albert Yoo
Penumbra, Inc.
Siu Po Sit
Lynne Ammar
Denise Meyer
Leticia Barraza
Jessica Harpel
Susana S. Hak
Yosephine Lumintang
Sophia S. Kuo
Nam Nguyen
Hope Buell
Dawn Ueda

Q&A