national tb program (ntp) th edition tuberculosis tuberculosis.pdf · 384 tuberculosis thcpm 7...
TRANSCRIPT

383
CPM 7th EDItION tUBERCULOSIS
National Center for Disease Prevention and ControlDepartment of Health San Lazaro Compound, Rizal Avenue, Sta. Cruz, ManilaTelephone No: 743-8301 loc.2350/2352
NATIONAL TB PROGRAM (NTP) Staff
DirectorIII Jaime Y. Lagahid, M.D., M.P.H. MedicalSpecialistIV Rosalind G. Vianzon, M.D., M.P.H. MedicalSpecialistIV Vivian S. Lofranco, M.D. MedicalSpecialistIV AnnaMarieCelinaG.Garfin,M.D. MedicalSpecialistII Ernesto A. Bontuyan, Jr., M.D. Supervising Health Program Officers Cirila D. Negad, R.N., MAN Ma. Arlene T. Rivera, M.M.D.M. Senior Health Program Officers Agnes Ma. Oliva V. Del Rosario, R.N.D., M.P.S-FNP Ferdinand Lala Puebla, BSSC., M.A.Candidate
National TB Program (NTP)

384
tUBERCULOSIS CPM 7th EDItION
Algorithm for Flow of NTP Activities
TB inCommunity
Symptoms:• Cough for 2 weeks or more• With or without expectoration• Fever•Significantweightloss• Hemoptysis• Chest and/or back pains
Case FindingsSputum specimens
(3 specimens) with request
form for sputum examination
Microscopy centerResults of the sputum smear examination
(sputum - smear examination for
diagnosis)
1
2
3
4
Figure 1
Diagnosispositive?
Y
5
Initiation of treatment
6
Refer the patient to MHO
(Municipal HealthOfficer)
for further assessment
N8
Case holding with DOTS Sputum specimens (3 specimens) with request
form for sputum examination
7
Go to # 4.
9
10
Treatmentcomplete?
Y
N
11
Report treatment outcome.
Continue monitoring
and supervision.

385
CPM 7th EDItION tUBERCULOSIS
Algorithm for the Diagnosis of Pulmonary Tuberculosis
Collect three (3) sputum specimens.
TB symptomatic(Cough for 2
weeks or more)
2 or 3 smear positive?
Classify as smear-
positive TB. See Tables 1
and 3.
only one (1) smear positive?
See Figure 3.
Collect another
3 sputum specimen
immediately.
at least one (1) smearpositive?
Classify as smear
positive TB.
Request for chest x-ray
(CXR).
Classify as smear
positive TB
Is it consistent with
active TB?
Figure 2
Observation/ further exam,
if necessary
1
2
3
6 7 8
4
5
9
1110
12
Y
N
N
Y Y
N
Y
N

386
tUBERCULOSIS CPM 7th EDItION
Algorithm for the Diagnosis of Smear-Negative Pulmonary Tuberculosis
Refer to MHO (symptomatic treatment for 2-3 weeks)
All 3 smear
If symptoms persists, collect another three (3) sputum specimens
2 or 3 smear positive?
Classify as smear-
positive TB. See Tables 1,
and 3.
only one (1) smear positive?
See Figure 2, # 5.
All 3 smear negative See Figure 3a.
4 5
6
7
3
1
2
Figure 3
Y
Y
N
N

387
CPM 7th EDItION tUBERCULOSIS
All 3 smear negative
abnormal findingson
CXR?
CXR
Refer to TB Diagnostics Committee
consistent with active
TB?
Classify as smear-
negative TB. See Tables 1
and 3.
observation / further
exam
observation/ further exam
Figure 3a
1
4
2
5
3
6 7
N
Y
Y
N
8

388
tUBERCULOSIS CPM 7th EDItION
NtP treatment Card(tobeaccomplishedbytheRuralHealthMidwives(RHM))/Nurse
Record o f the ind iv idual patients• TB Case number•Classification,typeand
regimen• Sputum examination results on diagnosis, for follow-up• Drug collection• Defaulter action
Algorithm for Guide to Ensure Treatment
TB Patient
positive muco-purulent, salivary
specimen?
Refer to RHM
NtP tB Register(tobeaccomplishedbythePublicHealthNurse(PHN))
Record of treatment Activity in the RhU (Rural health Unit)• TB case number•Classification,typeandregimen• Sputum examination results on diagnosis and for follow-up• Defaulter action• Treatment outcome
PhN should check the following information initially. these are:- Is the diagnosis correct?- Is the treatment regimen appropriate?Check weekly:- Are all smear-positive cases registered and treated
properly with DOt?- Are drugs collected on time?- Are follow-up exams done on time?- Are treatments regular and effective?- Are actions taken to retrieve defaulters?
Y
N
1
5
6
2
4
Figure 4
Laboratory Register(tobeaccomplishedbythe
MedicalTechnologist(MT))
Record of laboratory examination results• 3 sputum collection• Sputum-smear examina-
tion results on diagnosis/follow-up
3

389
CPM 7th EDItION tUBERCULOSIS
A. CASE FINDING
ThebasicstepinTBcontrolistheidentificationanddiagnosis of TB cases among individuals with suspected signs and symptoms of TB. This is referred to as case finding.Fundamentaltocasefindingisthedetectionof infectious cases through direct sputum-smear examination. This is the principal diagnostic method adapted by the new NTP because of the following reasons:
1. ItprovidesadefinitivediagnosisofactiveTB.2. The procedure is simple.3. It is economical.4. A microscopy center could be organized even in
remote areas.
I. Objective
Thegeneralobjectiveofcasefindingistheearlyiden-tificationanddiagnosisofTBcases.
II. Policies
1. Direct sputum-smear examination shall be the primary diagnostic tool in NTP case finding.
a. AllTBsymptomatics identifiedshallbemade toundergo smear examination for diagnosis prior to initiation of treatment, regardless of whether they have available x-ray results or whether they are suspected of having extra-pulmonary TB. Theonlycontraindicationforsputumcollectionismassivehemoptysis.
b. It is only after a pulmonary TB symptomatics has undergone a sputum examination for diagnosis with three sputum specimens and subsequently yielded negative results that he shall be made to undergo other diagnostic tests such as x-ray, culture and others, if necessary.
c. Sputum smear examination is the preferred method for the diagnosis of TB. No diagnosis of TB shall be made based on the result of x-ray examinations alone. Skin tests for TB infection (PPD skin test) should not be used as a basis for the diagnosis of TB in adults.
d. Allmunicipal and city health offices shall beencouraged to establish and maintain at least one sputum microscopy unit in their areas of ju-risdiction.
2. Passive case finding shall be implemented in all health stations.
Concomitant activecasefinding shallbeencour-
aged only in areas where a cure rate of 85 percent or higher has been achieved, or in areas where no sputum smear positive case has been reported in the last three months.
3. Only adequately trained medical technologist or NtP microscopist shall perform sputum-smear examination (smearing, fixing and staining of sputum specimens, reading the smear).
III. Procedures
1. Identification of TB symptomatics is the respon-sibility of all RhU (Rural health Unit) and BhS (Barangay health Station) staff.
• The responsible person (all health workers) shall identify TB symptomatics among patients consult-ing at the health center. These are persons having cough for two or more weeks duration, and those with or without one or more of the following signs and symptoms:
a) fever b) sputum expectoration c) significantweightloss d) hemoptysis or recurrent blood-streaked spu-
tum e) chest and/or back pains not referable to any
musculo-skeletal disorders f) other symptoms such as sweat with chills,
fatigue, body malaise, shortness of breath• The responsible person, who can be any health
workers,shalleducateandencourageidentifiedTBsymptomatic cases for sputum submission.
• tB Symptomatics Masterlist / tB Symptomatics target Client List (or TB Symptomatics Target Cli-entList)maybeoptionallyutilizedforconfirmationof three sputum collection in addition to Laboratory Request Form for Sputum Examination.
• The responsible person shall encourage household members of identifiedTB cases,who also havesymptoms suspecting TB, to undergo sputum ex-amination.
2. Collection and transport of sputum specimens to the Microscopy Center are the responsibilities
National Tuberculosis Program - Manual of Policies and Procedures

390
tUBERCULOSIS CPM 7th EDItION Guide to Case Finding
Sputum Collection Unit(TobeaccomplishedbytheRHM/PHN/MHO)
1. (Optional) Register the patient in TBSymptomatics*Masterlist(or TBSymptomaticsTargetClientList).
2. Explain the importance of three (3) sputum collection to the TB symptomatics.
3. Label each sputum containers (name and serial no. 1, 2, 3).
4. Collect three (3) sputum specimens (spot, early morning, spot).
5. Fill-up the LaboratoryRequestFormforSputumExamination.Confirmthree(3)sputumcollection.
6. Pack and send the specimen/s to the Microscopy Center with the Laboratory Request Form for Sputum Examination.
* TBSymptomaticswithsymptomsas:Coughfor2weeksormore,sputumexpectoration,fever,significantweight loss, chest and/or back pains, hemoptysis.
MICROSCOPY CENtER(TobeaccomplishedbytheMT)
1. Register in the NTPLaboratoryRegister.
2. Record the date received and the Laboratory Serial No. in the LaboratoryRequestFormfortheSputumExamination.
3. Sputum-SmearExamination:smearing,fixing,stainingandreadingslides.
4. Record the results in the LaboratoryRequestFormforSputumExamination and in the NTP Laboratory Register.
5. Send back accomplished Laboratory Request Form for Sputum Examination to the collection unit.
SPUtUM COLLECtION UNIt(TobeaccomplishedbytheRHM/PHN/MHO)
1. (Optional) Record the results in the TBSymptomaticsMasterlist (orTBSymptomaticsTargetClientList).
2. Inform and explain the result to the patient (if doubtful, immediately collect another 3 specimens for con-firmation).
3. Refer to MHO and PHN.
DIAGNOSIS AND INItIAtION OF tREAtMENt

391
CPM 7th EDItION tUBERCULOSIS
Guide to Diagnosis and Initiation of treatment
Clinical Diagnosis•TodeterminepatienttypeandclassificationandisdonebyRHM,PHN,MHO•
1. Verify information gathered on case finding • Symptoms/condition of patient • Result of sputum examination • Result of further examination (i.e., CXR, culture, etc.) • Source of infection
2. Verify sputum smear examination results
3. Review history of previous treatment
INItIAtION OF tREAtMENt
to be done by MhO
1. Physical assessment and prescription of appropriate regimen for the tB patient ac-cording to the patient type and the classification
to be done by PhN (ini-tially)
2. Registration• Fill-up the NTPTreatmentCard.• Fill-up two NTPIDCards, oneisforthetreatmentpartnerandtheotherisforthepatient.• Register in the TBRegister.
to be done by the health workers
3. health education with emphasis on key messages such as:• TB is infectious.• TB can be cured but requires regular drug intake.• Results of irregular drug intake.• Side effects of anti-TB drugs.• Importance of follow-up sputum smear examinations.• Importance of family/treatment partner support.
to be done by PhN
4. Intake of first dose• Record the date when treatment started.• Record the due date of the 1st follow-up sputum examination in the NTP Treatment
Card
to be done by the health workers and t re a t m e n t partners
5. DOt• Assign a treatment partner.• Do DOT for both intensive and Maintenance phases of treatment.• Conduct weekly consultation meeting at the health facility during the whole course of treatment.
to be done by:1. PhN2. RhM3.treatment
partner4. tB patient
6. Record keeping1. Maintain and update the TBRegister.2. Maintain and update the NTPTreatmentCard at the RHU/BHS.3. Maintain and update the NTPIDCards both of the treatment partner and the patient.4. Keep the NTPIDCard.

392
tUBERCULOSIS CPM 7th EDItION
of MhO (MunicipalHealthOfficer)/ PhN (Public Health Nurse) / RhMS (Rural Health Midwives) at the RhU and BhS.
• It is crucial for TB symptomatics to under-stand the importance of submitting three sputum specimens during their consultation. MHO/PHN/RHMS, who are in charge of the initial consultation, shall educate TB symptomatics on the purpose of sputum examination.
• It is essential to obtain quality sputum speci-men for proper diagnosis of TB. The responsible health worker shall demonstrate how to produce good sputum by instructing TB symptomatics as follows:
Rinse his / her mouth with water.Breathe deeply two times, holding the breath
for a few seconds after each inhalation and then exhaling slowly.
After inhaling deeply the third time, at the height of inspiration cough strongly and spit the sputum in the container.
• The responsible health worker shall supervise the patient from behind during the procedure and ob-serve contamination precautions. It is recommended to collect sputum specimens outside where aerosols containing TB bacilli are diluted and sterilized by direct sunlight in order to prevent health workers from inhalation hazards.
• The responsible health worker shall collect three sputum specimens within two days according to these procedures:
First specimen is also referred to as spot specimen. It is collected at the time of consul-tation, or as soon as the TB symptomatics is identified.
Second specimen or early morning specimen. It is theveryfirst sputumproducedearly inthe morning immediately after waking up, and collected by the patient according to the instructions given by the health workers.
third specimen is also referred to as spot specimen. It is collected at the time the TB symptomatics comes back to health facility to submit the second specimen.
• The responsible health worker shall label the body of the sputum cup with the patient’s complete name and the name of the referring unit, seal each sputum specimen container, pack it securely and transport it to a microscopy unit or laboratory as soon as possible or not later than four days from collec-tion. Otherwise, the specimens should be properly
stored in cool, dark, and safe place. No specimen shall remain unexamined over the weekend. The specimen should be sent together with the laboratory request form for sputum smear examination to the microscopy center.
3. Smearing, fixing, staining and reading of sputum specimens are the responsibilities of the trained NtP medical technologist or NtP microscopist at the microscopy center. they will do the follow-ing:
a. Record the information in the NTP Laboratory
Register. b.Smear,fix,stain,andreadtheslides. c. Interpret smear examination result or the indi-
vidual readings of the three specimens and the finalwrittenlaboratorydiagnosisinthesputummicroscopy results portion of the returned Laboratory Request Form for Sputum Exami-nation, to determine diagnosticclassification,such as:
Smear positive result occurs when at least
two sputum smear results are positive. When the sputum collection unit receives this posi-tive result, the nurse/midwife shall inform the patient of the result of the sputum examination and refer him/her to the MHO for assessment and initiation of treatment.
Doubtful result shows only one positive out of three sputum specimens examined. The nurse shall inform the midwife of the result of the sputum examination to allow her to collect another three sputum specimens.
If at least one specimen from the second
set of specimen turns out to be positive, the laboratory diagnosis is positive. Refer the patient to MHO assessment and initiation of treatment.
If all three specimens from the second set of specimen turn out to be negative, the labora-tory diagnosis is negative. Refer the patient to MHO for assessment with X-ray examina-tion.
Smear negative shows that all three sputum
smear results are negative. The nurse shall inform the TB symptomatics about the result of the sputum examination and refer the patient to MHO for further assessment. The municipalhealthofficermaytreatthepatientwith symptomatics treatment of antibiotics

393
CPM 7th EDItION tUBERCULOSIS
ment is referred to as case holding. Chemotherapy is the only way to stop the transmission of TB. It is senseless to search for cases if they could not be treated properly after they have been found. It would only encourage false hopes on the part of the patient. While effective anti-TB drugs are available in the country, there are still many TB patients who are not cured. This is due to many patients who stop taking or irregularly take their drugs. The long duration of treatment, six months on the average, makes it most likely for patients to be remiss in drug intake. Treat-ment compliance is necessary to cure TB and avoid drug resistance.
Poor treatment compliance may lead to the following outcomes: Chronic infectious illness, death or drug
and/or anti-cough agents for two to three weeks. If symptoms persist, collect another three specimens for smear examination.
d. Record the examination results in the NTP
Laboratory Register and the lower portion of the Laboratory Request Form for Sputum Examina-tion.
e. Inform the responsible health worker of the results of the examination as soon as it is available by sending back the accomplished Laboratory Request Form for Sputum Exa-mination.
B. CASE hOLDING
The procedure that ensures that patients complete treat-
Table 1. Classification of TB Cases
Location of Lesion Sputum-Smear Examination Definition of Terms Smear Positive
Smear Negative
1. A patient with at least two sputum specimens positive for AFB (acid-fast bacilli) with or without radiographic abnor-malities consistent with active TB, or
2. A patient with one sputum specimen positive for AFB and with radiographic abnormalities consistent with active TB as determined by a clinician, or
3. A patient with one sputum specimen positive for AFB with sputum culture positive for M.tuberculosis.
A patient with at least three sputum specimens negative for AFB with ra-diographic abnormalities consistent with active TB; and there has been no response to a course of antibiotics and/or symptomatic medications; and there is a decision by a Medi-calofficer to treat thepatientwithanti-TB drugs.
1. A patient with at least one mycobacterial smear/culture positive from an extra-pulmonary site (organs other than the lungs: pleura, lymph nodes, genito-urinary tract, skin, joints and bones, meninges, intestines, peritoneum and pericardium, among others); or
2. A patient with histological and/or clinical evidence consistent with active TBandthereisadecisionbyamedicalofficertotreatthepatientwithanti-TB drugs.
Extra-Pulmonary tB
Pulmonary tB

394
tUBERCULOSIS CPM 7th EDItION resistance. Second line anti-TB drugs for drug resistant cases are very expensive and most are not available in the country. The best way to prevent the occurrence of drug resistance is through regular intake of drugs for the prescribed duration. The strategy developed to ensure treatment compliance is called Directly Observed treatment (DOt). It is one of the key components ofDOTSinordertoachievesufficientcurerateand,at once, prevent drug resistant TB. DOT works by as-signing a responsible person to observe or watch the patient take the correct medications daily during the whole course of treatment.
I. Objective
The general objective of chemotherapy is to treat TB cases effectively and completely especially pulmonary sputum smear positive cases.
II. Definition of Terms
A. Classification of TB cases - TB cases shall also be classifiedbasedon the locationof lesionsaswell asthe result of sputum smear examination. (See Table 1 on page 10.)
B. types of tB cases - TB cases shall be categorized based on the history of anti-TB treatment. A thorough understanding on the types of TB cases is necessary in determining the correct treatment regimen. (See Table 2.)
C. Directly Observed treatment (DOt) - DOT is a strategy developed to ensure treatment compliance by providing constant and motivational supervision to TB patients. DOT works by having a responsible person, referred to as treatment partner, watching the TB pa-tient take medicines everyday during the whole course of treatment.
1. Who will undergo DOt?All smear positive TB cases should undergo DOT.
2. Who could serve as a treatment partner of a tB patient during DOt?Any of the following could serve as treatment partner of a TB patient:
Staff of the health center or clinic such as the mid-wife or the nurse.
Member of the community such as the BHW (Baran-gayHealthWorker),localgovernmentofficialorTBpatient.
Member of the patient family (last priority).
Note:Memberofthepatientfamilyisgenerallynotreli
A patient who has never had treatment for TB or who has taken anti-tuberculosis drugs for less than one month.
New
Relapse A patient previously treated for tuberculosis, who has been declared cured or treat-ment completed, and is diag-nosed with bacteriologically positive (smear or culture) tuberculosis.
Failure A patient who, while on treatment, is sputum smear positive at five months or later during the course of treatment.
Return after Default
A patient who returns to treatment with positive bac-teriology (smear or culture), following interruption of treatment for two months or more.
transfer-in A patient who has been trans-ferred from another facility with proper referral slip to continue treatment.
Other Allcaseswhodonotfitintoanyoftheabovedefinitions.
This group includes:
1. A patient who is starting treatment again after inter-rupting treatment for more than two months and has remained or became smear negative.
2. A patient, who was initially registered as new smear-negative case, turned out to be smear-positive during the treatment. (The treatmentoutcomeofthiscaseis "Treatment Failure."Reregisteras"Other"forthenexttreatment.)
3. Chronic case: A patient who is sputum positive at the end of a re-treatment regimen.
Definition of Termstypes of tB
Cases
table 2. types of tB Cases

395
CPM 7th EDItION tUBERCULOSIS
table 3. treatment Regimens
Regimen tB Patient to be Given treatment
Drugs and Duration of treatment
Dose Adjustment by Body Weight
Regimen I:2hRZE / 4hR • New pulmonary smear
positive cases• New seriously ill pulmo-
nary smear negative cases with extensive parenchy-mal involvement
• New severely ill extra-pul-monary TB cases
HRZE for two months dur-ing the intensive phase.
HR for 4 months during the maintenance phase.
Add one tablet of INH (100 mg), PZA (500 mg), and EB (400 mg) each for the patient with more than 50kg body weight before the initiation of the treatment.
Regimen II: 2hRZES /1hREZ / 5hRE
• Failure Cases• Relapse Cases• RAD (smear+)• Other (smear+)
HRZES for the first two months, then HRZE for the third month during the intensive phase.
HRE for the next five months during the main-tenance phase.
Regimen III:2 hRZ/4hR
• New smear-negative but with minimal pulmonary TB on radiography as confirmedbyamedicalofficer
• New extra-pulmonary TB (not serious)
HRZ for 2 months during the intensive phase.
HR for 4 months during the maintenance phase.
Add one tablet of INH (100 mg), PZA (500 mg) each for the patient with more than 50kg body weight before the initiation of the treatment.
ableasatreatmentpartnercomparedwiththehealthworkers.It is, therefore,not recommendedtoassignafamilymemberofthepatientasatreatmentpartnerexceptonweekendsandholidays.
3. Where to do DOt?
DOT can be done in any accessible and convenient place (e.g., health facility, treatmentpartner’shouse,patient’splaceofwork,patient'shouse) as long as the treatment partner can effectively ensure the patient’s intake of the prescribed drugs, and monitor his/her reactions to the drugs.
4. how long is treatment supervised?
The patient’s daily anti-TB drug intake should be super-vised during the intensive and maintenance phases of short-course chemotherapy for all smear-positive tB patients.
III. Policies
A. Treatment of all TB cases shall be based on reli-able diagnostic technique, namely sputum smear examinationasidefromclinicalfindings.
B. Domiciliary treatment shall be the preferred mode of care.
C. Patients recommended for hospitalization are those with the following conditions:1. massive hemoptysis2. pleural effusion obliterating more than 1/2 of
alungfield3. miliary TB4. TB meningitis5. TB pneumonia6. those requiring surgical intervention or with
complicationsD. No patient shall initiate treatment unless the patient
and health workers have agreed upon a case holding mechanism for treatment compliance.

396
tUBERCULOSIS CPM 7th EDItION
table 4. Drug Dosage Adjustment
Drug Dose per kg body weight and maximum dose Isoniazid 5 (4-6) mg/kg, and not to exceed 400 mg daily
Rifampicin 10 (8-12) mg/kg, and not to exceed 600 mg daily
Pyrazina- 25 (20-30) mg/kg, and not to mide exceed 2 g daily
Ethambutol 15 (15-20) mg/kg, and not to exceed 1.2 g daily
Strepto- 15 (12-18) mg/kg, and not to mycin exceed 1 g daily
table 5a. Schedule of Sputum Smear Follow- up Examination (Category I)
Schedule of Category 1 (2 hRZE/4 hR) Sputum Smear Follow-up Regular With One Examination treatment Month of Extension (hRZE)
Towards the YES (If positive) end of the 2nd month
Towards the (If negative) YES end of the 3rd month
Towards the YES end of the 4th
month
Towards the YES end of the 5th
month
In the beginning YES(*1)
of the 6th month
In the beginning YES(*1)
of the 7th month
*1Check the follow-up sputum smear examination at the end of the treatment (during the last week of treatment) for the patient who has smear positive in the last follow-up smear examination and shows smear negative in the repeated smear examination. (See Tables 7a and 7b.)
E. The national (regional) and local government units shall ensure the provision of drugs to all sputum positive TB cases.
F. treatment Regimens by Category - The following abbreviations mean:
H - Isoniazid (300 mg)R - Rifampicin (450 mg)Z - Pyrazinamide (1 g)E - Ethambutol (800 mg)S - Streptomycin (1 g)
G. Drug dosage adjustment according to the initial body weight of patient. Simply add one tablet of INH (100 mg), PZA (500 mg) and EB (400 mg) each for the patient with more than 50kg body weight before the initiation of the treatment (See Table 3). Modify drug dosage within acceptable limits ac-cording to the body weight of the patient weighing less than 30 kg at the time of diagnosis (See Table 4).
IV. Procedures
A. Registration and Initiation of treatment
1. Inform the patient that he/she has TB and motivate the patient to undergo treatment.
2. Referthepatienttoamedicalofficerforpre-treat-ment evaluation and initiation of treatment.
3. Open the NtP treatment Card and two NtP ID Cards (one is for the treatment partner and the other is for the patient) and start the treatment using any of the three treatment regimens best suited to the
patient’sdiseaseclassification, typeandprevioushistory of treatment.
4. Register the patient in the NtP tB Register. Refer the patient to the most accessible BHS
where he/she can have his/her treatment super-vised.
B. Ensuring treatment Compliance through “DOt”
1. Explain the importance of treatment compliance to the patient.
2. Administer the patient’s drugs daily. The patient and his/her treatment partner shall meet at their agreed treatment unit everyday. The treatment partner shall make sure that the patient takes his/her drugs daily. After intake of the drugs, the treat-
397
CPM 7th EDItION tUBERCULOSIS
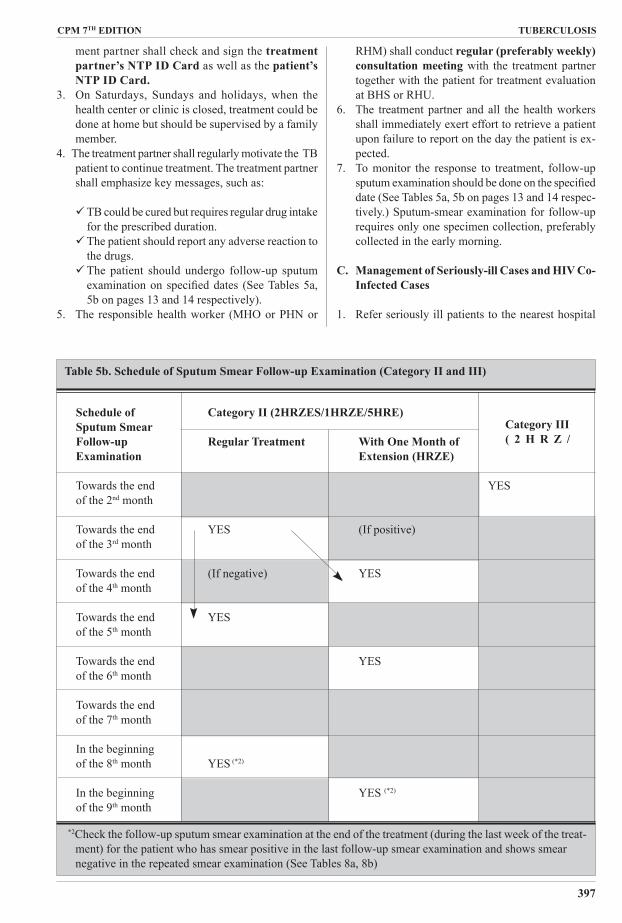
table 5b. Schedule of Sputum Smear Follow-up Examination (Category II and III)
Schedule of Category II (2hRZES/1hRZE/5hRE) Sputum Smear Follow-up Regular treatment With One Month of Examination Extension (hRZE)
Towards the end YES of the 2nd month
Towards the end YES (If positive) of the 3rd month Towards the end (If negative) YES of the 4th month
Towards the end YES of the 5th month
Towards the end YES of the 6th month
Towards the end of the 7th month
In the beginning of the 8th month YES (*2)
In the beginning YES (*2)
of the 9th month *2Check the follow-up sputum smear examination at the end of the treatment (during the last week of the treat-
ment) for the patient who has smear positive in the last follow-up smear examination and shows smear negative in the repeated smear examination (See Tables 8a, 8b)
Category III( 2 h R Z /
ment partner shall check and sign the treatment partner’s NtP ID Card as well as the patient’s NtP ID Card.
3. On Saturdays, Sundays and holidays, when the health center or clinic is closed, treatment could be done at home but should be supervised by a family member.
4. The treatment partner shall regularly motivate the TB patient to continue treatment. The treatment partner shall emphasize key messages, such as:
TB could be cured but requires regular drug intake for the prescribed duration.
The patient should report any adverse reaction to the drugs.
The patient should undergo follow-up sputum examinationon specifieddates (SeeTables5a,5b on pages 13 and 14 respectively).
5. The responsible health worker (MHO or PHN or
RHM) shall conduct regular (preferably weekly) consultation meeting with the treatment partner together with the patient for treatment evaluation at BHS or RHU.
6. The treatment partner and all the health workers shall immediately exert effort to retrieve a patient upon failure to report on the day the patient is ex-pected.
7. To monitor the response to treatment, follow-up sputumexaminationshouldbedoneonthespecifieddate (See Tables 5a, 5b on pages 13 and 14 respec-tively.) Sputum-smear examination for follow-up requires only one specimen collection, preferably collected in the early morning.
C. Management of Seriously-ill Cases and hIV Co-Infected Cases
1. Refer seriously ill patients to the nearest hospital

398
tUBERCULOSIS CPM 7th EDItION
table 6. Guide in Managing SCC Drugs Side Effects
Side Effects Drug(s) Responsible What to Do? 1. Gastrointestinal intolerance Rifampicin Give medication at bedtime
2. Mild skin reactions Any drugs Give antihistamines.
3. Orange/red colored urine Rifampicin Reassure the patient.
4. Pain at the injection site Streptomycin Apply warm compress. Rotate sites of injection.
5. Burning sensation of the feet Isoniazid Give pyridoxine (vitamin due to peripheral neuropathy B6): 100-200 mg daily for treatment; 10 mg daily for prevention
6. Arthralgia due to hyperurice- Pyrazinamide Give aspirin or NSAID. mia If symptoms persist, consi- der gout and give allopuri- nol.
7. Flu-like symptoms (fever, Rifampicin Give antipyretics. muscle pains, inflammation of the respiratory tract)
1. Severe skin rash due to hyper- Any drugs (espe- Discontinue anti-TB drugs sensitivity cially streptomycin) and refer to MHO/CHO. 2. Jaundice due to hepatitis Any drugs (especial- Discontinue anti-TB drugs ly isoniazid, rifampicin and refer to MHO/CHO. and pyrazinamide) If symptoms subside, re- sume treatment and moni- tor clinically.
3. Impairment of visual acuity Ethambutol Discontinue ethambutol and color vision due to optic and refer to an ophthalmo- neuritis logist.
4. hearing impairment, ringing Streptomycin Discontinue streptomycin of the ear and dizziness due to and refer to MHO/CHO. the damage of the eighth cranial nerve
5. Oliguria or albuminuria due Streptomycin Discontinue anti-TB drugs due to renal disorder Rifampicin and refer to MHO/CHO.
6. Psychosis and convulsion Isoniazid Discontinue isoniazid and refer to MHO/CHO.
7. thrombocytopenia, anemia, Rifampicin Discontinue anti-TB drugs shock and refer to MHO/CHO.
Minor Side Effects: Patient should be encouraged to continue taking medicines
Major Side Effects: Discontinue taking medicines and refer to MhO/ChO immediately

399
CPM 7th EDItION tUBERCULOSIS
Treatment Modifications Based on the Results of the Sputum Follow-up Examination
Regimen I Do sputum smear examinations for follow- up towards the end of the 2nd month of treatment. If the sputum examination result is NEGAtIVE, start maintenance phase (hR) and follow table 7a. If the sputum examination result is POSItIVE, extend intesive Phase (hRZE) for another one (1) month and refer to tables 7b1 on page 17 and table 7b2 on page 18.
Table 7a. Treatment Modifications Based on the Results of the Sputum Follow-Up Examination
towards the end In the beginning of the 6th month towards the end of the of the 4th month 6th month(*1)
If smear negative, If smear negative, complete the maintenance continue the phase until the end of the treatment course maintenance phase and declare as "Cure" (HR). If smear positive, If smear negative in the If smear negative, declare as repeat smear repeated smear examination "Cure." examination continue the maintenance immediately for phase (HR) and do the If smear positive, declare as confirmationand smearexaminationtowards "treatment Failure," then consult with the end of the 6th month of re-register as "Failure" and Provincial/City/ treatment start Regimen-II. CHD TB If smear positive again in the coordinators repeated smear examination through MHO/ declare as "treatment Fai- CHO lure," then re-register as "Failure" and start Regi- men II.
If smear positive, If smear negative, continue the maintenance phase If smear negative, declare as continue the (HR) and do the smear examination towards the "Cure." maintenance phase end of the 6th month of treatment. (HR). If smear positive, declare as "treatment Failure", then re-register as "Failure" and start Regimen-II. If smear positive, declare as "Treatment Failure", then re-register as "Failure" and start Regimen II.
*1 Check the follow-up sputum smear examination towards the end of the 6th month of the treatment only for the patient who has smear positive in the beginning of the 6th month and shows smear negative in the repeated smear examination; and for the patient who has smear positive towards the end of the 4th month turns out to be negative in the beginning of the 6th month.
facility for evaluation and appropriate treatment.2. Refer TB cases with known concomitant HIV in-
fectiontoamedicalofficerforappropriateaction.
D. Management of Adverse Reactions to Drugs Closely monitor the occurrence of minor and major
reactions to drugs, especially during the intensive phase. (See Table 6 on page 15).
E. Monitoring Patient Response to treatment Monitor the sputum smear status of all patients
under treatment, including initially sputum smear

400
tUBERCULOSIS CPM 7th EDItION
Table 7b1. Treatment Modifications Based on the Results of the Sputum Follow-up Examinations for Regimen-I with Extension
towards towards towards the the end of the end of In the beginning of the 7th month end of the the 3rd month the 5th month 7th month(*2)
If smear negative, start the mainte-nance phase (HR).
If smear nega-tive, continue the maintenance phase (HR).
If smear negative, complete the maintenance phase until the end of the treatment course and declare as "Cure."
If smear positive, repeat smear exami-nation immediately forconfirmationandconsult with Provin-cial/City/CHD TB Coordinators through MHO/CHO.
If smear negative in the repeated exami-nation, continue the maintenance phase (HR) and do the smear examination towards the end of the 7th month of treat-ment.
If smear positive in the repeated exami-nation, declare as "treatment Fail-ure," then re-register as "Failure" and start Reg. - II.
If smear negative, dec-lare as "Cure."
If smear positive, dec-lare as "treatment Failure," then re-re-gister as "Failure" and start Reg. - II.
If smear posi-tive, continue the maintenance phase (HR) any-way.
If smear negative, continue the maintenance phase (HR) and do the smear examination towards the end of the 7th month of treat-ment.
If still smear positive, declare as "treatment Failure," the re-register as "Failure" and start Reg. II.
If smear negative, dec-lare as "Cure."
If smear positive, dec-lare as "treatment Failure," then re-re-gister as "Failure" and start Reg. - II.
*2Check the follow-up sputum smear examination towards the end of the 7th month of treatment only for the patient who has smear positive in the beginning of the 7th month and shows smear negative in the repeated smear examination; and for the patient who has smear positive towards the end of the 5th month and turns out to be negative in the beginning of the 7th month.
negative patients, according to the standard schedule (See Tables 5a on page 13 and 5b on page 14.) and modify treatment based on the sputum follow-up examination results (See Tables 7a on page 16, 7b1 on page 17, 7b2 on page 18, 8a on page 19 and 8b on page 20).
F. Management of Lost and Referred Cases
1. Perform routine smear examination to lost and
defaulted cases, who came back for chemotherapy. Referpatienttoamedicalofficerforre-evaluationand re-treatment.
2. New smear-positive patients who interrupted treat-ment, shall be managed according to recommended schedule (See Table 9a on page 21).
3. Relapse and failure cases who interrupted treat-ment, shall be managed according to recommended schedule (see Table 9b on page 22).
4. Treatment will be continued for patients who were

401
CPM 7th EDItION tUBERCULOSIS
If smear positive, start the mainte-nance phase (HR) anyway.
Table 7b2. Treatment Modifications Based on the Results of the Sputum Follow-up Examinations for Regimen-I with Extension
If smear negative, continue the main-tenance phase (HR).
If smear negative, complete the maintenance phase until the end of the treatment course and declare as "Cure."
towards towards towards the the end of the end of In the beginning of the 7th month end of the the 3rd month the 5th month 7th month(*2)
If smear positive, r e p e a t s m e a r examination im-m e d i a t e l y f o r confirmation and consult Provincial/City/CHD TB Coor-dinators through MHO/CHO.
If smear negative in the repeated examination, continue the mainte-nance phase (HR) and do the smear exami-nation towards the end of the 7th month of treatment.
If smear negative, dec-lare as "Cure."
If smear positive, dec-lare as "treatment Failure," then re-re-gister as "Failure" and start Reg. - II.
If smear positive in the repeated examination, declare as "treatment Failure," then re-reg-ister as "Failure" and start Reg. - II.
If still smear po-sitive, declare as "treatment Fail-ure," then re-reg-ister as "Failure" and start Reg. - II.
*2Check the follow-up sputum smear examination towards the end of the 7th month of treatment only for the patient who has smear positive in the beginning of the 7th month and shows smear negative in the repeated smear examination; and for the patient who has smear positive towards the end of the 5th month and turns out to be negative in the beginning of the 7th month.
properly referred or transferred with referral slip. However, sputum smear examination for diagnosis should be performed for patients without an ac-companyingproperlyfilledreferral/transferslip.
C. OUtCOME OF tREAtMENt A TB patient who undergoes treatment may achieve any of the following treatment outcomes:
1. Cure: A sputum smear-positive patient who has been completed treatment and is sputum smear negative in the last month of treatment and on at least one previous occasion.
(Note: We have changed the definition of "cure" as above,however,wehavenotchangedthepolicytocollect followupsputumspecimenwiththreeoccasionsforsmearpositivecaseattheendoftheintensivephase,inthemiddleofthemaintenancephase,andattheendofthemaintenancephase.)
2. treatment Completed: A patient who has com-pleted treatment but does not meet the criteria to beclassifiedascureorfailure.
This group includes: • A sputum smear-positive patient initially who has
completed treatment without follow-up sputum examinations during the treatment, or with only one negative sputum examination during the

402
tUBERCULOSIS CPM 7th EDItION
Table 8a. Treatment Modifications Based on the Results of the Sputum Follow-up Examinations for Regimen - II Without Extension
*3 Check the follow-up sputum smear examination towards the end of the 8th month of the treatment only for the patient who has smear positive in the beginning of the 8th month and shows smear negative in the repeated smear examination; and for the patient who has smear positive towards the end of the 5th month turns out to be negative in the beginning of the 8th month.
towards the end In the beginning of the 8th month towards the end of the of the 5th month 8th month(*3)
If smear negative, If smear negative, complete the maintenance continue the phase until the end of the treatment course maintenance phase and declare as "Cure." (HRE). If smear positive, If smear negative in the If smear negative, declare as repeat smear repeated smear examination , "Cure." examination continue the maintenance immediately for phase (HRE) and do the If smear positive, declare as confirmationand smearexaminationtowards "treatment Failure," consult with the end of the 8th month. Provincial/City/ CHD TB If smear positive again in the coordinators repeated smear examination through MHO/ complete the maintenance CHO phase (HRE) until the end of the treatment course and dec- lare as "treatment Failure." If smear positive, If smear negative, continue the maintenance phase If smear negative, declare as continue the (HRE) and do the sputum smear examination "Cure." maintenance phase towards the end of the 8th month. (HRE) anyway. If smear positive, declare as "treatment Failure" If smear positive, complete the maintenance phase (HRE) until the end of the treatment course and declare as "treatment Failure."
REGIMEN IIDo sputum smear examinations for follow- up towards the end of the 3rd month of treatment. If the sputum examination result is NEGAtIVE, start Maintenance Phase (hRE) and refer to table 8a. If the sputum examination result is POSItIVE, extend Intesive Phase (hRZE) for another one (1) month and refer to table 8b.
treatment, or without sputum examination in the last month of treatment.
• A sputum smear-negative patient who has com-pleted treatment.
3. Died: A patient who dies for any reason during the course of treatment.
4. treatment Failure: •Apatientwhoissputumsmear-positiveatfive
months or later during the treatment. • A sputum smear-negative patient initially before starting treatment and becomes smear-
positive during the treatment. (Note:Thiscasewillbereregisteredas"Other"
withanewTBcasenumber.)5. Defaulter: A patient whose treatment was inter-
rupted for two consecutive months or more.6. transfer out: A patient who has been transferred
to another facility with proper referral/transfer slip for continuation of treatment.

403
CPM 7th EDItION tUBERCULOSIS
Table 8b. Treatment Modifications Based on the Results of the Sputum Follow-up Examinations for Regimen - II With Extension
* 4 Check the follow-up sputum smear examination towards the end of the 9th month of treatment only for the patient who has smear positive in the beginning of the 9th month and shows smear negative in the repeated smear examination; and for the patient who has smear positive at the end of the 6th month and turns out to be negative in the beginning of the 9th month.
towards towards towards the the end of the end of In the beginning of the 9th month end of the the 4th month the 6th month 9th month(*4)
If smear posi- If smear nega- If smear negative, complete the tive, or smear tive continue maintenance phase until the end of negative start the mainte- the treatment course and declare the mainte- nance phase as "Cure." nance phase (HRE). (HRE) anyway.
If smear negative, continue the main-tenance phase (HRE) and do the smear examination towards the end of the 9th
month of treatment.
If smear negative, declare as "Cure."
If still smear positive, complete the maintenance phase (HRE) until the end of the treatment course and declare as "treatment Failure."
If smear positive complete the main-tenance phase (HRE) until the end of the treatment course and declare as "treat-ment Failure."
If smear posi-tive, continue the maintenance phase (HRE) anyway.
If smear positive, repeat smear examination im-mediately for confirmationandconsult with Pro-vincial/City/CHD TB Coordinators through MHO/CHO.
If smear negative in the repeated smear examination contin-ue the maintenance phase (HRE) and do the smear examina-tion towards the end of the 9th month of treatment.
If smear posi-tive again in the re-peated smear examination, com-plete the mainte-nance phase (HRE) until the end and declare as "treat-ment Fail-ure."
If smear negative dec-lare as "Cure."
If smear positive, dec-lare as "treatment Failure."

404
tUBERCULOSIS CPM 7th EDItION
Table 9a. Treatment Modifications for New Smear-Positive Cases Who Interrupted Treatment
Length of treatment
Length of Interruption
Do a Smear?
Result of Smear
Register Again? treatment Modification
Less than one month
Less than 2 weeks No No, use the same treatment
card.Continue
Regimen-I
2 weeks or more
YesPositive No, open a new treatment
card.Start again on
Regimen-I
Negative No, use the same treatment card.
Continue Regimen-I
One to two months
Less than 2 weeks No No, use the same treatment
card.Continue
Regimen-I
2 to 8 weeks
Yes Positive
No, use the same treatment card.
Complete the remaining Inten-sive Phase, add one extra month
of Intensive Phase.
Negative No, use the same treatment card.
Continue Regimen-I
More than 8 weeks
Yes
PositiveClose the previous registration as "Defaulter," then re-reg-ister as "RAD," open a new treatment card.
Start on Regimen-II
NegativeClose the previous registration as "Defaulter," then re-regis-ter as "Other," but use the same treatment card.
Continue Regimen-I
More than two months
Less than 2 weeks No No, use the same treatment
card.Continue
Regimen-I
2 to 8 weeks
YesPositive
Close the previous registra-tion as "Defaulter,"(*1) then re-register as "RAD," open a new treatment card.
Start on Regimen-II
NegativeNo, use the same treatment card.
Continue Regimen-I
More than 8 weeks
Yes
PositiveClose the previous registration as "Defaulter," then re-reg-ister as "RAD," open a new treatment card.
Start on Regimen-II
Negative
Close the previous registration as "Defaulter," then re-register as "Other," open a new treat-ment card.
Continue Regimen-I
*1Thisistheexceptionalcasetodefineas"Defaulter" for a patient who interrupted treatment of less than eight weeks.
405
CPM 7th EDItION tUBERCULOSIS
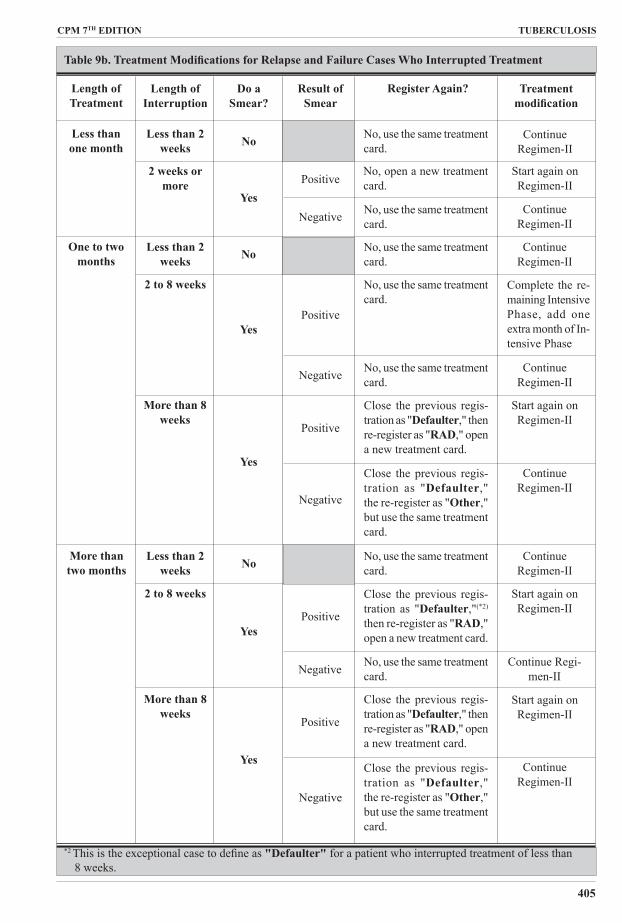
Table 9b. Treatment Modifications for Relapse and Failure Cases Who Interrupted Treatment
Length of treatment
Length of Interruption
Do a Smear?
Result of Smear
Register Again? treatment modification
Less than one month
Less than 2 weeks No No, use the same treatment
card.Continue
Regimen-II
2 weeks or more
YesPositive
No, open a new treatment card.
Start again on Regimen-II
Negative No, use the same treatment card.
Continue Regimen-II
One to two months
Less than 2 weeks No No, use the same treatment
card.Continue
Regimen-II
2 to 8 weeks
YesPositive
No, use the same treatment card.
Complete the re-maining Intensive Phase, add one extra month of In-tensive Phase
Negative No, use the same treatment card.
Continue Regimen-II
More than 8 weeks
Yes
Positive
Close the previous regis-tration as "Defaulter," then re-register as "RAD," open a new treatment card.
Start again on Regimen-II
Negative
Close the previous regis-tration as "Defaulter," the re-register as "Other," but use the same treatment card.
Continue Regimen-II
More than two months
Less than 2 weeks No No, use the same treatment
card.Continue
Regimen-II
2 to 8 weeks
YesPositive
Close the previous regis-tration as "Defaulter,"(*2) then re-register as "RAD," open a new treatment card.
Start again on Regimen-II
Negative No, use the same treatment card.
Continue Regi-men-II
More than 8 weeks
Yes
Positive
Close the previous regis-tration as "Defaulter," then re-register as "RAD," open a new treatment card.
Start again on Regimen-II
Negative
Close the previous regis-tration as "Defaulter," the re-register as "Other," but use the same treatment card.
Continue Regimen-II
*2 Thisistheexceptionalcasetodefineas "Defaulter" for a patient who interrupted treatment of less than 8 weeks.

407
tUBERCULOSIS CPM 7th EDItION
Introduction
Why will the National TB Control Program (NTP) shift from Single-Drug Formulation (SDF) Short Course Chemotherapy (SCC) to Fixed-Dose Combinations (FDCs)?
1. It simplifies treatment of TB patients. FDCs will enhance treatment compliance since the number of tablets that a TB patient will take will be reduced. For example, a patient under Regimen I with an average weight will only take three tablets of FDCs instead of six of single-drug formulation (1 Rifam-picin, 2 PZA, 1 INH and 2 Ethambutol) currently being used in the Program. Also, it is easier to cal-culate the required dosage, hence, the risk of’giving wrong dosage will be minimized.
2. It simplifies management of drug supply. This will facilitate the procurement and distribution proc-ess. Instead of ordering anti-TB drug preparation such as BP type I, BP type II and the loose prepa-ration of INH, Ethambutol and PZA from various suppliers, the FDCs and others will be supplied by only one source. This also solves the chronic problem of mismatching of delivery of BP type I and II.
3. ItpreventsmonotherapyorselectiveintakeofantiTBdrugs. This will help reduce the emergence of drug resistant TB.
4. It reduces the risk of using Rifampicin for conditions other than TB.
What is the situation that led to the shift to FDCs?
The Philippines is one of the twenty-two countries with high TB burden. In response to this problem, the Directly Observed Treatment Short Course (DOTS) strategy was initiated in 1996. Within six years more than 90% of the population have access to this strat-egy. One of the major concerns ot NTP in the past years is the availability of effective anti-drugs in the health centers. Hence, there is always a constant search for approaches to improve management of drug supply.
In 2002, the Philippines requested and were granted free anti-TB drugs from the Global Drug Facility (GDF). The preparations are in FDCs and these are expected to arrive in March, 2003. These will be initially distributed and used in selected areas and its use expanded later. This development will require a major change from the single drug formulation of SCC that NTP had used since 1987 to FDCs. This change will require careful planning and systematic implementation to be successful. Hence.
Guidelines on the use of Fixed-Dose Combination Anti-TB Drugs for the National TB Program
these guidelines are prepared to guide the implementors in the advance implementation sites (AIS) in adopting this change.
How will the change from SDF to FDC be implemented nationwide?
Thechangewillbeimplementedinphases.Onthefirstyear, one province or big city per region will use the FDCs. These areas will be selected by the Centers for Health Development (CHD) in consultation with the InfectiousDiseaseOffice-NationalCenterforDiseasePrevention and Control (IDO-NCDPC) and with the agreementof theconcernedProvincialHealthOffice(PHO)orCityHealthOffice(CHO).Theseareaswillhe known as advanced implementation sites (AIS). After a year, the use of FDC will be expanded to other provinces and cities. This staggered implementation will give adequate time to assess the initial experiences and address whatever constraints will arise.
Facts About FDCs
What are FDCs?
The Fixed-Dose Combinations (FDCs) are anti-TB drug preparationswhereby twoormorefirst line anti-TBdrugs are combined in one tablet. There are 2-, 3-, or 4-drugfixed-dosecombinations.
Are FDCs being used in other countries?
Yes. Many countries are already using it. The World Health Organization (WHO) and the International Union Against Tuberculosis (IUATLD) had endorsed the use of FDCs by the NTP since 1994. The 4-drug and 2-drug combinations are included in the WHO Model List of Essential drugs since 1999.
What is the composition of FDCs that will be used in AIS?
There will be two types of FDCs - the 4-drug and the 2-drug combinations. The composition is as follows: See Table 1.
table 1
Drug FDC-A FDC-B 4Drug(RHZE)2Drug(RH)Rifampicin (R) 150 mg 150 mg INH (H) 75 mg 75 mg PZA (Z) 400 mg Ethambutol (E) 275 mg

408
CPM 7th EDItION tUBERCULOSIS
Aside from FDCs, single preparation drug such as ethambutol, pyrazinamide, and streptomycin will be used.
How much is the cost of treatment using FDC per TB patient?
The cost of treating one TB patient belonging to 38 - 54 kg group under Regimen 1 (See Table 2) is almost equal to the cost of the SDF currently being used by NTP (about $11).With simplified procurement anddistribution process, FDC will be more cost-effective than the SDF.
How is the quality of FDC s assured?
One of the issues of FDCs is the bioavailability of rifampicin. To ensure that the FDCs meet the quality requirements, FDCs will be provided through the Global Drug Facility,which supplies FDCs of WHO-recom-mended strengths and of proven quality.
What will be the dosage schedule of FDCs?
The treatment regimens remain the same-- only the
table 2. 2 RhZE/4Rh
Body weight (kg)
No. of tablets per day Intensive
Phase (2 Months) RHZE
No. of tablets per day Continu-ation Phase (4
months) RH
30-3738-5455-70>71
2345
2345
vehicle has changed. The dosage will follow the guidelines of WHO and IUATLD for individual anti-TB drugs as contained in page 26 of the Manual of Procedures (MOP). The number of tablets of FDC per patient will depend on the body weight. Hence, all patients must be weighed (using kilogram as a unit) before treatment is started.
Steps in Introducing FDCs in the Advanced Imple-mentation Sites
How will the FDCs be introduced at AIS?
There will be three phases of implementation:
Phase 1: Preparation of areas
• OrientationofallstaffprovidingantiTBtreatmentsuchasthosefromRuralHealthUnits(RHU),hospital,PPMDclinics.
• OrderinganddistributionofFDC's
Phase 2: Implementation of new treatment guidelines on FDCs:
• IntroductionofFDCs
Phase 3: Monitoring, supervision, and evaluation
It is estimated that initial introduction of FDC in AIS and its evaluation will last for one year. However, this might vary from area to area.
Phase 1: Preparation of areas
Activity 1. Orientation of staff
Whowillbeoriented?
The approach will be like what was done with the DOTS strategy - a cascading approach. The regional and pro-vincial TB coordinators/trainers will orient the doctors
table 3. 2RhZES/RhZE/5RhE
Body weight (kg) Intensive Phase Maintenance PhaseFirst two months Third month
RHZE Streptomycin RHZERH E 400 mg
30-3738-5455-70>71
2345
.75 g
.75 g
.75 g
.75 g
2345
2345
1223
table 4. 2RhZ/4Rh
Body weight (kg) No. of tablets per day Intesive Phase (2 Months)
No. of tablets per day Maintenance Phase (4 months)
RH Z (400 mg) RH30-3738-5455-70>71
2345
2345
2345

409
tUBERCULOSIS CPM 7th EDItION and nurses of the RHUs, hospitals and clinics. They will in turn orient the midwives. The midwife will orient the BHWs and other treatment partners. These guidelines will be used in the orientation.
Whowillfundtheorientation?
The Department of Health, both the IDO- NCDPC and CHD,will be responsible for ensuring that funds are available for the orientation of the regional and provincial/city coordinators and physicians and nurses of RHUs, hospitals and clinics. The LGUs will be requested to fund the orientation of midwives and treatment partners. To reduce the cost, orientation may be done during the regular meeting of midwives and BHWs.
Activity 2: Initial ordering and distribution of drugs
HowwilltheFDCsbedistributed?
The IDO will directly distribute the six-month re-quirement plus a buffer stock of six months (total of 12 months) to the CHD. This will include the FDCs and SDF. The CHD will transfer all these drugs to the PHOs and CHOs of the participating provinces and cities. The provincial/city TB Coordinator will then distribute to the health facilities their three-month re-quirement plus three-month buffer stock for the initial order. Filling-up of the Order Form will be part of the orientation.
Will FDCs be included in the Contract DistributionScheme(CDS)?
For the AIS, the FDC will not be included in the CDS. The CDS is not yet fully implemented and the system does not yet allow inclusion of FDCs.
WhatwillhappentothecurrentsupplyofSDF?
This will depend on the available stocks and expiration dates of the SDF. Hence, all implementing units must conduct an inventory of their anti-TB drugs. They must retain adequate quantity of SDF for TB patients undergoing treatment. The excess must be returned to the PHO/CHO with proper documentation. The pro-vincial TB coordinator will record all these returned drugs. A reserve stock of SDF must be maintained at the PHO/CHO for patients who may need them due to adverse reactions to any of the drug component of FDCs. Allocate SDF for at least 5% of the expected total TB cases in a year. The excess SDF drugs must be returned to the CHD. The latter will distribute this to non-AIS areas.
Howmuchdrugswillbeordered?
To simplify the process of ordering, the number of tablets to be ordered will be based on the weight cat-egory where most of the patientswould fall (i.e., 38-54 kg group). The number of tablets per patient will be
as follows:
Priorities for Regimen 3 are the new cases. For the initial order, the implementing health facilities will compute for one-quarter requirement plus a one month buffer stock. Subsequent order will be for only one quarter. See order form on page 21.
What will be the counterpart of the LGUs re: drugsupply?
The LGUs are expected to share in the procurement of single formulation drug such as INH, PZA, ethambutol and rifampicin.
Phase 2: Implementation of new treatment guide-lines on FDCs
WhenwilltheshiftfromSDFtoFDCsstart?
Start giving the FDCs to newly-registered TB patients once the following conditions are met:
1. All the RHU/ hospital /clinic staff and treatment partners who are involved in the treatment of TB patients had been oriented.
2. Adequate quantity of FDCs are already in the RHUs.
3. Records and reports are in place.
WhatwillhappentothepatientsunderSDF?
TB patients w ho had been initiated with the SDF must continue using these preparation until they have com-pleted the required duration.
WilltheintakeofFDCshesupervised?
Yes. The patient and the treatment partner will agree upon the time of drug intake. It must be two hours after a regular meal.
WhatiftherearesideeffectstoFDCs?
If there are major side effects, the responsible drug must be discontinued. In this situation, shift from FDC to SDF. Studies showed that this might happen to about 5% of total cases. Hence, RHUs must have at least sup-plied of SDF for two patients. The PHO will also have a reserve of SDF for this situation.
Wouldtherebenewrecordsandreports?
There will be no change in the format or content of treatment records and reports. However, to facilitate
Regimen 1Regimen 2Regimen 3
RhZE Rh Z E Streptomycin
No. of blister packs No. of vials69
121518 6
5610

410
CPM 7th EDItION tUBERCULOSIS
monitoring and evaluation, records of TB patients under FDCs must be marked. For the Treatment Cards, put a red bar (-) using a red ink pen at the right upper corner. For the NTP Registry, put a red asterisk (*) opposite thefirstentryofthefirstpatientunderFDCandalsowrite under comments the “start of FDC”.The patient number must be continuous.
Phase 3: Monitoring, supervision and evaluation of implementation
What will be the process of monitoring and evalua-tion?
It is important that the entire process be regularly monitored and assessed. Supervision is also critical in ensuring that the guidelines are properly implemented. Lessons gathered during this advanced implementation will be useful during the expansion to other areas.
Regional and provincial/city coordinators must moni-tor the implementing health facilities monthly during thefirstthreemonthsofimplementationandquarterlythereafter. Provincial or city quarterly assessment must also be organized by the regional and provincial/city coordinators. The results must be sent to IDO-NCDPC. The latter will convene semi-annual evaluation work-shop of the FDC implementation at AIS.
The physician and nurse of the RHUs, clinics and hos-pitals will then supervise their subordinates.
What will be supervised?
The supervisors must observe how the staff does the following activities:
• orientation of midwives and treatment partners• giving instructions by health staff to TB patients• dosage given to patients• drug intake of TB patients• management of side effects• filling-upof treatment records suchasTreatment
Card and NTP Registry• preparing reports• storage and distribution of drugs• filling-upofOrderForm
Feedback must be immediately provided to the supervi-sor and the next higher level.
What will be monitored and evaluated?
The following guide questions will help in the monitor-ing and evaluation of various program activities:
Orientation of staff
• Were all the staff oriented? If not, why?• What is the duration of orientation per category of
health workers?• What approaches were used in the orientation (e.g.,
modular, lecture type)? Which is the most cost-ef-
fective approach?• Were funds available and adequate?• Were the guidelines useful? Are there things to be
changed? Added? Deleted?• What were the common issues raised during the
orientation?Whatissuesneedclarification?
FDC ordering and distribution
• What was the ordering and distribution process used? What were the constraints?
• Is theorderingformappropriate?Properlyfilled-up?
• Did the FDCs come on time?• Were they adequate?• Were there problems in storage?• Were there buffer stocks?• Were there SDF reserve stocks at the province? At
the RHU?
FDC distribution to patients
• Wasthereanydifficultyinexplainingthetreatmentprotocol? By doctors? Nurse? Midwife? Treatment partner?
• Did the patient understand and follow the instruc-tions?Anyspecificdifficulty’?
• Were there instances that SDF need to be given for adverse reactions? What percentages of cases need the SDF? Are these available? At what level?
• What are the feedbacks from TB patients? From treatment partners?
• Is there a problem in recording?
Monitoring, supervision and evaluation
• How frequent was the monitoring done by the pro-vincial/regional coordinator?
• How frequent was the supervision done by doc-tors/nurses?
• What are the common issues/ problems en-countered?
• Was feedback given to higher level and supervisor?• Is there a problem in reporting?• Were there quarterly assessment conducted? What
were the results?
Treatment outcome
• How is the treatment outcome compared to the outcome before FDC implementation?
NOtE:
Policies and guidelines of other program components suchascasefinding,caseholding,sputumfollow-up,health education, recording and reporting and others shall still be based on the 2001 Manual of Procedures.
Management of side effects of FDCs
There are major side effects that necessitate withdrawal

411
tUBERCULOSIS CPM 7th EDItION of the responsible drug. In this case, FDC must be changed to SDF.
Policies on the use of the Fixed-Dose Combination (FDC) anti-tB drugs to be incorporated in the manual of procedures of the National tuberculosis Control Program
1. The Fixed-Dose of Combination (FDCs) Anti-TB drugs will gradually replace the Single Drug For-mulation (SDF) for treatment of TB patients under the National Tuberculosis Control Program (NTP). The FDCs shall be initially introduced in one prov-ince or city per region, which will be known as the Advanced Implementation Sites (AIS). After a year of experience on FDCs at AIS, this will be expanded to other provinces and cities until all the regions are using the FDCs.
2. The dosage schedule will be in accordance to the internationally prescribed dosage. Intake must be supervised.
3. The Department of Health will provide the FDCs to the local government units and the other health facilities for free. However, LGUs will be encour-aged to procure a portion of the requirements for SDF for those with adverse reactions necessitating withdrawal of FDC.
4. Staff of health facilities such as Rural Health Units, hospitals, government and private clinics and treat-ment partners who will be involved in treatment of TB cases shall be properly trained on the use of FDCs and other new treatment guidelines.
5. Quality of FDCs must be ensured by ordering them from a source with track record of producing FDCs according to World Health Organization (WHO) prescribed strength and standards of quality.
6. The shift from SDF to FDC will be regularly monitored and assessed by the Infectious Disease Office-NationalCenterforDiseasePreventionandControl, Centers for Health Development. Provin-cialHealthOfficesandtheCityHealthOffices.
.
Drug FDC-A4Drug(RHZE)
FDC-B2Drug(RH)
Rifampicin (R)INH (H)PZA (Z)Ethambutol (E)
150 mg
75 mg400 mg275 mg
150 mg75 mg
FACtS ABOUt FDC
Thefixed-dosecombination(FDCs)areanti-TBdrugpreparationswhereby twoormorefirst line anti-TBdrugs are combined in one tablet. The WHO and the International Union Against Tuberculosis recommend the use of FDCs since 1994. They are also included in the WHO Model List of Essential Drugs.
There will be two types of FDCs. These are the 4-drug and the 2-drug types that will be used by NTP. The composition will be as follows:
Initial supply will be provided through the Global Drug Facility--a project of the STOP TB Partnership.
The FDC and single drug formulation of ethambutol and pyrazinamidearefilm-coatedtabletsandpackagedinblister packs. There are 28 tablets per blister pack.

412
tUBERCULOSIS CPM 7th EDItION
Drugs Mentioned in the Treatment Guideline
AntituberculosisEthambutol Am-Europharma Ethambutol HCl Biogenerics Ethambutol Odetol Pharex EthambutolEthambutol/Isoniazid/Vit B6
Alveodril/ Alveodril Forte Ebutol EMB Forte Etham 500 Ethambin-INH Ethamizid Ethi 400 Fevram Forbutol Norvit Plus PacibutolEthambutol/Isoniazid/
Rifampicin MyrinEthambutol/Rifampicin/
Isoniazid/Pyrazinamide 4D Econokit Econokit-MDR Myrin-P Forte Quadtab Rimstar 4Ethambutol/Rifampicin/Pyrazi-
namide/Vitamins Continukit PlusEthambutol/Rifampicin/ Pyrazinamide/Isoniazid/
Vitamins SCC Kit ViperIsobutol/Rifampicin/Pyrazina-
mide Molecure 1 & 2Isoniazid Am-Europharma Isoniazid Bacciter Biogenerics Isoniazid Curazid Forte
Thisindexlistsdrugs/drugclassificationsmentionedinthetreatmentguideline.Prescribinginformationofthesedrugs can be found in PPD reference systems.
Norvit Pharex Isoniazid UL Isoniazid 400Isoniazid/Rifampicin Continupack Isoniazid/Vit B6
Comprilex Pediatric Syrup Isoxin Koccid Nicetal Norvit Plus Odinah Therabacule Trisofort Trisovit UL Isoniazid 400Isoniazid/Vitamins Trisofort TrisovitPyrazinamide Am-Europharma Pyrazinamide Biogenerics Pyrazinamide Drugmaker's Biotech
Pyrazinamide Mycobak Pharex Pyrazinamide Pyramin Pyrasol PZA-Ciba RiteMED Pyrazinamide Zapedia Zcure ZinaplexRifampicin Am-Europharma Rifampicin Biogenerics Rifampicin Carfamin Crisarfarm Dipicin Drugmaker's Biotech
Rifampicin Fampisec Fevram Koccifam Lypro-cap Medifam
Natricin Forte Odifam Pharex Rifampicin PMI Rifampicin Ramicin Refam Rexilan Ricyn Rifadin Rifamax Rimactane Rimaped RiteMED Rifampicin TubercoxRifampicin/Isoniazid Bifix Continupack Kidz Kit 2 Rifinah Rifzin Rimactazid 225/Rimactazid
300/Rimactazid 450/ Rimactazid 600
Rifampicin/Isoniazid/Ethambutol Combikids Combi Pack Continukit TRES Tri-Pack TritabRifampicin/Isoniazid/Pyrazina-
mide Bio Combi Pack 1/Bio Combi Pack 2 Econopack Econopack-TDR Kidz Kit 3 M-O-P/M-O Compliance Pack Rifater Streptomycin YSS Streptomycin Sulfate