national partnership to improve dementia care in nursing ... · quality assurance and performance...
TRANSCRIPT

National Partnership to Improve Dementia Care in Nursing Homes & Quality Assurance and Performance Improvement (QAPI)
December 14, 2017

2
• AHCA - American Health Care Association
• BPSD - Behavioral and Psychological Symptoms of Dementia
• CDC - Centers for Disease Control and Prevention
• CMP - Civil Money Penalty
• DON - Director of Nursing
• IDT - Interdisciplinary Team
• MVH - Maine Veterans’ Homes
• PIP - Performance Improvement Project
• PRN - Pro Re Nata
• QAA - Quality Assessment and Assurance
• QAPI - Quality Assurance and Performance Improvement
• QIN-QIO - Quality Innovation Network – Quality Improvement Organizations
• SHC - Signature HealthCARE
• SNF - Skilled Nursing Facility
• TO - Telephone Orders
• UTI - Urinary Tract Infections
Acronyms in this Presentation

3
Working with Physicians to Ensure Dr. Arif Nazir, Signature HealthCARE
Compliance with the New Psychotropic
Prescribing Requirements
Putting the New QAPI Requirements Debra Lyons, CMS
into Practice Debra Fournier, Maine Veterans' Homes
Sarah Schumann, Brookside Inn (Colorado)
Agenda

4
Working with Physicians to Ensure Compliance with the New Psychotropic Prescribing Requirements
Arif Nazir MD FACP CMD
Associate Clinical Professor of Family and Geriatric Medicine,
University of Louisville,
Chief Medical Officer, Signature HealthCARE

5
• Describe prevalence of behaviors among residents living with dementia in Skilled
Nursing Facilities (SNF)
• List serious side effects of pharmacologic options
• Describe role of physician leaders in appropriate psychotropic prescribing
• Describe impact of facility culture and staff competence for high quality care for
dementia
Objectives

6
• A 3-star urban facility with 125 beds
• Psychotropic rates are above State average
• At the QAPI meeting Director of Nursing (DON) announces “we will cut
psychotropics by 50%”
• Committee is formed and Dr. Smith (medical director) is invited
• The DON and social director are other members
• What’s the best initial advice Dr. Smith should provide?
QAPI at Happy Fellows Facility

7
1. Utilize pharmacy consultant better so he can provide a taper schedule on all
residents, unless contraindicated
2. Facility assessment of quality of care and team member competence
3. Ask hospital psychiatrist to provide consulting services at the facility
4. Build a multi-sensory room by next quarter
Select Best First Step to Impact Psychotropic Use

8
• Of the estimated 5.5 million Americans living with Alzheimer's dementia in 2017, an
estimated 5.3 million are age 65 and older
• BPSD affect up to 90% of those diagnosed with dementia at any given point in the
duration of their illness
Prevalence of Behavioral and Psychological Symptoms of Dementia (BPSD)

9
BPSD
• Verbal or Physical
• Aggression
• Personality clashes
• Wandering
• Depression
• Resistance with activities of
daily living
• Screaming• Suspiciousness,
accusations, paranoia• Insomnia• Repetitive questions or
demands• Sexually inappropriate
1) Baumgarten M, et al. Ann Intern Med 1994
2) 2) International Psychogenic Association, Behavioral and Psychological Symptoms of Dementia Educational Pack,
Module 4, 1998

10
• Impaired quality of life
• Rapid cognitive decline, and tremendous caregiver burden
• Shortened time to nursing home placement by as much as 2 years
• Some studies report increased mortality
• Higher cost of care
Effects on the Resident
Phillips VL, Diwan S, J Am Geriatr Soc. 2003;51{2}:188-193
Salzman C, Jeste DV, Meyer RE, et al. J clin Psychiatry.2008:69(6):889-898

11
• Three possible strategies:• Use non-pharmacologic approach
• Use pharmacologic approach
• Use a combo
• But how to decide?
• Taking the best approach requires sound person-centered reasoning
• Besides the Interdisciplinary Team (IDT), role of physicians, other practitioners, and
medical directors is critical
Tackling BPSD in Nursing Homes

12
• Collect and analyze information
• Detailed problem identification
• Decide on interventions
• Monitor and adjust
Assessing BPSD: No Different than other Clinical Conditions
Reforming Management of Behavior Symptoms and Psychiatric Conditions in Long-Term Care Facilities: A Different Perspective.
Levenson, Steven A. et al. Journal of the American Medical Directors Association , Volume 18 , Issue 4 , 284 - 289

13
• Accept heterogeneity and drop “biases”
• Most symptoms are non-specific and not diagnostic
• Caution against treating prematurely (e.g. agitation)
• Premature intervention could lead to harm
• Team needs to decipher the “story” behind the complaint and its impact on the
resident and others
• Important to consider broad differential diagnosis
BPSD Assessment Key Principles:
Reforming Management of Behavior Symptoms and Psychiatric Conditions in Long-Term Care Facilities: A Different Perspective.
Levenson, Steven A. et al. Journal of the American Medical Directors Association , Volume 18 , Issue 4 , 284 - 289
14
• Medical causes: delirium, medical conditions, medications
• Major psychiatric causes: psychosis, exacerbation of chronic mental illness
• Mood and anxiety disorders: anxiety, depression, demoralization, etc.
• Other: rare medical causes, substance-abuse, personality disorder
• Role of dementia and other neurocognitive disorders
• Role of environmental and psychosocial causes
Differential Diagnosis:

15
Facility Factors May Contribute to BPSD
Personnel Environmental
Changes in schedule
Changes in caregivers
Rushing with care
provided
Not talking to and
comforting the resident
Surprising the resident
Noisy areas – or areas
with many sources of
noise at one time
Poor lighting
Rooms that are too hot
or too cold
Being left alone for long
periods of time
16
• Vitals and detailed examination every time
• Assessing and managing pain (avoid opioid use as first-line)
• “Cleaning” diagnoses list (encephalopathies, psychosis, delirium, organic brain
syndrome, etc.)
• Comprehensive medication review with de-prescribing questionable medications
• Formal Advance Care Planning to understand resident/family/representative goals
of care
Key Broad Interventions
17
• Music therapy
• Activities and physical exercise
• Light therapy
• Aromatherapy
• Interactive dolls and pets
• Cognitive rehabilitation
• Multi-sensory rooms
Individualized Non-Pharmacologic Approaches
De Oliveira AM, Radanovic M, de Mello PCH, et al. Nonpharmacological Interventions to Reduce Behavioral and
Psychological Symptoms of Dementia: A Systematic Review. BioMed Research International. 2015;2015:218980.
doi:10.1155/2015/218980.

18
• Avoid generic approaches including sole focus on de-prescribing
• Individualize care plans for specified behaviors and document impact of intervention
• Modify plan as new “intel” received
• Intensify monitoring if medication is added with clear criteria to adjust/discontinue if
ineffective
• Role of consultants is key, they need to be integrated into the team
Active Monitoring of BPSD

19
• Not U.S. Food & Drug Administration approved for BPSD
• Serious adverse effects (pneumonia, stroke, and death)
• >1.5 times mortality risk (atypical and conventional antipsychotic agents)
• For BPSD used after non-pharmacologic approaches maximized and detailed risk/benefit discussions
• Residents living with dementia at high risk of inappropriate use
• SNFs with large number of providers at high risk of inappropriate use
How About Antipsychotic Rx Options?
Organizational Factors Associated With Inappropriate Neuroleptic Drug Prescribing in Nursing Homes: A Multilevel Approach.
Laffon de Mazières, Clarisse et al. Journal of the American Medical Directors Association , Volume 16 , Issue 7 , 590 - 597

20
• Systematic review of 23 double blind randomized controlled trials
• Conclusion: Aripiprazole and Risperidone may show benefit that may be offset by
adverse effects
Antipsychotic Medications: Are there Benefits?
Tan et al. Alzheimer's Research & Therapy (2015) 7:20;DOI 10.1186/s13195-015-0102-9

21
• Review resident’s overall health/care
• Clear definition and documentation
• Regular orientation/interaction needed (just like 3 hour turning!)
• Medications will not help unless etiology addressed
• Multipronged intervention
• Recurrence is high and expected
• Stop medications once wound is healed
Think of Behavior as a Pressure Ulcer

22
1. Utilize pharmacy consultant better so he can provide a taper schedule on all
residents, unless contraindicated
2. Facility assessment of quality of care and team member competence
3. Ask help from hospital psychiatrist to provide consulting services at the facility
4. Plan to build a multi-sensory room by next quarter
Back to Case: Select Best Advice By Dr. Smith

23
• Review overall care practices:• Person-centered approaches, staff competence broadly and around behaviors, polypharmacy,
INTERACT etc.
• Behavior team that includes a physician, frontline staff, pharmacy, social services,
nursing
• Focus on documenting, assessing, and monitoring behaviors
• Detail history (resident/family/staff) to plan non-pharmacological measures
• Use psychotropics as last resort:• Risk/benefit discussion with resident/family/representative
• Target behaviors noted/monitored after start of treatment
• Clear documentation about side effect monitoring
• Consider gradual dose reduction once behaviors resolve
• Psychiatric consultation for difficult behaviors, only after doing “homework”
Recommended Plans for Improving Behavior Care at Your Facility

24
• Psychotropic definition expansion: any drug that affects brain activities associated
with mental processes and behavior (antipsychotic, anti-depressant, anti-anxiety,
hypnotic)
• Pro Re Nata (PRN) use limited to 14 days with extension based on prescriber
rationale
• Renewal of anti-psychotic medications requires prescriber evaluation of the resident
Recent Changes to Antipsychotic and Psychotropic Prescribing-Final Rule

25
Updated Pharmacy Tags
F757
Drug Regimen is Free From
Unnecessary Drugs F329
F758
Free from Unnecessary Psychotropic
Medications/PRN Use F329
F758
Free from Unnecessary Psychotropic
Medications/PRN Use F428
F759
Free of Medication Error Rates of 5%
or More F332
F760
Residents Are Free of Significant
Medication Errors F333
26
• For all psychotropics: • Attempt in 2 separate quarters separated by month (unless clinically contraindicated)
• After 1 year, perform annually unless contraindicated
• Clear prescriber documentation needed for psychotropics, regardless of the
indication - dementia vs. bipolar, schizophrenia, other psychoses• Why it is being used
• What non-pharmacologic approaches have been tried
Gradual Dose Reduction Schedules

27
Clinical Practice Guidelines

28
Signature HealthCARE Holistic Approach
Person-centered
BPSD Care
Staff Training
Quality of Life
Initiatives
Medical Director
Role
Special Team
(Serenity Care)
29
• Setting expectations around key aspects of their role
• Ongoing education through articles and webinars
• Their role in disseminating evidence-based practices
• Role in resident-side education for IDT
• Focus on polypharmacy (not just psychotropics)
• Specialized focus on Advance Care Planning discussions
• American Medical Directors Association membership and professional development
• Medical Director Scorecard (coming soon)
Engaging Medical Directors

30
• iCARE approaches
• Eden Alternative registries
• Resident vacations
• Senior Olympics
• Patient surveys
• Others
Signature HealthCARE (SHC) Quality of Life Initiatives

31
• Customer service training provided to all stakeholders
I-Care Approaches

32
• 46 registered; 2 Milestone 4, 13 on Milestone 3, and rest on Milestone 2
Eden Alternative Registry
General Stores offer purpose! Archie’s Café is a replica of a local favorite!

33
• Creating “normalcy” in resident’s lives
• Offering residents new opportunities for growth and exploration
SHC Resident Vacations
Celebrating their 60th at Disney World! First time at Fenway Park!

34
• Increases/improves self-esteem and confidence
• Competition is part of normal life!
Senior Olympics

35
• Summer Camps
• After school groups
• “Snow Days” groups
Intergenerational Connectedness

36
• Serenity Development Model• Behavioral specialists
• Free-Standing Behavioral Health Centers (nursing facilities specializing in behavioral health)
• Behavioral Risk Management Center – a call center to assist residents with the management of
chronic behavioral health
Serenity HealthCARE
37
• BPSD are burdensome for residents and staff
• Physicians and medical directors are key team members
• Focus on facility culture and competence for high quality care lays the foundation
• Detailed history and assessments are key to individualized care for BPSD
• If used, antipsychotic medications should be regularly reviewed and dose-
reduction performed
Summary

38
• Arif Nazir MD
989-906-3932
Thank You!

39
Putting the New QAPI Requirements into Practice
Debra Lyons, CMS
Debra Fournier, Maine Veterans' Homes (MVH)
Sarah Schumann, Brookside Inn - Colorado
40
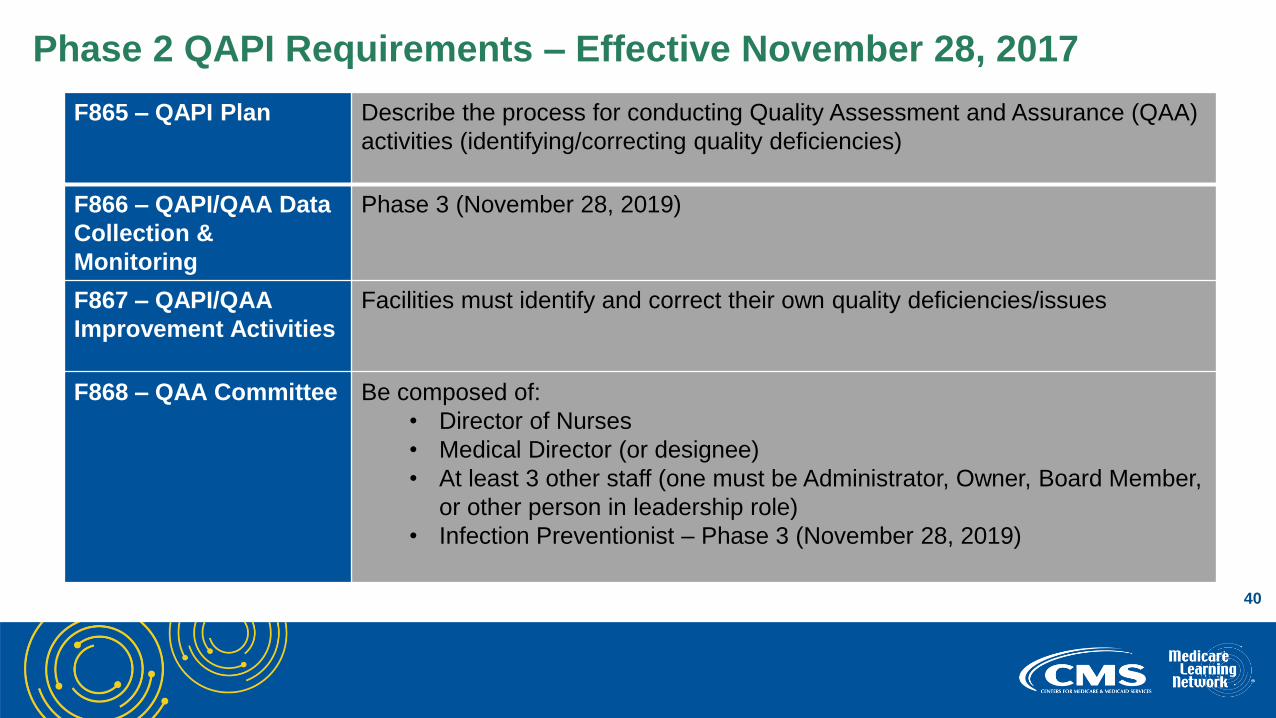
Phase 2 QAPI Requirements – Effective November 28, 2017
F865 – QAPI Plan Describe the process for conducting Quality Assessment and Assurance (QAA)
activities (identifying/correcting quality deficiencies)
F866 – QAPI/QAA Data
Collection &
Monitoring
Phase 3 (November 28, 2019)
F867 – QAPI/QAA
Improvement Activities
Facilities must identify and correct their own quality deficiencies/issues
F868 – QAA Committee Be composed of:
• Director of Nurses
• Medical Director (or designee)
• At least 3 other staff (one must be Administrator, Owner, Board Member,
or other person in leadership role)
• Infection Preventionist – Phase 3 (November 28, 2019)

41
MVH:• An independent non-profit organization caring for Maine’s Veterans and their families
• 5 skilled nursing care centers ranging from 40-120 beds each
• Core values of excellence, team, and lead the way are driving direction of programs
• Strategic priority is hardwiring excellence
• American Health Care Association’s (AHCA) Quality Award Program
• Performance Excellence Framework from Malcolm Baldrige Quality Program
42
Where did we start?
• Structure• QAA committees were in place at the homes
• Began applying for AHCA Bronze Level Quality Award
• Organizational profile
• Formed a corporate steering committee: QAPI Workgroup
• Senior leaders from 6 homes and central office
• Developed charter for the workgroup
• Develop and implement MVH QAPI plan
• Develop and implement a results dashboard
• Develop a data driven decision making culture that is transparent without blame
• Implemented governing body oversight and reporting structures
Putting QAPI into Practice

43
What tools did the MVH QAPI
Workgroup use to develop the
QAPI Program and Plan?
• QAPI self-assessment
• QAPI at a glance
• Performance Excellence FrameworkR
• Prioritization and key measure matrix
tools
Tools for QAPI Program and Plan Development

44
What tools were used to operationalize
QAPI?
• Standardized QAPI education
• MVH Results Dashboard
• Plan Do Check Act methodology for
improvement
• Performance Improvement Project (PIP) tools
and education
• Root Cause Analysis tools and education
• Prioritization Matrix tool
• Data Monitoring Matrix tool
• Staff town hall meetings
Tools to operationalize QAPI

45
• Education – 21 times to learn new behaviors and hardwire
• Data Analysis
• PIP Facilitation
• Champion
• Leadership, Leadership, Leadership
• Importance of Improvement Mindset
Challenges
46
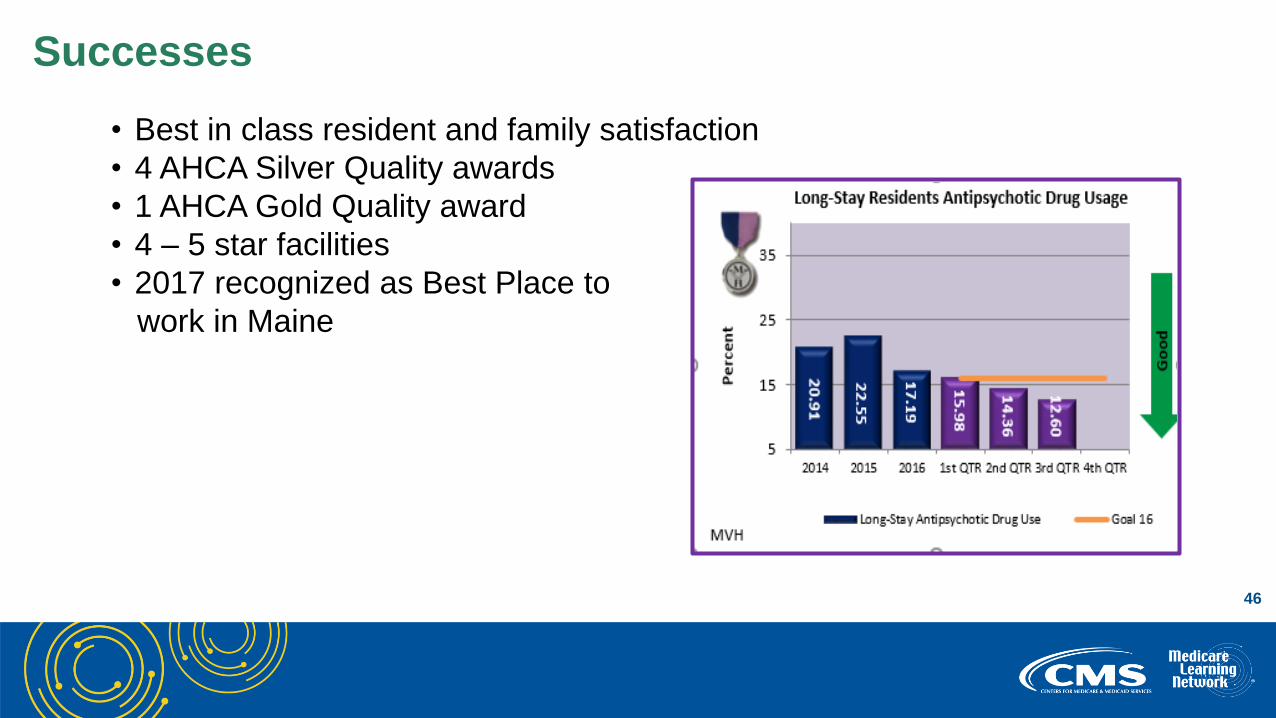
• Best in class resident and family satisfaction
• 4 AHCA Silver Quality awards
• 1 AHCA Gold Quality award
• 4 – 5 star facilities
• 2017 recognized as Best Place to
work in Maine
Successes

47
Next steps• Facility Assessment
• Continued hardwiring of systems for sustaining excellence
• Celebration and acknowledgment of achievements and successes
Next Steps

48
• Debra Fournier, MSB, CPHQ, NHA
Chief Operations Officer
Maine Veterans’ Homes
mobile: 207-671-1996
Contact Information
49
• Independently owned, serving 120 residents
• Commitment to Quality• QAA monthly meetings since inception (20 years)
• Recipient of Silver Award based upon Baldrige Criteria through AHCA
• CMS Five-Star Quality Rating
Brookside Inn Skilled Nursing Facility
50
• Identify a Champion
• Involvement and commitment from Board for QAPI
• “We have data, lots of data”
• “Now what do we do???”• Review data and compare to the QAPI dashboard goals
• Do a root cause analysis and PIP if appropriate
• Review daily at IDT meeting, weekly to subcommittees and/or QAPI as appropriate
• Communication to and involvement of staff, residents and family about QAPI PIPs
QAPI Evolution at Brookside Inn

51
• Telligen – Colorado Quality Innovation Network – Quality Improvement
Organizations (QIN-QIO)
• AHCA
• Colorado Medicaid Pay for Performance Program
• CMS resources – QAPI tools, QAPI self-assessment
• Team training by Board, each other and by consultant
• Colorado Department of Public Health and Environment – Epidemiology Division
• Electronic Medication Administration Record and Software Systems
Resources Utilized to Implement QAPI

52
Establish a process and educate to that process• Identify a Champion – Director of Nursing Services available 24/7 to support staff
• Constant communication and education to staff, physicians, residents
• Commitment of Brookside Inn for non-pharmacological interventions
• High psycho-social staffing pattern (1:12 ratio)
• Complementary and Alternative Modalities
• Spiritual Services program
• IDT reviews telephone orders (TO) daily
• Review, track and trend data at QAPI
• Compare outcomes to established goals
• Root cause analysis and PIP as needed
• Adjust process, implement new interventions
• Monitor results and success
QAPI Projects: Medication Review and Reduction Success

53
• Communication
• Abundance of Data
• Maintaining a focus on QAPI with all of the competing demands
• New Requirements of Participation: Integrating the Facility Assessment
• Changes in staff, physicians and residents• Continual education required
QAPI Projects: CHALLENGES
54
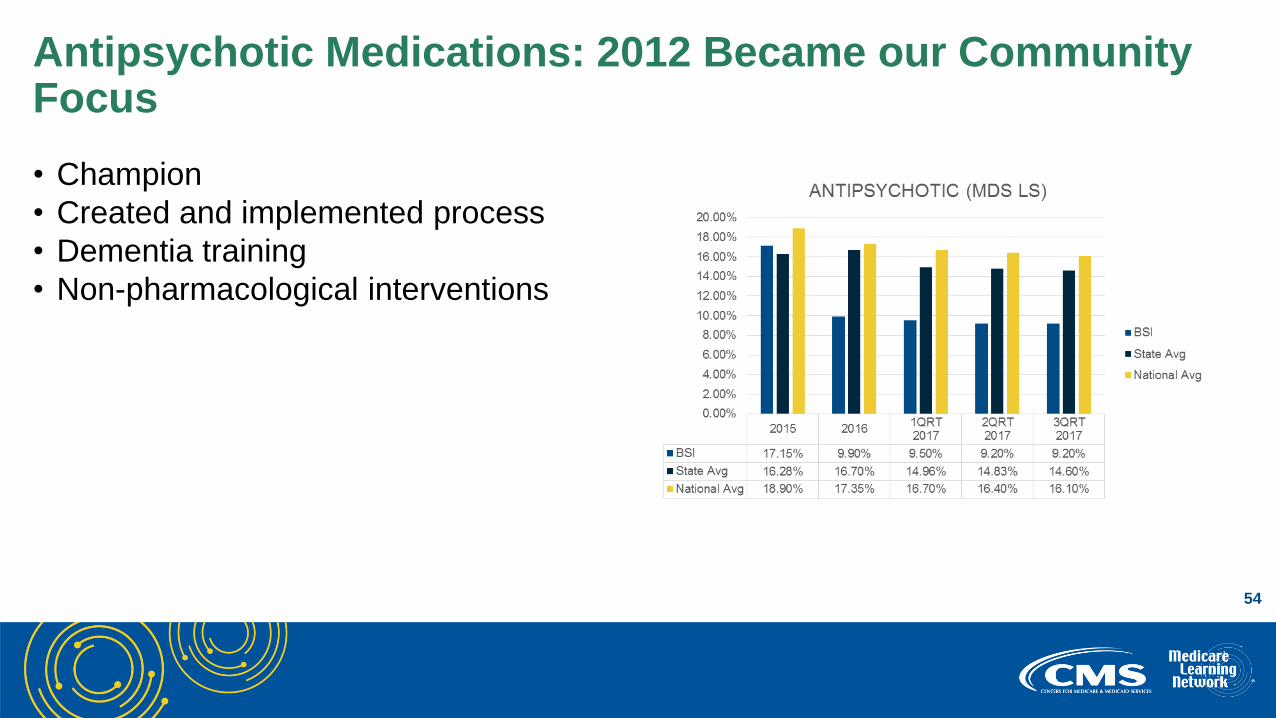
• Champion
• Created and implemented process
• Dementia training
• Non-pharmacological interventions
Antipsychotic Medications: 2012 Became our Community Focus

55
• Implemented Centers for Disease
Control and Prevention (CDC)
Core Elements of Antibiotic
Stewardship in long-term care
• McGeer’s Criteria implemented
for urinary tract Infections (UTI),
upper respiratory infections, skin
& soft tissue infections
Antibiotic Stewardship: 2015 Became our Community Focus

56
• January 2017 began to track community usage
• Champion
• Implemented process utilized for psychotropic and antibiotics stewardship
• CMS and CDC resources for calculating the total daily dose of opioids
• Review TOs daily
• Pharmacy consultant critical to success
• Year to date success: reduction of 5 prescriptions in our community, with pain still
being managed
Opioid Medications: 2017 Became our Community Focus
57
• Sarah C. Schumann, M.Div.
Brookside Inn Skilled Nursing Facility
Castle Rock, CO
720-573-4335
Contact Information

58
• CDC Calculating Total Daily Dose of Opioids for Safer Dosage
• CMS Opioid Oral Morphine Milligram Equivalent Conversion Factors
• Nursing Home QAPI Webpage
• QAPI Written Plan - How To Guide
• QAPI at a Glance
• QAPI Self-Assessment Tool
• Baldrige Excellence Framework
• Locate your QIN-QIO: http://qioprogram.org/contact
QAPI Resources

59
National Partnership Updates
Michele Laughman, CMS
60
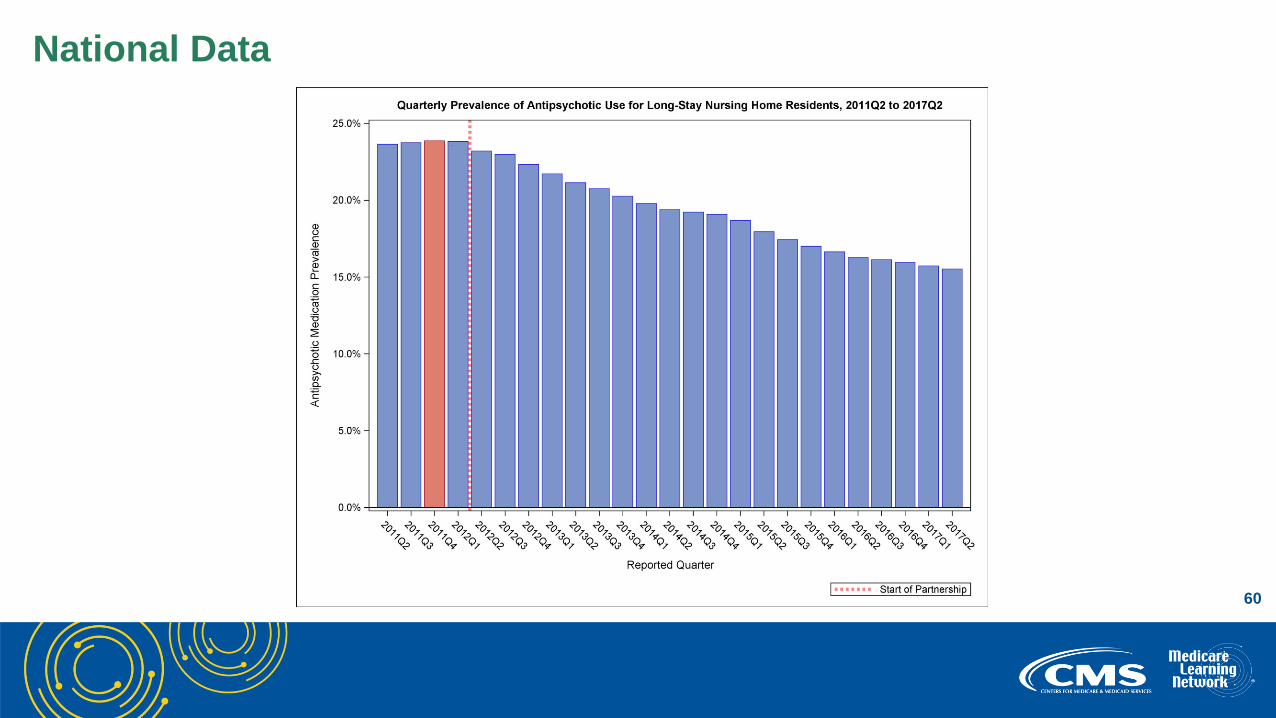
National Data

61
Regional Data

62
• Nursing homes with low rates of antipsychotic medication use are encouraged to
continue their efforts and maintain their success
• Nursing homes with high rates of use are to work to decrease antipsychotic
medication use by 15 percent, for long-stay residents, by the end of 2019
https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2017-Fact-Sheet-items/2017-10-02.html
2019 Goal

63
Best Practice Strategies:• Direct facility outreach
• Workshops and conferences
• Training opportunities (i.e., Hand in Hand training series)
• Use of Civil Money Penalty (CMP) funds for –
• Education/Training
• Conferences
• Implementation of person-centered intervention strategies (i.e., Music and Memory Program)
State Dementia Care Coalition Best Practice Strategies
State Dementia Care Coalitions

64
• Collaboration with State Dementia Care Coalitions, CMS Regional Offices, and
State Survey Agencies
• Comprehensive focus on poor performing nursing homes
• Focused Dementia Care and Schizophrenia Surveys
• Revision of Hand in Hand training series
• Data tracking and distribution
• Federal CMP fund initiative
• Medicare Learning Network calls
What’s Ahead

65National Nursing Home Quality Improvement Campaign Webpage
Resources & Tools

66
• Visit the National Partnership to Improve Dementia Care in Nursing Homes
webpage
• Contact us at [email protected]
National Partnership Resources
67
Question & Answer Session

68
Share your thoughts to help us improve – Evaluate today’s event
Visit:
• MLN Events webpage for more information on our conference call and webcast presentations
• Medicare Learning Network homepage for other free educational materials for health care professionals
The Medicare Learning Network® and MLN Connects® are registered trademarks of the U.S. Department of Health and Human Services (HHS).
Thank You – Please Evaluate Your Experience
69
This presentation was current at the time it was published or uploaded onto the web. Medicare policy
changes frequently so links to the source documents have been provided within the document for your
reference.
This presentation was prepared as a service to the public and is not intended to grant rights or impose
obligations. This presentation may contain references or links to statutes, regulations, or other policy
materials. The information provided is only intended to be a general summary. It is not intended to take
the place of either the written law or regulations. We encourage readers to review the specific statutes,
regulations, and other interpretive materials for a full and accurate statement of their contents.
Disclaimer