national institute on drug abuse (nida) principles of drug ... · 2 table of contents principles of...
TRANSCRIPT

1
NationalInstituteonDrugAbuse(NIDA)
PrinciplesofDrugAddictionTreatment:AResearch-BasedGuide(ThirdEdition)
LastUpdatedJanuary2018
https://www.drugabuse.gov

2
TableofContents
PrinciplesofDrugAddictionTreatment:AResearch-BasedGuide(ThirdEdition)
Preface
PrinciplesofEffectiveTreatment
FrequentlyAskedQuestions
DrugAddictionTreatmentintheUnitedStates
Evidence-BasedApproachestoDrugAddictionTreatment
Resources
Acknowledgments

3
Preface
Drugaddictionisacomplexillness.
Itischaracterizedbyintenseand,attimes,uncontrollabledrugcraving,alongwithcompulsivedrugseekingandusethatpersisteveninthefaceofdevastatingconsequences.ThisupdateoftheNationalInstituteonDrugAbuse’sPrinciplesofDrugAddictionTreatmentisintendedtoaddressaddictiontoawidevarietyofdrugs,includingnicotine,alcohol,andillicitandprescriptiondrugs.Itisdesignedtoserveasaresourceforhealthcareproviders,familymembers,andotherstakeholderstryingtoaddressthemyriadproblemsfacedbypatientsinneedoftreatmentfordrugabuseoraddiction.
Addictionaffectsmultiplebraincircuits,includingthoseinvolvedinrewardandmotivation,learningandmemory,andinhibitorycontroloverbehavior.Thatiswhyaddictionisabraindisease.Someindividualsaremorevulnerablethanotherstobecomingaddicted,dependingontheinterplaybetweengeneticmakeup,ageofexposuretodrugs,andotherenvironmentalinfluences.Whileapersoninitiallychoosestotakedrugs,overtimetheeffectsofprolongedexposureonbrainfunctioningcompromisethatabilitytochoose,andseekingandconsumingthedrugbecomecompulsive,ofteneludingaperson’sself-controlorwillpower.
Butaddictionismorethanjustcompulsivedrugtaking—itcanalsoproducefar-reachinghealthandsocialconsequences.Forexample,drugabuseandaddictionincreaseaperson’sriskforavarietyofothermentalandphysicalillnessesrelatedtoadrug-abusinglifestyleorthetoxiceffectsofthedrugsthemselves.Additionally,thedysfunctionalbehaviorsthatresultfromdrugabusecaninterferewithaperson’snormalfunctioninginthefamily,theworkplace,andthebroadercommunity.
Becausedrugabuseandaddictionhavesomanydimensionsanddisruptsomanyaspectsofanindividual’slife,treatmentisnotsimple.Effectivetreatmentprogramstypicallyincorporatemanycomponents,eachdirectedtoaparticularaspectoftheillnessanditsconsequences.Addictiontreatmentmusthelpthe

4
individualstopusingdrugs,maintainadrug-freelifestyle,andachieveproductivefunctioninginthefamily,atwork,andinsociety.Becauseaddictionisadisease,mostpeoplecannotsimplystopusingdrugsforafewdaysandbecured.Patientstypicallyrequirelong-termorrepeatedepisodesofcaretoachievetheultimategoalofsustainedabstinenceandrecoveryoftheirlives.Indeed,scientificresearchandclinicalpracticedemonstratethevalueofcontinuingcareintreatingaddiction,withavarietyofapproacheshavingbeentestedandintegratedinresidentialandcommunitysettings.
Aswelooktowardthefuture,wewillharnessnewresearchresultsontheinfluenceofgeneticsandenvironmentongenefunctionandexpression(i.e.,epigenetics),whichareheraldingthedevelopmentofpersonalizedtreatmentinterventions.Thesefindingswillbeintegratedwithcurrentevidencesupportingthemosteffectivedrugabuseandaddictiontreatmentsandtheirimplementation,whicharereflectedinthisguide.
NoraD.Volkow,M.D.DirectorNationalInstituteonDrugAbuse

5
PrinciplesofEffectiveTreatment
1. Addictionisacomplexbuttreatablediseasethataffectsbrainfunctionandbehavior.Drugsofabusealterthebrain’sstructureandfunction,resultinginchangesthatpersistlongafterdrugusehasceased.Thismayexplainwhydrugabusersareatriskforrelapseevenafterlongperiodsofabstinenceanddespitethepotentiallydevastatingconsequences.
2. Nosingletreatmentisappropriateforeveryone.Treatmentvariesdependingonthetypeofdrugandthecharacteristicsofthepatients.Matchingtreatmentsettings,interventions,andservicestoanindividual’sparticularproblemsandneedsiscriticaltohisorherultimatesuccessinreturningtoproductivefunctioninginthefamily,workplace,andsociety.
3. Treatmentneedstobereadilyavailable.Becausedrug-addictedindividualsmaybeuncertainaboutenteringtreatment,takingadvantageofavailableservicesthemomentpeoplearereadyfortreatmentiscritical.Potentialpatientscanbelostiftreatmentisnotimmediatelyavailableorreadilyaccessible.Aswithotherchronicdiseases,theearliertreatmentisofferedinthediseaseprocess,thegreaterthelikelihoodofpositiveoutcomes.
4. Effectivetreatmentattendstomultipleneedsoftheindividual,notjusthisorherdrugabuse.Tobeeffective,treatmentmustaddresstheindividual’sdrugabuseandanyassociatedmedical,psychological,social,vocational,andlegalproblems.Itisalsoimportantthattreatmentbeappropriatetotheindividual’sage,gender,ethnicity,andculture.
5. Remainingintreatmentforanadequateperiodoftimeiscritical.Theappropriatedurationforanindividualdependsonthetypeanddegreeofthepatient’sproblemsandneeds.Researchindicatesthatmostaddictedindividualsneedatleast3monthsintreatmenttosignificantlyreduceorstoptheirdruguseandthatthebestoutcomesoccurwithlongerdurationsoftreatment.Recoveryfromdrugaddictionisalong-termprocessandfrequentlyrequiresmultipleepisodesoftreatment.Aswithotherchronicillnesses,relapsestodrugabusecanoccurandshouldsignalaneedfortreatmenttobereinstatedoradjusted.Becauseindividualsoftenleavetreatmentprematurely,programsshouldincludestrategiestoengageand

6
keeppatientsintreatment.
6. Behavioraltherapies—includingindividual,family,orgroupcounseling—arethemostcommonlyusedformsofdrugabusetreatment.Behavioraltherapiesvaryintheirfocusandmayinvolveaddressingapatient’smotivationtochange,providingincentivesforabstinence,buildingskillstoresistdruguse,replacingdrug-usingactivitieswithconstructiveandrewardingactivities,improvingproblem-solvingskills,andfacilitatingbetterinterpersonalrelationships.Also,participationingrouptherapyandotherpeersupportprogramsduringandfollowingtreatmentcanhelpmaintainabstinence.
7. Medicationsareanimportantelementoftreatmentformanypatients,especiallywhencombinedwithcounselingandotherbehavioraltherapies.Forexample,methadone,buprenorphine,andnaltrexone(includinganewlong-actingformulation)areeffectiveinhelpingindividualsaddictedtoheroinorotheropioidsstabilizetheirlivesandreducetheirillicitdruguse.Acamprosate,disulfiram,andnaltrexonearemedicationsapprovedfortreatingalcoholdependence.Forpersonsaddictedtonicotine,anicotinereplacementproduct(availableaspatches,gum,lozenges,ornasalspray)oranoralmedication(suchasbupropionorvarenicline)canbeaneffectivecomponentoftreatmentwhenpartofacomprehensivebehavioraltreatmentprogram.
8. Anindividual'streatmentandservicesplanmustbeassessedcontinuallyandmodifiedasnecessarytoensurethatitmeetshisorherchangingneeds.Apatientmayrequirevaryingcombinationsofservicesandtreatmentcomponentsduringthecourseoftreatmentandrecovery.Inadditiontocounselingorpsychotherapy,apatientmayrequiremedication,medicalservices,familytherapy,parentinginstruction,vocationalrehabilitation,and/orsocialandlegalservices.Formanypatients,acontinuingcareapproachprovidesthebestresults,withthetreatmentintensityvaryingaccordingtoaperson’schangingneeds.
9. Manydrug-addictedindividualsalsohaveothermentaldisorders.Becausedrugabuseandaddiction—bothofwhicharementaldisorders—oftenco-occurwithothermentalillnesses,patientspresentingwithoneconditionshouldbeassessedfortheother(s).Andwhentheseproblemsco-occur,treatmentshouldaddressboth(orall),includingtheuseofmedicationsasappropriate.
7
10. Medicallyassisteddetoxificationisonlythefirststageofaddictiontreatmentandbyitselfdoeslittletochangelong-termdrugabuse.Althoughmedicallyassisteddetoxificationcansafelymanagetheacutephysicalsymptomsofwithdrawalandcan,forsome,pavethewayforeffectivelong-termaddictiontreatment,detoxificationaloneisrarelysufficienttohelpaddictedindividualsachievelong-termabstinence.Thus,patientsshouldbeencouragedtocontinuedrugtreatmentfollowingdetoxification.Motivationalenhancementandincentivestrategies,begunatinitialpatientintake,canimprovetreatmentengagement.
11. Treatmentdoesnotneedtobevoluntarytobeeffective.Sanctionsorenticementsfromfamily,employmentsettings,and/orthecriminaljusticesystemcansignificantlyincreasetreatmententry,retentionrates,andtheultimatesuccessofdrugtreatmentinterventions.
12. Druguseduringtreatmentmustbemonitoredcontinuously,aslapsesduringtreatmentdooccur.Knowingtheirdruguseisbeingmonitoredcanbeapowerfulincentiveforpatientsandcanhelpthemwithstandurgestousedrugs.Monitoringalsoprovidesanearlyindicationofareturntodruguse,signalingapossibleneedtoadjustanindividual’streatmentplantobettermeethisorherneeds.
13. TreatmentprogramsshouldtestpatientsforthepresenceofHIV/AIDS,hepatitisBandC,tuberculosis,andotherinfectiousdiseasesaswellasprovidetargetedrisk-reductioncounseling,linkingpatientstotreatmentifnecessary.Typically,drugabusetreatmentaddressessomeofthedrug-relatedbehaviorsthatputpeopleatriskofinfectiousdiseases.Targetedcounselingfocusedonreducinginfectiousdiseaseriskcanhelppatientsfurtherreduceoravoidsubstance-relatedandotherhigh-riskbehaviors.Counselingcanalsohelpthosewhoarealreadyinfectedtomanagetheirillness.Moreover,engaginginsubstanceabusetreatmentcanfacilitateadherencetoothermedicaltreatments.Substanceabusetreatmentfacilitiesshouldprovideonsite,rapidHIVtestingratherthanreferralstooffsitetesting—researchshowsthatdoingsoincreasesthelikelihoodthatpatientswillbetestedandreceivetheirtestresults.Treatmentprovidersshouldalsoinformpatientsthathighlyactiveantiretroviraltherapy(HAART)hasproveneffectiveincombatingHIV,includingamongdrug-abusingpopulations,andhelplinkthemtoHIVtreatmentiftheytestpositive.

8
FrequentlyAskedQuestions
Treatmentvariesdependingonthetypeofdrugandthecharacteristicsofthepatient.Thebestprogramsprovideacombinationoftherapiesandotherservices.
Whydodrug-addictedpersonskeepusingdrugs?
Nearlyalladdictedindividualsbelieveattheoutsetthattheycanstopusingdrugsontheirown,andmosttrytostopwithouttreatment.Althoughsomepeoplearesuccessful,manyattemptsresultinfailuretoachievelong-termabstinence.Researchhasshownthatlong-termdrugabuseresultsinchangesinthebrainthatpersistlongafterapersonstopsusingdrugs.Thesedrug-inducedchangesinbrainfunctioncanhavemanybehavioralconsequences,includinganinabilitytoexertcontrolovertheimpulsetousedrugsdespiteadverseconsequences—thedefiningcharacteristicofaddiction.
Long-termdruguseresultsinsignificantchangesinbrainfunctionthatcanpersistlongaftertheindividualstopsusingdrugs.
Understandingthataddictionhassuchafundamentalbiologicalcomponentmayhelpexplainthedifficultyofachievingandmaintainingabstinencewithouttreatment.Psychologicalstressfromwork,familyproblems,psychiatricillness,painassociatedwithmedicalproblems,socialcues(suchasmeetingindividualsfromone’sdrug-usingpast),orenvironmentalcues(suchasencounteringstreets,objects,orevensmellsassociatedwithdrugabuse)cantriggerintensecravingswithouttheindividualevenbeingconsciouslyawareofthetriggeringevent.Anyoneofthesefactorscanhinderattainmentofsustainedabstinenceandmakerelapsemorelikely.Nevertheless,researchindicatesthatactiveparticipationintreatmentisanessentialcomponentforgoodoutcomes
9
andcanbenefiteventhemostseverelyaddictedindividuals.
Whatisdrugaddictiontreatment?
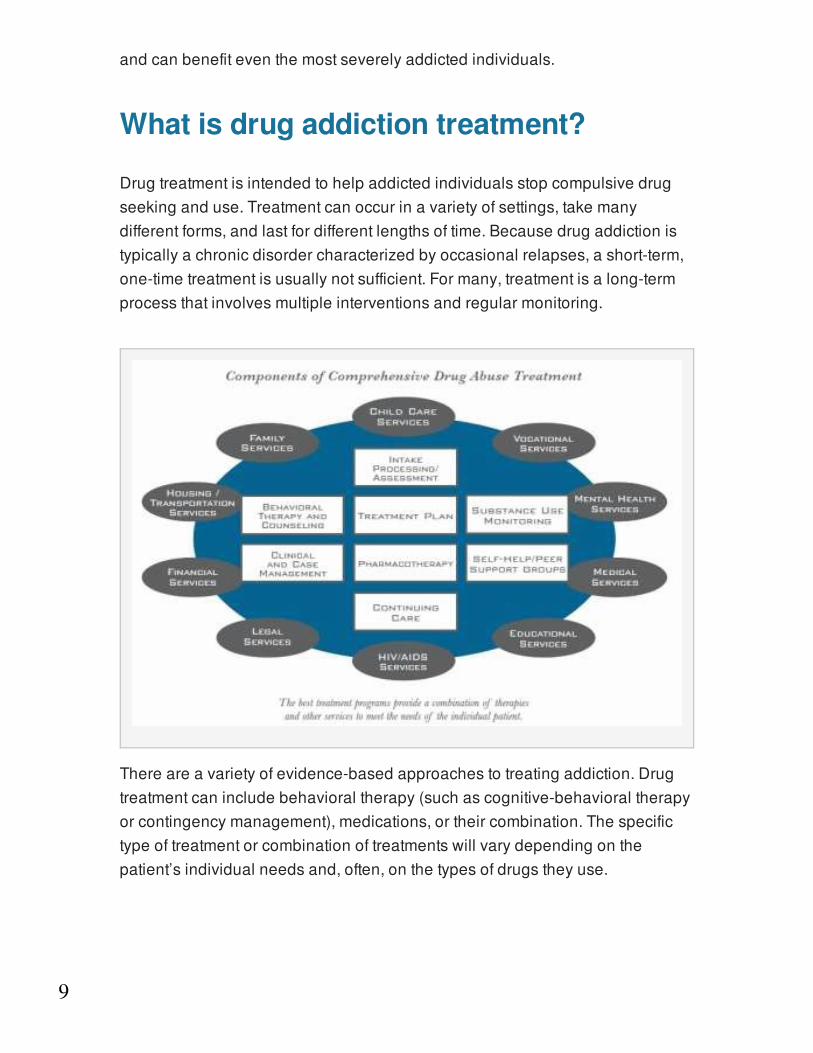
Drugtreatmentisintendedtohelpaddictedindividualsstopcompulsivedrugseekinganduse.Treatmentcanoccurinavarietyofsettings,takemanydifferentforms,andlastfordifferentlengthsoftime.Becausedrugaddictionistypicallyachronicdisordercharacterizedbyoccasionalrelapses,ashort-term,one-timetreatmentisusuallynotsufficient.Formany,treatmentisalong-termprocessthatinvolvesmultipleinterventionsandregularmonitoring.
Thereareavarietyofevidence-basedapproachestotreatingaddiction.Drugtreatmentcanincludebehavioraltherapy(suchascognitive-behavioraltherapyorcontingencymanagement),medications,ortheircombination.Thespecifictypeoftreatmentorcombinationoftreatmentswillvarydependingonthepatient’sindividualneedsand,often,onthetypesofdrugstheyuse.

10
Drugaddictiontreatmentcanincludemedications,behavioraltherapies,ortheircombination.
Treatmentmedications,suchasmethadone,buprenorphine,andnaltrexone(includinganewlong-actingformulation),areavailableforindividualsaddictedtoopioids,whilenicotinepreparations(patches,gum,lozenges,andnasalspray)andthemedicationsvareniclineandbupropionareavailableforindividualsaddictedtotobacco.Disulfiram,acamprosate,andnaltrexonearemedicationsavailablefortreatingalcoholdependence, whichcommonlyco-occurswithotherdrugaddictions,includingaddictiontoprescriptionmedications.
Treatmentsforprescriptiondrugabusetendtobesimilartothoseforillicitdrugsthataffectthesamebrainsystems.Forexample,buprenorphine,usedtotreatheroinaddiction,canalsobeusedtotreataddictiontoopioidpainmedications.Addictiontoprescriptionstimulants,whichaffectthesamebrainsystemsasillicitstimulantslikecocaine,canbetreatedwithbehavioraltherapies,astherearenotyetmedicationsfortreatingaddictiontothesetypesofdrugs.
Behavioraltherapiescanhelpmotivatepeopletoparticipateindrugtreatment,offerstrategiesforcopingwithdrugcravings,teachwaystoavoiddrugsandpreventrelapse,andhelpindividualsdealwithrelapseifitoccurs.Behavioraltherapiescanalsohelppeopleimprovecommunication,relationship,andparentingskills,aswellasfamilydynamics.
Manytreatmentprogramsemploybothindividualandgrouptherapies.Grouptherapycanprovidesocialreinforcementandhelpenforcebehavioralcontingenciesthatpromoteabstinenceandanon-drug-usinglifestyle.Someofthemoreestablishedbehavioraltreatments,suchascontingencymanagementandcognitive-behavioraltherapy,arealsobeingadaptedforgroupsettingstoimproveefficiencyandcost-effectiveness.However,particularlyinadolescents,therecanalsobeadangerofunintendedharmful(oriatrogenic)effectsofgrouptreatment—sometimesgroupmembers(especiallygroupsofhighlydelinquentyouth)canreinforcedruguseandtherebyderailthepurposeofthetherapy.Thus,trainedcounselorsshouldbeawareofandmonitorforsuch
1
11
effects.
Becausetheyworkondifferentaspectsofaddiction,combinationsofbehavioraltherapiesandmedications(whenavailable)generallyappeartobemoreeffectivethaneitherapproachusedalone.
Finally,peoplewhoareaddictedtodrugsoftensufferfromotherhealth(e.g.,depression,HIV),occupational,legal,familial,andsocialproblemsthatshouldbeaddressedconcurrently.Thebestprogramsprovideacombinationoftherapiesandotherservicestomeetanindividualpatient’sneeds.Psychoactivemedications,suchasantidepressants,anti-anxietyagents,moodstabilizers,andantipsychoticmedications,maybecriticalfortreatmentsuccesswhenpatientshaveco-occurringmentaldisorderssuchasdepression,anxietydisorders(includingpost-traumaticstressdisorder),bipolardisorder,orschizophrenia.Inaddition,mostpeoplewithsevereaddictionabusemultipledrugsandrequiretreatmentforallsubstancesabused.
Treatmentfordrugabuseandaddictionisdeliveredinmanydifferentsettingsusingavarietyofbehavioralandpharmacologicalapproaches.
Anotherdrug,topiramate,hasalsoshownpromiseinstudiesandissometimesprescribed(off-label)forthispurposealthoughithasnotreceivedFDAapprovalasatreatmentforalcoholdependence.
Howeffectiveisdrugaddictiontreatment?
Inadditiontostoppingdrugabuse,thegoaloftreatmentistoreturnpeopletoproductivefunctioninginthefamily,workplace,andcommunity.Accordingtoresearchthattracksindividualsintreatmentoverextendedperiods,mostpeoplewhogetintoandremainintreatmentstopusingdrugs,decreasetheircriminalactivity,andimprovetheiroccupational,social,andpsychologicalfunctioning.Forexample,methadonetreatmenthasbeenshowntoincrease
1

12
participationinbehavioraltherapyanddecreasebothdruguseandcriminalbehavior.However,individualtreatmentoutcomesdependontheextentandnatureofthepatient’sproblems,theappropriatenessoftreatmentandrelatedservicesusedtoaddressthoseproblems,andthequalityofinteractionbetweenthepatientandhisorhertreatmentproviders.
Relapseratesforaddictionresemblethoseofotherchronicdiseasessuchasdiabetes,hypertension,andasthma.
Likeotherchronicdiseases,addictioncanbemanagedsuccessfully.Treatmentenablespeopletocounteractaddiction’spowerfuldisruptiveeffectsonthebrainandbehaviorandtoregaincontroloftheirlives.Thechronicnatureofthediseasemeansthatrelapsingtodrugabuseisnotonlypossiblebutalsolikely,withsymptomrecurrenceratessimilartothoseforotherwell-characterizedchronicmedicalillnesses—suchasdiabetes,hypertension,andasthma(seefigure,"ComparisonofRelapseRatesBetweenDrugAddictionandOtherChronicIllnesses”)—thatalsohavebothphysiologicalandbehavioralcomponents.

13
Unfortunately,whenrelapseoccursmanydeemtreatmentafailure.Thisisnotthecase:Successfultreatmentforaddictiontypicallyrequirescontinualevaluationandmodificationasappropriate,similartotheapproachtakenforotherchronicdiseases.Forexample,whenapatientisreceivingactivetreatmentforhypertensionandsymptomsdecrease,treatmentisdeemedsuccessful,eventhoughsymptomsmayrecurwhentreatmentisdiscontinued.Fortheaddictedindividual,lapsestodrugabusedonotindicatefailure—rather,theysignifythattreatmentneedstobereinstatedoradjusted,orthatalternatetreatmentisneeded(seefigure,"WhyisAddictionTreatmentEvaluatedDifferently?").
Isdrugaddictiontreatmentworthitscost?
SubstanceabusecostsourNationover$600billionannuallyandtreatmentcanhelpreducethesecosts.Drugaddictiontreatmenthasbeenshowntoreduceassociatedhealthandsocialcostsbyfarmorethanthecostofthetreatmentitself.Treatmentisalsomuchlessexpensivethanitsalternatives,suchasincarceratingaddictedpersons.Forexample,theaveragecostfor1fullyearofmethadonemaintenancetreatmentisapproximately$4,700perpatient,whereas1fullyearofimprisonmentcostsapproximately$24,000perperson.

14
Drugaddictiontreatmentreducesdruguseanditsassociatedhealthandsocialcosts.
Accordingtoseveralconservativeestimates,everydollarinvestedinaddictiontreatmentprogramsyieldsareturnofbetween$4and$7inreduceddrug-relatedcrime,criminaljusticecosts,andtheft.Whensavingsrelatedtohealthcareareincluded,totalsavingscanexceedcostsbyaratioof12to1.Majorsavingstotheindividualandtosocietyalsostemfromfewerinterpersonalconflicts;greaterworkplaceproductivity;andfewerdrug-relatedaccidents,includingoverdosesanddeaths.
Howlongdoesdrugaddictiontreatmentusuallylast?
Individualsprogressthroughdrugaddictiontreatmentatvariousrates,sothereisnopredeterminedlengthoftreatment.However,researchhasshownunequivocallythatgoodoutcomesarecontingentonadequatetreatmentlength.Generally,forresidentialoroutpatienttreatment,participationforlessthan90daysisoflimitedeffectiveness,andtreatmentlastingsignificantlylongerisrecommendedformaintainingpositiveoutcomes.Formethadonemaintenance,12monthsisconsideredtheminimum,andsomeopioid-addictedindividualscontinuetobenefitfrommethadonemaintenanceformanyyears.
Goodoutcomesarecontingentonadequatetreatmentlength.
Treatmentdropoutisoneofthemajorproblemsencounteredbytreatmentprograms;therefore,motivationaltechniquesthatcankeeppatientsengagedwillalsoimproveoutcomes.Byviewingaddictionasachronicdiseaseandofferingcontinuingcareandmonitoring,programscansucceed,butthiswilloftenrequiremultipleepisodesoftreatmentandreadilyreadmittingpatientsthathaverelapsed.
15
Whathelpspeoplestayintreatment?
Becausesuccessfuloutcomesoftendependonaperson’sstayingintreatmentlongenoughtoreapitsfullbenefits,strategiesforkeepingpeopleintreatmentarecritical.Whetherapatientstaysintreatmentdependsonfactorsassociatedwithboththeindividualandtheprogram.Individualfactorsrelatedtoengagementandretentiontypicallyincludemotivationtochangedrug-usingbehavior;degreeofsupportfromfamilyandfriends;and,frequently,pressurefromthecriminaljusticesystem,childprotectionservices,employers,orfamily.Withinatreatmentprogram,successfulclinicianscanestablishapositive,therapeuticrelationshipwiththeirpatients.Theclinicianshouldensurethatatreatmentplanisdevelopedcooperativelywiththepersonseekingtreatment,thattheplanisfollowed,andthattreatmentexpectationsareclearlyunderstood.Medical,psychiatric,andsocialservicesshouldalsobeavailable.
Whetherapatientstaysintreatmentdependsonfactorsassociatedwithboththeindividualandtheprogram.
Becausesomeproblems(suchasseriousmedicalormentalillnessorcriminalinvolvement)increasethelikelihoodofpatientsdroppingoutoftreatment,intensiveinterventionsmayberequiredtoretainthem.Afteracourseofintensivetreatment,theprovidershouldensureatransitiontolessintensivecontinuingcaretosupportandmonitorindividualsintheirongoingrecovery.
Howdowegetmoresubstance-abusingpeopleintotreatment?
Ithasbeenknownformanyyearsthatthe"treatmentgap”ismassive—thatis,amongthosewhoneedtreatmentforasubstanceusedisorder,fewreceiveit.In2011,21.6millionpersonsaged12orolderneededtreatmentforanillicitdrugoralcoholuseproblem,butonly2.3millionreceivedtreatmentataspecialtysubstanceabusefacility.

16
Reducingthisgaprequiresamultiprongedapproach.Strategiesincludeincreasingaccesstoeffectivetreatment,achievinginsuranceparity(nowinitsearliestphaseofimplementation),reducingstigma,andraisingawarenessamongbothpatientsandhealthcareprofessionalsofthevalueofaddictiontreatment.Toassistphysiciansinidentifyingtreatmentneedintheirpatientsandmakingappropriatereferrals,NIDAisencouragingwidespreaduseofscreening,briefintervention,andreferraltotreatment(SBIRT)toolsforuseinprimarycaresettingsthroughitsNIDAMEDinitiative.SBIRT,whichevidenceshowstobeeffectiveagainsttobaccoandalcoholuse—and,increasingly,againstabuseofillicitandprescriptiondrugs—hasthepotentialnotonlytocatchpeoplebeforeseriousdrugproblemsdevelop,butalsotoidentifypeopleinneedoftreatmentandconnectthemwithappropriatetreatmentproviders.
Howcanfamilyandfriendsmakeadifferenceinthelifeofsomeoneneedingtreatment?
Familyandfriendscanplaycriticalrolesinmotivatingindividualswithdrugproblemstoenterandstayintreatment.Familytherapycanalsobeimportant,especiallyforadolescents.Involvementofafamilymemberorsignificantotherinanindividual'streatmentprogramcanstrengthenandextendtreatmentbenefits.
Wherecanfamilymembersgoforinformationontreatmentoptions?
Tryingtolocateappropriatetreatmentforalovedone,especiallyfindingaprogramtailoredtoanindividual'sparticularneeds,canbeadifficultprocess.However,therearesomeresourcestohelpwiththisprocess.Forexample,NIDA’shandbookSeekingDrugAbuseTreatment:KnowWhattoAskoffersguidanceinfindingtherighttreatmentprogram.Numerousonlineresourcescanhelplocatealocalprogramorprovideotherinformation,including:

17
TheSubstanceAbuseandMentalHealthServicesAdministration(SAMHSA)maintainsaWebsite(www.findtreatment.samhsa.gov)thatshowsthelocationofresidential,outpatient,andhospitalinpatienttreatmentprogramsfordrugaddictionandalcoholismthroughoutthecountry.Thisinformationisalsoaccessiblebycalling1-800-662-HELP.
TheNationalSuicidePreventionLifeline(1-800-273-TALK)offersmorethanjustsuicideprevention—itcanalsohelpwithahostofissues,includingdrugandalcoholabuse,andcanconnectindividualswithanearbyprofessional.
TheNationalAllianceonMentalIllness(www.nami.org)andMentalHealthAmerica(www.mentalhealthamerica.net)arealliancesofnonprofit,self-helpsupportorganizationsforpatientsandfamiliesdealingwithavarietyofmentaldisorders.BothhaveStateandlocalaffiliatesthroughoutthecountryandmaybeespeciallyhelpfulforpatientswithcomorbidconditions.
TheAmericanAcademyofAddictionPsychiatryandtheAmericanAcademyofChildandAdolescentPsychiatryeachhavephysicianlocatortoolspostedontheirWebsitesataaap.organdaacap.org,respectively.
Faces&VoicesofRecovery(facesandvoicesofrecovery.org),foundedin2001,isanadvocacyorganizationforindividualsinlong-termrecoverythatstrategizesonwaystoreachouttothemedical,publichealth,criminaljustice,andothercommunitiestopromoteandcelebraterecoveryfromaddictiontoalcoholandotherdrugs.
ThePartnershipatDrugfree.org(drugfree.org)isanorganizationthatprovidesinformationandresourcesonteendruguseandaddictionforparents,tohelpthempreventandinterveneintheirchildren’sdruguseorfindtreatmentforachildwhoneedsit.Theyofferatoll-freehelplineforparents(1-855-378-4373).
TheAmericanSocietyofAddictionMedicine(asam.org)isasocietyofphysiciansaimedatincreasingaccesstoaddictiontreatment.TheirWebsitehasanationwidedirectoryofaddictionmedicineprofessionals.
NIDA’sNationalDrugAbuseTreatmentClinicalTrialsNetwork(drugabuse.gov/about-nida/organization/cctn/ctn)providesinformationforthoseinterestedinparticipatinginaclinicaltrialtestingapromisingsubstanceabuseintervention;orvisitclinicaltrials.gov.
NIDA’sDrugPubsResearchDisseminationCenter

18
(drugpubs.drugabuse.gov)providesbooklets,pamphlets,factsheets,andotherinformationalresourcesondrugs,drugabuse,andtreatment.
TheNationalInstituteonAlcoholAbuseandAlcoholism(niaaa.nih.gov)providesinformationonalcohol,alcoholuse,andtreatmentofalcohol-relatedproblems(niaaa.nih.gov/search/node/treatment).
Howcantheworkplaceplayaroleinsubstanceabusetreatment?
ManyworkplacessponsorEmployeeAssistancePrograms(EAPs)thatoffershort-termcounselingand/orassistanceinlinkingemployeeswithdrugoralcoholproblemstolocaltreatmentresources,includingpeersupport/recoverygroups.Inaddition,therapeuticworkenvironmentsthatprovideemploymentfordrug-abusingindividualswhocandemonstrateabstinencehavebeenshownnotonlytopromoteacontinueddrug-freelifestylebutalsotoimprovejobskills,punctuality,andotherbehaviorsnecessaryforactiveemploymentthroughoutlife.Urinetestingfacilities,trainedpersonnel,andworkplacemonitorsareneededtoimplementthistypeoftreatment.
Whatrolecanthecriminaljusticesystemplayinaddressingdrugaddiction?
Itisestimatedthataboutone-halfofStateandFederalprisonersabuseorareaddictedtodrugs,butrelativelyfewreceivetreatmentwhileincarcerated.Initiatingdrugabusetreatmentinprisonandcontinuingituponreleaseisvitaltobothindividualrecoveryandtopublichealthandsafety.Variousstudieshaveshownthatcombiningprison-andcommunity-basedtreatmentforaddictedoffendersreducestheriskofbothrecidivismtodrug-relatedcriminalbehaviorandrelapsetodruguse—which,inturn,netshugesavingsinsocietalcosts.A2009studyinBaltimore,Maryland,forexample,foundthatopioid-addictedprisonerswhostartedmethadonetreatment(alongwithcounseling)inprisonandthencontinueditafterreleasehadbetteroutcomes(reduceddruguseandcriminalactivity)thanthosewhoonlyreceivedcounselingwhileinprisonorthosewhoonlystartedmethadonetreatmentaftertheirrelease.

19
Individualswhoentertreatmentunderlegalpressurehaveoutcomesasfavorableasthosewhoentertreatmentvoluntarily.
Themajorityofoffendersinvolvedwiththecriminaljusticesystemarenotinprisonbutareundercommunitysupervision.Forthosewithknowndrugproblems,drugaddictiontreatmentmayberecommendedormandatedasaconditionofprobation.Researchhasdemonstratedthatindividualswhoentertreatmentunderlegalpressurehaveoutcomesasfavorableasthosewhoentertreatmentvoluntarily.
Thecriminaljusticesystemrefersdrugoffendersintotreatmentthroughavarietyofmechanisms,suchasdivertingnonviolentoffenderstotreatment;stipulatingtreatmentasaconditionofincarceration,probation,orpretrialrelease;andconveningspecializedcourts,ordrugcourts,thathandledrugoffensecases.Thesecourtsmandateandarrangefortreatmentasanalternativetoincarceration,activelymonitorprogressintreatment,andarrangeforotherservicesfordrug-involvedoffenders.
Themosteffectivemodelsintegratecriminaljusticeanddrugtreatmentsystemsandservices.Treatmentandcriminaljusticepersonnelworktogetherontreatmentplanning—includingimplementationofscreening,placement,testing,monitoring,andsupervision—aswellasonthesystematicuseofsanctionsandrewards.Treatmentforincarcerateddrugabusersshouldincludecontinuingcare,monitoring,andsupervisionafterincarcerationandduringparole.Methodstoachievebettercoordinationbetweenparole/probationofficersandhealthprovidersarebeingstudiedtoimproveoffenderoutcomes.(Formoreinformation,pleaseseeNIDA’sPrinciplesofDrugAbuseTreatmentforCriminalJusticePopulations:AResearch-BasedGuide[revised2012].)
Whataretheuniqueneedsofwomenwithsubstanceusedisorders?
Gender-relateddrugabusetreatmentshouldattendnotonlytobiological
20
differencesbutalsotosocialandenvironmentalfactors,allofwhichcaninfluencethemotivationsfordruguse,thereasonsforseekingtreatment,thetypesofenvironmentswheretreatmentisobtained,thetreatmentsthataremosteffective,andtheconsequencesofnotreceivingtreatment.Manylifecircumstancespredominateinwomenasagroup,whichmayrequireaspecializedtreatmentapproach.Forexample,researchhasshownthatphysicalandsexualtraumafollowedbypost-traumaticstressdisorder(PTSD)ismorecommonindrug-abusingwomenthaninmenseekingtreatment.Otherfactorsuniquetowomenthatcaninfluencethetreatmentprocessincludeissuesaroundhowtheycomeintotreatment(aswomenaremorelikelythanmentoseektheassistanceofageneralormentalhealthpractitioner),financialindependence,andpregnancyandchildcare.
Whataretheuniqueneedsofpregnantwomenwithsubstanceusedisorders?
Usingdrugs,alcohol,ortobaccoduringpregnancyexposesnotjustthewomanbutalsoherdevelopingfetustothesubstanceandcanhavepotentiallydeleteriousandevenlong-termeffectsonexposedchildren.Smokingduringpregnancycanincreaseriskofstillbirth,infantmortality,suddeninfantdeathsyndrome,pretermbirth,respiratoryproblems,slowedfetalgrowth,andlowbirthweight.Drinkingduringpregnancycanleadtothechilddevelopingfetalalcoholspectrumdisorders,characterizedbylowbirthweightandenduringcognitiveandbehavioralproblems.
Prenataluseofsomedrugs,includingopioids,maycauseawithdrawalsyndromeinnewbornscalledneonatalabstinencesyndrome(NAS).BabieswithNASareatgreaterriskofseizures,respiratoryproblems,feedingdifficulties,lowbirthweight,andevendeath.
Researchhasestablishedthevalueofevidence-basedtreatmentsforpregnantwomen(andtheirbabies),includingmedications.Forexample,althoughnomedicationshavebeenFDA-approvedtotreatopioiddependenceinpregnantwomen,methadonemaintenancecombinedwithprenatalcareandacomprehensivedrugtreatmentprogramcanimprovemanyofthedetrimental

21
outcomesassociatedwithuntreatedheroinabuse.However,newbornsexposedtomethadoneduringpregnancystillrequiretreatmentforwithdrawalsymptoms.Recently,anothermedicationoptionforopioiddependence,buprenorphine,hasbeenshowntoproducefewerNASsymptomsinbabiesthanmethadone,resultinginshorterinfanthospitalstays.Ingeneral,itisimportanttocloselymonitorwomenwhoaretryingtoquitdruguseduringpregnancyandtoprovidetreatmentasneeded.
Whataretheuniqueneedsofadolescentswithsubstanceusedisorders?
Adolescentdrugabusershaveuniqueneedsstemmingfromtheirimmatureneurocognitiveandpsychosocialstageofdevelopment.Researchhasdemonstratedthatthebrainundergoesaprolongedprocessofdevelopmentandrefinementfrombirththroughearlyadulthood.Overthecourseofthisdevelopmentalperiod,ayoungperson’sactionsgofrombeingmoreimpulsivetobeingmorereasonedandreflective.Infact,thebrainareasmostcloselyassociatedwithaspectsofbehaviorsuchasdecision-making,judgment,planning,andself-controlundergoaperiodofrapiddevelopmentduringadolescenceandyoungadulthood.
Adolescentdrugabuseisalsooftenassociatedwithotherco-occurringmentalhealthproblems.Theseincludeattention-deficithyperactivitydisorder(ADHD),oppositionaldefiantdisorder,andconductproblems,aswellasdepressiveandanxietydisorders.
Adolescentsarealsoespeciallysensitivetosocialcues,withpeergroupsandfamiliesbeinghighlyinfluentialduringthistime.Therefore,treatmentsthatfacilitatepositiveparentalinvolvement,integrateothersystemsinwhichtheadolescentparticipates(suchasschoolandathletics),andrecognizetheimportanceofprosocialpeerrelationshipsareamongthemosteffective.Accesstocomprehensiveassessment,treatment,casemanagement,andfamily-supportservicesthataredevelopmentally,culturally,andgender-appropriateisalsointegralwhenaddressingadolescentaddiction.

22
Medicationsforsubstanceabuseamongadolescentsmayincertaincasesbehelpful.Currently,theonlyaddictionmedicationsapprovedbyFDAforpeopleunder18areover-the-countertransdermalnicotineskinpatches,chewinggum,andlozenges(physicianadviceshouldbesoughtfirst).Buprenorphine,amedicationfortreatingopioidaddictionthatmustbeprescribedbyspeciallytrainedphysicians,hasnotbeenapprovedforadolescents,butrecentresearchsuggestsitcouldbeeffectiveforthoseasyoungas16.Studiesareunderwaytodeterminethesafetyandefficacyofthisandothermedicationsforopioid-,nicotine-,andalcohol-dependentadolescentsandforadolescentswithco-occurringdisorders.
Aretherespecificdrugaddictiontreatmentsforolderadults?
Withtheagingofthebabyboomergeneration,thecompositionofthegeneralpopulationischangingdramaticallywithrespecttothenumberofolderadults.Suchachange,coupledwithagreaterhistoryoflifetimedruguse(thanpreviousoldergenerations),differentculturalnormsandgeneralattitudesaboutdruguse,andincreasesintheavailabilityofpsychotherapeuticmedications,isalreadyleadingtogreaterdrugusebyolderadultsandmayincreasesubstanceuseproblemsinthispopulation.Whilesubstanceabuseinolderadultsoftengoesunrecognizedandthereforeuntreated,researchindicatesthatcurrentlyavailableaddictiontreatmentprogramscanbeaseffectiveforthemasforyoungeradults.
Canapersonbecomeaddictedtomedicationsprescribedbyadoctor?
Yes.Peoplewhoabuseprescriptiondrugs—thatis,takingtheminamanneroradoseotherthanprescribed,ortakingmedicationsprescribedforanotherperson—riskaddictionandotherserioushealthconsequences.Suchdrugsincludeopioidpainrelievers,stimulantsusedtotreatADHD,andbenzodiazepinestotreatanxietyorsleepdisorders.Indeed,in2010,anestimated2.4millionpeople12oroldermetcriteriaforabuseofordependence

23
onprescriptiondrugs,thesecondmostcommonillicitdruguseaftermarijuana.Tominimizetheserisks,aphysician(orotherprescribinghealthprovider)shouldscreenpatientsforpriororcurrentsubstanceabuseproblemsandassesstheirfamilyhistoryofsubstanceabuseoraddictionbeforeprescribingapsychoactivemedicationandmonitorpatientswhoareprescribedsuchdrugs.Physiciansalsoneedtoeducatepatientsaboutthepotentialriskssothattheywillfollowtheirphysician’sinstructionsfaithfully,safeguardtheirmedications,anddisposeofthemappropriately.
Isthereadifferencebetweenphysicaldependenceandaddiction?
Yes.Addiction—orcompulsivedrugusedespiteharmfulconsequences—ischaracterizedbyaninabilitytostopusingadrug;failuretomeetwork,social,orfamilyobligations;and,sometimes(dependingonthedrug),toleranceandwithdrawal.Thelatterreflectphysicaldependenceinwhichthebodyadaptstothedrug,requiringmoreofittoachieveacertaineffect(tolerance)andelicitingdrug-specificphysicalormentalsymptomsifdruguseisabruptlyceased(withdrawal).Physicaldependencecanhappenwiththechronicuseofmanydrugs—includingmanyprescriptiondrugs,eveniftakenasinstructed.Thus,physicaldependenceinandofitselfdoesnotconstituteaddiction,butitoftenaccompaniesaddiction.Thisdistinctioncanbedifficulttodiscern,particularlywithprescribedpainmedications,forwhichtheneedforincreasingdosagescanrepresenttoleranceoraworseningunderlyingproblem,asopposedtothebeginningofabuseoraddiction.
Howdoothermentaldisorderscoexistingwithdrugaddictionaffectdrugaddictiontreatment?
Drugaddictionisadiseaseofthebrainthatfrequentlyoccurswithothermentaldisorders.Infact,asmanyas6in10peoplewithanillicitsubstanceusedisorderalsosufferfromanothermentalillness;andratesaresimilarforusersoflicitdrugs—i.e.,tobaccoandalcohol.Fortheseindividuals,onecondition

24
becomesmoredifficulttotreatsuccessfullyasanadditionalconditionisintertwined.Thus,peopleenteringtreatmenteitherforasubstanceusedisorderorforanothermentaldisordershouldbeassessedfortheco-occurrenceoftheothercondition.Researchindicatesthattreatingboth(ormultiple)illnessessimultaneouslyinanintegratedfashionisgenerallythebesttreatmentapproachforthesepatients.
Istheuseofmedicationslikemethadoneandbuprenorphinesimplyreplacingoneaddictionwithanother?
No.Buprenorphineandmethadoneareprescribedoradministeredundermonitored,controlledconditionsandaresafeandeffectivefortreatingopioidaddictionwhenusedasdirected.Theyareadministeredorallyorsublingually(i.e.,underthetongue)inspecifieddoses,andtheireffectsdifferfromthoseofheroinandotherabusedopioids.
Heroin,forexample,isofteninjected,snorted,orsmoked,causinganalmostimmediate"rush,"orbriefperiodofintenseeuphoria,thatwearsoffquicklyandendsina"crash."Theindividualthenexperiencesanintensecravingtousethedrugagaintostopthecrashandreinstatetheeuphoria.
Thecycleofeuphoria,crash,andcraving—sometimesrepeatedseveraltimesaday—isahallmarkofaddictionandresultsinseverebehavioraldisruption.Thesecharacteristicsresultfromheroin’srapidonsetandshortdurationofactioninthebrain.
Asusedinmaintenancetreatment,methadoneandbuprenorphinearenotheroin/opioidsubstitutes.
Incontrast,methadoneandbuprenorphinehavegradualonsetsofactionandproducestablelevelsofthedruginthebrain.Asaresult,patientsmaintained

25
onthesemedicationsdonotexperiencearush,whiletheyalsomarkedlyreducetheirdesiretouseopioids.
Ifanindividualtreatedwiththesemedicationstriestotakeanopioidsuchasheroin,theeuphoriceffectsareusuallydampenedorsuppressed.Patientsundergoingmaintenancetreatmentdonotexperiencethephysiologicalorbehavioralabnormalitiesfromrapidfluctuationsindruglevelsassociatedwithheroinuse.Maintenancetreatmentssavelives—theyhelptostabilizeindividuals,allowingtreatmentoftheirmedical,psychological,andotherproblemssotheycancontributeeffectivelyasmembersoffamiliesandofsociety.
Wheredo12-steporself-helpprogramsfitintodrugaddictiontreatment?
Self-helpgroupscancomplementandextendtheeffectsofprofessionaltreatment.Themostprominentself-helpgroupsarethoseaffiliatedwithAlcoholicsAnonymous(AA),NarcoticsAnonymous(NA),andCocaineAnonymous(CA),allofwhicharebasedonthe12-stepmodel.Mostdrugaddictiontreatmentprogramsencouragepatientstoparticipateinself-helpgrouptherapyduringandafterformaltreatment.Thesegroupscanbeparticularlyhelpfulduringrecovery,offeringanaddedlayerofcommunity-levelsocialsupporttohelppeopleachieveandmaintainabstinenceandotherhealthylifestylebehaviorsoverthecourseofalifetime.
Canexerciseplayaroleinthetreatmentprocess?
Yes.Exerciseisincreasinglybecomingacomponentofmanytreatmentprogramsandhasproveneffective,whencombinedwithcognitive-behavioraltherapy,athelpingpeoplequitsmoking.Exercisemayexertbeneficialeffectsbyaddressingpsychosocialandphysiologicalneedsthatnicotinereplacementalonedoesnot,byreducingnegativefeelingsandstress,andbyhelpingpreventweightgainfollowingcessation.Researchtodetermineifandhow

26
exerciseprogramscanplayasimilarroleinthetreatmentofotherformsofdrugabuseisunderway.
HowdoesdrugaddictiontreatmenthelpreducethespreadofHIV/AIDS,HepatitisC(HCV),andotherinfectiousdiseases?
Drug-abusingindividuals,includinginjectingandnon-injectingdrugusers,areatincreasedriskofhumanimmunodeficiencyvirus(HIV),hepatitisCvirus(HCV),andotherinfectiousdiseases.Thesediseasesaretransmittedbysharingcontaminateddruginjectionequipmentandbyengaginginriskysexualbehaviorsometimesassociatedwithdruguse.EffectivedrugabusetreatmentisHIV/HCVpreventionbecauseitreducesactivitiesthatcanspreaddisease,suchassharinginjectionequipmentandengaginginunprotectedsexualactivity.CounselingthattargetsarangeofHIV/HCVriskbehaviorsprovidesanaddedlevelofdiseaseprevention.
DrugabusetreatmentisHIVandHCVprevention.
InjectiondruguserswhodonotentertreatmentareuptosixtimesmorelikelytobecomeinfectedwithHIVthanthosewhoenterandremainintreatment.ParticipationintreatmentalsopresentsopportunitiesforHIVscreeningandreferraltoearlyHIVtreatment.Infact,recentresearchfromNIDA’sNationalDrugAbuseTreatmentClinicalTrialsNetworkshowedthatprovidingrapidonsiteHIVtestinginsubstanceabusetreatmentfacilitiesincreasedpatients’likelihoodofbeingtestedandofreceivingtheirtestresults.HIVcounselingandtestingarekeyaspectsofsuperiordrugabusetreatmentprogramsandshouldbeofferedtoallindividualsenteringtreatment.GreateravailabilityofinexpensiveandunobtrusiverapidHIVtestsshouldincreaseaccesstotheseimportantaspectsofHIVpreventionandtreatment.
27
DrugAddictionTreatmentintheUnitedStates
Treatmentfordrugabuseandaddictionisdeliveredinmanydifferentsettings,usingavarietyofbehavioralandpharmacologicalapproaches.
Drugaddictionisacomplexdisorderthatcaninvolvevirtuallyeveryaspectofanindividual'sfunctioning—inthefamily,atworkandschool,andinthecommunity.
Becauseofaddiction'scomplexityandpervasiveconsequences,drugaddictiontreatmenttypicallymustinvolvemanycomponents.Someofthosecomponentsfocusdirectlyontheindividual'sdruguse;others,likeemploymenttraining,focusonrestoringtheaddictedindividualtoproductivemembershipinthefamilyandsociety(Seediagram"ComponentsofComprehensiveDrugAbuseTreatment"),enablinghimorhertoexperiencetherewardsassociatedwithabstinence.
Treatmentfordrugabuseandaddictionisdeliveredinmanydifferentsettingsusingavarietyofbehavioralandpharmacologicalapproaches.IntheUnitedStates,morethan14,500specializeddrugtreatmentfacilitiesprovidecounseling,behavioraltherapy,medication,casemanagement,andothertypesofservicestopersonswithsubstanceusedisorders.
Alongwithspecializeddrugtreatmentfacilities,drugabuseandaddictionaretreatedinphysicians'officesandmentalhealthclinicsbyavarietyofproviders,includingcounselors,physicians,psychiatrists,psychologists,nurses,andsocialworkers.Treatmentisdeliveredinoutpatient,inpatient,andresidentialsettings.Althoughspecifictreatmentapproachesoftenareassociatedwithparticulartreatmentsettings,avarietyoftherapeuticinterventionsorservicescanbeincludedinanygivensetting.

28
Becausedrugabuseandaddictionaremajorpublichealthproblems,alargeportionofdrugtreatmentisfundedbylocal,State,andFederalgovernments.Privateandemployer-subsidizedhealthplansalsomayprovidecoveragefortreatmentofaddictionanditsmedicalconsequences.Unfortunately,managedcarehasresultedinshorteraveragestays,whileahistoricallackoforinsufficientcoverageforsubstanceabusetreatmenthascurtailedthenumberofoperationalprograms.Therecentpassageofparityforinsurancecoverageofmentalhealthandsubstanceabuseproblemswillhopefullyimprovethisstateofaffairs.HealthCareReform(i.e.,thePatientProtectionandAffordableCareActof2010,"ACA")alsostandstoincreasethedemandfordrugabusetreatmentservicesandpresentsanopportunitytostudyhowinnovationsinservicedelivery,organization,andfinancingcanimproveaccesstoanduseofthem.
TypesofTreatmentPrograms
Researchstudiesonaddictiontreatmenttypicallyhaveclassifiedprogramsintoseveralgeneraltypesormodalities.Treatmentapproachesandindividualprogramscontinuetoevolveanddiversify,andmanyprogramstodaydonotfitneatlyintotraditionaldrugadictiontreatmentclassifications.
Most,however,startwithdetoxificationandmedicallymanagedwithdrawal,oftenconsideredthefirststageoftreatment.Detoxification,theprocessbywhichthebodyclearsitselfofdrugs,isdesignedtomanagetheacuteandpotentiallydangerousphysiologicaleffectsofstoppingdruguse.Asstatedpreviously,detoxificationalonedoesnotaddressthepsychological,social,andbehavioralproblemsassociatedwithaddictionandthereforedoesnottypicallyproducelastingbehavioralchangesnecessaryforrecovery.Detoxificationshouldthusbefollowedbyaformalassessmentandreferraltodrugaddictiontreatment.
Becauseitisoftenaccompaniedbyunpleasantandpotentiallyfatalsideeffectsstemmingfromwithdrawal,detoxificationisoftenmanagedwithmedicationsadministeredbyaphysicianinaninpatientoroutpatientsetting;therefore,itisreferredtoas"medicallymanagedwithdrawal.”Medicationsareavailabletoassistinthewithdrawalfromopioids,benzodiazepines,alcohol,nicotine,

29
barbiturates,andothersedatives.
FurtherReading:
Kleber,H.D.Outpatientdetoxificationfromopiates.PrimaryPsychiatry1:42-52,1996.
Long-TermResidentialTreatment
Long-termresidentialtreatmentprovidescare24hoursaday,generallyinnon-hospitalsettings.Thebest-knownresidentialtreatmentmodelisthetherapeuticcommunity(TC),withplannedlengthsofstayofbetween6and12months.TCsfocusonthe"resocialization"oftheindividualandusetheprogram’sentirecommunity—includingotherresidents,staff,andthesocialcontext—asactivecomponentsoftreatment.Addictionisviewedinthecontextofanindividual’ssocialandpsychologicaldeficits,andtreatmentfocusesondevelopingpersonalaccountabilityandresponsibilityaswellassociallyproductivelives.Treatmentishighlystructuredandcanbeconfrontationalattimes,withactivitiesdesignedtohelpresidentsexaminedamagingbeliefs,self-concepts,anddestructivepatternsofbehaviorandadoptnew,moreharmoniousandconstructivewaystointeractwithothers.ManyTCsoffercomprehensiveservices,whichcanincludeemploymenttrainingandothersupportservices,onsite.ResearchshowsthatTCscanbemodifiedtotreatindividualswithspecialneeds,includingadolescents,women,homelessindividuals,peoplewithseverementaldisorders,andindividualsinthecriminaljusticesystem(see"TreatingCriminalJustice-InvolvedDrugAbusersandAddictedIndividuals").
FurtherReading:
Lewis,B.F.;McCusker,J.;Hindin,R.;Frost,R.;andGarfield,F.Fourresidentialdrugtreatmentprograms:ProjectIMPACT.In:J.A.Inciardi,F.M.Tims,andB.W.Fletcher(eds.),InnovativeApproachesintheTreatmentofDrugAbuse,Westport,CT:GreenwoodPress,pp.45-60,1993.
Sacks,S.;Banks,S.;McKendrick,K.;andSacks,J.Y.Modifiedtherapeuticcommunityforco-occurringdisorders:Asummaryoffourstudies.Journalof
30
SubstanceAbuseTreatment34(1):112-122,2008.
Sacks,S.;Sacks,J.;DeLeon,G.;Bernhardt,A.;andStaines,G.Modifiedtherapeuticcommunityformentallyillchemical"abusers":Background;influences;programdescription;preliminaryfindings.SubstanceUseandMisuse32(9):1217-1259,1997.
Stevens,S.J.,andGlider,P.J.Therapeuticcommunities:Substanceabusetreatmentforwomen.In:F.M.Tims,G.DeLeon,andN.Jainchill(eds.),TherapeuticCommunity:AdvancesinResearchandApplication,NationalInstituteonDrugAbuseResearchMonograph144,NIHPub.No.94-3633,U.S.GovernmentPrintingOffice,pp.162-180,1994.
Sullivan,C.J.;McKendrick,K.;Sacks,S.;andBanks,S.M.ModifiedtherapeuticcommunityforoffenderswithMICAdisorders:Substanceuseoutcomes.AmericanJournalofDrugandAlcoholAbuse33(6):823-832,2007.
Short-TermResidentialTreatment
Short-termresidentialprogramsprovideintensivebutrelativelybrieftreatmentbasedonamodified12-stepapproach.Theseprogramswereoriginallydesignedtotreatalcoholproblems,butduringthecocaineepidemicofthemid-1980s,manybegantotreatothertypesofsubstanceusedisorders.Theoriginalresidentialtreatmentmodelconsistedofa3-to6-weekhospital-basedinpatienttreatmentphasefollowedbyextendedoutpatienttherapyandparticipationinaself-helpgroup,suchasAA.Followingstaysinresidentialtreatmentprograms,itisimportantforindividualstoremainengagedinoutpatienttreatmentprogramsand/oraftercareprograms.Theseprogramshelptoreducetheriskofrelapseonceapatientleavestheresidentialsetting.
FurtherReading:
Hubbard,R.L.;Craddock,S.G.;Flynn,P.M.;Anderson,J.;andEtheridge,R.M.Overviewof1-yearfollow-upoutcomesintheDrugAbuseTreatmentOutcomeStudy(DATOS).PsychologyofAddictiveBehaviors11(4):291-298,1998.

31
Miller,M.M.Traditionalapproachestothetreatmentofaddiction.In:A.W.GrahamandT.K.Schultz(eds.),PrinciplesofAddictionMedicine(2nded.).Washington,D.C.:AmericanSocietyofAddictionMedicine,1998.
OutpatientTreatmentPrograms
Outpatienttreatmentvariesinthetypesandintensityofservicesoffered.Suchtreatmentcostslessthanresidentialorinpatienttreatmentandoftenismoresuitableforpeoplewithjobsorextensivesocialsupports.Itshouldbenoted,however,thatlow-intensityprogramsmayofferlittlemorethandrugeducation.Otheroutpatientmodels,suchasintensivedaytreatment,canbecomparabletoresidentialprogramsinservicesandeffectiveness,dependingontheindividualpatient’scharacteristicsandneeds.Inmanyoutpatientprograms,groupcounselingcanbeamajorcomponent.Someoutpatientprogramsarealsodesignedtotreatpatientswithmedicalorothermentalhealthproblemsinadditiontotheirdrugdisorders.
FurtherReading:
Hubbard,R.L.;Craddock,S.G.;Flynn,P.M.;Anderson,J.;andEtheridge,R.M.Overviewof1-yearfollow-upoutcomesintheDrugAbuseTreatmentOutcomeStudy(DATOS).PsychologyofAddictiveBehaviors11(4):291-298,1998.
InstituteofMedicine.TreatingDrugProblems.Washington,D.C.:NationalAcademyPress,1990.
McLellan,A.T.;Grisson,G.;Durell,J.;Alterman,A.I.;Brill,P.;andO'Brien,C.P.Substanceabusetreatmentintheprivatesetting:Aresomeprogramsmoreeffectivethanothers?JournalofSubstanceAbuseTreatment10:243-254,1993.
Simpson,D.D.,andBrown,B.S.Treatmentretentionandfollow-upoutcomesintheDrugAbuseTreatmentOutcomeStudy(DATOS).PsychologyofAddictiveBehaviors11(4):294-307,1998.

32
IndividualizedDrugCounseling
Individualizeddrugcounselingnotonlyfocusesonreducingorstoppingillicitdrugoralcoholuse;italsoaddressesrelatedareasofimpairedfunctioning—suchasemploymentstatus,illegalactivity,andfamily/socialrelations—aswellasthecontentandstructureofthepatient’srecoveryprogram.Throughitsemphasisonshort-termbehavioralgoals,individualizedcounselinghelpsthepatientdevelopcopingstrategiesandtoolstoabstainfromdruguseandmaintainabstinence.Theaddictioncounselorencourages12-stepparticipation(atleastoneortwotimesperweek)andmakesreferralsforneededsupplementalmedical,psychiatric,employment,andotherservices.
GroupCounseling
Manytherapeuticsettingsusegrouptherapytocapitalizeonthesocialreinforcementofferedbypeerdiscussionandtohelppromotedrug-freelifestyles.Researchhasshownthatwhengrouptherapyeitherisofferedinconjunctionwithindividualizeddrugcounselingorisformattedtoreflecttheprinciplesofcognitive-behavioraltherapyorcontingencymanagement,positiveoutcomesareachieved.Currently,researchersaretestingconditionsinwhichgrouptherapycanbestandardizedandmademorecommunity-friendly.
TreatingCriminalJustice-InvolvedDrugAbusersandAddictedIndividuals
Often,drugabuserscomeintocontactwiththecriminaljusticesystemearlierthanotherhealthorsocialsystems,presentingopportunitiesforinterventionandtreatmentpriorto,during,after,orinlieuofincarceration.Researchhasshownthatcombiningcriminaljusticesanctionswithdrugtreatmentcanbeeffectiveindecreasingdrugabuseandrelatedcrime.Individualsunderlegalcoerciontendtostayintreatmentlongeranddoaswellasorbetterthanthosenotunderlegalpressure.Studiesshowthatforincarceratedindividualswithdrugproblems,startingdrugabusetreatmentinprisonandcontinuingthesametreatmentuponrelease—inotherwords,aseamlesscontinuumofservices—resultsinbetteroutcomes:lessdruguseandlesscriminalbehavior.Moreinformationonhowthecriminaljusticesystemcanaddresstheproblemofdrug

33
addictioncanbefoundinPrinciplesofDrugAbuseTreatmentforCriminalJusticePopulations:AResearch-BasedGuide(NationalInstituteonDrugAbuse,revised2012).
TreatingCriminalJustice-InvolvedDrugAbusersandAddictedIndividuals
Often,drugabuserscomeintocontactwiththecriminaljusticesystemearlierthanotherhealthorsocialsystems,presentingopportunitiesforinterventionandtreatmentpriorto,during,after,orinlieuofincarceration.Researchhasshownthatcombiningcriminaljusticesanctionswithdrugtreatmentcanbeeffectiveindecreasingdrugabuseandrelatedcrime.Individualsunderlegalcoerciontendtostayintreatmentlongeranddoaswellasorbetterthanthosenotunderlegalpressure.Studiesshowthatforincarceratedindividualswithdrugproblems,startingdrugabusetreatmentinprisonandcontinuingthesametreatmentuponrelease—inotherwords,aseamlesscontinuumofservices—resultsinbetteroutcomes:lessdruguseandlesscriminalbehavior.MoreinformationonhowthecriminaljusticesystemcanaddresstheproblemofdrugaddictioncanbefoundinPrinciplesofDrugAbuseTreatmentforCriminalJusticePopulations:AResearch-BasedGuide(NationalInstituteonDrugAbuse,revised2012).

34
Evidence-BasedApproachestoDrugAddictionTreatment
Eachapproachtodrugtreatmentisdesignedtoaddresscertainaspectsofdrugaddictionanditsconsequencesfortheindividual,family,andsociety.
Thissectionpresentsexamplesoftreatmentapproachesandcomponentsthathaveanevidencebasesupportingtheiruse.Eachapproachisdesignedtoaddresscertainaspectsofdrugaddictionanditsconsequencesfortheindividual,family,andsociety.Someoftheapproachesareintendedtosupplementorenhanceexistingtreatmentprograms,andothersarefairlycomprehensiveinandofthemselves.
ThefollowingsectionisbrokendownintoPharmacotherapies,BehavioralTherapies,andBehavioralTherapiesPrimarilyforAdolescents.Theyarefurthersubdividedaccordingtoparticularsubstanceusedisorders.Thislistisnotexhaustive,andnewtreatmentsarecontinuallyunderdevelopment.
Pharmacotherapies
OpioidAddiction
Methadone
Methadoneisalong-actingsyntheticopioidagonistmedicationthatcanpreventwithdrawalsymptomsandreducecravinginopioid-addictedindividuals.Itcanalsoblocktheeffectsofillicitopioids.Ithasalonghistoryofuseintreatmentofopioiddependenceinadultsandistakenorally.MethadonemaintenancetreatmentisavailableinallbutthreeStatesthroughspeciallylicensedopioidtreatmentprogramsormethadonemaintenanceprograms.

35
Combinedwithbehavioraltreatment:Researchhasshownthatmethadonemaintenanceismoreeffectivewhenitincludesindividualand/orgroupcounseling,withevenbetteroutcomeswhenpatientsareprovidedwith,orreferredto,otherneededmedical/psychiatric,psychological,andsocialservices(e.g.,employmentorfamilyservices).
FurtherReading:
Dole,V.P.;Nyswander,M.;andKreek,M.J.Narcoticblockade.ArchivesofInternalMedicine118:304–309,1966.
McLellan,A.T.;Arndt,I.O.;Metzger,D.;Woody,G.E.;andO’Brien,C.P.Theeffectsofpsychosocialservicesinsubstanceabusetreatment.TheJournaloftheAmericanMedicalAssociation269(15):1953–1959,1993.
TheRockerfellerUniversity.Thefirstpharmacologicaltreatmentfornarcoticaddiction:Methadonemaintenance.TheRockefellerUniversityHospitalCentennial,2010.Availableatcentennial.rucares.org/index.php?page=Methadone_Maintenance.
Woody,G.E.;Luborsky,L.;McClellan,A.T.;O’Brien,C.P.;Beck,A.T.;Blaine,J.;Herman,I.;andHole,A.Psychotherapyforopiateaddicts:Doesithelp?ArchivesofGeneralPsychiatry40:639–645,1983.
Buprenorphine
Buprenorphineisasyntheticopioidmedicationthatactsasapartialagonistatopioidreceptors—itdoesnotproducetheeuphoriaandsedationcausedbyheroinorotheropioidsbutisabletoreduceoreliminatewithdrawalsymptomsassociatedwithopioiddependenceandcarriesalowriskofoverdose.
Buprenorphineiscurrentlyavailableintwoformulationsthataretakensublingually:(1)apureformofthedrugand(2)amorecommonlyprescribedformulationcalledSuboxone,whichcombinesbuprenorphinewiththedrugnaloxone,anantagonist(orblocker)atopioidreceptors.Naloxonehasnoeffect

36
whenSuboxoneistakenasprescribed,butifanaddictedindividualattemptstoinjectSuboxone,thenaloxonewillproduceseverewithdrawalsymptoms.Thus,thisformulationlessensthelikelihoodthatthedrugwillbeabusedordivertedtoothers.
Buprenorphinetreatmentfordetoxificationand/ormaintenancecanbeprovidedinoffice-basedsettingsbyqualifiedphysicianswhohavereceivedawaiverfromtheDrugEnforcementAdministration(DEA),allowingthemtoprescribeit.Theavailabilityofoffice-basedtreatmentforopioidaddictionisacost-effectiveapproachthatincreasesthereachoftreatmentandtheoptionsavailabletopatients.
Buprenorphineisalsoavailableasinanimplantandinjection.TheU.S.FoodandDrugAdministration(FDA)approveda6-monthsubdermalbuprenorphineimplantinMay2016andaonce-monthlybuprenorphineinjectioninNovember2017.
FurtherReading:
Fiellin,D.A.;Pantalon,M.V.;Chawarski,M.C.;Moore,B.A.;Sullivan,L.E.;O’Connor,P.G.;andSchottenfeld,R.S.Counselingplusbuprenorphine/naloxonemaintenancetherapyforopioiddependence.TheNewEnglandJournalofMedicine355(4):365–374,2006.
FudalaP.J.;Bridge,T.P.;Herbert,S.;Williford,W.O.;Chiang,C.N.;Jones,K.;Collins,J.;Raisch,D.;Casadonte,P.;Goldsmith,R.J.;Ling,W.;Malkerneker,U.;McNicholas,L.;Renner,J.;Stine,S.;andTusel,D.fortheBuprenorphine/NaloxoneCollaborativeStudyGroup.Office-basedtreatmentofopiateaddictionwithasublingual-tabletformulationofbuprenorphineandnaloxone.TheNewEnglandJournalofMedicine349(10):949–958,2003.
Kosten,T.R.;andFiellin,D.A.U.S.NationalBuprenorphineImplementationProgram:Buprenorphineforoffice-basedpractice.Consensusconferenceoverview.TheAmericanJournalonAddictions13(Suppl.1):S1–S7,2004.

37
McCance-Katz,E.F.Office-basedbuprenorphinetreatmentforopioid-dependentpatients.HarvardReviewofPsychiatry12(6):321–338,2004.
Treatment,notSubstitution
Becausemethadoneandbuprenorphinearethemselvesopioids,somepeopleviewthesetreatmentsforopioiddependenceasjustsubstitutionsofoneaddictivedrugforanother(seeQuestion19).Buttakingthesemedicationsasprescribedallowspatientstoholdjobs,avoidstreetcrimeandviolence,andreducetheirexposuretoHIVbystoppingordecreasinginjectiondruguseanddrug-relatedhigh-risksexualbehavior.Patientsstabilizedonthesemedicationscanalsoengagemorereadilyincounselingandotherbehavioralinterventionsessentialtorecovery.
Naltrexone
Naltrexoneisasyntheticopioidantagonist—itblocksopioidsfrombindingtotheirreceptorsandtherebypreventstheireuphoricandothereffects.Ithasbeenusedformanyyearstoreverseopioidoverdoseandisalsoapprovedfortreatingopioidaddiction.Thetheorybehindthistreatmentisthattherepeatedabsenceofthedesiredeffectsandtheperceivedfutilityofabusingopioidswillgraduallydiminishcravingandaddiction.Naltrexoneitselfhasnosubjectiveeffectsfollowingdetoxification(thatis,apersondoesnotperceiveanyparticulardrugeffect),ithasnopotentialforabuse,anditisnotaddictive.
Naltrexoneasatreatmentforopioidaddictionisusuallyprescribedinoutpatientmedicalsettings,althoughthetreatmentshouldbeginaftermedicaldetoxificationinaresidentialsettinginordertopreventwithdrawalsymptoms.
Naltrexonemustbetakenorally—eitherdailyorthreetimesaweek—butnoncompliancewithtreatmentisacommonproblem.Manyexperiencedclinicianshavefoundnaltrexonebestsuitedforhighlymotivated,recentlydetoxifiedpatientswhodesiretotalabstinencebecauseofexternalcircumstances—forinstance,professionalsorparolees.Recently,along-acting
38
injectableversionofnaltrexone,calledVivitrol,wasapprovedtotreatopioidaddiction.Becauseitonlyneedstobedeliveredonceamonth,thisversionofthedrugcanfacilitatecomplianceandoffersanalternativeforthosewhodonotwishtobeplacedonagonist/partialagonistmedications.
FurtherReading:
Cornish,J.W.;Metzger,D.;Woody,G.E.;Wilson,D.;McClellan,A.T.;andVandergrift,B.Naltrexonepharmacotherapyforopioiddependentfederalprobationers.JournalofSubstanceAbuseTreatment14(6):529–534,1997.
Gastfriend,D.R.Intramuscularextended-releasenaltrexone:currentevidence.AnnalsoftheNewYorkAcademyofSciences1216:144–166,2011.
Krupitsky,E.;Illerperuma,A.;Gastfriend,D.R.;andSilverman,B.L.Efficacyandsafetyofextended-releaseinjectablenaltrexone(XR-NTX)forthetreatmentofopioiddependence.Paperpresentedatthe2010annualmeetingoftheAmericanPsychiatricAssociation,NewOrleans,LA.
ComparingBuprenorphineandNaltrexone
ANIDAstudycomparingtheeffectivenessofabuprenorphine/naloxonecombinationandanextendedreleasenaltrexoneformulationontreatingopioidusedisorderhasfoundthatbothmedicationsaresimilarlyeffectiveintreatingopioidusedisorderoncetreatmentisinitiated.Becausenaltrexonerequiresfulldetoxification,initiatingtreatmentamongactiveopioiduserswasmoredifficultwiththismedication.However,oncedetoxificationwascomplete,thenaltrexoneformulationhadasimilareffectivenessasthebuprenorphine/naloxonecombination.
TobaccoAddiction
NicotineReplacementTherapy(NRT)
Avarietyofformulationsofnicotinereplacementtherapies(NRTs)nowexist,

39
includingthetransdermalnicotinepatch,nicotinespray,nicotinegum,andnicotinelozenges.Becausenicotineisthemainaddictiveingredientintobacco,therationaleforNRTisthatstablelowlevelsofnicotinewillpreventwithdrawalsymptoms—whichoftendrivecontinuedtobaccouse—andhelpkeeppeoplemotivatedtoquit.Researchshowsthatcombiningthepatchwithanotherreplacementtherapyismoreeffectivethanasingletherapyalone.
Bupropion(Zyban )
Bupropionwasoriginallymarketedasanantidepressant(Wellbutrin).Itproducesmildstimulanteffectsbyblockingthereuptakeofcertainneurotransmitters,especiallynorepinephrineanddopamine.Aserendipitousobservationamongdepressedpatientswasthatthemedicationwasalsoeffectiveinsuppressingtobaccocraving,helpingthemquitsmokingwithoutalsogainingweight.Althoughbupropion’sexactmechanismsofactioninfacilitatingsmokingcessationareunclear,ithasFDAapprovalasasmokingcessationtreatment.
Varenicline(Chantix )
VareniclineisthemostrecentlyFDA-approvedmedicationforsmokingcessation.Itactsonasubsetofnicotinicreceptorsinthebrainthoughttobeinvolvedintherewardingeffectsofnicotine.Vareniclineactsasapartialagonist/antagonistatthesereceptors—thismeansthatitmidlystimulatesthenicotinereceptorbutnotsufficientlytotriggerthereleaseofdopamine,whichisimportantfortherewardingeffectsofnicotine.Asanantagonist,vareniclinealsoblockstheabilityofnicotinetoactivatedopamine,interferingwiththereinforcingeffectsofsmoking,therebyreducingcravingsandsupportingabstinencefromsmoking.
CombinedWithBehavioralTreatment
Eachoftheabovepharmacotherapiesisrecommendedforuseincombinationwithbehavioralinterventions,includinggroupandindividualtherapies,aswellastelephonequitlines.Behavioralapproachescomplementmosttobaccoaddictiontreatmentprograms.Theycanamplifytheeffectsofmedicationsby
®
®
40
teachingpeoplehowtomanagestress,recognizeandavoidhigh-risksituationsforsmokingrelapse,anddevelopalternativecopingstrategies(e.g.,cigaretterefusalskills,assertiveness,andtimemanagementskills)thattheycanpracticeintreatment,social,andworksettings.Combinedtreatmentisurgedbecausebehavioralandpharmacologicaltreatmentsarethoughttooperatebydifferentyetcomplementarymechanismsthatcanhaveadditiveeffects.
FurtherReading:
Alterman,A.I.;Gariti,P.;andMulvaney,F.Short-andlong-termsmokingcessationforthreelevelsofintensityofbehavioraltreatment.PsychologyofAddictiveBehaviors15:261-264,2001.
Hall,S.M.;Humfleet,G.L.;Muñoz,R.F.;V.I;Prochaska,J.J.;andRobbins,J.A.Usingextendedcognitivebehavioraltreatmentandmedicationtotreatdependentsmokers.AmericanJournalofPublicHealth101:2349–2356,2011.
Jorenby,D.E.;Hays,J.T.;Rigotti,N.A.;Azoulay,S.;Watsky,E.J.;Williams,K.E.;Billing,C.B.;Gong,J.;andReeves,K.R.VareniclinePhase3StudyGroup.Efficacyofvarenicline,an42nicotinicacetylcholinereceptorpartialagonistvs.placeboorsustained-releasebupropionforsmokingcessation:Arandomizedcontrolledtrial.TheJournaloftheAmericanMedicalAssociation296(1):56–63,2006.
King,D.P.;Paciqa,S.;Pickering,E.;Benowitz,N.L.;Bierut,L.J.;Conti,D.V.;Kaprio,J.;Lerman,C.;andPark,P.W.Smokingcessationpharmacogenetics:Analysisofvareniclineandbupropioninplacebo-controlledclinicaltrials.Neuropsychopharmacology37:641–650,2012.
Raupach,T.;andvanSchayck,C.P.Pharmacotherapyforsmokingcessation:Currentadvancesandresearchtopics.CNSDrugs25:371–382,2011.
Shah,S.D.;Wilken,L.A.;Winkler,S.R.;andLin,S.J.Systematicreviewandmeta-analysisofcombinationtherapyforsmokingcessation.JournaloftheAmericanPharmaceuticalAssociation48(5):659–665,2008.
41
Smith,S.S;McCarthy,D.E.;JapuntichS.J.;Christiansen,B.;Piper,M.E.;Jorenby,D.E.;Fraser,D.L.;Fiore,M.C.;Baker,T.B.;andJackson,T.C.Comparativeeffectivenessof5smokingcessationpharmacotherapiesinprimarycareclinics.ArchivesofInternalMedicine169:2148–2155,2009.
Stitzer,M.Combinedbehavioralandpharmacologicaltreatmentsforsmokingcessation.Nicotine&TobaccoResearch1:S181–S187,1999.
AlcoholAddiction
Naltrexone
Naltrexoneblocksopioidreceptorsthatareinvolvedintherewardingeffectsofdrinkingandthecravingforalcohol.Ithasbeenshowntoreducerelapsetoproblemdrinkinginsomepatients.Anextendedreleaseversion,Vivitrol—administeredonceamonthbyinjection—isalsoFDA-approvedfortreatingalcoholism,andmayofferbenefitsregardingcompliance.
Acamprosate
Acamprosate(Campral )actsonthegamma-aminobutyricacid(GABA)andglutamateneurotransmittersystemsandisthoughttoreducesymptomsofprotractedwithdrawal,suchasinsomnia,anxiety,restlessness,anddysphoria.Acamprosatehasbeenshowntohelpdependentdrinkersmaintainabstinenceforseveralweekstomonths,anditmaybemoreeffectiveinpatientswithseveredependence.
Disulfiram
Disulfiram(Antabuse )interfereswithdegradationofalcohol,resultingintheaccumulationofacetaldehyde,which,inturn,producesaveryunpleasantreactionthatincludesflushing,nausea,andplapitationsifapersondrinksalcohol.Theutilityandeffectivenessofdisulfiramareconsideredlimitedbecausecomplianceisgenerallypoor.However,amongpatientswhoarehighlymotivated,disulfiramcanbeeffective,andsomepatientsuseit
®
®

42
episodicallyforhigh-risksituations,suchassocialoccasionswherealcoholispresent.Itcanalsobeadministeredinamonitoredfashion,suchasinaclinicorbyaspouse,improvingitsefficacy.
Topiramate
Topiramateisthoughttoworkbyincreasinginhibitory(GABA)neurotransmissionandreducingstimulatory(glutamate)neurotransmission,althoughitsprecisemechanismofactionisnotknown.AlthoughtopiramatehasnotyetreceivedFDAapprovalfortreatingalcoholaddiction,itissometimesusedoff-labelforthispurpose.Topiramatehasbeenshowninstudiestosignificantlyimprovemultipledrinkingoutcomes,comparedwithaplacebo.
CombinedWithBehavioralTreatment
Whileanumberofbehavioraltreatmentshavebeenshowntobeeffectiveinthetreatmentofalcoholaddiction,itdoesnotappearthatanadditiveeffectexistsbetweenbehavioraltreatmentsandpharmacotherapy.Studieshaveshownthatjustgettinghelpisoneofthemostimportantfactorsintreatingalcoholaddiction;theprecisetypeoftreatmentreceivedisnotasimportant.
FurtherReading:
Anton,R.F.;O’Malley,S.S.;Ciraulo,D.A.;Cisler,R.A.;Couper,D.;Donovan,D.M.;Gastfriend,D.R.;Hosking,J.D.;Johnson,B.A.;LoCastro,J.S.;Longabaugh,R.;Mason,B.J.;Mattson,M.E.;Miller,W.R.;Pettinati,H.M.;Randall,C.L.;Swift,R.;Weiss,R.D.;Williams,L.D.;andZweben,A.,fortheCOMBINEStudyResearchGroup.Combinedpharmacotherapiesandbehavioralinterventionsforalcoholdependence:TheCOMBINEstudy:Arandomizedcontrolledtrial.TheJournaloftheAmericanMedicalAssociation295(17):2003–2017,2006.
NationalInstituteonAlcoholAbuseandAlcoholism.HelpingPatientsWhoDrinkTooMuch:AClinician’sGuide,Updated2005Edition.Bethesda,MD:NIAAA,updated2005.Availableatpubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/clinicians_guide.htm

43
BehavioralTherapies
Behavioralapproacheshelpengagepeopleindrugabusetreatment,provideincentivesforthemtoremainabstinent,modifytheirattitudesandbehaviorsrelatedtodrugabuse,andincreasetheirlifeskillstohandlestressfulcircumstancesandenvironmentalcuesthatmaytriggerintensecravingfordrugsandpromptanothercycleofcompulsiveabuse.Belowareanumberofbehavioraltherapiesshowntobeeffectiveinaddressingsubstanceabuse(effectivenesswithparticulardrugsofabuseisdenotedinparentheses).
Cognitive-BehavioralTherapy(Alcohol,Marijuana,Cocaine,Methamphetamine,Nicotine)
Cognitive-BehavioralTherapy(CBT)wasdevelopedasamethodtopreventrelapsewhentreatingproblemdrinking,andlateritwasadaptedforcocaine-addictedindividuals.Cognitive-behavioralstrategiesarebasedonthetheorythatinthedevelopmentofmaladaptivebehavioralpatternslikesubstanceabuse,learningprocessesplayacriticalrole.IndividualsinCBTlearntoidentifyandcorrectproblematicbehaviorsbyapplyingarangeofdifferentskillsthatcanbeusedtostopdrugabuseandtoaddressarangeofotherproblemsthatoftenco-occurwithit.
AcentralelementofCBTisanticipatinglikelyproblemsandenhancingpatients’self-controlbyhelpingthemdevelopeffectivecopingstrategies.Specifictechniquesincludeexploringthepositiveandnegativeconsequencesofcontinueddruguse,self-monitoringtorecognizecravingsearlyandidentifysituationsthatmightputoneatriskforuse,anddevelopingstrategiesforcopingwithcravingsandavoidingthosehigh-risksituations.
Researchindicatesthattheskillsindividualslearnthroughcognitive-behavioralapproachesremainafterthecompletionoftreatment.CurrentresearchfocusesonhowtoproduceevenmorepowerfuleffectsbycombiningCBTwithmedicationsfordrugabuseandwithothertypesofbehavioraltherapies.Acomputer-basedCBTsystemhasalsobeendevelopedandhasbeenshowntobeeffectiveinhelpingreducedrugusefollowingstandarddrugabuse

44
treatment.
FurtherReading:
Carroll,K.M.,Easton,C.J.;Nich,C.;Hunkele,K.A.;Neavins,T.M.;Sinha,R.;Ford,H.L.;Vitolo,S.A;Doebrick,C.A.;andRounsaville,B.J.Theuseofcontingencymanagementandmotivational/skills-buildingtherapytotreatyoungadultswithmarijuanadependence.JournalofConsultingandClinicalPsychology74(5):955–966,2006.
Carroll,K.M.;andOnken,L.S.Behavioraltherapiesfordrugabuse.TheAmericanJournalofPsychiatry168(8):1452–1460,2005.
Carroll,K.M.;Sholomskas,D.;Syracuse,G.;Ball,S.A.;Nuro,K.;andFenton,L.R.Wedon’ttraininvain:Adisseminationtrialofthreestrategiesoftrainingcliniciansincognitive-behavioraltherapy.JournalofConsultingandClinicalPsychology73(1):106–115,2005.
Carroll,K.;Fenton,L.R.;Ball,S.A.;Nich,C.;Frankforter,T.L.;Shi,J.;andRounsaville,B.J.Efficacyofdisulfiramandcognitivebehaviortherapyincocaine-dependentoutpatients:Arandomizedplacebo-controlledtrial.ArchivesofGeneralPsychiatry61(3):264–272,2004.
Carroll,K.M.;Ball,S.A.;Martino,S.;Nich,C.;Babuscio,T.A.;Nuro,K.F.;Gordon,M.A.;Portnoy,G.A.;andRounsaville,B.J.Computer-assisteddeliveryofcognitive-behavioraltherapyforaddiction:arandomizedtrialofCBT4CBT.TheAmericanJournalofPsychiatry165(7):881–888,2008.
ContingencyManagementInterventions/MotivationalIncentives(Alcohol,Stimulants,Opioids,Marijuana,Nicotine)
Researchhasdemonstratedtheeffectivenessoftreatmentapproachesusingcontingencymanagement(CM)principles,whichinvolvegivingpatients

45
tangiblerewardstoreinforcepositivebehaviorssuchasabstinence.Studiesconductedinbothmethadoneprogramsandpsychosocialcounselingtreatmentprogramsdemonstratethatincentive-basedinterventionsarehighlyeffectiveinincreasingtreatmentretentionandpromotingabstinencefromdrugs.
Voucher-BasedReinforcement(VBR)augmentsothercommunity-basedtreatmentsforadultswhoprimarilyabuseopioids(especiallyheroin)orstimulants(especiallycocaine)orboth.InVBR,thepatientreceivesavoucherforeverydrug-freeurinesampleprovided.Thevoucherhasmonetaryvaluethatcanbeexchangedforfooditems,moviepasses,orothergoodsorservicesthatareconsistentwithadrug-freelifestyle.Thevouchervaluesarelowatfirst,butincreaseasthenumberofconsecutivedrug-freeurinesamplesincreases;positiveurinesamplesresetthevalueofthevoucherstotheinitiallowvalue.VBRhasbeenshowntobeeffectiveinpromotingabstinencefromopioidsandcocaineinpatientsundergoingmethadonedetoxification.
PrizeIncentivesCMappliessimilarprinciplesasVBRbutuseschancestowincashprizesinsteadofvouchers.Overthecourseoftheprogram(atleast3months,oneormoretimesweekly),participantssupplyingdrug-negativeurineorbreathtestsdrawfromabowlforthechancetowinaprizeworthbetween$1and$100.Participantsmayalsoreceivedrawsforattendingcounselingsessionsandcompletingweeklygoal-relatedactivities.Thenumberofdrawsstartsatoneandincreaseswithconsecutivenegativedrugtestsand/orcounselingsessionsattendedbutresetstoonewithanydrug-positivesampleorunexcusedabsence.Thepractitionercommunityhasraisedconcernsthatthisinterventioncouldpromotegambling—asitcontainsanelementofchance—andthatpathologicalgamblingandsubstanceusedisorderscanbecomorbid.However,studiesexaminingthisconcernfoundthatPrizeIncentivesCMdidnotpromotegamblingbehavior.
FurtherReading:
Budney,A.J.;Moore,B.A.;Rocha,H.L.;andHiggins,S.T.Clinicaltrialofabstinence-basedvouchersandcognitivebehavioraltherapyforcannabisdependence.JournalofConsultingandClinicalPsychology74(2):307–316,2006.

46
Budney,A.J.;Roffman,R.;Stephens,R.S.;andWalker,D.Marijuanadependenceanditstreatment.AddictionScience&ClinicalPractice4(1):4–16,2007.
Elkashef,A.;Vocci,F.;Huestis,M.;Haney,M.;Budney,A.;Gruber,A.;andel-Guebaly,N.Marijuananeurobiologyandtreatment.SubstanceAbuse29(3):17–29,2008.
Peirce,J.M.;Petry,N.M.;Stitzer,M.L.;Blaine,J.;Kellogg,S.;Satterfield,F.;Schwartz,M.;Krasnansky,J.;Pencer,E.;Silva-Vazquez,L.;Kirby,K.C.;Royer-Malvestuto,C.;Cohen,A.;Copersino,M.L.;Kolodner,K.;andLi,R.Effectsoflower-costincentivesonstimulantabstinenceinmethadonemaintenancetreatment:ANationalDrugAbuseTreatmentClinicalTrialsNetworkstudy.ArchivesofGeneralPsychiatry63(2):201–208,2006.
Petry,N.M.;Peirce,J.M.;Stitzer,M.L.;Blaine,J.;Roll,J.M.;Cohen,A.;Obert,J.;Killeen,T.;Saladin,M.E.;Cowell,M.;Kirby,K.C.;Sterling,R.;Royer-Malvestuto,C.;Hamilton,J.;Booth,R.E.;Macdonald,M.;Liebert,M.;Rader,L.;Burns,R;DiMaria,J.;Copersino,M.;Stabile,P.Q.;Kolodner,K.;andLi,R.Effectofprizebasedincentivesonoutcomesinstimulantabusersinoutpatientpsychosocialtreatmentprograms:ANationalDrugAbuseTreatmentClinicalTrialsNetworkstudy.ArchivesofGeneralPsychiatry62(10):1148–1156,2005.
Petry,N.M.;Kolodner,K.B.;Li,R.;Peirce,J.M.;Roll,J.M.;Stitzer,M.L.;andHamilton,J.A.Prize-basedcontingencymanagementdoesnotincreasegambling.DrugandAlcoholDependence83(3):269–273,2006.
Prendergast,M.;Podus,D.;Finney,J.;Greenwell,L.;andRoll,J.Contingencymanagementfortreatmentofsubstanceusedisorders:Ameta-analysis.Addiction101(11):1546–1560,2006.
Roll,J.M.;Petry,N.M.;Stitzer,M.L.;Brecht,M.L.;Peirce,J.M.;McCann,M.J.;Blaine,J.;MacDonald,M.;DiMaria,J.;Lucero,L.;andKellogg,S.Contingencymanagementforthetreatmentofmethamphetamineusedisorders.TheAmericanJournalofPsychiatry163(11):1993–1999,2006.
47
CommunityReinforcementApproachPlusVouchers(Alcohol,Cocaine,Opioids)
CommunityReinforcementApproach(CRA)PlusVouchersisanintensive24-weekoutpatienttherapyfortreatingpeopleaddictedtococaineandalcohol.Itusesarangeofrecreational,familial,social,andvocationalreinforcers,alongwithmaterialincentives,tomakeanon-drug-usinglifestylemorerewardingthansubstanceuse.Thetreatmentgoalsaretwofold:
Tomaintainabstinencelongenoughforpatientstolearnnewlifeskillstohelpsustainit;and
Toreducealcoholconsumptionforpatientswhosedrinkingisassociatedwithcocaineuse
Patientsattendoneortwoindividualcounselingsessionseachweek,wheretheyfocusonimprovingfamilyrelations,learnavarietyofskillstominimizedruguse,receivevocationalcounseling,anddevelopnewrecreationalactivitiesandsocialnetworks.Thosewhoalsoabusealcoholreceiveclinic-monitoreddisulfiram(Antabuse)therapy.Patientssubmiturinesamplestwoorthreetimeseachweekandreceivevouchersforcocaine-negativesamples.AsinVBR,thevalueofthevouchersincreaseswithconsecutivecleansamples,andthevouchersmaybeexchangedforretailgoodsthatareconsistentwithadrug-freelifestyle.Studiesinbothurbanandruralareashavefoundthatthisapproachfacilitatespatients’engagementintreatmentandsuccessfullyaidsthemingainingsubstantialperiodsofcocaineabstinence.
Acomputer-basedversionofCRAPlusVoucherscalledtheTherapeuticEducationSystem(TES)wasfoundtobenearlyaseffectiveastreatmentadministeredbyatherapistinpromotingabstinencefromopioidsandcocaineamongopioid-dependentindividualsinoutpatienttreatment.AversionofCRAforadolescentsaddressesproblem-solving,coping,andcommunicationskillsandencouragesactiveparticipationinpositivesocialandrecreationalactivities.
FurtherReading:

48
Brooks,A.C.;Ryder,D.;Carise,D.;andKirby,K.C.Feasibilityandeffectivenessofcomputer-basedtherapyincommunitytreatment.JournalofSubstanceAbuseTreatment39(3):227–235,2010.
Higgins,S.T.;Sigmon,S.C.;Wong,C.J.;Heil,S.H.;Badger,G.J.;Donham,R.;Dantona,R.L.;andAnthony,S.Communityreinforcementtherapyforcocaine-dependentoutpatients.ArchivesofGeneralPsychiatry60(10):1043–1052,2003.
Roozen,H.G.;Boulogne,J.J.;vanTulder,M.W.;vandenBrink,W.;DeJong,C.A.J.;andKerhof,J.F.M.Asystemicreviewoftheeffectivenessofthecommunityreinforcementapproachinalcohol,cocaineandopioidaddiction.DrugandAlcoholDependence74(1):1–13,2004.
Silverman,K.;Higgins,S.T.;Brooner,R.K.;Montoya,I.D.;Cone,E.J.;Schuster,C.R.;andPreston,K.L.Sustainedcocaineabstinenceinmethadonemaintenancepatientsthroughvoucher-basedreinforcementtherapy.ArchivesofGeneralPsychiatry53(5):409–415,1996.
Smith,J.E.;Meyers,R.J.;andDelaney,H.D.Thecommunityreinforcementapproachwithhomelessalcohol-dependentindividuals.JournalofConsultingandClinicalPsychology66(3):541–548,1998.
Stahler,G.J.;Shipley,T.E.;Kirby,K.C.;Godboldte,C.;Kerwin,M.E;Shandler,I.;andSimons,L.Developmentandinitialdemonstrationofacommunity-basedinterventionforhomeless,cocaine-using,African-Americanwomen.JournalofSubstanceAbuseTreatment28(2):171–179,2005.
MotivationalEnhancementTherapy(Alcohol,Marijuana,Nicotine)
MotivationalEnhancementTherapy(MET)isacounselingapproachthathelpsindividualsresolvetheirambivalenceaboutengagingintreatmentandstoppingtheirdruguse.Thisapproachaimstoevokerapidandinternallymotivatedchange,ratherthanguidethepatientstepwisethroughtherecoveryprocess.

49
Thistherapyconsistsofaninitialassessmentbatterysession,followedbytwotofourindividualtreatmentsessionswithatherapist.Inthefirsttreatmentsession,thetherapistprovidesfeedbacktotheinitialassessment,stimulatingdiscussionaboutpersonalsubstanceuseandelicitingself-motivationalstatements.Motivationalinterviewingprinciplesareusedtostrengthenmotivationandbuildaplanforchange.Copingstrategiesforhigh-risksituationsaresuggestedanddiscussedwiththepatient.Insubsequentsessions,thetherapistmonitorschange,reviewscessationstrategiesbeingused,andcontinuestoencouragecommitmenttochangeorsustainedabstinence.Patientssometimesareencouragedtobringasignificantothertosessions.
ResearchonMETsuggeststhatitseffectsdependonthetypeofdrugusedbyparticipantsandonthegoaloftheintervention.Thisapproachhasbeenusedsuccessfullywithpeopleaddictedtoalcoholtobothimprovetheirengagementintreatmentandreducetheirproblemdrinking.METhasalsobeenusedsuccessfullywithmarijuana-dependentadultswhencombinedwithcognitive-behavioraltherapy,constitutingamorecomprehensivetreatmentapproach.TheresultsofMETaremixedforpeopleabusingotherdrugs(e.g.,heroin,cocaine,nicotine)andforadolescentswhotendtousemultipledrugs.Ingeneral,METseemstobemoreeffectiveforengagingdrugabusersintreatmentthanforproducingchangesindruguse.
FurtherReading:
Baker,A.;Lewin,T.;Reichler,H.;Clancy,R.;Carr,V.;Garrett,R.;Sly,K.;Devir,H.;andTerry,M.Evaluationofamotivationalinterviewforsubstanceusewithpsychiatricin-patientservices.Addiction97(10):1329-1337,2002.
Haug,N.A.;Svikis,D.S.;andDiclemente,C.Motivationalenhancementtherapyfornicotinedependenceinmethadone-maintainedpregnantwomen.PsychologyofAddictiveBehaviors18(3):289-292,2004.
MarijuanaTreatmentProjectResearchGroup.Brieftreatmentsforcannabisdependence:Findingsfromarandomizedmultisitetrial.JournalofConsultingandClinicalPsychology72(3):455-466,2004.
50
Miller,W.R.;Yahne,C.E.;andTonigan,J.S.Motivationalinterviewingindrugabuseservices:Arandomizedtrial.JournalofConsultingandClinicalPsychology71(4):754-763,2003.
Stotts,A.L.;Diclemente,C.C.;andDolan-Mullen,P.One-to-one:Amotivationalinterventionforresistantpregnantsmokers.AddictiveBehaviors27(2):275-292,2002.
TheMatrixModel(Stimulants)
TheMatrixModelprovidesaframeworkforengagingstimulant(e.g.,methamphetamineandcocaine)abusersintreatmentandhelpingthemachieveabstinence.Patientslearnaboutissuescriticaltoaddictionandrelapse,receivedirectionandsupportfromatrainedtherapist,andbecomefamiliarwithself-helpprograms.Patientsaremonitoredfordrugusethroughurinetesting.
Thetherapistfunctionssimultaneouslyasteacherandcoach,fosteringapositive,encouragingrelationshipwiththepatientandusingthatrelationshiptoreinforcepositivebehaviorchange.Theinteractionbetweenthetherapistandthepatientisauthenticanddirectbutnotconfrontationalorparental.Therapistsaretrainedtoconducttreatmentsessionsinawaythatpromotesthepatient’sself-esteem,dignity,andself-worth.Apositiverelationshipbetweenpatientandtherapistiscriticaltopatientretention.
Treatmentmaterialsdrawheavilyonothertestedtreatmentapproachesand,thus,includeelementsofrelapseprevention,familyandgrouptherapies,drugeducation,andself-helpparticipation.Detailedtreatmentmanualscontainworksheetsforindividualsessions;othercomponentsincludefamilyeducationgroups,earlyrecoveryskillsgroups,relapsepreventiongroups,combinedsessions,urinetests,12-stepprograms,relapseanalysis,andsocialsupportgroups.
AnumberofstudieshavedemonstratedthatparticipantstreatedusingtheMatrixModelshowstatisticallysignificantreductionsindrugandalcoholuse,improvementsinpsychologicalindicators,andreducedriskysexualbehaviors

51
associatedwithHIVtransmission.
FurtherReading:
Huber,A.;Ling,W.;Shoptaw,S.;Gulati,V.;Brethen,P.;andRawson,R.Integratingtreatmentsformethamphetamineabuse:Apsychosocialperspective.JournalofAddictiveDiseases16(4):41-50,1997.
Rawson,R.;Shoptaw,S.J.;Obert,J.L.;McCann,M.J.;Hasson,A.L.;Marinelli-Casey,P.J.;Brethen,P.R.;andLing,W.Anintensiveoutpatientapproachforcocaineabuse:TheMatrixmodel.JournalofSubstanceAbuseTreatment12(2):117-127,1995.
Rawson,R.A.;Huber,A.;McCann,M.;Shoptaw,S.;Farabee,D.;Reiber,C.;andLing,W.Acomparisonofcontingencymanagementandcognitive-behavioralapproachesduringmethadonemaintenancetreatmentforcocainedependence.ArchivesofGeneralPsychiatry59(9):817-824,2002.
12-StepFacilitationTherapy(Alcohol,Stimulants,Opiates)
Twelve-stepfacilitationtherapyisanactiveengagementstrategydesignedtoincreasethelikelihoodofasubstanceabuserbecomingaffiliatedwithandactivelyinvolvedin12-stepself-helpgroups,therebypromotingabstinence.Threekeyideaspredominate:(1)acceptance,whichincludestherealizationthatdrugaddictionisachronic,progressivediseaseoverwhichonehasnocontrol,thatlifehasbecomeunmanageablebecauseofdrugs,thatwillpoweraloneisinsufficienttoovercometheproblem,andthatabstinenceistheonlyalternative;(2)surrender,whichinvolvesgivingoneselfovertoahigherpower,acceptingthefellowshipandsupportstructureofotherrecoveringaddictedindividuals,andfollowingtherecoveryactivitieslaidoutbythe12-stepprogram;and(3)activeinvolvementin12-stepmeetingsandrelatedactivities.Whiletheefficacyof12-stepprograms(and12-stepfacilitation)intreatingalcoholdependencehasbeenestablished,theresearchonitsusefulnessforotherformsofsubstanceabuseismorepreliminary,butthetreatmentappears

52
promisingforhelpingdrugabuserssustainrecovery.
FurtherReading:
Carroll,K.M.;Nich,C.;Ball,S.A.;McCance,E.;Frankforter,T.L.;andRounsaville,B.J.One-yearfollow-upofdisulfiramandpsychotherapyforcocaine-alcoholusers:Sustainedeffectsoftreatment.Addiction95(9):1335-1349,2000.
DonovanD.M.,andWellsE.A."Tweaking12-step":Thepotentialroleof12-Stepself-helpgroupinvolvementinmethamphetaminerecovery.Addiction102(Suppl.1):121-129,2007.
ProjectMATCHResearchGroup.Matchingalcoholismtreatmentstoclientheterogeneity:ProjectMATCHposttreatmentdrinkingoutcomes.JournalofStudiesonAlcohol58(1)7-29,1997.
FamilyBehaviorTherapy
FamilyBehaviorTherapy(FBT),whichhasdemonstratedpositiveresultsinbothadultsandadolescents,isaimedataddressingnotonlysubstanceuseproblemsbutotherco-occurringproblemsaswell,suchasconductdisorders,childmistreatment,depression,familyconflict,andunemployment.FBTcombinesbehavioralcontractingwithcontingencymanagement.
FBTinvolvesthepatientalongwithatleastonesignificantothersuchasacohabitingpartneroraparent(inthecaseofadolescents).Therapistsseektoengagefamiliesinapplyingthebehavioralstrategiestaughtinsessionsandinacquiringnewskillstoimprovethehomeenvironment.PatientsareencouragedtodevelopbehavioralgoalsforpreventingsubstanceuseandHIVinfection,whichareanchoredtoacontingencymanagementsystem.Substance-abusingparentsarepromptedtosetgoalsrelatedtoeffectiveparentingbehaviors.Duringeachsession,thebehavioralgoalsarereviewed,withrewardsprovidedbysignificantotherswhengoalsareaccomplished.Patientsparticipateintreatmentplanning,choosingspecificinterventionsfromamenuofevidence-

53
basedtreatmentoptions.Inaseriesofcomparisonsinvolvingadolescentswithandwithoutconductdisorder,FBTwasfoundtobemoreeffectivethansupportivecounseling.
FurtherReading:
Azrin,N.H.;Donohue,B.;Besalel,V.A.;Kogan,E.S.;andAcierno,R.Youthdrugabusetreatment:acontrolledoutcomestudy.JournalofChildandAdolescentSubstanceAbuse3:1–16,1994.
Carroll,K.M.;andOnken,L.S.Behavioraltherapiesfordrugabuse.AmericanJournalofPsychiatry168(8):1452–1460,2005.
Donohue,B.;Azrin,N.;Allen,D.N.;Romero,V.;Hill,H.H.;Tracy,K.;Lapota,H.;Gorney,S.;Abdel-al,R.;Caldas,D.;Herdzik,K.;Bradshaw,K.;Valdez,R.;andVanHasselt,V.B.FamilyBehaviorTherapyforsubstanceabuse:Areviewofitsinterventioncomponentsandapplicability.BehaviorModification33:495–519,2009.
LaPota,H.B.;Donohue,B.;Warren,C.S.;andAllen,D.N.IntegrationofaHealthyLivingcurriculumwithinFamilyBehaviorTherapy:Aclinicalcaseexampleinawomanwithahistoryofdomesticviolence,childneglect,drugabuse,andobesity.JournalofFamilyViolence26:227–234,2011.
BehavioralTherapiesPrimarilyforAdolescents
Drug-abusingandaddictedadolescentshaveuniquetreatmentneeds.Researchhasshownthattreatmentsdesignedforandtestedinadultpopulationsoftenneedtobemodifiedtobeeffectiveinadolescents.Familyinvolvementisaparticularlyimportantcomponentforinterventionstargetingyouth.Belowareexamplesofbehavioralinterventionsthatemploytheseprinciplesandhaveshownefficacyfortreatingaddictioninyouth.
MultisystemicTherapy

54
MultisystemicTherapy(MST)addressesthefactorsassociatedwithseriousantisocialbehaviorinchildrenandadolescentswhoabusealcoholandotherdrugs.Thesefactorsincludecharacteristicsofthechildoradolescent(e.g.,favorableattitudestowarddruguse),thefamily(poordiscipline,familyconflict,parentaldrugabuse),peers(positiveattitudestowarddruguse),school(dropout,poorperformance),andneighborhood(criminalsubculture).Byparticipatinginintensivetreatmentinnaturalenvironments(homes,schools,andneighborhoodsettings),mostyouthsandfamiliescompleteafullcourseoftreatment.MSTsignificantlyreducesadolescentdruguseduringtreatmentandforatleast6monthsaftertreatment.Fewerincarcerationsandout-of-homejuvenileplacementsoffsetthecostofprovidingthisintensiveserviceandmaintainingtheclinicians’lowcaseloads.
FurtherReading:
Henggeler,S.W.;Clingempeel,W.G.;Brondino,M.J.;andPickrel,S.G.Four-yearfollow-upofmultisystemictherapywithsubstance-abusingandsubstance-dependentjuvenileoffenders.JournaloftheAmericanAcademyofChildandAdolescentPsychiatry41(7):868-874,2002.
Henggeler,S.W.;Rowland,M.D.;Randall,J.;Ward,D.M.;Pickrel,S.G.;Cunningham,P.B.;Miller,S.L.;Edwards,J.;Zealberg,J.J.;Hand,L.D.;andSantos,A.B.Home-basedmultisystemictherapyasanalternativetothehospitalizationofyouthsinpsychiatriccrisis:Clinicaloutcomes.JournaloftheAmericanAcademyofChildandAdolescentPsychiatry38(11):1331-1339,1999.
Henggeler,S.W.;Halliday-Boykins,C.A.;Cunningham,P.B.;Randall,J.;Shapiro,S.B.;andChapman,J.E.Juveniledrugcourt:Enhancingoutcomesbyintegratingevidence-basedtreatments.JournalofConsultingandClinicalPsychology74(1):42–54,2006.
Henggeler,S.W.;Pickrel,S.G.;Brondino,M.J.;andCrouch,J.L.Eliminating(almost)treatmentdropoutofsubstance-abusingordependentdelinquentsthroughhome-basedmultisystemictherapy.TheAmericanJournalofPsychiatry153(3):427–428,1996.

55
Huey,S.J.;Henggeler,S.W.;Brondino,M.J.;andPickrel,S.G.Mechanismsofchangeinmultisystemictherapy:Reducingdelinquentbehaviorthroughtherapistadherenceandimprovedfamilyfunctioning.JournalofConsultingandClinicalPsychology68(3):451–467,2000.
MultidimensionalFamilyTherapy
MultidimensionalFamilyTherapy(MDFT)foradolescentsisanoutpatient,family-basedtreatmentforteenagerswhoabusealcoholorotherdrugs.MDFTviewsadolescentdruguseintermsofanetworkofinfluences(individual,family,peer,community)andsuggeststhatreducingunwantedbehaviorandincreasingdesirablebehavioroccurinmultiplewaysindifferentsettings.Treatmentincludesindividualandfamilysessionsheldintheclinic,inthehome,orwithfamilymembersatthefamilycourt,school,orothercommunitylocations.
Duringindividualsessions,thetherapistandadolescentworkonimportantdevelopmentaltasks,suchasdevelopingdecision-making,negotiation,andproblem-solvingskills.Teenagersacquirevocationalskillsandskillsincommunicatingtheirthoughtsandfeelingstodealbetterwithlifestressors.Parallelsessionsareheldwithfamilymembers.Parentsexaminetheirparticularparentingstyles,learningtodistinguishinfluencefromcontrolandtohaveapositiveanddevelopmentallyappropriateinfluenceontheirchildren.
FurtherReading:
Dennis,M.;Godley,S.H.;Diamond,G.;Tims,F.M.;Babor,T.;Donaldson,J.;Liddle,H.;Titus,J.C.;Kaminer,Y.;Webb,C.;Hamilton,N.;andFunk,R.TheCannabisYouthTreatment(CYT)Study:Mainfindingsfromtworandomizedclinicaltrials.JournalofSubstanceAbuseTreatment27(3):197-213,2004.
Liddle,H.A.;Dakof,G.A.;Parker,K.;Diamond,G.S.;Barrett,K;,andTejeda,M.Multidimensionalfamilytherapyforadolescentdrugabuse:Resultsofarandomizedclinicaltrial.TheAmericanJournalofDrugandAlcoholAbuse27(4):651-688,2001.

56
Liddle,H.A.,andHogue,A.Multidimensionalfamilytherapyforadolescentsubstanceabuse.InE.F.WagnerandH.B.Waldron(eds.),InnovationsinAdolescentSubstanceAbuseInterventions.London:Pergamon/ElsevierScience,pp.227-261,2001.
Liddle,H.A.;Rowe,C.L.;Dakof,G.A.;Ungaro,R.A.;andHenderson,C.E.Earlyinterventionforadolescentsubstanceabuse:Pretreatmenttoposttreatmentoutcomesofarandomizedclinicaltrialcomparingmultidimensionalfamilytherapyandpeergrouptreatment.JournalofPsychoactiveDrugs36(1):49-63,2004.
Schmidt,S.E.;Liddle,H.A.;andDakof,G.A.Effectsofmultidimensionalfamilytherapy:Relationshipofchangesinparentingpracticestosymptomreductioninadolescentsubstanceabuse.JournalofFamilyPsychology10(1):1-16,1996.
BriefStrategicFamilyTherapy
BriefStrategicFamilyTherapy(BSFT)targetsfamilyinteractionsthatarethoughttomaintainorexacerbateadolescentdrugabuseandotherco-occurringproblembehaviors.Suchproblembehaviorsincludeconductproblemsathomeandatschool,oppositionalbehavior,delinquency,associatingwithantisocialpeers,aggressiveandviolentbehavior,andriskysexualbehavior.BSFTisbasedonafamilysystemsapproachtotreatment,inwhichfamilymembers’behaviorsareassumedtobeinterdependentsuchthatthesymptomsofonemember(thedrug-abusingadolescent,forexample)areindicative,atleastinpart,ofwhatelseisoccurringinthefamilysystem.TheroleoftheBSFTcounseloristoidentifythepatternsoffamilyinteractionthatareassociatedwiththeadolescent’sbehaviorproblemsandtoassistinchangingthoseproblem-maintainingfamilypatterns.BSFTismeanttobeaflexibleapproachthatcanbeadaptedtoabroadrangeoffamilysituationsinvarioussettings(mentalhealthclinics,drugabusetreatmentprograms,othersocialservicesettings,andfamilies’homes)andinvarioustreatmentmodalities(asaprimaryoutpatientintervention,incombinationwithresidentialordaytreatment,andasanaftercare/continuing-careservicefollowingresidentialtreatment).
FurtherReading:

57
Coatsworth,J.D.;Santisteban,D.A.;McBride,C.K.;andSzapocznik,J.BriefStrategicFamilyTherapyversuscommunitycontrol:Engagement,retention,andanexplorationofthemoderatingroleofadolescentseverity.FamilyProcess40(3):313-332,2001.
Kurtines,W.M.;Murray,E.J.;andLaperriere,A.Efficacyofinterventionforengagingyouthandfamiliesintotreatmentandsomevariablesthatmaycontributetodifferentialeffectiveness.JournalofFamilyPsychology10(1):35–44,1996.
Santisteban,D.A.;Coatsworth,J.D.;Perez-Vidal,A.;Mitrani,V.;Jean-Gilles,M.;andSzapocznik,J.BriefStructural/StrategicFamilyTherapywithAfrican-AmericanandHispanichigh-riskyouth.JournalofCommunityPsychology25(5):453-471,1997.
Santisteban,D.A.;Suarez-Morales,L.;Robbins,M.S.;andSzapocznik,J.Briefstrategicfamilytherapy:Lessonslearnedinefficacyresearchandchallengestoblendingresearchandpractice.FamilyProcess45(2):259-271,2006.
Santisteban,D.A.;Szapocznik,J.;Perez-Vidal,A.;Mitrani,V.;Jean-Gilles,M.;andSzapocznik,J.BriefStructural/StrategicFamilyTherapywithAfrican-AmericanandHispanichigh-riskyouth.JournalofCommunityPsychology25(5):453–471,1997.
Szapocznik,J.,etal.Engagingadolescentdrugabusersandtheirfamiliesintreatment:Astrategicstructuralsystemsapproach.JournalofConsultingandClinicalPsychology56(4):552-557,1988.
FunctionalFamilyTherapy
FunctionalFamilyTherapy(FFT)isanothertreatmentbasedonafamilysystemsapproach,inwhichanadolescent’sbehaviorproblemsareseenasbeingcreatedormaintainedbyafamily’sdysfunctionalinteractionpatterns.FFTaimstoreduceproblembehaviorsbyimprovingcommunication,problem-solving,conflictresolution,andparentingskills.Theinterventionalways

58
includestheadolescentandatleastonefamilymemberineachsession.Principaltreatmenttacticsinclude(1)engagingfamiliesinthetreatmentprocessandenhancingtheirmotivationforchangeand(2)bringingaboutchangesinfamilymembers’behaviorusingcontingencymanagementtechniques,communicationandproblem-solving,behavioralcontracts,andotherbehavioralinterventions.
FurtherReading:
Waldron,H.B.;Slesnick,N.;Brody,J.L.;Turner,C.W.;andPeterson,T.R.Treatmentoutcomesforadolescentsubstanceabuseat4-and7-monthassessments.JournalofConsultingandClinicalPsychology69:802–813,2001.
Waldron,H.B.;Turner,C.W.;andOzechowski,T.J.Profilesofdrugusebehaviorchangeforadolescentsintreatment.AddictiveBehaviors30:1775–1796,2005.
AdolescentCommunityReinforcementApproachandAssertiveContinuingCare
TheAdolescentCommunityReinforcementApproach(A-CRA)isanothercomprehensivesubstanceabusetreatmentinterventionthatinvolvestheadolescentandhisorherfamily.Itseekstosupporttheindividual’srecoverybyincreasingfamily,social,andeducational/vocationalreinforcers.Afterassessingtheadolescent’sneedsandlevelsoffunctioning,thetherapistchoosesfromamong17A-CRAprocedurestoaddressproblem-solving,coping,andcommunicationskillsandtoencourageactiveparticipationinpositivesocialandrecreationalactivities.A-CRAskillstraininginvolvesrole-playingandbehavioralrehearsal.
AssertiveContinuingCare(ACC)isahome-basedcontinuing-careapproachtopreventingrelapse.Weeklyhomevisitstakeplaceovera12-to14-weekperiodafteranadolescentisdischargedfromresidential,intensiveoutpatient,orregularoutpatienttreatment.Usingpositiveandnegativereinforcementtoshapebehaviors,alongwithtraininginproblem-solvingandcommunication
59
skills,ACCcombinesA-CRAandassertivecasemanagementservices(e.g.,useofamultidisciplinaryteamofprofessionals,round-the-clockcoverage,assertiveoutreach)tohelpadolescentsandtheircaregiversacquiretheskillstoengageinpositivesocialactivities.
FurtherReading:
Dennis,M.;Godley,S.H.;Diamond,G.;Tims,F.M.;Babor,T.;Donaldson,J.;Liddle,H.;Titus,J.C.;Kamier,Y.;Webb,C.;Hamilton,N.;andFunkR.TheCannabisYouthTreatment(CYT)Study:Mainfindingsfromtworandomizedtrials.JournalofSubstanceAbuseTreatment27:197–213,2004.
Godley,S.H.;Garner,B.R.;Passetti,L.L.;Funk,R.R.;Dennis,M.L.;andGodley,M.D.Adolescentoutpatienttreatmentandcontinuingcare:Mainfindingsfromarandomizedclinicaltrial.DrugandAlcoholDependenceJul1;110(1-2):44–54,2010.
Godley,M.D.;Godley,S.H.;Dennis,M.L.;Funk,R.;andPassetti,L.L.Preliminaryoutcomesfromtheassertivecontinuingcareexperimentforadolescentsdischargedfromresidentialtreatment.JournalofSubstanceAbuseTreatment23:21–32,2002.

60
Resources
NationalAgencies
TheNationalInstituteonDrugAbuse(NIDA)leadstheNationinscientificresearchonthehealthaspectsofdrugabuseandaddiction.Itsupportsandconductsresearchacrossabroadrangeofdisciplines,includinggenetics,functionalneuroimaging,socialneuroscience,prevention,medicationandbehavioraltherapies,andhealthservices.Itthendisseminatestheresultsofthatresearchtosignificantlyimprovepreventionandtreatmentandtoinformpolicyasitrelatestodrugabuseandaddiction.Additionalinformationisavailableatdrugabuse.govorbycalling301-443-1124.
NationalInstituteonAlcoholAbuseandAlcoholism(NIAAA)
TheNationalInstituteonAlcoholAbuseandAlcoholism(NIAAA)providesleadershipinthenationalefforttoreducealcohol-relatedproblemsbyconductingandsupportingresearchinawiderangeofscientificareas,includinggenetics,neuroscience,epidemiology,healthrisksandbenefitsofalcoholconsumption,prevention,andtreatment;coordinatingandcollaboratingwithotherresearchinstitutesandFederalprogramsonalcohol-relatedissues;collaboratingwithinternational,national,State,andlocalinstitutions,organizations,agencies,andprogramsengagedinalcohol-relatedwork;andtranslatinganddisseminatingresearchfindingstohealthcareproviders,researchers,policymakers,andthepublic.Additionalinformationisavailableatwww.niaaa.nih.govorbycalling301-443-3860.
NationalInstituteofMentalHealth(NIMH)
ThemissionofNationalInstituteofMentalHealth(NIMH)istotransformtheunderstandingandtreatmentofmentalillnessesthroughbasicandclinicalresearch,pavingthewayforprevention,recovery,andcure.Insupportofthismission,NIMHgeneratesresearchandpromotesresearchtrainingtofulfillthefollowingfourobjectives:(1)promotediscoveryinthebrainandbehavioralsciencestofuelresearchonthecausesofmentaldisorders;(2)chartmental

61
illnesstrajectoriestodeterminewhen,where,andhowtointervene;(3)developnewandbetterinterventionsthatincorporatethediverseneedsandcircumstancesofpeoplewithmentalillnesses;and(4)strengthenthepublichealthimpactofNIMH-supportedresearch.Additionalinformationisavailableatnimh.nih.govorbycalling301-443-4513.
CenterforSubstanceAbuseTreatment(CSAT)
TheCenterforSubstanceAbuseTreatment(CSAT),apartoftheSubstanceAbuseandMentalHealthServicesAdministration(SAMHSA),isresponsibleforsupportingtreatmentservicesthroughablockgrantprogram,aswellasdisseminatingfindingstothefieldandpromotingtheiradoption.CSATalsooperatesthe24-hourNationalTreatmentReferralHotline(1-800-662-HELP),whichoffersinformationandreferralservicestopeopleseekingtreatmentprogramsandotherassistance.CSATpublicationsareavailablethroughSAMHSA'sStore(store.samhsa.gov).AdditionalinformationaboutCSATcanbefoundonSAMHSA'sWebsiteatwww.samhsa.gov/about-us/who-we-are/offices-centers/csat.
SelectedNIDAEducationalResourcesonDrugAddictionTreatment
ThefollowingareavailablefromtheNIDADrugPubsResearchDisseminationCenter,theNationalTechnicalInformationService(NTIS),ortheGovernmentPrintingOffice(GPO).Toorder,refertotheDrugPubs(877-NIDANIH[643-2644]),NTIS(1-800-553-6847),orGPO(202-512-1800)numberprovidedwiththeresourcedescription.
Blendingproducts.NIDA'sBlendingInitiative—ajointventurewithSAMHSAanditsnationwidenetworkofAddictionTechnologyTransferCenters(ATTCs)—uses"BlendingTeams"ofcommunitypractitioners,SAMHSAtrainers,andNIDAresearcherstocreateproductsanddevisestrategicdisseminationplansforthem.CompletedproductsincludethosethataddressthevalueofbuprenorphinetherapyandonsiterapidHIVtestingincommunitytreatmentprograms;strategiesfortreatingprescriptionopioiddependence;andtheneedtoenhancehealthcareworkers'proficiencyinusingtoolssuchastheAddiction

62
SeverityIndex(ASI),motivationalinterviewing,andmotivationalincentives.FormoreinformationonBlendingproducts,pleasevisitNIDA'sWebsiteatdrugabuse.gov/blending-initiative.
AddictionSeverityIndex.Providesastructuredclinicalinterviewdesignedtocollectinformationaboutsubstanceuseandfunctioninginlifeareasfromadultclientsseekingdrugabusetreatment.FormoreinformationonusingtheASIandtoobtaincopiesofthemostrecentedition,pleasevisittriweb.tresearch.org/index.php/tools/download-asiinstruments-manuals/.
Drugs,Brains,andBehavior:TheScienceofAddiction(Reprinted2010).Thispublicationprovidesanoverviewofthesciencebehindthediseaseofaddiction.Publication#NIH10-5605.Availableonlineatdrugabuse.gov/publications/science-addiction.
SeekingDrugAbuseTreatment:KnowWhatToAsk(2011).Thislay-friendlypublicationoffersguidanceinseekingdrugabusetreatmentandlistsfivequestionstoaskwhensearchingforatreatmentprogram.NIDAPublication#12-7764.Availableonlineatdrugabuse.gov/publications/seeking-drug-abuse-treatment.
PrinciplesofDrugAbuseTreatmentforCriminalJusticePopulations:AResearch-BasedGuide(Revised2012).Provides13essentialtreatmentprinciplesandincludesresourceinformationandanswerstofrequentlyaskedquestions.NIHPublicationNo.:11-5316.Availableonlineatdrugabuse.gov/publications/principles-drug-abuse-treatment-criminal-justice-populations-research-based-guide.
NIDADrugFacts:TreatmentApproachesforDrugAddiction(Revised2009).Thisisafactsheetcoveringresearchfindingsoneffectivetreatmentapproachesfordrugabuseandaddiction.Availableonlineatdrugabuse.gov/publications/drugfacts/treatment-approaches-drugaddiction.
AlcoholAlert(publishedbyNIAAA).Thisisaquarterlybulletinthatdisseminatesimportantresearchfindingsonalcoholabuseandalcoholism.Availableonlineatwww.niaaa.nih.gov/publications/journals-and-

63
reports/alcohol-alert.
HelpingPatientsWhoDrinkTooMuch:AClinicians'sguide(publishedbyNIAAA).Thisbookletiswrittenforprimarycareandmentalhealthcliniciansandprovidesguidanceinscreeningandmanagingalcohol-dependentpatients.Availableonlineatpubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/clinicians_guide.htm.
ResearchReportSeries:TherapeuticCommunity(2002).Thisreportprovidesinformationontheroleofresidentialdrug-freesettingsandtheirroleinthetreatmentprocess.NIHPublication#02-4877.Availableonlineatdrugabuse.gov/publications/research-reports/therapeutic-community.
InitiativesDesignedtoMoveTreatmentResearchintoPractice
ClinicalTrialsNetwork
Assessingthereal-worldeffectivenessofevidence-basedtreatmentsisacrucialstepinbringingresearchtopractice.Establishedin1999,NIDA’sNationalDrugAbuseTreatmentClinicalTrialsNetwork(CTN)usescommunitysettingswithdiversepatientpopulationsandconditionstoadjustandtestprotocolstomeetthepracticalneedsofaddictiontreatment.Sinceitsinception,theCTNhastestedpharmacologicalandbehavioralinterventionsfordrugabuseandaddiction,alongwithcommonco-occurringconditions(e.g.,HIVandPTSD)amongvarioustargetpopulations,includingadolescentdrugabusers,pregnantdrug-abusingwomen,andSpanish-speakingpatients.TheCTNhasalsotestedpreventionstrategiesindrug-abusinggroupsathighriskforHCVandHIVandhasbecomeakeyelementofNIDA’smultiprongedapproachtomovepromisingscience-baseddrugaddictiontreatmentsrapidlyintocommunitysettings.FormoreinformationontheCTN,pleasevisitdrugabuse.gov/CTN.
CriminalJustice-DrugAbuseTreatmentStudies
NIDAistakinganapproachsimilartotheCTNtoenhancetreatmentfordrug-
64
addictedindividualsinvolvedwiththecriminaljusticesystemthroughCriminalJustice–DrugAbuseTreatmentStudies(CJ-DATS).WhereasNIDA’sCTNhasasitsoverridingmissiontheimprovementofthequalityofdrugabusetreatmentbymovinginnovativeapproachesintothelargercommunity,researchsupportedthroughCJ-DATSisdesignedtoeffectchangebybringingnewtreatmentmodelsintothecriminaljusticesystemandtherebyimproveoutcomesforoffenderswithsubstanceusedisorders.ItseekstoachievebetterintegrationofdrugabusetreatmentwithotherpublichealthandpublicsafetyforumsandrepresentsacollaborationamongNIDA;SAMHSA;theCentersforDiseaseControlandPrevention(CDC);DepartmentofJusticeagencies;andahostofdrugtreatment,criminaljustice,andhealthandsocialserviceprofessionals.
BlendingTeams
AnotherwayinwhichNIDAisseekingtoactivelymovescienceintopracticeisthroughajointventurewithSAMHSAanditsnationwidenetworkofAddictionTechnologyTransferCenters(ATTCs).Thisprocessinvolvesthecollaborativeeffortsofcommunitytreatmentpractitioners,SAMHSAtrainers,andNIDAresearchers,someofwhomform"BlendingTeams"tocreateproductsanddevisestrategicdisseminationplansforthem.Throughthecreationofproductsdesignedtofosteradoptionofnewtreatmentstrategies,BlendingTeamsareinstrumentalingettingthelatestevidence-basedtoolsandpracticesintothehandsoftreatmentprofessionals.Todate,anumberofproductshavebeencompleted.Topicshaveincludedincreasingawarenessofthevalueofbuprenorphinetherapyandenhancinghealthcareworkers'proficiencyinusingtoolssuchastheASI,motivationalinterviewing,andmotivationalincentives.FormoreinformationonBlendingproducts,pleasevisitNIDA’sWebsiteatdrugabuse.gov/nidasamhsa-blending-initiative.
OtherFederalResources
NIDADrugPubsResearchDisseminationCenter.NIDApublicationsandtreatmentmaterialsareavailablefromthisinformationsource.StaffprovideassistanceinEnglishandSpanish,andhaveTTY/TDDcapability.Phone:877-NIDA-NIH(877-643-2644);TTY/TDD:240-645-0228;fax:240-645-0227;e-mail:[email protected];Website:drugpubs.drugabuse.gov.

65
TheNationalRegistryofEvidence-BasedProgramsandPractices.ThisdatabaseofinterventionsforthepreventionandtreatmentofmentalandsubstanceusedisordersismaintainedbySAMHSAandcanbeaccessedatnrepp.samhsa.gov.
SAMHSA'sStorehasawiderangeofproducts,includingmanuals,brochures,videos,andotherpublications.Phone:800-487-4889;Website:store.samhsa.gov.
TheNationalInstituteofJustice.AstheresearchagencyoftheDepartmentofJustice,theNationalInstituteofJustice(NIJ)supportsresearch,evaluation,anddemonstrationprogramsrelatingtodrugabuseinthecontextofcrimeandthecriminaljusticesystem.Forinformation,includingawealthofpublications,contacttheNationalCriminalJusticeReferenceServiceat800-851-3420or301-519-5500;orvisitnij.gov.
ClinicalTrials.Formoreinformationonfederallyandprivatelysupportedclinicaltrials,pleasevisitclinicaltrials.gov.
ThispublicationisavailableforyouruseandmaybereproducedinitsentiretywithoutpermissionfromtheNIDA.Citationofthesourceisappreciated,usingthefollowinglanguage:Source:NationalInstituteonDrugAbuse;NationalInstitutesofHealth;U.S.DepartmentofHealthandHumanServices.

66
Acknowledgments
TheNationalInstituteonDrugAbusewishestothankthefollowingindividualsforreviewingthispublication.
MartinW.Adler,Ph.D.TempleUniversitySchoolofMedicine
KathleenBrady,M.D.,Ph.D.MedicalUniversityofSouthCarolina
GregBrigham,Ph.D.Maryhaven,Inc.
KathleenM.Carroll,Ph.D.YaleUniversitySchoolofMedicine
RichardR.Clayton,Ph.D.UniversityofKentucky
LindaB.Cottler,Ph.D.WashingtonUniversitySchoolofMedicine
DavidP.Friedman,Ph.D.WakeForestUniversityBowmanGraySchoolofMedicine
ReeseT.Jones,M.D.UniversityofCaliforniaatSanFrancisco
NancyK.Mello,Ph.D.HarvardMedicalSchool

67
WilliamR.Miller,Ph.D.UniversityofNewMexico
CharlesP.O’Brien,M.D.,Ph.D.UniversityofPennsylvania
JeffreySelzer,M.D.ZuckerHillsideHospital
EricJ.Simon,Ph.D.NewYorkUniversityLangoneMedicalCenter
JoseSzapocznik,Ph.D.UniversityofMiamiMillerSchoolofMedicine
GeorgeWoody,M.D.UniversityofPennsylvania